Leveraging EHR to Improve Patient Safety: A Davies Story
|
|
|
- Jeremy Reeves
- 10 years ago
- Views:
Transcription
1 Leveraging EHR to Improve Patient Safety: A Davies Story Claudia Colgan, Vice President of Quality Initiatives Bruce Darrow, MD, PhD, Interim Chief Medical Information Officer Jill Kalman, MD, Director of Cardiomyopathy Program, Medical Director, PACT Program DISCLAIMER: The views and opinions expressed in this presentation are those of the author and do not necessarily represent official policy or position of HIMSS.

2 Conflict of Interest Disclosure Claudia Colgan Bruce Darrow, MD, PhD Jill Kalman, MD Has no real or apparent conflicts of interest to report HIMSS

3 Learning Objectives 1. Describe the business case for integrating of transitional care/care coordination objectives and IT 2. Identify the methods used to build tools and analytics to enhance program effectiveness 3. Discuss the lessons learned in transitioning from a low tech to a high tech solution

4 Background Knowledge Founded in ,171 bed tertiary care teaching and research Hospital 183 Hospital based practices 3,500 Physicians, residents, and fellows 2000 Nurses 58,000 Discharges 95,000 ED visits One million ambulatory visits in hospital clinics and Family Practice Associates

5 Background Knowledge U.S. News & World Report Best Hospitals The Mount Sinai Medical Center ranked 14th out of approximately 5,000 hospitals nationwide MSMC retained top billing on U.S. News Honor Roll of the nation s most outstanding hospitals Overall, Mount Sinai ranked in 11 of 16 specialties Geriatrics (No. 2), Gastroenterology (No. 7), Heart and Heart Surgery (No. 10) Mount Sinai has achieved HIMSS Stage 6 EMR Adoption Model

6 Executive Summary The MSMC Preventable Admissions Care Team (PACT) is dramatically reducing readmissions PACT included a combination of EHR and care model innovations EHR enhanced ability to identify patients at high risk of readmission Psychosocial drivers of readmission addressed through a 35 day social work lead transitional care intervention In addition to greater use of MSMC s homecare partner (VNA), open access was provided to the MSMC PACT clinic
, open access was provided to the MSMC")
7 Executive Summary The MSMC Preventable Admissions Care Team (PACT) is dramatically reducing readmissions EHR allowed hard wiring of workflows needed to reduce readmissions, improve care, and lower costs of care 56% reduction in 30 day readmissions by patients in the PACT program 91% of patients made follow up appointments in 7 10 days 84% of patients kept their appointment

8 Problems Addressed Medicare will begin reducing reimbursement for certain 30 day readmissions Admission history was traditionally used to identify patients at high risk of readmission, so interventions could be targeted Without integrated EHR, identification was very labor and paper intensive It did not identify those with a high risk for readmission, but do not have a history of admissions PACT needed an automated process to assist in the workflow

9 Readmission Rates Nearly 20% of Medicare hospitalizations are followed by readmission within 30 days 90% of re hospitalizations within 30 days appear to be unplanned, the result of clinical deterioration Only half of the patients re hospitalized within 30 days had a physician visit before readmission Unknown if lack of physician visit causes readmissions but poor continuity of care, especially for many chronically ill patients 19% of Medicare discharges are followed by an adverse event within 30 days 2/3 are drug events, usually deemed "preventable"

10 e1 PACT Timeline May 1, 2011 Epic Go Live

11 Slide 10 e1 e535cco, 1/23/2013

12 e2

13 Slide 11 e2 e535cco, 1/23/2013

14 Transformational Change and Integration of Resources

15 Design Several enhancements to the EHR became key enablers to reducing readmissions A readmission within 30 days prediction model was developed using logistic regression and did not depend on admission data The risk prediction score was integrated into the EHR identifying at risk patients and increasing awareness of the patients

16
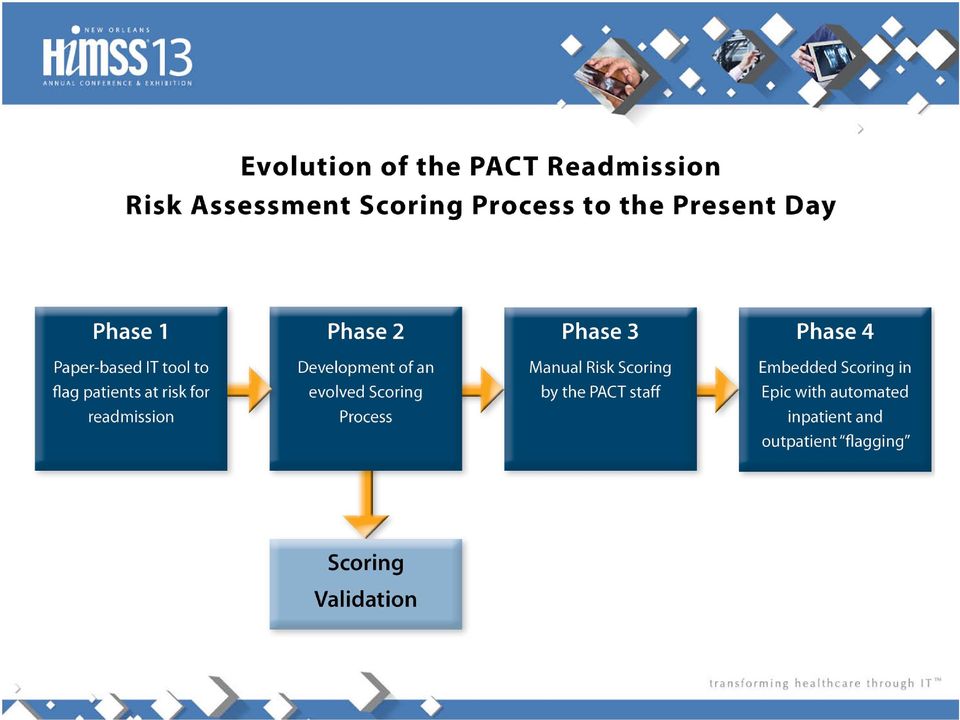
17 Design Several enhancements to the EHR became key enablers to reducing readmissions An admissions history form was created that gathered required, discrete data elements Have the patient profile indicate a high risk for readmission Produce rounding reports with identified patients so PACT team can conduct interventional rounding

