Dimensional Massage Therapy Techniques for Soft-tissue Conditions of the Elbow and Radioulnar Joints, Hand and Wrist. AMTA National Convention
|
|
|
- Audra Austin
- 7 years ago
- Views:
Transcription
1 Dimensional Massage Therapy Techniques for Soft-tissue Conditions of the Elbow and Radioulnar Joints, Hand and Wrist AMTA National Convention Date: Wednesday September 17, 2014 Place: Denver, CO By Nancy W. Dail, BA, LMT, NCTMB

2 The contents of this handout for Dimensional Massage Therapy Techniques for Softtissue Conditions of the Elbow and Radioulnar Joints, Hand and Wrist are solely for instructional purposes only at the workshop held at the AMTA National Convention in Denver, CO and as such may not be reprinted or copied in any way without prior written permission from the Downeast School of Massage and Nancy Dail. Published 5/24/13 NWD Nancy W. Dail, BA, LMT, NCTMB PO Box 24 Waldoboro, ME cell: Downeast School of Massage 2

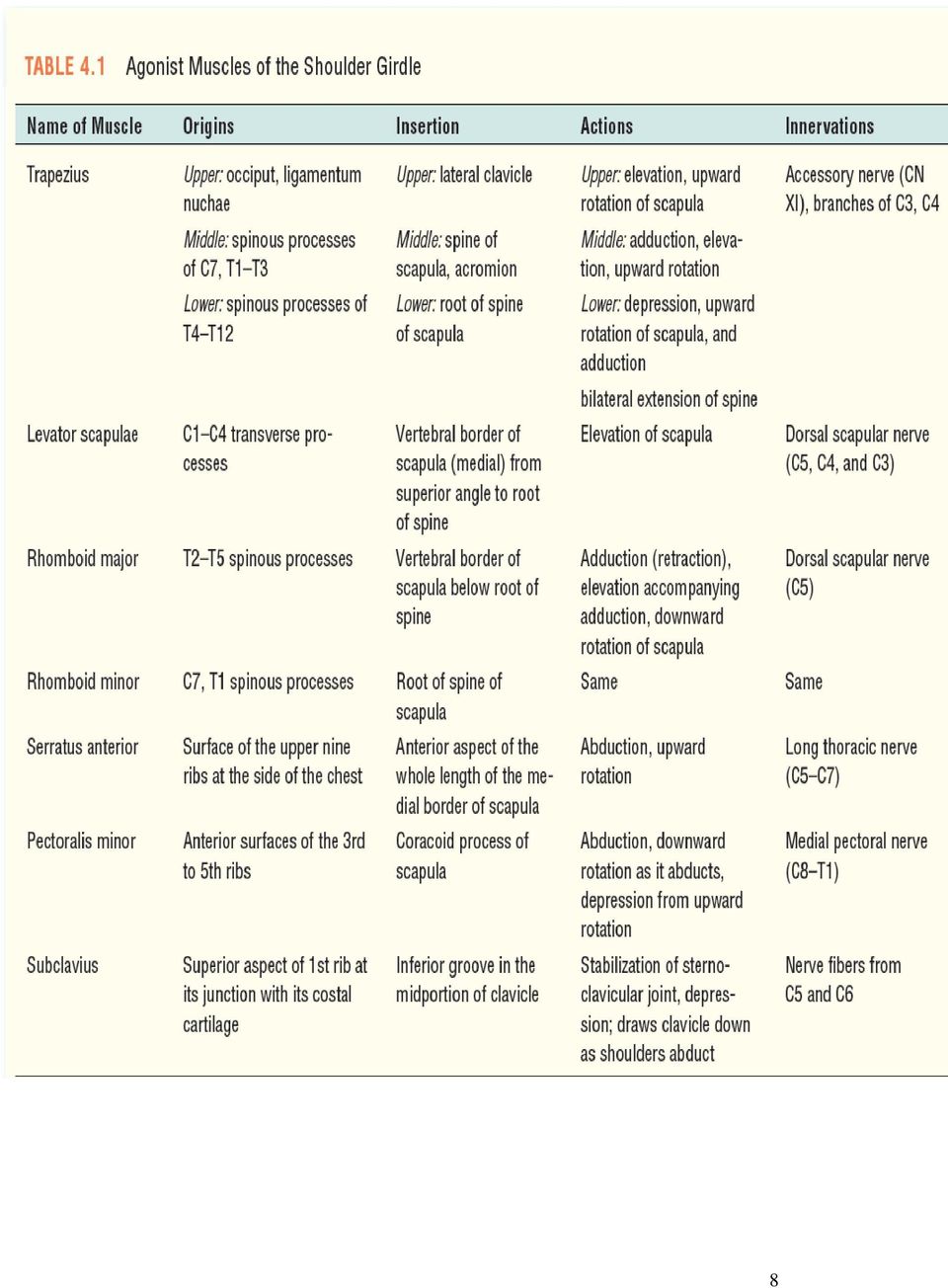
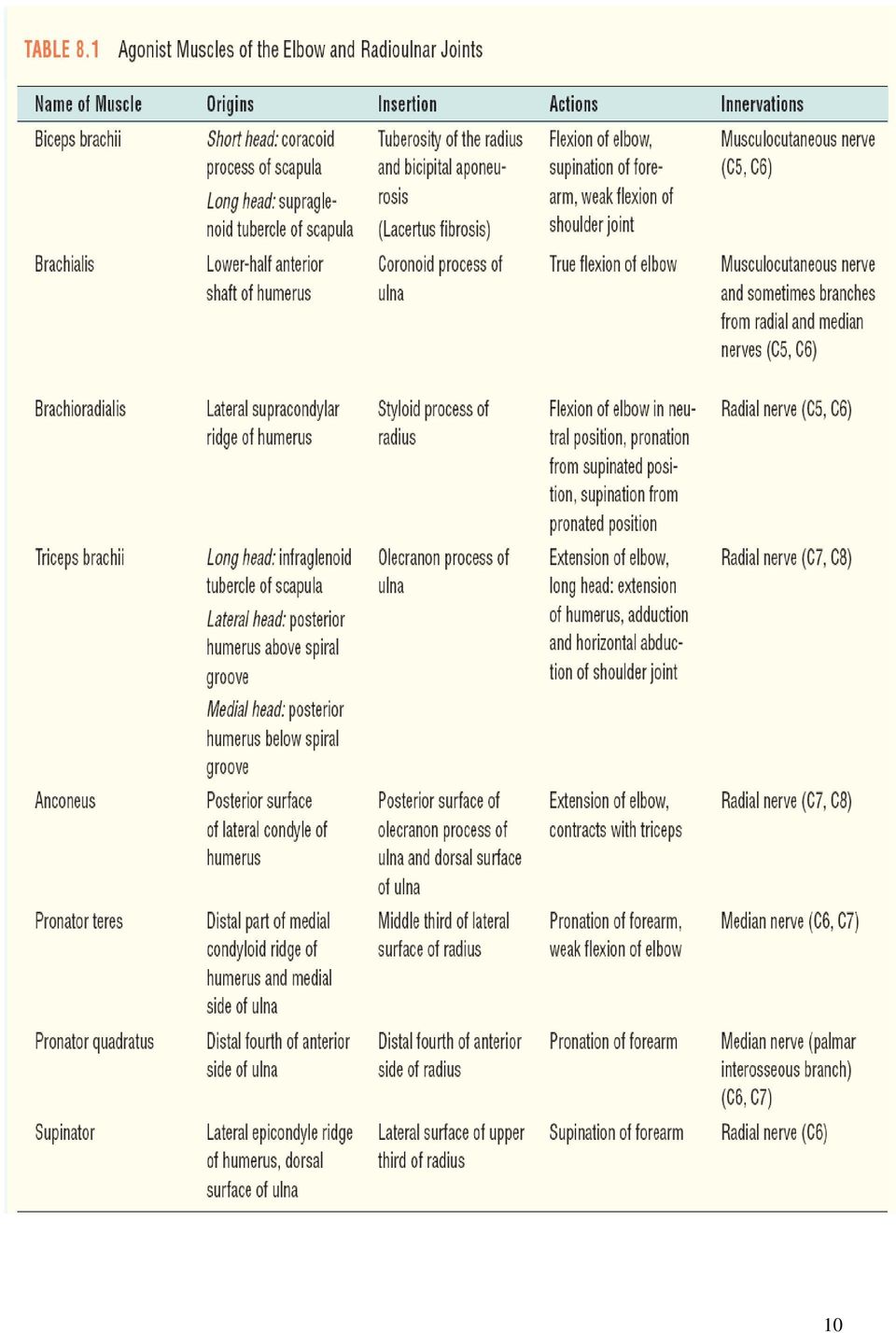
3 Table of Contents Syllabus Pages 4-7 Shoulder Girdle Muscles Page 8 Glenohumeral Joint Muscles Page 9 Radio-ulnar and Elbow Joint Muscles Page 10 Anatomy, Palpation, Exam Procedures Pages Postural Abnormalities Pages Short Upper Arms Page 21 Repetitive Action Injuries Pages Dimensional Massage Therapy Page 24 Neck and Shoulder Techniques Supine Page Supine Chest and Upper Extremity Techniques Pages Forearm Techniques Pages Forearm, Hand, and Wrist Muscles Pages Hand and Wrist Techniques Pages Bibliography Pages

4 Dimensional Massage Therapy Techniques for Soft-tissue Conditions of the Elbow and Radioulnar Joints, Hand and Wrist Including Short Upper Arms, Lateral and Medial Epicondylitis, Tendonitis, Tendonosis, Tenosynovitis, Cubital Tunnel Syndrome, Pronator Teres Syndrome, Double Crush Syndrome, Bicipital Tendonitis, Bursitis, Sprains and Strains, Carpal Tunnel Syndrome, Dupuytren s Contracture, De Quervain s Tenosynovitis, Osteoarthritis, and Ganglion Cysts 8 hours Course Description: The body is all connected. It has depth, width, and length. The joints in the body provide a network of anatomical structures designed for regular use. Repetitive actions cause a constant torque on our guy-wire tendons and muscles that enable our joints to function. How many of your clients have repetitive action conditions of the forearm, hand and wrist? Consider a Dimensional approach to this vast area of concern! In this workshop participants will explore, evaluate and treat a variety of common difficult conditions affecting the forearm region. Nancy will lecture on the skeletal and neurological anatomy of the upper extremity, with particular emphasis on the brachial plexus and its distal destinations. She will also address the specific etiologies, signs, symptoms and massage treatments related to the pathologies of these areas. She will demonstrate hands-on evaluation techniques designed to assess the pathologies discussed. Special attention will be given to discuss the history and exam findings that would warrant health professional referral. Nancy will provide by lecture and power point review of the muscles and soft tissue structures of the arm and forearm. She will discuss trigger points, and referred pain patterns and repetitive actions that affect the arm, forearm, hand and wrist. Nancy will demonstrate techniques used in Dimensional Massage Therapy and provide supervision for hands-on practice by participants. Dimensional Massage Therapy techniques are deep tissue strokes and methods that have been designed to balance joints by working on all the muscles that produce, assist in, or oppose the actions of, or stabilize the joints. They include a wide variety of dual-hand techniques, elliptical movement of soft tissues, active engagement techniques and determining the appropriate sequence for forearm, wrist, or hand conditions. Careful attention will be given to the execution of these techniques, specific muscles and their idiosyncrasies, and to the individual structure of the receiving person on the table. Good body mechanics and safe use of the hands and wrists will be emphasized. Tables and minimal lubrication are required for the hands-on exchange. Nancy W. Dail, BA, LMT, NCTMB has been a professional practicing massage therapist and AMTA member since She is the founder and director of the Downeast School of Massage in Waldoboro, Maine (USA) (1980). A leader in her field, Nancy presents workshops internationally, is certified in Orthopedic and Sports Massage, and has developed the working philosophy of Dimensional Massage Therapy as lead author in Kinesiology for Manual Therapies published by McGraw-Hill. Her BA in Health, Arts, and Science from Goddard College helps her balance her administrative 4

