Standardization of Response Assessment: Methods, Analysis and Reporting: From RECIST to PERCIST 1.0
|
|
|
- Chad Noel Norton
- 7 years ago
- Views:
Transcription
1 Standardization of Response Assessment: Methods, Analysis and Reporting: From RECIST to PERCIST 1.0 Richard L. Wahl, M.D. Division of Nuclear Medicine Johns Hopkins Medical Institutes Baltimore, MD
2 PET/CT is a Qualitative and a Quantitative Method Most applications to date have been Qualitative In treatment response assessment, especially if looking for small treatment induced changes, Quantitation will be needed Quantitation requires greater attention to technical details than qualitative imaging Standardization of methods including Analytical Methods is required
3 No standardized and validated quantitative metabolic response criteria exist

4 EORTC 1999
5 CR EORTC Response Criteria Complete Disappearance of all Metabolically Active Tumor (i.e. decreased to background levels) PR >15% decline in SUV after 1 cycle, >25% decline after 2 or more cycles. Reduction in extent (size) of FDG uptake is not required SD PMD Increase in FDG SUV of <25% or decrease of <15% in SUV and no increase in extent of uptake (<20% in longest dimension) Increase in SUV of over 25%, Increase in extent of FDG uptake by >20%, New FDG positive metastases
6 EORTC Criteria Limitations Individual tumor changes in SUV Retrospective data Limited patient number tumor and treatment types Young et al. Eur J Cancer 1999;35:1773
7 Questions Remaining? What Size ROI What SUV value Best cut-off values for SUV percent change vs. absolute floor different diseases and treatments Number of lesions How to calculate percent change Discrepancies on PET & anatomic imaging
8 If there were RECIST Criteria for PET, they Would be Defined as
9 PERCIST Positron Emission Response Criteria in Solid Tumors
10 J Nucl Med : 122S-150S
11 Standardized PET Techniques National Cancer Institute Shankar et al. J Nucl Med 2006;47: Netherlands protocol Boellaard et al. Eur J Nucl Med Mol Imaging 2008;35:
12 Key Elements of PERCIST Suggested Standardization of: Tumor to be assessed (hottest, statistical considerations applied vs background) Size of ROI applied, Type of SUV (SUV lean) Timing of scan (explicit allowances) Quality of Data: including normal tissue reference region Reporting: Continous, Timing, Normal tissue
13 What is Measured? Lean Body Mass Corrected SUV SUL Peak In Hottest Tumor Focus
14 Figure 1a. Graphs depict the relationships between patient body weight and blood SUVs: (a) SUVbw, (b) SUVibw, (c) SUVlbm, or (d) SUVbsa Sugawara, Y. et al. Radiology 1999;213: Copyright Radiological Society of North America, 1999
15 Figure 1c. Graphs depict the relationships between patient body weight and blood SUVs: (a) SUVbw, (b) SUVibw, (c) SUVlbm, or (d) SUVbsa Sugawara, Y. et al. Radiology 1999;213: Copyright Radiological Society of North America, 1999
16 Introduction A number of different ROI definitions have been employed including: Mean within an irregular ROI defined by isocontours. Isocontour Mean within a fixed size ROI centered on the most metabolically active region. Maximum pixel within a large ROI encompassing the entire tumor. Fixed size SUV max has been widely used although single pixel measurements of this sort may be compromised when images have high levels of noise. Maximum pixel
17 Quantifying Metabolic Tumor Response to Therapy: The Influence of Image Noise on Maximum and Mean SUV. MA Lodge, J P Leal, RL Wahl Russell H. Morgan Department of Radiology and Radiological Sciences Johns Hopkins University School of Medicine Baltimore, MD

18 Results: Statistical Quality 2D 3D 0.5 min 2 min 3.5 min 5 min 20 min Statistical quality of the images deteriorates with decreasing scan duration for both 2D and 3D. Decay of the isotope also contributes to increasing noise.

19 Results: ROI max 0.5 minute acquisition SUV max = minute acquisition SUV max = 2.57 Insert has an SUV of 2.5 (2.5:1 insert-to-background ratio).
20 Conclusions ROI max Maximum pixel within lesion. Increasing positive bias as noise increased. ROI 42% Mean of all pixels within an irregular ROI based on an isocontour at 42% of the maximum pixel. Increasing positive bias as noise increased. ROI 9x9 Mean of all pixels within a small 9 mm x 9 mm region. No bias found as noise increased.
21 SUL max Limitations Size of ROI variable scanner matrix size slice thickness scanner diameter Precision depends on ROI size Single-pixel more variable due to noise* Nahmias, Wahl LM. J Nucl Med 2008;49:1804 Boellard et al. J Nucl Med 2004;45:1519
22 SUL peak 1.2 cm diameter (1 cm 3 volume sphere) Centered around hottest area in tumor Standardizes ROI size Maybe less variance than SUL max
23 Intra-subject Variability of SUV Same tumor measured multiple times Large tumors with high metabolism Best ~ 6-10% Worst ~43% Larger fixed ROIs more reproducible Current scanners smaller voxel size Minn et al. Radiology 1995;196:167 Weber et al. J Nucl Med 1999;40:1771 Nakamoto et al. Mol Imaging Biol 2002;4:171
24 Other methods Threshold Varies w/variability of single pixel max Tumor lesion glycolysis Less practical Based on threshold method Exploratory Still promising
25 Partial-volume Effect Not included in PERCIST Size measurements possible with PET/CT errors particularly small tumors No standardized accepted method
26 Factors that Affect SUV Uptake time Blood glucose level Body weight Injection technique Camera calibration Partial volume Region of interest (ROI) Reconstruction method Matrix size Sugawara et al. Radiology 1999; 213:521 Hamberg et al. J Nucl Med 1994; 35:1308 Weber WA et al. J Nucl Med 1999; 40:1771 Torizuka T et al. Radiology 1997; 203:169 Jaskowiak CJ et al. J Nucl Med 2005; 46:424 Schoder H, et al. J Nucl Med 2004; 45:559
27 Consistency in SUV lean Same Scanner or Model Calibrated Same software Similar technical parameters Sugawara et al. Radiology 1999; 213:521 Hamberg et al. J Nucl Med 1994; 35:1308 Weber WA et al. J Nucl Med 1999; 40:1771 Torizuka T et al. Radiology 1997; 203:169 Jaskowiak CJ et al. J Nucl Med 2005; 46:424 Schoder H, et al. J Nucl Med 2004; 45:559
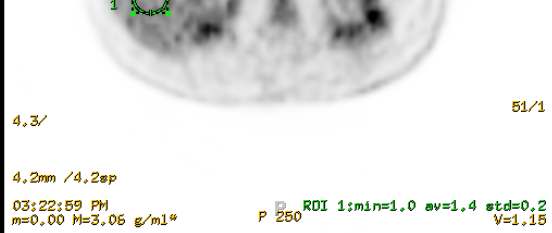
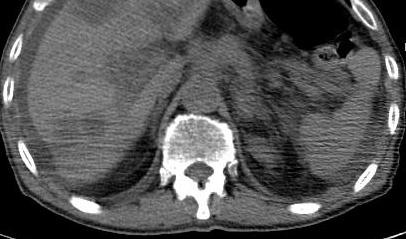
28 What is Measured? PERCIST Measurable target lesion is hottest single tumor lesion SUL of maximal 1.2 cm diameter volume ROI in tumor (SUL peak). SUL peak is at least 1.5 fold greater than liver SUL mean+ 2SD(in 3 cm spherical ROI in normal right lobe of liver). If liver is abnormal, primary tumor should have uptake >2.0 times SUL mean of blood pool in a 1 cm diameter ROI in the descending thoracic aorta extended over 2 cm Z axis. The tumor with the maximum SUL peak is assessed post -treatment. While typically this is in the same region of the tumor with the highest SUL peak at baseline, it need not be.
29 What is Measured? Uptake measurements should be made for the peak and maximum single voxel tumor SUL. Other SUV metrics including SUL mean at 50 or 70% of SUV peak can be collected as exploratory data, TLG can be collected ideally based on voxels more intense than 2SD above liver mean SUL These parameters on up to 5 measurable target lesions can be recorded as exploratory data, typically the 5 hottest lesions, which are typically the largest, not over 2 /organ. Tumor size of these lesions can be determined per RECIST 1.1.
30 Measurable Lesions FDG uptake and not tumor size Minimum uptake 1.5 x liver SUL mean + 2 SD To allow for sufficient fall in SUL posttreatment Alternatives: 2 x blood pool SUL mean + 2 SD 1.35 x hepatic uptake (prob too low as exploratory alternative)
31 Normalization for Quality Control -Normal liver SUL must be within 20% (and <0.3 SUL mean units) for baseline and follow up study to be assessable.-if liver is abnormal, blood pool SUL must be within 20% (and <0.3 SUL mean units) for baseline and follow up study to be assessable.- Uptake time of baseline study and follow up study 2 must be within 15 minutes of one another to be assessable. Typically, these are at a mean of 60 minutes post injection, but not less than 50 min post injection.
