Movement Disorders and Extrapyramidal System. Doç.. Dr. Sibel Ertan
|
|
|
- Leonard Smith
- 10 years ago
- Views:
Transcription
1 Movement Disorders and Extrapyramidal System Doç.. Dr. Sibel Ertan İ.Ü.. CTF. Nöroloji N ABD.

2 Motor System I. neuron (corticospinal pathway) Extrapyramidal system (basal ganglia) Cerebellum Loops for praxis II. neuron: Anterior horn cells of the spinal cord Cranial cell nuclei in the brain stem Peripheral nerve, motor cranial nerves Neuromuscular junction Muscle

3 Definition Neurologic syndromes in which there is either an excess of movement, or a paucity of voluntary and automatic movements unrelated to weakness or spasticity.

4 Most movement disorders are associated with pathologic alterations in the basal ganglia or their connections.

5 But disorders of the Cerebellum or its pathways Cerebral cortex Thalamus Brain stem Spinal cord Peripheral nerves may also cause several movement disorders.

6 Cerebral cortex Thalamus Cerebellum Basal ganglia Dopaminergic system Dopaminergic system Spinal cord

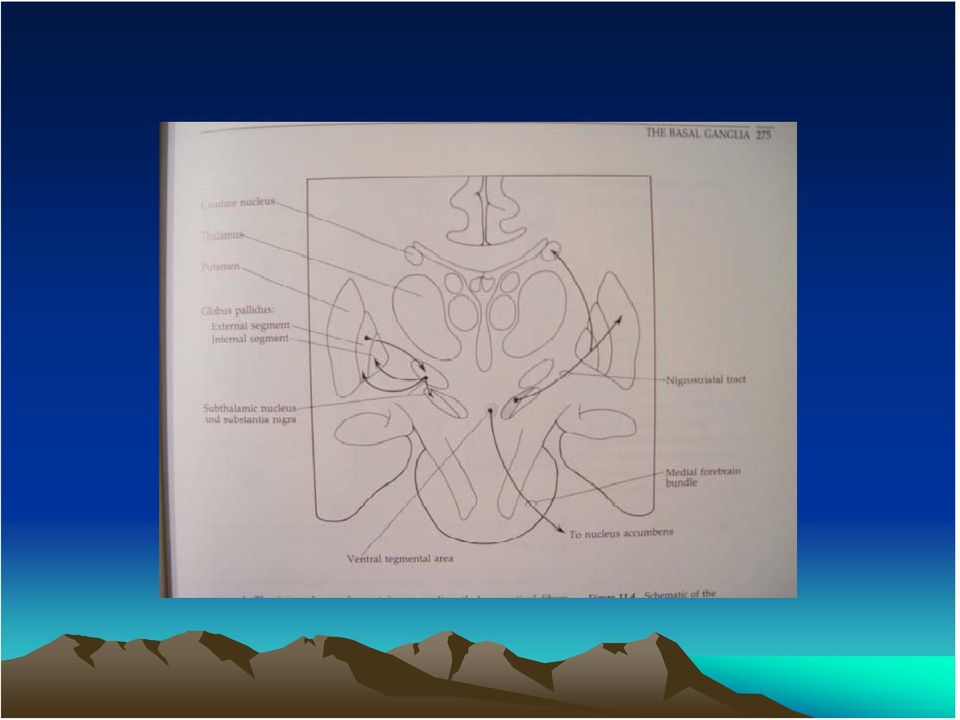
7 Basal Ganglia Caudate PutamenGPe GPi Thalamus STN SNr SNc

8 Basal ganglia subcortical nuclei: caudate putamen globus pallidus caudate, putamen & globus pallidus are named corpus striatum Caudate &putamen are named striatum globus pallidus & putamen are named lentiform nuclei

9
10 Definition The term extrapyramidal system, coined by British neurologist Kinnier Wilson, refers to the basal ganglia and an array of brain stem nuclei (red nucleus, reticular formation etc.) to which they are connected.

11 Striatum (caudate+putamen) is the principle receptive structure of the basal ganglia. Globus pallidus is the principle output structure of the basal ganglia.

12 SENSORY-MOTOR LOOP Cerebral cortex Somatic sensory Primary motor Premotor upplementary motor Putamen Gpi SNr Thalamic nuclei Ventral lateral

13 ASSOCIATIVE - LOOP Cerebral cortex Posterior parietal Premotor Prefrontal Caudate (head) SNr Gpi Thalamic nuclei Ventral ant.,dorsal medial

14 LIMBIC - LOOP Cerebral cortex Thalamic nuclei Medial, lateral temporal lobs, hippocampal form., Ant. cingulate, Orbitofrontal cortex Ventral Striatum caudate (head) Ventral Pallidum Gpi SNr Dorsomedial, Ventral anterior
 Ventral Pallidum Gpi SNr Dorsomedial,")
15 OCULOMOTOR - LOOP Cerebral cortex Posterior parietal Prefrontal Frontal eye field caudate (body) SNr Gpi Thalamic nuclei Ventral ant., Dorsal medial

16

17 Diseases of the basal ganglia are associated with abnormal involuntary movements that typically occur at rest and disappear in sleep. They are generally divided into two categories: Hyperkinetic and hypokinetic The hyperkinetic variety is seen in such disorders as chorea, athetosis, ballism, dystonia, tremor, and tics. The hypokinetic variety is seen largely in Parkinson s disease. Following anatomic loci for pathology are agreed on: - Substantia nigra in Parkinson s disease - Caudate nucleus in chorea - Subthalamic nucleus in ballism - Caudate or lentiform nucleus (especially putamen) in dystonia

18 Hypokinetic Disorders
19 Parkinsonism Six cardinal features: 1. Tremor at rest 2. Rigidity 3. Bradykinesia-hypokinesia 4. Flexed posture 5. Loss of postural reflexes 6. Freezing phenomenon

20 Tremor, rigidity, and flexed posture are referred positive phenomena. Bradykinesia, loss of postural reflexes, and freezing are negative phenomena.

