Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions
|
|
|
- Scot Casey
- 9 years ago
- Views:
Transcription
1 Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions Leslie Becker RN, BS Jennifer Smith RN, MSN, MBA Leslie Frain MSN, RN Jan Machanis MSN, RN Kathy Benjamin MSN, RN Donna McNally MSN, BSN, RN Susan Morby MSN, RN, NE-BC Randy Parker PhD, RN, NEA-BC

2 Introduction Four culturally and socio-economically diverse community hospitals in the United States implemented a Nurse Transition Coach Model (NTCM) that significantly reduced readmission rates in patients with congestive heart failure (CHF) from 2011 through 2013.
")
3 Background In Medicare fee-for-service data identified 30-day readmission rates for heart failure to be 26.9% Reduction in hospital readmission rates have been identified by Congress and President Obama as a source to reduce Medicare spending Health care costs impose an increased burden on the Federal budget On March 23, 2010 comprehensive healthcare reform legislation was signed into law by President Obama; Patient Protection and Affordable Care Act Stephen F. Jencks, M.D., and Eric A. Coleman, M.D., M.P.H., Rehospitalization among Patients in the Medicare Fee-For Service Program, New England Journal of Medicine, vol. 360(April 2, 2009),pp

4 Patient Protection and Affordable Care Act Provisions Reduce preventable readmissions by reducing Medicare payments to hospitals with high preventable readmission rates Demonstration projects to test reform of Medicare payment system Demonstration projects to test improvements to patient care for people with chronic illness across the continuum 2012 hospitals were penalized up to 1% of every Medicare payment 2013 hospitals were penalized up to 2% of every Medicare payment 2017 Medicare may penalize providers and hospitals 8% if they fail to substantially reduce readmission rates Julie Stone, Specialist in Health Care Financing, Geoffrey J. Hoffman, Analyst in Health Care Financing for The Congressional Research Service (CRS), Report to Congress: Medicare Hospital Readmissions: Issues, Policy Options and PPACA, September 21, See

5 Objectives To improve care of patients vulnerable for readmission across the continuum Reduction of preventable CHF readmissions at our facilities from 25-17% in 2011, to 11% in 2013, by developing a NTCM utilizing evidence based practice Avoid loss of revenue from Medicare penalties

6 Definition Readmission Readmit to same or different hospital Planned or unplanned surgical or medical procedure Within a specified time frame 30 days

7 Factors Associated with Readmissions Handoff of medical care information during transition to the next level of care and the primary care physician Patient education about diagnosis and the discharge planning which begins on admission Follow-up from hospital to next level of care: home, SNF, sub-acute Medication reconciliation and realistic plan for obtaining; resulting in medication errors Comprehension of a plan if condition worsens (notify PCP, TC, HHC) Discharge summary Discharge instructions: diet, activity level, follow up appointment with primary care physician, daily weights, plan is symptoms worsen, medication education

8 Method Establish discharge planning stakeholders committee Research service delivery models Develop a transitional discharge model Implement the discharge model Evaluate, improve, and evolve into The Nurse Transition Coach Model

9 Preventing Avoidable Readmissions by Improving Transitions in Care A Systematic Review Conclusion: No single intervention implemented alone was regularly associated with reduced risk for 30-day rehospitalization. Luke O. Hansen, M.D.,M.H.S., Robert S. Young, M.d., M.S., Keikl Hinami, M.D., M.S., Alicia Leung, M.D., and Mark V. Williams, M.D., Interventions to Reduce 30-Day Rehospitalization: A Systematic Review, Annals of Internal Medicine 2011; 155(8), pp

10 Promising Approaches to Reduce Readmissions Improved Transitions Out of the Hospital Project Red Boost IHI s Transforming Care at the Bedside Hospital to Home H2H (ACC/IHI)

11 More Promising Approaches Supplemental Transitional Care after Discharge from the Hospital Care Transitions Intervention (Coleman) Transitional Care Intervention (Naylor) Alternative or Intensive Care Management for High Risk Patients Proactive palliative care for patients with advanced illness Evercare Model Heart failure clinics PACE Program; programs for dual eligibles Intensive care management from primary care or health plan

12 Nurse Transition Coach Model Ground in Jean Watson s theory of human caring emphasizing rapport and trust building with patient s and their families Establish a care continuum hand off with bi-directional communication to insure shared accountability for collaborative decision making Multidisciplinary rounds Patient/caregiver follow-up within 48 hours of discharge and weekly for 30 days Hand off to complex care managers after 30 days Homecare case-manager weekly report SNF or sub-acute weekly report Process Improvement Bedside post readmission meeting with transition coach, CNO, CMO, case management Readmission Review Weekly Meeting and root cause analysis of all readmissions Monthly Readmit Care Meeting with community care, home care, social work, case management, quality, transition coaches

13 Nurse Transition Coach Model, A Patient Centered Approach Upon Admission we establish a mutually responsible relationship with patient and family; patient centered and specific Assess the patient s understanding, goals, and needs (transportation, caregivers, money for medications.) Individualize each patient s care and liberate resources needed There is no single answer for our patients, they are all different, with their own story and circumstance, their own vision of quality of life. The transition coach is their teammate, coach, facilitator, organizer, planner, teacher, and partner, always available to help with even their most fundamental need of respect, trust, and consistency. The transition coach is the voice that is always available inpatient and outpatient.