32
33 Normal Background Scan to Scan Difference Within ± 20% and 0.3 SUL units Comparable uptake times!
34 Complete Metabolic Response Complete metabolic response (CMR) complete resolution of [18F]-FDG uptake within the measurable target lesion so that it is less than mean liver activity and indistinguishable from surrounding background blood pool levels. Disappearance of all other lesions to background blood pool levels. % decline in SUL should be recorded from measurable region as well as (ideally) time in weeks after treatment was begun (i.e. CMR -90, 4). No new FDG avid lesions in a pattern typical of cancer. If progression by RECIST must verify with follow up


35 Continued declines out to 24 weeks A B C CT PET FUSED
36 Partial Metabolic Response (PMR) Reduction of a minimum of 30% in target measurable tumor FDG SUL peak. Absolute drop in SUL must be at least 0.8 SUL units, as well. Measurement is commonly in the same lesion as the baseline, but can be another lesion if that lesion was previously present and is most active lesion after treatment. ROI does not have to be in precisely the same area as baseline scan, though typically it is. No increase, >30% in SUL or size of target or non target lesions (i.e. no PD by RECIST or IWC) (If PD anatomically, must verify with follow up). A reduction in the extent of the tumor FDG uptake is not a requirement for partial metabolic response. % decline in SUL should be recorded as well as (ideally) time in weeks after treatment was begun (i.e. PMR -40, 3). No new lesions.
37 Partial Response 30% SUL peak EORTC: 15-25% 10-20% variability of SUV Lower thresholds, medically relevant 25% of a low number not much change 0.8 SUL units 0.9 and 0.5 SUV units previously proposed* *Weber et al. J Nucl Med 1999;40:1771 *Nahmias et al. J Nucl Med 2008;49:1804
38 Partial Response Target All others 30% SUL peak No 30% SUL or size 0.8 SUL units No new FDG avid lesions Anatomic PD verify
39 1 2
40 Stable Metabolic Disease Stable metabolic disease (SMD) Not CMR, PMR nor PMD. Note, the SUL peak in metabolic target lesion should be recorded as well as (ideally) time from start of most recent therapy in weeks (i.e. SMD - 15,7). No new lesions
41 Progressive metabolic disease >30% increase in FDG SUL peak, with >0.8 SUL unit increase in tumor SUV peak from the baseline scan in pattern typical of tumor and not of infection/treatment effect. OR- Visible increase in the extent of [18F]-FDG tumor uptake (75% in TLG volume with no decline in SUL. OR - new [18F]-FDG avid lesions which are typical of cancer and not related to treatment effect or infection. PMD other than new visceral lesions should be confirmed on follow up study within 1 month unless PMD also is clearly associated with progressive disease by RECIST 1.1. PMD should be reported to include % change in SUV peak, (ideally time post treatment in weeks) and whether new lesions are present/absent and their number (i.epmd, +35, 4, New-5).

42 1 2
43 PERCIST Continuous Response Scale SUL is a continuous variable Dividing response criteria into a limited number of somewhat arbitrary response categories loses much data. PERCIST preserves percent declines in the SUV peak in each reported category. The rapidity with which a scan normalizes is important (faster appears better), PERCIST 1.0 includes time from start of treatment as part of the reporting. CMR 90, 1 is probably superior to a CMR 90, 10, especially if the latter patient were SMD 20,1. More than one measurement of PET response may be needed at differing times and it may be treatment type dependent.
44 Number of Lesions: PET Early studies: 1 large lesion Not specified in 1999 EORTC criteria Various approaches
45 Number of Lesions PERCIST 1.0 only evaluates the SUL peak of the hottest tumor. This is a possible limitation of the approach, but lesions and their responses are highly correlated in general. Additional data are required to determine how many lesions should be assessed over 1. An option is to include the 5 hottest lesions, or the 5 observed on RECIST 1.1 which are the most measurable. % change in SUL can be reported for the single lesion with the largest increase in uptake or the smallest decline in uptake. Additional studies will be needed to define how many lesions are optimal for assessment and whether summed TLG of all lesions is superior

46
47 FDG PET Quantitative Metabolic Tumor Response Assessment: Is the Number of Target Lesions Evaluated Important? H.A. Jacene and R.L. Wahl Russell H. Morgan Department of Radiology and Radiological Science Johns Hopkins University Baltimore, MD
48 Objective To determine if there is a difference in quantitative metabolic tumor response classification on FDG PET/CT based on 1, 3, 5 or 6 target lesions
49 Methods 30 pts receiving RIT for lymphoma 6 target lesions with highest SUV (SULmax) SUVs of these 6 target lesions summed Pre-RIT summed SUV Post-RIT summed SUV Percent change in summed SUV determined Repeated w/1, 3, & 5 lesions w/highest SUVs Jacene et al. J Nucl Med 2009;50:8
50 Correlation % Change in SUL No. Lesions p<0.01 Jacene et al. J Nucl Med 2009;50:8
51 Biologically Relevant? 1 o response predicts outcomes in metastases Same lesions before and after treatment Worst responding lesion lesion with least change highest uptake before and after treatment
52 18% Lin et al. J Nucl Med 2007;48:1626
53 PERCIST: Primary Response Analysis Single hottest lesions Percent change in SUL peak
54 Elements of Reporting Time from injection until imaging SUV mean of liver Serum Glucose SUV Lean Peak of hottest lesion (and max) Structured reporting including key parametric indices Presence and # of new lesions
55 Baseline Post 2 cycles SMD, -20, 8
56 Exploratory Analyses SUL peak for up to 5 lesions Change in summed SUL Total lesion glycolysis
57 Some of the Limitations Actually getting SUL peak Is the minimum value too high? Lack of good data for progression
58 Inter-Observer Variability of SUV Same tumor data set measured multiple times by independent observers 100% agreement in SUV determination Minn et al, Radiology, tumors each measured twice by 2 independent observers Semi-automated image analysis software Good inter-observer agreement Marom et al J Thorac Imaging readers measured 20 primary tumors four times Untreated primary lung cancers on average > 2 cm
59 Assessment of Inter-observer Reproducibility in Quantitative FDG PET and CT Measurements of Tumor Response to Therapy HA Jacene, S Leboulleux, S Baba, D Chatzifotiadis, B Goudarzi, O Teytelbaum, Horton, I Kamel, K Macura, H Tsai, J Kowalski and RL Wahl J Nucl Med 2009;50:
60 Objectives To directly compare inter-observer reproducibility of 1) SUV & CT size measurements in malignant tumors pre- and post-therapy 2) % change in SUV & CT size measurements in response to therapy Jacene et al. J Nucl Med 2009;50:1760-9
61 Percent change 2D CT size ICC 0.33 Jacene et al. J Nucl Med 2009;50:1760-9
62 Percent change Longest CT size ICC 0.70 Jacene et al. J Nucl Med 2009;50:1760-9
63 Percent change SUV bw max ICC 0.94 Jacene et al. J Nucl Med 2009;50:1760-9
64 PET Metric of SUV More Reproducible than Tumor Size for Rx Response Tests of change in metabolism and lesion size by experienced anatomic and metabolic readers. WHO 2D size change least reproducible RECIST 1D size change intermediate PERCIST-like SUV max change most reproducible
65 Suggestions for PERCIST 1.0 Implementation Collect the data in a consistent manner Determine prognostic value Determine deficiencies Refine Consider including PERCIST elements in structured reports (i.e. uptake time, normal tissue SUV lean, SUL hottest lesion). Suggested starting point for clinical trials and practice including PET quantitation.
66 Summary Standardization of acquisitions and analysis of PET data is essential for comparability of studies across centers PERCIST provides a framework for analysis and allows exploration of alternative metrics Comparison of reader studies of treatment response shows quantitation of PET response assessments are MUCH more reproducible than accepted WHO or RECIST criteria.
67 Heather Jacene, M.D. Martin Lodge, Ph.D. Yvette Kasamon, M.D. Acknowledgements
Moving Beyond RECIST
 Moving Beyond RECIST Ihab R. Kamel, M.D., Ph.D. ikamel@jhmi.edu Associate Professor Clinical Director, MRI Department of Radiology The Johns Hopkins University School of Medicine Outline Standard measures
Moving Beyond RECIST Ihab R. Kamel, M.D., Ph.D. ikamel@jhmi.edu Associate Professor Clinical Director, MRI Department of Radiology The Johns Hopkins University School of Medicine Outline Standard measures
Quantitative Imaging In Clinical Trials Using PET/CT: Update
 Quantitative Imaging In Clinical Trials Using PET/CT: Update Paul Kinahan, Robert Doot Imaging Research Laboratory Department of Radiology University of Washington, Seattle, WA Supported by RSNA Quantitative
Quantitative Imaging In Clinical Trials Using PET/CT: Update Paul Kinahan, Robert Doot Imaging Research Laboratory Department of Radiology University of Washington, Seattle, WA Supported by RSNA Quantitative
Comparison of Threshold-Based Segmentation Methods on Pre- and Post- Therapy PET Scans
 M. Phillips, S.F. Barrington, D.L.G. Hill, P.K. Marsden 1 Comparison of Threshold-Based Segmentation Methods on Pre- and Post- Therapy PET Scans Michael Phillips 1 Michael.Phillips.1@city.ac.uk Sally F.
