Class I and II Indirect Tooth-Colored Restorations
|
|
|
- Adelia Weaver
- 9 years ago
- Views:
Transcription
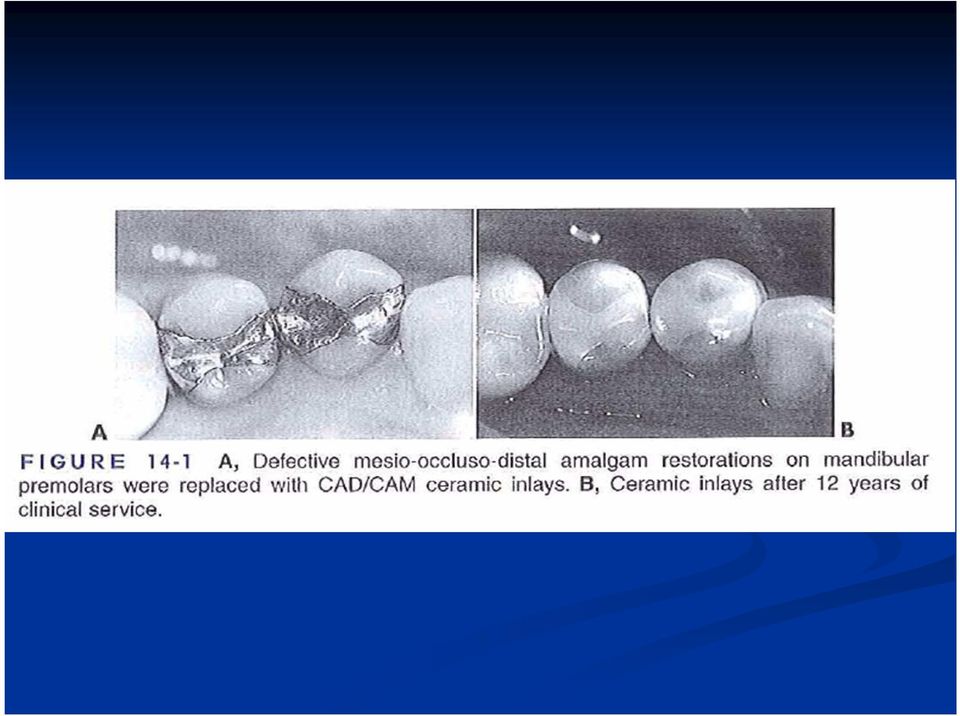
1 Class I and II Indirect Tooth-Colored Restorations

2 Most indirect restorations are made on a replica of the prepared tooth in a dental laboratory by a trained technician. Tooth-colored indirect systems include laboratory-processed composites and ceramics, such as porcelain fired on refractory dies or hot pressed glasses.

3 In addition, chairside computer-aided design/computer-assisted manufacturing (CAD/CAM) systems are currently available and are used to fabricate ceramic restorations.

4
5 Indications
6 * Esthetics. * Large defects or previous restorations. * Economic factors: Some patients desire the best dental treatment available, regardless of cost.

7 Contraindications
8 * Heavy occlusal forces

9 * Inability to maintain a dry field. * Deep subgingival preparations.

10 Advantages

11 * Improved physical properties: A wide variety of high-strength tooth-colored restorative materials, including laboratory-processed and computer-milled composites and ceramics, can be used with indirect techniques.

12 * Variety of materials and techniques: Indirect tooth-colored restorations can be fabricated with either composites or ceramics using various laboratory processes or CAD/CAM methods.

13 * Wear resistance: Ceramic restorations are more wear-resistant than direct composite restorations, an especially critical factor when restoring large occlusal areas of posterior teeth. Laboratoryprocessed composite restorations wear more than ceramics, but less than direct composites in laboratory studies.

14 * Reduced polymerization shrinkage: Polymerization shrinkage and its resulting stresses are a major shortcoming of direct composite restorations.

15 * Ability to strengthen remaining tooth structure: Tooth structure weakened by caries, trauma, or preparation can be strengthened by adhesively bonding indirect tooth-colored restorations.

16 * More precise control of contours and contacts: Indirect techniques usually provide better contours (especially proximal contours) and occlusal contacts than direct restorations because of the improved access and visibility outside the mouth.

17 * Biocompatibility and good tissue response: Ceramic materials are considered the most chemically inert of all materials.

18 * Increased auxiliary support: Most indirect techniques allow the fabrication of the restoration to be totally or partially delegated to dental laboratory technicians.

19 Disadvantages

20 * Increased cost and time: Most indirect techniques require two patient appointments, plus fabrication of a temporary restoration. These factors, along with laboratory fees, contribute to the higher cost of indirect restorations relative to direct restorations.

