Abdominal Pedicle Flaps To The Hand And Forearm John C. Kelleher M.D., F.A.C.S.
|
|
|
- Madlyn Doyle
- 7 years ago
- Views:
Transcription
1 Abdominal Pedicle Flaps To The Hand And Forearm John C. Kelleher M.D., F.A.C.S. Global-HELP Publications

2 Chapter Eight: TECHNICAL REQUIREMENTS FOR FORMATION OF A TUBED PEDICLE FLAP Creating a tube pedicle is advantageous in many situations, therefore principles of tube formation are important. Donor Site: Usually the abdomen or groin are the best donor sites. There are considerations: a. Scars from previous surgery or trauma b. The amount of skin required should be planned (see chapter 5). c. Blood supply must be considered. A major vessel should be incorporated into a tube pedicle when possible (superior epigastric, superficial inferior epigastric, superficial circumflex iliac). d. Avoid hairy areas when possible and consider moving the flap laterally if possible. Layout of the Plan for the Tube Pedicle: It is well to layout this plan in the office or the hospital well before the time of the actual performance of the surgery. This allows the surgeon to think about the area of skin requirements and the previous scars that might interfere with the blood supply. Also other factors such as the presence of abdominal hair or the thickness of the abdominal fat can be considered. Usually one can grasp the roll of skin of the abdomen between the thumb and fingers to get an idea of how much skin needs to be carried between the parallel incisions in order for the tube to be closed with limited tension. This also gives a prediction of the ability to close the donor site. If the donor site area cannot be closed it can be covered with a split thickness skin graft (see drawing 8.1). Parallel lines are drawn on the skin of the abdomen of the appropriate length. Parallel incisions are then made down to the deep fascia (see drawing 8.2). The surrounding skin is undermined and closed in layers with absorbable sutures and then interrupted 4-0 nylon sutures in the skin. Using traction sutures of nylon at the distal ends of the skin to be tubed, the seam of the tube is closed with interrupted 4-0 nylon sutures.

3 next

4 Chapter Eight: TECHNICAL REQUIREMENTS FOR FORMATION OF A TUBED PEDICLE FLAP If the tension with the closure of the skin edges is judged to be too excessive then it should be opened. Using sharp tissue scissors, some fat is removed until the skin can be closed without tension. Lot Howard described an alternate method of forming a tubed pedicle that gives a little more laxity to the skin and does not have opposing seams in the tissue closure (see drawing 8.3). Another method is to make use of staggered parallel incisions which provide a wider pedicle of circulatory inflow at each end and make for easier donor site closure (see drawing 8.4). Drains are usually not required. Dressings consist of only a single dry gauze 4x4 between the tube and the donor site which is changed frequently. Of course a tie over dressing would also be used in the event of a split thickness skin graft covering the donor site. Alternate sutures are removed at two weeks and the remaining sutures are removed at three weeks.
.")
5 next

6 Chapter Eight: TECHNICAL REQUIREMENTS FOR FORMATION OF A TUBED PEDICLE FLAP EXAMPLES OF HAND RECONSTRUCTION USING TUBED FLAPS - Case No. 1: A 26-year-old man caught his right dominant hand in a paint roller and was taken to a local hospital for care. At the time of the injury, the little finger was amputated at the metacarpal base and 3 weeks later the thumb was amputated at the mid proximal phalanx. A meshed skin graft was applied. A month later a poorly planned "Alpha type" flap was applied to the palmar aspect of the hand. Note the inadequate size, straight line scars and biscuit shape of that flap (see photos 8.1A, 8.1B). These photos were taken 7 months after injury and this surgical treatment prior to his transfer here. Photo 8.1A Photo 8.1B Our examination revealed heavy scarring and limited motion. Action of the extensor pollicis longus could not be demonstrated because of scarring in the area. It was decided to make use of a tubed flap because of the need for cover on both sides of the hand and wrist (see photos 8.1C, 8.1D).
.")
7 Photo 8.1C Photo 8.1D A superior "pancake" of tissue with W darts is used on the border to replace the scar on the ulnar side of the hand (see photo 8.1E). Photo 8.1E Although not depicted in photographs, this tube was then transferred after several "delays" to cover the Palm of the hand and thumb as seen in the final photos (see photos 8.1F, 8.1G). Photo 8.1F

8 Photo 8.1G next

9 Chapter Eight: TECHNICAL REQUIREMENTS FOR FORMATION OF A TUBED PEDICLE FLAP Case No. 2: A 35-year-old man caught his left hand in a punch press suffering loss of all parts of the thumb through the distal end of the metacarpal along with avulsion of the skin of the thumb-index web space. There was also a partial amputation of the tips of the index and long fingers. (see photo 8.2A). His surgical treatment involved 3 operations. Photo 8.2A Stage I. A patterned abdominal tubed flap was raised in the left lower quadrant based on the superficial inferior epigastric vessels. This type of skin coverage was selected to effectively cover the web space and to have additional skin and fat for future stages in the thumb reconstruction. (see drawing 8.5 and photo 8.2B). Photo 8.2B The donor site was closed primarily. The proximal portion of the flap was tubed as described above and the distal portion of the flap to be applied to the open web space was thinned of excess fat just deep to the subdermal plexus. Stage II. Three weeks later the tube flap was detached with closure of the abdominal wound and closure of the distal stump of the tube flap. (see photos 8.2C and 8.2D). There was some delayed wound healing and a small foreign body that had to be removed in the healing phase.

10 Photo 8.2C Photo 8.2D Stage III. Nineteen weeks following the injury a transposition of the left index finger to the thumb metacarpal was performed. (see photos 8.2E and 8.2F). These photos were taken 18 years later. Photo 8.2E Photo 8.2F next
.")
11 Chapter Eight: TECHNICAL REQUIREMENTS FOR FORMATION OF A TUBED PEDICLE FLAP EXAMPLES OF HAND RECONSTRUCTION USING TUBED FLAPS Case No. 3: A 37-year-old man had a punch press injury suffering avulsion of the distal portion of the thumb and fractures of the proximal phalanx with amputation of the index finger through the mid proximal phalanx. There was also an injury to the distal phalanx of the long finger (see photos 8.3A, 8.3B). Photo 8.3A Photo 8.3B Stage I. The injuries to the fingers were closed primarily and this required removal of the remaining proximal phalanx of the index finger. The tube flap was selected to cover the skin loss of the proximal phalanx of the thumb (see photo 8.3C). The tube was raised from the right lower quadrant of the abdomen based on the superficial inferior epigastric vessels. The distal end of the tube had multiple W' s or darts to break up the straight line circular scar around the base of the thumb. Photo 8.3C Stage II. One month later the tube was divided and closed. There was some delay in healing which is not uncommon and his appearance is noted five weeks later (see photo 8.3D).

12 Photo 8.3D Stage III. It was felt that the patient would benefit from more length and better sensation in the thumb. We elected to do this by using a bone graft of the index metacarpal and by resurfacing the reconstruction with a neurovascular island flap based on the index finger. The bone graft consisted of the distal 1/2-2/3 of the index metacarpal turned backwards and inserted ("Dunce hat") over the remaining proximal phalanx of the thumb (see photos 8.3E and 8.3F). Photo 8.3E Photo 8.3F next
 over the")
13 Chapter Eight: TECHNICAL REQUIREMENTS FOR FORMATION OF A TUBED PEDICLE FLAP EXAMPLES OF HAND RECONSTRUCTION USING TUBED FLAPS Case No. 4: A 26-year-old man suffered loss of his entire thumb including the metacarpal, the index finger at the MP joint and the long finger at the PIP joint. This was his dominant right hand. His initial repair was done elsewhere and consisted of a split thickness skin graft on the radial side of the hand and closure of the amputation of the long finger. The base of the thumb metacarpal was present, the abductor insertion was present and there was still some thenar muscle mass present (see photos 8.4A, 8.4B). Photo 8.4A Photo 8.4B My operative plan was to provide the skin coverage necessary for the reconstruction with a tube flap placed initially on the dorsum of the hand in the area of the bases of the index and long metacarpals. The base or abdominal end of the tube will be delayed once then transferred to replace the skin graft and scar at the base of the thenar eminence. The tube flap is used for deferred coverage of both sides of the reconstructed thumb index web space. At the time of the bony reconstruction, this tube will be opened in the center to allow access for the thumb reconstruction. The tube should not be opened and defatted until the deep bone and tendon work is completed otherwise the tissue will dry out and cause problems with circulation. Stage I. A tube flap was raised from the right lower quadrant measuring 9 cm in width by 18 cm in length. The superior end of the flap was defatted and inserted into a "Y" shaped incision on the dorsal aspect of the hand at the base of the ring and long finger metacarpals (see photos 8.4C, 8.4D). A heavy Kirschner wire was driven across the ulna into the radius to hold the hand in full pronation and provide a point of traction at the wrist. Photo 8.4C Photo 8.4D Stage II Three weeks later a primary delay (see photo 8.4E).