14 Successful Innovative Strategies to Prevent Hospital Readmissions Receives a starter pack of discharge medications regardless of ability to pay Discharged with a follow-up appointment with 72 hours Given access to affordable transportation for physician visits (i.e., $2:00 a ride) Referred to homecare and seen with hours of discharge with recommended visit frequencies Bedside report/debriefing for each readmission at 8:00a.m. with the Readmit Care Team Primary care physician intervene at readmission to treat and discharge in observation status


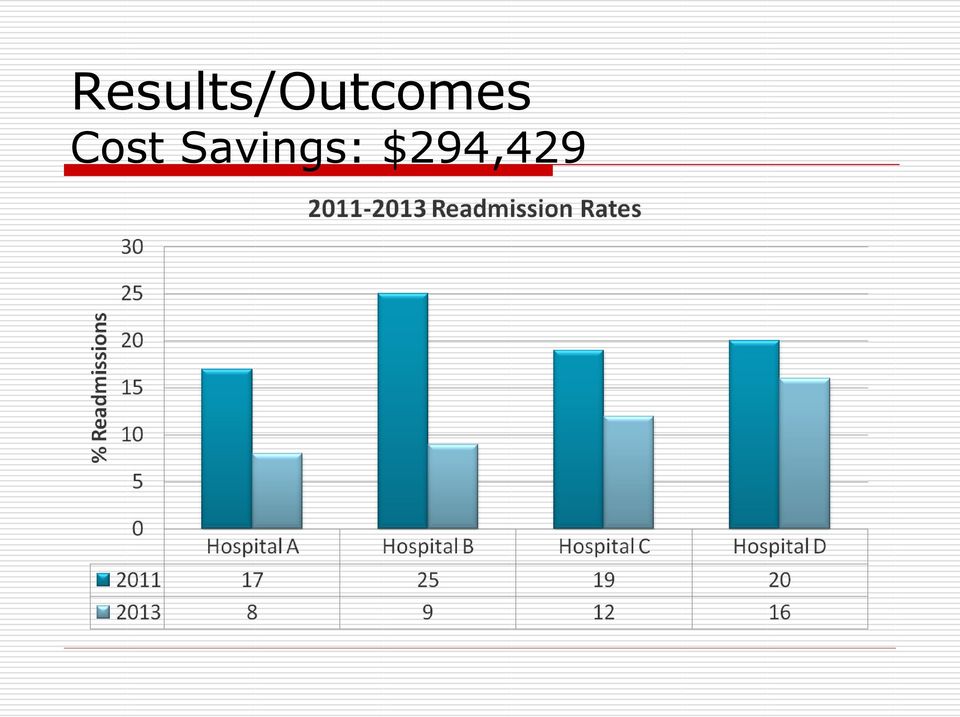
15 Results/Outcomes Cost Savings: $294,429
16 Future Directions Broaden the NTCM to a larger population, expand to all patients Expand to all payers Risk stratification tool Tele-health Meaningful use Leveraging technology

17 References Stephen F. Jencks, M.D., and Eric A. Coleman, M.D., M.P.H., Rehospitalization among Patients in the Medicare Fee-For-Service Program, New England Journal of Medicine, vol. 360(April 2, 2009),pp Julie Stone, Specialist in Health Care Financing, Geoffrey J. Hoffman, Analyst in Health Care Financing for The Congressional Research Service (CRS), Report to Congress: Medicare Hospital Readmissions: Issues, Policy Options and PPACA, September 21, See Luke O. Hansen, M.D.,M.H.S., Robert S. Young, M.d., M.S., Keikl Hinami, M.D., M.S., Alicia Leung, M.D., and Mark V. Williams, M.D., Interventions to Reduce 30-Day Rehospitalization: A Systematic Review, Annals of Internal Medicine 2011; 155(8), pp
, pp.")
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION
 Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Health Care Leader Action Guide to Reduce Avoidable Readmissions
 Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
1. Executive Summary Problem/Opportunity: Evidence: Baseline Data: Intervention: Results:
 A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education
 1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
Readmissions as an Enterprise Priority. Presenters 4/17/2014
 Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center [email protected] Eileen
Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center [email protected] Eileen
PCMH and Care Management: Where do we start?