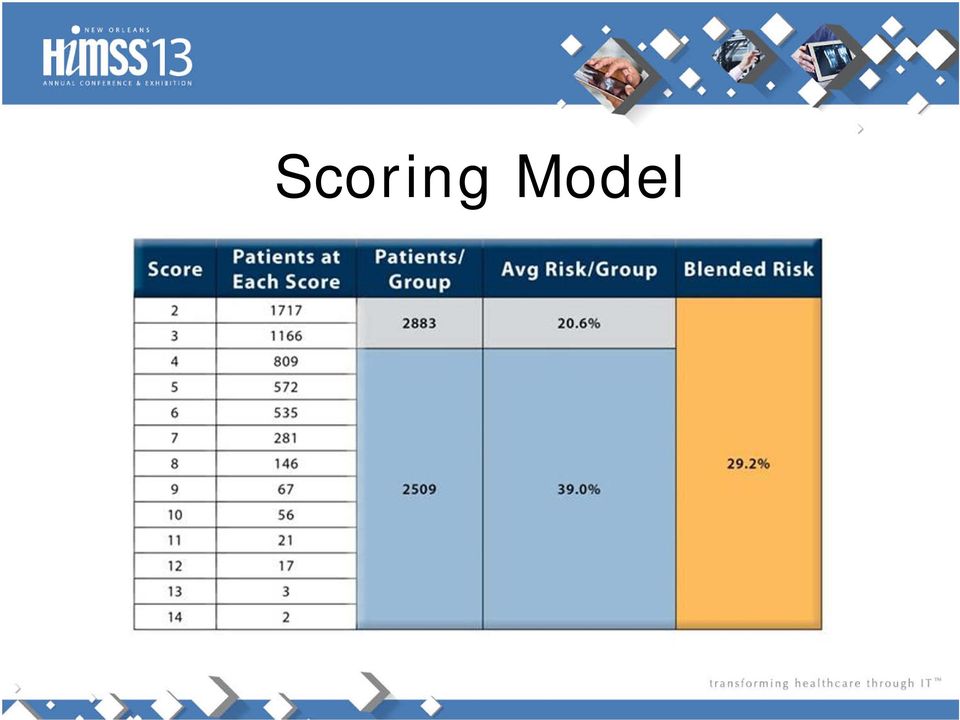
18 Scoring Model

19 Scoring Model
20 Design Several enhancements to the EHR became key enablers to reducing readmissions Excel spreadsheets extracted from the legacy EHR were ed throughout the hospital to identify high risk patients A logistic regression model was developed by the MSMC Health Evidence and Policy Department which used a sophisticated statistical tool and added both past medical admissions and comorbidities into the model The model still required some manual additions by the caregivers to get to the final risk score

