Locking the Revolving Door of Readmissions
|
|
|
- Solomon Beasley
- 10 years ago
- Views:
Transcription
1 Locking the Revolving Door of Readmissions The Pharmacist s Role in Keeping Patients Healthy, Happy and At Home Steve Riddle, BS Pharm, BCPS, FASHP VP of Clinical Affairs, Pharmacy OneSource

2 Objectives Provide background information on the current state of hospital readmissions in the U.S. Describe common causes for readmissions and the patient risk factors associated with these events. Discuss the potential consequences of readmissions on performance measurement and financial reimbursement for health-systems Describe various solutions and successful programs that have reduced hospital readmissions Discuss specific approaches involving pharmacist-supported care processes that have impacted readmissions

3 Action Steps to Reduce Readmissions 1. Examine your hospital s current rate of readmissions Understanding readmissions data Trends in readmissions Important reimbursement/regulatory issues 2. Assess and prioritize your improvement opportunities 3. Develop an action plan of strategies to implement 4. Monitor your progress

4 Readmissions are Frequent 18% of all Medicare hospitalizations are 30-day re-hospitalizations Average rates are >20% for certain patient populations Potentially avoidable 76% of Medicare re-hospitalizations were potentially preventable Costly $15B annually in Medicare of which $13B may be unnecessary Actionable for improvement Research and quality improvement initiatives have demonstrated >30% reduction of 30-day readmission rates for a variety of populations MedPAC 2007 Report to Congress; Promoting Greater Efficiency in Medicare


5 Readmission Rates for Medicare Beneficiaries, 2005 Based on data from Jencks et al. N Engl J Med 2009;360:

6 Not All Readmissions Are Preventable What is an avoidable or preventable readmission? Excludes planned admissions Excludes admissions for unrelated causes How does the index admission diagnosis (DRG) relate to the readmission DRG?


7 Readmission Evaluations MedPac 2007 Report to Congress: Promoting Greater Efficiency in Medicare

8 CMS has chosen 30 days for their measurement period What is the time frame examining readmissions? 7, 14, 30 days? 3, 6, 12 months?


9 State Readmission Rates (30 days) The rates include all patients in fee-for-service Medicare programs who were discharged between October 1, 2003, and September 30, 2004 Jencks et al. N Engl J Med 2009;360:


10 Timing of Readmissions Impact of length of stay? Source: UHC Clinical Data Base FFY2008 (10/07 9/08)

11 Hospital Readmissions for 7 Conditions 7 Conditions account for 30% of 15- day readmissions and costs MedPac 2007 Report to Congress: Promoting Greater Efficiency in Medicare. 3M analysis of Medicare 2005 discharge claims

12 What are your hospital s rates for readmissions? Internal data? External Sources 3 rd parties and payers Consider: Rates based on conditions Rates per practitioners Rates by readmission source (home, SNF, NH) Rates per time intervals (7, 15, 30 and 90 days) Remember that your internal data will not capture readmissions to other hospitals!
 Rates per time intervals (7, 15, 30 and 90")

13 Hospital Compare: Readmission Data Source

14
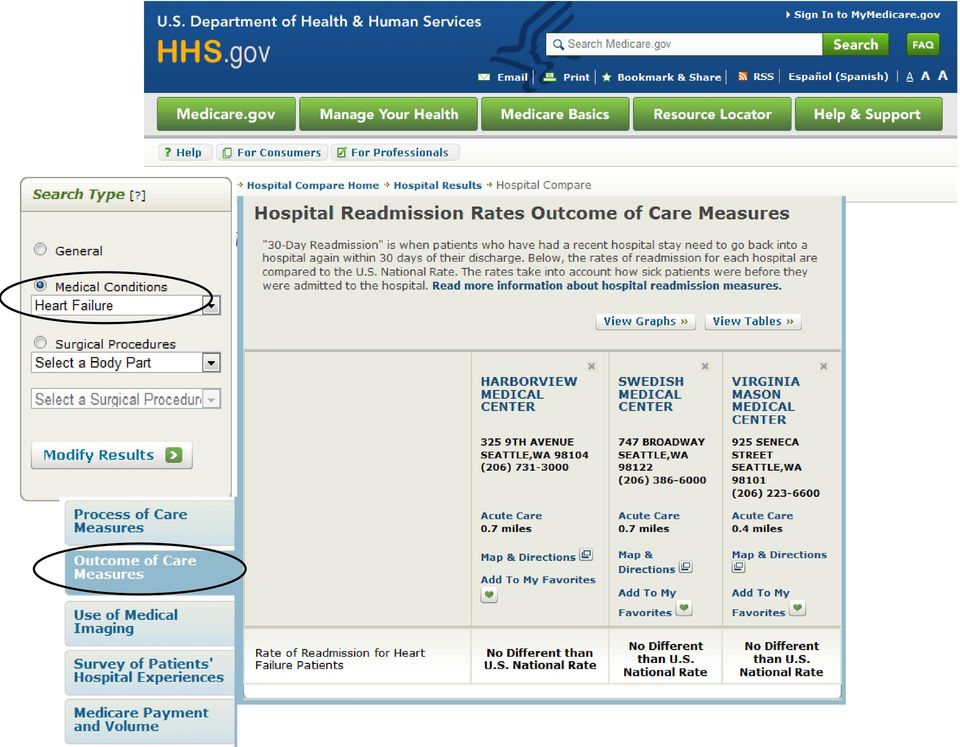

15 Hospital Compares Readmission Data

16 If rehospitalizations are frequent, costly, and able to be reduced, why haven t they been? Hospital-level barriers Financial disincentives (volume-revenue), no financial incentives, not part of P4P contracts, not high on priority list, limited disease-specific efforts Current payment scheme pays for hospitalizations, but not for coordinating care across settings. Community-level barriers Not common to engage organizations across continuum to collaborate on improving care, lack of IT connectivity, no reimbursement for coordination State-level barriers Lack of population-based data, lack of understanding costs of poor quality on systems, effect of fragmented payer market and lack of CMS participation

17 Healthcare Reform Value-based purchasing Public reporting

18 The Patient Protection and Affordable Care Act (H.R. 3590) Value-Based Purchasing (VBP) AMI, PNE, HF SCIP/HOP Core Measures (Section 3001) CLABSI SSI Healthcare-Associated Infections (HAI) (Section 3001) At Risk: 1% in FY2013 growing annually to 2% in FY2017 (70% Core Measures + HAI and 30% HCAHPS) Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) (Section 3001) Medicare Reimbursement 5 CAUTI, Vascular Catheter Associated Infections, Poor Glycemic Control Hospital Acquired Conditions (HAC) (Section 3008) At Risk: 1% reduction beginning FY2015 Foreign Object Postop, Air Embolism, Blood Incompatibility, Pressure Ulcer, Falls/Trauma At Risk: 1% reduction in FY2013 and will Rise to 3% by FY2015 Readmission Rates (Section 3025) COPD, CABG, PTCA, etc. AMI, PNE, HF
 (Section 3008) At Risk: 1% reduction beginning FY2015 Foreign Object Postop, Air Embolism, Blood Incompatibility,")
19 CMS Plan Hospital Readmissions Payment Policy Effective Oct. 1, 2012 Reduces Medicare inpatient payments for hospitals with higher than expected risk-adjusted readmission rates for certain conditions. Reduced Medicare payments for every discharge.

