Statement on Disability: Pulmonary Hypertension
|
|
|
- Christal Logan
- 9 years ago
- Views:
Transcription
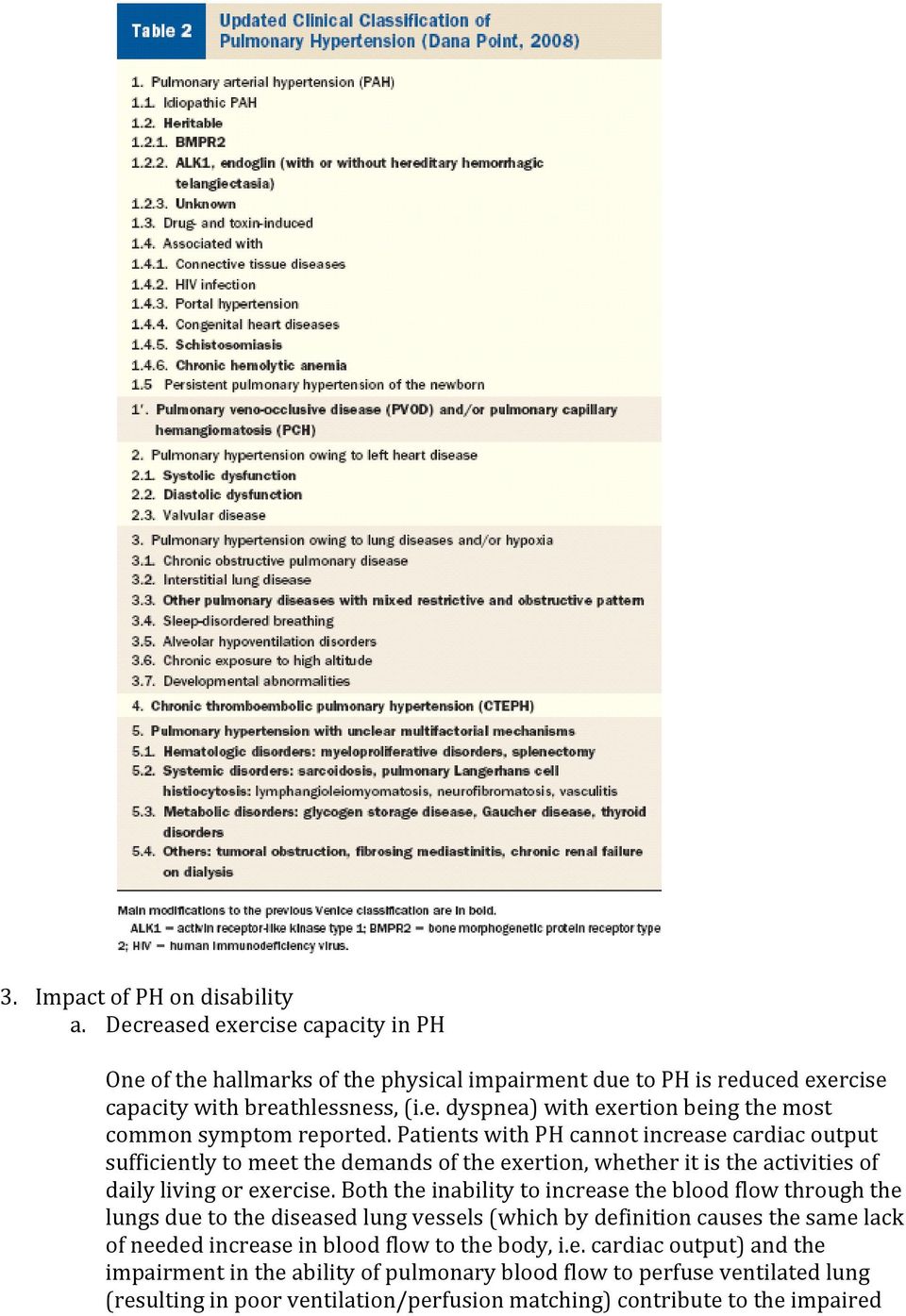
1 Statement on Disability: Pulmonary Hypertension Ronald J. Oudiz, MD and Robyn J. Barst, MD on behalf of Pulmonary Hypertension Association The Scientific Leadership Council of the Pulmonary Hypertension Association (PHA) drafted this document to provide guidance for the development of disability criteria for patients with pulmonary hypertension by the Institute of Medicine (IOM) for the Social Security Administration (SSA). Pulmonary hypertension (PH) is defined as an abnormal elevation of pulmonary arterial pressure, and can result in progressive enlargement and dysfunction of the right ventricle (the right side of the heart), often leading to rapidly progressive clinical heart failure and death 1. Disability due to PH is multifactorial, and can depend on factors such as the PH patient s degree of aerobic impairment, functional limitation, compensatory physiologic mechanisms, psychological impact of the disease, as well as the burden and side effects of the treatments used to treat the PH. It should be noted that to date, while there is an abundance of data from the literature demonstrating the physiologic impact of PH and poor outcomes in patients with PH, there have been no studies specifically evaluating the impact of PH on work ability. 1. Definition of PH a. Pulmonary hypertension (PH) is defined as an abnormal elevation of pulmonary arterial pressure. The hemodynamic definition of PH requires cardiac catheterization demonstrating a mean pulmonary artery pressure (PAP) > 25 mmhg and pulmonary vascular resistance (PVR) >3 Wood units Etiology of PH a. PH can be the result of various disorders of the cardiovascular and/or respiratory systems. The table below shows the current PH classification, grouped by similar clinical symptoms and similar pathology/pathobiology 2.
