John Gasman, MD Alec Jamieson, RN, MSN Kim Clifforth, RN, BSN, MSN, CNS Thomas T. Lam, MD. June 18, 2013
|
|
|
- Jeremy Gilmore
- 8 years ago
- Views:
Transcription

1 John Gasman, MD Alec Jamieson, RN, MSN Kim Clifforth, RN, BSN, MSN, CNS Thomas T. Lam, MD June 18, 2013

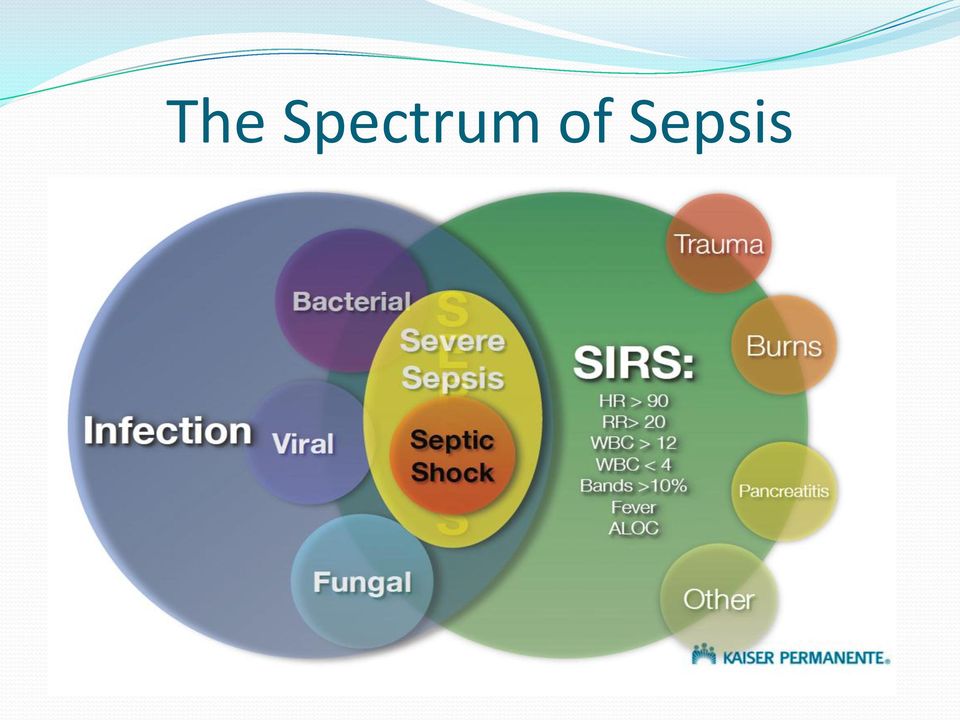
2 Objectives Acquire knowledge on defining sepsis, severe sepsis and septic shock Recognize SIRS criteria. Define sepsis as it relates to pathophysiological changes in patients Describe methods used to improve EGDT 6 Hour measures.

3 Leverage and Optimize KPHC Culture of Safety and Teamwork World Class Hospital Goal Drivers Focus Areas Do No Harm Prevent Infections Prevent Falls Prevent Pressure Ulcers Medication Safety Surgical Safety Perinatal Safety The Quality Leader Evidence Based Care Acute Myocardial Infarction Heart Failure Pneumonia Surgical Care Stroke Sepsis Perinatal Care Critical Care Delirium Management Patient Mobility Pediatrics Coordinated Care Palliative Care Life Care Planning Excellent Transitions 3

4 Sepsis A clinical syndrome Systemic inflammation due to infection A continuum: Sepsis > severe sepsis > shock 750,000 cases / year in U.S. Any age, race, gender, or ethic groups 200,000 fatalities Mortality rate is 40% or more for severe sepsis or septic shock.

5 Sepsis in Perspective - NCAL AMI Admissions AMI Mortality Sepsis Admissions Sepsis Mortality AMI mortality rate 4.7% Sepsis mortality rate 24%

6 How Big an Issue is Sepsis? 205,548 Adult Hospital Admissions 2007 KPNC Adult Hospital Stays, includes OB 24% of All Deaths 1,364 Deaths from Sepsis 2.7% of All Admissions 5,558 Sepsis Admissions 199,990 Other Admissions 4,302 Deaths from Everything Else Mortality Rate 25% A Big Issue: 1 in 4 deaths Eleven times the mortality rate Mortality Rate 2.2%

7 The Spectrum of Sepsis
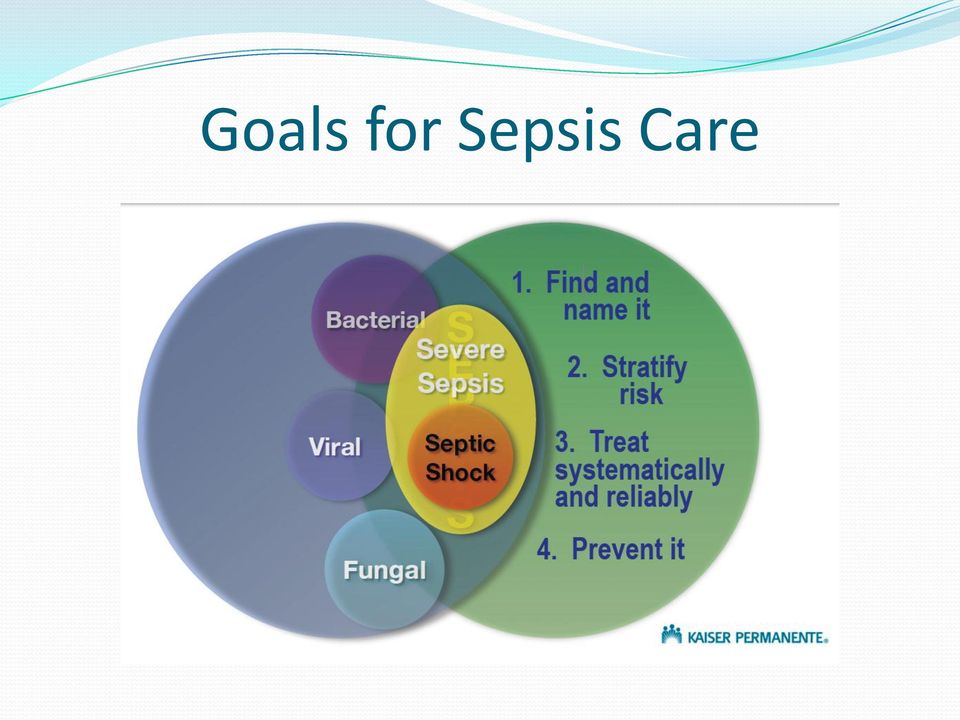
8 Goals for Sepsis Care
9 Does Early Goal Directed Therapy Work? Mortality (16% absolute reduction) Organ dysfunction Need for vasopressors (15%) Sudden cardiopulmonary complications (100%) ICU LOS and Health Care Resources (20%) From Henry Ford Hospital, E. Rivers NEJM 2001: 345;
 From Henry Ford Hospital, E.")
10 Treatment of Sepsis Supportive care Respiratory support Hemodynamic support Assure perfusion to vital organs Control the Septic Focus Obtain cultures Remove source and debride or drain Antibiotics Septic Exotica Corticosteroids

11 Prognostic Value of Elevated Lactate * Source: Gabriel Escobar, MD DOR

 426 high (>4) lactates 5 patients a day 10% mortality 32% mortality 165 deaths 136 deaths -1 in 10 dies- -1 in 3 dies- 55% of lactate-associated mortalities are in intermediate lactate group.")
12 Impact of Elevated Lactate 2079 elevated lactates KPNC Q Results based on elevated lactate in ED for patients then admitted, not specific to sepsis 18 patients a day 1653 intermediate lactates (2-4) 426 high (>4) lactates 5 patients a day 10% mortality 32% mortality 165 deaths 136 deaths -1 in 10 dies- -1 in 3 dies- 55% of lactate-associated mortalities are in intermediate lactate group. This group accounts for over 10% of all hospital mortalities. The intermediate lactate mortality was more than double that of our AMI patients. High lactate mortality was 7X the AMI mortality rate.

13 Identify at triage if suspected infection and 2 SIRS criteria T < 96.8 (36.0) or > (38.0) HR > 90 RR > 20 WBC > 12K or < 4K or > 10% bands -OR- Altered LOC CBC, Lactate, BC Consider IV fluids and ABX EGDT Goals from Time Zero 1. Start Antibiotic 1 hr 2. First CVP or ScvO2 within 2 hrs 3. CVP 8-12 within 6 hrs 4. MAP 65 within 6 hrs 5. ScvO2 70 within 6 hrs 6. Repeat lactate < initial lactate within 3-12 hrs Suspected Sepsis Document SIRS SBP 90 w/transient improvement (2 hr) Time Zero (1 hr from Initial) Hypotension Document Septic Shock SBP 90? 20 ml/kg fluid bolus in 1 st hour YES SBP 90 (1 hr) Time Zero Document Septic Shock Time Zero = Sepsis Alert NO SBP > 90 Document SEPSIS < 2.0 Lactate high? 4 Time Zero Document Severe Sepsis EGDT Aggressive fluid resuscitation Within 1 hr: Start ABX Within 2 hrs: Measure CVP or ScvO2 Last Modified: 10/13/10 Quality Management S:\Quality\Sepsis\Work Flows\SEPSIS Algorithm Document Severe Sepsis *Repeat lactate in 3-6 hours
 Time Zero (1 hr from Initial) Hypotension Document Septic Shock SBP 90?")
14 EGDT Bundle for Severe Sepsis/Shock & 2013 Goals Diagnose Severe Sepsis or Septic Shock Central Line Placed 1 st CVP or SvcO2 MAP CVP ScvO 2 at Goal Repeat Lactate is Lower than First Lactate Screen all patients at risk ABX started IV Fluid Time Zero 1 hour 2 hours 6 hours Within 12 hours 2013 Goals: 90% 70% EGDT bundle: 50%

15

16 Summary Early Diagnosis with sepsis screening tools. Risk stratification with lactate level and follow up of lactate trends Document the Sepsis diagnosis. Early resuscitation improves mortality, confirmed by RCT. Use of a Sepsis Order Set for uniformity of basic care. Collaborative team effort.