21 Design The model was validated in actual clinical practice The PACT model was fully implemented in Epic Medicare data was used so the model could incorporate any prior admissions in New York, not just those occurring at Mount Sinai Social workers now document the psychosocial assessment and scoring using Epic automation The flag symbol is now displayed on various screens for clinicians across the continuum of care
22 Areas of Psychosocial Strain What services and issues outside the hospital influence the ability to change readmission rates?
23 Design Building the admissions history form in Epic to ask discrete questions such as: Has the patient seen his or her primary care physician in the past 12 months? Has the patient been seen in an ED in the past six months? The patient profile in Epic noticeably indicates via a red flag that the patient is high risk for readmission generating a daily rounding report PACT can then assist patient with the 15 areas of psychosocial strain
24 Overall Process of the PACT Program
25 Outcomes For 1 st 615 patients completing 5 week intervention, a 56% reduction in 30 day readmissions were seen Using each patient as own control, pre PACT admits were 952; post PACT was % of PACT enrollees had risk score > 3, meaning an admission rate of 19 29%
26 Outcomes MSMC measured outcomes six months before and after PACT interventions: 43% reduction in hospitalizations 54% reduction in ED visits 91% of patients enrolled in PACT had 7 10 day follow up appointments 84% of patients kept their appointments
27 Costs During pilot phase, cost was $627 per patient per year ($376,000 annually) IT costs were approximately $14,500 Health Policy and Physician involvement was provided in house CMS prohibits disclosure of approved blended rate under recent CCTP award
28 Benefits A National Public Radio investigation followed a medically complex patient example Showed PACT reduced a year of Medicare spending by $85,000 A number of grants have provided funding, including a recent Community Based Care Transitions Program (CCTP) award from CMS (in partnership with the Institute of Family Health) In an ACO model, PACT was estimated to save $1.6M in health care spending over a 6 month period
29 Lessons Learned Industry standard assessments identify high risk patients based on diagnosis and comorbidities When data specific to past medical encounter history and key demographic data were added, the identification process was greatly enhanced Effective use of the of the patient s problem list was very important If MSMC had started looking for data earlier (as soon as the Epic go live), we could have been more accurate with population and future needs predictions
30 Lessons Learned Point of care integration was desired Integration required external calculations, reporting, modifier setting, and flagging Flagging for more than just reporting This integration has proven useful to many other of our Care Coordination Efforts including our Accountable Care Organization Project would have benefited from starting with an IT design group focusing on process; this would have assisted in helping locate patients
31 Contact Information Claudia Colgan, Vice President of Quality Initiatives Bruce Darrow, MD, PhD, Interim Chief Medical Information Officer Jill Kalman, MD, Director of Cardiomyopathy Program, Medical Director, PACT Program
32 Questions
Transitional Care at Mount Sinai The PACT Program
 Transitional Care at Mount Sinai The PACT Program Maria Basso Lipani, LCSW Program Director, PACT Mount Sinai Hospital Mount Sinai Medical Center Founded in 1852 1,171-bed tertiary-care teaching and research
Transitional Care at Mount Sinai The PACT Program Maria Basso Lipani, LCSW Program Director, PACT Mount Sinai Hospital Mount Sinai Medical Center Founded in 1852 1,171-bed tertiary-care teaching and research
Reducing Readmissions with Predictive Analytics
 Reducing Readmissions with Predictive Analytics Conway Regional Health System uses analytics and the LACE Index from Medisolv s RAPID business intelligence software to identify patients poised for early
Reducing Readmissions with Predictive Analytics Conway Regional Health System uses analytics and the LACE Index from Medisolv s RAPID business intelligence software to identify patients poised for early
Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights
 Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights Emily Brower Executive Director Accountable Care Programs [email protected] November 2013 1 Contents Overview of
Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights Emily Brower Executive Director Accountable Care Programs [email protected] November 2013 1 Contents Overview of
How MissionPoint Health is Using Population Health Insights to Achieve ACO Success
 How MissionPoint Health is Using Population Health Insights to Achieve ACO Success Background The United States spends more per capita on healthcare than other country, yet is ranked last among industrialized
How MissionPoint Health is Using Population Health Insights to Achieve ACO Success Background The United States spends more per capita on healthcare than other country, yet is ranked last among industrialized
Pushing the Envelope of Population Health
 Pushing the Envelope of Population Health Timothy Ferris, MD, MPH Senior Vice President, Population Health Management, Partners HealthCare May 15, 2014 DISCLAIMER: The views and opinions expressed in this
Pushing the Envelope of Population Health Timothy Ferris, MD, MPH Senior Vice President, Population Health Management, Partners HealthCare May 15, 2014 DISCLAIMER: The views and opinions expressed in this
Six Communication Best Practices for Transitional Care Management
 WHITE PAPER Six Communication Best Practices for Transitional Care Management In the era of chronic illness and historically long lifespans, patient care transitions to home or another facility have become
WHITE PAPER Six Communication Best Practices for Transitional Care Management In the era of chronic illness and historically long lifespans, patient care transitions to home or another facility have become
#Aim2Innovate. Share session insights and questions socially. UCLA Primary Care Innovation Model 6/13/2015. Mark S. Grossman, MD, MBA, FAAP, FACP
 UCLA Primary Care Innovation Model Mark S. Grossman, MD, MBA, FAAP, FACP Chief Medical Office, UCLA Community Physicians & Specialty Care Networks June 16, 2015 DISCLAIMER: The views and opinions expressed