21 * Technique sensitivity: Restorations made using indirect techniques require a high level of operator skill.
22 * Brittleness of ceramics: A ceramic restoration can fracture if the preparation does not provide adequate thickness to resist occlusal forces or if the restoration is not appropriately supported by the cement medium and the preparation.
23 * Wear of opposing dentition and restorations: Ceramic materials can cause excessive wear of opposing enamel or restorations.
24 * Resin-to-resin bonding difficulties: Laboratoryprocessed composites are highly cross-linked, so few double bonds remain available for chemical adhesion of the composite cement.
25 * Short clinical track record: Indirect bonded tooth-colored restorations have become relatively popular only in recent years and are still not placed by many practitioners.
26 * Low potential for repair: Indirect restorations, particularly ceramic inlays/onlays, are difficult to repair in the event of a partial fracture.
27 * Difficult try-in and delivery: Ceramics are more difficult to polish because of potential resin-filled marginal gaps and the hardness of the ceramic surfaces.
28 Laboratory-Processed Composite Inlays and Onlays
29 Processed composite restorations are indicated when:
30 (1) maximum wear resistance is desired from a composite restoration,
31 (2) achievement of proper contours and contacts would otherwise be difficult, and
32 (3) a ceramic restoration is not indicated because of cost or concerns about wear of the opposing dentition. Regarding the last-mentioned, the indirect composite would likely cause less wear of the opposing dentition than a similar ceramic restoration.
33 The fabrication steps for one representative system can be summarized as follows:
34 1. The indirect composite restoration is initially formed on a replica of the prepared tooth.
35
36
37 2. The composite is built up in layers, polymerizing each layer with a brief exposure to a visible light-curing unit.
38
39 3. After it is built to full contour, the restoration is coated with a special gel to block out air and thus prevent formation of an oxygen-inhibited surface layer.
40 4. Final curing is accomplished by inserting the inlay into an oven-like device that exposes the composite to additional light and heat, in some cases, pressure.
41
42 5. The cured composite inlay is trimmed, finished, and polished in the laboratory.
43
44 Ceramic Inlays and Onlays
45 Among the ceramic materials used are feldspathic porcelain, hot pressed ceramics, and machinable ceramics designed for use with CAD/CAM systems.
46 The physical and mechanical properties of ceramics come closer to matching those of enamel than do composites. They have excellent wear resistance and a coefficient of thermal expansion very close to that of tooth structure.
47 Feldspathic Porcelain Inlays and Onlays
48 The fabrication steps for fired ceramic inlays and onlays can be summarized as follows:
49 Master cast for MOD ceramic inlay. Die spacer is usually applied to axial walls and pulpal floor before duplication Master die is impressed, then a duplicate die is poured with refractory investment
50 Dental porcelains are added and fired in increments until inlay is the correct shape. Inlay is cleaned of all investment, then seated on master die for final adjustments and finishing. Ceramic inlay is now ready for delivery
51
52
53
54 Hot Pressed Glass-Ceramics
55 The fabrication steps for one type of leucitereinforced hot pressed ceramic restoration are summarized as follows:
56 Wax pattern for ceramic inlay Wax pattern on sprue base, ready to be invested
57 Device for pressing heated ceramic Ceramic inlay as pressed and before surface characterization
58 Inlay following surface characterization
59 Computed-Aided Design/Computed- Assisted Manufacturing: CAD/CAM
60 Rapid improvements in technology have spawned several computerized devices that can fabricate ceramic inlays and onlays from highquality ceramics in a matter of minutes.
61 Some CAD/CAM systems are very expensive laboratory-based units requiring the submission of an impression or working cast of the prepared tooth.
62 The CEREC system
63 The CEREC system was the first commercially available CAD/CAM system developed for the rapid chairside design and fabrication of ceramic restorations. The 2005 version of this device is the CEREC 3.
64 A B CEREC 2 (A) and CEREC 3 (B) CAD/CAM devices. These chairside units are compact and mobile.
65 Generation of a CEREC restoration begins after the dentist prepares the tooth and uses a scanning device to collect information about the shape of the preparation and its relationship with the surrounding structures.
66 An optical impression is made by placing a small video camera or scanner over the prepared tooth.
67 The restoration is designed on the computer screen by drawing position of gingival margins and proximal contacts.
68 B A, Computer-driven software controls two small, diamondcoated milling devices that cut the restoration out of a block of high-quality ceramic. B, The ceramic block rotates as the diamond cutting instruments move as needed to generate the restoration.
69 A major advantage is the quality of the restorative material. Manufacturers make blocks of "machinable ceramics" or "machinable composites" specifically for computer-assisted milling devices. Because these materials are fabricated under ideal industrial conditions, their physical properties have been optimized.
70 The major disadvantages of CAD/CAM systems are high cost and the need for extra training. However, CAD/CAM technology is changing rapidly, with each new generation of devices having more capability, accuracy, and ease of use.
71 CLINICAL PROCEDURES
72 Tooth Preparation
73 By definition, an onlay caps all cusps; an inlay may cap none, or may cap all but one cusp.
74 As a first clinical step: 1- The patient is anesthetized and the area isolated, preferably using rubber dam.
75 2- The compromised restoration (if present) is completely removed, and all the caries is excavated.
76 3- If necessary, the walls are restored to a more nearly ideal form with a light-cured glass-ionomer liner/base or a composite restorative material.
77 Preparations for indirect tooth-colored inlays and onlays are designed to provide adequate thickness for the restorative material and simultaneously a passive insertion pattern with rounded internal angles and well-defined margins.
78 1- All margins should have a 90- degree cavosurface angle to ensure marginal strength of the restoration.
79 2- All line and point angles, internal and external, should be rounded to avoid stress concentrations in the restoration and tooth, reducing the potential for fractures.
80
81
82
83 The carbide bur or diamond used for tooth preparation should be a tapering instrument that creates occlusally divergent facial and lingual walls.
84
85 The occlusal step should be prepared 1.5 to 2 mm in depth. Most composite and ceramic systems require that any isthmus be at least 2 mm wide to decrease the possibility of fracture of the restoration.
86 The pulpal floor should be smooth and relatively flat.
87 The facial, lingual, and gingival margins of the proximal boxes should be extended to clear the adjacent tooth by at least 0.5 mm. These clearances will provide adequate access to the margins for impression material and for finishing and polishing instruments.
88 For all walls, a 90-degree cavosurface margin is desired because composite and ceramic inlays are fragile in thin crosssection.
89 The gingival margin should be extended as minimally as possible because margins in enamel are greatly preferred for bonding, and because deep gingival margins are difficult to impress and to isolate properly during cementation.
90 A cusp usually should be capped if the extension is two thirds or greater than the distance from any primary groove to the cusp tip.
91
92
93 Impression
94 Most tooth-colored indirect inlay/onlay systems require an impression of the prepared tooth and the adjacent teeth as well as interocclusal records, which allow the restoration to be fabricated on a working cast in the laboratory
95 Temporary Restoration
96 A provisional restoration is necessary when using indirect systems that require two appointments. The temporary restoration protects the pulpdentin complex in vital teeth, maintains the position of the prepared tooth in the arch, and protects the soft tissues adjacent to prepared areas.
97 Temporary restorations for porcelain-fused-tometal and cast gold restorations typically are cemented with eugenol-based temporary cements.
98 Eeugenol is believed to interfere with resin polymerization, however, and potentially could reduce the adhesion of the permanent composite cement to tooth structure. Use of a noneugenol temporary cement is recommended.