5 duties as Director with teaching Dimensional Massage Therapy, Advanced Skills, Kinesiology, Ethics and related subjects at DSM. Course Objectives: 1. To provide a close examination of the muscular, skeletal and neurological structures of the upper extremity focusing on the elbow and radio-ulnar joint, as well as the forearm, hand, and wrist. 2. To review pathologies and conditions affecting the elbow joint, radio-ulnar joint, hand and wrist. 3. To discuss historical considerations of aspects of disorders that would warrant clinical referral. 4. To take a critical look at how posture and repetitive holding patterns affect the muscles of the upper extremities. 5. To provide a hands-on physical assessment 6. To review trigger points and referred pain patterns of the muscles of the elbow joint and radio-ulnar joints as contributing to lateral epicondylitis and other repetitive action conditions of the hand and wrist. 7. To discuss an appropriate Medical History Questionnaire. 8. To demonstrate Dimensional Massage Therapy Techniques and practice the techniques under supervision. 9. To explore ways to critically think about sequences, muscles, and techniques. 10. To answer questions in relation to the workshop. 11. To provide a Bibliography for additional reading and study. Outline: Date: September 17, hours 8AM-12PM I. Introduction - Overview of the workshop II. Postural Assessment of Elbow, Forearm, Wrist, and Fingers A. Short upper arms and ramifications B. Protracted shoulders C. Head forward posture D. Upper cross syndrome III. Repetitive action injuries of the upper extremities an overview A. Lateral epicondylitis tennis elbow - facts B. Muscles and causes C. Clinical and non-clinical solutions D. The whole body response 5

6 IV. Pathology Etiology, Pathogenesis, S&S, Diagnosis, Contraindications, Treatment A. Common Sprain/Strain C. Tendonitis D. Tenosynovitis E. Tendonosis F. Lateral and Medial Epicondylitis G. Cubital Tunnel Syndrome H. Pronator Teres Syndrome I. Double Crush Syndrome J. Bicipital Tendonitis K. Bursitis V. Muscle Specifics Elbow Joint A. Origin and Insertions B. Trigger points C. Pain patterns D. Postural perspectives VI. Exam Procedures A. History B. Subjective Questionnaires C. Exam (lecture then hands-on) 1. Observation 2. Palpation bony landmarks, nerves 3. Muscle Strength 4. Orthopedic tests for elbow, wrist and hand 5. Neurological VII. Dimensional Massage Therapy The Philosophy: An Art and Science Mix A. Pre and Post Treatment Protocols 1. Medical History subjective include pain scale, objective, assessment, active and passive ROM, plan; SOAP notes for records 2. Palpation 3. Passively shorten muscles/ position shoulders and scapula 4. Work superficial to deep 5. Release hypertonic muscles 6. Use dual hand distraction methods when possible 7. Work individual muscles, their attachments, synergists, stabilizers, and antagonists study the myotactic unit 8. Do not overwork and do trigger point work last on passively shortened muscles B. First Treatment What is the treatment goal? C. Comfort level Ice? D. Environment 6

7 E. Positions VIII. Dimensional Massage Therapy Techniques Treatment Adaptability A. Reduce hypertonicities B. Return tissues to function C. Elongate fibers D. Types of techniques E. Rehabilitation protocol F. Techniques for Upper Extremity IX. Hands On Dimensional Massage Therapy Techniques for the Elbow Joint Lunch 12PM-1:00PM Afternoon Session: 1:00-5:00PM I. Muscle Specifics Hand and Wrist A. Origin and Insertions B. Trigger points C. Pain patterns D. Postural perspectives II. Pathology Etiology, Pathogenesis, S&S, Diagnosis, Contraindications, Treatment A. Carpal Tunnel B. Common Sprain/Strain C. Tendonitis D. Tenosynovitis E. Tendonosis F. Duputren s Contracture M. De Quervain s Tenosynovitis Finklestein s test N. Ganglion Cysts III. Practical Sessions Hand and Wrist Techniques A. Sequence suggestions for forearm and hand and wrist B. Acute, subacute, and chronic when can I work? C. Ice and hydrotherapy questions D. Integration with chiropractic, medical and other professional health therapies IV. Wrap-up, Questions, and Evaluations Notes: 7

8 8
9 9

10 10
11 Treatment Approach differences My perspective Massage therapy treatment is directed towards normalizing soft tissue abnormalities This can be achieved by techniques designed to restore the proper soft tissue length, tone and nutrition. Complimentary Integration Proper joint kinesthetic feedback achieved with proper joint movement helps restore normal soft tissue length, tone and nutrition locally. Normalized soft tissue length, tone and nutrition help restore proper joint motion therefore proper kinesthetic feedback Anatomy Shoulder A. Osteology 1. Scapula a. Acromion Process b. Supraspinous Fossa c. Spine of Scapula d. Infraspinous Fossa e. Coracoid process f. Superior Angle g. Inferior Angle h. Glenoid Cavity i. Infraglenoid, Supraglenoid Tubercles j. Superior, Lateral and Medial Borders k. Subscapular Fossa 2. Humerus a. Head of Humerus b. Greater Tubercle (superior, middle & inferior facets) c. Lesser Tubercle d. Deltoid Tuberosity e. Bicipital Groove f. Medial and Lateral Epicondyles 3. Clavicle a. Sternal end b. Acromial end B. Joints 1. Glenohumeral Joint 2. Acromiolclavicular Joint 11

12 3. Sternoclavicular Joint 4. Scapulothoracic Articulation C. Bones and Joints of Forearm, Hand and Wrist 1. Ulna Elbow joint a. Olecranon Process b. Coronoid Process 2. Radius Radial Ulna Joint a. Radial Tuberosity b. Styloid Process 3. Interosseous Membrane 4. Carpals, Metacarpals, Phalanges 5. Wrist Joint Metacarpal Phalangeal Joints - Condyloid 6. Carpals Gliding 7. Phalanges Hinge (Ginglymus) 8. Thumb Saddle Joint D. Neurology 1. Brachial Plexus 2. Radial 3. Axillary 4. Musculocutaneus 5. Median 6. Ulnar Palpation of Elbow Joint and Radial Ulna Joint Muscles Biceps see above Class Exploration Brachialis Triceps Anconeus Supinator Pronator Teres Brachioradialis Pronator Quadratus Palpation of Forearm Hand and Wrist Muscles Flexors - Class Exploration Palmaris Longus Flexor Carpi Radialis Flexor Carpi Ulnaris Flexor Digitorum Superficialis Flexor Digitorum Profundus Flexor Pollicis Longus 12

13 Extensors Class Exploration Extensor Carpi Ulnaris Extensor Carpi Radialis Brevis Extensor Carpi Radialis Longus Extensor Digitorum Extensor Indicis Extensor Digiti Minimi Extensor Pollicis Longus Extensor Pollicis Brevis Abductor Pollicis Longus Exam Procedures A. History 1. Chief Complaint Onset, Quality (achy, sharp, throbbing, numbness, burning.),severity (VAS, pain Scale), Timing (duration, frequency), What makes worse/better, Associated manifestations 2. Past & Present Medical History 3. Systems Review / Family History 4. History questioning associated with postural exam - They generally do not present to you with postural problems as the major complaint - Was there any Injury if so were there any postures that caused or relieved pain - Currently are there any postures that cause or relieve pain - Family history of postural problems e.g. Scoliosis - Does footwear make a difference? - Has there been a growth spurt (if a child) - Any neurological symptoms - Having a hard time with clothes fitting - Difficulty breathing e.g. scoliosis - What's the dominant hand? B. Observation 1. Determine your dominant eye: Make a circle with the first fingers and thumbs, then overlap the circles and hold arms out in front of the face and observe an object across the room through the circles with both eyes opened. Close one eye if the object is still in the circle that s the dominant eye. (Generally the eye you instinctually look into a camera with) 13

14 * Attempts should be made to allow dominant eye closest to the center of what's being viewed. 2. Adequately undressed for the areas to be observed 3. No shoes worn initially. You can observe changes in posture with shoes on after. 4. Provide time for the patient to adopt there relaxed posture. 5. Look for asymmetry 6. Note any muscle atrophy, soft tissue swelling, boney enlargement, scars, skin changes C. Postural Assessment of the Shoulder 1. Standing Postural Assessment a. Posterior View: Should be done first! Position of Head Straight on shoulders, not tilted or rotated Trapezius neck line Equal on both sides * slope on the dominant side may be greater Shoulder level Level and should not droop or slump forward * slightly lower on the dominant side Scapulae Good alignment, flat against back. Arm positioning and length - Hanging relaxed at their sides. Angle of elbow - Slightly bent so that the forearm is slightly anterior to arm. Palm position - Flat against thighs, hanging at the same distance bilaterally or neutral. b. Lateral View: Ear - In line with the acromion process, the high point of iliac crest, the midline of the lateral knee joint line and just anterior to the lateral malleolus Position of Head - Neither flexed nor extended, Eye should have a level view 14

15 Cervical Curve -Slight reverse C shape Shoulders - Should not droop or slump forward Angle of elbow - Slightly bent so that the forearm is slightly anterior to arm. Palm position -Palms are flat against thighs. c. Anterior View: Helps to provide addition info at the end Position of Head - Straight on shoulders, not tilted or rotated Nose - Tip of the nose is in line with the Sternum and belly button Position of Jaw - Generally lips are close together, teeth are slightly apart Trapezius neck line - Equal on both sides * slope on the dominant side may be greater Shoulders - Level and should not droop or slump forward Clavicles & A-C joints - Should be level and symmetrical Facial symmetry Note changes of facial expression from side to side d. Sitting: Position patient with feet flat on the floor and back is unsupported Observation is the same with standing Note any changes between sitting and standing postures of the head and neck and shoulders e. Forward flexion: Is there asymmetry of the rib cage or spinal musculature? Is there any restriction to movement e.g. tight hamstrings? f. Supine Lying- note head neck and shoulder girdle position g. Prone Lying- note head neck and shoulder girdle position C. Palpation- Note the muscle spasm, tenderness, or abnormal bumps. Take careful note of differences from side to side 15

16 Postural Abnormalities A. Postural Abnormalities 1. Normal posture - Posture is a composite of the positions of all the joints of the body at any given time. - Correct posture is the position in which minimum stress is applied to each joint. 2. Abnormal postures General statements about faulty posture When muscle imbalances occur some muscles become inhibited and weak, while others become tight. Such imbalances lead to tissue changes that may result in inappropriate patterns of movement Vladimir Janda, MD, DSc Muscle imbalance usually precedes recurrent joint dysfunction. Karel Lewit, MD, PhD Muscle imbalances play an important role in the development of musculoskeletal complaints that are presented in clinical practice Faulty posture can cause painful conditions, but it can also exist with out causing complaints. General statements about faulty posture cont What usually makes a faulty posture symptomatic no matter whether it is a severe or minimal fault is the constancy of the fault. An individual who has a major postural fault but maintains mobility to the area is more likely to be asymptomatic. Whereas a person even with a minor fault can experience complaints if mobility is limited. Cumulative effects of constant or repeated small stresses can give rise to the same difficulties a sudden severe stress 3. Examples of Abnormal Posture Upper crossed syndrome 16

17 This syndrome is based on Dr. Vladimir Janda's pioneering work in researching and understanding the predictable pattern of muscular compensation and postural imbalances in the body. He postulated that faulty movement patterns on a poor postural base contribute to habitual overuse in isolated joints, while they minimize normal movement in others, thus creating a self-perpetuating cycle of dysfunction and eventual injury. Upper crossed syndrome leads to: A forward head posture causing strain to the muscular attachments of the shoulder and shoulder blade. An anterior tilt and abduction ( flaring out ) of the shoulder blades occurs, producing a rounded shoulder appearance. Due to the rounded shoulder posture, the mechanical axis of rotation of the glenoid fossa (shoulder socket) becomes altered. The humerus now requires additional stabilization from muscles that typically are quiet: Levator scapulae Upper trapezius Subscapularis Pectoralis minor Supraspinatus muscles Postural overdevelopment of these muscles creates a deltoid shear (crossing of rotator cuff under AC joint), leading to a host of shoulder problems including shoulder impingement, tendonitis and bursitis syndromes. Due to chronic shortening, tightness and weakness in the primary stabilizers of the shoulder (supraspinatus, infraspinatus, teres minor and subscapularis), muscular adhesions and trigger points develop that must be removed before active/passive stretching. 17
 of the shoulder blades occurs, producing a rounded shoulder appearance.")
18 Upper crossed syndrome cont. Pathologies cont Postural examination tends to reveal: A marked anterior head carriage Upper cervical hyperextension Elevated and protracted shoulders (rounded) A hyper-kyphotic thoracic spine Other findings: Cervical ranges of motion restrictions with the report of pulling muscular pain elicited at the end ranges Thoracic ranges of motion restrictions Tender myofascial trigger points were detected in the suboccipital, SCM, levator scapulae, and upper trapezii muscle groups bilaterally Treatment: Ultrasound the infraspinatus or subscapularis, depending on the most painful area of palpation and trigger-point referral pattern. Laser therapy also may be used. Typical dose is 170 Joules per point. Shoulder -blade retraction exercises for building the serratus anterior/posterior, trapezius and rhomboids, and for restoring scapular stabilization strength. Rotator cuff protocol: External rotation (three sets of repetitions). Internal rotation not recommended due to the tendency of the subscapularis to become tight and overdeveloped. Y,T, W, L Exercises on the stability ball to restore and enhance muscular recruitment patterns. Manipulation of the 5th and 6th cervical vertebrae and upper thoracics. At-home treatment consists of rest and TENS to control pain. The tennis ball massage technique on the trapezius and infraspinatus (five to seven times per day) is extremely beneficial for breaking up active/latent trigger points. Self myofascial release with foam rollers on the upper back, lower latissimus dorsi, teres major/minor and infraspinatus will accelerate healing. 18

