Stress Echocardiography Boot Camp Review. Arunima Misra, M.D. Baylor College of Medicine Ben Taub General Hospital April 29, 2016
|
|
|
- Bruce Johns
- 7 years ago
- Views:
Transcription
1 Stress Echocardiography Boot Camp Review Arunima Misra, M.D. Baylor College of Medicine Ben Taub General Hospital April 29, 2016
2 Indications for Stress Echo Diagnosis of CAD in patients with chest pain Determination of the location and severity of inducible myocardial ischemia Assessment of viability prior to revascularization Preoperative evaluation in select patients Risk stratification post-myocardial infarction and in stable CAD Assessment of severity of stenotic and regurgitant valvular disease Assessment of dynamic gradient in HCM

3 Ischemic Cascade Sensitivity Myocardial perfusion Echocardiography LV filling pressure Specificity Treadmill

4 Cardiac Anatomy and Views wikimedia.org/wikipedia/commons

5 Myocardial Segments* Lang JASE 2005

6 Coronary Territories* Lang JASE 2005
7 Imaging in Stress Echocardiography Tissue harmonic imaging should always be used Reduces near-field artifact Improves resolution Enhances myocardial definition Contrast should be used when two or more contiguous segments are not well visualized
8 Protocols for Stress Echo Exercise Treadmill: Bruce protocol most used Bicycle: Supine for ischemia or valve assessment Pharmacologic: Dobutamine: mcg/kg every 3 min Can add atropine to improve HR response Dipyridamole: 0.56 mg/kg to 0.84mg/kg Adenosine: 140 mcg/kg per min Other Atrial pacing (if pt with pacemaker) Programmed pacing Handgrip (can use to augment HR response)
9 Exercise or Non-exercise Stress Exercise capacity adds prognostic information to the stress data It is independent of any demonstration of ischemia Generally use treadmill or bicycle Can be symptom limited or until target heart rate is achieved
10 Exercise Stress Protocol Treadmill: Imaging done at rest and immediately after exercise Bruce protocol to achieve 85% of MPHR Bicycle: Imaging done at rest, initial workload of 25W, peak stress and recovery (4 stages) In young pts, initial workload maybe higher HR lower but BP higher, may not achieve good RPP if unable to exercise Better for hemodynamic assessment for valvular disease
11 Pharmacologic Stress Dobutamine Adenosine or dipyridamole Atropine (usually added to dobutamine when target heart rate not achieved)
12 Pharmacology of Dobutamine β 1 agonist but also can activate α and β 2 receptors Increases myocardial oxygen demand by increased inotropy and chronotropy Half-life is 2 minutes Can increase BP at low/normal doses and can decrease BP at higher doses due to β 2 activation
13 Dobutamine Stress Protocol Dobutamine to assess regional wall motion abnormalities Start at 5 mcg/kg/min, increasing every 3min to 10, 20, 30 and maximum of 40 mcg/kg/min In some instances can give up to 50 mcg/kg/min Atropine can be given in divided doses of 0.25 to 0.5 mg for maximum of 2.0 mg to achieve target heart rate helps in those who are on beta blocker therapy Increases sensitivity by 5% in single vessel CAD and in those on beta blockers
14 Contraindications to DSE Uncontrolled hypertension Uncontrolled dysrhythmia Unstable angina (as with any stress test) For atropine: untreated narrow angle glaucoma and severe urinary retention
15 Side Effects to Dobutamine Palpitations Chest pain Tremor Headache Dizziness Urinary urgency Nausea Dyspnea Hypertension Hypotension Arrhythmias
16 Endpoints to DSE Peak dose with atropine Target heart rate reached Moderate or extensive wall motion abnormalities Significant arrhythmias Hypotension or severe hypertension Intolerable symptoms (pt request)
17 Adenosine or Dipyridamole Vasodilators Increase adenosine (directly or indirectly with dipyridamole which increases endogenous levels) Usually response is mild hypotension with some reflex tachycardia Wall thickening is related to endocardial blood flow reserve rather than increase in oxygen demand
18 Side Effects of Vasodilator Stress Minor and greater with adenosine than dipyridamole Adenosine with much shorter half-life, less than 10 seconds (difficult for stress echo imaging) Flushing, AV block, headache, chest pain, nausea, bronchospasm, coughing
19 Vasodilator Stress Contraindications Adenosine Severe bronchospasm Theophylline 2 nd or 3 rd degree heart block Dipyridamole As above Hypotension Unstable carotid disease
20 Comparisons of Patient Factors and Choice of Stressors
21 Pharmacologic Reversal Agents Dobutamine: IV esmolol or metoprolol Dipyridamole: IV aminophylline Adenosine: usually not necessary due to short half life, can use IV aminophylline
22 Safety of Stress Echocardiography Safety was evaluated using an international registry of over 85,000 examinations from 71 centers in over 17 countries From Cases included exercise, dobutamine and dipyridamole stressors All were shown to be safe, but there were relative differences There were 6 deaths: 5 with dobutamine and 1 with dipyridamole Am J Cardiol 2006; 98:541-43
23 Complications During Stress Echocardiography Complication Dobutamine Dipyridamole Exercise Acute myocardial infarction Sustained ventricular tachycardia Ventricular fibrillation Cardiac rupture Asystole Transient ischemic attack/stroke Hypotension/shock Third-degree atrioventricular block Modified from Am J Cardiol 2006; 98:541-43
24 Abdominal Aortic Aneurysms No cited incidence of aortic aneurysm rupture Compared to exercise, the blood pressure response tends to be less with dobutamine and therefore, it is likely safer than exercise Pellika in 1996 demonstrated no events in 98 pts with AAA 4 cm
25 Pacemaker Stress Protocol Patient with permanent pacemaker: can achieve MPHR by increasing pacing rate Can be done with or without dobutamine Transesophageal pacing can also be done in pts who are not able to exercise Can increase heart rate every 2 min until 85% MPHR is achieved
26 Comparison of Stress Modalities Bicycle Treadmill Dobutamine Dipyridamole Improved sensitivity Easier protocol Cumbersome protocol Easier protocol Decreased specificity Images difficult to capture Better image quality Less sensitive Lower workload Higher workload Easier to reach required workload Not as much data Leg fatigue Better tolerated by patients More side effects and risk More side effects Bicycle stress echo may be more sensitive than treadmill exercise
27 Validation Sensitivity True positives/all positives Specificity True negatives/all negatives Accuracy True positives + True negatives/all tests Always dependent on pre-test likelihood
28 Sensitivity and Specificity of Stress Echo Sensitivity Specificity Accuracy Exercise 85% 77% 85% Dobutamine 80% 86% 83% Dipyridamole (Not well studied) 74% 94% 77% Modified from Heart 2003 and Beleslin Circ 1994
29 ECHO VERSUS SPECT ECHO SPECT ACCURACY 85% ~85% HYPERTENSION/ LVH WOMEN Better specificity Better accuracy Better sensitivity Decreased accuracy COST <$500 >$500
30 Why Stress Echo Global LV and RV function Chamber sizes Wall thickness Valve structure and function Pericardium Aorta Hemodynamics

