Best of New Jersey: Readmission Reduction Successes INTERACT Quality Improvement Program Version 3.0
|
|
|
- Annice Jackson
- 10 years ago
- Views:
Transcription
1 Best of New Jersey: Readmission Reduction Successes INTERACT Quality Improvement Program Version 3.0 Loretta Kaes, BSN, RN-B-C, C-AL, LNHA, CALA Director, Quality Improvement & Clinical Services Health Care Association of New Jersey Janet Knoth, BS, RN, CHPN Quality Improvement Specialist Healthcare Quality Strategies, Inc. This material was prepared by Healthcare Quality Strategies, Inc., (HQSI), the Medicare Quality Improvement Organization for New Jersey, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. 10SOW-NJ-C /2013
, the Medicare Quality Improvement Organization for New Jersey, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services.")
2 INTERACT Webinar Series Overview and Communication Tools March 14, 2013 Advance Care Planning Tools April 11, 2013 Quality Improvement Tools June 26, 2013 Best of New Jersey: Readmission Reduction Successes August 21,

3 Housekeeping Materials at qualitynet.webex.com Submit chat questions to All Participants Phone lines have been muted Evaluation poll at the end of the presentation Webinar will be recorded and available on HQSI.org 3

4 Today s Presenters 4

5 INTERACT Quality Improvement Program: A Hospital Perspective Teresa De Peralta, MSN, ANP-BC Transitional Care Coordinator Robert Wood Johnson University Hospital- New Brunswick 5

6 Identifying Partners When RWJUH started its program how did you identify/ select/invite facilities to participate? RWJ TCP started enrolling Jan 2012 May 2012 invited area SARs to dinner meeting to Outline TCP program Set expectations of SARs Communicate what help RWJ can give to SARs Care One East Brunswick charter partner with Care Navigator Model Other preferred partners Bridgeway Care Center Aristacare Genesis 6

7 Engagement How did you engage nursing facilities with INTERACT Quality Improvement Program? Reviewed SAR QI programs to recommend Recommended Care One and Bridgeway for INTERACT National study National INTERACT training Offered to help SARs with INTERACT implementation Follow up meetings in facilities or TCP meetings 7

8 Community Collaboration 8 Current active INTERACT Partners Strategies Care One E. Brunswick Bridgeway Care Center Merwick Care Center Genesis Care Center New implementation Bridgeway Re- start/re-energize / re-focus Is it truly implemented? Provide model for evaluation Statistics Root cause analysis Workflow modification

9 Lessons Learned Barriers RWJ management Legal and risk management requirements RWJ Foundation need to stay prominent for future funding RWJ VNA Staff education focus on problem of readmission Nursing facilities Champions & early adapters Identify facility-specific project owner Effective and efficient implementation Other nursing facilities Lack of corporate QI strategy Need for education re: readmission problem 9

10 Lessons Learned Benefits What have been your lessons learned in collaborating with facilities? There will always be champions and forward thinkers A new program is best partnered with early adaptors What benefits does RWJUH receive? Reduction in readmission for targeted diagnoses Increased collaboration with area NH and PACs What benefits does RWJUH provide the nursing facilities? Subsidized care navigator model through RWJVNA NJ Health Connect 10

11 The Program What aspects of the INTERACT Quality Improvement Program are the most valuable to your hospital? Capabilities checklist Triage caremaps Do you find that your providers are utilizing interact2.net? Both Interact 2 and Interact 3 11

12 Measurements Sample preferred partner data: 2013 Re-hospitalization Rates: GOAL: 3% decline per quarter ending at 20.4% st Qtr 2nd Qtr 3rd Qtr 4th Qtr %All cause %Penalty Penalty GOAL 12

13 Analysis of 2012 and Plan for 2013 Partner 1 overall re-hospitalization rate was comparable to NJ averages, however our re-hospitalization rate for penalty diagnoses was significantly higher. In addition to following patients on our Transitional Care Program, the Care Navigator also evolved into a program development advisor. This resulted in programs such as the Walgreens Program, and a new process for Discharge Medication Reconciliation for Transitional Care Patients. This became a facility-wide model in The Care Navigator is also involved in roll-out of INTERACT 3, CHF, COPD and Palliative Care Programs, partnerships with Cardiology Groups, Staff in-services and Case Studies, NJ Relay, and EMR.