UCLA Primary Care Innovation Model Mark S. Grossman, MD, MBA, FAAP, FACP Chief Medical Office, UCLA Community Physicians & Specialty Care Networks June 16, 2015 DISCLAIMER: The views and opinions expressed
Using Predictive Analytics to Reduce COPD Readmissions
 Using Predictive Analytics to Reduce COPD Readmissions Agenda Information about PinnacleHealth Today s Environment PinnacleHealth Case Study Questions? PinnacleHealth System Non-profit, community teaching
Using Predictive Analytics to Reduce COPD Readmissions Agenda Information about PinnacleHealth Today s Environment PinnacleHealth Case Study Questions? PinnacleHealth System Non-profit, community teaching
Home Health Care Today: Higher Acuity Level of Patients Highly skilled Professionals Costeffective Uses of Technology Innovative Care Techniques
 Comprehensive EHR Infrastructure Across the Health Care System The goal of the Administration and the Department of Health and Human Services to achieve an infrastructure for interoperable electronic health
Comprehensive EHR Infrastructure Across the Health Care System The goal of the Administration and the Department of Health and Human Services to achieve an infrastructure for interoperable electronic health
Analytic-Driven Quality Keys Success in Risk-Based Contracts. Ross Gustafson, Vice President Allina Performance Resources, Health Catalyst
 Analytic-Driven Quality Keys Success in Risk-Based Contracts March 2 nd, 2016 Ross Gustafson, Vice President Allina Performance Resources, Health Catalyst Brian Rice, Vice President Network/ACO Integration,
Analytic-Driven Quality Keys Success in Risk-Based Contracts March 2 nd, 2016 Ross Gustafson, Vice President Allina Performance Resources, Health Catalyst Brian Rice, Vice President Network/ACO Integration,
Kick off Meeting November 11 13, 2015. MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF)
") Kick off Meeting November 11 13, 2015 MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF) Team Composition Justin Huynh, MD Internal Medicine, Physician Champion Mary Laubinger,
Kick off Meeting November 11 13, 2015 MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF) Team Composition Justin Huynh, MD Internal Medicine, Physician Champion Mary Laubinger,
Dual Eligible and High Risk Populations: A Case for Integrated Care and Redesign
 Dual Eligible and High Risk Populations: A Case for Integrated Care and Redesign Peggy Johnson, MD Chief of Psychiatry, Commonwealth Care Alliance Twitter Handle CCABoston May 15, 2014 DISCLAIMER: The
Dual Eligible and High Risk Populations: A Case for Integrated Care and Redesign Peggy Johnson, MD Chief of Psychiatry, Commonwealth Care Alliance Twitter Handle CCABoston May 15, 2014 DISCLAIMER: The
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION
 Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Predictive Analytics in Action: Tackling Readmissions
 Predictive Analytics in Action: Tackling Readmissions Jason Haupt Sr. Statistician & Manager of Clinical Analysis July 17, 2013 Agenda Background Lifecycle Current status Discussion 2 Goals for today Describe
Predictive Analytics in Action: Tackling Readmissions Jason Haupt Sr. Statistician & Manager of Clinical Analysis July 17, 2013 Agenda Background Lifecycle Current status Discussion 2 Goals for today Describe
Developing Nurse Mangers Through Competency Based Informatics Education Session 39 Kathleen Guiney RN MN DISCLAIMER: The views and opinions expressed
 Developing Nurse Mangers Through Competency Based Informatics Education Session 39 Kathleen Guiney RN MN DISCLAIMER: The views and opinions expressed in this presentation are those of the author and do
Developing Nurse Mangers Through Competency Based Informatics Education Session 39 Kathleen Guiney RN MN DISCLAIMER: The views and opinions expressed in this presentation are those of the author and do
Dual RFI Response Summary
 Dual RFI Response Summary Improving Care through Integrated Medicare and Medi- Cal Delivery Models Stuart Levine, MD., MHA. Keith Wilson, MD Robert Margolis, MD. Stakeholder Meeting August 30, 2011 1 Organization
Dual RFI Response Summary Improving Care through Integrated Medicare and Medi- Cal Delivery Models Stuart Levine, MD., MHA. Keith Wilson, MD Robert Margolis, MD. Stakeholder Meeting August 30, 2011 1 Organization
Early Lessons learned from strong revenue cycle performers
 Healthcare Informatics June 2012 Accountable Care Organizations Early Lessons learned from strong revenue cycle performers Healthcare Informatics Accountable Care Organizations Early Lessons learned from
Healthcare Informatics June 2012 Accountable Care Organizations Early Lessons learned from strong revenue cycle performers Healthcare Informatics Accountable Care Organizations Early Lessons learned from
Population Health Solutions for Employers MEDIA RESOURCES
 Population Health Solutions for Employers MEDIA RESOURCES ABOUT MISSIONPOINT MissionPoint s mission is to make healthcare more affordable, accessible and improve the quality of care for our members. MissionPoint
Population Health Solutions for Employers MEDIA RESOURCES ABOUT MISSIONPOINT MissionPoint s mission is to make healthcare more affordable, accessible and improve the quality of care for our members. MissionPoint
HIMSS Davies Enterprise Application --- COVER PAGE ---
 HIMSS Davies Enterprise Application --- COVER PAGE --- Applicant Organization: Hawai i Pacific Health Organization s Address: 55 Merchant Street, 27 th Floor, Honolulu, Hawai i 96813 Submitter s Name:
HIMSS Davies Enterprise Application --- COVER PAGE --- Applicant Organization: Hawai i Pacific Health Organization s Address: 55 Merchant Street, 27 th Floor, Honolulu, Hawai i 96813 Submitter s Name:
Accountable Care Organizations: What Are They and Why Should I Care?
 Accountable Care Organizations: What Are They and Why Should I Care? Adrienne Green, MD Associate Chief Medical Officer, UCSF Medical Center Ami Parekh, MD, JD Med. Director, Health System Innovation,
Accountable Care Organizations: What Are They and Why Should I Care? Adrienne Green, MD Associate Chief Medical Officer, UCSF Medical Center Ami Parekh, MD, JD Med. Director, Health System Innovation,
Be Careful What You Ask For A Predictive Model That Really Works
 Be Careful What You Ask For A Predictive Model That Really Works Rod Christensen, MD President, Allina Health Clinics Cheryl Hermann, RN, MBA Vice President, Clinic Operations & Patient Care Services Karen
