Improving Transitions & Reducing Readmissions from Skilled Nursing Facilities. Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies
|
|
|
- Mervin Lloyd
- 10 years ago
- Views:
Transcription
1 Improving Transitions & Reducing Readmissions from Skilled Nursing Facilities Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies

2 Agenda Why this is so important What we know: a review of the data Getting started: best practices Applications for other post acute and community based providers & group discussion

3 Objectives Describe why improving transitions & reducing readmissions from SNF is an immediate priority in MD Describe major policy, payment or market forces that align incentives between hospitals & SNFs to reduce readmissions Restate the current average 30-day readmission rate from SNFs Identify INTERACT-3 as the gold-standard reference for improving processes to reduce avoidable hospital transfers from SNF Non-SNF, community based providers make links to their settings

4 Why this is so important now

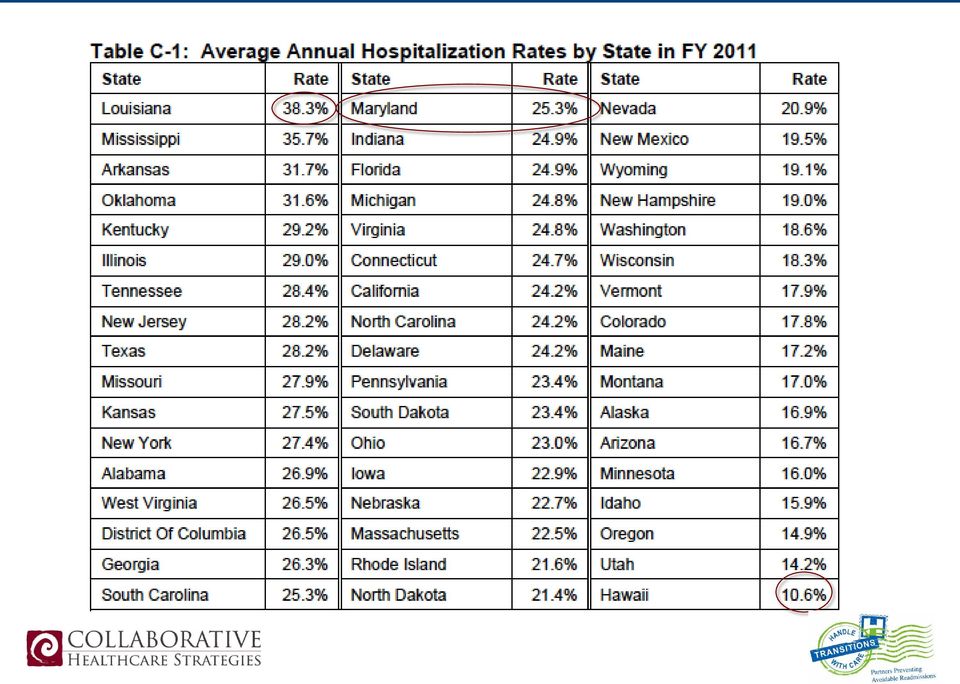
5 Why This Is Important Now - MD Maryland has a substantially higher readmission rate than the US Maryland must close the gap over the next 5 years to meet the US average rate of readmissions This will require a faster pace of improvement in MD than the nation! 2014 financial pressure on hospitals to intensify efforts to reduce RA Attention from state-level stakeholders and associations 125 people from 80 SNFs in MD trained in INTERACT June 2013

6 Why This Is Important Now - National CMS has data on all SNF readmissions Reported quarterly for the US and state-by-state CMS is developing a SNF 30-day all cause readmission measure CMS is developing readmission penalties for SNFs (2017) projected to total $2.2 billion over 10 years Office of the Inspector General s November 2013 report analyzed hospitalizations from SNFs SNF by SNF