99 When the temporary phase is expected to last longer than 2 to 3 weeks, zinc phosphate or polycarboxylate cement can be used to increase retention of the temporary restoration.
100 Computer-Aided Design/Computer- Assisted Manufacturing (CAD/CAM) Techniques
101 Using the CEREC system, an experienced dentist can prepare the tooth, fabricate an inlay, and deliver it in approximately 1 hour. This system eliminates the need for a conventional impression, temporary restoration, and multiple patient appointments.
102
103 A, CEREC inlay being milled. B, Completed inlay B
104 Try-in and Cementation
105 The inlay or onlay is placed into the preparation using very light pressure to evaluate its fit. If the restoration does not seat completely, the most likely cause is an overcontoured proximal surface.
106 A, Initial try-in of CEREC inlay. Proximal contacts are too tight and must be adjusted. B, Inlay seated after contact adjustment. Proximal surfaces of the inlay must be polished before cementation.
107 Cementation
108 For most laboratory-processed composite inlays/ onlays, the resin matrix has been polymerized to such an extent that few bonding sites are available for the composite cement to chemically bond to the internal surfaces of the restoration.
109 For ceramic inlays and onlays, hydrofluoric acid usually is used to etch the internal surfaces of the restoration.
110
111 Chairside ceramic etching is done with a 2- minute application of 10% hydrofluoric acid on the internal surfaces of the inlay/onlay.
112 After etching, the ceramic is treated with a silane coupling agent to facilitate chemical bonding of the composite cement.
113 Clear plastic matrix strips may be applied in each affected proximal area and wedged. The inlay/onlay can be tried in again and checked for fit.
114
115 The preparation surfaces are etched and treated with the components of an appropriate enamel/dentin bonding system. Typically, the final step of the bonding system (e.g., an unfilled resin) also is applied to the internal surfaces of the restoration previously etched and silanated.
116 A dual-cure composite cement is mixed and inserted into the preparation. The internal surfaces of the restoration are also coated with the composite cement and the inlay is immediately inserted into the prepared tooth, using light pressure.
117 A ball burnisher applied with a slight vibrating motion is usually sufficient to seat the restoration. Excess composite cement is removed with thin-bladed composite instruments, brushes, or an explorer
118 The operator must be careful not to remove composite from the marginal interface between the tooth and the inlay. The cement is now light-cured from occlusal, facial, and lingual directions for a minimum exposure of 60 seconds from each direction.
119 A, Enamel and dentin are etched with phosphoric acid. B, Dual-cured composite cement is applied to inlay. C, After application of the adhesive system, cement is applied to the preparation. D, CEREC ceramic inlay is seated into preparation.
120 Cont'd E and F, Before curing, excess composite cement is removed with explorer, brushes, and IPC carver. G, The composite cement is light-cured from occlusal, facial, and lingual directions.
121 Finishing and Polishing Procedures
122 A, Slender, fine-grit, flame-shaped, diamond instruments are used to remove flash along facial and lingual margins of CEREC ceramic inlay. B, 30-fluted finishing burs are used to smooth areas that were adjusted with diamonds.
123 A, Removing excess composite cement using a surgical blade. B, Smoothing the interproximal area with abrasive finishing strip.
124 Polishing sequence for ceramic inlays. A, After using fine-grit diamonds and 30-fluted carbide finishing burs to adjust contours and margins, rubber abrasive points and cups of successively finer grits are used at slow speed. B, Final polish imparted by porcelain polishing paste applied with bristle brush. C, Occlusal view of polished ceramic inlay.
125
126 Common Problems and Solutions
127 The most common cause of failure of tooth-colored inlays and onlays is bulk fracture. If bulk fracture occurs, replacement of the restoration is almost always indicated.
128 Repair of Tooth-Colored Inlays and Onlays
129 For composite and ceramic inlays, the repair procedure is initiated by mechanical roughening of involved surface.
130 For ceramic restorations, the initial mechanical roughening is followed by brief (typically 2 minutes) application of 10% hydrofluoric acid gel. Hydrofluoric acid etches the surface, creating further microdefects to facilitate mechanical bonding.
131 Although many indirect composites contain etchable glass filler particles, hydrofluoric acid treatment of composites is neither necessary nor recommended. However, a brief application of phosphoric acid may be used to clean the composite surface after roughening.
132 The next step in the repair procedure is application of a silane coupling agent. Silanes mediate chemical bonding between ceramics and resins and also may improve the predictability of resin-resin repairs.
133 After the silane has been applied, a resin adhesive agent is applied and light cured. A composite of the appropriate shade is placed, cured, contoured, and polished.
CHAPTER 10 RESTS AND PREPARATIONS. 4. Serve as a reference point for evaluating the fit of the framework to the teeth.
 CHAPTER 10 RESTS AND DEFINITIONS A REST is any rigid part of an RPD framework which contacts a properly prepared surface of a tooth. A REST PREPARATION or REST SEAT is any portion of a tooth or restoration
CHAPTER 10 RESTS AND DEFINITIONS A REST is any rigid part of an RPD framework which contacts a properly prepared surface of a tooth. A REST PREPARATION or REST SEAT is any portion of a tooth or restoration
Universal Crown and Bridge Preparation
 Universal Crown and Bridge Preparation The All-Ceramic Crown Preparation Technique for Predictable Success According to Dr. Ronald E. Goldstein Expect the Best. Buy Direct. The Universal * Crown and Bridge
Universal Crown and Bridge Preparation The All-Ceramic Crown Preparation Technique for Predictable Success According to Dr. Ronald E. Goldstein Expect the Best. Buy Direct. The Universal * Crown and Bridge
priti crown Your patients deserve you
 priti crown Your patients deserve you 3 and you deserve the priti crown So close to nature priti crown is a high-tech solution for making perfect crown and bridge restorations using state-of-the-art CAD/CAM
priti crown Your patients deserve you 3 and you deserve the priti crown So close to nature priti crown is a high-tech solution for making perfect crown and bridge restorations using state-of-the-art CAD/CAM
Implants in your Laboratory: Abutment Design
 1/2 point CDT documented scientific credit. See Page 41. Implants in your Laboratory: Abutment Design By Leon Hermanides, CDT A patient s anatomical limitations have the greatest predictive value for successful
1/2 point CDT documented scientific credit. See Page 41. Implants in your Laboratory: Abutment Design By Leon Hermanides, CDT A patient s anatomical limitations have the greatest predictive value for successful
Full Crown Module: Learner Level 1
 Full Crown Module Restoration / Tooth # Full Gold Crown (FGC) / 30 Extensions: Porcelain Fused to Metal (PFM) / 12 All Ceramic / 8 Learner Level 1 Mastery of Tooth Preparation Estimated Set Up Time: 30
Full Crown Module Restoration / Tooth # Full Gold Crown (FGC) / 30 Extensions: Porcelain Fused to Metal (PFM) / 12 All Ceramic / 8 Learner Level 1 Mastery of Tooth Preparation Estimated Set Up Time: 30
porcelain fused to metal crown
 Lectur.5 Dr.Adel F.Ibraheem porcelain fused to metal crown the most widely used fixed restoration,it is full metal crown having facial surface (or all surfaces) covered by ceramic material. It consist
Lectur.5 Dr.Adel F.Ibraheem porcelain fused to metal crown the most widely used fixed restoration,it is full metal crown having facial surface (or all surfaces) covered by ceramic material. It consist
20TDNH 214. Course Description:
 Revised: Fall 2015 20TDNH 214 20TPractical Materials for Dental Hygiene Course Description: 37TStudies the current technologic advances, expanded functions, and clinical/laboratory materials used in dental
Revised: Fall 2015 20TDNH 214 20TPractical Materials for Dental Hygiene Course Description: 37TStudies the current technologic advances, expanded functions, and clinical/laboratory materials used in dental
Jacket crown. Advantage : Crown and Bridge
 Crown and Bridge Lecture 1 Dr.Nibras AL-Kuraine Jacket crown It is a type of crown that is formed by a tooth colored material. It is mainly used as a single unit in the anterior quadrant of the mouth.
