REGIONAL SYSTEMS OF CARE DEMONSTRATION PROJECT: MISSION: LIFELINE STEMI SYSTEMS ACCELERATOR
|
|
|
- Julian Cooper
- 10 years ago
- Views:
Transcription
1 REGIONAL SYSTEMS OF CARE DEMONSTRATION PROJECT: MISSION: LIFELINE STEMI SYSTEMS ACCELERATOR Version 5.0 July Duke Center for Educational Excellence Edited by Daniel Muñoz, MD, MPA Duke University Page 1

2 Table of Contents Introduction....3 A Changing Landscape: The New Guidelines 5 EMS: Dispatch..6 EMS: Initial Contact (EMT Basic or Intermediate Provider). 7 EMS: Initial Contact (EMT Paramedic) EMS: Inter-facility Transfer (EMT Basic/Intermediate, Paramedic) EMS: Chest Pain (Suspected Cardiac Event) EMS: Diversion from non-pci hospital to PCI hospital EMS: Air Medical Transfer Non-PCI Hospital Primary PCI Hospital Cardiogenic Shock: Available Tools Government: Local Government: State and Federal Payers Reperfusion Regimen A Primary PCI Reperfusion Regimen B Fibrinolysis Reperfusion Checklist for STEMI Medication Dosing Guidelines Glossary of Terms References Appendix A: Checklists Page 2

3 INTRODUCTION REGIONAL SYSTEMS OF CARE DEMONSTRATION PROJECT: MISSION: LIFELINE STEMI SYSTEMS ACCELERATOR Across the United States, hospitals and emergency medical systems are organizing coordinated regional plans for ST segment elevation myocardial infarction (STEMI) diagnosis and rapid reperfusion. This demonstration project is an educational outcomes research study and will enroll 20 regional sites in the U.S. (map on following page) for comprehensive implementation of regional emergency cardiac care systems. KEY PROCESS OBJECTIVES: Project Overview 1) Markedly accelerate the development of regional systems to diagnose and treat acute myocardial infarction. Regional systems will be composed of all hospitals and emergency medical service providers within a geographic region following agreed upon diagnostic and treatment protocols and supported by ongoing data collection and feedback. Building upon national guidelines and local consensus, these networks will facilitate effective delivery of emergency cardiac care in a timely, coordinated and consistent manner. 2) Bring together leading health care providers and institutions in a collaborative fashion facilitated by professional organizations, national experts in regional system organization, key local thought leaders in cardiology and emergency medicine, and leading emergency cardiac care businesses. 3) Identify and establish regional leadership in emergency cardiac care that includes key physicians and administrators in hospitals, emergency medicine, and cardiology. SPECIFIC OBJECTIVES: a) Increase the rate and speed of reperfusion specifically from the time the STEMI patient accesses the health care system or self presents to the emergency department to reperfusion (preferred primary PCI first device deployed or fibrinolysis delivered when time goals for primary PCI cannot be met). b) Establish a predetermined plan for identification of STEMI, acute treatment, and timely disposition to the most appropriate hospital no matter where the STEMI patient enters the system. c) Empower the EMS and non-pci emergency departments to determine the best reperfusion plan and most appropriate destination protocol through pre-hospital ECG and telephone support by PCI hospitals. d) according to guideline directed, evidenced based medicine. e) Perform a baseline assessment to through ongoing data assessment and feedback on a quarterly basis for a minimum of 1 year. Page 3
 for comprehensive implementation of regional emergency cardiac care systems.")
4 Great Rivers Columbus, OH Central, PA Philadelphia, PA Louisville, KY Midwest Detroit St. Louis East Wisconsin Central Indiana Founders New York City N. New Jersey Greater South East East Tennessee Tampa Western States Kern County, CA Hawaii South West Colorado (East Range) Houston San Antonio Oklahoma City Page 4
 Houston San Antonio Oklahoma City")

5 A Changing Landscape for Reperfusion Times & Processes: American College of Cardiology/American Heart Association/Society for Cardiovascular Angiography & Interventions Guidelines for Percutaneous Coronary Intervention In November 2011, the ACC/AHA/SCAI PCI guidelines underwent an important change with implications for the optimal design of regional STEMI systems. For STEMI patients presenting to non-pci centers who require inter-hospital transfer for primary PCI, prior guidelines recommended device activation within 90 minutes of initial presentation. The new guidelines extend this window from 90 minutes to 120 minutes of first medical contact. Of note, this new 120 minute window applies specifically and exclusively to transferred STEMI patients. For STEMI patients presenting directly to PCI-capable centers, the guidelines still call for reperfusion within 90 minutes of initial presentation. Nevertheless, this change in the guidelines reflects collective recognition that timely PCI is the preferred reperfusion strategy for STEMI. It additionally serves as an opportunity to design regional systems of care that extend primary PCI to a larger geographic region. This manual aims to provide specific strategic and tactical guidance on how to design and implement successful regional systems, particularly in the context of the new guidelines. Page 5

6 EMS: Dispatch Basic recommendations Establish a STEMI Plan: Coordinated regional plan focused on providing timely EMS response and transfer in collaboration with all hospitals and emergency medical systems in the region. Plan should require early notification from field to receiving hospitals for all STEMI patients, including communication with a physician capable of activating a reperfusion plan. EMS units may cross county lines when necessary for timely reperfusion. Train 911 operators to recognize acute cardiac symptoms and dispatch appropriate EMS resources with the ability to perform 12 lead ECG. Target total scene time of 15 minutes or less from from EMS arrival to departure includinga acquistion of ECG. Empower EMS units identifying STEMI patients to bypass the closest non-pci hospital and go directly to a primary PCI capable hospital, if: a. first medical contact to device deployment can be achieved within 90 minutes AND/OR b. reperfusion checklist shows contraindication to fibrinolysis Page 6

7 EMS: Initial Contact EMT Basic or Intermediate Provider Basic recommendations Extend 12 lead ECG acquisition to basic providers including EMT basic and first responders. Obtain ECG on all patients with typical acute coronary symptoms age 30 and older, patients with atypical symptoms (epigastric pain, arm pain, diaphoresis, shortness of breath) age 50 and older, and patients 80 years old with abdominal pain or nausea/vomiting. Obtain in-the-field ECG (to be interpreted by receiving physician after transmission, or by machine read with notification of receiving facility). Document symptom onset date and time. Goal scene time of < 15 minutes. Keep patient on ambulance stretcher for STEMI evaluation in hospitals that routinely transfer by same ambulance. EMS: Initial Contact EMT Paramedic Basic recommendations Train field personnel to diagnose ST-elevation MI by symptoms and 12 lead ECG. Document symptom onset date and time. Goal scene time of < 15 minutes. Obtain ECG on all patients with typical acute coronary symptoms age 30 and older, patients with atypical symptoms (epigastric pain, arm pain, diaphoresis, shortness of breath) age 50 and older, and patients 80 years old with abdominal pain or nausea/vomiting. Administer reperfusion checklist (review of potential contraindications to fibrinolysis) in situations where a patient may be taken to a hospital that uses fibrinolytic therapy. If patient is fibrinolytic ineligible, EMS notifies and diverts to a primary PCI capable hospital. Page 7
. Document symptom onset date and time.")
8 Keep patient on ambulance stretcher for STEMI evaluation in hospitals that routinely transfer by same ambulance. Provide early notification from the field to the receiving hospital for all STEMI patients, including communication with a physician capable of activating a reperfusion plan. Notification should include symptom onset, ECG findings, and reperfusion checklist as appropriate. Administer aspirin (4 x 81mg totaling 324mg chewed or a single adult 325 mg dose chewed) to chest pain patients suspected of having a STEMI, unless contraindicated or an adequate dose of immediate-release aspirin can be verified as taken. Leave copy of ECG tracing that includes acquisition time in receiving hospital. Make EMS run sheets immediately available to receiving hospitals. EMS run sheets should include all time elements that are necessary for quality assessment & improvement efforts Suggestions for making EMS data available: allow adequate time for EMS crews to complete run sheets before hospital departure provide paper or electronic format that is readily accessible to hospital personnel give hospital access to electronic EMS records send EMS records to hospital within 24 hours Essential run sheet data: EMS unit identification Scene arrival time Hospital pre-notification time Hospital arrival time Dispatch time Symptom onset time & description Scene departure time Medications, procedures, and complications in transfer Empower EMS units identifying STEMI patients to bypass the closest non-pci hospital and go directly to a primary PCI hospital capable of first medical contact to device deployment within 90 minutes (see flowchart Interventional Catheterization Laboratory Destination ). Advanced recommendations Equip EMS with same IV tubing as receiving hospitals. Establish and refine pre-hospital fibrinolysis system as appropriate for local resources and needs. Transmit 12-lead ECG if technically feasible, reliable, and if system exists for immediate ECG interpretation by a physician. This is particularly helpful for ECGs with uncertain EMS interpretations. Link EMS data to hospital data in an electronic format. Certify paramedics capable of STEMI diagnosis by ECG. Page 8
 to chest pain patients suspected of having a STEMI, unless contraindicated or an adequate dose of")
9 EMS: Inter-Hospital Transfer EMT Basic/Intermediate, Paramedic Basic recommendations Assign same priority to STEMI patient transfer process as to 911 calls or trauma. Use a local, paramedic-staffed EMS ambulance to transport hemodynamically stable STEMI patients when: 1) ambulance is available, and 2) drive time to destination hospital is less than 45 minutes. Keep patient on stretcher for myocardial infarction evaluation if inter-hospital transfer possible or likely. Establish transfer plan including preferred transport modality and backup transport modality. Transport directly to catheterization laboratory when laboratory is staffed and available. When possible, minimize or avoid continuous IV infusions such as nitroglycerin or heparin. Transfer protocol should focus on rapid transport to cath lab, rather than on pain relief with medications. Transfer patients to PCI hospital with same priority as trauma patients. Use structured approach to patient registration, bed availability, and accepting physician (use dummy registration numbers, accept all STEMI patients regardless of bed availability or diversion status, rely on single accepting physician on call 24 hours/7 days per week). When transporting a patient treated with fibrinolysis who has continued chest pain and/or < 50% ST resolution 60 to 90 minutes after the initiation of fibrinolysis, notify the receiving hospital about the potential need for rescue PCI. Fax hospital records to the receiving catheterization laboratory, so as not to delay patient pickup. Complete the EMTALA/COBRA/medical necessity of transfer form as soon as the decision to transfer is made Advanced life support units serving a hospital should be willing to transfer patient to any available PCI facility in cases where another transport option is not immediately available. Page 9



10 EMS: Chest Pain Suspected Cardiac Event ST Elevation-Myocardial Infarction (STEMI) is diagnosed by presence of both: Cardiac symptoms greater than 15 minutes and less than 12 hours ECG criteria of 1 mm ST-elevation in 2 or more leads or LBBB not known to be old in a patient with typical symptoms. There are three methods of ECG interpretation: 1) Paramedic read; ST segment elevation (left) and left bundle branch block (right) 2) Machine read (e.g. ***ACUTE MI SUSPECTED or >>> Acute MI); 3) ECG transmission with immediate recieving physician or medical control read. The preferred method of diagnosis is paramedic read. When available, transmit ECGs to the receiving hospital during EMS transport. Transmission is particularly helpful for ECG with a questionable diagnosis. PCI-capable facilities should agree to activate the cath lab based upon EMT-Paramedic read alone. Interventional Cardiac Catheterization Laboratory Facilities are designated by the EMS Director. Each facility should have: 1. 24/7 capability within 30 minutes of notification (including interventional cardiologist present at start of case). 2. Single call activation capability by trained paramedics and emergency physicians for which the cath lab is called in with initial notification of a definite STEMI patient. 3. Ability to accept any STEMI patient, regardless of bed availability. 4. On-site cardiac surgery. 5. Ongoing data collection in a regional or national myocardial infarction registry such as the ACTION-GWTG Registry and willingness to share these data in regional system reports. 6. Concurrent feedback to the EMS (including cardiologist to EMS call at the end of case, quarterly meetings to review cases, and data exchange with the EMS). Page 10

 age 50 and older, and patients 80 years old with abdominal pain or nausea/vomiting. Goal for STEMI patients is to Load and Go.")
11 EMS: Chest Pain Suspected Cardiac Event Operational and Clinical Pearls Obtain ECG on all patients with typical acute coronary symptoms age 30 and older, all patients with atypical symptoms (epigastric pain, arm pain, diaphoresis, shortness of breath) age 50 and older, and patients 80 years old with abdominal pain or nausea/vomiting. Goal for STEMI patients is to Load and Go. Document any known allergies and their severity: morphine, aspirin, IV contrast dye Exam: Mental Status, Skin, Neck, Lung, Heart, Abdomen, Back, Extremities, Neurologic. Avoid nitroglycerin in any patient who has used Viagra or Levitra in the past 24 hours or Cialis in the past 36 hours due to potential for severe hypotension. If patient has taken nitroglycerin without relief, consider medication s potency. Is it past expiration date? If positive ECG changes, establish a second IV (left arm is preferred) while en route to the hospital. Monitor for hypotension after administration of nitroglycerin and morphine. Patients with chest pain but without ST-segment elevation on their ECG should be transported to the hospital of their choice. Only STEMI patients should be encouraged to go directly to a facility capable of emergency PCI. Diabetic and geriatric STEMI patients often have atypical pain, or only generalized complaints. Document 12-lead ECG and transmission status using "12-lead ECG" procedure in the call reporting system. Cocaine can cause vasospasm, non-stemi, or STEMI. ECG read remains critically important for diagnosis! Page 11