19 Lower body imbalances affect the overall posture and if left untreated would contribute to/or sustain an upper body postural disorder. Lewit states the most important imbalance in the lumbopelvic region is between weak gluteal muscles with hyperactive hip flexors, and hyperactive lumbar erector spinal with weak abdominal muscles. 19

20 20
21 Short Upper Arms By Nancy Dail Often in a practice we run across individuals with similar problems in a series that can sometimes be blamed on the season or weather. Certainly clients with back issues come to us after shoveling snow or during gardening season. For what ever reason, however, lately, I am seeing several clients with short upper arm structures and resulting issues from their genetic frame. Normally, if you measure the arm or humerus in our upper extremity it expands from the glenoid fossa of the scapula superiorly to the distal end (olecranon process of the ulna) inferiorly to the waist and iliac crest. Individuals with short upper arms have humeral bones that do not measure down to the iliac crest. Usually they have no idea why they have leaned forward their entire lives or why they may not have been able to reach something on a top shelf when someone the same size can. Often these folks will have more trouble with work stations and are likely to develop carpal tunnel-like symptoms. A medical history and a visual observation will reveal clients with short upper arms present with over pronated forearms; very hypertonic pronator teres and resulting numbness and tingling to wrist and fingers. The structure itself lends to abducted scapulae with prominent medial humeral rotation, more so on the dominant upper extremity. Add repetitive actions and non-ergonomic work areas and you have a laundry list of muscles to unravel and release entrapments and a recipe for carpal tunnel syndrome, pronator teres syndrome and possibly double crush syndrome. A Dimensional approach begins the sequence in a supine position with techniques to release hypertonic trapezius, SCM, posterior cervical muscles and pectoralis minor and major muscles. Active engagements techniques help to pin and stretch pectoralis minor and subscapularis. Both muscles are usually very tight on these types of frames. Moving on to the upper arm, release and stretch arm muscles with elliptical movement and dualdistraction moves. Release the elbow joint with movement and techniques. Elliptically move the forearm muscles and release the pronator teres. Sidelying is next with serratus anterior as a star target. Position the client prone lastly to release the soft tissue of the back. Exercises are suggested. There are a wide variety of techniques massage therapy uses on clients with all kinds of structural issues. The above is my approach for short upper arms and clinical issues that often present themselves to this target group. Other considerations could be hip and pelvic positions, gait, and lower extremity factors. One fact remains apparent that the structure we have contributes to a reaction to our repetitive activities. A wise massage therapist will see beyond the repetitive action! 21
22 Repetitive Action Injuries I. Repetitive action injuries of the upper extremities A. 56% of upper extremity cumulative trauma disorders are occupational injuries B. Lateral epicondylitis is one of the most common of these upper extremity overuse problems C. Other disorders include: carpal tunnel syndrome, pronator teres syndrome, double crush syndrome, ulnar nerve compression, medial epicondylitis, radial nerve compression, strains, sprains, slip and fall, tenosynovitis, tendonitis, tendinosis D. Cyriax 4 varieties of tendonitis 1. Teno periosteal partial tear at ligamenous attachment of hand and finger extensor muscle to lateral epicondyle produces painful scar rest and injection. 2. Muscular extensor carpi radialis 3. Tendinous lesion in body of tendon, common extensor tendon at level of head of radius extensor carpi radialis brevis. 4-8 massages 4. Supracondylar tender pt along supracondylar ridge above lateral epicondyle at origin of extensor carpi radialis longus. Deep massage. II. Muscles involved: A. Brachioradialis, Supinator, Extensor Digitorum, Extensor Carpi Radialis Brevis, Extensor Carpi Radialis Longus, Biceps, Triceps, Brachialis B. Causes: 1. Excessive amounts of concentric wrist extension or eccentric wrist flexors 2. Isometric contraction chronic tension mouse 3. Eccentric load on extensors 4. Excessive use of supinators and pronators causing flexors and extensors to hold the hand with isometric positions 5. All could lead to myofascial trigger pts making it a concurrent problem 6. Posture and use of body/sleep positions 7. Slip and fall injury III. Clinical and non-clinical solutions A. Bracing B. Rest from activities C. Ice applications D. Rehabilitative exercises E. Anti-inflammatory meds and injections corticosteroids F. Surical resection G. Arthroscopy H. Laser surgery 22
23 I. Reduce hypertonicity through dimensional approach of the entire upper extremity and cervical region IV. Muscles Repetitive action injury due to action in concentrated area not using the whole body A. Muscles involved in elbow and forearm B. Shoulder girdle and shoulder joint compensatory changes V. Medical History Questionnaire Orthopedic Assessment A. Take a good history B. Questions on pain type and quality C. Observation D. Palpation E. Active, Passive, Manual Resistive ROM 1. Contractile, muscle strain, spasm, tendonitis, tendinosis, tenosynovitis 2. Inert, Scar tissue, impingement, bursa or nerve, ligaments, joint capsule, joint pathology 3. Pain nerve entrapment pins and needles, radiating burning pain or numbness 4. Active ROM contractile or inert causes tension 5. Passive inert structures 6. Manual resistive Lateral epicondylitis test F. Special Tests Orthopedic tests Hoppenfeld, Magee, Lowe G. Soap notes VI. Pre and post treatment protocols match physiology of tissue injury with the physiological effects of treatment A. Treatment plan acute, subacute, chronic B. Therapeutic environment C. Positions sidelying, supine, prone, seated D. Soap notes VII. Dimensional Techniques and Additional techniques Treatment Adaptability A. Reduce hypertonicities passively shorten muscles for efficiency B. Return collagen fibers to optimal function C. Elongate fibers and spread fibers D. Deep transverse friction versus circular friction E. TP work with passive shortening F. Massage with passive movement G. Massage with active engagement H. Broadening with active engagement I. Lengthening with active engagement J. Always end with effleurage VIII. Rehabilitation protocol A. Normalize soft tissue dysfunction B. Improve flexibility C. Restore proper movement patterns D. Strengthening and conditioning 23
24 Technique and Practice: Dimensional Massage in Action Dimensional Massage Therapy A Philosophy The body is all connected: it has depth, width, and length. The joints in the body provide a network of anatomical structures designed for constant use. In order to properly relax and unwind soft tissue, the massage therapist must manipulate as many of these structures as possible. Each joint is a collection of muscles that work in groups and in paired opposition. By systematically working on specific muscles that share contraction and opposite action, Dimensional Massage Therapy helps to create balance to the joint structures. Dimensional Massage Therapy encompasses an approach to technique and structure, as well as to the sequence of the specific techniques for a particular soft tissue problem. The techniques are a collection of soft tissue manipulations that are designed to be efficient and sequentially specific to unwind the most resistant hypertonicities. Dimensional Massage Therapy should provide the least amount of discomfort to the client in the therapeutic process and, if performed correctly, the techniques should be easy on the therapist s hands and body. Many DMT techniques first utilize passive shortening of the length of the muscle to efficiently soften fibers. Other DMT manipulations require rhythmically moving a joint at the same time as unwinding specific muscles, or alternating clockwise and counterclockwise movements to joints or muscles. These distractions provide a mechanism for the client to give up holding patterns and the soft tissue fibers release built-up tension. All techniques should be sequenced according to the individual structure of the client. The therapist needs to build a large tool belt consisting of many techniques to adapt to the wide variety of structures and repetitive actions that plague humanity. Dimensional Massage Therapy provides a philosophical approach, sequence, and methodology of techniques for the massage therapist to utilize in a therapeutic practice. Sequence is always determined by the client s medical history, the structure, and the area of the body needing work. Evaluation of pressure and technique will be determined by the stage of the condition: acute, subacute, or chronic. Never dive into the structure. Use superficial strokes to experiment with your palpation skills, preparing the involved joint or joints for further deep tissue techniques. Unwinding an area involves patience, structural knowledge, and intelligent use of your sequence of techniques. Warm-up techniques include an efficient use of effleurage. Depending on the problem, one would utilize techniques requiring no lubrication first. If possible, remember to place the body part and muscle in a passively shortened position. The following sequence should give the student a solid foundation for a full body massage and prepare for using the philosophy of Dimensional Massage Therapy. 24
25 Neck and Shoulder Techniques Supine Check shoulders for roundness, position, unequal height. Reach under the back and pull the scapula in a superior direction. Palpate for hypertonic muscles. Passively shorten area muscles whenever possible. Relax the muscles under the occipital protuberance if you have not already worked on the client s scalp. Hold the head in your hands and apply your fingers to below the occipital ridge. Push the chin up slightly with the palms of your hands. Engage the muscles below the ridge with circular friction and motion. Palpate the whole ridge area. 1. Edging the Upper Trap Stand at the head of the table behind your client who is a supine position. Bend the client s elbow to passively shorten the upper trap. For the left upper trap, place your right hand under the client s neck and engage the edge of the upper trap on the same side you intend to stretch. Place your left thumb on the client s left upper trap close to the insertion at the clavicle and draw your hands away from each other stretching the trap in opposite directions. Be careful to use slight to no lubrication with this technique. 2. Petrissage Back of Neck while Edging the Upper Trap While in the same position as above, petrissage the back of the neck while edging the upper trap. 3. Repeat 1 and 2 on the Other Side of the Neck 4. Effleurage Around Shoulders and up Neck Start with gingers of both hands pointing toward each other flat underneath the clavicles bilaterally. Stroke with smooth rhythm and complete contact around shoulders and up the sides and back of neck to the occipital ridge and attachment of the upper trap. Hold in a slight traction before repeating the sequence again. 25
26 5. Petrissage Traps Alternately and Together Turn head slightly to the side and support the head with your forearm as you grasp the traps with your hand. Petrissage the traps on the other side with your other hand. Do other side. 6. Alternating Hands Neck Stretch Start at the base of the neck, cupping the cervical spine with one hand, the spine in between the index and thumb and stroke with pressure up to atlas axis area; other hand takes the place of first hand alternating and repeating the stretch-stroke. Keep the head fairly straight and arch the neck as you draw towards C1 and C2. 26
27 7. Hands Under Back - to lower thoracic up spine in any combination of effleurage, vibration or friction or circular friction with pressure. 8. Head Rotation Bilaterally Place the left hand on the left lateral side of the forehead and the opposite hand on the right lateral and posterior occipital protuberance. Gently, passively rotate the head first in one direction and then switch hands to rotate in the opposite direction. 9. Neck Stretch to Side, stroking alternately while stretching with the other hand. First, gently turn the head laterally. Place one hand on the shoulder and one hand on the back of the head. Slide the hand from the shoulder to the head. Take the other hand off the head and place it on the shoulder. Stretch. Slide. Stretch. 27