Crown and Bridge Lecture 1 Dr.Nibras AL-Kuraine Jacket crown It is a type of crown that is formed by a tooth colored material. It is mainly used as a single unit in the anterior quadrant of the mouth.
Restorative Guidelines
 Restorative Guidelines Contents Restorative Guidelines 4.1 Neoss Implant System 4.2 4.2 Esthetiline Solution 4.3 4.3 Provisional Abutments 4.8 4.4 Impression Techniques Implant Level 4.12 4.5 NeoLink
Restorative Guidelines Contents Restorative Guidelines 4.1 Neoss Implant System 4.2 4.2 Esthetiline Solution 4.3 4.3 Provisional Abutments 4.8 4.4 Impression Techniques Implant Level 4.12 4.5 NeoLink
your talent. our technology. the perfect fit.
 your talent. our technology. the perfect fit. itero - exclusively distributed in Europe by The digital revolution Changing the Face of Dentistry Digital technology ensures a more accurate impression from
your talent. our technology. the perfect fit. itero - exclusively distributed in Europe by The digital revolution Changing the Face of Dentistry Digital technology ensures a more accurate impression from
CLASS II AMALGAM. Design Principles
 CLASS II AMALGAM Design Principles CLASS II Class II cavitated caries lesions Class II cavitated caries lesions opaque white haloes identify areas of enamel undermining and decalcification from within
CLASS II AMALGAM Design Principles CLASS II Class II cavitated caries lesions Class II cavitated caries lesions opaque white haloes identify areas of enamel undermining and decalcification from within
portion of the tooth such as 3/4 Crown, 7/8Crown.
 Lecture.1 Dr.Adel F.Ibraheem Crown and Bridge: It s a branch of dental science that deals with restoration of damaged teeth with artificial crown replacing the missing natural teeth by a cast prosthesis
Lecture.1 Dr.Adel F.Ibraheem Crown and Bridge: It s a branch of dental science that deals with restoration of damaged teeth with artificial crown replacing the missing natural teeth by a cast prosthesis
Composite artistry- speedy mock up
 Case Report: Composite artistry- speedy mock up Dr.Shikha Kanodia*, Dr.Manjit Kaur**, Dr.Girish J. Parmar*** * Asst. Professor, **Post Graduate Part 3, ***Head and Dean, Department of Conservative Dentistry
Case Report: Composite artistry- speedy mock up Dr.Shikha Kanodia*, Dr.Manjit Kaur**, Dr.Girish J. Parmar*** * Asst. Professor, **Post Graduate Part 3, ***Head and Dean, Department of Conservative Dentistry
Tooth preparation J. C. Davenport, 1 R. M. Basker, 2 J. R. Heath, 3 J. P. Ralph, 4 P-O. Glantz, 5 and P. Hammond, 6
 12 5 Tooth preparation J. C. Davenport, 1 R. M. Basker, 2 J. R. Heath, 3 J. P. Ralph, 4 P-O. Glantz, 5 and P. Hammond, 6 This final article in the series describes the modification of teeth to improve
12 5 Tooth preparation J. C. Davenport, 1 R. M. Basker, 2 J. R. Heath, 3 J. P. Ralph, 4 P-O. Glantz, 5 and P. Hammond, 6 This final article in the series describes the modification of teeth to improve
WAX-UP AND CERAMIC EXTENSIVE COURSE Dr. Dario Adolfi Dr. Ivan Ronald Huanca
 WAX-UP AND CERAMIC EXTENSIVE COURSE Dr. Dario Adolfi Dr. Ivan Ronald Huanca Duration: 6 meses STEP 1: WAX-UP OF FOUR UPPER POSTERIOR TEETH with Dr. Ivan Ronald Huanca The objective of this course s step
WAX-UP AND CERAMIC EXTENSIVE COURSE Dr. Dario Adolfi Dr. Ivan Ronald Huanca Duration: 6 meses STEP 1: WAX-UP OF FOUR UPPER POSTERIOR TEETH with Dr. Ivan Ronald Huanca The objective of this course s step
STEP-BY-STEP INSTRUCTIONS ON THE PROSTHETIC PROCEDURES. Straumann Anatomic IPS e.max Abutment
 STEP-BY-STEP INSTRUCTIONS ON THE PROSTHETIC PROCEDURES Straumann Anatomic IPS e.max Abutment The ITI (International Team for Implantology) is academic partner of Institut Straumann in the areas of research
STEP-BY-STEP INSTRUCTIONS ON THE PROSTHETIC PROCEDURES Straumann Anatomic IPS e.max Abutment The ITI (International Team for Implantology) is academic partner of Institut Straumann in the areas of research
IPS e.max CAD C16. Larger Size Block Low translucency Shades: A1, A2, A3, A3.5, B1, B2, C1, C2, D2, BL2 Indicated for single unit restorations
 IPS e.max CAD C16 IPS e.max CAD C16 Larger Size Block Low translucency Shades: A1, A2, A3, A3.5, B1, B2, C1, C2, D2, BL2 Indicated for single unit restorations Full and partial coverage single units Large
IPS e.max CAD C16 IPS e.max CAD C16 Larger Size Block Low translucency Shades: A1, A2, A3, A3.5, B1, B2, C1, C2, D2, BL2 Indicated for single unit restorations Full and partial coverage single units Large
Advances in All Ceramic Restorations. Alaa AlQutub Umm AlQura University, Faculty of Dentistry
 Advances in All Ceramic Restorations Alaa AlQutub Umm AlQura University, Faculty of Dentistry Types of materials used in esthetic zone I. Metal ceramic restoration: Metal ceramic alloy features : Produce
Advances in All Ceramic Restorations Alaa AlQutub Umm AlQura University, Faculty of Dentistry Types of materials used in esthetic zone I. Metal ceramic restoration: Metal ceramic alloy features : Produce
ATLANTIS abutments design guide CAD/CAM patient-specific abutments
 ATLANTIS abutments design guide CAD/CAM patient-specific abutments Contents Introduction 4 This manual helps you to explore all the benefits of ATLANTIS CAD/CAM patient-specific abutments. It gives you
ATLANTIS abutments design guide CAD/CAM patient-specific abutments Contents Introduction 4 This manual helps you to explore all the benefits of ATLANTIS CAD/CAM patient-specific abutments. It gives you
CLASSIFICATION OF CARIOUS LESIONS AND TOOTH PREPARATION.
 CLASSIFICATION OF CARIOUS LESIONS AND TOOTH PREPARATION. ١ G.V. BLACK who is known as the father of operative dentistry,he classified carious lesions into groups according to their locations in permanent
CLASSIFICATION OF CARIOUS LESIONS AND TOOTH PREPARATION. ١ G.V. BLACK who is known as the father of operative dentistry,he classified carious lesions into groups according to their locations in permanent
Prosthetic Manual. Implant System. Contact Us: Smarter thinking. Simpler design. Phone: 866-902-9272 781-328-3490. Fax: 866-903-9272 781-328-3400
 Contact Us: Implant System Phone: 866-902-9272 781-328-3490 Fax: 866-903-9272 781-328-3400 Prosthetic Manual Mail: Keystone Dental, Inc. 144 Middlesex Turnpike Burlington, MA 01803 USA www.keystonedental.com
Contact Us: Implant System Phone: 866-902-9272 781-328-3490 Fax: 866-903-9272 781-328-3400 Prosthetic Manual Mail: Keystone Dental, Inc. 144 Middlesex Turnpike Burlington, MA 01803 USA www.keystonedental.com
How to Achieve Shade Harmony With Different Restorations
 Procera Alumina vs. Feldspathic Porcelain How to Achieve Shade Harmony With Different Restorations Luke S. Kahng, CDT Key Words: Stump shade, Feldspathic Porcelain, Zirconia, Alumina, LSK Treatment Plan
Procera Alumina vs. Feldspathic Porcelain How to Achieve Shade Harmony With Different Restorations Luke S. Kahng, CDT Key Words: Stump shade, Feldspathic Porcelain, Zirconia, Alumina, LSK Treatment Plan
Anterior crowns used in children
 Anterior crowns used in children Objectives of this session Discuss strip crowns, temporary crown use and acrylic jacket crowns. Discuss the possible use of porcelain jacket crowns in paediatric dental
Anterior crowns used in children Objectives of this session Discuss strip crowns, temporary crown use and acrylic jacket crowns. Discuss the possible use of porcelain jacket crowns in paediatric dental
Replacement of the upper left central incisor with a Straumann Bone Level Implant and a Straumann Customized Ceramic Abutment
 Replacement of the upper left central incisor with a Straumann Bone Level Implant and a Straumann Customized Ceramic Abutment by Dr. Ronald Jung and Master Dental Technician Xavier Zahno Initial situation
Replacement of the upper left central incisor with a Straumann Bone Level Implant and a Straumann Customized Ceramic Abutment by Dr. Ronald Jung and Master Dental Technician Xavier Zahno Initial situation
Implant Abutments and Crowns on your CEREC. Welcome
 Welcome Welcome Welcome Robert Marcus D.M.D. UConn Dental 1993 Poway (SD) office since 1997 CEREC user since 2004 CEREC Mentor and Trainer Founder of Kick Your Apps, Inc. Control Freak Welcome Many thanks
Welcome Welcome Welcome Robert Marcus D.M.D. UConn Dental 1993 Poway (SD) office since 1997 CEREC user since 2004 CEREC Mentor and Trainer Founder of Kick Your Apps, Inc. Control Freak Welcome Many thanks
American Academy of Cosmetic Dentistry. Laboratory Technician Clinical Case Type II. One or Two Indirect Restorations
 American Academy of Cosmetic Dentistry Laboratory Technician Clinical Case Type II One or Two Indirect Restorations AACD Member ID # 00000 EXAMPLE REPORT Treatment List #8, #9 All Ceramic Crowns Restorative