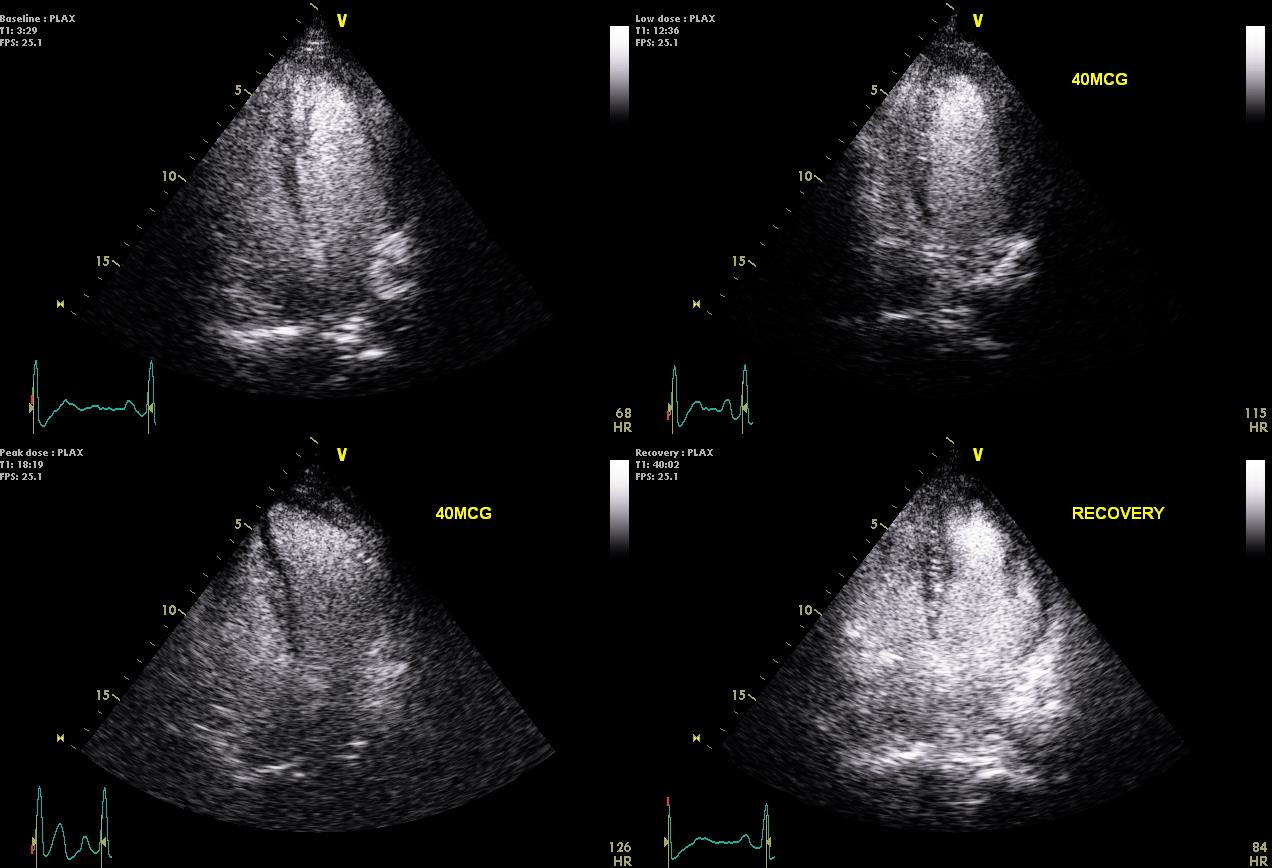
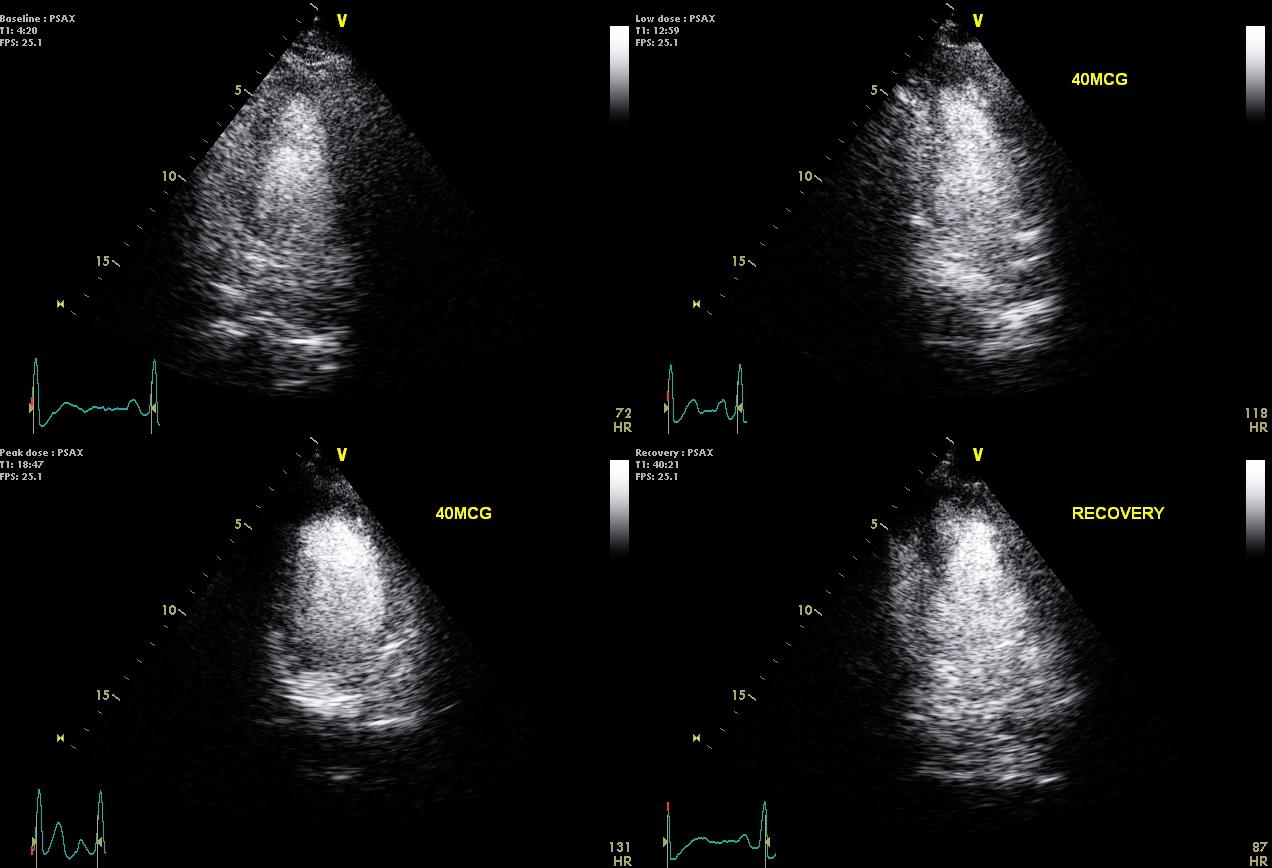
31 Normal Stress Echo
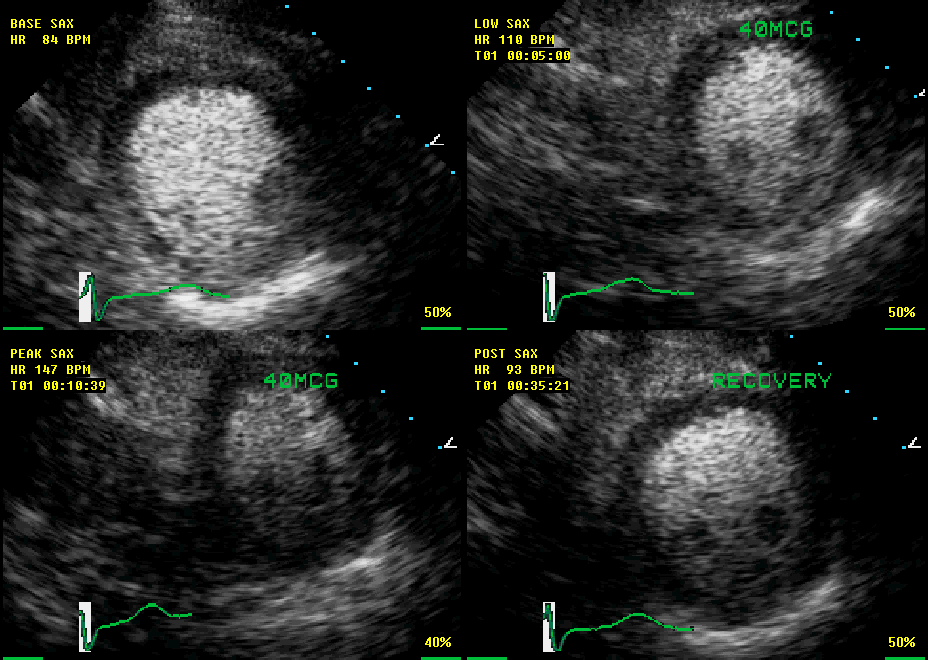
32
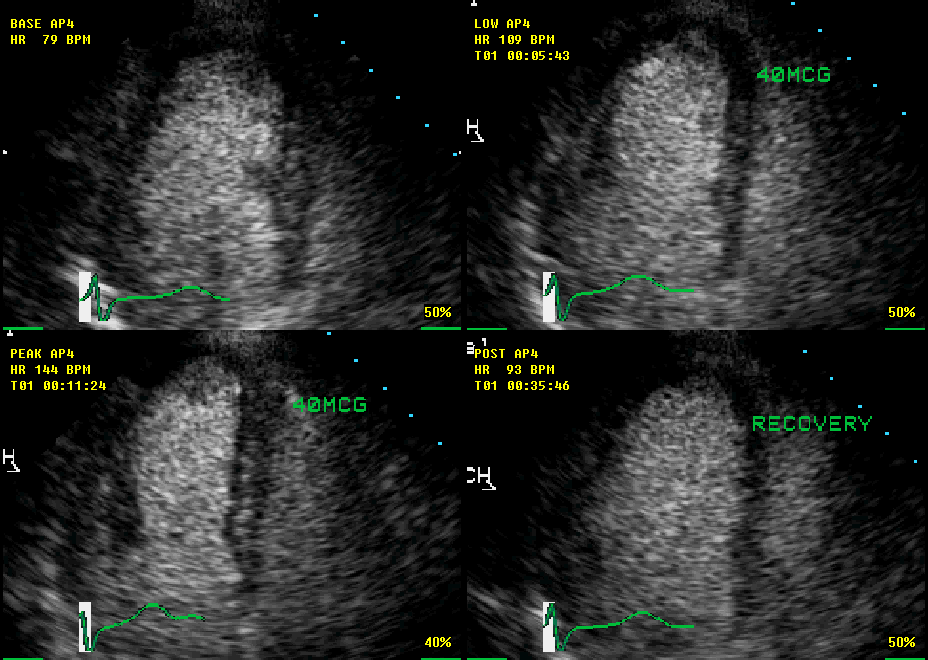
33

34
35 Interpretation of Stress Echo: Regional Wall Motion Scoring 0= Hyperkinesis 1= Normal 2= Hypokinesis 3= Akinesis 4= Dyskinesis 5= Aneurysmal Baseline Scoring
36 Normal Responses to Stress Hypercontractile wall motion Wall thickening, normal is >50% Improved endocardial excursion Smaller LV chamber size in systole and diastole Flat response is not specific for ischemia
37 Wall Motion and Severity of Stenosis At rest, wall motion may be normal with stenosis of < 85% (when flow at rest is still within normal) Hypokinesis can be seen in a reduction of coronary blood flow by 10-20% Akinesis is observed when there is an 80% reduction in coronary blood flow With stress, a stenosis of 50% can cause regional wall motion abnormality The decrease in wall thickening is more closely coupled to subendocardial rather than subepicardial blood flow, i.e. can be affected by amount of stress, wall thickness, collaterals, diffuse disease
38 Abnormal Response to Stress Hypokinesia: less than normal (5 mm) degree of inward myocardial excursion or thickening (40%) Akinesia: complete lack of inward motion and thickening (<10%) Dyskinesia: paradoxical (outward motion during systole) Aneurysm: thinning and bulging during systole and diastole Otto, The Practice of Clinical Echocardiography

39 Abnormal Response to Stress Extreme example of myocardial stunning due to multivessel disease Senior, et al Heart 2005
40 Case 1 58 yo man with history of hyperlipidemia, gastroesophageal reflux disease, and atypical chest pain with a treadmill ECG test that revealed ischemic ST changes in the absence of chest pain at 10 METs of exercise on a Bruce protocol. Duke treadmill score was -1 (intermediate risk). He, therefore, was sent for dobutamine stress echo for further risk stratification.