. Photo 8.4A Photo 8.")
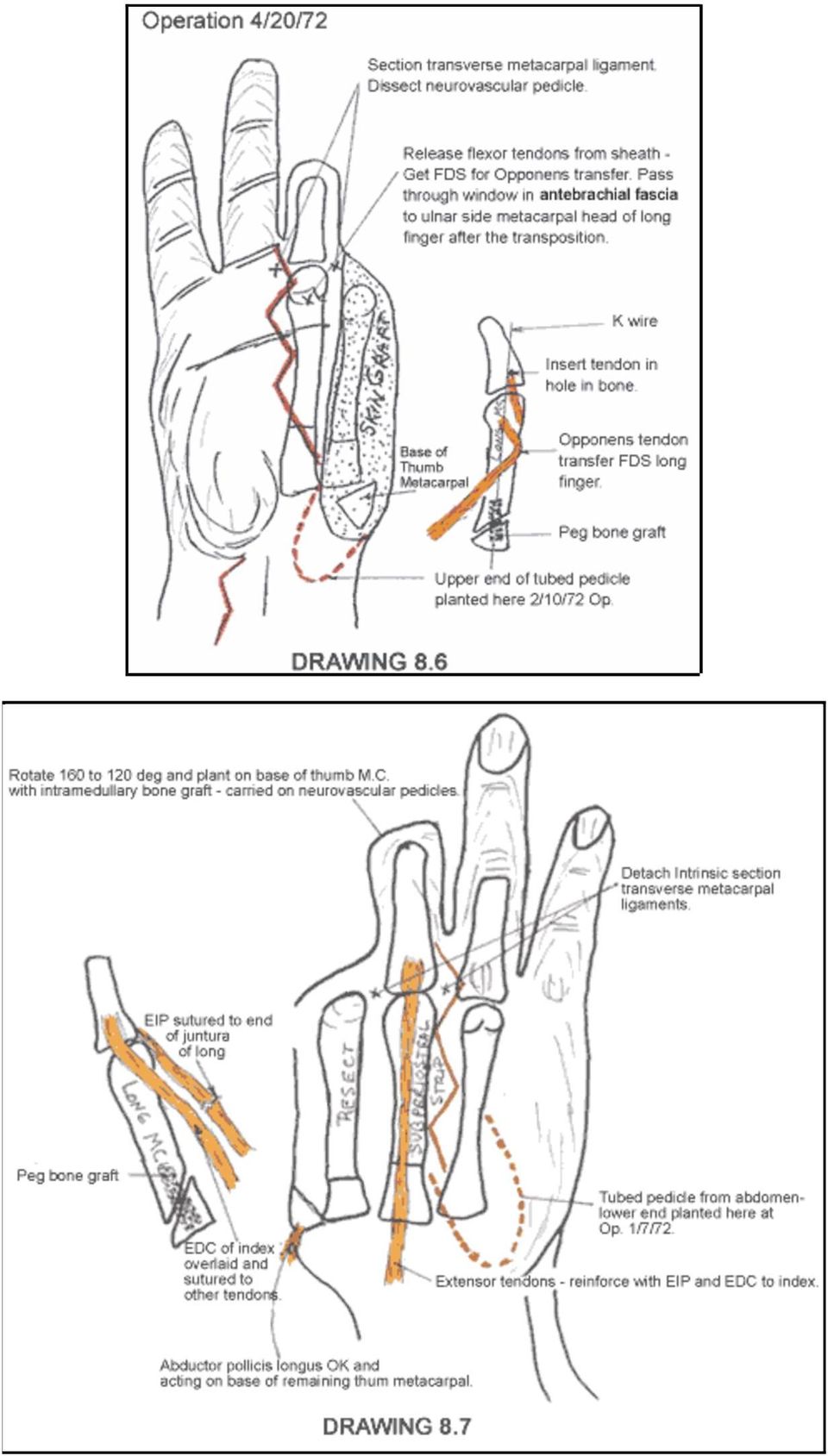
14 Photo 8.4E Stage III. Ten days later the base of the flap was divided from the abdomen, defatted and placed over the proximal area previously covered by the split thickness skin graft at the base of the thenar eminence (see photos 8.4F, 8.4G). Photo 8.4F Photo 8.4G Stage IV Ten weeks later a transposition of the remaining long finger metacarpal and proximal phalanx was performed to the base of the thumb metacarpal with the use of bone grafts and internal fixation. A temporary bayonet shaped Kirschner wire, inserted into the metacarpals, was used to separate and hold the position of the new web space. (see drawing 8.6, 8.7, 8.8).

15
16 The tube flap was then transected horizontally at its midpoint. The tube on the volar side was opened, defatted and trimmed to fit the skin defect on the volar side of the thenar eminence. The tube on the dorsal side was opened, defatted and thinned to cover the open dorsal and ulnar side of the web space (see photos 8.4H, 8.4I). Photo 8.4H Photo 8.4I His final function was excellent and photos are shown taken six years post injury with excellent grasp and strong pinch between the reconstructed thumb and the remaining digits (see photos 8.4J, 8.4K, 8.4L).
. Photo 8.4H Photo 8.")
17 Photo 8.4J Photo 8.4K Photo 8.4L next

18 Chapter Eight: TECHNICAL REQUIREMENTS FOR FORMATION OF A TUBED PEDICLE FLAP EXAMPLES OF HAND RECONSTRUCTION USING TUBED FLAPS Case No. 5: A 40-year-old man suffered a crush/avulsion injury of the left-hand with loss of the phalanges III, IV, and V and near complete degloving on both sides of the hand (see photos 8.5A, 8.5B). Photo 8.5A Photo 8.5B Stage I. The wound was extensively debrided and W's were incorporated along the skin line of attachment for the flap. The W's were not as large as I would use today. A large patterned flap was planned on paper and placed over the left lower quadrant measuring 19 cm in width and extending from the midline of the abdomen and the left hip area incorporating the superficial inferior epigastric vessels. The proximal portion of the flap was tubed and the distal portion to be applied to the hand was thinned of fat. The tube was rotated 90 so that the palmar skin would be taken from the lateral flank which was free of hair. The donor site was closed by advancement and with a split thickness skin graft. Because of the concavity of the palmar surface, a suction drain was used to obliterate dead space. A spreader was used to maintain the thumb index web space. The Kirschner wire was used through the thumb as a point of suspension to keep the hand away from the abdomen and keep the flap in good position (see photos 8.5C, 8.5D). Photo 8.5C Photo 8.5D

19 Stage II. Three weeks later a primary delay was performed close to where the flap joined the hand. Stage III. Four weeks after attaching the flap, the pedicle was divided. The remaining tube was opened to replace the split thickness skin graft previously used to close the donor site. The postoperative result is shown eight years later (see photo 8.5E). This case illustrates the usefulness of the tubed abdominal flap to cover both sides of the hand. Photo 8.5E next
.")
Most active and intricate part of the upper extremity Especially vulnerable to injury Do not respond well to serious trauma. Magee, 2008. pg.