20 Targeted MS-DRGs and Timelines Year 1: FY2012 Heart failure Myocardial infarction Pneumonia Year 3: FY2014 COPD CABG PTCA & other vascular procedures Year 4: FY2015 Expand to other conditions (TBD)


21 VBP Model HR 3590 Sect 3008 EXAMPLE $$$ at Risk: 1% or $621,311 2% or $1.25 million 3% or $ 1.9 million 9
22 Other Payment and Process Drivers Public reporting Hospital Compare State reporting Impacting Readmissions Bundled payments for Episodes of Care Single inpatient payment replaced with payment that includes costs for services 30-days postdischarge HCAHPS Hospital Consumer Assessment of Healthcare Providers & Systems (Patient Satisfaction Survey) Now 30% of CMS value-based purchasing score Gainsharing Allows participating providers to share in cost savings realized from adopting new care delivery models while maintaining or improving quality Examples: Accountable Care Organizations (ACO), Patient-centered Medical Homes (PCMH)
23
24 Action Steps to Reduce Readmissions 1. Examine your hospital s current rate of readmissions 2. Assess and prioritize your improvement opportunities Which patients should you be targeting? 3. Develop an action plan of strategies to implement 4. Monitor your progress
25 Evaluating Patient Risks: Where should your efforts be targeted? Conditions? HF, COPD, surgical procedures Patient populations? Demographics: age, payer (dual eligible), race Combined risk analyses? Consider modifiable vs. non-modifiable factors
26 Top US Hospital 30-day Readmission Rates by Condition Medical Conditions 30-day Readmission Rate % of all Readmissions Heart Failure 26.9% 7.6% Pneumonia 20.1% 6.3% COPD 22.6% 4.0% Psychoses 24.6% 3.5% GI related problems 19.2% 3.1% Surgical Conditions 30-day Readmission Rate % of all Readmissions Cardiac Stent 14.5% 1.6% Major Hip or Knee Surgery 9.9% 1.5% Vascular Surgery 23.9% 1.4% Major Bowel Surgery 16.6% 1.0% Other Hip/Femur Surgery 17.9% 0.9% Jencks et al. Rehospitalizations among Patients in the Medicare Fee-for-Service Program N Engl J Med 2009;360:
27 Predictors of Rehospitalization within 30 Days after Discharge.* *Data are for patients in Medicare fee-for-service programs who were discharged from the hospital between April 1, 2004, and September 30, 2004, and were followed until October 31, Data were analyzed with the use of the Cox proportional-hazards model. P<0.001 for all variables except an age of 65 to 69 years N Engl J Med 2009;360:
28 Factors in Readmissions: Prospective Study 142 inpatients 50 years with a previous hospitalization in 6 months (Australia) Examined biological, functional and psychosocial variables. Overall readmission rate = 38.7% Bivariate Analysis of Potential Predictors of Unplanned Readmission with 6 Months (n = 142) Variable # (%) % Readmitted P value BMI 0.02 BMI underweight 11 (8) 72% BMI - obese 32 (23) 50% Chronic disease 27 (19) 67% Depressive Symptoms (GDS 5) Mudge et al. Hospital Medicine 2011;6: (51) 47% 0.04
29 We believe that the focus of the clinical intervention on the combined effects of primary health problems, comorbid conditions, and other health and social issues common in this patient population, rather than on the management of a single disease, was a major factor in its success. Mary Naylor, RN, PhD From Comprehensive Discharge Planning and Home Follow-up of Hospitalized Elders JAMA. 1999;281:

30 A Risk Evaluation Tool: Project Boost
31 Action Steps to Reduce Readmissions 1. Examine your hospital s current rate of readmissions 2. Assess and prioritize your improvement opportunities 3. Develop an action plan of strategies to implement High level strategies and resources Pharmacy-specific interventions and evidence 4. Monitor your progress
32 High-Level Strategies for Readmissions and Improving Continuity of Care
33 IHI STAAR Initiative: STate Action on Avoidable Rehospitalizations IHI completed groundwork with key groups to determine issues related to readmissions 4-year, multi-state initiative (started in 2009) to measurably reduce avoidable rehospitalizations Provision of tool kits, regular meetings, community of participants and expert advisors. Reduce rehospitalizations by working across organizational boundaries and engaging payers, state and national stakeholders, patients and families, and caregivers at multiple care sites and clinical interfaces.
34 IHI STAAR Initiative and Ideal Transition from Hospital to Home I. Perform Enhanced Admission Assessment for Post-Hospital Needs Include family caregivers and community providers as full partners in completing standardized assessments, planning discharge, and predicting home-going needs. Reconcile medications upon admission. Initiate a standard plan of care based on the results of the assessment. II. Provide Effective Teaching and Enhanced Learning Identify all learners on admission. Customize the patient education process for patients, family caregivers Use Teach Back daily in the hospital and during follow-up phone calls III. Conduct Real-Time Patient & Family-Centered Communication Reconcile medications at discharge. Provide customized, real-time critical information to the next care provider(s). IV. Ensure Post-Hospital Care Follow-Up Risk stratify patients and ensure appropriate follow-up (in-person, telephone) as indicated within 5-7 days.
35 The Care Transitions Program: Four Pillars Medication self-management: Patient is knowledgeable about medications and has a medication management system. Use of a dynamic patient-centered record: Patient understands and utilizes the Personal Health Record (PHR) to facilitate communication and ensure continuity of care plan across providers and settings. The patient or informal caregiver manages the PHR. Primary Care and Specialist Follow-Up: Patient schedules and completes follow-up visit with the primary care physician or specialist physician and is empowered to be an active participant in these interactions. Knowledge of Red Flags: Patient is knowledgeable about indications that their condition is worsening and how to respond