41 Indications for Stress Testing in Symptomatic Patients JACC Vol. 63, No. 4, 2014

42

43
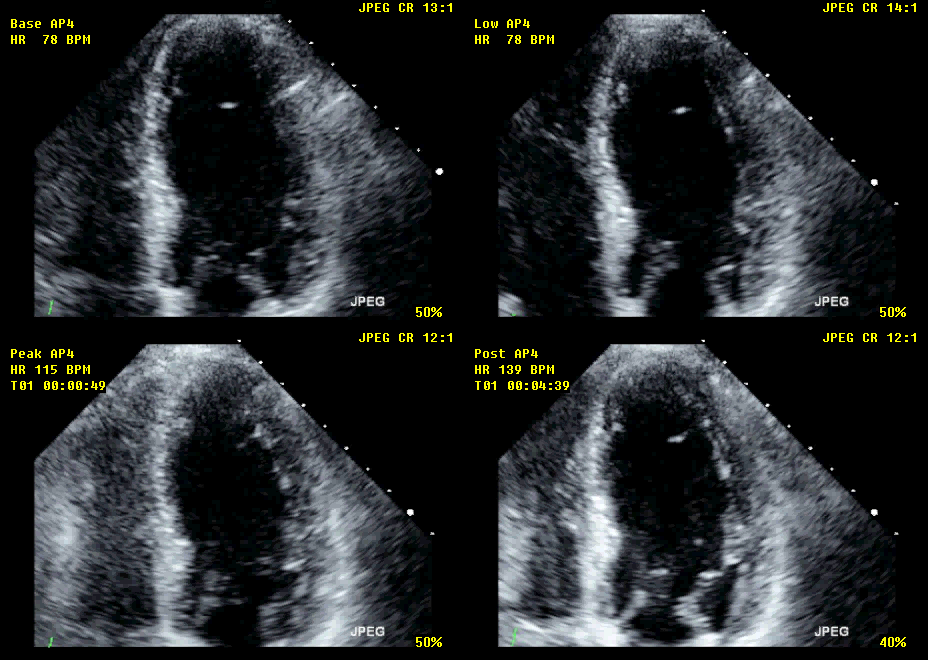
44

45
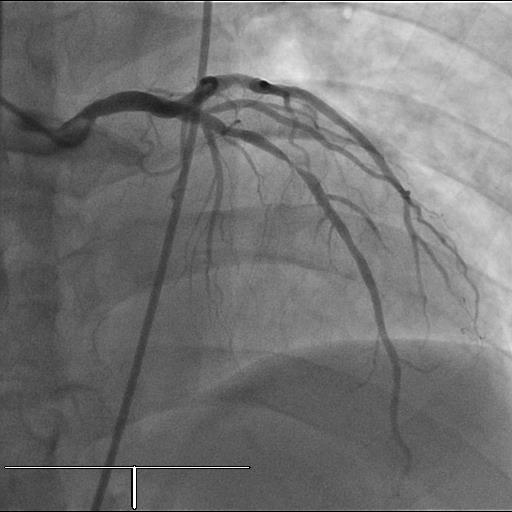
46 Catheterization Results
47 Other Causes of Wall Motion Abnormalities LBBB Paced rhythm Nonischemic cardiomyopathy Myocarditis Right ventricular volume or pressure overload Post-operative septal motion
48 Qualitative Interpretation: Clinical Implications of Stress Echo Responses Rest Stress Implication Normal Hyperdynamic No CAD, no ischemia Normal Hypokinetic or akinetic CAD present, ischemia induced Abnormal No change CAD present, no inducible ischemia only scar Abnormal New hypokinesis or akinesis CAD present, additional areas of ischemia are noted Abnormal Abnormal Improved wall motion at all levels of stress (sustained) Improved at low dose dobutamine and hypokinesis/akinesis at high dose Nonischemic cardiomyopathy Biphasic response suggestive of viability Modified from J Am Soc Echocardiogr 1998; 11:97-104
49 Interpretation of Stress Echo Can be interpreted qualitatively with a descriptive summary of the myocardial response: for example, normal hyperdynamic response, decrease in cavity size, no new wall motion abnormalities Can be interpreted quantitatively using the standardized segments with numeric descriptions
50 17 Segment Model Apical cap Comparison among imaging modalities is done using the 17 segment model Apical cap is the thinnest portion of LV and does not contract or thicken and is not scored
 =sum of scores/number of segments visualized RWMSI=1 is normal RWMSI >1 is abnormal J Am Soc")
51 Quantitative Interpretation*: ASE Guidelines for Calculating Summed Stress Score 1= Normal 2= Hypokinesis 3= Akinesis 4= Dyskinesis 5= Aneurysmal RWMSI= 20/16 or 1.25 For each of the segments: Scoring from 1-5 REGIONAL WALL MOTION SCORE INDEX (RWMSI) =sum of scores/number of segments visualized RWMSI=1 is normal RWMSI >1 is abnormal J Am Soc Echocardiogr 1989;2:358
52 Changes in Sensitivity and Specificity with Abnormal Findings Specificity Flat response Single segment new WMA 2 segments new WMA Extensive new WMA LV dilation Sensitivity

53 Quantitation of Regional Function Centroid method: forming multiple radii, extending from a geometric center of mass (centroid) to the endocardial and epicardial surfaces Centerline methods: generation of chords to the endocardium and epicardium generated perpendicular to the LV long-axis cardiovascres. oxfordjournals. org
54 Methods of Assessing Wall Motion Advantages Endocardial Excursion Wall Thickening Relies on readily defined interface More readily measured around entire circumference of ventricle Independent of a center of reference Unaffected by shape changes Disadvantages Centroid-dependent Difficult to measure around entire circumference due to poor epicardial definition Affected by translation and rotation Difficult to correlate with results of radionuclide or contrast ventriculograms Mann et al: Prog Cardiovasc Dis, 1986
55 Appropriate Use Criteria Asymptomatic Symptomatic Preoperative assessment

56 Testing in Asymptomatic Patients JACC Vol. 63, No. 4, 2014
57 Case Presentation 56 yo man with no significant PMH or risk factors for CAD, except maybe tobacco use in the past, needed a preoperative assessment prior to knee replacement due to osteoarthritis. Since patient could not walk effectively on a treadmill, he underwent a dobutamine stress echo.

58
59
60
61
62 Interpretation Sustained improvement in all segments with increasing stress without worsening at higher doses Nonischemic cardiomyopathy

63 Preoperative Assessment J Am Soc Echocardiogr 2011;24:229-67
64 Using Stress Echo to Delineate Myocardium at Risk Use to quantify severity and extent of myocardium at risk Can use this information to provide prognostic risk Total risk can be calculated by summing the abnormal segmental score at peak stress divided by the number of segments (16) according to the ASE guidelines
65 Risk of MI and Death Very Low Risk (<1%) Death, Cardiac Events Normal exercise stress echo at good workload Women >5METs Men >7METs Low Risk (<2%) Death, MI Normal pharmacologic stress echo with adequate >85% of MPRHR Low to intermediate pretest likelihood High Risk (>4% risk) Extensive rest WMA (4-5 segments) Extensive ischemia (4-5 segments) Multivessel ischemia Rest WMA with new ischemia in different territory Low ischemic threshold Dobutamine <20 mcg/kg/min or vasodilator Baseline EF <40% Journal of the American Society of Echocardiography Volume 20 Number 9
66 Mortality of Patients According to Total Extent of WMA Marwick, et al, Circulation 2001
67 Mortality after Dobutamine Stress Echo Marwick, et al, Circulation 2001
68 Stress Echo Adds to Duke Treadmill Score Senior, et al Heart 2005
69 Dobutamine Stress Echo and Viability Viability (as seen in hibernating myocardium) is present if there is improvement in contractility with low dose, i.e mcg of dobutamine If there is return to baseline or further reduction in wall motion with higher dose, ischemia is demonstrated A biphasic response is considered to predict the best outcome with revascularization J Am Coll Cardiol 1998;32:921-6

70 Evaluating Stress Echo Using Diastology Recording from a 65-year-old patient with noncardiac dyspnea. Recording from a 56-year- old patient with exertional dyspnea. May be helpful in diagnosing patients with HFpEF Circ Cardiovasc ImagingJuly 2011
71 Agreement in DSE and SPECT Am J Cardiol 2007;100:
 without demonstrable wall motion abnormalities.")
72 Regional Diastolic Dysfunction: Strain Strain imaging from apical 2-chamber view at baseline (left) and 5 minutes after completion of exercise (right) in a 72-year-old man with inferior wall ischemia, demonstrating delayed myocardial relaxation in the basal and mid-inferior wall (yellow) without demonstrable wall motion abnormalities. Circ Cardiovasc ImagingJuly 2011
 at rest, but there is a failure to increase SR (lack of a red hue) and")
73 Strain Imaging and Regional Deformation Abnormalities Color M-mode SR tracings at rest (upper panel) and after treadmill stress (lower panel) of septum and lateral LV. The SR is normal (yellow brown hue, except at the apex, which is uninterpretable because of the perpendicular sampling angle) at rest, but there is a failure to increase SR (lack of a red hue) and postsystolic shortening (PSS) in the left anterior descending territory, indicative of ischemia. Circ Cardiovasc Imaging March 2011

74 Comparison Between Doppler and 2D Strain
75 Myocardial Contrast Echo Helps to discern the endocardium during stress echocardiography Allows for visualization in patients who might otherwise not have adequate images Several studies have shown significant improvement in the assessment of left ventricular function and volumes with the use of contrast when compared to MR as a gold standard JASE, Article in press 2008
76 Contrast Safety The Food and Drug Administration (FDA) removed the black-box warning contraindicating the use of echo contrast agents in patients who are acutely unwell (eg, acute myocardial infarction or worsening congestive cardiac failure) Contrast is contraindicated in patients with known right to left shunts and previous hypersensitivity or anaphylactoid response to contrast
77 Case Presentations
78 CASE 3 60 yo with HTN, HLD with atypical chest pain until 3 wks ago when started having pain after working or walking fast. Pain radiates to bilateral arms. He had a treadmill test in which he had same sx after exercising for only 5.5 min with nondiagnostic ECG changes. Underwent DSE in which he had same arm pain and had ST elevation in inferior leads but no other changes. He reached target HR.
79