 is defined as an abnormal elevation of pulmonary arterial pressure, and can result in progressive enlargement and dysfunction of the right ventricle (the right side of the")
2 3. Impact of PH on disability a. Decreased exercise capacity in PH One of the hallmarks of the physical impairment due to PH is reduced exercise capacity with breathlessness, (i.e. dyspnea) with exertion being the most common symptom reported. Patients with PH cannot increase cardiac output sufficiently to meet the demands of the exertion, whether it is the activities of daily living or exercise. Both the inability to increase the blood flow through the lungs due to the diseased lung vessels (which by definition causes the same lack of needed increase in blood flow to the body, i.e. cardiac output) and the impairment in the ability of pulmonary blood flow to perfuse ventilated lung (resulting in poor ventilation/perfusion matching) contribute to the impaired
3 exercise capacity and dyspnea and fatigue experienced by patients with PH. i. Measurement of exercise capacity in PH Decreased exercise capacity can be quantitated using various standardized measures of exercise capacity, including treadmill and cycle testing 3 (measures of exercise tolerance), as well as the commonly used 6 minute walk test 4 (measure of exercise endurance). When measurements of gas exchange are also measured (such as oxygen uptake and carbon dioxide output), more precise physiologic assessments of the cause(s) of the reduced exercise capacity can often be made 3. ii. Degree of impairment in exercise capacity The degree of impairment in exercise capacity has been best quantified using 6 minute walk testing and cardiopulmonary exercise testing (CPET). Studies have shown that these measures are prognostic parameters for survival in PH patients 5 6 and that the degree of their impairment correlates with other clinical measures of PH severity including the modified New York Heart Association (NYHA) functional classification for PH, quality of life, and hemodynamic severity. b. Reduced functional capacity in PH The NYHA functional class (and World Health Organization [WHO] functional class, modified for PH) correlates with hospitalization and survival in patients with PH. As in heart failure associated with other cardiovascular disorders, patients with functional class III and IV are limited to the extent that they must modify their daily activities due to their underlying illness. c. Compensatory mechanisms in PH i. Hemodynamic considerations The degree of elevation in pulmonary artery pressure (PAP) does not correlate with functional PH severity as well as other markers of PH severity 7. Adaptation of the cardiopulmonary system in response to the impairment of pulmonary blood flow is variable, with some patients able to compensate via an increased right ventricular (RV) response (RV hypertrophy with preserved RV systolic function), and others who develop rapid decrements in RV function. Fluid retention and impaired renal handling of sodium directly affect the RV response to PH. Higher right atrial pressure and lower cardiac output, correlate well survival in PH, as these measures evaluate the physiologic effects of the impaired pulmonary circulation. Physical examination may be revealing in PH patients with RV failure, with neck vein distension, enlarged liver (i.e. hepatomegaly, and peripheral swelling (i.e. edema, however many PH patients only manifest symptoms during exercise, when the demand for increased blood pulmonary and
, more precise physiologic assessments of the cause(s) of the reduced exercise capacity can often")
