Kick off Meeting November 11 13, MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF)
|
|
|
- Clare Hopkins
- 8 years ago
- Views:
Transcription
1 Kick off Meeting November 11 13, 2015 MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF)

2

3

4 Team Composition Justin Huynh, MD Internal Medicine, Physician Champion Mary Laubinger, RN, MSN Executive Director of Quality Laura Tuschhoff, RN, BSN Clinical Outcomes Manager Cathy Martin, RN, BSN, CCM Director, Care Management Christopher Keppler, CHTS PW Senior EMR Analyst Margaret Rechtien, GNP BC, CCM Project Manager Laura Pastrana, RN, BSN Nurse Care Manager HF Supportive Care Team Megan Geyer, RN, BSN Nurse Care Manager HF Supportive Care Team Lori Tasche, RN, BSN, CCM Nurse Care Manager HF Supportive Care Team Jean Young, RN, BSN Nurse Care Manager HF Supportive Care Team Multidisciplinary Readmission Task Force Team, with membership from both our hospitals and clinics.

5 HF Goals & Objectives What are your HF goal(s) and/or objective(s)? To reduce hospital readmissions for HF. To develop a systematic way to manage and improve care for patients with complex psychosocial and medical needs. To provide the right supportive care at the right time (e.g. virtual care in the patient s home, cardiac rehab, home health, palliative care, hospice, etc.). Where are you now? The 30 day HF All Cause Readmission Rate at our Heart & Vascular Hospital in St. Louis was 18.9% in CY Many of our end stage HF patients are admitted to hospice on the day that they die. We need a better way of bringing in supportive care services at the right time. In October 2015, we assembled a HF Supportive Care Team that consists of 4 RN case managers and 2 social workers. Their sole focus is on HF. Mercy opened the world s first Virtual Care Center in St. Louis on October 6, This will allow patients with chronic conditions, such as HF, to be monitored from their home by a physician on a daily basis.

6 HF Readmission Rate Jan Dec 2014
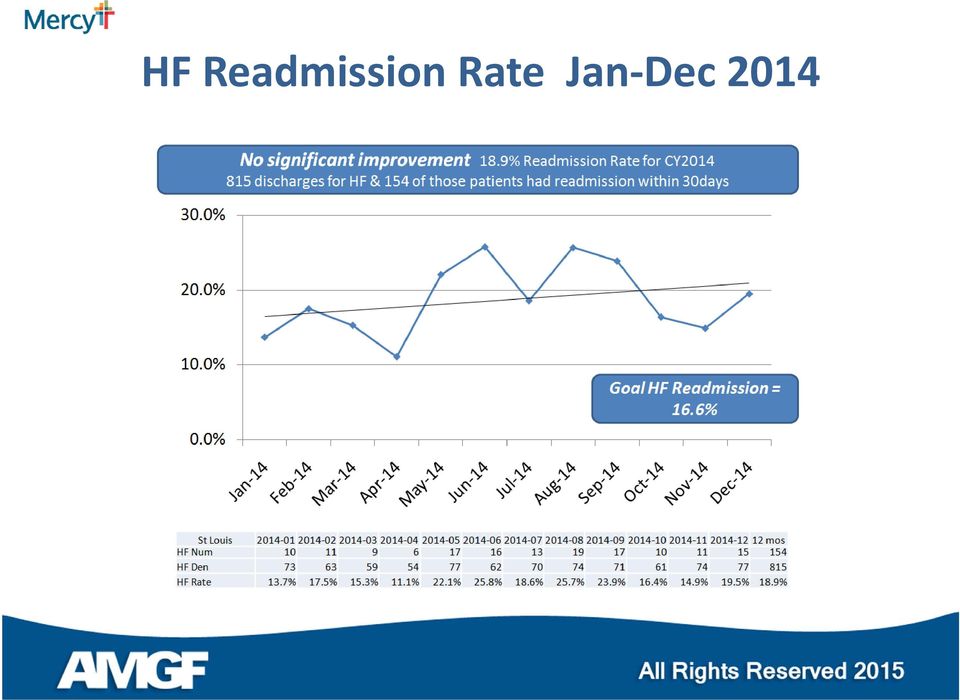
7 HF Intervention & Population Baseline Describe your target HF population(s) and how you identified them. Our emphasis will be on HF patients who are seen at our 96 bed Heart & Vascular Hospital and 980 bed Acute Care Hospital in St. Louis. In CY14, our 30 day HF All Cause Readmission Rates were trending up at these entities. Provide demographics on target population(s). Both urban and rural. Did you set up a HF registry to identify patients, collect additional data elements, etc? We have a HF registry in EPIC. Additionally, Optum TM One allows us to easily identify patients with HF. Describe what went on behind the scenes to implement this intervention? We saw a need to improve care, and assembled a Supportive CM Program for HF patients. This group began seeing patients in October What changes, if any, required in the workflow. We need to incorporate Virtual Care for home monitoring of HF patients. Addition of standing orders for medications adjusting in the home setting. We need a better way of utilizing supportive care services at the right time.

8 HF Intervention & Population Baseline How was healthcare information technology used in this intervention? Inpatient Care Path for Heart Failure (Epic) Daily Discharge Report (Epic) HF 30 Day Readmission Report (Epic) High Risk Readmission Report (Optum TM One) Describe how staff were involved in this intervention. The Inpatient Care Path for HF was designed using evidence based research to guide clinical practice. It is EHR integrated, and helps define the sequencing of timing of health interventions by outlining clear milestones and patient outcomes that must be met daily. Reports help our inpatient and ambulatory Care Management teams target HF patients. What methods were used to change physician practices? 1:1 education about in home care management support for HF patients. Data is shared via our hospital and clinic based committees. Provider scorecards are shared monthly. Medical directors, operations and our quality department perform triple aim rounds every 2 months in the primary care offices. During triple aim rounds, this team meets with providers face to face, to review and discuss their specific quality data. Key quality measures are also tied to provider performance and compensation.

