Coordinating Transitions of Care: It Takes a Village
|
|
|
- Gerald Miles
- 10 years ago
- Views:
Transcription
1 Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence

2
3 Situation/Background Patients face significant challenges when moving from one health care setting to another. Poor patient preparedness for transitions of care or incorrect selection of the appropriate post acute level of care can compromise patient safety and patient health outcomes. Nurses, collaborating with our physician partners and the multidisciplinary team, identified opportunities to improve patient safety, quality and the service provided to patients. Here is our story

4 AdvocateCare Programs Coordination of Care Transitions Outpatient Acute Care Post-Acute Embedded Care Managers Multi Condition Centers Advanced Medical Practice Practice Operations Coaches Urgent/ Walk-In Care Community Outreach ED ED Care Coordination Optimization Post-ED Care Transitions Level Of Care Transitions Inpatient Inpatient Readmission Risk Assessment & Focused Interventions Interventions Inpatient Care Inpatient Coordination Care Redesign Coordination Redesign Acute To Post Acute Transitions Acute To Post Acute Transitions Hospital to Home Transition Coach Program SNF Care Model Palliative Care Data & Analytics Population Health Management

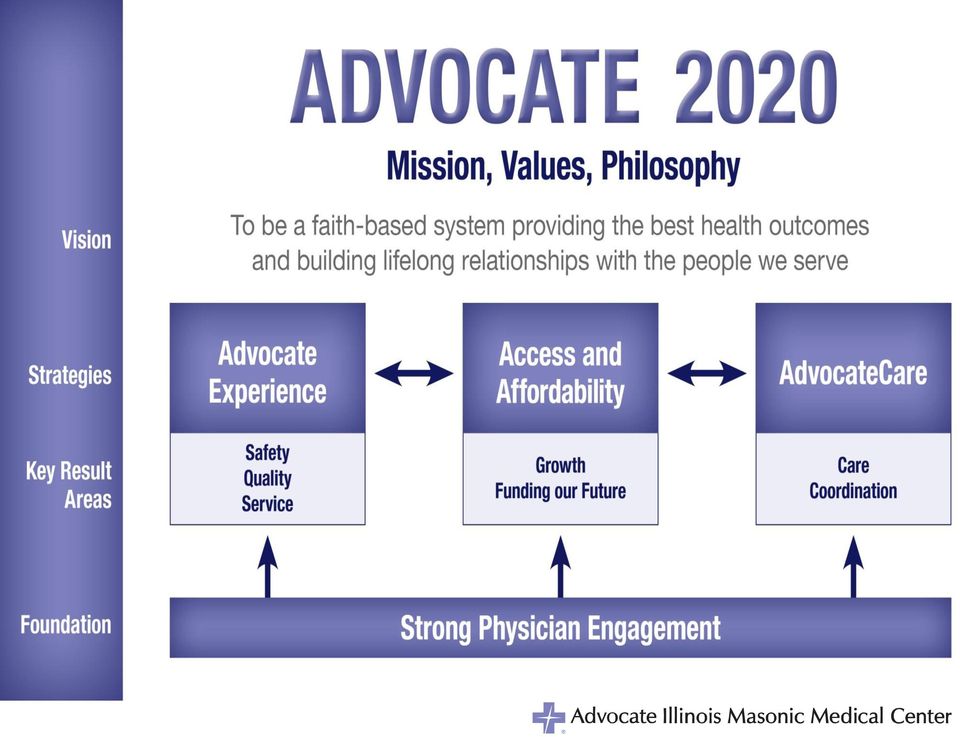
5 KEY QUESTION: How do we integrate care delivery, acute care coordination and transition management into continuum care coordination? Acute Care Coordination + Transitions Guiding Principles* Patient centric care, providing each patient with the right care, at the right time, in the right amount in the proper setting; Achievement of world-class clinical outcomes, guided by the best evidence and practices that are subject to rigorous data analysis and continuous improvement; Patient engagement by challenging, encouraging and ultimately expecting patients to take an active role in their own care management; Reliably exceptional and safe experience for our patients, their families and referring providers wherever they receive care in the system; Effective collaborative partnerships between caregivers across our system and continuum partners; Cost efficient care ensuring resources are available for those activities that impact value the most; and Continuous innovation and improvement by understanding that advances in automation, information technology and training will likely render today s models obsolete in the near future. 5


6 Key Optimization Areas Identified Care Coordination Activities Transitions with Referring Provider/PCP Patient/Family Engagement Nurses provide key care Nurse Case Managers provide coordination Nurses provide activities key care for patient care delivery, and collaborate on care seamless Nurse Case coordination Managers of provide coordination activities for patient care transition care delivery, coordination and collaborate on care between seamless the coordination acute and post-acutesetting between the acute and post-acute- of care Nurses transition innovate coordination and standardize processes Nurses innovate and tools and for standardize managing setting and processes monitoring and patient tools for Nurse Case Managers Innovate and progress managing toward transition standardize Nurse Case processes Managers and Innovate tools to and and monitoring patient progress Innovative toward transition & Standard Processes for support standardize patient processes transitions. and tools to Patient Innovative Education & Standard Processes for support patient transitions. 1. Teach Patient back Education method Implementation of High Yield Ask Teach me 3 back method Transition Implementation Recommendations of High Yield 2. Ask me 3 Transition Recommendations 3. Protected discharge times Going Protected home discharge envelopes times 1.Risk Stratification White Going boards home envelopes 2.Health 1.Risk Care Stratification Team Coordination. 5. White boards 3.Teach 2.Health Back Care Methodology Team Coordination. Patient 6. Hand-offs Education 3.Teach Back Methodology Patient Ensuring 6. Hand-offs accurate information flow 4.Med Education Rec/Adherence to Ensuring the continuum accurate of care information flow to the continuum of care 5.Post 4.Med Acute Rec/Adherence Follow-up Appointment 6.Post 5.Post Acute Acute Partnerships Follow-up Appointment 7.Post-Acute 6.Post Acute Handoffs Partnerships 8.Post-Acute 7.Post-Acute Follow-up Handoffs Call 8.Post-Acute Follow-up Call A common approach to patient and family A common engagement approach in acute to patient care and coordination family engagement and transitions, in acute focuses care on providing coordination patients and and transitions, families with focuses the on right providing information patients in the and right families amount with at the the right information time the in right the way right amount at the right time in the right way standard processes and tools for patient Standard family processes engagement and tools. for 1. patient A and family engagement. 1. AIDET 2. Peer Coaching 2. Peer Coaching Patient Self Management: Patient Self Management: Patient fear and apprehension is reduced Patient as fear the and patient apprehension is prepared is for transition reduced through as the patient teach back is prepared education for methods transition at the through literacy teach level back and education language methods of at the the patient literacy level and language of the patient

