Essentia Health. Heart Failure and Remote Monitoring. Denise Buxbaum, RN, BSN, CHFN Heart Failure Program Manager
|
|
|
- Julie Phillips
- 8 years ago
- Views:
Transcription
1 Essentia Health Heart Failure and Remote Monitoring Denise Buxbaum, RN, BSN, CHFN Heart Failure Program Manager

2 Essentia Health Oct 2014 No reproduction without permission

3 Why Heart Failure? Prevalence Affects 5.8 million in the U.S. Over 650,000 new patients annually The lifetime risk of developing HF is 20% for Americans 40 years of age. HF is the most frequent cause of hospitalization in elderly (> 65 y/o) Prognosis 1/2 of people who develop HF die within 5 years of their diagnosis Less than 25% are alive at 10 years
 Prognosis 1/2 of")
4 Heart Failure Progression is Inevitable Population of the US is aging Survival rates has improved HF is not always treated correctly Patients do not adhere to diet and medication regime Projections show the prevalence of HF will increase 46% from 2012 to 2030, resulting in >8 million people 18 years of age with HF AHA Heart Disease & Stroke Statistics 2014 Update

5 Conventional HF Care Nurtures a Cycle of Acute Care Dependency Failure to recognize early symptoms, neglects to seek timely help Clinic Management outside of HF clinic maybe be incomplete relative to HF patients complex needs Hospital stay may not be sufficient to find best medical regimen & educate patient. Lack of preparedness increases odds of early readmission. Hospital Patient decompensates and requires hospitalization


6 Interesting Comparisons Deaths per year Research Dollars in Millions Heart Failure Lung Cancer Breast Cancer Heart Failure Lung Cancer Breast Cancer HF: 282,800 deaths/year Lung Cancer : 64,475 Breast Cancer: 41,737 HF: $28.7 million Lung Cancer : $285 million Breast Cancer: $559 million

7 What will it Cost? Estimated lifetime cost per each individual HF patient is $110,000/year In 2012, total cost for HF was estimated to be $30.7 million Projections show that by 2030, the total cost of HF will increase almost 127% to $69.7 billion from 2012

8 Current Fee for Service world More we do, the more we are paid

9 We like our patients sick! Sicker the patients more tests, ER visits, surgeries, admissions, readmissions. $$$$$

10 So What? Why do we have to change We re happy just the way it is. Well times are a changing!

11 Essentia Health as an ACO One of six health care systems in Country to achieve: NCQA Accreditation as an Accountable Care Organization Definition A provider-based organization that take responsibility for meeting the health care needs of a defined population with the goal of simultaneously improving health, improving patient experience and reducing per capita costs. (Triple Aim)

 1 PA, 4 NPs, 4 RNs Superior (Staff from Main) Fargo 1 NP & recruiting")
12 PROGRAM STAFF Medical Director Cardiologist oversight of program, clinical leadership Cardiologists Essentia s HF Program 1998 Duluth Only 1 CNP 1 RN 1 CMA Accurate diagnosis and treatment plan Essentia s HF Program Today Virginia 2 NPs, 2 RNs Spooner/Hayward 1 PA & 1 NP, 2 RNs Ashland 1 NP, 1 RN Duluth (Main hub) 1 PA, 4 NPs, 4 RNs Superior (Staff from Main) Fargo 1 NP & recruiting another,2 RNs Brainerd 2 NPs & several RN s who float
 Fargo 1 NP & recruiting another,2 RNs Brainerd 2 NPs & several RN s who")
13 Essentia Health HF Program Sites HF Program Site Outreach Site

14 Essentia s HF Program Model Consult 5-7 days after hospital discharge Patients managed by APP in ambulatory setting Seen by cardiologist initially, annually and as needed Registered nurses provide continuous case management: Phone triage Follow-up on labs/ test results Utilize protocols Manage telescale data ONGOING PATIENT EDUCATION

15 PROGRAM DYNAMICS Patient and Family Centered Care - Goals Multidisciplinary team approach to care Continuity of care Coaching and support Education Immediate feedback on health choices Relationship building with patient/family Engaged/passionate staff

 Patient requiring increased doses of diuretics to manage volume Any heart failure patient needing extra education, support, close management High risk (HFSA criteria) multiple")
16 Referrals to HF Program Admission for HF in last 6 months or a HF exacerbation treated as outpatient in last 6 months Newly diagnosed cardiomyopathy Any patient with CRT (special pacemaker for HF patients) Patient requiring increased doses of diuretics to manage volume Any heart failure patient needing extra education, support, close management High risk (HFSA criteria) multiple co-morbidities: Renal insufficiency, Low output state, DM, COPD, NYHA III or IV, Frequent hospitalization for any cause, Cognitive impairment, History of depression, Inadequate social support, Poor health literacy, and Persistent non-adherence to therapy Patient agrees to plan

17 SHOW ME THE MONEY!!

18 Piloting a Heart Failure Program Pilot of 25 patients in 2000 This pilot revealed: 82% Reduction in HF hospitalizations 81% Decrease in Length of Stay 88% Decrease in ER Visits

19 Second Pilot with Payer BCBS of MN 29 patients in 2002 Type of Care Pre- Program 6 months Post- Program 6 months Percent Change Inpatient $1,149,080 $185,134-84% Outpatient $124,884 $125,498 0% ER $379,852 $66,318-83% Prof. Fees $674,428 $706,298 5% Lab/Radiol $138,781 $118,064-15% Pharmacy $124,229 $137,312 11% Total $2,591,254 $1,338,624-48% Savings of $1.25 Million

20 6 Month Readmission Rate for HF FY 05 FY 06 FY 07 FY 08 FY 09 FY 10 National Average St. Mary's HF Program Telescale (<1%)

21 30 Day Hospital Readmissions National St. Mary s HF Program
22 2014 YEAR END SUMMARY HF Program Patients 2,288 HF Admissions (209) 9.1% All Cause 30 Day Readmissions (34) 16.3% HF 30 Day Readmissions (10) 4.8%
23
24 Appropriate use of telescales Consider for: Patients with 2 or more hospitalizations for HF during the past year Patients unable to self-report weights within given parameters and/or inadequate social support Patients who live great distances from clinic and have difficulty getting to office visits Not recommended for: Dialysis patients Weight loss program Patients residing in skilled nursing facility with 24 hour care Unsteady patients

