Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals
|
|
|
- Elfreda Griffin
- 10 years ago
- Views:
Transcription
1 Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals 12/18/ /18/ , American Heart Association 1

2 Thank you for Joining the Webinar Today. The Presentation will Begin Shortly. 12/18/ , American Heart Association 2

3 Presenters: Nasir Sulemanjee, MD, FACC, Clinical Adjunct Assistant Professor for the University of Wisconsin School of Medicine & Public Health and Advanced Heart Failure & Transplant Cardiologist for Aurora St Luke s Medical Center Anthony Valente, M.D., FACP, Vice President of Medical Affairs for Hazleton General Hospital Andrea Andrews, RN, CHCQM, FAIHQ, Director of Quality/ Case Management/ Stroke Coordinator/ Accreditation Contact for Hazleton General Hospital 12/18/ , American Heart Association 3

4 Heart Failure Best Practice Strategies: Experience from Aurora St. Luke s Medical Center Nasir Sulemanjee, MD FACC Advanced HF & Transplant Cardiologist Aurora St Luke s Medical Center

5 Webinar Objectives To share our experience on how we achieved best practice in heart failure management To help understand the past and ongoing challenges in achieving these goals Every institution will have some common and some unique challenges; its how you approach them which determines your success...

6 Target HF initiative Target: Heart Failure is a national initiative of the American Heart Association that provides healthcare professionals with resources and materials designed to help advance heart failure awareness, prevention, and treatment.

7 Heart Failure in the US ~ 6 million Americans with HF (2.8% adult US population) NHANES ,000 new cases/year (1 in 5 Lifetime risk for ages> 40y) 281,000 annual deaths (1 in 8 death certificates mention HF) 1.1 million hospitalizations for ADHF each year & 6.5 million hospital days (LOS 6.4 days) 1.8 million ambulatory visits each year #1 reason for hospitalization of people >65y Readmission rate of 25% - Medicare to penalize for all reimbursements Cost $ 39.2 billion with $21 billion annual hospitalization cost ($160 billion by 2030) Mortality 50% at 5 years; 34% at 1 year after a single hospitalization

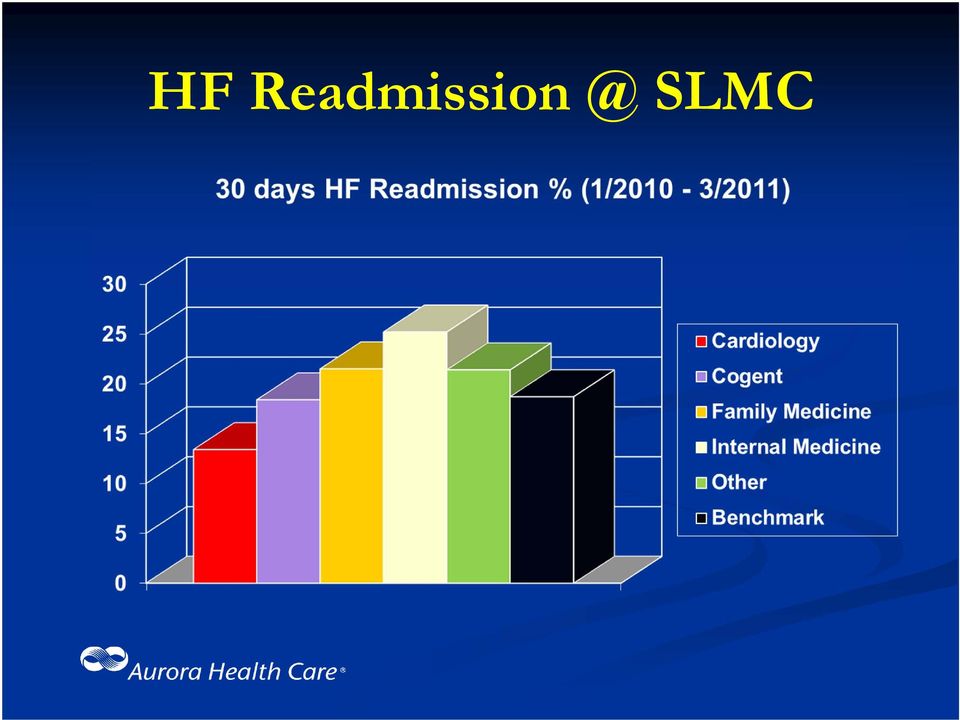
8 State of Heart Failure Management at Aurora St Luke s Medical Center National Recognition for Cardiac Care Top 50 Best Hospitals in the US #1 Hospital for Cardiac Care in Milwaukee Awarded Gold-Star recognition for Quality Management of Heart Failure (ACC/AHA Get with the Guidelines Program ) for the past 3 Years Over 1000 ADHF admissions annually Readmission rate is 18.1% (significantly below national average) Length of Stay ~ 4.5 days (significantly better than national average) Average Cost of HF admission is ~ $5,500 per patient better than national average
 Length of Stay ~ 4.")
9 The Aurora Experience: Historical Perspective The HF management at Aurora St. Luke s Medical Center was not always like this As recently as : Our readmission rate for HF was 25% Our use of evidence-based medications were < 50% Our average Length of Stay for HF admission was ~ 9 days Our Inpatient Mortality for HF was above national average

10 Oh, how we have changed STRATEGY Recognize the state of heart failure management at your institution Identify & understand the challenges Develop partnerships Implement strategies Create an accountable system

11 Recognize the State of HF Management at Your Institution Complete and Accurate Data Collection Allocate resources and personnel Provide appropriate access Use electronic medical records Analyze the data Identify areas you are excelling Identify areas you need improvement Compare with local and national institutes

12 Identify Challenges Health Care providers awareness and education Local cultural challenges Infrastructure for HF management Logistical challenges Resources availability Financial implications to hospitals and providers

13 Develop Partnerships Identify and recruit key personnel to this cause Content Expert (HF Physicians/Cardiologists) Nursing leaders Administrators Allied Health Staff (Social Work, Pharmacist, Dietary, Rehab Team, VNA, Palliative Health, etc.) Local physicians/stake holders IT personnel/emr expert Data collection/quality department representative
 Local physicians/stake holders IT personnel/emr expert Data collection/quality")
14 Implement Strategies Literature review of best practice strategies Get approval from all Executive Committee s Media blitz Get everyone to buy in Grand Rounds Memo s Website Announcements Personal meetings In-Hospital Advertisements

15 Create An Accountable System Quarterly report submitted to all providers Percent of revenue (bonus) attached to quality metrics. Disciplinary action algorithm in place for providers, with involvement of the Medical Staff Office, Physician Evaluation Committee (PEC) and Nursing Council.