7 The AIMMC Approach to Perfect Transitions Nursing Physician and Multidisciplinary Team Nursing Case Management Ready, Set, Go, Phase 1 Literacy, Education Process Improvement Tools Ready, Set, Go, Phase 2 Knowledge and skills competency validation and emphasis on discharge education. Assessing and documenting the patient preferred learning method, ability to learn, barriers and outcomes Ready, Set, Go, Phase 3 Monitoring and evaluation practice change to ensure sustainability Bedside shift report Provide and receive information from nursing and nursing case management Collaborative sharing of information to coordinate care and patient transitions Ensure patient care is delivered in the most appropriate setting and if the Acute Setting the most appropriate Level of care. Connect Unassigned Patients to PCP s Initiate risk readmission stratification tool Work with PCP to arrange post acute follow up visit prior to discharge Recommend In-Network home health, home infusion, therapies, SNF s to better manage transitions back to PCP/Specialists and to reduce readmissions. Educate patients regarding the importance and benefit of coordinated care within the Advocate system

8 Ready, Set, Go! Innovation and Peer Support Launch our Patients to a Successful Discharge The purpose of the CPC process improvement project was to improve the patient discharge process in an acute care facility with an outcome measure of patient satisfaction scores.

9 Iowa Model EBP Implementation: Phase I Direct Care RNs on discharge team identified key areas for improvement: Health Literacy Process Improvement Protected discharge time Going home envelopes Patient and Staff Education: EMR patient discharge resources Teach back technique CBT with contact hours awarded upon quiz completion Peer Coaching



10 Phase I: How to use the Teach Back Technique Healthcare providers ask patients to state in their own words (i.e. teach back) key concepts, decisions, or instructions just discussed. What is my main problem? What do I need to do? Why is it important for me to do this?

11 Iowa Model EBP Implementation Phase II: Knowledge and Skills Competency Validation Emphasis on Discharge Education

12 Iowa Model EBP Implementation Phase III: Monitoring and Evaluating Practice Change Ensuring Sustainability 1. Ongoing monthly documentation audits 1. Conducted by Discharge Team Members 2. Peer coaching 2. Continued emphasis regarding teach back technique 3. Reinforcing protected discharge time during patient/family discharge teaching (sign on door, others covering call lights, etc). 4. Discharge CBT: 1. New on boarding requirement for GNO and RN Residency 2. Updated on an annual basis 5. All units to utilize the yellow Going Home envelopes for the written discharge instructions
. 4.")
13 Results: Stay Tuned!

14 AdvocateCare Post Acute Transitions The Long Walk Home Just Got Easier for Advocate Patients


15 VSA Scope Post Acute Transition LTACH Home w/home Care

16 Post-Acute Referral Decision Process This decision tree does not cover all dispositions Care Managers to consider other post-acute care options such as assisted living, custodial care, palliative care etc. as appropriate This decision process starts with discharge planning assessment on admission and is re-assessed daily. The goal is to ANTICIPATE DISCHARGE needs as early as possible, to explore alternatives, and advance as needed. Re-admission risk assessment also completed (within 24 hours) Re-assess daily and develop alternate plans until clarity emerges Unclear Will patient be safe and appropriate to go home? Yes Patient meets criteria for Home Care?* Yes Refer to Home Care No No Patient transitions to Home Patient transitions to SNF* No Will patient need post-acute hospital level care? (if unclear, consult Physiatry) Is patient s risk score >=8? # Yes Refer to Transition Program** No Yes Patient transitions to LTACH* Medical Will primary need be functional recovery or medical? Functional Patient transitions to Acute Inpatient Rehab* Note: In general, acute spinal cord and brain injury patients and complex stroke are most appropriate for acute inpatient rehab * Patient meets criteria based on applicable Milliman guidelines. Refer to Post-Acute Service Availability Grid; Home Care patients must meet home-bound status ** Transition program offered by Advocate at Home: check with your site for availability and specific patient inclusion criteria # The readmission risk tool should be used in conjunction with sound clinical judgment when used to help determine post acute care setting and/or intensity. The expected probability of readmission increases with an increase in score, but for any individual patient, other factors (i.e. literacy, social, financial) may impact whether or not the patient actually is actually readmitted
 Re-assess daily and develop alternate plans until clarity emerges Unclear Will patient be safe and appropriate to go home?")