9 Improvement Interventions Our Heart & Vascular Hospital has an inpatient heart failure service with a dedicated team for inpatient care This team does rounding on inpatients with HF, and provides discharge planning that includes transitions of care. Based on the patient s readmission risk assessment score, a follow up appointment is scheduled to occur between 2 7 days post discharge with a PCP or cardiologist. Embedded in our EMR (Epic), we have an inpatient care path for HF. The Inpatient Care Path for HF was designed using evidence based research to guide clinical practice. It helps define the sequencing of timing of health interventions by outlining clear milestones and patient outcomes that must be met daily. The focus of the pathway is to provide the highest quality of care to our patients, speed the delivery of care, minimize delays, reduce variation, manage complexity, foster appropriate resource utilization, and most importantly, improve quality and outcomes. Implementation of a pop up EMR (Epic) that alerts/communicates with any member of the healthcare team that comes in contact with this frail, HF patient. Design of an integrated careplan for all disciplines (inpatient/ambulatory) to access and use.
, we have an inpatient care path for HF. The Inpatient Care Path for HF was designed using evidence based research to guide clinical practice.")
10 Improvement Interventions (continued) Assembling a team of ambulatory nurse care managers and social workers whose sole focus is on HF patients. This team provides in home and telephonic support. The home visit team tries to visit the patient within 24 hours of hospital discharge, and can see patients long term. A social worker is available to address complex social and/or financial needs. This service is FREE for the patient. The team also provides nursing home visits to monitor patient status. They are currently working on standing orders for diuretics, weights, pulse ox, BP, etc. Developing an interdisciplinary team, with a focus on high risk discharges and HF readmissions. This team began meeting weekly on October 15. Those at the table included: ED, Primary Care, Cardiology, Hospitalists, Nutrition, Home Care, Palliative Care, Hospice, Cardiac Rehab and the HF Supportive Care Team. This team discusses patient cases and examines any breakdown in the system which lead to a readmission.

11 Improvement Interventions (continued) Larger ambulatory care management team focuses on patients with less risk. Is an extension of our primary care clinic. This team provides in home and telephonic support and meets weekly with a medical director to review cases. Our HF Supportive Care Team provides transition of care phone calls, as well as in home monitoring of weight, BP and HF symptoms with telephonic and Interactive Voice Response (IVR) products. Patients with HF can submit vital signs, weight and take customized surveys via a home telemonitoring system. The HF Resource Center also provides telephonic disease management education to engage the patient in self management of their heart failure. NEW Virtual Care Center for home monitoring.

12 Measures Used What national clinical standards, if any, did you use as your guideposts and why? CMS readmission standards. Describe data sources and data collection processes, measures, and results. Mercy wide data on hospital readmission rates (CY %) Beta blocker for LVEF < 40% (CY %) ACEI/ARB for LVSD in HF patients (CY14 100%)

13 Challenges or Obstacles What were/are your biggest challenges? Siloed, fragmented care and poor communication amongst our 980 bed acute care hospital, 96 bed heart and vascular hospital, cardiologists, hospitalists, PCPs, ancillary departments and supportive care teams. Changing the culture of ED utilization. Primary care, cardiology and patients are accustomed to using the emergency room for any potential signs of decompensation in HF. Approximately 70% of our admissions and readmissions for patients with HF are for comorbid conditions and diagnoses unrelated to HF. Psychosocial factors have been the source of many of these admissions. Many of our HF patients are critically ill and nearing the end of their lives, and we have seen inadequate enrollment in palliative care and hospice for these patients. Non integrated primary care physicians/cardiologists and the breakdown in communication in regards to discharge plans and follow up care.

14 Outcomes and Successes What are the key elements that will contribute to the success of your initiative? We have created a HF inpatient service to provide optimal diuretic management, medication regimens, length of stay and use of novel technology like CardioMEMS (pulmonary artery pressure monitoring system). We plan to follow patients closely in a longitudinal fashion via our HF Supportive Care Team. They will provide aggressive oral diuretic management and if needed IV diuretic management in the outpatient setting. We plan to integrate our palliative care services into the heart failure team, and will transition patients into palliative care or hospice when appropriate. What are the results? Too soon to determine. Our ambulatory HF Supportive Care Team began seeing patients in October 2015.

15 Future Steps What are your next steps? Weekly interdisciplinary team meetings to discuss challenges and issues. Virtual care resource center. What do you hope to achieve? Better coordination of care for patients. Better access. Better psychosocial support. Better end of life planning.

16 Lessons Learned Describe your lessons learned. In such a large health system, it s easy to lose track of what others are doing.

17 Questions Do you have any questions you would like to pose to the group? Are there any other health systems who are working on HF readmissions, using an ambulatory care management approach?