 and")
16 HF Admission SLMC Hospitalist IM

17 HF SLMC
18
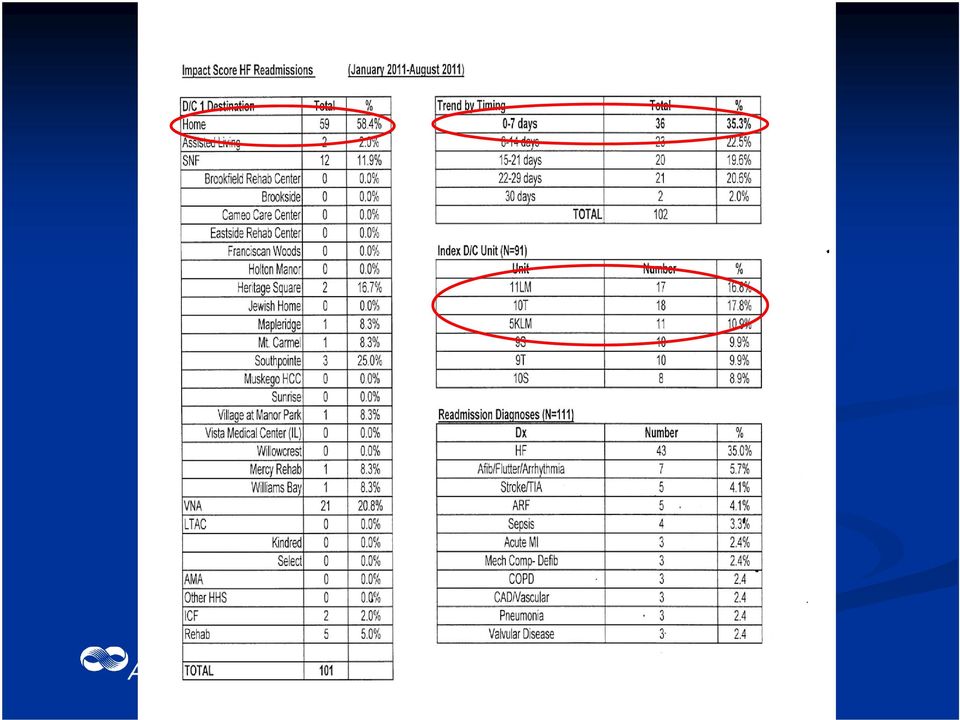
19 In Summary. Best Practice guidelines were being followed: When multi-disciplinary team (including cardiologist, HF coordinators, social work, etc.) was involved in the care for HF patients Those patients had better outcomes inpatient mortality and 30-day readmission Majority were being readmitted from home and within 7 days after discharge.
 was involved in the care for HF patients Those patients had better outcomes")
20 Strategies Employed at Aurora St. Luke s Medical Center Launch hospital-wide HF education and awareness Cardiology/Heart Failure Team Consult Heart Failure Education by HF Care Coordinators Effective use of EMR Order sets, discharge checklist, etc. Discharge follow-up within 1 week with a primary care, cardiologist or the heart failure clinic Eligible patients being referred to community-based services (such as VNA, telemedicine, nursing homes, hospice care, etc.) Referral to Heart Failure Clinic Multidisciplinary Team Designated Heart Failure Inpatient Units

21
22 Significant improvement in Length of Stay demonstrated by utilizing the HF designated unit(s).
23 Nasir Sulemanjee, MD, FACC Advanced Heart Failure & Transplant Cardiologist Clinical Adjunct Assistant Professor University of Wisconsin School of Medicine & Public Health 2801 W Kinnickinnic River Parkway, Suite #175 Milwaukee, WI Phone: (414) /Fax: (414) [email protected]
24 AN OVERVIEW of TARGET HF: QUALIFYING for the HONOR ROLL and a DETAILED FOCUS on MEDICATION COMPLIANCE (ACE/ARB, ADLOSTERONE ANTAGONIST, and EBBB) HAZLETON GENERAL HOSPITAL HAZLETON, PENNSYLVANIA PRESENTERS: ANDREA ANDREWS, RN / CHCQM DIRECTOR QUALITY / CASE MANAGEMENT ANTHONY VALENTE, MD / FACP VICE PRESIDENT OF MEDICAL AFFAIRS
25 Our objectives for this teleconference will be to: (1) Discuss ways to improve quality, care transitions, and outcomes for patients with heart failure utilizing patient centered domains, and (2) Discuss medication optimization in heart failure patients. 25
26 Target: Heart Failure is a national initiative of the American Heart Association that provides healthcare professionals with resources and materials designed to help advance heart failure awareness, prevention, and treatment. Hazleton General Hospital is committed to providing quality, evidencebased standard of care for our heart failure patient population. Heart failure is one of our top 5 DRG admissions and one of our top readmit DRG s. To help you better understand our care of the heart failure patient, let me provide you with a background of our journey. 26
27 We began our journey in the care of our heart failure patients in January, 2007, when we were invited to be a part of the Accelerating Best Care (ABC) in Pennsylvania Program funded by our state legislature. Representatives from The Baylor Health Care System, who developed the ABC at Baylor program, showed us the results of their quality improvement program. They explained the cultural changes needed to improve quality and the practical tools needed to accomplish their goals. The basis of the ABC Program is to break a problem down into small pieces, like a puzzle, quickly analyze the problem through data collection, implement interventions, and analyze results adding additional interventions if needed, all in a short period of time. 27
28 Prior to learning the methodology of the ABC Program, departments would identify problems and tackle the whole problem. Findings were: Team work with other affected departments was sometimes present, but not always; Months and months of data would be collected; Interventions were delayed; quality targets were not always met and Improvements were not noted in a timely fashion. A core group of 14 individuals, from different disciplines within our organization, began rigorous training on the ABC process in January, Training, conducted by coaches from Baylor and Thomas Jefferson, focused on the structure, process, and outcomes of improving quality using the ABC methodology 28 and laid the groundwork for projects the core group were to complete.