21 Rest Tremor 4-5 Hz Present in the extremities, almost always distally Classic pill-rolling tremor involves the thumb and the forefinger Rest tremor disappears with action but reemerges as the limb maintain a posture. Rest tremor is also common in the lips, chin, and tongue Rest tremor of the hands increases with walking Stress worsens the tremor
22 Rigidity Increased resistance (muscle tone) to passive movement elicited when the exami.ner moves the patient s limbs, neck or trunk Equal in all directions The underlying tremor may cause cogwheeling
23 Flexed posture Commonly begins in the arms and spreads to involve the entire body Striatal hand Striatal toe Lateral tilting of the trunk is common
24 Bradykinesia Slowness of movement, difficulty in initiating a movement, and loss of automatic movement Hypokinesia is the reduction in amplitude of movement
25 Loss of postural reflexes Pulltest is positive With progress of the disease frequent fallings The patient collapses into the chair on attempting to sit down (sitting en bloc)
26 Freezing Inability to perform active movements (motor block) Often involves the legs when walking but can also involve eyelid opening,speaking and writing.
27
28 The many causes of parkinsonism are divided into four categories: 1.Idiopathic 2. Symptomatic 3. Parkinson-plus syndromes 4. Heredodegenerative diseases
29 The core biochemical pathology in parkinsonism is decreased dopaminergic neurotransmission in the basal ganglia. Degeneration of the nigrostriatal dopamine system Degeneration of the striatum with loss of dopamine receptors Drug induced parkinsonism as the result of blockade of dopamine receptors.
30 Nigral Dopaminergic Neuron Terminals and Striatal Receptors Parkinson s Disease Parkinson-plus Syndromes Drug-induced Parkinsonizm
31 Parkinson s disease (primary parkinsonism) Degeneration of the neuromelanin-containing neurons in the brain stem, especially in substantia nigra pars compacta and in the locus ceruleus. Many of the surviving neurons contain eosinophilic cytoplasmic inclusions known as Lewy bodies. By the time symptoms appear, the substantia nigra already has lost about 60% of dopaminergic neurons and the dopamine content in the striatum is about 80% less than normal.
32
33 Parkinson s disease (primary parkinsonism) PD makes up approximately 80% of cases of parkinsonism. Mean age at onset in both sexes is 55 years (range:20-80). Male/female = 3/2. Prevalence 160/ and incidence 20/ /yr. The cause of PD is unknown.
34 Parkinson s disease (primary parkinsonism) Treatment Treatment is aimed at controlling symptoms because no drug or surgicl approach unequivocally prevents progression of PD. Treatment is lifelong. Treatment includes pharmacotherapy, physiotherapy and surgery.
35 Parkinson s disease (primary parkinsonism) Treatment Therapeutic choices for Parkinson s disease Medications Dopamine precursor: levodopa (LD)±carbidopa or benserazide Dopamine agonists: bromocriptine, pergolide, pramipexole, ropinirole, apomorphine, cabergoline. Catecholamine-O-methyl transferase inhibitors:tolcapone and entacapone. Dopamine releaser: Amantadine. Monoamine oxidase type B inhibitor: selegiline. Anticholinergics:trihexyphenidyl, benztropine, biperidene... Antihistaminics:diphenhydramine, orphenadrine, phenindamine
36 Parkinson s disease (primary parkinsonism) Treatment Therapeutic choices for Parkinson s disease Surgery Ablative surgery:thalamotomy, pallidotomy. Restorative surgery:embryonic dopaminergic tissue transplantation Deep brain stimulation:thalamic stimulation, pallidal stimulation, subthalamic stimulation
37 Parkinson s disease (primary parkinsonism) Treatment All symptomatic drugs can induce side effects, and if a patient is not troubled socially or occupationally by mild symptoms, dru therapy can be delayed until symptoms become more pronounced. LD is the most effective drug, BUT 75% of patients have serious complications after 5 years of LD therapy. Younger patients, in particular, are more likely to show response fluctuations. DOPA-SPARING STRATEGY:Other antiparkinsonian drugs should be used first to delay the introduction of LD. Selegiline delays the need for LD therapy by an average of 9 months.
38 Hyperkinetic Disorders
39 Tremor * Involuntary oscillations of a body part produced by alternating or synchronous contractions of reciprocally innervated muscles. * Physiological tremor These tremors are very small amplitude and are demonstrable only by means of accelerometer. Enhanced physiological tremor: medical conditions, drugs, anxiety, fear
40 * Essential tremor ET Typically a postural tremor (4-12 Hz) but may be accentuated by goal-directed movements. The site of involvement in most cases is the hands and it is frequently asymmetric initially. * Parkinsonian tremor Tremor at rest, at a frequency of 4-5 Hz, is the most characteristic and the most prominent type of tremor in PD, but postural and kinetic tremor are also frequently seen. Onset of the tremor is usually in one of the hands; rarely, it may begin in the legs. * Intention tremor Rhythmic involuntary oscillations that undergo exacerbation as the hand or foot approaches the target of a voluntary movement. It indicates involvement of the cerebellum or its connections.
41
42 Chorea ( dance ) Characterized by sudden, frequent involuntary, arrhythmic, purposeless, and quick jerks of the trunk, extremities, and head associated with facial grimaces. They are usually distal and of low amplitude. Causes of chorea are hereditary, autoimmune, vascular, metabolic, toxic, inflammatory or drug induced. Athetosis ( without position ) Slow, writhing, continuous, wormlike movements of the distal parts of the extremities, chiefly the fingers, which show bizarre posturing.
43 Ballism ( jump or throw ) Sudden, quick, continuous, unusually violent, and flinging in nature. Usually confined to the contralateral vascular lesion in the subthalamic nucleus. Dystonia ( bad tone ) Twisting, slow, contorting, involuntary movement, that is somewhat sustained and often repetitive. Dystonia can involve any part of the body. Dystonia is classified as (1) focal, (2) segmental, (3)multifocal, (4) hemidystonia, (5) generalized
44
45 Myoclonus Sudden shock-like muscle contractions. They can be focal, multifocal, or generalized. Myoclonus may be regular and rhythmic like tremor, but it is usually random and irregular like chorea. It differs from tremor in that there are visible pauses in between the jerks. It differs from chorea, which is flowing and resembles fragments of normal movements. Tics can resemble myoclonus but are voluntarily supressible for short periods; furthermore, an inner buildup of tension occurs during the supression of tics.
46
