WellSpan Health Care Management Strategy. October, 2013
|
|
|
- Maximilian Hawkins
- 10 years ago
- Views:
Transcription
1 WellSpan Health Care Management Strategy October, 2013

 Bundled Payments Shared Savings")
2 We will realize a fundamental, yet gradual, shift in how we deliver and receive payment for care From: A system that treats people mostly when they are sick or injured To: A system that PROACTIVELY manages the health of populations Revenue based on volume Revenue based on value From: Rewards based on volume = = + Quality + Efficiency + Satisfaction = Fee for Service Per Case (DRG) Bundled Payments Shared Savings Capitation
3 Striving for the Triple Aim Improve Population Health Access Communication Coordination Collaboration Integration Patient/Family PCM Home PCM Neighborhood Improve Patient Experience Reduce Costs
4 Driven by Mission, Guided by Strategies Our Mission Strategies Execution Working as one to improve health through exceptional care for all, lifelong wellness and healthy communities Achieve clinical excellence, Improve the health of populations in our community Provide a patient and family-centered experience Maintain our historical financial strength Build a clinically integrated physician organization This proposed care management strategy: Leverages efficient and effective clinical programs Advances population health management interventions and offers case management to identified individuals.
5 Early 2012 Organizational Structure

 Care Management 49% of the population consumes only 4% of the total spend (each spends <")
6 WellSpan s Population Health Strategy Focuses on the Different Needs of People at Different Stages of the Continuum of Care % Total Healthcare Spend Those with severe, acute illnesses or injuries Those with chronic illness Those who are well or think they are well % of patients 10% of the population consumes 66% of the total spend (member with > $10,000 expenses) Care Management 49% of the population consumes only 4% of the total spend (each spends < $1,000)
?? Target population for intensive case management (2,500)?")
7 Different populations receive different care management interventions Chronic illness and preventive health registry patients (100,000) Population for whom we take financial risk (50,000)?? Target population for intensive case management (2,500)?? Total population of York and Adams counties (550,000) Total WellSpan Medical Group population (~250,000)
8 WellSpan s Functional Definition of Care Management Care Management is the term we use to describe the successful management of the health care needs of individuals and populations. Our success depends upon the design of our clinical programs and the use of population health management and case management interventions. We apply these activities across the span of an individual s life from wellness through illness and injury, to death with dignity.

9 Care Management Functional Design Clinical Program Care Design The Medical Home and its Neighborhood Population Management Actions that improve the health of groups of people Case Management Actions that improve an individual s care
10 Simple Rules of Care Management 1. MEDICAL HOME Medical Homes are the locus for coordination for all Care Management. 2. SHARED CARE PLAN We help patients develop their own Shared Care Plan that they and their family control and change over time. The patient's Shared Care Plan guides our efforts to promote their mental and physical wellness to restore their health, to palliate their symptoms, and to support death with dignity. 3. SELF-MANAGEMENT We promote health literacy and activation to engage a patient in their health care decisions. 4. ALWAYS AVAILABLE SUPPORT Our support services, in conjunction with community resources, are always available to help selected patients coordinate their health care needs, provide transportation, translation service, medication assistance, and food and shelter, if necessary. 5. PROACTIVE CARE We anticipate the social and clinical needs of individuals who are at risk of deterioration in health status that might be avoided by timely interventions by care management teams. 6. APPROPRIATE CARE Evidence-based care is the foundation of our care management program. When evidence-based recommendations are not available, we use WellSpan s consensus-based approach to define appropriate care.

11 ( Care Management Elements People Programs Payment We build too many walls and not enough bridges ~ Isaac Newton Processes Platform
12 Care Management Functional Design Clinical Program Care Design The Medical Home and its Neighborhood Each of WellSpan s clinical programs should be: Patient and Family Centered Reliable Accessible Coordinated Population Management Actions that improve the health of groups of people Case Management Actions that improve an individual s care
13 Programs our clinical programs must support individuals across the continuum of care Our Clinical Programs employ consistent care (re)design principles Patient Centered Medical Homes the locus for patient planning and coordination Clinical care consistent with our interpretation of evidence-based practices, whenever possible We identify specific providers outside of our System who provide care we are unable to offer Community programs Select regional and national referral centers based on System, not individual, choice
14 A deeper dive on the Patient-Centered Medical Home WellSpan is redesigning care around patient-centered medical homes (PCMH) within the Medical Neighborhood. Access Personal physician Physician directed medical practice Technology and process support Whole person orientation Performance reporting Patient selfmanagement support Care is coordinated and/or integrated