17
18 Key Components to Success Appropriate education and Training Frontline staff engagement, ownership and involvement Transparency of data: collection and review Multidisciplinary collaboration Clearly delineated roles, responsibilities and processes Standardization of practices In Other Words Build a Solid Foundation on Which to Build a Sustainable and Reliable Practice!!

19 Where we were Mortality rate 19.5% Sepsis Summit Nov 2008



20 The beginning Why was mortality in this population so high? Several key issues identified: We cause it Increased mortality We underestimate it We under treat it

21 The Beginning cont. What did we need to do to address these problems? 1. Find (Name and Document) Sepsis 2. Stratify Risk 3. Reliable Care at All Levels of Risk

22 Time Pain* BP P R T GCS* MAP* FiO2/ CVP RASS* Intervention (EMV) Note actions taken in response to the findings on SpO2 mm/hg Score Score Character SCVO2 the left. TOTALS SITE GAUGE TYPE STARTED ABSORBED Team Training Abx in 1 hr CL in 2 hrs How?: #1- The Power of Teams Develop Teams Kaiser Foundation Hospital - San Jose Tools and Equipment EMERGENCY DEPARTMENT DRAFT ED NURSES FLOW SHEET Addressograph Date Pg of ADDRESSOGRAPH Room / Bed # EARLY GOAL DIRECTED THERAPY (EGDT) ED AND ICU ORDERSET Page 1 of 4 X Check box to activate an order Diagnosis of of Severe Severe Sepsis Sepsis or or Septic Septic Shock Shock Aggressive fluid fluid resuscitation Within Within 11 hr: hr: Start Start ABX ABX Within Within2 2 hrs: hrs: Central Central Line Line Placed Placed Adopt Algorithms CVP 8-12? MAP 65? ScvO2 70? 70 Lower Lactate <8-12 < 65 <70 E A R L Y G O A L 500 to 1000 ml Fluid boluses q 30 min Norepinephrine If Hct low, transfuse to 30 <70 Dobutamine D I R E C T E D T H E R A P Y Train Measure Lactates Lactates on ED Blood Cultures Sepsis Care Sepsis Implementation 55% DENOM 47% 44% 84% 37% 69% 91% 29% 85% 32% 77% 37% 99% 80% 36% 63% 66% 58% 56% 100% 0% 0% 0% Mark chart: Allergic to No Known Allergies Weight (kg) Height Check if applies: Pregnant Lactating ED ORDERS ICU ORDERS Administer oxygen titrate FiO2 to maintain SpO2 between 90-94%. Notify physician if patient requires over 50% FiO2 via face mask or more than 10% increase in 1 hour to achieve needed goal Continue Discontinue, RN (Date/Time) OUTPUT INTAKE PARENTERAL FLUIDS Time TYPE AMOUNT Time TYPE AMOUNT Time # Insert Foley catheter, RN (Date/Time) VITAL SIGNS Measure intake and output hourly, RN (Date/Time) Continue Discontinue Continue Discontinue Initals Signature/Title Initials Signature/Title Initials Signature/Title Record vital signs (heart rate, blood pressure, respiratory rate, SpO2) per unit standards and as needed, RN (Date/Time) Continue Discontinue Measure central venous pressure (CVP) every 30 minutes until goal has been achieved and for at least 2 hours after goal has been reached, then monitor per unit standards and as needed, RN (Date/Time) Continue Discontinue Monitor mixed venous oxygen saturation (ScvO2) continuously, RN (Date/Time) Continue Discontinue Collaborate! Collaborate! 22

23 How?: #2-The Power of Standardization
24 Kaiser Fresno s Process 1. Identify stake holders and Engage the Frontline staff: ED and CCU identified as primary stake holders. 2. Have the right tools and equipment ready to use 3. Adopt Algorithms and Have a Scripted Process 4. Develop and implement education and training 5. Implement EGDT 6. Measure 7. Process Improvement Collaborate!!: Interdisciplinary AND Interdepartmental
25 1. Identify your stake holders and Engage the Frontline staff ED and CCU identified as primary stake holders Develop teams Develop departmental champions and experts: involve them in process development, education and communication Share data and stories with frontline staff and solicit feedback
26 2. Have the right tools and equipment ready to use Ensure that ALL equipment and supplies are readily available and operational these are tools to help, not obstacles to overcome. Central line kits and sterile barriers SvO2 monitoring central line Ultrasound Machines and probe covers CVP transducers, pressure bags etc. Create a Sepsis Cart where all supplies and equipment are centrally located and easily accessed
27 3. Adopt Algorithms and Have a Scripted Process Provides clear and consistent communication as to process steps and outcome measures Provides for reliable execution Standardized ordersets used for ALL EGDT cases: ordersets follow the EGDT algorithms Fluid resuscitation Antibiotics Vasopressors Blood products
28 Identify at triage if suspected infection and 2 SIRS criteria T o < 96.8 (36.0) or > (38.0) HR > 90 SUSPECTED SEPSIS RR > 20 DOCUMENT SIRS WBC > 12K or < 4K or > 10% bands -OR- Altered LOC E A R L Y R E C O G N I T I O N CBC, Lactate, BC Consider IV fluids and ABX SBP 90? yes 20 ml/kg fluid bolus in 1 st hr SBP 90 no SBP >90 Document Septic Shock (Time Zero) Document Sepsis <2 Lactate high? 4 EGDT Aggressive fluid resuscitation Within 1 hr: Start ABX Within 2 hrs: Measure CVP or ScvO Document Severe Sepsis (Time Zero) Sepsis Resuscitation The Golden Hours Aggressive IV fluid resuscitation Early ABX Repeat lactate in 3-6 hrs Document Severe Sepsis CVP MAP 65? 65 ScvO2 70? 70 Repeat lactate 3-12 hrs < 8 < 65 <70 EGDT Goals from Time Zero 1. Start Antibiotic in 1 hr 2. First CVP or ScvO2 within 2 hrs 3. CVP 8-12 within 6 hrs 4. MAP 65 within 6 hrs 5. ScvO 2 70 within 6 hrs 6. Repeat lactate is lower than initial lactate w/in 3-12 hrs E A R L Y G O A L ml Fluid boluses q 30 min Norepinephrine If Hct low, transfuse to 30 <70 Dobutamine D I R E C T E D T H E R A P Y
29 4. Develop and Implement Education and Training Regional Education: November 2008 Sepsis Summit: Introduction to formalized EGDT process for all EDs and ICUs All 21 northern California Kaiser medical centers attended Data presented Tools presented Algorithms presented Goals set
30 Develop and Implement Education and Training Regional learning brought back to Fresno and local, Facility specific training and education was developed and implemented Focused on frontline staff learning algorithms, tools and goals Development of unit based teams with departmental champions and experts spearheading the educational efforts with frontline staff Small group in the moment hands-on training Staff engagement through direct involvement of implementation efforts
31 RN Education and Training: Round Two: November 2009 All RNs completed online training course on EGDT Comprehensive training for a small group of Super Users. 2-3 per shift Trained in tandem with CCU RNs (establish common understanding of workflows and roles and responsibilities-teamwork) Superusers became departmental champions and trained staff one on one: SIRS recognition, equipment setup and calibration, managing CVP and SCVO2.
32 Implementing Our EGDT Treatment Algorithms
33 Early recognition Identify patients at risk for sepsis as early as possible How? Front line staff key to this effort Education and training as to SIRS and S/Sx Development and implementation of screening tool ALL patients screened upon presentation at triage/arrival Raised awareness Standardized process of assessment

34 Screening Tool
35 Risk Stratification: Lactates in the ED Relatively inexpensive ($ 1- $ 3) Available at the bedside in the ED Marker of tissue hypoxia Increased lactate in setting of infection is an indicator of increased mortality What do levels of > 2 or > 4 Mean?

