Stuart Levine MD MHA Corporate Medical Director, HealthCare Partners Assistant Clinical Professor, Internal Medicine and Psychiatry, UCLA David
|
|
|
- Amberly Scott
- 7 years ago
- Views:
Transcription
1 Stuart Levine MD MHA Corporate Medical Director, HealthCare Partners Assistant Clinical Professor, Internal Medicine and Psychiatry, UCLA David Geffen School of Medicine 1

2 HealthCare Partners Delivery System Full Risk and Capitation Physician Owned Centrally coordinated Regionally Driven Strong Medical Management Infrastructure Robust Business support units Long-term Win-Win Hospital Relationships 2

3 HCP Approach to Patients Patient Centric- meet the needs of all patients Facilitate Access and Partnership with Patients and their families Not Benefit driven nor benefit demand mentality Right Care at the right time for the right medical situation Patient and Family Empowerment for their health Health Promotion, Education and Prevention Extensive Focus on Advanced Care Planning Build for the needs of Frail Seniors, Apply to All Patients 3

4 Technology to Improve Care Coordination Electronic Medical Records and TouchWorks/ NexGen & CCMIS/ CM Improved Communication Improved Documentation Protocol Driven Care ("Care Guides", embedded decision support tools) Disease Registry and Risk Stratification for Patients Patients for the Most Appropriate care Use of the Internet PiP Physician Portal and POP Patient Portal CME Patient and Family Access to Care and Education Use of Home Technology Home Monitoring of Patients Patient Education at Home Care Management Eyes and Ears 4

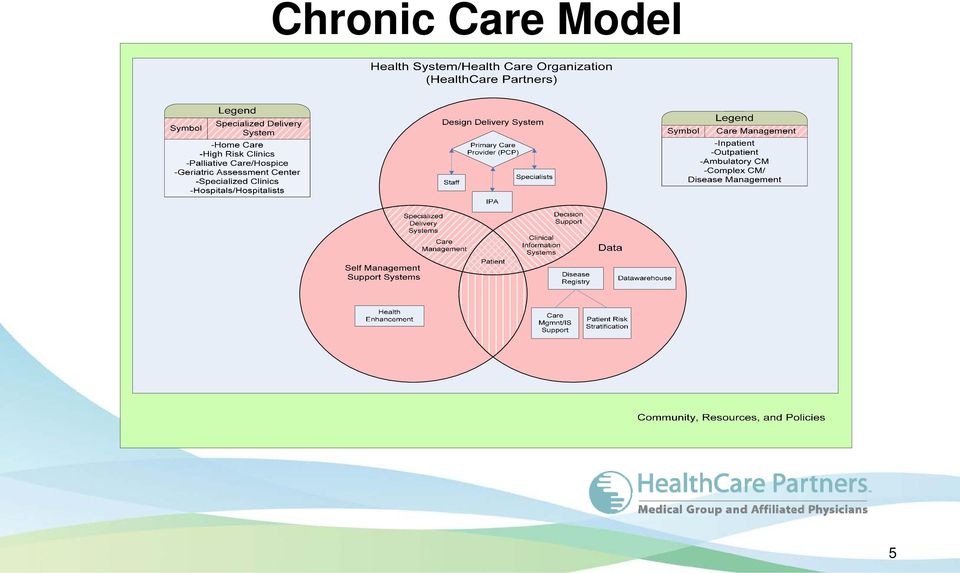
5 Chronic Care Model 5
6 EBM: Drives Chronic Care Model Outcomes Improvement 6

7 Stratifying Patients into the Appropriate Program Hospice/Palliative Care Home Care Management Provides in-home medical and palliative care management by Specialized Physicians, Nurse Care Managers and Social Workers for chronically frail seniors that have physical, mental, social and financial limitations that limits access to outpatient care, forcing unnecessary utilization of hospitals Level 4 Home Care Management $250 $260 High PMPM $220 $200 ESRD Medical Home High Risk Clinics and Care Management intensive one-on-one physician /nurse patient care and case management for the highest risk, most complex of the population. As the risk for hospitalization is reduced, patient is transferred to Level 2. Physicians and Care Managers are highly trained and closely Integrated into community resources and Physician offices or clinics. Level 3 High Risk Clinics $130 $140 Complex Care and Disease Management Provides long-term whole person care enhancement for the population using a multidisciplinary team approach. Diabetes, COPD, CHF, CKD, Depression, Dementia Self Management, PCP Provides self-management for people with chronic disease. Level 2 Complex Care and Disease Management Level 1 Self-Management & Health Education Programs 7 $ 50 $100 Low PMPM

8 Programs Overlap Health Support Care Support No or Low Claims Intense & Frequent Claims Risk Low High Outcome Healthy Lifestyle Issues Chronic Catastrophic Terminal Palliative Catastrophic Care Complex Care Management Disease Management Screening and Secondary Prevention Education and Information Sharing Health Promotion, Wellness, Primary Prevention Decision Support 8

9 Care Model HomeCare Palliative Care ESRD Dialysis Hospitalist Program/Urgent Care Comprehensive Care Center Primary Care SNF Program Complex Care Management CHF COPD DM CKD 9

10 How do all Programs fit together? Before Integrated HomeCare HomeCare High Risk ESRD High Risk ESRD 10

11 Target Patient Population Risk Stratified Patients HomeCare Graduates PCP/Specialist/CMCC Referrals Post-Discharge Patients (Hospital, ER, UC, SNF) Comprehensive Care Center 11

12 Hospitalist Program Admitted to Hospital Hospitalist lead and coordinate the patient s work-up and involve care manager and social worker in utilizing appropriate community resources Enter Emergency Department Admit Procedure Admitted to SNF SW and CM Intervene to address social and medical needs CM Team coordinates care with outpatient setting Discharged CM Team coordinates follow-up outpatient Care 12

13 Advanced Care Planning and Palliative Care Improve Competency in End of Life Management Focus on Goals of Care, Quality, & Dignity Complete an Advance Care Plan (Advance Directive & Medical Note) Patient s Values Treatment Options Expectations & Limits Communication End of Life Care Plan Patient s Clinical Condition Prognosis & Quality of Life 13

14 Future Innovations All of these innovations are planned and included for implementation for 2010 as a pilot in at least one region PACE Program Hospice Palliative Care Program Electronic Home Monitoring Care Transitions to Care Management Areas Application of Risk Stratification of Patients and appropriate targeting of patients with clinical innovations 14

Dual RFI Response Summary
 Dual RFI Response Summary Improving Care through Integrated Medicare and Medi- Cal Delivery Models Stuart Levine, MD., MHA. Keith Wilson, MD Robert Margolis, MD. Stakeholder Meeting August 30, 2011 1 Organization
Dual RFI Response Summary Improving Care through Integrated Medicare and Medi- Cal Delivery Models Stuart Levine, MD., MHA. Keith Wilson, MD Robert Margolis, MD. Stakeholder Meeting August 30, 2011 1 Organization
The Evolution of Managed Care as the Foundation for Health Reform ACO s as the Vehicle for Integration and Coordination of Care for All Patients
 The Evolution of Managed Care as the Foundation for Health Reform ACO s as the Vehicle for Integration and Coordination of Care for All Patients Stuart Levine MD MHA Corporate/ Regional Medical Dir., Asst.