29 Five quality initiatives were selected to go through the ABC methodology of quality improvement during the training period. One of these projects involved our HF core measures, first focusing on HF discharge instructions. WHY HEART FAILURE? Top Admission Diagnosis Most Common Reason for Readmission Core Measure Financial Impact Our HF Team was formed and the assessment of all patients on the telemetry unit was our focus. The baseline for our heart failure discharge instruction core measure compliance for January, 2007 was 79%. 29
30 Our team identified the need for standing order sets for CHF admissions. These were implemented and made mandatory for use by the Medical Staff, with support from the Medical Executive Committee leadership. To increase compliance with our core measures more importantly to provide quality care to each of our CHF patients every time all the time, we placed a yellow CHF form on the front of the charts for all CHF patients with the words STOP CHF on them. A CHF discharge instruction form was developed and implemented to be utilized for all CHF discharges. This form addressed all the required elements by CMS which include the following: Diet Activity Medications Weight Symptoms 30 Follow up
31 After implementation of these interventions, our compliance for heart failure discharge instructions went to 100% in May, For a better understanding of where HGH began its journey with HF core measures, and where it journeyed to, please note the following: Evaluation Baseline Data in 2004 LVS Function 67% ACE or ARB for LVSD 48% Adult Smoking Cessation 19% Discharge Instructions 14% 31
32 Fourth Quarter 2012 First Quarter 2013 Second Quarter 2013 Third Quarter 2013 LVS Function 100% 100% 100% 100% ACE or ARB for LVSD 100% 100% 100% 100% Discharge Instructions 100% 100% 100% 100% HF Patient Appropriateness of Care Compliance 100% 100% 100% 100% 32
33 To sustain our HF compliance, as evidenced by the previous slide, we have implemented the following through our ABC process: Placed a clinical quality data RN specialist on the clinical units monitoring the care our HF patients receive in real time Have revised our HF discharge instructions to include a follow up call to the patient within 72 hours of discharge Collaborated with our home health agency in utilizing home telehealth monitors for our HF patients who request our agency and who meet criteria for these monitors. 33
34 These monitors assess weight, blood pressure, 02 saturations, and pulse, along with a set of questions individually selected for each patient regarding edema, shortness of breath, meds, etc. These monitors are set up to be checked daily and the information is then sent to a secure website, which our home health nurses check on a daily basis (Monday Friday) and identify any real or potential problems. If a problem is identified, the home health nurse calls the patient for more information and then either calls the physician or sends a nurse out to evaluate. 34
35 ACCOMPLISMENTS AT HGH with OUR HF CORE MEASURE PROCESS Have submitted our CHF order sets and medication forms to the AHA, and were chosen to have our CHF tools posted in the GWTG Tool Library. Remain a HF mentor hospital for the IHI 5,000,000 Lives Campaign Had an article, showcasing our Heart Failure Tools, appear in the December, 2009 issue of Critical Pathways in Cardiology journal. Received our Target: HF first time Status/Recognition in 2012 and again in Received the Gold Plus Heart Failure Award in 2013 (5 years in a row). Have received the five star rating for treatment of our HF patients from Healthgrades. 35
36 When providing optimal HF care, we benefit in many ways: LOS is decreased Utilization of resources is decreased and most importantly, patient satisfaction is increased. Hazleton General Hospital continued its journey in caring for the heart failure patient by submitting an honor roll award application for Target: HF in We were one of two hospitals in the Nation that was recognized as a Target Heart Failure Honor Roll Hospital in The US New and World Report ad in August,
37 Our compliance to the required measures (where 50% compliance was needed) is as follows (for 07/01/ /30/2013). (1) ACE/ARB at discharge 100% compliance (2) EBBB 85% compliance (3) Aldosterone Antagonist at Discharge 58.8% compliance (4) Follow up visit within 7 days or less 89.7% compliance (5) Referred to HF disease management, 60 minutes patient education, or HF interactive workbook 96.9% compliance The Target: Heart Failure Mission involves 3 key patient centered care domains that I will address at this time, as they pertain to Hazleton General Hospital and it s heart failure patients. 37
38 38
39 39
40 40
41 41
42 42
43 43
44 44
45 1. Medication optimization regarding discharge use of ACE/ARB, EBBB, and Aldosterone antagonist in all eligible heart failure patients. (a) ACE/ARB at discharge for fiscal year 2012/2013, we are at 100% compliance. (b) EBBB for fiscal year 2012/2013, we are at 85% compliance. In order to address the EBBB and Aldosterone antagonist medication optimization, we have revised our HF order sets to include these meds. We have also heightened awareness with our medical staff, Pharmacy and nursing in regards to medication optimization of our heart failure patients through use of evidence based standards of care and team collaboration. 45
46 (c) Aldosterone antagonist at discharge for fiscal year 2012/2013, we are at 58.8% compliance. This measure addresses heart failure patients with LVSD with no contraindications or documented intolerance to this medication. 46
47 47
48 48
49 49
50 50
51 2. Early follow up and care coordination early post discharge followup with visit or phone call scheduled to occur within 7 days of hospital discharge for fiscal year 2012/2013, we are at 89.7% compliance. Nursing is responsible for meeting this measure and we have a Clinical Quality Data RN Specialist who reviews this daily. We also try to place our heart failure patients on our telemetry unit. We also make the post discharge appointment for heart failure patients, whom we have identified as our high risk population for fiscal year 2012/2013, we are at 96.6% compliance. 51
52 3. Enhanced patient education this involves referral to HF disease management, 60 minutes of patient education, or HF interactive workbook for fiscal year 2012/2013, we are at 96.9% compliance. We have revised our CHF Discharge Instructions to include the AHA s Information Prescription for Healthier Living with HF which we give to the patient. 52
53 53
54 54
55 We also begin HF education / teaching on admission, and reiterate again at discharge. We use the CHF teaching / discharge instruction form. 55
56 56
57 We have an ABC team that remains in place working with nursing, the medical staff, home health and other involved ancillary departments in providing the best care to our HF patients every time, all the time utilizing evidence based standards of care and team collaboration. We definitely have room for improvement with EBBB and Aldosterone antagonists ordered at discharge, and this is where our focus will be with our ABC team as we strive to improve the care of our heart failure patients and maintain Target: HF Status/Recognition. 57
58 For more information contact: Andrea Andrews Director of Quality / Case Management Hazleton General Hospital [email protected] Anthony Valente, M.D./FACP Vice President of Medical Affairs 58
59 Want to learn more about Advanced Certification in Heart Failure? Please visit or us at 59
60 12/18/ , American Heart Association 60