7 Leadership Perspectives

8 What we know: A Review of the Data

9

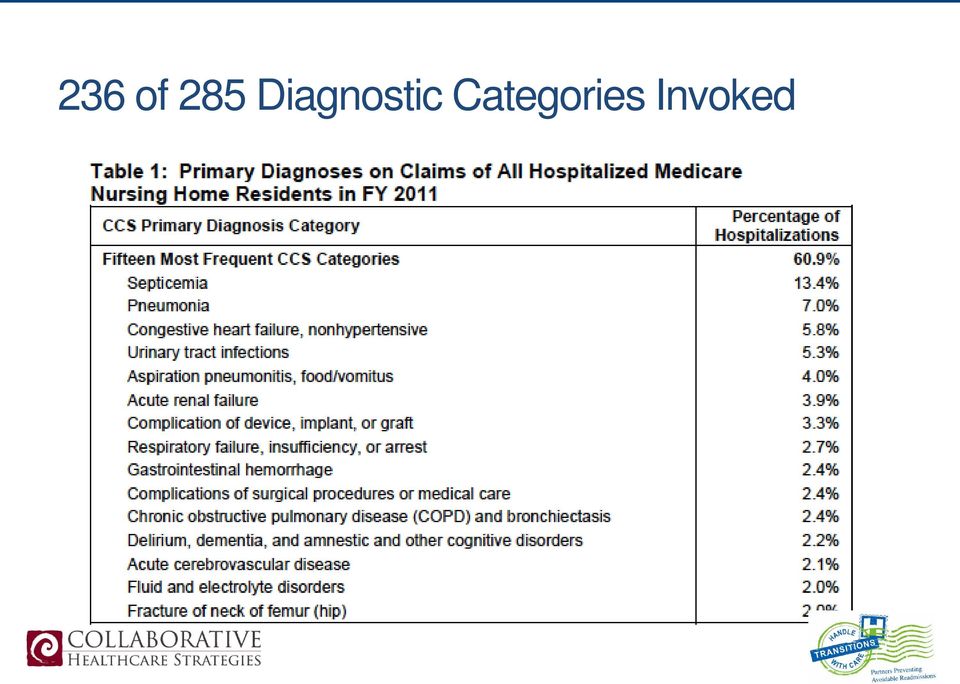
10 when physicians and nursing staff determine require acute care Facility-by-facility analysis SNF and LTC; rates, diagnoses, and $$ analyzed variation across facilities 1 in 4 residents hospitalized >$14 Billion Range of diagnoses, sepsis #1 Wide variation across facilities Measure NH hospitalizations; surveyors to focus on this

11
12 SNF hospitalizations cost more than average Hospitalization of patients from SNF/LTC averages $11,255 Average Medicare hospitalization cost is $8,447 33% higher

13 236 of 285 Diagnostic Categories Invoked
14 Cost of Hospitalization from SNF Reason for Hospitalization Total Cost $ / Hospitalization Sepsis $3 billion $17,430 Pneumonia $850 million $9,500 CHF $640 million $8,700 Aspiration Pneumonia $618 million $12,200 Complications $450 million $14,600 OIG November 2013

15 SNF Readmissions: Focus of Ongoing Research Effect of Hospital-SNF Referral Linkages on Rehospitalization Rahman et al, December 2013 Stronger hospital-snf linkages were found to reduce readmission rates The greater the concentration of discharges a hospital sends to a single SNF, the lower the rate of readmission Specifically lower rates of immediate bounce-backs (days 0-3)

16 SNF Readmissions in Maryland (Medicare) 59% of d/c to home 55% of all RA from home 19% RA rate 25,654 RA in from home % of d/c to HH; 14% of all RA from HH 21% RA rate 6,262 HH RA in % of d/c to SNF; 21% of all RA from SNF 22% RA rate 9,879 SNF RA in 2012

17 Planning for Success: Crunching the Numbers 9, 879 readmissions 230 SNFs in Maryland 9879 / 230 = 43 readmissions on average per facility per year 43 readmissions per year / 12 = 3.5 readmissions per SNF /month Avoid 1 readmission/facility/month 230 x 12 = 2,760 per year! Reduce annual SNF RA from 9879 to 7119!

18 Getting Started: Best Practices

19 INTERACT Interventions to Reduce Acute Care Transfers Developed by Dr Joe Ouslander & colleagues Quality improvement approach & tools Focused on identifying changes early & providing staff tools to act on those observations Provides protocols for managing common issues on-site Supports improved communication between SNF ED Increase hospital awareness of SNF capabilities Advanced care planning.adaptations to assisted living & home health care settings

20 INTERACT-2 Nursing facilities who fully engaged in the quality improvements and tools in the INTERACT program reduced 30-day readmissions by 24%