The Evolution of Managed Care as the Foundation for Health Reform ACO s as the Vehicle for Integration and Coordination of Care for All Patients Stuart Levine MD MHA Corporate/ Regional Medical Dir., Asst.
Mission Every Day. Vision for the Future
 Our Vision for the Future We will be the role model for integrated and coordinated care, leading the transformation of the national healthcare delivery system to assure quality, access, and affordable
Our Vision for the Future We will be the role model for integrated and coordinated care, leading the transformation of the national healthcare delivery system to assure quality, access, and affordable
How Models Work: Care Coordination from an IT Perspective
 How Models Work: Care Coordination from an IT Perspective Steve Davis, DO Roberta Sniderman DISCLAIMER: The views and opinions expressed in this presentation are those of the author and do not necessarily
How Models Work: Care Coordination from an IT Perspective Steve Davis, DO Roberta Sniderman DISCLAIMER: The views and opinions expressed in this presentation are those of the author and do not necessarily
Game Changer at the Primary Care Practice Embedded Care Management. Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012
 Game Changer at the Primary Care Practice Embedded Care Management Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012 Objectives To describe the recent evolution of care management at
Game Changer at the Primary Care Practice Embedded Care Management Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012 Objectives To describe the recent evolution of care management at
Ann Hablitzel, RN, BSN, MBA Hospice Care of California
 Ann Hablitzel, RN, BSN, MBA Hospice Care of California Objectives Describe the creations of new community based palliative care programs Identify criteria for admission Discuss philosophy and goals Analyze
Ann Hablitzel, RN, BSN, MBA Hospice Care of California Objectives Describe the creations of new community based palliative care programs Identify criteria for admission Discuss philosophy and goals Analyze
Connect4 Patients CCCM Primary Care Community. Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM
 Connect4 Patients CCCM Primary Care Community Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM September 17, 2015 Objectives: Describe innovative care management
Connect4 Patients CCCM Primary Care Community Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM September 17, 2015 Objectives: Describe innovative care management
Building an Accountable Care Organization. Jean Malouin, MD MPH University of Michigan Health System September 21, 2012
 Building an Accountable Care Organization Jean Malouin, MD MPH University of Michigan Health System September 21, 2012 Agenda UMHS overview PGP demo ACO precursor Current efforts underway Role of primary
Building an Accountable Care Organization Jean Malouin, MD MPH University of Michigan Health System September 21, 2012 Agenda UMHS overview PGP demo ACO precursor Current efforts underway Role of primary
Patient to Person. Transitions of Care. Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM
 Patient to Person Transitions of Care Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM Transitions of Care Transitioning from school to adult services (vocational, medical day, etc.)
Patient to Person Transitions of Care Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM Transitions of Care Transitioning from school to adult services (vocational, medical day, etc.)
Finding Meaning and Purpose in Palliative Care
 Finding Meaning and Purpose in PALLIATIVE CARE WHAT IS IT? Jeffrey Rubins, MD Director, Palliative Medicine Hennepin Health Services deriv. from pallium, to cloak How do you pronounce palliative? medical
Finding Meaning and Purpose in PALLIATIVE CARE WHAT IS IT? Jeffrey Rubins, MD Director, Palliative Medicine Hennepin Health Services deriv. from pallium, to cloak How do you pronounce palliative? medical
Expanding the team to the health care community. One practice s experience Holly Cleney, MD
 Expanding the team to the health care community One practice s experience Holly Cleney, MD Objectives Develop a strategy for coordinating care effectively for patients across hospital stays and through
Expanding the team to the health care community One practice s experience Holly Cleney, MD Objectives Develop a strategy for coordinating care effectively for patients across hospital stays and through
5/13/2011. ACO Partnerships A Case Study. Contents: The Strategic Imperative for Accountable Care
 ACO Partnerships A Case Study Bob Edmondson, MPH Vice President, Innovation West Penn Allegheny Health System Pittsburgh, PA 1 Contents: 1. The Strategic Imperative for Accountable Care 2. Population Health
ACO Partnerships A Case Study Bob Edmondson, MPH Vice President, Innovation West Penn Allegheny Health System Pittsburgh, PA 1 Contents: 1. The Strategic Imperative for Accountable Care 2. Population Health
High Desert Medical Group Connections for Life Program Description
 High Desert Medical Group Connections for Life Program Description POLICY: High Desert Medical Group ("HDMG") promotes patient health and wellbeing by actively coordinating services for members with multiple
High Desert Medical Group Connections for Life Program Description POLICY: High Desert Medical Group ("HDMG") promotes patient health and wellbeing by actively coordinating services for members with multiple
Henry Ford Health System Care Coordination and Readmissions Update
 Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
Care Management Approach for People Who Are at High Risk
 Care Management Approach for People Who Are at High Risk Presented by: Ann Larsen RN, CDE Care Manger - Herefordshire Clinic/Trainer Care Management Plus June 11, 2013 Welcome! Type questions into the