M. Phillips, S.F. Barrington, D.L.G. Hill, P.K. Marsden 1 Comparison of Threshold-Based Segmentation Methods on Pre- and Post- Therapy PET Scans Michael Phillips 1 Michael.Phillips.1@city.ac.uk Sally F.
False positive PET in lymphoma
 False positive PET in lymphoma Thomas Krause Introduction and conclusion 2 3 Introduction 4 FDG-PET in staging of lymphoma 34 studies with 2227 Patients CT FDG-PET Sensitivity 63 % 89 % (58%-100%) (63%-100%)
False positive PET in lymphoma Thomas Krause Introduction and conclusion 2 3 Introduction 4 FDG-PET in staging of lymphoma 34 studies with 2227 Patients CT FDG-PET Sensitivity 63 % 89 % (58%-100%) (63%-100%)
QUANTITATIVE IMAGING IN MULTICENTER CLINICAL TRIALS: PET
 Centers for Quantitative Imaging Excellence (CQIE) LEARNING MODULE QUANTITATIVE IMAGING IN MULTICENTER CLINICAL TRIALS: PET American College of Radiology Clinical Research Center v.1 Centers for Quantitative
Centers for Quantitative Imaging Excellence (CQIE) LEARNING MODULE QUANTITATIVE IMAGING IN MULTICENTER CLINICAL TRIALS: PET American College of Radiology Clinical Research Center v.1 Centers for Quantitative
Malignant Pleural Diseases Advances Clinicians Should Know F Gleeson
 Malignant Pleural Diseases Advances Clinicians Should Know F Gleeson The following relevant disclosures, conflicts of interest and/ or financial relationships exist related to this presentation: Consultant
Malignant Pleural Diseases Advances Clinicians Should Know F Gleeson The following relevant disclosures, conflicts of interest and/ or financial relationships exist related to this presentation: Consultant
Uso della PET nella valutazione della risposta
 La diagnostica per immagini e la radioterapia: una cooperazione nel nostro futuro Uso della PET nella valutazione della risposta Cagliari, 21 giugno 2008 Arturo Chiti Medicina Nucleare, Istituto Clinico
La diagnostica per immagini e la radioterapia: una cooperazione nel nostro futuro Uso della PET nella valutazione della risposta Cagliari, 21 giugno 2008 Arturo Chiti Medicina Nucleare, Istituto Clinico
Case Report: Whole-body Oncologic Imaging with syngo TimCT
 Case Report: Whole-body Oncologic Imaging with syngo TimCT Eric Hatfield, M.D. 1 ; Agus Priatna, Ph.D. 2 ; John Kotyk, Ph.D. 1 ; Benjamin Tan, M.D. 1 ; Alto Stemmer 3 ; Stephan Kannengiesser, Ph.D. 3 ;
Case Report: Whole-body Oncologic Imaging with syngo TimCT Eric Hatfield, M.D. 1 ; Agus Priatna, Ph.D. 2 ; John Kotyk, Ph.D. 1 ; Benjamin Tan, M.D. 1 ; Alto Stemmer 3 ; Stephan Kannengiesser, Ph.D. 3 ;
Objective tumor response and RECIST criteria in cancer clinical trials Jian Yu, I3, Indianapolis, Indiana
 Paper PO01 Objective tumor response and RECIST criteria in cancer clinical trials Jian Yu, I3, Indianapolis, Indiana Abstract Objective tumor response is one of primary endpoints for efficacy in cancer
Paper PO01 Objective tumor response and RECIST criteria in cancer clinical trials Jian Yu, I3, Indianapolis, Indiana Abstract Objective tumor response is one of primary endpoints for efficacy in cancer
PET. Can we afford PET-CT. Positron annihilation. PET-CT scanner. PET detection
 PET-CT Can we afford PET-CT John Buscombe New technology Combines functional information-pet anatomical information-ct Machine able to perform both studies in single imaging episode PET imaging depends
PET-CT Can we afford PET-CT John Buscombe New technology Combines functional information-pet anatomical information-ct Machine able to perform both studies in single imaging episode PET imaging depends
PET/CT: Basic Principles, Applications in Oncology
 PET/CT: Basic Principles, Applications in Oncology Mabel Djang, HMS III Overview PET Basics and Limitations PET/CT - Advantages and Limitations Applications of PET/CT in oncology Summary 2 Principles of
PET/CT: Basic Principles, Applications in Oncology Mabel Djang, HMS III Overview PET Basics and Limitations PET/CT - Advantages and Limitations Applications of PET/CT in oncology Summary 2 Principles of
Response Criteria for Malignant Lymphoma 2007. Cheson Criteria. Quick Reference Guide
 Response Criteria for Malignant Lymphoma 2007 Cheson Criteria Quick Reference Guide Table of Contents Summary of Assessments...3 Baseline Lesion Burden...4 What isameasurable Lesion?...5 Choosing Target
Response Criteria for Malignant Lymphoma 2007 Cheson Criteria Quick Reference Guide Table of Contents Summary of Assessments...3 Baseline Lesion Burden...4 What isameasurable Lesion?...5 Choosing Target
PET/CT-MRI First clinical experience
 20 th April 2013, Barcelona, Sp PET/CT-MRI First clinical experience Philippe Appenzeller, MD Staff Radiologist and Nuclear Medicine Physician Department Medical Imaging, University Hospital Zurich PET/CT-MR
20 th April 2013, Barcelona, Sp PET/CT-MRI First clinical experience Philippe Appenzeller, MD Staff Radiologist and Nuclear Medicine Physician Department Medical Imaging, University Hospital Zurich PET/CT-MR
PET/CT in Lung Cancer
 PET/CT in Lung Cancer Rodolfo Núñez Miller, M.D. Nuclear Medicine and Diagnostic Imaging Section Division of Human Health International Atomic Energy Agency Vienna, Austria GLOBOCAN 2012 #1 #3 FDG-PET/CT
PET/CT in Lung Cancer Rodolfo Núñez Miller, M.D. Nuclear Medicine and Diagnostic Imaging Section Division of Human Health International Atomic Energy Agency Vienna, Austria GLOBOCAN 2012 #1 #3 FDG-PET/CT
PET/CT in Lymphoma. Ur Metser, M.D. Division Head, Molecular Imaging Joint Department of Medical Imaging, UHN- MSH- WCH University of Toronto
 PET/CT in Lymphoma Ur Metser, M.D. Division Head, Molecular Imaging Joint Department of Medical Imaging, UHN- MSH- WCH University of Toronto Outline 1. Introduction: PET/CT, how does it work? 2.Current
PET/CT in Lymphoma Ur Metser, M.D. Division Head, Molecular Imaging Joint Department of Medical Imaging, UHN- MSH- WCH University of Toronto Outline 1. Introduction: PET/CT, how does it work? 2.Current
Validation and Calibration. Definitions and Terminology
 Validation and Calibration Definitions and Terminology ACCEPTANCE CRITERIA: The specifications and acceptance/rejection criteria, such as acceptable quality level and unacceptable quality level, with an
Validation and Calibration Definitions and Terminology ACCEPTANCE CRITERIA: The specifications and acceptance/rejection criteria, such as acceptable quality level and unacceptable quality level, with an
Molecular Imaging in Early Phase Oncology Trials
 Molecular Imaging in Early Phase Oncology Trials Lessons Learned Potential Role for SNM Network Susan Galbraith MB BChir PhD Vice-President Oncology Discovery Medicine & Clinical Biomarkers Bristol-Myers
Molecular Imaging in Early Phase Oncology Trials Lessons Learned Potential Role for SNM Network Susan Galbraith MB BChir PhD Vice-President Oncology Discovery Medicine & Clinical Biomarkers Bristol-Myers
Multi-slice Helical CT Scanning of the Chest
 Multi-slice Helical CT Scanning of the Chest Comparison of different low-dose acquisitions Lung cancer is the main cause of deaths due to cancer in human males and the incidence is constantly increasing.
Multi-slice Helical CT Scanning of the Chest Comparison of different low-dose acquisitions Lung cancer is the main cause of deaths due to cancer in human males and the incidence is constantly increasing.