17


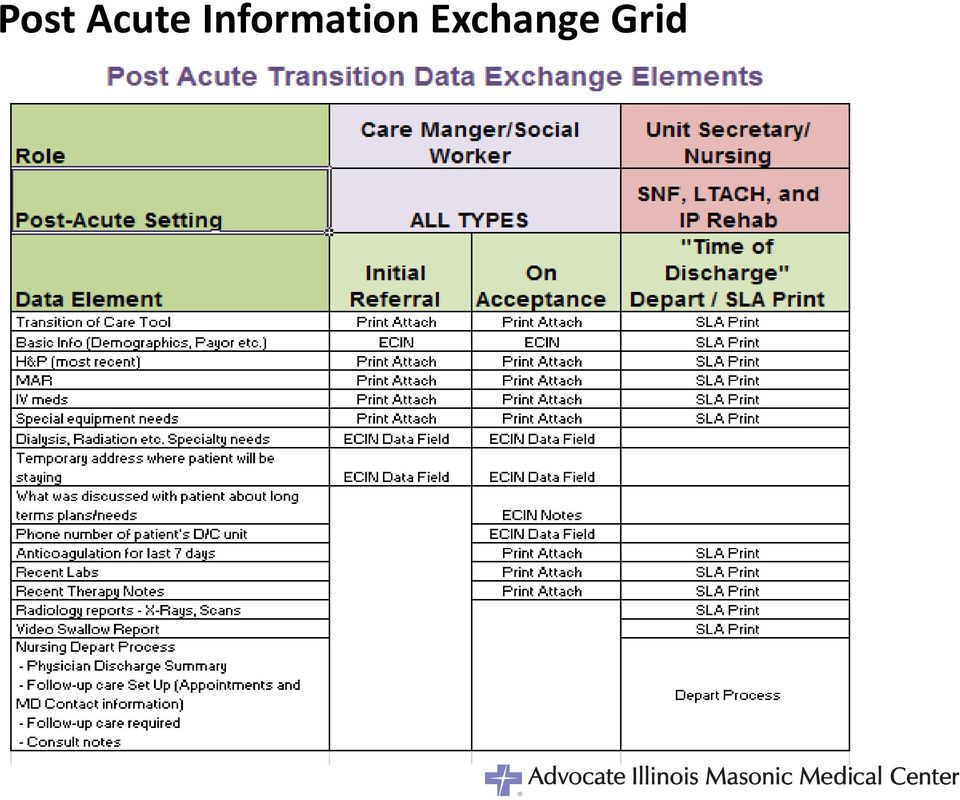
18 Post Acute Information Exchange Grid
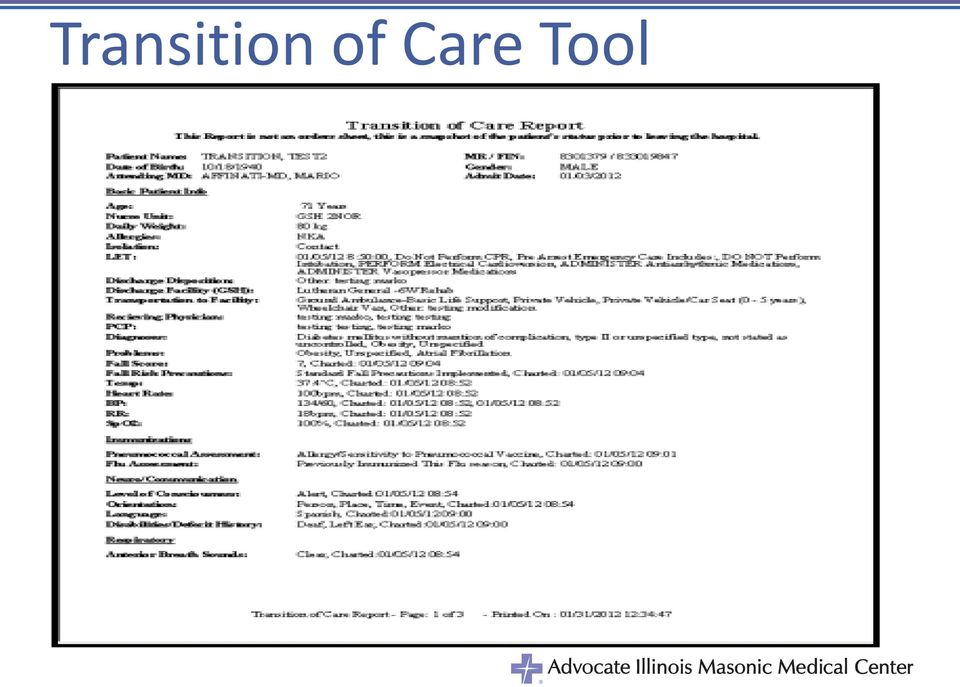
19 Transition of Care Tool
20 Measurement: HCAPHS Discharge Domain: Patient satisfaction with the service we provide 30 Day-Readmissions: Transitioning patients to the right level of care at the right time. A patient readmitted within 30 days of transition is being correlated with substandard quality Results accentuated by the dual approach

21 HCAHPS Two Global Questions: 1. What number would you use to rate this hospital during your stay? (1 to 10) 2. Would you recommend this hospital to your family and friends? 7 Domains 1. Communication with Nurses 2. Responsiveness of Hospital Staff 3. Communication with physicians 4. Cleanliness and quietness of environment 5. Pain Control 6. Communication about Medications 7. Discharge Instructions
22 Milestones and Outcomes of Discharge Education Project KRA Benchmark 2010 COTH All Press Ganey DB AIMMC Inpatient - Patient Satisfaction with Discharge HCAHPS Discharge Domain Percentile Ranks by Discharge Date (KRA Benchmark) Surveys Returned (Quarterly Avg) May 2009 First Discharge Team Meeting: Goals Set PowerPoint Drafted February 2010 Presentation of Discharge Policies to CPC Intervention Preliminary Data Q Q Q Q Q Q Q Q August 2009 Development of Discharge Policies for ED and Inpatient February 2010 Rollout of CareConnection view module August 2010 Inpatient and ED Discharge Policies published online INTERVENTION November 2010 CBTs available in ALEX, including INA credit for quiz completion January 2011 CBT quiz completion & skills validation for Inpatient and ED nurses April 2011 Monthly chart audits begin (tracking documentation compliance)

23 Care Transition HCAHPS Continue to Exceed Target AIMMC Leads System 23

24 Hospital Readmissions Prevalent (CMS, 2012) National rate ~ 17% National average ~ 19% for Medicare beneficiaries Highest in Chicago Hospital Region ~27%
25 How Are We Doing? Discharged and Readmitted to AIMMC: Great!!!!! Rolling 6 month all patients: 9.3% - AIMMC and LGH Top Quartile performers nationally Medicare: 15% Medicaid: 7.1% BCBSI attributed: Discharged and Readmitted to any Hospital: OFI Medicare: PEPPER Report: Includes Behavioral Health, Acute Rehab CHF: 24.7% - Same as: Pneumonia: 19.7% -Same as: AMI: 15.5% - Same As: BCBSI: Advocatecare Index: Solid Medicaid: OFI
26 AIMMC Adult Acute Care 30 Day Readmissions 2010 Baseline 2011 Target 2012 Target 11.6% 11.3% 11.0% January February March April May % 8.8% 10.9% 9.2% 9.0% 8.6% 9.5% 9.5% June Rolling 6 Month Average 2012 YTD Percent Readmission by Discharge Disposition Percent Readmission by Payer Percent Medicare Readmission by Diagnosis 2010 Baseline 2010 Baseline State Benchmark 2011 Target 2011 Target National Benchmark 2012 Target Total Skilled Nursing Facilities 24% 18% 18% Long Term Acute Care 12% 12% 12% Total Home Health Care 13% 11% 10% Total Home/Self Care 9% 8% 8% All Other Dispositions 11% 11% 11% 2012 Target Medicare 18% 17% 15% Medicaid 15% 12% 11% Blue Cross Blue Shield of Illinois 8% 7% 6% All Other Managed Care 9% 8% 7% Other 11% 11% 10% 2012 Target Pneumonia* 19.1% 18.3% 17.5% January February March April May % 12.2% 13.5% 15.2% 15.9% 10.7% 13.2% 13.2% % 14.3% 14.3% 0.0% 0.0% 14.3% 9.5% 9.5% % 7.5% 9.5% 5.8% 8.1% 7.2% 7.8% % 8.8% 9.5% 10.2% 8.1% 7.2% 9.0% 9.0% % 6.2% 16.5% 8.3% 3.2% 14.1% 11.1% 11.1% Rolling 6 Month January February March April May June 2012 YTD Average % 11.4% 14.4% 12.7% 12.3% 10.7% 13.1% 13.1% % 12.7% 10.0% 5.9% 5.0% 3.8% 7.1% 7.1% % 6.1% 6.0% 6.1% 8.7% 9.2% 6.9% 6.9% % 4.4% 10.2% 9.0% 6.9% 6.4% 7.0% 7.0% % 8.8% 10.1% 7.9% 6.8% 10.9% 8.8% 8.8% January February March April May Rolling 6 Month Average 2012 YTD % 16.1% 8.6% 12.5% 10.0% 5.3% 11.3% 11.3% June June Rolling 6 M onth Average 2012 YTD 7.8%
27 Performance Improvement Results: Look What We Have Accomplished. We Are Ahead of the Curve! Improved safety, quality care and patient service Improved care coordination Reduced readmissions Improved patient satisfaction results Increases staff satisfaction
28 Patient Preparedness for Transition Home Care Skills: Expected behaviors for patient or family member/significant other to demonstrate prior to discharge Communicate understanding of disease process Communicate signs and symptoms of complications Know when to call physician or to call or return to the hospital Demonstrate necessary skills for home care by teach back