Be Careful What You Ask For A Predictive Model That Really Works Rod Christensen, MD President, Allina Health Clinics Cheryl Hermann, RN, MBA Vice President, Clinic Operations & Patient Care Services Karen
Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015
 Leveraging the Continuum to Avoid Unnecessary Utilization While Improving Quality Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015 Karim A. Habibi, FHFMA, MPH, MS Senior
Leveraging the Continuum to Avoid Unnecessary Utilization While Improving Quality Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015 Karim A. Habibi, FHFMA, MPH, MS Senior
Empowering Value-Based Healthcare
 Empowering Value-Based Healthcare Episode Connect, Remedy s proprietary suite of software applications, is a powerful platform for managing value-based payment programs. Delivered via the web or mobile
Empowering Value-Based Healthcare Episode Connect, Remedy s proprietary suite of software applications, is a powerful platform for managing value-based payment programs. Delivered via the web or mobile
Using EHRs, HIE, & Data Analytics to Support Accountable Care. Jonathan Shoemaker June 2014
 Using EHRs, HIE, & Data Analytics to Support Accountable Care Jonathan Shoemaker June 2014 Agenda Allina Health overview ACO framework- setting the stage Health Information Technology and ACOs Role of
Using EHRs, HIE, & Data Analytics to Support Accountable Care Jonathan Shoemaker June 2014 Agenda Allina Health overview ACO framework- setting the stage Health Information Technology and ACOs Role of
DRIVING VALUE IN HEALTHCARE: PERSPECTIVES FROM TWO ACO EXECUTIVES, PART I
 DRIVING VALUE IN HEALTHCARE: PERSPECTIVES FROM TWO ACO EXECUTIVES, PART I A firm understanding of the key components and drivers of healthcare reform is increasingly important within the pharmaceutical,
DRIVING VALUE IN HEALTHCARE: PERSPECTIVES FROM TWO ACO EXECUTIVES, PART I A firm understanding of the key components and drivers of healthcare reform is increasingly important within the pharmaceutical,
Population Health 2.0: Bending the Cost Curve by Moving Beyond the Pyramid
 Population Health 2.0: Bending the Cost Curve by Moving Beyond the Pyramid Advocate Health Care $5 Billion Annual Revenue AA Rated 12 Acute Care Hospitals 1 Children s Hospital 5 Level 1 Trauma Centers
Population Health 2.0: Bending the Cost Curve by Moving Beyond the Pyramid Advocate Health Care $5 Billion Annual Revenue AA Rated 12 Acute Care Hospitals 1 Children s Hospital 5 Level 1 Trauma Centers
How To Analyze Health Data
 POPULATION HEALTH ANALYTICS ANALYTICALLY-DRIVEN INSIGHTS FOR POPULATION HEALTH LAURIE ROSE, PRINCIPAL CONSULTANT HEALTH CARE GLOBAL PRACTICE DISCUSSION TOPICS Population Health: What & Why Now? Population
POPULATION HEALTH ANALYTICS ANALYTICALLY-DRIVEN INSIGHTS FOR POPULATION HEALTH LAURIE ROSE, PRINCIPAL CONSULTANT HEALTH CARE GLOBAL PRACTICE DISCUSSION TOPICS Population Health: What & Why Now? Population
1900 K St. NW Washington, DC 20006 c/o McKenna Long
 1900 K St. NW Washington, DC 20006 c/o McKenna Long Centers for Medicare & Medicaid Services U. S. Department of Health and Human Services Attention CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re:
1900 K St. NW Washington, DC 20006 c/o McKenna Long Centers for Medicare & Medicaid Services U. S. Department of Health and Human Services Attention CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re:
The Value Quadrant of Healthcare Reform. 2008 Pharos Innovations, LLC. All Rights Reserved.
 The Value Quadrant of Healthcare Reform ACOs in PPACA Provider Organizations or networked groups Accountable for quality, cost and overall care of defined population of Medicare FFS benes Key metrics to
The Value Quadrant of Healthcare Reform ACOs in PPACA Provider Organizations or networked groups Accountable for quality, cost and overall care of defined population of Medicare FFS benes Key metrics to
Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education
 1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
The Mount Sinai Health System Is Formed to Provide Expanded Access to Primary, Specialty, and Ambulatory Care
 The Mount Sinai Health System Is Formed to Provide Expanded Access to Primary, Specialty, and Ambulatory Care Seven Member Hospital Campuses and a Single Medical School Serve as Basis for Integrated Health
The Mount Sinai Health System Is Formed to Provide Expanded Access to Primary, Specialty, and Ambulatory Care Seven Member Hospital Campuses and a Single Medical School Serve as Basis for Integrated Health
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
An Essential Ingredient for a Successful ACO: The Clinical Knowledge Exchange
 An Essential Ingredient for a Successful ACO: The Clinical Knowledge Exchange Jonathan Everett Director, Health Information Technology Chinese Community Health Care Association Darren Schulte, MD, MPP
An Essential Ingredient for a Successful ACO: The Clinical Knowledge Exchange Jonathan Everett Director, Health Information Technology Chinese Community Health Care Association Darren Schulte, MD, MPP
Mastering the Data Game: Accelerating
 Mastering the Data Game: Accelerating Integration and Optimization Healthcare systems are breaking new barriers in analytics as they seek to meet aggressive quality and financial goals. Mastering the Data
Mastering the Data Game: Accelerating Integration and Optimization Healthcare systems are breaking new barriers in analytics as they seek to meet aggressive quality and financial goals. Mastering the Data
TRUSTED PATIENT EDUCATION FOR BETTER OUTCOMES. MICROMEDEX Patient Connect. Patient Education & Engagement
 TRUSTED PATIENT EDUCATION FOR BETTER OUTCOMES MICROMEDEX Patient Connect Patient Education & Engagement Trusted Patient Education for Better Outcomes All your training, experience, tools, and technology
TRUSTED PATIENT EDUCATION FOR BETTER OUTCOMES MICROMEDEX Patient Connect Patient Education & Engagement Trusted Patient Education for Better Outcomes All your training, experience, tools, and technology
Supporting a Continuous Process Improvement Model With A Cost-Effective Data Warehouse
 Supporting a Continuous Process Improvement Model With A Cost-Effective Data Warehouse Dave Hynson, Vice President and CIO Juan Negrin, Manager of BI and Data Governance OVERVIEW I. ALIGNMENT TO BUSINESS
Supporting a Continuous Process Improvement Model With A Cost-Effective Data Warehouse Dave Hynson, Vice President and CIO Juan Negrin, Manager of BI and Data Governance OVERVIEW I. ALIGNMENT TO BUSINESS