 PTA 216 Most active and intricate part of the upper extremity Especially vulnerable to injury Do not respond well to serious trauma Magee, 2008. pg. 396 28 bones Numerous articulations 19 intrinsic muscles
PTA 216 Most active and intricate part of the upper extremity Especially vulnerable to injury Do not respond well to serious trauma Magee, 2008. pg. 396 28 bones Numerous articulations 19 intrinsic muscles
Chapter 29. Initial Care
 Chapter 29 FINGERTIP AND NAIL BED INJURIES KEY FIGURES: Digital tourniquet Bone rongeur Fingernail with hematoma Thenar flap Repair of nail bed Hand injuries are commonly encountered by health care providers
Chapter 29 FINGERTIP AND NAIL BED INJURIES KEY FIGURES: Digital tourniquet Bone rongeur Fingernail with hematoma Thenar flap Repair of nail bed Hand injuries are commonly encountered by health care providers
EXTENSOR POLLICIS TENDONITIS SYNDROME
 EXTENSOR POLLICIS TENDONITIS SYNDROME The extensor pollicis longus muscle has its origin on the lateral part of the middle third of the ulnar shaft on the dorsal border below the abductor pollicis longus
EXTENSOR POLLICIS TENDONITIS SYNDROME The extensor pollicis longus muscle has its origin on the lateral part of the middle third of the ulnar shaft on the dorsal border below the abductor pollicis longus
Scaphoid Fracture of the Wrist
 Page 1 of 6 Scaphoid Fracture of the Wrist Doctors commonly diagnose a sprained wrist after a patient falls on an outstretched hand. However, if pain and swelling don't go away, doctors become suspicious
Page 1 of 6 Scaphoid Fracture of the Wrist Doctors commonly diagnose a sprained wrist after a patient falls on an outstretched hand. However, if pain and swelling don't go away, doctors become suspicious
Mini TightRope CMC Surgical Technique
 Mini TightRope CMC Surgical Technique Mini TightRope CMC Mini TightRope CMC Fixation The Mini TightRope provides a unique means to suspend the thumb metacarpal after partial or complete trapezial resection
Mini TightRope CMC Surgical Technique Mini TightRope CMC Mini TightRope CMC Fixation The Mini TightRope provides a unique means to suspend the thumb metacarpal after partial or complete trapezial resection
Chapter 7 The Wrist and Hand Joints
 Chapter 7 The Wrist and Hand Manual of Structural Kinesiology R.T. Floyd, EdD, ATC, CSCS Many Archery, Relate wrist require sports require precise functioning of flexion, & hand & hand functional combined
Chapter 7 The Wrist and Hand Manual of Structural Kinesiology R.T. Floyd, EdD, ATC, CSCS Many Archery, Relate wrist require sports require precise functioning of flexion, & hand & hand functional combined
Chapter 35. Volar forearm fasciotomy incisions Hand/dorsal forearm fasciotomy incisions Finger fasciotomy incisions
 Chapter 35 HAND CRUSH INJURY AND COMPARTMENT SYNDROME KEY FIGURES: Volar forearm fasciotomy incisions Hand/dorsal forearm fasciotomy incisions Finger fasciotomy incisions The previous chapters about the
Chapter 35 HAND CRUSH INJURY AND COMPARTMENT SYNDROME KEY FIGURES: Volar forearm fasciotomy incisions Hand/dorsal forearm fasciotomy incisions Finger fasciotomy incisions The previous chapters about the
International Standards for the Classification of Spinal Cord Injury Motor Exam Guide
 C5 Elbow Flexors Biceps Brachii, Brachialis Patient Position: The shoulder is in neutral rotation, neutral flexion/extension, and adducted. The elbow is fully extended, with the forearm in full supination.
C5 Elbow Flexors Biceps Brachii, Brachialis Patient Position: The shoulder is in neutral rotation, neutral flexion/extension, and adducted. The elbow is fully extended, with the forearm in full supination.
TENDON INJURIES OF THE HAND KEY FIGURES:
 Chapter 32 TENDON INJURIES OF THE HAND KEY FIGURES: Extensor surface of hand Mallet finger Mallet splints Injured finger in stack splint Repair of open mallet Most hand specialists believe that the earlier
Chapter 32 TENDON INJURIES OF THE HAND KEY FIGURES: Extensor surface of hand Mallet finger Mallet splints Injured finger in stack splint Repair of open mallet Most hand specialists believe that the earlier
Extremity Trauma. William Schecter, MD
 Extremity Trauma William Schecter, MD Approach to the Evaluation of the Patient with an Extremity Injury Blood Supply Skeleton Neurologic Function Risk for Compartment Syndrome? Coverage (Skin and Soft
Extremity Trauma William Schecter, MD Approach to the Evaluation of the Patient with an Extremity Injury Blood Supply Skeleton Neurologic Function Risk for Compartment Syndrome? Coverage (Skin and Soft
Coding for Difficult Tendon Repairs and Transfers. Current Procedural Terminology 2013 American Medical Association. All Rights Reserved.
 Coding for Difficult Tendon Repairs and Transfers Rotator Cuff Repair 23420 February 2002 page 11 Code 23420 describes a repair of a complete shoulder (rotator) cuff avulsion, referring to the repair of
Coding for Difficult Tendon Repairs and Transfers Rotator Cuff Repair 23420 February 2002 page 11 Code 23420 describes a repair of a complete shoulder (rotator) cuff avulsion, referring to the repair of
INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D.
 05/05/2007 INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D. Hand injuries, especially the fractures of metacarpals and phalanges, are the most common fractures in the skeletal system. Hand injuries
05/05/2007 INJURIES OF THE HAND AND WRIST By Derya Dincer, M.D. Hand injuries, especially the fractures of metacarpals and phalanges, are the most common fractures in the skeletal system. Hand injuries
Integumentary System Individual Exercises
 Integumentary System Individual Exercises 1. A physician performs an incision and drainage of a subcutaneous abscess in his office for a particularly uncooperative established patient. How should this
Integumentary System Individual Exercises 1. A physician performs an incision and drainage of a subcutaneous abscess in his office for a particularly uncooperative established patient. How should this
Wrist and Hand. Patient Information Guide to Bone Fracture, Bone Reconstruction and Bone Fusion: Fractures of the Wrist and Hand: Carpal bones
 Patient Information Guide to Bone Fracture, Bone Reconstruction and Bone Fusion: Wrist and Hand Fractures of the Wrist and Hand: Fractures of the wrist The wrist joint is made up of the two bones in your
Patient Information Guide to Bone Fracture, Bone Reconstruction and Bone Fusion: Wrist and Hand Fractures of the Wrist and Hand: Fractures of the wrist The wrist joint is made up of the two bones in your
Chapter 33. Nerve Physiology
 Chapter 33 NERVE AND VASCULAR INJURIES OF THE HAND KEY FIGURES: Digital nerve location on finger Epineurial repair Nerves and blood vessels of the hand and fingers usually are quite delicate, and some
Chapter 33 NERVE AND VASCULAR INJURIES OF THE HAND KEY FIGURES: Digital nerve location on finger Epineurial repair Nerves and blood vessels of the hand and fingers usually are quite delicate, and some
Chapter 34. Neglected hand Escharotomy
 Chapter 34 HAND BURNS KEY FIGURES: Neglected hand Escharotomy Severe hand burns are especially problematic injuries because of their propensity for causing long-term disability. Proper treatment of the
Chapter 34 HAND BURNS KEY FIGURES: Neglected hand Escharotomy Severe hand burns are especially problematic injuries because of their propensity for causing long-term disability. Proper treatment of the
www.ghadialisurgery.com
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