12 EMS: Chest Pain Suspected Cardiac Event Chest Pain Suspicious for a Cardiac Event Destination: Interventional Cardiac Catheterization-Equipped Facility Page 12


13 EMS: Diversion from non-pci hospital to PCI hospital Develop diversion plans in collaboration with local EMS, medical, and hospital leadership. Consider EMS diversion from a non-pci hospital to a PCI hospital in two circumstances: 1. Diversion for primary PCI - The EMS unit can diagnose a STEMI, directly activate an interventional cardiac catheterization facility, and achieve a first medical contact to device deployment time within 90 minutes on a consistent basis. 2. Fibrinolytic ineligible - The EMS unit can diagnoses a STEMI, directly activate an interventional cardiac catheterization facility, and the patient is ineligible for fibrinolysis according to the reperfusion checklist. Page 13


14 Page 14 Diversion for Fibrinolytic Ineligible Patients (For a system that locally designates fibrinolysis as primary reperfusion method)

15 EMS: Air Medical Transfer Basic recommendations Helicopter crews should never be pressured to achieve faster transport times. Safe transport must remain their primary mission. Helicopter transport is most suitable for transporting patients to an interventional cardiac catheterization facility when first medical contact to device deployment can be safely achieved within 120 minutes on a consistent basis. This reflects a change in the ACC/AHA Guidelines in November of Helicopter transport is also suitable for transporting hemodynamically unstable patients. For the transport of hemodynamically stable patients with less than 50 minute travel times, local EMS ambulance staffed by paramedics is generally faster. Deployment of helicopter transport can be done via one of four strategies: Page 15 1) As the primary method of inter-hospital transfer for primary PCI 2) As a reserve method of inter-hospital transfer when local EMS is not available 3) As a reserve method of inter-hospital transfer when patients are fibrinolytic ineligible, fail to reperfuse after fibrinolysis, or are hemodynamically unstable 4) As a primary method of transport from a STEMI medical scene or designated helicopter landing zone when ground transport is not feasible or too long. Hospitals and Emergency Medical Systems that rely on helicopter transport must have a suitable back-up plan in place when helicopter transport is not available. Back up plans may include mutual aid agreements with other air medical services, ground transportation, and/or diversion to a closer hospital. If first medical contact to device cannot be achieved within 120 minutes using alternate transportation modalities, fibrinolysis should be considered. STEMI patients transported from the field to a helicopter landing zone adjacent to a hospital do not require medical evaluation by that hospital unless deemed necessary by the EMS crew. When helicopter transport to PCI center is the primary strategy, referring hospital should designate a landing zone as close to its emergency department as possible. Remote landing zones should generally be avoided.


16 EMS: Air Medical Transfer Immediately activate helicopter transport during initial communication with the receiving hospital regarding the need for reperfusion. Medical Helicopter Transfer: STEMI Medical Scene For hemodynamically stable patients, critical care nurses and paramedics should minimize time on the ground with an overall goal of 10 minute package and load time. When possible, minimize or avoid continuous IV infusions such as nitroglycerine or heparin. Bolus dosing is simpler and faster. When the catheterization laboratory has adequate staff, patients should be transported directly to the laboratory. Stop in the PCI hospital's emergency department only if catheterization lab staff has not arrived. When transporting a patient treated with fibrinolysis who has continued chest pain and/or less than 50% ST resolution 60 to 90 minutes after the initiation of fibrinolysis, notify the receiving hospital about the potential need for rescue PCI. Air medical services should establish mutual aid policies with neighboring services for STEMI patients that include transport of patients to the closest interventional cardiac catheterization facility upon request. For emergency medical services that use air medical transport, institute protocols that include: criteria for air medical activation, communication, helicopter landing zones, patient packaging, alternate transportation plans, training, and ongoing monitoring and feedback. Honor patient requests for a specific air medical service when the circumstances will neither jeopardize patient safety nor delay patient care. Page 16

17 EMS: Air Medical Transfer Air Medical Policies: Air medical helicopter may be activated for ST elevation myocardial infarction (STEMI) requiring transport to an interventional cardiac catheterization laboratory facility in the following situations: a. Air medical transport is part of the established EMS protocol for STEMI and first medical contact to device can be achieved within 120 minutes. b. Ground transport time to interventional hospital greater than 50 minutes. c. Ground transport not available. d. Use of local ground ambulance leaves local community with inadequate ambulance coverage. EMS units will directly communicate with and activate Air Medical transport and Interventional Hospital. If direct communication not possible, the dispatch center will relay communications. Information given to Air Medical/Interventional Hospital: a. EMT name and EMS unit. b. Designation of patient as code STEMI protocol. c. Type and duration of cardiac symptoms and location and height of ST segment elevation on ECG. d. Demographics including height, weight, age, gender, date of birth. e. Vital signs (blood pressure, pulse, respiratory rate). f. Major complications such as cardiac arrest or cardiogenic shock. g. Landing zone location. h. Estimated arrival time to landing zone. k. How to contact on scene EMS personnel and landing zone officer. Air medical helicopters should generally transport STEMI patients to closest interventional cardiac catheterization laboratory facility (defined by the EMS director to include 24/7 capability within 30 minutes of notification, interventional cardiologist present at start of procedure, single call activation, accept patients regardless of bed availability, on-site cardiac surgery, and ongoing data monitoring and feedback). Page 17

18 EMS personnel will honor a patient request for a specific air medical service when the circumstances will not jeopardize patient safety or delay patient care. If a helicopter is not immediately available, air medical dispatch will arrange air medical transport through an alternate provider. If air medical transport is not feasible due to weather, protocol established alternative method of ground transport will be activated. Air medical transport is not appropriate for do not resuscitate (DNR) patients. If as part of the EMS protocol, EMS activates helicopter evacuation of an individual with a potential emergency medical condition (EMC), the hospital that has the helipad does not have an EMTALA obligation if they are not the recipient hospital. The use of a hospital s helipad by local ambulance services or other hospitals for the transport of individuals to tertiary hospitals does not trigger an EMTALA obligation for the hospital that has the helipad on its property, unless a request is made by EMS personnel, the individual or a legally responsible person acting on the individual s behalf for the examination or treatment of an EMC. (CMS Guidance Document March 21, 2008, Hospitals Revised State Operations Manual Appendix V EMTALA Tag A-2406/C-2406 Interpretive Guidelines (a)) Landing Zone (LZ) requirements Minimum 60 x 60 feet for day operations, 100 x 100 feet for night operations. < 10% slope. Firm ground or pavement. Minimize obstacles such as tall trees, power lines, poles, etc. Ensure two approach/departure paths to landing zone. Identify contact frequency and LZ commander. Do not illuminate the LZ with flares. Instead, use truck lights or LZ light markers for night operations. Patient Packaging Oxygen Aspirin, if not already taken by the patient. Two IV s if possible, with left arm preference (Transport should NOT be delayed for second IV). Remove as much clothing as possible. Advise air medical dispatch of the patient s actual or estimated weight. Defibrillator pads (if compatible with air medical defibrillator). Three ECG electrode patches. Page 18
 patients.")
19 Transferring (Non-PCI) Hospitals Basic recommendations Senior management should commit to optimal STEMI care and demonstrate this commitment through provision of necessary resources to establish a successful system. Establish a STEMI team composed of emergency department, cardiology, emergency transport, communications, quality assurance, nursing, and senior management involved in acute myocardial infarction care. Hold periodic team meetings to review and revise system. Establish a predetermined, institution-specific, written protocol for rapid reperfusion (see Reperfusion Regimens, A: Primary PCI or B: Fibrinolysis) agreed upon by all cardiology and emergency department physicians and staff that includes: Page 19 Emergency physician on duty activates the reperfusion plan according to established local guidelines/care pathways. Perform ECG in all patients presenting to ED with potential STEMI symptoms within 10 minutes, regardless of room or nurse availability (all patients age 30 and older with typical symptoms of acute coronary syndrome, all patients age 50 and older with atypical symptoms including epigastric pain, arm pain, diaphoresis, shortness of breath, and patients 80 years old with abdominal pain or nausea/vomiting). Promptly identify patients requiring ECG through nurse interview prior to registration ( nurse first ) or through training of registration personnel. Specify system for rapid ECG acquisition including having ECG equipment in the ED and specifying a location that affords prompt access and adequate patient privacy. Obtain EMS records and forward to the PCI facility. Reperfusion checklist for hospitals with a predetermined plan for fibrinolysis. Door to needle time within 30 minutes for hospitals with a predetermined plan for fibrinolysis. After fibrinolysis, non-pci centers should then aim to transfer patients to a PCI center within 3-24 hours as part of a pharmaco-invasive approach to STEMI care. Door in door out time within 30 minutes for hospitals with a predetermined plan for transfer for PCI, and for patients ineligible for fibrinolysis or in cardiogenic shock. Aim to achieve first medical contact to device deployment within 120 minutes. While the updated ACC/AHA/SCAI PCI guidelines allow for 120 minutes from first medical contact to device deployment, 90 minutes should remain a systems goal.

20 Transferring (Non-PCI) Hospitals Standard pharmacologic regimen for all STEMI patients agreed upon by all cardiology and emergency department physicians. Fibrinolytic agent stored in the emergency department and the intensive care unit. Ability to reconstitute and administer fibrinolytic in emergency department. If contraindication to fibrinolysis or uncertain diagnosis, expedited transfer plan to primary PCI facility. Ongoing training and assessment program. Data collection and rapid feedback within 24 hours to all care providers in the STEMI chain of care. Establish transfer plan including preferred transport modality and backup transport modality. Patient registration should be treated in similar fashion to trauma patients with the ability to fast-track critical labs, such as creatinine and PT/INR. Minimize ED waiting time. Provide reperfusion or rapid transfer as soon as possible. Collect data and provide feedback to emergency department and medical staff regarding performance and quality of reperfusion of STEMI patients. Participate in a regional or national myocardial infarction registry. Use improvement science to increase quality of care (e.g. process mapping, team organization, multidisciplinary team work, cause analysis, report cards, measures of dispersion, continuous quality improvement, and data collection, measurement, and feedback). Arrange for transport of STEMI patient. Page 20