21
22
23
24
25 INTERACT Clinical Decision Support
26 INTERACT Care Planning Tools
27
28
29
30
31 SNF Circle Back Warm Handoffs SNF Circle Back Questions (Hospital calls back SNF 3-24h after d/c) 1. Did the patient arrive safely? 2. Did you find admission packet in order? 3. Were the medication orders correct? 4. Does the patient s presentation reflect the information you received? 5. Is patient and/or family satisfied with the transition from the hospital to your facility? 6. Have we provided you everything you need to provide excellent care to the patient? Insights Transitions are a PROCESS (forms are useful, but only a tool to achieve intent) Best done ITERATIVELY with COMMUNICATION Source: Emily Skinner, Carolinas Healthcare System
32 Success from Meritus Medical Center Andrea Horton, RN, BSN, ACM
33 ALL Skilled Nursing Facility Readmits Total SNF Readmits
34 Relevance for other PAC & Community Providers Group Discussion
35 Areas of Relevance with INTERACT Review readmissions when they happen Track & monitor readmissions from your service/agency Improve reception into your care Identify key information you need from hospitals & articulate that Improved medication review & clarification procedures Consistent discussions about care preferences Consistent documentation of end of life wishes Monitor clients to identify changes early Use tools to capture those observations Specify reasons to escalate issues to responding providers SBAR, clinical decision aids Develop protocols to manage common issues without ED transfer Communicate your setting/agency s capabilities to hospital Improve communication with hospital Create options for ED to evaluate & return patient to your care
36 Thank you! Next Webinar: January pm Topic: Reducing Readmissions from Home Health
Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services
 Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services Objectives Understand the new consequences to hospitals for discharged clients being re-admitted within selected time
Avoiding Rehospitalizations in LTC Chris Osterberg, RN BSN Pathway Health Services Objectives Understand the new consequences to hospitals for discharged clients being re-admitted within selected time
Readmissions as an Enterprise Priority. Presenters 4/17/2014
 Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center [email protected] Eileen
Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center [email protected] Eileen
2.b.vii Implementing the INTERACT Project (Inpatient Transfer Avoidance Program for SNF)
") 2.b.vii Implementing the INTERACT Project (Inpatient Transfer Avoidance Program for SNF) Project Objective: Skilled nursing facilities (SNFs) will implement the evidence based INTERACT program developed
2.b.vii Implementing the INTERACT Project (Inpatient Transfer Avoidance Program for SNF) Project Objective: Skilled nursing facilities (SNFs) will implement the evidence based INTERACT program developed
Using Root Cause Analysis to Determine Why Readmissions are High. Presentation Objectives. Background Information 11/30/2011
 Using Root Cause Analysis to Determine Why Readmissions are High Nancy Seck RBN, BSN, MPH, CPHQ Director, Quality Management Glendale Memorial Hospital and Health Center Presentation Objectives Identify
Using Root Cause Analysis to Determine Why Readmissions are High Nancy Seck RBN, BSN, MPH, CPHQ Director, Quality Management Glendale Memorial Hospital and Health Center Presentation Objectives Identify
BUNDLING ARE INPATIENT REHABILITATION FACILITIES PREPARED FOR THIS PAYMENT REFORM?
 BUNDLING ARE INPATIENT REHABILITATION FACILITIES PREPARED FOR THIS PAYMENT REFORM? Uniform Data System for Medical Rehabilitation Annual Conference August 10, 2012 Presented by: Donna Cameron Rich Bajner
BUNDLING ARE INPATIENT REHABILITATION FACILITIES PREPARED FOR THIS PAYMENT REFORM? Uniform Data System for Medical Rehabilitation Annual Conference August 10, 2012 Presented by: Donna Cameron Rich Bajner
The INTERACT Program: What is It and Why Does It Matter?
 2 Agenda Housekeeping/Introductions An overview of INTERACT II An overview of a new CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Resources/Next training Questions/Comments
2 Agenda Housekeeping/Introductions An overview of INTERACT II An overview of a new CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Resources/Next training Questions/Comments
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
How Will Hospital Readmission Penalties Impact Skilled Nursing Facilities?
 How Will Hospital Readmission Penalties Impact Skilled Nursing Facilities? Patrick V. Trotta, CPA Director of ElderCare Provider Services Glass Jacobson [email protected] 410 356 1000 Presentation
How Will Hospital Readmission Penalties Impact Skilled Nursing Facilities? Patrick V. Trotta, CPA Director of ElderCare Provider Services Glass Jacobson [email protected] 410 356 1000 Presentation
Home Care s Pivotal Role in Patient Transitions from Acute to Post Acute Care Settings:
 Home Care s Pivotal Role in Patient Transitions from Acute to Post Acute Care Settings: Experiences of a Successful CCTP Program And So Much More! Jane Pike-Benton Senior Director, Home Health & Post Acute