29 Care Transition Management Past State: Discharge Planning Focus on discharge out of hospital Risk Stratification Target patients at highest risk Standardized across system Focus Areas by Organizational Accountability Hospital Medication Management Patient Self-Management Post Acute Follow-up Skilled Nursing Facilities Palliative Care Current State: Transition Management Focus on transitioning from within hospital to next setting Physician Hand-offs Post Acute Follow-up Palliative Care
30 Realities in Healthcare Today Key market realities throughout the remainder of the decade We will be judged by the value we provide for the overall health of the population we serve The bar for safety, quality and service will continue to be raised We must decrease cost since we will be paid less for the same service There will be financial penalties for complications in care delivery


31 Stakeholders working together Physicians/Nurses/NCT s/case Manager/LCSW/Post Acute Partners Patient
32 We are a community of HealthCare Providers, and It takes a Village to safely transition a patient
A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates. April 11, 2014
 A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates April 11, 2014 About the QIO Program Leading rapid, large-scale change in health quality: Goals are bolder. The patient is at
A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates April 11, 2014 About the QIO Program Leading rapid, large-scale change in health quality: Goals are bolder. The patient is at
Care Coordination at Frederick Regional Health System. Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care
 Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Get With The Guidelines - Stroke PMT Special Initiatives Tab for Ohio Coverdell Stroke Program CODING INSTRUCTIONS Effective 10-24-15
 Get With The Guidelines - Stroke PMT Special Initiatives Tab for Ohio Coverdell Stroke Program CODING INSTRUCTIONS Effective 10-24-15 Date and time first seen by ED MD: The time entered should be the earliest
Get With The Guidelines - Stroke PMT Special Initiatives Tab for Ohio Coverdell Stroke Program CODING INSTRUCTIONS Effective 10-24-15 Date and time first seen by ED MD: The time entered should be the earliest
PREVENTING HEART FAILURE READMISSIONS
 PREVENTING HEART FAILURE READMISSIONS Tanya Sprinkle, BSN, RN, CCM Patient and Family Services Coordinator [email protected] 704-878-4534 Michelle Roseman, NHA, MBA Chief Operating Officer/Catawba
PREVENTING HEART FAILURE READMISSIONS Tanya Sprinkle, BSN, RN, CCM Patient and Family Services Coordinator [email protected] 704-878-4534 Michelle Roseman, NHA, MBA Chief Operating Officer/Catawba
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates
 Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015
 Leveraging the Continuum to Avoid Unnecessary Utilization While Improving Quality Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015 Karim A. Habibi, FHFMA, MPH, MS Senior
Leveraging the Continuum to Avoid Unnecessary Utilization While Improving Quality Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015 Karim A. Habibi, FHFMA, MPH, MS Senior
Elim Park Health Care Center. Clinical Excellence and Quality Report
 2014 Elim Park Health Care Center Clinical Excellence and Quality Report Welcome to Elim Park Health Care Center s 2014 Clinical Excellence and Quality Report. We have been providing patient focused quality
2014 Elim Park Health Care Center Clinical Excellence and Quality Report Welcome to Elim Park Health Care Center s 2014 Clinical Excellence and Quality Report. We have been providing patient focused quality
Ann Hablitzel, RN, BSN, MBA Hospice Care of California
 Ann Hablitzel, RN, BSN, MBA Hospice Care of California Objectives Describe the creations of new community based palliative care programs Identify criteria for admission Discuss philosophy and goals Analyze
Ann Hablitzel, RN, BSN, MBA Hospice Care of California Objectives Describe the creations of new community based palliative care programs Identify criteria for admission Discuss philosophy and goals Analyze
Nurse Credentialing: How to Impact Patient Outcomes in the Marketplace
 Nurse Credentialing: How to Impact Patient Outcomes in the Marketplace Donna King, BSN, MBA, RN, NE-BC, FACHE Vice President, Clinical Operations/Chief Nurse Executive Overview... About Advocate Health
Nurse Credentialing: How to Impact Patient Outcomes in the Marketplace Donna King, BSN, MBA, RN, NE-BC, FACHE Vice President, Clinical Operations/Chief Nurse Executive Overview... About Advocate Health
1. Executive Summary Problem/Opportunity: Evidence: Baseline Data: Intervention: Results:
 A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS. Karen Unholz, RN, BSN
 INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
How To Manage Health Care Needs
 HEALTH MANAGEMENT CUP recognizes the importance of promoting effective health management and preventive care for conditions that are relevant to our populations, thereby improving health care outcomes.
HEALTH MANAGEMENT CUP recognizes the importance of promoting effective health management and preventive care for conditions that are relevant to our populations, thereby improving health care outcomes.
Mount Sinai Rehabilitation Center. 2014 Outcomes. Mount Sinai Rehabilitation Center 2014 Outcomes
 Mount Sinai Rehabilitation Center 2014 Outcomes Mount Sinai Rehabilitation Center 2014 Outcomes TABLE OF CONTENTS A Message from the Chair... 3 About Our Programs. 4-5 Inpatient Rehabilitation. 6-12 Outpatient
Mount Sinai Rehabilitation Center 2014 Outcomes Mount Sinai Rehabilitation Center 2014 Outcomes TABLE OF CONTENTS A Message from the Chair... 3 About Our Programs. 4-5 Inpatient Rehabilitation. 6-12 Outpatient
CCNC Care Management
 CCNC Care Management Community Care of North Carolina (CCNC) is a statewide population management and care coordination infrastructure founded on the primary care medical home model. CCNC incorporates
CCNC Care Management Community Care of North Carolina (CCNC) is a statewide population management and care coordination infrastructure founded on the primary care medical home model. CCNC incorporates
Readmissions as an Enterprise Priority. Presenters 4/17/2014
 Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center [email protected] Eileen
Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center [email protected] Eileen
Patients Receive Recommended Care for Community-Acquired Pneumonia
 Patients Receive Recommended Care for Community-Acquired Pneumonia For New Jersey to be a state in which all people live long, healthy lives. DSRIP LEARNING COLLABORATIVE PRESENTATION The Care you Trust!
Patients Receive Recommended Care for Community-Acquired Pneumonia For New Jersey to be a state in which all people live long, healthy lives. DSRIP LEARNING COLLABORATIVE PRESENTATION The Care you Trust!
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION
 Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Five Myths Surrounding the Business of Population Health Management
 Five Myths Surrounding the Business of Population Health Management Joan Moss, RN, MSN Robert Sehring Chief Nursing Officer and Chief Ministry Services Officer, Senior Vice President, Sg2 OSF HealthCare
Five Myths Surrounding the Business of Population Health Management Joan Moss, RN, MSN Robert Sehring Chief Nursing Officer and Chief Ministry Services Officer, Senior Vice President, Sg2 OSF HealthCare
Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services
 Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services Objectives Understand the new consequences to hospitals for discharged clients being re-admitted within selected time
Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services Objectives Understand the new consequences to hospitals for discharged clients being re-admitted within selected time
Chapter 4 Health Care Management Unit 1: Care Management
 Chapter 4 Health Care Unit 1: Care In This Unit Topic See Page Unit 1: Care Care 2 6 Emergency 7 4.1 Care Healthcare Healthcare (HMS), Highmark Blue Shield s medical management division, is responsible
Chapter 4 Health Care Unit 1: Care In This Unit Topic See Page Unit 1: Care Care 2 6 Emergency 7 4.1 Care Healthcare Healthcare (HMS), Highmark Blue Shield s medical management division, is responsible
High Desert Medical Group Connections for Life Program Description
 High Desert Medical Group Connections for Life Program Description POLICY: High Desert Medical Group ("HDMG") promotes patient health and wellbeing by actively coordinating services for members with multiple
High Desert Medical Group Connections for Life Program Description POLICY: High Desert Medical Group ("HDMG") promotes patient health and wellbeing by actively coordinating services for members with multiple
Reducing Avoidable Readmissions Effectively (RARE) Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement
 Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement") Reducing Avoidable Readmissions Effectively (RARE) Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement Martha and James Acute Episodes Family Doctor Life Expectancy from chronic diseases
Reducing Avoidable Readmissions Effectively (RARE) Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement Martha and James Acute Episodes Family Doctor Life Expectancy from chronic diseases
Connect4 Patients CCCM Primary Care Community. Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM
 Connect4 Patients CCCM Primary Care Community Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM September 17, 2015 Objectives: Describe innovative care management
Connect4 Patients CCCM Primary Care Community Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM September 17, 2015 Objectives: Describe innovative care management
BUNDLING ARE INPATIENT REHABILITATION FACILITIES PREPARED FOR THIS PAYMENT REFORM?
 BUNDLING ARE INPATIENT REHABILITATION FACILITIES PREPARED FOR THIS PAYMENT REFORM? Uniform Data System for Medical Rehabilitation Annual Conference August 10, 2012 Presented by: Donna Cameron Rich Bajner
BUNDLING ARE INPATIENT REHABILITATION FACILITIES PREPARED FOR THIS PAYMENT REFORM? Uniform Data System for Medical Rehabilitation Annual Conference August 10, 2012 Presented by: Donna Cameron Rich Bajner
Henry Ford Health System Care Coordination and Readmissions Update
 Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
2.b.vii Implementing the INTERACT Project (Inpatient Transfer Avoidance Program for SNF)
") 2.b.vii Implementing the INTERACT Project (Inpatient Transfer Avoidance Program for SNF) Project Objective: Skilled nursing facilities (SNFs) will implement the evidence based INTERACT program developed
2.b.vii Implementing the INTERACT Project (Inpatient Transfer Avoidance Program for SNF) Project Objective: Skilled nursing facilities (SNFs) will implement the evidence based INTERACT program developed
How To Reduce Hospital Readmission
 Reducing Hospital Readmissions & The Affordable Care Act The Game Has Changed Drastically Reducing MSPB Measures Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE
Reducing Hospital Readmissions & The Affordable Care Act The Game Has Changed Drastically Reducing MSPB Measures Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE
3/11/15. COPD Disease Management Tackling the Transition. Objectives. Describe the multidisciplinary approach to inpatient care for COPD patients
 Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
RT AS PROJECT MANAGER:
 RT AS PROJECT MANAGER: IMPROVING CARE TRANSITIONS DECREASES UNPLANNED READMISSIONS TAMMY JARNAGIN, BHS, RRT DIRECTOR CARDIOPULMONARY SERVICES, NEURODIAGNOSTICS, HOME MEDICAL EQUIPMENT Objectives Recognize
RT AS PROJECT MANAGER: IMPROVING CARE TRANSITIONS DECREASES UNPLANNED READMISSIONS TAMMY JARNAGIN, BHS, RRT DIRECTOR CARDIOPULMONARY SERVICES, NEURODIAGNOSTICS, HOME MEDICAL EQUIPMENT Objectives Recognize
Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights
 Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights Emily Brower Executive Director Accountable Care Programs [email protected] November 2013 1 Contents Overview of
Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights Emily Brower Executive Director Accountable Care Programs [email protected] November 2013 1 Contents Overview of
Sharp HealthCare ACO. Pioneer Introduction to the FSSB November 8, 2012
 Sharp HealthCare ACO Pioneer Introduction to the FSSB November 8, 2012 Sharp HealthCare Not-for-profit serving 3.1 million residents of San Diego County Grew from one hospital in 1955 to an integrated
Sharp HealthCare ACO Pioneer Introduction to the FSSB November 8, 2012 Sharp HealthCare Not-for-profit serving 3.1 million residents of San Diego County Grew from one hospital in 1955 to an integrated
PCMH and Care Management: Where do we start?
 PCMH and Care Management: Where do we start? Patricia Bohs, RN, BSN Quality Assurance Manager Kelly McCloughan QA Data Manager Wayne Memorial Community Health Centers Honesdale, PA Wayne Memorial Community
PCMH and Care Management: Where do we start? Patricia Bohs, RN, BSN Quality Assurance Manager Kelly McCloughan QA Data Manager Wayne Memorial Community Health Centers Honesdale, PA Wayne Memorial Community
Innovations@Home. Home Health Initiatives Reduce Avoidable Readmissions by Leveraging Innovation
 How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
Integrating Post-Acute Providers with Health System Strategies
 Integrating Post-Acute Providers with Health System Strategies Bridging the Acute and Post-Acute Worlds The opinions expressed are those of the presenter and do not necessarily state or reflect the views
Integrating Post-Acute Providers with Health System Strategies Bridging the Acute and Post-Acute Worlds The opinions expressed are those of the presenter and do not necessarily state or reflect the views