28 10. Effleurage Shoulders 3 times. 11. Closed Palm Shaping with the dorsal side of hand make a relaxed loose fist, and while the other side of the head is supported with your opposite hand, stroke posterior to SCM superiorly to inferiorly and back. 12. Knuckling with loose fists move your hands in circular motion in the traps bilaterally close to, but not on, the spine and away from the bones of the shoulders. Make sure the upper arms are in a relaxed bent elbow position to un-tense the traps as much as possible. 13. Cervical Work petrissage as close to the vertebrae as possible C-7 to C-1 and back. Your fingers should be in between the body of the vertebrae and the transverse processes. Explore Suboccipitals and attachments to C1 and C2 spinous process and transverse processes. DTF interspinales in between spinous processes. 14. Stripping Bilateral Cervical Muscles Lift the back of the head with one hand and with the other hand straddle the cervical spine as close to the occiput as possible. Crook your index finger on one side and your thumb should be on the other side of the cervical spine. Glide down to C7 as firmly as possible. The neck should arch if you do this technique correctly and the client is relaxed. 28
29 15. Scalenes Lift the back of the head with one hand. Laterally flex the head toward the shoulder that you are working. Place your thumb behind the SCM on that same side and glide toward the first and or second rib as you continue to flex the head forward. Repeat several times. 16. SCM Techniques and Posterior Occipital Ridge Muscles Assess how tight the SCM is bilaterally. Laterally tilt the head toward the shoulder and slightly flex the head forward. On the side closest to the shoulder repeatedly Strip the fibers of the SCM from the mastoid process for a couple of inches toward the origins of the muscle (Fig. 15). DTF the origins of the muscle at the sternum and clavicle. Jostle the length of the muscle and work the muscle fibers between your thumb and index finger. Do a pincer palpation to the trigger points in the muscles. Check in with the client for the appropriate pressure these trigger points can be exquisitely painful, and some might refer to the head. Remember to stretch the muscle after you treat the trigger points. Repeat the routine on the opposite SCM. 29
30 Now that all the superficial layers of muscles have been treated and relaxed, the deeper posterior cervical muscles have to be visited. If the headache has gone, then the routine is over. Working deeply on these muscles might make the headache return with a vengeance, so check in with the client and use caution. Supine Position Chest and Upper Extremity 1. Pectoralis Major Compression Standing next to the client at the side of the table, place your hand closest to the client on the Pectoralis Major. Hold the client s arm at about 90 degrees from his/ her body. Compress the Pec while you pull the arm at the wrist away from the body. Be careful not to compress the anterior deltoid so you do not irritate the subdeltoid bursa. 30
31 2. Pec Major Jostling Place you hand on the pec with your fingers on the ventral side of the muscle and your thumb in the axillary region. Jostle the muscle. 3. Pec Major Elliptical Movement Place all fingers of both hands on the pec major. Place your thumbs in the axillary region. Alternately move the muscle in a clockwise and then counterclockwise movement. 4. DTF and Circular Friction Pec Major Attachments Locate the clavicular head of the Pec Major. DTF and circular friction the attachment. Repeat to the sternal attachments. You may need to work over a towel for a woman. 5. Coracobrachialis Pick up the client s arm at the elbow and hold it over the trunk at a right angle. With your hand that is closest to the body locate the coracoid process. Palpate the coracobrachialis from the coracoid process to the humeral attachment. You will have to palpate through the pec major and anterior deltoid. DTF the muscle and its attachments. It will be tender. Be careful of brachial plexus. 6. Subscapularis Locate the Trigger points and DTF the fibers. Standing next to the supine client, grasp the client s arm above the elbow and bring the arm out to about 90 degrees laterally in an abducted position. Place your inferior fingers under the scapula and your thumb in the axillary region. The client s forearm will rest over your forearm of the hand that is in position to work the subscapularis. Locate the anterior scapula with your thumb. Apply pressure on Trigger points and DTF fibers. Be aware this may be very tender and work with client feedback. (Active Engagement of Subscapularis). 7. Deltoids, Elliptical Motion Do the over-the-head stretch. When you are in position holding the upper extremity over the head, grasp the deltoid on both sides of the 31
32 muscle. Gently but firmly alternately move the muscle in a clockwise and counterclockwise motion. 8. Deltoids Rock and roll the deltoids around the humerus. Petrissage the muscles. 9. Stretch the Deltoids Cradle the arm over the top of the head for one stretch. Draw the arm across the body by grasping the elbow and pulling across from the other side of the table. Move the entire joint. 10. Pec Minor Active Engagement Place your hands one on top of another in the direction of the fibers around the 4 th rib fingers down away from the coracoid process. Ask the client to reach toward the knee on that side of the body and then elevate the shoulder slowly and carefully. Keep pinning the fibers during the elevation of the shoulder and ask for feedback from the client. 11. Active Broadening of Biceps Broaden the biceps as the client flexes the forearm. 12. Active Lengthening of Biceps Lengthen fibers of the biceps as the client extends the forearm. 13. Longitudinal Stripping of Bicep Tendon Locate the bicipital groove. Strip the long head of the bicep tendon lengthwise. Be sure to notice the size and depth of the groove and size of tubercles. Do not do stripping if tendon is vulnerable to sliding out of the groove. 32
33 Forearm Place the forearm in a neutral position. Compression of brachioradialis and forearm muscles. Straddle the brachioradialis and stroke deeply to the elbow. Jostle the brachioradialis. Grasp the muscle and with a slight to insertion. traction vibrate it from origin 33
34 Broaden brachioradialis Elliptical Movement of Forearm Muscles Grip both sides of the forearm, with thumbs on the dorsal side of the forearm and the sides of the index fingers on the supine side of the forearm. In a deep alternating motion, move the muscles of the forearm around the bones. The radius will move on the ulna, with the motion effectively stretching tissue. Myofascial stretch brachioradialis Draw fibers over your thumbs starting close to the elbow joint and work distal. Parallel thumbs brachioradialis Roll one thumb over the other down the length of the muscle proximal to distal. Strip origin of brachioradialis, Strip insertion of brachioradialis 34
35 Petrissage Myofascial humeral twist Petrissage elbow muscles with distraction Range of Motion with Elbow Joint - Cup the olecranon process with one hand and, with the other hand on the client s wrist, passively rotate the forearm, first in one direction and then in another. Go to the complete range of motion of the client. Shake the Upper Extremity Passively Grasp the wrist lightly and gently shake the whole extremity with a bent elbow. Effleurage entire extremity wrist to shoulder joint. 35
36 FLEXORS of the Hand and Wrist Palmaris longus Origin: Medial epicondyle of humerus Insertion: Palmaris aponeurosis of the second, third and fourth and fifth metacarpals Action: Assists in flexion of wrist, weak flexion of elbow joint Innervations: Median nerve Flexor carpi radiali Origin: Medial epicondyle of humerus Insertion: Base of 2nd and 3rd metacarpals palmer surface Action: Flexion of hand, abduction of hand at wrist, weak flexion of elbow Innervations: Median nerve Flexor carpi ulnaris Origin: Medial epicondyle of humerus via common tendon, posterior aspect of proximal ulna Insertion: Base of 5th metacarpal, pisiform (hamate) Action: Flexion and adduction wrist, weak flexion of elbow Innervations: Ulnar nerve Flexor digitorum superficialis (3 heads ) Origin: Medial epicondyle of humerus via common tendon; ulna - medial coronoid process of ulna; radial oblique line of radius Insertion: Sides of shafts of middle phalanges of 4 fingers Action: Flexion of four fingers at pip jt, flexion hand and wrist, weak flexion of elbow. Innervations: Median nerve Flexor digitorum profundus Origin: Proximal 3/4 of the anterior and medial ulna Insertion: Base of the distal phalanges of the four fingers Action: Flexion of 4 fingers at the DIP, PIP and MP joints, flexion of the wrist Innervations: Median nerve to 2 nd and 3 rd fingers, Ulnar nerve to 4 th and 5 th fingers Flexor pollicis longus Origin: Middle anterior radius, anterior medial border of ulnar (just distal to coronoid process), interosseous membrane Insertion: Distal phalanx of thumb Action: Flexion of thumb at IP jt - tip, assists flexion of wrist Innervations: Median nerve, palmar interosseous branch EXTENSORS of the Hand and Wrist Extensor carpi ulnaris Origin: Lateral epicondyle of humerus (common extensor tendon), middle two fourths of posterior border of ulna 36
37 Insertion: Base of 5th metacarpal Actions: Extension of wrist, adduction of wrist, weak extension of forearm Innervations: Radial nerve Extensor carpi radialis brevis Origin: Lateral epicondyle of humerus (common extensor tendon) Insertion: Base of 3 rd metacarpal (dorsal) Action: Extension of wrist, abduction of wrist, weak flexion of elbow Innervations: Radial nerve Extensor carpi radialis longus Origin: Supracondylar ridge and lateral epicondyle of the humerus Insertion: Base of the 2 nd metacarpal (dorsal ) Action: Extension and abduction of wrist, weak flexion of elbow Innervations: Radial nerve Extensor digitorum Origin: Lateral epicondyle of humerus Insertion: Base of middle phalanges of 4 fingers, extensor expansion of 4 fingers (dorsal) Actions: Extension of MP joints of 4 fingers (phalanges of fingers) extension of wrist, extension of elbow Innervations: Radial nerve Extensor indicis Origin: Middle to distal one third of posterior ulna, interosseous membrane Insertion: Head of 2 nd metacarpal and extensor expansion of index finger Actions: Extension of index finger at the metacarpophalangeal jt, weak wrist extension Innervations: Radial nerve Extensor digiti minimi Origin: Lateral epicondyle of humerus Insertion: Proximal phalanx of the 5th phalange (dorsal) Actions: Extension of little finger at the metacarpophalangeal jt, weak wrist extension Innervations: Radial nerve Extensor pollicis longus - anatomical snuffbox Origin: Posterior middle to lower ulna and interosseous membrane Insertion: Base of distal phalanx of thumb (dorsal) Actions: Extension of thumb at IP, MP, and CMP joint, extension of wrist Innervations: Radial nerve Extensor pollicis brevis Origin: Posterior surface of lower middle radius Insertion: Base of proximal phalanx of the thumb dorsal Actions: Extension of thumb, weak wrist extension 37
38 Innervations: Radial nerve Abductor pollicis longus Origin: Posterior aspect of the radius and midshaft of ulna Insertion: Base of the 1 st metacarpal (dorsal) Actions: Abduction of thumb and wrist CMP, abduction of wrist Innervations: Radial nerve Palpation of Forearm Hand and Wrist Muscles Flexors - Class Exploration Palmaris Longus Flexor Carpi Radialis Flexor Carpi Ulnaris Flexor Digitorum Superficialis Flexor Digitorum Profundus Flexor Pollicis Longus Extensors Class Exploration Extensor Carpi Ulnaris Extensor Carpi Radialis Brevis Extensor Carpi Radialis Longus Extensor Digitorum Extensor Indicis Extensor Digiti Minimi Extensor Pollicis Longus Extensor Pollicis Brevis Abductor Pollicis Longus 38
39 Dimensional Massage Therapy Forearm, Hand and Wrist Drape one of the upper extremities. Effleurage Whole Extremity Effleurage entire extremity, starting at the wrist and rounding the shoulder, then gliding back down in a light nerve stroke. Repeat the stroke and increase pressure until you are sinking into the tissues. Hand and Wrist *Note: Can also use alternate routine included here* Lift hand and alternately grasp the palm. Pick the hand up and spread the hand with alternating strokes. Work on all the sections of the hand. Notes: 39