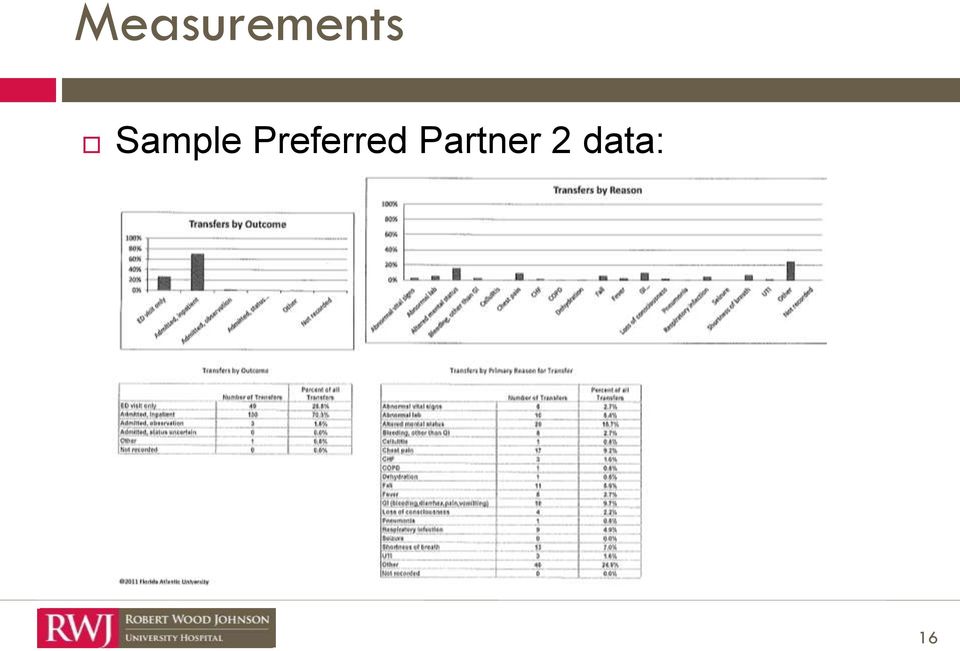
14 Measurements Sample Preferred Partner 2 data: 14
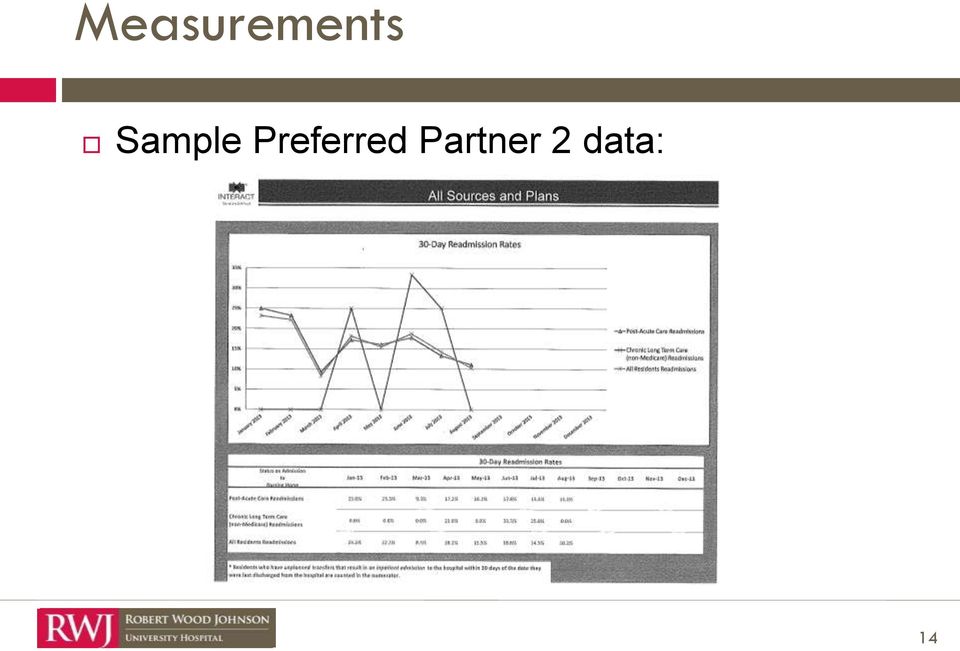
15 Measurements Sample preferred partner data: 15

16 Measurements Sample Preferred Partner 2 data: 16
17 Measurements Qualitative Increased communication and learning from regular TCP meeting attendance Improved data presentation and communication Case studies Root cause analysis skills honed Better follow up and feedback 17

18 RWJ Readmission Data - CMS 18 Metrics Medicare readmission rates for AMI Medicare readmission rates for CHF Medicare readmission rates for PNA Combined (AMI, CHF, PNA) Jan 09 Dec 11 Jan Dec12 (36 mos) (12 mos) % Reduction 23.55% 22.3% 5.3% 27.59% 24% 12.7% 23.74% 19.5% 17.9% 25.5% 22.49% 11.8% Improvement applied over prior 30 months = 107 less AMI, PNA, HF readmissions

19 RWJ Readmission Date - CMS 19 Metrics Jan 09 - Dec 11 Jan Dec 12 % Reduction All Cause Readmission to RWJ All Cause Readmission to Any Hospital 17.3% 16.5% 4.6% 22.87% 21.7% 5.1% Improvement applied over prior 30 months = 280 less readmissions

20 Contact Information Teresa De Peralta, MSN, NP-C Transitional Care Coordinator Robert Wood Johnson University Hospital Phone Numbers: Office: Cell:

21 Questions
22 The Journey of Victoria Manor in Reducing Readmissions Donna Mayer, RN, BSN Director of Nursing Victoria Manor Denise Raymond, CDP, LPN, CSW, NJCALA Senior Admissions and Marketing Director Genesis HealthCare 22
23 Decision Makers Genesis HealthCare presented a global implementation of INTERACT Quality Improvement Program to its facilities Goal: Reduce readmissions to acute care facilities 23
24 Championing Quality Improvement Directors of Nursing Root cause analysis Evaluate where change needs to take place Identify the best tools possible ( Fill your gaps with viable tools Do not duplicate existing forms 24
25 Discovering the INTERACT Quality Improvement Program INTERACT Care Paths have been a part of clinical education Root cause analysis identified reasons for transfer Goals: Catch patient changes in condition sooner Manage patients at facility If transfer needed, send the best report possible 25
26 INTERACT Tools and Staff Education Care Paths Clinical staff Stop and Watch Support staff SBAR Clinical staff Nursing Capabilities list Physician, nurse practitioner, and clinical staff 26
27 INTERACT Tools and Goals Care Paths Consistent clinical protocol Stop and Watch Engage additional staff members SBAR Consistent reporting Track patient condition changes Nursing Home Capabilities List Provide to the hospital ED and primary care physicians Every transfer is not an admission 27
28 Barriers and Successes Barriers Corporate initiatives are sometimes challenged Culture-change Time consuming (initial concern of nurses) Successes New unit managers quickly adapted to new system Improved communication increased ED awareness of Nursing Facilities Capabilities list SBAR improved staff confidence when giving report 28