47 Tourette syndrome Characterized by motor and vocal tics. Motor tics are sudden, brief, involuntary movements involving muscles in different body parts such as eye blinking and shoulder shrugging. Vocal tics consist of gutteral sounds, grunts, or verbalization of words and phrases. Motor manifestations are often associated with behavioral abnormalities such as attention defisits and compulsive ritualistic behaviours.
48 Akathisia The motor activity in akathisia is described by patients as a voluntary effort to relieve uncomfortable sensations. Akathisia is usually expressed as changes in body position, standing, or pacing. In milder forms this can be voluntarily suppressed. In severe cases the need for motor activity is beyond control.
49 Wilson disease (Hepatolenticular degeneration) Autosomal recessive disorder with the gene being located on the long arm of chromosome 13. The gene encodes a copper transporting P-type ATPase that is expressed in liver and kidney Two fundamental defects: 1.reduced biliary transport of copper, 2.impaired formation of plasma ceruloplasmin Free Cu in serum is increased Overflow of copper from the liver produces accumulation in other organs, mainly in brain, kidney, and cornea.
50 Wilson disease (Hepatolenticular degeneration) In cornea, copper is deposited close to the endothelial surface of the Descement membrane (Kayser-Fleischer ring; most important diagnostic feature) Symptoms begin between the ages of 11 and 25 years Wilson disease is a disorder of motor function; there are no sensory symptoms and reflex alterations. Symptoms of basal ganglia damage usually predominate but cerebellar symptoms may occasionally be in the foreground. Tremors and rigidity are the most common early signs. Seizures can occur at any stage of the disease.
51 Wilson disease (Hepatolenticular degeneration) Treatment Initial phase of the treatment (toxic copper levels are brought under control) Penicllamine Ammonium tetrathiomolybdate Triethylene tetramine dihydrohloride (trientine) Maintenance therapy Zinc acetate Trientine + Zinc acetate
52
Basal Ganglia. Motor systems
 409 systems Basal Ganglia You have just read about the different motorrelated cortical areas. Premotor areas are involved in planning, while MI is involved in execution. What you don t know is that the
409 systems Basal Ganglia You have just read about the different motorrelated cortical areas. Premotor areas are involved in planning, while MI is involved in execution. What you don t know is that the
Clinical Psychopharmacology
 Clinical Psychopharmacology Antiparkinsonian drugs Department of Pharmacy, GGZ WNB Chair on Pharmacotherapy in Psychiatric Patients/Anton Loonen May 2015 2 Basal ganglia diseases Parkinson s disease and
Clinical Psychopharmacology Antiparkinsonian drugs Department of Pharmacy, GGZ WNB Chair on Pharmacotherapy in Psychiatric Patients/Anton Loonen May 2015 2 Basal ganglia diseases Parkinson s disease and
Cerebellum and Basal Ganglia
 Cerebellum and Basal Ganglia 1 Contents Cerebellum and Basal Ganglia... 1 Introduction... 3 A brief review of cerebellar anatomy... 4 Basic Circuit... 4 Parallel and climbing fiber input has a very different
Cerebellum and Basal Ganglia 1 Contents Cerebellum and Basal Ganglia... 1 Introduction... 3 A brief review of cerebellar anatomy... 4 Basic Circuit... 4 Parallel and climbing fiber input has a very different
Motor dysfunction 2: Spinal cord injury and subcortical motor disorders ANATOMY REVIEW: Basal Ganglia
 Motor dysfunction 2: Spinal cord injury and subcortical motor disorders ANATOMY REVIEW: Basal Ganglia A group of subcortical nuclei caudate, putamen, globus pallidus Caudate & Putamen = Neostriatum caudate
Motor dysfunction 2: Spinal cord injury and subcortical motor disorders ANATOMY REVIEW: Basal Ganglia A group of subcortical nuclei caudate, putamen, globus pallidus Caudate & Putamen = Neostriatum caudate
GLOSSARY OF TERMS. This glossary explains the terms and words often used in association with Parkinson s.
 Antagonist This glossary explains the terms and words often used in association with Parkinson s. Medications which have a negative effect on particular cells in the body. In Parkinson s dopamine antagonists
Antagonist This glossary explains the terms and words often used in association with Parkinson s. Medications which have a negative effect on particular cells in the body. In Parkinson s dopamine antagonists
Chapter 28. Drug Treatment of Parkinson s Disease
 Chapter 28 Drug Treatment of Parkinson s Disease 1. Introduction Parkinsonism Tremors hands and head develop involuntary movements when at rest; pin rolling sign (finger and thumb) Muscle rigidity arthritis
Chapter 28 Drug Treatment of Parkinson s Disease 1. Introduction Parkinsonism Tremors hands and head develop involuntary movements when at rest; pin rolling sign (finger and thumb) Muscle rigidity arthritis
Meeting Report: XX WFN World Congress on Parkinson s Disease and Related Disorders
 Meeting Report: XX WFN World Congress on Parkinson s Disease and Related Disorders Karen Frei, Erik Ch. Wolters Abstract: The twentieth World Congress on Parkinson s Disease and Related Disorders was held
Meeting Report: XX WFN World Congress on Parkinson s Disease and Related Disorders Karen Frei, Erik Ch. Wolters Abstract: The twentieth World Congress on Parkinson s Disease and Related Disorders was held
Movement disorders and gait disturbances. Kovács Norbert PTE ÁOK Neurológiai Klinika Pécs
 Movement disorders and gait disturbances Kovács Norbert PTE ÁOK Neurológiai Klinika Pécs 1 MD pathophysiology Genetic mutation or environmental injury of basal ganglia functioning Pallidum, thalamus, subthalamic
Movement disorders and gait disturbances Kovács Norbert PTE ÁOK Neurológiai Klinika Pécs 1 MD pathophysiology Genetic mutation or environmental injury of basal ganglia functioning Pallidum, thalamus, subthalamic
Parkinson s Disease - A Junior Doctor s Survival Guide
 Parkinson s Disease - A Junior Doctor s Survival Guide Professor Richard Walker Consultant Geriatrician Hon. Professor of Ageing & Interna
Parkinson s Disease - A Junior Doctor s Survival Guide Professor Richard Walker Consultant Geriatrician Hon. Professor of Ageing & Interna
Circuit Disorders of the Basal Ganglia: Parkinson s Disease Pathophysiology and Surgical Treatments
 Circuit Disorders of the Basal Ganglia: Parkinson s Disease Pathophysiology and Surgical Treatments Mahlon R. DeLong M.D. W. P. Timmie Professor of Neurology Emory University School of Medicine The Basal
Circuit Disorders of the Basal Ganglia: Parkinson s Disease Pathophysiology and Surgical Treatments Mahlon R. DeLong M.D. W. P. Timmie Professor of Neurology Emory University School of Medicine The Basal
PARKINSON S DISEASE AND PARKINSONISM. Dr Phil Wood Geriatrician, Waitemata DHB Clinical Unit Leader, Waikato DHB
 PARKINSON S DISEASE AND PARKINSONISM Dr Phil Wood Geriatrician, Waitemata DHB Clinical Unit Leader, Waikato DHB OUTLINE Covering:- Why this is an important area of Medical and Psychiatric care The variety