40 Separate the Carpals Place your thumbs on the dorsal side of the hand and the side of your index fingers on the palm side of the client s hand. In an up-and-down motion, move the carpals as if to separate and stretch ligaments. Thumbs on supine palm, spread palm alternately. Knuckles on palm relaxed knuckles in a circular motion in the palm of the hand. Thumb pressure in palm, pushing the palm into the thumb. Elliptical movement of carpals (separate the carpals). Mobilize each finger and thumb with range of motion. Tendon valley slide start at the thumb web adductor pollicis. Place thumb in between the metacarpals dorsally and index finger on the palm side. Press the two together and slide distally out the web. Move onto the next one. Interlace and traction interlace the fingers of your hand with the client s fingers. Hold onto the client s wrist with the other hand. Apply a little traction with the interlaced fingers and slowly slide out of the fingers. Flipping wrist place your thumbs on either side of the wrist at the joint. Put your index fingers on the palm side of the hand. Gently flex the hand at the wrist, using thumbs and fingers alternately. Abduction and adduction of wrist place the medial portion of your palms on the either side of the wrist, your fingers facing towards forearm. Alternately shake the wrist laterally and back. Hand and Wrist Bonus Alternate Routine! Hand Sandwich Hold the hand of the client by placing the client s hand in between both of your hands. Place the palm of your hand to the palm of the client s hand. Rest your other hand on the dorsal side of the client s hand. The fingers of both of your hands should be pointing toward the client s wrist. Take a deep breath and relax in this position. The client s hand should be just resting in your hand. Dorsal Hand Strokes 40
41 Hold the client s hand palm down. Wrap your hands around the client s hand so that your fingers support the palm and your thumbs rest parallel to the arm, pointing towards the elbow, on the dorsal side of the client s hand. Using the pad of your thumbs, make strokes that are overlapping half circles over the dorsal side of the hand. Maintaining position, gently raise and lower the client s hand at the wrist. Petrissage Hand Holding the hand in the same position, alternately petrissage both sides of the hand while moving the wrist in abduction and adduction. Hand Squeeze Continue to hold the hand in the same way. Rest the thumbs fully on the back of the client s hand. Using light pressure, squeeze the client s hand very gently while moving thumbs to respective sides. Work entire surface. Finger Strokes Use one hand to support the client s hand in a way that is comfortable for both. Use the other hand to massage fingers. Starting at the base of the finger, with your thumb on one side and your index finger on the other, do one or a combination of the following: Walk the thumb and index finger up the client s finger by quickly alternating movement toward fingertip. With a gentle squeeze, perform thumb circles on top of the finger from base to tip. Squeeze client s finger between thumb and fingers. Release. Move distal a little, repeat. Continue to fingertip. Repeat strokes 2-4 times per finger. Finally, squeeze fingers gently but firmly while stroking up the finger in one even motion. Slide off the fingertip. Complete sequence on one finger. Move to the next finger smoothly and repeat entire sequence. It is all right to switch hands to do the thumb with the opposite hand, if it is easier for you. Tendon Valley Slide Stroke proximally to distally on either side of the metacarpals, then out web of each finger and thumb, using thumb dorsally and index finger supine. Range of Motion Fingers With one hand, support the client s hand at the base of the fingers. Use the other hand to grasp one finger (start with the thumb or little finger). Holding the finger straight, rotate it several times in each direction. Then bend it down and up from the joint closest to the hand. Next, with the supporting hand hold the base of the finger still and move it up and down from the middle knuckle. Repeat with the distal phalanx. Continue until all fingers have been done. Include the thumb. Draw it across the palm and back as an additional motion. Stretch Carpals and Metacarpals Joints 41
42 Grasp the hand as you did in the dorsal hand strokes, just above the wrist. Your thumbs should be on top of the carpals and your fingers on the palm of the hand underneath. In an up-and-down motion, move the carpals as if to gently separate and stretch ligaments. Move up to the metacarpals and repeat across the hand. Rotate and Stretch Wrist Grasp the wrist with one hand. Interlace the fingers of the client s hand with the fingers of your hand. Rotate the wrist and, with a little traction at the wrist, pull gently to free your fingers from the client s. Flipping Hand Place your thumbs on either side of the wrist at the joint. Put your index fingers on the palm side of the hand. Gently flex the hand at the wrist, using thumbs and fingers alternately. Shake Wrist: Abduction, adduction. Place the medial portion of your palms on the either side of the wrist, your fingers facing towards forearm. Alternately shake the wrist laterally and back. Neutral Position Turn the client s forearm so that it rests in a neutral position. The ulnar side of the hand will be on the pillow and the thumb side should be up. Hold the client s hand by the ulnar side. With your opposite hand, interlock your thumb and forefinger with the client s thumb and forefinger. Do a circular kneading motion with your interlocking hand. Pressure to the Adductor Pollicis In the same position as above, apply a small amount of pressure with your thumb and forefinger to the fleshy pad between the client s thumb and forefinger. Palm Strokes Turn the client s hand over and place your thumbs in the client s palm. Your fingers of both hands will be holding the dorsal side of the client s hand. Make circles with your thumbs across the palm. Apply gentle pressure with your thumbs into the palmar tissue. Relaxed Fist Circles Support the client s hand with one hand. Place relaxed, loose fist in the client s palm and, using your mid knuckles and flat part between them, make circle around the palm. Stretch Palm Interlock your little finger and next finger of one hand with the little finger and next finger of the client s. With your other hand, interlock your little finger and next finger with the client s thumb. Stretch the palm with your thumbs. Place hand on table and prepare to move on to forearm techniques. 42
THE SHOULDER JOINT T H E G L E N O H U M E R A L ( G H ) J O I N T
 J O I N T") THE SHOULDER JOINT T H E G L E N O H U M E R A L ( G H ) J O I N T CLARIFICATION OF TERMS Shoulder girdle = scapula and clavicle Shoulder joint (glenohumeral joint) = scapula and humerus Lippert, p115
THE SHOULDER JOINT T H E G L E N O H U M E R A L ( G H ) J O I N T CLARIFICATION OF TERMS Shoulder girdle = scapula and clavicle Shoulder joint (glenohumeral joint) = scapula and humerus Lippert, p115
International Standards for the Classification of Spinal Cord Injury Motor Exam Guide
 C5 Elbow Flexors Biceps Brachii, Brachialis Patient Position: The shoulder is in neutral rotation, neutral flexion/extension, and adducted. The elbow is fully extended, with the forearm in full supination.
C5 Elbow Flexors Biceps Brachii, Brachialis Patient Position: The shoulder is in neutral rotation, neutral flexion/extension, and adducted. The elbow is fully extended, with the forearm in full supination.
Elbow & Forearm H O W V I T A L I S T H E E L B O W T O O U R D A I L Y L I V E S?
 Elbow & Forearm H O W V I T A L I S T H E E L B O W T O O U R D A I L Y L I V E S? Clarification of Terms The elbow includes: 3 bones (humerus, radius, and ulna) 2 joints (humeroulnar and humeroradial)
Elbow & Forearm H O W V I T A L I S T H E E L B O W T O O U R D A I L Y L I V E S? Clarification of Terms The elbow includes: 3 bones (humerus, radius, and ulna) 2 joints (humeroulnar and humeroradial)
Ken Ross BSc ST, Nat Dip ST
 Ken Ross BSc ST, Nat Dip ST Trunk Most people will suffer from back pain at some point in their lives. Good spinal posture places minimal strain on the muscles which maintain the natural curve of the spine
Ken Ross BSc ST, Nat Dip ST Trunk Most people will suffer from back pain at some point in their lives. Good spinal posture places minimal strain on the muscles which maintain the natural curve of the spine
Chapter 7 The Wrist and Hand Joints
 Chapter 7 The Wrist and Hand Manual of Structural Kinesiology R.T. Floyd, EdD, ATC, CSCS Many Archery, Relate wrist require sports require precise functioning of flexion, & hand & hand functional combined
Chapter 7 The Wrist and Hand Manual of Structural Kinesiology R.T. Floyd, EdD, ATC, CSCS Many Archery, Relate wrist require sports require precise functioning of flexion, & hand & hand functional combined
Chapter 5. The Shoulder Joint. The Shoulder Joint. Bones. Bones. Bones
 Copyright The McGraw-Hill Companies, Inc. Reprinted by permission. Chapter 5 The Shoulder Joint Structural Kinesiology R.T. Floyd, Ed.D, ATC, CSCS Structural Kinesiology The Shoulder Joint 5-1 The Shoulder
Copyright The McGraw-Hill Companies, Inc. Reprinted by permission. Chapter 5 The Shoulder Joint Structural Kinesiology R.T. Floyd, Ed.D, ATC, CSCS Structural Kinesiology The Shoulder Joint 5-1 The Shoulder
Muscles of Mastication
 Muscles of Mastication Masseter Zygomatic Arch Mandibular angle Elevates mandible Mandibular ramus Temporalis Temporal fossa of the temporal bone Coronoid process of the mandible Elevates mandible Retracts
Muscles of Mastication Masseter Zygomatic Arch Mandibular angle Elevates mandible Mandibular ramus Temporalis Temporal fossa of the temporal bone Coronoid process of the mandible Elevates mandible Retracts
Skin of eyebrows galea aponeurotica. Muscle and skin of mouth
 : SEE ALSO THE AP SITE FOR OTHER TABLES GROSS ANATOMY OF THE MUSCULAR SYSTEMM Muscles of the Head and Neck: Occipitofrontalis Frontalis Occipitalis Orbicularis oculi Orbicularis oris Buccinator Masseter
: SEE ALSO THE AP SITE FOR OTHER TABLES GROSS ANATOMY OF THE MUSCULAR SYSTEMM Muscles of the Head and Neck: Occipitofrontalis Frontalis Occipitalis Orbicularis oculi Orbicularis oris Buccinator Masseter
Muscles of the Forearm and Hand
 8 Muscles of the Forearm and Hand 132 PRONATOR TERES Strengthening exercises Pronation with strength bar Self stretches Weight of stick increases supination via gravity PRONATOR TERES 133 Latin, pronate,
8 Muscles of the Forearm and Hand 132 PRONATOR TERES Strengthening exercises Pronation with strength bar Self stretches Weight of stick increases supination via gravity PRONATOR TERES 133 Latin, pronate,
Rotator Cuff Pathophysiology. treatment program that will effectively treat it. The tricky part about the shoulder is that it is a ball and
 Rotator Cuff Pathophysiology Shoulder injuries occur to most people at least once in their life. This highly mobile and versatile joint is one of the most common reasons people visit their health care
Rotator Cuff Pathophysiology Shoulder injuries occur to most people at least once in their life. This highly mobile and versatile joint is one of the most common reasons people visit their health care
Upper Limb QUESTIONS UPPER LIMB: QUESTIONS
 1 Upper Limb QUESTIONS 1.1 Which of the following statements best describes the scapula? a. It usually overlies the 2nd to 9th ribs. b. The spine continues laterally as the coracoid process. c. The suprascapular
1 Upper Limb QUESTIONS 1.1 Which of the following statements best describes the scapula? a. It usually overlies the 2nd to 9th ribs. b. The spine continues laterally as the coracoid process. c. The suprascapular
Clarification of Terms
 Shoulder Girdle Clarification of Terms Shoulder girdle = scapula and clavicle Shoulder joint (glenohumeral joint) = scapula and humerus What is the purpose (or function) of the shoulder and entire upper
Shoulder Girdle Clarification of Terms Shoulder girdle = scapula and clavicle Shoulder joint (glenohumeral joint) = scapula and humerus What is the purpose (or function) of the shoulder and entire upper
Muscle Movements, Types, and Names
 Muscle Movements, Types, and Names A. Gross Skeletal Muscle Activity 1. With a few exceptions, all muscles cross at least one joint 2. Typically, the bulk of the muscle lies proximal to the joint it crossed
Muscle Movements, Types, and Names A. Gross Skeletal Muscle Activity 1. With a few exceptions, all muscles cross at least one joint 2. Typically, the bulk of the muscle lies proximal to the joint it crossed
Muscles of the Neck and Vertebral Column Sternocleidomastoid (anterior neck) Origin Insertion Action
 Origin Insertion Action") Muscular movements of the head (at the cervical spine/neck) and of the torso (thoracic and lumbar spine/upper, middle, and lower back): flexion, extension, lateral flexion, rotation. Muscles of the Neck
Muscular movements of the head (at the cervical spine/neck) and of the torso (thoracic and lumbar spine/upper, middle, and lower back): flexion, extension, lateral flexion, rotation. Muscles of the Neck
Injuries to Upper Limb
 Injuries to Upper Limb 1 The following is a list of common sporting conditions and injuries. The severity of each condition may lead to different treatment protocols and certainly varying levels of intervention.
Injuries to Upper Limb 1 The following is a list of common sporting conditions and injuries. The severity of each condition may lead to different treatment protocols and certainly varying levels of intervention.
Massage and Movement
 Massage and Movement Incorporating Movement into Massage Part One: Theory and Technique in Prone With Lee Stang, LMT NCBTMB #450217-06 1850 West Street Southington, CT 06489 860.747.6388 www.bridgestohealthseminars.com