29 Embedding INTERACT at Victoria Manor Stop and Watch Used by therapy and aides Left on medication cart; decreases interruption during medication pass Passed on to unit manager; actively trends patient SBAR Left in MARS for consistent review and update Report at shift change 29
30 Embedding INTERACT at Victoria Manor continued Nursing Capabilities List Face-to-face meeting with two hospital ED liaisons Include Nursing Capabilities Flyer in transfer envelope INTERACT Transfer Envelope EMT staff expectation of envelope value during transfer Improved relationship with ED staff 30
31 Continuous Quality Improvement Quality Improvement Review Ongoing clinical review of all hospital readmissions Using root cause analysis Including staff involved with transfer Quality Assurance Meetings Quarterly readmission report Ongoing staff input about implementation process of INTERACT Quality Improvement Tools 31
32 Contact Information Donna Mayer, RN Director of Nursing Victoria Manor (609) Denise Raymond, CDP, LPN, CSW, NJCALA Senior Admissions and Marketing Director Genesis Healthcare (609)
33 Polling Question #1 What barriers do you need to remove? Leadership/staff buy-in Lack of physician collaboration and cooperation Families want residents hospitalized Your facility already has similar forms and processes 33
34 Let s Discuss the INTERACT Quality Improvement Program in Assisted Living Communities Interviewer: Loretta Kaes BSN, RN-B-C, C-AL, LNHA, CALA Director, Quality Improvement & Clinical Services Health Care Association of New Jersey Interviewee: Elaine Jeffers RN, LNC, CCM, CDP, C-AL Regional Director of Health Services Chairperson of NJ Assisted Living Nurses Association Chelsea Senior Living 34
35 Discovering INTERACT The assisted living INTERACT Quality Improvement Program is still in the pilot stage. How did you find out about the INTERACT Quality Improvement Program? Who would make the decision to implement INTERACT? 35
36 Implementation Do you think champions/ co-champions would be effective in your setting? How would you implement INTERACT? Would it be by area or system wide? 36
37 The Tools Which INTERACT tools would you use and why? Stop and Watch SBAR Capabilities List Other Have you found interact2.net useful, such as resident education handouts and/or guidance for having end-of-life conversations? 37
38 Advance Care Planning Will you consider using the INTERACT Quality Improvement Program tools to increase awareness of advance care planning? Has your facility incorporated the POLST form in patient education? 38
39 Barriers and Successes Often assisted living communities follow the mantra, When in doubt send them out. What challenges do you anticipate in changing the culture in order to improve transfers and reduce readmissions? 39
40 Measurement Are you measuring resident transfers and readmissions? Have root cause analyses of readmissions been effective for identifying areas that may need reassessment? 40
41 Assisted Living Capabilities Considering that the goal is to keep residents out of the hospital and improve communication between healthcare providers: What services would you include on the assisted living capabilities list? (i.e., stat blood work, Doppler studies, UTI treatment, etc.?) 41
42 INTERACT Quality Improvement Program How do you anticipate that using the INTERACT Quality Program will increase resident satisfaction and quality of life? 42
43 Contact Information Loretta Kaes BSN, RN-B-C, C-AL, LNHA, CALA Director of Quality Improvement & Clinical Services Health Care Association of New Jersey (609) Elaine Jeffers RN, LNC, CCM, CDP, C-AL Regional Director of Health Services Chairperson of NJ Assisted Living Nurses Association Chelsea Senior Living (908)
44 Polling Question #2 What do you see as the biggest value in the INTERACT Quality Improvement Program? Developing a shared vision within your facility Focusing on continuous quality improvement Streamlining work processes and avoiding redundancies Developing cross-continuum partnerships 44
45 Implementing the INTERACT Quality Improvement Program Karen Gentile, RN Director of Nursing/Assistant Administrator Inglemoor Rehabilitation and Care Center 45
46 The Decision Makers Nursing administration was supported by management Looking to be the leader in reducing readmissions from our long-term care/sub-acute facility back to hospital 46
47 Champions 1 nurse and 1 CNA from each of the 4 units (we had to work with staff on changing the culture) 47
48 Discovering INTERACT INTERACT was the buzzword for everyone in the long-term care/sub-acute industry Researched online ( and the information was easy to use Training session at Health Care Association of New Jersey (HCANJ) 48
49 Implementation Implemented with the nurses on all 4 units to emphasize: Early identification through frequent assessments/ reassessments using the INTERACT Care Paths Evaluating, documenting, and communicating changes (with SBAR) in patients assessment Rolled out the Stop and Watch with aides, dietary, and housekeeping staff
50 The Tools Stop and Watch SBAR Nursing Home Capabilities List Interact2.net Struggled a little because the CNAs were not completing the form, although they were communicating the information Utilizing the SBAR for over 8 months. It has increased communication and nurses credibility Use of SBAR allows nurses to capture and communicate critical information Share capability list with hospitals to update them on services offered A wealth of information and resources to help roll out the program