Negative Pressure Wound Therapy Incorporating Early Exercise Therapy in Hand Surgery: Bag-type Negative Pressure Wound Therapy
 2013 67 4 271 276 Negative Pressure Wound Therapy Incorporating Early Exercise Therapy in Hand Surgery: ag-type Negative Pressure Wound Therapy * 272 67 4 14 15 17 ugust 2013 ag-type Negative Pressure
2013 67 4 271 276 Negative Pressure Wound Therapy Incorporating Early Exercise Therapy in Hand Surgery: ag-type Negative Pressure Wound Therapy * 272 67 4 14 15 17 ugust 2013 ag-type Negative Pressure
Integra. MCP Joint Replacement PATIENT INFORMATION
 Integra MCP Joint Replacement PATIENT INFORMATION Integra MCP Patient Information This brochure summarizes information about the use, risks, and benefits of the Integra MCP finger implant. Be sure to discuss
Integra MCP Joint Replacement PATIENT INFORMATION Integra MCP Patient Information This brochure summarizes information about the use, risks, and benefits of the Integra MCP finger implant. Be sure to discuss
Chapter 30. Rotational deformity Buddy taping Reduction of metacarpal fracture
 Chapter 30 FINGER FRACTURES AND DISLOCATIONS KEY FIGURES: Rotational deformity Buddy taping Reduction of metacarpal fracture Because we use our hands for so many things, finger fractures and dislocations
Chapter 30 FINGER FRACTURES AND DISLOCATIONS KEY FIGURES: Rotational deformity Buddy taping Reduction of metacarpal fracture Because we use our hands for so many things, finger fractures and dislocations
Anatomic Percutaneous Ankle Reconstruction of Lateral Ligaments (A Percutaneous Anti ROLL)
") Anatomic Percutaneous Ankle Reconstruction of Lateral Ligaments (A Percutaneous Anti ROLL) Mark Glazebrook James Stone Masato Takao Stephane Guillo Introduction Ankle stabilization is required when a patient
Anatomic Percutaneous Ankle Reconstruction of Lateral Ligaments (A Percutaneous Anti ROLL) Mark Glazebrook James Stone Masato Takao Stephane Guillo Introduction Ankle stabilization is required when a patient
The Hand Exam: Tips and Tricks
 The Hand Exam: Tips and Tricks Nikki Strauss Schroeder, MD Assistant Clinical Professor, UCSF Department of Orthopaedic Surgery November 4, 2013 Outline Surface Anatomy Hand Anatomy Exam Management of
The Hand Exam: Tips and Tricks Nikki Strauss Schroeder, MD Assistant Clinical Professor, UCSF Department of Orthopaedic Surgery November 4, 2013 Outline Surface Anatomy Hand Anatomy Exam Management of
Fractures around wrist
 Fractures around wrist Colles Fracture Smiths fracture Barton s fracture Chauffer s fracture Scaphoid fracture Lunate dislocation Vivek Pandey Colles fracture Definition: Fracture of the distal end radius
Fractures around wrist Colles Fracture Smiths fracture Barton s fracture Chauffer s fracture Scaphoid fracture Lunate dislocation Vivek Pandey Colles fracture Definition: Fracture of the distal end radius
Chapter 11. Everting skin edges
 Chapter 11 PRIMARY WOUND CLOSURE KEY FIGURE: Everting skin edges In primary wound closure, the skin edges of the wound are sutured together to close the defect. Whenever possible and practical, primary
Chapter 11 PRIMARY WOUND CLOSURE KEY FIGURE: Everting skin edges In primary wound closure, the skin edges of the wound are sutured together to close the defect. Whenever possible and practical, primary
10/15/2012. The Hand. Clarification of Terms. Osteology of the Hand (Bones) http://www.youtube.com/watch?v=idxuwerttj A&feature=related
 http://www.youtube.com/watch?v=idxuwerttj A&feature=related") The Hand http://www.youtube.com/watch?v=idxuwerttj A&feature=related Clarification of Terms The hand is made up of the thumb, metacarpals, and phalanges The digits are numbered (with the thumb being #1
The Hand http://www.youtube.com/watch?v=idxuwerttj A&feature=related Clarification of Terms The hand is made up of the thumb, metacarpals, and phalanges The digits are numbered (with the thumb being #1
Muscle Movements, Types, and Names
 Muscle Movements, Types, and Names A. Gross Skeletal Muscle Activity 1. With a few exceptions, all muscles cross at least one joint 2. Typically, the bulk of the muscle lies proximal to the joint it crossed
Muscle Movements, Types, and Names A. Gross Skeletal Muscle Activity 1. With a few exceptions, all muscles cross at least one joint 2. Typically, the bulk of the muscle lies proximal to the joint it crossed
Hand and Upper Extremity Injuries in Outdoor Activities. John A. Schneider, M.D.
 Hand and Upper Extremity Injuries in Outdoor Activities John A. Schneider, M.D. Biographical Sketch Dr. Schneider is an orthopedic surgeon that specializes in the treatment of hand and upper extremity
Hand and Upper Extremity Injuries in Outdoor Activities John A. Schneider, M.D. Biographical Sketch Dr. Schneider is an orthopedic surgeon that specializes in the treatment of hand and upper extremity
Surgical Art. Formulaic Drawing Method. DRAWING WORKSHOP Learning to sketch for patient notes
 DRAWING WORKSHOP Learning to sketch for patient notes Surgical Art Formulaic Drawing Method Formulaic figure drawing systems involve using abstract rhythms and interlocking shapes to construct the human
DRAWING WORKSHOP Learning to sketch for patient notes Surgical Art Formulaic Drawing Method Formulaic figure drawing systems involve using abstract rhythms and interlocking shapes to construct the human
Adult Forearm Fractures
 Adult Forearm Fractures Your forearm is made up of two bones, the radius and ulna. In most cases of adult forearm fractures, both bones are broken. Fractures of the forearm can occur near the wrist at
Adult Forearm Fractures Your forearm is made up of two bones, the radius and ulna. In most cases of adult forearm fractures, both bones are broken. Fractures of the forearm can occur near the wrist at
The Abdominal Wall And Hernias. Stanley Kurek, DO, FACS Associate Professor of Surgery UTMCK
 The Abdominal Wall And Hernias Stanley Kurek, DO, FACS Associate Professor of Surgery UTMCK The Abdominal Wall The structure of the abdominal wall is similar in principle to the thoracic wall. There are
The Abdominal Wall And Hernias Stanley Kurek, DO, FACS Associate Professor of Surgery UTMCK The Abdominal Wall The structure of the abdominal wall is similar in principle to the thoracic wall. There are
Chapter 12. Anatomy of Skin. Epidermis. Dermis
 Chapter 12 SKIN GRAFTS KEY FIGURES: Skin anatomy with graft thickness Humby knife Using the dermatome Using the Humby knife Mesher Skin graft Tying the dressing in place Defatting the FTSG A skin graft
Chapter 12 SKIN GRAFTS KEY FIGURES: Skin anatomy with graft thickness Humby knife Using the dermatome Using the Humby knife Mesher Skin graft Tying the dressing in place Defatting the FTSG A skin graft
Plastic Surgery Jewish General Hospital / Montreal General Hospital
 Plastic Surgery Jewish General Hospital / Montreal General Hospital Structure of the Rotation Duration: Two weeks. Activities: Emergency Department consults Minor surgery Major surgery Plastics clinic
Plastic Surgery Jewish General Hospital / Montreal General Hospital Structure of the Rotation Duration: Two weeks. Activities: Emergency Department consults Minor surgery Major surgery Plastics clinic
Achilles Tendon Repair, Operative Technique
 *smith&nephew ANKLE TECHNIQUE GUIDE Achilles Tendon Repair, Operative Technique Prepared in Consultation with: C. Niek van Dijk, MD, PhD KNEE HIP SHOULDER EXTREMITIES Achilles Tendon Repair, Operative
*smith&nephew ANKLE TECHNIQUE GUIDE Achilles Tendon Repair, Operative Technique Prepared in Consultation with: C. Niek van Dijk, MD, PhD KNEE HIP SHOULDER EXTREMITIES Achilles Tendon Repair, Operative