21 PCI Hospitals Basic recommendations Senior management should commit to optimal STEMI care and demonstrate this commitment through provision of necessary resources to establish a successful system Establish a STEMI team composed of ED, cardiology, emergency transport, ICU, cardiac cath lab communications, quality assurance, and senior management involved in acute myocardial infarction care. Hold monthly team meetings to review and revise system. Designate a STEMI Coordinator to work closely with physicians, program organizers, and referring hospitals. See job description in appendix. Establish a predetermined, institution-specific, written protocol for rapid primary PCI agreed upon by all cardiology and ED physicians and staff. Advanced recommendation First door to device deployment goal < 60 minutes. Emergency Department ED physician on duty activates reperfusion plan according to established local guidelines/care pathways. Perform ECG in all patients presenting to ED with STEMI symptoms within 10 minutes, regardless of room or nurse availability (all patients with typical acute coronary symptoms age 30 and older, patients with atypical symptoms including epigastric pain, arm pain, diaphoresis, shortness of breath, age 50 and older, and patients 80 years old with abdominal pain or nausea/vomiting). Promptly identify patients requiring ECG through nurse interview prior to registration ( nurse first ) or through training of registration personnel. Specify system for rapidly ECG acquisition including having ECG equipment in the ED and specifying a location that affords prompt access and adequate patient privacy. Door to device deployment time within 90 minutes. Overall system goal of first medical contact to device deployment within 90 minutes. Employ a standard pharmacologic regimen for all STEMI patients agreed upon by all cardiology and emergency department physicians. Ongoing training and assessment program. Page 21
22 PCI Hospitals Catheterization Laboratory Authorize emergency physicians to activate the catheterization laboratory. Authorize qualified paramedics to activate the catheterization laboratory. Provide a single telephone number that is available 24 hours per day/7 days per week to activate primary PCI team and initiate transfer of patients from outside hospitals. This call may be answered by a non-interventional cardiologist. Immediately accept all patients regardless of bed availability or diversion status. Page 22 When beds are not available, employ pre-determined protocols: 1) Care by the cath lab, ED, or ICU staff 2) House the patient in an emergency, procedure, or recovery room until an appropriate hospital bed is available. Establish a daily primary PCI operator schedule that is coordinated between all cardiologists, and involves a single rotating physician. Interventional cardiologist is present and directs entire procedure from cath lab arrival. Cath lab team in lab & ready in 30 minutes on 24 hours/7 days per week basis. Employ strategies that accelerate readiness: Provide sleeping quarters close to the hospital Designate protected parking zone for STEMI team Require on-call staff to stay close enough to hospital to ensure readiness in < 30 minutes. Establish a back-up reperfusion plan to be employed when cath lab(s) are down or filled with cases that cannot be delayed or moved. Back-up plans may include rapid activation of an additional cath lab team, diversion of second patient to a nearby primary PCI hospital or rapid fibrinolysis (first medical contact to needle within 30 minutes).
23 PCI Hospitals Receive referral transfers directly from EMS transport to lab when the lab is staffed and available. If the lab is not yet available upon patient arrival to hospital, prep patient in ED or ICU. Establish cross-training and multi-disciplinary teams to expedite cath lab readiness and patient care. Teams may include ICU staff and/or ED staff. Update history and physical on transfer to catheterization table. Establish a dedicated fax machine for receiving medical records from Non-PCI Hospitals. Provide prompt data feedback immediately after procedures, including a call by the interventional cardiologist to the referring ED physician or EMT. Generate an the day following primary PCI to all personnel involved in care outlining performance including the following times (call to decision, decision to arrival in cath lab, arrival in cath lab to device deployment), catheterization results, false activations, deaths in transfer, and systematic delays. Collect data systematically & provide ongoing feedback to ED, cath lab, and transferring facility regarding primary PCI performance and quality. Focus attention on performance variation, rather than average performance. Expedite device time when possible/appropriate: use a guide catheter to initially image the suspected infarct-related artery, delay ventriculography until after coronary flow is restored Patient registration should be treated in similar fashion to trauma patients with the ability to fast-track critical labs, such as creatinine and PT/INR. Minimize ED waiting time. Provide reperfusion or rapid transfer as soon as possible. Advanced recommendations Provide 24 hours per day/7 days per week telephone ( hotline ) and fax support of reperfusion decision for referring hospitals by a cardiologist on call. Record and routinely review calls to the cath lab referral line. Use improvement science to increase quality of care (e.g. process mapping, team organization, multidisciplinary team work, cause analysis, report cards, measures of dispersion, continuous quality improvement, and data collection, measurement, and feedback). Page 23
24 Cardiogenic Shock Cardiogenic shock is defined as inadequate organ perfusion due to low heart output. Approximately 9% of STEMI patients develop cardiogenic shock. Early recognition of shock in STEMI patients is essential, as is implementation of advanced supportive therapies. SHOCK - FAST FACTS * STEMI patients with shock have exceedingly high in-hospital mortality rates. One in three dies before hospital discharge. * Early recognition and revascularization has been shown to lower mortality in a randomized controlled trial. 1 * Of patients with acute MI complicated by shock, one-third present in shock, while two-thirds develop shock during their hospital course. This requires both early and ongoing vigilance on the part of the entire STEMI team, from EMS to the post-pci care team. EARLY INDICATORS OF SHOCK in Acute MI Hypotension (systolic blood pressure 90 mmhg) Narrow pulse pressure (SBP to DBP difference of < 20 mm Hg) Page 24 INDICATORS OF PROGRESSIVE SHOCK in Acute MI Low urine output Altered mental status, confusion Respiratory distress/hypoxia from pulmonary edema Cool extremities Rising creatinine Lactic and metabolic acidosis Characteristic pulmonary artery catheter readings Low cardiac index ( 2.0 L/min/m 2 ) High pulmonary capillary wedge pressure ( mm Hg) High systemic vascular resistance ( 1200 dynes cm sec)
25 Cardiogenic Shock The ACC/AHA STEMI guidelines make two specific recommendations for cardiogenic shock patients: 1) Revascularize: Perform primary PCI in patients with STEMI who develop severe heart failure or cardiogenic shock as soon as possible, irrespective of time delay. 2) Support hemodynamics: Use a hemodynamic support device (table on next page) for STEMI patients with cardiogenic shock who do not quickly stabilize with initial therapies. In addition, we recommend aggressive hemodynamic management in an ICU setting. HEMODYNAMIC SUPPORT DEVICES Intra-Aortic Balloon Pump (IABP) Impella Tandem Heart ECMO Page 25
26 Cardiogenic Shock Device Availability Insertion site & size (1 French = 1/3 mm) Most Femoral artery hospitals with cath 7-8 French lab facilities Intra-aortic balloon pump (IABP) - balloon in aorta inflates in diastole, augmenting coronary perfusion; deflates in systole, reducing afterload Approx. Advantages / set-up time disadvantages 5 mins Widely available Can be placed in femoral access site after PCI Portable for interhospital transport Limited hemodynamic support Impella Pump - sits across aortic valve; pulls blood from left ventricle, expels blood into ascending aorta Select hospitals Femoral artery 9 French 20+ mins Can be placed in femoral access site after PCI Portable for inter hospital transport Tandem Heart - pulls blood from the left atrium and returns blood to systemic arterial circulation Select hospitals Femoral artery Femoral vein French 20+ mins Placement of inlet catheter across atrial septum into left atrium requires greater skill ECMO (extra-corporeal membrane oxygenator) - when used in shock/stemi, pulls blood from venous circulation and returns blood to arterial circulation; bypasses both lungs & heart Hospitals with surgery on-site Femoral artery Femoral vein French 30+ mins Provides complete cardiopulmonary support Requires cardiac surgery expertise & advanced ICU capabilities Page 26
27 Basic recommendations Equip ambulances responding to potential STEMI calls with ECG machines & ECG-trained providers. Assign same priority to STEMI patient reperfusion ("STEMI medical scene") as to 911 calls and trauma calls. Transfer patients across county lines to the nearest facility for primary PCI if reperfusion cannot be performed in the county. If vehicle transfer to remote counties is not feasible, consider alternatives including cross-coverage of county by adjacent county EMS, transfer of patients to county line for transfer to receiving ambulance, or establishment of medical scene helicopter transport protocols. Helicopter transport protocols should include EMS and ED protocols capable of launching helicopters to medical scenes and establishment of helicopter landing zones (LZ). Patients transported to LZs adjacent to hospitals should not require medical evaluation by that hospital unless deemed necessary by the EMS crew. Support continuing education programs for STEMI care, including 12 lead ECG training. Arrange for EMS IV tubing that matches that of receiving hospitals. Make EMS run sheets immediately available to receiving hospitals. Provide adequate time for EMS crews to complete run sheets before hospital departure and provide paper or electronic format that is readily accessible to hospital personnel. Leave copy of ECG tracing that includes acquisition time. Essential run sheet data should include: EMS unit identification dispatch time scene arrival time symptom onset time description of symptoms hospital pre-notification time scene departure time hospital arrival time medications and procedures complications in transfer Advanced recommendations Provide all first responders with AEDs. Respond to all potential ST-elevation myocardial infarction patients with ACLS providers. Selectively provide facilities and training for pre-hospital fibrinolysis. Provide equipment on ACLS response vehicle to transmit ECGs to predetermined medical control facility and/or receiving hospital. Page 27
28 State Basic recommendations Implement state and local policies that support treatment of all STEMI patients, including: 1) Uniform, statewide implementation of EMS care of STEMI care according to the EMSPIC Acute Cardiac Care Toolkit. This implementation should include training, data support, and funding. 2) Provide regional STEMI care coordinators similar to that of the North Carolina Trauma Regional Advisory Committee (RAC) system. 3) Extend performance of ECGs to all EMT levels (verification should remain with EMT-P). Require private ambulance and helicopter providers to meet regional standards and fully participate in regional systems of STEMI care before responding to potential STEMI calls or transporting STEMI patients. Direct existing agencies with data collection capability to regularly measure, monitor, and provide feedback regarding STEMI care. Feature statewide STEMI education for residents, communities, emergency medical services, physicians, and hospitals. Advanced recommendations Enact policies that eliminate financial and administrative barriers (actual or perceived) for patients seeking emergency care for a possible myocardial infarction, even if subsequent medical evaluation is negative. Link state, EMS, hospital, and vitals status data, making patient level data available to all entities participating in regional STEMI systems. Update these data and make it available on at least a quarterly basis. Page 28
29 Federal Basic recommendations Use federal resources to promote the establishment of national standards whereby every person suffering a STEMI is treated in a systematic, coordinated manner that includes diagnosis within 10 minutes of presentation, early notification and direct activation of coronary reperfusion by EMS & ED personnel and provisions for rapid PCI by regional centers. These standards should be established promptly with similar priority to the trauma system, given that three to four times as many Americans die from myocardial infarctions each year compared to motor vehicle accidents. Establish designated leadership within the Office of Emergency Medical Services or other pertinent agency within the Department of Health & Human Services for regional medical scene care that includes STEMI care. Develop and support regional systems of STEMI care. Remove financial barriers related to optimal emergency ST-elevation MI care for patients and hospitals. 1) Enact policies that eliminate financial and administrative barriers (actual or perceived) for patients seeking emergency care for a possible STEMI, even if subsequent medical evaluation is negative. 2) Include STEMI patients transferred from the ED to another hospital in calculations of Medicare hospital case-mix adjustment. Add reperfusion rate for eligible patients to current reperfusion quality measures. Establish a uniform national definition of first medical contact that can be applied at the earliest possible point in the evolution of an ST-elevation myocardial infarction. Provide adequate funding and direction for the infrastructure required for STEMI systems including specification of regional protocols pertinent to urban or rural settings, establishment of uniform algorithms for ECG transmission and archiving, and expansion of the National Emergency Medical System Information System (NEMSIS). Expand NEMSIS to include elements pertinent to STEMI care. Develop an interface for efficient electronic exchange of corresponding hospital data. Deploy NEMSIS uniformly in all emergency medical systems. Page 29
30 Basic recommendations Remove financial barriers related to optimal emergency ST-elevation MI care for patients and hospitals. Enact policies that eliminate financial and administrative barriers (actual or perceived) for patients seeking emergency care for a possible STEMI, even if subsequent medical evaluation is negative Provide adequate reimbursement to fund regional emergency responses to STEMI that takes into account: 1) EMS funding 2) Rural and critical access hospitals 3) Inter-hospital transport 4) 24 hours per day/7 days per week operations Add reperfusion rate for eligible patients to current reperfusion quality measures. Page 30
31 Preferred if able to meet time goals of PCI within 90 minutes (direct presenters) Or 120 minutes (transfers) of 1st medical contact and For all patients who are fibrinolysis ineligible or with cardiogenic shock (To be used with institution-specific standing orders/protocols for STEMI patients) Eligible Patients Within 12 hours of symptom onset. ST-segment elevation in 2 or more contiguous leads 1mm or presumed new left bundle branch block. Primary PCI is also the best option for: 1) Cardiogenic Shock; Killip class III. 2) Possible ST-elevation MI but uncertain of diagnosis. 3) Contraindication to fibrinolysis. Goal is first device deployment with 90 minutes of first medical contact*. For patients requiring inter-hospital transfer, the acceptable window is now 120 minutes. *(EMS scene arrival or ED registration arrival). ED physician makes the decision about need for primary PCI if possible. Cardiology consultation should be limited to situations of uncertainty. Activate catheterization laboratory immediately using single call activation. Complete EMTALA form as a priority. Fax patient records including ECG to receiving hospital while patient in transfer. Use continuous IV infusions only if required for stability during transfer. Page 31
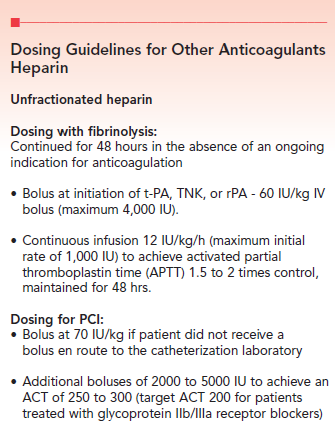
32 ACCF/AHA/SCAI Class I recommended Anticoagulant & Antiplatelet Pharmacotherapy 1) Heparin bolus at 70 IU/kg IV. No maintenance infusion during transfer. OR Bivalirudin bolus 0.75 mg/kg IV (if prior UFH administered, start 30 minutes after last bolus, or in all cases before PCI regardless of the ACT); infusion 1.75 mg/kg/h, not titrated to ACT; terminated at procedure s end unless prolonged anti-thrombin is deemed clinically necessary by a physician. 2) Aspirin (4 x 81mg totaling 324mg chewed or a single adult 325 mg dose chewed) 3) Clopidogrel loading dose 600 mg PO times 1 dose, followed by 75 to 150 mg per day for seven days, followed by 75 mg per day. Clopidogrel administered on presentation. OR Prasugrel loading dose 60 mg PO times 1 dose, followed by 10 mg per day.* OR Ticagrelor loading dose 180mg PO times 1 does, followed by 90mg PO BID. (* Warnings and precaution with prasugrel: Do not use in patients with active bleeding or history of TIA or stroke. Caution for patients at high risk for bleeding, including elderly (75 years of age or older), low body weight (less than 60 kg or 132 lbs.), urgent need for surgery including coronary artery bypass grafting, propensity to bleed, and with medications that increase bleeding risk including oral anticoagulation, chronic NSAIDs, and fibrinolytic therapy.) PRN Medications 1) Nitroglycerin paste 1 to 2 inches topically PRN chest pain. 2) Morphine Sulfate 2-10mg IV (in divided doses) for chest pain unrelieved by Nitroglycerin PRN. Page 32
33 (To be used with institution specific standing orders/protocols for STEMI patients) Eligible Patients Within 12 hours of symptom onset. ST-segment elevation in 2 or more contiguous leads 1mm or presumed new left bundle branch block. Absence of contraindications (see below). Goal is door to needle time within 30 minutes. Fibrinolysis Regimens 1) Tenecteplase (TNK) regimen Single IV bolus over 5 seconds Use TNK dose chart (right) to determine dose. Patient weight kg Patient-specific dose mg (not to exceed 50mg) OR 2) Reteplase (rpa) regimen 10 units IV over 2 minutes given twice at 30-minute intervals. In nurses notes and medication administration record, please note EXACT TIME of fibrinolytic administration, and obtain ECG 30 minutes after fibrinolytic administered. Page 33
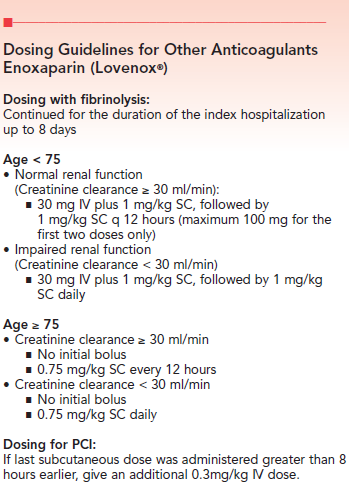
34 Anticoagulant & Antiplatelet Medications 1) Anticoagulation with Heparin or Enoxaparin. (Enoxaparin generally preferred) 2) Aspirin (4 x 81mg totaling 324mg chewed or a single adult 325 mg dose chewed) 3) Clopidogrel 300 mg PO loading dose followed by 75 mg per day. If age over 75, omit loading dose. Rescue PCI Strategy for Fibrinolysis Initiate urgent rescue PCI for failed reperfusion, defined by less than 50 percent ST-segment resolution within 60 to 90 minutes of the initiation of fibrinolysis (with or without chest pain). Contraindications to Fibrinolysis ABSOLUTE contraindications Any prior intracranial hemorrhage Suspected aortic dissection Known structural cerebral vascular lesion (AVM, for e.g.) Active bleeding or bleeding diathesis (excluding menses) Significant closed head or facial trauma within 3 months Known intracranial neoplasm (primary or metastatic) Ischemic stroke within 3 months EXCEPT acute ischemic stroke within 3 hours RELATIVE contraindications History of chronic severe, poorly controlled hypertension Severe hypertension on presentation (systolic blood pressure greater than 180 mm Hg or diastolic blood pressure greater than 110 mm Hg) History of prior ischemic stroke greater than 3 months, dementia, or known intracranial pathology not covered in contraindications Traumatic or prolonged (greater than 10 minutes) CPR or major surgery (less than 3 weeks) Recent (within 2 to 4 weeks) internal bleeding Non-compressible vascular punctures Current pregnancy Page 34
")
35 Page 35 If YES, proceed to Step TWO (next page)