Connect4 Patients CCCM Primary Care Community. Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM
 Connect4 Patients CCCM Primary Care Community Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM September 17, 2015 Objectives: Describe innovative care management
Connect4 Patients CCCM Primary Care Community Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM September 17, 2015 Objectives: Describe innovative care management
Kick-off Meeting November 11-13, 2015
 Kick-off Meeting November 11-13, 2015 Cornerstone Health Care Heart Function Program Carolina Cardiology Cornerstone Cornerstone Health Care Founded in 1995 as a Physician owned and led Multidisciplinary
Kick-off Meeting November 11-13, 2015 Cornerstone Health Care Heart Function Program Carolina Cardiology Cornerstone Cornerstone Health Care Founded in 1995 as a Physician owned and led Multidisciplinary
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates
 Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals
 Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals 12/18/2013 12/18/13 2013, American Heart Association 1 Thank you for Joining the Webinar Today. The Presentation will Begin
Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals 12/18/2013 12/18/13 2013, American Heart Association 1 Thank you for Joining the Webinar Today. The Presentation will Begin
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT. Norris Vivatrat, MD Associate Medical Director Monarch HealthCare
 PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT
 PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
Essentia Health. Heart Failure and Remote Monitoring. Denise Buxbaum, RN, BSN, CHFN Heart Failure Program Manager
 Essentia Health Heart Failure and Remote Monitoring Denise Buxbaum, RN, BSN, CHFN Heart Failure Program Manager Essentia Health Oct 2014 No reproduction without permission Why Heart Failure? Prevalence
Essentia Health Heart Failure and Remote Monitoring Denise Buxbaum, RN, BSN, CHFN Heart Failure Program Manager Essentia Health Oct 2014 No reproduction without permission Why Heart Failure? Prevalence
3/11/15. COPD Disease Management Tackling the Transition. Objectives. Describe the multidisciplinary approach to inpatient care for COPD patients
 Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
Using Predictive Analytics to Reduce COPD Readmissions
 Using Predictive Analytics to Reduce COPD Readmissions Agenda Information about PinnacleHealth Today s Environment PinnacleHealth Case Study Questions? PinnacleHealth System Non-profit, community teaching
Using Predictive Analytics to Reduce COPD Readmissions Agenda Information about PinnacleHealth Today s Environment PinnacleHealth Case Study Questions? PinnacleHealth System Non-profit, community teaching
Parkview Health s Population Health Journey
 Parkview Health s Population Health Journey Susan McAlister DNP, RN Director Enterprise Care Management Christine Howell BSN, RN Community Based Registered Nurse Objectives: By the completion of the webinar
Parkview Health s Population Health Journey Susan McAlister DNP, RN Director Enterprise Care Management Christine Howell BSN, RN Community Based Registered Nurse Objectives: By the completion of the webinar
Hospital to Physician Office to Home: A Respiratory Led Program Across the Continuum of Care
 Hospital to Physician Office to Home: A Respiratory Led Program Across the Continuum of Care Charley P. Starnes, RRT, RCP Clinical Respiratory Specialist- COPD Education Important Milestones July 2011-
Hospital to Physician Office to Home: A Respiratory Led Program Across the Continuum of Care Charley P. Starnes, RRT, RCP Clinical Respiratory Specialist- COPD Education Important Milestones July 2011-
Care Coordination. The Embedded Care Manager. Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed
 Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
DATA DRIVEN HEALTH CARE TRANSFORMATION
 DATA DRIVEN HEALTH CARE TRANSFORMATION Population Health Analytics as the Foundation for Primary Care Redesign Sylvia Meltzer, MD, LSSGBC Laura Spurr, MPS, PMP Learning Objectives Organization description
DATA DRIVEN HEALTH CARE TRANSFORMATION Population Health Analytics as the Foundation for Primary Care Redesign Sylvia Meltzer, MD, LSSGBC Laura Spurr, MPS, PMP Learning Objectives Organization description
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System
 Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
Best Practices in Managing Patients With Chronic Obstructive Pulmonary Disease (COPD)
") Best Practices in Managing Patients With Chronic Obstructive Pulmonary Disease (COPD) DuPage Medical Group Case Study Organization Profile Established in 1999, DuPage Medical Group (DMG) is a multispecialty
Best Practices in Managing Patients With Chronic Obstructive Pulmonary Disease (COPD) DuPage Medical Group Case Study Organization Profile Established in 1999, DuPage Medical Group (DMG) is a multispecialty
Leveraging EHR to Improve Patient Safety: A Davies Story
 Leveraging EHR to Improve Patient Safety: A Davies Story Claudia Colgan, Vice President of Quality Initiatives Bruce Darrow, MD, PhD, Interim Chief Medical Information Officer Jill Kalman, MD, Director
Leveraging EHR to Improve Patient Safety: A Davies Story Claudia Colgan, Vice President of Quality Initiatives Bruce Darrow, MD, PhD, Interim Chief Medical Information Officer Jill Kalman, MD, Director
UCare provides case management for all UCare members not affiliated with one of the above listed care systems. 2011 UCare for Seniors
 Case Requirements Updated 3/16/2011 According to the Case Society of America (CMSA), Case Model Act of 2009, Case management is a collaborative process of assessment, planning, facilitation, care coordination,
Case Requirements Updated 3/16/2011 According to the Case Society of America (CMSA), Case Model Act of 2009, Case management is a collaborative process of assessment, planning, facilitation, care coordination,
What do ACO s and Hospitals want from SNF s and CCRC s
 What do ACO s and Hospitals want from SNF s and CCRC s Presented to the Institute of Senior Living, April 11, 2013 A Division of Kindred Healthcare 1 Assessing the match: What hospitals and ACO s currently
What do ACO s and Hospitals want from SNF s and CCRC s Presented to the Institute of Senior Living, April 11, 2013 A Division of Kindred Healthcare 1 Assessing the match: What hospitals and ACO s currently
Population Health Management: Banner Health Network s Perspective. Neta Faynboym, Medical Director Banner Health Network
 Population Health Management: Banner Health Network s Perspective Neta Faynboym, Medical Director Banner Health Network 29 Acute Care Hospitals BANNER AT A GLANCE Banner Health Network with 400K lives
Population Health Management: Banner Health Network s Perspective Neta Faynboym, Medical Director Banner Health Network 29 Acute Care Hospitals BANNER AT A GLANCE Banner Health Network with 400K lives