PARKINSON S DISEASE AND PARKINSONISM Dr Phil Wood Geriatrician, Waitemata DHB Clinical Unit Leader, Waikato DHB OUTLINE Covering:- Why this is an important area of Medical and Psychiatric care The variety
Welcome to the Medical Risk Webinar: a taster of Assessing and Managing Medical Risk for Insurers courses. 26 April 2013
 Welcome to the Medical Risk Webinar: a taster of Assessing and Managing Medical Risk for Insurers courses 26 April 2013 1 Parkinson s Disease & Multiple Sclerosis Dr Nick Niven Jenkins 2 Movement Human
Welcome to the Medical Risk Webinar: a taster of Assessing and Managing Medical Risk for Insurers courses 26 April 2013 1 Parkinson s Disease & Multiple Sclerosis Dr Nick Niven Jenkins 2 Movement Human
Parkinson's s disease - a
 Parkinson's Disease Parkinson's s disease - a progressive disorder of the nervous system that affects movement. The most common perception of Parkinson s is the patient having tremors. Hands shaking, inability
Parkinson's Disease Parkinson's s disease - a progressive disorder of the nervous system that affects movement. The most common perception of Parkinson s is the patient having tremors. Hands shaking, inability
Dementia & Movement Disorders
 Dementia & Movement Disorders A/Prof Michael Davis Geriatrician ACT Health & GSAHS ANU Medical School Eastern Dementia Network Aged and Dementia Care Symposium Bateman s Bay, 22 October 2010 Types of Dementia
Dementia & Movement Disorders A/Prof Michael Davis Geriatrician ACT Health & GSAHS ANU Medical School Eastern Dementia Network Aged and Dementia Care Symposium Bateman s Bay, 22 October 2010 Types of Dementia
Motor Fluctuations in Parkinson s
 Motor Fluctuations in Parkinson s What are motor fluctuations? Motor fluctuations are associated with longterm use of levodopa (trade names Sinemet or Madopar, Co-careldopa or Co-beneldopa), and usually
Motor Fluctuations in Parkinson s What are motor fluctuations? Motor fluctuations are associated with longterm use of levodopa (trade names Sinemet or Madopar, Co-careldopa or Co-beneldopa), and usually
What is PD? Dr Catherine Dotchin MD MRCP Consultant Geriatrician
 What is PD? Dr Catherine Dotchin MD MRCP Consultant Geriatrician Overview of presentation Case history Video example pre and post treatment Historical review PD in the UK Epidemiology and aetiology Making
What is PD? Dr Catherine Dotchin MD MRCP Consultant Geriatrician Overview of presentation Case history Video example pre and post treatment Historical review PD in the UK Epidemiology and aetiology Making
Unit 2 - Subcortical systems, neurochemistry and brain function
 Unit 2 - Subcortical systems, neurochemistry and brain function Subcortical anatomy: Most of the five major subdivisions of the brain are subcortical. I. Telencephalon (cortical - part of forebrain) -
Unit 2 - Subcortical systems, neurochemistry and brain function Subcortical anatomy: Most of the five major subdivisions of the brain are subcortical. I. Telencephalon (cortical - part of forebrain) -
Reflex Physiology. Dr. Ali Ebneshahidi. 2009 Ebneshahidi
 Reflex Physiology Dr. Ali Ebneshahidi Reflex Physiology Reflexes are automatic, subconscious response to changes within or outside the body. a. Reflexes maintain homeostasis (autonomic reflexes) heart
Reflex Physiology Dr. Ali Ebneshahidi Reflex Physiology Reflexes are automatic, subconscious response to changes within or outside the body. a. Reflexes maintain homeostasis (autonomic reflexes) heart
CENTRAL NERVOUS SYSTEM MANAGEMENT OF PARKINSON S DISEASE
 MANAGEMENT CENTRAL NERVOUS SYSTEM MANAGEMENT OF PARKINSON S DISEASE Parkinson s Disease is classically determined by the triad or rest tremor (usually starting in one arm) with bradykinesia (slowing of
MANAGEMENT CENTRAL NERVOUS SYSTEM MANAGEMENT OF PARKINSON S DISEASE Parkinson s Disease is classically determined by the triad or rest tremor (usually starting in one arm) with bradykinesia (slowing of
NEUROLOCALIZATION MADE EASY
 NEUROLOCALIZATION MADE EASY Jared B. Galle, DVM, Diplomate ACVIM (Neurology) Dogwood Veterinary Referral Center 4920 Ann Arbor-Saline Road Ann Arbor, MI 48103 Localizing a neurologic problem to an anatomical
NEUROLOCALIZATION MADE EASY Jared B. Galle, DVM, Diplomate ACVIM (Neurology) Dogwood Veterinary Referral Center 4920 Ann Arbor-Saline Road Ann Arbor, MI 48103 Localizing a neurologic problem to an anatomical
CEREBRAL PALSY CLASSIFICATION BY SEVERITY LEVEL
 Patient Name: Today s Date: CAUSE OF CEREBRAL PALSY Hypoxic-Ischemic Encephalopathy (HIE) or Intrapartum Asphyxia - Brain injury Lack of oxygen to the brain or asphyxia. Intracranial Hemorrhage (IVH) Brain
Patient Name: Today s Date: CAUSE OF CEREBRAL PALSY Hypoxic-Ischemic Encephalopathy (HIE) or Intrapartum Asphyxia - Brain injury Lack of oxygen to the brain or asphyxia. Intracranial Hemorrhage (IVH) Brain
Deep Brain Stimulation for Essential Tremor and Parkinson s Disease (NCD 160.24)
") Policy Number Reimbursement Policy 160.24 Approved By UnitedHealthcare Medicare Reimbursement Policy Committee Current Approval Date 06/10/2015 IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy
Policy Number Reimbursement Policy 160.24 Approved By UnitedHealthcare Medicare Reimbursement Policy Committee Current Approval Date 06/10/2015 IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy
Anti-Parkinsonism Drugs
 Anti-Parkinsonism Drugs Pharma Team 429 Fahad Alrumaih Ibrahim Alshiddi Sultan Alsalem Ismail Raslan Suhail Asiri Parkinsonism - Could be: primary [idiopathic] or secondary [viral infection or drug induced
Anti-Parkinsonism Drugs Pharma Team 429 Fahad Alrumaih Ibrahim Alshiddi Sultan Alsalem Ismail Raslan Suhail Asiri Parkinsonism - Could be: primary [idiopathic] or secondary [viral infection or drug induced
How To Understand The Function Of The Basal Ganglia
 122 NEUROCIRCUITRY OF PARKINSON S DISEASE THOMAS WICHMANN MAHLON R. DELONG Recent progress in neuroscience research has led to major insights into the structure and function of the basal ganglia and into
122 NEUROCIRCUITRY OF PARKINSON S DISEASE THOMAS WICHMANN MAHLON R. DELONG Recent progress in neuroscience research has led to major insights into the structure and function of the basal ganglia and into
Mini-atlas of the Marmoset Brain
 Mini-atlas of the Marmoset Brain http://marmoset-brain.org Aya Senoo Tokyo University of Agriculture and Technology Hironobu Tokuno Tokyo Metropolitan Institute of Medical Science Charles Watson Curtin
Mini-atlas of the Marmoset Brain http://marmoset-brain.org Aya Senoo Tokyo University of Agriculture and Technology Hironobu Tokuno Tokyo Metropolitan Institute of Medical Science Charles Watson Curtin
Lauren Schrock, M.D Assistant Professor of Neurology University of Utah Co-Director, Movement Disorders Program