36 Page 36

37 Page 37
.")
38 Bivalirudin (Angiomax ) Dosing for PCI: Give bolus of 0.75 mg/kg (TBW) IV prior to PCI. This should be followed by continuous infusion of 1.75 mg/kg/h (Continuous infusion dosing for patients with renal insufficiency: See below). Infusion should be terminated at the end of the procedure OR extended up to 4 hours postprocedure at physician s discretion. If prior UFH administered, start bivalirudin 30 minutes after last bolus, or in all cases before PCI regardless of the ACT. Measure ACT 5 min after initial bolus and give additional bolus of 0.3 mg/kg if needed. Terminate infusion at procedure s end. If extended antithrombin therapy is deemed clinically necessary, a 0.2 mg/kg/h infusion may be administered. CrCl (ml/min) & Intra-Procedure Infusion Dose (mg/kg/h) 30 ml/min No change < 30 ml/min 1.0 mg/kg/h Dialysis dependent 0.25 mg/kg/h Page 38
: Routine pre-catheterization laboratory (e.g., ambulance or emergency department) administration of GP IIb/IIIa inhibitors as part of an upstream strategy for patients with STEMI undergoing PCI is not beneficial.")
39 Glycoprotein IIb/IIIa Receptor Blockers Abciximab (Reopro ) Eptifibatide (Integrillin ) ***The updated 2011 ACC/AHA/SCAI PCI guidelines state that the use of this class of medications in STEMI is no longer routinely recommended.*** Their use in STEMI is now considered Class III (no benefit): Routine pre-catheterization laboratory (e.g., ambulance or emergency department) administration of GP IIb/IIIa inhibitors as part of an upstream strategy for patients with STEMI undergoing PCI is not beneficial. - ACC/AHA/SCAI PCI Guidelines, 2011 Page 39
40 Page 40

41 Clopidogrel Dosing for PCI: Loading dose 600 mg PO times 1 dose (300mg if within 24 hours of having received fibrinolysis), followed by 75 mg per day. Dosing with fibrinolysis: Clopidogrel 300 mg PO loading dose followed by 75 mg per day. If age over 75, omit loading dose. Prasugrel Dosing for PCI: Loading dose 60 mg PO times 1 dose, followed by 10 mg per day.* Dosing with fibrinolysis: Do not use within 24 hours of fibrin-specific fibrinolytic therapy or within 48 hours of non fibrin-specific fibrinolytic therapy. Ticagrelor Dosing for PCI: Loading dose 180 mg PO times 1 dose, followed by 90 mg BID. *Warnings and precaution with Prasugrel: Do not use in patients with active bleeding or history of TIA or stroke. Caution for patients at high risk for bleeding, including elderly (75 years of age or older), low body weight (less than 60 kg or 132 lbs.), urgent need for surgery including coronary artery bypass grafting, propensity to bleed, and with medications that increase bleeding risk including oral anticoagulation, chronic NSAIDs, and fibrinolytic therapy. Page 41
42 Page 42