Stakeholder s Report. 2525 SW 75 th Ave Miami, Florida 33155 305.262.6800 www.westgablesrehabhospital.com
 212 Stakeholder s Report 2525 SW 75 th Ave Miami, Florida 33155 35.262.68 www.westgablesrehabhospital.com PROFILE REPORT For more than 25 years, West Gables Rehabilitation Hospital has made a mission of
212 Stakeholder s Report 2525 SW 75 th Ave Miami, Florida 33155 35.262.68 www.westgablesrehabhospital.com PROFILE REPORT For more than 25 years, West Gables Rehabilitation Hospital has made a mission of
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System
 Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
Disease Management Identifications and Stratification Health Risk Assessment Level 1: Level 2: Level 3: Stratification
 Disease Management UnitedHealthcare Disease Management (DM) programs are part of our innovative Care Management Program. Our Disease Management (DM) program is guided by the principles of the UnitedHealthcare
Disease Management UnitedHealthcare Disease Management (DM) programs are part of our innovative Care Management Program. Our Disease Management (DM) program is guided by the principles of the UnitedHealthcare
Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions
 Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions Leslie Becker RN, BS Jennifer Smith RN, MSN, MBA Leslie Frain MSN, RN Jan Machanis
Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions Leslie Becker RN, BS Jennifer Smith RN, MSN, MBA Leslie Frain MSN, RN Jan Machanis
Game Changer at the Primary Care Practice Embedded Care Management. Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012
 Game Changer at the Primary Care Practice Embedded Care Management Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012 Objectives To describe the recent evolution of care management at
Game Changer at the Primary Care Practice Embedded Care Management Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012 Objectives To describe the recent evolution of care management at
CCNC Care Management Standardized Plan
 Standardization & Reporting: Why is standardization important? Community Care Networks are responsible for the delivery of targeted care management services that will improve quality of care while containing
Standardization & Reporting: Why is standardization important? Community Care Networks are responsible for the delivery of targeted care management services that will improve quality of care while containing
CHANGING YOUR CASE MANAGEMENT MODEL OF CARE. Jan Lear, RN, CMC Director of Case Management MedStar Franklin Square Medical Center
 CHANGING YOUR CASE MANAGEMENT MODEL OF CARE Jan Lear, RN, CMC Director of Case Management MedStar Franklin Square Medical Center 1 Program Objectives To be able to describe the compliance and regulatory
CHANGING YOUR CASE MANAGEMENT MODEL OF CARE Jan Lear, RN, CMC Director of Case Management MedStar Franklin Square Medical Center 1 Program Objectives To be able to describe the compliance and regulatory
WHITE PAPER. How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience
 WHITE PAPER How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience Vocera Communications, Inc. June, 2014 SUMMARY Hospitals that reduce readmission rates
WHITE PAPER How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience Vocera Communications, Inc. June, 2014 SUMMARY Hospitals that reduce readmission rates
Empowering Value-Based Healthcare
 Empowering Value-Based Healthcare Episode Connect, Remedy s proprietary suite of software applications, is a powerful platform for managing value-based payment programs. Delivered via the web or mobile
Empowering Value-Based Healthcare Episode Connect, Remedy s proprietary suite of software applications, is a powerful platform for managing value-based payment programs. Delivered via the web or mobile
WHITE PAPER. 9 Steps to Better Patient Flow and Decreased Readmissions in Your Emergency Department
 Communication Solutions WHITE PAPER 9 Steps to Better Patient Flow and Decreased Readmissions in Your Emergency Department Increase patient satisfaction and reduce readmissions all while building loyalty,
Communication Solutions WHITE PAPER 9 Steps to Better Patient Flow and Decreased Readmissions in Your Emergency Department Increase patient satisfaction and reduce readmissions all while building loyalty,
Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education
 1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
Patient Experience. The Cleveland Clinic Journey. American Medical Group Association Orlando, Florida March 14, 2013
 Patient Experience The Cleveland Clinic Journey American Medical Group Association Orlando, Florida March 14, 2013 James Merlino, MD Chief Experience Officer Overview How did Cleveland Clinic change their
Patient Experience The Cleveland Clinic Journey American Medical Group Association Orlando, Florida March 14, 2013 James Merlino, MD Chief Experience Officer Overview How did Cleveland Clinic change their
Care Coordination. The Embedded Care Manager. Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed
 Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
Population Health Solutions for Employers MEDIA RESOURCES
 Population Health Solutions for Employers MEDIA RESOURCES ABOUT MISSIONPOINT MissionPoint s mission is to make healthcare more affordable, accessible and improve the quality of care for our members. MissionPoint
Population Health Solutions for Employers MEDIA RESOURCES ABOUT MISSIONPOINT MissionPoint s mission is to make healthcare more affordable, accessible and improve the quality of care for our members. MissionPoint
Empowering Value-Based Healthcare
 Empowering Value-Based Healthcare Episode Connect, Remedy s proprietary suite of software applications, is a powerful platform for managing value based payment programs. Delivered via the web or mobile
Empowering Value-Based Healthcare Episode Connect, Remedy s proprietary suite of software applications, is a powerful platform for managing value based payment programs. Delivered via the web or mobile
Standards of Practice & Scope of Services. for Health Care Delivery System Case Management and Transitions of Care (TOC) Professionals
 Professionals") A M E R I C A N C A S E M A N A G E M E N T A S S O C I A T I O N Standards of Practice & Scope of Services for Health Care Delivery System Case Management and Transitions of Care (TOC) Professionals O
A M E R I C A N C A S E M A N A G E M E N T A S S O C I A T I O N Standards of Practice & Scope of Services for Health Care Delivery System Case Management and Transitions of Care (TOC) Professionals O
The Third National Medicare RAC Summit
 The Third National Medicare RAC Summit Major Hospital Vulnerabilities II: Medical Necessity and Clinical Documentation Issues in Medicaid and RAC Audits Edmund L. Lafer, MD Temple University Health System
The Third National Medicare RAC Summit Major Hospital Vulnerabilities II: Medical Necessity and Clinical Documentation Issues in Medicaid and RAC Audits Edmund L. Lafer, MD Temple University Health System