51 Advance Care Planning POLST education for patients is the focus for our social workers, physicians, and nurses
52 Barriers and Successes Barriers Biggest barrier is CHANGE; staff education is ongoing Nurses had to realize that they were capable of caring for more acute patient conditions Mindset had to be changed: sending a patient out to the emergency room is better Successes Staff is better trained to handle more acute patients Patient changes assessed more consistently Increased communication across the board Decreased readmissions Better patient outcomes
53 Measurements Tracking transfers (planned/unplanned) and acute care readmissions Continuing to see a decrease in readmissions, as well as improving patient outcomes Conducting root cause analysis helps nurses to see a transfer through fresh eyes, such as: Assessment was not as complete as it could have been Information could have been better communicated Covering physician was not fully informed and chose to inappropriately send a patient to the emergency room
54 Success/Patient Story Prior to INTERACT implementation, cardiac patients (with diagnosis of CHF, COPD) would bounce back and forth between the hospital and our facility Empowered staff (with physician support) to better assess and recognize changes INTERACT Care Paths and Acute Change in Condition File Cards have significantly reduced the number of patients readmitted to the hospital Symptom management has improved our patients satisfaction
55 Contact Information Karen Gentile, RN Director of Nursing/Assistant Administrator Inglemoor Rehabilitation and Care Center (973) , ext
56 Questions?
57 Contact us Loretta J. Kaes, BSN, RN-B-C, C-AL, LNHA, CALA Director, Quality Improvement & Clinical Services Health Care Association of New Jersey (609) Janet Knoth, BS, RN, CHPN Quality Improvement Specialist Healthcare Quality Strategies, Inc. (732) , ext
Development and Implementation of a Universal Transfer Form The New Jersey Journey Toward Improved Transitions
 Development and Implementation of a Universal Transfer Form The New Jersey Journey Toward Improved Transitions Healthcare Quality Strategies, Inc. 557 Cranbury Road Suite 21 East Brunswick, NJ 08816-5419
Development and Implementation of a Universal Transfer Form The New Jersey Journey Toward Improved Transitions Healthcare Quality Strategies, Inc. 557 Cranbury Road Suite 21 East Brunswick, NJ 08816-5419
The Best of New Jersey: Care Transitions Communities
 The Best of New Jersey: Care Transitions Communities June 25, 2014 H e a l t h c a r e Q u a l i t y S t r a t e g i e s, I n c. 557 Cranbury Road Suite 21 East Brunswick, NJ 08816-5419 Phone: 732-238-5570
The Best of New Jersey: Care Transitions Communities June 25, 2014 H e a l t h c a r e Q u a l i t y S t r a t e g i e s, I n c. 557 Cranbury Road Suite 21 East Brunswick, NJ 08816-5419 Phone: 732-238-5570
Ann Hablitzel, RN, BSN, MBA Hospice Care of California
 Ann Hablitzel, RN, BSN, MBA Hospice Care of California Objectives Describe the creations of new community based palliative care programs Identify criteria for admission Discuss philosophy and goals Analyze
Ann Hablitzel, RN, BSN, MBA Hospice Care of California Objectives Describe the creations of new community based palliative care programs Identify criteria for admission Discuss philosophy and goals Analyze
Improving Transitions & Reducing Readmissions from Skilled Nursing Facilities. Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies
 Improving Transitions & Reducing Readmissions from Skilled Nursing Facilities Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies Agenda Why this is so important What we know: a review of the
Improving Transitions & Reducing Readmissions from Skilled Nursing Facilities Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies Agenda Why this is so important What we know: a review of the
Readmissions as an Enterprise Priority. Presenters 4/17/2014
 Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center [email protected] Eileen
Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center [email protected] Eileen
Innovations@Home. Home Health Initiatives Reduce Avoidable Readmissions by Leveraging Innovation
 How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
Game Changer at the Primary Care Practice Embedded Care Management. Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012
 Game Changer at the Primary Care Practice Embedded Care Management Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012 Objectives To describe the recent evolution of care management at
Game Changer at the Primary Care Practice Embedded Care Management Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012 Objectives To describe the recent evolution of care management at
How To Embed QAPI In Your Transition Process
 How To Embed QAPI In Your Transition Process Objective 3 Getting Started With Your Care Transitions PIP Sarah Dereniuk, MHA, NHA Program Administrator This material was prepared by Healthcentric Advisors,
How To Embed QAPI In Your Transition Process Objective 3 Getting Started With Your Care Transitions PIP Sarah Dereniuk, MHA, NHA Program Administrator This material was prepared by Healthcentric Advisors,
Kick off Meeting November 11 13, 2015. MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF)
") Kick off Meeting November 11 13, 2015 MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF) Team Composition Justin Huynh, MD Internal Medicine, Physician Champion Mary Laubinger,
Kick off Meeting November 11 13, 2015 MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF) Team Composition Justin Huynh, MD Internal Medicine, Physician Champion Mary Laubinger,
Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services
 Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services Objectives Understand the new consequences to hospitals for discharged clients being re-admitted within selected time
Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services Objectives Understand the new consequences to hospitals for discharged clients being re-admitted within selected time
Early warning of changes in a resident s condition is critical.
 Approximately 60% of senior care residents are sent to emergency rooms and 25% are admitted to hospitals each year. What can senior care providers do to reduce hospital readmissions? Although hospitalizations
Approximately 60% of senior care residents are sent to emergency rooms and 25% are admitted to hospitals each year. What can senior care providers do to reduce hospital readmissions? Although hospitalizations
INTERACT Webinar Series
 INTERACT Webinar Series Session 1: Introduction to the Program February 25, 2015 with presenters: Carol Dietz, RN, MBA Florence Johnson, MSN, MHA Sheila Eckenrode, BSN, MA Today s Session Objectives Welcome