How to measure effect of treatment? chest radiography CT scan MRI scan PET scan ultrasound physical examination bone scintygraphy
 respons meting Bonne Biesma Franz Schramel Terschelling 2012 How to measure effect of treatment chest radiography CT scan MRI scan PET scan ultrasound physical examination bone scintygraphy guidelines
respons meting Bonne Biesma Franz Schramel Terschelling 2012 How to measure effect of treatment chest radiography CT scan MRI scan PET scan ultrasound physical examination bone scintygraphy guidelines
PET and PET/CT in Clinical Trials
 PET and PET/CT in Clinical Trials Nathan C. Hall, M.D., Ph.D. The Ohio State University Medical Center CALGB Imaging Core Lab CALGB Imaging Committee Outline Introduction to PET Positron Emitter Physics
PET and PET/CT in Clinical Trials Nathan C. Hall, M.D., Ph.D. The Ohio State University Medical Center CALGB Imaging Core Lab CALGB Imaging Committee Outline Introduction to PET Positron Emitter Physics
Treating Thyroid Cancer using I-131 Maximum Tolerable Dose Method
 Treating Thyroid Cancer using I-131 Maximum Tolerable Dose Method Christopher Martel, M.Sc., CHP Lisa Thornhill,, NRRPT, RT(NM) Boston University Medical Center Thyroid Carcinoma New cases and deaths in
Treating Thyroid Cancer using I-131 Maximum Tolerable Dose Method Christopher Martel, M.Sc., CHP Lisa Thornhill,, NRRPT, RT(NM) Boston University Medical Center Thyroid Carcinoma New cases and deaths in
Low-dose CT Imaging. Edgar Fearnow, M.D. Section Chief, Computed Tomography, Lancaster General Hospital
 Lung Cancer Screening with Low-dose CT Imaging Edgar Fearnow, M.D. Section Chief, Computed Tomography, Lancaster General Hospital Despite recent declines in the incidence of lung cancer related to the
Lung Cancer Screening with Low-dose CT Imaging Edgar Fearnow, M.D. Section Chief, Computed Tomography, Lancaster General Hospital Despite recent declines in the incidence of lung cancer related to the
Interview with David Djang, MD On PET Scan in Oncology: Principles and Practice
 Interview with David Djang, MD On PET Scan in Oncology: Principles and Practice By Howard (Jack) West, MD May, 2009 Hello and welcome to the GRACE audio podcast on PET scanning. This one is with Dr. David
Interview with David Djang, MD On PET Scan in Oncology: Principles and Practice By Howard (Jack) West, MD May, 2009 Hello and welcome to the GRACE audio podcast on PET scanning. This one is with Dr. David
New Evaluation Criteria for Response and Toxicity in Lung Cancer Treatment
 Lung Cancer New Evaluation Criteria for Response and Toxicity in Lung Cancer Treatment JMAJ 46(12): 554 558, 2003 Masahiko SHIBUYA Chief, Division of Respiratory Medicine, Tokyo Metropolitan Komagome Hospital
Lung Cancer New Evaluation Criteria for Response and Toxicity in Lung Cancer Treatment JMAJ 46(12): 554 558, 2003 Masahiko SHIBUYA Chief, Division of Respiratory Medicine, Tokyo Metropolitan Komagome Hospital
In Practice Whole Body MR for Visualizing Metastatic Prostate Cancer
 In Practice Whole Body MR for Visualizing Metastatic Prostate Cancer Prostate cancer is the second most common cancer in men worldwide, accounting for 15% of all new cancer cases. 1 Great strides have
In Practice Whole Body MR for Visualizing Metastatic Prostate Cancer Prostate cancer is the second most common cancer in men worldwide, accounting for 15% of all new cancer cases. 1 Great strides have
Variations in PET/CT Methodology for Oncologic Imaging at U.S. Academic Medical Centers: An Imaging Response Assessment Team Survey
 Variations in PET/CT Methodology for Oncologic Imaging at U.S. Academic Medical Centers: An Imaging Response Assessment Team Survey Michael M. Graham 1, Ramsey D. Badawi 2, and Richard L. Wahl 3 1 University
Variations in PET/CT Methodology for Oncologic Imaging at U.S. Academic Medical Centers: An Imaging Response Assessment Team Survey Michael M. Graham 1, Ramsey D. Badawi 2, and Richard L. Wahl 3 1 University
CA 125 definitions agreed by GCIG November 2005
 CA 125 definitions agreed by GCIG November 2005 The GCIG has agreed criteria for defining response and progression of ovarian carcinoma which use the serum marker CA 125, and the situations where these
CA 125 definitions agreed by GCIG November 2005 The GCIG has agreed criteria for defining response and progression of ovarian carcinoma which use the serum marker CA 125, and the situations where these
Recent advances in PET Monte Carlo simulations and PET image quantification towards enhancement of the role of PET in cancer patients
 Recent advances in PET Monte Carlo simulations and PET image quantification towards enhancement of the role of PET in cancer patients Irène Buvat IMNC UMR 8165 CNRS Paris 11 University Orsay, France buvat@imnc.in2p3.fr
Recent advances in PET Monte Carlo simulations and PET image quantification towards enhancement of the role of PET in cancer patients Irène Buvat IMNC UMR 8165 CNRS Paris 11 University Orsay, France buvat@imnc.in2p3.fr
PET/CT in Breast Cancer
 PET/CT in Breast Cancer Rodolfo Núñez Miller, M.D. Nuclear Medicine and Diagnostic Imaging Section Division of Human Health International Atomic Energy Agency Vienna, Austria Overview Introduction Locorregional
PET/CT in Breast Cancer Rodolfo Núñez Miller, M.D. Nuclear Medicine and Diagnostic Imaging Section Division of Human Health International Atomic Energy Agency Vienna, Austria Overview Introduction Locorregional
New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1)
") E U R O P E A N J O U R NA L O F CA N C E R45 (2009) 228 247 available at www.sciencedirect.com journal homepage: www.ejconline.com New response evaluation criteria in solid tumours: Revised RECIST guideline
E U R O P E A N J O U R NA L O F CA N C E R45 (2009) 228 247 available at www.sciencedirect.com journal homepage: www.ejconline.com New response evaluation criteria in solid tumours: Revised RECIST guideline
Salute to Dr. Saul Hertz Diagnostic and Therapeutic Uses of Radioiodine
 Salute to Dr. Saul Hertz Diagnostic and Therapeutic Uses of Radioiodine Salute to Dr. Saul Hertz Diagnostic and Therapeutic Uses of Radioiodine Douglas Van Nostrand, MD, FACP, FACNM Director, Nuclear Medicine
Salute to Dr. Saul Hertz Diagnostic and Therapeutic Uses of Radioiodine Salute to Dr. Saul Hertz Diagnostic and Therapeutic Uses of Radioiodine Douglas Van Nostrand, MD, FACP, FACNM Director, Nuclear Medicine
Come valutare la risposta o la progressione nei pazienti in trattamento con terapie biologiche
 Come valutare la risposta o la progressione nei pazienti in trattamento con terapie biologiche Andrea Busolo U.O. di Radiologia Rocco De Vivo U.O. di Oncologia Medica ULSS 6 - Vicenza Activity and efficacy
Come valutare la risposta o la progressione nei pazienti in trattamento con terapie biologiche Andrea Busolo U.O. di Radiologia Rocco De Vivo U.O. di Oncologia Medica ULSS 6 - Vicenza Activity and efficacy
Sodium Fluoride PET/CT Bone Imaging: Theory and Practice
 Sodium Fluoride PET/CT Bone Imaging: Theory and Practice George Segall, M.D. Stanford University Why F-18 Fluoride? Faster Higher Resolution Anatomic Correlation Chemiadsorption Hydroxyapatite Ca10(PO4)6(OH)2
Sodium Fluoride PET/CT Bone Imaging: Theory and Practice George Segall, M.D. Stanford University Why F-18 Fluoride? Faster Higher Resolution Anatomic Correlation Chemiadsorption Hydroxyapatite Ca10(PO4)6(OH)2
University of Texas Medical School at Houston. April 14, 2015
 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control Center WO66-G609 Silver Spring, MD 20993-0002 University of Texas Medical
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control Center WO66-G609 Silver Spring, MD 20993-0002 University of Texas Medical
LUNG CANCER SCREENING: UNDERSTANDING LUNG NODULES. 1-800-298-2436 LungCancerAlliance.org
 LUNG CANCER SCREENING: UNDERSTANDING LUNG NODULES 1-800-298-2436 LungCancerAlliance.org 1 1 CONTENTS What is a Nodule?...3 Finding Nodules...4 If a Nodule Is Found...5 What Happens Next?...7 Questions
LUNG CANCER SCREENING: UNDERSTANDING LUNG NODULES 1-800-298-2436 LungCancerAlliance.org 1 1 CONTENTS What is a Nodule?...3 Finding Nodules...4 If a Nodule Is Found...5 What Happens Next?...7 Questions
R/F. Efforts to Reduce Exposure Dose in Chest Tomosynthesis Targeting Lung Cancer Screening. 3. Utility of Chest Tomosynthesis. 1.