Home Care s Pivotal Role in Patient Transitions from Acute to Post Acute Care Settings: Experiences of a Successful CCTP Program And So Much More! Jane Pike-Benton Senior Director, Home Health & Post Acute
Preparing for the Hospital Readmission Reduction Program
 Preparing for the Hospital Readmission Reduction Program Hospital readmission rates have been rising throughout the years, and the cost of healthcare with them. According to a study conducted by Vincent
Preparing for the Hospital Readmission Reduction Program Hospital readmission rates have been rising throughout the years, and the cost of healthcare with them. According to a study conducted by Vincent
PACCR Webinar Series Presents: The INTERACT Quality Improvement Program Joseph G. Ouslander, M.D.
 paccr.org PACCR Webinar Series Presents: The INTERACT Quality Improvement Program Joseph G. Ouslander, M.D. January 14, 2015 2013 Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior
paccr.org PACCR Webinar Series Presents: The INTERACT Quality Improvement Program Joseph G. Ouslander, M.D. January 14, 2015 2013 Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior
A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates. April 11, 2014
 A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates April 11, 2014 About the QIO Program Leading rapid, large-scale change in health quality: Goals are bolder. The patient is at
A Project to Reengineer Discharges Reduces 30-Day Hospital Readmission Rates April 11, 2014 About the QIO Program Leading rapid, large-scale change in health quality: Goals are bolder. The patient is at
How To Reduce Hospital Readmission
 Reducing Hospital Readmissions & The Affordable Care Act The Game Has Changed Drastically Reducing MSPB Measures Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE
Reducing Hospital Readmissions & The Affordable Care Act The Game Has Changed Drastically Reducing MSPB Measures Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE
Coordinating Transitions of Care: It Takes a Village
 Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
Best of New Jersey: Readmission Reduction Successes INTERACT Quality Improvement Program Version 3.0
 Best of New Jersey: Readmission Reduction Successes INTERACT Quality Improvement Program Version 3.0 Loretta Kaes, BSN, RN-B-C, C-AL, LNHA, CALA Director, Quality Improvement & Clinical Services Health
Best of New Jersey: Readmission Reduction Successes INTERACT Quality Improvement Program Version 3.0 Loretta Kaes, BSN, RN-B-C, C-AL, LNHA, CALA Director, Quality Improvement & Clinical Services Health
Reducing Avoidable Readmissions Effectively (RARE) Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement
 Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement") Reducing Avoidable Readmissions Effectively (RARE) Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement Martha and James Acute Episodes Family Doctor Life Expectancy from chronic diseases
Reducing Avoidable Readmissions Effectively (RARE) Kathy Cummings, RN, BSN, MA Institute for Clinical Systems Improvement Martha and James Acute Episodes Family Doctor Life Expectancy from chronic diseases
Telemedicine Reduces Unnecessary Transfers for Rural Long Term Care Residents. September 18, 2014. Start time is 12:00 PM (central time)
") Telemedicine Reduces Unnecessary Transfers for Rural Long Term Care Residents September 18, 2014. Start time is 12:00 PM (central time) Featured Presenters Shari Davis e-access Director, Avera Health Jacci
Telemedicine Reduces Unnecessary Transfers for Rural Long Term Care Residents September 18, 2014. Start time is 12:00 PM (central time) Featured Presenters Shari Davis e-access Director, Avera Health Jacci
Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights
 Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights Emily Brower Executive Director Accountable Care Programs [email protected] November 2013 1 Contents Overview of
Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights Emily Brower Executive Director Accountable Care Programs [email protected] November 2013 1 Contents Overview of
Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions
 Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions Leslie Becker RN, BS Jennifer Smith RN, MSN, MBA Leslie Frain MSN, RN Jan Machanis
Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions Leslie Becker RN, BS Jennifer Smith RN, MSN, MBA Leslie Frain MSN, RN Jan Machanis
Integrating Post-Acute Providers with Health System Strategies
 Integrating Post-Acute Providers with Health System Strategies Bridging the Acute and Post-Acute Worlds The opinions expressed are those of the presenter and do not necessarily state or reflect the views
Integrating Post-Acute Providers with Health System Strategies Bridging the Acute and Post-Acute Worlds The opinions expressed are those of the presenter and do not necessarily state or reflect the views
September 4, 2012. Submitted Electronically
 September 4, 2012 Ms. Marilyn Tavenner Acting Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1589-P P.O. Box 8016 Baltimore, MD 21244-8016