Care Management Approach for People Who Are at High Risk Presented by: Ann Larsen RN, CDE Care Manger - Herefordshire Clinic/Trainer Care Management Plus June 11, 2013 Welcome! Type questions into the
Population Health Solutions for Employers MEDIA RESOURCES
 Population Health Solutions for Employers MEDIA RESOURCES ABOUT MISSIONPOINT MissionPoint s mission is to make healthcare more affordable, accessible and improve the quality of care for our members. MissionPoint
Population Health Solutions for Employers MEDIA RESOURCES ABOUT MISSIONPOINT MissionPoint s mission is to make healthcare more affordable, accessible and improve the quality of care for our members. MissionPoint
HealthCare Partners of Nevada. Heart Failure
 HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
Our Patient-Centered Medical Home a Process, not a Click
 Our Patient-Centered Medical Home a Process, not a Click Richard Johnston, M.D. President, Medical Clinic of North Texas, P.A. Medical Clinic of North Texas, P.A. MCNT Physician Owned Primary Care Medical
Our Patient-Centered Medical Home a Process, not a Click Richard Johnston, M.D. President, Medical Clinic of North Texas, P.A. Medical Clinic of North Texas, P.A. MCNT Physician Owned Primary Care Medical
May 9, 2013. FaithAnn Amond, RN Navigator Care Central Ellis Medicine
 A Systems Approach to Diabetes Care Hospital to Home. Improving Care Transitions and Outcomes Helen Hayes Hospital West Haverstraw, NY James Desemone, MD Director of Medical Staff Quality Diabetes and
A Systems Approach to Diabetes Care Hospital to Home. Improving Care Transitions and Outcomes Helen Hayes Hospital West Haverstraw, NY James Desemone, MD Director of Medical Staff Quality Diabetes and
Community Care of North Carolina. Statewide program for managing Carolina Access recipients
 Community Care of North Carolina Statewide program for managing Carolina Access recipients Key Goals Improve access to, quality of, and coordination of care for Carolina Access Medicaid patients. By doing
Community Care of North Carolina Statewide program for managing Carolina Access recipients Key Goals Improve access to, quality of, and coordination of care for Carolina Access Medicaid patients. By doing
V. Utilization Management (UM) Program
 Program") V. Utilization Management (UM) Program Overview Better Health Network s Utilization Management (UM) Program is designed to provide quality, cost-effective and medically necessary services while meeting
V. Utilization Management (UM) Program Overview Better Health Network s Utilization Management (UM) Program is designed to provide quality, cost-effective and medically necessary services while meeting
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS. Karen Unholz, RN, BSN
 INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
What is Palliative Care
 What is Palliative Care Maine Quality Counts Portland Regional Forum Isabella N. Stumpf, DO Division Director, Palliative Medicine, Maine Medical Center Medical Director, Palliative Care, MaineHealth Disclosure
What is Palliative Care Maine Quality Counts Portland Regional Forum Isabella N. Stumpf, DO Division Director, Palliative Medicine, Maine Medical Center Medical Director, Palliative Care, MaineHealth Disclosure
Patient Centered Medical Home: An Approach for the Health Plan
 : An Approach for the Health Plan By Marissa A. Harper and JoAnn E. Balara Excellence in healthcare consulting The Medical Home Concept Works Recent Medicare demonstration projects on Patient Centered
: An Approach for the Health Plan By Marissa A. Harper and JoAnn E. Balara Excellence in healthcare consulting The Medical Home Concept Works Recent Medicare demonstration projects on Patient Centered
3/11/15. COPD Disease Management Tackling the Transition. Objectives. Describe the multidisciplinary approach to inpatient care for COPD patients
 Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
KNOWLEDGEABLE SERVICE ROBOTS FOR AGING
 KNOWLEDGEABLE SERVICE ROBOTS FOR AGING Workshop on ICT and Robotics for Care and Service An advanced care system Hamburg December 2012 Dr. Hadas Lewy Maccabi Healthcare Services Maccabi Healthcare Services
KNOWLEDGEABLE SERVICE ROBOTS FOR AGING Workshop on ICT and Robotics for Care and Service An advanced care system Hamburg December 2012 Dr. Hadas Lewy Maccabi Healthcare Services Maccabi Healthcare Services
The Wyoming Pay for Participation Program for Medicaid Health Management
 The Wyoming Pay for Participation Program for Medicaid Health Management 2010 Medicaid Congress James Bush, M.D. State Medicaid Medical Officer Wyoming Department of Health Wyoming Medicaid- EqualityCare
The Wyoming Pay for Participation Program for Medicaid Health Management 2010 Medicaid Congress James Bush, M.D. State Medicaid Medical Officer Wyoming Department of Health Wyoming Medicaid- EqualityCare
Contact: Jessica Lorenzo, M.P.H., Senior Project Manager. E-mail: Jessica.Lorenzo@mountsinai.org
 Mount Sinai School of Medicine: Improving Access to High Quality Asthma Care in East Harlem Grant Results Report October 2008 BACKGROUND INFORMATION Mount Sinai School of Medicine Division of General Internal
Mount Sinai School of Medicine: Improving Access to High Quality Asthma Care in East Harlem Grant Results Report October 2008 BACKGROUND INFORMATION Mount Sinai School of Medicine Division of General Internal
Population Health Management Innovation Payer and Provider Collaboration. Population Health Management Innovation Payer and Provider Collaboration
 Population Health Management Innovation Payer and Provider Collaboration Population Health Management Innovation Payer and Provider Collaboration Agenda Strategic Context Population Health Journey Key