36 HRET/AHA Guide to Reduce Avoidable Readmissions Health Research & Educational Trust (HRET), an affiliate of the American Hospital Association (AHA)
37 Examining the Role of the Pharmacist in Preventing Readmissions
38 Opportunities for Pharmacy: Readmissions Preventing Interventions Phase of Care Admission Inpatient Stay Discharge Home Service Perform Admission Assessment Determine factors in admission/readmission Medication history Medication reconciliation Errors of omission (EBM) Adverse drug events (ADE) Medication adherence Medication access Determine post-hospital needs Where will patient likely receive care? Who are caregivers? Barriers to care? Care Optimization Provide effective teaching & enhanced learning Identify barriers to learning Medication management Disease self-management Medication adherence Use Teach Back method Provide tools Optimize the medication regimen Initiate indicated medications Discontinue unnecessary or unsafe medications Simplify the medication regimen Prepare for Transition in Care Medication regimen review Medication reconciliation Provide medication list and related information to: o Patient/caregiver o Physician/medical team o Pharmacy/pharmacist Verify appropriate post-discharge care plan Match discharge follow-up to need (readmission risk stratification) Ensure proper information is provided regarding contact information, action plan for care and symptom or AE management Provide Appropriate Post- Discharge Care Contact patient/caregiver Live or virtual visit Patient status and medication review Medication reconciliation Medication adherence ADE surveillance Medication access Med management/ Disease management Communicate to other providers any pertinent medical information or findings
39 Discharge Process TARGET INTERVENTION KEY PLAYERS Care plan, medication management Reengineered Discharge Process (RED) Pharmacist, RN discharge advocate (DA) Trial Population: 749 hospitalized adults at urban teaching hospital Description of Intervention: Inpatient via nurse discharge advocate (DA) Educate patient on diagnosis and condition management Make and coordinate post-dsch appointments and testing Discuss lab or study results and needed follow-up Confirm medication plan (reconcile, educate, access) Align care plan with protocols, policies and EBM Transmit discharge summary to stakeholders Assess patient understanding of care plan (using teach back) Post-Discharge Care Plan (via DA) Provide patient written after-hospital care plan ( AHCP ) Post-Discharge Telephone Component (via pharmacist) Call patients 2 to 4 days after discharge to reinforce the discharge plan, review medications and solve problems Citation: A Reengineered Hospital Discharge Program to Decrease Rehospitalization. Ann Intern Med. 2009;150:
40 Discharge Process TARGET INTERVENTION KEY PLAYERS ED use and rehospitalization Reengineered Discharge Process (RED) Pharmacist, RN discharge advocate (DA) Results: Participants in the intervention group (n 370) had a lower rate of hospital utilization than those receiving usual care (n = 368) (0.314 vs visit per person per month; incidence rate ratio, [95% CI, to 0.937]; P 0.009). Cumulative hazard rate of hospital utilization for 30 days after index hospital discharge Cost savings of $149,995 or $412 per person 33.9% lower observed cost compared to standard care group Citation: A Reengineered Hospital Discharge Program to Decrease Rehospitalization. Ann Intern Med. 2009;150:
41 Discharge Process TARGET INTERVENTION KEY PLAYERS ED use and rehospitalization Reengineered Discharge Process (RED) Pharmacist, RN discharge advocate (DA) Comments on Pharmacy Interventions: Successfully contacted 228 (62%) of the intervention participants a median of 4 days after discharge (IQR, 3 to 6 days) Completed medication review with 195 (53%) participants. 126 of 195 (65%) intervention participants at least 1 medication problem and 103 (53%) needed corrective action such as contacting the PCP. It took a median of 2 attempts (IQR, 1 to 3 attempts) to reach participants by telephone. Median total pharmacist time was approximately 26 minutes (IQR, 18 to 36 minutes) per participant. Estimated weekly pharmacist time (following 14 participants per week) was 6.1 hours or approximately 0.15 full-time equivalent. Citation: A Reengineered Hospital Discharge Program to Decrease Rehospitalization. Ann Intern Med. 2009;150:
42 Discharge Process TARGET INTERVENTION KEY PLAYERS Improved pharmaceutical care Medication discharge summary, pharmacist home visit, info transfer Pharmacists Trial Population: 43 elderly patients prescribed more than 4 medications discharged to home from hospital (UK) compared to normal discharge process (control) group. Description of Intervention: Patients received discharge tools, medication and information discharge summary (MIDS) and medicine reminder card. Each patient s GP was sent a copy of MIDS on discharge. Pre-discharge a pharmacist counseled study patients about their medicines and compliance. A research pharmacist visited patients in their home approximately 2 3 weeks and at 3 months post-discharge to determine their drug knowledge, compliance, home medicine stocks and any healthcare related events. Citation: Al-Rashed et al. The value of inpatient pharmaceutical counseling to elderly patients prior to discharge. Br J Clin Pharmacol. 2002;54:
43 Discharge Process TARGET INTERVENTION KEY PLAYERS Improved pharmaceutical care Medication discharge summary, pharmacist home visit Pharmacists Results: Outcome Study (V1) Control (V1) Study (V2) Control (V2) Med Adherence 48.4** ** 15.8 GP visits 19* 27 24* 32 Readmissions 5* 19 3* 15 * p < 0.05, ** p< 0.001, Comments: Inpatient counseling = 30 min contact time 1 st Home Visit = 30 min (+ travel) Citation: Al-Rashed et al. The value of inpatient pharmaceutical counseling to elderly patients prior to discharge. Br J Clin Pharmacol. 2002;54:
44 Discharge Process TARGET INTERVENTION KEY PLAYERS Patient satisfaction, Decreased resource utilization Post-discharge telephone follow-up Pharmacists Trail Design: 110 patients recently discharged home from large academic medical center randomized to receive intervention. Patients were mailed a satisfaction survey 2-6 weeks after discharge. Description of Intervention: Patients received phone call from a pharmacist within 2 days of discharge and were asked How they had been feeling If they had any questions about their recent hospital stay If they were able to obtain all their medications If they understood how to take all their medications If they had experienced any possible medication adverse effects If they had any other questions or concerns Pharmacists intervened to correct any medication related problems Pharmacists communicated problems to the medical team Citation: Dudas et al. The Impact of Follow-up Telephone Calls to Patients After Hospitalization. Am J Med. 2001;111(9B):26S 30S.
45 Discharge Process TARGET INTERVENTION KEY PLAYERS Patient satisfaction, Decreased resource utilization Post-discharge telephone follow-up Pharmacists Results: 1. Patient Satisfaction: % very satisfied with medication care instructions Control = 61% Intervention = 86% p = ED visits within 30 days of discharge Control = 27 (24%) Intervention = 11 (10%) p = Hospital Readmissions Control = 25% Intervention = 15% p = 0.07 Discussion: Key finding was that 19% of patients had difficulty obtaining all their discharge medications. Standard pharmacy medication counseling discharge process takes 30 minutes. Home phone call required an additional 10 minutes on average. Citation: Dudas et al. The Impact of Follow-up Telephone Calls to Patients After Hospitalization. Am J Med. 2001;111(9B):26S 30S.
46 Discharge Process TARGET INTERVENTION KEY PLAYERS Patient education and empowerment and participation in self-care Care transitions coach, home/tele visits Nurse (transitions coach), patient Trial Design: Randomized controlled trial at large IDN involving 75 community dwelling enrollees admitted to study hospital for any of 11 conditions. Description of Intervention: Focused on 4 pillars Assistance with medication self-management A patient-centered record owned and maintained by the patient Timely follow-up with primary or specialty care A list of red flags indicative of a worsening condition and instructions on how to respond to them. Intervention Process: TC meets patient during inpatient stay, develops rapport, initiates PHR Home visit (48-72 hours) post-discharge. 3 follow-up phone calls through day 28 postdischarge. Home visit: Reconcile medications using the Medication Discrepancy Tool and educate patient on self-management. Citation: Coleman et al. The Care Transitions Intervention: Results of a Randomized Controlled Trial. Archives of Internal Medicine 2006;166:

47 Discharge Process Results: TARGET INTERVENTION KEY PLAYERS Patient education and empowerment and participation in self-care Care transitions coach Nurse (transitions coach), patient Annual Cost Savings: Projected at nearly $300k Comments: The transition coaches managed panels of patients Citation: Coleman et al.the Care Transitions Intervention: Results of a Randomized Controlled Trial Archives of Internal Medicine 2006;166:
48 Discharge Process TARGET INTERVENTION KEY PLAYERS Medication management, early intervention Home-based intervention (HBI)1 week post-discharge Pharmacists, nurses Trail Design: 97 heart failure patients identified as high-risk for readmission were prospectively examined after hospital discharge and randomized to receive the intervention. Tertiary referral hospital, elderly population, lower socioeconomic status, high prevalence of chronic illness and admission rates per capita for the region (Australia) Description of Intervention: Brief pre-discharge visit from study nurse regarding compliance with care plan 1 week post discharge visit by nurse and pharmacist that included: Assessment of medication knowledge Assess compliance/adherence with medications Education intervention for poor performers including: counseling, adherence training and tools, provision of medication reminder card, referral to a community pharmacist for regular follow-up Patients were evaluated for clinical deterioration or adverse events and issues addressed or referrals made. Citation: Stewart et al. Effects of a Home-Based Intervention Among Patients With Congestive Heart Failure Discharged From Acute Hospital Care. Arch Intern Med. 1998;158:
49 Discharge Process TARGET INTERVENTION KEY PLAYERS Medication management, early intervention Home-based intervention (HBI)1 week post-discharge Pharmacists, nurses Results: Unplanned readmission at 6 months plus out-of hospital death) (Primary) HBI 0.8±0.9 vs Control 1.4±1.8 (mean ± SD) (P = 0.03) Readmissions: 36 vs 63; P=.03 Out-of-hospital deaths:1 vs 5; P=0.11 Comments: Analysis of the pattern and potential predictors suggest that this type of HBI is most effective among patients with problems that contribute to poor control of their HF or less social support. Citation: Effects of a Home-Based Intervention Among Patients With Congestive Heart Failure Discharged From Acute Hospital Care. Arch Intern Med. 1998;158:
50 Discharge Process Trial Population: TARGET INTERVENTION KEY PLAYERS Medication discrepancies Medication review, reconciliation, counseling and education. Adherence checks. Post-discharge telephone f/u. Pharmacists 358 patients identified as high-risk for medication-related adverse events at a large, academic medical center. Description of Intervention: The pharmacist attended interdisciplinary discharge rounds conducted patient interviews assessed appropriateness and accuracy of discharge medications performed medication reconciliation to identify and resolve discrepancies ensured that a follow-up plan for medication monitoring after discharge was identified and communicated to the patient provided medication counseling, verified patient comprehension with medication instructions identified and addressed potential adherence concerns communicated a reconciled medication list to the patient s follow-up health care provider provided post-discharge follow-up by telephone at 72 hours and 30 days to assist with medicationrelated problems and identify additional concerns. Citation: Walker et al. Impact of a Pharmacist-Facilitated Hospital Discharge Program; A Quasi-Experimental Study. Arch Intern Med. 2009;169(21):