80
81
82

83 CATHETERIZATION RESULTS
84 Possible Board Questions from ASE Echo Review Course
85 For comparative studies of MRI, SPECT and echo, how many segments are recommended?
86 Which segment cannot be seen in the parasternal long view? 1. Mid inferoseptum 2. Basal inferolateral wall 3. Mid anteroseptum 4. Mid anterior wall 5. 1 and and 4
87 Regarding methods of quantitation of regional wall motion: 1. Endocardial excursion method is centroid independent 2. Wall thickening method is independent of center of reference 3. Translation and rotation do not affect endocardial excursion method 4. Centroid methods improve sensitivity of stress echo
123 Main St NY, New York 12345 ph: (202) 555 5555 fax: (202) 555 5555
 555 5555 fax: (202) 555 5555") Patient Name: DOE, JOHN D. Gender: M Date of Study: 4/2/2013 Date of birth: 6/28/1962 Age: 50 Medical Record #: 45869725 Ordering Physician: JANE INTERNIST, MD History: Atypical Angina, Abn ECG, High Cholesterol,
Patient Name: DOE, JOHN D. Gender: M Date of Study: 4/2/2013 Date of birth: 6/28/1962 Age: 50 Medical Record #: 45869725 Ordering Physician: JANE INTERNIST, MD History: Atypical Angina, Abn ECG, High Cholesterol,
Section 8: Clinical Exercise Testing. a maximal GXT?
 Section 8: Clinical Exercise Testing Maximal GXT ACSM Guidelines: Chapter 5 ACSM Manual: Chapter 8 HPHE 4450 Dr. Cheatham Outline What is the purpose of a maximal GXT? Who should have a maximal GXT (and
Section 8: Clinical Exercise Testing Maximal GXT ACSM Guidelines: Chapter 5 ACSM Manual: Chapter 8 HPHE 4450 Dr. Cheatham Outline What is the purpose of a maximal GXT? Who should have a maximal GXT (and
38 year old female with mild obesity. She is planning an exercise program to loose weight. She has no other known risk factors for CAD.
 Stress Testing: Wael A. Jaber, MD,FACC 38 year old female with mild obesity She is planning an exercise program to loose weight. She has no other known risk factors for CAD. You recommend: A. Exercise
Stress Testing: Wael A. Jaber, MD,FACC 38 year old female with mild obesity She is planning an exercise program to loose weight. She has no other known risk factors for CAD. You recommend: A. Exercise
Is it really so? : Varying Presentations for ACS among Elderly, Women and Diabetics. Yen Tibayan, M.D. Division of Cardiovascular Medicine
 Is it really so? : Varying Presentations for ACS among Elderly, Women and Diabetics Yen Tibayan, M.D. Division of Cardiovascular Medicine Case Presentation 69 y.o. woman calls 911 with the complaint of
Is it really so? : Varying Presentations for ACS among Elderly, Women and Diabetics Yen Tibayan, M.D. Division of Cardiovascular Medicine Case Presentation 69 y.o. woman calls 911 with the complaint of
Efficient Evaluation of Chest Pain
 Efficient Evaluation of Chest Pain Vikranth Gongidi, DO FACC FACOI Indian River Medical Center Vero Beach, FL No Disclosures Outline Background Chest pain pathway Indications for stress test Stress test
Efficient Evaluation of Chest Pain Vikranth Gongidi, DO FACC FACOI Indian River Medical Center Vero Beach, FL No Disclosures Outline Background Chest pain pathway Indications for stress test Stress test
Diagnostic and Therapeutic Procedures
 Diagnostic and Therapeutic Procedures Diagnostic and therapeutic cardiovascular s are central to the evaluation and management of patients with cardiovascular disease. Consistent with the other sections,
Diagnostic and Therapeutic Procedures Diagnostic and therapeutic cardiovascular s are central to the evaluation and management of patients with cardiovascular disease. Consistent with the other sections,
Non Invasive Testing for CAD
 Non Invasive Testing for CAD Wael A. Jaber, MD Section of Cardiac Imaging Heart and Vascular Institute Cleveland Clinic 38 year old female with mild obesity She is planning an exercise program to loose
Non Invasive Testing for CAD Wael A. Jaber, MD Section of Cardiac Imaging Heart and Vascular Institute Cleveland Clinic 38 year old female with mild obesity She is planning an exercise program to loose
Perioperative Cardiac Evaluation
 Perioperative Cardiac Evaluation Caroline McKillop Advisor: Dr. Tam Psenka 10-3-2007 Importance of Cardiac Guidelines -Used multiple times every day -Patient Safety -Part of Surgical Care Improvement Project
Perioperative Cardiac Evaluation Caroline McKillop Advisor: Dr. Tam Psenka 10-3-2007 Importance of Cardiac Guidelines -Used multiple times every day -Patient Safety -Part of Surgical Care Improvement Project
The Role Of Early Stress Testing In Assessing Low Risk Chest Pain Patients Admitted Through The Emergency Department
 The Role Of Early Stress Testing In Assessing Low Risk Chest Pain Patients Admitted Through The Emergency Department Simbo Chiadika LAY ABSTRACT A. Study purpose Cardiac stress testing has been recommended
The Role Of Early Stress Testing In Assessing Low Risk Chest Pain Patients Admitted Through The Emergency Department Simbo Chiadika LAY ABSTRACT A. Study purpose Cardiac stress testing has been recommended
RACE I Rapid Assessment by Cardiac Echo. Intensive Care Training Program Radboud University Medical Centre NIjmegen
 RACE I Rapid Assessment by Cardiac Echo Intensive Care Training Program Radboud University Medical Centre NIjmegen RACE Goal-directed study with specific questions Excludes Doppler ultrasound Perform 50
RACE I Rapid Assessment by Cardiac Echo Intensive Care Training Program Radboud University Medical Centre NIjmegen RACE Goal-directed study with specific questions Excludes Doppler ultrasound Perform 50
Treating AF: The Newest Recommendations. CardioCase presentation. Ethel s Case. Wayne Warnica, MD, FACC, FACP, FRCPC
 Treating AF: The Newest Recommendations Wayne Warnica, MD, FACC, FACP, FRCPC CardioCase presentation Ethel s Case Ethel, 73, presents with rapid heart beating and mild chest discomfort. In the ED, ECG
Treating AF: The Newest Recommendations Wayne Warnica, MD, FACC, FACP, FRCPC CardioCase presentation Ethel s Case Ethel, 73, presents with rapid heart beating and mild chest discomfort. In the ED, ECG
MYOCARDIAL PERFUSION COMPUTED TOMOGRAPHY PhD course in Medical Imaging. Anne Günther Department of Radiology OUS Rikshospitalet
 MYOCARDIAL PERFUSION COMPUTED TOMOGRAPHY PhD course in Medical Imaging Anne Günther Department of Radiology OUS Rikshospitalet CORONARY CT ANGIOGRAPHY (CTA) Accurate method in the assessment of possible
MYOCARDIAL PERFUSION COMPUTED TOMOGRAPHY PhD course in Medical Imaging Anne Günther Department of Radiology OUS Rikshospitalet CORONARY CT ANGIOGRAPHY (CTA) Accurate method in the assessment of possible
How To Understand What You Know
 Heart Disorders Glossary ABG (Arterial Blood Gas) Test: A test that measures how much oxygen and carbon dioxide are in the blood. Anemia: A condition in which there are low levels of red blood cells in
Heart Disorders Glossary ABG (Arterial Blood Gas) Test: A test that measures how much oxygen and carbon dioxide are in the blood. Anemia: A condition in which there are low levels of red blood cells in
Exchange solutes and water with cells of the body
 Chapter 8 Heart and Blood Vessels Three Types of Blood Vessels Transport Blood Arteries Carry blood away from the heart Transport blood under high pressure Capillaries Exchange solutes and water with cells
Chapter 8 Heart and Blood Vessels Three Types of Blood Vessels Transport Blood Arteries Carry blood away from the heart Transport blood under high pressure Capillaries Exchange solutes and water with cells
Provider Checklist-Outpatient Imaging. Checklist: Nuclear Stress Test, Thallium/Technetium/Sestamibi (CPT Code 78451-78454 78469)
") Provider Checklist-Outpatient Imaging Checklist: Nuclear Stress Test, Thallium/Technetium/Sestamibi (CPT Code 78451-78454 78469) Medical Review Note: Per InterQual, if any of the following are present,
Provider Checklist-Outpatient Imaging Checklist: Nuclear Stress Test, Thallium/Technetium/Sestamibi (CPT Code 78451-78454 78469) Medical Review Note: Per InterQual, if any of the following are present,
Pharmacologic Stress Agents
 Pharmacologic Stress Agents Donna Lesniak, RN, CCRC Mallinckrodt Institute of Radiology Washington University School of Medicine Saint Louis, Missouri Disclosure Neither I nor my immediate family members
Pharmacologic Stress Agents Donna Lesniak, RN, CCRC Mallinckrodt Institute of Radiology Washington University School of Medicine Saint Louis, Missouri Disclosure Neither I nor my immediate family members
2/20/2015. Cardiac Evaluation of Potential Solid Organ Transplant Recipients. Issues Specific to Transplantation. Kidney Transplantation.
 DISCLOSURES I have no relevant financial relationships to disclose. Cardiac Evaluation of Potential Solid Organ Transplant Recipients Michele Hamilton, MD Director, Heart Failure Program Cedars Sinai Heart
DISCLOSURES I have no relevant financial relationships to disclose. Cardiac Evaluation of Potential Solid Organ Transplant Recipients Michele Hamilton, MD Director, Heart Failure Program Cedars Sinai Heart
Medical management of CHF: A New Class of Medication. Al Timothy, M.D. Cardiovascular Institute of the South
 Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
Tips and Tricks to Demystify 12 Lead ECG Interpretation
 Tips and Tricks to Demystify 12 Lead ECG Interpretation Mission: Lifeline North Dakota Regional EMS and Hospital Conference Samantha Kapphahn, DO Essentia Health- Interventional Cardiology June 5th, 2014
Tips and Tricks to Demystify 12 Lead ECG Interpretation Mission: Lifeline North Dakota Regional EMS and Hospital Conference Samantha Kapphahn, DO Essentia Health- Interventional Cardiology June 5th, 2014