15 PCMH Secret Sauce Data Meeting Structure Culture Accountabilities Central Support
16 Live Dashboard Overview The Data Layered: WMG Practice Provider Care Team Patient Transparent Comparative Trended over time Refreshed monthly Baseline, goals and benchmarks Developed with WMG Quality Council provider input

17 Star awards Baseline Target Pacer line Trends 18
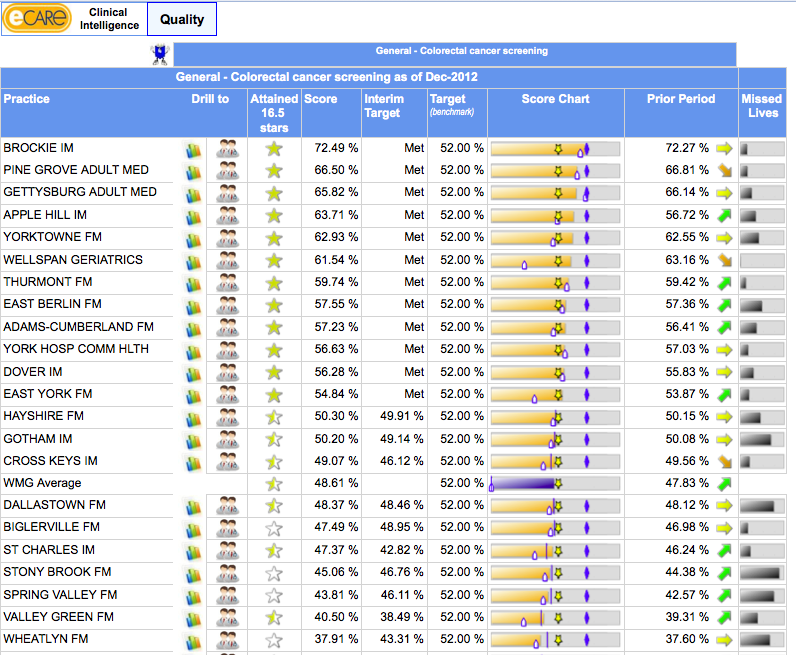
18

19 Care Coordination Teams Optimizing deployment of existing staff PCMH Nurse Case Managers Health Plan And Hospital Health Coaches Social Workers
20 Each PCMH has an embedded care management support structure known as a Care Coordination Team (CCT). CCT Health Coach: full time presence at the PCMH practice who helps patients Address patients chronic and preventive health care issues Promote behavioral changes to improve their health Work with the case manager and social worker to address care coordination needs. CCT Social Worker: Shift their focus from hospital unit to PCMH practice Based in the hospital, but has defined office hours. Addresses financial issues that impact a patient s care decisions Identifies and coordinates community resources Assists patients with hospital discharge planning as well as support through the office setting Works daily with the health coach and case manager to identify and address care coordination needs of the patients. CCT Case Manager: Shift their focus from hospital unit to PCMH practice Based in the hospital setting but has defined office hours. Registered nurse who is trained and certified in case management Assists patients with identifying clinical resources to support the patient s goals for health. Has an understanding of benefit plans, payer processes, and health care standards to help advocate for the patent s plan. Works daily with the health coach and social worker to identify and address care coordination needs of the patients for the practice/providers.
21

22 Our information system enables us to do data mining for high utilization and/or high risk patients. This enables WellSpan to successfully manage the health of populations of patients.
23 Current state PCMH CCT Deployed Case Managers and Social Workers to manage hospital patients by community PCP (YH and GH). CMRN and SW assigned WMG Practice for hospital and community outreach Community PCPs for hospital Case Management work Indentified Case Management liaison for SIBR rounds for each area. Identify CM specialty content expert area and developing neighborhood environment. Incorporating other support roles in the PCMH model Pharmacy Behavioral Health services Rehabilitation Services
24 LVAD Program HC CM SW Hospital Care Stroke program
25 Continued Identify specialty program coordinators (Service Lines) and develop CCT relationship: CVS: MSL: NSL: Ortho: OSL: SSL: BHS: WSL: LVAD Open Heart Medical Weight Loss Stroke Spine Neurological Programs (Concussion, Movement disorders) Joint Replacement Nurse Navigators PHAS Nurse navigators Mood Disorders High Risk Peri-natal
26
27 Who Moved My Cheese? A new mental model for our providers FROM My Patient TO Our Patient My clinical preferences Oriented only to my practice site My plan for the patient I documented my thoughts in my medical record I coordinate my patient s care WellSpan s clinical standards and preferences Oriented to my practice within WellSpan s neighborhood The patient s Shared Care Plan I share my thoughts with colleagues in both written and verbal format My team works with others in the Neighborhood to coordinate care WellSpan s Medical Neighborhood
28 Understanding and Meeting Patients Unique Needs: Our Journey Fall Participate in IHI Learning Network Managing Complex Populations (Care Oregon, Cambridge Health Alliance ) Feb Jeff Brenner, MD ( HotSpotters ) visits York to help kick off pilot (2 visits to Camden, 1 to AtlantiCare) March August 2011 Monthly Superutilizer pilot o 12 patients o Monthly Community Meetings o Extra calls, social work input/contact, appointments, some home visits o Behavioral health consult and access, Trac Phones, fax machines, transportation, teleconferences, Area Agency on Aging, County Human Service, hospitalists June 2012 WellSpan funds strategic initiative Working As One September 2012 WellSpan Bridges to Health opens
29 What is an Ambulatory ICU? Bridges to Health Practice Studies Yale, Massachusetts General Hospital, British Health Service Virtual Ward Boeing Intensive Outpatient Care Program Hotel and Restaurant Employees International Union Hotspotter New York Times - AtlantiCare Now Las Vegas, Dartmouth-Hitchcock, Stanford


30 Analysis of Health Care Costs Reflect a Disproportionate Spend Those with severe, acute illness or injuries % Total Healthcare Spend PCMHs Those with chronic illness Those who are well or think they are well SuperUtilizer Programs % of Members
31
Proven Innovations in Primary Care Practice
 Proven Innovations in Primary Care Practice October 14, 2014 The opinions expressed are those of the presenter and do not necessarily state or reflect the views of SHSMD or the AHA. 2014 Society for Healthcare
Proven Innovations in Primary Care Practice October 14, 2014 The opinions expressed are those of the presenter and do not necessarily state or reflect the views of SHSMD or the AHA. 2014 Society for Healthcare
Realizing ACO Success with ICW Solutions
 Realizing ACO Success with ICW Solutions A Pathway to Collaborative Care Coordination and Care Management Decrease Healthcare Costs Improve Population Health Enhance Care for the Individual connect. manage.
Realizing ACO Success with ICW Solutions A Pathway to Collaborative Care Coordination and Care Management Decrease Healthcare Costs Improve Population Health Enhance Care for the Individual connect. manage.