September 4, 2012 Ms. Marilyn Tavenner Acting Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1589-P P.O. Box 8016 Baltimore, MD 21244-8016
Post-acute care providers: Shortcomings in Medicare s fee-for-service highlight the need for broad reforms
 C h a p t e r7 Post-acute care providers: Shortcomings in Medicare s fee-for-service highlight the need for broad reforms C H A P T E R 7 Post-acute care providers: Shortcomings in Medicare s fee-for-service
C h a p t e r7 Post-acute care providers: Shortcomings in Medicare s fee-for-service highlight the need for broad reforms C H A P T E R 7 Post-acute care providers: Shortcomings in Medicare s fee-for-service
Kim Olmedo, LCSW, CCM CSW-G Social Work Manager, Silverback Care Management
 Kim Olmedo, LCSW, CCM CSW-G Social Work Manager, Silverback Care Management According to AARP, about 8000 people turn 65 every day The Medicare Trustees have estimated that Medicare will run out of money
Kim Olmedo, LCSW, CCM CSW-G Social Work Manager, Silverback Care Management According to AARP, about 8000 people turn 65 every day The Medicare Trustees have estimated that Medicare will run out of money
PL 111-148 and Amendments: Impact on Post-Acute Care for Health Care Systems
 PL 111-148 and Amendments: Impact on Post-Acute Care for Health Care Systems By Kathleen M. Griffin, PhD. There are three key provisions of the law that will have direct impact on post-acute care needs
PL 111-148 and Amendments: Impact on Post-Acute Care for Health Care Systems By Kathleen M. Griffin, PhD. There are three key provisions of the law that will have direct impact on post-acute care needs
Patient to Person. Transitions of Care. Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM
 Patient to Person Transitions of Care Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM Transitions of Care Transitioning from school to adult services (vocational, medical day, etc.)
Patient to Person Transitions of Care Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM Transitions of Care Transitioning from school to adult services (vocational, medical day, etc.)
ACO Operational Innovations Featuring the Winners of NAACOS Call for Innovation
 ACO Operational Innovations Featuring the Winners of NAACOS Call for Innovation January 14, 2014 Brian Silverstein, MD Managing Partner HC Wisdom [email protected] April 24,2014 AGENDA INNOVATION
ACO Operational Innovations Featuring the Winners of NAACOS Call for Innovation January 14, 2014 Brian Silverstein, MD Managing Partner HC Wisdom [email protected] April 24,2014 AGENDA INNOVATION
It Takes Two to ACO A Unique Management Partnership
 AMGA 2014 Annual Conference, April 4, 2014 It Takes Two to ACO A Unique Management Partnership Scott Hayworth MD, President & CEO Mount Kisco Medical Group Alan Bernstein MD, Senior Medical Director Mount
AMGA 2014 Annual Conference, April 4, 2014 It Takes Two to ACO A Unique Management Partnership Scott Hayworth MD, President & CEO Mount Kisco Medical Group Alan Bernstein MD, Senior Medical Director Mount
Using Data to Understand the Medicare Spending Per Beneficiary Measure
 Using Data to Understand the Medicare Spending Per Beneficiary Measure Mary Wheatley, AAMC Jacqueline Matthews, Cleveland Clinic Keely Macmillan, Partners Healthcare December 17, 2013 Webinar Details The
Using Data to Understand the Medicare Spending Per Beneficiary Measure Mary Wheatley, AAMC Jacqueline Matthews, Cleveland Clinic Keely Macmillan, Partners Healthcare December 17, 2013 Webinar Details The
Optum s Role in Mycare Ohio
 Optum s Role in Mycare Ohio What is MyCare Ohio? New opportunities generated by the Affordable Care Act have allowed Ohio to implement the MyCare Ohio program. MyCare Ohio is a demonstration project that
Optum s Role in Mycare Ohio What is MyCare Ohio? New opportunities generated by the Affordable Care Act have allowed Ohio to implement the MyCare Ohio program. MyCare Ohio is a demonstration project that
Creating Strategic Alliances for Post-Acute Coordination of Care
 Creating Strategic Alliances for Post-Acute Coordination of Care Kathleen Yosko, PhD President/CEO Wheaton Franciscan Health Care Sole Illinois property Free-standing facility 101 IRF beds 27 SNF beds
Creating Strategic Alliances for Post-Acute Coordination of Care Kathleen Yosko, PhD President/CEO Wheaton Franciscan Health Care Sole Illinois property Free-standing facility 101 IRF beds 27 SNF beds
Providing and Billing Medicare for Transitional Care Management
 PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
Centers for Medicare & Medicaid Services Special Innovation Projects Overview. Sara Butterfield, RN, BSN, CPHQ October 2015
 Centers for Medicare & Medicaid Services Special Innovation Projects Overview Sara Butterfield, RN, BSN, CPHQ October 2015 Objectives Provide an overview of the CMS Special Innovation Project (SIP) Awards
Centers for Medicare & Medicaid Services Special Innovation Projects Overview Sara Butterfield, RN, BSN, CPHQ October 2015 Objectives Provide an overview of the CMS Special Innovation Project (SIP) Awards
Innovations@Home. Home Health Initiatives Reduce Avoidable Readmissions by Leveraging Innovation