Cardiac Assessment for Renal Transplantation: Pre-Operative Clearance is Only the Tip of the Iceberg
 Cardiac Assessment for Renal Transplantation: Pre-Operative Clearance is Only the Tip of the Iceberg 2 nd Annual Duke Renal Transplant Symposium March 1, 2014 Durham, NC Joseph G. Rogers, M.D. Associate
Cardiac Assessment for Renal Transplantation: Pre-Operative Clearance is Only the Tip of the Iceberg 2 nd Annual Duke Renal Transplant Symposium March 1, 2014 Durham, NC Joseph G. Rogers, M.D. Associate
6/5/2014. Objectives. Acute Coronary Syndromes. Epidemiology. Epidemiology. Epidemiology and Health Care Impact Pathophysiology
 Objectives Acute Coronary Syndromes Epidemiology and Health Care Impact Pathophysiology Unstable Angina NSTEMI STEMI Clinical Clues Pre-hospital Spokane County EMS Epidemiology About 600,000 people die
Objectives Acute Coronary Syndromes Epidemiology and Health Care Impact Pathophysiology Unstable Angina NSTEMI STEMI Clinical Clues Pre-hospital Spokane County EMS Epidemiology About 600,000 people die
NAME OF THE HOSPITAL: 1. Coronary Balloon Angioplasty: M7F1.1/ Angioplasty with Stent(PTCA with Stent): M7F1.3
: M7F1.3") 1. Coronary Balloon Angioplasty: M7F1.1/ Angioplasty with Stent(PTCA with Stent): M7F1.3 1. Name of the Procedure: Coronary Balloon Angioplasty 2. Select the Indication from the drop down of various indications
1. Coronary Balloon Angioplasty: M7F1.1/ Angioplasty with Stent(PTCA with Stent): M7F1.3 1. Name of the Procedure: Coronary Balloon Angioplasty 2. Select the Indication from the drop down of various indications
Diagnosis Code Crosswalk : ICD-9-CM to ICD-10-CM Cardiac Rhythm and Heart Failure Diagnoses
 Diagnosis Code Crosswalk : to 402.01 Hypertensive heart disease, malignant, with heart failure 402.11 Hypertensive heart disease, benign, with heart failure 402.91 Hypertensive heart disease, unspecified,
Diagnosis Code Crosswalk : to 402.01 Hypertensive heart disease, malignant, with heart failure 402.11 Hypertensive heart disease, benign, with heart failure 402.91 Hypertensive heart disease, unspecified,
Pharmacologic Stress Test: Adenosine
 Pharmacologic Stress Test: Adenosine OVERVIEW The purpose of this document is to specifically identify the critical components involved in performing a pharmacologic stress test with adenosine. This information
Pharmacologic Stress Test: Adenosine OVERVIEW The purpose of this document is to specifically identify the critical components involved in performing a pharmacologic stress test with adenosine. This information
4/7/2015. Cardiac Rehabilitation: From the other side of the glass door. Chicago, circa 1999. Objectives. No disclosures, no conflicts
 Cardiac Rehabilitation: From the other side of the glass door No disclosures, no conflicts Charles X. Kim, MD, FACC, ABVM Objectives 1. Illustrate common CV benefits of CV rehab in real world practice.
Cardiac Rehabilitation: From the other side of the glass door No disclosures, no conflicts Charles X. Kim, MD, FACC, ABVM Objectives 1. Illustrate common CV benefits of CV rehab in real world practice.
Potential Causes of Sudden Cardiac Arrest in Children
 Potential Causes of Sudden Cardiac Arrest in Children Project S.A.V.E. When sudden death occurs in children, adolescents and younger adults, heart abnormalities are likely causes. These conditions are
Potential Causes of Sudden Cardiac Arrest in Children Project S.A.V.E. When sudden death occurs in children, adolescents and younger adults, heart abnormalities are likely causes. These conditions are
ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY. Guidelines for Use of Intravenous Isoproterenol
 ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Isoproterenol Major Indications Status Asthmaticus As a last resort for
ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Isoproterenol Major Indications Status Asthmaticus As a last resort for
Specific Basic Standards for Osteopathic Fellowship Training in Cardiology
 Specific Basic Standards for Osteopathic Fellowship Training in Cardiology American Osteopathic Association and American College of Osteopathic Internists BOT 07/2006 Rev. BOT 03/2009 Rev. BOT 07/2011
Specific Basic Standards for Osteopathic Fellowship Training in Cardiology American Osteopathic Association and American College of Osteopathic Internists BOT 07/2006 Rev. BOT 03/2009 Rev. BOT 07/2011
ACLS PHARMACOLOGY 2011 Guidelines
 ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
INTRODUCTION TO EECP THERAPY
 INTRODUCTION TO EECP THERAPY is an FDA cleared, Medicare approved, non-invasive medical therapy for the treatment of stable and unstable angina, congestive heart failure, acute myocardial infarction, and
INTRODUCTION TO EECP THERAPY is an FDA cleared, Medicare approved, non-invasive medical therapy for the treatment of stable and unstable angina, congestive heart failure, acute myocardial infarction, and
Flash, Rocking on others Added value in DCM and CRT. C. Parsai Polyclinique des Fleurs France
 Flash, Rocking on others Added value in DCM and CRT C. Parsai Polyclinique des Fleurs France Cleland JGF et al. (2007) Nat Clin Pract Cardiovasc Med 4: 90 101 Predicting CRT Response Device Related Patient
Flash, Rocking on others Added value in DCM and CRT C. Parsai Polyclinique des Fleurs France Cleland JGF et al. (2007) Nat Clin Pract Cardiovasc Med 4: 90 101 Predicting CRT Response Device Related Patient
HEART HEALTH WEEK 3 SUPPLEMENT. A Beginner s Guide to Cardiovascular Disease HEART FAILURE. Relatively mild, symptoms with intense exercise
 WEEK 3 SUPPLEMENT HEART HEALTH A Beginner s Guide to Cardiovascular Disease HEART FAILURE Heart failure can be defined as the failing (insufficiency) of the heart as a mechanical pump due to either acute
WEEK 3 SUPPLEMENT HEART HEALTH A Beginner s Guide to Cardiovascular Disease HEART FAILURE Heart failure can be defined as the failing (insufficiency) of the heart as a mechanical pump due to either acute
Name: Age: Resting BP: Wt. kg: Est. HR max : 85%HR max : Resting HR:
 Bruce Protocol - Submaximal GXT Name: Age: Resting BP: Wt. kg: Est. HR max : 85%HR max : Resting HR: Stage Min. % Grade MPH METs 2min HR 3min HR BP RPE 1 0-3 10 1.7 4.7 2 3-6 12 2.5 7.0 3 6-9 14 3.4 10.1
Bruce Protocol - Submaximal GXT Name: Age: Resting BP: Wt. kg: Est. HR max : 85%HR max : Resting HR: Stage Min. % Grade MPH METs 2min HR 3min HR BP RPE 1 0-3 10 1.7 4.7 2 3-6 12 2.5 7.0 3 6-9 14 3.4 10.1
2015 Reimbursement Guide
 Reimbursement Guide - Cardiology 2015 Reimbursement Guide for Myocardial Perfusion Imaging including radiopharmaceuticals and related product information 2015 Reimbursement Guide for Myocardial Perfusion
Reimbursement Guide - Cardiology 2015 Reimbursement Guide for Myocardial Perfusion Imaging including radiopharmaceuticals and related product information 2015 Reimbursement Guide for Myocardial Perfusion
National Imaging Associates, Inc. Clinical guidelines
 National Imaging Associates, Inc. Clinical guidelines Original Date: February 2010 STRESS ECHOCARDIOLOGY Page 1 of 15 CPT Codes: 93350, 93351, + 93352 Last Reviewed Date: June 2012 Guideline Number: NIA_CG_026
National Imaging Associates, Inc. Clinical guidelines Original Date: February 2010 STRESS ECHOCARDIOLOGY Page 1 of 15 CPT Codes: 93350, 93351, + 93352 Last Reviewed Date: June 2012 Guideline Number: NIA_CG_026
Scott Hubbell, MHSc, RRT-NPS, C-NPT, CCT Clinical Education Coordinator/Flight RRT EagleMed
 Scott Hubbell, MHSc, RRT-NPS, C-NPT, CCT Clinical Education Coordinator/Flight RRT EagleMed Identify the 12-Lead Views Explain the vessels of occlusion Describe the three I s Basic Interpretation of 12-Lead
Scott Hubbell, MHSc, RRT-NPS, C-NPT, CCT Clinical Education Coordinator/Flight RRT EagleMed Identify the 12-Lead Views Explain the vessels of occlusion Describe the three I s Basic Interpretation of 12-Lead
How should we treat atrial fibrillation in heart failure
 Advances in Cardiac Arrhhythmias and Great Innovations in Cardiology Torino, 23/24 Ottobre 2015 How should we treat atrial fibrillation in heart failure Matteo Anselmino Dipartimento Scienze Mediche Città
Advances in Cardiac Arrhhythmias and Great Innovations in Cardiology Torino, 23/24 Ottobre 2015 How should we treat atrial fibrillation in heart failure Matteo Anselmino Dipartimento Scienze Mediche Città
Cardiovascular diseases. pathology
 Cardiovascular diseases pathology Atherosclerosis Vascular diseases A disease that results in arterial wall thickens as a result of build- up of fatty materials such cholesterol, resulting in acute and
Cardiovascular diseases pathology Atherosclerosis Vascular diseases A disease that results in arterial wall thickens as a result of build- up of fatty materials such cholesterol, resulting in acute and
Management of the Patient with Aortic Stenosis undergoing Non-cardiac Surgery
 Management of the Patient with Aortic Stenosis undergoing Non-cardiac Surgery Srinivasan Rajagopal M.D. Assistant Professor Division of Cardiothoracic Anesthesia Objectives Describe the pathophysiology
Management of the Patient with Aortic Stenosis undergoing Non-cardiac Surgery Srinivasan Rajagopal M.D. Assistant Professor Division of Cardiothoracic Anesthesia Objectives Describe the pathophysiology
Cardiovascular Guidelines for DOT Physical Exams By Maureen Collins MSN, APRN, BC
 Cardiovascular Guidelines for DOT Physical Exams By Maureen Collins MSN, APRN, BC The Federal Motor Carrier Safety Administration (FMCSA) administers the Federal Motor Carrier Safety Regulations (FMCSRs)