INTERACT Webinar Series Session 1: Introduction to the Program February 25, 2015 with presenters: Carol Dietz, RN, MBA Florence Johnson, MSN, MHA Sheila Eckenrode, BSN, MA Today s Session Objectives Welcome
Using Root Cause Analysis to Determine Why Readmissions are High. Presentation Objectives. Background Information 11/30/2011
 Using Root Cause Analysis to Determine Why Readmissions are High Nancy Seck RBN, BSN, MPH, CPHQ Director, Quality Management Glendale Memorial Hospital and Health Center Presentation Objectives Identify
Using Root Cause Analysis to Determine Why Readmissions are High Nancy Seck RBN, BSN, MPH, CPHQ Director, Quality Management Glendale Memorial Hospital and Health Center Presentation Objectives Identify
Coordinating Transitions of Care: It Takes a Village
 Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
Welcome to the New Jersey DSRIP Learning Collaborative
 Welcome to the New Jersey DSRIP Learning Collaborative October 08, 2015 New Jersey Department of Health (NJDOH) 1 Objectives Review DSRIP Program Updates Improvement Target Goals Chart/ EHR Submission
Welcome to the New Jersey DSRIP Learning Collaborative October 08, 2015 New Jersey Department of Health (NJDOH) 1 Objectives Review DSRIP Program Updates Improvement Target Goals Chart/ EHR Submission
2.b.vii Implementing the INTERACT Project (Inpatient Transfer Avoidance Program for SNF)
") 2.b.vii Implementing the INTERACT Project (Inpatient Transfer Avoidance Program for SNF) Project Objective: Skilled nursing facilities (SNFs) will implement the evidence based INTERACT program developed
2.b.vii Implementing the INTERACT Project (Inpatient Transfer Avoidance Program for SNF) Project Objective: Skilled nursing facilities (SNFs) will implement the evidence based INTERACT program developed
Eastern Massachusetts Pioneer Accountable Care Organization (ACO) Quality Standards COMMON EXPECTATIONS FOR SKILLED NURSING FACILITIES.
 Quality Standards COMMON EXPECTATIONS FOR SKILLED NURSING FACILITIES.") Eastern Massachusetts Pioneer Accountable Care Organization (ACO) Quality Standards COMMON EXPECTATIONS FOR SKILLED NURSING FACILITIES Draft 12-5-12 General: 1. Staffing: a. Low staff turnover rate. b.
Eastern Massachusetts Pioneer Accountable Care Organization (ACO) Quality Standards COMMON EXPECTATIONS FOR SKILLED NURSING FACILITIES Draft 12-5-12 General: 1. Staffing: a. Low staff turnover rate. b.
Nurses: Architects of an Integrated Healthcare Delivery System. Billie Lynn Allard, MS, RN Administrative Director of Outpatient Services
 Nurses: Architects of an Integrated Healthcare Delivery System Billie Lynn Allard, MS, RN Administrative Director of Outpatient Services Presentation ID: 338 1 Disclosure Today s presenters do not have
Nurses: Architects of an Integrated Healthcare Delivery System Billie Lynn Allard, MS, RN Administrative Director of Outpatient Services Presentation ID: 338 1 Disclosure Today s presenters do not have
Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals
 Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals 12/18/2013 12/18/13 2013, American Heart Association 1 Thank you for Joining the Webinar Today. The Presentation will Begin
Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals 12/18/2013 12/18/13 2013, American Heart Association 1 Thank you for Joining the Webinar Today. The Presentation will Begin
Understanding Care Transitions as a Patient Safety Issue
 Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
Reducing Avoidable Readmissions Effectively (RARE) Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement
 Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement") Reducing Avoidable Readmissions Effectively (RARE) Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement Martha and James Acute Episodes Family Doctor Life Expectancy from chronic diseases
Reducing Avoidable Readmissions Effectively (RARE) Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement Martha and James Acute Episodes Family Doctor Life Expectancy from chronic diseases
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates
 Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Care Coordination. The Embedded Care Manager. Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed
 Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
Five Myths Surrounding the Business of Population Health Management
 Five Myths Surrounding the Business of Population Health Management Joan Moss, RN, MSN Robert Sehring Chief Nursing Officer and Chief Ministry Services Officer, Senior Vice President, Sg2 OSF HealthCare
Five Myths Surrounding the Business of Population Health Management Joan Moss, RN, MSN Robert Sehring Chief Nursing Officer and Chief Ministry Services Officer, Senior Vice President, Sg2 OSF HealthCare
Care Coordination at Frederick Regional Health System. Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care
 Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions
 Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions Leslie Becker RN, BS Jennifer Smith RN, MSN, MBA Leslie Frain MSN, RN Jan Machanis
Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions Leslie Becker RN, BS Jennifer Smith RN, MSN, MBA Leslie Frain MSN, RN Jan Machanis
It Takes Two to ACO A Unique Management Partnership
 AMGA 2014 Annual Conference, April 4, 2014 It Takes Two to ACO A Unique Management Partnership Scott Hayworth MD, President & CEO Mount Kisco Medical Group Alan Bernstein MD, Senior Medical Director Mount
AMGA 2014 Annual Conference, April 4, 2014 It Takes Two to ACO A Unique Management Partnership Scott Hayworth MD, President & CEO Mount Kisco Medical Group Alan Bernstein MD, Senior Medical Director Mount
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION
 Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
PREVENTING HEART FAILURE READMISSIONS
 PREVENTING HEART FAILURE READMISSIONS Tanya Sprinkle, BSN, RN, CCM Patient and Family Services Coordinator [email protected] 704-878-4534 Michelle Roseman, NHA, MBA Chief Operating Officer/Catawba
PREVENTING HEART FAILURE READMISSIONS Tanya Sprinkle, BSN, RN, CCM Patient and Family Services Coordinator [email protected] 704-878-4534 Michelle Roseman, NHA, MBA Chief Operating Officer/Catawba
An Introduction to HealthInfoNet s HIE Reporting & Analytics. 6th Annual APS Healthcare Maine Conference May 14, 2015
 An Introduction to HealthInfoNet s HIE Reporting & Analytics 6th Annual APS Healthcare Maine Conference May 14, 2015 Presentation Outline HealthInfoNet Background Current Status of health information exchange