43 Page 43
44 Automatic external defibrillator (AED) device that can be used by anyone with a minimal amount of training to shock (or defibrillate) a patient whose heart has stopped. Cardiogenic shock inadequate organ perfusion due to low heart output. This condition is frequently a precursor to death, and can be recognized by the presence of hypotension (systolic blood pressure of 90 mmhg or less) in the setting of a myocardial infarction. Contraindication a specific situation in which a drug or procedure should NOT be used, because it may be more harmful than beneficial to the patient. Coronary arteries arteries that originate in the aorta immediately above the heart that supply oxygenated blood to the muscular tissue of the heart. Diversion plan an emergency medical service protocol to divert patients with ST elevation myocardial infarction from the closest non-pci hospital to a PCI capable hospital. Diversion protocols are particularly useful when patients have a contraindication to fibrinolysis, or first medical contact to device deployment at the PCI hospital can be achieved within 90 minutes on a consistent basis. Door to Needle Time the time elapsed from hospital arrival or emergency department registration arrival to the initial infusion of fibrinolytic medication. Electrocardiogram (ECG) a recorded tracing of the electrical activity of the heart. Emergency medical service (EMS) a system of health care professionals, facilities, and equipment providing pre-hospital emergency care. Emergency medical technician (EMT) an emergency responder trained to provide pre-hospital emergency medical services (EMS) to the critically ill and injured. Emergency Medical Treatment and Active Labor Act (EMTALA) a statute that governs when and how a patient may be (1) refused treatment or (2) transferred from one hospital to another when in unstable condition. The EMTALA was passed as part of the Comprehensive Omnibus Budget Reconciliation Act of 1986, and is sometimes referred to as "the COBRA law." Fibrinolysis the breakdown of fibrin, usually by the enzymatic action of plasmin. Fibrin is a protein necessary for blood clotting that forms a web-like mesh that traps red blood cells and platelets and holds clots together. In the case of myocardial infarction, the administration of drugs that facilitate fibrin breakdown is referred to as fibrinolysis. Fibrinolytic an agent used to facilitate fibrin breakdown by activating plasminogen. Page 44
45 First medical contact to device time the time elapsed from the first medical contact (i.e. EMS scene arrival or ED registration arrival) to the first device deployment in the coronary artery. Killip class a system for estimating the risk of death with myocardial infarction according to four classifications: Class 1: Absence of rales over the lung fields and absence of S3 Class 2: Rales over 50% or less of the lung fields or the presence of an S3 Class 3: Rales over more than 50% of the lung fields Class 4: Cardiogenic shock. Left bundle branch block (LBBB) an electrocardiographic pattern in which the left bundle fails to conduct to the left ventricle, manifested by deep S waves in lead V1, predominant R waves in lead V6 and I, and a wide QRS complex. ST-segment elevation with a myocardial infarction cannot be reliably detected in the setting of left bundle branch block. Myocardial infarction (MI) sudden onset of myocardial necrosis due to the formation of a blood clot in the coronary arterial system obstructing arterial blood flow to the area of cardiac muscle supplied by that artery. This condition is often manifested by symptoms of coronary insufficiency and electrocardiographic changes of ST-segment elevation. (Commonly known as a heart attack.) Percutaneous coronary intervention (PCI) a procedure used to open or widen narrowed or blocked blood vessels supplying the heart. The blood vessels are accessed through the skin over the leg (femoral) or arm (radial or brachial) arteries. A thin catheter is advanced over a soft-tipped guide-wire through the arterial tree to the base of the heart where the coronary arteries arise. A smaller guide-wire is then advanced into the coronary artery and across the blockage, followed by balloon-dilation catheters, stents, and other artery opening devices as needed. Primary percutaneous coronary intervention the use of percutaneous coronary intervention to open an occluded coronary artery in the setting of an ST-elevation myocardial infarction. Reperfusion the restoration of blood flow to an organ or tissue that has had its blood supply cut off, as after a myocardial infarction. Rescue PCI- in the event that fibrinolysis fails to open the occluded coronary artery; the artery is opened by percutaneous coronary intervention. Approximately 25% of coronary arteries fail to open with fibrinolysis. Patients whose arteries fail to open typically have persistent chest pain and ST-segment elevation more than 60 minutes after fibrinolysis is administered. ST-Elevation myocardial infarction (STEMI) a myocardial infarction for which the ECG shows ST-segment elevation, usually associated with a recently closed coronary artery. Patients suffering this type of myocardial infarction are more likely to survive if their coronary artery is opened within 12 hours of onset. Page 45
46 Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA, Hand M, Hochman JS, Krumholz HM, Kushner FG, Lamas GA, Mullany CJ, Ornato JP, Pearle DL, Sloan MA, Smith SC Jr. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: executive summary: a report of the ACC/AHA Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines on the Management of Patients With Acute Myocardial Infarction). Circulation. 2004;110: Antman EM, Hand M, Armstrong PW, Bates ER, Green LA, Halasyamani, LK, Hochman J S, Krumholz HM, Lamas GA, Mullany C J, Pearle DL, Sloan M A, Smith, SC focused update of the ACC/AHA 2004 Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Group to Review New Evidence and Update the ACC/AHA 2004 Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction). Circulation. 2008;117: Bhatt DL. Prasugrel in clinical practice. N. Engl. J. Med. 2009;361: Dauerman HL, Sobel BE. Toward a comprehensive approach to pharmacoinvasive therapy for patients with st segment elevation acute myocardial infarction. J. Thromb. Thrombolysis Glickman SW, Shofer FS, Wu MC, Scholer MJ, Ndubuizu A, Peterson ED, Granger CB, Cairns CB, Glickman LT. Development and validation of a prioritization rule for obtaining an immediate 12-lead electrocardiogram in the emergency department to identify st-elevation myocardial infarction. Am. Heart J. 2012;163: Graff L, Palmer AC, LaMonica P, Wolf S. Rule of rapid ECG Triage of Patients for a Rapid (5-Minute) Electrocardiogram: A Rule Based on Presenting Chief Complaints. Annals of Emergency Medicine. 2000; 36: Hochman JS, Sleeper LA, Webb JG, Dzavik V, Buller CE, Aylward P, Col J, White HD. Early revascularization and long-term survival in cardiogenic shock complicating acute myocardial infarction. JAMA. 2006;295: Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, Chambers CE, Ellis SG, Guyton RA, Hollenberg SM, Khot UN, Lange RA, Mauri L, Mehran R, Moussa ID, Mukherjee D, Nallamothu BK, Ting HH ACCF/AHA/SCAI guideline for percutaneous coronary intervention: A report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines and the society for cardiovascular angiography and interventions. Circulation. 2011;124:e Wiviott SD, Braunwald E, McCabe CH, Montalescot G, Ruzyllo W, Gottlieb S, Neumann FJ, Ardissino D, De Servi S, Murphy SA, Riesmeyer J, Weerakkody G, Gibson CM, Antman EM. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2007;357: Page 46
47 Appendix A The following pages contain the checklists listed below. Each checklist page can be detached by tearing along the perforated edge Non PCI Centers Primary PCI Systems for Direct Admits Primary PCI Systems for Transfer Patients EMS Systems for Transfer Centers EMS Systems for PCI Centers EMS Systems Inter-facility Transport Page 47
48 Early recognition of CP or CP equivalent patients Documentation of symptom onset ED arrival to ECG < 10 minutes (use EMS ECG if available) ECG interpretation = STEMI implement STEMI plan Early notification of the receiving hospital Early activation of transport plan Implement treatment protocol avoid continuous IV drips If giving fibrinolytics, door to lytic goal < 30 minutes (ED physician should only consult cardiology if case is not clear cut) If transferring for primary PCI, first door to device activation goal < 120 mins. (including lytic ineligible patients) Send medical records including EMS information, ECGs, record of treatments with times, and EMTALA forms (can fax info to primary PCI hospital if need time to complete as soon as possible EMTALA must be sent with patient) Expect feedback from the PCI center share with staff Page 48
49 Early recognition of CP or CP equivalent patients Documentation of symptom onset ED arrival to ECG < 10 minutes (use EMS ECG if available) ECG interpretation = STEMI implement STEMI plan Early notification of the receiving hospital Early activation of the cath lab (EMS or ED) cath team arrival < 30 minutes Door to device for walk-ins goal < 90 minutes EMS first medical contact to device goal < 90 minutes Consider door to device goal < 60 minutes Consider direct admit to cath lab if EMS patient Cath lab to device activation < 30 minutes Door to device < 90 minutes First medical contact to device < 90 minutes Data feedback within hours to staff and EMS Process in place to obtain EMS records and ECG STEMI team meetings to discuss STEMI process Page 49
50 Receive call from transfer facility to the STEMI hotline Accept patient accepted regardless of bed availability or diversion status Early cath lab activation if transferring for primary PCI. Cath team arrival should occur in < 30 minutes. Lytic patient can be admitted directly to bed if reperfused If not reperfused, EMS should notify receiving center to activate the cath team Patient admitted directly to cath lab if team ready Patient admitted to ED if team not ready staff should be aware of arrival time to outlying facility to achieve first door to device < 120 minutes Cath lab to device < 30 minutes First medical contact to device goal of < 120 minutes Data feedback within hours to transfer center, with specific feedback directed at transfer center ED physicians, nursing staff, and EMS staff STEMI team meetings to discuss STEMI process Page 50
51 Early recognition of CP or CP equivalent patients Document symptom onset First medical contact to ECG < 10 minutes Early notification of the receiving hospital: EMS activation of the cath lab for obvious STEMI Implement bypass protocol to closest PCI center if first medical contact to device is achievable in < 90 minutes Complete fibrinolytic checklist * If patient is ineligible, consider bypass protocol Implement treatment protocol Scene time < 15 minutes Leave run sheets and/or information of pre-hospital care Leave a copy of the ECG Expect and seek feedback from the PCI center/transfer center Page 51
52 Early recognition of CP or CP equivalent patients Document symptom onset First medical contact to ECG < 10 minutes Early notification of the receiving hospital: EMS activation of the cath lab for obvious STEMI Implement treatment protocol Scene time < 15 minutes Admit directly to the cath lab if team is ready Leave run sheets and/or information of pre-hospital care Leave a copy of the ECG Expect and seek feedback from the PCI center/transfer center Page 52
53 STEMI calls are considered a priority call Implement transport protocol * should include taking patient to the most appropriate PCI Hospital Minimize or avoid continuous IV infusions Obtain all available records from the transferring hospital including ECG do not hold up transfer for charting complete EMTALA and fax other documents Consider transferring patient directly to the cath lab if team is ready If lytic patient has not reperfused and/or continues with pain, notify receiving facility about the potential need for rescue PCI Leave run sheets and transferring hospital documentation Expect and seek feedback from the PCI center/transfer center Page 53
REFERRAL HOSPITAL. The Importance of Door In Door Out Time DIDO
 REFERRAL HOSPITAL The Importance of Door In Door Out Time DIDO Time to Treatment is critical for STEMI patients For patients with ST-segment elevation myocardial infarction (STEMI), percutaneous coronary
REFERRAL HOSPITAL The Importance of Door In Door Out Time DIDO Time to Treatment is critical for STEMI patients For patients with ST-segment elevation myocardial infarction (STEMI), percutaneous coronary
Mission: Lifeline Recommendations for Criteria for STEMI Systems of Care
 Mission: Lifeline Recommendations for Criteria for STEMI Systems of Care The Mission: Lifeline Certification Program will acknowledge STEMI Systems, EMS, Non-PCI/STEMI Referral Centers and PCI/STEMI Receiving
Mission: Lifeline Recommendations for Criteria for STEMI Systems of Care The Mission: Lifeline Certification Program will acknowledge STEMI Systems, EMS, Non-PCI/STEMI Referral Centers and PCI/STEMI Receiving
Mission: Lifeline EMS Recognition Guide
 Mission: Lifeline EMS Recognition Guide This Mission: Lifeline EMS Recognition Guide was developed to provide information about Mission: Lifeline EMS Recognition processes and criteria. If you have any
Mission: Lifeline EMS Recognition Guide This Mission: Lifeline EMS Recognition Guide was developed to provide information about Mission: Lifeline EMS Recognition processes and criteria. If you have any
California Health and Safety Code, Section 1256.01
 California Health and Safety Code, Section 1256.01 1256.01. (a) The Elective Percutaneous Coronary Intervention (PCI) Pilot Program is hereby established in the department. The purpose of the pilot program
California Health and Safety Code, Section 1256.01 1256.01. (a) The Elective Percutaneous Coronary Intervention (PCI) Pilot Program is hereby established in the department. The purpose of the pilot program
Acute Myocardial Infarction (the formulary thrombolytic for AMI at AAMC is TNK, please see the TNK monograph in this manual for information)
") ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Alteplase (Tissue Plasminogen Activator (t-pa)), Activase in the Treatment
ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Alteplase (Tissue Plasminogen Activator (t-pa)), Activase in the Treatment
Official Online ACLS Exam