 PCMH and Care Management: Where do we start? Patricia Bohs, RN, BSN Quality Assurance Manager Kelly McCloughan QA Data Manager Wayne Memorial Community Health Centers Honesdale, PA Wayne Memorial Community
PCMH and Care Management: Where do we start? Patricia Bohs, RN, BSN Quality Assurance Manager Kelly McCloughan QA Data Manager Wayne Memorial Community Health Centers Honesdale, PA Wayne Memorial Community
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment
 Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015
 Leveraging the Continuum to Avoid Unnecessary Utilization While Improving Quality Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015 Karim A. Habibi, FHFMA, MPH, MS Senior
Leveraging the Continuum to Avoid Unnecessary Utilization While Improving Quality Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015 Karim A. Habibi, FHFMA, MPH, MS Senior
From the Ground Up: The implementation of a Transition Care Program (TOC) and its impact in COPD 30-day readmissions
 and its impact in COPD 30-day readmissions") From the Ground Up: The implementation of a Transition Care Program (TOC) and its impact in COPD 30-day readmissions Cristiane L. Fukuda RN, MSN, ANP-BC Email: [email protected] Office: 404-851-6914
From the Ground Up: The implementation of a Transition Care Program (TOC) and its impact in COPD 30-day readmissions Cristiane L. Fukuda RN, MSN, ANP-BC Email: [email protected] Office: 404-851-6914
Hospital readmissions contribute to the increasing. Deployment of Lean Six Sigma in Care Coordination An Improved Discharge Process
 Professional Case Management Vol. 19, No. 2, 77-83 Copyright 2014 Wolters Kluwer Health Lippincott Williams & Wilkins Deployment of Lean Six Sigma in Care Coordination An Improved Discharge Process Susan
Professional Case Management Vol. 19, No. 2, 77-83 Copyright 2014 Wolters Kluwer Health Lippincott Williams & Wilkins Deployment of Lean Six Sigma in Care Coordination An Improved Discharge Process Susan
Transitions of Care: The need for a more effective approach to continuing patient care
 H O T T O P I C S I N H E A L T H C A R E Transitions of Care: The need for a more effective approach to continuing patient care The need for a more effective approach to continuing patient care This paper
H O T T O P I C S I N H E A L T H C A R E Transitions of Care: The need for a more effective approach to continuing patient care The need for a more effective approach to continuing patient care This paper
Understanding Care Transitions as a Patient Safety Issue
 Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
hospital readmission rate reduction: building better interfaces within the community.
 hospital readmission rate reduction: building better interfaces within the community. Whitepaper By Ken Taverner, M.Sc. the issue of hospital readmission rates Leaving the hospital after being admitted
hospital readmission rate reduction: building better interfaces within the community. Whitepaper By Ken Taverner, M.Sc. the issue of hospital readmission rates Leaving the hospital after being admitted
Using Root Cause Analysis to Determine Why Readmissions are High. Presentation Objectives. Background Information 11/30/2011
 Using Root Cause Analysis to Determine Why Readmissions are High Nancy Seck RBN, BSN, MPH, CPHQ Director, Quality Management Glendale Memorial Hospital and Health Center Presentation Objectives Identify
Using Root Cause Analysis to Determine Why Readmissions are High Nancy Seck RBN, BSN, MPH, CPHQ Director, Quality Management Glendale Memorial Hospital and Health Center Presentation Objectives Identify
10/24/2014. 9 th Annual Nursing Research Conference Presented By: Heather Powell & Jeanmarie Okoniewski
 9 th Annual Nursing Research Conference Presented By: Heather Powell & Jeanmarie Okoniewski Heather J. Powell, MSN, RN, RN-BC Kimberly D. Williams, MPH Jeanmarie Okoniewski, MSN, RN, RN-BC Melinda Acevedo,
9 th Annual Nursing Research Conference Presented By: Heather Powell & Jeanmarie Okoniewski Heather J. Powell, MSN, RN, RN-BC Kimberly D. Williams, MPH Jeanmarie Okoniewski, MSN, RN, RN-BC Melinda Acevedo,
WHITE PAPER. How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience
 WHITE PAPER How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience Vocera Communications, Inc. June, 2014 SUMMARY Hospitals that reduce readmission rates
WHITE PAPER How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience Vocera Communications, Inc. June, 2014 SUMMARY Hospitals that reduce readmission rates
Patient Centered Medical Home: An Approach for the Health Plan
 : An Approach for the Health Plan By Marissa A. Harper and JoAnn E. Balara Excellence in healthcare consulting The Medical Home Concept Works Recent Medicare demonstration projects on Patient Centered
: An Approach for the Health Plan By Marissa A. Harper and JoAnn E. Balara Excellence in healthcare consulting The Medical Home Concept Works Recent Medicare demonstration projects on Patient Centered
A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates. April 11, 2014
 A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates April 11, 2014 About the QIO Program Leading rapid, large-scale change in health quality: Goals are bolder. The patient is at
A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates April 11, 2014 About the QIO Program Leading rapid, large-scale change in health quality: Goals are bolder. The patient is at
FINANCIAL IMPLICATIONS OF EXCESS HOSPITAL READMISSIONS JOSESPH B. HENDERSON, J.D.