51 Discharge Process Outcomes: TARGET INTERVENTION KEY PLAYERS Medication discrepancies Medication review, reconciliation, counseling and education. Adherence checks. Post-discharge telephone f/u. Pharmacists Utilization of health care resources: 14- and 30-day readmission rates and ED visits within 72 hours after discharge. Results: Citation: Impact of a Pharmacist-Facilitated Hospital Discharge Program; A Quasi-Experimental Study. Arch Intern Med. 2009;169(21):

52 Discharge Process Outcomes: TARGET INTERVENTION KEY PLAYERS Medication discrepancies Medication review, reconciliation, counseling and education. Adherence checks. Post-discharge telephone f/u. Pharmacists Utilization of health care resources: 14- and 30-day readmission rates and ED visits within 72 hours after discharge. Results: Citation: Impact of a Pharmacist-Facilitated Hospital Discharge Program; A Quasi-Experimental Study. Arch Intern Med. 2009;169(21):

53 Discharge Process Results: TARGET INTERVENTION KEY PLAYERS Medication discrepancies Medication review, reconciliation, counseling and education. Adherence checks. Post-discharge telephone f/u. Pharmacists Citation: Impact of a Pharmacist-Facilitated Hospital Discharge Program; A Quasi-Experimental Study. Arch Intern Med. 2009;169(21):
54 Discharge Process TARGET INTERVENTION KEY PLAYERS Improved evidence-based medication use & communications from hospital to LTC facility Addition of a pharmacist transition coordinator Pharmacists, physicians, nurses Trail Design: Randomized, single blind, controlled trial enrolled 110 hospitalized older adults awaiting transfer to a long-term residential care facility for the first time. Sites included 3 metropolitan hospitals and 85 metropolitan long term care facilities. (AUSTRALIA) Description of Intervention: The pharmacist transition coordinator Compiled a medication transfer summary Transferred the summary to: patient s primary physician, community pharmacist/pharmacy, nurses at the LTC facility. Organized medication review by community pharmacist within days of discharge. Coordinated a case review between all stakeholders at days post-discharge Citation: Does the Addition of a Pharmacist Transition Coordinator Improve Evidence-Based Medication Management and Health Outcomes in Older Adults Moving from the Hospital to a Long-Term Care Facility? Results of a Randomized, Controlled Trial. Am J Pharm. 2004; 2(4):
55 Discharge Process TARGET INTERVENTION KEY PLAYERS Improved evidence-based medication use & communications from hospital to LTC facility Addition of a pharmacist transition coordinator Pharmacists, physicians, nurses Results: Primary: No significant difference in quality of prescribing based on MAI tool (orders from discharge to Week 8) Secondary: Unplanned ED visits or hospital readmission, adverse drug events, falls, worsening mobility or pain or increased confusion. Event Intervention Control RR 95% CI P Hosp use 5 (11.4) 13 (29.5) Comments: Secondary outcomes questionable due to low N/power. Citation: Does the Addition of a Pharmacist Transition Coordinator Improve Evidence-Based Medication Management and Health Outcomes in Older Adults Moving from the Hospital to a Long-Term Care Facility? Results of a Randomized, Controlled Trial. Am J Pharm. 2004; 2(4):
56 Summary of Opportunities for Pharmacy with Readmissions Prevention There are many potential areas for targeting interventions The research and study data to date shows both successful and unsuccessful attempts to decrease rates using a broad scope of interventions The data is extremely heterogeneous making absolute conclusions about what services to provide difficult It would appear that using very targeted interventions aimed at patients at high-risk for readmission would be the most practical and cost effective way to proceed Focusing on the discharge process with a consideration for a posthospital follow-up within 72 hours of discharge to determine medication-related problems or health issues has delivered value in hospital resource reduction in a number of trials.
57 Action Steps to Reduce Readmissions 1. Examine your hospital s current rate of readmissions 2. Assess and prioritize your improvement opportunities 3. Develop an action plan of strategies to implement 4. Monitor your progress
58 Tracking Progress Almost all hospitals will need help in gauging their performance with respect to rehospitalizations, because they have no access to data on the 20 to 40% of their patients who are rehospitalized elsewhere. Only holders of all-hospital discharge data, such as governments and other third party payers, have the ability to track patients across providers and systems.
59 Readmissions Information Sources IHI (STAAR Initiative) voidablerehospitalizationsstaar.htm IHI Transforming Care at the Bedsite (TCAB) areatthebedside.htm CMS Affordable Care Act: Readmission payment reform Community Care Transitions Program (CCTP) Care Transitions Project Information and tools, including the Med Discrepancy Tool
60 Readmissions Information Sources Project Boost Robust info site with tools, etc on care transitions CT_Home.cfm National Priorities Partnership 7 key targets, including Continuity of Care
61 IHI Readmission Risk Assessment Tool