Partnerships in Primary and Behavioral Health Care ACO Survival Integrated Care
 Partnerships in Primary and Behavioral Health Care ACO Survival Integrated Care Ensuring Success for ACOs September 22 23 Joyce Wale LCSW Vice President, Institute for Behavioral Healthcare Improvement
Partnerships in Primary and Behavioral Health Care ACO Survival Integrated Care Ensuring Success for ACOs September 22 23 Joyce Wale LCSW Vice President, Institute for Behavioral Healthcare Improvement
Parkview Health s Population Health Journey
 Parkview Health s Population Health Journey Susan McAlister DNP, RN Director Enterprise Care Management Christine Howell BSN, RN Community Based Registered Nurse Objectives: By the completion of the webinar
Parkview Health s Population Health Journey Susan McAlister DNP, RN Director Enterprise Care Management Christine Howell BSN, RN Community Based Registered Nurse Objectives: By the completion of the webinar
National Clinical Programmes
 National Clinical Programmes Section 3 Background information on the National Clinical Programmes Mission, Vision and Objectives July 2011 V0. 6_ 4 th July, 2011 1 National Clinical Programmes: Mission
National Clinical Programmes Section 3 Background information on the National Clinical Programmes Mission, Vision and Objectives July 2011 V0. 6_ 4 th July, 2011 1 National Clinical Programmes: Mission
Best Practices in Managing Patients With Chronic Obstructive Pulmonary Disease (COPD)
") Best Practices in Managing Patients With Chronic Obstructive Pulmonary Disease (COPD) DuPage Medical Group Case Study Organization Profile Established in 1999, DuPage Medical Group (DMG) is a multispecialty
Best Practices in Managing Patients With Chronic Obstructive Pulmonary Disease (COPD) DuPage Medical Group Case Study Organization Profile Established in 1999, DuPage Medical Group (DMG) is a multispecialty
Building an Accountable Care Organization. Jean Malouin, MD MPH University of Michigan Health System September 21, 2012
 Building an Accountable Care Organization Jean Malouin, MD MPH University of Michigan Health System September 21, 2012 Agenda UMHS overview PGP demo ACO precursor Current efforts underway Role of primary
Building an Accountable Care Organization Jean Malouin, MD MPH University of Michigan Health System September 21, 2012 Agenda UMHS overview PGP demo ACO precursor Current efforts underway Role of primary
Population Health Solutions for Employers MEDIA RESOURCES
 Population Health Solutions for Employers MEDIA RESOURCES ABOUT MISSIONPOINT MissionPoint s mission is to make healthcare more affordable, accessible and improve the quality of care for our members. MissionPoint
Population Health Solutions for Employers MEDIA RESOURCES ABOUT MISSIONPOINT MissionPoint s mission is to make healthcare more affordable, accessible and improve the quality of care for our members. MissionPoint
What is Home Care Case Management?
 What is Home Care Case Management? Printed in USA Arcadia Home Care & Staffing www.arcadiahomecare.com Case Management: What is it why is it important? While different approaches to healthcare today are
What is Home Care Case Management? Printed in USA Arcadia Home Care & Staffing www.arcadiahomecare.com Case Management: What is it why is it important? While different approaches to healthcare today are
Premier ACO Collaboratives Driving to a Patient-Centered Health System
 Premier ACO Collaboratives Driving to a Patient-Centered Health System As a nation we all must work to rein in spiraling U.S. healthcare costs, expand access, promote wellness and improve the consistency
Premier ACO Collaboratives Driving to a Patient-Centered Health System As a nation we all must work to rein in spiraling U.S. healthcare costs, expand access, promote wellness and improve the consistency
Population Health Management Helps Utica Park Clinic Ease the Transition to Value-Based Care
 CASE STUDY Utica Park Clinic Population Health Management Helps Utica Park Clinic Ease the Transition to Value-Based Care The transition from fee-for-service to value-based reimbursement has been a challenge
CASE STUDY Utica Park Clinic Population Health Management Helps Utica Park Clinic Ease the Transition to Value-Based Care The transition from fee-for-service to value-based reimbursement has been a challenge
Care Coordination. The Embedded Care Manager. Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed
 Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
CMS Innovation Center Improving Care for Complex Patients
 CMS Innovation Center Improving Care for Complex Patients ECRI Institute Dr. Patrick Conway, M.D., MSc CMS Chief Medical Officer and Deputy Administrator for Innovation and Quality Director, Center for
CMS Innovation Center Improving Care for Complex Patients ECRI Institute Dr. Patrick Conway, M.D., MSc CMS Chief Medical Officer and Deputy Administrator for Innovation and Quality Director, Center for
Population Health Management for Critical Access Hospitals
 Population Health Management for Critical Access Hospitals John A. Gale, MS National Organization of State Offices of Rural Health Region E Grantee Meeting Rapid City, SD July 23, 2014 Overview Defining
Population Health Management for Critical Access Hospitals John A. Gale, MS National Organization of State Offices of Rural Health Region E Grantee Meeting Rapid City, SD July 23, 2014 Overview Defining
Ann Hablitzel, RN, BSN, MBA Hospice Care of California
 Ann Hablitzel, RN, BSN, MBA Hospice Care of California Objectives Describe the creations of new community based palliative care programs Identify criteria for admission Discuss philosophy and goals Analyze
Ann Hablitzel, RN, BSN, MBA Hospice Care of California Objectives Describe the creations of new community based palliative care programs Identify criteria for admission Discuss philosophy and goals Analyze
Subdomain Weight (%)
") CLINICAL NURSE LEADER (CNL ) CERTIFICATION EXAM BLUEPRINT SUBDOMAIN WEIGHTS (Effective June 2014) Subdomain Weight (%) Nursing Leadership Horizontal Leadership 7 Interdisciplinary Communication and Collaboration
CLINICAL NURSE LEADER (CNL ) CERTIFICATION EXAM BLUEPRINT SUBDOMAIN WEIGHTS (Effective June 2014) Subdomain Weight (%) Nursing Leadership Horizontal Leadership 7 Interdisciplinary Communication and Collaboration
Analytic-Driven Quality Keys Success in Risk-Based Contracts. Ross Gustafson, Vice President Allina Performance Resources, Health Catalyst