 R/F Efforts to Reduce Exposure Dose in Chest Tomosynthesis Targeting Lung Cancer Screening Department of Radiology, National Cancer Center Hospital East Kaoru Shimizu Ms. Kaoru Shimizu 1. Introduction
R/F Efforts to Reduce Exposure Dose in Chest Tomosynthesis Targeting Lung Cancer Screening Department of Radiology, National Cancer Center Hospital East Kaoru Shimizu Ms. Kaoru Shimizu 1. Introduction
Disease/Illness GUIDE TO ASBESTOS LUNG CANCER. What Is Asbestos Lung Cancer? www.simpsonmillar.co.uk Telephone 0844 858 3200
 GUIDE TO ASBESTOS LUNG CANCER What Is Asbestos Lung Cancer? Like tobacco smoking, exposure to asbestos can result in the development of lung cancer. Similarly, the risk of developing asbestos induced lung
GUIDE TO ASBESTOS LUNG CANCER What Is Asbestos Lung Cancer? Like tobacco smoking, exposure to asbestos can result in the development of lung cancer. Similarly, the risk of developing asbestos induced lung
There are 2 types of clinical trials that are of interest to the. The Clinical Trials Network of the Society of Nuclear Medicine
 The Clinical Trials Network of the Society of Nuclear Medicine Michael M. Graham, PhD, MD The Clinical Trials Network of the Society of Nuclear Medicine was formed to provide quality assurance of both
The Clinical Trials Network of the Society of Nuclear Medicine Michael M. Graham, PhD, MD The Clinical Trials Network of the Society of Nuclear Medicine was formed to provide quality assurance of both
KIDNEY FUNCTION RELATION TO SIZE OF THE TUMOR IN RENAL CELL CANCINOMA
 KIDNEY FUNCTION RELATION TO SIZE OF THE TUMOR IN RENAL CELL CANCINOMA O.E. Stakhvoskyi, E.O. Stakhovsky, Y.V. Vitruk, O.A. Voylenko, P.S. Vukalovich, V.A. Kotov, O.M. Gavriluk National Canсer Institute,
KIDNEY FUNCTION RELATION TO SIZE OF THE TUMOR IN RENAL CELL CANCINOMA O.E. Stakhvoskyi, E.O. Stakhovsky, Y.V. Vitruk, O.A. Voylenko, P.S. Vukalovich, V.A. Kotov, O.M. Gavriluk National Canсer Institute,
Patterns of nodal spread in thoracic malignancies
 Patterns of nodal spread in thoracic malignancies Poster No.: C-0977 Congress: ECR 2010 Type: Educational Exhibit Topic: Chest Authors: R. dos Santos, M. Duarte, J. Alpendre, J. Castaño, Z. Seabra, Â.
Patterns of nodal spread in thoracic malignancies Poster No.: C-0977 Congress: ECR 2010 Type: Educational Exhibit Topic: Chest Authors: R. dos Santos, M. Duarte, J. Alpendre, J. Castaño, Z. Seabra, Â.
BEYOND 18 F-FDG: INTRODUCTION TO NEW RADIOPHARMACEUTICALS
 BEYOND F-FDG: INTRODUCTION TO NEW RADIOPHARMACEUTICALS Asti Mattia Nuclear Medicine Department Santa Maria Nuova Hospital, Reggio Emilia, Italy SUMMARY: F-Labelled Choline analogues. Comparison between
BEYOND F-FDG: INTRODUCTION TO NEW RADIOPHARMACEUTICALS Asti Mattia Nuclear Medicine Department Santa Maria Nuova Hospital, Reggio Emilia, Italy SUMMARY: F-Labelled Choline analogues. Comparison between
Improvements in quality and quantification of 3D PET images
 Improvements in quality and quantification of 3D PET images The resolution of PET depends on some effects impossible to be readily corrected The implementation of 3D spatially-variant PSF (radially asymmetric)
Improvements in quality and quantification of 3D PET images The resolution of PET depends on some effects impossible to be readily corrected The implementation of 3D spatially-variant PSF (radially asymmetric)
Society of Nuclear Medicine 1850 Samuel Morse Drive Reston, VA 20190-5316 www.snm.org
 What is nuclear medicine? Nuclear medicine is a medical specialty that is used to diagnose and treat diseases in a safe and painless way. Nuclear medicine procedures permit the determination of medical
What is nuclear medicine? Nuclear medicine is a medical specialty that is used to diagnose and treat diseases in a safe and painless way. Nuclear medicine procedures permit the determination of medical
Imaging Informatics Ann Scherzinger, PhD, CIIP C-TRIC Lecture Series, May 18, 2011
 Imaging Informatics Ann Scherzinger, PhD, CIIP C-TRIC Lecture Series, May 18, 2011 Science of Information and Information Processing! Breadth, depth of current activities in human medical imaging informatics!
Imaging Informatics Ann Scherzinger, PhD, CIIP C-TRIC Lecture Series, May 18, 2011 Science of Information and Information Processing! Breadth, depth of current activities in human medical imaging informatics!
Spatial mismatch in CT-defined vs. NaF PET-defined lesions: implications for diagnostic bone biopsies
 Spatial mismatch in CT-defined vs. NaF PET-defined lesions: implications for diagnostic bone biopsies Stephanie Harmon, Song Chen, Peter Ferjancic, Timothy Perk, Michael Tuite, and Robert Jeraj University
Spatial mismatch in CT-defined vs. NaF PET-defined lesions: implications for diagnostic bone biopsies Stephanie Harmon, Song Chen, Peter Ferjancic, Timothy Perk, Michael Tuite, and Robert Jeraj University
HOVON Staging and Response Criteria for Non-Hodgkin s Lymphomas Page 1
 HOVON Staging and Response Criteria for Non-Hodgkin s Lymphomas Page 1 This document describes the minimally required staging and evaluation procedures and response criteria that will be applied in all
HOVON Staging and Response Criteria for Non-Hodgkin s Lymphomas Page 1 This document describes the minimally required staging and evaluation procedures and response criteria that will be applied in all
Positron Emission Tomography - For Patients
 Positron Emission Tomography - For Patients A physician s written order is required for any PET-CT tests. How should I prepare for my PET-CT? PET-CT is more complicated than most other tests you may be
Positron Emission Tomography - For Patients A physician s written order is required for any PET-CT tests. How should I prepare for my PET-CT? PET-CT is more complicated than most other tests you may be
Integrating Chemotherapy and Liver Surgery for the Management of Colorectal Metastases
 I Congresso de Oncologia D Or July 5-6, 2013 Integrating Chemotherapy and Liver Surgery for the Management of Colorectal Metastases Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University
I Congresso de Oncologia D Or July 5-6, 2013 Integrating Chemotherapy and Liver Surgery for the Management of Colorectal Metastases Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University
Objectives. Mylene T. Truong, MD. Malignant Pleural Mesothelioma Background
 Imaging of Pleural Tumors Mylene T. Truong, MD Imaging of Pleural Tumours Mylene T. Truong, M. D. University of Texas M.D. Anderson Cancer Center, Houston, TX Objectives To review tumors involving the
Imaging of Pleural Tumors Mylene T. Truong, MD Imaging of Pleural Tumours Mylene T. Truong, M. D. University of Texas M.D. Anderson Cancer Center, Houston, TX Objectives To review tumors involving the
A Three-Dimensional Correlation Method for Registration of Medical Images in Radiology
 A Three-Dimensional Correlation Method for Registration of Medical Images in Radiology Michalakis F. Georgiou 1, Joachim H. Nagel 2, George N. Sfakianakis 3 1,3 Department of Radiology, University of Miami
A Three-Dimensional Correlation Method for Registration of Medical Images in Radiology Michalakis F. Georgiou 1, Joachim H. Nagel 2, George N. Sfakianakis 3 1,3 Department of Radiology, University of Miami
PET Imaging of Hypoxia
 PET Imaging of Hypoxia John Humm, PhD Dept. of Medical Physics MSKCC AAPM Session: Introduction to Cancer Biology Tuesday 20 th July Many strong hypoxia radiotracer imaging programs University of Washington
PET Imaging of Hypoxia John Humm, PhD Dept. of Medical Physics MSKCC AAPM Session: Introduction to Cancer Biology Tuesday 20 th July Many strong hypoxia radiotracer imaging programs University of Washington
Disclosures for Elena Zamagni
 Prognostic relevance of 18F-FDG PET/CT in newly diagnosed multiple myeloma patients receiving upfront autologous stem-cell transplantation: a prospective study Zamagni E. 1, Nanni C. 2, Patriarca F. 3,
Prognostic relevance of 18F-FDG PET/CT in newly diagnosed multiple myeloma patients receiving upfront autologous stem-cell transplantation: a prospective study Zamagni E. 1, Nanni C. 2, Patriarca F. 3,
QAV-PET: A Free Software for Quantitative Analysis and Visualization of PET Images
 QAV-PET: A Free Software for Quantitative Analysis and Visualization of PET Images Brent Foster, Ulas Bagci, and Daniel J. Mollura 1 Getting Started 1.1 What is QAV-PET used for? Quantitative Analysis
QAV-PET: A Free Software for Quantitative Analysis and Visualization of PET Images Brent Foster, Ulas Bagci, and Daniel J. Mollura 1 Getting Started 1.1 What is QAV-PET used for? Quantitative Analysis
UNDERSTANDING SERIES LUNG NODULES. 1-800-298-2436 LungCancerAlliance.org
 UNDERSTANDING SERIES LUNG NODULES 1-800-298-2436 LungCancerAlliance.org CONTENTS What is a Nodule?...2 Finding Nodules...3 If a Nodule is Found... 4 What Happens Next?...6 Questions to Ask about Your Results...7