 \ Official Online ACLS Exam Please fill out this form before you take the exam. Name : Email : Phone : 1. Hypovolemia initially produces which arrhythmia? A. PEA B. Sinus tachycardia C. Symptomatic bradyarrhythmia
\ Official Online ACLS Exam Please fill out this form before you take the exam. Name : Email : Phone : 1. Hypovolemia initially produces which arrhythmia? A. PEA B. Sinus tachycardia C. Symptomatic bradyarrhythmia
The Cardiac Society of Australia and New Zealand
 The Cardiac Society of Australia and New Zealand Guidelines on Support Facilities for Coronary Angiography and Percutaneous Coronary Intervention (PCI) including Guidelines on the Performance of Procedures
The Cardiac Society of Australia and New Zealand Guidelines on Support Facilities for Coronary Angiography and Percutaneous Coronary Intervention (PCI) including Guidelines on the Performance of Procedures
ACLS PRE-TEST ANNOTATED ANSWER KEY
 ACLS PRE-TEST ANNOTATED ANSWER KEY June, 2011 Question 1: Question 2: There is no pulse with this rhythm. Question 3: Question 4: Question 5: Question 6: Question 7: Question 8: Question 9: Question 10:
ACLS PRE-TEST ANNOTATED ANSWER KEY June, 2011 Question 1: Question 2: There is no pulse with this rhythm. Question 3: Question 4: Question 5: Question 6: Question 7: Question 8: Question 9: Question 10:
Implementing a Prehospital 12-Lead Program
 Implementing a Prehospital 12-Lead Program Corey M. Slovis, M.D. Professor and Chairman Department of Emergency Medicine Vanderbilt University Medical Center Medical Director, Metro Nashville Fire Department
Implementing a Prehospital 12-Lead Program Corey M. Slovis, M.D. Professor and Chairman Department of Emergency Medicine Vanderbilt University Medical Center Medical Director, Metro Nashville Fire Department
CLINICAL QUALITY MEASURES FINALIZED FOR ELIGIBLE HOSPITALS AND CRITICAL ACCESS HOSPITALS BEGINNING WITH FY 2014
 CLINICAL QUALITY MEASURES FINALIZED FOR ELIGIBLE HOSPITALS AND CRITICAL ACCESS HOSPITALS BEGINNING WITH FY 2014 e 55 0495 2 Emergency Department (ED)- 1 Emergency Department Throughput Median time from
CLINICAL QUALITY MEASURES FINALIZED FOR ELIGIBLE HOSPITALS AND CRITICAL ACCESS HOSPITALS BEGINNING WITH FY 2014 e 55 0495 2 Emergency Department (ED)- 1 Emergency Department Throughput Median time from
Heart Attack: What You Need to Know
 A WorkLife4You Guide Heart Attack: What You Need to Know What is a Heart Attack? The heart works 24 hours a day, pumping oxygen and nutrient-rich blood to the body. Blood is supplied to the heart through
A WorkLife4You Guide Heart Attack: What You Need to Know What is a Heart Attack? The heart works 24 hours a day, pumping oxygen and nutrient-rich blood to the body. Blood is supplied to the heart through
COUNTY OF KERN EMERGENCY MEDCAL SERVICES DEPARTMENT. EMS Aircraft Dispatch-Response-Utilization Policies & Procedures
 COUNTY OF KERN EMERGENCY MEDCAL SERVICES DEPARTMENT Final - May 2, 2002 Russ Blind Interim Director Robert Barnes, M.D. Medical Director TABLE OF CONTENTS Section: Topic: Page #: I. Definitions 3-4 II.
COUNTY OF KERN EMERGENCY MEDCAL SERVICES DEPARTMENT Final - May 2, 2002 Russ Blind Interim Director Robert Barnes, M.D. Medical Director TABLE OF CONTENTS Section: Topic: Page #: I. Definitions 3-4 II.
6/5/2014. Objectives. Acute Coronary Syndromes. Epidemiology. Epidemiology. Epidemiology and Health Care Impact Pathophysiology
 Objectives Acute Coronary Syndromes Epidemiology and Health Care Impact Pathophysiology Unstable Angina NSTEMI STEMI Clinical Clues Pre-hospital Spokane County EMS Epidemiology About 600,000 people die
Objectives Acute Coronary Syndromes Epidemiology and Health Care Impact Pathophysiology Unstable Angina NSTEMI STEMI Clinical Clues Pre-hospital Spokane County EMS Epidemiology About 600,000 people die
Duration of Dual Antiplatelet Therapy After Coronary Stenting
 Duration of Dual Antiplatelet Therapy After Coronary Stenting C. DEAN KATSAMAKIS, DO, FACC, FSCAI INTERVENTIONAL CARDIOLOGIST ADVOCATE LUTHERAN GENERAL HOSPITAL INTRODUCTION Coronary artery stents are
Duration of Dual Antiplatelet Therapy After Coronary Stenting C. DEAN KATSAMAKIS, DO, FACC, FSCAI INTERVENTIONAL CARDIOLOGIST ADVOCATE LUTHERAN GENERAL HOSPITAL INTRODUCTION Coronary artery stents are
Level III Stroke Center Data Collection Requirements
 Who? Level III Stroke Center Data Collection Requirements All LERN Level III Stroke Centers. LERN Level I and II Stroke Centers have reporting requirements to The Joint Commission or other Board approved
Who? Level III Stroke Center Data Collection Requirements All LERN Level III Stroke Centers. LERN Level I and II Stroke Centers have reporting requirements to The Joint Commission or other Board approved
ACTION Registry GWTG Version 2.4
 ACTION Registry GWTG Version 2.4 Dr. Joanne Foody Kim Hustler The following relationships exist: Dr. Foody:Janssen, Sanofi, Genzyme, Aegerion, Amarin, BristolMeyersSquibb, Abbott, Gilead, ACC, Pfizer,
ACTION Registry GWTG Version 2.4 Dr. Joanne Foody Kim Hustler The following relationships exist: Dr. Foody:Janssen, Sanofi, Genzyme, Aegerion, Amarin, BristolMeyersSquibb, Abbott, Gilead, ACC, Pfizer,
Planning: Patient Goals and Expected Outcomes The patient will: Remain free of unusual bleeding Maintain effective tissue perfusion Implementation
 Obtain complete heath history including allergies, drug history and possible drug Assess baseline coagulation studies and CBC Assess for history of bleeding disorders, GI bleeding, cerebral bleed, recent
Obtain complete heath history including allergies, drug history and possible drug Assess baseline coagulation studies and CBC Assess for history of bleeding disorders, GI bleeding, cerebral bleed, recent
DO YOU LIVE IN A CARDIAC READY COMMUNITY?
 DO YOU LIVE IN A CARDIAC READY COMMUNITY? If someone in your community suffers a sudden cardiac arrest tomorrow, how likely is he or she to survive due to rapid access to life-saving treatment? Cities
DO YOU LIVE IN A CARDIAC READY COMMUNITY? If someone in your community suffers a sudden cardiac arrest tomorrow, how likely is he or she to survive due to rapid access to life-saving treatment? Cities
Utilizing the Cath Lab for Cardiac Arrest
 Utilizing the Cath Lab for Cardiac Arrest Khaled M. Ziada, MD Director, Cardiovascular Catheterization Laboratories Gill Heart Institute, University of Kentucky UK/AHA Strive to Revive Symposium May 2013
Utilizing the Cath Lab for Cardiac Arrest Khaled M. Ziada, MD Director, Cardiovascular Catheterization Laboratories Gill Heart Institute, University of Kentucky UK/AHA Strive to Revive Symposium May 2013
Aktuelle Literatur aus der Notfallmedizin
 05.02.2014 Aktuelle Literatur aus der Notfallmedizin prä- und innerklinisch Aktuelle Publikationen aus 2012 / 2013 PubMed hits zu emergency medicine 12,599 Abstract OBJECTIVES: Current American Heart
05.02.2014 Aktuelle Literatur aus der Notfallmedizin prä- und innerklinisch Aktuelle Publikationen aus 2012 / 2013 PubMed hits zu emergency medicine 12,599 Abstract OBJECTIVES: Current American Heart
Update on Antiplatelets and anticoagulants. Outlines. Antiplatelets and Anticoagulants 1/23/2013. Timir Paul, MD, PhD
 Update on Antiplatelets and anticoagulants Timir Paul, MD, PhD Antiplatelets Indications Doses Long term use (beyond 12 months) ASA and combination use of NSAIDS ASA resistance Plavix resistance Plavix
Update on Antiplatelets and anticoagulants Timir Paul, MD, PhD Antiplatelets Indications Doses Long term use (beyond 12 months) ASA and combination use of NSAIDS ASA resistance Plavix resistance Plavix
Intermedix Inc. EMR 2006 Data Element Name. Compliant. Data Number. Elements
 D01_01 EMS Agency X D01_02 EMS Agency D01_03 EMS Agency State X D01_04 EMS Agency County X D01_05 Primary Type of Service D01_06 Other Types of Service D01_07 Level of Service X D01_08 Organizational Type
D01_01 EMS Agency X D01_02 EMS Agency D01_03 EMS Agency State X D01_04 EMS Agency County X D01_05 Primary Type of Service D01_06 Other Types of Service D01_07 Level of Service X D01_08 Organizational Type
Antiplatelet and Antithrombotics From clinical trials to guidelines
 Antiplatelet and Antithrombotics From clinical trials to guidelines Ashraf Reda, MD, FESC Prof and head of Cardiology Dep. Menofiya University Preisedent of EGYBAC Chairman of WGLVR One of the big stories
Antiplatelet and Antithrombotics From clinical trials to guidelines Ashraf Reda, MD, FESC Prof and head of Cardiology Dep. Menofiya University Preisedent of EGYBAC Chairman of WGLVR One of the big stories
ACLS PHARMACOLOGY 2011 Guidelines
 ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
Mission: Lifeline North Texas STEMI Workshop. The Model STEMI Referring Center (non-pci capable) Trisha Wren, RN, BSN
 Trisha Wren, RN, BSN") STEMI Workshop The Model STEMI Referring Center (non-pci capable) Trisha Wren, RN, BSN Faculty Disclosure Information Trisha Wren, RN, BSN The Model STEMI Referring Center (non PCI capable) FINANCIAL DISCLOSURE:
STEMI Workshop The Model STEMI Referring Center (non-pci capable) Trisha Wren, RN, BSN Faculty Disclosure Information Trisha Wren, RN, BSN The Model STEMI Referring Center (non PCI capable) FINANCIAL DISCLOSURE:
If you do not wish to print the entire pre-test you may print Page 2 only to write your answers, score your test, and turn in to your instructor.
 This is a SAMPLE of the pretest you can access with your AHA PALS Course Manual at Heart.org/Eccstudent using your personal code that comes with your PALS Course Manual The American Heart Association strongly
This is a SAMPLE of the pretest you can access with your AHA PALS Course Manual at Heart.org/Eccstudent using your personal code that comes with your PALS Course Manual The American Heart Association strongly
ANESTHESIA FOR PATIENTS WITH CORONARY STENTS FOR NON CARDIAC SURGERY. Dr. Mahesh Vakamudi. Professor and Head
 ANESTHESIA FOR PATIENTS WITH CORONARY STENTS FOR NON CARDIAC SURGERY Dr. Mahesh Vakamudi Professor and Head Department of Anesthesiology, Critical Care and Pain Medicine Sri Ramachandra University INTRODUCTION
ANESTHESIA FOR PATIENTS WITH CORONARY STENTS FOR NON CARDIAC SURGERY Dr. Mahesh Vakamudi Professor and Head Department of Anesthesiology, Critical Care and Pain Medicine Sri Ramachandra University INTRODUCTION
STEMI System of Care: Upland Hills Health A Transferring Non-PCI Facility. Estimated ground transport time: 54 minutes
 STEMI System of Care: Upland Hills Health A Transferring Non-PCI Facility Estimated ground transport time: 54 minutes STEMI CARE as A Transfer Facility American College of Cardiology Guidelines Call for
STEMI System of Care: Upland Hills Health A Transferring Non-PCI Facility Estimated ground transport time: 54 minutes STEMI CARE as A Transfer Facility American College of Cardiology Guidelines Call for
INTRODUCTION TO EECP THERAPY
 INTRODUCTION TO EECP THERAPY is an FDA cleared, Medicare approved, non-invasive medical therapy for the treatment of stable and unstable angina, congestive heart failure, acute myocardial infarction, and
INTRODUCTION TO EECP THERAPY is an FDA cleared, Medicare approved, non-invasive medical therapy for the treatment of stable and unstable angina, congestive heart failure, acute myocardial infarction, and
Your Guide to Express Critical Illness Insurance Definitions
 Your Guide to Express Critical Illness Insurance Definitions Your Guide to EXPRESS Critical Illness Insurance Definitions This guide to critical illness definitions will help you understand the illnesses
Your Guide to Express Critical Illness Insurance Definitions Your Guide to EXPRESS Critical Illness Insurance Definitions This guide to critical illness definitions will help you understand the illnesses
EMS Patient Care Report Navigation Logic for Record Creation
 EMS Patient Report Navigation Logic for Record Creation This document serves to provide specifications regarding data entry and data element completion requirements for PreMIS Version 2 web-based application
EMS Patient Report Navigation Logic for Record Creation This document serves to provide specifications regarding data entry and data element completion requirements for PreMIS Version 2 web-based application
INTERFACILITY TRANSFERS
 POLICY NO: 7013 PAGE 1 OF 8 EFFECTIVE DATE: 07-01-06 REVISED DATE: 03-15-12 APPROVED: Bryan Cleaver EMS Administrator Dr. Mark Luoto EMS Medical Director AUTHORITY: Health and Safety Code, Section 1798.172,
POLICY NO: 7013 PAGE 1 OF 8 EFFECTIVE DATE: 07-01-06 REVISED DATE: 03-15-12 APPROVED: Bryan Cleaver EMS Administrator Dr. Mark Luoto EMS Medical Director AUTHORITY: Health and Safety Code, Section 1798.172,
Emergency Management Strategies for Acute Myocardial Infarction - Code R at LGH
 Emergency Management Strategies for Acute Myocardial Infarction - Code R at LGH PAUL N. CASALE, M.D., F.A.C.C. Chief, Division of Cardiology and Medical Director of Cardiology, Lancaster General Hospital
Emergency Management Strategies for Acute Myocardial Infarction - Code R at LGH PAUL N. CASALE, M.D., F.A.C.C. Chief, Division of Cardiology and Medical Director of Cardiology, Lancaster General Hospital
TIME LOST IS BRAIN LOST. TARGET: STROKE CAMPAIGN MANUAL
 TIME LOST IS BRAIN LOST. TARGET: STROKE CAMPAIGN MANUAL 2010, American Heart Association TARGET: STROKE CAMPAIGN MANUAL 01 INTRODUCTION Welcome to the Target: Stroke. The purpose of this manual is to provide
TIME LOST IS BRAIN LOST. TARGET: STROKE CAMPAIGN MANUAL 2010, American Heart Association TARGET: STROKE CAMPAIGN MANUAL 01 INTRODUCTION Welcome to the Target: Stroke. The purpose of this manual is to provide
At Elite Ambulance, we are always here to serve you.
 FAQ Important Disclaimer: The following FAQ section includes information regarding health provider decisions, health and payment matters not financial matters. None of the following questions or answers
FAQ Important Disclaimer: The following FAQ section includes information regarding health provider decisions, health and payment matters not financial matters. None of the following questions or answers
Inpatient Anticoagulation Safety. To provide safe and effective anticoagulation therapy through a collaborative approach.
 Inpatient Anticoagulation Safety Purpose: Policy: To provide safe and effective anticoagulation therapy through a collaborative approach. Upon the written order of a physician, Heparin, Low Molecular Weight
Inpatient Anticoagulation Safety Purpose: Policy: To provide safe and effective anticoagulation therapy through a collaborative approach. Upon the written order of a physician, Heparin, Low Molecular Weight
EMSPIC State NEMSIS Datasets
 E01_01 Patient Care Report Number X X E01_02 Software Creator X X E01_03 Software Name X X E01_04 Sofware Version X X E02_01 EMS Agency Number X X E02_02 Incident Number X E02_03 EMS Unit (Vehicle) Response