American Academy of Cosmetic Dentistry Laboratory Technician Clinical Case Type II One or Two Indirect Restorations AACD Member ID # 00000 EXAMPLE REPORT Treatment List #8, #9 All Ceramic Crowns Restorative
stone model bonding tray improve the accuracy
 indirectbonding Bonding brackets to the patient s stone model and transferring the bonding tray to the patient s mouth Developed to improve the accuracy of bracket placement (especially premolars) advantagesdisadvantages
indirectbonding Bonding brackets to the patient s stone model and transferring the bonding tray to the patient s mouth Developed to improve the accuracy of bracket placement (especially premolars) advantagesdisadvantages
Choosing the right type of abutment
 50 Producing custom implant abutments using CAD/CAM Choosing the right type of abutment S. KHALILOVA 1, F. KISTLER 2, S. ADLER 3, S. WEISS 3, S. KISTLER 2 AND J. NEUGEBAUER 2,4 Rapid developments in the
50 Producing custom implant abutments using CAD/CAM Choosing the right type of abutment S. KHALILOVA 1, F. KISTLER 2, S. ADLER 3, S. WEISS 3, S. KISTLER 2 AND J. NEUGEBAUER 2,4 Rapid developments in the
Implant Bar Overdenture Utilizing Locator Attachments
 Utilizing Locator Attachments Step-by-Step Restorative Protocol Implant Bar Overdentures offer a removable implant solution for edentulous patients desiring a stable and esthetic prosthesis that improves
Utilizing Locator Attachments Step-by-Step Restorative Protocol Implant Bar Overdentures offer a removable implant solution for edentulous patients desiring a stable and esthetic prosthesis that improves
Contents. Cement retained restoration. Screw retained restoration. Overdenture retained restoration. TS Implant System. 70 ComOcta Gold Abutment
 Contents TS Implant System Cement retained restoration Screw retained restoration 06 Cement-retained bridges with the Solid abutment system (non- 72 Screw retained crown with the ComOcta Gold abutment
Contents TS Implant System Cement retained restoration Screw retained restoration 06 Cement-retained bridges with the Solid abutment system (non- 72 Screw retained crown with the ComOcta Gold abutment
STEPS IN CARVING AMALGAM class 2 cavity 2004-2005
 1 STEPS IN CARVING AMALGAM class 2 cavity 2004-2005 Word to the wise: Study of the occlusion, together with the remaining tooth contour and position of the adjacent tooth, before starting a cavity preparation,
1 STEPS IN CARVING AMALGAM class 2 cavity 2004-2005 Word to the wise: Study of the occlusion, together with the remaining tooth contour and position of the adjacent tooth, before starting a cavity preparation,
Restoration of a screw retained single tooth restoration in the upper jaw with Thommen Titanium base abutment.
 Restoration of a screw retained single tooth restoration in the upper jaw with Thommen Titanium base abutment. Dr. med. dent. David McFadden, Dallas County, USA Initial situation (single X-ray) Tooth 16
Restoration of a screw retained single tooth restoration in the upper jaw with Thommen Titanium base abutment. Dr. med. dent. David McFadden, Dallas County, USA Initial situation (single X-ray) Tooth 16
ATLANTIS abutments as individual as your patients
 ATLANTIS abutments as individual as your patients ATLANTIS the freedom of unlimited possibilities Discover why ATLANTIS CAD/CAM abutments are the natural choice for patientspecific, cement-retained implant
ATLANTIS abutments as individual as your patients ATLANTIS the freedom of unlimited possibilities Discover why ATLANTIS CAD/CAM abutments are the natural choice for patientspecific, cement-retained implant
PROSTHETICS. Crown and bridge restorations with the synocta prosthetic system. www.straumann.com
 PROSTHETICS Crown and bridge restorations with the synocta prosthetic system www.straumann.com Straumann is the exclusive industrial partner of the ITI (International Team for Implantology) in the areas
PROSTHETICS Crown and bridge restorations with the synocta prosthetic system www.straumann.com Straumann is the exclusive industrial partner of the ITI (International Team for Implantology) in the areas
Do s and Don ts of Porcelain Laminate Veneers
 Do s and Don ts of Porcelain Laminate Veneers Chad J. Anderson, MS, DMD; Gerard Kugel, DMD, MS, PhD; Shradha Sharma, BDS, DMD Continuing Education Units: 2 hours Online Course: www.dentalcare.com/en-us/dental-education/continuing-education/ce333/ce333.aspx
Do s and Don ts of Porcelain Laminate Veneers Chad J. Anderson, MS, DMD; Gerard Kugel, DMD, MS, PhD; Shradha Sharma, BDS, DMD Continuing Education Units: 2 hours Online Course: www.dentalcare.com/en-us/dental-education/continuing-education/ce333/ce333.aspx
ARTICLE 20-03 DENTAL ASSISTANTS CHAPTER 20-03-01 DUTIES
 ARTICLE 20-03 DENTAL ASSISTANTS Chapter 20-03-01 Duties CHAPTER 20-03-01 DUTIES Section 20-03-01-01 Duties 20-03-01-01.1 Expanded Duties of Registered Dental Assistants 20-03-01-02 Prohibited Services
ARTICLE 20-03 DENTAL ASSISTANTS Chapter 20-03-01 Duties CHAPTER 20-03-01 DUTIES Section 20-03-01-01 Duties 20-03-01-01.1 Expanded Duties of Registered Dental Assistants 20-03-01-02 Prohibited Services
THE VOICE OF TECHNO-CLINICAL DENTISTRY
 May 2009 Vol. 3, No. 2 THE VOICE OF TECHNO-CLINICAL DENTISTRY The Enhanced Restoration of Removables Jim Collis, CDT Patients with existing full or partial dentures often report that they would like to
May 2009 Vol. 3, No. 2 THE VOICE OF TECHNO-CLINICAL DENTISTRY The Enhanced Restoration of Removables Jim Collis, CDT Patients with existing full or partial dentures often report that they would like to
BASIC INFORMATION ON THE STRAUMANN VARIOBASE ABUTMENT. Straumann Variobase Abutment
 BASIC INFORMATION ON THE STRAUMANN VARIOBASE ABUTMENT Straumann Variobase Abutment 1 The ITI (International Team for Implantology) is academic partner of Institut Straumann AG in the areas of research
BASIC INFORMATION ON THE STRAUMANN VARIOBASE ABUTMENT Straumann Variobase Abutment 1 The ITI (International Team for Implantology) is academic partner of Institut Straumann AG in the areas of research
ADA Insurance Codes for Laboratory Procedures:
 ADA Insurance Codes for Laboratory Procedures: Inlay/Onlay Restorations D2510 Inlay - metallic - one surface D2520 Inlay - metallic - two surfaces D2530 Inlay - metallic - three or more surfaces D2542
ADA Insurance Codes for Laboratory Procedures: Inlay/Onlay Restorations D2510 Inlay - metallic - one surface D2520 Inlay - metallic - two surfaces D2530 Inlay - metallic - three or more surfaces D2542
dental fillings facts About the brochure:
 dental fillings facts About the brochure: Your dentist is dedicated to protecting and improving oral health while providing safe dental treatment. This fact sheet provides information you need to discuss
dental fillings facts About the brochure: Your dentist is dedicated to protecting and improving oral health while providing safe dental treatment. This fact sheet provides information you need to discuss
Another Implant Option for Missing Teeth with Challenging Symmetry Patrick Gannon, DDS and Luke Kahng, CDT
 Another Implant Option for Missing Teeth with Challenging Symmetry Patrick Gannon, DDS and Luke Kahng, CDT Introduction A 58 year old male had been missing teeth #7=12 for approximately 28 years. During
Another Implant Option for Missing Teeth with Challenging Symmetry Patrick Gannon, DDS and Luke Kahng, CDT Introduction A 58 year old male had been missing teeth #7=12 for approximately 28 years. During
The Attractive Glass Abutment System (ZX-27) HANDOUT
 HANDOUT") The Attractive Glass Abutment System () HANDOUT! " " # $ % $ # & ' ( ) FAQs New Solutions Pharmaceuticals Tel.: +971 6 7460661 Fax : +971 6 7460771 P.O.Box. 18161 Ajman - UAE e-mail : [email protected]
The Attractive Glass Abutment System () HANDOUT! " " # $ % $ # & ' ( ) FAQs New Solutions Pharmaceuticals Tel.: +971 6 7460661 Fax : +971 6 7460771 P.O.Box. 18161 Ajman - UAE e-mail : [email protected]
Seeing CAD/CAM in a new light.
 CAD/ CAM SYSTEMS INSTRUMENTS HYGIENE SYSTEMS TREATMENT CENTERS IMAGING SYSTEMS CEREC NEW PRODUCTS 2009 Seeing CAD/CAM in a new light. T h e D e n t a l C o m p a n y Precision and simplicity redefined.
CAD/ CAM SYSTEMS INSTRUMENTS HYGIENE SYSTEMS TREATMENT CENTERS IMAGING SYSTEMS CEREC NEW PRODUCTS 2009 Seeing CAD/CAM in a new light. T h e D e n t a l C o m p a n y Precision and simplicity redefined.
Structur. Structur 2 SC / Structur Premium EXCELLENT TEMPORARIES WITH STRUCTUR
 Structur Structur 2 SC / Structur Premium EXCELLENT TEMPORARIES WITH STRUCTUR Simple to use Reliable products are required to provide your patients with prosthetic treatments, especially with regard to
Structur Structur 2 SC / Structur Premium EXCELLENT TEMPORARIES WITH STRUCTUR Simple to use Reliable products are required to provide your patients with prosthetic treatments, especially with regard to