 How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
Harnessing the Power of EHR Data to Improve Patient Outcomes: Yale New Haven Health System and the Rothman Index
 Harnessing the Power of EHR Data to Improve Patient Outcomes: Yale New Haven Health System and the Rothman Index Joan Rimar, RN, DNSc Clinical Management Consultant, Strategic Analytics Yale New Haven
Harnessing the Power of EHR Data to Improve Patient Outcomes: Yale New Haven Health System and the Rothman Index Joan Rimar, RN, DNSc Clinical Management Consultant, Strategic Analytics Yale New Haven
Transitions of Care Management Coding (TCM Code) Tutorial. 1. Introduction Meaning of moderately and high complexity 2
 Tutorial. 1. Introduction Meaning of moderately and high complexity 2") Transitions of Care Management Coding (TCM Code) Tutorial Index 1. Introduction Meaning of moderately and high complexity 2 2. SETMA s Tools for using TCM Code 3 Alert that patient is eligible for TCM
Transitions of Care Management Coding (TCM Code) Tutorial Index 1. Introduction Meaning of moderately and high complexity 2 2. SETMA s Tools for using TCM Code 3 Alert that patient is eligible for TCM
Reducing Avoidable Readmissions by Improving Transitions in Care New Jersey Hospital Association, Princeton, NJ
 Reducing Avoidable Readmissions by Improving Transitions in Care New Jersey Hospital Association, Princeton, NJ Sept. 29, 2015 Registration: 7:45 a.m. Location: NJHA Conference and Event Center Program:
Reducing Avoidable Readmissions by Improving Transitions in Care New Jersey Hospital Association, Princeton, NJ Sept. 29, 2015 Registration: 7:45 a.m. Location: NJHA Conference and Event Center Program:
CURRENT AND FUTURE TRENDS IN POST ACUTE CARE The Value and Role of Acute Inpatient Rehab
 CURRENT AND FUTURE TRENDS IN POST ACUTE CARE The Value and Role of Acute Inpatient Rehab Robert S. Djergaian, M.D. Medical Director Banner Good Samaritan Rehabilitation Institute Stewardship Profitability
CURRENT AND FUTURE TRENDS IN POST ACUTE CARE The Value and Role of Acute Inpatient Rehab Robert S. Djergaian, M.D. Medical Director Banner Good Samaritan Rehabilitation Institute Stewardship Profitability
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS. Karen Unholz, RN, BSN
 INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
WHITE PAPER. How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience
 WHITE PAPER How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience Vocera Communications, Inc. June, 2014 SUMMARY Hospitals that reduce readmission rates
WHITE PAPER How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience Vocera Communications, Inc. June, 2014 SUMMARY Hospitals that reduce readmission rates
Transitional Care Management (TCM) Presented by Noridian Part B Medicare Provider Outreach and Education May 2016
 Presented by Noridian Part B Medicare Provider Outreach and Education May 2016") Transitional Care Management (TCM) Presented by Noridian Part B Medicare Provider Outreach and Education DISCLAIMER This information release is the property of Noridian Administrative Services, LLC (NAS).
Transitional Care Management (TCM) Presented by Noridian Part B Medicare Provider Outreach and Education DISCLAIMER This information release is the property of Noridian Administrative Services, LLC (NAS).
PREVENTING HEART FAILURE READMISSIONS
 PREVENTING HEART FAILURE READMISSIONS Tanya Sprinkle, BSN, RN, CCM Patient and Family Services Coordinator [email protected] 704-878-4534 Michelle Roseman, NHA, MBA Chief Operating Officer/Catawba
PREVENTING HEART FAILURE READMISSIONS Tanya Sprinkle, BSN, RN, CCM Patient and Family Services Coordinator [email protected] 704-878-4534 Michelle Roseman, NHA, MBA Chief Operating Officer/Catawba
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION
 Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Massachusetts Acute Care Hospital Readmissions Profile: July, 2012 to June, 2013 Boston Medical Center September 2015
 Massachusetts Acute Care Hospital Readmissions Profile: July, 2012 to June, 2013 Boston Medical Center September 2015 In June, 2015 the Center for Health Information and Analysis (CHIA) released Hospital-Wide
Massachusetts Acute Care Hospital Readmissions Profile: July, 2012 to June, 2013 Boston Medical Center September 2015 In June, 2015 the Center for Health Information and Analysis (CHIA) released Hospital-Wide
Ann Hablitzel, RN, BSN, MBA Hospice Care of California
 Ann Hablitzel, RN, BSN, MBA Hospice Care of California Objectives Describe the creations of new community based palliative care programs Identify criteria for admission Discuss philosophy and goals Analyze
Ann Hablitzel, RN, BSN, MBA Hospice Care of California Objectives Describe the creations of new community based palliative care programs Identify criteria for admission Discuss philosophy and goals Analyze
Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes. FINANCIAL DISCLOSURE: No relevant financial relationship exists
 Cheri Basso BSN, RN-BC, CHFN Mary Washington Healthcare Fredericksburg, VA Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes FINANCIAL DISCLOSURE: No relevant financial relationship