Reducing Readmissions with Predictive Analytics
 Reducing Readmissions with Predictive Analytics Conway Regional Health System uses analytics and the LACE Index from Medisolv s RAPID business intelligence software to identify patients poised for early
Reducing Readmissions with Predictive Analytics Conway Regional Health System uses analytics and the LACE Index from Medisolv s RAPID business intelligence software to identify patients poised for early
Presented by: Char Brar, ACNP, MS(Chem.), MSN, RN Cardiology Nurse Practitioner JBVAMC, Chicago
, MSN, RN Cardiology Nurse Practitioner JBVAMC, Chicago") Presented by: Char Brar, ACNP, MS(Chem.), MSN, RN Cardiology Nurse Practitioner JBVAMC, Chicago 200 bed acute care facility 4 Community Based Out-patient Clinics (CBOCs) 58,000 Veterans IN FY 2008 : 768
Presented by: Char Brar, ACNP, MS(Chem.), MSN, RN Cardiology Nurse Practitioner JBVAMC, Chicago 200 bed acute care facility 4 Community Based Out-patient Clinics (CBOCs) 58,000 Veterans IN FY 2008 : 768
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment
 Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
Readmissions as an Enterprise Priority. Presenters 4/17/2014
 Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center Vmaniscalco@parkmanorrehab.com Eileen
Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center Vmaniscalco@parkmanorrehab.com Eileen
Be Careful What You Ask For A Predictive Model That Really Works
 Be Careful What You Ask For A Predictive Model That Really Works Rod Christensen, MD President, Allina Health Clinics Cheryl Hermann, RN, MBA Vice President, Clinic Operations & Patient Care Services Karen
Be Careful What You Ask For A Predictive Model That Really Works Rod Christensen, MD President, Allina Health Clinics Cheryl Hermann, RN, MBA Vice President, Clinic Operations & Patient Care Services Karen
1. Executive Summary Problem/Opportunity: Evidence: Baseline Data: Intervention: Results:
 A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
Dual RFI Response Summary
 Dual RFI Response Summary Improving Care through Integrated Medicare and Medi- Cal Delivery Models Stuart Levine, MD., MHA. Keith Wilson, MD Robert Margolis, MD. Stakeholder Meeting August 30, 2011 1 Organization
Dual RFI Response Summary Improving Care through Integrated Medicare and Medi- Cal Delivery Models Stuart Levine, MD., MHA. Keith Wilson, MD Robert Margolis, MD. Stakeholder Meeting August 30, 2011 1 Organization
Implementing a clustered acute stroke unit at a community hospital improves patient care
 Implementing a clustered acute stroke unit at a community hospital improves patient care Linda Dykes, BScPT Manager, Sarnia Lambton District Stroke Centre Krista Steeves, BHScPT Physiotherapist, Bluewater
Implementing a clustered acute stroke unit at a community hospital improves patient care Linda Dykes, BScPT Manager, Sarnia Lambton District Stroke Centre Krista Steeves, BHScPT Physiotherapist, Bluewater
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS. Karen Unholz, RN, BSN
 INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
Game Changer at the Primary Care Practice Embedded Care Management. Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012
 Game Changer at the Primary Care Practice Embedded Care Management Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012 Objectives To describe the recent evolution of care management at
Game Changer at the Primary Care Practice Embedded Care Management Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012 Objectives To describe the recent evolution of care management at
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION
 Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Understanding Care Transitions as a Patient Safety Issue
 Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
Cloud Computing / Tele- Health in a Novel Integrated CHF Disease Management Program: The Israeli Experience
 Cloud Computing / Tele- Health in a Novel Integrated CHF Disease Management Program: The Israeli Experience Haim Silber MD Programs Initiator Maccabi Health Care services and Gertner Institute, ISRAEL
Cloud Computing / Tele- Health in a Novel Integrated CHF Disease Management Program: The Israeli Experience Haim Silber MD Programs Initiator Maccabi Health Care services and Gertner Institute, ISRAEL
2.b.vii Implementing the INTERACT Project (Inpatient Transfer Avoidance Program for SNF)
") 2.b.vii Implementing the INTERACT Project (Inpatient Transfer Avoidance Program for SNF) Project Objective: Skilled nursing facilities (SNFs) will implement the evidence based INTERACT program developed
2.b.vii Implementing the INTERACT Project (Inpatient Transfer Avoidance Program for SNF) Project Objective: Skilled nursing facilities (SNFs) will implement the evidence based INTERACT program developed
CARE MANAGEMENT SERIES Part 6 Developing a Staffing Model That Works
 CARE MANAGEMENT SERIES Part 6 Developing a Staffing Model That Works We will get to staffing but let s start by reviewing core functions. Care Management As we have discussed previously, Care Management
CARE MANAGEMENT SERIES Part 6 Developing a Staffing Model That Works We will get to staffing but let s start by reviewing core functions. Care Management As we have discussed previously, Care Management
High Desert Medical Group Connections for Life Program Description
 High Desert Medical Group Connections for Life Program Description POLICY: High Desert Medical Group ("HDMG") promotes patient health and wellbeing by actively coordinating services for members with multiple
High Desert Medical Group Connections for Life Program Description POLICY: High Desert Medical Group ("HDMG") promotes patient health and wellbeing by actively coordinating services for members with multiple
Care Coordination at Frederick Regional Health System. Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care
 Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
NYSPFP Preventable Readmissions Initiative: Pilot Review and Post Hospital Care
 NYSPFP Preventable Readmissions Initiative: Pilot Review and Post Hospital Care June 17, 2014 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association
NYSPFP Preventable Readmissions Initiative: Pilot Review and Post Hospital Care June 17, 2014 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association
Ann Hablitzel, RN, BSN, MBA Hospice Care of California
 Ann Hablitzel, RN, BSN, MBA Hospice Care of California Objectives Describe the creations of new community based palliative care programs Identify criteria for admission Discuss philosophy and goals Analyze
Ann Hablitzel, RN, BSN, MBA Hospice Care of California Objectives Describe the creations of new community based palliative care programs Identify criteria for admission Discuss philosophy and goals Analyze
Realizing ACO Success with ICW Solutions