 Analytic-Driven Quality Keys Success in Risk-Based Contracts March 2 nd, 2016 Ross Gustafson, Vice President Allina Performance Resources, Health Catalyst Brian Rice, Vice President Network/ACO Integration,
Analytic-Driven Quality Keys Success in Risk-Based Contracts March 2 nd, 2016 Ross Gustafson, Vice President Allina Performance Resources, Health Catalyst Brian Rice, Vice President Network/ACO Integration,
Population Health Management: Banner Health Network s Perspective. Neta Faynboym, Medical Director Banner Health Network
 Population Health Management: Banner Health Network s Perspective Neta Faynboym, Medical Director Banner Health Network 29 Acute Care Hospitals BANNER AT A GLANCE Banner Health Network with 400K lives
Population Health Management: Banner Health Network s Perspective Neta Faynboym, Medical Director Banner Health Network 29 Acute Care Hospitals BANNER AT A GLANCE Banner Health Network with 400K lives
Guidelines for Patient-Centered Medical Home (PCMH) Recognition and Accreditation Programs. February 2011
 Recognition and Accreditation Programs. February 2011") American Academy of Family Physicians (AAFP) American Academy of Pediatrics (AAP) American College of Physicians (ACP) American Osteopathic Association (AOA) Guidelines for Patient-Centered Medical Home
American Academy of Family Physicians (AAFP) American Academy of Pediatrics (AAP) American College of Physicians (ACP) American Osteopathic Association (AOA) Guidelines for Patient-Centered Medical Home
Building a High Performance Integrated Population Health Infrastructure. Fulfilling Our New Medical Management Responsibilities
 Building a High Performance Integrated Population Health Infrastructure Fulfilling Our New Medical Management Responsibilities Presenters Betsy Hampton, RN, MBA Vice President, Population Health Reliant
Building a High Performance Integrated Population Health Infrastructure Fulfilling Our New Medical Management Responsibilities Presenters Betsy Hampton, RN, MBA Vice President, Population Health Reliant
POPULATION HEALTH MANAGEMENT The Lynchpin of Emerging Healthcare Delivery Improve Patient Outcomes, Engage Physicians, and Manage Risk
 POPULATION HEALTH MANAGEMENT The Lynchpin of Emerging Healthcare Delivery Improve Patient Outcomes, Engage Physicians, and Manage Risk Julia Andrieni, MD, FACP Vice President, Population Health and Primary
POPULATION HEALTH MANAGEMENT The Lynchpin of Emerging Healthcare Delivery Improve Patient Outcomes, Engage Physicians, and Manage Risk Julia Andrieni, MD, FACP Vice President, Population Health and Primary
I n t e r S y S t e m S W h I t e P a P e r F O R H E A L T H C A R E IT E X E C U T I V E S. In accountable care
 I n t e r S y S t e m S W h I t e P a P e r F O R H E A L T H C A R E IT E X E C U T I V E S The Role of healthcare InfoRmaTIcs In accountable care I n t e r S y S t e m S W h I t e P a P e r F OR H E
I n t e r S y S t e m S W h I t e P a P e r F O R H E A L T H C A R E IT E X E C U T I V E S The Role of healthcare InfoRmaTIcs In accountable care I n t e r S y S t e m S W h I t e P a P e r F OR H E
ST JOHN S LUTHERAN MINISTRIES. Kent Burgess President & CEO
 ST JOHN S LUTHERAN MINISTRIES Kent Burgess President & CEO WHAT S CHANGING MAYBE? -The way we get paid (Reduce Cost) -The way we get measured (Better Care) -What will be required of us (More) -Partnerships/Affiliations
ST JOHN S LUTHERAN MINISTRIES Kent Burgess President & CEO WHAT S CHANGING MAYBE? -The way we get paid (Reduce Cost) -The way we get measured (Better Care) -What will be required of us (More) -Partnerships/Affiliations
A white paper. Collaborative Accountable Care. CIGNA s Approach to Accountable Care Organizations. 841282 a 11/11
 A white paper Collaborative Accountable Care CIGNA s Approach to Accountable Care Organizations 841282 a 11/11 Transforming the Health Care System Successfully transforming the U.S. health care system
A white paper Collaborative Accountable Care CIGNA s Approach to Accountable Care Organizations 841282 a 11/11 Transforming the Health Care System Successfully transforming the U.S. health care system
Stakeholder s Report. 2525 SW 75 th Ave Miami, Florida 33155 305.262.6800 www.westgablesrehabhospital.com
 212 Stakeholder s Report 2525 SW 75 th Ave Miami, Florida 33155 35.262.68 www.westgablesrehabhospital.com PROFILE REPORT For more than 25 years, West Gables Rehabilitation Hospital has made a mission of
212 Stakeholder s Report 2525 SW 75 th Ave Miami, Florida 33155 35.262.68 www.westgablesrehabhospital.com PROFILE REPORT For more than 25 years, West Gables Rehabilitation Hospital has made a mission of
Coordinating Transitions of Care: It Takes a Village
 Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
Coordinating Transitions of Care: It Takes a Village Ken Laube RN, BSN, MBA: Vice President Clinical Excellence Situation/Background Patients face significant challenges when moving from one health care
Modern care management
 The care management challenge Health plans and care providers spend billions of dollars annually on care management with the expectation of better utilization management and cost control. That expectation
The care management challenge Health plans and care providers spend billions of dollars annually on care management with the expectation of better utilization management and cost control. That expectation
UCSF Clinical Enterprise Strategic Plan 2014-2019
 UCSF HEALTH SYSTEM UCSF Clinical Enterprise Strategic Plan 2014-2019 Building the Health System 1 UCSF Health System Five Year Strategic Plan: FY 2014-2019 Advancing the Health System A revolution is underway
UCSF HEALTH SYSTEM UCSF Clinical Enterprise Strategic Plan 2014-2019 Building the Health System 1 UCSF Health System Five Year Strategic Plan: FY 2014-2019 Advancing the Health System A revolution is underway
Stuart Levine MD MHA Corporate Medical Director, HealthCare Partners Assistant Clinical Professor, Internal Medicine and Psychiatry, UCLA David
 Stuart Levine MD MHA Corporate Medical Director, HealthCare Partners Assistant Clinical Professor, Internal Medicine and Psychiatry, UCLA David Geffen School of Medicine 1 HealthCare Partners Delivery
Stuart Levine MD MHA Corporate Medical Director, HealthCare Partners Assistant Clinical Professor, Internal Medicine and Psychiatry, UCLA David Geffen School of Medicine 1 HealthCare Partners Delivery
Designing the Role of the Embedded Care Manager
 Designing the Role of the Embedded By Patricia Hines, Ph.D., RN and Marge Mercury, RN, MS, CMCE The Embedded The use of an Embedded ( ECM ) to coordinate within the complex delivery system is sharply increasing.