 Lauren Schrock, M.D Assistant Professor of Neurology University of Utah Co-Director, Movement Disorders Program Brief clinical overview What are tics? Definition of TS and related tic disorders What we
Lauren Schrock, M.D Assistant Professor of Neurology University of Utah Co-Director, Movement Disorders Program Brief clinical overview What are tics? Definition of TS and related tic disorders What we
Diagram 2(i): Structure of the Neuron
: Structure of the Neuron") Diagram 2(i): Structure of the Neuron Generally speaking, we can divide the nervous system into different parts, according to location and function. So far we have mentioned the central nervous system
Diagram 2(i): Structure of the Neuron Generally speaking, we can divide the nervous system into different parts, according to location and function. So far we have mentioned the central nervous system
Abnormal Involuntary Movement Disorders (Dyskinesias)
") Essentials of Clinical Neurology: Abnormal Involuntary Movement Disorders (Dyskinesias) 20-1 Chapter 20 Abnormal Involuntary Movement Disorders (Dyskinesias) Abnormal involuntary movement disorders are
Essentials of Clinical Neurology: Abnormal Involuntary Movement Disorders (Dyskinesias) 20-1 Chapter 20 Abnormal Involuntary Movement Disorders (Dyskinesias) Abnormal involuntary movement disorders are
Neurogenic Disorders of Speech in Children and Adults
 Neurogenic Disorders of Speech in Children and Adults Complexity of Speech Speech is one of the most complex activities regulated by the nervous system It involves the coordinated contraction of a large
Neurogenic Disorders of Speech in Children and Adults Complexity of Speech Speech is one of the most complex activities regulated by the nervous system It involves the coordinated contraction of a large
CSE511 Brain & Memory Modeling. Lect04: Brain & Spine Neuroanatomy
 CSE511 Brain & Memory Modeling CSE511 Brain & Memory Modeling Lect02: BOSS Discrete Event Simulator Lect04: Brain & Spine Neuroanatomy Appendix of Purves et al., 4e Larry Wittie Computer Science, StonyBrook
CSE511 Brain & Memory Modeling CSE511 Brain & Memory Modeling Lect02: BOSS Discrete Event Simulator Lect04: Brain & Spine Neuroanatomy Appendix of Purves et al., 4e Larry Wittie Computer Science, StonyBrook
Disorders Considered. A Brief Synopsis of Select Neurological Disorders. Neurological and Psychiatric Symptoms. Neurological Basis
 Disorders Considered A Brief Synopsis of Select Neurological Disorders Four neurological disorders are examined to illustrate pathological conditions that can develop related to course material Myasthenia
Disorders Considered A Brief Synopsis of Select Neurological Disorders Four neurological disorders are examined to illustrate pathological conditions that can develop related to course material Myasthenia
Diagnosis and Treatment of Parkinson s Disease: A Systematic Review of the Literature
 Evidence Report/Technology Assessment Number 57 Diagnosis and Treatment of Parkinson s Disease: A Systematic Review of the Literature Prepared for: Agency for Healthcare Research and Quality U.S. Department
Evidence Report/Technology Assessment Number 57 Diagnosis and Treatment of Parkinson s Disease: A Systematic Review of the Literature Prepared for: Agency for Healthcare Research and Quality U.S. Department
Management in the pre-hospital setting
 Management in the pre-hospital setting Inflammation of the joints Two main types: Osteoarthritis - cartilage loss from wear and tear Rheumatoid arthritis - autoimmune disorder Affects all age groups,
Management in the pre-hospital setting Inflammation of the joints Two main types: Osteoarthritis - cartilage loss from wear and tear Rheumatoid arthritis - autoimmune disorder Affects all age groups,
PARKINSON S DISEASE IN LONG-TERM-CARE SETTINGS
 PARKINSON S DISEASE IN LONG-TERM-CARE SETTINGS De Anna Looper, RN CHPN Corporate Clinical Consultant / Legal Nurse Consultant Carrefour Associates L.L.C. PARKINSON S DISEASE IN LONG-TERM-CARE SETTINGS
PARKINSON S DISEASE IN LONG-TERM-CARE SETTINGS De Anna Looper, RN CHPN Corporate Clinical Consultant / Legal Nurse Consultant Carrefour Associates L.L.C. PARKINSON S DISEASE IN LONG-TERM-CARE SETTINGS
WHAT IS CEREBRAL PALSY?
 WHAT IS CEREBRAL PALSY? Cerebral Palsy is a dysfunction in movement resulting from injury to or poor development of the brain prior to birth or in early childhood. Generally speaking, any injury or disease
WHAT IS CEREBRAL PALSY? Cerebral Palsy is a dysfunction in movement resulting from injury to or poor development of the brain prior to birth or in early childhood. Generally speaking, any injury or disease
Sheep Brain Dissection
 Sheep Brain Dissection http://www.carolina.com/product/preserved+organisms/preserved+animals+%28mammal s%29/sheep+organs/preserved+sheep+dissection.do Michigan State University Neuroscience Program Brain
Sheep Brain Dissection http://www.carolina.com/product/preserved+organisms/preserved+animals+%28mammal s%29/sheep+organs/preserved+sheep+dissection.do Michigan State University Neuroscience Program Brain
About Brain Injury: A Guide to Brain Anatomy Information from http://www.waiting.com, 1997-2002, Becca, Ltd.
 About Brain Injury: A Guide to Brain Anatomy Information from http://www.waiting.com, 1997-2002, Becca, Ltd. Brain Anatomy Definitions Brainstem: The lower extension of the brain where it connects to the
About Brain Injury: A Guide to Brain Anatomy Information from http://www.waiting.com, 1997-2002, Becca, Ltd. Brain Anatomy Definitions Brainstem: The lower extension of the brain where it connects to the
Journal Club. Parkinsonismo iatrogeno
 PROGETTO UNIVA 2013 Journal Club Parkinsonismo iatrogeno Pietro Gareri, MD, PhD Geriatra ASP Catanzaro Lamezia Terme 3 Luglio 2013 Drug-induced parkinsonism (DIP) was recognized in the early 1950s as a
PROGETTO UNIVA 2013 Journal Club Parkinsonismo iatrogeno Pietro Gareri, MD, PhD Geriatra ASP Catanzaro Lamezia Terme 3 Luglio 2013 Drug-induced parkinsonism (DIP) was recognized in the early 1950s as a
Doncaster & Bassetlaw Medicines Formulary
 Doncaster & Bassetlaw Medicines Formulary Section 4.9: Drugs Used in Parkinsonism and related Disorders Co-Beneldopa 12.5/50, 25/100 and 50/200 (Madopar) Capsules Co-Beneldopa 12.5/50 and 25/100 Dispersible
Doncaster & Bassetlaw Medicines Formulary Section 4.9: Drugs Used in Parkinsonism and related Disorders Co-Beneldopa 12.5/50, 25/100 and 50/200 (Madopar) Capsules Co-Beneldopa 12.5/50 and 25/100 Dispersible
Musculoskeletal System
 CHAPTER 3 Impact of SCI on the Musculoskeletal System Voluntary movement of the body is dependent on a number of systems. These include: The brain initiates the movement and receives feedback to assess
CHAPTER 3 Impact of SCI on the Musculoskeletal System Voluntary movement of the body is dependent on a number of systems. These include: The brain initiates the movement and receives feedback to assess