61 For more information and to register for Target: HF, go to In order to claim your continuing education credits for attending this Target: Heart Failure webinar please download the document entitled Instructions for Claiming CME/CE Credits or download the instructions from click on icon that says webinars/slide decks. Find this event and download the document. Please follow the instructions listed in this document. Remember to visit learn.heart.org This is also a great site that the American Heart Association provides where you can Learn at Heart with the latest Cardiovascular and Stroke CME/CE activities Thank You! 12/18/ American Heart Association 61
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates
 Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Kick off Meeting November 11 13, 2015. MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF)
") Kick off Meeting November 11 13, 2015 MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF) Team Composition Justin Huynh, MD Internal Medicine, Physician Champion Mary Laubinger,
Kick off Meeting November 11 13, 2015 MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF) Team Composition Justin Huynh, MD Internal Medicine, Physician Champion Mary Laubinger,
3/11/15. COPD Disease Management Tackling the Transition. Objectives. Describe the multidisciplinary approach to inpatient care for COPD patients
 Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
HealthCare Partners of Nevada. Heart Failure
 HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
Coordinating Transitions of Care: It Takes a Village
 Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
What do ACO s and Hospitals want from SNF s and CCRC s
 What do ACO s and Hospitals want from SNF s and CCRC s Presented to the Institute of Senior Living, April 11, 2013 A Division of Kindred Healthcare 1 Assessing the match: What hospitals and ACO s currently
What do ACO s and Hospitals want from SNF s and CCRC s Presented to the Institute of Senior Living, April 11, 2013 A Division of Kindred Healthcare 1 Assessing the match: What hospitals and ACO s currently
Understanding Care Transitions as a Patient Safety Issue
 Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
1. Executive Summary Problem/Opportunity: Evidence: Baseline Data: Intervention: Results:
 A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
Readmissions as an Enterprise Priority. Presenters 4/17/2014
 Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center [email protected] Eileen
Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center [email protected] Eileen
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System
 Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
Innovations@Home. Home Health Initiatives Reduce Avoidable Readmissions by Leveraging Innovation
 How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
5/6/2014. Physiologic Monitoring Tools & Use with Patients with Chronic Health Conditions. Objectives. The Issue at Hand
 Physiologic Monitoring Tools & Use with Patients with Chronic Health Conditions Kelly Brittain, PhD, RN Assistant Professor MCRH-Nursing Grand Rounds May 8, 2014 Objectives 1. Summarize previous research
Physiologic Monitoring Tools & Use with Patients with Chronic Health Conditions Kelly Brittain, PhD, RN Assistant Professor MCRH-Nursing Grand Rounds May 8, 2014 Objectives 1. Summarize previous research
The Role of Telemedicine in Home Monitoring and Long Term Care June 7, 2012. Penny S. Milanovich President UPMC Visiting Nurses Association
 The Role of Telemedicine in Home Monitoring and Long Term Care June 7, 2012 Penny S. Milanovich President UPMC Visiting Nurses Association Cost of Chronic Conditions An average of 40-50% of healthcare
The Role of Telemedicine in Home Monitoring and Long Term Care June 7, 2012 Penny S. Milanovich President UPMC Visiting Nurses Association Cost of Chronic Conditions An average of 40-50% of healthcare
Post-Acute Care Transitions: An Essential Component of Accountable Care
 : An Essential Component of Accountable Care Bruce C. Smith, MD, FACP Associate Medical Director, Strategy Deployment Group Health Physicians, Seattle, WA [email protected] AMGA 2012 Institute for Quality
: An Essential Component of Accountable Care Bruce C. Smith, MD, FACP Associate Medical Director, Strategy Deployment Group Health Physicians, Seattle, WA [email protected] AMGA 2012 Institute for Quality
Hospital to Physician Office to Home: A Respiratory Led Program Across the Continuum of Care
 Hospital to Physician Office to Home: A Respiratory Led Program Across the Continuum of Care Charley P. Starnes, RRT, RCP Clinical Respiratory Specialist- COPD Education Important Milestones July 2011-
Hospital to Physician Office to Home: A Respiratory Led Program Across the Continuum of Care Charley P. Starnes, RRT, RCP Clinical Respiratory Specialist- COPD Education Important Milestones July 2011-
Successful Heart Failure Management Nurse/NP Run Clinics
 Dagmar Knot RN BScN CCCN Transplant Coordination Team Leader Organ Transplant Center KFSHRC Riyadh, KSA Heart Failure Nurses Role, responsibilities & education Successful Heart Failure Management Nurse/NP
Dagmar Knot RN BScN CCCN Transplant Coordination Team Leader Organ Transplant Center KFSHRC Riyadh, KSA Heart Failure Nurses Role, responsibilities & education Successful Heart Failure Management Nurse/NP
Congestive Heart Failure Management Program
 Congestive Heart Failure Management Program The Congestive Heart Failure Program is the third statewide disease management program developed by CCNC. The clinical directors reviewed prevalence and outcome
Congestive Heart Failure Management Program The Congestive Heart Failure Program is the third statewide disease management program developed by CCNC. The clinical directors reviewed prevalence and outcome
RT AS PROJECT MANAGER:
 RT AS PROJECT MANAGER: IMPROVING CARE TRANSITIONS DECREASES UNPLANNED READMISSIONS TAMMY JARNAGIN, BHS, RRT DIRECTOR CARDIOPULMONARY SERVICES, NEURODIAGNOSTICS, HOME MEDICAL EQUIPMENT Objectives Recognize
RT AS PROJECT MANAGER: IMPROVING CARE TRANSITIONS DECREASES UNPLANNED READMISSIONS TAMMY JARNAGIN, BHS, RRT DIRECTOR CARDIOPULMONARY SERVICES, NEURODIAGNOSTICS, HOME MEDICAL EQUIPMENT Objectives Recognize
Essentia Health. Heart Failure and Remote Monitoring. Denise Buxbaum, RN, BSN, CHFN Heart Failure Program Manager
 Essentia Health Heart Failure and Remote Monitoring Denise Buxbaum, RN, BSN, CHFN Heart Failure Program Manager Essentia Health Oct 2014 No reproduction without permission Why Heart Failure? Prevalence
Essentia Health Heart Failure and Remote Monitoring Denise Buxbaum, RN, BSN, CHFN Heart Failure Program Manager Essentia Health Oct 2014 No reproduction without permission Why Heart Failure? Prevalence
Call-A-Nurse Location
 Call-A-Nurse A 24-hour medical call center, specializing in registered nurse telephone triage, answering service, physician and service referral, and class registration. Call-A-Nurse Location Call-A-Nurse
Call-A-Nurse A 24-hour medical call center, specializing in registered nurse telephone triage, answering service, physician and service referral, and class registration. Call-A-Nurse Location Call-A-Nurse
Patients Receive Recommended Care for Community-Acquired Pneumonia
 Patients Receive Recommended Care for Community-Acquired Pneumonia For New Jersey to be a state in which all people live long, healthy lives. DSRIP LEARNING COLLABORATIVE PRESENTATION The Care you Trust!
Patients Receive Recommended Care for Community-Acquired Pneumonia For New Jersey to be a state in which all people live long, healthy lives. DSRIP LEARNING COLLABORATIVE PRESENTATION The Care you Trust!