Designing the Role of the Embedded By Patricia Hines, Ph.D., RN and Marge Mercury, RN, MS, CMCE The Embedded The use of an Embedded ( ECM ) to coordinate within the complex delivery system is sharply increasing.
The 2014 Patient- Centered Primary Care Home (PCPCH) Recognition Criteria
 Recognition Criteria") The 2014 Patient- Centered Primary Care Home (PCPCH) Recognition Criteria Deepti Shinde, MPP and E. Dawn Creach, MS Patient-Centered Primary Care Home Program Oregon Health Authority October 2, 2013 Welcome!
The 2014 Patient- Centered Primary Care Home (PCPCH) Recognition Criteria Deepti Shinde, MPP and E. Dawn Creach, MS Patient-Centered Primary Care Home Program Oregon Health Authority October 2, 2013 Welcome!
Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions
 Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions Scott Flinn MD Deborah Schutz RN JD Fritz Steen RN Arch Health Partners A medical foundation formed
Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions Scott Flinn MD Deborah Schutz RN JD Fritz Steen RN Arch Health Partners A medical foundation formed
2016 MEDICAL REHABILITATION PROGRAM DESCRIPTIONS
 2016 MEDICAL REHABILITATION PROGRAM DESCRIPTIONS Contents Comprehensive Integrated Inpatient Rehabilitation Program... 2 Outpatient Medical Rehabilitation Program... 2 Home and Community Services... 3
2016 MEDICAL REHABILITATION PROGRAM DESCRIPTIONS Contents Comprehensive Integrated Inpatient Rehabilitation Program... 2 Outpatient Medical Rehabilitation Program... 2 Home and Community Services... 3
DSRIP QUARTERLY REVIEW PROCESS: Project Requirement - Timeframe. Project Requirement - Unit Level Reporting
 DSRIP QUARTERLY REVIEW PROCESS: PPSs will submit a quarterly report to the Independent Assessor throughout the DSRIP program via the automated MAPP tool which includes Domain 1 DSRIP Requirement Milestone
DSRIP QUARTERLY REVIEW PROCESS: PPSs will submit a quarterly report to the Independent Assessor throughout the DSRIP program via the automated MAPP tool which includes Domain 1 DSRIP Requirement Milestone
ACOs: Six Things Specialty Practices Should Know
 ACOs: Six Things Specialty Practices Should Know =TOS Newsletter, July/August 2014= Authors: John P. Schmitt, Ph.D. and J. Garrett Schmitt, MBA, PCMH CCE INTRODUCTION Do you remember the analogy of four
ACOs: Six Things Specialty Practices Should Know =TOS Newsletter, July/August 2014= Authors: John P. Schmitt, Ph.D. and J. Garrett Schmitt, MBA, PCMH CCE INTRODUCTION Do you remember the analogy of four
Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education
 1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
Montefiore s Population Health Management Services. October 23, 2015
 Montefiore s Population Health Management Services October 23, 2015 Integrated Delivery System Our Locations 3,092 Acute Beds Across 10 Hospitals Including 132 beds at the Children s Hospital at Montefiore
Montefiore s Population Health Management Services October 23, 2015 Integrated Delivery System Our Locations 3,092 Acute Beds Across 10 Hospitals Including 132 beds at the Children s Hospital at Montefiore
Call-A-Nurse Location
 Call-A-Nurse A 24-hour medical call center, specializing in registered nurse telephone triage, answering service, physician and service referral, and class registration. Call-A-Nurse Location Call-A-Nurse
Call-A-Nurse A 24-hour medical call center, specializing in registered nurse telephone triage, answering service, physician and service referral, and class registration. Call-A-Nurse Location Call-A-Nurse
6/12/2015. Dignity Health Population Health Management and Compliance Programs. Moving Towards Accountable Care. Dignity Health Poised for Innovation
 Dignity Health Population Health Management and Compliance Programs Julie Bietsch, VP Population Health Management Dawnese Kindelt, Senior Compliance Director, Clinical Integration June 8, 2015 Moving
Dignity Health Population Health Management and Compliance Programs Julie Bietsch, VP Population Health Management Dawnese Kindelt, Senior Compliance Director, Clinical Integration June 8, 2015 Moving
Game Changer at the Primary Care Practice Embedded Care Management. Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012
 Game Changer at the Primary Care Practice Embedded Care Management Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012 Objectives To describe the recent evolution of care management at
Game Changer at the Primary Care Practice Embedded Care Management Ruth Clark, RN, BSN, MPA Integrated Health Partners October 30, 2012 Objectives To describe the recent evolution of care management at
Second Forum on Health Care Management & Policy November 28 30, 2012. Discussion Report. Care Management
 Second Forum on Health Care Management & Policy November 28 30, 2012 Discussion Report Care Management Thomas G. Rundall Henry J. Kaiser Emeritus Professor of Organized Health Systems School of Public
Second Forum on Health Care Management & Policy November 28 30, 2012 Discussion Report Care Management Thomas G. Rundall Henry J. Kaiser Emeritus Professor of Organized Health Systems School of Public
The New Complex Patient. of Diabetes Clinical Programming
 The New Complex Patient as Seen Through the Lens of Diabetes Clinical Programming 1 Valerie Garrett, M.D. Medical Director, Diabetes Center at Mission Health System Nov 6, 2014 Diabetes Health Burden High