 Realizing ACO Success with ICW Solutions A Pathway to Collaborative Care Coordination and Care Management Decrease Healthcare Costs Improve Population Health Enhance Care for the Individual connect. manage.
Realizing ACO Success with ICW Solutions A Pathway to Collaborative Care Coordination and Care Management Decrease Healthcare Costs Improve Population Health Enhance Care for the Individual connect. manage.
caresy caresync Chronic Care Management
 caresy Chronic Care Management THE PROBLEM Chronic diseases and conditions, including heart disease, diabetes, COPD and obesity, are among the most common, expensive, and preventable health problems in
caresy Chronic Care Management THE PROBLEM Chronic diseases and conditions, including heart disease, diabetes, COPD and obesity, are among the most common, expensive, and preventable health problems in
1. TITLE: Colin A. Banas MD, MSHA Chief Medical Information Officer Secondary Point of Contact: 804-827- 4196, cbanas@mcvh-vcu.edu
 1. TITLE: Using Health Information Technology - CPOE to Advance Performance Improvement in Heart Failure Patients at Virginia Commonwealth University Health System 2. ORGANIZATION: Virginia Commonwealth
1. TITLE: Using Health Information Technology - CPOE to Advance Performance Improvement in Heart Failure Patients at Virginia Commonwealth University Health System 2. ORGANIZATION: Virginia Commonwealth
National Clinical Programmes
 National Clinical Programmes Section 3 Background information on the National Clinical Programmes Mission, Vision and Objectives July 2011 V0. 6_ 4 th July, 2011 1 National Clinical Programmes: Mission
National Clinical Programmes Section 3 Background information on the National Clinical Programmes Mission, Vision and Objectives July 2011 V0. 6_ 4 th July, 2011 1 National Clinical Programmes: Mission
Innovations@Home. Home Health Initiatives Reduce Avoidable Readmissions by Leveraging Innovation
 How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
COPD 30 Day Readmission Project SAINT THOMAS RUTHERFORD MURFREESBORO, TN SEPTEMBER 15, 2015 DAVID M. SELLERS, MD, MBA
 COPD 30 Day Readmission Project SAINT THOMAS RUTHERFORD MURFREESBORO, TN SEPTEMBER 15, 2015 DAVID M. SELLERS, MD, MBA USA COPD Data 24 Million Americans under the age of 65 with COPD Almost 20% readmit
COPD 30 Day Readmission Project SAINT THOMAS RUTHERFORD MURFREESBORO, TN SEPTEMBER 15, 2015 DAVID M. SELLERS, MD, MBA USA COPD Data 24 Million Americans under the age of 65 with COPD Almost 20% readmit
Five Myths Surrounding the Business of Population Health Management
 Five Myths Surrounding the Business of Population Health Management Joan Moss, RN, MSN Robert Sehring Chief Nursing Officer and Chief Ministry Services Officer, Senior Vice President, Sg2 OSF HealthCare
Five Myths Surrounding the Business of Population Health Management Joan Moss, RN, MSN Robert Sehring Chief Nursing Officer and Chief Ministry Services Officer, Senior Vice President, Sg2 OSF HealthCare
Henry Ford Health System Care Coordination and Readmissions Update
 Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
New York Presbyterian Innovations in Health Care Reform at Academic Medical Centers
 New York Presbyterian Innovations in Health Care Reform at Academic Medical Centers October 28, 2011 Timothy G Ferris, MD, MPH Mass General Physicians Organization, Medical Director Associate Professor,
New York Presbyterian Innovations in Health Care Reform at Academic Medical Centers October 28, 2011 Timothy G Ferris, MD, MPH Mass General Physicians Organization, Medical Director Associate Professor,
Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions
 Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions Scott Flinn MD Deborah Schutz RN JD Fritz Steen RN Arch Health Partners A medical foundation formed
Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions Scott Flinn MD Deborah Schutz RN JD Fritz Steen RN Arch Health Partners A medical foundation formed
Carolina s Journey: Turning Big Data Into Better Care. Michael Dulin, MD, PhD
 Carolina s Journey: Turning Big Data Into Better Care Michael Dulin, MD, PhD Current State: Massive investments in EMR systems Rapidly Increase Amount of Data (Velocity, Volume, Veracity) The Data has
Carolina s Journey: Turning Big Data Into Better Care Michael Dulin, MD, PhD Current State: Massive investments in EMR systems Rapidly Increase Amount of Data (Velocity, Volume, Veracity) The Data has
9/23/2014. Mission To improve the health of the people in the communities we serve.
 Big Data & Reduced Readmissions Chris Myers, MS, RN, CCM, Director of Care Transitions, Texas Health Harris Methodist Hospital Hurst-Euless- Bedford Anand Shah, MD, Vice President, Parkland Center for
Big Data & Reduced Readmissions Chris Myers, MS, RN, CCM, Director of Care Transitions, Texas Health Harris Methodist Hospital Hurst-Euless- Bedford Anand Shah, MD, Vice President, Parkland Center for
Predictive Analytics in Action: Tackling Readmissions
 Predictive Analytics in Action: Tackling Readmissions Jason Haupt Sr. Statistician & Manager of Clinical Analysis July 17, 2013 Agenda Background Lifecycle Current status Discussion 2 Goals for today Describe
Predictive Analytics in Action: Tackling Readmissions Jason Haupt Sr. Statistician & Manager of Clinical Analysis July 17, 2013 Agenda Background Lifecycle Current status Discussion 2 Goals for today Describe
8/20/2013. Objectives
 Improving Wound Outcomes with a Coordinated Cross Continuum Wound Service Debra Healey, MSN, RN, CPHRM, NEA-BC Objectives 1. Describe several examples of innovative business planning to provide quality
Improving Wound Outcomes with a Coordinated Cross Continuum Wound Service Debra Healey, MSN, RN, CPHRM, NEA-BC Objectives 1. Describe several examples of innovative business planning to provide quality
2013 ACO Quality Measures
 ACO 1-7 Patient Satisfaction Survey Consumer Assessment of HealthCare Providers Survey (CAHPS) 1. Getting Timely Care, Appointments, Information 2. How well Your Providers Communicate 3. Patient Rating
ACO 1-7 Patient Satisfaction Survey Consumer Assessment of HealthCare Providers Survey (CAHPS) 1. Getting Timely Care, Appointments, Information 2. How well Your Providers Communicate 3. Patient Rating
Congestive Heart Failure Management Program
 Congestive Heart Failure Management Program The Congestive Heart Failure Program is the third statewide disease management program developed by CCNC. The clinical directors reviewed prevalence and outcome
Congestive Heart Failure Management Program The Congestive Heart Failure Program is the third statewide disease management program developed by CCNC. The clinical directors reviewed prevalence and outcome
Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination of care for both services.
 Domain 3 Projects 3.a.i Integration of Primary Care and Behavioral Health Services Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination
Domain 3 Projects 3.a.i Integration of Primary Care and Behavioral Health Services Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination
MEDICAL MANAGEMENT PROGRAM LAKELAND REGIONAL MEDICAL CENTER
 MEDICAL MANAGEMENT PROGRAM LAKELAND REGIONAL MEDICAL CENTER Publication Year: 2013 Summary: The Medical Management Program provides individualized care plans for frequent visitors presenting to the Emergency
MEDICAL MANAGEMENT PROGRAM LAKELAND REGIONAL MEDICAL CENTER Publication Year: 2013 Summary: The Medical Management Program provides individualized care plans for frequent visitors presenting to the Emergency
Berkshire Medical Center Heart Failure Program
 Berkshire Medical Center Heart Failure Program Reducing Readmissions A Multi Disciplinary Approach 1 Project Goals To improve the overall care of Berkshire County Heart Failure Patients Reduce 30 day readmission
Berkshire Medical Center Heart Failure Program Reducing Readmissions A Multi Disciplinary Approach 1 Project Goals To improve the overall care of Berkshire County Heart Failure Patients Reduce 30 day readmission
Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015
 Leveraging the Continuum to Avoid Unnecessary Utilization While Improving Quality Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015 Karim A. Habibi, FHFMA, MPH, MS Senior
Leveraging the Continuum to Avoid Unnecessary Utilization While Improving Quality Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015 Karim A. Habibi, FHFMA, MPH, MS Senior
The University of Chicago Medicine: Driving Engagement With Interactive Care
 The University of Chicago Medicine: Driving Engagement With Interactive Care 1 Training front-line clinical and administrative staff to encourage patients to use technology, but also reminding them of
The University of Chicago Medicine: Driving Engagement With Interactive Care 1 Training front-line clinical and administrative staff to encourage patients to use technology, but also reminding them of
Population Health Solutions for Employers MEDIA RESOURCES
 Population Health Solutions for Employers MEDIA RESOURCES ABOUT MISSIONPOINT MissionPoint s mission is to make healthcare more affordable, accessible and improve the quality of care for our members. MissionPoint
Population Health Solutions for Employers MEDIA RESOURCES ABOUT MISSIONPOINT MissionPoint s mission is to make healthcare more affordable, accessible and improve the quality of care for our members. MissionPoint
Post-Acute Care Transitions: An Essential Component of Accountable Care
 : An Essential Component of Accountable Care Bruce C. Smith, MD, FACP Associate Medical Director, Strategy Deployment Group Health Physicians, Seattle, WA Smith.bc@ghc.org AMGA 2012 Institute for Quality
: An Essential Component of Accountable Care Bruce C. Smith, MD, FACP Associate Medical Director, Strategy Deployment Group Health Physicians, Seattle, WA Smith.bc@ghc.org AMGA 2012 Institute for Quality
Making the Transition: Improving Coordination, Lowering Readmission, and Expanding the Care Team through Data-Driven Risk Stratification at Discharge
 Making the Transition: Improving Coordination, Lowering Readmission, and Expanding the Care Team through Data-Driven Risk Stratification at Discharge Jennifer McNay, MD Cindi Goddard, MPH, BSN, RN Mercy
Making the Transition: Improving Coordination, Lowering Readmission, and Expanding the Care Team through Data-Driven Risk Stratification at Discharge Jennifer McNay, MD Cindi Goddard, MPH, BSN, RN Mercy
ACO Project Overview and Key Elements. Presented to FSSA September 3, 2013. 2013 Franciscan Alliance, Inc.
 ACO Project Overview and Key Elements Presented to FSSA September 3, 2013 2013 Franciscan Alliance, Inc. Background of Presentation House Enrolled Act 1328 requires the Indiana Family and Social Services
ACO Project Overview and Key Elements Presented to FSSA September 3, 2013 2013 Franciscan Alliance, Inc. Background of Presentation House Enrolled Act 1328 requires the Indiana Family and Social Services
Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights
 Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights Emily Brower Executive Director Accountable Care Programs Emily_Brower@AtriusHealth.org November 2013 1 Contents Overview of
Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights Emily Brower Executive Director Accountable Care Programs Emily_Brower@AtriusHealth.org November 2013 1 Contents Overview of
DSRIP QUARTERLY REVIEW PROCESS: Project Requirement - Timeframe. Project Requirement - Unit Level Reporting
 DSRIP QUARTERLY REVIEW PROCESS: PPSs will submit a quarterly report to the Independent Assessor throughout the DSRIP program via the automated MAPP tool which includes Domain 1 DSRIP Requirement Milestone
DSRIP QUARTERLY REVIEW PROCESS: PPSs will submit a quarterly report to the Independent Assessor throughout the DSRIP program via the automated MAPP tool which includes Domain 1 DSRIP Requirement Milestone
Pediatric Cardiac Rehabilitation Program. Lynne Telfer, RN
 Pediatric Cardiac Rehabilitation Program Lynne Telfer, RN Introduction Congenital heart disease is the number 1 birth defect in the world. Heart disease is second only to asthma as the leading cause of
Pediatric Cardiac Rehabilitation Program Lynne Telfer, RN Introduction Congenital heart disease is the number 1 birth defect in the world. Heart disease is second only to asthma as the leading cause of
CHANGING YOUR CASE MANAGEMENT MODEL OF CARE. Jan Lear, RN, CMC Director of Case Management MedStar Franklin Square Medical Center
 CHANGING YOUR CASE MANAGEMENT MODEL OF CARE Jan Lear, RN, CMC Director of Case Management MedStar Franklin Square Medical Center 1 Program Objectives To be able to describe the compliance and regulatory
CHANGING YOUR CASE MANAGEMENT MODEL OF CARE Jan Lear, RN, CMC Director of Case Management MedStar Franklin Square Medical Center 1 Program Objectives To be able to describe the compliance and regulatory
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
PREVENTING HEART FAILURE READMISSIONS
 PREVENTING HEART FAILURE READMISSIONS Tanya Sprinkle, BSN, RN, CCM Patient and Family Services Coordinator tanya.sprinkle@iredellmemorial.org 704-878-4534 Michelle Roseman, NHA, MBA Chief Operating Officer/Catawba
PREVENTING HEART FAILURE READMISSIONS Tanya Sprinkle, BSN, RN, CCM Patient and Family Services Coordinator tanya.sprinkle@iredellmemorial.org 704-878-4534 Michelle Roseman, NHA, MBA Chief Operating Officer/Catawba
Home Health Care Today: Higher Acuity Level of Patients Highly skilled Professionals Costeffective Uses of Technology Innovative Care Techniques
 Comprehensive EHR Infrastructure Across the Health Care System The goal of the Administration and the Department of Health and Human Services to achieve an infrastructure for interoperable electronic health