The majority of parkinsonism (approx. 80%) is due to idiopathic PD other causes include drug therapy (Table 1),toxins and trauma.
 is due to idiopathic PD other causes include drug therapy (Table 1),toxins and trauma.") THE TREATMENT OF PARKINSON S DISEASE SUMMARY Levodopa (L-dopa) administered in conjunction with a dopa decarboxylase inhibitor (DDCI) remains the mainstay of therapy for Parkinson s disease. New drugs
THE TREATMENT OF PARKINSON S DISEASE SUMMARY Levodopa (L-dopa) administered in conjunction with a dopa decarboxylase inhibitor (DDCI) remains the mainstay of therapy for Parkinson s disease. New drugs
Chapter 3 The Anatomy of the Nervous System
 Chapter 3 The Anatomy of the Nervous System Systems, Structures, and Cells That Make Up Your Nervous System 1 General Layout of the Nervous System Central Nervous System (CNS) Brain (in the skull) Spinal
Chapter 3 The Anatomy of the Nervous System Systems, Structures, and Cells That Make Up Your Nervous System 1 General Layout of the Nervous System Central Nervous System (CNS) Brain (in the skull) Spinal
F r e q u e n t l y A s k e d Q u e s t i o n s
 Myasthenia Gravis Q: What is myasthenia gravis (MG)? A: Myasthenia gravis (meye-uhss- THEEN-ee-uh GRAV uhss) (MG) is an autoimmune disease that weakens the muscles. The name comes from Greek and Latin
Myasthenia Gravis Q: What is myasthenia gravis (MG)? A: Myasthenia gravis (meye-uhss- THEEN-ee-uh GRAV uhss) (MG) is an autoimmune disease that weakens the muscles. The name comes from Greek and Latin
Parkinson s Disease (PD)
") Parkinson s Disease (PD) Parkinson s disease (PD) is a movement disorder that worsens over time. About 1 in 100 people older than 60 has Parkinson s. The exact cause of PD is still not known, but research
Parkinson s Disease (PD) Parkinson s disease (PD) is a movement disorder that worsens over time. About 1 in 100 people older than 60 has Parkinson s. The exact cause of PD is still not known, but research
DISSECTION OF THE SHEEP'S BRAIN
 DISSECTION OF THE SHEEP'S BRAIN Introduction The purpose of the sheep brain dissection is to familiarize you with the threedimensional structure of the brain and teach you one of the great methods of studying
DISSECTION OF THE SHEEP'S BRAIN Introduction The purpose of the sheep brain dissection is to familiarize you with the threedimensional structure of the brain and teach you one of the great methods of studying
 CAMBRIDGE UNIVERSITY CENTRE FOR BRAIN REPAIR A layman's account of our scientific objectives What is Brain Damage? Many forms of trauma and disease affect the nervous system to produce permanent neurological
CAMBRIDGE UNIVERSITY CENTRE FOR BRAIN REPAIR A layman's account of our scientific objectives What is Brain Damage? Many forms of trauma and disease affect the nervous system to produce permanent neurological
ABC s of Parkinson s Disease 4/29/15 Karen Parenti, MS, PsyD
 ABC s of Parkinson s Disease 4/29/15 Karen Parenti, MS, PsyD What is Parkinson s Disease? Parkinson's disease is a progressive disorder of the nervous system that affects movement. It develops gradually,
ABC s of Parkinson s Disease 4/29/15 Karen Parenti, MS, PsyD What is Parkinson s Disease? Parkinson's disease is a progressive disorder of the nervous system that affects movement. It develops gradually,
Vocabulary & General Concepts of Brain Organization
 Vocabulary & General Concepts of Brain Organization Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine Course Outline Lecture 1: Vocabulary & General Concepts of Brain
Vocabulary & General Concepts of Brain Organization Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine Course Outline Lecture 1: Vocabulary & General Concepts of Brain
Jellow. for the Cerebral Palsy. Antara Hazarika, Kumar Anchal, Priti Thankar, Samraat Sardesai. a study by
 Jellow for the Cerebral Palsy a study by Antara Hazarika, Kumar Anchal, Priti Thankar, Samraat Sardesai Index Understanding the world of CP Modes of communication The need for the product ( product rational)
Jellow for the Cerebral Palsy a study by Antara Hazarika, Kumar Anchal, Priti Thankar, Samraat Sardesai Index Understanding the world of CP Modes of communication The need for the product ( product rational)
Benign tremulous Parkinson s disease
 Acta neurol. belg., 2008, 108, 48-52 Benign tremulous Parkinson s disease Alev LEVENTOGLU 1 and Ali Ihsan BAYSAL 2 1 Ufuk University Faculty of Medicine and 2 Güven Hospital, Department of Neurology, Ankara,
Acta neurol. belg., 2008, 108, 48-52 Benign tremulous Parkinson s disease Alev LEVENTOGLU 1 and Ali Ihsan BAYSAL 2 1 Ufuk University Faculty of Medicine and 2 Güven Hospital, Department of Neurology, Ankara,
Neurophysiological assessment of movement disorders. By Dr Carla Cordivari
 Neurophysiological assessment of movement disorders By Dr Carla Cordivari NEUROPHYSIOLOGICAL ASSESSMENT OF MOVEMENT DISORDERS Neurophysiological investigations in movement disorders are objective methods
Neurophysiological assessment of movement disorders By Dr Carla Cordivari NEUROPHYSIOLOGICAL ASSESSMENT OF MOVEMENT DISORDERS Neurophysiological investigations in movement disorders are objective methods
Multifocal Motor Neuropathy. Jonathan Katz, MD Richard Lewis, MD
 Multifocal Motor Neuropathy Jonathan Katz, MD Richard Lewis, MD What is Multifocal Motor Neuropathy? Multifocal Motor Neuropathy (MMN) is a rare condition in which multiple motor nerves are attacked by
Multifocal Motor Neuropathy Jonathan Katz, MD Richard Lewis, MD What is Multifocal Motor Neuropathy? Multifocal Motor Neuropathy (MMN) is a rare condition in which multiple motor nerves are attacked by
Dr. Enas Elsayed. Brunnstrom Approach
 Brunnstrom Approach Learning Objectives: By the end of this lab, the student will be able to: 1. Demonstrate different reflexes including stimulus and muscle tone response. 2. Demonstrate how to evoke
Brunnstrom Approach Learning Objectives: By the end of this lab, the student will be able to: 1. Demonstrate different reflexes including stimulus and muscle tone response. 2. Demonstrate how to evoke
Movement Disorders: Diagnosis i and Treatment. Movement Disorders: Classification
 Movement Disorders: Diagnosis i and Treatment Lawrence Elmer, MD, PhD Professor Dept. of Neurology University of Toledo College of Medicine Movement Disorders: Review Movement Disorders: Classification
Movement Disorders: Diagnosis i and Treatment Lawrence Elmer, MD, PhD Professor Dept. of Neurology University of Toledo College of Medicine Movement Disorders: Review Movement Disorders: Classification
Management of Parkinson s Disease in Primary Care
 Management of Parkinson s Disease in Primary Care Dr June Tan National University Hospital System (NUHS) Division of Neurology Senior Consultant Topics: Diagnosing PD Choice of medication in the de novo