The New Complex Patient as Seen Through the Lens of Diabetes Clinical Programming 1 Valerie Garrett, M.D. Medical Director, Diabetes Center at Mission Health System Nov 6, 2014 Diabetes Health Burden High
2015 ASHP STRATEGIC PLAN
 2015 ASHP STRATEGIC PLAN ASHP Vision ASHP s vision is that medication use will be optimal, safe, and effective for all people all of the time. ASHP Mission The mission of pharmacists is to help people
2015 ASHP STRATEGIC PLAN ASHP Vision ASHP s vision is that medication use will be optimal, safe, and effective for all people all of the time. ASHP Mission The mission of pharmacists is to help people
Be Careful What You Ask For A Predictive Model That Really Works
 Be Careful What You Ask For A Predictive Model That Really Works Rod Christensen, MD President, Allina Health Clinics Cheryl Hermann, RN, MBA Vice President, Clinic Operations & Patient Care Services Karen
Be Careful What You Ask For A Predictive Model That Really Works Rod Christensen, MD President, Allina Health Clinics Cheryl Hermann, RN, MBA Vice President, Clinic Operations & Patient Care Services Karen
HEDIS 2012 Results
 Capital District Physicians Health Plan, Inc. Nonprofit Health Plan Albany, New York Capital District Physicians Health Plan, Inc. (CDPHP ) is featured as a high performer in cardiovascular care, identified
Capital District Physicians Health Plan, Inc. Nonprofit Health Plan Albany, New York Capital District Physicians Health Plan, Inc. (CDPHP ) is featured as a high performer in cardiovascular care, identified
Day 1 Follow-Up: Panelist Suggestions and Final Topic Ranking. IHS Advisory Panel Meeting April 20, 2013 (Day 2) Chad Boult, MD, MPH, MBA Director
 Chad Boult, MD, MPH, MBA Director") Day 1 Follow-Up: Panelist Suggestions and Final Topic Ranking IHS Advisory Panel Meeting April 20, 2013 (Day 2) Chad Boult, MD, MPH, MBA Director 1 Suggestions From Panelists 2 Use One Care Management
Day 1 Follow-Up: Panelist Suggestions and Final Topic Ranking IHS Advisory Panel Meeting April 20, 2013 (Day 2) Chad Boult, MD, MPH, MBA Director 1 Suggestions From Panelists 2 Use One Care Management
Breathe With Ease. Asthma Disease Management Program
 Breathe With Ease Asthma Disease Management Program MOLINA Breathe With Ease Pediatric and Adult Asthma Disease Management Program Background According to the National Asthma Education and Prevention Program
Breathe With Ease Asthma Disease Management Program MOLINA Breathe With Ease Pediatric and Adult Asthma Disease Management Program Background According to the National Asthma Education and Prevention Program
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
1900 K St. NW Washington, DC 20006 c/o McKenna Long
 1900 K St. NW Washington, DC 20006 c/o McKenna Long Centers for Medicare & Medicaid Services U. S. Department of Health and Human Services Attention CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re:
1900 K St. NW Washington, DC 20006 c/o McKenna Long Centers for Medicare & Medicaid Services U. S. Department of Health and Human Services Attention CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re:
Better Health. Better Care Better Teams Better Value
 SUNRISE HEALTH REGION STRATEGIC PLAN Better Health Better Care Better Teams Better Value FIVE-YEAR PLAN 2012-2017 Date: May 30, 2012 Page 2 of 15 SUNRISE HEALTH REGION Message from the Board Chair and
SUNRISE HEALTH REGION STRATEGIC PLAN Better Health Better Care Better Teams Better Value FIVE-YEAR PLAN 2012-2017 Date: May 30, 2012 Page 2 of 15 SUNRISE HEALTH REGION Message from the Board Chair and
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment
 Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
Kaiser Permanente of Ohio
 Kaiser Permanente of Ohio Chronic Disease Management Program March 11, 2011 Presenters: Amy Kramer and Audrey L. Callahan 1 Objectives 1. Define the roles and responsibilities of the Care Managers in the
Kaiser Permanente of Ohio Chronic Disease Management Program March 11, 2011 Presenters: Amy Kramer and Audrey L. Callahan 1 Objectives 1. Define the roles and responsibilities of the Care Managers in the
Analytics Tools for Population Health Management. Arumani Manisundaram Director - Center for Connected Health Adventist HealthCare
 Analytics Tools for Population Health Management Arumani Manisundaram Director - Center for Connected Health Adventist HealthCare About Our Organization(s) Adventist HealthCare Five acute-care and specialty
Analytics Tools for Population Health Management Arumani Manisundaram Director - Center for Connected Health Adventist HealthCare About Our Organization(s) Adventist HealthCare Five acute-care and specialty
How To Analyze Health Data
 POPULATION HEALTH ANALYTICS ANALYTICALLY-DRIVEN INSIGHTS FOR POPULATION HEALTH LAURIE ROSE, PRINCIPAL CONSULTANT HEALTH CARE GLOBAL PRACTICE DISCUSSION TOPICS Population Health: What & Why Now? Population
POPULATION HEALTH ANALYTICS ANALYTICALLY-DRIVEN INSIGHTS FOR POPULATION HEALTH LAURIE ROSE, PRINCIPAL CONSULTANT HEALTH CARE GLOBAL PRACTICE DISCUSSION TOPICS Population Health: What & Why Now? Population
Who are Parent Navigators?
 Parent Navigators: A New Care Team Member in Your Medical Home or Specialty Practice Faculty Disclosure: We have no financial relationships to disclose relating to the subject matter of this presentation.
Parent Navigators: A New Care Team Member in Your Medical Home or Specialty Practice Faculty Disclosure: We have no financial relationships to disclose relating to the subject matter of this presentation.