 FINANCIAL IMPLICATIONS OF EXCESS HOSPITAL READMISSIONS JOSESPH B. HENDERSON, J.D. Executive MHA Candidate, 2013 University of Southern California Sol Price School of Public Policy Abstract A 2007 Medicare
FINANCIAL IMPLICATIONS OF EXCESS HOSPITAL READMISSIONS JOSESPH B. HENDERSON, J.D. Executive MHA Candidate, 2013 University of Southern California Sol Price School of Public Policy Abstract A 2007 Medicare
Coordinating Transitions of Care: It Takes a Village
 Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
IDENTIFYING INFORMATION MANAGEMENT CHALLENGES FACED BY HOME HEALTHCARE PROFESSIONALS MANAGING OLDER ADULTS TRANSITIONS FROM HOSPITAL TO HOME CARE
 IDENTIFYING INFORMATION MANAGEMENT CHALLENGES FACED BY HOME HEALTHCARE PROFESSIONALS MANAGING OLDER ADULTS TRANSITIONS FROM HOSPITAL TO HOME CARE Alicia Arbaje, M.D., M.P.H. Assistant Professor of Medicine,
IDENTIFYING INFORMATION MANAGEMENT CHALLENGES FACED BY HOME HEALTHCARE PROFESSIONALS MANAGING OLDER ADULTS TRANSITIONS FROM HOSPITAL TO HOME CARE Alicia Arbaje, M.D., M.P.H. Assistant Professor of Medicine,
Presented by: Char Brar, ACNP, MS(Chem.), MSN, RN Cardiology Nurse Practitioner JBVAMC, Chicago
, MSN, RN Cardiology Nurse Practitioner JBVAMC, Chicago") Presented by: Char Brar, ACNP, MS(Chem.), MSN, RN Cardiology Nurse Practitioner JBVAMC, Chicago 200 bed acute care facility 4 Community Based Out-patient Clinics (CBOCs) 58,000 Veterans IN FY 2008 : 768
Presented by: Char Brar, ACNP, MS(Chem.), MSN, RN Cardiology Nurse Practitioner JBVAMC, Chicago 200 bed acute care facility 4 Community Based Out-patient Clinics (CBOCs) 58,000 Veterans IN FY 2008 : 768
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS. Karen Unholz, RN, BSN
 INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
Z Take this folder with you to your
 my health care notebook Why? Being an active part of your health care team helps you feel better and helps you get even better care. Starting on Day 1, you can keep track of important information and questions.
my health care notebook Why? Being an active part of your health care team helps you feel better and helps you get even better care. Starting on Day 1, you can keep track of important information and questions.
Care Coordination and Transitions in Behavioral Health
 Care Coordination and Transitions in Behavioral Health Pam Pietruszewski Integrated Health Consultant The National Council for Behavioral Health This product is supported by the Florida Department of Children
Care Coordination and Transitions in Behavioral Health Pam Pietruszewski Integrated Health Consultant The National Council for Behavioral Health This product is supported by the Florida Department of Children
Learning Collaborative
 Care Transitions Intervention Model to Reduce 30-Day Readmissions for Chronic Cardiac Conditions Learning Collaborative Dr. Norma Jean-Francois, DNP, APN-C Dr. Mary Anne Marra, DNP, MSN, RN, NEA-BC 1 OVERVIEW
Care Transitions Intervention Model to Reduce 30-Day Readmissions for Chronic Cardiac Conditions Learning Collaborative Dr. Norma Jean-Francois, DNP, APN-C Dr. Mary Anne Marra, DNP, MSN, RN, NEA-BC 1 OVERVIEW
Care Coordination at Frederick Regional Health System. Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care
 Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home
 RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
Population Health Management: Banner Health Network s Perspective. Neta Faynboym, Medical Director Banner Health Network
 Population Health Management: Banner Health Network s Perspective Neta Faynboym, Medical Director Banner Health Network 29 Acute Care Hospitals BANNER AT A GLANCE Banner Health Network with 400K lives
Population Health Management: Banner Health Network s Perspective Neta Faynboym, Medical Director Banner Health Network 29 Acute Care Hospitals BANNER AT A GLANCE Banner Health Network with 400K lives
RT AS PROJECT MANAGER:
 RT AS PROJECT MANAGER: IMPROVING CARE TRANSITIONS DECREASES UNPLANNED READMISSIONS TAMMY JARNAGIN, BHS, RRT DIRECTOR CARDIOPULMONARY SERVICES, NEURODIAGNOSTICS, HOME MEDICAL EQUIPMENT Objectives Recognize
RT AS PROJECT MANAGER: IMPROVING CARE TRANSITIONS DECREASES UNPLANNED READMISSIONS TAMMY JARNAGIN, BHS, RRT DIRECTOR CARDIOPULMONARY SERVICES, NEURODIAGNOSTICS, HOME MEDICAL EQUIPMENT Objectives Recognize
Providing and Billing Medicare for Transitional Care Management
 PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
