SECTION 1 General Principles
|
|
|
- Valentine Morris
- 7 years ago
- Views:
Transcription
1 SECTION 1 General Principles Pierre-Alain Clavien Michael G. Sarr

2 Introduction Pierre A. Clavien, Michael G. Sarr A competent surgeon must be aware of all the general aspects of a surgical procedure to be able to perform specific interventions successfully and expeditiously. The old adage that exposure, exposure, and exposure are the three most important factors for the good outcome of a surgical procedure remains true for both open and laparoscopic approaches. Each procedure must start with careful positioning of the patient prior to wide disinfection of the operative field, draping, and incision. The first chapter covers the various options for positioning of the patient on the operating table and describes the incisions that are available to enter the abdominal cavity. The second chapter focuses on different principles of exposure through the use of various types of retractors, providing examples of the most commonly used retractors. The third chapter addresses the use of mechanical staplers. Currently, staplers are increasingly being used for many open and laparoscopic procedures, and the industry has partnered actively with the surgical field in developing new devices enabling sophisticated maneuvers, often to reach otherwise small and inaccessible areas. Proper knowledge of the general principles of the use and function of mechanical staplers is mandatory for modern surgery, because their misuse may result in devastating complications such as anastomotic leakage or bleeding. Finally, while Billroth claimed more than a century ago that drainage saves many lives, the use of the time-honored surgical drain has changed dramatically, because accumulating studies have shown convincingly that drains are often useless or even harmful in many procedures. Open drains are rarely needed today. The last chapter presents the principles of the various types of drains including a table of evidence-based utility of drains for upper abdominal surgery. These chapters covering the general aspects of surgery were prepared in a simple, yet comprehensive manner. We believe that the didactic and basic information provided in these introductory chapters of the Atlas will be of value for both trainees and specialized surgeons.

3 Positioning and Accesses Yvonne Knoblauch, Dieter Hahnloser Positioning Correct and stable positioning of the patient is the first step for a successful operation. Safe arm and leg positioning are crucial in preventing pressure lesions, such as ulnar or peroneal neuropathy. Supine Position The supine position is used for most abdominal procedures. The arms can be left out (A-1) or kept close to the body (A-2), depending on the type of operation to be performed. Anchor the patient s legs and/or ankles with a strap in case tilt is required Protect arms with a pillowcase, gauze sponge, or silicone pad Avoid traction on the brachial plexus (abduction of the shoulder should be <90 ) A-1 A-2
 or kept close to the body (A-2), depending on the type of operation to be performed.")
4 6 SECTION 1 General Principles French Position The French position is one possible patient position for a laparoscopic cholecystectomy (the American supine position with both arms tucked alongside the body being the other). The patient s legs are placed in stirrups or supported under the knee Legs need to be placed horizontally or slightly declining to allow free movements with laparoscopic tools Avoid any pressure on the peroneal (lateral popliteal) nerve

5 Positioning and Accesses 7 Beach Chair Position The beach chair position is used for most laparoscopic obesity surgery procedures Requires a special weight-bearing table The patient is sitting on the table Avoid any pressure on arms, the brachial plexus, and the peroneal (lateral popliteal) nerve

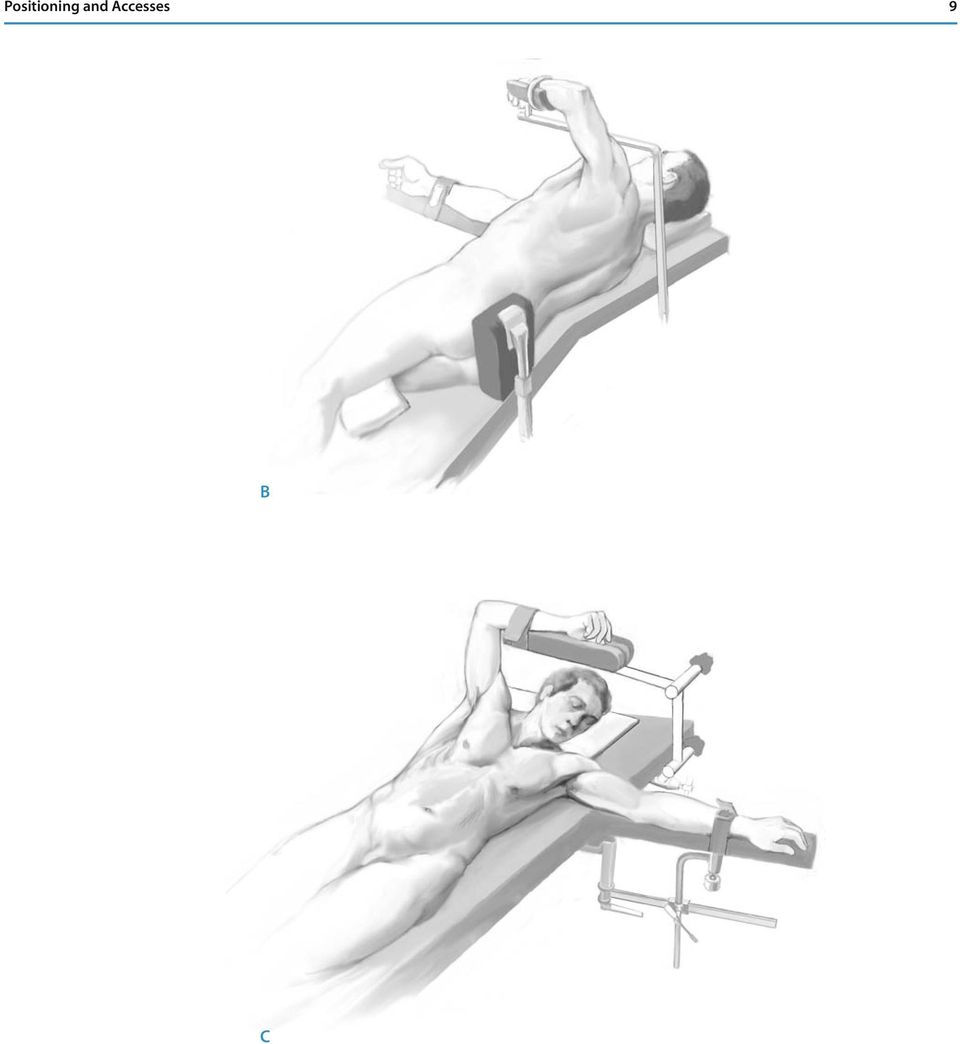
6 8 SECTION 1 General Principles Positioning for Esophageal Surgery For esophageal resection and reconstruction, several approaches can be used. Depending on the location of the disease and the surgical approach, the positioning is adapted accordingly. The positions used are: a) Supine position with overextended thoracic spine, the head rotated to the right and extended. The right arm is left out and the left arm is tucked alongside the body (A). This position is commonly used for transhiatal esophagectomies enabling: Good exposure of the upper abdomen Good exposure for the cervical anastomosis b) Right or left lateral decubitus (B) For the intrathoracic anastomosis Procedures on the upper thoracic esophagus are approached via a right posterolateral thoracotomy, and similar procedures on the lower esophagus are best approached through the same incision on the left side The table is slightly kinked at the thoracic level, further opening the thoracic cavity after thoracotomy c) 45 lateral decubitus or screw position (C) An advantage is that the abdominal, the thoracic, and/or cervical phase of the procedure can be performed without changing the position For optimal access, the operating table can be tilted The main disadvantage is a more limited exposure A
 Right or left lateral decubitus (B) For the")
7 Positioning and Accesses 9 B C
8 10 SECTION 1 General Principles Incisions Abdomen The choice of the approach for entering the abdominal cavity depends upon: The accuracy of the preoperative diagnosis The location and extent of the disease Previous scars The requirement of a possible extension of the incision Anatomic structures, such as skin, fascia, muscles, nerves, and blood vessels. The abdominal wall should stay functional. Whenever possible, incisions are placed along the skin split lines, also called the lines of Langer, and muscles and fascia are divided along their fibers Mark the incision prior to cutting to prevent malpositioning Midline Incision The midline incision is the most expedient choice for opening the abdomen and provides unrestricted access, regardless of the patient s size or shape (including exposure of the pelvis). The advantages of a midline incision are: Can be extended into a median sternotomy Minimal blood loss No muscle fibers are divided No nerves are injured Is suitable for repeated celiotomies Offers best exposure in an emergency situation with unclear diagnosis The Steps Place skin incision exactly in the midline, above and below the umbilicus from the tip of the xiphoid to the pubis (extension as needed) (A-1) Deflect the incision around the umbilicus to the left or the right. The evasion of the umbilicus on the left side is preferred, because of possible rudimentary umbilical vessels. In general, use the opposite side of the umbilicus if an ostomy is planned The scalpel or the cautery can be used all the way By pulling the wound, the fat spreads and the midline plane separates down to the fascia (A-2, A-3) Apply digital pressure to minimize bleeding Incise the fascia with the scalpel or cautery just above or below the umbilicus, as the linea alba is widest around the umbilicus Gently lift up the peritoneum with pickups before opening to avoid small bowel lesions (A-4) Care to incise the linea alba without exposing the rectus muscles markedly facilitates the closure

9 Positioning and Accesses 11 A-1 A-3 A-2 A-4

10 12 SECTION 1 General Principles Subcostal Incision (A-1) The subcostal incision is usually made for cholecystectomy or common bile duct exploration (right subcostal incision) and for elective splenectomy (left subcostal incision). The major advantage of the subcostal incisions over the upper midline incision are greater lateral exposure and less pain. The disadvantage is that the operation takes longer, because there are more layers to close. The subcostal incision generally heals well with little risk of hernia formation. The Steps Place skin incision two finger breadths below the costal margin. This facilitates closure so that the incision line is not on or over the costal margin Incise the anterior and posterior sheet of the rectus muscle. The muscle is cut slowly with the cautery (A-2); care should be taken to ligate or cauterize the inferior epigastric vessels Laterally, the fascia of the transverse muscle may need to be cut Try not to incise the fascia in the midline, but if necessary, extend the incision medially A-1 A-2

11 Positioning and Accesses 13 Bilateral Subcostal Incision The bilateral subcostal incision is used to access the liver for transplant and major liver resections. Also, most pancreas resections are performed with this incision. The exposure is often helped with a vertical extension to the xiphoid (the so-called Mercedes star incision). The Steps Incision of skin and fascia as described above For pancreas resections, the incision is generally placed three to four finger breadths below the costal margin Mobilization of the liver begins with the division of the falciform ligament (the liver s reflection of peritoneum with the anterior wall) Division of the round ligament (a fibrous cord resulting from the obliteration of the umbilical vein), which should be ligated to avoid bleeding, particularly in the presence of portal hypertension It is preferable to mobilize the liver prior to the use of stationary retractors to reduce the necessity of frequent repositioning J-shaped Incision The J-shaped incision is used most frequently for surgery on the right liver (see page 374 ). This incision provides a particularly good access to the area between the inferior vena cava and the right hepatic vein. The J-shaped incision can be extended laterally to a thoracotomy for better exposure.