Transitions of Care Management Coding (TCM Code) Tutorial. 1. Introduction Meaning of moderately and high complexity 2
 Tutorial. 1. Introduction Meaning of moderately and high complexity 2") Transitions of Care Management Coding (TCM Code) Tutorial Index 1. Introduction Meaning of moderately and high complexity 2 2. SETMA s Tools for using TCM Code 3 Alert that patient is eligible for TCM
Transitions of Care Management Coding (TCM Code) Tutorial Index 1. Introduction Meaning of moderately and high complexity 2 2. SETMA s Tools for using TCM Code 3 Alert that patient is eligible for TCM
Home Care s Pivotal Role in Patient Transitions from Acute to Post Acute Care Settings:
 Home Care s Pivotal Role in Patient Transitions from Acute to Post Acute Care Settings: Experiences of a Successful CCTP Program And So Much More! Jane Pike-Benton Senior Director, Home Health & Post Acute
Home Care s Pivotal Role in Patient Transitions from Acute to Post Acute Care Settings: Experiences of a Successful CCTP Program And So Much More! Jane Pike-Benton Senior Director, Home Health & Post Acute
CURRENT AND FUTURE TRENDS IN POST ACUTE CARE The Value and Role of Acute Inpatient Rehab
 CURRENT AND FUTURE TRENDS IN POST ACUTE CARE The Value and Role of Acute Inpatient Rehab Robert S. Djergaian, M.D. Medical Director Banner Good Samaritan Rehabilitation Institute Stewardship Profitability
CURRENT AND FUTURE TRENDS IN POST ACUTE CARE The Value and Role of Acute Inpatient Rehab Robert S. Djergaian, M.D. Medical Director Banner Good Samaritan Rehabilitation Institute Stewardship Profitability
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT. Norris Vivatrat, MD Associate Medical Director Monarch HealthCare
 PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
What is an Accountable Care Organization & Why is it Important to Your Home Infusion Company?
 What is an Accountable Care Organization & Why is it Important to Your Home Infusion Company? Lisa Harvey McPherson RN, MBA, MPPM EMHS Vice President Continuum of Care & Chief Advocacy Officer Disclosures
What is an Accountable Care Organization & Why is it Important to Your Home Infusion Company? Lisa Harvey McPherson RN, MBA, MPPM EMHS Vice President Continuum of Care & Chief Advocacy Officer Disclosures
HealthCare Partners of Nevada. Heart Failure
 HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
What do ACO s and Hospitals want from SNF s and CCRC s
 What do ACO s and Hospitals want from SNF s and CCRC s Presented to the Institute of Senior Living, April 11, 2013 A Division of Kindred Healthcare 1 Assessing the match: What hospitals and ACO s currently
What do ACO s and Hospitals want from SNF s and CCRC s Presented to the Institute of Senior Living, April 11, 2013 A Division of Kindred Healthcare 1 Assessing the match: What hospitals and ACO s currently
Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions
 Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions Scott Flinn MD Deborah Schutz RN JD Fritz Steen RN Arch Health Partners A medical foundation formed
Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions Scott Flinn MD Deborah Schutz RN JD Fritz Steen RN Arch Health Partners A medical foundation formed
Synchronous vs. Asynchronous Communications in Virtual Care. Robert Smith, MD, FAAFP Co-Founder, NowDox
 Synchronous vs. Asynchronous Communications in Virtual Care Robert Smith, MD, FAAFP Co-Founder, NowDox #DHC12 @NYeHealth Synchronous & Asynchronous Communications In Virtual Care Robert L. Smith, MD, FAAFP
Synchronous vs. Asynchronous Communications in Virtual Care Robert Smith, MD, FAAFP Co-Founder, NowDox #DHC12 @NYeHealth Synchronous & Asynchronous Communications In Virtual Care Robert L. Smith, MD, FAAFP
Health Care Leader Action Guide to Reduce Avoidable Readmissions
 Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
Patient to Person. Transitions of Care. Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM
 Patient to Person Transitions of Care Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM Transitions of Care Transitioning from school to adult services (vocational, medical day, etc.)
Patient to Person Transitions of Care Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM Transitions of Care Transitioning from school to adult services (vocational, medical day, etc.)
Post-Acute Care Transitions: An Essential Component of Accountable Care
 : An Essential Component of Accountable Care Bruce C. Smith, MD, FACP Associate Medical Director, Strategy Deployment Group Health Physicians, Seattle, WA [email protected] AMGA 2012 Institute for Quality
: An Essential Component of Accountable Care Bruce C. Smith, MD, FACP Associate Medical Director, Strategy Deployment Group Health Physicians, Seattle, WA [email protected] AMGA 2012 Institute for Quality
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services. Discharge Planning
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services ICN 908184 October 2014 This booklet was current at the time it was published or uploaded onto the web. Medicare policy
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services ICN 908184 October 2014 This booklet was current at the time it was published or uploaded onto the web. Medicare policy
CHAPTER 535 HEALTH HOMES. Background... 2. Policy... 2. 535.1 Member Eligibility and Enrollment... 2. 535.2 Health Home Required Functions...
 TABLE OF CONTENTS SECTION PAGE NUMBER Background... 2 Policy... 2 535.1 Member Eligibility and Enrollment... 2 535.2 Health Home Required Functions... 3 535.3 Health Home Coordination Role... 4 535.4 Health
TABLE OF CONTENTS SECTION PAGE NUMBER Background... 2 Policy... 2 535.1 Member Eligibility and Enrollment... 2 535.2 Health Home Required Functions... 3 535.3 Health Home Coordination Role... 4 535.4 Health
ST JOHN S LUTHERAN MINISTRIES. Kent Burgess President & CEO
 ST JOHN S LUTHERAN MINISTRIES Kent Burgess President & CEO WHAT S CHANGING MAYBE? -The way we get paid (Reduce Cost) -The way we get measured (Better Care) -What will be required of us (More) -Partnerships/Affiliations
ST JOHN S LUTHERAN MINISTRIES Kent Burgess President & CEO WHAT S CHANGING MAYBE? -The way we get paid (Reduce Cost) -The way we get measured (Better Care) -What will be required of us (More) -Partnerships/Affiliations
Changing the culture of any organization is well known to be a long process,
 Creative Nursing, Volume 18, Issue 4, 2012 Impact of Unit Practice Councils on Culture and Outcomes Susan Wessel, MS, MBA, RN, NEA-BC This article describes positive outcomes in culture, Hospital Consumer
Creative Nursing, Volume 18, Issue 4, 2012 Impact of Unit Practice Councils on Culture and Outcomes Susan Wessel, MS, MBA, RN, NEA-BC This article describes positive outcomes in culture, Hospital Consumer
National Stroke Association s Guide to Choosing Stroke Rehabilitation Services