Cheri Basso BSN, RN-BC, CHFN Mary Washington Healthcare Fredericksburg, VA Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes FINANCIAL DISCLOSURE: No relevant financial relationship
Understanding Care Transitions as a Patient Safety Issue
 Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015
 Leveraging the Continuum to Avoid Unnecessary Utilization While Improving Quality Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015 Karim A. Habibi, FHFMA, MPH, MS Senior
Leveraging the Continuum to Avoid Unnecessary Utilization While Improving Quality Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015 Karim A. Habibi, FHFMA, MPH, MS Senior
Henry Ford Health System Care Coordination and Readmissions Update
 Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates
 Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
1,146 1,097 1,008. 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 Year
 Chairman Brady, Ranking Member McDermott, distinguished Committee members. I am Mark Miller, executive director of the Medicare Payment Advisory Commission (MedPAC). I appreciate the opportunity to be
Chairman Brady, Ranking Member McDermott, distinguished Committee members. I am Mark Miller, executive director of the Medicare Payment Advisory Commission (MedPAC). I appreciate the opportunity to be
10/16/2013. Partnering with Skilled Nursing Facilities & Home Health Agencies to Prevent Hospital Readmissions. Cedars-Sinai Health System
 Partnering with Skilled Nursing Facilities & Home Health Agencies to Prevent Hospital Readmissions Kelley Hart, LVN, Katie Gurvitz, MHA, Michelle Hofhine, RN Turning on the High Beams October 10, 2013
Partnering with Skilled Nursing Facilities & Home Health Agencies to Prevent Hospital Readmissions Kelley Hart, LVN, Katie Gurvitz, MHA, Michelle Hofhine, RN Turning on the High Beams October 10, 2013
FINANCIAL IMPLICATIONS OF EXCESS HOSPITAL READMISSIONS JOSESPH B. HENDERSON, J.D.
 FINANCIAL IMPLICATIONS OF EXCESS HOSPITAL READMISSIONS JOSESPH B. HENDERSON, J.D. Executive MHA Candidate, 2013 University of Southern California Sol Price School of Public Policy Abstract A 2007 Medicare
FINANCIAL IMPLICATIONS OF EXCESS HOSPITAL READMISSIONS JOSESPH B. HENDERSON, J.D. Executive MHA Candidate, 2013 University of Southern California Sol Price School of Public Policy Abstract A 2007 Medicare
4/27/2015. LeadingAge Michigan 2015 Annual Conference Dearborn, MI Monday May 18th, 2015. Jon Golm, President
 LeadingAge Michigan 2015 Annual Conference Dearborn, MI Monday May 18th, 2015 Jon Golm, President Aging Improving Enriched Post Discharge Services, LLC Outcomes Mike Logan, SVP/COO Wellspring Lutheran
LeadingAge Michigan 2015 Annual Conference Dearborn, MI Monday May 18th, 2015 Jon Golm, President Aging Improving Enriched Post Discharge Services, LLC Outcomes Mike Logan, SVP/COO Wellspring Lutheran
What do ACO s and Hospitals want from SNF s and CCRC s
 What do ACO s and Hospitals want from SNF s and CCRC s Presented to the Institute of Senior Living, April 11, 2013 A Division of Kindred Healthcare 1 Assessing the match: What hospitals and ACO s currently
What do ACO s and Hospitals want from SNF s and CCRC s Presented to the Institute of Senior Living, April 11, 2013 A Division of Kindred Healthcare 1 Assessing the match: What hospitals and ACO s currently
Financial Implications: The Push from Inpatient to Outpatient Care
 Financial Implications: The Push from Inpatient to Outpatient Care Brian Baumgardner & Mitchell Mongell THE TRANSFORMATION TO CONSUMER-DRIVEN HEALTHCARE FINANCIAL IMPLICATIONS:THE PUSH FROM INPATIENT TO
Financial Implications: The Push from Inpatient to Outpatient Care Brian Baumgardner & Mitchell Mongell THE TRANSFORMATION TO CONSUMER-DRIVEN HEALTHCARE FINANCIAL IMPLICATIONS:THE PUSH FROM INPATIENT TO
Benchmarks and Best Practices in the Emergency Department. Jeanne McGrayne Premier Consulting Solutions
 1 Benchmarks and Best Practices in the Emergency Department Jeanne McGrayne Premier Consulting Solutions 2 Agenda How we use benchmarks to improve and sustain performance Introduction to tools available
1 Benchmarks and Best Practices in the Emergency Department Jeanne McGrayne Premier Consulting Solutions 2 Agenda How we use benchmarks to improve and sustain performance Introduction to tools available
Blueprint for Post-Acute
 Blueprint for Post-Acute Care Reform Post-acute care is a critical component within our nation s healthcare system and an essential aspect of care for many patients making a full recovery possible after
Blueprint for Post-Acute Care Reform Post-acute care is a critical component within our nation s healthcare system and an essential aspect of care for many patients making a full recovery possible after
Care Transitions: Evidence-based best practices for Case Managers
 Care Transitions: Evidence-based best practices for Case Managers Mary D. Naylor, PhD, FAAN, RN Marian S. Ware Professor in Gerontology Director, NewCourtlandCenter for Transitions & Health University