Population Health Management Innovation Payer and Provider Collaboration Population Health Management Innovation Payer and Provider Collaboration Agenda Strategic Context Population Health Journey Key
Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights
 Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights Emily Brower Executive Director Accountable Care Programs Emily_Brower@AtriusHealth.org November 2013 1 Contents Overview of
Atrius Health Pioneer ACO: First Year Accomplishments, Results and Insights Emily Brower Executive Director Accountable Care Programs Emily_Brower@AtriusHealth.org November 2013 1 Contents Overview of
Care Management Resource Guide for Tufts Health Plan Medicare Preferred
 Care Management Resource Guide for Tufts Health Plan Medicare Preferred March 2016 DMS# 2158556, Rev. 4 Copyright 2015 by Tufts Associated Health Plans, Inc. All rights reserved. No part of this document
Care Management Resource Guide for Tufts Health Plan Medicare Preferred March 2016 DMS# 2158556, Rev. 4 Copyright 2015 by Tufts Associated Health Plans, Inc. All rights reserved. No part of this document
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System
 Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Commercial ACOs: Trials and Tribulations
 Commercial ACOs: Trials and Tribulations June 12, 2015 Agenda: John Jenrette, MD, CEO, Sharp Community Medical Group Moderator Nancy Greenstreet, MD, Medical Director, Physicians Medical Group of Santa
Commercial ACOs: Trials and Tribulations June 12, 2015 Agenda: John Jenrette, MD, CEO, Sharp Community Medical Group Moderator Nancy Greenstreet, MD, Medical Director, Physicians Medical Group of Santa
08/04/2014. Tim Hogan, RRT, PhD Primary Care Home Health Director. University of Missouri Health Care Department of Family and Community Medicine
 Tim Hogan, RRT, PhD, Primary Care Home Health Director Joan Asbee, RN, BSN, CWOCN, Nurse Care Manager Karli Urban, MD, Assistant Professor of Clinical Family and Community Medicine University of Missouri
Tim Hogan, RRT, PhD, Primary Care Home Health Director Joan Asbee, RN, BSN, CWOCN, Nurse Care Manager Karli Urban, MD, Assistant Professor of Clinical Family and Community Medicine University of Missouri
Service Inventory of Managed Care Entities to Support Development of a Health Homes State Plan Amendment
 Service Inventory of Managed Care Entities to Support Development of a Health Homes State Plan Amendment March 2012 MassHealth Managed Care Entities (MCO, SCO, PACE) Health Homes Inventory to Support State
Service Inventory of Managed Care Entities to Support Development of a Health Homes State Plan Amendment March 2012 MassHealth Managed Care Entities (MCO, SCO, PACE) Health Homes Inventory to Support State
Population Health Management: Banner Health Network s Perspective. Neta Faynboym, Medical Director Banner Health Network
 Population Health Management: Banner Health Network s Perspective Neta Faynboym, Medical Director Banner Health Network 29 Acute Care Hospitals BANNER AT A GLANCE Banner Health Network with 400K lives
Population Health Management: Banner Health Network s Perspective Neta Faynboym, Medical Director Banner Health Network 29 Acute Care Hospitals BANNER AT A GLANCE Banner Health Network with 400K lives
Health Care Leader Action Guide to Reduce Avoidable Readmissions
 Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
PAYMENT INNOVATIONS SUPPORTING BEHAVIORAL HEALTHCARE DELIVERY IMPROVEMENT. NGA July 2015
 PAYMENT INNOVATIONS SUPPORTING BEHAVIORAL HEALTHCARE DELIVERY IMPROVEMENT NGA July 2015 My Background Medicaid Director Previously DMH Medical Director 20 years Practicing Psychiatrist CMHCs 10 years FQHC
PAYMENT INNOVATIONS SUPPORTING BEHAVIORAL HEALTHCARE DELIVERY IMPROVEMENT NGA July 2015 My Background Medicaid Director Previously DMH Medical Director 20 years Practicing Psychiatrist CMHCs 10 years FQHC
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home
 RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
Introduction to the GLPTN Program. Provider Office & Physician Organization Briefing
 Introduction to the GLPTN Program Provider Office & Physician Organization Briefing What is the GLPTN? The GLPTN is one of 29 Practice Transformation Networks (PTNs) funded under the brand new CMS Transforming
Introduction to the GLPTN Program Provider Office & Physician Organization Briefing What is the GLPTN? The GLPTN is one of 29 Practice Transformation Networks (PTNs) funded under the brand new CMS Transforming
1. Executive Summary Problem/Opportunity: Evidence: Baseline Data: Intervention: Results:
 A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
Transforming traditional case management through local provider partnerships
 Transforming traditional case management through local provider partnerships Introduction The dramatic changes sweeping the health care industry are driving a strong interest in engaging patients at the
Transforming traditional case management through local provider partnerships Introduction The dramatic changes sweeping the health care industry are driving a strong interest in engaging patients at the
Care Transitions. Provide Your Patients with Effective Transitional Care Without Changing Your Operating Model. Share This
 Care Transitions Provide Your Patients with Effective Transitional Care Without Changing Your Operating Model Brought to you by Amedisys: Architects of a leading patient-centered Care Transitions network.
Care Transitions Provide Your Patients with Effective Transitional Care Without Changing Your Operating Model Brought to you by Amedisys: Architects of a leading patient-centered Care Transitions network.