STEMI Systems of Care
 STEMI Systems of Care Rich Lundy, MBA, RRT, FACCA Vice President Heart and Vascular Services, Imaging Services Cone Health May 2013 STEMI Systems of Care Objectives Demonstrate the clinical and operational
STEMI Systems of Care Rich Lundy, MBA, RRT, FACCA Vice President Heart and Vascular Services, Imaging Services Cone Health May 2013 STEMI Systems of Care Objectives Demonstrate the clinical and operational
ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION)
") ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION) Hello and welcome. Thank you for taking part in this presentation entitled "Essentia Health as an ACO or Accountable Care Organization -- What
ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION) Hello and welcome. Thank you for taking part in this presentation entitled "Essentia Health as an ACO or Accountable Care Organization -- What
November 15, 2013. Ann Laramee MS ANP-BC ACNS-BC CHFN FletcherAllen.org
 Advance Care Planning with Heart Failure: Results of a Primary Care Practitioners Needs Survey 5 th Annual Nursing Research and Evidence Based Practice Symposium November 15, 2013 Ann Laramee MS ANP-BC
Advance Care Planning with Heart Failure: Results of a Primary Care Practitioners Needs Survey 5 th Annual Nursing Research and Evidence Based Practice Symposium November 15, 2013 Ann Laramee MS ANP-BC
Medication Error. Medication Errors. Transitions in Care: Optimizing Intern Resources
 Transitions in Care: Optimizing Intern Resources DeeDee Hu PharmD, MBA Clinical Specialist Critical Care and Cardiology PGY1 Program Director Memorial Hermann Memorial City Medical Center Medication Error
Transitions in Care: Optimizing Intern Resources DeeDee Hu PharmD, MBA Clinical Specialist Critical Care and Cardiology PGY1 Program Director Memorial Hermann Memorial City Medical Center Medication Error
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT. Norris Vivatrat, MD Associate Medical Director Monarch HealthCare
 PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
Henry Ford Health System Care Coordination and Readmissions Update
 Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
Hospital Based Transitions of Care Program. Dr Jeffery Liles, MD FHM. Providence Health Care
 Outcomes and Applications of a Hospital Based Transitions of Care Program. Dr Jeffery Liles, MD FHM Medical Director Care Management Providence Health Care -Importance of D/C planning and transitions of
Outcomes and Applications of a Hospital Based Transitions of Care Program. Dr Jeffery Liles, MD FHM Medical Director Care Management Providence Health Care -Importance of D/C planning and transitions of
Kaiser Permanente: Transition Care Performance and Strategies
 Kaiser Permanente: Transition Care Performance and Strategies Carol Ann Barnes, PT, DPT, GCS [email protected] April 2009 Netta Conyers-Haynes, October, 2014 Principal Consultant, Communications Agenda
Kaiser Permanente: Transition Care Performance and Strategies Carol Ann Barnes, PT, DPT, GCS [email protected] April 2009 Netta Conyers-Haynes, October, 2014 Principal Consultant, Communications Agenda
Care Coordination. The Embedded Care Manager. Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed
 Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home
 RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
Transitions of Care Management Coding (TCM Code) Tutorial. 1. Introduction Meaning of moderately and high complexity 2
 Tutorial. 1. Introduction Meaning of moderately and high complexity 2") Transitions of Care Management Coding (TCM Code) Tutorial Index 1. Introduction Meaning of moderately and high complexity 2 2. SETMA s Tools for using TCM Code 3 Alert that patient is eligible for TCM
Transitions of Care Management Coding (TCM Code) Tutorial Index 1. Introduction Meaning of moderately and high complexity 2 2. SETMA s Tools for using TCM Code 3 Alert that patient is eligible for TCM
Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions
 Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions Scott Flinn MD Deborah Schutz RN JD Fritz Steen RN Arch Health Partners A medical foundation formed
Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions Scott Flinn MD Deborah Schutz RN JD Fritz Steen RN Arch Health Partners A medical foundation formed
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Introduction. Mary Collier RN, MSN. Monica Worrell RN,MSN
 UC Health Introduction Mary Collier RN, MSN Monica Worrell RN,MSN OBJECTIVES Discuss Evidence Based Practice Highlight UC Health Medical Centers Heart Failure Clinical Practice Guidelines Share our Heart
UC Health Introduction Mary Collier RN, MSN Monica Worrell RN,MSN OBJECTIVES Discuss Evidence Based Practice Highlight UC Health Medical Centers Heart Failure Clinical Practice Guidelines Share our Heart
Centers for Medicare & Medicaid Services Special Innovation Projects Overview. Sara Butterfield, RN, BSN, CPHQ October 2015
 Centers for Medicare & Medicaid Services Special Innovation Projects Overview Sara Butterfield, RN, BSN, CPHQ October 2015 Objectives Provide an overview of the CMS Special Innovation Project (SIP) Awards
Centers for Medicare & Medicaid Services Special Innovation Projects Overview Sara Butterfield, RN, BSN, CPHQ October 2015 Objectives Provide an overview of the CMS Special Innovation Project (SIP) Awards
CHAPTER 535 HEALTH HOMES. Background... 2. Policy... 2. 535.1 Member Eligibility and Enrollment... 2. 535.2 Health Home Required Functions...