UNDERSTANDING SERIES LUNG NODULES 1-800-298-2436 LungCancerAlliance.org CONTENTS What is a Nodule?...2 Finding Nodules...3 If a Nodule is Found... 4 What Happens Next?...6 Questions to Ask about Your Results...7
MDCT Technology. Kalpana M. Kanal, Ph.D., DABR Assistant Professor Department of Radiology University of Washington Seattle, Washington
 MDCT Technology Kalpana M. Kanal, Ph.D., DABR Assistant Professor Department of Radiology University of Washington Seattle, Washington ACMP Annual Meeting 2008 - Seattle, WA Educational Objectives Historical
MDCT Technology Kalpana M. Kanal, Ph.D., DABR Assistant Professor Department of Radiology University of Washington Seattle, Washington ACMP Annual Meeting 2008 - Seattle, WA Educational Objectives Historical
SITE IMAGING MANUAL ACRIN 6698
 SITE IMAGING MANUAL ACRIN 6698 Diffusion Weighted MR Imaging Biomarkers for Assessment of Breast Cancer Response to Neoadjuvant Treatment: A sub-study of the I-SPY 2 TRIAL Version: 1.0 Date: May 28, 2012
SITE IMAGING MANUAL ACRIN 6698 Diffusion Weighted MR Imaging Biomarkers for Assessment of Breast Cancer Response to Neoadjuvant Treatment: A sub-study of the I-SPY 2 TRIAL Version: 1.0 Date: May 28, 2012
kv-& MV-CBCT Imaging for Daily Localization: Commissioning, QA, Clinical Use, & Limitations
 kv-& MV-CBCT Imaging for Daily Localization: Commissioning, QA, Clinical Use, & Limitations Moyed Miften, PhD Dept of Radiation Oncology University of Colorado Denver Questions Disease Stage (local, regional,
kv-& MV-CBCT Imaging for Daily Localization: Commissioning, QA, Clinical Use, & Limitations Moyed Miften, PhD Dept of Radiation Oncology University of Colorado Denver Questions Disease Stage (local, regional,
CPT CODE PROCEDURE DESCRIPTION. CT Scans 70450 CT HEAD/BRAIN W/O CONTRAST 70460 CT HEAD/BRAIN W/ CONTRAST 70470 CT HEAD/BRAIN W/O & W/ CONTRAST
 CPT CODE PROCEDURE DESCRIPTION CT Scans 70450 CT HEAD/BRAIN W/O CONTRAST 70460 CT HEAD/BRAIN W/ CONTRAST 70470 CT HEAD/BRAIN W/O & W/ CONTRAST 70480 CT ORBIT W/O CONTRAST 70481 CT ORBIT W/ CONTRAST 70482
CPT CODE PROCEDURE DESCRIPTION CT Scans 70450 CT HEAD/BRAIN W/O CONTRAST 70460 CT HEAD/BRAIN W/ CONTRAST 70470 CT HEAD/BRAIN W/O & W/ CONTRAST 70480 CT ORBIT W/O CONTRAST 70481 CT ORBIT W/ CONTRAST 70482
2/28/2011. MIPPA overview and CMS requirements. CT accreditation. Today s agenda. About MIPPA. Computed Tomography
 Today s agenda Computed Tomography Presented by: Dina Hernandez, BSRT, RT (R), CT, QM Krista Bush, RT, MBA Leonard Lucey, JD ACR Quality & Safety MIPPA overview and CMS requirements CT accreditation How
Today s agenda Computed Tomography Presented by: Dina Hernandez, BSRT, RT (R), CT, QM Krista Bush, RT, MBA Leonard Lucey, JD ACR Quality & Safety MIPPA overview and CMS requirements CT accreditation How
GE Healthcare. pet/ct for simulation. Precision in motion.
 GE Healthcare pet/ct for simulation. Precision in motion. Patient profile H: 5 10 W: 370 lbs BMI: 53 Each cancer patient is just as unique as his or her cancer. Approaches to cancer treatment are changing
GE Healthcare pet/ct for simulation. Precision in motion. Patient profile H: 5 10 W: 370 lbs BMI: 53 Each cancer patient is just as unique as his or her cancer. Approaches to cancer treatment are changing
In the last 2 years, PET imaging in oncology has been. PET/CT Imaging Artifacts* 156 JOURNAL OF NUCLEAR MEDICINE TECHNOLOGY
 PET/CT Imaging Artifacts* Waheeda Sureshbabu, CNMT, PET 1 ; and Osama Mawlawi, PhD 2 1 Nuclear Medicine, M.D. Anderson Cancer Center, Houston, Texas; and 2 Imaging Physics, M. D. Anderson Cancer Center,
PET/CT Imaging Artifacts* Waheeda Sureshbabu, CNMT, PET 1 ; and Osama Mawlawi, PhD 2 1 Nuclear Medicine, M.D. Anderson Cancer Center, Houston, Texas; and 2 Imaging Physics, M. D. Anderson Cancer Center,
UNDERSTANDING MULTIPLE MYELOMA AND LABORATORY VALUES Benjamin Parsons, DO bmparson@gundersenhealth.org Gundersen Health System Center for Cancer and
 UNDERSTANDING MULTIPLE MYELOMA AND LABORATORY VALUES Benjamin Parsons, DO bmparson@gundersenhealth.org Gundersen Health System Center for Cancer and Blood Disorders La Crosse, WI UNDERSTANDING MULTIPLE
UNDERSTANDING MULTIPLE MYELOMA AND LABORATORY VALUES Benjamin Parsons, DO bmparson@gundersenhealth.org Gundersen Health System Center for Cancer and Blood Disorders La Crosse, WI UNDERSTANDING MULTIPLE
CT for the production floor: Recent developments in Hard- and Software for industrial CT Systems
 CT for the production floor: Recent developments in Hard- and Software for industrial CT Systems GE s Industrial X-ray and CT Forum, Cologne July 7 th 2015 Oliver Brunke GE Sensing & Inspection Technologies
CT for the production floor: Recent developments in Hard- and Software for industrial CT Systems GE s Industrial X-ray and CT Forum, Cologne July 7 th 2015 Oliver Brunke GE Sensing & Inspection Technologies
Chemotherapy for patients with malignant pleural mesothelioma
 Early Prediction of Response to Chemotherapy and Survival in Malignant Pleural Mesothelioma Using a Novel Semiautomated 3-Dimensional Volume-Based Analysis of Serial 18 F-FDG PET Scans Roslyn J. Francis
Early Prediction of Response to Chemotherapy and Survival in Malignant Pleural Mesothelioma Using a Novel Semiautomated 3-Dimensional Volume-Based Analysis of Serial 18 F-FDG PET Scans Roslyn J. Francis
At present, combined modality treatment (chemotherapy
 Methods to Monitor Response to Chemotherapy in Non Small Cell Lung Cancer with 18 F-FDG PET Corneline J. Hoekstra, MD 1,2 ; Otto S. Hoekstra, MD, PhD 1,3 ; Sigrid G. Stroobants, MD 4 ; Johan Vansteenkiste,
Methods to Monitor Response to Chemotherapy in Non Small Cell Lung Cancer with 18 F-FDG PET Corneline J. Hoekstra, MD 1,2 ; Otto S. Hoekstra, MD, PhD 1,3 ; Sigrid G. Stroobants, MD 4 ; Johan Vansteenkiste,
RADIOLOGY SERVICES. By Dr Lim Eng Kok 1
 INTRODUCTION RADIOLOGY SERVICES By Dr Lim Eng Kok 1 Radiology is the branch of medicine that deals with the use of ionising (e.g. x- rays and radio-isotopes) and non-ionising radiation (e.g. ultrasound
INTRODUCTION RADIOLOGY SERVICES By Dr Lim Eng Kok 1 Radiology is the branch of medicine that deals with the use of ionising (e.g. x- rays and radio-isotopes) and non-ionising radiation (e.g. ultrasound
Recommendations for cross-sectional imaging in cancer management, Second edition
 www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Breast cancer Faculty of Clinical Radiology www.rcr.ac.uk Contents Breast cancer 2 Clinical background 2 Who
www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Breast cancer Faculty of Clinical Radiology www.rcr.ac.uk Contents Breast cancer 2 Clinical background 2 Who
AN INVESTIGATION INTO THE USEFULNESS OF THE ISOCS MATHEMATICAL EFFICIENCY CALIBRATION FOR LARGE RECTANGULAR 3 x5 x16 NAI DETECTORS
 AN INVESTIGATION INTO THE USEFULNESS OF THE ISOCS MATHEMATICAL EFFICIENCY CALIBRATION FOR LARGE RECTANGULAR 3 x5 x16 NAI DETECTORS Frazier L. Bronson CHP Canberra Industries, Inc. 800 Research Parkway,
AN INVESTIGATION INTO THE USEFULNESS OF THE ISOCS MATHEMATICAL EFFICIENCY CALIBRATION FOR LARGE RECTANGULAR 3 x5 x16 NAI DETECTORS Frazier L. Bronson CHP Canberra Industries, Inc. 800 Research Parkway,
Post-PET Restaging Cancer Form National Oncologic PET Registry
 Post-PET Restaging Cancer Form National Oncologic PET Registry Facility ID #: Registry Case Number: Patient Name: Your patient had a PET scan on: mm/dd/yyyy. The PET scan was done for restaging of (cancer
Post-PET Restaging Cancer Form National Oncologic PET Registry Facility ID #: Registry Case Number: Patient Name: Your patient had a PET scan on: mm/dd/yyyy. The PET scan was done for restaging of (cancer
The Medical Imaging Detective
 Solving Medical Mysteries with Imaging Richard S. Breiman, M.D. Professor of Radiology and Biomedical Imaging (Medical Imaging Detective) UCSF The Medical Imaging Detective Peering into the Patient to
Solving Medical Mysteries with Imaging Richard S. Breiman, M.D. Professor of Radiology and Biomedical Imaging (Medical Imaging Detective) UCSF The Medical Imaging Detective Peering into the Patient to
Crosswalk for Positron Emission Tomography (PET) Imaging Codes G0230 G0030, G0032, G0034, G0036, G0038, G0040, G0042, G0044, G0046
 Imaging Codes G0230 G0030, G0032, G0034, G0036, G0038, G0040, G0042, G0044, G0046") Positron Emission Tomography (PET) CPT to HCPCS Level Crosswalk Changes below from CMS Change Request 3741 Transmittals 518 & 31 published on April 1, 2005; mplementation of CPT codes are effective January
Positron Emission Tomography (PET) CPT to HCPCS Level Crosswalk Changes below from CMS Change Request 3741 Transmittals 518 & 31 published on April 1, 2005; mplementation of CPT codes are effective January
SBRT (Elekta), 45 Gy in fractions of 3 Gy 3x/week for 5 weeks (N=22) vs.