36 What Does Elevated Lactate Mean? * Source: Gabriel Escobar, MD DOR
37 Identify at triage if suspected infection and 2 SIRS criteria T < 96.8 (36.0) or > (38.0) HR > 90 RR > 20 WBC > 12K or < 4K or > 10% bands -OR- Altered LOC CBC, Lactate, BC Consider IV fluids and ABX EGDT Goals from Time Zero 1. Start Antibiotic 1 hr 2. First CVP or ScvO2 within 2 hrs 3. CVP 8-12 within 6 hrs 4. MAP 65 within 6 hrs 5. ScvO2 70 within 6 hrs 6. Repeat lactate < initial lactate within 3-12 hrs Suspected Sepsis Document SIRS SBP 90 w/transient improvement (2 hr) Time Zero (1 hr from Initial) Hypotension Document Septic Shock SBP 90? 30 ml/kg fluid bolus in 1 st hour YES SBP 90 (1 hr) Time Zero Document Septic Shock Time Zero = Sepsis Alert NO SBP > 90 Document SEPSIS < 2.0 Lactate high? 4 Time Zero Document Severe Sepsis EGDT Aggressive fluid resuscitation Within 1 hr: Start ABX Within 2 hrs: Measure CVP or ScvO2 Last Modified: 10/13/10 Quality Management S:\Quality\Sepsis\Work Flows\SEPSIS Algorithm Document Severe Sepsis *Repeat lactate in 3-6 hours
38 Sepsis Alert! If: Lactate greater than 4 or refractory hypotension in the presence of 2 or more SIRS criteria and a suspected source of infection Call a Sepsis Alert! Overhead Alert in the ED Initiated by primary/charge RN after discussion with physician Mobilizes resources in the ED Raises awareness to all House supervisor alerted CCU alerted
 HR > 90 SUSPECTED SEPSIS RR > 20 DOCUMENT SIRS WBC > 12K or < 4K or > 10% bands -OR- Altered LOC E A R L Y R E C O G N I T I O N CBC, Lactate, BC Consider IV fluids and ABX SBP 90?")
39 Identify at triage if suspected infection and 2 SIRS criteria T o < 96.8 (36.0) or > (38.0) HR > 90 SUSPECTED SEPSIS RR > 20 DOCUMENT SIRS WBC > 12K or < 4K or > 10% bands -OR- Altered LOC E A R L Y R E C O G N I T I O N CBC, Lactate, BC Consider IV fluids and ABX SBP 90? yes 20 ml/kg fluid bolus in 1 st hr SBP 90 no SBP >90 Document Septic Shock (Time Zero) Document Sepsis <2 Lactate high? 4 EGDT Aggressive fluid resuscitation Within 1 hr: Start ABX Within 2 hrs: Measure CVP or ScvO Document Severe Sepsis (Time Zero) Sepsis Resuscitation The Golden Hours Aggressive IV fluid resuscitation Early ABX Repeat lactate in 3-6 hrs Document Severe Sepsis CVP MAP 65? 65 ScvO2 70? 70 Repeat lactate 3-12 hrs < 8 < 65 <70 EGDT Goals from Time Zero 1. Start Antibiotic in 1 hr 2. First CVP or ScvO2 within 2 hrs 3. CVP 8-12 within 6 hrs 4. MAP 65 within 6 hrs 5. ScvO 2 70 within 6 hrs 6. Repeat lactate is lower than initial lactate w/in 3-12 hrs E A R L Y G O A L ml Fluid boluses q 30 min Norepinephrine If Hct low, transfuse to 30 <70 Dobutamine D I R E C T E D T H E R A P Y
40 ED to CCU Transition: Communication, communication, communication Fresno SEPSIS PATIENT HAND-OFF: Worksheet NOTE: This worksheet is not a part of the patient s medical record. SIRS Criteria Met (2 or more of following): Temp Greater than 38 or Less than 36 Tachycardia (or greater than 90/min) Tachypnea (or greater than 20/min) WBCs less than 4000 or greater than New Onset Altered Mental Status Sepsis Patient Hand-off: Sending RN to Receiving RN Key Information Sending RN Receiving RN TIME ZERO and reason (circle reason) Initial Lactate Level Was Lactate Level Intermediate?(2-3.9) What is BUN? ( Lactate + BUN = Mortality Risk) Repeat Lactate Level (if drawn) (Time, Value) Repeat Lactate Level Due (if not yet drawn) TIME Yes / No VALUE BP or Lactate Yes/No : Time Due: Blood Cultures/ UA Sent (Time, Yes / No) / Yes / No, Yes / No Expected/Confirmed Source of Sepsis Initial HR/BP/RR Current HR/BP/RR IV Fluids Given (Time, Med, Dose) Vasospressor(s) (Time, Med, Dose) Antibiotic Given (Time, Med, Dose) Source: Fluid: Med: Med: Central Line Placed & Cleared (Times, Yes / No) / Yes / No, Yes / No Vigileo Attached; In vivo Calibration Completed Yes / No Dose Initial CVP (Value) Current CVP (Value) Initial ScvO2 (Value) &/or Mixed Venous Blood Gas Current ScvO2 (Value)
41 Data collection and transparency Quality analysts abstracted all data Presented and reviewed data with ED and CCU Transparency key to success Learnings for improvement Results presented to frontline staff on regular basis: data presented as well as tangible aspect (lives saved)
42 Sharing The Data Dec EGDT Goals From Jun Jan - 13 Feb - 13 Mar - 13 Apr -13 May-13 Jul-12 Aug-12 Sep-12 Oct-12 Nov-12 Time Zero Targets EGDT Composite has demonstrated an upward trend since November 2010 and started to drift in June & July Upward trend in August EGDT Cases Abx in 1 hour 90% 100% 100% 100% 100% 83% 100% 100% 100% 100% 100% 100% 100% 1 st CVP or ScvO2 within 2 hours of EGDT 70% 75% 50% 100% 67% 83% 100% 100% 100% 100% 75% 86% 100% Target CVP Achieved None 75% 100% 100% 86% 83% 50% 100% 100% 100% 80% 100% 100% Target MAP Achieved None 100% 100% 100% 100% 83% 100% 100% 100% 100% 80% 100% 100% Target ScvO2 Achieved None 75% 100% 100% 86% 83% 100% 100% 100% 75% 60% 86% 100% Improved Repeat Lactate for EGDT Patients None 100% 50% 100% 100% 67% 100% 100% 100% 100% 100% 100% 100% 6 Hour Bundle 50% 75% 50% 100% 71.% 67% 50% 100% 100% 75% 40% 86% 100% EGDT Composite None 87.5% 83.3% 100% 90% 81% 91.7% 100% 100% 96% 82.8% 90% Mortality 12% 14.8% 4.2% 8.2% 7.7% 8.2% 11.5% 12.9% 14.5% 6.2% 8.2% 6.5% Diagnosis Rates per 1,000 Total Admits (exclude deliveries)
43 PI process Worked closely with quality analysts: collaborative and transparent Multi-disciplinary approach Small tests of change with rapid review Solicited feedback from staff Tracked all Correlated with results
44 How To Improve From Here Act Study Plan Do Review Each Case For early feedback For learning For redesign Aggressiveness of Fluid Resuscitation Handoffs- every minute matters Timing Documentation 44
45 Where we are now! Mortality Rate 9.6%!
46 What we have learned Build strong teams and have solid education and training in place Early recognition and Diagnosis of sepsis is key to success Risk stratify by lactate & follow trends- reevaluate. Document Sepsis diagnosis. Early resuscitation goals improve mortality- the Six Hour Bundle Use standardized processes. i.e. EGDT algorithms and EGDT order set Collaborative team efforts are essential to success
47
Lynda Richardson, RN, BSN Sepsis/Septic Shock Abstractor. No disclosures
 Lynda Richardson, RN, BSN Sepsis/Septic Shock Abstractor No disclosures 1 2 3 Discuss data requirements -3 hour bundle -6 hour bundle Challenges and compliance issues Success 4 Based on the Surviving Sepsis
Lynda Richardson, RN, BSN Sepsis/Septic Shock Abstractor No disclosures 1 2 3 Discuss data requirements -3 hour bundle -6 hour bundle Challenges and compliance issues Success 4 Based on the Surviving Sepsis
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Sepsis Core Measures Bundle Requirements
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Sepsis Core Measures Bundle Requirements
SE5h, Sepsis Education.pdf. Surviving Sepsis
 Surviving Sepsis 1 Scope and Impact of the Problem: Severe sepsis is a major healthcare problem that affects millions of people around the world each year with an extremely high mortality rate of 30 to
Surviving Sepsis 1 Scope and Impact of the Problem: Severe sepsis is a major healthcare problem that affects millions of people around the world each year with an extremely high mortality rate of 30 to
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy
 The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
Decreasing Sepsis Mortality at the University of Colorado Hospital
 Decreasing Sepsis Mortality at the University of Colorado Hospital Maureen Dzialo, RN, BSN - Nurse Manager, Cardiac Intensive Care Unit Olivia Kerveillant, RN Clinical Nurse III, Medical Intensive Care
Decreasing Sepsis Mortality at the University of Colorado Hospital Maureen Dzialo, RN, BSN - Nurse Manager, Cardiac Intensive Care Unit Olivia Kerveillant, RN Clinical Nurse III, Medical Intensive Care
Inpatient Code Sepsis March Update. Sarah Prebil
 Inpatient Code Sepsis March Update Sarah Prebil 3 hour bundle Time is life Kumar et al. Crit Care Med 2006; 34:1589-1596 But Sarah, why are you harassing us about sepsis? Pilot Results 10 Code Sepsis pabents
Inpatient Code Sepsis March Update Sarah Prebil 3 hour bundle Time is life Kumar et al. Crit Care Med 2006; 34:1589-1596 But Sarah, why are you harassing us about sepsis? Pilot Results 10 Code Sepsis pabents
Sepsis: Identification and Treatment
 Sepsis: Identification and Treatment Daniel Z. Uslan, MD Associate Clinical Professor Division of Infectious Diseases Medical Director, UCLA Sepsis Task Force Severe Sepsis: A Significant Healthcare Challenge
Sepsis: Identification and Treatment Daniel Z. Uslan, MD Associate Clinical Professor Division of Infectious Diseases Medical Director, UCLA Sepsis Task Force Severe Sepsis: A Significant Healthcare Challenge
Septic Shock: Pharmacologic Agents for Hemodynamic Support. Nathan E Cope, PharmD PGY2 Critical Care Pharmacy Resident