Management of Parkinson s Disease in Primary Care Dr June Tan National University Hospital System (NUHS) Division of Neurology Senior Consultant Topics: Diagnosing PD Choice of medication in the de novo
Multiple System Atrophy
 Multiple System Atrophy U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health Multiple System Atrophy What is multiple system atrophy? Multiple system atrophy
Multiple System Atrophy U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health Multiple System Atrophy What is multiple system atrophy? Multiple system atrophy
Aetna Nerve Conduction Study Policy
 Aetna Nerve Conduction Study Policy Policy Aetna considers nerve conduction velocity (NCV) studies medically necessary when both of the following criteria are met: 1. Member has any of the following indications:
Aetna Nerve Conduction Study Policy Policy Aetna considers nerve conduction velocity (NCV) studies medically necessary when both of the following criteria are met: 1. Member has any of the following indications:
STROKE CARE NOW NETWORK CONFERENCE MAY 22, 2014
 STROKE CARE NOW NETWORK CONFERENCE MAY 22, 2014 Rehabilitation Innovations in Post- Stroke Recovery Madhav Bhat, MD Fort Wayne Neurological Center DISCLOSURE Paid speaker for TEVA Neuroscience Program.
STROKE CARE NOW NETWORK CONFERENCE MAY 22, 2014 Rehabilitation Innovations in Post- Stroke Recovery Madhav Bhat, MD Fort Wayne Neurological Center DISCLOSURE Paid speaker for TEVA Neuroscience Program.
Parkinson s Disease: A Review of Motor and Nonmotor Symptoms
 Diana Hong Parkinson s Disease: A Review of Motor and Nonmotor Symptoms Abstract: Although Parkinson s disease (PD) is considered a motor system disorder caused by the degeneration of dopaminergic neurons
Diana Hong Parkinson s Disease: A Review of Motor and Nonmotor Symptoms Abstract: Although Parkinson s disease (PD) is considered a motor system disorder caused by the degeneration of dopaminergic neurons
Pharmacology of the Central Nervous System (CNS) Dr. Sabry Attia. November 2006
 Dr. Sabry Attia. November 2006") Pharmacology of the Central Nervous System (CNS) Dr. Sabry Attia November 2006 Neurodegenerative disease Neurodegenerative disease is a condition which affects brain function. They are result from deterioration
Pharmacology of the Central Nervous System (CNS) Dr. Sabry Attia November 2006 Neurodegenerative disease Neurodegenerative disease is a condition which affects brain function. They are result from deterioration
Guide to Deep Brain Stimulation Therapy
 Parkinson s Disease: Guide to Deep Brain Stimulation Therapy By: Michael S. Okun, MD Medical Director, National Parkinson Foundation Center of Excellence Co-Director, Center for Movement Disorders and
Parkinson s Disease: Guide to Deep Brain Stimulation Therapy By: Michael S. Okun, MD Medical Director, National Parkinson Foundation Center of Excellence Co-Director, Center for Movement Disorders and
NEUROIMAGING in Parkinsonian Syndromes
 NEUROIMAGING in Parkinsonian Syndromes (Focus on Structural Techniques: CT and MRI) Dr. Roberto Cilia Parkinson Institute, ICP, Milan, Italy OUTLINE Primary Parkinsonism Idiopathic Parkinson s Disease
NEUROIMAGING in Parkinsonian Syndromes (Focus on Structural Techniques: CT and MRI) Dr. Roberto Cilia Parkinson Institute, ICP, Milan, Italy OUTLINE Primary Parkinsonism Idiopathic Parkinson s Disease
Slide 1: Introduction Introduce the purpose of your presentation. Indicate that you will explain how the brain basically works and how and where
 Slide 1: Introduction Introduce the purpose of your presentation. Indicate that you will explain how the brain basically works and how and where drugs such as heroin and cocaine work in the brain. Tell
Slide 1: Introduction Introduce the purpose of your presentation. Indicate that you will explain how the brain basically works and how and where drugs such as heroin and cocaine work in the brain. Tell
Nervous System: Spinal Cord and Spinal Nerves (Chapter 13) Lecture Materials for Amy Warenda Czura, Ph.D. Suffolk County Community College
 Lecture Materials for Amy Warenda Czura, Ph.D. Suffolk County Community College") Nervous System: Spinal Cord and Spinal Nerves (Chapter 13) Lecture Materials for Amy Warenda Czura, Ph.D. Suffolk County Community College Primary Sources for figures and content: Eastern Campus Marieb,
Nervous System: Spinal Cord and Spinal Nerves (Chapter 13) Lecture Materials for Amy Warenda Czura, Ph.D. Suffolk County Community College Primary Sources for figures and content: Eastern Campus Marieb,
Norepinephrine Effects On the System
 Norepinephrine Effects On the System NE Conversion to Epinephrine in the Circulation Under stress, the increased norepinephrine produced is transmitted throughout the system. This increased level represents
Norepinephrine Effects On the System NE Conversion to Epinephrine in the Circulation Under stress, the increased norepinephrine produced is transmitted throughout the system. This increased level represents
Cerebral Palsy. In order to function, the brain needs a continuous supply of oxygen.
 Cerebral Palsy Introduction Cerebral palsy, or CP, can cause serious neurological symptoms in children. Up to 5000 children in the United States are diagnosed with cerebral palsy every year. This reference
Cerebral Palsy Introduction Cerebral palsy, or CP, can cause serious neurological symptoms in children. Up to 5000 children in the United States are diagnosed with cerebral palsy every year. This reference
UNIVERSITY OF BOLTON EDUCATION & PSYCHOLOGY PSYCHOLOGY SEMESTER 1 EXAMINATIONS 2014/2015 COGNITIVE & BIOLOGICAL PERSPECTIVES MODULE NO: PSC4003
 [EDP 005] UNIVERSITY OF BOLTON EDUCATION & PSYCHOLOGY PSYCHOLOGY SEMESTER 1 EXAMINATIONS 2014/2015 COGNITIVE & BIOLOGICAL PERSPECTIVES MODULE NO: PSC4003 Date: Wednesday 21 st January, 2015 Time: 2.00pm
[EDP 005] UNIVERSITY OF BOLTON EDUCATION & PSYCHOLOGY PSYCHOLOGY SEMESTER 1 EXAMINATIONS 2014/2015 COGNITIVE & BIOLOGICAL PERSPECTIVES MODULE NO: PSC4003 Date: Wednesday 21 st January, 2015 Time: 2.00pm
Function (& other notes)
") LAB 8. ANATOMY OF THE HUMAN BRAIN In this exercise you each will map the human brain both anatomy and function so that you can develop a more accurate picture of what s going on in your head :-) EXTERNAL
LAB 8. ANATOMY OF THE HUMAN BRAIN In this exercise you each will map the human brain both anatomy and function so that you can develop a more accurate picture of what s going on in your head :-) EXTERNAL
3) Cerebral Cortex & Functions of the 4 LOBES. 5) Cranial Nerves (Nerves In the Cranium, i.e., Head)
 Cerebral Cortex & Functions of the 4 LOBES. 5) Cranial Nerves (Nerves In the Cranium, i.e., Head)") Lecture 5 (Oct 8 th ): ANATOMY and FUNCTION OF THE NERVOUS SYSTEM Lecture Outline 1) Basic Divisions (CNS vs. PNS, Somatic vs. Autonomic) and Directional Terms 2) The Brain (Hindbrain/ Midbrain/ Forebrain)