25 30 day Re-admission for HF Yearly HF Admission Rate # of Patients on scales
26 Advantages to Tele-monitoring Facilitates early intervention and prevents ER visits and hospitalizations Improved patient adherence with care plan Patients get immediate feedback on life style choices High patient satisfaction Family reassured Provides additional opportunity to educate patients Builds trust between patient and provider
27
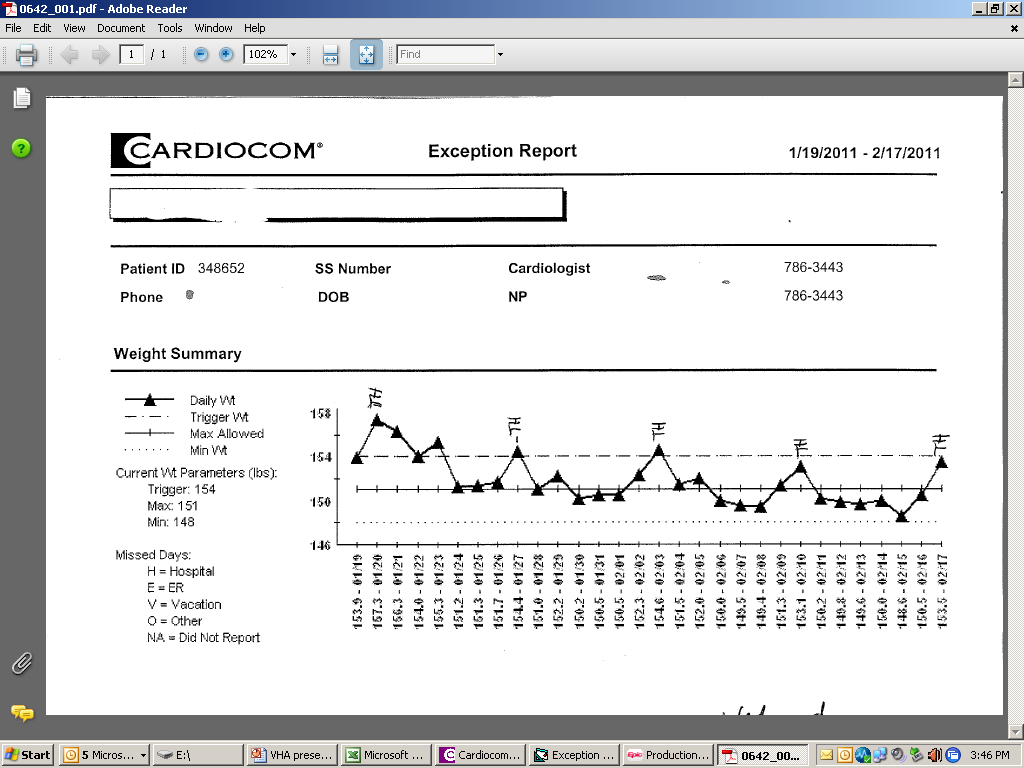
28 Monitoring and Exception Review Patient alerts in Cardiocom Nurse reviews data in both Cardiocom and EPIC Makes decision if patient needs to be contacted If assessment is needed the nurse considers the following: Nursing assessment and education needs Review medication list Dietary compliance Follows diuretic protocol as indicated/or talks with provider Initiate office visits or primary care referrals as needed Care plan monitoring; hospitalization initiation Communication with team members (other specialties)
29
30
31
32
33 Tele-monitoring Exception Review RN calls patient and assesses the following: Nursing Assessment Medication list reviewed Dietary Compliance Educational needs Follows Diuretic protocol as indicated/or talks with NP/PA Makes follow-up recommendations Initiate office visits or primary care referrals Care Plan monitoring; Hospitalization initiation Communication with team member (other specialties)
34 THEN Fee for Service Model Expense Center HF Program NOW ACO model Greatly improves the quality of care for HF patients Little if any payment for services Reimbursement reducer Prevents admissions, readmissions and ED visits Reduces the cost of medical care by reducing admissions, readmissions and ED visits Improved service and experience for patients with close monitoring and coordination of care ACOs rewarded for improving quality of care and controlling costs.
35 Growth of HF Program Added Telehealth video visits to remote sites Opened additional HF Program sites Integrated home scale data into electronic medical records Cross coverages options with other sites Advance Care Planning Pilot Program
36 Vision for Essentia Health HF Program Be more involved with hospitalized HF patients Seamless interface with primary care Patients hospitalized with a primary diagnosis of heart failure will be enrolled in the heart failure program Tele-health available at all sites for timely access Major contribution to the ACO model and continue to meet the triple aim; Quality/Cost/Service Expand Advance Care Planning
37 I ve learned that people will forget what you said, people will forget what you did, but people will never forget how you made them feel. Maya Angelou