 Division of the round ligament (a fibrous cord resulting from the obliteration of the")
12 14 SECTION 1 General Principles Esophageal Surgery Like the various positions used in esophageal surgery, there are different incisions used depending on the location of the disease, the level of the anastomosis, and the surgeon s preference. Most of the time, a combination of two or more of the following incisions are used: a) Upper midline laparotomy As described in the previous section on the abdomen Can be combined with a transverse laparotomy for better exposure b) Thoracotomy Anterolateral: skin incision usually in the fourth or fifth intercostal space Posterolateral: skin incision in the seventh intercostal space at the angle of the scapula (A-1). A paravertebral or anterior extension is possible The intercostal muscle is freed from the upper border of the rib (avoids damaging the intercostal nerve and blood vessels, which lie behind the inferior border of the rib) (A-2) The parietal pleura is opened with scissors, and the ribs are separated with a retractor c) Cervical incision (B-1) Incision along the anterior border of the sternocleidomastoid muscle (B-2) Division of the platysma in the direction of the incision The omohyoid muscle (B-3) and, if necessary, the inferior thyroid artery and/or middle thyroid vein are divided to provide clear exposure The sternocleidomastoid muscle and carotid sheath and its contents are retracted laterally, and the trachea and larynx are retracted medially No retractor should be placed against the recurrent laryngeal nerve in the tracheoesophageal groove during the entire cervical phase of the procedure For better exposure, the medial part of the sternocleidomastoid muscle can be cut inferiorly close to the clavicle bone Identification of the flat, decompressed esophagus can be helped by inserting a large tube into the esophagus by the anesthesiologist In patients with a bull neck habitus or with osteoarthritis preventing extension of the neck, a partial upper sternal split can provide the prerequisite access to the high retrosternal esophagus
 Thoracotomy Anterolateral: skin incision usually in the fourth or fifth intercostal space Posterolateral: skin incision in the seventh intercostal space at the angle")
13 Positioning and Accesses 15 B-1 A-1 B-2 A-2 B-3

14 16 SECTION 1 General Principles Laparoscopic Surgery Establishing Pneumoperitoneum Pneumoperitoneum can be established using a Veress needle or by an open approach. The open technique is generally preferred, as it minimizes the risks of inherent lesions to the small bowel. However, in obese patients, the Veress needle is used, as the thick subcutis does not allow visualization of the fascia through a 1 2cm incision. Gaining Access with a Veress Needle Incision of the skin (generally infraumbilical in the midline) and blunt dissection of the subcutaneous tissue The fascia is grasped with a hook retractor or a Kocher clamp and is pulled anteriorly (A-1) Before inserting the Veress needle, its correct functioning must be checked Insertion of the needle at a 90 angle to the abdominal wall. As the needle s springloaded safety mechanism crosses the abdominal fascia and then the peritoneum, two clicks are heard and are usually felt Verification of the needle s intraperitoneal location by injecting 3ml of saline with no resistance (A-2) followed by the hanging drop test (A-3) (i.e., a drop of saline is placed on the top of the needle, which is sucked into the needle when the abdominal fascia is lifted up) Pneumoperitoneum. When a pressure of 13 15mmHg is reached, the Veress needle is withdrawn, and a sharp-tipped camera trocar is blindly inserted through the same incision A-2 A-1 A-3
 and blunt dissection of the subcutaneous tissue The fascia is grasped with a hook retractor or a")
15 Positioning and Accesses 17 Gaining Access with the Open Technique Incision of the skin (generally infraumbilical in the midline) and blunt dissection of the subcutaneous tissue Incision of the fascia (1 2cm) and opening of the peritoneum with scissors (two sutures can be placed to lift up the abdominal wall and to later secure the port) (A-1) Entry into the abdominal cavity is easily confirmed by inserting a finger A blunt-tipped camera trocar is inserted and fixed with the two sutures if needed (A-2) A-1 A-2

16 18 SECTION 1 Placement of Accessory Ports General Principles Selecting the insertion sites of working trocars is dependent on the procedure to be performed and also depends on the surgeon s preference, the patient s body habitus, and the presence or absence of previous scars or intra-abdominal adhesions. The Steps The size of the skin incision must be planned carefully. If the incision is too small, friction will develop between the skin and the port, and greater force will be required for insertion, which will increase the risk of uncontrolled insertion. If the incision is too large, gas may leak and the port may dislocate more easily Transillumination of the skin can help to avoid cutting through major blood vessels (A-1) The trocar is optimally inserted by holding it between the index and the middle fingers. The shaft of the trocar should also be supported by the opposite hand as the body wall is traversed (A-2) A-1 A-2
 The trocar is optimally")
17 Positioning and Accesses 19 Closures General the length of the suture material should be 4:1 to the length of the wound avoid excessive tension on the suture closure of the fascial edgestraction as it may compromise vascularization of the wound edges below the umbilicus, the posterior fascia (rostral to the smi-circular line caudal to which there is no posterior rectus fascia) and then the anterior fascia of the rectus abdominis muscle can bei closed as separate layers Grasp the needle with the tip of the instrument Midline Laparotomy The fascia is closed with a running loop of monofilament, absorbable suture material (e.g., PDS II-1 loop or Maxon-1 loop) with or without inclusion of the peritoneum The subcutaneous fatty layer is not closed and subcutaneous drains are rarely needed The skin is preferably closed with a running intracutaneous absorbable monofilament suture (e.g., Maxon 5-0) or with staples Subcostal Incision In contrast to the midline laparotomy, the fascia should be closed in two layers Trocar Wound Closure Ports are removed under direct vision with the camera and port sites should be routinely watched for 10s to exclude port site bleeding All fascial defects of trocars greater than 5mm are closed with absorbable sutures (e.g., Vicryl 0) The skin is closed with interrupted mattress sutures (e.g., Dermalon 4-0) or with staples Tricks of the Senior Surgeon The surgeon should personally check the correct positioning of the patient and the adequate protection of the extremities before draping. Marking the incision site before the beginning of the procedure is useful for teaching and prevents malpositioning. The incision should always be large enough to guarantee good visualization of the operative fields and to guarantee a safe and efficient operation Avoid extensive traction on the wound edges, as it may compromise healing. Place trocars carefully according to the operative need and according to the body habitus of the patient (eg. obesity). Visualize the port site for at least 10s after removal of the trocar to check for bleeding.