 TABLE OF CONTENTS SECTION PAGE NUMBER Background... 2 Policy... 2 535.1 Member Eligibility and Enrollment... 2 535.2 Health Home Required Functions... 3 535.3 Health Home Coordination Role... 4 535.4 Health
TABLE OF CONTENTS SECTION PAGE NUMBER Background... 2 Policy... 2 535.1 Member Eligibility and Enrollment... 2 535.2 Health Home Required Functions... 3 535.3 Health Home Coordination Role... 4 535.4 Health
Be Careful What You Ask For A Predictive Model That Really Works
 Be Careful What You Ask For A Predictive Model That Really Works Rod Christensen, MD President, Allina Health Clinics Cheryl Hermann, RN, MBA Vice President, Clinic Operations & Patient Care Services Karen
Be Careful What You Ask For A Predictive Model That Really Works Rod Christensen, MD President, Allina Health Clinics Cheryl Hermann, RN, MBA Vice President, Clinic Operations & Patient Care Services Karen
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION
 Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Philips Hospital to Home: redefining healthcare. through innovation in telehealth
 Philips Hospital to Home: redefining healthcare through innovation in telehealth Healthcare costs are at a crisis point, forcing the federal government to make comprehensive changes to healthcare payment
Philips Hospital to Home: redefining healthcare through innovation in telehealth Healthcare costs are at a crisis point, forcing the federal government to make comprehensive changes to healthcare payment
Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions
 Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions Leslie Becker RN, BS Jennifer Smith RN, MSN, MBA Leslie Frain MSN, RN Jan Machanis
Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions Leslie Becker RN, BS Jennifer Smith RN, MSN, MBA Leslie Frain MSN, RN Jan Machanis
Leveraging Big Data & Deep Analytics to Improve Care
 Leveraging Big Data & Deep Analytics to Improve Care A Complimentary Webinar From healthsystemcio.com Sponsored by SAS Your Line Will Be Silent Until Our Event Begins at 1:00 ET Thank You! Housekeeping
Leveraging Big Data & Deep Analytics to Improve Care A Complimentary Webinar From healthsystemcio.com Sponsored by SAS Your Line Will Be Silent Until Our Event Begins at 1:00 ET Thank You! Housekeeping
Connect4 Patients CCCM Primary Care Community. Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM
 Connect4 Patients CCCM Primary Care Community Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM September 17, 2015 Objectives: Describe innovative care management
Connect4 Patients CCCM Primary Care Community Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM September 17, 2015 Objectives: Describe innovative care management
National Clinical Programmes
 National Clinical Programmes Section 3 Background information on the National Clinical Programmes Mission, Vision and Objectives July 2011 V0. 6_ 4 th July, 2011 1 National Clinical Programmes: Mission
National Clinical Programmes Section 3 Background information on the National Clinical Programmes Mission, Vision and Objectives July 2011 V0. 6_ 4 th July, 2011 1 National Clinical Programmes: Mission
Main Section of the proposal: 1. Overall Aim & Objectives:
 Main Section of the proposal: 1. Overall Aim & Objectives: Over the past two decades Providence Health & Services has developed a comprehensive tobacco cessation program within our health system. The foundation
Main Section of the proposal: 1. Overall Aim & Objectives: Over the past two decades Providence Health & Services has developed a comprehensive tobacco cessation program within our health system. The foundation
Transitions of Care: The need for a more effective approach to continuing patient care
 H O T T O P I C S I N H E A L T H C A R E Transitions of Care: The need for a more effective approach to continuing patient care The need for a more effective approach to continuing patient care This paper
H O T T O P I C S I N H E A L T H C A R E Transitions of Care: The need for a more effective approach to continuing patient care The need for a more effective approach to continuing patient care This paper
What is an Accountable Care Organization & Why is it Important to Your Home Infusion Company?
 What is an Accountable Care Organization & Why is it Important to Your Home Infusion Company? Lisa Harvey McPherson RN, MBA, MPPM EMHS Vice President Continuum of Care & Chief Advocacy Officer Disclosures
What is an Accountable Care Organization & Why is it Important to Your Home Infusion Company? Lisa Harvey McPherson RN, MBA, MPPM EMHS Vice President Continuum of Care & Chief Advocacy Officer Disclosures
REACHING ZERO DEFECTS IN CORE MEASURES. Mary Brady, RN, MS Ed, Senior Nursing Consultant, Healthcare Transformations LLC,
 REACHING ZERO DEFECTS IN CORE MEASURES Mary Brady, RN, MS Ed, Senior Nursing Consultant, Healthcare Transformations LLC, 165 Lake Linden Dr., Bluffton SC 29910, 843-364-3408, [email protected] Primary
REACHING ZERO DEFECTS IN CORE MEASURES Mary Brady, RN, MS Ed, Senior Nursing Consultant, Healthcare Transformations LLC, 165 Lake Linden Dr., Bluffton SC 29910, 843-364-3408, [email protected] Primary
Implementing an Evidence Based Hospital Discharge Process
 Implementing an Evidence Based Hospital Discharge Process Learning from the experience of Project Re-Engineered Discharge (RED) Webinar January 14, 2013 Chris Manasseh, MD Director, Boston HealthNet Inpatient
Implementing an Evidence Based Hospital Discharge Process Learning from the experience of Project Re-Engineered Discharge (RED) Webinar January 14, 2013 Chris Manasseh, MD Director, Boston HealthNet Inpatient
2013 ACO Quality Measures
 ACO 1-7 Patient Satisfaction Survey Consumer Assessment of HealthCare Providers Survey (CAHPS) 1. Getting Timely Care, Appointments, Information 2. How well Your Providers Communicate 3. Patient Rating
ACO 1-7 Patient Satisfaction Survey Consumer Assessment of HealthCare Providers Survey (CAHPS) 1. Getting Timely Care, Appointments, Information 2. How well Your Providers Communicate 3. Patient Rating
Interactive Voice Response Technology To Prevent Type 2 Diabetes in Cardiac Population
 Interactive Voice Response Technology To Prevent Type 2 Diabetes in Cardiac Population Overview The University of Ottawa Heart Institute (UOHI) with an annual rate of 6000 admissions is committed to understanding,
Interactive Voice Response Technology To Prevent Type 2 Diabetes in Cardiac Population Overview The University of Ottawa Heart Institute (UOHI) with an annual rate of 6000 admissions is committed to understanding,
Z Take this folder with you to your
 my health care notebook Why? Being an active part of your health care team helps you feel better and helps you get even better care. Starting on Day 1, you can keep track of important information and questions.
my health care notebook Why? Being an active part of your health care team helps you feel better and helps you get even better care. Starting on Day 1, you can keep track of important information and questions.