Cardiovascular Guidelines for DOT Physical Exams By Maureen Collins MSN, APRN, BC The Federal Motor Carrier Safety Administration (FMCSA) administers the Federal Motor Carrier Safety Regulations (FMCSRs)
Adult Cardiac Surgery ICD9 to ICD10 Crosswalks
 164.1 Malignant neoplasm of heart C38.0 Malignant neoplasm of heart 164.1 Malignant neoplasm of heart C45.2 Mesothelioma of pericardium 198.89 Secondary malignant neoplasm of other specified sites C79.89
164.1 Malignant neoplasm of heart C38.0 Malignant neoplasm of heart 164.1 Malignant neoplasm of heart C45.2 Mesothelioma of pericardium 198.89 Secondary malignant neoplasm of other specified sites C79.89
ATRIAL FIBRILLATION (RATE VS RHYTHM CONTROL)
") ATRIAL FIBRILLATION (RATE VS RHYTHM CONTROL) By Prof. Dr. Helmy A. Bakr Mansoura Universirty 2014 AF Classification: Mechanisms of AF : Selected Risk Factors and Biomarkers for AF: WHY AF? 1. Atrial fibrillation
ATRIAL FIBRILLATION (RATE VS RHYTHM CONTROL) By Prof. Dr. Helmy A. Bakr Mansoura Universirty 2014 AF Classification: Mechanisms of AF : Selected Risk Factors and Biomarkers for AF: WHY AF? 1. Atrial fibrillation
Atrial Fibrillation Management Across the Spectrum of Illness
 Disclosures Atrial Fibrillation Management Across the Spectrum of Illness NONE Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University Objectives AF Discuss the pathophysiology, diagnosis,
Disclosures Atrial Fibrillation Management Across the Spectrum of Illness NONE Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University Objectives AF Discuss the pathophysiology, diagnosis,
BASIC STANDARDS FOR RESIDENCY TRAINING IN CARDIOLOGY
 BASIC STANDARDS FOR RESIDENCY TRAINING IN CARDIOLOGY American Osteopathic Association and the American College of Osteopathic Internists Specific Requirements For Osteopathic Subspecialty Training In Cardiology
BASIC STANDARDS FOR RESIDENCY TRAINING IN CARDIOLOGY American Osteopathic Association and the American College of Osteopathic Internists Specific Requirements For Osteopathic Subspecialty Training In Cardiology
HYPERTROPHIC CARDIOMYOPATHY
 HYPERTROPHIC CARDIOMYOPATHY Most often diagnosed during infancy or adolescence, hypertrophic cardiomyopathy (HCM) is the second most common form of heart muscle disease, is usually genetically transmitted,
HYPERTROPHIC CARDIOMYOPATHY Most often diagnosed during infancy or adolescence, hypertrophic cardiomyopathy (HCM) is the second most common form of heart muscle disease, is usually genetically transmitted,
Cardiology ICD-10-CM Coding Tip Sheet Overview of Key Chapter Updates for Cardiology
 Cardiology ICD-10-CM Coding Tip Sheet Overview of Key Chapter Updates for Cardiology Chapter 4: Endocrine, Nutritional, and Metabolic Diseases (E00-E89) The diabetes mellitus codes are combination codes
Cardiology ICD-10-CM Coding Tip Sheet Overview of Key Chapter Updates for Cardiology Chapter 4: Endocrine, Nutritional, and Metabolic Diseases (E00-E89) The diabetes mellitus codes are combination codes
The P Wave: Indicator of Atrial Enlargement
 Marquette University e-publications@marquette Physician Assistant Studies Faculty Research and Publications Health Sciences, College of 8-12-2010 The P Wave: Indicator of Atrial Enlargement Patrick Loftis
Marquette University e-publications@marquette Physician Assistant Studies Faculty Research and Publications Health Sciences, College of 8-12-2010 The P Wave: Indicator of Atrial Enlargement Patrick Loftis
Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations.
 INTRODUCTION Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations. Although decrease in cardiovascular mortality still major cause of morbidity & burden of disease.
INTRODUCTION Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations. Although decrease in cardiovascular mortality still major cause of morbidity & burden of disease.
Objectives. Cardiac Substrate Metabolism. 2004 SNM Mid-Winter Educational Symposium
 Myocardial Viability Imaging With PET Marcelo F. Di Carli,, MD Brigham and Women s Hospital Harvard Medical School Boston, MA Conflict of Interest: : No Relations to disclose To review: Basic principles
Myocardial Viability Imaging With PET Marcelo F. Di Carli,, MD Brigham and Women s Hospital Harvard Medical School Boston, MA Conflict of Interest: : No Relations to disclose To review: Basic principles
RISK STRATIFICATION for Acute Coronary Syndrome in the Emergency Department
 RISK STRATIFICATION for Acute Coronary Syndrome in the Emergency Department Sohil Pothiawala FAMS (EM), MRCSEd (A&E), M.Med (EM), MBBS Consultant Dept. of Emergency Medicine Singapore General Hospital
RISK STRATIFICATION for Acute Coronary Syndrome in the Emergency Department Sohil Pothiawala FAMS (EM), MRCSEd (A&E), M.Med (EM), MBBS Consultant Dept. of Emergency Medicine Singapore General Hospital
CHEST PAIN EVALUATION TOOL
 CHEST PAIN EVALUATION TOOL Chest pain or discomfort is one of the commonest causes for presentation to the Emergency Room (ER) or physicians office. There are many causes for chest discomfort. The serious
CHEST PAIN EVALUATION TOOL Chest pain or discomfort is one of the commonest causes for presentation to the Emergency Room (ER) or physicians office. There are many causes for chest discomfort. The serious
Perioperative Risk Stratification for Noncardiac Surgical Patients with Cardiac Diagnosis. Michael A. Blazing
 Perioperative Risk Stratification for Noncardiac Surgical Patients with Cardiac Diagnosis Michael A. Blazing Outline The coming crush A practical approach to clinical risk assessment Classic approach to
Perioperative Risk Stratification for Noncardiac Surgical Patients with Cardiac Diagnosis Michael A. Blazing Outline The coming crush A practical approach to clinical risk assessment Classic approach to
Atrial Fibrillation Peter Santucci, MD Revised May, 2008
 Atrial Fibrillation Peter Santucci, MD Revised May, 2008 Atrial fibrillation (AF) is an irregular, disorganized rhythm characterized by a lack of organized mechanical atrial activity. The atrial rate is
Atrial Fibrillation Peter Santucci, MD Revised May, 2008 Atrial fibrillation (AF) is an irregular, disorganized rhythm characterized by a lack of organized mechanical atrial activity. The atrial rate is
Heart and Vascular System Practice Questions
 Heart and Vascular System Practice Questions Student: 1. The pulmonary veins are unusual as veins because they are transporting. A. oxygenated blood B. de-oxygenated blood C. high fat blood D. nutrient-rich
Heart and Vascular System Practice Questions Student: 1. The pulmonary veins are unusual as veins because they are transporting. A. oxygenated blood B. de-oxygenated blood C. high fat blood D. nutrient-rich
Novartis Gilenya FDO Program Clinical Protocol and Highlights from Prescribing Information (PI)
") Novartis Gilenya FDO Program Clinical Protocol and Highlights from Prescribing Information (PI) Highlights from Prescribing Information - the link to the full text PI is as follows: http://www.pharma.us.novartis.com/product/pi/pdf/gilenya.pdf
Novartis Gilenya FDO Program Clinical Protocol and Highlights from Prescribing Information (PI) Highlights from Prescribing Information - the link to the full text PI is as follows: http://www.pharma.us.novartis.com/product/pi/pdf/gilenya.pdf
Osama Jarkas. in Chest Pain Patients. STUDENT NAME: Osama Jarkas DATE: August 10 th, 2015
 STUDENT NAME: Osama Jarkas DATE: August 10 th, 2015 PROJECT TITLE: Analysis of ECG Exercise Stress Testing and Framingham Risk Score in Chest Pain Patients PRIMARY SUPERVISOR NAME: Dr. Edward Tan DEPARTMENT:
STUDENT NAME: Osama Jarkas DATE: August 10 th, 2015 PROJECT TITLE: Analysis of ECG Exercise Stress Testing and Framingham Risk Score in Chest Pain Patients PRIMARY SUPERVISOR NAME: Dr. Edward Tan DEPARTMENT:
Atrial & Junctional Dysrhythmias
 Atrial & Junctional Dysrhythmias Atrial & Junctional Dysrhythmias Atrial Premature Atrial Complex Wandering Atrial Pacemaker Atrial Tachycardia (ectopic) Multifocal Atrial Tachycardia Atrial Flutter Atrial
Atrial & Junctional Dysrhythmias Atrial & Junctional Dysrhythmias Atrial Premature Atrial Complex Wandering Atrial Pacemaker Atrial Tachycardia (ectopic) Multifocal Atrial Tachycardia Atrial Flutter Atrial
Atrial Fibrillation and Cardiac Device Therapy RAKESH LATCHAMSETTY, MD DIVISION OF ELECTROPHYSIOLOGY UNIVERSITY OF MICHIGAN HOSPITAL ANN ARBOR, MI
 Atrial Fibrillation and Cardiac Device Therapy RAKESH LATCHAMSETTY, MD DIVISION OF ELECTROPHYSIOLOGY UNIVERSITY OF MICHIGAN HOSPITAL ANN ARBOR, MI Outline Atrial Fibrillation What is it? What are the associated
Atrial Fibrillation and Cardiac Device Therapy RAKESH LATCHAMSETTY, MD DIVISION OF ELECTROPHYSIOLOGY UNIVERSITY OF MICHIGAN HOSPITAL ANN ARBOR, MI Outline Atrial Fibrillation What is it? What are the associated
Managing Mitral Regurgitation: Repair, Replace, or Clip? Michael Howe, MD Traverse Heart & Vascular
 Managing Mitral Regurgitation: Repair, Replace, or Clip? Michael Howe, MD Traverse Heart & Vascular Mitral Regurgitation Anatomy Mechanisms of MR Presentation Evaluation Management Repair Replace Clip
Managing Mitral Regurgitation: Repair, Replace, or Clip? Michael Howe, MD Traverse Heart & Vascular Mitral Regurgitation Anatomy Mechanisms of MR Presentation Evaluation Management Repair Replace Clip
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL
 Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
Atrial Fibrillation: Do We Have A Cure? Raymond Kawasaki, MD AMG Electrophysiology February 21, 2015