18

26. Port Site Closure Methods and Hernia Prevention
 26. Port Site Closure Methods and Hernia Prevention Chandrakanth Are, M.D. Mark A. Talamini, M.D. Laparoscopic port site hernias have been frequently reported (incidence of 0.02% 5% with an average of
26. Port Site Closure Methods and Hernia Prevention Chandrakanth Are, M.D. Mark A. Talamini, M.D. Laparoscopic port site hernias have been frequently reported (incidence of 0.02% 5% with an average of
The Abdominal Wall And Hernias. Stanley Kurek, DO, FACS Associate Professor of Surgery UTMCK
 The Abdominal Wall And Hernias Stanley Kurek, DO, FACS Associate Professor of Surgery UTMCK The Abdominal Wall The structure of the abdominal wall is similar in principle to the thoracic wall. There are
The Abdominal Wall And Hernias Stanley Kurek, DO, FACS Associate Professor of Surgery UTMCK The Abdominal Wall The structure of the abdominal wall is similar in principle to the thoracic wall. There are
The Whipple Procedure. Sally Hodges, Ph.D.(c) Given the length and difficulty of the procedure, regardless of the diagnosis, certain
 Given the length and difficulty of the procedure, regardless of the diagnosis, certain") The Whipple Procedure Sally Hodges, Ph.D.(c) Preoperative procedures Given the length and difficulty of the procedure, regardless of the diagnosis, certain assurances must occur prior to offering a patient
The Whipple Procedure Sally Hodges, Ph.D.(c) Preoperative procedures Given the length and difficulty of the procedure, regardless of the diagnosis, certain assurances must occur prior to offering a patient
SILS. Port Insertion By Homero Rivas, MD, MBA, FACS. Single incision. Single port. Simple choice.
 SILS Port Insertion By Homero Rivas, MD, MBA, FACS Single incision. Single port. Simple choice. SILS Port Insertion By Homero Rivas, MD, MBA, FACS For the last 20 years, there has given surgical procedure.
SILS Port Insertion By Homero Rivas, MD, MBA, FACS Single incision. Single port. Simple choice. SILS Port Insertion By Homero Rivas, MD, MBA, FACS For the last 20 years, there has given surgical procedure.
RADICAL HYSTERECTOMY IN ROBOTIC SURGERY
 RADICAL HYSTERECTOMY IN ROBOTIC SURGERY FLORENCE BOCHU CENTRE OSCAR LAMBRET LILLE PATRICIA VARUMBEKE CENTRE OSCAR LAMBRET LILLE MELANIE FLAMENT CENTRE OSCAR LAMBRET LILLE More and more centers across the
RADICAL HYSTERECTOMY IN ROBOTIC SURGERY FLORENCE BOCHU CENTRE OSCAR LAMBRET LILLE PATRICIA VARUMBEKE CENTRE OSCAR LAMBRET LILLE MELANIE FLAMENT CENTRE OSCAR LAMBRET LILLE More and more centers across the
Laparoscopic Sleeve gastrectomy
 Restrictive procedure Laparoscopic Sleeve gastrectomy Dr. R. Peterli Professional Education 1 2 Introduction Gastric sleeve resection is the restrictive part of the biliopancreatic diversion duodenal switch,
Restrictive procedure Laparoscopic Sleeve gastrectomy Dr. R. Peterli Professional Education 1 2 Introduction Gastric sleeve resection is the restrictive part of the biliopancreatic diversion duodenal switch,
Instructions for Use
 Pleural Effusion Shunt with External Pump Chamber Catalog No. 42-9005 Instructions for Use Denver Biomedical, Inc. Table of Contents Description 2 Indications 2 Contraindications 2 Warnings 4 Cautions
Pleural Effusion Shunt with External Pump Chamber Catalog No. 42-9005 Instructions for Use Denver Biomedical, Inc. Table of Contents Description 2 Indications 2 Contraindications 2 Warnings 4 Cautions
Laparoscopic Anatomy of the Pelvis
 2 Laparoscopic Anatomy of the Pelvis Intra-Abdominal Anatomy of the Male Pelvic Region Bladder Medial Umbilical Ligaments Lateral Umbilical Ligaments Spermatic Cords Iliac Vessels Ureters Seminal Vesicular
2 Laparoscopic Anatomy of the Pelvis Intra-Abdominal Anatomy of the Male Pelvic Region Bladder Medial Umbilical Ligaments Lateral Umbilical Ligaments Spermatic Cords Iliac Vessels Ureters Seminal Vesicular
Integumentary System Individual Exercises
 Integumentary System Individual Exercises 1. A physician performs an incision and drainage of a subcutaneous abscess in his office for a particularly uncooperative established patient. How should this
Integumentary System Individual Exercises 1. A physician performs an incision and drainage of a subcutaneous abscess in his office for a particularly uncooperative established patient. How should this
Case 2. 30 year old involved in a MVA complaining of chest pain. Bruising over the right upper chest. Your Diagnosis
 Case 2 30 year old involved in a MVA complaining of chest pain. Bruising over the right upper chest. Your Diagnosis Diagnosis: Posterior Sterno-clavicular dislocation [PSCD] A posterior sterno-clavicular
Case 2 30 year old involved in a MVA complaining of chest pain. Bruising over the right upper chest. Your Diagnosis Diagnosis: Posterior Sterno-clavicular dislocation [PSCD] A posterior sterno-clavicular
PRACTICE GUIDELINE TITLE: INTRAVENOUS LINE INSERTION: PERIPHERAL AND CENTRAL
 PRACTICE GUIDELINE Effective Date: 9-17-04 Manual Reference: Deaconess Trauma Services TITLE: INTRAVENOUS LINE INSERTION: PERIPHERAL AND CENTRAL PURPOSE: To outline the indications and options for intravenous
PRACTICE GUIDELINE Effective Date: 9-17-04 Manual Reference: Deaconess Trauma Services TITLE: INTRAVENOUS LINE INSERTION: PERIPHERAL AND CENTRAL PURPOSE: To outline the indications and options for intravenous
Abdominal Pedicle Flaps To The Hand And Forearm John C. Kelleher M.D., F.A.C.S.