38 Thank you!! Questions?? Denise Buxbaum, RN, BSN, CHFN Heart Failure Program Manager Essentia Health Heart & Vascular Center 407 East Third Street Duluth, MN P F Denise.Buxbaum@EssentiaHealth.org
Connect4 Patients CCCM Primary Care Community. Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM
 Connect4 Patients CCCM Primary Care Community Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM September 17, 2015 Objectives: Describe innovative care management
Connect4 Patients CCCM Primary Care Community Presented By: Veronica Mansfield, DNP, APRN, AE-C, CCM Kit McKinnon, MBA, BSN, RN, CDE, CCM September 17, 2015 Objectives: Describe innovative care management
Hypertension Best Practices Symposium
 essentia health: east region 1 Hypertension Best Practices Symposium RN Hypertension Management Pilot Essentia Health: East Region Duluth, MN ORGANIZATION PROFILE Essentia Health is an integrated health
essentia health: east region 1 Hypertension Best Practices Symposium RN Hypertension Management Pilot Essentia Health: East Region Duluth, MN ORGANIZATION PROFILE Essentia Health is an integrated health
Call-A-Nurse Location
 Call-A-Nurse A 24-hour medical call center, specializing in registered nurse telephone triage, answering service, physician and service referral, and class registration. Call-A-Nurse Location Call-A-Nurse
Call-A-Nurse A 24-hour medical call center, specializing in registered nurse telephone triage, answering service, physician and service referral, and class registration. Call-A-Nurse Location Call-A-Nurse
1. Executive Summary Problem/Opportunity: Evidence: Baseline Data: Intervention: Results:
 A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
Kick off Meeting November 11 13, 2015. MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF)
") Kick off Meeting November 11 13, 2015 MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF) Team Composition Justin Huynh, MD Internal Medicine, Physician Champion Mary Laubinger,
Kick off Meeting November 11 13, 2015 MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF) Team Composition Justin Huynh, MD Internal Medicine, Physician Champion Mary Laubinger,
ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION)
") ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION) Hello and welcome. Thank you for taking part in this presentation entitled "Essentia Health as an ACO or Accountable Care Organization -- What
ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION) Hello and welcome. Thank you for taking part in this presentation entitled "Essentia Health as an ACO or Accountable Care Organization -- What
Henry Ford Health System Care Coordination and Readmissions Update
 Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
HealthCare Partners of Nevada. Heart Failure
 HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
Presented by: Char Brar, ACNP, MS(Chem.), MSN, RN Cardiology Nurse Practitioner JBVAMC, Chicago
, MSN, RN Cardiology Nurse Practitioner JBVAMC, Chicago") Presented by: Char Brar, ACNP, MS(Chem.), MSN, RN Cardiology Nurse Practitioner JBVAMC, Chicago 200 bed acute care facility 4 Community Based Out-patient Clinics (CBOCs) 58,000 Veterans IN FY 2008 : 768
Presented by: Char Brar, ACNP, MS(Chem.), MSN, RN Cardiology Nurse Practitioner JBVAMC, Chicago 200 bed acute care facility 4 Community Based Out-patient Clinics (CBOCs) 58,000 Veterans IN FY 2008 : 768
Ann Hablitzel, RN, BSN, MBA Hospice Care of California
 Ann Hablitzel, RN, BSN, MBA Hospice Care of California Objectives Describe the creations of new community based palliative care programs Identify criteria for admission Discuss philosophy and goals Analyze
Ann Hablitzel, RN, BSN, MBA Hospice Care of California Objectives Describe the creations of new community based palliative care programs Identify criteria for admission Discuss philosophy and goals Analyze
Nurse Practitioners (NPs) and Physician Assistants (PAs): What s the Difference?
 and Physician Assistants (PAs): What s the Difference?") Nurse Practitioners (NPs) and Physician Assistants (PAs): What s the Difference? More than ever before, patients receive medical care from a variety of practitioners, including physicians, physician assistants
Nurse Practitioners (NPs) and Physician Assistants (PAs): What s the Difference? More than ever before, patients receive medical care from a variety of practitioners, including physicians, physician assistants
Table 1 Performance Measures. Quality Monitoring P4P Yr1 Yr2 Yr3. Specification Source. # Category Performance Measure
 Table 1 Performance Measures # Category Performance Measure 1 Behavioral Health Risk Assessment and Follow-up 1) Behavioral Screening/ Assessment within 60 days of enrollment New Enrollees who completed
Table 1 Performance Measures # Category Performance Measure 1 Behavioral Health Risk Assessment and Follow-up 1) Behavioral Screening/ Assessment within 60 days of enrollment New Enrollees who completed
PCMH and Care Management: Where do we start?
 PCMH and Care Management: Where do we start? Patricia Bohs, RN, BSN Quality Assurance Manager Kelly McCloughan QA Data Manager Wayne Memorial Community Health Centers Honesdale, PA Wayne Memorial Community
PCMH and Care Management: Where do we start? Patricia Bohs, RN, BSN Quality Assurance Manager Kelly McCloughan QA Data Manager Wayne Memorial Community Health Centers Honesdale, PA Wayne Memorial Community
Peter Munk Cardiac Centre, University Health Network. Allied Health Personnel Symposium American Association of Thoracic Surgery April 26, 2014
 The Expanding Role of the Nurse Practitioner and Physician Assistant Across the Continuum of Care for the CTS Patient: Preoperative, Postoperative, and After Discharge Jane MacIver RN NP PhD Peter Munk
The Expanding Role of the Nurse Practitioner and Physician Assistant Across the Continuum of Care for the CTS Patient: Preoperative, Postoperative, and After Discharge Jane MacIver RN NP PhD Peter Munk
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Home Health Care: A More Cost-Effective Approach to Medicaid in Illinois Illinois HomeCare & Hospice Council December 2010
 Home Health Care: A More Cost-Effective Approach to Medicaid in Illinois Illinois HomeCare & Hospice Council December 2010 As the Illinois Legislature prepares to act on the future of Medicaid, it is important
Home Health Care: A More Cost-Effective Approach to Medicaid in Illinois Illinois HomeCare & Hospice Council December 2010 As the Illinois Legislature prepares to act on the future of Medicaid, it is important
Emerging g Trends in Home Care
 Emerging g Trends in Home Care Dana Sheer, ACNP, MSN Susan Beausoliel, BSN, MS, DNP 1 The Triple Aim Goals Quality Improve Patient Outcomes Goal Readmissions Cost Reduce costs/penalties associated w/ readmissions
Emerging g Trends in Home Care Dana Sheer, ACNP, MSN Susan Beausoliel, BSN, MS, DNP 1 The Triple Aim Goals Quality Improve Patient Outcomes Goal Readmissions Cost Reduce costs/penalties associated w/ readmissions
Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes. FINANCIAL DISCLOSURE: No relevant financial relationship exists
 Cheri Basso BSN, RN-BC, CHFN Mary Washington Healthcare Fredericksburg, VA Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes FINANCIAL DISCLOSURE: No relevant financial relationship