 Septic Shock: Pharmacologic Agents for Hemodynamic Support Nathan E Cope, PharmD PGY2 Critical Care Pharmacy Resident Objectives Define septic shock and briefly review pathophysiology Outline receptor
Septic Shock: Pharmacologic Agents for Hemodynamic Support Nathan E Cope, PharmD PGY2 Critical Care Pharmacy Resident Objectives Define septic shock and briefly review pathophysiology Outline receptor
Sepsis Reassess patient Monitor and maintain respiratory/ hemodynamic status
 Patient exhibits two or more of the following SIRS criteria: Temperature greater than 38 o C (100.4 o F) or less SIRS than criteria 36 o C (96.8 o F) Heart Rate greater than 90 beats/minute Respiratory
Patient exhibits two or more of the following SIRS criteria: Temperature greater than 38 o C (100.4 o F) or less SIRS than criteria 36 o C (96.8 o F) Heart Rate greater than 90 beats/minute Respiratory
How To Review A Sepsis Case In Qmp Quality Management Portal
 Quality Management Portal (QMP) & Sepsis Data Analysis Lessons Learned & Progress To Date Nicole Falgout, RN Sepsis Coordinator Rei Cates Sr. Software Engineer UCLA Quality Management Services 1 Quality
Quality Management Portal (QMP) & Sepsis Data Analysis Lessons Learned & Progress To Date Nicole Falgout, RN Sepsis Coordinator Rei Cates Sr. Software Engineer UCLA Quality Management Services 1 Quality
Subject: Severe Sepsis/Septic Shock Published Date: August 9, 2013 Scope: Hospital Wide Original Creation Date: August 9, 2013
 Stony Brook Medicine Severe Sepsis/Septic Shock Recognition and Treatment Protocols Subject: Severe Sepsis/Septic Shock Published Date: August 9, 2013 Scope: Hospital Wide Original Creation Date: August
Stony Brook Medicine Severe Sepsis/Septic Shock Recognition and Treatment Protocols Subject: Severe Sepsis/Septic Shock Published Date: August 9, 2013 Scope: Hospital Wide Original Creation Date: August
Southern California Patient Safety First Collaborative Long Beach Memorial Medical Center Team Presentation. September 17, 2014
 Southern California Patient Safety First Collaborative Long Beach Memorial Medical Center Team Presentation September 17, 2014 1907 2014 Not-for-profit, community-based One of few campuses home to adult
Southern California Patient Safety First Collaborative Long Beach Memorial Medical Center Team Presentation September 17, 2014 1907 2014 Not-for-profit, community-based One of few campuses home to adult
BUNDLES IN 2013: SURVIVING SEPSIS CAMPAIGN
 BUNDLES IN 2013: SURVIVING SEPSIS CAMPAIGN R. Phillip Dellinger MD, MSc, MCCM Professor of Medicine Cooper Medical School of Rowan University Professor of Medicine University Medicine and Dentistry of
BUNDLES IN 2013: SURVIVING SEPSIS CAMPAIGN R. Phillip Dellinger MD, MSc, MCCM Professor of Medicine Cooper Medical School of Rowan University Professor of Medicine University Medicine and Dentistry of
A Protocol for Early Goal Directed Therapy in the Emergency Department: Can we change compliance?
 Luke Benvenuto CRC Rotation IRB Proposal A Protocol for Early Goal Directed Therapy in the Emergency Department: Can we change compliance? Study Purpose and Rationale The systemic inflammatory response
Luke Benvenuto CRC Rotation IRB Proposal A Protocol for Early Goal Directed Therapy in the Emergency Department: Can we change compliance? Study Purpose and Rationale The systemic inflammatory response
Ruchika D. Husa, MD, MS Assistant t Professor of Medicine in the Division of Cardiology The Ohio State University Wexner Medical Center
 Modified Early Warning Score (MEWS) Ruchika D. Husa, MD, MS Assistant t Professor of Medicine i in the Division of Cardiology The Ohio State University Wexner Medical Center MEWS Simple physiological scoring
Modified Early Warning Score (MEWS) Ruchika D. Husa, MD, MS Assistant t Professor of Medicine i in the Division of Cardiology The Ohio State University Wexner Medical Center MEWS Simple physiological scoring
Telemedicine Resuscitation & Arrest Trials (TreAT)
") Telemedicine Resuscitation & Arrest Trials (TreAT) Telemedicine within the ED for treating Severe Sepsis: A Hub and Spoke Telemedicine pilot SUMR Intern: Karole Collier Mentor: Dr. Brendan Carr & Dr. Anish
Telemedicine Resuscitation & Arrest Trials (TreAT) Telemedicine within the ED for treating Severe Sepsis: A Hub and Spoke Telemedicine pilot SUMR Intern: Karole Collier Mentor: Dr. Brendan Carr & Dr. Anish
Using Predictive Analytics to Improve Sepsis Outcomes 4/23/2014
 Using Predictive Analytics to Improve Sepsis Outcomes 4/23/2014 Ryan Arnold, MD Department of Emergency Medicine and Value Institute Christiana Care Health System, Newark, DE Susan Niemeier, RN Chief Nursing
Using Predictive Analytics to Improve Sepsis Outcomes 4/23/2014 Ryan Arnold, MD Department of Emergency Medicine and Value Institute Christiana Care Health System, Newark, DE Susan Niemeier, RN Chief Nursing
Organization: MedStar Union Memorial Hospital. Solution Title: Call 911: Our Documentation Died! Program/Project Description, including Goal:
 Organization: MedStar Union Memorial Hospital Solution Title: Call 911: Our Documentation Died! Program/Project Description, including Goal: Our Emergency Department (ED) converted to an electronic medical
Organization: MedStar Union Memorial Hospital Solution Title: Call 911: Our Documentation Died! Program/Project Description, including Goal: Our Emergency Department (ED) converted to an electronic medical
Michelle Pinelle RN, BSN, CCRN & Jamie Roney RN, BSN, CCRN Texas Tech University Health Sciences Center, Lubbock, Texas
 Michelle Pinelle RN, BSN, CCRN & Jamie Roney RN, BSN, CCRN Texas Tech University Health Sciences Center, Lubbock, Texas AGREE II Tool Evaluation of Sepsis Guidelines 1. The learner will be able to discuss
Michelle Pinelle RN, BSN, CCRN & Jamie Roney RN, BSN, CCRN Texas Tech University Health Sciences Center, Lubbock, Texas AGREE II Tool Evaluation of Sepsis Guidelines 1. The learner will be able to discuss
Suffolk County Community College School of Nursing NUR 133 ADULT NURSING I
 Suffolk County Community College School of Nursing NUR 133 ADULT NURSING I Page # 1 Instructions for students: Case study # 1 For this lab, you are planning to provide care to the following client: CB
Suffolk County Community College School of Nursing NUR 133 ADULT NURSING I Page # 1 Instructions for students: Case study # 1 For this lab, you are planning to provide care to the following client: CB
 Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Patient Care Services Quality Report Evaluation of 2013 Outcomes August 2014
 Patient Care Services Quality Report Evaluation of 2013 Outcomes August 2014 Submitted by, Carol A Dwyer, MSN, MM, RN, CENP Vice President, Patient Care Services Chief Nursing Officer 1 Index INTRODUCTION...3
Patient Care Services Quality Report Evaluation of 2013 Outcomes August 2014 Submitted by, Carol A Dwyer, MSN, MM, RN, CENP Vice President, Patient Care Services Chief Nursing Officer 1 Index INTRODUCTION...3
Case Study: Using Predictive Analytics to Reduce Sepsis Mortality
 Case Study: Using Predictive Analytics to Reduce Sepsis Mortality 1 Learning Objectives 1. Understand how an automated, real time IT intervention can help care teams recognize and intervene on critical,
Case Study: Using Predictive Analytics to Reduce Sepsis Mortality 1 Learning Objectives 1. Understand how an automated, real time IT intervention can help care teams recognize and intervene on critical,
The Initial and 24 h (After the Patient Rehabilitation) Deficit of Arterial Blood Gases as Predictors of Patients Outcome
 Deficit of Arterial Blood Gases as Predictors of Patients Outcome") Biomedical & Pharmacology Journal Vol. 6(2), 259-264 (2013) The Initial and 24 h (After the Patient Rehabilitation) Deficit of Arterial Blood Gases as Predictors of Patients Outcome Vadod Norouzi 1, Ali
Biomedical & Pharmacology Journal Vol. 6(2), 259-264 (2013) The Initial and 24 h (After the Patient Rehabilitation) Deficit of Arterial Blood Gases as Predictors of Patients Outcome Vadod Norouzi 1, Ali
Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi
 Clinical Sessions 2011 By Bhavin Doshi") Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi What is EWS? After qualifying, junior doctors are expected to distinguish between the moderately sick patients who can be managed in the
Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi What is EWS? After qualifying, junior doctors are expected to distinguish between the moderately sick patients who can be managed in the
Vasopressors. Judith Hellman, M.D. Associate Professor Anesthesia and Perioperative Care University of California, San Francisco
 Vasopressors Judith Hellman, M.D. Associate Professor Anesthesia and Perioperative Care University of California, San Francisco Overview Define shock states Review drugs commonly used to treat hypotension
Vasopressors Judith Hellman, M.D. Associate Professor Anesthesia and Perioperative Care University of California, San Francisco Overview Define shock states Review drugs commonly used to treat hypotension