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates
 Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Idaho Health Home State Plan Amendment Matrix: Summary Overview. Overview of Approved Health Home SPAs
 Idaho Health Home State Plan Amendment Matrix: Summary Overview This matrix outlines key program design features from health home State Plan Amendments (SPAs) approved by the Centers for Medicare & Medicaid
Idaho Health Home State Plan Amendment Matrix: Summary Overview This matrix outlines key program design features from health home State Plan Amendments (SPAs) approved by the Centers for Medicare & Medicaid
Enabling Healthcare in Out-Patient Settings and The Patient Centered Medical Home of the Future
 Enabling Healthcare in Out-Patient Settings and The Patient Centered Medical Home of the Future Gregory J. Raglow, MD, FAAFP Group Health Informatics Officer Abu Dhabi Health Services SEHA Objectives List
Enabling Healthcare in Out-Patient Settings and The Patient Centered Medical Home of the Future Gregory J. Raglow, MD, FAAFP Group Health Informatics Officer Abu Dhabi Health Services SEHA Objectives List
Home Health Care Today: Higher Acuity Level of Patients Highly skilled Professionals Costeffective Uses of Technology Innovative Care Techniques
 Comprehensive EHR Infrastructure Across the Health Care System The goal of the Administration and the Department of Health and Human Services to achieve an infrastructure for interoperable electronic health
Comprehensive EHR Infrastructure Across the Health Care System The goal of the Administration and the Department of Health and Human Services to achieve an infrastructure for interoperable electronic health
It Takes Two to ACO A Unique Management Partnership
 AMGA 2014 Annual Conference, April 4, 2014 It Takes Two to ACO A Unique Management Partnership Scott Hayworth MD, President & CEO Mount Kisco Medical Group Alan Bernstein MD, Senior Medical Director Mount
AMGA 2014 Annual Conference, April 4, 2014 It Takes Two to ACO A Unique Management Partnership Scott Hayworth MD, President & CEO Mount Kisco Medical Group Alan Bernstein MD, Senior Medical Director Mount
Continuity of Care Guide for Ambulatory Medical Practices
 Continuity of Care Guide for Ambulatory Medical Practices www.himss.org t ra n sf o r m i ng he a lth c a re th rou g h IT TM Table of Contents Introduction 3 Roles and Responsibilities 4 List of work/responsibilities
Continuity of Care Guide for Ambulatory Medical Practices www.himss.org t ra n sf o r m i ng he a lth c a re th rou g h IT TM Table of Contents Introduction 3 Roles and Responsibilities 4 List of work/responsibilities
Kick off Meeting November 11 13, 2015. MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF)
") Kick off Meeting November 11 13, 2015 MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF) Team Composition Justin Huynh, MD Internal Medicine, Physician Champion Mary Laubinger,
Kick off Meeting November 11 13, 2015 MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF) Team Composition Justin Huynh, MD Internal Medicine, Physician Champion Mary Laubinger,
New Models of Care and Approaches to Payment
 New Models of Care and Approaches to Payment Richard Lopez, MD Chief Medical Officer Richard_Lopez@AtriusHealth.org September 30, 2014 Atrius Health Non-profit alliance of six leading independent medical
New Models of Care and Approaches to Payment Richard Lopez, MD Chief Medical Officer Richard_Lopez@AtriusHealth.org September 30, 2014 Atrius Health Non-profit alliance of six leading independent medical
With New Models of Value-Based Care. September 1, 2015
 With New Models of Value-Based Care September 1, 2015 Using Community Care Coordination and Mobile Technology to Impact Health Outcomes and Reduce Avoidable Hospital Encounters Presenters: Chris Parsons,
With New Models of Value-Based Care September 1, 2015 Using Community Care Coordination and Mobile Technology to Impact Health Outcomes and Reduce Avoidable Hospital Encounters Presenters: Chris Parsons,
Discharge Planning. Home Care 1. Objectives. Where are they Going?
 Discharge Planning Heidi White, MD Associate Professor of Medicine Yvonne Spurney, RN Associate Chief Nurse Cristina C. Hendrix, DNS, GNP-BC Associate Professor of Nursing Objectives Describe challenges
Discharge Planning Heidi White, MD Associate Professor of Medicine Yvonne Spurney, RN Associate Chief Nurse Cristina C. Hendrix, DNS, GNP-BC Associate Professor of Nursing Objectives Describe challenges
The ROI of Palliative Care. James Mittelberger, MD MPH March 22, 2104
 The ROI of Palliative Care James Mittelberger, MD MPH March 22, 2104 Provide the evidence and tools to develop the most effective palliative care program possible Purpose Palliative Care Financial Return
The ROI of Palliative Care James Mittelberger, MD MPH March 22, 2104 Provide the evidence and tools to develop the most effective palliative care program possible Purpose Palliative Care Financial Return
#Aim2Innovate. Share session insights and questions socially. UCLA Primary Care Innovation Model 6/13/2015. Mark S. Grossman, MD, MBA, FAAP, FACP
 UCLA Primary Care Innovation Model Mark S. Grossman, MD, MBA, FAAP, FACP Chief Medical Office, UCLA Community Physicians & Specialty Care Networks June 16, 2015 DISCLAIMER: The views and opinions expressed
UCLA Primary Care Innovation Model Mark S. Grossman, MD, MBA, FAAP, FACP Chief Medical Office, UCLA Community Physicians & Specialty Care Networks June 16, 2015 DISCLAIMER: The views and opinions expressed
Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination of care for both services.
 Domain 3 Projects 3.a.i Integration of Primary Care and Behavioral Health Services Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination
Domain 3 Projects 3.a.i Integration of Primary Care and Behavioral Health Services Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination
MedStar Family Choice (MFC) Case Management Program. Cyd Campbell, MD, FAAP Medical Director, MFC MCAC June 24, 2015
 Case Management Program. Cyd Campbell, MD, FAAP Medical Director, MFC MCAC June 24, 2015") MedStar Family Choice (MFC) Case Management Program Cyd Campbell, MD, FAAP Medical Director, MFC MCAC June 24, 2015 Case Management Program Presentation Overview CM Programs Disease Management Complex
MedStar Family Choice (MFC) Case Management Program Cyd Campbell, MD, FAAP Medical Director, MFC MCAC June 24, 2015 Case Management Program Presentation Overview CM Programs Disease Management Complex
NYSPFP Preventable Readmissions Initiative: Pilot Review and Post Hospital Care
 NYSPFP Preventable Readmissions Initiative: Pilot Review and Post Hospital Care June 17, 2014 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association
NYSPFP Preventable Readmissions Initiative: Pilot Review and Post Hospital Care June 17, 2014 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association
Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions
 Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions Leslie Becker RN, BS Jennifer Smith RN, MSN, MBA Leslie Frain MSN, RN Jan Machanis
Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions Leslie Becker RN, BS Jennifer Smith RN, MSN, MBA Leslie Frain MSN, RN Jan Machanis
Reinsurance for Early Retirees Program
 Summary of Programs Disease Management CareFirst's approach to disease management seeks better management of members diagnosed with certain high frequency, high cost diseases through the early detection
Summary of Programs Disease Management CareFirst's approach to disease management seeks better management of members diagnosed with certain high frequency, high cost diseases through the early detection
Call-A-Nurse Location
 Call-A-Nurse A 24-hour medical call center, specializing in registered nurse telephone triage, answering service, physician and service referral, and class registration. Call-A-Nurse Location Call-A-Nurse
Call-A-Nurse A 24-hour medical call center, specializing in registered nurse telephone triage, answering service, physician and service referral, and class registration. Call-A-Nurse Location Call-A-Nurse
Modern care management
 The care management challenge Health plans and care providers spend billions of dollars annually on care management with the expectation of better utilization management and cost control. That expectation
The care management challenge Health plans and care providers spend billions of dollars annually on care management with the expectation of better utilization management and cost control. That expectation
Personal Health Systems and COPD how to integrate into routine health delivery?