Cheri Basso BSN, RN-BC, CHFN Mary Washington Healthcare Fredericksburg, VA Cheri Basso BSN, RN-BC,CHFN Hospital Initiatives to Improve Outcomes FINANCIAL DISCLOSURE: No relevant financial relationship
The Role of Telemedicine in Home Monitoring and Long Term Care June 7, 2012. Penny S. Milanovich President UPMC Visiting Nurses Association
 The Role of Telemedicine in Home Monitoring and Long Term Care June 7, 2012 Penny S. Milanovich President UPMC Visiting Nurses Association Cost of Chronic Conditions An average of 40-50% of healthcare
The Role of Telemedicine in Home Monitoring and Long Term Care June 7, 2012 Penny S. Milanovich President UPMC Visiting Nurses Association Cost of Chronic Conditions An average of 40-50% of healthcare
The New Complex Patient. of Diabetes Clinical Programming
 The New Complex Patient as Seen Through the Lens of Diabetes Clinical Programming 1 Valerie Garrett, M.D. Medical Director, Diabetes Center at Mission Health System Nov 6, 2014 Diabetes Health Burden High
The New Complex Patient as Seen Through the Lens of Diabetes Clinical Programming 1 Valerie Garrett, M.D. Medical Director, Diabetes Center at Mission Health System Nov 6, 2014 Diabetes Health Burden High
November 15, 2013. Ann Laramee MS ANP-BC ACNS-BC CHFN FletcherAllen.org
 Advance Care Planning with Heart Failure: Results of a Primary Care Practitioners Needs Survey 5 th Annual Nursing Research and Evidence Based Practice Symposium November 15, 2013 Ann Laramee MS ANP-BC
Advance Care Planning with Heart Failure: Results of a Primary Care Practitioners Needs Survey 5 th Annual Nursing Research and Evidence Based Practice Symposium November 15, 2013 Ann Laramee MS ANP-BC
Innovations@Home. Home Health Initiatives Reduce Avoidable Readmissions by Leveraging Innovation
 How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
Population Health Management Program
 Population Health Management Program Program (formerly Disease Management) is dedicated to improving our members health and quality of life. Our Population Health Management Programs aim to improve care
Population Health Management Program Program (formerly Disease Management) is dedicated to improving our members health and quality of life. Our Population Health Management Programs aim to improve care
Approaches to Asthma Management:
 Approaches to Asthma Management: BY CAROL MCPHILLIPS-TANGUM AND CAROLINE M. ERCEG ASTHMA IS A CHRONIC DISEASE that affects millions of people in the United States and disproportionately impacts children,
Approaches to Asthma Management: BY CAROL MCPHILLIPS-TANGUM AND CAROLINE M. ERCEG ASTHMA IS A CHRONIC DISEASE that affects millions of people in the United States and disproportionately impacts children,
SPECIALTY CASE MANAGEMENT
 SPECIALTY CASE MANAGEMENT Our Specialty Case Management programs boost ROI and empower members to make informed decisions and work with their physicians to better manage their health. KEPRO is Effectively
SPECIALTY CASE MANAGEMENT Our Specialty Case Management programs boost ROI and empower members to make informed decisions and work with their physicians to better manage their health. KEPRO is Effectively
3/11/15. COPD Disease Management Tackling the Transition. Objectives. Describe the multidisciplinary approach to inpatient care for COPD patients
 Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
Faculty Disclosures COPD Disease Management Tackling the Transition Dr. Cappelluti has no actual or potential conflicts of interest associated with this presentation. Jane Reardon has no actual or potential
MedStar Family Choice (MFC) Case Management Program. Cyd Campbell, MD, FAAP Medical Director, MFC MCAC June 24, 2015
 Case Management Program. Cyd Campbell, MD, FAAP Medical Director, MFC MCAC June 24, 2015") MedStar Family Choice (MFC) Case Management Program Cyd Campbell, MD, FAAP Medical Director, MFC MCAC June 24, 2015 Case Management Program Presentation Overview CM Programs Disease Management Complex
MedStar Family Choice (MFC) Case Management Program Cyd Campbell, MD, FAAP Medical Director, MFC MCAC June 24, 2015 Case Management Program Presentation Overview CM Programs Disease Management Complex
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates
 Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Get With The Guidelines Best Practices: A look at reducing 30-day heart failure readmission rates Thank you for joining the webinar! The presentation will begin shortly. *Please make sure your computer
Telehealth and the Homebound Heart Failure Patient
 Telehealth and the Homebound Heart Failure Patient By Karen Malin Garfield, RN, BSN 104 HEART 2010 The Official Guide to a Strong Heart and Healthy Lifestyle PTS Article Heart2010_Suncrest.indd 1 Health
Telehealth and the Homebound Heart Failure Patient By Karen Malin Garfield, RN, BSN 104 HEART 2010 The Official Guide to a Strong Heart and Healthy Lifestyle PTS Article Heart2010_Suncrest.indd 1 Health
5/6/2014. Physiologic Monitoring Tools & Use with Patients with Chronic Health Conditions. Objectives. The Issue at Hand
 Physiologic Monitoring Tools & Use with Patients with Chronic Health Conditions Kelly Brittain, PhD, RN Assistant Professor MCRH-Nursing Grand Rounds May 8, 2014 Objectives 1. Summarize previous research
Physiologic Monitoring Tools & Use with Patients with Chronic Health Conditions Kelly Brittain, PhD, RN Assistant Professor MCRH-Nursing Grand Rounds May 8, 2014 Objectives 1. Summarize previous research
Readmissions as an Enterprise Priority. Presenters 4/17/2014
 Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center Vmaniscalco@parkmanorrehab.com Eileen
Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center Vmaniscalco@parkmanorrehab.com Eileen
DELIVERING VALUE THROUGH TECHNOLOGY
 DELIVERING VALUE THROUGH TECHNOLOGY Mark Nelson, MD - EMR Physician Champion Krishna Ramachandran - Chief Information and Transformation Officer Karen Adamson - Director, Epic Clinical Applications DuPage
DELIVERING VALUE THROUGH TECHNOLOGY Mark Nelson, MD - EMR Physician Champion Krishna Ramachandran - Chief Information and Transformation Officer Karen Adamson - Director, Epic Clinical Applications DuPage
Pushing the Boundaries of Population Health Management: How University Hospitals Launched Three ACOs July 26, 2013 American Hospital Association
 Pushing the Boundaries of Population Health Management: How University Hospitals Launched Three ACOs July 26, 2013 American Hospital Association Eric J. Bieber, M.D. Chief Medical Officer, University Hospitals
Pushing the Boundaries of Population Health Management: How University Hospitals Launched Three ACOs July 26, 2013 American Hospital Association Eric J. Bieber, M.D. Chief Medical Officer, University Hospitals
ACO Project Overview and Key Elements. Presented to FSSA September 3, 2013. 2013 Franciscan Alliance, Inc.
 ACO Project Overview and Key Elements Presented to FSSA September 3, 2013 2013 Franciscan Alliance, Inc. Background of Presentation House Enrolled Act 1328 requires the Indiana Family and Social Services
ACO Project Overview and Key Elements Presented to FSSA September 3, 2013 2013 Franciscan Alliance, Inc. Background of Presentation House Enrolled Act 1328 requires the Indiana Family and Social Services
Community Care of North Carolina