 Atrial Fibrillation: Do We Have A Cure? Raymond Kawasaki, MD AMG Electrophysiology February 21, 2015 Disclaimer I have no relationships to disclose Do we have a cure for Atrial Fibrillation? The short
Atrial Fibrillation: Do We Have A Cure? Raymond Kawasaki, MD AMG Electrophysiology February 21, 2015 Disclaimer I have no relationships to disclose Do we have a cure for Atrial Fibrillation? The short
Case III. Disscussion. the UHP ultrasound protocol. Novel Ultrasound Approach to the Empiric Evaluation of the Undifferentiated Hypotensive Patient
 The UHP Ultrasound Protocol: A Novel Ultrasound Approach to the Empiric Evaluation of the Undifferentiated Hypotensive Patient JOHN S. ROSE, MD,* AARON E. BAIR, MD,* DIKU MANDAVIA, MD, AND DONNA J. KINSER,
The UHP Ultrasound Protocol: A Novel Ultrasound Approach to the Empiric Evaluation of the Undifferentiated Hypotensive Patient JOHN S. ROSE, MD,* AARON E. BAIR, MD,* DIKU MANDAVIA, MD, AND DONNA J. KINSER,
Pharmacologic Stress Agents: Protocol and Safety
 Pharmacologic Stress Agents: Protocol and Safety Donna Lesniak, RN, CCRC Mallinckrodt Institute of Radiology Washington University School of Medicine Saint Louis, Missouri Disclosure Neither I nor my immediate
Pharmacologic Stress Agents: Protocol and Safety Donna Lesniak, RN, CCRC Mallinckrodt Institute of Radiology Washington University School of Medicine Saint Louis, Missouri Disclosure Neither I nor my immediate
Listen to your heart: Good Cardiovascular Health for Life
 Listen to your heart: Good Cardiovascular Health for Life Luis R. Castellanos MD, MPH Assistant Clinical Professor of Medicine University of California San Diego School of Medicine Sulpizio Family Cardiovascular
Listen to your heart: Good Cardiovascular Health for Life Luis R. Castellanos MD, MPH Assistant Clinical Professor of Medicine University of California San Diego School of Medicine Sulpizio Family Cardiovascular
Automatic External Defibrillators
 Last Review Date: May 27, 2016 Number: MG.MM.DM.10dC2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Last Review Date: May 27, 2016 Number: MG.MM.DM.10dC2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
1 Congestive Heart Failure & its Pharmacological Management
 Harvard-MIT Division of Health Sciences and Technology HST.151: Principles of Pharmocology Instructor: Prof. Keith Baker 1 Congestive Heart Failure & its Pharmacological Management Keith Baker, M.D., Ph.D.
Harvard-MIT Division of Health Sciences and Technology HST.151: Principles of Pharmocology Instructor: Prof. Keith Baker 1 Congestive Heart Failure & its Pharmacological Management Keith Baker, M.D., Ph.D.
12-Lead EKG Interpretation. Judith M. Haluka BS, RCIS, EMT-P
 12-Lead EKG Interpretation Judith M. Haluka BS, RCIS, EMT-P ECG Grid Left to Right = Time/duration Vertical measure of voltage (amplitude) Expressed in mm P-Wave Depolarization of atrial muscle Low voltage
12-Lead EKG Interpretation Judith M. Haluka BS, RCIS, EMT-P ECG Grid Left to Right = Time/duration Vertical measure of voltage (amplitude) Expressed in mm P-Wave Depolarization of atrial muscle Low voltage
Signal-averaged electrocardiography late potentials
 SIGNAL AVERAGED ECG INTRODUCTION Signal-averaged electrocardiography (SAECG) is a special electrocardiographic technique, in which multiple electric signals from the heart are averaged to remove interference
SIGNAL AVERAGED ECG INTRODUCTION Signal-averaged electrocardiography (SAECG) is a special electrocardiographic technique, in which multiple electric signals from the heart are averaged to remove interference
ST Segment Elevation Nothing is ever as hard (or easy) as it looks
 as it looks") ST Segment Elevation Nothing is ever as hard (or easy) as it looks Cameron Guild, MD Division of Cardiology University of Mississippi Medical Center February 17, 2012 Objectives 1. Describe the electrical
ST Segment Elevation Nothing is ever as hard (or easy) as it looks Cameron Guild, MD Division of Cardiology University of Mississippi Medical Center February 17, 2012 Objectives 1. Describe the electrical
Practical class 3 THE HEART
 Practical class 3 THE HEART OBJECTIVES By the time you have completed this assignment and any necessary further reading or study you should be able to:- 1. Describe the fibrous pericardium and serous pericardium,
Practical class 3 THE HEART OBJECTIVES By the time you have completed this assignment and any necessary further reading or study you should be able to:- 1. Describe the fibrous pericardium and serous pericardium,
Acute heart failure may be de novo or it may be a decompensation of chronic heart failure.
 Management of Acute Left Ventricular Failure Acute left ventricular failure presents as pulmonary oedema due to increased pressure in the pulmonary capillaries. It is important to realise though that left
Management of Acute Left Ventricular Failure Acute left ventricular failure presents as pulmonary oedema due to increased pressure in the pulmonary capillaries. It is important to realise though that left
Magnetic Resonance Quantitative Analysis. MRV MR Flow. Reliable analysis of heart and peripheral arteries in the clinical workflow
 Magnetic Resonance Quantitative Analysis MRV MR Flow Reliable analysis of heart and peripheral arteries in the clinical workflow CAAS MRV Functional Workflow Designed for imaging specialists, CAAS MRV
Magnetic Resonance Quantitative Analysis MRV MR Flow Reliable analysis of heart and peripheral arteries in the clinical workflow CAAS MRV Functional Workflow Designed for imaging specialists, CAAS MRV
MRI of Sarcoid Heart Disease
 MRI of Sarcoid Heart Disease Saurabh Jha MBBS, University of Pennsylvania, Philadelphia I will discuss the off label use of gadolinium Objectives To appreciate the pathophysiology and clinical presentation
MRI of Sarcoid Heart Disease Saurabh Jha MBBS, University of Pennsylvania, Philadelphia I will discuss the off label use of gadolinium Objectives To appreciate the pathophysiology and clinical presentation
HISTORY. Questions: 1. What diagnosis is suggested by this history? 2. How do you explain her symptoms during pregnancy?
 HISTORY 33-year-old woman. CHIEF COMPLAINT: months duration. Dyspnea, fatigue and nocturnal wheezing of six PRESENT ILLNESS: At ages 5 and 9, she had migratory arthritis. At age 29, in the third trimester
HISTORY 33-year-old woman. CHIEF COMPLAINT: months duration. Dyspnea, fatigue and nocturnal wheezing of six PRESENT ILLNESS: At ages 5 and 9, she had migratory arthritis. At age 29, in the third trimester
ACLS PRE-TEST ANNOTATED ANSWER KEY
 ACLS PRE-TEST ANNOTATED ANSWER KEY June, 2011 Question 1: Question 2: There is no pulse with this rhythm. Question 3: Question 4: Question 5: Question 6: Question 7: Question 8: Question 9: Question 10:
ACLS PRE-TEST ANNOTATED ANSWER KEY June, 2011 Question 1: Question 2: There is no pulse with this rhythm. Question 3: Question 4: Question 5: Question 6: Question 7: Question 8: Question 9: Question 10:
1p36 and the Heart. John Lynn Jefferies, MD, MPH, FACC, FAHA
 1p36 and the Heart John Lynn Jefferies, MD, MPH, FACC, FAHA Director, Advanced Heart Failure and Cardiomyopathy Services Associate Professor, Pediatric Cardiology and Adult Cardiovascular Diseases Associate
1p36 and the Heart John Lynn Jefferies, MD, MPH, FACC, FAHA Director, Advanced Heart Failure and Cardiomyopathy Services Associate Professor, Pediatric Cardiology and Adult Cardiovascular Diseases Associate
GENERAL HEART DISEASE KNOW THE FACTS
 GENERAL HEART DISEASE KNOW THE FACTS WHAT IS Heart disease is a broad term meaning any disease affecting the heart. It is commonly used to refer to coronary heart disease (CHD), a more specific term to
GENERAL HEART DISEASE KNOW THE FACTS WHAT IS Heart disease is a broad term meaning any disease affecting the heart. It is commonly used to refer to coronary heart disease (CHD), a more specific term to
Cilostazol versus Clopidogrel after Coronary Stenting
 Cilostazol versus Clopidogrel after Coronary Stenting Seong-Wook Park, MD, PhD, FACC Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine Seoul, Korea AMC, 2004 Background
Cilostazol versus Clopidogrel after Coronary Stenting Seong-Wook Park, MD, PhD, FACC Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine Seoul, Korea AMC, 2004 Background
GUIDELINE 11.9 MANAGING ACUTE DYSRHYTHMIAS. (To be read in conjunction with Guideline 11.7 Post-Resuscitation Therapy in Adult Advanced Life Support)
") AUSTRALIAN RESUSCITATION COUNCIL GUIDELINE 11.9 MANAGING ACUTE DYSRHYTHMIAS (To be read in conjunction with Guideline 11.7 Post-Resuscitation Therapy in Adult Advanced Life Support) The term cardiac arrhythmia
AUSTRALIAN RESUSCITATION COUNCIL GUIDELINE 11.9 MANAGING ACUTE DYSRHYTHMIAS (To be read in conjunction with Guideline 11.7 Post-Resuscitation Therapy in Adult Advanced Life Support) The term cardiac arrhythmia
Atrial Fibrillation 2014 How to Treat How to Anticoagulate. Allan Anderson, MD, FACC, FAHA Division of Cardiology
 Atrial Fibrillation 2014 How to Treat How to Anticoagulate Allan Anderson, MD, FACC, FAHA Division of Cardiology Projection for Prevalence of Atrial Fibrillation: 5.6 Million by 2050 Projected number of
Atrial Fibrillation 2014 How to Treat How to Anticoagulate Allan Anderson, MD, FACC, FAHA Division of Cardiology Projection for Prevalence of Atrial Fibrillation: 5.6 Million by 2050 Projected number of
Systematic Approach to 12 Lead EKG Interpretation
 Systematic Approach to 12 Lead EKG Interpretation Maureen Knechtel MPAS, PA-C Wellmont CVA Heart Institute Disclosure Statement of Financial Interest I, Maureen Knechtel, do not have a financial interest/arrangement