Suture Patterns. Objectives. Role of Suture Patterns. Inverting Suture Patterns. Appositional Suture Patterns
 Suture Patterns Objectives Introduction to Surgery Classify suture patterns based on their effect on tissue apposition Describe the steps involved in the accurate placement of basic suture patterns Discuss
Suture Patterns Objectives Introduction to Surgery Classify suture patterns based on their effect on tissue apposition Describe the steps involved in the accurate placement of basic suture patterns Discuss
FUNCTIONS OF THE SKIN
 FUNCTIONS OF THE SKIN Skin is the largest organ of the body. The average adult has 18 square feet of skin which account for 16% of the total body weight. Skin acts as a physical barrier for you to the
FUNCTIONS OF THE SKIN Skin is the largest organ of the body. The average adult has 18 square feet of skin which account for 16% of the total body weight. Skin acts as a physical barrier for you to the
Dressing and bandage
 Dressing and bandage Mihajlo Lojpur, M.D., Ph.D. INTRODUCTION The terms dressing and bandage are often used synonymously. In fact, the term dressing refers more correctly to the primary layer in contact
Dressing and bandage Mihajlo Lojpur, M.D., Ph.D. INTRODUCTION The terms dressing and bandage are often used synonymously. In fact, the term dressing refers more correctly to the primary layer in contact
Wrist Fracture. Please stick addressograph here
 ORTHOPAEDIC UNIT: 01-293 8687 /01-293 6602 UPMC BEACON CENTRE FOR ORTHOPAEDICS: 01-2937575 PHYSIOTHERAPY DEPARTMENT: 01-2936692 GUIDELINES FOR PATIENTS FOLLOWING WRIST FRACTURE Please stick addressograph
ORTHOPAEDIC UNIT: 01-293 8687 /01-293 6602 UPMC BEACON CENTRE FOR ORTHOPAEDICS: 01-2937575 PHYSIOTHERAPY DEPARTMENT: 01-2936692 GUIDELINES FOR PATIENTS FOLLOWING WRIST FRACTURE Please stick addressograph
ACUTE HAND INJURY PROTOCOLS
 ACUTE HAND INJURY PROTOCOLS I. FRACTURES OF THE HAND AND DIGITS Digital and hand fractures are seen in workers who use their hands, due to the exposed nature of the hand (in most functions) at work. Most
ACUTE HAND INJURY PROTOCOLS I. FRACTURES OF THE HAND AND DIGITS Digital and hand fractures are seen in workers who use their hands, due to the exposed nature of the hand (in most functions) at work. Most
KnifeLight. Carpal Tunnel Ligament Release. Operative Technique
 KnifeLight Carpal Tunnel Ligament Release Operative Technique Contents Page 1. Features & Benefits 3 Intended Use and Indications 3 Contraindications 3 Features & Benefits 3 2. Operative Technique 4 Antegrade
KnifeLight Carpal Tunnel Ligament Release Operative Technique Contents Page 1. Features & Benefits 3 Intended Use and Indications 3 Contraindications 3 Features & Benefits 3 2. Operative Technique 4 Antegrade
Elbow, Forearm, Wrist, & Hand. Bony Anatomy. Objectives. Bones. Bones. Bones
 Objectives Elbow, Forearm, Wrist, & Hand Chapter 19 Identify and discuss the functional anatomy of the elbow and forearm Discuss the common injuries associated with these anatomical structures Bones Humerus
Objectives Elbow, Forearm, Wrist, & Hand Chapter 19 Identify and discuss the functional anatomy of the elbow and forearm Discuss the common injuries associated with these anatomical structures Bones Humerus
ESSENTIALPRINCIPLES. Wrist Pain. Radial and Ulnar Collateral Ligament Injuries. By Ben Benjamin
 ESSENTIALPRINCIPLES Wrist Pain Radial and Ulnar Collateral Ligament Injuries By Ben Benjamin 92 MASSAGE & BODYWORK FEBRUARY/MARCH 2005 Ulnar Collateral Ligament Radial Collateral Ligament Right wrist,
ESSENTIALPRINCIPLES Wrist Pain Radial and Ulnar Collateral Ligament Injuries By Ben Benjamin 92 MASSAGE & BODYWORK FEBRUARY/MARCH 2005 Ulnar Collateral Ligament Radial Collateral Ligament Right wrist,
Pediatric Sports Injuries of the Wrist and Hand. Sunni Alford, OTR/L,CHT Preferred Physical Therapy
 Pediatric Sports Injuries of the Wrist and Hand Sunni Alford, OTR/L,CHT Preferred Physical Therapy Wrist injuries TFCC ECU/ FCU tendonitis Instability Growth Plate Fractures Ulnar abutment syndrome Triangular
Pediatric Sports Injuries of the Wrist and Hand Sunni Alford, OTR/L,CHT Preferred Physical Therapy Wrist injuries TFCC ECU/ FCU tendonitis Instability Growth Plate Fractures Ulnar abutment syndrome Triangular
13 Adductor Muscle Group Excision
 Malawer Chapter 13 21/02/2001 15:36 Page 243 13 Adductor Muscle Group Excision Martin Malawer and Paul Sugarbaker OVERVIEW The adductor muscle group is the second most common site for high- and low-grade
Malawer Chapter 13 21/02/2001 15:36 Page 243 13 Adductor Muscle Group Excision Martin Malawer and Paul Sugarbaker OVERVIEW The adductor muscle group is the second most common site for high- and low-grade
How To Recover From A Surgical Wound From A Cast
 Care of Your Wounds After Amputation Surgery by Paddy Rossbach, RN Depending on the reason for your amputation and the state of your limb at the time of surgery, definitive closure of the wound may take
Care of Your Wounds After Amputation Surgery by Paddy Rossbach, RN Depending on the reason for your amputation and the state of your limb at the time of surgery, definitive closure of the wound may take
PHaSES: Practical Hands-on Surgical Education System
 U.S. Toll Free 866-GOLIMBS PHaSES Range PHaSES: Practical Hands-on Surgical Education System Limbs & Things is pleased to introduce the PHaSES Range. The range is based upon our well known basic & general
U.S. Toll Free 866-GOLIMBS PHaSES Range PHaSES: Practical Hands-on Surgical Education System Limbs & Things is pleased to introduce the PHaSES Range. The range is based upon our well known basic & general
Breast Reconstruction Frequently Asked Questions
 Breast Reconstruction Frequently Asked Questions GENERAL Do I need to have breast reconstruction? It is never medically necessary to have breast reconstruction. This is considered an elective procedure,
Breast Reconstruction Frequently Asked Questions GENERAL Do I need to have breast reconstruction? It is never medically necessary to have breast reconstruction. This is considered an elective procedure,
Surgical Technique. coflex Surgical Technique
 Surgical Technique coflex Surgical Technique Interspinous Implant Overview I. Preparation II. Microsurgical Decompression III. Implant Site Preparation IV. Implant Insertion Preparation Patient Positioning
Surgical Technique coflex Surgical Technique Interspinous Implant Overview I. Preparation II. Microsurgical Decompression III. Implant Site Preparation IV. Implant Insertion Preparation Patient Positioning
LSU Health Sciences Center Occupational Therapy Flexor Tendon Injury Treatment Protocol
 . LSU Health Sciences Center Occupational Therapy Flexor Tendon Injury Treatment Protocol DIP PIP MCP Zone 1 Zone 2 T 1 T 2 Zone 3 T 3 Zone 4 Zone 5 Zone 5 cs Carla M. Saulsbery LOTR, CHT Dr. A. Hollister,
. LSU Health Sciences Center Occupational Therapy Flexor Tendon Injury Treatment Protocol DIP PIP MCP Zone 1 Zone 2 T 1 T 2 Zone 3 T 3 Zone 4 Zone 5 Zone 5 cs Carla M. Saulsbery LOTR, CHT Dr. A. Hollister,
Spinal Arthrodesis Group Exercises
 Spinal Arthrodesis Group Exercises 1. Two surgeons work together to perform an arthrodesis. Dr. Bonet, a general surgeon, makes the anterior incision to gain access to the spine for the arthrodesis procedure.
Spinal Arthrodesis Group Exercises 1. Two surgeons work together to perform an arthrodesis. Dr. Bonet, a general surgeon, makes the anterior incision to gain access to the spine for the arthrodesis procedure.