Abutment Solutions For customized implant restorations fabricated with CEREC and inlab. Digital all around.
 Abutment Solutions For customized implant restorations fabricated with CEREC and inlab Digital all around. The digital treatment workflow Digital impression taking Coordinated digital workflows in CAD/CAM
Abutment Solutions For customized implant restorations fabricated with CEREC and inlab Digital all around. The digital treatment workflow Digital impression taking Coordinated digital workflows in CAD/CAM
Procedures & Products. NobelEsthetics
 Procedures & Products NobelEsthetics First from Nobel Biocare. NobelPerfect, (NP, RP, WP), NobelDirect (NP, RP, WP), Brånemark System, NobelReplace and NobelSpeedy Implants. A complete assortment with
Procedures & Products NobelEsthetics First from Nobel Biocare. NobelPerfect, (NP, RP, WP), NobelDirect (NP, RP, WP), Brånemark System, NobelReplace and NobelSpeedy Implants. A complete assortment with
Porcelain Veneers for Children and Teens. By Fred S. Margolis, D.D.S., F.I.C.D., F.A.C.D., F.A.D.I. Abstract
 Porcelain Veneers for Children and Teens By Fred S. Margolis, D.D.S., F.I.C.D., F.A.C.D., F.A.D.I. Abstract This article will discuss the advantages of providing our young patients and their parents an
Porcelain Veneers for Children and Teens By Fred S. Margolis, D.D.S., F.I.C.D., F.A.C.D., F.A.D.I. Abstract This article will discuss the advantages of providing our young patients and their parents an
FABRICATING CUSTOM ABUTMENTS
 FABRICATING CUSTOM ABUTMENTS LUC AND PATRICK RUTTEN How much should a Dental Technician know about the clinical aspects of implantology? The answer is clear: as much as possible. This is the distinction
FABRICATING CUSTOM ABUTMENTS LUC AND PATRICK RUTTEN How much should a Dental Technician know about the clinical aspects of implantology? The answer is clear: as much as possible. This is the distinction
Chart 1. Chart 2. How to Use the Following Charts. Be sure to follow the legal requirements to perform dental radiographic procedures.
 These data are presented for informational purposes only and are not intended as a legal opinion regarding dental practice in any state. DANB confers with each state s dental board at least annually regarding
These data are presented for informational purposes only and are not intended as a legal opinion regarding dental practice in any state. DANB confers with each state s dental board at least annually regarding
Chart 1. Chart 2. How to Use the Following Charts. Be sure to follow the legal requirements to perform dental radiographic procedures.
 These data are presented for informational purposes only and are not intended as a legal opinion regarding dental practice in any state. DANB confers with each state s dental board at least annually regarding
These data are presented for informational purposes only and are not intended as a legal opinion regarding dental practice in any state. DANB confers with each state s dental board at least annually regarding
Clinical randomized controlled study of Class II restorations of a highly filled nanohybrid resin composite (4U)
") 215-3-3 Clinical randomized controlled study of Class II restorations of a highly filled nanohybrid resin composite () One year report JWV van Dijken, Professor Director Clinical Research Biomaterial Research
215-3-3 Clinical randomized controlled study of Class II restorations of a highly filled nanohybrid resin composite () One year report JWV van Dijken, Professor Director Clinical Research Biomaterial Research
procedures & products NOBELESTHETICS including Procera
 procedures & products NOBELESTHETICS including Procera First from Nobel Biocare. NOBELPERFECT, (NP, RP, WP), NOBELDIRECT (NP, RP, WP), Brånemark System, NOBELREPLACE and NOBELSPEEDY Implants. A complete
procedures & products NOBELESTHETICS including Procera First from Nobel Biocare. NOBELPERFECT, (NP, RP, WP), NOBELDIRECT (NP, RP, WP), Brånemark System, NOBELREPLACE and NOBELSPEEDY Implants. A complete
ZIRCONIA INFORMATION FOR DENTISTS. FAQ S from the dental practice ENGLISH
 ZIRCONIA INFORMATION FOR DENTISTS FAQ S from the dental practice ENGLISH Zr Facts and Answers 2 Facts and Answers What is Zirconia? Zirconium (ZrSiO ) belongs to the mineral group of silicates and 4 was
ZIRCONIA INFORMATION FOR DENTISTS FAQ S from the dental practice ENGLISH Zr Facts and Answers 2 Facts and Answers What is Zirconia? Zirconium (ZrSiO ) belongs to the mineral group of silicates and 4 was
Full Crown Module: Learner Level 3
 Full Crown Module Restoration / Tooth # Full Gold Crown (FGC) / mesially tilted 30 Extensions: Porcelain Fused to Metal (PFM) / lingually 21 All Ceramic / rotated 12 Learner Level 3 Preparation of Malpositioned
Full Crown Module Restoration / Tooth # Full Gold Crown (FGC) / mesially tilted 30 Extensions: Porcelain Fused to Metal (PFM) / lingually 21 All Ceramic / rotated 12 Learner Level 3 Preparation of Malpositioned
PROSTHETIC PROCEDURE. for HG IMPLANT SYSTEM
 PROSTHETIC PROCEDURE for HG IMPLANT SYSTEM PROSTHETIC PROCEDURE for HG IMPLANT SYSTEM HG Implant System Contents Cement retained restoration Rigid abutment When abutment reduction is unnecessary When abutment
PROSTHETIC PROCEDURE for HG IMPLANT SYSTEM PROSTHETIC PROCEDURE for HG IMPLANT SYSTEM HG Implant System Contents Cement retained restoration Rigid abutment When abutment reduction is unnecessary When abutment
DENT 5351 Final Examination 2007 NAME
 NAME DENT 5351 Spring Semester 2007 INTRDUCTIN T BIMATERIALS FINAL EXAMINATIN (40 questions) February 16, 2007 8:00 a.m. 9:00 a.m. This final examination consists of 7 pages and 40 questions. Mark all
NAME DENT 5351 Spring Semester 2007 INTRDUCTIN T BIMATERIALS FINAL EXAMINATIN (40 questions) February 16, 2007 8:00 a.m. 9:00 a.m. This final examination consists of 7 pages and 40 questions. Mark all
Digital impression solutions. 3M True Definition Scanner. Precise. impressions. in a jiffy
 Digital impression solutions 3M True Definition Scanner Precise impressions in a jiffy True Definition Scanner Digital impressioning redefined Easy handling. Desired result. With the 3M True Definition
Digital impression solutions 3M True Definition Scanner Precise impressions in a jiffy True Definition Scanner Digital impressioning redefined Easy handling. Desired result. With the 3M True Definition
Waxing up. Waxing up. Crown and bridgework. Friedrich Jetter Christian Pilz. Ideas for dental technology
 Waxing up Waxing up Crown and bridgework Friedrich Jetter Christian Pilz Ideas for dental technology Waxing-up units Waxing-up units Waxlectric II The Waxlectric II is an electrically regulated sculpting
Waxing up Waxing up Crown and bridgework Friedrich Jetter Christian Pilz Ideas for dental technology Waxing-up units Waxing-up units Waxlectric II The Waxlectric II is an electrically regulated sculpting
Crown and Bridge Restorations. Straumann synocta Prosthetic System
 Crown and Bridge Restorations Straumann synocta Prosthetic System The ITI (International Team for Implantology) is academic partner of Institut Straumann AG in the areas of research and education. Contents
Crown and Bridge Restorations Straumann synocta Prosthetic System The ITI (International Team for Implantology) is academic partner of Institut Straumann AG in the areas of research and education. Contents
PROSTHETICS. Crown and Bridge Restorations with the synocta Prosthetic System DENTAL IMPLANT SYSTEM
 PROSTHETICS Crown and Bridge Restorations with the synocta Prosthetic System DENTAL IMPLANT SYSTEM IMPORTANT NOTES Disclaimer of liability The ITI dental implant is part of an overall concept and may only
PROSTHETICS Crown and Bridge Restorations with the synocta Prosthetic System DENTAL IMPLANT SYSTEM IMPORTANT NOTES Disclaimer of liability The ITI dental implant is part of an overall concept and may only
Amalgam Fillings. Are dental amalgams safe?
 Amalgam Fillings Used by dentists for more than a century, dental amalgam is the most thoroughly researched and tested restorative material among all those in use. It is durable, easy to use, highly resistant
Amalgam Fillings Used by dentists for more than a century, dental amalgam is the most thoroughly researched and tested restorative material among all those in use. It is durable, easy to use, highly resistant
ADA Standards Committee on Dental Products National Standards Status of Projects. Standard # Title of Standard WG Status Activity
 ANSI/ADA 1-2003 (R2013) Alloy for Dental Amalgam 1.2 AS 0 ADA 6-1987 Dental Mercury 1.2 AS 0 ANSI/ADA 15-2008 (R2013) Artificial Teeth for Dental Prostheses 2.11 AP 0 ANSI/ADA 17-1983 (R2014) Denture Base