4 systemic blood flow cannot be met due to the diseased blood vessels in the lungs 8. These patients may not manifest the typical findings of RV failure, but exercise capacity may be severely limited. Conversely, patients with overt signs of RV failure may in fact have relatively minor symptoms owing to physiologic adaptations, however these patients should still avoid workday stresses because of their propensity for sudden decompensation, which occurs frequently in the PH population. ii. Neurohormonal considerations A variable neurohormonal response may also play a role in the variable clinical response to PH. Circulating vasoconstrictor (i.e. constricting and narrowing of the blood vessels) and vasodilator (i.e. relaxing and opening of the blood vessels) responses mediate detrimental and adaptive responses, respectively to PH. iii. Metabolic and organ systems considerations Responses to PH including increased oxidative stress and impaired renal perfusion contribute to the above neurohormonal and hemodynamic changes that modulate the clinical presentation of PH. The common use of diuretics used to treat the fluid retention in PH patients also contributes to renal impairment. A particularly common abnormality seen in patients with PH is hypoxemia (i.e. decreased oxygen in the blood supplying the body). Patients with underlying parenchymal lung disease and/or pulmonary venous hypertension due to left sided heart disease may develop hypoxemia. In addition, patients without these conditions can develop hypoxemia. In many patients, shunting of deoxygenated blood (i.e. right to left shunting of blood bypassing the lungs resulting in inadequate oxygen in the blood) results in systemic desaturation, (i.e. low oxygen in the blood going to the body), due to increased right sided pressure that forces blood through a patent foramen ovale (i.e. a small hole in the heart that remains open in ~30 40% of individuals) 9. d. Treatment side effects and burden of treatment i. PH treatments The treatments for PH vary, and include supportive interventions and medications such as continuous oxygen and diuretics (i.e. to decrease swelling from fluid retention). Some PH patients benefit from medications used to improve symptoms and exercise capacity. These medications range from oral (taken one to three times per day) and inhaled treatments (four to 9 times per day) to continuous (24/7) parenteral (subcutaneous or intravenous) treatments.
 and vasodilator (i.")
5 ii. PH treatment side effects Common side effects of PH treatments include, but are not limited to: increased thirst and urination, dry mouth, hypokalemia with muscle cramping, flushing, hypotension (i.e. low blood pressure), dizziness, headache, jaw pain, leg and back pain, diarrhea, and rash. iii. Burden of PH treatment and associated effects Depending on the medications, the burden of PH treatments can include the daily need for preparing PH medications under sterile conditions, carrying ice packs to keep medication in the infusion pump refrigerated, carrying and maintaining two infusion pumps (one pump is needed for backup due to the short half life of the medication, which can be as short as 2 minutes, thereby necessitating the 24/7 treatment), cleaning, protecting and maintaining an indwelling central venous or subcutaneous catheter, and carrying, maintaining and preparing a nebulizer for inhalation 4 9 times daily with inhaled treatment delivery times ranging from 2 15 minutes per treatment. Being off of the 24/7 therapies, even for a few minutes, can be life threatening. The burden of continuous oxygen therapy includes the need for transporting a continuous supply of oxygen (i.e. not infrequently large and heavy tanks) and use of nasal cannula. Additional side effects associated with some PH treatments include pain at the medication injection site (which in itself can be debilitating), frequent catheter infection and sepsis, requiring hospitalization and catheter removal, and coughing after inhalation of PH medications. Replacement of central venous catheters are not without significant risk in part due to limited number of veins that the catheter can be inserted into.