Transition of Care (TOC) Log Instructions (Effective: 4/15/14)
 Log Instructions (Effective: 4/15/14)") Transition of Care (TOC) Log Instructions (Effective: 4/15/14) General Instructions: Please note that each transition requires a separate form. For example, an admission to the hospital should have one
Transition of Care (TOC) Log Instructions (Effective: 4/15/14) General Instructions: Please note that each transition requires a separate form. For example, an admission to the hospital should have one
THE 2015 QUALIS HEALTH AWARDS OF EXCELLENCE IN HEALTHCARE QUALITY
 THE 2015 QUALIS HEALTH AWARDS OF EXCELLENCE IN HEALTHCARE QUALITY Since 2002, Qualis Health has presented the annual Awards of Excellence in Healthcare Quality to outstanding organizations in Idaho and
THE 2015 QUALIS HEALTH AWARDS OF EXCELLENCE IN HEALTHCARE QUALITY Since 2002, Qualis Health has presented the annual Awards of Excellence in Healthcare Quality to outstanding organizations in Idaho and
Assessing Risk of Readmission. NoCVA Preventing Avoidable Readmission Collaborative Laura Maynard, MDiv, NCQC Amanda Hobbs, NCQC July 31, 2013
 Assessing Risk of Readmission NoCVA Preventing Avoidable Readmission Collaborative Laura Maynard, MDiv, NCQC Amanda Hobbs, NCQC July 31, 2013 Collaborative Goals Reduce readmission rates by 20% Increase
Assessing Risk of Readmission NoCVA Preventing Avoidable Readmission Collaborative Laura Maynard, MDiv, NCQC Amanda Hobbs, NCQC July 31, 2013 Collaborative Goals Reduce readmission rates by 20% Increase
THE SAN DIEGO CARE TRANSITIONS PARTNERSHIP
 THE SAN DIEGO CARE TRANSITIONS PARTNERSHIP Transforming Care Across the Continuum Julianne R. Howell, Ph.D. Senior Health Policy Advisor County of San Diego Health and Human Services Agency SAN DIEGO COUNTY
THE SAN DIEGO CARE TRANSITIONS PARTNERSHIP Transforming Care Across the Continuum Julianne R. Howell, Ph.D. Senior Health Policy Advisor County of San Diego Health and Human Services Agency SAN DIEGO COUNTY
Improving Care Transitions using PDSA Methodology
 Improving Care Transitions using PDSA Methodology Catherine Payne, MD, FHM Care Transitions Physician Champion Medical Director of Clinical Informatics Erlanger Medical Center Chattanooga, Tennessee Objectives
Improving Care Transitions using PDSA Methodology Catherine Payne, MD, FHM Care Transitions Physician Champion Medical Director of Clinical Informatics Erlanger Medical Center Chattanooga, Tennessee Objectives
THE EVOLUTION OF CMS PAYMENT MODELS
 THE EVOLUTION OF CMS PAYMENT MODELS December 3, 2015 Dayton Benway, Principal AGENDA Legislative Background Payment Model Categories Life Cycle The Models LEGISLATIVE BACKGROUND Medicare Modernization
THE EVOLUTION OF CMS PAYMENT MODELS December 3, 2015 Dayton Benway, Principal AGENDA Legislative Background Payment Model Categories Life Cycle The Models LEGISLATIVE BACKGROUND Medicare Modernization
MANITOWOC COUNTY CARE TRANSITION PROGRAM
 MANITOWOC COUNTY CARE TRANSITION PROGRAM A U G U S T 1 5, 2 0 1 3 Judy Rank Director Cathy Ley Supervisor Care Transitions Coach MANITOWOC COUNTY CARE TRANSITION PROGRAM Julie Place, Director of Nursing
MANITOWOC COUNTY CARE TRANSITION PROGRAM A U G U S T 1 5, 2 0 1 3 Judy Rank Director Cathy Ley Supervisor Care Transitions Coach MANITOWOC COUNTY CARE TRANSITION PROGRAM Julie Place, Director of Nursing
5/13/2011. ACO Partnerships A Case Study. Contents: The Strategic Imperative for Accountable Care
 ACO Partnerships A Case Study Bob Edmondson, MPH Vice President, Innovation West Penn Allegheny Health System Pittsburgh, PA 1 Contents: 1. The Strategic Imperative for Accountable Care 2. Population Health
ACO Partnerships A Case Study Bob Edmondson, MPH Vice President, Innovation West Penn Allegheny Health System Pittsburgh, PA 1 Contents: 1. The Strategic Imperative for Accountable Care 2. Population Health
Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes. FINANCIAL DISCLOSURE: No relevant financial relationship exists
 Cheri Basso BSN, RN-BC, CHFN Mary Washington Healthcare Fredericksburg, VA Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes FINANCIAL DISCLOSURE: No relevant financial relationship
Cheri Basso BSN, RN-BC, CHFN Mary Washington Healthcare Fredericksburg, VA Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes FINANCIAL DISCLOSURE: No relevant financial relationship
What Really Works for High- Risk, High-Cost Patients?