 Community Care of North Carolina CCNC Transitional Care Management Jennifer Cockerham, RN, BSN, CDE Director, Chronic Care Programs & Quality Management 1 Chronic Care Population Within the NC Medicaid
Community Care of North Carolina CCNC Transitional Care Management Jennifer Cockerham, RN, BSN, CDE Director, Chronic Care Programs & Quality Management 1 Chronic Care Population Within the NC Medicaid
Patient to Person. Transitions of Care. Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM
 Patient to Person Transitions of Care Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM Transitions of Care Transitioning from school to adult services (vocational, medical day, etc.)
Patient to Person Transitions of Care Colby Bearch, MA-SF, MA-M, BA, RN, CDONA Sharyn King, RN, BSN, CCM Transitions of Care Transitioning from school to adult services (vocational, medical day, etc.)
Nurse Practitioner Outcomes: The Integration & Future Directions of The Liver Transplant NP. Amanda Tinning MN NP October 13, 2011
 Nurse Practitioner Outcomes: The Integration & Future Directions of The Liver Transplant NP Amanda Tinning MN NP October 13, 2011 Overview Define clinical outcomes Discuss the contributions of the NP role
Nurse Practitioner Outcomes: The Integration & Future Directions of The Liver Transplant NP Amanda Tinning MN NP October 13, 2011 Overview Define clinical outcomes Discuss the contributions of the NP role
THE ROLE OF HEALTH INFORMATION TECHNOLOGY IN PATIENT-CENTERED CARE COLLABORATION. 2012 Louisiana HIPAA & EHR Conference Presenter: Chris Williams
 THE ROLE OF HEALTH INFORMATION TECHNOLOGY IN PATIENT-CENTERED CARE COLLABORATION 2012 Louisiana HIPAA & EHR Conference Presenter: Chris Williams Agenda Overview Impact of HIT on Patient-Centered Care (PCC)
THE ROLE OF HEALTH INFORMATION TECHNOLOGY IN PATIENT-CENTERED CARE COLLABORATION 2012 Louisiana HIPAA & EHR Conference Presenter: Chris Williams Agenda Overview Impact of HIT on Patient-Centered Care (PCC)
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 Page1 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify G.6 When to Notify G.11 Case Management Services G.14 Special Needs Services G.16 Health Management Programs
Page1 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify G.6 When to Notify G.11 Case Management Services G.14 Special Needs Services G.16 Health Management Programs
Building a Specialty Pharmacy Business. Kyle Skiermont, PharmD Director of Specialty/Infusion Operation Fairview Pharmacy Services
 Building a Specialty Pharmacy Business Kyle Skiermont, PharmD Director of Specialty/Infusion Operation Fairview Pharmacy Services Overview Agenda Brief overview of Fairview Barriers for hospital/health
Building a Specialty Pharmacy Business Kyle Skiermont, PharmD Director of Specialty/Infusion Operation Fairview Pharmacy Services Overview Agenda Brief overview of Fairview Barriers for hospital/health
5/10/13 HEALTH CARE REFORM LONGITUDINAL CARE COORDINATION HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO WHY WHAT HOW WHEN WHO
 TRANSITION CARE TRANSITION CARE WHY WHAT HOW WHEN WHO HEALTH CARE REFORM HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO Cost/Quality equation Higher cost care has not/does not equate with higher
TRANSITION CARE TRANSITION CARE WHY WHAT HOW WHEN WHO HEALTH CARE REFORM HEALTH CARE REFORM WHY = VALUE WHY WHAT HOW WHEN WHO Cost/Quality equation Higher cost care has not/does not equate with higher
Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals
 Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals 12/18/2013 12/18/13 2013, American Heart Association 1 Thank you for Joining the Webinar Today. The Presentation will Begin
Heart Failure Best Practice Strategies: Featuring Target: HF Honor Roll Hospitals 12/18/2013 12/18/13 2013, American Heart Association 1 Thank you for Joining the Webinar Today. The Presentation will Begin
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home
 RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
How To Plan A Rehabilitation Program
 Project Plan to Rehabilitation Service Connecting and Collaborating in the Continuity of Care in Rehabilitation Presented By: Arlene Whitehead, May 31, 2011 Rehabilitation Collaborative Overview OUTLINE
Project Plan to Rehabilitation Service Connecting and Collaborating in the Continuity of Care in Rehabilitation Presented By: Arlene Whitehead, May 31, 2011 Rehabilitation Collaborative Overview OUTLINE
Managing End-Stage Renal Disease Improving clinical outcomes and reducing the cost of care for Medicare Advantage, Medicaid and Commercial Populations
 White Paper Managing End-Stage Renal Disease Improving clinical outcomes and reducing the cost of care for Medicare Advantage, Medicaid and Commercial Populations Optum www.optum.com Page 1 Executive Summary
White Paper Managing End-Stage Renal Disease Improving clinical outcomes and reducing the cost of care for Medicare Advantage, Medicaid and Commercial Populations Optum www.optum.com Page 1 Executive Summary
Welcome to Magellan Complete Care
 Magellan Complete Care of Florida Provider Newsletter Welcome to Magellan Complete Care On behalf of Magellan Complete Care of Florida, thank you for your continued support and collaboration. As the only
Magellan Complete Care of Florida Provider Newsletter Welcome to Magellan Complete Care On behalf of Magellan Complete Care of Florida, thank you for your continued support and collaboration. As the only
Necessity is the Mother of Invention:
 June, 2013 Necessity is the Mother of Invention: Utilizing Technology to Provide High Quality Healthcare to Rural Areas of the Upper Midwest Wayne Booze, MPA, Program Officer, The Helmsley Charitable Trust
June, 2013 Necessity is the Mother of Invention: Utilizing Technology to Provide High Quality Healthcare to Rural Areas of the Upper Midwest Wayne Booze, MPA, Program Officer, The Helmsley Charitable Trust
New Models of Care and Approaches to Payment
 New Models of Care and Approaches to Payment Richard Lopez, MD Chief Medical Officer Richard_Lopez@AtriusHealth.org September 30, 2014 Atrius Health Non-profit alliance of six leading independent medical
New Models of Care and Approaches to Payment Richard Lopez, MD Chief Medical Officer Richard_Lopez@AtriusHealth.org September 30, 2014 Atrius Health Non-profit alliance of six leading independent medical
Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Coventry Health and Life Insurance Company Commercial Lines of Business
 Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Coventry Health and Life Insurance Company Commercial Lines of Business Quality Management Program 2012 Overview Quality Improvement
Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Coventry Health and Life Insurance Company Commercial Lines of Business Quality Management Program 2012 Overview Quality Improvement
High Desert Medical Group Connections for Life Program Description
 High Desert Medical Group Connections for Life Program Description POLICY: High Desert Medical Group ("HDMG") promotes patient health and wellbeing by actively coordinating services for members with multiple
High Desert Medical Group Connections for Life Program Description POLICY: High Desert Medical Group ("HDMG") promotes patient health and wellbeing by actively coordinating services for members with multiple
A Call to Duty. Transforming Veteran s End-of-Life Care. Julie Benson, MD. Medical Director Hospice and Palliative Care. Jessica Martensen, RN