, 45 Gy in fractions of 3 Gy 3x/week for 5 weeks (N=22) vs.") Uitgangsvraag 6: Wat is de plaats van stereotactische radiotherapiebehandeling (SBRT) bij HCC patiënten? Primaire studies I Study ID II Method III Patient characteristics IV Intervention(s) V Results primary
Uitgangsvraag 6: Wat is de plaats van stereotactische radiotherapiebehandeling (SBRT) bij HCC patiënten? Primaire studies I Study ID II Method III Patient characteristics IV Intervention(s) V Results primary
ARTICLE IN PRESS. European Journal of Radiology xxx (2009) xxx xxx. Contents lists available at ScienceDirect. European Journal of Radiology
 xxx xxx. Contents lists available at ScienceDirect. European Journal of Radiology") European Journal of Radiology xxx (2009) xxx xxx Contents lists available at ScienceDirect European Journal of Radiology journal homepage: www.elsevier.com/locate/ejrad Three-dimensional evaluation of
European Journal of Radiology xxx (2009) xxx xxx Contents lists available at ScienceDirect European Journal of Radiology journal homepage: www.elsevier.com/locate/ejrad Three-dimensional evaluation of
This handout is for informational purposes only. Talk with your doctor or health care team if you have any questions about your care.
 PATIENT EDUCATION patienteducation.osumc.edu PET stands for Positron Emission Tomography. The scan looks at metabolic activity (cell activity) inside the body. Your doctor uses this information to help
PATIENT EDUCATION patienteducation.osumc.edu PET stands for Positron Emission Tomography. The scan looks at metabolic activity (cell activity) inside the body. Your doctor uses this information to help
An Update on Lung Cancer Diagnosis
 An Update on Lung Cancer Diagnosis Dr Michael Fanning MBBS FRACGP FRACP RESPIRATORY AND SLEEP PHYSICIAN Mater Medical Centre Outline Risk factors for lung cancer Screening for lung cancer Radiologic follow-up
An Update on Lung Cancer Diagnosis Dr Michael Fanning MBBS FRACGP FRACP RESPIRATORY AND SLEEP PHYSICIAN Mater Medical Centre Outline Risk factors for lung cancer Screening for lung cancer Radiologic follow-up
Elements of PET/CT Reporting
 Elements of PET/CT Reporting 1. Clinical History a. Indication i. tumor type ii. abnormality to be evaluated iii. specific clinical question b. Relevent history i. biopsy results ii. chemotherapy iii.
Elements of PET/CT Reporting 1. Clinical History a. Indication i. tumor type ii. abnormality to be evaluated iii. specific clinical question b. Relevent history i. biopsy results ii. chemotherapy iii.
SPECT and PET imaging in porcine inflammation and infection models. UCPH pig model network seminar
 SPECT and PET imaging in porcine inflammation and infection models UCPH pig model network seminar Friday November 21. 2014, 8.30 12.00, auditorium A2 70.02, Thorvaldsensvej 40, 1871 Frederiksberg C. See
SPECT and PET imaging in porcine inflammation and infection models UCPH pig model network seminar Friday November 21. 2014, 8.30 12.00, auditorium A2 70.02, Thorvaldsensvej 40, 1871 Frederiksberg C. See
Exploratory data analysis (Chapter 2) Fall 2011
 Fall 2011") Exploratory data analysis (Chapter 2) Fall 2011 Data Examples Example 1: Survey Data 1 Data collected from a Stat 371 class in Fall 2005 2 They answered questions about their: gender, major, year in school,
Exploratory data analysis (Chapter 2) Fall 2011 Data Examples Example 1: Survey Data 1 Data collected from a Stat 371 class in Fall 2005 2 They answered questions about their: gender, major, year in school,
Truly digital PET imaging
 Truly digital PET imaging Philips proprietary Digital Photon Counting technology Vereos PET/CT is the first commercially available scanner to offer truly digital PET, resulting in significantly improved
Truly digital PET imaging Philips proprietary Digital Photon Counting technology Vereos PET/CT is the first commercially available scanner to offer truly digital PET, resulting in significantly improved
What If I Have a Spot on My Lung? Do I Have Cancer? Patient Education Guide
 What If I Have a Spot on My Lung? Do I Have Cancer? Patient Education Guide A M E R I C A N C O L L E G E O F C H E S T P H Y S I C I A N S Lung cancer is one of the most common cancers. About 170,000
What If I Have a Spot on My Lung? Do I Have Cancer? Patient Education Guide A M E R I C A N C O L L E G E O F C H E S T P H Y S I C I A N S Lung cancer is one of the most common cancers. About 170,000
4D Scanning. Image Guided Radiation Therapy. Outline. A Simplified View of the RT Process. Outline. Steve B. Jiang, Ph.D.
 4D Scanning Steve B. Jiang, Ph.D. Department of Radiation Oncology jiang.steve@mgh.harvard.edu http://gray.mgh.harvard.edu/ Outline Problems with free breathing 3D scanning What is 4D CT? How does it work?
4D Scanning Steve B. Jiang, Ph.D. Department of Radiation Oncology jiang.steve@mgh.harvard.edu http://gray.mgh.harvard.edu/ Outline Problems with free breathing 3D scanning What is 4D CT? How does it work?