 What Really Works for High- Risk, High-Cost Patients? National Academy of Medicine Workshop Models of Care for High-Need Patients Washington, DC January 19, 2016 Randall Brown, Ph.D. Mathematica Policy
What Really Works for High- Risk, High-Cost Patients? National Academy of Medicine Workshop Models of Care for High-Need Patients Washington, DC January 19, 2016 Randall Brown, Ph.D. Mathematica Policy
Connect4 Patients CCCM Primary Care Community. Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM
 Connect4 Patients CCCM Primary Care Community Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM September 17, 2015 Objectives: Describe innovative care management
Connect4 Patients CCCM Primary Care Community Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM September 17, 2015 Objectives: Describe innovative care management
Innovations@Home. Home Health Initiatives Reduce Avoidable Readmissions by Leveraging Innovation
 How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
How To Reduce Hospital Readmission
 Reducing Hospital Readmissions By Jenny Minott November 2008 www.academyhealth.org 1 Introduction For most patients who leave the hospital, the last thing they want is to return anytime soon. Yet, many
Reducing Hospital Readmissions By Jenny Minott November 2008 www.academyhealth.org 1 Introduction For most patients who leave the hospital, the last thing they want is to return anytime soon. Yet, many
Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases
 Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases Epidemiology Over 145 million people ( nearly half the population) - suffer from asthma, depression and other chronic
Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases Epidemiology Over 145 million people ( nearly half the population) - suffer from asthma, depression and other chronic
Visiting Nurse Service of New York. New York State Department of Health Medicaid Incentive Payment System (MIPS) External Stakeholder Feedback
 External Stakeholder Feedback") New York State Department of Health Medicaid Incentive Payment System (MIPS) External Stakeholder Feedback Visiting Nurse Service of New York February 19, 2010 11:30 a.m. 12:30 p.m. New York State Department
New York State Department of Health Medicaid Incentive Payment System (MIPS) External Stakeholder Feedback Visiting Nurse Service of New York February 19, 2010 11:30 a.m. 12:30 p.m. New York State Department
Patient to Person. Transitions of Care. Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM
 Patient to Person Transitions of Care Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM Transitions of Care Transitioning from school to adult services (vocational, medical day, etc.)
Patient to Person Transitions of Care Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM Transitions of Care Transitioning from school to adult services (vocational, medical day, etc.)
Henry Ford Health System Care Coordination and Readmissions Update
 Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
RED, BOOST, and You: Improving the Discharge Transition of Care
 RED, BOOST, and You: Improving the Discharge Transition of Care Jeffrey L. Greenwald, MD, SFHM Massachusetts General Hospital - Clinician Educator Service Co-Investigator Project RED & Project BOOST The
RED, BOOST, and You: Improving the Discharge Transition of Care Jeffrey L. Greenwald, MD, SFHM Massachusetts General Hospital - Clinician Educator Service Co-Investigator Project RED & Project BOOST The
08/04/2014. Tim Hogan, RRT, PhD Primary Care Home Health Director. University of Missouri Health Care Department of Family and Community Medicine
 Tim Hogan, RRT, PhD, Primary Care Home Health Director Joan Asbee, RN, BSN, CWOCN, Nurse Care Manager Karli Urban, MD, Assistant Professor of Clinical Family and Community Medicine University of Missouri
Tim Hogan, RRT, PhD, Primary Care Home Health Director Joan Asbee, RN, BSN, CWOCN, Nurse Care Manager Karli Urban, MD, Assistant Professor of Clinical Family and Community Medicine University of Missouri
Decreasing 30 day Readmissions on a Medical Surgical Telemetry Unit
 Decreasing 30 day Readmissions on a Medical Surgical Telemetry Unit Presented By: Dr. Micah Beachy, Rickelle Collins and Nicole Turille Context As part of healthcare reform, hospitals are being challenged
Decreasing 30 day Readmissions on a Medical Surgical Telemetry Unit Presented By: Dr. Micah Beachy, Rickelle Collins and Nicole Turille Context As part of healthcare reform, hospitals are being challenged
Kaiser Permanente: Transition Care Performance and Strategies
 Kaiser Permanente: Transition Care Performance and Strategies Carol Ann Barnes, PT, DPT, GCS [email protected] April 2009 Netta Conyers-Haynes, October, 2014 Principal Consultant, Communications Agenda
Kaiser Permanente: Transition Care Performance and Strategies Carol Ann Barnes, PT, DPT, GCS [email protected] April 2009 Netta Conyers-Haynes, October, 2014 Principal Consultant, Communications Agenda
Cheryl Schraeder, RN, PhD, FAAN. The demographic landscape of America is changing at an accelerated pace
 Stepping up to the challenge: Changing the way we deliver care Cheryl Schraeder, RN, PhD, FAAN 1 Goals of Presentation To Identify: The key challenges in delivering evidence-based & cost-effective care
Stepping up to the challenge: Changing the way we deliver care Cheryl Schraeder, RN, PhD, FAAN 1 Goals of Presentation To Identify: The key challenges in delivering evidence-based & cost-effective care