UTILIZATION MANAGEMENT PROGRAM Introduction Health Care Services
 UTILIZATION MANAGEMENT PROGRAM Introduction Health Care Services Call us: 1-888-898-7969, Option 1, then Option 4 Fax us: 1-800-594-7404 Business hours: Monday Friday (excluding holidays), 8:30 a.m. to
UTILIZATION MANAGEMENT PROGRAM Introduction Health Care Services Call us: 1-888-898-7969, Option 1, then Option 4 Fax us: 1-800-594-7404 Business hours: Monday Friday (excluding holidays), 8:30 a.m. to
Limb Preservation Strategies: Quality Outcomes for the ACO Model. SPEAKERS: Audrey K Moyer-Harris MBA BSN RN CWCN Martha Kelso RN HBOT COO MWS LEAP
 Limb Preservation Strategies: Quality Outcomes for the ACO Model SPEAKERS: Audrey K Moyer-Harris MBA BSN RN CWCN Martha Kelso RN HBOT COO MWS LEAP Disclosures Audrey K Moyer-Harris MBA BSN RN CWCN Executive
Limb Preservation Strategies: Quality Outcomes for the ACO Model SPEAKERS: Audrey K Moyer-Harris MBA BSN RN CWCN Martha Kelso RN HBOT COO MWS LEAP Disclosures Audrey K Moyer-Harris MBA BSN RN CWCN Executive
Patient Optimization Improves Outcomes, Lowers Cost of Care >
 Patient Optimization Improves Outcomes, Lowers Cost of Care > Consistent preoperative processes ensure better care for orthopedic patients The demand for primary total joint arthroplasty is projected to
Patient Optimization Improves Outcomes, Lowers Cost of Care > Consistent preoperative processes ensure better care for orthopedic patients The demand for primary total joint arthroplasty is projected to
Group Health Centre Sault Ste. Marie, Ontario
 Group Health Centre Sault Ste. Marie, Ontario Breakout Session: Thriving Models That Haven t Spread: Why Not? Picking Up the Pace Conference November 2, 2010 In 1960, a group of 50 original canvassers
Group Health Centre Sault Ste. Marie, Ontario Breakout Session: Thriving Models That Haven t Spread: Why Not? Picking Up the Pace Conference November 2, 2010 In 1960, a group of 50 original canvassers
A STRATIFIED APPROACH TO PATIENT SAFETY THROUGH HEALTH INFORMATION TECHNOLOGY
 A STRATIFIED APPROACH TO PATIENT SAFETY THROUGH HEALTH INFORMATION TECHNOLOGY Table of Contents I. Introduction... 2 II. Background... 2 III. Patient Safety... 3 IV. A Comprehensive Approach to Reducing
A STRATIFIED APPROACH TO PATIENT SAFETY THROUGH HEALTH INFORMATION TECHNOLOGY Table of Contents I. Introduction... 2 II. Background... 2 III. Patient Safety... 3 IV. A Comprehensive Approach to Reducing
Reducing Avoidable Readmissions Effectively (RARE) Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement
 Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement") Reducing Avoidable Readmissions Effectively (RARE) Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement Martha and James Acute Episodes Family Doctor Life Expectancy from chronic diseases
Reducing Avoidable Readmissions Effectively (RARE) Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement Martha and James Acute Episodes Family Doctor Life Expectancy from chronic diseases
Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services
 Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services Objectives Understand the new consequences to hospitals for discharged clients being re-admitted within selected time
Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services Objectives Understand the new consequences to hospitals for discharged clients being re-admitted within selected time
DELIVERING VALUE THROUGH TECHNOLOGY
 DELIVERING VALUE THROUGH TECHNOLOGY Mark Nelson, MD - EMR Physician Champion Krishna Ramachandran - Chief Information and Transformation Officer Karen Adamson - Director, Epic Clinical Applications DuPage
DELIVERING VALUE THROUGH TECHNOLOGY Mark Nelson, MD - EMR Physician Champion Krishna Ramachandran - Chief Information and Transformation Officer Karen Adamson - Director, Epic Clinical Applications DuPage
How To Run A Hospital
 Baptist Hospital Inpatient Medicine Program Mark Hauser, MD, FACP, FCCP Chief Medical Officer and Vice President of Medical Affairs Baptist Hospital of Miami Tomas Villanueva, DO, MBA, FACPE, SFHM Assistant
Baptist Hospital Inpatient Medicine Program Mark Hauser, MD, FACP, FCCP Chief Medical Officer and Vice President of Medical Affairs Baptist Hospital of Miami Tomas Villanueva, DO, MBA, FACPE, SFHM Assistant
MANITOWOC COUNTY CARE TRANSITION PROGRAM
 MANITOWOC COUNTY CARE TRANSITION PROGRAM A U G U S T 1 5, 2 0 1 3 Judy Rank Director Cathy Ley Supervisor Care Transitions Coach MANITOWOC COUNTY CARE TRANSITION PROGRAM Julie Place, Director of Nursing
MANITOWOC COUNTY CARE TRANSITION PROGRAM A U G U S T 1 5, 2 0 1 3 Judy Rank Director Cathy Ley Supervisor Care Transitions Coach MANITOWOC COUNTY CARE TRANSITION PROGRAM Julie Place, Director of Nursing
MODULE 11: Developing Care Management Support
 MODULE 11: Developing Care Management Support In this module, we will describe the essential role local care managers play in health care delivery improvement programs and review some of the tools and
MODULE 11: Developing Care Management Support In this module, we will describe the essential role local care managers play in health care delivery improvement programs and review some of the tools and
Presented by: Char Brar, ACNP, MS(Chem.), MSN, RN Cardiology Nurse Practitioner JBVAMC, Chicago
, MSN, RN Cardiology Nurse Practitioner JBVAMC, Chicago") Presented by: Char Brar, ACNP, MS(Chem.), MSN, RN Cardiology Nurse Practitioner JBVAMC, Chicago 200 bed acute care facility 4 Community Based Out-patient Clinics (CBOCs) 58,000 Veterans IN FY 2008 : 768
Presented by: Char Brar, ACNP, MS(Chem.), MSN, RN Cardiology Nurse Practitioner JBVAMC, Chicago 200 bed acute care facility 4 Community Based Out-patient Clinics (CBOCs) 58,000 Veterans IN FY 2008 : 768
#Aim2Innovate. Share session insights and questions socially. UCLA Primary Care Innovation Model 6/13/2015. Mark S. Grossman, MD, MBA, FAAP, FACP
 UCLA Primary Care Innovation Model Mark S. Grossman, MD, MBA, FAAP, FACP Chief Medical Office, UCLA Community Physicians & Specialty Care Networks June 16, 2015 DISCLAIMER: The views and opinions expressed
UCLA Primary Care Innovation Model Mark S. Grossman, MD, MBA, FAAP, FACP Chief Medical Office, UCLA Community Physicians & Specialty Care Networks June 16, 2015 DISCLAIMER: The views and opinions expressed
A Guide to Patient Services. Cedars-Sinai Health Associates
 A Guide to Patient Services Cedars-Sinai Health Associates Welcome Welcome to Cedars-Sinai Health Associates. We appreciate the trust you have placed in us by joining our dedicated network of independent-practice
A Guide to Patient Services Cedars-Sinai Health Associates Welcome Welcome to Cedars-Sinai Health Associates. We appreciate the trust you have placed in us by joining our dedicated network of independent-practice