 Personal Health Systems and COPD how to integrate into routine health delivery? From HealthCare to Health Promotion Josep Roca Hospital Clinic.IDIBAPS.University of Barcelona HIGHLIGHTS CHALLENGE OF CHRONIC
Personal Health Systems and COPD how to integrate into routine health delivery? From HealthCare to Health Promotion Josep Roca Hospital Clinic.IDIBAPS.University of Barcelona HIGHLIGHTS CHALLENGE OF CHRONIC
MERCY-CR/UI HEALTH CARE ACCOUNTABLE CARE ORGANIZATION Dan Fick, M.D. Timothy Quinn, M.D.
 MERCY-CR/UI HEALTH CARE ACCOUNTABLE CARE ORGANIZATION Dan Fick, M.D. Timothy Quinn, M.D. November, 2012 Accountable Care Organization An ACO is a group of health care providers who agree to take on a shared
MERCY-CR/UI HEALTH CARE ACCOUNTABLE CARE ORGANIZATION Dan Fick, M.D. Timothy Quinn, M.D. November, 2012 Accountable Care Organization An ACO is a group of health care providers who agree to take on a shared
American Diabetes Association Education Recognition Program Overview
 American Diabetes Association Education Recognition Program Overview A brief history of the National Standards for Diabetes Self-Management Education and Support and a walk through the 10 DSME/S standards
American Diabetes Association Education Recognition Program Overview A brief history of the National Standards for Diabetes Self-Management Education and Support and a walk through the 10 DSME/S standards
The Medical Home. The Triple Aim Institute for Healthcare Improvement. Compiled by: Douglas Eby MD MPH CPE Workgroup Coordinator
 The Medical Home The Triple Aim Institute for Healthcare Improvement April 16, 2009 Compiled by: Douglas Eby MD MPH CPE Workgroup Coordinator IHI Medical Home Work Group Medical Home IHI Triple Aim Page
The Medical Home The Triple Aim Institute for Healthcare Improvement April 16, 2009 Compiled by: Douglas Eby MD MPH CPE Workgroup Coordinator IHI Medical Home Work Group Medical Home IHI Triple Aim Page
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment
 Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
Collaborating for care: Embedded case managers, extending care management value
 Collaborating for care: Embedded case managers, extending care management value Randall Krakauer, MD, FACP, FACR Vice President, National Medical Director Medicare Strategy, AETNA Patrice Sminkey Chief
Collaborating for care: Embedded case managers, extending care management value Randall Krakauer, MD, FACP, FACR Vice President, National Medical Director Medicare Strategy, AETNA Patrice Sminkey Chief
Pushing the Envelope of Population Health
 Pushing the Envelope of Population Health Timothy Ferris, MD, MPH Senior Vice President, Population Health Management, Partners HealthCare May 15, 2014 DISCLAIMER: The views and opinions expressed in this
Pushing the Envelope of Population Health Timothy Ferris, MD, MPH Senior Vice President, Population Health Management, Partners HealthCare May 15, 2014 DISCLAIMER: The views and opinions expressed in this
Service delivery interventions
 Service delivery interventions S A S H A S H E P P E R D D E P A R T M E N T O F P U B L I C H E A L T H, U N I V E R S I T Y O F O X F O R D CO- C O O R D I N A T I N G E D I T O R C O C H R A N E E P
Service delivery interventions S A S H A S H E P P E R D D E P A R T M E N T O F P U B L I C H E A L T H, U N I V E R S I T Y O F O X F O R D CO- C O O R D I N A T I N G E D I T O R C O C H R A N E E P
Care Management: Reducing Risks. Project ECHO Consultation. Amy J. Khan, MD, MPH. Mia McCallum-Crawford, RN
 Care Management: Improving Health & Reducing Risks Project ECHO Consultation February 19, 2015 Amy J. Khan, MD, MPH Lisa Moreno, RN Mia McCallum-Crawford, RN Objectives 1. Consider patient factors and
Care Management: Improving Health & Reducing Risks Project ECHO Consultation February 19, 2015 Amy J. Khan, MD, MPH Lisa Moreno, RN Mia McCallum-Crawford, RN Objectives 1. Consider patient factors and
Palliative Medicine and The Nurse Practitioner
 Palliative Medicine and The Nurse Practitioner ANNE MOORE, FNP-C CONTACT INFO: JEWISH HOME CENTER FOR PALLIATIVE MEDICINE A PROGRAM OF SKIRBALL HOSPICE AND THE LOS ANGELES JEWISH HOME 6345 BALBOA BLVD.
Palliative Medicine and The Nurse Practitioner ANNE MOORE, FNP-C CONTACT INFO: JEWISH HOME CENTER FOR PALLIATIVE MEDICINE A PROGRAM OF SKIRBALL HOSPICE AND THE LOS ANGELES JEWISH HOME 6345 BALBOA BLVD.