Palomar Health: Ready Set RUN Configuration of Actionable Alerts Ben Kanter MD FCCP, CMIO Jennifer Sloane, RN, BSN, MBA, PMP
 Palomar Health: Ready Set RUN Configuration of Actionable Alerts Ben Kanter MD FCCP, CMIO Jennifer Sloane, RN, BSN, MBA, PMP DISCLAIMER: The views and opinions expressed in this presentation are those
Palomar Health: Ready Set RUN Configuration of Actionable Alerts Ben Kanter MD FCCP, CMIO Jennifer Sloane, RN, BSN, MBA, PMP DISCLAIMER: The views and opinions expressed in this presentation are those
Transforming traditional case management through local provider partnerships
 Transforming traditional case management through local provider partnerships Introduction The dramatic changes sweeping the health care industry are driving a strong interest in engaging patients at the
Transforming traditional case management through local provider partnerships Introduction The dramatic changes sweeping the health care industry are driving a strong interest in engaging patients at the
Empowering Value-Based Healthcare
 Empowering Value-Based Healthcare Episode Connect, Remedy s proprietary suite of software applications, is a powerful platform for managing value based payment programs. Delivered via the web or mobile
Empowering Value-Based Healthcare Episode Connect, Remedy s proprietary suite of software applications, is a powerful platform for managing value based payment programs. Delivered via the web or mobile
CCNC Care Management
 CCNC Care Management Community Care of North Carolina (CCNC) is a statewide population management and care coordination infrastructure founded on the primary care medical home model. CCNC incorporates
CCNC Care Management Community Care of North Carolina (CCNC) is a statewide population management and care coordination infrastructure founded on the primary care medical home model. CCNC incorporates
Health Care Leader Action Guide to Reduce Avoidable Readmissions
 Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
Strategies and Considerations for Extending EHR Technology to Affiliated Practices/Community Physicians
 Strategies and Considerations for Extending EHR Technology to Affiliated Practices/Community Physicians Dr. Phil Oravetz, MD, MPH, MBA Medical Director, Accountable Care Ochsner Health System Brad Boyd
Strategies and Considerations for Extending EHR Technology to Affiliated Practices/Community Physicians Dr. Phil Oravetz, MD, MPH, MBA Medical Director, Accountable Care Ochsner Health System Brad Boyd
Michael J. Tronolone, MD, MMM, Chief Medical Officer Michelle Matin, MD, FAAFP Associate Medical Director for Quality The Polyclinic Seattle, WA
 Succeed with Population Health Management in a Fee-for-Service Environment and Improve Clinical Quality Measures While Transitioning to Value- Based Care Michael J. Tronolone, MD, MMM, Chief Medical Officer
Succeed with Population Health Management in a Fee-for-Service Environment and Improve Clinical Quality Measures While Transitioning to Value- Based Care Michael J. Tronolone, MD, MMM, Chief Medical Officer
Innovations@Home. Home Health Initiatives Reduce Avoidable Readmissions by Leveraging Innovation
 How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
DATA ACROSS THE CARE CONTINUUM
 FierceHealthIT Sponsored by: A FierceHealthIT Executive Summary share: DATA ACROSS THE CARE CONTINUUM Health IT execs share challenges, rewards of data analytics at live event in Chicago By Gienna Shaw
FierceHealthIT Sponsored by: A FierceHealthIT Executive Summary share: DATA ACROSS THE CARE CONTINUUM Health IT execs share challenges, rewards of data analytics at live event in Chicago By Gienna Shaw
October 18, 2013. Articulating the Value Proposition of Innovative Medical Technologies in the Healthcare Reform Landscape
 October 18, 2013 Articulating the Value Proposition of Innovative Medical Technologies in the Healthcare Reform Landscape Outline The Changing Landscape Evolving Care Delivery and Incentive Models Provider
October 18, 2013 Articulating the Value Proposition of Innovative Medical Technologies in the Healthcare Reform Landscape Outline The Changing Landscape Evolving Care Delivery and Incentive Models Provider
Frequently Asked Questions: Electronic Health Records (EHR) Incentive Payment Program
 Incentive Payment Program") 1. Where did the Electronic Health Records (EHR) Incentive Program originate? The American Recovery and Reinvestment Act (ARRA) was signed into law on February 17, 2009, and established a framework of
1. Where did the Electronic Health Records (EHR) Incentive Program originate? The American Recovery and Reinvestment Act (ARRA) was signed into law on February 17, 2009, and established a framework of
Emerging Technologies That Support Transitions of Care. 8 June 2016 Elaine Remmlinger, Senior Partner, and Robin Settle, Partner
 Emerging Technologies That Support Transitions of Care 8 June 2016 Elaine Remmlinger, Senior Partner, and Robin Settle, Partner Topics of Discussion Drivers of Transitions of Care Technology Perspective:
Emerging Technologies That Support Transitions of Care 8 June 2016 Elaine Remmlinger, Senior Partner, and Robin Settle, Partner Topics of Discussion Drivers of Transitions of Care Technology Perspective:
WHITE PAPER. QualityAnalytics. Bridging Clinical Documentation and Quality of Care
 WHITE PAPER QualityAnalytics Bridging Clinical Documentation and Quality of Care 2 EXECUTIVE SUMMARY The US Healthcare system is undergoing a gradual, but steady transformation. At the center of this transformation
WHITE PAPER QualityAnalytics Bridging Clinical Documentation and Quality of Care 2 EXECUTIVE SUMMARY The US Healthcare system is undergoing a gradual, but steady transformation. At the center of this transformation
Quantitative study reveals data about VNA, ECM and clinical content
 Quantitative study reveals data about VNA, ECM and clinical content Survey reveals preference for a patient-centric, unified health record that presents all relevant data at the point of care Fueled by
Quantitative study reveals data about VNA, ECM and clinical content Survey reveals preference for a patient-centric, unified health record that presents all relevant data at the point of care Fueled by
How to Use Telehealth to Improve Outcomes: Banner Health s Experience with Patients in its Pioneer ACO. Objectives
 How to Use Telehealth to Improve Outcomes: Banner Health s Experience with Patients in its Pioneer ACO 2015 NAHC Annual Meeting Session 603 October 30 th, 2015 Julie Reisetter, MS, RN CNO, Banner Telehealth