E01_01 Patient Care Report Number X X E01_02 Software Creator X X E01_03 Software Name X X E01_04 Sofware Version X X E02_01 EMS Agency Number X X E02_02 Incident Number X E02_03 EMS Unit (Vehicle) Response
Ambulance Services. Provider Manual
 Provider Manual Provider 1 April 1, 2014 TABLE OF CONTENTS Chapter I. General Program Policies Chapter II. Member Eligibility Chapter IV. Billing Iowa Medicaid Appendix III. Provider-Specific Policies
Provider Manual Provider 1 April 1, 2014 TABLE OF CONTENTS Chapter I. General Program Policies Chapter II. Member Eligibility Chapter IV. Billing Iowa Medicaid Appendix III. Provider-Specific Policies
Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations.
 INTRODUCTION Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations. Although decrease in cardiovascular mortality still major cause of morbidity & burden of disease.
INTRODUCTION Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations. Although decrease in cardiovascular mortality still major cause of morbidity & burden of disease.
THE INTERNET STROKE CENTER PRESENTATIONS AND DISCUSSIONS ON STROKE MANAGEMENT
 THE INTERNET STROKE CENTER PRESENTATIONS AND DISCUSSIONS ON STROKE MANAGEMENT Stroke Prevention in Atrial Fibrillation Gregory Albers, M.D. Director Stanford Stroke Center Professor of Neurology and Neurological
THE INTERNET STROKE CENTER PRESENTATIONS AND DISCUSSIONS ON STROKE MANAGEMENT Stroke Prevention in Atrial Fibrillation Gregory Albers, M.D. Director Stanford Stroke Center Professor of Neurology and Neurological
Module Two: EMS Systems. Wisconsin EMS Medical Director s Course
 : EMS Systems Wisconsin EMS Medical Director s Course Objectives List the components of EMS systems Outline organizational and design options for EMS systems Outline system staffing and response configurations
: EMS Systems Wisconsin EMS Medical Director s Course Objectives List the components of EMS systems Outline organizational and design options for EMS systems Outline system staffing and response configurations
ELSO GUIDELINES FOR ECMO CENTERS
 ELSO GUIDELINES FOR ECMO CENTERS PURPOSE These guidelines developed by the Extracorporeal Life Support Organization, outline the ideal institutional requirements needed for effective use of extracorporeal
ELSO GUIDELINES FOR ECMO CENTERS PURPOSE These guidelines developed by the Extracorporeal Life Support Organization, outline the ideal institutional requirements needed for effective use of extracorporeal
URN: Family name: Given name(s): Address:
: Address:") State of Queensland (Queensland Health) 2015 Licensed under: http://creativecommons.org/licenses/by-nc-nd/3.0/au/deed.en Contact: [email protected] Facility:... Clinical pathways
State of Queensland (Queensland Health) 2015 Licensed under: http://creativecommons.org/licenses/by-nc-nd/3.0/au/deed.en Contact: [email protected] Facility:... Clinical pathways
A Patient s Guide to Primary and Secondary Prevention of Cardiovascular Disease Using Blood-Thinning (Anticoagulant) Drugs
 Drugs") A Patient s Guide to Primary and Secondary Prevention of PATIENT EDUCATION GUIDE What Is Cardiovascular Disease? Cardiovascular disease (CVD) is a broad term that covers any disease of the heart and circulatory
A Patient s Guide to Primary and Secondary Prevention of PATIENT EDUCATION GUIDE What Is Cardiovascular Disease? Cardiovascular disease (CVD) is a broad term that covers any disease of the heart and circulatory
Interfacility Transfer Guidelines for Children
 Interfacility Transfer Guidelines for Children Dear Hospital CEO: As you may know, recent evidence shows that the best outcomes for critically ill and injured children are achieved when treated at facilities
Interfacility Transfer Guidelines for Children Dear Hospital CEO: As you may know, recent evidence shows that the best outcomes for critically ill and injured children are achieved when treated at facilities
Use of Antithrombotic Agents In The Presence Of Neuraxial Anesthesia
 Use of Antithrombotic Agents In The Presence Of Neuraxial Anesthesia Insertion, removal or presence of a catheter in selected sites can place a patient who is antithrombotic agent at risk for a local bleeding
Use of Antithrombotic Agents In The Presence Of Neuraxial Anesthesia Insertion, removal or presence of a catheter in selected sites can place a patient who is antithrombotic agent at risk for a local bleeding
RISK STRATIFICATION for Acute Coronary Syndrome in the Emergency Department
 RISK STRATIFICATION for Acute Coronary Syndrome in the Emergency Department Sohil Pothiawala FAMS (EM), MRCSEd (A&E), M.Med (EM), MBBS Consultant Dept. of Emergency Medicine Singapore General Hospital
RISK STRATIFICATION for Acute Coronary Syndrome in the Emergency Department Sohil Pothiawala FAMS (EM), MRCSEd (A&E), M.Med (EM), MBBS Consultant Dept. of Emergency Medicine Singapore General Hospital
Medical Direction and Practices Board WHITE PAPER
 Medical Direction and Practices Board WHITE PAPER Use of Pressors in Pre-Hospital Medicine: Proper Indication and State of the Science Regarding Proper Choice of Pressor BACKGROUND Shock is caused by a
Medical Direction and Practices Board WHITE PAPER Use of Pressors in Pre-Hospital Medicine: Proper Indication and State of the Science Regarding Proper Choice of Pressor BACKGROUND Shock is caused by a
DUAL ANTIPLATELET THERAPY. Dr Robert S Mvungi, MD(Dar), Mmed (Wits) FCP(SA), Cert.Cardio(SA) Phy Tanzania Cardiac Society Dar es Salaam Tanzania
, Mmed (Wits) FCP(SA), Cert.Cardio(SA) Phy Tanzania Cardiac Society Dar es Salaam Tanzania") DUAL ANTIPLATELET THERAPY Dr Robert S Mvungi, MD(Dar), Mmed (Wits) FCP(SA), Cert.Cardio(SA) Phy Tanzania Cardiac Society Dar es Salaam Tanzania DUAL ANTIPLATELET THERAPY (DAPT) Dual antiplatelet regimen
DUAL ANTIPLATELET THERAPY Dr Robert S Mvungi, MD(Dar), Mmed (Wits) FCP(SA), Cert.Cardio(SA) Phy Tanzania Cardiac Society Dar es Salaam Tanzania DUAL ANTIPLATELET THERAPY (DAPT) Dual antiplatelet regimen
Dabigatran (Pradaxa) Guidelines
 Guidelines") Dabigatran (Pradaxa) Guidelines Dabigatran is a new anticoagulant for reducing the risk of stroke in patients with atrial fibrillation. Dabigatran is a direct thrombin inhibitor, similar to warfarin, without
Dabigatran (Pradaxa) Guidelines Dabigatran is a new anticoagulant for reducing the risk of stroke in patients with atrial fibrillation. Dabigatran is a direct thrombin inhibitor, similar to warfarin, without
Copyright 2009, National Academy of Ambulance Coding Unauthorized copying/distribution is strictly prohibited
 Your instructor Levels of Service National Academy of Ambulance Coding Steve Wirth Founding Partner, Page, Wolfberg & Wirth LLC Over 30 years experience as an EMT, Paramedic, Flight Medic, EMS Instructor,
Your instructor Levels of Service National Academy of Ambulance Coding Steve Wirth Founding Partner, Page, Wolfberg & Wirth LLC Over 30 years experience as an EMT, Paramedic, Flight Medic, EMS Instructor,
Lifecheque Basic Critical Illness Insurance
 Lifecheque Basic Critical Illness Insurance Strong. Reliable. Trustworthy. Forward-thinking. Extra help on the road to recovery Surviving a critical illness can be very challenging financially Few of us
Lifecheque Basic Critical Illness Insurance Strong. Reliable. Trustworthy. Forward-thinking. Extra help on the road to recovery Surviving a critical illness can be very challenging financially Few of us
It is recommended that the reader review each medical directive presented in this presentation along with the actual PCP Core medical directive.
 It is recommended that the reader review each medical directive presented in this presentation along with the actual PCP Core medical directive. This presentation will highlight the changes and any new
It is recommended that the reader review each medical directive presented in this presentation along with the actual PCP Core medical directive. This presentation will highlight the changes and any new
UW MEDICINE PATIENT EDUCATION. Aortic Stenosis. What is heart valve disease? What is aortic stenosis?
 UW MEDICINE PATIENT EDUCATION Aortic Stenosis Causes, symptoms, diagnosis, and treatment This handout describes aortic stenosis, a narrowing of the aortic valve in your heart. It also explains how this
UW MEDICINE PATIENT EDUCATION Aortic Stenosis Causes, symptoms, diagnosis, and treatment This handout describes aortic stenosis, a narrowing of the aortic valve in your heart. It also explains how this
Cardiac Catheterization Curriculum for Fellows in Cardiology Dartmouth-Hitchcock Medical Center Level 1 and Level 2 Training 2008-2009
 Cardiac Catheterization Curriculum for Fellows in Cardiology Dartmouth-Hitchcock Medical Center Level 1 and Level 2 Training 2008-2009 I. Overview of Training in Cardiac Catheterization Cardiac catheterization
Cardiac Catheterization Curriculum for Fellows in Cardiology Dartmouth-Hitchcock Medical Center Level 1 and Level 2 Training 2008-2009 I. Overview of Training in Cardiac Catheterization Cardiac catheterization
Children's Medical Services (CMS) Regional Perinatal Intensive Care Center (RPICC) Neonatal Extracorporeal Life Support (ECLS) Centers Questionnaire
 Regional Perinatal Intensive Care Center (RPICC) Neonatal Extracorporeal Life Support (ECLS) Centers Questionnaire") Children's Medical Services (CMS) Regional Perinatal Intensive Care Center (RPICC) Neonatal Extracorporeal Life Support (ECLS) Centers Questionnaire Date: RPICC Facility: CMS use only Include the following
Children's Medical Services (CMS) Regional Perinatal Intensive Care Center (RPICC) Neonatal Extracorporeal Life Support (ECLS) Centers Questionnaire Date: RPICC Facility: CMS use only Include the following
State of Wisconsin. Department of Health and Family Services Division of Public Health. Bureau of Local Health Support and Emergency Medical Services
 State of Wisconsin Department of Health and Family Services Division of Public Health Bureau of Local Health Support and Emergency Medical Services 2006 Interfacility Transport Guidelines Table of Contents
State of Wisconsin Department of Health and Family Services Division of Public Health Bureau of Local Health Support and Emergency Medical Services 2006 Interfacility Transport Guidelines Table of Contents
Chest Pain Evaluation (NSW Chest Pain Pathway)
") Policy Directive Ministry of Health, SW 73 Miller Street orth Sydney SW 2060 Locked Mail Bag 961 orth Sydney SW 2059 Telephone (02) 9391 9000 Fax (02) 9391 9101 http//www.health.nsw.gov.au/policies/ Chest
Policy Directive Ministry of Health, SW 73 Miller Street orth Sydney SW 2060 Locked Mail Bag 961 orth Sydney SW 2059 Telephone (02) 9391 9000 Fax (02) 9391 9101 http//www.health.nsw.gov.au/policies/ Chest
COUNTY OF KERN EMERGENCY MEDICAL SERVICES DEPARTMENT
 COUNTY OF KERN EMERGENCY MEDICAL SERVICES DEPARTMENT AMBULANCE PATIENT TRANSPORT DESTINATION - HOSPITAL EMERGENCY DEPARTMENT STATUS POLICIES & PROCEDURES December 16, 1999 FRED DREW Director ROBERT BARNES,
COUNTY OF KERN EMERGENCY MEDICAL SERVICES DEPARTMENT AMBULANCE PATIENT TRANSPORT DESTINATION - HOSPITAL EMERGENCY DEPARTMENT STATUS POLICIES & PROCEDURES December 16, 1999 FRED DREW Director ROBERT BARNES,
404 Section 5 Shock and Resuscitation. Scene Size-up. Primary Assessment. History Taking
 404 Section 5 and Resuscitation Scene Size-up Scene Safety Mechanism of Injury (MOI)/ Nature of Illness (NOI) Ensure scene safety and address hazards. Standard precautions should include a minimum of gloves
404 Section 5 and Resuscitation Scene Size-up Scene Safety Mechanism of Injury (MOI)/ Nature of Illness (NOI) Ensure scene safety and address hazards. Standard precautions should include a minimum of gloves
Developing a Dynamic Team Approach to Stroke Care. Emergency Medical Services 2015
 Developing a Dynamic Team Approach to Stroke Care Emergency Medical Services 2015 Why Stroke, Why now? A recent study showed that 80 percent of people in the United States live within an hour s drive of
Developing a Dynamic Team Approach to Stroke Care Emergency Medical Services 2015 Why Stroke, Why now? A recent study showed that 80 percent of people in the United States live within an hour s drive of
BRIGHT Trial. Bivalirudin versus Heparin and Heparin plus Tirofiban in Patients with AMI Undergoing PCI. Thirty-Day and One-Year Outcomes of the
 Bivalirudin versus Heparin and Heparin plus Tirofiban in Patients with AMI Undergoing PCI Thirty-Day and One-Year Outcomes of the BRIGHT Trial Yaling Han, MD, FACC On behalf of the BRIGHT investigators
Bivalirudin versus Heparin and Heparin plus Tirofiban in Patients with AMI Undergoing PCI Thirty-Day and One-Year Outcomes of the BRIGHT Trial Yaling Han, MD, FACC On behalf of the BRIGHT investigators
Stent for Life Initiative How can we improve system delay and patients delay in STEMI
 Stent for Life Initiative How can we improve system delay and patients delay in STEMI Z. Kaifoszova SFL Initiative Europe 2011 Stent for Life Initiative 10 countries participate in the program Declaration
Stent for Life Initiative How can we improve system delay and patients delay in STEMI Z. Kaifoszova SFL Initiative Europe 2011 Stent for Life Initiative 10 countries participate in the program Declaration
Emergency Medical Services Agency. Report to the Local Agency Formation Commission
 Emergency Medical Services Agency August 8, 2012 Report to the Local Agency Formation Commission The Relationship of Fire First Response to Emergency Medical Services On September 26, 2011, the Contra
Emergency Medical Services Agency August 8, 2012 Report to the Local Agency Formation Commission The Relationship of Fire First Response to Emergency Medical Services On September 26, 2011, the Contra
MLFD Standard Operating Guidelines SOG# 12-22 Subject: Patient Transfer of Care Initiated 1/30/2013
 MLFD Standard Operating Guidelines SOG# 12-22 Subject: Patient Transfer of Care Initiated 1/30/2013 Approved: Revised PURPOSE It is the purpose of this SOG to provide and ensure the highest level of patient
MLFD Standard Operating Guidelines SOG# 12-22 Subject: Patient Transfer of Care Initiated 1/30/2013 Approved: Revised PURPOSE It is the purpose of this SOG to provide and ensure the highest level of patient
SUBJECT: PRIVATE PROVIDER AGENCY (EMT, PARAMEDIC, MICN) TRANSPORT/RESPONSE GUIDELINES REFERENCE NO. 517
 TRANSPORT/RESPONSE GUIDELINES REFERENCE NO. 517") DEPARTMENT OF HEALTH SERVICES COUNTY OF LOS ANGELES SUBJECT: PRIVATE PROVIDER AGENCY (EMT, PARAMEDIC, MICN) TRANSPORT/RESPONSE PURPOSE: To provide guidelines for private ambulance providers handling requests