Building an Accountable Care Organization. Jean Malouin, MD MPH University of Michigan Health System September 21, 2012
 Building an Accountable Care Organization Jean Malouin, MD MPH University of Michigan Health System September 21, 2012 Agenda UMHS overview PGP demo ACO precursor Current efforts underway Role of primary
Building an Accountable Care Organization Jean Malouin, MD MPH University of Michigan Health System September 21, 2012 Agenda UMHS overview PGP demo ACO precursor Current efforts underway Role of primary
The Role of Telemedicine in Home Monitoring and Long Term Care June 7, 2012. Penny S. Milanovich President UPMC Visiting Nurses Association
 The Role of Telemedicine in Home Monitoring and Long Term Care June 7, 2012 Penny S. Milanovich President UPMC Visiting Nurses Association Cost of Chronic Conditions An average of 40-50% of healthcare
The Role of Telemedicine in Home Monitoring and Long Term Care June 7, 2012 Penny S. Milanovich President UPMC Visiting Nurses Association Cost of Chronic Conditions An average of 40-50% of healthcare
ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION)
") ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION) Hello and welcome. Thank you for taking part in this presentation entitled "Essentia Health as an ACO or Accountable Care Organization -- What
ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION) Hello and welcome. Thank you for taking part in this presentation entitled "Essentia Health as an ACO or Accountable Care Organization -- What
The Value Quadrant of Healthcare Reform. 2008 Pharos Innovations, LLC. All Rights Reserved.
 The Value Quadrant of Healthcare Reform ACOs in PPACA Provider Organizations or networked groups Accountable for quality, cost and overall care of defined population of Medicare FFS benes Key metrics to
The Value Quadrant of Healthcare Reform ACOs in PPACA Provider Organizations or networked groups Accountable for quality, cost and overall care of defined population of Medicare FFS benes Key metrics to
Game Changer at the Primary Care Practice Embedded Care Management. Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012
 Game Changer at the Primary Care Practice Embedded Care Management Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012 Objectives To describe the recent evolution of care management at
Game Changer at the Primary Care Practice Embedded Care Management Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012 Objectives To describe the recent evolution of care management at
Locking the Revolving Door of Readmissions
 Locking the Revolving Door of Readmissions The Pharmacist s Role in Keeping Patients Healthy, Happy and At Home Steve Riddle, BS Pharm, BCPS, FASHP VP of Clinical Affairs, Pharmacy OneSource Objectives
Locking the Revolving Door of Readmissions The Pharmacist s Role in Keeping Patients Healthy, Happy and At Home Steve Riddle, BS Pharm, BCPS, FASHP VP of Clinical Affairs, Pharmacy OneSource Objectives
Blueprint for Post-Acute
 Blueprint for Post-Acute Care Reform Post-acute care is a critical component within our nation s healthcare system and an essential aspect of care for many patients making a full recovery possible after
Blueprint for Post-Acute Care Reform Post-acute care is a critical component within our nation s healthcare system and an essential aspect of care for many patients making a full recovery possible after
Performance Measurement in CMS Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS
 Performance Measurement in CMS Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS Mind the Gap: Improving Quality Measures in Accountable Care Systems October
Performance Measurement in CMS Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS Mind the Gap: Improving Quality Measures in Accountable Care Systems October
Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services
 Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services Objectives Understand the new consequences to hospitals for discharged clients being re-admitted within selected time
Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services Objectives Understand the new consequences to hospitals for discharged clients being re-admitted within selected time
Safe Transitions Best Practice Measures for
 Safe Transitions Best Practice Measures for Hospitals Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Safe Transitions Best Practice Measures for Hospitals Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Health Plan Innovations in Patient-Centered Care. Transitions of Care. April 2012 2012 ACHP
 Health Plan Innovations in Patient-Centered Care April 2012 Transitions of Care : Transitions of Care from Hospital to Home Practices Used by Community-Based Health Plans to Facilitate Successful Care
Health Plan Innovations in Patient-Centered Care April 2012 Transitions of Care : Transitions of Care from Hospital to Home Practices Used by Community-Based Health Plans to Facilitate Successful Care
Kim Olmedo, LCSW, CCM CSW-G Social Work Manager, Silverback Care Management
 Kim Olmedo, LCSW, CCM CSW-G Social Work Manager, Silverback Care Management According to AARP, about 8000 people turn 65 every day The Medicare Trustees have estimated that Medicare will run out of money