 Abdominal Pedicle Flaps To The Hand And Forearm John C. Kelleher M.D., F.A.C.S. Global-HELP Publications Chapter Eight: TECHNICAL REQUIREMENTS FOR FORMATION OF A TUBED PEDICLE FLAP Creating a tube pedicle
Abdominal Pedicle Flaps To The Hand And Forearm John C. Kelleher M.D., F.A.C.S. Global-HELP Publications Chapter Eight: TECHNICAL REQUIREMENTS FOR FORMATION OF A TUBED PEDICLE FLAP Creating a tube pedicle
Open Ventral Hernia Repair
 Ventral Hernias Open Ventral Hernia Repair UCSF Postgraduate Course in General Surgery Maui, HI March 21, 2011 Hobart W. Harris, MD, MPH Ventral Hernias: National Experience Occur following 11-23% of laparotomies,
Ventral Hernias Open Ventral Hernia Repair UCSF Postgraduate Course in General Surgery Maui, HI March 21, 2011 Hobart W. Harris, MD, MPH Ventral Hernias: National Experience Occur following 11-23% of laparotomies,
PERCUTANEOUS PD CATHETER IMPLANTATION SYSTEM
 Place on Patient s Cranial Border of the Pubic Symphysis IMPLANTATION STENCIL Classic Exit Cuff Site PERCUTANEOUS PD CATHETER IMPLANTATION SYSTEM INSTRUCTIONS FOR USE VP 511 and VP-511M Implantation System
Place on Patient s Cranial Border of the Pubic Symphysis IMPLANTATION STENCIL Classic Exit Cuff Site PERCUTANEOUS PD CATHETER IMPLANTATION SYSTEM INSTRUCTIONS FOR USE VP 511 and VP-511M Implantation System
Ventral Hernia Repair
 Ventral Hernia Repair Open and Laparoscopic Ventral Hernia Repair Technique Guide Ventrio ST Hernia Patch Ventrio Hernia Patch This Technique Guide contains the opinions of and personal surgical techniques
Ventral Hernia Repair Open and Laparoscopic Ventral Hernia Repair Technique Guide Ventrio ST Hernia Patch Ventrio Hernia Patch This Technique Guide contains the opinions of and personal surgical techniques
Minimally Invasive Spine Surgery
 Chapter 1 Minimally Invasive Spine Surgery 1 H.M. Mayer Primum non nocere First do no harm In the long history of surgery it always has been a basic principle to restrict the iatrogenic trauma done to
Chapter 1 Minimally Invasive Spine Surgery 1 H.M. Mayer Primum non nocere First do no harm In the long history of surgery it always has been a basic principle to restrict the iatrogenic trauma done to
ANTERIOR LUMBAR INTERBODY FUSION (ALIF) Basic Anatomical Landmarks: Anterior Lumbar Spine
 Basic Anatomical Landmarks: Anterior Lumbar Spine") (ALIF) Anterior In human anatomy, referring to the front surface of the body or the position of one structure relative to another Lumbar Relating to the loins or the section of the back and sides between
(ALIF) Anterior In human anatomy, referring to the front surface of the body or the position of one structure relative to another Lumbar Relating to the loins or the section of the back and sides between
LUMBAR LAMINECTOMY AND DISCECTOMY. Basic Anatomical Landmarks: Posterior View Lumbar Spine
 Lumbar Relating to the loins or the section of the back and sides between the ribs and the pelvis. In the spinal column, the last five vertebrae (from superior to inferior, L1-L5) Laminectomy Surgical
Lumbar Relating to the loins or the section of the back and sides between the ribs and the pelvis. In the spinal column, the last five vertebrae (from superior to inferior, L1-L5) Laminectomy Surgical
PHaSES: Practical Hands-on Surgical Education System
 U.S. Toll Free 866-GOLIMBS PHaSES Range PHaSES: Practical Hands-on Surgical Education System Limbs & Things is pleased to introduce the PHaSES Range. The range is based upon our well known basic & general
U.S. Toll Free 866-GOLIMBS PHaSES Range PHaSES: Practical Hands-on Surgical Education System Limbs & Things is pleased to introduce the PHaSES Range. The range is based upon our well known basic & general
Anatomy and Physiology 121: Muscles of the Human Body
 Epicranius Anatomy and Physiology 121: Muscles of the Human Body Covers upper cranium Raises eyebrows, surprise, headaches Parts Frontalis Occipitalis Epicranial aponeurosis Orbicularis oculi Ring (sphincter)
Epicranius Anatomy and Physiology 121: Muscles of the Human Body Covers upper cranium Raises eyebrows, surprise, headaches Parts Frontalis Occipitalis Epicranial aponeurosis Orbicularis oculi Ring (sphincter)
TRANSVERSUS ABDOMINIS PLANE (TAP) BLOCK
 BLOCK") THE JOURNAL OF NEW YORK SCHOOL M a y 2 0 0 9 V o l u m e OF REGIONAL ANESTHESIA 1 2 TRANSVERSUS ABDOMINIS PLANE (TAP) BLOCK By Karim Mukhtar, MB BCh, MSc, FRCA Royal Liverpool and Broadgreen University
THE JOURNAL OF NEW YORK SCHOOL M a y 2 0 0 9 V o l u m e OF REGIONAL ANESTHESIA 1 2 TRANSVERSUS ABDOMINIS PLANE (TAP) BLOCK By Karim Mukhtar, MB BCh, MSc, FRCA Royal Liverpool and Broadgreen University
Laparoscopic extended right hemicolectomy for transverse colon
 Laparoscopic extended right hemicolectomy for transverse colon cancer Elsa B. Valsdottir, MD Department of General Surgery University Hospital of Iceland Hringbraut 101 Reykjavik Iceland Phone +354 543
Laparoscopic extended right hemicolectomy for transverse colon cancer Elsa B. Valsdottir, MD Department of General Surgery University Hospital of Iceland Hringbraut 101 Reykjavik Iceland Phone +354 543
ANTERIOR CERVICAL DISCECTOMY AND FUSION. Basic Anatomical Landmarks: Anterior Cervical Spine
 Anterior In the human anatomy, referring to the front surface of the body or position of one structure relative to another Cervical Relating to the neck, in the spine relating to the first seven vertebrae
Anterior In the human anatomy, referring to the front surface of the body or position of one structure relative to another Cervical Relating to the neck, in the spine relating to the first seven vertebrae
MODIFIED STRAYER GASTROCNEMIUS RECESSION: A Technique Guide for the Supine Positioned Patient
 C H A P T E R 4 5 MODIFIED STRAYER GASTROCNEMIUS RECESSION: A Technique Guide for the Supine Positioned Patient M. Jay Groves, IV, DPM Gastrosoleal equinus is a common deforming force on the foot and ankle.
C H A P T E R 4 5 MODIFIED STRAYER GASTROCNEMIUS RECESSION: A Technique Guide for the Supine Positioned Patient M. Jay Groves, IV, DPM Gastrosoleal equinus is a common deforming force on the foot and ankle.
Surgical scissors and forceps Product List
 Surgical scissors and forceps Product List Sr. No Items Picture of Product Product specification 1 Grasping forceps-- 5 MM Grasping forceps are used to remove stones and retrieve foreign objects under
Surgical scissors and forceps Product List Sr. No Items Picture of Product Product specification 1 Grasping forceps-- 5 MM Grasping forceps are used to remove stones and retrieve foreign objects under
Cracking CPT Codes: An Interactive Discussion Presented by Tom Loughrey, CCS-P. Jumping Right In!
 Cracking CPT Codes: An Interactive Discussion Presented by Tom Loughrey, CCS-P Jumping Right In! Code the following: 38 year old female for right breast biopsy with percutaneous needle core using image
Cracking CPT Codes: An Interactive Discussion Presented by Tom Loughrey, CCS-P Jumping Right In! Code the following: 38 year old female for right breast biopsy with percutaneous needle core using image
Muscles of the Spinal Column. Chapter 12
 Muscles of the Spinal Column Chapter 12 Cervical Muscles Splenius Splenius (capitis and cervicis) Origin: Cervicis spinous process of T3-T6 Capitis - lower half of ligmentum nuchea & spinous process of
Muscles of the Spinal Column Chapter 12 Cervical Muscles Splenius Splenius (capitis and cervicis) Origin: Cervicis spinous process of T3-T6 Capitis - lower half of ligmentum nuchea & spinous process of
FREEDOM INGUINAL Hernia Repair System TECHNIQUE GUIDE
 FREEDOM INGUINAL Hernia Repair System TECHNIQUE GUIDE The following describes the open surgical preparation and implantation technique for the Freedom Inguinal Hernia Repair System. 1) Anesthesia can be
FREEDOM INGUINAL Hernia Repair System TECHNIQUE GUIDE The following describes the open surgical preparation and implantation technique for the Freedom Inguinal Hernia Repair System. 1) Anesthesia can be
Minimally Invasive Hip Replacement through the Direct Lateral Approach
 Surgical Technique INNOVATIONS IN MINIMALLY INVASIVE JOINT SURGERY Minimally Invasive Hip Replacement through the Direct Lateral Approach *smith&nephew Introduction Prosthetic replacement of the hip joint
Surgical Technique INNOVATIONS IN MINIMALLY INVASIVE JOINT SURGERY Minimally Invasive Hip Replacement through the Direct Lateral Approach *smith&nephew Introduction Prosthetic replacement of the hip joint
Lesions, and Masses, and Tumors Oh My!!
 Lesions, and Masses, and Tumors Oh My!! Presented by: Susan Ward, CPC, CPC-H, CPC-I, CPCD, CEMC, CPRC 1 1 CPT GUIDELINES Agenda CPT DEFINITIONS OP REPORT CASES 2 Definitions Cyst - a closed sac having
Lesions, and Masses, and Tumors Oh My!! Presented by: Susan Ward, CPC, CPC-H, CPC-I, CPCD, CEMC, CPRC 1 1 CPT GUIDELINES Agenda CPT DEFINITIONS OP REPORT CASES 2 Definitions Cyst - a closed sac having
Bankart Repair using the Smith & Nephew BIORAPTOR 2.9 Suture Anchor
 Shoulder Series Technique Guide *smith&nephew BIORAPTOR 2.9 Suture Anchor Bankart Repair using the Smith & Nephew BIORAPTOR 2.9 Suture Anchor Gary M. Gartsman, M.D. Introduction Arthroscopic studies of
Shoulder Series Technique Guide *smith&nephew BIORAPTOR 2.9 Suture Anchor Bankart Repair using the Smith & Nephew BIORAPTOR 2.9 Suture Anchor Gary M. Gartsman, M.D. Introduction Arthroscopic studies of
Clarification of Terms
 Shoulder Girdle Clarification of Terms Shoulder girdle = scapula and clavicle Shoulder joint (glenohumeral joint) = scapula and humerus What is the purpose (or function) of the shoulder and entire upper
Shoulder Girdle Clarification of Terms Shoulder girdle = scapula and clavicle Shoulder joint (glenohumeral joint) = scapula and humerus What is the purpose (or function) of the shoulder and entire upper
THE BENJAMIN INSTITUTE PRESENTS. Excerpt from Listen To Your Pain. Assessment & Treatment of. Low Back Pain. Ben E. Benjamin, Ph.D.