ANSI/ADA 1-2003 (R2013) Alloy for Dental Amalgam 1.2 AS 0 ADA 6-1987 Dental Mercury 1.2 AS 0 ANSI/ADA 15-2008 (R2013) Artificial Teeth for Dental Prostheses 2.11 AP 0 ANSI/ADA 17-1983 (R2014) Denture Base
Taking the Mystique out of Implant Dentistry. Dr. Michael Weinberg B.Sc., DDS, FICOI
 Taking the Mystique out of Implant Dentistry Dr. Michael Weinberg B.Sc., DDS, FICOI What is Restorative Implant Dentistry? Restorative implant dentistry involves taking a few simple mechanical principles
Taking the Mystique out of Implant Dentistry Dr. Michael Weinberg B.Sc., DDS, FICOI What is Restorative Implant Dentistry? Restorative implant dentistry involves taking a few simple mechanical principles
DENTAL ADVANTAGE HELPFUL HINTS FOR THE RDA PRACTICAL EXAM
 DENTAL ADVANTAGE HELPFUL HINTS FOR THE RDA PRACTICAL EXAM 1. Arrive early for the exam. Bring with you: *lab coat *protective eyewear *gloves *mask *optional flashlight and watch *deposit for rental kit
DENTAL ADVANTAGE HELPFUL HINTS FOR THE RDA PRACTICAL EXAM 1. Arrive early for the exam. Bring with you: *lab coat *protective eyewear *gloves *mask *optional flashlight and watch *deposit for rental kit
IPS Empress CAD for CAD/CAM technology Information for Dentists. Confidence. Reliability. Esthetics. Empress CAD. The world s leading all-ceramic
 CAD for CAD/CAM technology Information for Dentists Confidence Reliability Esthetics The world s leading all-ceramic A time-tested system with new possibilities More versatility with revolutionized the
CAD for CAD/CAM technology Information for Dentists Confidence Reliability Esthetics The world s leading all-ceramic A time-tested system with new possibilities More versatility with revolutionized the
IPS. Special Edition. Press-on-Metal Ceramic. Harald Gritsch Max Wörishofer Christoph Zobler
 InLine PoM Press-on-Metal Ceramic IPS Special Edition Harald Gritsch Max Wörishofer Christoph Zobler Press-on technique on metal frameworks Combining the widely known casting technique and press technique
InLine PoM Press-on-Metal Ceramic IPS Special Edition Harald Gritsch Max Wörishofer Christoph Zobler Press-on technique on metal frameworks Combining the widely known casting technique and press technique
Dentalworkers JOB DESCRIPTIONS Great Team Members make your Office function!
 Dentalworkers JOB DESCRIPTIONS Great Team Members make your Office function! Dental Assistant Registered Dental Assistant with Expanded Function: RDAEF Sterilization Assistant Dental Hygienist General
Dentalworkers JOB DESCRIPTIONS Great Team Members make your Office function! Dental Assistant Registered Dental Assistant with Expanded Function: RDAEF Sterilization Assistant Dental Hygienist General
Implant Parts. A Radford Heath Guide http://www.radfordheath.com 1
 Implant Parts A Radford Heath Guide http://www.radfordheath.com 1 Disclaimer The information given in this document has been provided in good faith for basic information purposes only and the information
Implant Parts A Radford Heath Guide http://www.radfordheath.com 1 Disclaimer The information given in this document has been provided in good faith for basic information purposes only and the information
A collection of pus. Usually forms because of infection. A tooth or tooth structure which is responsible for the anchorage of a bridge or a denture.
 Abscess A collection of pus. Usually forms because of infection. Abutment A tooth or tooth structure which is responsible for the anchorage of a bridge or a denture. Amalgam A silver filling material.
Abscess A collection of pus. Usually forms because of infection. Abutment A tooth or tooth structure which is responsible for the anchorage of a bridge or a denture. Amalgam A silver filling material.
Prosthodontist s Perspective
 Unless otherwise noted, the content of this course material is licensed under a Creative Commons Attribution - Non-Commercial - Share Alike 3.0 License. Copyright 2008, Dr. Jeff Shotwell. The following
Unless otherwise noted, the content of this course material is licensed under a Creative Commons Attribution - Non-Commercial - Share Alike 3.0 License. Copyright 2008, Dr. Jeff Shotwell. The following
1- Fatigue-Resistance and Microleakage of CAD/CAM Ceramic and Composite Molar crowns
 1- Fatigue-Resistance and Microleakage of CAD/CAM Ceramic and Composite Molar crowns A. KASSEM1, O. ATTA1, and O. EL-MOWAFY2, 1Suez Canal University, Ismailia, Egypt, 2University of Toronto, Toronto, ON,
1- Fatigue-Resistance and Microleakage of CAD/CAM Ceramic and Composite Molar crowns A. KASSEM1, O. ATTA1, and O. EL-MOWAFY2, 1Suez Canal University, Ismailia, Egypt, 2University of Toronto, Toronto, ON,
Press Abutment Solutions
 Press Abutment Solutions Efficiency and esthetics redefined all ceramic all you need More press ceramic options... Press ceramics have been synonymous with the ideal combination of accuracy of fit, shape
Press Abutment Solutions Efficiency and esthetics redefined all ceramic all you need More press ceramic options... Press ceramics have been synonymous with the ideal combination of accuracy of fit, shape
Treatment planning for the class 0, 1A, 1B dental arches
 Treatment planning for the class 0, 1A, 1B dental arches Dr.. Peter Hermann Dr Reminder: Torquing movement on tooth supported denture : no movement Class 1 movement in one direction (depression) Class
Treatment planning for the class 0, 1A, 1B dental arches Dr.. Peter Hermann Dr Reminder: Torquing movement on tooth supported denture : no movement Class 1 movement in one direction (depression) Class
Structur 3. Gloss without polishing. Structur 3. Composite material for the fabrication of
 Composite material for the fabrication of temporary crowns and bridges Gloss without polishing 3 for temporary crowns and bridges with a sheen is a self-polymerising composite material for the fabrication
Composite material for the fabrication of temporary crowns and bridges Gloss without polishing 3 for temporary crowns and bridges with a sheen is a self-polymerising composite material for the fabrication
Removing fixed prostheses using the ATD automatic crown and bridge remover
 Removing fixed prostheses using the ATD automatic crown and bridge remover By Dr. Ian E. Shuman, Baltimore, MD. Information provided by J. Morita USA When removing cemented provisionals and final fixed
Removing fixed prostheses using the ATD automatic crown and bridge remover By Dr. Ian E. Shuman, Baltimore, MD. Information provided by J. Morita USA When removing cemented provisionals and final fixed
LOCATOR ROOT ATTACHMENT SYSTEM
 TECHNIQUE MANUAL LOCATOR ROOT ATTACHMENT SYSTEM IMPORTANT: This document contains the most current instructions for use. Please, read and retain. DESCRIPTION: Universal hinge, resilient attachment for
TECHNIQUE MANUAL LOCATOR ROOT ATTACHMENT SYSTEM IMPORTANT: This document contains the most current instructions for use. Please, read and retain. DESCRIPTION: Universal hinge, resilient attachment for
Call 1-800-445-0345 today to find a course near you!
 LEARN THE MOST EXCITING DEVELOPMENT IN SMILE ENHANCEMENT DON T FORGET TO ASK ABOUT CERINATE COURSES: DESTINATION EDUCATION 3-day seminar in vacation locations CERINATE SMILE DESIGN WORKSHOPS 2-day hands-on
LEARN THE MOST EXCITING DEVELOPMENT IN SMILE ENHANCEMENT DON T FORGET TO ASK ABOUT CERINATE COURSES: DESTINATION EDUCATION 3-day seminar in vacation locations CERINATE SMILE DESIGN WORKSHOPS 2-day hands-on
2007 Insurance Benefits Guide. Dental and Dental Plus. Dental and. Dental Plus. www.eip.sc.gov Employee Insurance Program 91
 Dental and www.eip.sc.gov Employee Insurance Program 91 Table of Contents Introduction...93 Your Dental Benefits at a Glance...94 Claim Examples (using Class III procedure claims)...95 How to File a Dental
Dental and www.eip.sc.gov Employee Insurance Program 91 Table of Contents Introduction...93 Your Dental Benefits at a Glance...94 Claim Examples (using Class III procedure claims)...95 How to File a Dental
CDT 2015 Code Change Summary New codes effective 1/1/2015
 CDT 2015 Code Change Summary New codes effective 1/1/2015 Code Nomenclature Delta Dental Policy D0171 Re-Evaluation Post Operative Office Visit Not a Covered Benefit D0351 3D Photographic Image Not a Covered
CDT 2015 Code Change Summary New codes effective 1/1/2015 Code Nomenclature Delta Dental Policy D0171 Re-Evaluation Post Operative Office Visit Not a Covered Benefit D0351 3D Photographic Image Not a Covered
Zirconium Abutments for Improved Esthetics in Anterior Restorations
 Zirconium Abutments for Improved Esthetics in Anterior Restorations by Luke S., C.D.T. Mr. is the founder and owner of Capital Dental Technology Laboratory, Inc., in Naperville, Illinois. The laboratory
Zirconium Abutments for Improved Esthetics in Anterior Restorations by Luke S., C.D.T. Mr. is the founder and owner of Capital Dental Technology Laboratory, Inc., in Naperville, Illinois. The laboratory