Diagnosis and Prognosis of Pancreatic Cancer
 Main Page Risk Factors Reducing Your Risk Screening Symptoms Diagnosis Treatment Overview Chemotherapy Radiation Therapy Surgical Procedures Lifestyle Changes Managing Side Effects Talking to Your Doctor
Main Page Risk Factors Reducing Your Risk Screening Symptoms Diagnosis Treatment Overview Chemotherapy Radiation Therapy Surgical Procedures Lifestyle Changes Managing Side Effects Talking to Your Doctor
NEW HYBRID IMAGING TECHNOLOGY MAY HAVE BIG POTENTIAL FOR IMPROVING DIAGNOSIS OF PROSTATE CANCER
 Media Release April 7, 2009 For Immediate Release NEW HYBRID IMAGING TECHNOLOGY MAY HAVE BIG POTENTIAL FOR IMPROVING DIAGNOSIS OF PROSTATE CANCER London, Ontario Improved hybrid imaging techniques developed
Media Release April 7, 2009 For Immediate Release NEW HYBRID IMAGING TECHNOLOGY MAY HAVE BIG POTENTIAL FOR IMPROVING DIAGNOSIS OF PROSTATE CANCER London, Ontario Improved hybrid imaging techniques developed
Pfizer Forms Global Alliance with Merck KGaA, Darmstadt, Germany to Accelerate Presence in Immuno-Oncology. November 17, 2014
 Pfizer Forms Global Alliance with Merck KGaA, Darmstadt, Germany to Accelerate Presence in Immuno-Oncology November 17, 2014 Forward-looking statements Our discussions during this conference call will
Pfizer Forms Global Alliance with Merck KGaA, Darmstadt, Germany to Accelerate Presence in Immuno-Oncology November 17, 2014 Forward-looking statements Our discussions during this conference call will
Saturation Biopsy vs. 3D Spatial Biopsy vs. Free Hand Ultrasound biopsy for Targeted Prostate Cancer Therapies
 Saturation Biopsy vs. 3D Spatial Biopsy vs. Free Hand Ultrasound biopsy for Targeted Prostate Cancer Therapies John F. Ward, MD Assistant Professor University of Texas M. D. Anderson Cancer Center Ablation
Saturation Biopsy vs. 3D Spatial Biopsy vs. Free Hand Ultrasound biopsy for Targeted Prostate Cancer Therapies John F. Ward, MD Assistant Professor University of Texas M. D. Anderson Cancer Center Ablation
Continuing Medical Education Article Imaging of Multiple Myeloma and Related Plasma Cell Dyscrasias JNM, July 2012, Volume 53, Number 7
 Continuing Medical Education Article Imaging of Multiple Myeloma and Related Plasma Cell Dyscrasias JNM, July 2012, Volume 53, Number 7 Authors Ronald C. Walker 1,2, Tracy L. Brown 3, Laurie B. Jones-Jackson
Continuing Medical Education Article Imaging of Multiple Myeloma and Related Plasma Cell Dyscrasias JNM, July 2012, Volume 53, Number 7 Authors Ronald C. Walker 1,2, Tracy L. Brown 3, Laurie B. Jones-Jackson
UMHS-PUHSC JOINT INSTITUTE
 Imaging Biomarkers for Staging and Assessing Response to Therapy in Multiple Myeloma Qian Dong, MD. Radiology University of Michigan Wei Guo, MD. Orthopedic Oncology Peking University Second Hospital Team
Imaging Biomarkers for Staging and Assessing Response to Therapy in Multiple Myeloma Qian Dong, MD. Radiology University of Michigan Wei Guo, MD. Orthopedic Oncology Peking University Second Hospital Team
Lymphoma and Chronic Lymphocytic Leukemia Clinical Trials
 Recommendations for Implementing Assessment Criteria Guidelines in Lymphoma and Chronic Lymphocytic Leukemia Clinical Trials A PAREXEL Company Lymphoma Assessment Guidelines Standardized assessment criteria
Recommendations for Implementing Assessment Criteria Guidelines in Lymphoma and Chronic Lymphocytic Leukemia Clinical Trials A PAREXEL Company Lymphoma Assessment Guidelines Standardized assessment criteria
A PATIENT S GUIDE TO ABLATION THERAPY
 A PATIENT S GUIDE TO ABLATION THERAPY THE DIVISION OF VASCULAR/INTERVENTIONAL RADIOLOGY THE ROBERT WOOD JOHNSON UNIVERSITY HOSPITAL Treatment options for patients with cancer continue to expand, providing
A PATIENT S GUIDE TO ABLATION THERAPY THE DIVISION OF VASCULAR/INTERVENTIONAL RADIOLOGY THE ROBERT WOOD JOHNSON UNIVERSITY HOSPITAL Treatment options for patients with cancer continue to expand, providing
Cancer and the immune system: can we beat cancer at its own game?
 Cancer and the immune system: can we beat cancer at its own game? Andrew R. Haas, MD, PhD Assistant Professor of Medicine University of Pennsylvania Medical Center Philadelphia, Pa Why can t immune
Cancer and the immune system: can we beat cancer at its own game? Andrew R. Haas, MD, PhD Assistant Professor of Medicine University of Pennsylvania Medical Center Philadelphia, Pa Why can t immune
Clinical Trials of Lapatinib in Patients with Brain Metastases. Nancy U Lin, MD Dana Farber Cancer Institute March 1, 2009
 Clinical Trials of Lapatinib in Patients with Brain Metastases from HER2+ Breast Cancer Nancy U Lin, MD Dana Farber Cancer Institute March 1, 2009 Background ~1/3 of women with HER2+ MBC develop brain
Clinical Trials of Lapatinib in Patients with Brain Metastases from HER2+ Breast Cancer Nancy U Lin, MD Dana Farber Cancer Institute March 1, 2009 Background ~1/3 of women with HER2+ MBC develop brain
DEVELOPMENT OF AN IMAGING SYSTEM FOR THE CHARACTERIZATION OF THE THORACIC AORTA.
 DEVELOPMENT OF AN IMAGING SYSTEM FOR THE CHARACTERIZATION OF THE THORACIC AORTA. Juan Antonio Martínez Mera Centro Singular de Investigación en Tecnoloxías da Información Universidade de Santiago de Compostela
DEVELOPMENT OF AN IMAGING SYSTEM FOR THE CHARACTERIZATION OF THE THORACIC AORTA. Juan Antonio Martínez Mera Centro Singular de Investigación en Tecnoloxías da Información Universidade de Santiago de Compostela
Thomas de los Reyes PGY 1 Department of Urologic Sciences University of British Columbia. Meet Mr. S
 Thomas de los Reyes PGY 1 Department of Urologic Sciences University of British Columbia Meet Mr. S 74 M admitted for back pain X-ray: sclerotic lesions along spine PSA 800 Nuclear Medicine Bone Scan 1
Thomas de los Reyes PGY 1 Department of Urologic Sciences University of British Columbia Meet Mr. S 74 M admitted for back pain X-ray: sclerotic lesions along spine PSA 800 Nuclear Medicine Bone Scan 1
AMINO ACID ANALYSIS By High Performance Capillary Electrophoresis
 AMINO ACID ANALYSIS By High Performance Capillary Electrophoresis Analysis of Amino Acid Standards Label free analysis using the HPCE-512 ABSTRACT Capillary electrophoresis using indirect UV detection
AMINO ACID ANALYSIS By High Performance Capillary Electrophoresis Analysis of Amino Acid Standards Label free analysis using the HPCE-512 ABSTRACT Capillary electrophoresis using indirect UV detection
A new score predicting the survival of patients with spinal cord compression from myeloma
 A new score predicting the survival of patients with spinal cord compression from myeloma (1) Sarah Douglas, Department of Radiation Oncology, University of Lubeck, Germany; sarah_douglas@gmx.de (2) Steven
A new score predicting the survival of patients with spinal cord compression from myeloma (1) Sarah Douglas, Department of Radiation Oncology, University of Lubeck, Germany; sarah_douglas@gmx.de (2) Steven
LYMPHOMA IN DOGS. Diagnosis/Initial evaluation. Treatment and Prognosis
 LYMPHOMA IN DOGS Lymphoma is a relatively common cancer in dogs. It is a cancer of lymphocytes (a type of white blood cell) and lymphoid tissues. Lymphoid tissue is normally present in many places in the
LYMPHOMA IN DOGS Lymphoma is a relatively common cancer in dogs. It is a cancer of lymphocytes (a type of white blood cell) and lymphoid tissues. Lymphoid tissue is normally present in many places in the
Next Generation Small Animal PET Technology
 G4 PET/X-ray P R O D U C T N O T E Pre-clinical in vivo Imaging Key Benefits: High performance, ultra-sensitive PET technology designed for pre-clinical imaging 3D PET and X-ray whole body images Purpose
G4 PET/X-ray P R O D U C T N O T E Pre-clinical in vivo Imaging Key Benefits: High performance, ultra-sensitive PET technology designed for pre-clinical imaging 3D PET and X-ray whole body images Purpose
GE Medical Systems Training in Partnership. Module 8: IQ: Acquisition Time
 Module 8: IQ: Acquisition Time IQ : Acquisition Time Objectives...Describe types of data acquisition modes....compute acquisition times for 2D and 3D scans. 2D Acquisitions The 2D mode acquires and reconstructs
Module 8: IQ: Acquisition Time IQ : Acquisition Time Objectives...Describe types of data acquisition modes....compute acquisition times for 2D and 3D scans. 2D Acquisitions The 2D mode acquires and reconstructs
New Advances in Cancer Treatments. March 2015
 New Advances in Cancer Treatments March 2015 Safe Harbour Statement This presentation document contains certain forward-looking statements and information (collectively, forward-looking statements ) within
New Advances in Cancer Treatments March 2015 Safe Harbour Statement This presentation document contains certain forward-looking statements and information (collectively, forward-looking statements ) within
PET/CT QC/QA. Quality Control in PET. Magnus Dahlbom, Ph.D. Verify the operational integrity of the system. PET Detectors
 Quality Control in PET PET/CT QC/QA Magnus Dahlbom, Ph.D. Division of Nuclear Medicine Ahmanson Biochemical Imaging Clinic David Geffen School of Medicine at UCLA Los Angeles Verify the operational integrity
Quality Control in PET PET/CT QC/QA Magnus Dahlbom, Ph.D. Division of Nuclear Medicine Ahmanson Biochemical Imaging Clinic David Geffen School of Medicine at UCLA Los Angeles Verify the operational integrity