 THE BENJAMIN INSTITUTE PRESENTS Excerpt from Listen To Your Pain Assessment & Treatment of Low Back Pain A B E N J A M I N I N S T I T U T E E B O O K Ben E. Benjamin, Ph.D. 2 THERAPIST/CLIENT MANUAL The
THE BENJAMIN INSTITUTE PRESENTS Excerpt from Listen To Your Pain Assessment & Treatment of Low Back Pain A B E N J A M I N I N S T I T U T E E B O O K Ben E. Benjamin, Ph.D. 2 THERAPIST/CLIENT MANUAL The
Sonography of Hernias
 Sonography of Hernias Cindy Rapp BS, RDMS, FAIUM, FSDMS Sr. Clinical Marketing Manager Toshiba America Medical Systems Tustin, California What is a hernia? A hernia is a protrusion of an organ or tissue
Sonography of Hernias Cindy Rapp BS, RDMS, FAIUM, FSDMS Sr. Clinical Marketing Manager Toshiba America Medical Systems Tustin, California What is a hernia? A hernia is a protrusion of an organ or tissue
X-Plain Inguinal Hernia Repair Reference Summary
 X-Plain Inguinal Hernia Repair Reference Summary Introduction Hernias are common conditions that affect men and women of all ages. Your doctor may recommend a hernia operation. The decision whether or
X-Plain Inguinal Hernia Repair Reference Summary Introduction Hernias are common conditions that affect men and women of all ages. Your doctor may recommend a hernia operation. The decision whether or
24. Implications of Subcutaneous Emphysema and How to Avoid and/or Limit Its Development
 24. Implications of Subcutaneous Emphysema and How to Avoid and/or Limit Its Development Kirk A. Ludwig, M.D. There are two basic means of providing exposure within the abdominal cavity for laparoscopic
24. Implications of Subcutaneous Emphysema and How to Avoid and/or Limit Its Development Kirk A. Ludwig, M.D. There are two basic means of providing exposure within the abdominal cavity for laparoscopic
THORACIC OUTLET SYNDROME
 THORACIC OUTLET SYNDROME The Problem The term thoracic outlet syndrome is used to describe a condition of compression of the nerves and/or blood vessels in the region around the neck and collarbone, called
THORACIC OUTLET SYNDROME The Problem The term thoracic outlet syndrome is used to describe a condition of compression of the nerves and/or blood vessels in the region around the neck and collarbone, called
Surgical Art. Formulaic Drawing Method. DRAWING WORKSHOP Learning to sketch for patient notes
 DRAWING WORKSHOP Learning to sketch for patient notes Surgical Art Formulaic Drawing Method Formulaic figure drawing systems involve using abstract rhythms and interlocking shapes to construct the human
DRAWING WORKSHOP Learning to sketch for patient notes Surgical Art Formulaic Drawing Method Formulaic figure drawing systems involve using abstract rhythms and interlocking shapes to construct the human
Spinal Arthrodesis Group Exercises
 Spinal Arthrodesis Group Exercises 1. Two surgeons work together to perform an arthrodesis. Dr. Bonet, a general surgeon, makes the anterior incision to gain access to the spine for the arthrodesis procedure.
Spinal Arthrodesis Group Exercises 1. Two surgeons work together to perform an arthrodesis. Dr. Bonet, a general surgeon, makes the anterior incision to gain access to the spine for the arthrodesis procedure.
Chapter 5. The Shoulder Joint. The Shoulder Joint. Bones. Bones. Bones
 Copyright The McGraw-Hill Companies, Inc. Reprinted by permission. Chapter 5 The Shoulder Joint Structural Kinesiology R.T. Floyd, Ed.D, ATC, CSCS Structural Kinesiology The Shoulder Joint 5-1 The Shoulder
Copyright The McGraw-Hill Companies, Inc. Reprinted by permission. Chapter 5 The Shoulder Joint Structural Kinesiology R.T. Floyd, Ed.D, ATC, CSCS Structural Kinesiology The Shoulder Joint 5-1 The Shoulder
Abdomen X-Ray (AXR) Collimation is ideally from diaphragms to lower border of the symphysis pubis and the lateral skin margins.
 Collimation is ideally from diaphragms to lower border of the symphysis pubis and the lateral skin margins.") Abdomen X-Ray (AXR) Collimation is ideally from diaphragms to lower border of the symphysis pubis and the lateral skin margins. LMP of child-bearing age female patients should be checked. 1. Acute abdomen
Abdomen X-Ray (AXR) Collimation is ideally from diaphragms to lower border of the symphysis pubis and the lateral skin margins. LMP of child-bearing age female patients should be checked. 1. Acute abdomen
X-Plain Subclavian Inserted Central Catheter (SICC Line) Reference Summary
 Reference Summary") X-Plain Subclavian Inserted Central Catheter (SICC Line) Reference Summary Introduction A Subclavian Inserted Central Catheter, or subclavian line, is a long thin hollow tube inserted in a vein under the
X-Plain Subclavian Inserted Central Catheter (SICC Line) Reference Summary Introduction A Subclavian Inserted Central Catheter, or subclavian line, is a long thin hollow tube inserted in a vein under the
Integra. Subtalar MBA and bioblock Implant SURGICAL TECHNIQUE
 Integra Subtalar MBA and bioblock Implant SURGICAL TECHNIQUE Table of contents Introduction Description... 2 Indications... 2 Contraindications... 2 Surgical Technique Step 1: Incision and Dissection...3
Integra Subtalar MBA and bioblock Implant SURGICAL TECHNIQUE Table of contents Introduction Description... 2 Indications... 2 Contraindications... 2 Surgical Technique Step 1: Incision and Dissection...3
Aesculap Spine activ L
 Aesculap Spine activ L Lumbar intervertebral disc prosthesis Operating technique 2 activ L Contents A) Pre-operative planning A.1 Size estimation 4 A.2 Patient positioning 4 B) Approach B.1 Marking the
Aesculap Spine activ L Lumbar intervertebral disc prosthesis Operating technique 2 activ L Contents A) Pre-operative planning A.1 Size estimation 4 A.2 Patient positioning 4 B) Approach B.1 Marking the
Gallbladder Surgery with an Incision (Cholecystectomy)
") Gallbladder Surgery with an Incision (Cholecystectomy) It is normal to have questions about your surgery. This handout gives you information about what will happen to you before, during and after your
Gallbladder Surgery with an Incision (Cholecystectomy) It is normal to have questions about your surgery. This handout gives you information about what will happen to you before, during and after your
Sutures and needles. Sutures
 Sutures and needles Sutures A wide variety of material is available for suturing and ligating tissues. Sutures are selected for use according to the required function. For example, arteries are sutured
Sutures and needles Sutures A wide variety of material is available for suturing and ligating tissues. Sutures are selected for use according to the required function. For example, arteries are sutured
Upper Limb QUESTIONS UPPER LIMB: QUESTIONS
 1 Upper Limb QUESTIONS 1.1 Which of the following statements best describes the scapula? a. It usually overlies the 2nd to 9th ribs. b. The spine continues laterally as the coracoid process. c. The suprascapular
1 Upper Limb QUESTIONS 1.1 Which of the following statements best describes the scapula? a. It usually overlies the 2nd to 9th ribs. b. The spine continues laterally as the coracoid process. c. The suprascapular
by joseph e. muscolino, DO photography by yanik chauvin
 by joseph e. muscolino, DO photography by yanik chauvin body mechanics palpation of the anterior neck ESOUCES For more information go to www.medlineplus.gov and search under anterior neck. The anterior
by joseph e. muscolino, DO photography by yanik chauvin body mechanics palpation of the anterior neck ESOUCES For more information go to www.medlineplus.gov and search under anterior neck. The anterior
Posterior Cervical Decompression
 Posterior Cervical Decompression Spinal Unit Tel: 01473 702032 or 702097 Issue 2: January 2009 Following your recent MRI scan and consultation with your spinal surgeon, you have been diagnosed with a
Posterior Cervical Decompression Spinal Unit Tel: 01473 702032 or 702097 Issue 2: January 2009 Following your recent MRI scan and consultation with your spinal surgeon, you have been diagnosed with a
Spinal Exercise Program/Core Stabilization Program Adapted from The Spine in Sports: Robert G. Watkins