Hand Mobility Deficits. 883.2 Open wound of finger with tendon involvement
 1 Hand Mobility Deficits ICD-9-CM codes: 882.2 Open wound of hand with tendon involvement 883.2 Open wound of finger with tendon involvement ICF codes: Activities and Participation code: d4301 Carrying
1 Hand Mobility Deficits ICD-9-CM codes: 882.2 Open wound of hand with tendon involvement 883.2 Open wound of finger with tendon involvement ICF codes: Activities and Participation code: d4301 Carrying
Median Nerve Injuries in, Fractures in the Region of the Wrist
 252 Median Nerve Injuries in, Fractures in the Region of the Wrist N. MEADOFF, M.D., Bakersfield SUMMARY Injuries of the median nerve in fractures in the region of the wrist are not uncommon. Median nerve
252 Median Nerve Injuries in, Fractures in the Region of the Wrist N. MEADOFF, M.D., Bakersfield SUMMARY Injuries of the median nerve in fractures in the region of the wrist are not uncommon. Median nerve
3. Be able to perform a detailed clinical examination of the forearm and wrist.
 Patient Care: 1. Demonstrate appropriate evaluation and treatment of patients with hand/wrist surgery problems in the emergency room and as part of the inpatient consultation service, including application
Patient Care: 1. Demonstrate appropriate evaluation and treatment of patients with hand/wrist surgery problems in the emergency room and as part of the inpatient consultation service, including application
MANAGEMENT OF HAND INJURIES: A SIX YEAR EXPERIENCE FROM KOMFO ANOKYE TEACHING HOSPITAL, KUMASI, GHANA
 September 2013 Vol. 2, No. 2 Postgraduate Medical Journal of Ghana MANAGEMENT OF HAND INJURIES: A SIX YEAR EXPERIENCE FROM KOMFO ANOKYE TEACHING HOSPITAL, KUMASI, GHANA Adu E J K Department of Surgery,
September 2013 Vol. 2, No. 2 Postgraduate Medical Journal of Ghana MANAGEMENT OF HAND INJURIES: A SIX YEAR EXPERIENCE FROM KOMFO ANOKYE TEACHING HOSPITAL, KUMASI, GHANA Adu E J K Department of Surgery,
At the completion of the rotation, the resident will have acquired the following competencies and will function effectively as:
 Goals and Objectives Orthopedic Surgery Residency Program - Memorial University Plastic Surgery DEFINITION Traumatic or acquired problems of the musculoskeletal system frequently have a soft tissue component
Goals and Objectives Orthopedic Surgery Residency Program - Memorial University Plastic Surgery DEFINITION Traumatic or acquired problems of the musculoskeletal system frequently have a soft tissue component
A Patient s Guide to Guyon s Canal Syndrome
 A Patient s Guide to DISCLAIMER: The information in this booklet is compiled from a variety of sources. It may not be complete or timely. It does not cover all diseases, physical conditions, ailments or
A Patient s Guide to DISCLAIMER: The information in this booklet is compiled from a variety of sources. It may not be complete or timely. It does not cover all diseases, physical conditions, ailments or
Scaphoid Non-union. Dr. Mandel Dr. Gyomorey. May 3 rd 2006
 Scaphoid Non-union Dr. Mandel Dr. Gyomorey May 3 rd 2006 Introduction Scaphoid fracture incidence: 8-38/100,000 Non-union 5% (0-22%) Adams and Leonard (1928) first described operative treatment of the
Scaphoid Non-union Dr. Mandel Dr. Gyomorey May 3 rd 2006 Introduction Scaphoid fracture incidence: 8-38/100,000 Non-union 5% (0-22%) Adams and Leonard (1928) first described operative treatment of the
SUTURING. 1. Promote wound healing with least amount of scar and deformity. Adherence to these 2 principles will dictate how a wound is handled, the
 SUTURIN Purpose A. Functional Close wound 2 Promote more rapid healing of wound Prevent Preserve infection function. Cosmetic 1. Promote wound healing with least amount of scar and deformity Adherence
SUTURIN Purpose A. Functional Close wound 2 Promote more rapid healing of wound Prevent Preserve infection function. Cosmetic 1. Promote wound healing with least amount of scar and deformity Adherence
NOTEWORTHY DECISION SUMMARY. Decision: WCAT-2005-02255-RB Panel: Rob Kyle Decision Date: April 29, 2005
 NOTEWORTHY DECISION SUMMARY Decision: WCAT-2005-02255-RB Panel: Rob Kyle Decision Date: April 29, 2005 Is Worker Occupation a Factor to Consider when Calculating Functional Impairment Permanent Disability
NOTEWORTHY DECISION SUMMARY Decision: WCAT-2005-02255-RB Panel: Rob Kyle Decision Date: April 29, 2005 Is Worker Occupation a Factor to Consider when Calculating Functional Impairment Permanent Disability
Fracture Care Coding September 28, 2011
 Fracture Care Coding September 28, 2011 Julie Edens Leu, CPC, CPCO, CPMA, CPC-I 1 Disclaimer Every reasonable effort has been made to ensure that the educational material provided today is accurate and
Fracture Care Coding September 28, 2011 Julie Edens Leu, CPC, CPCO, CPMA, CPC-I 1 Disclaimer Every reasonable effort has been made to ensure that the educational material provided today is accurate and
Definition: A joint or articulation is a place in the body where two bones come together.
 Definition: A joint or articulation is a place in the body where two bones come together. CLASSES OF JOINTS. 1. Joints are classified according to how the bones are held together. 2. The three types of
Definition: A joint or articulation is a place in the body where two bones come together. CLASSES OF JOINTS. 1. Joints are classified according to how the bones are held together. 2. The three types of
Self-Range of Motion Exercises for Shoulders, Arms, Wrists, Fingers
 Self-Range of Motion Exercises for Shoulders, Arms, Wrists, Fingers These exercises will help keep your muscles strong and mobile, and your joints flexible. Other benefits of these exercises include: C
Self-Range of Motion Exercises for Shoulders, Arms, Wrists, Fingers These exercises will help keep your muscles strong and mobile, and your joints flexible. Other benefits of these exercises include: C
Zimmer DeNovo NT Natural Tissue Graft
 Zimmer DeNovo NT Natural Tissue Graft Surgical Technique Biologic treatment for early intervention and cartilage repair. Overview DeNovo NT Natural Tissue Graft (Fig. 1) is an off-the-shelf human tissue,
Zimmer DeNovo NT Natural Tissue Graft Surgical Technique Biologic treatment for early intervention and cartilage repair. Overview DeNovo NT Natural Tissue Graft (Fig. 1) is an off-the-shelf human tissue,
.org. Rotator Cuff Tears: Surgical Treatment Options. When Rotator Cuff Surgery is Recommended. Surgical Repair Options
 Rotator Cuff Tears: Surgical Treatment Options Page ( 1 ) The following article provides in-depth information about surgical treatment for rotator cuff injuries, and is a continuation of the article Rotator
Rotator Cuff Tears: Surgical Treatment Options Page ( 1 ) The following article provides in-depth information about surgical treatment for rotator cuff injuries, and is a continuation of the article Rotator
Wrist and Hand Injuries Keep Your Edge: Hockey Sports Medicine 2015 Toronto, Canada August 28-30
 Wrist and Hand Injuries Keep Your Edge: Hockey Sports Medicine 2015 Toronto, Canada August 28-30 Steven E. Rokito, MD Division Chief, Sports Medicine, NSLIJ Associate team orthopedist NY Islanders Wrist
Wrist and Hand Injuries Keep Your Edge: Hockey Sports Medicine 2015 Toronto, Canada August 28-30 Steven E. Rokito, MD Division Chief, Sports Medicine, NSLIJ Associate team orthopedist NY Islanders Wrist
Provided by the American Venous Forum: veinforum.org
 CHAPTER 17 SURGICAL THERAPY FOR DEEP VALVE INCOMPETENCE Original author: Seshadri Raju Abstracted by Gary W. Lemmon Introduction Deep vein valvular incompetence happens when the valves in the veins (tubes
CHAPTER 17 SURGICAL THERAPY FOR DEEP VALVE INCOMPETENCE Original author: Seshadri Raju Abstracted by Gary W. Lemmon Introduction Deep vein valvular incompetence happens when the valves in the veins (tubes
Foot and Ankle Technique Guide Proximal Inter-Phalangeal (PIP) Fusion
 Fusion") Surgical Technique Foot and Ankle Technique Guide Proximal Inter-Phalangeal (PIP) Fusion Prepared in consultation with: Phinit Phisitkul, MD Department of Orthopedics and Rehabilitation University of Iowa