6 Disability criteria and scoring system for patients with pulmonary hypertension (PH) Weighted Criteria Score Syncope 3 WHO Functional Class IV 3 Mean RAP > 14 or SVO2 < 70% 3 Clinical right-sided heart failure 3 WHO Functional Class III (do not count if NYHA IV; see above) 2 Troponin elevation 2 Resting SBP <100 mmhg or 2 Resting HR >100 bpm Pericardial Effusion 2 Mild or greater echo RV enlargement or mild or worse echo RV dysfunction 2 6MWD < 300 m or peak VO2 < 14 ml/kg/min 2 BNP > 180 pg/ml or NT-proBNP > 450 pg/ml 2 Serum sodium <130 meq/l 2 Continuous parenteral PH Therapy 2 Hypoxia (SaO2<92% at rest) requiring supplemental O2 or Hypoxia (SaO2<90% with exertion) requiring supplemental O2 2 WHO Functional Class II (do not count if NYHA III or IV; see above) 1 Pleural Effusion 1 6MWD < 400 m (do not count if <300 m; see above) 1 Peak exercise SBP <120 mmhg 1 Medication side effects preventing work outside of home 1 IF PVR >12 IF PVR >8, 12 IF PVR >3, 8 AND AND AND weighted score > 3 weighted score > 8 weighted score > 12 THEN Disability THEN Disability THEN Disability
 requiring supplemental O2 or Hypoxia (SaO2<90% with exertion) requiring supplemental O2 2 WHO Functional Class II (do not count if NYHA III or IV; see above) 1 Pleural")
7 Tabular Listing of Impairments in pulmonary hypertension (PH) Patients Risk Factor Modifier Rationale Syncope Recurrent Poor survival; predictor of sudden death Right ventricular heart failure Late stage of decompensation; lack of cardiac reserve*** WHO functional class** III, IV Late stage of decompensation; lack Resting systolic blood pressure of cardiac reserve*** <100 mmhg Denotes low cardiac output; late stage of decompensation; lack of cardiac reserve*** Resting heart rate > 90 bpm Late stage of decompensation; lack of cardiac reserve*** CXR Pleural effusions Denotes right ventricular heart failure ; late state of decompensation ; lack of cardiac reserve*** Echocardiography Pericardial effusion not otherwise explained (any size); RV dilation/ dysfunction; decreased right sided clearance with cavitation study Independent predictor of poor survival; late stage of decompensation; lack of cardiac reserve*** 6 minute walk distance*+ <425 meters Significant functional limitation; independent predictor of poor survival CPET+ Peak VO 2 < 18 ml/kg/min; Peak systolic blood pressure during exercise < 130 mm Hg Significant functional limitation; independent predictor of poor survival Platelet count <50,000/μl Late state of decompensation Serum sodium < 135 meq/l Predictor of poor survival with or without right heart failure Total bilirubin 2.5 mg/dl Denotes severe right heart failure Hospitalization for worsening PH Independent predictor of poor survival Uric acid >11 mg/dl Independent predictor of poor survival; marker of severe oxidative stress Renal insufficiency Denotes low cardiac output; Late stage of decompensation; lack of cardiac reserve*** BNP > 180 pg/ml Marker of right ventricular heart failure Troponin Positive Right ventricular ischemia Hemodynamics mrap>14 mmhg CI<2.2L/min/m2; PVR > 12 Wood units; SVO2 < 70% Late stage of decompensation; lack of cardiac reserve***
; RV dilation/ dysfunction; decreased")
8 Disease Severity necessitating Parenteral Therapy Disease Severity necessitating Supplemental Oxygen Therapy for SaO2 < 92% at rest or with exertion Memory Loss/Learning Disabilities Denotes advanced disease and/or inadequate responses to nonparenteral therapies. Burden of medication delivery systems, indwelling catheters is high; increased risk of life threatening bacteremia, sepsis and/or thromboembolic events, e.g. CVA, PE Denotes advanced disease. Burden delivery system is high. Related to inadequate cerebral perfusion, i.e. inadequate cardiac output; increases burden of parenteral and/or inhaled PAH medications Medication side effects Diarrhea, foot pain, back pain Prevents work outside the home Note regarding disability in patients with PH: While FDA approved therapies are indicated for patients with WHO Group 1 PAH, the disability and associated morbidity (and mortality) of PH resulting from any underlying etiology is significant, and is the result of the same cardiovascular consequences (i.e. right ventricular [RV] failure) as PAH. In addition, in order to fully address a disability claim of a patient with congenital heart disease (CHD, discussed separately on 05 April, 2010), cross referencing this document with the CHD guidelines is suggested. *6 MWD is affected by age, gender, and height **WHO class is the functional classification for PH (modification of the New York Heart Association functional classification for PH) + limits to sustain performance on a daily basis as required in order to work ***Lack of cardiac reserve can progress to severe heart failure with not infrequently insignificant stresses (that are tolerated by subjects with adequate cardiopulmonary reserve), e.g. upper respiratory tract infection, bronchitis, clinical pneumonia, flu; anemia; hyperthyroid state. PVR reflects the impact of both the elevated pulmonary artery pressure and the reduced cardiac output upon the cardiovascular system. Abbreviations: PVR = pulmonary vascular resistance; RV = right ventricle; WHO = World Health Organization; 6MWD = 6 minute walk distance; peak VO 2 = peak oxygen uptake during exercise; CPET = cardiopulmonary exercise testing; RAP = right atrial pressure; CI = cardiac index; SVO2