Comprehensive EHR Infrastructure Across the Health Care System The goal of the Administration and the Department of Health and Human Services to achieve an infrastructure for interoperable electronic health
Disease Management Identifications and Stratification Health Risk Assessment Level 1: Level 2: Level 3: Stratification
 Disease Management UnitedHealthcare Disease Management (DM) programs are part of our innovative Care Management Program. Our Disease Management (DM) program is guided by the principles of the UnitedHealthcare
Disease Management UnitedHealthcare Disease Management (DM) programs are part of our innovative Care Management Program. Our Disease Management (DM) program is guided by the principles of the UnitedHealthcare
Table 1 Performance Measures. Quality Monitoring P4P Yr1 Yr2 Yr3. Specification Source. # Category Performance Measure
 Table 1 Performance Measures # Category Performance Measure 1 Behavioral Health Risk Assessment and Follow-up 1) Behavioral Screening/ Assessment within 60 days of enrollment New Enrollees who completed
Table 1 Performance Measures # Category Performance Measure 1 Behavioral Health Risk Assessment and Follow-up 1) Behavioral Screening/ Assessment within 60 days of enrollment New Enrollees who completed
University of Colorado Health Sciences Center
 University of Colorado Health Sciences Center Colorado Palliative Medicine Fellowship Program Thank you for your interest in the Colorado Palliative Medicine Fellowship Program at the University of Colorado
University of Colorado Health Sciences Center Colorado Palliative Medicine Fellowship Program Thank you for your interest in the Colorado Palliative Medicine Fellowship Program at the University of Colorado
THE ADVANCED CARE PROJECT
 THE ADVANCED CARE PROJECT Table of Contents Executive Summary... 2 Background... 3 Advanced Illness: Challenges and Responses... 4 Advanced Care: Creating a New Continuum of Care... 4 The Advanced Care
THE ADVANCED CARE PROJECT Table of Contents Executive Summary... 2 Background... 3 Advanced Illness: Challenges and Responses... 4 Advanced Care: Creating a New Continuum of Care... 4 The Advanced Care
Pushing the Envelope of Population Health
 Pushing the Envelope of Population Health Timothy Ferris, MD, MPH Senior Vice President, Population Health Management, Partners HealthCare May 15, 2014 DISCLAIMER: The views and opinions expressed in this
Pushing the Envelope of Population Health Timothy Ferris, MD, MPH Senior Vice President, Population Health Management, Partners HealthCare May 15, 2014 DISCLAIMER: The views and opinions expressed in this
DELIVERING VALUE THROUGH TECHNOLOGY
 DELIVERING VALUE THROUGH TECHNOLOGY Mark Nelson, MD - EMR Physician Champion Krishna Ramachandran - Chief Information and Transformation Officer Karen Adamson - Director, Epic Clinical Applications DuPage
DELIVERING VALUE THROUGH TECHNOLOGY Mark Nelson, MD - EMR Physician Champion Krishna Ramachandran - Chief Information and Transformation Officer Karen Adamson - Director, Epic Clinical Applications DuPage
The New Complex Patient. of Diabetes Clinical Programming
 The New Complex Patient as Seen Through the Lens of Diabetes Clinical Programming 1 Valerie Garrett, M.D. Medical Director, Diabetes Center at Mission Health System Nov 6, 2014 Diabetes Health Burden High
The New Complex Patient as Seen Through the Lens of Diabetes Clinical Programming 1 Valerie Garrett, M.D. Medical Director, Diabetes Center at Mission Health System Nov 6, 2014 Diabetes Health Burden High
Plenary Session 1. Health Dimensions Group. 2010 Health Dimensions Group
 Plenary Session 1 Kathleen M. Griffin, PhD Health Dimensions Group March 31, 2011 Hospital, Post Acute and Long-Term Care Collaboration in Health Care Reform: Critical Success Factors National Summit:
Plenary Session 1 Kathleen M. Griffin, PhD Health Dimensions Group March 31, 2011 Hospital, Post Acute and Long-Term Care Collaboration in Health Care Reform: Critical Success Factors National Summit:
LOURDES MEDICAL CENTER BURLINGTON COUNTY
 LOURDES MEDICAL CENTER BURLINGTON COUNTY DSRIP Learning Collaborative February 12, 2015 Dr. Michael J. Horwitz, D.O. Cardiologist Lourdes Cardiology Services LOURDES MEDICAL CENTER BURLINGTON COUNTY (LMCBC)
LOURDES MEDICAL CENTER BURLINGTON COUNTY DSRIP Learning Collaborative February 12, 2015 Dr. Michael J. Horwitz, D.O. Cardiologist Lourdes Cardiology Services LOURDES MEDICAL CENTER BURLINGTON COUNTY (LMCBC)
Main Section of the proposal: 1. Overall Aim & Objectives:
 Main Section of the proposal: 1. Overall Aim & Objectives: Over the past two decades Providence Health & Services has developed a comprehensive tobacco cessation program within our health system. The foundation
Main Section of the proposal: 1. Overall Aim & Objectives: Over the past two decades Providence Health & Services has developed a comprehensive tobacco cessation program within our health system. The foundation
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
Population Health Management Infrastructure
 Population Health Management Infrastructure William Pagano MD, MPH SVP of Clinical Operations Doreen Colella RN, MSN AVP of Quality Interfaces The Azara reporting tool interfaces with multiple systems.
Population Health Management Infrastructure William Pagano MD, MPH SVP of Clinical Operations Doreen Colella RN, MSN AVP of Quality Interfaces The Azara reporting tool interfaces with multiple systems.
From the Ground Up: The implementation of a Transition Care Program (TOC) and its impact in COPD 30-day readmissions
 and its impact in COPD 30-day readmissions") From the Ground Up: The implementation of a Transition Care Program (TOC) and its impact in COPD 30-day readmissions Cristiane L. Fukuda RN, MSN, ANP-BC Email: cristiane.fukuda@northside.com Office: 404-851-6914
From the Ground Up: The implementation of a Transition Care Program (TOC) and its impact in COPD 30-day readmissions Cristiane L. Fukuda RN, MSN, ANP-BC Email: cristiane.fukuda@northside.com Office: 404-851-6914
GP SERVICES COMMITTEE Conferencing and Telephone Management INCENTIVES. Revised 2015. Society of General Practitioners
 GP SERVICES COMMITTEE Conferencing and Telephone Management INCENTIVES Revised 2015 Society of General Practitioners Conference & Telephone Fees (G14077, G14015, G14016, G14017, G14018, G14019, G14021,
GP SERVICES COMMITTEE Conferencing and Telephone Management INCENTIVES Revised 2015 Society of General Practitioners Conference & Telephone Fees (G14077, G14015, G14016, G14017, G14018, G14019, G14021,
HealthCare Partners of Nevada. Heart Failure
 HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
Patient to Person. Transitions of Care. Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM
 Patient to Person Transitions of Care Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM Transitions of Care Transitioning from school to adult services (vocational, medical day, etc.)