 National Stroke Association s Guide to Choosing Stroke Rehabilitation Services Rehabilitation, often referred to as rehab, is an important part of stroke recovery. Through rehab, you: Re-learn basic skills
National Stroke Association s Guide to Choosing Stroke Rehabilitation Services Rehabilitation, often referred to as rehab, is an important part of stroke recovery. Through rehab, you: Re-learn basic skills
TRUSTED PATIENT EDUCATION FOR BETTER OUTCOMES. MICROMEDEX Patient Connect. Patient Education & Engagement
 TRUSTED PATIENT EDUCATION FOR BETTER OUTCOMES MICROMEDEX Patient Connect Patient Education & Engagement Trusted Patient Education for Better Outcomes All your training, experience, tools, and technology
TRUSTED PATIENT EDUCATION FOR BETTER OUTCOMES MICROMEDEX Patient Connect Patient Education & Engagement Trusted Patient Education for Better Outcomes All your training, experience, tools, and technology
Population Health Management: Banner Health Network s Perspective. Neta Faynboym, Medical Director Banner Health Network
 Population Health Management: Banner Health Network s Perspective Neta Faynboym, Medical Director Banner Health Network 29 Acute Care Hospitals BANNER AT A GLANCE Banner Health Network with 400K lives
Population Health Management: Banner Health Network s Perspective Neta Faynboym, Medical Director Banner Health Network 29 Acute Care Hospitals BANNER AT A GLANCE Banner Health Network with 400K lives
2014 Model of Care Training SHP_2014838A
 2014 Model of Care Training SHP_2014838A 1 Model of Care Training This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plans. It also ensures
2014 Model of Care Training SHP_2014838A 1 Model of Care Training This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plans. It also ensures
Optum s Role in Mycare Ohio
 Optum s Role in Mycare Ohio What is MyCare Ohio? New opportunities generated by the Affordable Care Act have allowed Ohio to implement the MyCare Ohio program. MyCare Ohio is a demonstration project that
Optum s Role in Mycare Ohio What is MyCare Ohio? New opportunities generated by the Affordable Care Act have allowed Ohio to implement the MyCare Ohio program. MyCare Ohio is a demonstration project that
V. Utilization Management (UM) Program
 Program") V. Utilization Management (UM) Program Overview Better Health Network s Utilization Management (UM) Program is designed to provide quality, cost-effective and medically necessary services while meeting
V. Utilization Management (UM) Program Overview Better Health Network s Utilization Management (UM) Program is designed to provide quality, cost-effective and medically necessary services while meeting
1900 K St. NW Washington, DC 20006 c/o McKenna Long
 1900 K St. NW Washington, DC 20006 c/o McKenna Long Centers for Medicare & Medicaid Services U. S. Department of Health and Human Services Attention CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re:
1900 K St. NW Washington, DC 20006 c/o McKenna Long Centers for Medicare & Medicaid Services U. S. Department of Health and Human Services Attention CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re:
PL 111-148 and Amendments: Impact on Post-Acute Care for Health Care Systems
 PL 111-148 and Amendments: Impact on Post-Acute Care for Health Care Systems By Kathleen M. Griffin, PhD. There are three key provisions of the law that will have direct impact on post-acute care needs
PL 111-148 and Amendments: Impact on Post-Acute Care for Health Care Systems By Kathleen M. Griffin, PhD. There are three key provisions of the law that will have direct impact on post-acute care needs
Melissa Edmister, RN, BSN Clinical Manager Surgical Acute Unit Providence St. Peter Hospital
 Melissa Edmister, RN, BSN Clinical Manager Surgical Acute Unit Providence St. Peter Hospital Why do some organizations do well with safety initiatives while others do poorly or fail? The most important
Melissa Edmister, RN, BSN Clinical Manager Surgical Acute Unit Providence St. Peter Hospital Why do some organizations do well with safety initiatives while others do poorly or fail? The most important
Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals
 Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals 12/18/2013 12/18/13 2013, American Heart Association 1 Thank you for Joining the Webinar Today. The Presentation will Begin
Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals 12/18/2013 12/18/13 2013, American Heart Association 1 Thank you for Joining the Webinar Today. The Presentation will Begin
IRG/APS Healthcare Utilization Management Guidelines for West Virginia Health Homes - Bipolar and Hepatitis
 IRG/APS Healthcare Utilization Management Guidelines for West Virginia Health Homes - Bipolar and Hepatitis CHANGE LOG Medicaid Chapter Policy # Effective Date Chapter 535 Health Homes 535.1 Bipolar and
IRG/APS Healthcare Utilization Management Guidelines for West Virginia Health Homes - Bipolar and Hepatitis CHANGE LOG Medicaid Chapter Policy # Effective Date Chapter 535 Health Homes 535.1 Bipolar and
A Guide for Transitioning to Home After a Rehab Stay
 A Guide for Transitioning to Home After a Rehab Stay Transitioning home after a rehab stay can present unique challenges for patients and/or their caregivers. Patients who have had a debilitating illness
A Guide for Transitioning to Home After a Rehab Stay Transitioning home after a rehab stay can present unique challenges for patients and/or their caregivers. Patients who have had a debilitating illness
Patient Care Services Quality Report Evaluation of 2013 Outcomes August 2014
 Patient Care Services Quality Report Evaluation of 2013 Outcomes August 2014 Submitted by, Carol A Dwyer, MSN, MM, RN, CENP Vice President, Patient Care Services Chief Nursing Officer 1 Index INTRODUCTION...3
Patient Care Services Quality Report Evaluation of 2013 Outcomes August 2014 Submitted by, Carol A Dwyer, MSN, MM, RN, CENP Vice President, Patient Care Services Chief Nursing Officer 1 Index INTRODUCTION...3
Modern care management
 The care management challenge Health plans and care providers spend billions of dollars annually on care management with the expectation of better utilization management and cost control. That expectation
The care management challenge Health plans and care providers spend billions of dollars annually on care management with the expectation of better utilization management and cost control. That expectation
Day 1 Follow-Up: Panelist Suggestions and Final Topic Ranking. IHS Advisory Panel Meeting April 20, 2013 (Day 2) Chad Boult, MD, MPH, MBA Director
 Chad Boult, MD, MPH, MBA Director") Day 1 Follow-Up: Panelist Suggestions and Final Topic Ranking IHS Advisory Panel Meeting April 20, 2013 (Day 2) Chad Boult, MD, MPH, MBA Director 1 Suggestions From Panelists 2 Use One Care Management
Day 1 Follow-Up: Panelist Suggestions and Final Topic Ranking IHS Advisory Panel Meeting April 20, 2013 (Day 2) Chad Boult, MD, MPH, MBA Director 1 Suggestions From Panelists 2 Use One Care Management