62 Medication Discrepancy Tool
63 The Teach-Back Method Studies have shown that percent of the medical information patients receive is forgotten immediately and nearly half of the information retained is incorrect. Teach-back is a way to confirm that you have explained to the patient what they need to know in a manner that the patient understands. Patient understanding is confirmed when they explain it back to you. Web site includes: Video instruction PowerPoint Handouts Self-evaluation
64 Questions and Discussion
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION
 Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
What Works for Preventing Hospital Readmissions? A review of the current evidence and best practices
 What Works for Preventing Hospital Readmissions? A review of the current evidence and best practices Steven M. Riddle, BS Pharm, BCPS, FASHP Vice President of Clinical Affairs Pharmacy OneSource/ Wolters
What Works for Preventing Hospital Readmissions? A review of the current evidence and best practices Steven M. Riddle, BS Pharm, BCPS, FASHP Vice President of Clinical Affairs Pharmacy OneSource/ Wolters
Preventing Readmissions
 Emerging Topics in Healthcare Reform Preventing Readmissions Janssen Pharmaceuticals, Inc. Preventing Readmissions The Patient Protection and Affordable Care Act (ACA) contains several provisions intended
Emerging Topics in Healthcare Reform Preventing Readmissions Janssen Pharmaceuticals, Inc. Preventing Readmissions The Patient Protection and Affordable Care Act (ACA) contains several provisions intended
Health Care Leader Action Guide to Reduce Avoidable Readmissions
 Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
Health Care Leader Action Guide to Reduce Avoidable Readmissions January 2010 TRANSFORMING HEALTH CARE THROUGH RESEARCH AND EDUCATION Osei-Anto A, Joshi M, Audet AM, Berman A, Jencks S. Health Care Leader
Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions
 Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions Leslie Becker RN, BS Jennifer Smith RN, MSN, MBA Leslie Frain MSN, RN Jan Machanis
Nurse Transition Coach Model: Innovative, Evidence-based, and Cost Effective Solutions to Reduce Hospital Readmissions Leslie Becker RN, BS Jennifer Smith RN, MSN, MBA Leslie Frain MSN, RN Jan Machanis
Value-Based Purchasing Program Overview. Maida Soghikian, MD Grand Rounds Scripps Green Hospital November 28, 2012
 Value-Based Purchasing Program Overview Maida Soghikian, MD Grand Rounds Scripps Green Hospital November 28, 2012 Presentation Overview Background and Introduction Inpatient Quality Reporting Program Value-Based
Value-Based Purchasing Program Overview Maida Soghikian, MD Grand Rounds Scripps Green Hospital November 28, 2012 Presentation Overview Background and Introduction Inpatient Quality Reporting Program Value-Based
Preventing Avoidable Re-Hospitalizations: Where Do You Fit in the Quality Care Puzzle?
 Speaker Disclosures Care Transitions Interventions: The Sussex County Transitional Care Program Dr. Wang has disclosed that he has no relevant financial relationship(s). George C. Wang, MD, PhD Medical
Speaker Disclosures Care Transitions Interventions: The Sussex County Transitional Care Program Dr. Wang has disclosed that he has no relevant financial relationship(s). George C. Wang, MD, PhD Medical
1. Executive Summary Problem/Opportunity: Evidence: Baseline Data: Intervention: Results:
 A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
A Clinical Nurse Leader led multidisciplinary Heart Failure Program: Integrating best practice across the care continuum to reduce avoidable 30 day readmissions. 1. Executive Summary Problem/Opportunity:
Innovations@Home. Home Health Initiatives Reduce Avoidable Readmissions by Leveraging Innovation
 How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
How Does CMS Measure the Rate of Acute Care Hospitalization (ACH)? Until January 2013, CMS measured Acute Care Hospitalization (ACH) through the Outcomes Assessment and Information Set (OASIS) reporting
hospital readmission rate reduction: building better interfaces within the community.
 hospital readmission rate reduction: building better interfaces within the community. Whitepaper By Ken Taverner, M.Sc. the issue of hospital readmission rates Leaving the hospital after being admitted
hospital readmission rate reduction: building better interfaces within the community. Whitepaper By Ken Taverner, M.Sc. the issue of hospital readmission rates Leaving the hospital after being admitted
From the Ground Up: The implementation of a Transition Care Program (TOC) and its impact in COPD 30-day readmissions
 and its impact in COPD 30-day readmissions") From the Ground Up: The implementation of a Transition Care Program (TOC) and its impact in COPD 30-day readmissions Cristiane L. Fukuda RN, MSN, ANP-BC Email: [email protected] Office: 404-851-6914
From the Ground Up: The implementation of a Transition Care Program (TOC) and its impact in COPD 30-day readmissions Cristiane L. Fukuda RN, MSN, ANP-BC Email: [email protected] Office: 404-851-6914
Care Coordination and Transitions in Behavioral Health
 Care Coordination and Transitions in Behavioral Health Pam Pietruszewski Integrated Health Consultant The National Council for Behavioral Health This product is supported by the Florida Department of Children
Care Coordination and Transitions in Behavioral Health Pam Pietruszewski Integrated Health Consultant The National Council for Behavioral Health This product is supported by the Florida Department of Children
Implementing an Evidence Based Hospital Discharge Process
 Implementing an Evidence Based Hospital Discharge Process Learning from the experience of Project Re-Engineered Discharge (RED) Webinar January 14, 2013 Chris Manasseh, MD Director, Boston HealthNet Inpatient
Implementing an Evidence Based Hospital Discharge Process Learning from the experience of Project Re-Engineered Discharge (RED) Webinar January 14, 2013 Chris Manasseh, MD Director, Boston HealthNet Inpatient
WHITE PAPER. How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience
 WHITE PAPER How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience Vocera Communications, Inc. June, 2014 SUMMARY Hospitals that reduce readmission rates
WHITE PAPER How a multi-tiered strategy can reduce readmission rates and significantly enhance patient experience Vocera Communications, Inc. June, 2014 SUMMARY Hospitals that reduce readmission rates
RED, BOOST, and You: Improving the Discharge Transition of Care
 RED, BOOST, and You: Improving the Discharge Transition of Care Jeffrey L. Greenwald, MD, SFHM Massachusetts General Hospital - Clinician Educator Service Co-Investigator Project RED & Project BOOST The
RED, BOOST, and You: Improving the Discharge Transition of Care Jeffrey L. Greenwald, MD, SFHM Massachusetts General Hospital - Clinician Educator Service Co-Investigator Project RED & Project BOOST The
National Provider Call: Hospital Value-Based Purchasing (VBP) Program
 Program") National Provider Call: Hospital Value-Based Purchasing (VBP) Program Fiscal Year 2016 Overview for Beneficiaries, Providers and Stakeholders Cindy Tourison, MSHI Lead, Hospital Inpatient Quality Reporting
National Provider Call: Hospital Value-Based Purchasing (VBP) Program Fiscal Year 2016 Overview for Beneficiaries, Providers and Stakeholders Cindy Tourison, MSHI Lead, Hospital Inpatient Quality Reporting
Hospital readmissions contribute to the increasing. Deployment of Lean Six Sigma in Care Coordination An Improved Discharge Process
 Professional Case Management Vol. 19, No. 2, 77-83 Copyright 2014 Wolters Kluwer Health Lippincott Williams & Wilkins Deployment of Lean Six Sigma in Care Coordination An Improved Discharge Process Susan
Professional Case Management Vol. 19, No. 2, 77-83 Copyright 2014 Wolters Kluwer Health Lippincott Williams & Wilkins Deployment of Lean Six Sigma in Care Coordination An Improved Discharge Process Susan
Value Based Care and Healthcare Reform
 Value Based Care and Healthcare Reform Dimensions in Cardiac Care November, 2014 Jacqueline Matthews, RN, MS Senior Director, Quality Reporting & Reform Quality and Patient Safety Institute Cleveland Clinic
Value Based Care and Healthcare Reform Dimensions in Cardiac Care November, 2014 Jacqueline Matthews, RN, MS Senior Director, Quality Reporting & Reform Quality and Patient Safety Institute Cleveland Clinic
Accountable Care Organizations
 Accountable Care Organizations Myth, Reality, Facts Why =System Failure Low Quality - IOM report High Cost Quality Cost disconnect Low Value Problems Disconnect between Quality and Cost Care is fragmented
Accountable Care Organizations Myth, Reality, Facts Why =System Failure Low Quality - IOM report High Cost Quality Cost disconnect Low Value Problems Disconnect between Quality and Cost Care is fragmented
Understanding Care Transitions as a Patient Safety Issue
 Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