Massage and Movement Incorporating Movement into Massage Part One: Theory and Technique in Prone With Lee Stang, LMT NCBTMB #450217-06 1850 West Street Southington, CT 06489 860.747.6388 www.bridgestohealthseminars.com
The Muscular System. Appendicular Musculature
 11 The Muscular System Appendicular Musculature CHAPTER OBJECTIVES 1. Describe the functions of the appendicular musculature. 2. Identify and locate the principal appendicular muscles of the body, together
11 The Muscular System Appendicular Musculature CHAPTER OBJECTIVES 1. Describe the functions of the appendicular musculature. 2. Identify and locate the principal appendicular muscles of the body, together
Elbow, Forearm, Wrist, & Hand. Bony Anatomy. Objectives. Bones. Bones. Bones
 Objectives Elbow, Forearm, Wrist, & Hand Chapter 19 Identify and discuss the functional anatomy of the elbow and forearm Discuss the common injuries associated with these anatomical structures Bones Humerus
Objectives Elbow, Forearm, Wrist, & Hand Chapter 19 Identify and discuss the functional anatomy of the elbow and forearm Discuss the common injuries associated with these anatomical structures Bones Humerus
Stretching in the Office
 Stretching in the Office Legs: Quads, Hamstrings, IT band, Hip flexors, Gluts, Calves Quads: Standing @ desk maintaining upright posture, grab one leg @ a time by foot or ankle and bring it towards backside
Stretching in the Office Legs: Quads, Hamstrings, IT band, Hip flexors, Gluts, Calves Quads: Standing @ desk maintaining upright posture, grab one leg @ a time by foot or ankle and bring it towards backside
The Pilates Studio of Los Angeles / PilatesCertificationOnline.com
 Anatomy Review Part I Anatomical Terminology and Review Questions (through pg. 80) Define the following: 1. Sagittal Plane 2. Frontal or Coronal Plane 3. Horizontal Plane 4. Superior 5. Inferior 6. Anterior
Anatomy Review Part I Anatomical Terminology and Review Questions (through pg. 80) Define the following: 1. Sagittal Plane 2. Frontal or Coronal Plane 3. Horizontal Plane 4. Superior 5. Inferior 6. Anterior
10/15/2012. The Hand. Clarification of Terms. Osteology of the Hand (Bones) http://www.youtube.com/watch?v=idxuwerttj A&feature=related
 http://www.youtube.com/watch?v=idxuwerttj A&feature=related") The Hand http://www.youtube.com/watch?v=idxuwerttj A&feature=related Clarification of Terms The hand is made up of the thumb, metacarpals, and phalanges The digits are numbered (with the thumb being #1
The Hand http://www.youtube.com/watch?v=idxuwerttj A&feature=related Clarification of Terms The hand is made up of the thumb, metacarpals, and phalanges The digits are numbered (with the thumb being #1
EXTENSOR POLLICIS TENDONITIS SYNDROME
 EXTENSOR POLLICIS TENDONITIS SYNDROME The extensor pollicis longus muscle has its origin on the lateral part of the middle third of the ulnar shaft on the dorsal border below the abductor pollicis longus
EXTENSOR POLLICIS TENDONITIS SYNDROME The extensor pollicis longus muscle has its origin on the lateral part of the middle third of the ulnar shaft on the dorsal border below the abductor pollicis longus
The wrist and hand are constructed of a series of complex, delicately balanced joints whose function is essential to almost every act of daily living.
 TOPIC OUTLINE 9- THE WRIST AND HAND. Introduction. The wrist and hand are constructed of a series of complex, delicately balanced joints whose function is essential to almost every act of daily living.
TOPIC OUTLINE 9- THE WRIST AND HAND. Introduction. The wrist and hand are constructed of a series of complex, delicately balanced joints whose function is essential to almost every act of daily living.
Lumbar/Core Strength and Stability Exercises
 Athletic Medicine Lumbar/Core Strength and Stability Exercises Introduction Low back pain can be the result of many different things. Pain can be triggered by some combination of overuse, muscle strain,
Athletic Medicine Lumbar/Core Strength and Stability Exercises Introduction Low back pain can be the result of many different things. Pain can be triggered by some combination of overuse, muscle strain,
Muscle Energy Technique. Applied to the Shoulder
 Muscle Energy Technique Applied to the Shoulder MUSCLE ENERGY Theory Muscle energy technique is a manual therapy procedure which involves the voluntary contraction of a muscle in a precisely controlled
Muscle Energy Technique Applied to the Shoulder MUSCLE ENERGY Theory Muscle energy technique is a manual therapy procedure which involves the voluntary contraction of a muscle in a precisely controlled
COMPUTER-RELATED MUSCLE, TENDON, AND JOINT INJURIES
 CHAPTER ELEVEN COMPUTER-RELATED MUSCLE, TENDON, AND JOINT INJURIES To reduce the risk of pain in your neck and shoulders, stay within these recommended ranges of movement: Neck Flexion: 0 o -15 o (bending
CHAPTER ELEVEN COMPUTER-RELATED MUSCLE, TENDON, AND JOINT INJURIES To reduce the risk of pain in your neck and shoulders, stay within these recommended ranges of movement: Neck Flexion: 0 o -15 o (bending
Rotator Cuff and Shoulder Conditioning Program. Purpose of Program
 Prepared for: Prepared by: OrthoInfo Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle.
Prepared for: Prepared by: OrthoInfo Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle.
SPINE. Postural Malalignments 4/9/2015. Cervical Spine Evaluation. Thoracic Spine Evaluation. Observations. Assess position of head and neck
 SPINE Observations Body type Postural alignments and asymmetries should be observed from all views Assess height differences between anatomical landmarks Figure 25-9 Figure 25-10 Figure 25-11 & 12 Postural
SPINE Observations Body type Postural alignments and asymmetries should be observed from all views Assess height differences between anatomical landmarks Figure 25-9 Figure 25-10 Figure 25-11 & 12 Postural
DSM Spine+Sport - Mobility
 To set yourself up for success, practice keeping a neutral spine throughout all of these movements. This will ensure the tissue mobilization is being applied to the correct area, and make the techniques
To set yourself up for success, practice keeping a neutral spine throughout all of these movements. This will ensure the tissue mobilization is being applied to the correct area, and make the techniques
Range of Motion. A guide for you after spinal cord injury. Spinal Cord Injury Rehabilitation Program
 Range of Motion A guide for you after spinal cord injury Spinal Cord Injury Rehabilitation Program This booklet has been written by the health care providers who provide care to people who have a spinal
Range of Motion A guide for you after spinal cord injury Spinal Cord Injury Rehabilitation Program This booklet has been written by the health care providers who provide care to people who have a spinal
Orthopaedic and Spine Institute 21 Spurs Lane, Suite 245, San Antonio, TX 78240 www.saspine.com Tel# 210-487-7463
 Phase I Passive Range of Motion Phase (postop week 1-2) Minimize shoulder pain and inflammatory response Achieve gradual restoration of gentle active range of motion Enhance/ensure adequate scapular function
Phase I Passive Range of Motion Phase (postop week 1-2) Minimize shoulder pain and inflammatory response Achieve gradual restoration of gentle active range of motion Enhance/ensure adequate scapular function
Flexibility Assessment and Improvement Compiled and Adapted by Josh Thompson
 Flexibility Assessment and Improvement Compiled and Adapted by Josh Thompson Muscles must have a full and normal range of motion in order for joints and skeletal structure to function properly. Flexibility
Flexibility Assessment and Improvement Compiled and Adapted by Josh Thompson Muscles must have a full and normal range of motion in order for joints and skeletal structure to function properly. Flexibility
A Patient s Guide to Shoulder Pain
 A Patient s Guide to Shoulder Pain Part 2 Evaluating the Patient James T. Mazzara, M.D. Shoulder and Elbow Surgery Sports Medicine Occupational Orthopedics Patient Education Disclaimer This presentation
A Patient s Guide to Shoulder Pain Part 2 Evaluating the Patient James T. Mazzara, M.D. Shoulder and Elbow Surgery Sports Medicine Occupational Orthopedics Patient Education Disclaimer This presentation
Biceps Tenodesis Protocol
 Department of Rehabilitation Services Physical Therapy The intent of this protocol is to provide the clinician with a guideline of the postoperative rehabilitation course of a patient that has undergone
Department of Rehabilitation Services Physical Therapy The intent of this protocol is to provide the clinician with a guideline of the postoperative rehabilitation course of a patient that has undergone
X-Plain Neck Exercises Reference Summary
 X-Plain Neck Exercises Reference Summary Introduction Exercising your neck can make it stronger, more flexible and reduce neck pain that is caused by stress and fatigue. This reference summary describes
X-Plain Neck Exercises Reference Summary Introduction Exercising your neck can make it stronger, more flexible and reduce neck pain that is caused by stress and fatigue. This reference summary describes
Hand and Upper Extremity Injuries in Outdoor Activities. John A. Schneider, M.D.
 Hand and Upper Extremity Injuries in Outdoor Activities John A. Schneider, M.D. Biographical Sketch Dr. Schneider is an orthopedic surgeon that specializes in the treatment of hand and upper extremity
Hand and Upper Extremity Injuries in Outdoor Activities John A. Schneider, M.D. Biographical Sketch Dr. Schneider is an orthopedic surgeon that specializes in the treatment of hand and upper extremity
Hemiplegic shoulder pain/shoulder subluxation
 UPPER LIMB NEUROMUSCULAR ELECTRICAL STIMULATION: Electrode positions Please note that the polarity (red and black leads) can be altered according to your clinical reasoning. The area in which you want
UPPER LIMB NEUROMUSCULAR ELECTRICAL STIMULATION: Electrode positions Please note that the polarity (red and black leads) can be altered according to your clinical reasoning. The area in which you want
Shoulder Tendonitis. Brett Sanders, MD Center For Sports Medicine and Orthopaedic 2415 McCallie Ave. Chattanooga, TN (423) 624-2696
 624-2696") Shoulder Tendonitis Brett Sanders, MD Center For Sports Medicine and Orthopaedic 2415 McCallie Ave. Chattanooga, TN (423) 624-2696 Shoulder tendinitis is a common overuse injury in sports (such as swimming,
Shoulder Tendonitis Brett Sanders, MD Center For Sports Medicine and Orthopaedic 2415 McCallie Ave. Chattanooga, TN (423) 624-2696 Shoulder tendinitis is a common overuse injury in sports (such as swimming,
Anatomy and Physiology 121: Muscles of the Human Body
 Epicranius Anatomy and Physiology 121: Muscles of the Human Body Covers upper cranium Raises eyebrows, surprise, headaches Parts Frontalis Occipitalis Epicranial aponeurosis Orbicularis oculi Ring (sphincter)
Epicranius Anatomy and Physiology 121: Muscles of the Human Body Covers upper cranium Raises eyebrows, surprise, headaches Parts Frontalis Occipitalis Epicranial aponeurosis Orbicularis oculi Ring (sphincter)
Psoas Syndrome. The pain is worse from continued standing and from twisting at the waist without moving the feet.
 Psoas Syndrome The iliopsoas muscle is a major body mover but seldom considered as a source of pain. Chronic lower back pain involving the hips, legs, or thoracic regions can often be traced to an iliopsoas
Psoas Syndrome The iliopsoas muscle is a major body mover but seldom considered as a source of pain. Chronic lower back pain involving the hips, legs, or thoracic regions can often be traced to an iliopsoas
McMaster Spikeyball Therapy Drills
 BODY BLOCKS In sequencing Breathing and Tempo Flexibility / Mobility and Proprioception (feel) Upper body segment Middle body segment Lower body segment Extension / Static Posture Office / Computer Travel
BODY BLOCKS In sequencing Breathing and Tempo Flexibility / Mobility and Proprioception (feel) Upper body segment Middle body segment Lower body segment Extension / Static Posture Office / Computer Travel
Ergonomics Monitor Training Manual
 Table of contents I. Introduction Ergonomics Monitor Training Manual II. Definition of Common Injuries Common Hand & Wrist Injuries Common Neck & Back Injuries Common Shoulder & Elbow Injuries III. Ergonomics
Table of contents I. Introduction Ergonomics Monitor Training Manual II. Definition of Common Injuries Common Hand & Wrist Injuries Common Neck & Back Injuries Common Shoulder & Elbow Injuries III. Ergonomics
Buccinator Presses cheek against molar teeth Facial (CNVII) wrinkles forehead
 wrinkles forehead") Muscles to Identify on the Cadaver and/or Models You are required to identify each of the following muscles or associated structures on the cadavers and/or models in lab. If the box is shaded in a particular
Muscles to Identify on the Cadaver and/or Models You are required to identify each of the following muscles or associated structures on the cadavers and/or models in lab. If the box is shaded in a particular
Integrated Manual Therapy & Orthopedic Massage For Low Back Pain, Hip Pain, and Sciatica