Lecture 5 (Oct 8 th ): ANATOMY and FUNCTION OF THE NERVOUS SYSTEM Lecture Outline 1) Basic Divisions (CNS vs. PNS, Somatic vs. Autonomic) and Directional Terms 2) The Brain (Hindbrain/ Midbrain/ Forebrain)
Chapter 7: The Nervous System
 Chapter 7: The Nervous System Objectives Discuss the general organization of the nervous system Describe the structure & function of a nerve Draw and label the pathways involved in a withdraw reflex Define
Chapter 7: The Nervous System Objectives Discuss the general organization of the nervous system Describe the structure & function of a nerve Draw and label the pathways involved in a withdraw reflex Define
ALL ABOUT SPASTICITY. www.almirall.com. Solutions with you in mind
 ALL ABOUT SPASTICITY www.almirall.com Solutions with you in mind WHAT IS SPASTICITY? The muscles of the body maintain what is called normal muscle tone, a level of muscle tension that allows us to hold
ALL ABOUT SPASTICITY www.almirall.com Solutions with you in mind WHAT IS SPASTICITY? The muscles of the body maintain what is called normal muscle tone, a level of muscle tension that allows us to hold
Chapter 13. The Nature of Somatic Reflexes
 Chapter 13 The Nature of Somatic Reflexes Nature of Reflexes (1 of 3) A reflex is an involuntary responses initiated by a sensory input resulting in a change in a gland or muscle tissue occur without our
Chapter 13 The Nature of Somatic Reflexes Nature of Reflexes (1 of 3) A reflex is an involuntary responses initiated by a sensory input resulting in a change in a gland or muscle tissue occur without our
MOTION AND E-MOTION. Andrea Cavanna MD PhD FRCP
 MOTION AND E-MOTION Andrea Cavanna MD PhD FRCP Consultant in Behavioural Neurology, BSMHFT, Birmingham, UK Hon Professor in Neuropsychiatry, Aston University, Birmingham, UK Hon Reader in Neuropsychiatry,
MOTION AND E-MOTION Andrea Cavanna MD PhD FRCP Consultant in Behavioural Neurology, BSMHFT, Birmingham, UK Hon Professor in Neuropsychiatry, Aston University, Birmingham, UK Hon Reader in Neuropsychiatry,
31.1 The Neuron. BUILD Vocabulary. Lesson Objectives
 Name Class Date 31.1 The Neuron Lesson Objectives Identify the functions of the nervous system. Describe the function of neurons. Describe how a nerve impulse is transmitted. BUILD Vocabulary A. The chart
Name Class Date 31.1 The Neuron Lesson Objectives Identify the functions of the nervous system. Describe the function of neurons. Describe how a nerve impulse is transmitted. BUILD Vocabulary A. The chart
BIO130 Chapter 14 The Brain and Cranial Nerves Lecture Outline
 BIO130 Chapter 14 The Brain and Cranial Nerves Lecture Outline Brain structure 1. Cerebrum Hemispheres: left & right Cerebral cortex Gyri Sulci Fissures Longitudinal fissure Corpus callosum Lobes Central
BIO130 Chapter 14 The Brain and Cranial Nerves Lecture Outline Brain structure 1. Cerebrum Hemispheres: left & right Cerebral cortex Gyri Sulci Fissures Longitudinal fissure Corpus callosum Lobes Central
Webinar title: Know Your Options for Treating Severe Spasticity
 Webinar title: Know Your Options for Treating Severe Spasticity Presented by: Dr. Gerald Bilsky, Physiatrist Medical Director of Outpatient Services and Associate Medical Director of Acquired Brain Injury
Webinar title: Know Your Options for Treating Severe Spasticity Presented by: Dr. Gerald Bilsky, Physiatrist Medical Director of Outpatient Services and Associate Medical Director of Acquired Brain Injury
Cerebral Palsy. 1995-2014, The Patient Education Institute, Inc. www.x-plain.com nr200105 Last reviewed: 06/17/2014 1
 Cerebral Palsy Introduction Cerebral palsy, or CP, can cause serious neurological symptoms in children. Thousands of children are diagnosed with cerebral palsy every year. This reference summary explains
Cerebral Palsy Introduction Cerebral palsy, or CP, can cause serious neurological symptoms in children. Thousands of children are diagnosed with cerebral palsy every year. This reference summary explains
Parkinson s Disease and Dementia. Dr N Samaniego Consultant Physician and Geriatrician
 Parkinson s Disease and Dementia Dr N Samaniego Consultant Physician and Geriatrician Case 68 year old female. Off legs for a few months, O/E no neurological deficit. -Slowing down -Needs help with dressing,
Parkinson s Disease and Dementia Dr N Samaniego Consultant Physician and Geriatrician Case 68 year old female. Off legs for a few months, O/E no neurological deficit. -Slowing down -Needs help with dressing,
Introduction to Psychology, 7th Edition, Rod Plotnik Module 3: Brain s Building Blocks. Module 3. Brain s Building Blocks
 Module 3 Brain s Building Blocks Structure of the Brain Genes chains of chemicals that are arranged like rungs on a twisting ladder there are about 100,000 genes that contain chemical instructions that
Module 3 Brain s Building Blocks Structure of the Brain Genes chains of chemicals that are arranged like rungs on a twisting ladder there are about 100,000 genes that contain chemical instructions that
THE LUMBAR SPINE (BACK)
") THE LUMBAR SPINE (BACK) At a glance Chronic back pain, especially in the area of the lumbar spine (lower back), is a widespread condition. It can be assumed that 75 % of all people have it sometimes or
THE LUMBAR SPINE (BACK) At a glance Chronic back pain, especially in the area of the lumbar spine (lower back), is a widespread condition. It can be assumed that 75 % of all people have it sometimes or
Effective SLP Interventions for Children with Cerebral Palsy
 Effective SLP Interventions for Children with Cerebral Palsy NDT/Traditional/Eclectic, PhD, CCC-SLP, C/NDT Contents Preface Acknowledgments Contributors ix x xi Chapter 1. The Development in Neurodevelopmental
Effective SLP Interventions for Children with Cerebral Palsy NDT/Traditional/Eclectic, PhD, CCC-SLP, C/NDT Contents Preface Acknowledgments Contributors ix x xi Chapter 1. The Development in Neurodevelopmental
Infant reflexes and stereotypies are very important in the process of development
 Infant Reflexes and Stereotypies Infant reflexes and stereotypies are very important in the process of development 2007 McGraw-Hill Higher Education. All rights reserved. Importance of Infant Reflexes
Infant Reflexes and Stereotypies Infant reflexes and stereotypies are very important in the process of development 2007 McGraw-Hill Higher Education. All rights reserved. Importance of Infant Reflexes
Nervous System Organization. PNS and CNS. Nerves. Peripheral Nervous System. Peripheral Nervous System. Motor Component.
 Nervous System Organization PNS and CNS Chapters 8 and 9 Peripheral Nervous System (PNS) connects CNS to sensory receptors, muscles and glands Central Nervous System (CNS) control/integrating center brain
Nervous System Organization PNS and CNS Chapters 8 and 9 Peripheral Nervous System (PNS) connects CNS to sensory receptors, muscles and glands Central Nervous System (CNS) control/integrating center brain