Oregon Standards for Certified Community Behavioral Health Clinics (CCBHCs)
") Oregon Standards for Certified Community Behavioral Health Clinics (CCBHCs) Senate Bill 832 directed the Oregon Health Authority (OHA) to develop standards for achieving integration of behavioral health
Oregon Standards for Certified Community Behavioral Health Clinics (CCBHCs) Senate Bill 832 directed the Oregon Health Authority (OHA) to develop standards for achieving integration of behavioral health
St. Luke s Hospital and Health Network Philosophy of Nursing:
 St. Luke s Hospital and Health Network Philosophy of Nursing: Nursing, a healing profession, is an essential component of St. Luke's Hospital & Health Network's commitment to providing safe, compassionate,
St. Luke s Hospital and Health Network Philosophy of Nursing: Nursing, a healing profession, is an essential component of St. Luke's Hospital & Health Network's commitment to providing safe, compassionate,
Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Summit Health Plan of Florida
 Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Summit Health Plan of Florida Medicare Quality Management Program Overview Quality Improvement (QI) Overview At Coventry, we
Coventry Health Care of Florida, Inc. Coventry Health Plan of Florida, Inc. Summit Health Plan of Florida Medicare Quality Management Program Overview Quality Improvement (QI) Overview At Coventry, we
Nursing Strategic Plan. Fiscal Year 2015. Shaping the Future of UCLA Nursing at Ronald Reagan UCLA Medical Center
 Nursing Strategic Plan Fiscal Year 2015 Shaping the Future of UCLA Nursing at Ronald Reagan UCLA Medical Center The strategic plan of the Ronald Reagan UCLA Medical Center Department of Nursing aligns
Nursing Strategic Plan Fiscal Year 2015 Shaping the Future of UCLA Nursing at Ronald Reagan UCLA Medical Center The strategic plan of the Ronald Reagan UCLA Medical Center Department of Nursing aligns
Population Health Management: Advancing Your Position in the Journey to Value-Based Care
 Population Health Management: Advancing Your Position in the Journey to Value-Based Care Webcast Session One: An Integrated Approach to Population Health Management 11 August 2015 Welcome & Introductions
Population Health Management: Advancing Your Position in the Journey to Value-Based Care Webcast Session One: An Integrated Approach to Population Health Management 11 August 2015 Welcome & Introductions
Dual RFI Response Summary
 Dual RFI Response Summary Improving Care through Integrated Medicare and Medi- Cal Delivery Models Stuart Levine, MD., MHA. Keith Wilson, MD Robert Margolis, MD. Stakeholder Meeting August 30, 2011 1 Organization
Dual RFI Response Summary Improving Care through Integrated Medicare and Medi- Cal Delivery Models Stuart Levine, MD., MHA. Keith Wilson, MD Robert Margolis, MD. Stakeholder Meeting August 30, 2011 1 Organization
Pushing the Envelope of Population Health
 Pushing the Envelope of Population Health Timothy Ferris, MD, MPH Senior Vice President, Population Health Management, Partners HealthCare May 15, 2014 DISCLAIMER: The views and opinions expressed in this
Pushing the Envelope of Population Health Timothy Ferris, MD, MPH Senior Vice President, Population Health Management, Partners HealthCare May 15, 2014 DISCLAIMER: The views and opinions expressed in this
Care Coordination at Frederick Regional Health System. Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care
 Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Care Coordination at Frederick Regional Health System Heather Kirby, MBA, LBSW, ACM Assistant Vice President of Integrated Care 1 About the Health System 258 Licensed acute beds Approximately 70,000 ED
Kick off Meeting November 11 13, 2015. MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF)
") Kick off Meeting November 11 13, 2015 MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF) Team Composition Justin Huynh, MD Internal Medicine, Physician Champion Mary Laubinger,
Kick off Meeting November 11 13, 2015 MERCY CLINIC EAST COMMUNITIES Management of Patients with Heart Failure (HF) Team Composition Justin Huynh, MD Internal Medicine, Physician Champion Mary Laubinger,
Accountable Care Platform
 The shift toward increased collaboration, outcome-based payment and new benefit design is transforming how we pay for health care and how health care is delivered. UnitedHealthcare is taking an industry
The shift toward increased collaboration, outcome-based payment and new benefit design is transforming how we pay for health care and how health care is delivered. UnitedHealthcare is taking an industry
#Aim2Innovate. Share session insights and questions socially. UCLA Primary Care Innovation Model 6/13/2015. Mark S. Grossman, MD, MBA, FAAP, FACP
 UCLA Primary Care Innovation Model Mark S. Grossman, MD, MBA, FAAP, FACP Chief Medical Office, UCLA Community Physicians & Specialty Care Networks June 16, 2015 DISCLAIMER: The views and opinions expressed
UCLA Primary Care Innovation Model Mark S. Grossman, MD, MBA, FAAP, FACP Chief Medical Office, UCLA Community Physicians & Specialty Care Networks June 16, 2015 DISCLAIMER: The views and opinions expressed
Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination of care for both services.
 Domain 3 Projects 3.a.i Integration of Primary Care and Behavioral Health Services Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination
Domain 3 Projects 3.a.i Integration of Primary Care and Behavioral Health Services Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination
NCQA Patient-Centered Medical Home. Improving experiences for patients, providers and practice staff
 NCQA Patient-Centered Medical Home Improving experiences for patients, providers and practice staff PCMH Recognition The patient-centered medical home is a model of care that emphasizes care coordination
NCQA Patient-Centered Medical Home Improving experiences for patients, providers and practice staff PCMH Recognition The patient-centered medical home is a model of care that emphasizes care coordination
H7833_150304MO01. Information for Care Providers about UnitedHealthcare Connected (Medicare- Medicaid Plan) in Harris County, Texas
 in Harris County, Texas") H7833_150304MO01 Information for Care Providers about UnitedHealthcare Connected (Medicare- Medicaid Plan) in Harris County, Texas Agenda Connecting Medicare and Medicaid Eligible Members Service Coordination
H7833_150304MO01 Information for Care Providers about UnitedHealthcare Connected (Medicare- Medicaid Plan) in Harris County, Texas Agenda Connecting Medicare and Medicaid Eligible Members Service Coordination
Job Descriptions. All jobs with Heart to Heart Hospice require reliable transportation as well as valid and current auto liability insurance.