9 mixed venous oxygen saturation; BNP = brain natriuretic peptide; RHC right heart catheterization REFERENCES 1 McLaughlin VV, Archer SL, Badesch DB, et al. American College of Cardiology Foundation Task Force on Expert Consensus Documents; American Heart Association; American College of Chest Physicians; American Thoracic Society, Inc; Pulmonary Hypertension Association. J Am Coll Cardiol 2009;53: Simonneau G, Robbins IM, Beghetti M, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol 2009;54:S Sun XG, Hansen JE, Oudiz RJ, Wasserman K. Exercise pathophysiology in patients with primary pulmonary hypertension. Circulation 2001;104: Guyatt GH, Sullivan MJ, Thompson PJ, et al. The 6 minute walk: a new measure of exercise capacity in patients with chronic heart failure. Can Med Assoc J 1985;132: Sitbon O, Humbert M, Nunes H, et al. Long term intravenous epoprostenol infusion in primary pulmonary hypertension: prognostic factors and survival. J Am Coll Cardiol 2002;40: Wensel R, Opitz CF, Anker SD, et al. Assessment of survival in patients with primary pulmonary hypertension: importance of cardiopulmonary exercise testing. Circulation 2002;106: McLaughlin VV, Shillington A, Rich S. Survival in primary pulmonary hypertension: the impact of epoprostenol therapy. Circulation 2002;106: Rubin LJ, Badesch DB. Evaluation and management of the patient with pulmonary arterial hypertension. Ann Intern Med 2005;143: Sun XG, Hansen JE, Oudiz RJ, Wasserman K. Gas exchange detection of exercise induced right to left shunt in patients with primary pulmonary hypertension. Circulation 2002;105:54 60.

Type II Pulmonary Hypertension: Pulmonary Hypertension due to Left Heart Disease
 Heart Failure Center Hadassah University Hospital Type II Pulmonary Hypertension: Pulmonary Hypertension due to Left Heart Disease Israel Gotsman MD The Heart Failure Center, Heart Institute Hadassah University
Heart Failure Center Hadassah University Hospital Type II Pulmonary Hypertension: Pulmonary Hypertension due to Left Heart Disease Israel Gotsman MD The Heart Failure Center, Heart Institute Hadassah University
Pulmonary Artery Hypertension
 Pulmonary Artery Hypertension Janet M. Pinson, RN, MSN, ACNP Maureen P. Flattery, RN, MS, ANP Virginia Commonwealth University Health System Richmond, VA Pulmonary artery hypertension (PAH) is defined
Pulmonary Artery Hypertension Janet M. Pinson, RN, MSN, ACNP Maureen P. Flattery, RN, MS, ANP Virginia Commonwealth University Health System Richmond, VA Pulmonary artery hypertension (PAH) is defined
PULMONARY HYPERTENSION. Charles A. Thompson, M.D., FACC, FSCAI Cardiovascular Institute of the South Zachary, Louisiana
 PULMONARY HYPERTENSION Charles A. Thompson, M.D., FACC, FSCAI Cardiovascular Institute of the South Zachary, Louisiana What is Pulmonary Hypertension? What is normal? Pulmonary artery systolic pressure
PULMONARY HYPERTENSION Charles A. Thompson, M.D., FACC, FSCAI Cardiovascular Institute of the South Zachary, Louisiana What is Pulmonary Hypertension? What is normal? Pulmonary artery systolic pressure
Riociguat Clinical Trial Program
 Riociguat Clinical Trial Program Riociguat (BAY 63-2521) is an oral agent being investigated as a new approach to treat chronic thromboembolic pulmonary hypertension (CTEPH) and pulmonary arterial hypertension
Riociguat Clinical Trial Program Riociguat (BAY 63-2521) is an oral agent being investigated as a new approach to treat chronic thromboembolic pulmonary hypertension (CTEPH) and pulmonary arterial hypertension
Pulmonary Diseases. Lung Disease: Pathophysiology, Medical and Exercise Programming. Overview of Pathophysiology
 Lung Disease: Pathophysiology, Medical and Exercise Programming Overview of Pathophysiology Ventilatory Impairments Increased airway resistance Reduced compliance Increased work of breathing Ventilatory
Lung Disease: Pathophysiology, Medical and Exercise Programming Overview of Pathophysiology Ventilatory Impairments Increased airway resistance Reduced compliance Increased work of breathing Ventilatory
Pulmonary Arterial Hypertension: Review and Updates. Is it Primary vs Secondary Pulmonary Hypertension? No!! Dated Nomenclature. Veronica Franco, MD