 Spinal Exercise Program/Core Stabilization Program Adapted from The Spine in Sports: Robert G. Watkins Below is a description of a Core Stability Program, designed to improve the strength and coordination
Spinal Exercise Program/Core Stabilization Program Adapted from The Spine in Sports: Robert G. Watkins Below is a description of a Core Stability Program, designed to improve the strength and coordination
Laparoscopic Hernia Repair. Hernia Repair. Laparoscopic Ventral. Several Different Types of Hernia
 Laparoscopic Hernia Repair David B Renton, MD Assistant Professor Department of Surgery The Ohio State University Advantages of Laparoscopic Ventral vs. Open Hernia Repair Lower wound infection rate: 2.6%
Laparoscopic Hernia Repair David B Renton, MD Assistant Professor Department of Surgery The Ohio State University Advantages of Laparoscopic Ventral vs. Open Hernia Repair Lower wound infection rate: 2.6%
Dept. of Medical Imaging University of Ottawa
 ED Visits Related to Bariatric Surgery: Review of Normal Post-Surgical Anatomy as Well as Complications Dept. of Medical Imaging University of Ottawa Disclosures Background Roux-en-Y Gastric Bypass Surgery
ED Visits Related to Bariatric Surgery: Review of Normal Post-Surgical Anatomy as Well as Complications Dept. of Medical Imaging University of Ottawa Disclosures Background Roux-en-Y Gastric Bypass Surgery
Laparoscopic Cholecystectomy (Removal of the Gallbladder)
") Laparoscopic Cholecystectomy (Removal of the Gallbladder) The gall bladder is a small pear-shaped organ that lies in the right upper quadrant of your abdomen under your liver (under your ribs). The liver
Laparoscopic Cholecystectomy (Removal of the Gallbladder) The gall bladder is a small pear-shaped organ that lies in the right upper quadrant of your abdomen under your liver (under your ribs). The liver
PERIPHERALLY INSERTED CENTRAL CATHETERS (PICC) Fong So Kwan APN, Haematology unit Medical Department, QMH
 Fong So Kwan APN, Haematology unit Medical Department, QMH") PERIPHERALLY INSERTED CENTRAL CATHETERS (PICC) Fong So Kwan APN, Haematology unit Medical Department, QMH 1 What is a PICC catheter? Primary vascular access device since their introduction in the mid-1970s,
PERIPHERALLY INSERTED CENTRAL CATHETERS (PICC) Fong So Kwan APN, Haematology unit Medical Department, QMH 1 What is a PICC catheter? Primary vascular access device since their introduction in the mid-1970s,
Medical Terminology, Anatompy & Physiology
 1. Which of the following BEST describes the anatomical position? a. Supine with arms crossed over the chest and knees slightly bent b. Standing, facing forward, with arms raised above the head c. Standing,
1. Which of the following BEST describes the anatomical position? a. Supine with arms crossed over the chest and knees slightly bent b. Standing, facing forward, with arms raised above the head c. Standing,
P REPLACEMENT SURGERY
 P REPLACEMENT SURGERY DIRECT ANTERIOR APPROACH M I N I M I Z I N G R E C O V E R Y. M A X I M I Z I N G R E S U L T S. CENTER FOR MINIMAL INVASIVE JOINT SURGERY 2301 25TH STREET SOUTH FARGO ND 58103 701-241-9300
P REPLACEMENT SURGERY DIRECT ANTERIOR APPROACH M I N I M I Z I N G R E C O V E R Y. M A X I M I Z I N G R E S U L T S. CENTER FOR MINIMAL INVASIVE JOINT SURGERY 2301 25TH STREET SOUTH FARGO ND 58103 701-241-9300
Chapter 7. Expose the Injured Area
 Chapter 7 GUNSHOT WOUNDS KEY FIGURES: Entrance/exit wounds This chapter describes how to treat the external, surface wounds caused by a bullet. The evaluation for underlying injury related to gunshot wounds
Chapter 7 GUNSHOT WOUNDS KEY FIGURES: Entrance/exit wounds This chapter describes how to treat the external, surface wounds caused by a bullet. The evaluation for underlying injury related to gunshot wounds
Significant nerve damage is uncommonly associated with a general anaesthetic
 Risks associated with your anaesthetic Section 10: Nerve damage associated with an operation under general anaesthetic Section 10: Significant nerve damage is uncommonly associated with a general anaesthetic
Risks associated with your anaesthetic Section 10: Nerve damage associated with an operation under general anaesthetic Section 10: Significant nerve damage is uncommonly associated with a general anaesthetic
Laparoscopic Trainer Product Catalog
 Laparoscopic Trainer Product Catalog Laparoscopic Trainer Product Catalog Simsei Table of Contents Laparoscopic Trainers 6 Organ Models 8 Skill Exercises 11 Accessories 12 Additional Information About
Laparoscopic Trainer Product Catalog Laparoscopic Trainer Product Catalog Simsei Table of Contents Laparoscopic Trainers 6 Organ Models 8 Skill Exercises 11 Accessories 12 Additional Information About
KnifeLight. Carpal Tunnel Ligament Release. Operative Technique
 KnifeLight Carpal Tunnel Ligament Release Operative Technique Contents Page 1. Features & Benefits 3 Intended Use and Indications 3 Contraindications 3 Features & Benefits 3 2. Operative Technique 4 Antegrade
KnifeLight Carpal Tunnel Ligament Release Operative Technique Contents Page 1. Features & Benefits 3 Intended Use and Indications 3 Contraindications 3 Features & Benefits 3 2. Operative Technique 4 Antegrade
Arthroscopic Shoulder Instability Repair Using the SUTUREFIX ULTRA Suture Anchor and SUTUREFIX ULTRA Instrumentation System
 *smith&nephew SHOULDER TECHNIQUE GUIDE Arthroscopic Shoulder Instability Repair Using the SUTUREFIX ULTRA Suture Anchor and SUTUREFIX ULTRA Instrumentation System KNEE HIP SHOULDER EXTREMITIES Arthroscopic
*smith&nephew SHOULDER TECHNIQUE GUIDE Arthroscopic Shoulder Instability Repair Using the SUTUREFIX ULTRA Suture Anchor and SUTUREFIX ULTRA Instrumentation System KNEE HIP SHOULDER EXTREMITIES Arthroscopic
Acute abdominal conditions Key Points
 7 Acute abdominal conditions Key Points 7.1 ASSESSMENT AND DIAGNOSIS Referred abdominal pain Fore gut pain (stomach, duodenum, gall bladder) is referred to the upper abdomen Mid gut pain (small intestine,
7 Acute abdominal conditions Key Points 7.1 ASSESSMENT AND DIAGNOSIS Referred abdominal pain Fore gut pain (stomach, duodenum, gall bladder) is referred to the upper abdomen Mid gut pain (small intestine,
SPINE. Postural Malalignments 4/9/2015. Cervical Spine Evaluation. Thoracic Spine Evaluation. Observations. Assess position of head and neck
 SPINE Observations Body type Postural alignments and asymmetries should be observed from all views Assess height differences between anatomical landmarks Figure 25-9 Figure 25-10 Figure 25-11 & 12 Postural
SPINE Observations Body type Postural alignments and asymmetries should be observed from all views Assess height differences between anatomical landmarks Figure 25-9 Figure 25-10 Figure 25-11 & 12 Postural
Patient Information. Posterior Cervical Surgery. Here to help. Respond Deliver & Enable
 Here to help Our Health Information Centre (HIC) provides advice and information on a wide range of health-related topics. We also offer: Services for people with disabilities. Information in large print,
Here to help Our Health Information Centre (HIC) provides advice and information on a wide range of health-related topics. We also offer: Services for people with disabilities. Information in large print,
ABThera Open Abdomen Negative Pressure Therapy for Active Abdominal Therapy. Case Series
 ABThera Open Abdomen Negative Pressure Therapy for Active Abdominal Therapy Case Series Summary of Cases: USER EXPERIENCE The ABThera OA NPT system was found by surgeons to be a convenient and effective
ABThera Open Abdomen Negative Pressure Therapy for Active Abdominal Therapy Case Series Summary of Cases: USER EXPERIENCE The ABThera OA NPT system was found by surgeons to be a convenient and effective
Anatomy & Physiology 120. Lab #7 Muscle Tissue and Skeletal Muscles
 Anatomy & Physiology 120 Lab #7 Muscle Tissue and Skeletal Muscles What you Need to Know Look briefly at the Structure of: 1) Skeletal, 2) Smooth & 3) Cardiac Muscle Naming, Identification, Functions You
Anatomy & Physiology 120 Lab #7 Muscle Tissue and Skeletal Muscles What you Need to Know Look briefly at the Structure of: 1) Skeletal, 2) Smooth & 3) Cardiac Muscle Naming, Identification, Functions You