Surgical Technique Foot and Ankle Technique Guide Proximal Inter-Phalangeal (PIP) Fusion Prepared in consultation with: Phinit Phisitkul, MD Department of Orthopedics and Rehabilitation University of Iowa
How To Fix A Radial Head Plate
 Mayo Clinic CoNGRUENT RADIAL HEAD PLATE Since 1988 Acumed has been designing solutions to the demanding situations facing orthopedic surgeons, hospitals and their patients. Our strategy has been to know
Mayo Clinic CoNGRUENT RADIAL HEAD PLATE Since 1988 Acumed has been designing solutions to the demanding situations facing orthopedic surgeons, hospitals and their patients. Our strategy has been to know
INTERNATIONAL MEDICAL COLLEGE
 INTERNATIONAL MEDICAL COLLEGE Joint Degree Master Program: Implantology and Dental Surgery (M.Sc.) Basic modules: List of individual modules Basic Module 1 Basic principles of general and dental medicine
INTERNATIONAL MEDICAL COLLEGE Joint Degree Master Program: Implantology and Dental Surgery (M.Sc.) Basic modules: List of individual modules Basic Module 1 Basic principles of general and dental medicine
A Patient's Guide to Arthritis of the Finger Joints
 Introduction A Patient's Guide to Arthritis of the Finger Joints When you stop to think about how much you use your hands, it's easy to see why the joints of the fingers are so important. Arthritis of
Introduction A Patient's Guide to Arthritis of the Finger Joints When you stop to think about how much you use your hands, it's easy to see why the joints of the fingers are so important. Arthritis of
A Patient s Guide to Carpal Tunnel Syndrome
 A Patient s Guide to Carpal Tunnel Syndrome 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a
A Patient s Guide to Carpal Tunnel Syndrome 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a
Ulnar nerve decompression
 Patient information Ulnar nerve decompression This information has been produced to help you gain the maximum benefit and understanding of your condition and its treatment. It includes the following information:
Patient information Ulnar nerve decompression This information has been produced to help you gain the maximum benefit and understanding of your condition and its treatment. It includes the following information:
Traumatic Primary Eyelid and Facial Laceration Repair. Riva Lee Asbell Philadelphia, PA
 Traumatic Primary Eyelid and Facial Laceration Repair Riva Lee Asbell Philadelphia, PA I INTRODUCTION I always have to work a little harder when coding for traumatic eyelid and facial repairs. There is
Traumatic Primary Eyelid and Facial Laceration Repair Riva Lee Asbell Philadelphia, PA I INTRODUCTION I always have to work a little harder when coding for traumatic eyelid and facial repairs. There is
Upper Extremity MMI and Impairment Rating
 Upper Extremity MMI and Impairment Rating 1 How to Determine Maximum Medical Improvement 1. Understand the definition of MMI 2. Review the DWC Form-032, Request for Designated Doctor Examination 3. Review
Upper Extremity MMI and Impairment Rating 1 How to Determine Maximum Medical Improvement 1. Understand the definition of MMI 2. Review the DWC Form-032, Request for Designated Doctor Examination 3. Review
Arthroscopy of the Hand and Wrist
 Arthroscopy of the Hand and Wrist Arthroscopy is a minimally invasive procedure whereby a small camera is inserted through small incisions of a few millimeters each around a joint to view the joint directly.
Arthroscopy of the Hand and Wrist Arthroscopy is a minimally invasive procedure whereby a small camera is inserted through small incisions of a few millimeters each around a joint to view the joint directly.
ARTHROSCOPIC HIP SURGERY
 ARTHROSCOPIC HIP SURGERY Hip Arthroscopy is a relatively simple procedure whereby common disorders of the hip can be diagnosed and treated using keyhole surgery. Some conditions, which previously were
ARTHROSCOPIC HIP SURGERY Hip Arthroscopy is a relatively simple procedure whereby common disorders of the hip can be diagnosed and treated using keyhole surgery. Some conditions, which previously were
Bard * PerFix * Plug. Technique Guide. A Modified Technique with the. Open Inguinal Hernia Repair
 A Modified Technique with the Bard * PerFix * Plug A quick and simple preperitoneal underlay Modified Technique for the repair of groin hernias Technique Guide Open Inguinal Hernia Repair This technique,
A Modified Technique with the Bard * PerFix * Plug A quick and simple preperitoneal underlay Modified Technique for the repair of groin hernias Technique Guide Open Inguinal Hernia Repair This technique,
Chapter 21. How to do fasciotomy. neighboring structures
 Chapter 21 FRACTURES OF THE TIBIA AND FIBULA KEY FIGURES: Calf anatomy How to do fasciotomy Gastrocnemius and neighboring structures Longstanding open fracture Gastrocnemius flap Fractures of the tibia
Chapter 21 FRACTURES OF THE TIBIA AND FIBULA KEY FIGURES: Calf anatomy How to do fasciotomy Gastrocnemius and neighboring structures Longstanding open fracture Gastrocnemius flap Fractures of the tibia
Bankart Repair using the Smith & Nephew BIORAPTOR 2.9 Suture Anchor
 Shoulder Series Technique Guide *smith&nephew BIORAPTOR 2.9 Suture Anchor Bankart Repair using the Smith & Nephew BIORAPTOR 2.9 Suture Anchor Gary M. Gartsman, M.D. Introduction Arthroscopic studies of
Shoulder Series Technique Guide *smith&nephew BIORAPTOR 2.9 Suture Anchor Bankart Repair using the Smith & Nephew BIORAPTOR 2.9 Suture Anchor Gary M. Gartsman, M.D. Introduction Arthroscopic studies of
Endoscopic Plantar Fasciotomy
 Endoscopic Plantar Fasciotomy Introduction Plantar fasciitis is a common condition that causes pain centralized around the heel. It may be severe enough to affect regular activities. Health care providers
Endoscopic Plantar Fasciotomy Introduction Plantar fasciitis is a common condition that causes pain centralized around the heel. It may be severe enough to affect regular activities. Health care providers
Ulnar sided Wrist Pain
 Ulnar sided Wrist Pain 1 Susan Cross, 1 Anshul Rastogi, 2 Brian Cohen, 1 Rosy Jalan 1 Dept of Radiology, Barts Health NHS Trust, London, UK 2 London Orthopaedic Centre Contact: susan.cross@bartshealth.nhs.uk
Ulnar sided Wrist Pain 1 Susan Cross, 1 Anshul Rastogi, 2 Brian Cohen, 1 Rosy Jalan 1 Dept of Radiology, Barts Health NHS Trust, London, UK 2 London Orthopaedic Centre Contact: susan.cross@bartshealth.nhs.uk
ADVANCED SUTURING WORKSHOP ANN BECKER, APRN-CNP; TONI PRATT-REID, APRN-CNP
 ADVANCED SUTURING WORKSHOP ANN BECKER, APRN-CNP; TONI PRATT-REID, APRN-CNP SUTURING WORKSHOP! The technique of suturing, as a method for closing cutaneous wounds has been a part of medicine for hundreds
ADVANCED SUTURING WORKSHOP ANN BECKER, APRN-CNP; TONI PRATT-REID, APRN-CNP SUTURING WORKSHOP! The technique of suturing, as a method for closing cutaneous wounds has been a part of medicine for hundreds
Calcaneus (Heel Bone) Fractures
 Fractures") Copyright 2010 American Academy of Orthopaedic Surgeons Calcaneus (Heel Bone) Fractures Fractures of the heel bone, or calcaneus, can be disabling injuries. They most often occur during high-energy collisions
Copyright 2010 American Academy of Orthopaedic Surgeons Calcaneus (Heel Bone) Fractures Fractures of the heel bone, or calcaneus, can be disabling injuries. They most often occur during high-energy collisions
PRACTICE GUIDELINE TITLE: INTRAVENOUS LINE INSERTION: PERIPHERAL AND CENTRAL
 PRACTICE GUIDELINE Effective Date: 9-17-04 Manual Reference: Deaconess Trauma Services TITLE: INTRAVENOUS LINE INSERTION: PERIPHERAL AND CENTRAL PURPOSE: To outline the indications and options for intravenous
PRACTICE GUIDELINE Effective Date: 9-17-04 Manual Reference: Deaconess Trauma Services TITLE: INTRAVENOUS LINE INSERTION: PERIPHERAL AND CENTRAL PURPOSE: To outline the indications and options for intravenous
Shoulder Arthroscopy
 Copyright 2011 American Academy of Orthopaedic Surgeons Shoulder Arthroscopy Arthroscopy is a procedure that orthopaedic surgeons use to inspect, diagnose, and repair problems inside a joint. The word
Copyright 2011 American Academy of Orthopaedic Surgeons Shoulder Arthroscopy Arthroscopy is a procedure that orthopaedic surgeons use to inspect, diagnose, and repair problems inside a joint. The word
Lesions, and Masses, and Tumors Oh My!!