Patient to Person Transitions of Care Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM Transitions of Care Transitioning from school to adult services (vocational, medical day, etc.)
HOW TO PREPARE FOR THE FUTURE COMPLEX CARE MANAGEMENT
 HOW TO PREPARE FOR THE FUTURE COMPLEX CARE MANAGEMENT #607 Friday, October 30, 2015 MARY NEWBERRY, MSN RN, DIRECTOR, HOME BASED & TRANSITIONAL CARE DEBORAH BRADLEY, MSN RN, MANAGER HOME HEALTH CARE BETH
HOW TO PREPARE FOR THE FUTURE COMPLEX CARE MANAGEMENT #607 Friday, October 30, 2015 MARY NEWBERRY, MSN RN, DIRECTOR, HOME BASED & TRANSITIONAL CARE DEBORAH BRADLEY, MSN RN, MANAGER HOME HEALTH CARE BETH
Medicare Shared Savings Program Quality Measure Benchmarks for the 2015 Reporting Year
 Medicare Shared Savings Program Quality Measure Benchmarks for the 2015 Reporting Year Release Notes/Summary of Changes (February 2015): Issued correction of 2015 benchmarks for ACO-9 and ACO-10 quality
Medicare Shared Savings Program Quality Measure Benchmarks for the 2015 Reporting Year Release Notes/Summary of Changes (February 2015): Issued correction of 2015 benchmarks for ACO-9 and ACO-10 quality
Affinity s Medical Home Journey Operational, Clinical and Financial Perspectives
 Affinity s Medical Home Journey Operational, Clinical and Financial Perspectives Dr. Christine Griger - President Timothy Loch - COO Jane Curran-Meuli Regional Director Affinity Health System Top 100 Integrated
Affinity s Medical Home Journey Operational, Clinical and Financial Perspectives Dr. Christine Griger - President Timothy Loch - COO Jane Curran-Meuli Regional Director Affinity Health System Top 100 Integrated
Stuart Levine MD MHA Corporate Medical Director, HealthCare Partners Assistant Clinical Professor, Internal Medicine and Psychiatry, UCLA David
 Stuart Levine MD MHA Corporate Medical Director, HealthCare Partners Assistant Clinical Professor, Internal Medicine and Psychiatry, UCLA David Geffen School of Medicine 1 HealthCare Partners Delivery
Stuart Levine MD MHA Corporate Medical Director, HealthCare Partners Assistant Clinical Professor, Internal Medicine and Psychiatry, UCLA David Geffen School of Medicine 1 HealthCare Partners Delivery
Community Care of North Carolina
 Community Care of North Carolina CCNC Transitional Care Management Jennifer Cockerham, RN, BSN, CDE Director, Chronic Care Programs & Quality Management 1 Chronic Care Population Within the NC Medicaid
Community Care of North Carolina CCNC Transitional Care Management Jennifer Cockerham, RN, BSN, CDE Director, Chronic Care Programs & Quality Management 1 Chronic Care Population Within the NC Medicaid
Health Analytics to Manage Turbulence in Patient Flow: A Field Study of Transitions in Care Processes
 Association for Information Systems AIS Electronic Library (AISeL) SAIS 2016 Proceedings Southern (SAIS) 2016 Health Analytics to Manage Turbulence in Patient Flow: A Field Study of Transitions in Care
Association for Information Systems AIS Electronic Library (AISeL) SAIS 2016 Proceedings Southern (SAIS) 2016 Health Analytics to Manage Turbulence in Patient Flow: A Field Study of Transitions in Care
Building an Accountable Care Organization. Jean Malouin, MD MPH University of Michigan Health System September 21, 2012
 Building an Accountable Care Organization Jean Malouin, MD MPH University of Michigan Health System September 21, 2012 Agenda UMHS overview PGP demo ACO precursor Current efforts underway Role of primary
Building an Accountable Care Organization Jean Malouin, MD MPH University of Michigan Health System September 21, 2012 Agenda UMHS overview PGP demo ACO precursor Current efforts underway Role of primary
Kaiser Permanente of Ohio
 Kaiser Permanente of Ohio Chronic Disease Management Program March 11, 2011 Presenters: Amy Kramer and Audrey L. Callahan 1 Objectives 1. Define the roles and responsibilities of the Care Managers in the
Kaiser Permanente of Ohio Chronic Disease Management Program March 11, 2011 Presenters: Amy Kramer and Audrey L. Callahan 1 Objectives 1. Define the roles and responsibilities of the Care Managers in the
The ROI of Palliative Care. James Mittelberger, MD MPH March 22, 2104
 The ROI of Palliative Care James Mittelberger, MD MPH March 22, 2104 Provide the evidence and tools to develop the most effective palliative care program possible Purpose Palliative Care Financial Return
The ROI of Palliative Care James Mittelberger, MD MPH March 22, 2104 Provide the evidence and tools to develop the most effective palliative care program possible Purpose Palliative Care Financial Return
October 2013 Family Choice: Best Practices in Care for Nursing Home Residents
 SNP Alliance Best Practices October 2013 Family Choice: Best Practices in Care for Nursing Home Residents Overview of Family Choice of New York I-SNP Independent Health s Medicare Advantage Family Choice
SNP Alliance Best Practices October 2013 Family Choice: Best Practices in Care for Nursing Home Residents Overview of Family Choice of New York I-SNP Independent Health s Medicare Advantage Family Choice
Best Practices in Managing Patients With Chronic Obstructive Pulmonary Disease (COPD)
") Best Practices in Managing Patients With Chronic Obstructive Pulmonary Disease (COPD) Geisinger Health System Case Study Profile Geisinger Health System is a physician-led, fully integrated healthcare
Best Practices in Managing Patients With Chronic Obstructive Pulmonary Disease (COPD) Geisinger Health System Case Study Profile Geisinger Health System is a physician-led, fully integrated healthcare
Emerging g Trends in Home Care
 Emerging g Trends in Home Care Dana Sheer, ACNP, MSN Susan Beausoliel, BSN, MS, DNP 1 The Triple Aim Goals Quality Improve Patient Outcomes Goal Readmissions Cost Reduce costs/penalties associated w/ readmissions
Emerging g Trends in Home Care Dana Sheer, ACNP, MSN Susan Beausoliel, BSN, MS, DNP 1 The Triple Aim Goals Quality Improve Patient Outcomes Goal Readmissions Cost Reduce costs/penalties associated w/ readmissions
Modern care management
 The care management challenge Health plans and care providers spend billions of dollars annually on care management with the expectation of better utilization management and cost control. That expectation
The care management challenge Health plans and care providers spend billions of dollars annually on care management with the expectation of better utilization management and cost control. That expectation
ENGAGING PHARMACISTS IN 1305
 ENGAGING PHARMACISTS IN 1305 UTAH EXAMPLES NICOLE BISSONETTE, MPH, MCHES EPICC PROGRAM MANAGER UTAH PROJECTS INVOLVING PHARMACISTS Prior to 1305 Select Health Pharmacist Hypertension Management Team Based
ENGAGING PHARMACISTS IN 1305 UTAH EXAMPLES NICOLE BISSONETTE, MPH, MCHES EPICC PROGRAM MANAGER UTAH PROJECTS INVOLVING PHARMACISTS Prior to 1305 Select Health Pharmacist Hypertension Management Team Based