Systematic Approach to 12 Lead EKG Interpretation Maureen Knechtel MPAS, PA-C Wellmont CVA Heart Institute Disclosure Statement of Financial Interest I, Maureen Knechtel, do not have a financial interest/arrangement
5. Management of rheumatic heart disease
 5. Management of rheumatic heart disease The fundamental goal in the long-term management of RHD is to prevent ARF recurrences, and therefore, prevent the progression of RHD, and in many cases allow for
5. Management of rheumatic heart disease The fundamental goal in the long-term management of RHD is to prevent ARF recurrences, and therefore, prevent the progression of RHD, and in many cases allow for
COVERAGE GUIDANCE: ABLATION FOR ATRIAL FIBRILLATION
 COVERAGE GUIDANCE: ABLATION FOR ATRIAL FIBRILLATION Question: How should the EGBS Coverage Guidance regarding ablation for atrial fibrillation be applied to the Prioritized List? Question source: Evidence
COVERAGE GUIDANCE: ABLATION FOR ATRIAL FIBRILLATION Question: How should the EGBS Coverage Guidance regarding ablation for atrial fibrillation be applied to the Prioritized List? Question source: Evidence
Blood Pressure. Blood Pressure (mm Hg) pressure exerted by blood against arterial walls. Blood Pressure. Blood Pressure
 pressure exerted by blood against arterial walls. Blood Pressure. Blood Pressure") Blood Pressure Blood Pressure (mm Hg) pressure exerted by blood against arterial walls Systolic pressure exerted on arteries during systole Diastolic pressure in arteries during diastole 120/80 Borderline
Blood Pressure Blood Pressure (mm Hg) pressure exerted by blood against arterial walls Systolic pressure exerted on arteries during systole Diastolic pressure in arteries during diastole 120/80 Borderline
Section Four: Pulmonary Artery Waveform Interpretation
 Section Four: Pulmonary Artery Waveform Interpretation All hemodynamic pressures and waveforms are generated by pressure changes in the heart caused by myocardial contraction (systole) and relaxation/filling
Section Four: Pulmonary Artery Waveform Interpretation All hemodynamic pressures and waveforms are generated by pressure changes in the heart caused by myocardial contraction (systole) and relaxation/filling
BIPOLAR LIMB LEADS UNIPOLAR LIMB LEADS PRECORDIAL (UNIPOLAR) LEADS VIEW OF EACH LEAD INDICATIVE ECG CHANGES
 LEADS VIEW OF EACH LEAD INDICATIVE ECG CHANGES") BIPOLAR LIMB LEADS Have both a distinctive positive and negative pole. Lead I LA (positive) RA (negative) Lead II LL (positive) RA (negative) Lead III LL (positive) LA (negative) UNIPOLAR LIMB LEADS Have
BIPOLAR LIMB LEADS Have both a distinctive positive and negative pole. Lead I LA (positive) RA (negative) Lead II LL (positive) RA (negative) Lead III LL (positive) LA (negative) UNIPOLAR LIMB LEADS Have
PVC s / PAC s What Do They Mean? What Should You Do? Jeffrey H. Neuhauser, D.O.,F.A.C.C. BHHI Primary Care Symposium February 27, 2015
 PVC s / PAC s What Do They Mean? What Should You Do? Jeffrey H. Neuhauser, D.O.,F.A.C.C. BHHI Primary Care Symposium February 27, 2015 Financial disclosures Paid speaker for Pfizer Learning Objectives
PVC s / PAC s What Do They Mean? What Should You Do? Jeffrey H. Neuhauser, D.O.,F.A.C.C. BHHI Primary Care Symposium February 27, 2015 Financial disclosures Paid speaker for Pfizer Learning Objectives
Cardiovascular System & Its Diseases. Lecture #4 Heart Failure & Cardiac Arrhythmias
 Cardiovascular System & Its Diseases Lecture #4 Heart Failure & Cardiac Arrhythmias Dr. Derek Bowie, Department of Pharmacology & Therapeutics, Room 1317, McIntyre Bldg, McGill University derek.bowie@mcgill.ca
Cardiovascular System & Its Diseases Lecture #4 Heart Failure & Cardiac Arrhythmias Dr. Derek Bowie, Department of Pharmacology & Therapeutics, Room 1317, McIntyre Bldg, McGill University derek.bowie@mcgill.ca
Anatomi & Fysiologi 060301. The cardiovascular system (chapter 20) The circulation system transports; What the heart can do;
 The circulation system transports; What the heart can do;") The cardiovascular system consists of; The cardiovascular system (chapter 20) Principles of Anatomy & Physiology 2009 Blood 2 separate pumps (heart) Many blood vessels with varying diameter and elasticity
The cardiovascular system consists of; The cardiovascular system (chapter 20) Principles of Anatomy & Physiology 2009 Blood 2 separate pumps (heart) Many blood vessels with varying diameter and elasticity
HEART MONITOR TREADMILL 12 LEAD EKG
 2 HEART MONITOR TREADMILL 12 LEAD EKG Portable ambulatory monitoring system Continuously records electrical activity of the heart for 24 hours or more Also known as ambulatory electrocardiographic monitor
2 HEART MONITOR TREADMILL 12 LEAD EKG Portable ambulatory monitoring system Continuously records electrical activity of the heart for 24 hours or more Also known as ambulatory electrocardiographic monitor
Congestive heart failure (CHF) is a. Diastolic Heart Failure. By Michel D Astous, MD, FRCPC
 is a. Diastolic Heart Failure. By Michel D Astous, MD, FRCPC") Diastolic Heart Failure The evaluation of both systolic and diastolic functions is of great importance among patients presenting with signs of CHF, as the treatment may be quite different depending on
Diastolic Heart Failure The evaluation of both systolic and diastolic functions is of great importance among patients presenting with signs of CHF, as the treatment may be quite different depending on
Episode 20 Atrial fibrillation Prepared by Dr. Lucas Chartier
 Episode 20 Atrial fibrillation Prepared by Dr. Lucas Chartier Most common dysrhythmia seen in ED, and incidence increasing with ageing population Presentation Common presentations: younger patients often
Episode 20 Atrial fibrillation Prepared by Dr. Lucas Chartier Most common dysrhythmia seen in ED, and incidence increasing with ageing population Presentation Common presentations: younger patients often
Elective Cardiac Catheterization Preauthorization
 STAT Bulletin PO Box 80 / Buffalo, New York 14240-0080 June 15, 2009 Volume 7:Issue 17 To: All Cardiologists Elective Cardiac Catheterization Preauthorization Contracts Affected: All Lines of Business
STAT Bulletin PO Box 80 / Buffalo, New York 14240-0080 June 15, 2009 Volume 7:Issue 17 To: All Cardiologists Elective Cardiac Catheterization Preauthorization Contracts Affected: All Lines of Business
Palpitations & AF. Richard Grocott Mason Consultant Cardiologist THH NHS Foundation Trust & Royal Brompton & Harefield NHS Foundation Trust
 Palpitations & AF Richard Grocott Mason Consultant Cardiologist THH NHS Foundation Trust & Royal Brompton & Harefield NHS Foundation Trust Palpitations Frequent symptom Less than 50% associated with arrhythmia
Palpitations & AF Richard Grocott Mason Consultant Cardiologist THH NHS Foundation Trust & Royal Brompton & Harefield NHS Foundation Trust Palpitations Frequent symptom Less than 50% associated with arrhythmia
RATE VERSUS RHYTHM CONTROL OF ATRIAL FIBRILLATION: SPECIAL CONSIDERATION IN ELDERLY. Charles Jazra
 RATE VERSUS RHYTHM CONTROL OF ATRIAL FIBRILLATION: SPECIAL CONSIDERATION IN ELDERLY Charles Jazra NO CONFLICT OF INTEREST TO DECLARE Relationship Between Atrial Fibrillation and Age Prevalence, percent
RATE VERSUS RHYTHM CONTROL OF ATRIAL FIBRILLATION: SPECIAL CONSIDERATION IN ELDERLY Charles Jazra NO CONFLICT OF INTEREST TO DECLARE Relationship Between Atrial Fibrillation and Age Prevalence, percent
Acute Coronary Syndrome. What Every Healthcare Professional Needs To Know
 Acute Coronary Syndrome What Every Healthcare Professional Needs To Know Background of ACS Acute Coronary Syndrome (ACS) is an umbrella term used to cover a spectrum of clinical conditions that are caused
Acute Coronary Syndrome What Every Healthcare Professional Needs To Know Background of ACS Acute Coronary Syndrome (ACS) is an umbrella term used to cover a spectrum of clinical conditions that are caused
Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University
 Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University Objectives Define exercise associated collapse (EAC) and exercise-associated postural hypotension
Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University Objectives Define exercise associated collapse (EAC) and exercise-associated postural hypotension
CARDIAC RISKS OF NON CARDIAC SURGERY
 CARDIAC RISKS OF NON CARDIAC SURGERY N E W S T U D I E S & N E W G U I D E L I N E S W. B. C A L H O U N, M D, F A C C 2014 ACC/AHA Guideline on perioperative cardiovascular evaluation and management
CARDIAC RISKS OF NON CARDIAC SURGERY N E W S T U D I E S & N E W G U I D E L I N E S W. B. C A L H O U N, M D, F A C C 2014 ACC/AHA Guideline on perioperative cardiovascular evaluation and management
Low-gradient severe aortic stenosis with normal LVEF: A disturbing clinical entity
 Low-gradient severe aortic stenosis with normal LVEF: A disturbing clinical entity Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Disclosures : None 77-year-old woman, mild dyspnea
Low-gradient severe aortic stenosis with normal LVEF: A disturbing clinical entity Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Disclosures : None 77-year-old woman, mild dyspnea
Ischemia and Infarction
 Harvard-MIT Division of Health Sciences and Technology HST.035: Principle and Practice of Human Pathology Dr. Badizadegan Ischemia and Infarction HST.035 Spring 2003 In the US: ~50% of deaths are due to
Harvard-MIT Division of Health Sciences and Technology HST.035: Principle and Practice of Human Pathology Dr. Badizadegan Ischemia and Infarction HST.035 Spring 2003 In the US: ~50% of deaths are due to