WellSpan Health Care Management Strategy. October, 2013
 WellSpan Health Care Management Strategy October, 2013 We will realize a fundamental, yet gradual, shift in how we deliver and receive payment for care From: A system that treats people mostly when they
WellSpan Health Care Management Strategy October, 2013 We will realize a fundamental, yet gradual, shift in how we deliver and receive payment for care From: A system that treats people mostly when they
DELIVERING VALUE THROUGH TECHNOLOGY
 DELIVERING VALUE THROUGH TECHNOLOGY Mark Nelson, MD - EMR Physician Champion Krishna Ramachandran - Chief Information and Transformation Officer Karen Adamson - Director, Epic Clinical Applications DuPage
DELIVERING VALUE THROUGH TECHNOLOGY Mark Nelson, MD - EMR Physician Champion Krishna Ramachandran - Chief Information and Transformation Officer Karen Adamson - Director, Epic Clinical Applications DuPage
Effective Partners: Home Health s Role in Chronic Care Management
 Effective Partners: Home Health s Role in Chronic Care Management Abstract Today, seven out of 10 Americans die each year from chronic disease and, in Pennsylvania, more than 60 percent of the population
Effective Partners: Home Health s Role in Chronic Care Management Abstract Today, seven out of 10 Americans die each year from chronic disease and, in Pennsylvania, more than 60 percent of the population
Member name, address, phone number, DOB, MC400 Member ID, MA Recipient Number
 CONNECTED CARE DATA TEMPLATE Member Tier Display SMI Tier 1, 2, or 3 (plus historical activity to show changes in tier) Member Demographics Member name, address, phone number, DOB, MC400 Member ID, MA
CONNECTED CARE DATA TEMPLATE Member Tier Display SMI Tier 1, 2, or 3 (plus historical activity to show changes in tier) Member Demographics Member name, address, phone number, DOB, MC400 Member ID, MA
Integrated Healthcare Management (IHM) Overview
 Overview") Integrated Healthcare Management (IHM) Overview MCO Case Management Presentations MCAC on June 24, 2015 Karen Dale, Market President Pillars of Our Strategy Care Management Care Coordination Care Customization
Integrated Healthcare Management (IHM) Overview MCO Case Management Presentations MCAC on June 24, 2015 Karen Dale, Market President Pillars of Our Strategy Care Management Care Coordination Care Customization
Post-Acute Care Transitions: An Essential Component of Accountable Care
 : An Essential Component of Accountable Care Bruce C. Smith, MD, FACP Associate Medical Director, Strategy Deployment Group Health Physicians, Seattle, WA Smith.bc@ghc.org AMGA 2012 Institute for Quality
: An Essential Component of Accountable Care Bruce C. Smith, MD, FACP Associate Medical Director, Strategy Deployment Group Health Physicians, Seattle, WA Smith.bc@ghc.org AMGA 2012 Institute for Quality
Population Health, DSRIP and the role of Case Management/Care Coordination
 Population Health, DSRIP and the role of Case Management/Care Coordination CMSA Long Island September 9, 2015 Joseph Lamantia Chief of Operations for Population Health Stony Brook Medicine A Century of
Population Health, DSRIP and the role of Case Management/Care Coordination CMSA Long Island September 9, 2015 Joseph Lamantia Chief of Operations for Population Health Stony Brook Medicine A Century of
Healthy Solutions for Life
 Healthy Solutions for Life 2015 Presentation Overview About Healthy Solutions for Life Disease Management Health Coaching Model DM Programs TeleCare Monitoring 2013 Nurtur Health, Inc. All Rights Reserved.
Healthy Solutions for Life 2015 Presentation Overview About Healthy Solutions for Life Disease Management Health Coaching Model DM Programs TeleCare Monitoring 2013 Nurtur Health, Inc. All Rights Reserved.
Diabetes Care 2011-2012
 Clinical Innovations in the Patient Centered Medical Home to Improve Diabetes Care Robert A. Gabbay, MD, PhD, FACP Chief Medical Officer & Senior Vice President Joslin Diabetes Center Harvard Medical School
Clinical Innovations in the Patient Centered Medical Home to Improve Diabetes Care Robert A. Gabbay, MD, PhD, FACP Chief Medical Officer & Senior Vice President Joslin Diabetes Center Harvard Medical School
For the Record: The Truth About Electronic Charting in Home Care
 For the Record: The Truth About Electronic Charting in Home Care Athena Lu Kreiser, MHA Senior Project Manager Jewish Home Lifecare akreiser@jhha.org Healthcare Unbound June 23, 2009 Seattle, WA Jewish
For the Record: The Truth About Electronic Charting in Home Care Athena Lu Kreiser, MHA Senior Project Manager Jewish Home Lifecare akreiser@jhha.org Healthcare Unbound June 23, 2009 Seattle, WA Jewish
Advanced Models of Primary Care: Care Management Plus pilot and dissemination
 Advanced Models of Primary Care: Care Management Plus pilot and dissemination Presented by David A. Dorr, MD, MS; Oregon Health & Science University, dorrd@ohsu.edu Funded by The John A. Hartford Foundation,
Advanced Models of Primary Care: Care Management Plus pilot and dissemination Presented by David A. Dorr, MD, MS; Oregon Health & Science University, dorrd@ohsu.edu Funded by The John A. Hartford Foundation,
DSRIP Domain 2-4 Projects for FQHCs
 In this document, CHCANYS presents information on select DSRIP projects from Domains 2, 3, and 4. These are projects that FQHCs should or could play a leadership or central role in designing and implementing.
In this document, CHCANYS presents information on select DSRIP projects from Domains 2, 3, and 4. These are projects that FQHCs should or could play a leadership or central role in designing and implementing.