Community Health Needs Assessment Implementation Plan FY 14-16
 Community Health Needs Assessment Implementation Plan FY 14-16 South Miami Hospital conducted a community health needs assessment in 2013 to better understand the healthcare needs of the community it serves
Community Health Needs Assessment Implementation Plan FY 14-16 South Miami Hospital conducted a community health needs assessment in 2013 to better understand the healthcare needs of the community it serves
Dual RFI Response Summary
 Dual RFI Response Summary Improving Care through Integrated Medicare and Medi- Cal Delivery Models Stuart Levine, MD., MHA. Keith Wilson, MD Robert Margolis, MD. Stakeholder Meeting August 30, 2011 1 Organization
Dual RFI Response Summary Improving Care through Integrated Medicare and Medi- Cal Delivery Models Stuart Levine, MD., MHA. Keith Wilson, MD Robert Margolis, MD. Stakeholder Meeting August 30, 2011 1 Organization
Cardiac Rehab and Success
 One Health System, Better Outcomes Department of Health and Human Services, GPO Box 125, Hobart, TAS, 7001 RE: THO North Cardiac Health and Rehabilitation Submission on the Green Paper The Cardiac Health
One Health System, Better Outcomes Department of Health and Human Services, GPO Box 125, Hobart, TAS, 7001 RE: THO North Cardiac Health and Rehabilitation Submission on the Green Paper The Cardiac Health
a Foundation for Change
 Continuous Quality Improvement ADEs: Steven Utilizing R. Abel, Measurement PharmD, FASHP as Nital Patel, PharmD. MBA a Foundation for Change Sheri Helms, PharmD Candidate Brian Heckman, PharmD Candidate
Continuous Quality Improvement ADEs: Steven Utilizing R. Abel, Measurement PharmD, FASHP as Nital Patel, PharmD. MBA a Foundation for Change Sheri Helms, PharmD Candidate Brian Heckman, PharmD Candidate
DRIVING VALUE IN HEALTHCARE: PERSPECTIVES FROM TWO ACO EXECUTIVES, PART I
 DRIVING VALUE IN HEALTHCARE: PERSPECTIVES FROM TWO ACO EXECUTIVES, PART I A firm understanding of the key components and drivers of healthcare reform is increasingly important within the pharmaceutical,
DRIVING VALUE IN HEALTHCARE: PERSPECTIVES FROM TWO ACO EXECUTIVES, PART I A firm understanding of the key components and drivers of healthcare reform is increasingly important within the pharmaceutical,
Get With The Guidelines - Stroke PMT Special Initiatives Tab for Ohio Coverdell Stroke Program CODING INSTRUCTIONS Effective 10-24-15
 Get With The Guidelines - Stroke PMT Special Initiatives Tab for Ohio Coverdell Stroke Program CODING INSTRUCTIONS Effective 10-24-15 Date and time first seen by ED MD: The time entered should be the earliest
Get With The Guidelines - Stroke PMT Special Initiatives Tab for Ohio Coverdell Stroke Program CODING INSTRUCTIONS Effective 10-24-15 Date and time first seen by ED MD: The time entered should be the earliest
Small and Rural Best Practices Webinar: Telemedicine Strategies. April 23, 2015
 Small and Rural Best Practices Webinar: Telemedicine Strategies April 23, 2015 Funding for this program was provided through the Medicare Rural Hospital Flexibility Grant program. 2 Continuing Education
Small and Rural Best Practices Webinar: Telemedicine Strategies April 23, 2015 Funding for this program was provided through the Medicare Rural Hospital Flexibility Grant program. 2 Continuing Education
AMERICAN BURN ASSOCIATION BURN CENTER VERIFICATION REVIEW PROGRAM Verificatoin Criterea EFFECTIVE JANUARY 1, 2015. Criterion. Level (1 or 2) Number
 Number") Criterion AMERICAN BURN ASSOCIATION BURN CENTER VERIFICATION REVIEW PROGRAM Criterion Level (1 or 2) Number Criterion BURN CENTER ADMINISTRATION 1. The burn center hospital is currently accredited by The
Criterion AMERICAN BURN ASSOCIATION BURN CENTER VERIFICATION REVIEW PROGRAM Criterion Level (1 or 2) Number Criterion BURN CENTER ADMINISTRATION 1. The burn center hospital is currently accredited by The
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS. Karen Unholz, RN, BSN
 INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
Department of Health Services. Behavioral Health Integrated Care. Health Home Certification Application
 Department of Health Services Behavioral Health Integrated Care Health Home Certification Application (Langlade, Lincoln, and Marathon Counties) December 18, 2013 1 Behavioral Health Integrated Care Health
Department of Health Services Behavioral Health Integrated Care Health Home Certification Application (Langlade, Lincoln, and Marathon Counties) December 18, 2013 1 Behavioral Health Integrated Care Health
Helen M. Simpson Rehabilitation Hospital Leveraging IT to Coordinate Care Transitions
 Helen M. Simpson Rehabilitation Hospital Leveraging IT to Coordinate Care Transitions All speakers have completed commercial bias disclosure forms and do not have any conflicts of interest Disclosures
Helen M. Simpson Rehabilitation Hospital Leveraging IT to Coordinate Care Transitions All speakers have completed commercial bias disclosure forms and do not have any conflicts of interest Disclosures
Southwark Clinical Commissioning Group Lambeth Clinical Commissioning Group
 Getting the Vision Right: A multi-disciplinary approach to providing integrated care for respiratory patients Dr Noel Baxter, GP NHS Southwark CCG Dr Irem Patel, Integrated Consultant Respiratory Physician
Getting the Vision Right: A multi-disciplinary approach to providing integrated care for respiratory patients Dr Noel Baxter, GP NHS Southwark CCG Dr Irem Patel, Integrated Consultant Respiratory Physician
Care Coordination at Frederick Regional Health System. Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care
 Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment
 Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
THE 2015 QUALIS HEALTH AWARDS OF EXCELLENCE IN HEALTHCARE QUALITY
 THE 2015 QUALIS HEALTH AWARDS OF EXCELLENCE IN HEALTHCARE QUALITY Since 2002, Qualis Health has presented the annual Awards of Excellence in Healthcare Quality to outstanding organizations in Idaho and
THE 2015 QUALIS HEALTH AWARDS OF EXCELLENCE IN HEALTHCARE QUALITY Since 2002, Qualis Health has presented the annual Awards of Excellence in Healthcare Quality to outstanding organizations in Idaho and
HCAHPS and Value-Based Purchasing Methods and Measurement. Deb Stargardt, Improvement Services Darrel Shanbour, Consulting Services
 HCAHPS and Value-Based Purchasing Methods and Measurement Deb Stargardt, Improvement Services Darrel Shanbour, Consulting Services Today s Learning Objectives Acquire new knowledge pertaining to: A. Hospital
HCAHPS and Value-Based Purchasing Methods and Measurement Deb Stargardt, Improvement Services Darrel Shanbour, Consulting Services Today s Learning Objectives Acquire new knowledge pertaining to: A. Hospital