 A Call to Duty Transforming Veteran s End-of-Life Care Julie Benson, MD Medical Director Hospice and Palliative Care Jessica Martensen, RN Director, Home Care and Hospice Lakewood Health System Staples,
A Call to Duty Transforming Veteran s End-of-Life Care Julie Benson, MD Medical Director Hospice and Palliative Care Jessica Martensen, RN Director, Home Care and Hospice Lakewood Health System Staples,
Care Coordination at Frederick Regional Health System. Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care
 Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Personalized Medicine
 Intelligent Health and Personalized Medicine Wireless Medical Devices Galen Institute March 25, 2010 Don Casey, CEO, West Wireless Health Institute West Wireless Health Institute An independent nonprofit
Intelligent Health and Personalized Medicine Wireless Medical Devices Galen Institute March 25, 2010 Don Casey, CEO, West Wireless Health Institute West Wireless Health Institute An independent nonprofit
POPULATION HEALTH MANAGEMENT The Lynchpin of Emerging Healthcare Delivery Improve Patient Outcomes, Engage Physicians, and Manage Risk
 POPULATION HEALTH MANAGEMENT The Lynchpin of Emerging Healthcare Delivery Improve Patient Outcomes, Engage Physicians, and Manage Risk Julia Andrieni, MD, FACP Vice President, Population Health and Primary
POPULATION HEALTH MANAGEMENT The Lynchpin of Emerging Healthcare Delivery Improve Patient Outcomes, Engage Physicians, and Manage Risk Julia Andrieni, MD, FACP Vice President, Population Health and Primary
National Clinical Programmes
 National Clinical Programmes Section 3 Background information on the National Clinical Programmes Mission, Vision and Objectives July 2011 V0. 6_ 4 th July, 2011 1 National Clinical Programmes: Mission
National Clinical Programmes Section 3 Background information on the National Clinical Programmes Mission, Vision and Objectives July 2011 V0. 6_ 4 th July, 2011 1 National Clinical Programmes: Mission
The Joint Commission Advanced DSC Certification for Inpatient Diabetes Care
 The Joint Commission Advanced DSC Certification for Inpatient Diabetes Care November 12, 2013 Caroline Isbey RN, MSN, CDE Associate Director Teresa Gomez Associate Project Director Specialist-SSM Carol
The Joint Commission Advanced DSC Certification for Inpatient Diabetes Care November 12, 2013 Caroline Isbey RN, MSN, CDE Associate Director Teresa Gomez Associate Project Director Specialist-SSM Carol
Developing a Successful TAVR Program/Clinic: The Team Approach
 Developing a Successful TAVR Program/Clinic: The Team Approach Kathryn Fidlow RN, BSN Senior Quality Management Specialist NYP-Columbia University Medical Center The Heart Valve Center NYP-Columbia University
Developing a Successful TAVR Program/Clinic: The Team Approach Kathryn Fidlow RN, BSN Senior Quality Management Specialist NYP-Columbia University Medical Center The Heart Valve Center NYP-Columbia University
A STRATIFIED APPROACH TO PATIENT SAFETY THROUGH HEALTH INFORMATION TECHNOLOGY
 A STRATIFIED APPROACH TO PATIENT SAFETY THROUGH HEALTH INFORMATION TECHNOLOGY Table of Contents I. Introduction... 2 II. Background... 2 III. Patient Safety... 3 IV. A Comprehensive Approach to Reducing
A STRATIFIED APPROACH TO PATIENT SAFETY THROUGH HEALTH INFORMATION TECHNOLOGY Table of Contents I. Introduction... 2 II. Background... 2 III. Patient Safety... 3 IV. A Comprehensive Approach to Reducing
Attachment A Minnesota DHS Community Service/Community Services Development
 Attachment A Minnesota DHS Community Service/Community Services Development Applicant Organization: First Plan of Minnesota Project Title: Implementing a Functional Daily Living Skills Assessment to Predict
Attachment A Minnesota DHS Community Service/Community Services Development Applicant Organization: First Plan of Minnesota Project Title: Implementing a Functional Daily Living Skills Assessment to Predict
Coordinating Transitions of Care: It Takes a Village
 Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
ST JOHN S LUTHERAN MINISTRIES. Kent Burgess President & CEO
 ST JOHN S LUTHERAN MINISTRIES Kent Burgess President & CEO WHAT S CHANGING MAYBE? -The way we get paid (Reduce Cost) -The way we get measured (Better Care) -What will be required of us (More) -Partnerships/Affiliations
ST JOHN S LUTHERAN MINISTRIES Kent Burgess President & CEO WHAT S CHANGING MAYBE? -The way we get paid (Reduce Cost) -The way we get measured (Better Care) -What will be required of us (More) -Partnerships/Affiliations
Statement on the Redirection of Nursing Education Medicare Funds to Graduate Nurse Education
 Statement on the Redirection of Nursing Education Medicare Funds to Graduate Nurse Education To the National Bipartisan Commission on the Future of Medicare Graduate Medical Education Study Group (January
Statement on the Redirection of Nursing Education Medicare Funds to Graduate Nurse Education To the National Bipartisan Commission on the Future of Medicare Graduate Medical Education Study Group (January
The Value Quadrant of Healthcare Reform. 2008 Pharos Innovations, LLC. All Rights Reserved.
 The Value Quadrant of Healthcare Reform ACOs in PPACA Provider Organizations or networked groups Accountable for quality, cost and overall care of defined population of Medicare FFS benes Key metrics to
The Value Quadrant of Healthcare Reform ACOs in PPACA Provider Organizations or networked groups Accountable for quality, cost and overall care of defined population of Medicare FFS benes Key metrics to
case management controlled
 The effecte ffects s of a nurse-led case management programme on patients undergoing peritoneal dialysis: a randomized controlled trial Susan Chow RN, PhD The HK Polytechnic University Frances Wong RN,
The effecte ffects s of a nurse-led case management programme on patients undergoing peritoneal dialysis: a randomized controlled trial Susan Chow RN, PhD The HK Polytechnic University Frances Wong RN,
9/23/2014. Mission To improve the health of the people in the communities we serve.
 Big Data & Reduced Readmissions Chris Myers, MS, RN, CCM, Director of Care Transitions, Texas Health Harris Methodist Hospital Hurst-Euless- Bedford Anand Shah, MD, Vice President, Parkland Center for
Big Data & Reduced Readmissions Chris Myers, MS, RN, CCM, Director of Care Transitions, Texas Health Harris Methodist Hospital Hurst-Euless- Bedford Anand Shah, MD, Vice President, Parkland Center for
The new Heart Failure pathway
 The new Heart Failure pathway An integrated and seamless Strategy Dr Sunil Balani Definition of Heart Failure The inability of the heart to pump blood at a rate commensurate with the requirements of metabolising
The new Heart Failure pathway An integrated and seamless Strategy Dr Sunil Balani Definition of Heart Failure The inability of the heart to pump blood at a rate commensurate with the requirements of metabolising
Population Health Management: Banner Health Network s Perspective. Neta Faynboym, Medical Director Banner Health Network
 Population Health Management: Banner Health Network s Perspective Neta Faynboym, Medical Director Banner Health Network 29 Acute Care Hospitals BANNER AT A GLANCE Banner Health Network with 400K lives