Care Coordination. The Embedded Care Manager. Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed
 Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases
 Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases Epidemiology Over 145 million people ( nearly half the population) - suffer from asthma, depression and other chronic
Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases Epidemiology Over 145 million people ( nearly half the population) - suffer from asthma, depression and other chronic
Realizing the Potential: Improving Population Health in Accountable Care. Healthcare in Transition: Current Trends
 Realizing the Potential: Improving Population Health in Accountable Care - ACOs - Another Passing Fad or Built to Last? - Jerry Vaccaro, MD President & CEO, APS Healthcare Richard Chung, MD Chief Clinical
Realizing the Potential: Improving Population Health in Accountable Care - ACOs - Another Passing Fad or Built to Last? - Jerry Vaccaro, MD President & CEO, APS Healthcare Richard Chung, MD Chief Clinical
Strategic Hospital Transformation Plan. Executive Summary
 Executive Summary Strategic Hospital Transformation Plan University of Maryland Upper Chesapeake Health (UMUCH) is actively building a system of care to address the needs of the residents of Harford County
Executive Summary Strategic Hospital Transformation Plan University of Maryland Upper Chesapeake Health (UMUCH) is actively building a system of care to address the needs of the residents of Harford County
GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services
 GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services Aged, Blind and Disabled Stakeholder Presentation Indiana Family and Social Services Administration August
GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services Aged, Blind and Disabled Stakeholder Presentation Indiana Family and Social Services Administration August
Assessing Risk of Readmission. NoCVA Preventing Avoidable Readmission Collaborative Laura Maynard, MDiv, NCQC Amanda Hobbs, NCQC July 31, 2013
 Assessing Risk of Readmission NoCVA Preventing Avoidable Readmission Collaborative Laura Maynard, MDiv, NCQC Amanda Hobbs, NCQC July 31, 2013 Collaborative Goals Reduce readmission rates by 20% Increase
Assessing Risk of Readmission NoCVA Preventing Avoidable Readmission Collaborative Laura Maynard, MDiv, NCQC Amanda Hobbs, NCQC July 31, 2013 Collaborative Goals Reduce readmission rates by 20% Increase
5/10/13 HEALTH CARE REFORM LONGITUDINAL CARE COORDINATION HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO WHY WHAT HOW WHEN WHO
 TRANSITION CARE TRANSITION CARE WHY WHAT HOW WHEN WHO HEALTH CARE REFORM HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO Cost/Quality equation Higher cost care has not/does not equate with higher
TRANSITION CARE TRANSITION CARE WHY WHAT HOW WHEN WHO HEALTH CARE REFORM HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO Cost/Quality equation Higher cost care has not/does not equate with higher
MaineCare Value Based Purchasing Initiative
 MaineCare Value Based Purchasing Initiative The Accountable Communities Strategy Jim Leonard, Deputy Director, MaineCare Peter Kraut, Acting Accountable Communities Program Manager Why Value-Based Purchasing
MaineCare Value Based Purchasing Initiative The Accountable Communities Strategy Jim Leonard, Deputy Director, MaineCare Peter Kraut, Acting Accountable Communities Program Manager Why Value-Based Purchasing
Integrating Data to Support Care Management Transformation
 Integrating Data to Support Care Management Transformation The Washington State Experience David Mancuso, PhD Director, Research and Data Analysis Division Washington State Department of Social and Health
Integrating Data to Support Care Management Transformation The Washington State Experience David Mancuso, PhD Director, Research and Data Analysis Division Washington State Department of Social and Health
Special Needs Plan Model of Care 101
 Special Needs Plan Model of Care 101 What is a Special Needs Plan? First of all it s a Medicare MA-PD, typically an HMO Consists of Medicare enrollees who meet special eligibility requirements In our case
Special Needs Plan Model of Care 101 What is a Special Needs Plan? First of all it s a Medicare MA-PD, typically an HMO Consists of Medicare enrollees who meet special eligibility requirements In our case
David Eubanks, RN, MSN Billie Papasifakis, RN-BC, MSN, AACC. Describe model of care most appropriate
 THE BRIDGE PROGRAM David Eubanks, RN, MSN Billie Papasifakis, RN-BC, MSN, AACC Pamela Teenier, RN, MBA, COC-C, C HCS-D HCSD 1 Objectives Describe model of care most appropriate for a Bridge program from
THE BRIDGE PROGRAM David Eubanks, RN, MSN Billie Papasifakis, RN-BC, MSN, AACC Pamela Teenier, RN, MBA, COC-C, C HCS-D HCSD 1 Objectives Describe model of care most appropriate for a Bridge program from
Learning Collaborative
 Care Transitions Intervention Model to Reduce 30-Day Readmissions for Chronic Cardiac Conditions Learning Collaborative Dr. Norma Jean-Francois, DNP, APN-C Dr. Mary Anne Marra, DNP, MSN, RN, NEA-BC 1 OVERVIEW
Care Transitions Intervention Model to Reduce 30-Day Readmissions for Chronic Cardiac Conditions Learning Collaborative Dr. Norma Jean-Francois, DNP, APN-C Dr. Mary Anne Marra, DNP, MSN, RN, NEA-BC 1 OVERVIEW
UCare provides case management for all UCare members not affiliated with one of the above listed care systems. 2011 UCare for Seniors
 Case Requirements Updated 3/16/2011 According to the Case Society of America (CMSA), Case Model Act of 2009, Case management is a collaborative process of assessment, planning, facilitation, care coordination,
Case Requirements Updated 3/16/2011 According to the Case Society of America (CMSA), Case Model Act of 2009, Case management is a collaborative process of assessment, planning, facilitation, care coordination,
Practice Redesign for Dementia: The UCLA Alzheimer's and Dementia Care Program
 Practice Redesign for Dementia: The UCLA Alzheimer's and Dementia Care Program Zaldy S. Tan, MD, MPH Medical Director, UCLA Alzheimer s and Dementia Care Program Director, California Geriatric Education
Practice Redesign for Dementia: The UCLA Alzheimer's and Dementia Care Program Zaldy S. Tan, MD, MPH Medical Director, UCLA Alzheimer s and Dementia Care Program Director, California Geriatric Education
Care Network of East Alabama, Inc.
 Care Network of East Alabama, Inc. Established in 2011 as a not-for-profit organization to promote the medical home and to address the needs of Patient 1st patients in east Alabama Timeline December 2010
Care Network of East Alabama, Inc. Established in 2011 as a not-for-profit organization to promote the medical home and to address the needs of Patient 1st patients in east Alabama Timeline December 2010