 Integrated Manual Therapy & Orthopedic Massage For Low Back Pain, Hip Pain, and Sciatica Assessment Protocols Treatment Protocols Treatment Protocols Corrective Exercises By Author & International Lecturer
Integrated Manual Therapy & Orthopedic Massage For Low Back Pain, Hip Pain, and Sciatica Assessment Protocols Treatment Protocols Treatment Protocols Corrective Exercises By Author & International Lecturer
For Deep Pressure Massage
 T H E R A C A N E O W N E R S M A N U A L For Deep Pressure Massage Thera Cane is a self massager used to apply pressure to sore muscles. The unique design of the Thera Cane lets you apply deep pressure
T H E R A C A N E O W N E R S M A N U A L For Deep Pressure Massage Thera Cane is a self massager used to apply pressure to sore muscles. The unique design of the Thera Cane lets you apply deep pressure
by joe muscolino body mechanics
 by joe muscolino body mechanics carpal tunnel syndrome The word carpal means wrist. Therefore, the carpal tunnel is a tunnel that is formed by the structural configuration of the wrist (carpal) bones.
by joe muscolino body mechanics carpal tunnel syndrome The word carpal means wrist. Therefore, the carpal tunnel is a tunnel that is formed by the structural configuration of the wrist (carpal) bones.
Examination of the Elbow. Elbow Examination. Structures to Examine. Active Range of Motion. Active Range of Motion 8/22/2012
 Examination of the Elbow The elbow is a complex modified hinge joint The humero-ulnar joint is a hinge joint allowing flexion and extension The radio-ulnar joint allows for pronation and supination of
Examination of the Elbow The elbow is a complex modified hinge joint The humero-ulnar joint is a hinge joint allowing flexion and extension The radio-ulnar joint allows for pronation and supination of
Muscle Name Origin Insertion Action Innervation Muscles of Upper Extremity Pectoralis Major Medial half of clavicle, front of sternum, costal
 Muscle Name Origin Insertion Action Innervation Muscles of Upper Extremity Pectoralis Major Medial half of clavicle, front of sternum, costal Crest of greater tubercle (Lateral lip of bicipital groove)
Muscle Name Origin Insertion Action Innervation Muscles of Upper Extremity Pectoralis Major Medial half of clavicle, front of sternum, costal Crest of greater tubercle (Lateral lip of bicipital groove)
SAMPLE WORKOUT Full Body
 SAMPLE WORKOUT Full Body Perform each exercise: 30 secs each x 2 rounds or 2-3 sets of 8-12 reps Monday & Wednesday or Tuesday & Thursday Standing Squat Muscles: glutes (butt), quadriceps (thigh) Stand
SAMPLE WORKOUT Full Body Perform each exercise: 30 secs each x 2 rounds or 2-3 sets of 8-12 reps Monday & Wednesday or Tuesday & Thursday Standing Squat Muscles: glutes (butt), quadriceps (thigh) Stand
SELF-MASSAGE HANDOUTS
 SELF-MASSAGE HANDOUTS Self-Massage for the Head and Face Self-Massage for the Low Back and Buttocks Self-Massage for Runners Self-Massage for the Neck Self-Massage for the Feet Self-Massage for the Arms
SELF-MASSAGE HANDOUTS Self-Massage for the Head and Face Self-Massage for the Low Back and Buttocks Self-Massage for Runners Self-Massage for the Neck Self-Massage for the Feet Self-Massage for the Arms
Muscular System. Student Learning Objectives: Identify the major muscles of the body Identify the action of major muscles of the body
 Muscular System Student Learning Objectives: Identify the major muscles of the body Identify the action of major muscles of the body Structures to be identified: Muscle actions: Extension Flexion Abduction
Muscular System Student Learning Objectives: Identify the major muscles of the body Identify the action of major muscles of the body Structures to be identified: Muscle actions: Extension Flexion Abduction
COMMON OVERUSE INJURIES ATTRIBUTED TO CYCLING, AND WAYS TO MINIMIZE THESE INJURIES
 COMMON OVERUSE INJURIES ATTRIBUTED TO CYCLING, AND WAYS TO MINIMIZE THESE INJURIES Listed are a few of the most common overuse injuries associated with cycling long distances. 1. Cervical and upper back
COMMON OVERUSE INJURIES ATTRIBUTED TO CYCLING, AND WAYS TO MINIMIZE THESE INJURIES Listed are a few of the most common overuse injuries associated with cycling long distances. 1. Cervical and upper back
Surgical Art. Formulaic Drawing Method. DRAWING WORKSHOP Learning to sketch for patient notes
 DRAWING WORKSHOP Learning to sketch for patient notes Surgical Art Formulaic Drawing Method Formulaic figure drawing systems involve using abstract rhythms and interlocking shapes to construct the human
DRAWING WORKSHOP Learning to sketch for patient notes Surgical Art Formulaic Drawing Method Formulaic figure drawing systems involve using abstract rhythms and interlocking shapes to construct the human
Don t. Hamstrings. Calf Muscles. both legs 2-3 times. stretch is felt in the back of the calf. Repeat with both legs 2-3 times.
 Remember to: Warm-up your muscles first before stretching (e.g. stretch after walking). Stretch until you feel mild discomfort, not pain. Never bounce or force a stretch. Hold the stretch for 10-30 seconds
Remember to: Warm-up your muscles first before stretching (e.g. stretch after walking). Stretch until you feel mild discomfort, not pain. Never bounce or force a stretch. Hold the stretch for 10-30 seconds
Completing the Loop: Management of the Adolescent Sports Injury. Adam Thomas, PT, DPT, ATC
 : Management of the Adolescent Sports Injury Adam Thomas, PT, DPT, ATC https://www.youtube.com/watch?v=vbufpo 8s3As On field assessment can be the most efficient when the health care provider has observed
: Management of the Adolescent Sports Injury Adam Thomas, PT, DPT, ATC https://www.youtube.com/watch?v=vbufpo 8s3As On field assessment can be the most efficient when the health care provider has observed
CHAPTER 3: BACK & ABDOMINAL STRETCHES. Standing Quad Stretch Athletic Edge - www.athleticedge.biz - (650) 815-6552
 815-6552") CHAPTER : BACK & ABDOMINAL STRETCHES Standing Quad Stretch ) Stand and grasp right ankle with same hand, use a wall or chair to Lower maintain Back balance with left hand. Maintain an upright Stretches
CHAPTER : BACK & ABDOMINAL STRETCHES Standing Quad Stretch ) Stand and grasp right ankle with same hand, use a wall or chair to Lower maintain Back balance with left hand. Maintain an upright Stretches
Most active and intricate part of the upper extremity Especially vulnerable to injury Do not respond well to serious trauma. Magee, 2008. pg.
 PTA 216 Most active and intricate part of the upper extremity Especially vulnerable to injury Do not respond well to serious trauma Magee, 2008. pg. 396 28 bones Numerous articulations 19 intrinsic muscles
PTA 216 Most active and intricate part of the upper extremity Especially vulnerable to injury Do not respond well to serious trauma Magee, 2008. pg. 396 28 bones Numerous articulations 19 intrinsic muscles
THORACIC OUTLET SYNDROME
 THORACIC OUTLET SYNDROME The Problem The term thoracic outlet syndrome is used to describe a condition of compression of the nerves and/or blood vessels in the region around the neck and collarbone, called
THORACIC OUTLET SYNDROME The Problem The term thoracic outlet syndrome is used to describe a condition of compression of the nerves and/or blood vessels in the region around the neck and collarbone, called
www.ghadialisurgery.com
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
CUMMULATIVE DISORDERS OF UPPER EXTIMITY DR HABIBOLLAHI
 CUMMULATIVE DISORDERS OF UPPER EXTIMITY DR HABIBOLLAHI Definition Musculoskeletal disorder (MSD) is an injury or disorder of the muscles, nerves, tendons, joints, cartilage,ligament and spinal discs. It
CUMMULATIVE DISORDERS OF UPPER EXTIMITY DR HABIBOLLAHI Definition Musculoskeletal disorder (MSD) is an injury or disorder of the muscles, nerves, tendons, joints, cartilage,ligament and spinal discs. It
Sheet 1A. Treating short/tight muscles using MET. Pectorals. Upper trapezius. Levator scapula
 Sheet 1A Treating short/tight muscles using MET Pectorals Once daily lie at edge of bed holding a half-kilo can, arm out sideways. Raise arm and hold for 10 seconds, then allow arm to hang down, stretching
Sheet 1A Treating short/tight muscles using MET Pectorals Once daily lie at edge of bed holding a half-kilo can, arm out sideways. Raise arm and hold for 10 seconds, then allow arm to hang down, stretching
HYPERLORDOSIS & PILATES TREATMENT
 HYPERLORDOSIS & PILATES TREATMENT Grace Tiangco 3/18/15 2012-2013 Abstract Sacramento/Mountain View Lordosis or Hyperlordosis is defined as a postural type in which the natural curves of the spine are
HYPERLORDOSIS & PILATES TREATMENT Grace Tiangco 3/18/15 2012-2013 Abstract Sacramento/Mountain View Lordosis or Hyperlordosis is defined as a postural type in which the natural curves of the spine are
Spine Conditioning Program Purpose of Program
 Prepared for: Prepared by: OrthoInfo Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle.
Prepared for: Prepared by: OrthoInfo Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle.
Shoulders (free weights)
") Dumbbell Shoulder Raise Dumbbell Shoulder Raise 1) Lie back onto an incline bench (45 or less) with a DB in each hand. (You may rest each DB on the corresponding thigh.) 2) Start position: Bring the DB
Dumbbell Shoulder Raise Dumbbell Shoulder Raise 1) Lie back onto an incline bench (45 or less) with a DB in each hand. (You may rest each DB on the corresponding thigh.) 2) Start position: Bring the DB
Shoulder Instability. Fig 1: Intact labrum and biceps tendon
 Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
Boxing/Kickboxing Shoulder Injuries and Prevention
 Boxing/Kickboxing Shoulder Injuries and Prevention Dr. Paul Newhart, D.C. Kickboxing and boxing are an excellent workout regimen, as long as precautions are taken so as not to injure the shoulders, elbows
Boxing/Kickboxing Shoulder Injuries and Prevention Dr. Paul Newhart, D.C. Kickboxing and boxing are an excellent workout regimen, as long as precautions are taken so as not to injure the shoulders, elbows
SHOULDER PULL DOWNS. To learn efficient use of the shoulder blades and arms while maintaining a neutral spine position.
 SHOULDER INTRODUCT ION Welcome to your shoulder exercise program The exercises in the program are designed to improve your shoulder mobility, posture and the control of the muscles in your neck and shoulder
SHOULDER INTRODUCT ION Welcome to your shoulder exercise program The exercises in the program are designed to improve your shoulder mobility, posture and the control of the muscles in your neck and shoulder
THE BENJAMIN INSTITUTE PRESENTS. Excerpt from Listen To Your Pain. Assessment & Treatment of. Low Back Pain. Ben E. Benjamin, Ph.D.
 THE BENJAMIN INSTITUTE PRESENTS Excerpt from Listen To Your Pain Assessment & Treatment of Low Back Pain A B E N J A M I N I N S T I T U T E E B O O K Ben E. Benjamin, Ph.D. 2 THERAPIST/CLIENT MANUAL The
THE BENJAMIN INSTITUTE PRESENTS Excerpt from Listen To Your Pain Assessment & Treatment of Low Back Pain A B E N J A M I N I N S T I T U T E E B O O K Ben E. Benjamin, Ph.D. 2 THERAPIST/CLIENT MANUAL The
Effects of Upper Extremity Mobilization Techniques on Fine-Motor Performance in Children with Neuromotor Disorders
 This program has been approved for CEUs by the American Occupational Therapy Association (AOTA), the Board of Certification (BOC), and is accepted for PDUs by the National Board of Certification of Occupational
This program has been approved for CEUs by the American Occupational Therapy Association (AOTA), the Board of Certification (BOC), and is accepted for PDUs by the National Board of Certification of Occupational
Elbow & Forearm. Notes. Notes. Lecture Slides - A.D.A.M. Lab Pics. Bones & Joints: Elbow & Forearm
 Elbow & Forearm Elbow & Forearm Notes Lecture Slides - A.D.A.M. Lab Pics Notes Bones & Joints: The elbow joint is a combination of joints but common reference is usually to the articulation of the distal
Elbow & Forearm Elbow & Forearm Notes Lecture Slides - A.D.A.M. Lab Pics Notes Bones & Joints: The elbow joint is a combination of joints but common reference is usually to the articulation of the distal
by joseph e. muscolino, DO photography by yanik chauvin
 by joseph e. muscolino, DO photography by yanik chauvin body mechanics palpation of the anterior neck ESOUCES For more information go to www.medlineplus.gov and search under anterior neck. The anterior
by joseph e. muscolino, DO photography by yanik chauvin body mechanics palpation of the anterior neck ESOUCES For more information go to www.medlineplus.gov and search under anterior neck. The anterior
CONSTRUCTION WORK and CUMULATIVE TRAUMA DISORDERS
 Connecticut Department of Public Health Environmental and Occupational Health Assessment Program 410 Capitol Avenue MS # 11OSP, PO Box 340308 Hartford, CT 06134-0308 (860) 509-7740 http://www.ct.gov/dph
Connecticut Department of Public Health Environmental and Occupational Health Assessment Program 410 Capitol Avenue MS # 11OSP, PO Box 340308 Hartford, CT 06134-0308 (860) 509-7740 http://www.ct.gov/dph