How to Use Telehealth to Improve Outcomes: Banner Health s Experience with Patients in its Pioneer ACO 2015 NAHC Annual Meeting Session 603 October 30 th, 2015 Julie Reisetter, MS, RN CNO, Banner Telehealth
Health Home Performance Enhancement through Novel Reuse of Syndromic Surveillance Data
 Health Home Performance Enhancement through Novel Reuse of Syndromic Surveillance Data Category: Fast Track Solutions Contact: Tim Robyn Chief Information Officer Office of Administration Information Technology
Health Home Performance Enhancement through Novel Reuse of Syndromic Surveillance Data Category: Fast Track Solutions Contact: Tim Robyn Chief Information Officer Office of Administration Information Technology
Premier ACO Collaboratives Driving to a Patient-Centered Health System
 Premier ACO Collaboratives Driving to a Patient-Centered Health System As a nation we all must work to rein in spiraling U.S. healthcare costs, expand access, promote wellness and improve the consistency
Premier ACO Collaboratives Driving to a Patient-Centered Health System As a nation we all must work to rein in spiraling U.S. healthcare costs, expand access, promote wellness and improve the consistency
What do ACO s and Hospitals want from SNF s and CCRC s
 What do ACO s and Hospitals want from SNF s and CCRC s Presented to the Institute of Senior Living, April 11, 2013 A Division of Kindred Healthcare 1 Assessing the match: What hospitals and ACO s currently
What do ACO s and Hospitals want from SNF s and CCRC s Presented to the Institute of Senior Living, April 11, 2013 A Division of Kindred Healthcare 1 Assessing the match: What hospitals and ACO s currently
1a-b. Title: Clinical Decision Support Helps Memorial Healthcare System Achieve 97 Percent Compliance With Pediatric Asthma Core Quality Measures
 1a-b. Title: Clinical Decision Support Helps Memorial Healthcare System Achieve 97 Percent Compliance With Pediatric Asthma Core Quality Measures 2. Background Knowledge: Asthma is one of the most prevalent
1a-b. Title: Clinical Decision Support Helps Memorial Healthcare System Achieve 97 Percent Compliance With Pediatric Asthma Core Quality Measures 2. Background Knowledge: Asthma is one of the most prevalent
US Hospital Information Systems Overview and Outlook, 2013 2020 Managing Information in an Era of Reform
 US Hospital Information Systems Overview and Outlook, 2013 2020 Managing Information in an Era of Reform December 2014 Contents Section Slide Number Executive Summary 11 Market Background 19 The EHR Landscape
US Hospital Information Systems Overview and Outlook, 2013 2020 Managing Information in an Era of Reform December 2014 Contents Section Slide Number Executive Summary 11 Market Background 19 The EHR Landscape
Population Health Management Systems
 Population Health Management Systems What are they and how can they help public health? August 18, 1:00 p.m. 2:30 p.m. EDT Presented by the Public Health Informatics Working Group Webinar sponsored by
Population Health Management Systems What are they and how can they help public health? August 18, 1:00 p.m. 2:30 p.m. EDT Presented by the Public Health Informatics Working Group Webinar sponsored by
HIMSS Electronic Health Record Definitional Model Version 1.0
 HIMSS Electronic Health Record Definitional Model Version 1.0 Prepared by HIMSS Electronic Health Record Committee Thomas Handler, MD. Research Director, Gartner Rick Holtmeier, President, Berdy Systems
HIMSS Electronic Health Record Definitional Model Version 1.0 Prepared by HIMSS Electronic Health Record Committee Thomas Handler, MD. Research Director, Gartner Rick Holtmeier, President, Berdy Systems
THE CHALLENGE OF COORDINATING EMR
 THE CHALLENGE OF COORDINATING EMR CLINICAL CONNECT: TWO YEARS OF REGIONAL ELECTRONIC HEALTH INFORMATION EXCHANGE NANCY A. LANDMAN, CIO INTERNATIONAL & COMMERCIAL SERVICES, UPMC 10/8/2014 2 UPMC Today:
THE CHALLENGE OF COORDINATING EMR CLINICAL CONNECT: TWO YEARS OF REGIONAL ELECTRONIC HEALTH INFORMATION EXCHANGE NANCY A. LANDMAN, CIO INTERNATIONAL & COMMERCIAL SERVICES, UPMC 10/8/2014 2 UPMC Today:
Shared Governance Models Optimize Outcomes, Adoption and User Perception
 Shared Governance Models Optimize Outcomes, Adoption and User Perception Nicole Martinez BSN, RN DISCLAIMER: The views and opinions expressed in this presentation are those of the author and do not necessarily
Shared Governance Models Optimize Outcomes, Adoption and User Perception Nicole Martinez BSN, RN DISCLAIMER: The views and opinions expressed in this presentation are those of the author and do not necessarily
Theresa Dolan COO Mount Sinai Care April 25, 2014
 Stephen Nuckolls CEO, Coastal Carolina Health Care, P.A Jeff Spight SVP, ACO Market Operations Universal American Theresa Dolan COO Mount Sinai Care April 25, 2014 Overview of the ACO Beneficiary Assignment
Stephen Nuckolls CEO, Coastal Carolina Health Care, P.A Jeff Spight SVP, ACO Market Operations Universal American Theresa Dolan COO Mount Sinai Care April 25, 2014 Overview of the ACO Beneficiary Assignment
The TeleHealth Model
 The Model CareCycle Solutions The Solution Calendar Year 2011 Company Overview CareCycle Solutions (CCS) specializes in managing the needs of chronically ill patients through the use of Interventional
The Model CareCycle Solutions The Solution Calendar Year 2011 Company Overview CareCycle Solutions (CCS) specializes in managing the needs of chronically ill patients through the use of Interventional
1. TITLE: Colin A. Banas MD, MSHA Chief Medical Information Officer Secondary Point of Contact: 804-827- 4196, [email protected]
 1. TITLE: Using Health Information Technology - CPOE to Advance Performance Improvement in Heart Failure Patients at Virginia Commonwealth University Health System 2. ORGANIZATION: Virginia Commonwealth
1. TITLE: Using Health Information Technology - CPOE to Advance Performance Improvement in Heart Failure Patients at Virginia Commonwealth University Health System 2. ORGANIZATION: Virginia Commonwealth
Interoperability and Analytics February 29, 2016
 Interoperability and Analytics February 29, 2016 Matthew Hoffman MD, CMIO Utah Health Information Network Conflict of Interest Matthew Hoffman, MD Has no real or apparent conflicts of interest to report.
Interoperability and Analytics February 29, 2016 Matthew Hoffman MD, CMIO Utah Health Information Network Conflict of Interest Matthew Hoffman, MD Has no real or apparent conflicts of interest to report.