 Job Descriptions All jobs with Heart to Heart Hospice require reliable transportation as well as valid and current auto liability insurance. Administrator Primary function is to assume overall responsibility
Job Descriptions All jobs with Heart to Heart Hospice require reliable transportation as well as valid and current auto liability insurance. Administrator Primary function is to assume overall responsibility
POSITION DESCRIPTION. As agreed
 POSITION DESCRIPTION POSITION TITLE REPORTS TO AWARD/AGREEMENT/CONTRACT POSITION TYPE e.g. Registered Nurse Div 1, Occupational Therapist Gr1, etc. HOURS PER WEEK Psychosocial Care Coordinator Spinal Community
POSITION DESCRIPTION POSITION TITLE REPORTS TO AWARD/AGREEMENT/CONTRACT POSITION TYPE e.g. Registered Nurse Div 1, Occupational Therapist Gr1, etc. HOURS PER WEEK Psychosocial Care Coordinator Spinal Community
Accountable Care and Value Based Payments 101: Government Programs Update
 1 Accountable Care and Value Based Payments 101: Government Programs Update June 24 th, 2014 Dave Neiman, FSA, MAAA Senior Consulting Actuary [email protected] (720) 226-9806 2 Caveats Opinions expressed
1 Accountable Care and Value Based Payments 101: Government Programs Update June 24 th, 2014 Dave Neiman, FSA, MAAA Senior Consulting Actuary [email protected] (720) 226-9806 2 Caveats Opinions expressed
Transforming traditional case management through local provider partnerships
 Transforming traditional case management through local provider partnerships Introduction The dramatic changes sweeping the health care industry are driving a strong interest in engaging patients at the
Transforming traditional case management through local provider partnerships Introduction The dramatic changes sweeping the health care industry are driving a strong interest in engaging patients at the
The ABCs of Population Health Management Jennifer Houlihan, MSP Director of CIN Strategy, Integration and Population Health
 The ABCs of Population Health Management Jennifer Houlihan, MSP Director of CIN Strategy, Integration and Population Health A view from the marketplace Employers seek Other health Systems for Clinically
The ABCs of Population Health Management Jennifer Houlihan, MSP Director of CIN Strategy, Integration and Population Health A view from the marketplace Employers seek Other health Systems for Clinically
Chapter 2 Essential Skills for Case Managers
 Chapter 2 Essential Skills for Case Managers 2.1 Essential Skill Overview If you ask ten people what case management means to them, you will most likely get ten different answers. Though case management
Chapter 2 Essential Skills for Case Managers 2.1 Essential Skill Overview If you ask ten people what case management means to them, you will most likely get ten different answers. Though case management
CHAPTER 535 HEALTH HOMES. Background... 2. Policy... 2. 535.1 Member Eligibility and Enrollment... 2. 535.2 Health Home Required Functions...
 TABLE OF CONTENTS SECTION PAGE NUMBER Background... 2 Policy... 2 535.1 Member Eligibility and Enrollment... 2 535.2 Health Home Required Functions... 3 535.3 Health Home Coordination Role... 4 535.4 Health
TABLE OF CONTENTS SECTION PAGE NUMBER Background... 2 Policy... 2 535.1 Member Eligibility and Enrollment... 2 535.2 Health Home Required Functions... 3 535.3 Health Home Coordination Role... 4 535.4 Health
Response to Serving the Medi Cal SPD Population in Alameda County
 Expanding Health Coverage and Increasing Access to High Quality Care Response to Serving the Medi Cal SPD Population in Alameda County As the State has acknowledged in the 1115 waiver concept paper, the
Expanding Health Coverage and Increasing Access to High Quality Care Response to Serving the Medi Cal SPD Population in Alameda County As the State has acknowledged in the 1115 waiver concept paper, the
Queens-Long Island Medical Center Improves Quality and Physician Satisfaction with EHR Backbone and Patient Centered Medical Home Initiative
 Queens-Long Island Medical Center Improves Quality and Physician Satisfaction with EHR Backbone and Patient Centered Medical Home Initiative Background: Primary medical care in America is in crisis, with
Queens-Long Island Medical Center Improves Quality and Physician Satisfaction with EHR Backbone and Patient Centered Medical Home Initiative Background: Primary medical care in America is in crisis, with
Profile: Incorporating Routine Behavioral Health Screenings Into the Patient-Centered Medical Home
 104 A LOOK TO THE FUTURE Profile: Incorporating Routine Behavioral Health Screenings Into the Patient-Centered Medical Home Background Management of chronic diseases can be challenging in primary care,
104 A LOOK TO THE FUTURE Profile: Incorporating Routine Behavioral Health Screenings Into the Patient-Centered Medical Home Background Management of chronic diseases can be challenging in primary care,
Accountable Care Organizations: What Are They and Why Should I Care?
 Accountable Care Organizations: What Are They and Why Should I Care? Adrienne Green, MD Associate Chief Medical Officer, UCSF Medical Center Ami Parekh, MD, JD Med. Director, Health System Innovation,
Accountable Care Organizations: What Are They and Why Should I Care? Adrienne Green, MD Associate Chief Medical Officer, UCSF Medical Center Ami Parekh, MD, JD Med. Director, Health System Innovation,
Philips Hospital to Home: redefining healthcare. through innovation in telehealth
 Philips Hospital to Home: redefining healthcare through innovation in telehealth Healthcare costs are at a crisis point, forcing the federal government to make comprehensive changes to healthcare payment
Philips Hospital to Home: redefining healthcare through innovation in telehealth Healthcare costs are at a crisis point, forcing the federal government to make comprehensive changes to healthcare payment