Article reprinted from Patient Safety & Quality Healthcare, May/June 2011 Understanding Care Transitions as a Patient Safety Issue By Sara Butterfield RN, BSN, CPHQ, CCM; Christine Stegel, RN, MS, CPHQ;
Care Transition Bundle Seven Essential Intervention Categories. Examples of Transition of Care Interventions
 1. Medications Management Ensuring the safe use of medications by patients and their families and based on patients plans of care a. Assessment of patient s medications intake b. Patient and family education
1. Medications Management Ensuring the safe use of medications by patients and their families and based on patients plans of care a. Assessment of patient s medications intake b. Patient and family education
Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases
 Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases Epidemiology Over 145 million people ( nearly half the population) - suffer from asthma, depression and other chronic
Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases Epidemiology Over 145 million people ( nearly half the population) - suffer from asthma, depression and other chronic
Readmissions as an Enterprise Priority. Presenters 4/17/2014
 Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center [email protected] Eileen
Readmissions as an Enterprise Priority April 24, 2014 Presenters Vincent A. Maniscalco, MPA, LNHA Administrator Middletown Park Rehabilitation and Health Care Center [email protected] Eileen
RT AS PROJECT MANAGER:
 RT AS PROJECT MANAGER: IMPROVING CARE TRANSITIONS DECREASES UNPLANNED READMISSIONS TAMMY JARNAGIN, BHS, RRT DIRECTOR CARDIOPULMONARY SERVICES, NEURODIAGNOSTICS, HOME MEDICAL EQUIPMENT Objectives Recognize
RT AS PROJECT MANAGER: IMPROVING CARE TRANSITIONS DECREASES UNPLANNED READMISSIONS TAMMY JARNAGIN, BHS, RRT DIRECTOR CARDIOPULMONARY SERVICES, NEURODIAGNOSTICS, HOME MEDICAL EQUIPMENT Objectives Recognize
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment
 Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
Person-Centered Nurse Care Management in Home Based Care: Impact on Well-Being and Cost Containment Donna Zazworsky, RN, MS, CCM, FAAN Vice President: Community Health and Continuum Care Carondelet Health
Modern care management
 The care management challenge Health plans and care providers spend billions of dollars annually on care management with the expectation of better utilization management and cost control. That expectation
The care management challenge Health plans and care providers spend billions of dollars annually on care management with the expectation of better utilization management and cost control. That expectation
Care Transition Bundle Seven Essential Intervention Categories
 Seven 1. Medications Management Ensuring the safe use of medications by patients and their families and based on patients plans of care a. Assessment of patient s medications intake b. Patient and family
Seven 1. Medications Management Ensuring the safe use of medications by patients and their families and based on patients plans of care a. Assessment of patient s medications intake b. Patient and family
Benefit Design and ACOs: How Will Private Employers and Health Plans Proceed?
 Benefit Design and ACOs: How Will Private Employers and Health Plans Proceed? Accountable Care Organizations: Implications for Consumers October 14, 2010 Washington, DC Sam Nussbaum, M.D. Executive Vice
Benefit Design and ACOs: How Will Private Employers and Health Plans Proceed? Accountable Care Organizations: Implications for Consumers October 14, 2010 Washington, DC Sam Nussbaum, M.D. Executive Vice
Linking Quality to Payment
 Linking Quality to Payment Background Our nation s health care delivery system is undergoing a major transformation as reimbursement moves from a volume-based methodology to one based on value and quality.
Linking Quality to Payment Background Our nation s health care delivery system is undergoing a major transformation as reimbursement moves from a volume-based methodology to one based on value and quality.
FINANCIAL IMPLICATIONS OF EXCESS HOSPITAL READMISSIONS JOSESPH B. HENDERSON, J.D.
 FINANCIAL IMPLICATIONS OF EXCESS HOSPITAL READMISSIONS JOSESPH B. HENDERSON, J.D. Executive MHA Candidate, 2013 University of Southern California Sol Price School of Public Policy Abstract A 2007 Medicare
FINANCIAL IMPLICATIONS OF EXCESS HOSPITAL READMISSIONS JOSESPH B. HENDERSON, J.D. Executive MHA Candidate, 2013 University of Southern California Sol Price School of Public Policy Abstract A 2007 Medicare
Tool 6: How To Monitor Re-Engineered Discharge Implementation and Outcomes
 Tool 6: How To Monitor Re-Engineered Discharge Implementation and Outcomes 6.. Purpose of This Tool Monitoring the RED lets you know whether each component of RED is being successfully implemented and
Tool 6: How To Monitor Re-Engineered Discharge Implementation and Outcomes 6.. Purpose of This Tool Monitoring the RED lets you know whether each component of RED is being successfully implemented and
How To Reduce Hospital Readmission
 Reducing Hospital Readmissions & The Affordable Care Act The Game Has Changed Drastically Reducing MSPB Measures Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE
Reducing Hospital Readmissions & The Affordable Care Act The Game Has Changed Drastically Reducing MSPB Measures Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE Chuck Bongiovanni, MSW, MBA, NCRP, CSA, CFE
A STRATIFIED APPROACH TO PATIENT SAFETY THROUGH HEALTH INFORMATION TECHNOLOGY
 A STRATIFIED APPROACH TO PATIENT SAFETY THROUGH HEALTH INFORMATION TECHNOLOGY Table of Contents I. Introduction... 2 II. Background... 2 III. Patient Safety... 3 IV. A Comprehensive Approach to Reducing
A STRATIFIED APPROACH TO PATIENT SAFETY THROUGH HEALTH INFORMATION TECHNOLOGY Table of Contents I. Introduction... 2 II. Background... 2 III. Patient Safety... 3 IV. A Comprehensive Approach to Reducing
SPECIALTY CASE MANAGEMENT
 SPECIALTY CASE MANAGEMENT Our Specialty Case Management programs boost ROI and empower members to make informed decisions and work with their physicians to better manage their health. KEPRO is Effectively
SPECIALTY CASE MANAGEMENT Our Specialty Case Management programs boost ROI and empower members to make informed decisions and work with their physicians to better manage their health. KEPRO is Effectively
Evidence Based Practice to. Value Based Purchasing. Barb Rogness BSN MS Building Bridges May 2013
 Evidence Based Practice to Value Based Purchasing Barb Rogness BSN MS Building Bridges May 2013 Why this topic? Value based Purchasing is here and not going away. It will grow by leaps and bounds. The
Evidence Based Practice to Value Based Purchasing Barb Rogness BSN MS Building Bridges May 2013 Why this topic? Value based Purchasing is here and not going away. It will grow by leaps and bounds. The
Performance Measurement in CMS Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS
 Performance Measurement in CMS Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS Mind the Gap: Improving Quality Measures in Accountable Care Systems October
Performance Measurement in CMS Programs Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS Mind the Gap: Improving Quality Measures in Accountable Care Systems October
HCAHPS and Value-Based Purchasing Methods and Measurement. Deb Stargardt, Improvement Services Darrel Shanbour, Consulting Services
 HCAHPS and Value-Based Purchasing Methods and Measurement Deb Stargardt, Improvement Services Darrel Shanbour, Consulting Services Today s Learning Objectives Acquire new knowledge pertaining to: A. Hospital
HCAHPS and Value-Based Purchasing Methods and Measurement Deb Stargardt, Improvement Services Darrel Shanbour, Consulting Services Today s Learning Objectives Acquire new knowledge pertaining to: A. Hospital
CCNC Care Management
 CCNC Care Management Community Care of North Carolina (CCNC) is a statewide population management and care coordination infrastructure founded on the primary care medical home model. CCNC incorporates
CCNC Care Management Community Care of North Carolina (CCNC) is a statewide population management and care coordination infrastructure founded on the primary care medical home model. CCNC incorporates
4/22/2013. Transitions Handoffs Vulnerable exchange points Adverse clinical events Unmet needs Poor patient satisfaction
 Objectives Transitions of Care and the Pharmacy Practice Model Initiative Emily Bennett, PharmD Melody Hartzler, PharmD, AE-C Describe the Affordable Care Act and it s implications on current healthcare
Objectives Transitions of Care and the Pharmacy Practice Model Initiative Emily Bennett, PharmD Melody Hartzler, PharmD, AE-C Describe the Affordable Care Act and it s implications on current healthcare
1900 K St. NW Washington, DC 20006 c/o McKenna Long
 1900 K St. NW Washington, DC 20006 c/o McKenna Long Centers for Medicare & Medicaid Services U. S. Department of Health and Human Services Attention CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re:
1900 K St. NW Washington, DC 20006 c/o McKenna Long Centers for Medicare & Medicaid Services U. S. Department of Health and Human Services Attention CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re:
Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education
 1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
1 Nancy L. Wilson Department of Medicine-Geriatrics Houston Center for Quality of Care& Utilization Studies Texas Consortium of Geriatric Education Centers Care for Elders Governing Council Acknowledge
Accountable Care Organizations and Future Healthcare Delivery
 Accountable Care Organizations and Future Healthcare Delivery Introduction Accountable care organizations (ACOs) are a key component of healthcare reform. This module covers the establishment of accountable
Accountable Care Organizations and Future Healthcare Delivery Introduction Accountable care organizations (ACOs) are a key component of healthcare reform. This module covers the establishment of accountable
caresy caresync Chronic Care Management
 caresy Chronic Care Management THE PROBLEM Chronic diseases and conditions, including heart disease, diabetes, COPD and obesity, are among the most common, expensive, and preventable health problems in
caresy Chronic Care Management THE PROBLEM Chronic diseases and conditions, including heart disease, diabetes, COPD and obesity, are among the most common, expensive, and preventable health problems in
Technician Learning Objectives 3/25/2014. Pharmacy Practice Changes in ACA Accountable Care Organizations
 Pharmacy Practice Changes in ACA Accountable Care Organizations Avani S. Desai, PharmD & Emory S. Martin PharmD Sunday, April 12, 2014 9:05 10:05 am Pharmacist Learning Objectives At the conclusion of
Pharmacy Practice Changes in ACA Accountable Care Organizations Avani S. Desai, PharmD & Emory S. Martin PharmD Sunday, April 12, 2014 9:05 10:05 am Pharmacist Learning Objectives At the conclusion of
The Care Transitions Intervention: Geriatric Care. During an episode of illness, older patients may receive care in multiple settings; often resulting
 The Care Transitions Intervention: A Patient-Centered Approach to Ensuring Effective Transfers Between Sites of Geriatric Care Abstract During an episode of illness, older patients may receive care in
The Care Transitions Intervention: A Patient-Centered Approach to Ensuring Effective Transfers Between Sites of Geriatric Care Abstract During an episode of illness, older patients may receive care in
Reducing Readmissions with Predictive Analytics
 Reducing Readmissions with Predictive Analytics Conway Regional Health System uses analytics and the LACE Index from Medisolv s RAPID business intelligence software to identify patients poised for early
Reducing Readmissions with Predictive Analytics Conway Regional Health System uses analytics and the LACE Index from Medisolv s RAPID business intelligence software to identify patients poised for early
Home Health Care: A More Cost-Effective Approach to Medicaid in Illinois Illinois HomeCare & Hospice Council December 2010
 Home Health Care: A More Cost-Effective Approach to Medicaid in Illinois Illinois HomeCare & Hospice Council December 2010 As the Illinois Legislature prepares to act on the future of Medicaid, it is important
Home Health Care: A More Cost-Effective Approach to Medicaid in Illinois Illinois HomeCare & Hospice Council December 2010 As the Illinois Legislature prepares to act on the future of Medicaid, it is important
ACCOUNTABLE CARE ANALYTICS: DEVELOPING A TRUSTED 360 DEGREE VIEW OF THE PATIENT
 ACCOUNTABLE CARE ANALYTICS: DEVELOPING A TRUSTED 360 DEGREE VIEW OF THE PATIENT Accountable Care Analytics: Developing a Trusted 360 Degree View of the Patient Introduction Recent federal regulations have
ACCOUNTABLE CARE ANALYTICS: DEVELOPING A TRUSTED 360 DEGREE VIEW OF THE PATIENT Accountable Care Analytics: Developing a Trusted 360 Degree View of the Patient Introduction Recent federal regulations have
Cheryl Schraeder, RN, PhD, FAAN. The demographic landscape of America is changing at an accelerated pace
 Stepping up to the challenge: Changing the way we deliver care Cheryl Schraeder, RN, PhD, FAAN 1 Goals of Presentation To Identify: The key challenges in delivering evidence-based & cost-effective care
Stepping up to the challenge: Changing the way we deliver care Cheryl Schraeder, RN, PhD, FAAN 1 Goals of Presentation To Identify: The key challenges in delivering evidence-based & cost-effective care
CMS Office of Public Affairs 202-690-6145 MEDICARE PROPOSES NEW HOSPITAL VALUE-BASED PURCHASING PROGRAM
 For Immediate Release: Friday, January 07, 2011 Contact: CMS Office of Public Affairs 202-690-6145 MEDICARE PROPOSES NEW HOSPITAL VALUE-BASED PURCHASING PROGRAM OVERVIEW: Today the Centers for Medicare
For Immediate Release: Friday, January 07, 2011 Contact: CMS Office of Public Affairs 202-690-6145 MEDICARE PROPOSES NEW HOSPITAL VALUE-BASED PURCHASING PROGRAM OVERVIEW: Today the Centers for Medicare
Henry Ford Health System Care Coordination and Readmissions Update
 Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
Henry Ford Health System Care Coordination and Readmissions Update September 2013 BACKGROUND Most hospital readmissions are viewed as avoidable, costly, and in some cases as a potential marker of poor
Coaching Patients to Improve Care Transitions in Pennsylvania. May 26, 2010
 Coaching Patients to Improve Care Transitions in Pennsylvania Naomi Hauser, RN, MPA, CLNC Director Care Transitions Quality Insights of Pennsylvania Dr. Eric Coleman, MPH Professor of Medicine University
Coaching Patients to Improve Care Transitions in Pennsylvania Naomi Hauser, RN, MPA, CLNC Director Care Transitions Quality Insights of Pennsylvania Dr. Eric Coleman, MPH Professor of Medicine University
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home
 RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
RIH Transitions of Care Collaboration with Coastal Medical To Improve Transitions for Patients Discharged Hospital To Home Sergio Petrillo, PharmD Clinical Pharmacist Specialist, Rhode Island Hospital
ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION)
") ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION) Hello and welcome. Thank you for taking part in this presentation entitled "Essentia Health as an ACO or Accountable Care Organization -- What
ESSENTIA HEALTH AS AN ACO (ACCOUNTABLE CARE ORGANIZATION) Hello and welcome. Thank you for taking part in this presentation entitled "Essentia Health as an ACO or Accountable Care Organization -- What
CCNC Care Management Standardized Plan
 Standardization & Reporting: Why is standardization important? Community Care Networks are responsible for the delivery of targeted care management services that will improve quality of care while containing
Standardization & Reporting: Why is standardization important? Community Care Networks are responsible for the delivery of targeted care management services that will improve quality of care while containing
GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services
 GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services Aged, Blind and Disabled Stakeholder Presentation Indiana Family and Social Services Administration August
GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services Aged, Blind and Disabled Stakeholder Presentation Indiana Family and Social Services Administration August
A bundle of activities linked to transitional care principles can reduce both short- and long-term readmission risk.
 Transitional care can reduce hospital readmissions A bundle of activities linked to transitional care principles can reduce both short- and long-term readmission risk. By Joan M. Nelson, DNP, ANP-BC, and
Transitional care can reduce hospital readmissions A bundle of activities linked to transitional care principles can reduce both short- and long-term readmission risk. By Joan M. Nelson, DNP, ANP-BC, and
Proven Innovations in Primary Care Practice
 Proven Innovations in Primary Care Practice October 14, 2014 The opinions expressed are those of the presenter and do not necessarily state or reflect the views of SHSMD or the AHA. 2014 Society for Healthcare
Proven Innovations in Primary Care Practice October 14, 2014 The opinions expressed are those of the presenter and do not necessarily state or reflect the views of SHSMD or the AHA. 2014 Society for Healthcare
Realizing ACO Success with ICW Solutions
 Realizing ACO Success with ICW Solutions A Pathway to Collaborative Care Coordination and Care Management Decrease Healthcare Costs Improve Population Health Enhance Care for the Individual connect. manage.
Realizing ACO Success with ICW Solutions A Pathway to Collaborative Care Coordination and Care Management Decrease Healthcare Costs Improve Population Health Enhance Care for the Individual connect. manage.
Transitions of Care: The need for a more effective approach to continuing patient care
 H O T T O P I C S I N H E A L T H C A R E Transitions of Care: The need for a more effective approach to continuing patient care The need for a more effective approach to continuing patient care This paper