An Introduction to HealthInfoNet s HIE Reporting & Analytics 6th Annual APS Healthcare Maine Conference May 14, 2015 Presentation Outline HealthInfoNet Background Current Status of health information exchange
Capacity Management: Patient Throughput and Case Management Improvement. February 25, 2015
 Capacity Management: Patient Throughput and Case Management Improvement February 25, 2015 Agenda Introduction Impetus for Change Approach to Improving Case and Capacity Management Client Case Study Key
Capacity Management: Patient Throughput and Case Management Improvement February 25, 2015 Agenda Introduction Impetus for Change Approach to Improving Case and Capacity Management Client Case Study Key
Massachusetts Department of Higher Education. Nursing Education Redesign Grant Program. Final Project Implementation Report
 Massachusetts Department of Higher Education Nursing Education Redesign Grant Program Final Project Implementation Report Submitted by: Berkshire Community College November 30, 2012 Executive Summary Overview
Massachusetts Department of Higher Education Nursing Education Redesign Grant Program Final Project Implementation Report Submitted by: Berkshire Community College November 30, 2012 Executive Summary Overview
DELIVERING VALUE THROUGH TECHNOLOGY
 DELIVERING VALUE THROUGH TECHNOLOGY Mark Nelson, MD - EMR Physician Champion Krishna Ramachandran - Chief Information and Transformation Officer Karen Adamson - Director, Epic Clinical Applications DuPage
DELIVERING VALUE THROUGH TECHNOLOGY Mark Nelson, MD - EMR Physician Champion Krishna Ramachandran - Chief Information and Transformation Officer Karen Adamson - Director, Epic Clinical Applications DuPage
Henry Ford Health System Care Coordination and Readmissions Update
 Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
National Clinical Programmes
 National Clinical Programmes Section 3 Background information on the National Clinical Programmes Mission, Vision and Objectives July 2011 V0. 6_ 4 th July, 2011 1 National Clinical Programmes: Mission
National Clinical Programmes Section 3 Background information on the National Clinical Programmes Mission, Vision and Objectives July 2011 V0. 6_ 4 th July, 2011 1 National Clinical Programmes: Mission
UnitedHealthcare Medicare Solutions Readmission Review Program for Medicare Advantage Plans
 UnitedHealthcare Medicare Solutions Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Updated May 2015 Introduction The UnitedHealthcare Medicare Solutions
UnitedHealthcare Medicare Solutions Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Updated May 2015 Introduction The UnitedHealthcare Medicare Solutions
Home Care s Pivotal Role in Patient Transitions from Acute to Post Acute Care Settings:
 Home Care s Pivotal Role in Patient Transitions from Acute to Post Acute Care Settings: Experiences of a Successful CCTP Program And So Much More! Jane Pike-Benton Senior Director, Home Health & Post Acute
Home Care s Pivotal Role in Patient Transitions from Acute to Post Acute Care Settings: Experiences of a Successful CCTP Program And So Much More! Jane Pike-Benton Senior Director, Home Health & Post Acute
1. Executive Summary Problem/Opportunity: Evidence: Baseline Data: Intervention: Results:
 A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
PACCR Webinar Series Presents: The INTERACT Quality Improvement Program Joseph G. Ouslander, M.D.
 paccr.org PACCR Webinar Series Presents: The INTERACT Quality Improvement Program Joseph G. Ouslander, M.D. January 14, 2015 2013 Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior
paccr.org PACCR Webinar Series Presents: The INTERACT Quality Improvement Program Joseph G. Ouslander, M.D. January 14, 2015 2013 Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
Reducing Readmissions with Predictive Analytics
 Reducing Readmissions with Predictive Analytics Conway Regional Health System uses analytics and the LACE Index from Medisolv s RAPID business intelligence software to identify patients poised for early
Reducing Readmissions with Predictive Analytics Conway Regional Health System uses analytics and the LACE Index from Medisolv s RAPID business intelligence software to identify patients poised for early
Connect4 Patients CCCM Primary Care Community. Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM
 Connect4 Patients CCCM Primary Care Community Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM September 17, 2015 Objectives: Describe innovative care management
Connect4 Patients CCCM Primary Care Community Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM September 17, 2015 Objectives: Describe innovative care management
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home
 RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes. FINANCIAL DISCLOSURE: No relevant financial relationship exists
 Cheri Basso BSN, RN-BC, CHFN Mary Washington Healthcare Fredericksburg, VA Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes FINANCIAL DISCLOSURE: No relevant financial relationship
Cheri Basso BSN, RN-BC, CHFN Mary Washington Healthcare Fredericksburg, VA Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes FINANCIAL DISCLOSURE: No relevant financial relationship
If you have any questions, please feel free to contact Vera Frey by phone at 518-462-4800, Ext. 21 or by email at [email protected].
 33 Elk Street, Suite 300 Albany, New York 12207-1010 518-462-4800 Fax: 518-426-4051 www.thefqc.org The Foundation for Quality Care, the research and education affiliate of the New York State Health Facilities
33 Elk Street, Suite 300 Albany, New York 12207-1010 518-462-4800 Fax: 518-426-4051 www.thefqc.org The Foundation for Quality Care, the research and education affiliate of the New York State Health Facilities
Patients Receive Recommended Care for Community-Acquired Pneumonia
 Patients Receive Recommended Care for Community-Acquired Pneumonia For New Jersey to be a state in which all people live long, healthy lives. DSRIP LEARNING COLLABORATIVE PRESENTATION The Care you Trust!
Patients Receive Recommended Care for Community-Acquired Pneumonia For New Jersey to be a state in which all people live long, healthy lives. DSRIP LEARNING COLLABORATIVE PRESENTATION The Care you Trust!
HealthCare Partners of Nevada. Heart Failure
 HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
9/28/2015. Nursing Home Quality Measures - Achieving 5 Stars. Nursing Home Quality Measures Achieving 5 Stars
 Welcome the webinar will begin shortly! Nursing Home Quality Measures - Achieving 5 Stars Audio for this presentation is being broadcast, so if you have not already done so, please enable the sound on
Welcome the webinar will begin shortly! Nursing Home Quality Measures - Achieving 5 Stars Audio for this presentation is being broadcast, so if you have not already done so, please enable the sound on