Clarification of Medicare Benefits Schedule rules for the Transport Accident Commission and WorkSafe Victoria
 Clarification of Medicare Benefits Schedule rules for the Transport Accident Commission and WorkSafe Victoria MAY 2013 When paying the reasonable costs of medical services, the TAC and WorkSafe pay in
Clarification of Medicare Benefits Schedule rules for the Transport Accident Commission and WorkSafe Victoria MAY 2013 When paying the reasonable costs of medical services, the TAC and WorkSafe pay in
Suture Patterns. Objectives. Role of Suture Patterns. Inverting Suture Patterns. Appositional Suture Patterns
 Suture Patterns Objectives Introduction to Surgery Classify suture patterns based on their effect on tissue apposition Describe the steps involved in the accurate placement of basic suture patterns Discuss
Suture Patterns Objectives Introduction to Surgery Classify suture patterns based on their effect on tissue apposition Describe the steps involved in the accurate placement of basic suture patterns Discuss
INFORMATION FOR PATIENTS CONSIDERING LAPAROSCOPIC INGUINAL HERNIA REPAIR
 INFORMATION FOR PATIENTS CONSIDERING A LAPAROSCOPIC INGUINAL HERNIA REPAIR Prepared By Mr Peter Willson Consultant Surgeon Contents 1. Background... 3 2. What is an inguinal Hernia?... 3 3. What are the
INFORMATION FOR PATIENTS CONSIDERING A LAPAROSCOPIC INGUINAL HERNIA REPAIR Prepared By Mr Peter Willson Consultant Surgeon Contents 1. Background... 3 2. What is an inguinal Hernia?... 3 3. What are the
Common Regional Nerve Blocks Quick Guide developed by UWHC Acute Pain Service Jan 2011
 Common Regional Nerve Blocks Quick Guide developed by UWHC Acute Pain Service Jan 2011 A single shot nerve block is the injection of local anesthetic to block a specific nerve distribution. It can be placed
Common Regional Nerve Blocks Quick Guide developed by UWHC Acute Pain Service Jan 2011 A single shot nerve block is the injection of local anesthetic to block a specific nerve distribution. It can be placed
ADVANCEMENTS IN PLANTAR FASCIA SURGERY
 C H A P T E R 3 3 ADVANCEMENTS IN PLANTAR FASCIA SURGERY James L. Bouchard, DPM Andrea Cass, DPM INTRODUCTION It has been estimated that 90% of patients with plantar fasciitis and heel spur syndrome get
C H A P T E R 3 3 ADVANCEMENTS IN PLANTAR FASCIA SURGERY James L. Bouchard, DPM Andrea Cass, DPM INTRODUCTION It has been estimated that 90% of patients with plantar fasciitis and heel spur syndrome get
TRAUMA SURGERY Dr. Michal Cheatham Orlando Regional Health PGY-4
 ROTATION LIAISON: INSTITUTION: LEVEL(S): TRAUMA SURGERY Dr. Michal Cheatham Orlando Regional Health PGY-4 I. GENERAL INFORMATION The General Surgery Department at Orlando Regional Health has three full
ROTATION LIAISON: INSTITUTION: LEVEL(S): TRAUMA SURGERY Dr. Michal Cheatham Orlando Regional Health PGY-4 I. GENERAL INFORMATION The General Surgery Department at Orlando Regional Health has three full
Anatomic Percutaneous Ankle Reconstruction of Lateral Ligaments (A Percutaneous Anti ROLL)
") Anatomic Percutaneous Ankle Reconstruction of Lateral Ligaments (A Percutaneous Anti ROLL) Mark Glazebrook James Stone Masato Takao Stephane Guillo Introduction Ankle stabilization is required when a patient
Anatomic Percutaneous Ankle Reconstruction of Lateral Ligaments (A Percutaneous Anti ROLL) Mark Glazebrook James Stone Masato Takao Stephane Guillo Introduction Ankle stabilization is required when a patient
Laparoscopic Surgery of the Colon and Rectum (Large Intestine) A Simple Guide to Help Answer Your Questions
 A Simple Guide to Help Answer Your Questions") Laparoscopic Surgery of the Colon and Rectum (Large Intestine) A Simple Guide to Help Answer Your Questions What are the Colon and Rectum? The colon and rectum together make up the large intestine. After
Laparoscopic Surgery of the Colon and Rectum (Large Intestine) A Simple Guide to Help Answer Your Questions What are the Colon and Rectum? The colon and rectum together make up the large intestine. After
Orthopaedic Spine Center. Anterior Cervical Discectomy and Fusion (ACDF) Normal Discs
 Normal Discs") Orthopaedic Spine Center Graham Calvert MD James Woodall MD PhD Anterior Cervical Discectomy and Fusion (ACDF) Normal Discs The cervical spine consists of the bony vertebrae, discs, nerves and other structures.
Orthopaedic Spine Center Graham Calvert MD James Woodall MD PhD Anterior Cervical Discectomy and Fusion (ACDF) Normal Discs The cervical spine consists of the bony vertebrae, discs, nerves and other structures.
KEYHOLE HERNIA SURGERY
 Disclaimer This movie is an educational resource only and should not be used to manage a hernia or abdominal pain. All decisions about the management of a hernia must be made in conjunction with your Physician
Disclaimer This movie is an educational resource only and should not be used to manage a hernia or abdominal pain. All decisions about the management of a hernia must be made in conjunction with your Physician
Carotid Endarterectomy. Mark Shikhman, MD, Ph.D., CSA Andrea Scott, CST
 Carotid Endarterectomy Mark Shikhman, MD, Ph.D., CSA Andrea Scott, CST This lecture presents one of the most often vascular surgical procedures carotid endarterectomy. This type of surgery is performed
Carotid Endarterectomy Mark Shikhman, MD, Ph.D., CSA Andrea Scott, CST This lecture presents one of the most often vascular surgical procedures carotid endarterectomy. This type of surgery is performed
Shoulder Arthroscopy
 Copyright 2011 American Academy of Orthopaedic Surgeons Shoulder Arthroscopy Arthroscopy is a procedure that orthopaedic surgeons use to inspect, diagnose, and repair problems inside a joint. The word
Copyright 2011 American Academy of Orthopaedic Surgeons Shoulder Arthroscopy Arthroscopy is a procedure that orthopaedic surgeons use to inspect, diagnose, and repair problems inside a joint. The word
C A R O L I N A S. Hernia Handbook ( C H A P T E R 2 ) B. Todd Heniford, MD
 B. Todd Heniford, MD") C A R O L I N A S Hernia Handbook ( C H A P T E R 2 ) B. Todd Heniford, MD C H A P T E R 2 Umbilical Hernias C A R O L I N A S H E R N I A H A N D B O O K 17 Umbilical Hernias W H AT I S A N U M B I L
C A R O L I N A S Hernia Handbook ( C H A P T E R 2 ) B. Todd Heniford, MD C H A P T E R 2 Umbilical Hernias C A R O L I N A S H E R N I A H A N D B O O K 17 Umbilical Hernias W H AT I S A N U M B I L
Cervicothoracic Mobility Exercises
 Cervicothoracic Mobility Exercises Upper Cervical Mobility Exercises... 2 Lower Cervical Mobility Exercises... 3 Cervicothoracic Junction Mobility Exercises... 4 1 st Rib Mobility Exercises... 5 Cervical
Cervicothoracic Mobility Exercises Upper Cervical Mobility Exercises... 2 Lower Cervical Mobility Exercises... 3 Cervicothoracic Junction Mobility Exercises... 4 1 st Rib Mobility Exercises... 5 Cervical
Breast Reconstruction Frequently Asked Questions
 Breast Reconstruction Frequently Asked Questions GENERAL Do I need to have breast reconstruction? It is never medically necessary to have breast reconstruction. This is considered an elective procedure,
Breast Reconstruction Frequently Asked Questions GENERAL Do I need to have breast reconstruction? It is never medically necessary to have breast reconstruction. This is considered an elective procedure,
Flexibility Assessment and Improvement Compiled and Adapted by Josh Thompson
 Flexibility Assessment and Improvement Compiled and Adapted by Josh Thompson Muscles must have a full and normal range of motion in order for joints and skeletal structure to function properly. Flexibility
Flexibility Assessment and Improvement Compiled and Adapted by Josh Thompson Muscles must have a full and normal range of motion in order for joints and skeletal structure to function properly. Flexibility
IV. DEFINITION OF LYMPH NODE GROUPS (FIGURE 1) Level IA: Submental Group
 Level IA: Submental Group") IV. DEFINITION OF LYMPH NODE GROUPS (FIGURE 1) Fig. 1 The level system is used for describing the location of lymph nodes in the neck: Level I, submental and submandibular group; Level II, upper jugular