 Lesions, and Masses, and Tumors Oh My!! Presented by: Susan Ward, CPC, CPC-H, CPC-I, CPCD, CEMC, CPRC 1 1 CPT GUIDELINES Agenda CPT DEFINITIONS OP REPORT CASES 2 Definitions Cyst - a closed sac having
Lesions, and Masses, and Tumors Oh My!! Presented by: Susan Ward, CPC, CPC-H, CPC-I, CPCD, CEMC, CPRC 1 1 CPT GUIDELINES Agenda CPT DEFINITIONS OP REPORT CASES 2 Definitions Cyst - a closed sac having
Common Hand and Wrist Conditions: When to Refer? Dr Tim Heath
 Common Hand and Wrist Conditions: When to Refer? Dr Tim Heath Difficult Balance Many hand conditions can be managed non-operatively / simply Missed injury or delayed diagnosis not uncommon Common Problems
Common Hand and Wrist Conditions: When to Refer? Dr Tim Heath Difficult Balance Many hand conditions can be managed non-operatively / simply Missed injury or delayed diagnosis not uncommon Common Problems
Ventral Hernia Repair
 Ventral Hernia Repair Open and Laparoscopic Ventral Hernia Repair Technique Guide Ventrio ST Hernia Patch Ventrio Hernia Patch This Technique Guide contains the opinions of and personal surgical techniques
Ventral Hernia Repair Open and Laparoscopic Ventral Hernia Repair Technique Guide Ventrio ST Hernia Patch Ventrio Hernia Patch This Technique Guide contains the opinions of and personal surgical techniques
CPT Coding for Hand and Upper Extremity Surgery
 CPT Coding for Hand and Upper Extremity Surgery Taizoon H Baxamusa, MD, FACS Hand, Upper Extremity, & Microvascular Surgery The Illinois Bone & Joint Institute Morton Grove, IL Orthopaedic Hand & Upper
CPT Coding for Hand and Upper Extremity Surgery Taizoon H Baxamusa, MD, FACS Hand, Upper Extremity, & Microvascular Surgery The Illinois Bone & Joint Institute Morton Grove, IL Orthopaedic Hand & Upper
Laparoscopic Repair of Hernias. A simple guide to help answer your questions
 Laparoscopic Repair of Hernias A simple guide to help answer your questions What is a hernia? A hernia is defined as a hole or defect in the abdominal (belly) wall. A hernia can either be congenital (a
Laparoscopic Repair of Hernias A simple guide to help answer your questions What is a hernia? A hernia is defined as a hole or defect in the abdominal (belly) wall. A hernia can either be congenital (a
Eric M. Kutz, D.O. Arlington Orthopedics Harrisburg, PA
 Eric M. Kutz, D.O. Arlington Orthopedics Harrisburg, PA 2 offices 805 Sir Thomas Court Harrisburg 3 Walnut Street Lemoyne Mechanism of injury Repetitive overhead activities Falls to the ground Falls with
Eric M. Kutz, D.O. Arlington Orthopedics Harrisburg, PA 2 offices 805 Sir Thomas Court Harrisburg 3 Walnut Street Lemoyne Mechanism of injury Repetitive overhead activities Falls to the ground Falls with
MAURICE CULMER O'SHEA, M.D. NEW YORK TABLE I NATURE OF AGENT CAUSING INJURY. i6 of 33 Known Causes Were Compensation Injuries
 SEVERED TENDONS AND NERVES OF THE HAND AND FOREARM MAURICE CULMER O'SHEA, M.D. NEW YORK FROM THE SECOND SURGICAL DIVISION, ST. VINCENT'S HOSPITAL, NEW YORK CITY, N. Y. Two HUNDRED NINETY severed tendons
SEVERED TENDONS AND NERVES OF THE HAND AND FOREARM MAURICE CULMER O'SHEA, M.D. NEW YORK FROM THE SECOND SURGICAL DIVISION, ST. VINCENT'S HOSPITAL, NEW YORK CITY, N. Y. Two HUNDRED NINETY severed tendons
WRIST EXAMINATION. Look. Feel. Move. Special Tests
 WRIST EXAMINATION Look o Dorsum, side, palmar- palmar flex wrist to exacerbate dorsal swellings o Deformity e.g. radial deviation after colles, prominent ulna o Swellings e.g. ganglion o Scars, muscle
WRIST EXAMINATION Look o Dorsum, side, palmar- palmar flex wrist to exacerbate dorsal swellings o Deformity e.g. radial deviation after colles, prominent ulna o Swellings e.g. ganglion o Scars, muscle
TREATMENT 1. Control bleeding by applying pressure over wound with Gauze Pads (Surgical Supply-4). 2. Contact Surgeon for laceration repair options.
. 2. Contact Surgeon for laceration repair options.") Page 1 of 8 pages NOTE Contact Surgeon before giving any medication marked with an asterisk. In an emergency or during Loss of Signal, begin appropriate treatment; then call Surgeon as soon as possible.
Page 1 of 8 pages NOTE Contact Surgeon before giving any medication marked with an asterisk. In an emergency or during Loss of Signal, begin appropriate treatment; then call Surgeon as soon as possible.
Managing cavity wounds Journal of Community Nursing March 1998 Author: Rosemary Pudner
 Managing cavity wounds Journal of Community Nursing March 1998 Author: Rosemary Pudner It has been seen in recent years, that an increasing number of patients are being discharged early into the community,
Managing cavity wounds Journal of Community Nursing March 1998 Author: Rosemary Pudner It has been seen in recent years, that an increasing number of patients are being discharged early into the community,
Preparing to Suture. 6 th Annual Pediatric Advanced Practice Conference Tuesday, February 9, 2016 1:30 pm. Workshop B: Suturing for Beginners
 Preparing to Suture Kristen Devick, MPAS, PA-C University of Colorado Department of Emergency Medicine NONE! Skin Anatomy Trott, 2012, p.11 Preparing to suture Initial evaluation Hemostasis Anesthesia
Preparing to Suture Kristen Devick, MPAS, PA-C University of Colorado Department of Emergency Medicine NONE! Skin Anatomy Trott, 2012, p.11 Preparing to suture Initial evaluation Hemostasis Anesthesia
Nursing Management of Patient with Casting
 Nursing Management of Patient with Casting Elsa CHUNG Workshop on Trauma Management with Cast Application 5 July 2009 (Sunday) Functions A rigid external immobilizer to secure body part To maintain support
Nursing Management of Patient with Casting Elsa CHUNG Workshop on Trauma Management with Cast Application 5 July 2009 (Sunday) Functions A rigid external immobilizer to secure body part To maintain support
ALBERTA HEALTH CARE INSURANCE PLAN
 ALBERTA HEALTH CARE INSURANCE PLAN Podiatry Procedure List As Of 01 October 2007 ALBERTA HEALTH CARE INSURANCE PLAN Page i Generated 2007/09/26 TABLE OF CONTENTS As of 2007/10/01 I. CERTAIN DIAGNOSTIC
ALBERTA HEALTH CARE INSURANCE PLAN Podiatry Procedure List As Of 01 October 2007 ALBERTA HEALTH CARE INSURANCE PLAN Page i Generated 2007/09/26 TABLE OF CONTENTS As of 2007/10/01 I. CERTAIN DIAGNOSTIC
Functional rehab after breast reconstruction surgery
 Functional rehab after breast reconstruction surgery UHN A guide for women who had DIEP, latissimus dorsi with a tissue expander or implant, or two-stage implant based breast reconstruction surgery Read
Functional rehab after breast reconstruction surgery UHN A guide for women who had DIEP, latissimus dorsi with a tissue expander or implant, or two-stage implant based breast reconstruction surgery Read