Lean-Ergonomic methods to reduce workers compensation costs (Part 2 of 2) Cumulative trauma disorders can be classified as: What is CTD?
 Cumulative trauma disorders can be classified as: What is CTD?") #425 Lean-ergonomic methods to reduce workers compensation costs, Part 2 of 2 Lean-Ergonomic methods to reduce workers compensation costs (Part 2 of 2) Govid Bharwani, Ph.D, Biomedical Engineering Thursday,
#425 Lean-ergonomic methods to reduce workers compensation costs, Part 2 of 2 Lean-Ergonomic methods to reduce workers compensation costs (Part 2 of 2) Govid Bharwani, Ph.D, Biomedical Engineering Thursday,
Rehabilitation after shoulder dislocation
 Physiotherapy Department Rehabilitation after shoulder dislocation Information for patients This information leaflet gives you advice on rehabilitation after your shoulder dislocation. It is not a substitute
Physiotherapy Department Rehabilitation after shoulder dislocation Information for patients This information leaflet gives you advice on rehabilitation after your shoulder dislocation. It is not a substitute
Temporo-Mandibular Joint Complex Exercise Suggestions
 Temporo-Mandibular Joint Complex Exercise Suggestions I. Exercise Generalizations: A. Patients with post-traumatic TMJ problems or with recent-onset dysfunction that is largely posture-related will generally
Temporo-Mandibular Joint Complex Exercise Suggestions I. Exercise Generalizations: A. Patients with post-traumatic TMJ problems or with recent-onset dysfunction that is largely posture-related will generally
How To Stretch Your Body
 Exercise Module A New Leaf Choices for Healthy Living University of North Carolina at Chapel Hill 2007 Center for Health Promotion and Disease Prevention Physical Activity Exercises for Keeping Active
Exercise Module A New Leaf Choices for Healthy Living University of North Carolina at Chapel Hill 2007 Center for Health Promotion and Disease Prevention Physical Activity Exercises for Keeping Active
Upper limb injuries. Traumatology RHS 231 Dr. Einas Al-Eisa
 Upper limb injuries Traumatology RHS 231 Dr. Einas Al-Eisa Pain in the limbs: May be classified under 4 headings: 1. Joint pain 2. Soft tissue pain 3. Neurogenic pain 4. Orthopaedic causes (fractures,
Upper limb injuries Traumatology RHS 231 Dr. Einas Al-Eisa Pain in the limbs: May be classified under 4 headings: 1. Joint pain 2. Soft tissue pain 3. Neurogenic pain 4. Orthopaedic causes (fractures,
by Ellen Saltonstall and Dr. Loren Fishman
 10 Yoga Poses for Low Back Pain Prevention by Ellen Saltonstall and Dr. Loren Fishman Introduction This series of poses is designed to prevent future back pain and also to relieve back pain that you may
10 Yoga Poses for Low Back Pain Prevention by Ellen Saltonstall and Dr. Loren Fishman Introduction This series of poses is designed to prevent future back pain and also to relieve back pain that you may
WRIST EXAMINATION. Look. Feel. Move. Special Tests
 WRIST EXAMINATION Look o Dorsum, side, palmar- palmar flex wrist to exacerbate dorsal swellings o Deformity e.g. radial deviation after colles, prominent ulna o Swellings e.g. ganglion o Scars, muscle
WRIST EXAMINATION Look o Dorsum, side, palmar- palmar flex wrist to exacerbate dorsal swellings o Deformity e.g. radial deviation after colles, prominent ulna o Swellings e.g. ganglion o Scars, muscle
CORRESPONDENCE EDUCATION PROGRAM
 Deep Tissue Massage CORRESPONDENCE EDUCATION PROGRAM Check your receipt for course expiration date. After that date no credit will be awarded for this program. 1 How to Complete this Program Thank you
Deep Tissue Massage CORRESPONDENCE EDUCATION PROGRAM Check your receipt for course expiration date. After that date no credit will be awarded for this program. 1 How to Complete this Program Thank you
Upper Extremity Special Tests. Cervical Tests. TMJ Dysfunction
 Upper Extremity Special Tests Cervical Tests Vertebral Artery Test: used to test for vertebral artery occlusion or insufficiency. The subject lies supine on the plinth with the examiner seated behind with
Upper Extremity Special Tests Cervical Tests Vertebral Artery Test: used to test for vertebral artery occlusion or insufficiency. The subject lies supine on the plinth with the examiner seated behind with
Chapter 4 The Shoulder Girdle
 Chapter 4 The Shoulder Girdle Key Manubrium Clavicle Coracoidprocess Acromionprocess bony landmarks Glenoid fossa Bones Lateral Inferior Medial border angle McGraw-Hill Higher Education. All rights reserved.
Chapter 4 The Shoulder Girdle Key Manubrium Clavicle Coracoidprocess Acromionprocess bony landmarks Glenoid fossa Bones Lateral Inferior Medial border angle McGraw-Hill Higher Education. All rights reserved.
Chapter 8. Muscular System: Skeletal Muscles of the Body
 Chapter 8 Muscular System: Skeletal Muscles of the Body INTRODUCTION This chapter continues our study of the muscular system by examining the distribution of muscles throughout the body. We learned in
Chapter 8 Muscular System: Skeletal Muscles of the Body INTRODUCTION This chapter continues our study of the muscular system by examining the distribution of muscles throughout the body. We learned in
Rehabilitation Exercises for Shoulder Injuries Pendulum Exercise: Wal Walk: Back Scratcher:
 Rehabilitation Exercises for Shoulder Injuries Begin these exercises when your pain has decreased about 25% from the time when your injury was most painful. Pendulum Exercise: Lean over with your uninjured
Rehabilitation Exercises for Shoulder Injuries Begin these exercises when your pain has decreased about 25% from the time when your injury was most painful. Pendulum Exercise: Lean over with your uninjured
Anatomy of Human Muscles
 Anatomy of Human Muscles PURPOSE: To develop skill in identifying muscle names and locations relative to other regional structures. To determine origin, insertion and principle action of muscles through
Anatomy of Human Muscles PURPOSE: To develop skill in identifying muscle names and locations relative to other regional structures. To determine origin, insertion and principle action of muscles through
INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D.
 05/05/2007 INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D. Hand injuries, especially the fractures of metacarpals and phalanges, are the most common fractures in the skeletal system. Hand injuries
05/05/2007 INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D. Hand injuries, especially the fractures of metacarpals and phalanges, are the most common fractures in the skeletal system. Hand injuries
Addressing Pelvic Rotation
 1 of 5 4/20/2008 10:31 AM http://www.strengthcoach.com Addressing Pelvic Rotation Aaron Brooks of Perfect Postures When trying to address your athlete's or client's limitations due to pain or joint restriction,
1 of 5 4/20/2008 10:31 AM http://www.strengthcoach.com Addressing Pelvic Rotation Aaron Brooks of Perfect Postures When trying to address your athlete's or client's limitations due to pain or joint restriction,
Passive Range of Motion Exercises
 Exercise and ALS The physical or occupational therapist will make recommendations for exercise based upon each patient s specific needs and abilities. Strengthening exercises are not generally recommended
Exercise and ALS The physical or occupational therapist will make recommendations for exercise based upon each patient s specific needs and abilities. Strengthening exercises are not generally recommended
Body Mechanics for Mammography Technologists
 Body Mechanics for Mammography Technologists Diane Rinella RT(R)(M)(BD)RDMS(BR)CDT Objectives Recognize causes and risk factors for Musculoskeletal Disorders (MSDs) for mammography technologists Understand
Body Mechanics for Mammography Technologists Diane Rinella RT(R)(M)(BD)RDMS(BR)CDT Objectives Recognize causes and risk factors for Musculoskeletal Disorders (MSDs) for mammography technologists Understand
Elbow Examination. Haroon Majeed
 Elbow Examination Haroon Majeed Key Points Inspection Palpation Movements Neurological Examination Special tests Joints above and below Before Starting Introduce yourself Explain to the patient what the
Elbow Examination Haroon Majeed Key Points Inspection Palpation Movements Neurological Examination Special tests Joints above and below Before Starting Introduce yourself Explain to the patient what the
What Are Bursitis and Tendinitis?
 Bursitis and tendinitis are both common conditions that cause swelling around muscles and bones. They occur most often in the shoulder, elbow, wrist, hip, knee, or ankle. A bursa is a small, fluid-filled
Bursitis and tendinitis are both common conditions that cause swelling around muscles and bones. They occur most often in the shoulder, elbow, wrist, hip, knee, or ankle. A bursa is a small, fluid-filled
The Elbow, Forearm, Wrist, and Hand
 Elbow - Bones The Elbow, Forearm, Wrist, and Hand Chapters 23 & 24 Humerus Distal end forms the medial & lateral condyles Lateral: capitulum Medial: trochlea Radius Ulna Sports Medicine II Elbow - Bones
Elbow - Bones The Elbow, Forearm, Wrist, and Hand Chapters 23 & 24 Humerus Distal end forms the medial & lateral condyles Lateral: capitulum Medial: trochlea Radius Ulna Sports Medicine II Elbow - Bones
STANDARD OPERATING PROCEDURES (SOP) FOR COMPUTER WORK, DESK TOP
 FOR COMPUTER WORK, DESK TOP") STANDARD OPERATING PROCEDURES (SOP) FOR COMPUTER WORK, DESK TOP General Guidelines-Best Practices: The following guidelines are applicable to office workers who sit at a desk and/or work on computers.
STANDARD OPERATING PROCEDURES (SOP) FOR COMPUTER WORK, DESK TOP General Guidelines-Best Practices: The following guidelines are applicable to office workers who sit at a desk and/or work on computers.
ESSENTIALPRINCIPLES. Wrist Pain. Radial and Ulnar Collateral Ligament Injuries. By Ben Benjamin
 ESSENTIALPRINCIPLES Wrist Pain Radial and Ulnar Collateral Ligament Injuries By Ben Benjamin 92 MASSAGE & BODYWORK FEBRUARY/MARCH 2005 Ulnar Collateral Ligament Radial Collateral Ligament Right wrist,
ESSENTIALPRINCIPLES Wrist Pain Radial and Ulnar Collateral Ligament Injuries By Ben Benjamin 92 MASSAGE & BODYWORK FEBRUARY/MARCH 2005 Ulnar Collateral Ligament Radial Collateral Ligament Right wrist,
Fact sheet Exercises for older adults undergoing rehabilitation
 Fact sheet Exercises for older adults undergoing rehabilitation Flexibility refers to the amount of movement possible around a joint and is necessary for normal activities of daily living such as stretching,
Fact sheet Exercises for older adults undergoing rehabilitation Flexibility refers to the amount of movement possible around a joint and is necessary for normal activities of daily living such as stretching,
How to Get and Keep a Healthy Back. Amy Eisenson, B.S. Exercise Physiologist
 How to Get and Keep a Healthy Back Amy Eisenson, B.S. Exercise Physiologist Lesson Objectives Statistics of Back Pain Anatomy of the Spine Causes of Back Pain Four Work Factors Core Muscles Connection
How to Get and Keep a Healthy Back Amy Eisenson, B.S. Exercise Physiologist Lesson Objectives Statistics of Back Pain Anatomy of the Spine Causes of Back Pain Four Work Factors Core Muscles Connection
.org. Shoulder Pain and Common Shoulder Problems. Anatomy. Cause
 Shoulder Pain and Common Shoulder Problems Page ( 1 ) What most people call the shoulder is really several joints that combine with tendons and muscles to allow a wide range of motion in the arm from scratching
Shoulder Pain and Common Shoulder Problems Page ( 1 ) What most people call the shoulder is really several joints that combine with tendons and muscles to allow a wide range of motion in the arm from scratching
THE THERAPIST S MANAGEMENT OF THE STIFF ELBOW MARK PISCHKE, OTR/L, CHT NOV, 17, 2014
 THE THERAPIST S MANAGEMENT OF THE STIFF ELBOW MARK PISCHKE, OTR/L, CHT NOV, 17, 2014 ELBOW FUNCTION 1. Required to provide stability for power and precision tasks for both open and closed kinetic chain
THE THERAPIST S MANAGEMENT OF THE STIFF ELBOW MARK PISCHKE, OTR/L, CHT NOV, 17, 2014 ELBOW FUNCTION 1. Required to provide stability for power and precision tasks for both open and closed kinetic chain
Preventing Overuse Injuries at Work
 Preventing Overuse Injuries at Work The Optimal Office Work Station Use an adjustable chair with good lumbar support. Keep your feet flat on a supportive surface (floor or foot rest). Your knees should
Preventing Overuse Injuries at Work The Optimal Office Work Station Use an adjustable chair with good lumbar support. Keep your feet flat on a supportive surface (floor or foot rest). Your knees should
General Guidelines. Neck Stretch: Side. Neck Stretch: Forward. Shoulder Rolls. Side Stretch
 Stretching Exercises General Guidelines Perform stretching exercises at least 2 3 days per week and preferably more Hold each stretch for 15 20 seconds Relax and breathe normally Stretching is most effective
Stretching Exercises General Guidelines Perform stretching exercises at least 2 3 days per week and preferably more Hold each stretch for 15 20 seconds Relax and breathe normally Stretching is most effective