IV. DEFINITION OF LYMPH NODE GROUPS (FIGURE 1) Fig. 1 The level system is used for describing the location of lymph nodes in the neck: Level I, submental and submandibular group; Level II, upper jugular
Surgical Approaches to Total Hip Arthroplasty
 Surgical Approaches to Total Hip Arthroplasty Daniel Kelmanovich, 1 Michael L. Parks, MD, 2 Raj Sinha, MD, PhD, 3 and William Macaulay, MD 4 Surgical exposure of the hip for trauma, infection, or reconstruction
Surgical Approaches to Total Hip Arthroplasty Daniel Kelmanovich, 1 Michael L. Parks, MD, 2 Raj Sinha, MD, PhD, 3 and William Macaulay, MD 4 Surgical exposure of the hip for trauma, infection, or reconstruction
Tissue Reinforcement with Strattice Reconstructive Tissue Matrix following Correction of Severe Breast Deformity
 Tissue Reinforcement with Strattice Reconstructive Tissue Matrix following Correction of Severe Breast Deformity Robert Cohen, MD, FACS* Paradise Valley, AZ Case summary A 41-year old woman with a history
Tissue Reinforcement with Strattice Reconstructive Tissue Matrix following Correction of Severe Breast Deformity Robert Cohen, MD, FACS* Paradise Valley, AZ Case summary A 41-year old woman with a history
ONSTEP Technique. Technique Guide * Anterior Approach to a Part Preperitoneal, Part Intramuscular Inguinal Hernia Repair
 ONSTEP Technique Technical Aspects of the ONSTEP Inguinal Hernia Repair Technique Using the PolySoft Hernia Patch with Interrupted Memory Recoil Ring Technique Guide * Anterior Approach to a Part Preperitoneal,
ONSTEP Technique Technical Aspects of the ONSTEP Inguinal Hernia Repair Technique Using the PolySoft Hernia Patch with Interrupted Memory Recoil Ring Technique Guide * Anterior Approach to a Part Preperitoneal,
Simple Thoracostomy Avoids Chest Drain Insertion in Prehospital Trauma
 Simple Thoracostomy Avoids Chest Drain Insertion in Prehospital Trauma Deakin, C. D. MA, MRCP, FRCA; Davies, G. MRCP; Wilson, A. FRCS Author Information From the Helicopter Emergency Medical Service, Royal
Simple Thoracostomy Avoids Chest Drain Insertion in Prehospital Trauma Deakin, C. D. MA, MRCP, FRCA; Davies, G. MRCP; Wilson, A. FRCS Author Information From the Helicopter Emergency Medical Service, Royal
NEEDLE THORACENTESIS Pneumothorax / Hemothorax
 NEEDLE THORACENTESIS Pneumothorax / Hemothorax By: Steven Jones, NREMT-P Pneumothorax Pneumothorax is a collection of air or gas in the pleural space of the lung, causing the lung to collapse. Pneumothorax
NEEDLE THORACENTESIS Pneumothorax / Hemothorax By: Steven Jones, NREMT-P Pneumothorax Pneumothorax is a collection of air or gas in the pleural space of the lung, causing the lung to collapse. Pneumothorax
DESPITE THE FACT that cubital tunnel syndrome is
 SURGICAL TECHNIQUE Endoscopic Cubital Tunnel Release Tyson K. Cobb, MD A minimally invasive endoscopic approach has been successfully applied to surgical treatment of cubital tunnel syndrome. This procedure
SURGICAL TECHNIQUE Endoscopic Cubital Tunnel Release Tyson K. Cobb, MD A minimally invasive endoscopic approach has been successfully applied to surgical treatment of cubital tunnel syndrome. This procedure
MET: Posterior (backward) Rotation of the Innominate Bone.
 Rotation of the Innominate Bone.") MET: Posterior (backward) Rotation of the Innominate Bone. Purpose: To reduce an anterior rotation of the innominate bone at the SI joint. To increase posterior (backward) rotation of the SI joint. Precautions:
MET: Posterior (backward) Rotation of the Innominate Bone. Purpose: To reduce an anterior rotation of the innominate bone at the SI joint. To increase posterior (backward) rotation of the SI joint. Precautions:
Human Anatomy & Physiology
 PowerPoint Lecture Slides prepared by Barbara Heard, Atlantic Cape Community College Ninth Edition Human Anatomy & Physiology C H A P T E R 7 The Skeleton: Part B Annie Leibovitz/Contact Press Images Vertebral
PowerPoint Lecture Slides prepared by Barbara Heard, Atlantic Cape Community College Ninth Edition Human Anatomy & Physiology C H A P T E R 7 The Skeleton: Part B Annie Leibovitz/Contact Press Images Vertebral
What is Separation of the Abdominal Muscles after Childbirth (also known as Divarication of Rectus Abdominis)?
?") What is Separation of the Abdominal Muscles after Childbirth (also known as Divarication of Rectus Abdominis)? Following your pregnancy and the birth of your baby your abdominal (tummy) muscles may have
What is Separation of the Abdominal Muscles after Childbirth (also known as Divarication of Rectus Abdominis)? Following your pregnancy and the birth of your baby your abdominal (tummy) muscles may have
Clinical anatomy of the abdominal wall: hernia surgery
 Page 1 of 7 Clinical Anatomy Clinical anatomy of the abdominal wall: hernia surgery TG Johnson, SJ Von, WW Hope* Abstract Introduction The surgeon s understanding of the anatomy of the anterior abdominal
Page 1 of 7 Clinical Anatomy Clinical anatomy of the abdominal wall: hernia surgery TG Johnson, SJ Von, WW Hope* Abstract Introduction The surgeon s understanding of the anatomy of the anterior abdominal
Arizona State University Institutional Animal Care and Use Committee STANDARD INSTITUTIONAL GUIDELINE RODENT SURGERY
 Arizona State University Institutional Animal Care and Use Committee STANDARD INSTITUTIONAL GUIDELINE RODENT SURGERY It is the policy of the IACUC that all survival surgeries involving rodents be conducted
Arizona State University Institutional Animal Care and Use Committee STANDARD INSTITUTIONAL GUIDELINE RODENT SURGERY It is the policy of the IACUC that all survival surgeries involving rodents be conducted
NIH Clinical Center Patient Education Materials Giving a subcutaneous injection
 NIH Clinical Center Patient Education Materials What is a subcutaenous injection? A subcutaneous injection is given in the fatty layer of tissue just under the skin. A subcutaneous injection into the fatty
NIH Clinical Center Patient Education Materials What is a subcutaenous injection? A subcutaneous injection is given in the fatty layer of tissue just under the skin. A subcutaneous injection into the fatty
Direct Lateral Interbody Fusion A Minimally Invasive Approach to Spinal Stabilization
 APPROVED IRN10389-1.1-04 Direct Lateral Interbody Fusion A Minimally Invasive Approach to Spinal Stabilization Because it involves accessing the spine through the patient s side, the Direct Lateral approach
APPROVED IRN10389-1.1-04 Direct Lateral Interbody Fusion A Minimally Invasive Approach to Spinal Stabilization Because it involves accessing the spine through the patient s side, the Direct Lateral approach
Contents. 1. Milestones in Hernia Surgery 1. 2. Surgical Anatomy of Hernia Sites 5. 3. Incidence, Prevalence of Hernia 32
 1. Milestones in Hernia Surgery 1 History of the Procedure 3 2. Surgical Anatomy of Hernia Sites 5 Surgical Anatomy of Hernia Sites 5 External Anatomy of Abdominal Wall The Surface Markings 6 The Fascia
1. Milestones in Hernia Surgery 1 History of the Procedure 3 2. Surgical Anatomy of Hernia Sites 5 Surgical Anatomy of Hernia Sites 5 External Anatomy of Abdominal Wall The Surface Markings 6 The Fascia
Surgical Technique. coflex Surgical Technique
 Surgical Technique coflex Surgical Technique Interspinous Implant Overview I. Preparation II. Microsurgical Decompression III. Implant Site Preparation IV. Implant Insertion Preparation Patient Positioning
Surgical Technique coflex Surgical Technique Interspinous Implant Overview I. Preparation II. Microsurgical Decompression III. Implant Site Preparation IV. Implant Insertion Preparation Patient Positioning
Urinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop
 Urinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop Why do I need this surgery? A urinary diversion is a surgical procedure that is performed to allow urine to safely pass from the kidneys into a
Urinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop Why do I need this surgery? A urinary diversion is a surgical procedure that is performed to allow urine to safely pass from the kidneys into a