Stacy McLaughlin, RN, MSN. Director of Quality & Performance Improvement
 Stacy McLaughlin, RN, MSN Director of Quality & Performance Improvement 25-bed CAH 21 beds: acute / observation / swingbed 4 bed ICU ED volumes: 14,400 encounters/year 5 Clinics: Rural Health / Primary
Stacy McLaughlin, RN, MSN Director of Quality & Performance Improvement 25-bed CAH 21 beds: acute / observation / swingbed 4 bed ICU ED volumes: 14,400 encounters/year 5 Clinics: Rural Health / Primary
Sue Carol Verrillo, RN, MSN, CRRN The Johns Hopkins Hospital November 14, 2014
 Early Detection of Patient Deterioration Using Remote Patient Monitoring with Wireless Nurse Notification Sue Carol Verrillo, RN, MSN, CRRN The Johns Hopkins Hospital November 14, 2014 1 Why Remote Patient
Early Detection of Patient Deterioration Using Remote Patient Monitoring with Wireless Nurse Notification Sue Carol Verrillo, RN, MSN, CRRN The Johns Hopkins Hospital November 14, 2014 1 Why Remote Patient
Sustainability: Achieving Clinical and Financial Benefits Through the Use of an EHR
 Sustainability: Achieving Clinical and Financial Benefits Through the Use of an EHR Bert Reese SVP and CIO of Sentara Healthcare Sentara Healthcare October 6, 2014 1 Sentara Healthcare 126-year not-for-profit
Sustainability: Achieving Clinical and Financial Benefits Through the Use of an EHR Bert Reese SVP and CIO of Sentara Healthcare Sentara Healthcare October 6, 2014 1 Sentara Healthcare 126-year not-for-profit
SARASOTA MEMORIAL HOSPITAL STANDARDS OF CARE STANDARDS OF PRACTICE
 UNIT: INTENSIVE CARE UNIT - ICU SARASOTA MEMORIAL HOSPITAL STANDARDS OF CARE STANDARDS OF PRACTICE STANDARD #: EFFECTIVE DATE: REVISED DATE: STANDARD TYPE: INTENSIVE CARE UNIT-ICU STANDARD I - SAFETY 3/88
UNIT: INTENSIVE CARE UNIT - ICU SARASOTA MEMORIAL HOSPITAL STANDARDS OF CARE STANDARDS OF PRACTICE STANDARD #: EFFECTIVE DATE: REVISED DATE: STANDARD TYPE: INTENSIVE CARE UNIT-ICU STANDARD I - SAFETY 3/88
Building an Emergency Response to Acute Stroke
 Great Lakes Stroke Network August 2006 Building an Emergency Response to Acute Stroke Wende N. Fedder RN, BSN, MBA Director, Stroke & Neurovascular Services Alexian Brothers Hospital Network Elk Grove
Great Lakes Stroke Network August 2006 Building an Emergency Response to Acute Stroke Wende N. Fedder RN, BSN, MBA Director, Stroke & Neurovascular Services Alexian Brothers Hospital Network Elk Grove
Patients Receive Recommended Care for Community-Acquired Pneumonia
 Patients Receive Recommended Care for Community-Acquired Pneumonia For New Jersey to be a state in which all people live long, healthy lives. DSRIP LEARNING COLLABORATIVE PRESENTATION The Care you Trust!
Patients Receive Recommended Care for Community-Acquired Pneumonia For New Jersey to be a state in which all people live long, healthy lives. DSRIP LEARNING COLLABORATIVE PRESENTATION The Care you Trust!
Improving Pediatric Emergency Department Patient Throughput and Operational Performance
 PERFORMANCE 1 Improving Pediatric Emergency Department Patient Throughput and Operational Performance Rachel Weber, M.S. 2 Abbey Marquette, M.S. 2 LesleyAnn Carlson, R.N., M.S.N. 1 Paul Kurtin, M.D. 3
PERFORMANCE 1 Improving Pediatric Emergency Department Patient Throughput and Operational Performance Rachel Weber, M.S. 2 Abbey Marquette, M.S. 2 LesleyAnn Carlson, R.N., M.S.N. 1 Paul Kurtin, M.D. 3
Unstoppable Report Removing a Barrier to Patient Flow by Nursing Process Redesign
 Unstoppable Report Removing a Barrier to Patient Flow by Nursing Process Redesign 17th Annual Society for Health Systems Management Engineering Forum February 12-13, 2005 Dallas, Texas Norwalk Hospital
Unstoppable Report Removing a Barrier to Patient Flow by Nursing Process Redesign 17th Annual Society for Health Systems Management Engineering Forum February 12-13, 2005 Dallas, Texas Norwalk Hospital
USC Pediatric Residency Program Quality Improvement Pre-Program Self Assessment
 USC Pediatric Residency Program Quality Improvement Pre-Program Self Assessment 1. Have you had previous experience in quality improvement (QI)? Yes No 2. How many formal quality improvement projects have
USC Pediatric Residency Program Quality Improvement Pre-Program Self Assessment 1. Have you had previous experience in quality improvement (QI)? Yes No 2. How many formal quality improvement projects have
AT&T Global Network Client for Windows Product Support Matrix January 29, 2015
 AT&T Global Network Client for Windows Product Support Matrix January 29, 2015 Product Support Matrix Following is the Product Support Matrix for the AT&T Global Network Client. See the AT&T Global Network
AT&T Global Network Client for Windows Product Support Matrix January 29, 2015 Product Support Matrix Following is the Product Support Matrix for the AT&T Global Network Client. See the AT&T Global Network
Inpatient Cerner Navigation and Documentation For Nursing Students
 Inpatient Cerner Navigation and Documentation For Nursing Students Audience Note: Purpose: Objectives: Cerner PowerChart training is for all students in the following inpatient areas Med/Surg, OSNO, Oncology,
Inpatient Cerner Navigation and Documentation For Nursing Students Audience Note: Purpose: Objectives: Cerner PowerChart training is for all students in the following inpatient areas Med/Surg, OSNO, Oncology,
Solution Title: Predicting Care Using Informatics/MEWS (Modified Early Warning System)
") Organization: Peninsula Regional Medical Center Solution Title: Predicting Care Using Informatics/MEWS (Modified Early Warning System) Program/Project Description, including Goals: Problem: As stated in
Organization: Peninsula Regional Medical Center Solution Title: Predicting Care Using Informatics/MEWS (Modified Early Warning System) Program/Project Description, including Goals: Problem: As stated in
Reliability Testing of a Modified Early Warning Scoring (MEWS) Tool Presented By: Lexie Scarborough Futrell, MSN, RN, CCRN Lubbock, Texas, USA
 Tool Presented By: Lexie Scarborough Futrell, MSN, RN, CCRN Lubbock, Texas, USA") Reliability Testing of a Modified Early Warning Scoring (MEWS) Tool Presented By: Lexie Scarborough Futrell, MSN, RN, CCRN Lubbock, Texas, USA Research Team: Erin Whitley, BSN, RN Jamie K. Roney, BSN,
Reliability Testing of a Modified Early Warning Scoring (MEWS) Tool Presented By: Lexie Scarborough Futrell, MSN, RN, CCRN Lubbock, Texas, USA Research Team: Erin Whitley, BSN, RN Jamie K. Roney, BSN,
Improving Outcomes and Saving Lives in Real Time: How Hospitals Can Use Predictive Analytics Across the Care Continuum Essential Hospitals Engagement
 Improving Outcomes and Saving Lives in Real Time: How Hospitals Can Use Predictive Analytics Across the Care Continuum Essential Hospitals Engagement Network February 18, 2015 CHAT FEATURE The chat tool
Improving Outcomes and Saving Lives in Real Time: How Hospitals Can Use Predictive Analytics Across the Care Continuum Essential Hospitals Engagement Network February 18, 2015 CHAT FEATURE The chat tool
Emergency Department Directors Academy Phase II. The ED is a Business: Intelligent Use of Dashboards
 Emergency Department Directors Academy Phase II The ED is a Business: Intelligent Use of Dashboards May 2011 The ED is a Business; Intelligent Use of Dashboards Katherine Haddix-Hill, RN, MSN Acknowledge:
Emergency Department Directors Academy Phase II The ED is a Business: Intelligent Use of Dashboards May 2011 The ED is a Business; Intelligent Use of Dashboards Katherine Haddix-Hill, RN, MSN Acknowledge:
Interfacility Transfer Guidelines for Children
 Interfacility Transfer Guidelines for Children Dear Hospital CEO: As you may know, recent evidence shows that the best outcomes for critically ill and injured children are achieved when treated at facilities
Interfacility Transfer Guidelines for Children Dear Hospital CEO: As you may know, recent evidence shows that the best outcomes for critically ill and injured children are achieved when treated at facilities
Benjamin M. Marlin Department of Computer Science University of Massachusetts Amherst marlin@cs.umass.edu January 21, 2011
 Modeling and Prediction With ICU Electronic Health Records Data Department of Computer Science University of Massachusetts Amherst marlin@cs.umass.edu January 21, 2011 The Big Picture: History of Medical
Modeling and Prediction With ICU Electronic Health Records Data Department of Computer Science University of Massachusetts Amherst marlin@cs.umass.edu January 21, 2011 The Big Picture: History of Medical
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, NP Education Specialist LRM Consulting Nashville, TN
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, NP Education Specialist LRM Consulting Nashville, TN Learning Outcomes Identify triggers to the IIR. Describe the pathophysiologic changes that
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, NP Education Specialist LRM Consulting Nashville, TN Learning Outcomes Identify triggers to the IIR. Describe the pathophysiologic changes that