Care Transitions: Evidence-based best practices for Case Managers Mary D. Naylor, PhD, FAAN, RN Marian S. Ware Professor in Gerontology Director, NewCourtlandCenter for Transitions & Health University
American Diabetes Association Education Recognition Program Overview
 American Diabetes Association Education Recognition Program Overview A brief history of the National Standards for Diabetes Self-Management Education and Support and a walk through the 10 DSME/S standards
American Diabetes Association Education Recognition Program Overview A brief history of the National Standards for Diabetes Self-Management Education and Support and a walk through the 10 DSME/S standards
PCMH and Care Management: Where do we start?
 PCMH and Care Management: Where do we start? Patricia Bohs, RN, BSN Quality Assurance Manager Kelly McCloughan QA Data Manager Wayne Memorial Community Health Centers Honesdale, PA Wayne Memorial Community
PCMH and Care Management: Where do we start? Patricia Bohs, RN, BSN Quality Assurance Manager Kelly McCloughan QA Data Manager Wayne Memorial Community Health Centers Honesdale, PA Wayne Memorial Community
Reimbursement Outlook and Analysis
 HIDA Webinar Series Reimbursement Outlook and Analysis SNFs, HHAs, & IRFs Agenda Current Regulatory Landscape Skilled Nursing Facilities Home Health Agencies Independent Rehab Facilities Healthcare Reform
HIDA Webinar Series Reimbursement Outlook and Analysis SNFs, HHAs, & IRFs Agenda Current Regulatory Landscape Skilled Nursing Facilities Home Health Agencies Independent Rehab Facilities Healthcare Reform
Discharge Planning. Home Care 1. Objectives. Where are they Going?
 Discharge Planning Heidi White, MD Associate Professor of Medicine Yvonne Spurney, RN Associate Chief Nurse Cristina C. Hendrix, DNS, GNP-BC Associate Professor of Nursing Objectives Describe challenges
Discharge Planning Heidi White, MD Associate Professor of Medicine Yvonne Spurney, RN Associate Chief Nurse Cristina C. Hendrix, DNS, GNP-BC Associate Professor of Nursing Objectives Describe challenges
Walden University Q & A continued from Webinar Todd Linden
 Walden University Q & A continued from Webinar Todd Linden General Note: The answers to these questions are my opinion. The mountain of rules and regulations that will be produced from this legislation
Walden University Q & A continued from Webinar Todd Linden General Note: The answers to these questions are my opinion. The mountain of rules and regulations that will be produced from this legislation
Eastern Massachusetts Pioneer Accountable Care Organization (ACO) Quality Standards COMMON EXPECTATIONS FOR SKILLED NURSING FACILITIES.
 Quality Standards COMMON EXPECTATIONS FOR SKILLED NURSING FACILITIES.") Eastern Massachusetts Pioneer Accountable Care Organization (ACO) Quality Standards COMMON EXPECTATIONS FOR SKILLED NURSING FACILITIES Draft 12-5-12 General: 1. Staffing: a. Low staff turnover rate. b.
Eastern Massachusetts Pioneer Accountable Care Organization (ACO) Quality Standards COMMON EXPECTATIONS FOR SKILLED NURSING FACILITIES Draft 12-5-12 General: 1. Staffing: a. Low staff turnover rate. b.
1900 K St. NW Washington, DC 20006 c/o McKenna Long
 1900 K St. NW Washington, DC 20006 c/o McKenna Long Centers for Medicare & Medicaid Services U. S. Department of Health and Human Services Attention CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re:
1900 K St. NW Washington, DC 20006 c/o McKenna Long Centers for Medicare & Medicaid Services U. S. Department of Health and Human Services Attention CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re:
An Introduction to HealthInfoNet s HIE Reporting & Analytics. 6th Annual APS Healthcare Maine Conference May 14, 2015
 An Introduction to HealthInfoNet s HIE Reporting & Analytics 6th Annual APS Healthcare Maine Conference May 14, 2015 Presentation Outline HealthInfoNet Background Current Status of health information exchange
An Introduction to HealthInfoNet s HIE Reporting & Analytics 6th Annual APS Healthcare Maine Conference May 14, 2015 Presentation Outline HealthInfoNet Background Current Status of health information exchange
Hospital readmissions contribute to the increasing. Deployment of Lean Six Sigma in Care Coordination An Improved Discharge Process
 Professional Case Management Vol. 19, No. 2, 77-83 Copyright 2014 Wolters Kluwer Health Lippincott Williams & Wilkins Deployment of Lean Six Sigma in Care Coordination An Improved Discharge Process Susan
Professional Case Management Vol. 19, No. 2, 77-83 Copyright 2014 Wolters Kluwer Health Lippincott Williams & Wilkins Deployment of Lean Six Sigma in Care Coordination An Improved Discharge Process Susan
Improving Outcomes and Saving Lives in Real Time: How Hospitals Can Use Predictive Analytics Across the Care Continuum Essential Hospitals Engagement
 Improving Outcomes and Saving Lives in Real Time: How Hospitals Can Use Predictive Analytics Across the Care Continuum Essential Hospitals Engagement Network February 18, 2015 CHAT FEATURE The chat tool
Improving Outcomes and Saving Lives in Real Time: How Hospitals Can Use Predictive Analytics Across the Care Continuum Essential Hospitals Engagement Network February 18, 2015 CHAT FEATURE The chat tool