DEPARTMENT OF HEALTH SERVICES COUNTY OF LOS ANGELES SUBJECT: PRIVATE PROVIDER AGENCY (EMT, PARAMEDIC, MICN) TRANSPORT/RESPONSE PURPOSE: To provide guidelines for private ambulance providers handling requests
The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010.
 ACLS Study Guide The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. Please read the below information carefully This letter is to confirm your
ACLS Study Guide The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. Please read the below information carefully This letter is to confirm your
Overview. Geriatric Overview. Chapter 26. Geriatrics 9/11/2012
 Chapter 26 Geriatrics Slide 1 Overview Trauma Common Medical Emergencies Special Considerations in the Elderly Medication Considerations Abuse and Neglect Expanding the Role of EMS Slide 2 Geriatric Overview
Chapter 26 Geriatrics Slide 1 Overview Trauma Common Medical Emergencies Special Considerations in the Elderly Medication Considerations Abuse and Neglect Expanding the Role of EMS Slide 2 Geriatric Overview
ALS INTERFACILITY TRANSFERS. SUPERSEDES: January 8, 2009
 EFFECTIVE: September 8, 2010 AUTHORIZATION: AR PAGE: 1 of 7 *This Administrative Requirement may be effectuated by an ambulance service only upon appropriate training of its EMS personnel.* Minimum Standards
EFFECTIVE: September 8, 2010 AUTHORIZATION: AR PAGE: 1 of 7 *This Administrative Requirement may be effectuated by an ambulance service only upon appropriate training of its EMS personnel.* Minimum Standards
Policies and Procedures. Related to. IABP Therapy
 Policies and Procedures Related to IABP Therapy Courtesy of Datascope Corp. Clinical Support Services The following policies and procedures are intended to serve as guidelines for developing hospital policy.
Policies and Procedures Related to IABP Therapy Courtesy of Datascope Corp. Clinical Support Services The following policies and procedures are intended to serve as guidelines for developing hospital policy.
Approved: Acute Stroke Ready Hospital Advanced Certification Program
 Approved: Acute Stroke Ready Hospital Advanced Certification Program The Joint Commission recently developed a new Disease- Specific Care Advanced Certification program for Acute Stroke Ready Hospitals
Approved: Acute Stroke Ready Hospital Advanced Certification Program The Joint Commission recently developed a new Disease- Specific Care Advanced Certification program for Acute Stroke Ready Hospitals
HAAD JAWDA Quality KPI; waiting times. December 2015
 HAAD JAWDA Quality KPI; waiting times December 2015 Page 1 of 13 Type: Waiting Time Indicator Indicator Number: WT001 Primary Care Appointment- Outpatient Setting Time to see a HAAD licensed family physician
HAAD JAWDA Quality KPI; waiting times December 2015 Page 1 of 13 Type: Waiting Time Indicator Indicator Number: WT001 Primary Care Appointment- Outpatient Setting Time to see a HAAD licensed family physician
Redefining the NSTEACS pathway in London
 Redefining the NSTEACS pathway in London Sotiris Antoniou Consultant Pharmacist, Cardiovascular Medicine, Barts and The London NHS Trust and Project Lead, North East London Cardiovascular and Stroke Network
Redefining the NSTEACS pathway in London Sotiris Antoniou Consultant Pharmacist, Cardiovascular Medicine, Barts and The London NHS Trust and Project Lead, North East London Cardiovascular and Stroke Network
Strategies for Each Payer Type. Medicare: Part 1. Medicare Coverage. Medicare. Medicare Requirements. Reimbursable Events
 Strategies for Each Payer Type Medicare: Part 1 Medicare Medicaid Commercial Insurance Auto Insurance Private Pay Contracts Medicare Largest Payer for Ambulance Services Coverage Rules Fee Schedule Medicare
Strategies for Each Payer Type Medicare: Part 1 Medicare Medicaid Commercial Insurance Auto Insurance Private Pay Contracts Medicare Largest Payer for Ambulance Services Coverage Rules Fee Schedule Medicare
STROKE PREVENTION IN ATRIAL FIBRILLATION. TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: ABBREVIATIONS: BACKGROUND:
 STROKE PREVENTION IN ATRIAL FIBRILLATION TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To guide clinicians in the selection of antithrombotic therapy for the secondary prevention
STROKE PREVENTION IN ATRIAL FIBRILLATION TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To guide clinicians in the selection of antithrombotic therapy for the secondary prevention
DATE: 29 August 2012 CONTEXT AND POLICY ISSUES
 TITLE: Dual Antiplatelet Therapy and Enoxaparin or Unfractionated Heparin for patients with ST-elevation Myocardial Infarction: A Review of the Clinical Evidence DATE: 29 August 2012 CONTEXT AND POLICY
TITLE: Dual Antiplatelet Therapy and Enoxaparin or Unfractionated Heparin for patients with ST-elevation Myocardial Infarction: A Review of the Clinical Evidence DATE: 29 August 2012 CONTEXT AND POLICY
ACCIDENT AND EMERGENCY DEPARTMENT/CARDIOLOGY
 Care Pathway Triage category ATRIAL FIBRILLATION PATHWAY ACCIDENT AND EMERGENCY DEPARTMENT/CARDIOLOGY AF/ FLUTTER IS PRIMARY REASON FOR PRESENTATION YES NO ONSET SYMPTOMS OF AF./../ TIME DURATION OF AF
Care Pathway Triage category ATRIAL FIBRILLATION PATHWAY ACCIDENT AND EMERGENCY DEPARTMENT/CARDIOLOGY AF/ FLUTTER IS PRIMARY REASON FOR PRESENTATION YES NO ONSET SYMPTOMS OF AF./../ TIME DURATION OF AF
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF)
 MANAGEMENT of Atrial Fibrillation (AF)") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF) Key priorities Identification and diagnosis Treatment for persistent AF Treatment for permanent AF Antithrombotic
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF) Key priorities Identification and diagnosis Treatment for persistent AF Treatment for permanent AF Antithrombotic
EMS Management of Stroke. Deaver Shattuck, M.D. Brian Wiseman, M.D. Keith Woodward, M.D.
 EMS Management of Stroke Deaver Shattuck, M.D. Brian Wiseman, M.D. Keith Woodward, M.D. Financial Disclosure: No relevant financial relationship exists Working Together to End Stroke Formed in 2013 Identified
EMS Management of Stroke Deaver Shattuck, M.D. Brian Wiseman, M.D. Keith Woodward, M.D. Financial Disclosure: No relevant financial relationship exists Working Together to End Stroke Formed in 2013 Identified
How To Be A Medical Flight Specialist
 Job Class Profile: Medical Flight Specialist Pay Level: CG-36 Point Band: 790-813 Accountability & Decision Making Development and Leadership Environmental Working Conditions Factor Knowledge Interpersonal
Job Class Profile: Medical Flight Specialist Pay Level: CG-36 Point Band: 790-813 Accountability & Decision Making Development and Leadership Environmental Working Conditions Factor Knowledge Interpersonal
Cardiac Arrest VF/Pulseless VT Learning Station Checklist
 Cardiac Arrest VF/Pulseless VT Learning Station Checklist VF/VT 00 American Heart Association Adult Cardiac Arrest Shout for Help/Activate Emergency Response Epinephrine every - min Amiodarone Start CPR
Cardiac Arrest VF/Pulseless VT Learning Station Checklist VF/VT 00 American Heart Association Adult Cardiac Arrest Shout for Help/Activate Emergency Response Epinephrine every - min Amiodarone Start CPR
CATRAC Mission: Lifeline Regional STEMI Field Guide
 CATRAC Mission: Lifeline Regional STEMI Field Guide CATRAC Mission: Lifeline Cardiac Care Workgroup Updated December 2013 Table of Contents Introduction... 3 CATRAC M:L... 3 Regional geography defined
CATRAC Mission: Lifeline Regional STEMI Field Guide CATRAC Mission: Lifeline Cardiac Care Workgroup Updated December 2013 Table of Contents Introduction... 3 CATRAC M:L... 3 Regional geography defined
ACLS Provider Manual Comparison Sheet Based on 2010 AHA Guidelines for CPR and ECC. BLS Changes
 ACLS Provider Manual Comparison Sheet Based on 2010 AHA Guidelines for CPR and ECC CPR Chest compressions, Airway, Breathing (C-A-B) BLS Changes New Old Rationale New science indicates the following order:
ACLS Provider Manual Comparison Sheet Based on 2010 AHA Guidelines for CPR and ECC CPR Chest compressions, Airway, Breathing (C-A-B) BLS Changes New Old Rationale New science indicates the following order:
CBT/OTEP 243 Aspirin Administration for ACS
 Seattle-King County EMS Seattle-King County Emergency Medical Services Division Public Health - Seattle/King County 401 5th Avenue, Suite 1200 Seattle, WA 98104 (206) 296-4693 February 2009 CBT/OTEP 243
Seattle-King County EMS Seattle-King County Emergency Medical Services Division Public Health - Seattle/King County 401 5th Avenue, Suite 1200 Seattle, WA 98104 (206) 296-4693 February 2009 CBT/OTEP 243
Field Trauma Triage & Air Ambulance Utilization. SWORBHP Answers
 Field Trauma Triage & Air Ambulance Utilization SWORBHP Answers Presented by : Dr. Mike Lewell, Regional Medical Director Dr. Mike Peddle, Local Medical Director Introduction/History What s this all about?
Field Trauma Triage & Air Ambulance Utilization SWORBHP Answers Presented by : Dr. Mike Lewell, Regional Medical Director Dr. Mike Peddle, Local Medical Director Introduction/History What s this all about?
Treating AF: The Newest Recommendations. CardioCase presentation. Ethel s Case. Wayne Warnica, MD, FACC, FACP, FRCPC
 Treating AF: The Newest Recommendations Wayne Warnica, MD, FACC, FACP, FRCPC CardioCase presentation Ethel s Case Ethel, 73, presents with rapid heart beating and mild chest discomfort. In the ED, ECG
Treating AF: The Newest Recommendations Wayne Warnica, MD, FACC, FACP, FRCPC CardioCase presentation Ethel s Case Ethel, 73, presents with rapid heart beating and mild chest discomfort. In the ED, ECG
Networking for optimal treatment of STEMI and NSTEMI. European Stent for life Project
 Networking for optimal treatment of STEMI and NSTEMI European Stent for life Project Dariusz Dudek on behalf of Department of Interventional Cardiology, Institute of Cardiology, Krakow, Poland The European
Networking for optimal treatment of STEMI and NSTEMI European Stent for life Project Dariusz Dudek on behalf of Department of Interventional Cardiology, Institute of Cardiology, Krakow, Poland The European
205 GROUND AMBULANCE TRANSPORTATION REIMBURSEMENT GUIDELINES FOR NON-CONTRACTED PROVIDERS
 205 GROUND AMBULANCE TRANSPORTATION REIMBURSEMENT GUIDELINES FOR NON-CONTRACTED PROVIDERS EFFECTIVE DATE: 05/01/2006, 04/01/2013 REVISION DATE: 04/04/2013 STAFF RESPONSIBLE FOR POLICY: DHCM ADMINISTRATION
205 GROUND AMBULANCE TRANSPORTATION REIMBURSEMENT GUIDELINES FOR NON-CONTRACTED PROVIDERS EFFECTIVE DATE: 05/01/2006, 04/01/2013 REVISION DATE: 04/04/2013 STAFF RESPONSIBLE FOR POLICY: DHCM ADMINISTRATION
CHADS score of 5 or 6 Recent (within 3mo) stroke or TIA Rheumatic valvular heart disease CHADs score of 3 or 4
 stroke or TIA Rheumatic valvular heart disease CHADs score of 3 or 4") LAMC Department of Pharmacy Services: ANTICOAGULATION: Surgical Intervention Table 1: Classification of Surgical interventions according to bleeding risk t required to discontinue anticoagulation Dental
LAMC Department of Pharmacy Services: ANTICOAGULATION: Surgical Intervention Table 1: Classification of Surgical interventions according to bleeding risk t required to discontinue anticoagulation Dental
Novel oral anticoagulant (NOAC) for stroke prevention in atrial fibrillation Special situations
 for stroke prevention in atrial fibrillation Special situations") Novel oral anticoagulant (NOAC) for stroke prevention in atrial fibrillation Special situations Dardo E. Ferrara MD Cardiac Electrophysiology North Cascade Cardiology PeaceHealth Medical Group Which anticoagulant
Novel oral anticoagulant (NOAC) for stroke prevention in atrial fibrillation Special situations Dardo E. Ferrara MD Cardiac Electrophysiology North Cascade Cardiology PeaceHealth Medical Group Which anticoagulant
Team Leader. Ensures high-quality CPR at all times Assigns team member roles Ensures that team members perform well. Bradycardia Management
 ACLS Megacode Case 1: Sinus Bradycardia (Bradycardia VF/Pulseless VT Asystole Out-of-Hospital Scenario You are a paramedic and arrive on the scene to find a 57-year-old woman complaining of indigestion.
ACLS Megacode Case 1: Sinus Bradycardia (Bradycardia VF/Pulseless VT Asystole Out-of-Hospital Scenario You are a paramedic and arrive on the scene to find a 57-year-old woman complaining of indigestion.
Inter-facility Patient Transfers
 Date: September 2004 Page 1 of 6 Inter-facility Patient Transfers Purpose: The purpose of this policy is to establish a uniform procedure for inter-facility transfers. 1. Responsibility: a. Patient transfer
Date: September 2004 Page 1 of 6 Inter-facility Patient Transfers Purpose: The purpose of this policy is to establish a uniform procedure for inter-facility transfers. 1. Responsibility: a. Patient transfer
3/25/14. To Clot or Not What s New In Anticoagulation? Clotting Cascade. Anticoagulant drug targets. Anita Ralstin, MS CNS CNP. Heparin.
 To Clot or Not What s New In Anticoagulation? Anita Ralstin, MS CNS CNP 1 Clotting Cascade 2 Anticoagulant drug targets Heparin XI VIII IX V X VII LMWH II Warfarin Fibrin clot 1 Who Needs Anticoagulation
To Clot or Not What s New In Anticoagulation? Anita Ralstin, MS CNS CNP 1 Clotting Cascade 2 Anticoagulant drug targets Heparin XI VIII IX V X VII LMWH II Warfarin Fibrin clot 1 Who Needs Anticoagulation
TRANSPORTATION SERVICES
 TRANSPORTATION SERVICES ADMINISTRATIVE POLICY Policy Number: TRANSPORT 002.15 T2 Effective Date: March 1, 2015 Table of Contents CONDITIONS OF COVERAGE... BENEFIT CONSIDERATIONS... COVERAGE RATIONALE...
TRANSPORTATION SERVICES ADMINISTRATIVE POLICY Policy Number: TRANSPORT 002.15 T2 Effective Date: March 1, 2015 Table of Contents CONDITIONS OF COVERAGE... BENEFIT CONSIDERATIONS... COVERAGE RATIONALE...
12 Lead ECGs: Ischemia, Injury & Infarction Part 2
 12 Lead ECGs: Ischemia, Injury & Infarction Part 2 McHenry Western Lake County EMS Localization: Left Coronary Artery Right Coronary Artery Right Ventricle Septal Wall Anterior Descending Artery Left Main
12 Lead ECGs: Ischemia, Injury & Infarction Part 2 McHenry Western Lake County EMS Localization: Left Coronary Artery Right Coronary Artery Right Ventricle Septal Wall Anterior Descending Artery Left Main
A3795 CONAWAY 2. AN ACT concerning the operation of air ambulance services and supplementing Title 26 of the Revised Statutes.
 ASSEMBLY, No. STATE OF NEW JERSEY th LEGISLATURE INTRODUCED DECEMBER, 00 Sponsored by: Assemblyman HERB CONAWAY, JR. District (Burlington and Camden) SYNOPSIS Establishes procedures for operation of air
ASSEMBLY, No. STATE OF NEW JERSEY th LEGISLATURE INTRODUCED DECEMBER, 00 Sponsored by: Assemblyman HERB CONAWAY, JR. District (Burlington and Camden) SYNOPSIS Establishes procedures for operation of air