Improving your margins
 Clinical Improving your margins Philip Newsome and Siobhan Owen A restoration s margin marks the transition between the restoration itself and the finishing line of the adjacent tooth tissue. This is a
Clinical Improving your margins Philip Newsome and Siobhan Owen A restoration s margin marks the transition between the restoration itself and the finishing line of the adjacent tooth tissue. This is a
Together with Course Program 2014
 Together with Course Program 2014 Welcome to Nordic Institute of Dental Education Are you interested in complementing your knowledge and skills as a dental professional? Nordic Institute of Dental Education
Together with Course Program 2014 Welcome to Nordic Institute of Dental Education Are you interested in complementing your knowledge and skills as a dental professional? Nordic Institute of Dental Education
In contemporary restorative dentistry, there are several ways
 Case Report Hybrid Combination REStoRAtion Vonlays: A Conservative Esthetic Alternative to Full-Coverage Crowns Edward A. McLaren, DDS, MDC; Johan Figueira, DDS; and Ronald E. Goldstein, DDS Abstract:
Case Report Hybrid Combination REStoRAtion Vonlays: A Conservative Esthetic Alternative to Full-Coverage Crowns Edward A. McLaren, DDS, MDC; Johan Figueira, DDS; and Ronald E. Goldstein, DDS Abstract:
Removable Partial Dentures 101 Back to the Basics. Luther A. Ison, CDT University of Minnesota School of Dentistry
 Removable Partial Dentures 101 Back to the Basics Luther A. Ison, CDT University of Minnesota School of Dentistry Anterior-Posterior Palatal Strap Major connector Lingual Bar Major Connector, Kennedy Class
Removable Partial Dentures 101 Back to the Basics Luther A. Ison, CDT University of Minnesota School of Dentistry Anterior-Posterior Palatal Strap Major connector Lingual Bar Major Connector, Kennedy Class
IMPLANT DENTISTRY EXAM BANK
 IMPLANT DENTISTRY EXAM BANK 1. Define osseointegration. (4 points, 1/4 2. What are the critical components of an acceptable clinical trial? (10 points) 3. Compare the masticatory performance of individuals
IMPLANT DENTISTRY EXAM BANK 1. Define osseointegration. (4 points, 1/4 2. What are the critical components of an acceptable clinical trial? (10 points) 3. Compare the masticatory performance of individuals
The LOCATOR concept. Simplicity and versatility for prosthesis fixation
 The concept Simplicity and versatility for prosthesis fixation The concept Experience the freedom in prosthesis fixation Simple and secure fixation of implant-supported prostheses is essential for successful
The concept Simplicity and versatility for prosthesis fixation The concept Experience the freedom in prosthesis fixation Simple and secure fixation of implant-supported prostheses is essential for successful
prosthetic technique manual
 prosthetic technique manual TABLE OF CONTENTS Introduction 1 Treatment Planning 2-5 Restorative Options Implant-level Cement-retained Restorations Implant-level Screw-retained Restorations Abutment-level
prosthetic technique manual TABLE OF CONTENTS Introduction 1 Treatment Planning 2-5 Restorative Options Implant-level Cement-retained Restorations Implant-level Screw-retained Restorations Abutment-level
Dental Bridges. What are they? What are the parts of a typical dental bridge (fixed)? When are dental bridges needed?
? When are dental bridges needed?") Dental Bridges What are they? Dental bridges are false teeth anchored on neighbouring teeth in order to replace one or more missing teeth. The false tooth is known as a pontic and is fused in between two
Dental Bridges What are they? Dental bridges are false teeth anchored on neighbouring teeth in order to replace one or more missing teeth. The false tooth is known as a pontic and is fused in between two
DESS. Screws. Tijuana Ventas: (664) 685 6294/95 [email protected]. For all major implant systems!! www.dabocorp.com
 685 6294/95 hirambogarin@dabocorp.com. For all major implant systems!! www.dabocorp.com") Screws Screws for definitive use. Made from medical grade 5 ELI Titanium Integrity and soundness guaranteed by stress tests of up to 150% of their nominal torques. Their designs ensure a perfect fit with
Screws Screws for definitive use. Made from medical grade 5 ELI Titanium Integrity and soundness guaranteed by stress tests of up to 150% of their nominal torques. Their designs ensure a perfect fit with
USAGE OF SELECTIVE LASER MELTING TECHNOLOGY CAPABILITIES IMPLEMENTATION FOR TEETH IMPLANTS METAL CONSTRUCTION IN TU-SOFIA
 USAGE OF SELECTIVE LASER MELTING TECHNOLOGY CAPABILITIES IMPLEMENTATION FOR TEETH IMPLANTS METAL CONSTRUCTION IN TU-SOFIA George TODOROV, Nikolay NIKOLOV, Victor MITOV, Yavor SOFRONOV Technical University
USAGE OF SELECTIVE LASER MELTING TECHNOLOGY CAPABILITIES IMPLEMENTATION FOR TEETH IMPLANTS METAL CONSTRUCTION IN TU-SOFIA George TODOROV, Nikolay NIKOLOV, Victor MITOV, Yavor SOFRONOV Technical University
EXPANDED FUNCTION DENTAL AUXILIARY EXAMINATION CANDIDATE INFORMATION BULLETIN
 PSI licensure: certification 3210 E Tropicana Las Vegas, NV 89121 www.psiexams.com EXPANDED FUNCTION DENTAL AUXILIARY EXAMINATION CANDIDATE INFORMATION BULLETIN CONTENT OUTLINE Examinations by PSI licensure:
PSI licensure: certification 3210 E Tropicana Las Vegas, NV 89121 www.psiexams.com EXPANDED FUNCTION DENTAL AUXILIARY EXAMINATION CANDIDATE INFORMATION BULLETIN CONTENT OUTLINE Examinations by PSI licensure:
Tooth Replacement Options
 Dr. Jordan Johnson Johnson Dental Associates http://www.beta.mydentalhub.com/ada/test/ (800) 947-4746 Tooth Replacement Options If you re missing one or more teeth, you may be all too aware of their importance
Dr. Jordan Johnson Johnson Dental Associates http://www.beta.mydentalhub.com/ada/test/ (800) 947-4746 Tooth Replacement Options If you re missing one or more teeth, you may be all too aware of their importance
SAME DAY VS. TRADITIONAL CROWNS. Which is the better choice? PRESENTED BY
 SAME DAY VS. TRADITIONAL CROWNS Which is the better choice? PRESENTED BY What is a dental crown & why do I need one? A dental crown is a hard, protective covering for a tooth. It improves or restores the
SAME DAY VS. TRADITIONAL CROWNS Which is the better choice? PRESENTED BY What is a dental crown & why do I need one? A dental crown is a hard, protective covering for a tooth. It improves or restores the
Encode Restorative System Procedure & Laboratory Manual
 Procedure & Laboratory Manual Encode Virtual Abutment Encode Abutment Blank Encode Abutment 1/2 Milled Encode Abutment Completed ENCODE RESTORATIVE SYSTEM Simply Impressive With the introduction of the
Procedure & Laboratory Manual Encode Virtual Abutment Encode Abutment Blank Encode Abutment 1/2 Milled Encode Abutment Completed ENCODE RESTORATIVE SYSTEM Simply Impressive With the introduction of the
SCOPE OF PRACTICE GENERAL DENTAL COUNCIL
 www.gdc-uk.org SCOPE OF PRACTICE Effective from 30 September 2013 2 SCOPE OF PRACTICE The scope of your practice is a way of describing what you are trained and competent to do. It describes the areas
www.gdc-uk.org SCOPE OF PRACTICE Effective from 30 September 2013 2 SCOPE OF PRACTICE The scope of your practice is a way of describing what you are trained and competent to do. It describes the areas
CHAPTER 12 SURVEY LINES. portion of the tooth is undercut to the path of placement of the denture. DEFINITIONS
 CHAPTER 12 portion of the tooth is undercut to the path of placement of the denture. SURVEY LINES DEFINITIONS A SURVEY LINE is a line produced on a cast by a surveyor or scribe marking the greatest prominence
CHAPTER 12 portion of the tooth is undercut to the path of placement of the denture. SURVEY LINES DEFINITIONS A SURVEY LINE is a line produced on a cast by a surveyor or scribe marking the greatest prominence
Renaissance of One-Piece Implants
 2 EDI Minimally invasive and patient-friendly treatment concepts using one-piece implants Renaissance of One-Piece Implants Hannes Thurm-Meyer, dentist, Bremen, Germany, Thomas Horn, master dental technician,
2 EDI Minimally invasive and patient-friendly treatment concepts using one-piece implants Renaissance of One-Piece Implants Hannes Thurm-Meyer, dentist, Bremen, Germany, Thomas Horn, master dental technician,
Flexible dentures an alternate for rigid dentures? Volume 1 Issue 1
 Flexible dentures an alternate for rigid dentures? Dr. Sunitha N Shamnur 1, Dr. Jagadeesh KN 1, Dr. Kalavathi SD 1, Dr. Kashinath KR 2 1 Senior Lecturer, 2 Professor & Head, Department of Prosthodontics,
Flexible dentures an alternate for rigid dentures? Dr. Sunitha N Shamnur 1, Dr. Jagadeesh KN 1, Dr. Kalavathi SD 1, Dr. Kashinath KR 2 1 Senior Lecturer, 2 Professor & Head, Department of Prosthodontics,