THE ROYAL CORNWALL HOSPITALS NHS TRUST RESPONSE TO INFORMATION REQUEST. Date Request Received: 20 October 2014 FOI Ref: 567
 FREEDOM OF INFORMATION ACT 2000 THE ROYAL CORNWALL HOSPITALS NHS TRUST RESPONSE TO INFORMATION REQUEST Date Request Received: 20 October 2014 FOI Ref: 567 Requested Information I would like to know whether
FREEDOM OF INFORMATION ACT 2000 THE ROYAL CORNWALL HOSPITALS NHS TRUST RESPONSE TO INFORMATION REQUEST Date Request Received: 20 October 2014 FOI Ref: 567 Requested Information I would like to know whether
Care Coordination at Frederick Regional Health System. Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care
 Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Clinical Nurse Specialist Practice Across the Continuum
 Clinical Nurse Specialist Practice Across the Continuum Angela Rowe, MSN, APRN, PCNS-BC Pediatric Clinical Nurse Specialist Arkansas Children s Hospital Presentation ID: CD3 Disclosure Today s presenters
Clinical Nurse Specialist Practice Across the Continuum Angela Rowe, MSN, APRN, PCNS-BC Pediatric Clinical Nurse Specialist Arkansas Children s Hospital Presentation ID: CD3 Disclosure Today s presenters
REMINDER: Please ensure all stroke and TIA patients admitted to hospital are designated as "Stroke Service" in Cerner.
 ACUTE STROKE CLINICAL PATHWAY QEH/HH PCH KCMH Souris Western Stewart Memorial O'Leary PATIENT ID INCLUSION CRITERIA* All patients admitted to hosptial with a suspected diagnosis of acute ischemic stroke
ACUTE STROKE CLINICAL PATHWAY QEH/HH PCH KCMH Souris Western Stewart Memorial O'Leary PATIENT ID INCLUSION CRITERIA* All patients admitted to hosptial with a suspected diagnosis of acute ischemic stroke
INR: RUPTURED ANEURYSM: POST EMBOLIZATION Patient Identification Page 1 of 5. Allergies: Weight: kg Diagnosis:
 Page 1 of 5 Allergies: Weight: kg Diagnosis: Service: Admission Admit to Inpatient Admit to Daypatient Place on Outpatient Observation Status Hospital Attending: Attending Physician Attending Provider:
Page 1 of 5 Allergies: Weight: kg Diagnosis: Service: Admission Admit to Inpatient Admit to Daypatient Place on Outpatient Observation Status Hospital Attending: Attending Physician Attending Provider:
9/16/2010. Contact Information. Objectives. Analgesic Ketamine (Ketalar )
") Analgesic Ketamine (Ketalar )..the long and winding road to clinical practice Contact Information Lois Pizzi BSN, RN-BC Inpatient Pain Management Clinician UPMC Presbyterian Shadyside pizzilj@upmc.edu
Analgesic Ketamine (Ketalar )..the long and winding road to clinical practice Contact Information Lois Pizzi BSN, RN-BC Inpatient Pain Management Clinician UPMC Presbyterian Shadyside pizzilj@upmc.edu
Value-Based Purchasing Program Overview. Maida Soghikian, MD Grand Rounds Scripps Green Hospital November 28, 2012
 Value-Based Purchasing Program Overview Maida Soghikian, MD Grand Rounds Scripps Green Hospital November 28, 2012 Presentation Overview Background and Introduction Inpatient Quality Reporting Program Value-Based
Value-Based Purchasing Program Overview Maida Soghikian, MD Grand Rounds Scripps Green Hospital November 28, 2012 Presentation Overview Background and Introduction Inpatient Quality Reporting Program Value-Based
How To Improve Care For Bronchiolitis
 Implementation of an Evidence- Based Care Guideline for Inpatient Bronchiolitis Management J E A N E T T E J O N E S, R N + T H O M A S M A Y E S, M D, M B A * + M A R I S S A M A R T I N E Z, M D + S
Implementation of an Evidence- Based Care Guideline for Inpatient Bronchiolitis Management J E A N E T T E J O N E S, R N + T H O M A S M A Y E S, M D, M B A * + M A R I S S A M A R T I N E Z, M D + S
Deborah Young, RN, BSN, CNOR Green Belt Charleston Area Medical Center
 Deborah Young, RN, BSN, CNOR Green Belt Charleston Area Medical Center Charleston Area Medical Center Charleston, West Virginia 5,818 Employees 913 Licensed Beds 392 General Hospital 375 Memorial Hospital
Deborah Young, RN, BSN, CNOR Green Belt Charleston Area Medical Center Charleston Area Medical Center Charleston, West Virginia 5,818 Employees 913 Licensed Beds 392 General Hospital 375 Memorial Hospital
Atrial Fibrillation in the ICU: Attempting to defend 4 controversial statements
 Atrial Fibrillation in the ICU: Attempting to defend 4 controversial statements Salmaan Kanji, Pharm.D. The Ottawa Hospital The Ottawa Hospital Research Institute Conflict of Interest No financial, proprietary
Atrial Fibrillation in the ICU: Attempting to defend 4 controversial statements Salmaan Kanji, Pharm.D. The Ottawa Hospital The Ottawa Hospital Research Institute Conflict of Interest No financial, proprietary
Go With The Flow- From Charge Nurse to Patient Flow Coordinator. Donna Ojanen Thomas, RN, MSN Cynthia J. Royall, RN, BSN
 Go With The Flow- From Charge Nurse to Patient Flow Coordinator Donna Ojanen Thomas, RN, MSN Cynthia J. Royall, RN, BSN Primary Children s Medical Center About PCMC Not for profit hospital, part of Intermountain
Go With The Flow- From Charge Nurse to Patient Flow Coordinator Donna Ojanen Thomas, RN, MSN Cynthia J. Royall, RN, BSN Primary Children s Medical Center About PCMC Not for profit hospital, part of Intermountain
It is recommended that the reader review each medical directive presented in this presentation along with the actual PCP Core medical directive.
 It is recommended that the reader review each medical directive presented in this presentation along with the actual PCP Core medical directive. This presentation will highlight the changes and any new
It is recommended that the reader review each medical directive presented in this presentation along with the actual PCP Core medical directive. This presentation will highlight the changes and any new
COMPARISON OF FIXED & VARIABLE RATES (25 YEARS) CHARTERED BANK ADMINISTERED INTEREST RATES - PRIME BUSINESS*
 CHARTERED BANK ADMINISTERED INTEREST RATES - PRIME BUSINESS*") COMPARISON OF FIXED & VARIABLE RATES (25 YEARS) 2 Fixed Rates Variable Rates FIXED RATES OF THE PAST 25 YEARS AVERAGE RESIDENTIAL MORTGAGE LENDING RATE - 5 YEAR* (Per cent) Year Jan Feb Mar Apr May Jun
COMPARISON OF FIXED & VARIABLE RATES (25 YEARS) 2 Fixed Rates Variable Rates FIXED RATES OF THE PAST 25 YEARS AVERAGE RESIDENTIAL MORTGAGE LENDING RATE - 5 YEAR* (Per cent) Year Jan Feb Mar Apr May Jun
COMPARISON OF FIXED & VARIABLE RATES (25 YEARS) CHARTERED BANK ADMINISTERED INTEREST RATES - PRIME BUSINESS*
 CHARTERED BANK ADMINISTERED INTEREST RATES - PRIME BUSINESS*") COMPARISON OF FIXED & VARIABLE RATES (25 YEARS) 2 Fixed Rates Variable Rates FIXED RATES OF THE PAST 25 YEARS AVERAGE RESIDENTIAL MORTGAGE LENDING RATE - 5 YEAR* (Per cent) Year Jan Feb Mar Apr May Jun
COMPARISON OF FIXED & VARIABLE RATES (25 YEARS) 2 Fixed Rates Variable Rates FIXED RATES OF THE PAST 25 YEARS AVERAGE RESIDENTIAL MORTGAGE LENDING RATE - 5 YEAR* (Per cent) Year Jan Feb Mar Apr May Jun
Retrospective review of the Modified Early Warning Score in critically ill surgical inpatients at a Canadian Hospital
 Retrospective review of the Modified Early Warning Score in critically ill surgical inpatients at a Canadian Hospital Alisha Mills PGY 4 General Surgery Northern Ontario School of Medicine S Disclosures
Retrospective review of the Modified Early Warning Score in critically ill surgical inpatients at a Canadian Hospital Alisha Mills PGY 4 General Surgery Northern Ontario School of Medicine S Disclosures
THE AIRWAY IN AEROMEDICAL EVACUATION. PBLD (Problem Based Learning Discussion)
") THE AIRWAY IN AEROMEDICAL EVACUATION PBLD (Problem Based Learning Discussion) D. John Doyle MD PhD 2012 Edition Image Credit: http://www.arabianaerospace.aero/media/images/stories/medevac%20services.jpg
THE AIRWAY IN AEROMEDICAL EVACUATION PBLD (Problem Based Learning Discussion) D. John Doyle MD PhD 2012 Edition Image Credit: http://www.arabianaerospace.aero/media/images/stories/medevac%20services.jpg
Session Number 312 FAILURE TO RESCUE: BE PROACTIVE NOT REACTIVE
 Content Description Session Number 312 FAILURE TO RESCUE: BE PROACTIVE NOT REACTIVE Linda Bucher, RN, PhD, CEN, CNE Staff Nurse Virtua Memorial Hospital Emergency Department Mt. Holly, NJ The purpose of
Content Description Session Number 312 FAILURE TO RESCUE: BE PROACTIVE NOT REACTIVE Linda Bucher, RN, PhD, CEN, CNE Staff Nurse Virtua Memorial Hospital Emergency Department Mt. Holly, NJ The purpose of
Menu Case Study 3: Medication Administration Record
 Menu Case Study 3: Medication Administration Record Applicant Organization: Ontario Shores Centre for Mental Health Sciences Organization s Address: 700 Gordon Street, Whitby, Ontario, Canada, L1N5S9 Submitter
Menu Case Study 3: Medication Administration Record Applicant Organization: Ontario Shores Centre for Mental Health Sciences Organization s Address: 700 Gordon Street, Whitby, Ontario, Canada, L1N5S9 Submitter
Jeopardy Topics: THE CLOT STOPS HERE (anticoagulants) SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins)
 SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins)") Jeopardy Topics: THE CLOT STOPS HERE (anticoagulants) SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins) I HEAR YA KNOCKING BUT YOU CAN T COME IN (electrolytes) TAKE MY BREATH AWAY (Opiates-morphine) OUT WITH
Jeopardy Topics: THE CLOT STOPS HERE (anticoagulants) SUGAR, SUGAR, HOW D YOU GET SO HIGH (insulins) I HEAR YA KNOCKING BUT YOU CAN T COME IN (electrolytes) TAKE MY BREATH AWAY (Opiates-morphine) OUT WITH
The New Complex Patient. of Diabetes Clinical Programming
 The New Complex Patient as Seen Through the Lens of Diabetes Clinical Programming 1 Valerie Garrett, M.D. Medical Director, Diabetes Center at Mission Health System Nov 6, 2014 Diabetes Health Burden High
The New Complex Patient as Seen Through the Lens of Diabetes Clinical Programming 1 Valerie Garrett, M.D. Medical Director, Diabetes Center at Mission Health System Nov 6, 2014 Diabetes Health Burden High
Health IT and Patient Safety: A Nursing Perspective from the United States
 Health IT and Patient Safety: A Nursing Perspective from the United States Patricia P. Sengstack DNP, RN-BC, CPHIMS Chief Nursing Informatics Officer Bon Secours Health System Marriottsville, Maryland
Health IT and Patient Safety: A Nursing Perspective from the United States Patricia P. Sengstack DNP, RN-BC, CPHIMS Chief Nursing Informatics Officer Bon Secours Health System Marriottsville, Maryland
Introducing a NEW simulation based training program for KGH / HDH Emergency Room Nurses
 Introducing a NEW simulation based training program for KGH / HDH Emergency Room Nurses Are you looking to improve your skills in ER nursing care? Have you heard about the benefits of simulation based
Introducing a NEW simulation based training program for KGH / HDH Emergency Room Nurses Are you looking to improve your skills in ER nursing care? Have you heard about the benefits of simulation based
ENROLLED NURSE GRADUATE PROGRAM: BENDIGO HEALTH. Dr Helen Aikman Manager of Nursing and Midwifery Education
 ENROLLED NURSE GRADUATE PROGRAM: BENDIGO HEALTH Dr Helen Aikman Manager of Nursing and Midwifery Education Insert title The need: Most professions have identified that early graduates need support Professional
ENROLLED NURSE GRADUATE PROGRAM: BENDIGO HEALTH Dr Helen Aikman Manager of Nursing and Midwifery Education Insert title The need: Most professions have identified that early graduates need support Professional
Medical Direction and Practices Board WHITE PAPER
 Medical Direction and Practices Board WHITE PAPER Use of Pressors in Pre-Hospital Medicine: Proper Indication and State of the Science Regarding Proper Choice of Pressor BACKGROUND Shock is caused by a
Medical Direction and Practices Board WHITE PAPER Use of Pressors in Pre-Hospital Medicine: Proper Indication and State of the Science Regarding Proper Choice of Pressor BACKGROUND Shock is caused by a
5/8/2015. Nursing Professional Role Development Program- Day 2. Learning Objectives. Application of Learned Models and Concepts
 Nursing Professional Role Development Program- Day 2 Learning Objectives 1. Share your Champion-session experience. 2. Describe the O Rourke 9-Step Decision-Making Model and its application in professional
Nursing Professional Role Development Program- Day 2 Learning Objectives 1. Share your Champion-session experience. 2. Describe the O Rourke 9-Step Decision-Making Model and its application in professional
Simulation Design Template
 Simulation Design Template Date: May 7, 2008 Discipline: Expected Simulation Run Time: 20 mins Location: hospital ER Admission Date: Today s Date: Brief Description of Client Name: Mr. Crash Gender: M
Simulation Design Template Date: May 7, 2008 Discipline: Expected Simulation Run Time: 20 mins Location: hospital ER Admission Date: Today s Date: Brief Description of Client Name: Mr. Crash Gender: M
1.4.4 Oxyhemoglobin desaturation
 Critical Care Therapy and Respiratory Care Section Category: Clinical Section: Clinical Monitoring Title: Monitoring of Patients Undergoing Conscious Sedation Policy #: 09 Revised: 05/00 1.0 DESCRIPTION
Critical Care Therapy and Respiratory Care Section Category: Clinical Section: Clinical Monitoring Title: Monitoring of Patients Undergoing Conscious Sedation Policy #: 09 Revised: 05/00 1.0 DESCRIPTION
VA SAN DIEGO HEALTHCARE SYSTEM MEMORANDUM 118-28 SAN DIEGO, CA
 GUIDELINES FOR PATIENT-CONTROLLED ANALGESIA (PCA) AND PATIENT- CONTROLLED EPIDURAL ANALGESIA (PCEA) FOR ACUTE PAIN MANAGEMENT 1. PURPOSE: To assure the safe and effective use of patient controlled analgesia
GUIDELINES FOR PATIENT-CONTROLLED ANALGESIA (PCA) AND PATIENT- CONTROLLED EPIDURAL ANALGESIA (PCEA) FOR ACUTE PAIN MANAGEMENT 1. PURPOSE: To assure the safe and effective use of patient controlled analgesia
Correctional Treatment CenterF
 0BCHAPTER 15 F 1BI. POLICY The California Department of Corrections and Rehabilitation (CDCR) shall maintain s (CTC) to house inmate-patients who do not require general acute care level of services but
0BCHAPTER 15 F 1BI. POLICY The California Department of Corrections and Rehabilitation (CDCR) shall maintain s (CTC) to house inmate-patients who do not require general acute care level of services but
RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND
 RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND Monitor patient on the ward to detect trends in vital signs and to manage accordingly To recognise deteriorating trends and request relevant medical/out
RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND Monitor patient on the ward to detect trends in vital signs and to manage accordingly To recognise deteriorating trends and request relevant medical/out
Lothian Diabetes Handbook MANAGEMENT OF DIABETIC KETOACIDOSIS
 MANAGEMENT OF DIABETIC KETOACIDOSIS 90 MANAGEMENT OF DIABETIC KETOACIDOSIS Diagnosis elevated plasma and/or urinary ketones metabolic acidosis (raised H + /low serum bicarbonate) Remember that hyperglycaemia,
MANAGEMENT OF DIABETIC KETOACIDOSIS 90 MANAGEMENT OF DIABETIC KETOACIDOSIS Diagnosis elevated plasma and/or urinary ketones metabolic acidosis (raised H + /low serum bicarbonate) Remember that hyperglycaemia,
Recommendations: Other Supportive Therapy of Severe Sepsis*
 Recommendations: Other Supportive Therapy of Severe Sepsis* K. Blood Product Administration 1. Once tissue hypoperfusion has resolved and in the absence of extenuating circumstances, such as myocardial
Recommendations: Other Supportive Therapy of Severe Sepsis* K. Blood Product Administration 1. Once tissue hypoperfusion has resolved and in the absence of extenuating circumstances, such as myocardial
Healthcare Inspection
 Department of Veterans Affairs Office of Inspector General Healthcare Inspection Excessive Length of Stay and Quality of Care Issues in the Emergency Department William Jennings Bryan Dorn VA Medical Center
Department of Veterans Affairs Office of Inspector General Healthcare Inspection Excessive Length of Stay and Quality of Care Issues in the Emergency Department William Jennings Bryan Dorn VA Medical Center
FROM DATA TO KNOWLEDGE: INTEGRATING ELECTRONIC HEALTH RECORDS MEANINGFULLY INTO OUR NURSING PRACTICE
 FROM DATA TO KNOWLEDGE: INTEGRATING ELECTRONIC HEALTH RECORDS MEANINGFULLY INTO OUR NURSING PRACTICE Rayne Soriano MS, RN Manager of Nursing Informatics and Clinical Transformation Program Kaiser Permanente
FROM DATA TO KNOWLEDGE: INTEGRATING ELECTRONIC HEALTH RECORDS MEANINGFULLY INTO OUR NURSING PRACTICE Rayne Soriano MS, RN Manager of Nursing Informatics and Clinical Transformation Program Kaiser Permanente
Lean thinking and Six sigma at the level of Clinical Service Delivery
 Lean thinking and Six sigma at the level of Clinical Service Delivery Hugh Rogers FRCS Associate, Service Transformation NHS Institute for Innovation & Improvement Healthcare Events 26 th February 2008
Lean thinking and Six sigma at the level of Clinical Service Delivery Hugh Rogers FRCS Associate, Service Transformation NHS Institute for Innovation & Improvement Healthcare Events 26 th February 2008
Summary of EWS Policy for NHSP Staff
 Summary of EWS Policy for NHSP Staff For full version see CMFT Intranet Contact Sister Donna Egan outreach coordinator bleep 8742 Tel: 0161 276 8742 Introduction The close monitoring of patients physiological
Summary of EWS Policy for NHSP Staff For full version see CMFT Intranet Contact Sister Donna Egan outreach coordinator bleep 8742 Tel: 0161 276 8742 Introduction The close monitoring of patients physiological
Eliminating Pressure Ulcers in Ascension Health
 Eliminating Pressure Ulcers in Ascension Health Cissy Shanks RN BSN CEN & Pam Kleinhelter RN MSN CNA-BC Nursing Managers St Vincent s Health System Jacksonville, Florida Objectives Participants will be
Eliminating Pressure Ulcers in Ascension Health Cissy Shanks RN BSN CEN & Pam Kleinhelter RN MSN CNA-BC Nursing Managers St Vincent s Health System Jacksonville, Florida Objectives Participants will be
Plumbing 101:! TXA and EMS! Jay H. Reich, MD FACEP! EMS Medical Director! City of Kansas City, Missouri/Kansas City Fire Department!