H O T T O P I C S I N H E A L T H C A R E Transitions of Care: The need for a more effective approach to continuing patient care The need for a more effective approach to continuing patient care This paper
CHAPTER 535 HEALTH HOMES. Background... 2. Policy... 2. 535.1 Member Eligibility and Enrollment... 2. 535.2 Health Home Required Functions...
 TABLE OF CONTENTS SECTION PAGE NUMBER Background... 2 Policy... 2 535.1 Member Eligibility and Enrollment... 2 535.2 Health Home Required Functions... 3 535.3 Health Home Coordination Role... 4 535.4 Health
TABLE OF CONTENTS SECTION PAGE NUMBER Background... 2 Policy... 2 535.1 Member Eligibility and Enrollment... 2 535.2 Health Home Required Functions... 3 535.3 Health Home Coordination Role... 4 535.4 Health
Accountable Care Organizations and Patient-Centered Medical Homes
 Emerging Topics in Healthcare Reform Accountable Care Organizations and Patient-Centered Medical Homes Janssen Pharmaceuticals, Inc. Accountable Care Organizations and Patient-Centered Medical Homes The
Emerging Topics in Healthcare Reform Accountable Care Organizations and Patient-Centered Medical Homes Janssen Pharmaceuticals, Inc. Accountable Care Organizations and Patient-Centered Medical Homes The
How Health Reform Will Affect Health Care Quality and the Delivery of Services
 Fact Sheet AARP Public Policy Institute How Health Reform Will Affect Health Care Quality and the Delivery of Services The recently enacted Affordable Care Act contains provisions to improve health care
Fact Sheet AARP Public Policy Institute How Health Reform Will Affect Health Care Quality and the Delivery of Services The recently enacted Affordable Care Act contains provisions to improve health care
Six Communication Best Practices for Transitional Care Management
 WHITE PAPER Six Communication Best Practices for Transitional Care Management In the era of chronic illness and historically long lifespans, patient care transitions to home or another facility have become
WHITE PAPER Six Communication Best Practices for Transitional Care Management In the era of chronic illness and historically long lifespans, patient care transitions to home or another facility have become
Disease Management Identifications and Stratification Health Risk Assessment Level 1: Level 2: Level 3: Stratification
 Disease Management UnitedHealthcare Disease Management (DM) programs are part of our innovative Care Management Program. Our Disease Management (DM) program is guided by the principles of the UnitedHealthcare
Disease Management UnitedHealthcare Disease Management (DM) programs are part of our innovative Care Management Program. Our Disease Management (DM) program is guided by the principles of the UnitedHealthcare
THE SAN DIEGO CARE TRANSITIONS PARTNERSHIP
 THE SAN DIEGO CARE TRANSITIONS PARTNERSHIP Transforming Care Across the Continuum Julianne R. Howell, Ph.D. Senior Health Policy Advisor County of San Diego Health and Human Services Agency SAN DIEGO COUNTY
THE SAN DIEGO CARE TRANSITIONS PARTNERSHIP Transforming Care Across the Continuum Julianne R. Howell, Ph.D. Senior Health Policy Advisor County of San Diego Health and Human Services Agency SAN DIEGO COUNTY
UnitedHealthcare Medicare Solutions Readmission Review Program for Medicare Advantage Plans
 UnitedHealthcare Medicare Solutions Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Updated May 2015 Introduction The UnitedHealthcare Medicare Solutions
UnitedHealthcare Medicare Solutions Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Updated May 2015 Introduction The UnitedHealthcare Medicare Solutions
Adverse Drug Events and Medication Safety: Diabetes Agents and Hypoglycemia
 Adverse Drug Events and Medication Safety: Diabetes Agents and Hypoglycemia Date: October 20, 2015 Presented by Mike Crooks, PharmD., PCMH-CCE Pharmacy Interventions, Technical Lead 11/9/2015 1 Objectives:
Adverse Drug Events and Medication Safety: Diabetes Agents and Hypoglycemia Date: October 20, 2015 Presented by Mike Crooks, PharmD., PCMH-CCE Pharmacy Interventions, Technical Lead 11/9/2015 1 Objectives:
Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015
 Leveraging the Continuum to Avoid Unnecessary Utilization While Improving Quality Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015 Karim A. Habibi, FHFMA, MPH, MS Senior
Leveraging the Continuum to Avoid Unnecessary Utilization While Improving Quality Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015 Karim A. Habibi, FHFMA, MPH, MS Senior
Providing and Billing Medicare for Transitional Care Management
 PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
HAI LEADERSHIP PARTNERING FOR ACCOUNTABLE CARE
 HAI LEADERSHIP PARTNERING FOR ACCOUNTABLE CARE Cepheid s Government Affairs Department Advocating for Patient Access to Molecular Diagnostics in the Era of Healthcare Reform A TEAM APPROACH Legislative
HAI LEADERSHIP PARTNERING FOR ACCOUNTABLE CARE Cepheid s Government Affairs Department Advocating for Patient Access to Molecular Diagnostics in the Era of Healthcare Reform A TEAM APPROACH Legislative
PCMH and Care Management: Where do we start?
 PCMH and Care Management: Where do we start? Patricia Bohs, RN, BSN Quality Assurance Manager Kelly McCloughan QA Data Manager Wayne Memorial Community Health Centers Honesdale, PA Wayne Memorial Community
PCMH and Care Management: Where do we start? Patricia Bohs, RN, BSN Quality Assurance Manager Kelly McCloughan QA Data Manager Wayne Memorial Community Health Centers Honesdale, PA Wayne Memorial Community
Identifying High-Risk Medicare Beneficiaries with Predictive Analytics
 Identifying High-Risk Medicare Beneficiaries with Predictive Analytics September 2014 Until recently, with the passage of the Affordable Care Act (ACA), Medicare Fee-for-Service (FFS) providers had little
Identifying High-Risk Medicare Beneficiaries with Predictive Analytics September 2014 Until recently, with the passage of the Affordable Care Act (ACA), Medicare Fee-for-Service (FFS) providers had little
PL 111-148 and Amendments: Impact on Post-Acute Care for Health Care Systems
 PL 111-148 and Amendments: Impact on Post-Acute Care for Health Care Systems By Kathleen M. Griffin, PhD. There are three key provisions of the law that will have direct impact on post-acute care needs
PL 111-148 and Amendments: Impact on Post-Acute Care for Health Care Systems By Kathleen M. Griffin, PhD. There are three key provisions of the law that will have direct impact on post-acute care needs
Health Plan Innovations in Patient-Centered Care. Transitions of Care. April 2012 2012 ACHP
 Health Plan Innovations in Patient-Centered Care April 2012 Transitions of Care : Transitions of Care from Hospital to Home Practices Used by Community-Based Health Plans to Facilitate Successful Care
Health Plan Innovations in Patient-Centered Care April 2012 Transitions of Care : Transitions of Care from Hospital to Home Practices Used by Community-Based Health Plans to Facilitate Successful Care
A white paper. Collaborative Accountable Care. CIGNA s Approach to Accountable Care Organizations. 841282 a 11/11
 A white paper Collaborative Accountable Care CIGNA s Approach to Accountable Care Organizations 841282 a 11/11 Transforming the Health Care System Successfully transforming the U.S. health care system
A white paper Collaborative Accountable Care CIGNA s Approach to Accountable Care Organizations 841282 a 11/11 Transforming the Health Care System Successfully transforming the U.S. health care system
CMS Innovation Center Improving Care for Complex Patients
 CMS Innovation Center Improving Care for Complex Patients ECRI Institute Dr. Patrick Conway, M.D., MSc CMS Chief Medical Officer and Deputy Administrator for Innovation and Quality Director, Center for
CMS Innovation Center Improving Care for Complex Patients ECRI Institute Dr. Patrick Conway, M.D., MSc CMS Chief Medical Officer and Deputy Administrator for Innovation and Quality Director, Center for
Re: CMS-1345-P; Medicare Program; Medicare Shared Savings Program: Accountable Care Organizations; Proposed Rule
 Department of Health and Human Services Attention: CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re: CMS-1345-P; Medicare Program; Medicare Shared Savings Program: Accountable Care Organizations;
Department of Health and Human Services Attention: CMS 1345 P P.O. Box 8013, Baltimore, MD 21244 8013 Re: CMS-1345-P; Medicare Program; Medicare Shared Savings Program: Accountable Care Organizations;
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
H O T T O P I C S I N H E A L T H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Effective C o l l a b o r a t i v e S u c
HealthCare Partners of Nevada. Heart Failure
 HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
June 25, 2012. Dear Acting Administrator Tavenner,
 June 25, 2012 Marilyn B. Tavenner, RN, Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Attention: CMS-1588-P P.O. Box 8011 Baltimore, MD 21244-1850
June 25, 2012 Marilyn B. Tavenner, RN, Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Attention: CMS-1588-P P.O. Box 8011 Baltimore, MD 21244-1850