Population Health Management: Banner Health Network s Perspective Neta Faynboym, Medical Director Banner Health Network 29 Acute Care Hospitals BANNER AT A GLANCE Banner Health Network with 400K lives
Welcome to the Emory Diabetes Education Training Academy!
 Welcome to the Emory Diabetes Education Training Academy! Session Title: DSME Program Overview: What a Coordinator Should Know About Reimbursement, Coding, Billing and Referrals Speakers: Amie Hardin,
Welcome to the Emory Diabetes Education Training Academy! Session Title: DSME Program Overview: What a Coordinator Should Know About Reimbursement, Coding, Billing and Referrals Speakers: Amie Hardin,
Proven Innovations in Primary Care Practice
 Proven Innovations in Primary Care Practice October 14, 2014 The opinions expressed are those of the presenter and do not necessarily state or reflect the views of SHSMD or the AHA. 2014 Society for Healthcare
Proven Innovations in Primary Care Practice October 14, 2014 The opinions expressed are those of the presenter and do not necessarily state or reflect the views of SHSMD or the AHA. 2014 Society for Healthcare
Patients Receive Recommended Care for Community-Acquired Pneumonia
 Patients Receive Recommended Care for Community-Acquired Pneumonia For New Jersey to be a state in which all people live long, healthy lives. DSRIP LEARNING COLLABORATIVE PRESENTATION The Care you Trust!
Patients Receive Recommended Care for Community-Acquired Pneumonia For New Jersey to be a state in which all people live long, healthy lives. DSRIP LEARNING COLLABORATIVE PRESENTATION The Care you Trust!
Physician Guide to Home Health Care Certification for Medicare Enrollees Steve Landers MD, MPH (landers@ccf.org) Director, Cleveland Clinic at Home
 Director, Cleveland Clinic at Home") Physician Guide to Home Health Care Certification for Medicare Enrollees Steve Landers MD, MPH (landers@ccf.org) Director, Cleveland Clinic at Home January 2011 Background Helping patients succeed at home
Physician Guide to Home Health Care Certification for Medicare Enrollees Steve Landers MD, MPH (landers@ccf.org) Director, Cleveland Clinic at Home January 2011 Background Helping patients succeed at home
Spalding Regional Hospital. Mobile Intergraded Health Care Shifting from Sick Care to Patient Centered Healthcare.
 Spalding Regional Hospital Mobile Intergraded Health Care Shifting from Sick Care to Patient Centered Healthcare. Where is Spalding County in all of this? 2014 Unemployment Rate: 8.5% NR 6.8% Living Below
Spalding Regional Hospital Mobile Intergraded Health Care Shifting from Sick Care to Patient Centered Healthcare. Where is Spalding County in all of this? 2014 Unemployment Rate: 8.5% NR 6.8% Living Below
The challenge. What we did. Highlights. Designing and delivering scalable telemonitoring and telecare through partnership.
 Telehealthcare Designing and delivering scalable telemonitoring and telecare through partnership The challenge Northern Ireland has a population of approximately 1.8 million people. Around two thirds of
Telehealthcare Designing and delivering scalable telemonitoring and telecare through partnership The challenge Northern Ireland has a population of approximately 1.8 million people. Around two thirds of
Cloud Computing / Tele- Health in a Novel Integrated CHF Disease Management Program: The Israeli Experience
 Cloud Computing / Tele- Health in a Novel Integrated CHF Disease Management Program: The Israeli Experience Haim Silber MD Programs Initiator Maccabi Health Care services and Gertner Institute, ISRAEL
Cloud Computing / Tele- Health in a Novel Integrated CHF Disease Management Program: The Israeli Experience Haim Silber MD Programs Initiator Maccabi Health Care services and Gertner Institute, ISRAEL
Disease Management Identifications and Stratification Health Risk Assessment Level 1: Level 2: Level 3: Stratification
 Disease Management UnitedHealthcare Disease Management (DM) programs are part of our innovative Care Management Program. Our Disease Management (DM) program is guided by the principles of the UnitedHealthcare
Disease Management UnitedHealthcare Disease Management (DM) programs are part of our innovative Care Management Program. Our Disease Management (DM) program is guided by the principles of the UnitedHealthcare
How To Manage Health Care Needs
 HEALTH MANAGEMENT CUP recognizes the importance of promoting effective health management and preventive care for conditions that are relevant to our populations, thereby improving health care outcomes.
HEALTH MANAGEMENT CUP recognizes the importance of promoting effective health management and preventive care for conditions that are relevant to our populations, thereby improving health care outcomes.
Objectives. Clinical Impact of An Inpatient Diabetes Care Model. Impact of Diabetes on Hospitals. The Nebraska Medical Center Stats 6/5/2014
 Objectives Clinical Impact of An Inpatient Diabetes Care Model Beth Pfeffer MSN, RN CDE Andjela Drincic, MD 1. Examine the development of the role of the diabetes case manager model in the inpatient setting
Objectives Clinical Impact of An Inpatient Diabetes Care Model Beth Pfeffer MSN, RN CDE Andjela Drincic, MD 1. Examine the development of the role of the diabetes case manager model in the inpatient setting
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION
 Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Risk Tools in Predicting Rehospitalization from Home Care. VNAA Best Practice for Home Health
 Risk Tools in Predicting Rehospitalization from Home Care VNAA Best Practice for Home Health Learning objectives The participant will be able to: Discuss the need for risk assessment for home health patients
Risk Tools in Predicting Rehospitalization from Home Care VNAA Best Practice for Home Health Learning objectives The participant will be able to: Discuss the need for risk assessment for home health patients
Cheryl Schraeder, RN, PhD, FAAN. The demographic landscape of America is changing at an accelerated pace
 Stepping up to the challenge: Changing the way we deliver care Cheryl Schraeder, RN, PhD, FAAN 1 Goals of Presentation To Identify: The key challenges in delivering evidence-based & cost-effective care
Stepping up to the challenge: Changing the way we deliver care Cheryl Schraeder, RN, PhD, FAAN 1 Goals of Presentation To Identify: The key challenges in delivering evidence-based & cost-effective care
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS. Karen Unholz, RN, BSN
 INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
2003 FIRST MINISTERS ACCORD
 2003 FIRST MINISTERS ACCORD ON HEALTH CARE RENEWAL 1 In September 2000, First Ministers agreed on a vision, principles and action plan for health system renewal. Building from this agreement, all governments
2003 FIRST MINISTERS ACCORD ON HEALTH CARE RENEWAL 1 In September 2000, First Ministers agreed on a vision, principles and action plan for health system renewal. Building from this agreement, all governments
DATA DRIVEN HEALTH CARE TRANSFORMATION
 DATA DRIVEN HEALTH CARE TRANSFORMATION Population Health Analytics as the Foundation for Primary Care Redesign Sylvia Meltzer, MD, LSSGBC Laura Spurr, MPS, PMP Learning Objectives Organization description
DATA DRIVEN HEALTH CARE TRANSFORMATION Population Health Analytics as the Foundation for Primary Care Redesign Sylvia Meltzer, MD, LSSGBC Laura Spurr, MPS, PMP Learning Objectives Organization description