 Plumbing 101:! TXA and EMS! Jay H. Reich, MD FACEP! EMS Medical Director! City of Kansas City, Missouri/Kansas City Fire Department! EMS Section Chief! Department of Emergency Medicine! University of Missouri-Kansas
Plumbing 101:! TXA and EMS! Jay H. Reich, MD FACEP! EMS Medical Director! City of Kansas City, Missouri/Kansas City Fire Department! EMS Section Chief! Department of Emergency Medicine! University of Missouri-Kansas
Clinical Study The Use of an Early Alert System to Improve Compliance with Sepsis Bundles and to Assess Impact on Mortality
 Critical Care Research and Practice Volume 2012, Article ID 980369, 8 pages doi:10.1155/2012/980369 Clinical Study The Use of an Early Alert System to Improve Compliance with Sepsis Bundles and to Assess
Critical Care Research and Practice Volume 2012, Article ID 980369, 8 pages doi:10.1155/2012/980369 Clinical Study The Use of an Early Alert System to Improve Compliance with Sepsis Bundles and to Assess
Using CDS (Clinical Decision Support) for Quality Initiatives at a Community Hospital
 for Quality Initiatives at a Community Hospital") Using CDS (Clinical Decision Support) for Quality Initiatives at a Community Hospital Jonathan Sykes MD, CMIO Jacalyn Liebowitz RN, MBA,NEA-BCFACHE VP Care Continuum Allegiance Health - Jackson, MI DISCLAIMER:
Using CDS (Clinical Decision Support) for Quality Initiatives at a Community Hospital Jonathan Sykes MD, CMIO Jacalyn Liebowitz RN, MBA,NEA-BCFACHE VP Care Continuum Allegiance Health - Jackson, MI DISCLAIMER:
CRRT: I and O. I and O Sheet
 CRRT: I and O I and O Sheet The following slide outlines a 12 hour CRRT I and O record. The individual lines of the I and O portion of the record will be reviewed. At the end of each hour, the ICU nurse
CRRT: I and O I and O Sheet The following slide outlines a 12 hour CRRT I and O record. The individual lines of the I and O portion of the record will be reviewed. At the end of each hour, the ICU nurse
Acute Myocardial Infarction (the formulary thrombolytic for AMI at AAMC is TNK, please see the TNK monograph in this manual for information)
") ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Alteplase (Tissue Plasminogen Activator (t-pa)), Activase in the Treatment
ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Alteplase (Tissue Plasminogen Activator (t-pa)), Activase in the Treatment
Sentara Healthcare EMR: Our Journey. Bert Reese, CIO and Senior Vice President
 Sentara Healthcare EMR: Our Journey Bert Reese, CIO and Senior Vice President Sentara Healthcare 123-year not-for-profit mission 10 hospitals; 2,349 beds; 3,700 physicians on staff 10 long term care/assisted
Sentara Healthcare EMR: Our Journey Bert Reese, CIO and Senior Vice President Sentara Healthcare 123-year not-for-profit mission 10 hospitals; 2,349 beds; 3,700 physicians on staff 10 long term care/assisted
Application of Engineering Principles to Patient Flow & Healthcare Delivery
 Application of Engineering Principles to Patient Flow & Healthcare Delivery Jeanne M Huddleston, MD, MS Medical Director, Health Care Systems Engineering Mayo Clinic 2013 MFMER slide-1 2013 MFMER slide-2
Application of Engineering Principles to Patient Flow & Healthcare Delivery Jeanne M Huddleston, MD, MS Medical Director, Health Care Systems Engineering Mayo Clinic 2013 MFMER slide-1 2013 MFMER slide-2
Overview of emar Electronic Medication Administration Record
 Overview of emar Electronic Medication Administration Record March 2006 WHAT IS emar? emar Electronic Medication Administration Record - Replaces the paper MAR MAK Medication Administration Check (Siemens)
Overview of emar Electronic Medication Administration Record March 2006 WHAT IS emar? emar Electronic Medication Administration Record - Replaces the paper MAR MAK Medication Administration Check (Siemens)
Pain Management in the Critically ill Patient
 Pain Management in the Critically ill Patient Jim Ducharme MD CM, FRCP President-Elect, IFEM Clinical Professor of Medicine, McMaster University Adjunct Professor of Family Medicine, Queens University
Pain Management in the Critically ill Patient Jim Ducharme MD CM, FRCP President-Elect, IFEM Clinical Professor of Medicine, McMaster University Adjunct Professor of Family Medicine, Queens University
Instructor Guide: CPOE (Order Entry) for the Nurse. Trainer Notes. Objective Learn about PowerPlans. Benefits of CPOE. Learn about Nurse Review
 for the Nurse. Trainer Notes. Objective Learn about PowerPlans. Benefits of CPOE. Learn about Nurse Review") Instructor Guide: CPOE (Order Entry) for the Nurse Trainer Notes Section Name Duration Order Entry 45 minutes Objective Learn about PowerPlans Benefits of CPOE Learn about Nurse Review You ll Need Parking
Instructor Guide: CPOE (Order Entry) for the Nurse Trainer Notes Section Name Duration Order Entry 45 minutes Objective Learn about PowerPlans Benefits of CPOE Learn about Nurse Review You ll Need Parking
ANTIBIOTICS IN SEPSIS
 ANTIBIOTICS IN SEPSIS Jennifer Curello, PharmD, BCPS Clinical Pharmacist, Infectious Diseases Antimicrobial Stewardship Program Ronald Reagan UCLA Medical Center October 27, 2014 The power of antibiotics
ANTIBIOTICS IN SEPSIS Jennifer Curello, PharmD, BCPS Clinical Pharmacist, Infectious Diseases Antimicrobial Stewardship Program Ronald Reagan UCLA Medical Center October 27, 2014 The power of antibiotics
Procedure for Inotrope Administration in the home
 Procedure for Inotrope Administration in the home Purpose This purpose of this procedure is to define the care used when administering inotropic agents intravenously in the home This includes: A. Practice
Procedure for Inotrope Administration in the home Purpose This purpose of this procedure is to define the care used when administering inotropic agents intravenously in the home This includes: A. Practice
Edwards FloTrac Sensor & Edwards Vigileo Monitor. Understanding Stroke Volume Variation and Its Clinical Application
 Edwards FloTrac Sensor & Edwards Vigileo Monitor Understanding Stroke Volume Variation and Its Clinical Application 1 Topics System Configuration Pulsus Paradoxes Reversed Pulsus Paradoxus What is Stroke
Edwards FloTrac Sensor & Edwards Vigileo Monitor Understanding Stroke Volume Variation and Its Clinical Application 1 Topics System Configuration Pulsus Paradoxes Reversed Pulsus Paradoxus What is Stroke
ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY. Guidelines for Use of Intravenous Isoproterenol
 ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Isoproterenol Major Indications Status Asthmaticus As a last resort for
ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Isoproterenol Major Indications Status Asthmaticus As a last resort for
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: MANAGEMENT OF THE PREGNANT PATIENT WITH EPIDURAL ANESTHESIA POLICY #: EFFECTIVE DATE: REVISED DATE: POLICY TYPE: PAGE: 126.722 (maternal) 10/88
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: MANAGEMENT OF THE PREGNANT PATIENT WITH EPIDURAL ANESTHESIA POLICY #: EFFECTIVE DATE: REVISED DATE: POLICY TYPE: PAGE: 126.722 (maternal) 10/88
DRG 416 Septicemia. ICD-9-CM Coding Guidelines
 oding uidelines Septicemia ICD-9-CM Coding Guidelines The below listed septicemia guidelines are not inclusive. The coder should refer to the applicable Coding Clinic guidelines for additional information.
oding uidelines Septicemia ICD-9-CM Coding Guidelines The below listed septicemia guidelines are not inclusive. The coder should refer to the applicable Coding Clinic guidelines for additional information.
Clinical Safety & Effectiveness Session # 6
 Clinical Safety & Effectiveness Session # 6 Increased Communication of Essential Elements in Patient Transfers of Care During Anesthesia by 50% in the 2nd Floor ORs at University Hospital Over a 4 month
Clinical Safety & Effectiveness Session # 6 Increased Communication of Essential Elements in Patient Transfers of Care During Anesthesia by 50% in the 2nd Floor ORs at University Hospital Over a 4 month
Cardiac Arrest. Perioperative. Summary of case. Length 15-20 minutes
 scenario overview Summary of case This 45-year-old obese patient is positioned on the OR table for left inguinal hernia repair. New Anesthesia Provider comes to the ED to relieve the current Anesthesia
scenario overview Summary of case This 45-year-old obese patient is positioned on the OR table for left inguinal hernia repair. New Anesthesia Provider comes to the ED to relieve the current Anesthesia
Improving Care Transitions using PDSA Methodology
 Improving Care Transitions using PDSA Methodology Catherine Payne, MD, FHM Care Transitions Physician Champion Medical Director of Clinical Informatics Erlanger Medical Center Chattanooga, Tennessee Objectives
Improving Care Transitions using PDSA Methodology Catherine Payne, MD, FHM Care Transitions Physician Champion Medical Director of Clinical Informatics Erlanger Medical Center Chattanooga, Tennessee Objectives