If you are interested in learning more about the Practice Change Leaders for Aging and Health, you can find more information here.
 Amy Vandenbroucke, JD Associate Director Center for Ethics in Health Care Oregon Health & Science University 3181 SW Sam Jackson Park Road Portland, OR 97239 The following document is a business plan that
Amy Vandenbroucke, JD Associate Director Center for Ethics in Health Care Oregon Health & Science University 3181 SW Sam Jackson Park Road Portland, OR 97239 The following document is a business plan that
MD-REPORTS. Comprehensive, specialty specific one stop solution for Office, Ambulatory and Hospital electronic document requirements
 MD-REPORTS COMPLETE SOFTWARE SOLUTION FOR OFFICE, SURGERY CENTER AND HOSPITAL Comprehensive, specialty specific one stop solution for Office, Ambulatory and Hospital electronic document requirements ONC-ATCB
MD-REPORTS COMPLETE SOFTWARE SOLUTION FOR OFFICE, SURGERY CENTER AND HOSPITAL Comprehensive, specialty specific one stop solution for Office, Ambulatory and Hospital electronic document requirements ONC-ATCB
Five Myths Surrounding the Business of Population Health Management
 Five Myths Surrounding the Business of Population Health Management Joan Moss, RN, MSN Robert Sehring Chief Nursing Officer and Chief Ministry Services Officer, Senior Vice President, Sg2 OSF HealthCare
Five Myths Surrounding the Business of Population Health Management Joan Moss, RN, MSN Robert Sehring Chief Nursing Officer and Chief Ministry Services Officer, Senior Vice President, Sg2 OSF HealthCare
ACCOUNTABLE CARE ANALYTICS: DEVELOPING A TRUSTED 360 DEGREE VIEW OF THE PATIENT
 ACCOUNTABLE CARE ANALYTICS: DEVELOPING A TRUSTED 360 DEGREE VIEW OF THE PATIENT Accountable Care Analytics: Developing a Trusted 360 Degree View of the Patient Introduction Recent federal regulations have
ACCOUNTABLE CARE ANALYTICS: DEVELOPING A TRUSTED 360 DEGREE VIEW OF THE PATIENT Accountable Care Analytics: Developing a Trusted 360 Degree View of the Patient Introduction Recent federal regulations have
Main Section of the proposal: 1. Overall Aim & Objectives:
 Main Section of the proposal: 1. Overall Aim & Objectives: Over the past two decades Providence Health & Services has developed a comprehensive tobacco cessation program within our health system. The foundation
Main Section of the proposal: 1. Overall Aim & Objectives: Over the past two decades Providence Health & Services has developed a comprehensive tobacco cessation program within our health system. The foundation
How To Prepare For A Patient Care System
 Preparing for Online Communication with Your Patients A Guide for Providers This easy-to-use, time-saving guide is designed to help medical practices and community clinics prepare for communicating with
Preparing for Online Communication with Your Patients A Guide for Providers This easy-to-use, time-saving guide is designed to help medical practices and community clinics prepare for communicating with
PRODUCT OVERVIEW. Sunrise Revenue Cycle. It s all about Outcomes
 PRODUCT OVERVIEW Revenue Cycle It s all about Outcomes How can health systems maximize reimbursement and reduce inefficiencies in uncertain times? The key to successfully overcoming these challenges is
PRODUCT OVERVIEW Revenue Cycle It s all about Outcomes How can health systems maximize reimbursement and reduce inefficiencies in uncertain times? The key to successfully overcoming these challenges is
A Blueprint for Building a Medical Group s Internal Quality and Cost Efficiency Infrastructure
 + A Blueprint for Building a Medical Group s Internal Quality and Cost Efficiency Infrastructure + Disclosures: Timothy Harlan: I have no actual or potential conflict of interest in relation to this presentation.
+ A Blueprint for Building a Medical Group s Internal Quality and Cost Efficiency Infrastructure + Disclosures: Timothy Harlan: I have no actual or potential conflict of interest in relation to this presentation.
Clintegrity 360 QualityAnalytics
 WHITE PAPER Clintegrity 360 QualityAnalytics Bridging Clinical Documentation and Quality of Care HEALTHCARE EXECUTIVE SUMMARY The US Healthcare system is undergoing a gradual, but steady transformation.
WHITE PAPER Clintegrity 360 QualityAnalytics Bridging Clinical Documentation and Quality of Care HEALTHCARE EXECUTIVE SUMMARY The US Healthcare system is undergoing a gradual, but steady transformation.
Unity Point Health PROBLEM LISTS IN THE ELECTRONIC HEALTH RECORD
 Unity Point Health PROBLEM LISTS IN THE ELECTRONIC HEALTH RECORD Introduction The problem list is a critical part of electronic documentation and serves as a communication tool between all care providers.
Unity Point Health PROBLEM LISTS IN THE ELECTRONIC HEALTH RECORD Introduction The problem list is a critical part of electronic documentation and serves as a communication tool between all care providers.
The use of EHR data in quality improvement reports and clinical automatic calculators in ICU
 The use of EHR data in quality improvement reports and clinical automatic calculators in ICU Jun 2014 Vitaly Herasevich, MD, PhD, MSs Assistant Professor of Medicine and Anesthesiology, Department of Anesthesiology,
The use of EHR data in quality improvement reports and clinical automatic calculators in ICU Jun 2014 Vitaly Herasevich, MD, PhD, MSs Assistant Professor of Medicine and Anesthesiology, Department of Anesthesiology,
A predictive analytics platform powered by non-medical staff reduces cost of care among high-utilizing Medicare fee-for-service beneficiaries
 A predictive analytics platform powered by non-medical staff reduces cost of care among high-utilizing Medicare fee-for-service beneficiaries Munevar D 1, Drozd E 1, & Ostrovsky A 2 1 Avalere Health, Inc.
A predictive analytics platform powered by non-medical staff reduces cost of care among high-utilizing Medicare fee-for-service beneficiaries Munevar D 1, Drozd E 1, & Ostrovsky A 2 1 Avalere Health, Inc.
Population Health Management Helps Utica Park Clinic Ease the Transition to Value-Based Care
 CASE STUDY Utica Park Clinic Population Health Management Helps Utica Park Clinic Ease the Transition to Value-Based Care The transition from fee-for-service to value-based reimbursement has been a challenge
CASE STUDY Utica Park Clinic Population Health Management Helps Utica Park Clinic Ease the Transition to Value-Based Care The transition from fee-for-service to value-based reimbursement has been a challenge