The Path to Excellence: How One Facility Received and Maintained a CMS 5 Star Rating
 The Path to Excellence: How One Facility Received and Maintained a CMS 5 Star Rating South Mountain Healthcare and Rehabilitation Center 2385 Springfield Avenue Vauxhall, NJ 07088 Author: Antonio Onday,
The Path to Excellence: How One Facility Received and Maintained a CMS 5 Star Rating South Mountain Healthcare and Rehabilitation Center 2385 Springfield Avenue Vauxhall, NJ 07088 Author: Antonio Onday,
Elim Park Health Care Center. Clinical Excellence and Quality Report
 2014 Elim Park Health Care Center Clinical Excellence and Quality Report Welcome to Elim Park Health Care Center s 2014 Clinical Excellence and Quality Report. We have been providing patient focused quality
2014 Elim Park Health Care Center Clinical Excellence and Quality Report Welcome to Elim Park Health Care Center s 2014 Clinical Excellence and Quality Report. We have been providing patient focused quality
The problem of hospital readmissions
 By Jennifer Markley, BSN, RN, Vanessa Andow, BHA, Karen Sabharwal, MPH, Ziyin Wang, PhD, Emilie Fennell, MPA, and Ron Dusek A Project to Reengineer Discharges Reduces 30-Day Readmission Rates A Texas hospital
By Jennifer Markley, BSN, RN, Vanessa Andow, BHA, Karen Sabharwal, MPH, Ziyin Wang, PhD, Emilie Fennell, MPA, and Ron Dusek A Project to Reengineer Discharges Reduces 30-Day Readmission Rates A Texas hospital
Life Choices. What is Palliative Care? Palliative? Palliative care emerged. A Program of Palliative Care
 Life Choices A Program of Palliative Care Relieves suffering and improves quality of life for patients with advanced illnesses What is Palliative Care? Medical treatment that aims to relieve suffering
Life Choices A Program of Palliative Care Relieves suffering and improves quality of life for patients with advanced illnesses What is Palliative Care? Medical treatment that aims to relieve suffering
How To Reduce Hospital Readmission
 Reducing Hospital Readmissions & The Affordable Care Act The Game Has Changed Drastically Reducing MSPB Measures Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE
Reducing Hospital Readmissions & The Affordable Care Act The Game Has Changed Drastically Reducing MSPB Measures Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE
CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes
 CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes Understanding CCM Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare
CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes Understanding CCM Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare
Stroke/VTE Quality Measure Build for Meaningful Use Stage 1
 Stroke/VTE Quality Measure Build for Meaningful Use Stage 1 Presented by Susan Haviland, BSN RN Senior Consult, Santa Rosa Consulting Meaningful Use Quality Measures Centers for Medicare and Medicaid Services
Stroke/VTE Quality Measure Build for Meaningful Use Stage 1 Presented by Susan Haviland, BSN RN Senior Consult, Santa Rosa Consulting Meaningful Use Quality Measures Centers for Medicare and Medicaid Services
Nurses at the Forefront: Care Delivery and Transformation through Health IT
 Nurses at the Forefront: Care Delivery and Transformation through Health IT Ann OBrien RN MSN CPHIMS National Senior Director of Clinical Informatics Kaiser Permanente Robert Wood Johnson Executive Nurse
Nurses at the Forefront: Care Delivery and Transformation through Health IT Ann OBrien RN MSN CPHIMS National Senior Director of Clinical Informatics Kaiser Permanente Robert Wood Johnson Executive Nurse
Adoption and Meaningful Use of EHR Technology in a Hospital
 Monday, March, 00 :5 :5 pm Adoption and Meaningful Use of EHR Technology in a Hospital Sanjay Shah, MBA, CMPE, FHIMSS President, HCIT+ (Former) VP & CIO, Cabell Huntington Hospital Anthony Adkins, RN Director
Monday, March, 00 :5 :5 pm Adoption and Meaningful Use of EHR Technology in a Hospital Sanjay Shah, MBA, CMPE, FHIMSS President, HCIT+ (Former) VP & CIO, Cabell Huntington Hospital Anthony Adkins, RN Director
Hospital readmissions contribute to the increasing. Deployment of Lean Six Sigma in Care Coordination An Improved Discharge Process
 Professional Case Management Vol. 19, No. 2, 77-83 Copyright 2014 Wolters Kluwer Health Lippincott Williams & Wilkins Deployment of Lean Six Sigma in Care Coordination An Improved Discharge Process Susan
Professional Case Management Vol. 19, No. 2, 77-83 Copyright 2014 Wolters Kluwer Health Lippincott Williams & Wilkins Deployment of Lean Six Sigma in Care Coordination An Improved Discharge Process Susan
Transitions of Care Management Coding (TCM Code) Tutorial. 1. Introduction Meaning of moderately and high complexity 2
 Tutorial. 1. Introduction Meaning of moderately and high complexity 2") Transitions of Care Management Coding (TCM Code) Tutorial Index 1. Introduction Meaning of moderately and high complexity 2 2. SETMA s Tools for using TCM Code 3 Alert that patient is eligible for TCM
Transitions of Care Management Coding (TCM Code) Tutorial Index 1. Introduction Meaning of moderately and high complexity 2 2. SETMA s Tools for using TCM Code 3 Alert that patient is eligible for TCM
A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates. April 11, 2014
 A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates April 11, 2014 About the QIO Program Leading rapid, large-scale change in health quality: Goals are bolder. The patient is at
A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates April 11, 2014 About the QIO Program Leading rapid, large-scale change in health quality: Goals are bolder. The patient is at
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment
 Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
Pamela Tropiano, RN, CCM, BSN, MPA. CareSource
 Annual Education Conference September 30 October 3, 2012 Orlando, FL 1.7 Creative Case Management Pamela Tropiano, RN, CCM, BSN, MPA Senior Vice President, Health hservices CareSource Mission: The CareSource
Annual Education Conference September 30 October 3, 2012 Orlando, FL 1.7 Creative Case Management Pamela Tropiano, RN, CCM, BSN, MPA Senior Vice President, Health hservices CareSource Mission: The CareSource
Patient to Person. Transitions of Care. Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM
 Patient to Person Transitions of Care Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM Transitions of Care Transitioning from school to adult services (vocational, medical day, etc.)
Patient to Person Transitions of Care Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM Transitions of Care Transitioning from school to adult services (vocational, medical day, etc.)