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment
 Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
Main Section of the proposal: 1. Overall Aim & Objectives:
 Main Section of the proposal: 1. Overall Aim & Objectives: Over the past two decades Providence Health & Services has developed a comprehensive tobacco cessation program within our health system. The foundation
Main Section of the proposal: 1. Overall Aim & Objectives: Over the past two decades Providence Health & Services has developed a comprehensive tobacco cessation program within our health system. The foundation
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System
 Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
Joan Carroll RN, CDMS, CCM Director of Care Transitions Lee Memorial Health System 1 Explain how patients experience transitions of care Identify variables that affect transitions due to lack of patient
MISSISSIPPI LEGISLATURE REGULAR SESSION 2014
 MISSISSIPPI LEGISLATURE REGULAR SESSION 2014 By: Senator(s) Burton To: Insurance SENATE BILL NO. 2646 (As Sent to Governor) 1 AN ACT TO CREATE NEW SECTION 83-9-353, MISSISSIPPI CODE OF 2 1972, TO REQUIRE
MISSISSIPPI LEGISLATURE REGULAR SESSION 2014 By: Senator(s) Burton To: Insurance SENATE BILL NO. 2646 (As Sent to Governor) 1 AN ACT TO CREATE NEW SECTION 83-9-353, MISSISSIPPI CODE OF 2 1972, TO REQUIRE
Presentation Objectives
 AMBULATORY NURSES DESCRIPTION OF THEIR SCOPE OF PRACTICE Nursing Research Team Presenters: Sharron Coffie, MSN, RN,CNS-BC, CHFN (PI); Katrina Petrie BSN, RN Olivia Stout, BSN, RN; Kristin Wuest BSN, RN;
AMBULATORY NURSES DESCRIPTION OF THEIR SCOPE OF PRACTICE Nursing Research Team Presenters: Sharron Coffie, MSN, RN,CNS-BC, CHFN (PI); Katrina Petrie BSN, RN Olivia Stout, BSN, RN; Kristin Wuest BSN, RN;
NH Broadband Conference May 16, 2014 Grappone Conference Center - Concord, NH
 NH Broadband Conference May 16, 2014 Grappone Conference Center - Concord, NH Track: Telehealth and Telemedicine SESSION 1-10:45 am - 11:20 am Telehealth and Telemedicine -The Dartmouth-Hitchcock Perspective
NH Broadband Conference May 16, 2014 Grappone Conference Center - Concord, NH Track: Telehealth and Telemedicine SESSION 1-10:45 am - 11:20 am Telehealth and Telemedicine -The Dartmouth-Hitchcock Perspective
2013 ACO Quality Measures
 ACO 1-7 Patient Satisfaction Survey Consumer Assessment of HealthCare Providers Survey (CAHPS) 1. Getting Timely Care, Appointments, Information 2. How well Your Providers Communicate 3. Patient Rating
ACO 1-7 Patient Satisfaction Survey Consumer Assessment of HealthCare Providers Survey (CAHPS) 1. Getting Timely Care, Appointments, Information 2. How well Your Providers Communicate 3. Patient Rating
Hospital to Physician Office to Home: A Respiratory Led Program Across the Continuum of Care
 Hospital to Physician Office to Home: A Respiratory Led Program Across the Continuum of Care Charley P. Starnes, RRT, RCP Clinical Respiratory Specialist- COPD Education Important Milestones July 2011-
Hospital to Physician Office to Home: A Respiratory Led Program Across the Continuum of Care Charley P. Starnes, RRT, RCP Clinical Respiratory Specialist- COPD Education Important Milestones July 2011-
See page 331 of HEDIS 2013 Tech Specs Vol 2. HEDIS specs apply to plans. RARE applies to hospitals. Plan All-Cause Readmissions (PCR) *++
 *++") Hospitalizations Inpatient Utilization General Hospital/Acute Care (IPU) * This measure summarizes utilization of acute inpatient care and services in the following categories: Total inpatient. Medicine.
Hospitalizations Inpatient Utilization General Hospital/Acute Care (IPU) * This measure summarizes utilization of acute inpatient care and services in the following categories: Total inpatient. Medicine.
Medicare Advantage Plans: An Overview
 Medicare Advantage Plans: An Overview June 2014 Prepared by: Penny Finch, Benefits Consultant Copyright 2014 by The Segal Group, Inc. All rights reserved. 5432273.1 CONTENTS Medicare 101 Understanding
Medicare Advantage Plans: An Overview June 2014 Prepared by: Penny Finch, Benefits Consultant Copyright 2014 by The Segal Group, Inc. All rights reserved. 5432273.1 CONTENTS Medicare 101 Understanding
Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Summit Health Plan of Florida
 Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Summit Health Plan of Florida Medicare Quality Management Program Overview Quality Improvement (QI) Overview At Coventry, we
Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Summit Health Plan of Florida Medicare Quality Management Program Overview Quality Improvement (QI) Overview At Coventry, we
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.9 Case Management Services G.12 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.9 Case Management Services G.12 Special Needs Services
A white paper. Collaborative Accountable Care. CIGNA s Approach to Accountable Care Organizations. 841282 a 11/11
 A white paper Collaborative Accountable Care CIGNA s Approach to Accountable Care Organizations 841282 a 11/11 Transforming the Health Care System Successfully transforming the U.S. health care system
A white paper Collaborative Accountable Care CIGNA s Approach to Accountable Care Organizations 841282 a 11/11 Transforming the Health Care System Successfully transforming the U.S. health care system
ACO CASE STUDY METRO HEALTH: GRAND RAPIDS, MICHIGAN
 ACO CASE STUDY METRO HEALTH: GRAND RAPIDS, MICHIGAN January 2011 ACO CASE STUDY METRO HEALTH: GRAND RAPIDS, MICHIGAN Prepared by: Keith D. Moore / kmoore@mcmanisconsulting.com & Dean C. Coddington / dcoddington@mcmanisconsulting.com
ACO CASE STUDY METRO HEALTH: GRAND RAPIDS, MICHIGAN January 2011 ACO CASE STUDY METRO HEALTH: GRAND RAPIDS, MICHIGAN Prepared by: Keith D. Moore / kmoore@mcmanisconsulting.com & Dean C. Coddington / dcoddington@mcmanisconsulting.com
Medicare Risk Adjustment and You. Health Plan of San Mateo Spring 2009
 Medicare Risk Adjustment and You Health Plan of San Mateo Spring 2009 Background CMS reimburses health plans on a risk-adjusted basis: The sicker a member is expected to be, the more CMS pays a plan, which
Medicare Risk Adjustment and You Health Plan of San Mateo Spring 2009 Background CMS reimburses health plans on a risk-adjusted basis: The sicker a member is expected to be, the more CMS pays a plan, which
caresy caresync Chronic Care Management
 caresy Chronic Care Management THE PROBLEM Chronic diseases and conditions, including heart disease, diabetes, COPD and obesity, are among the most common, expensive, and preventable health problems in
caresy Chronic Care Management THE PROBLEM Chronic diseases and conditions, including heart disease, diabetes, COPD and obesity, are among the most common, expensive, and preventable health problems in
Analytic-Driven Quality Keys Success in Risk-Based Contracts. Ross Gustafson, Vice President Allina Performance Resources, Health Catalyst
 Analytic-Driven Quality Keys Success in Risk-Based Contracts March 2 nd, 2016 Ross Gustafson, Vice President Allina Performance Resources, Health Catalyst Brian Rice, Vice President Network/ACO Integration,
Analytic-Driven Quality Keys Success in Risk-Based Contracts March 2 nd, 2016 Ross Gustafson, Vice President Allina Performance Resources, Health Catalyst Brian Rice, Vice President Network/ACO Integration,