Kim Olmedo, LCSW, CCM CSW-G Social Work Manager, Silverback Care Management According to AARP, about 8000 people turn 65 every day The Medicare Trustees have estimated that Medicare will run out of money
Home Health Care: A More Cost-Effective Approach to Medicaid in Illinois Illinois HomeCare & Hospice Council December 2010
 Home Health Care: A More Cost-Effective Approach to Medicaid in Illinois Illinois HomeCare & Hospice Council December 2010 As the Illinois Legislature prepares to act on the future of Medicaid, it is important
Home Health Care: A More Cost-Effective Approach to Medicaid in Illinois Illinois HomeCare & Hospice Council December 2010 As the Illinois Legislature prepares to act on the future of Medicaid, it is important
Second Forum on Health Care Management & Policy November 28 30, 2012. Discussion Report. Care Management
 Second Forum on Health Care Management & Policy November 28 30, 2012 Discussion Report Care Management Thomas G. Rundall Henry J. Kaiser Emeritus Professor of Organized Health Systems School of Public
Second Forum on Health Care Management & Policy November 28 30, 2012 Discussion Report Care Management Thomas G. Rundall Henry J. Kaiser Emeritus Professor of Organized Health Systems School of Public
Congestive Heart Failure Management Program
 Congestive Heart Failure Management Program The Congestive Heart Failure Program is the third statewide disease management program developed by CCNC. The clinical directors reviewed prevalence and outcome
Congestive Heart Failure Management Program The Congestive Heart Failure Program is the third statewide disease management program developed by CCNC. The clinical directors reviewed prevalence and outcome
Six Communication Best Practices for Transitional Care Management
 WHITE PAPER Six Communication Best Practices for Transitional Care Management In the era of chronic illness and historically long lifespans, patient care transitions to home or another facility have become
WHITE PAPER Six Communication Best Practices for Transitional Care Management In the era of chronic illness and historically long lifespans, patient care transitions to home or another facility have become
Tool 6: How To Monitor Re-Engineered Discharge Implementation and Outcomes
 Tool 6: How To Monitor Re-Engineered Discharge Implementation and Outcomes 6.. Purpose of This Tool Monitoring the RED lets you know whether each component of RED is being successfully implemented and
Tool 6: How To Monitor Re-Engineered Discharge Implementation and Outcomes 6.. Purpose of This Tool Monitoring the RED lets you know whether each component of RED is being successfully implemented and
Home Care s Pivotal Role in Patient Transitions from Acute to Post Acute Care Settings:
 Home Care s Pivotal Role in Patient Transitions from Acute to Post Acute Care Settings: Experiences of a Successful CCTP Program And So Much More! Jane Pike-Benton Senior Director, Home Health & Post Acute
Home Care s Pivotal Role in Patient Transitions from Acute to Post Acute Care Settings: Experiences of a Successful CCTP Program And So Much More! Jane Pike-Benton Senior Director, Home Health & Post Acute
The Cost-Effectiveness of Homecare
 The Cost-Effectiveness of Homecare Homecare Reduces Costs by 37 Percent for Heart Failure Patients The May 2004 Journal of the American Geriatrics Society reports a study conducted at six Philadelphia
The Cost-Effectiveness of Homecare Homecare Reduces Costs by 37 Percent for Heart Failure Patients The May 2004 Journal of the American Geriatrics Society reports a study conducted at six Philadelphia
Modern care management
 The care management challenge Health plans and care providers spend billions of dollars annually on care management with the expectation of better utilization management and cost control. That expectation
The care management challenge Health plans and care providers spend billions of dollars annually on care management with the expectation of better utilization management and cost control. That expectation
Philips Hospital to Home: redefining healthcare. through innovation in telehealth
 Philips Hospital to Home: redefining healthcare through innovation in telehealth Healthcare costs are at a crisis point, forcing the federal government to make comprehensive changes to healthcare payment
Philips Hospital to Home: redefining healthcare through innovation in telehealth Healthcare costs are at a crisis point, forcing the federal government to make comprehensive changes to healthcare payment
Reducing Readmissions Using Teach-Back: Enhancing Patient and Family Education.
 Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Reducing Readmissions Using Teach-Back: Enhancing Patient and Family Education. Debra Peter MSN, RN-BC Lehigh Valley Health
Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Reducing Readmissions Using Teach-Back: Enhancing Patient and Family Education. Debra Peter MSN, RN-BC Lehigh Valley Health
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
Improving Transitions & Reducing Readmissions from Skilled Nursing Facilities. Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies
 Improving Transitions & Reducing Readmissions from Skilled Nursing Facilities Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies Agenda Why this is so important What we know: a review of the
Improving Transitions & Reducing Readmissions from Skilled Nursing Facilities Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies Agenda Why this is so important What we know: a review of the