Clinical Impact of An Inpatient Diabetes Care Model. Objectives
 Clinical Impact of An Inpatient Diabetes Care Model Beth Pfeffer MSN, RN CDE June 4, 2014 Objectives 1. Examine the development of the role of the diabetes case manager model in the inpatient setting 2.
Clinical Impact of An Inpatient Diabetes Care Model Beth Pfeffer MSN, RN CDE June 4, 2014 Objectives 1. Examine the development of the role of the diabetes case manager model in the inpatient setting 2.
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/31/2015
 Narrative for Health Care Organizations in Ontario 3/31/2015") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/31/2015 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/31/2015 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
May 7, 2012. Submitted Electronically
 May 7, 2012 Submitted Electronically Secretary Kathleen Sebelius Department of Health and Human Services Office of the National Coordinator for Health Information Technology Attention: 2014 edition EHR
May 7, 2012 Submitted Electronically Secretary Kathleen Sebelius Department of Health and Human Services Office of the National Coordinator for Health Information Technology Attention: 2014 edition EHR
3/11/15. COPD Disease Management Tackling the Transition. Objectives. Describe the multidisciplinary approach to inpatient care for COPD patients
 Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
Z Take this folder with you to your
 my health care notebook Why? Being an active part of your health care team helps you feel better and helps you get even better care. Starting on Day 1, you can keep track of important information and questions.
my health care notebook Why? Being an active part of your health care team helps you feel better and helps you get even better care. Starting on Day 1, you can keep track of important information and questions.
Designing the Role of the Embedded Care Manager
 Designing the Role of the Embedded By Patricia Hines, Ph.D., RN and Marge Mercury, RN, MS, CMCE The Embedded The use of an Embedded ( ECM ) to coordinate within the complex delivery system is sharply increasing.
Designing the Role of the Embedded By Patricia Hines, Ph.D., RN and Marge Mercury, RN, MS, CMCE The Embedded The use of an Embedded ( ECM ) to coordinate within the complex delivery system is sharply increasing.
Comprehensive Cardiac Care Program
 PrograM Comprehensive Cardiac Care Program Empowering you to strengthen your heart. Trust In Our Care. Trust in Our Care The Comprehensive Cardiac Care Program is physician directed and focused on assisting
PrograM Comprehensive Cardiac Care Program Empowering you to strengthen your heart. Trust In Our Care. Trust in Our Care The Comprehensive Cardiac Care Program is physician directed and focused on assisting
Putting it All Together: A Strategy for Special Needs Services that Make Sense for Families Information Session
 Putting it All Together: A Strategy for Special Needs Services that Make Sense for Families Information Session Ministry of Children and Youth Services Ministry of Community and Social Services Ministry
Putting it All Together: A Strategy for Special Needs Services that Make Sense for Families Information Session Ministry of Children and Youth Services Ministry of Community and Social Services Ministry
Revenue Cycle in Post- Acute Care Deloitte & Touche LLP Victor Shutack, Senior Manager June 2015
 6/9/2015 Revenue Cycle in Post- Acute Care Deloitte & Touche LLP Victor Shutack, Senior Manager June 2015 Discussion topics Changing healthcare environment Understanding the home health care environment
6/9/2015 Revenue Cycle in Post- Acute Care Deloitte & Touche LLP Victor Shutack, Senior Manager June 2015 Discussion topics Changing healthcare environment Understanding the home health care environment
Learning Collaborative
 Care Transitions Intervention Model to Reduce 30-Day Readmissions for Chronic Cardiac Conditions Learning Collaborative Dr. Norma Jean-Francois, DNP, APN-C Dr. Mary Anne Marra, DNP, MSN, RN, NEA-BC 1 OVERVIEW
Care Transitions Intervention Model to Reduce 30-Day Readmissions for Chronic Cardiac Conditions Learning Collaborative Dr. Norma Jean-Francois, DNP, APN-C Dr. Mary Anne Marra, DNP, MSN, RN, NEA-BC 1 OVERVIEW
Empowering Value-Based Healthcare
 Empowering Value-Based Healthcare Episode Connect, Remedy s proprietary suite of software applications, is a powerful platform for managing value-based payment programs. Delivered via the web or mobile
Empowering Value-Based Healthcare Episode Connect, Remedy s proprietary suite of software applications, is a powerful platform for managing value-based payment programs. Delivered via the web or mobile
1. TITLE: Colin A. Banas MD, MSHA Chief Medical Information Officer Secondary Point of Contact: 804-827- 4196, [email protected]
 1. TITLE: Using Health Information Technology - CPOE to Advance Performance Improvement in Heart Failure Patients at Virginia Commonwealth University Health System 2. ORGANIZATION: Virginia Commonwealth
1. TITLE: Using Health Information Technology - CPOE to Advance Performance Improvement in Heart Failure Patients at Virginia Commonwealth University Health System 2. ORGANIZATION: Virginia Commonwealth
DRIVING VALUE IN HEALTHCARE: PERSPECTIVES FROM TWO ACO EXECUTIVES, PART I
 DRIVING VALUE IN HEALTHCARE: PERSPECTIVES FROM TWO ACO EXECUTIVES, PART I A firm understanding of the key components and drivers of healthcare reform is increasingly important within the pharmaceutical,
DRIVING VALUE IN HEALTHCARE: PERSPECTIVES FROM TWO ACO EXECUTIVES, PART I A firm understanding of the key components and drivers of healthcare reform is increasingly important within the pharmaceutical,
Home Health Care Today: Higher Acuity Level of Patients Highly skilled Professionals Costeffective Uses of Technology Innovative Care Techniques
 Comprehensive EHR Infrastructure Across the Health Care System The goal of the Administration and the Department of Health and Human Services to achieve an infrastructure for interoperable electronic health
Comprehensive EHR Infrastructure Across the Health Care System The goal of the Administration and the Department of Health and Human Services to achieve an infrastructure for interoperable electronic health
Thank You for Joining!
 Thank You for Joining! New England Nursing Home Quality Care Collaborative Massachusetts Learning & Sharing Webinar: QAPI Data Techniques August 25, 2015 Call-In Number: 855-309-6568 Access Code: 7523186
Thank You for Joining! New England Nursing Home Quality Care Collaborative Massachusetts Learning & Sharing Webinar: QAPI Data Techniques August 25, 2015 Call-In Number: 855-309-6568 Access Code: 7523186