 Pulmonary Arterial Hypertension: Review and Updates Veronica Franco, MD Section of Pulmonary Hypertension Section of Heart Failure and Transplantation Ohio State University Is it Primary vs Secondary Pulmonary
Pulmonary Arterial Hypertension: Review and Updates Veronica Franco, MD Section of Pulmonary Hypertension Section of Heart Failure and Transplantation Ohio State University Is it Primary vs Secondary Pulmonary
Pulmonary Arterial Hypertension. Matt Hegewald, MD FCCP St Charles Medical Center Intermountain Medical Center University of Utah
 Pulmonary Arterial Hypertension Matt Hegewald, MD FCCP St Charles Medical Center Intermountain Medical Center University of Utah Intermountain Pulmonary Arterial Hypertension Program Outline Causes of
Pulmonary Arterial Hypertension Matt Hegewald, MD FCCP St Charles Medical Center Intermountain Medical Center University of Utah Intermountain Pulmonary Arterial Hypertension Program Outline Causes of
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Health Technology Appraisal. Drugs for the treatment of pulmonary arterial hypertension
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Drugs for the treatment of Remit / Appraisal objective: Final scope To appraise the clinical and cost effectiveness of
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Drugs for the treatment of Remit / Appraisal objective: Final scope To appraise the clinical and cost effectiveness of
James F. Kravec, M.D., F.A.C.P
 James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy
 The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
Corporate Medical Policy
 Corporate Medical Policy Pulmonary Hypertension, Drug Management File Name: Origination: Last CAP Review: Next CAP Review: Last Review: pulmonary_hypertension_drug_management 06/1998 3/2015 3/2016 3/2015
Corporate Medical Policy Pulmonary Hypertension, Drug Management File Name: Origination: Last CAP Review: Next CAP Review: Last Review: pulmonary_hypertension_drug_management 06/1998 3/2015 3/2016 3/2015
Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations.
 INTRODUCTION Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations. Although decrease in cardiovascular mortality still major cause of morbidity & burden of disease.
INTRODUCTION Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations. Although decrease in cardiovascular mortality still major cause of morbidity & burden of disease.
Pulmonary Arterial Hypertension: Assessment of disease s severity
 Pulmonary Arterial Hypertension: Assessment of disease s severity Carmine Dario Vizza Dept. Cardiovascular and Respiratory Diseases La Sapienza University of Rome e-mail : [email protected] Pulmonary
Pulmonary Arterial Hypertension: Assessment of disease s severity Carmine Dario Vizza Dept. Cardiovascular and Respiratory Diseases La Sapienza University of Rome e-mail : [email protected] Pulmonary
Introduction to Cardiopulmonary Exercise Testing
 Introduction to Cardiopulmonary Exercise Testing 2 nd Edition Andrew M. Luks, MD Robb Glenny, MD H. Thomas Robertson, MD Division of Pulmonary and Critical Care Medicine University of Washington Section
Introduction to Cardiopulmonary Exercise Testing 2 nd Edition Andrew M. Luks, MD Robb Glenny, MD H. Thomas Robertson, MD Division of Pulmonary and Critical Care Medicine University of Washington Section
PAH has an incidence
 Pulmonary Arterial Hypertension: A Serious Problem Pulmonary arterial hypertension (PAH) is a serious disease with significant morbidity and mortality and no cure. In this article, Dr. Porhownik and Dr.
Pulmonary Arterial Hypertension: A Serious Problem Pulmonary arterial hypertension (PAH) is a serious disease with significant morbidity and mortality and no cure. In this article, Dr. Porhownik and Dr.
Heart Failure EXERCISES. Ⅰ. True or false questions (mark for true question, mark for false question. If it is false, correct it.
 Heart Failure EXERCISES Ⅰ. True or false questions (mark for true question, mark for false question. If it is false, correct it. ) 1. Heart rate increase is a kind of economic compensation, which should
Heart Failure EXERCISES Ⅰ. True or false questions (mark for true question, mark for false question. If it is false, correct it. ) 1. Heart rate increase is a kind of economic compensation, which should
Pulmonary Arterial Hypertension. Mark Rumbak, MD Professor of Medicine Morsani College of Medicine University of South Florida
 Pulmonary Arterial Hypertension Mark Rumbak, MD Professor of Medicine Morsani College of Medicine University of South Florida PAH Disease State Module Outline Background and definition Clinical classification
Pulmonary Arterial Hypertension Mark Rumbak, MD Professor of Medicine Morsani College of Medicine University of South Florida PAH Disease State Module Outline Background and definition Clinical classification
Understanding Hypoventilation and Its Treatment by Susan Agrawal
 www.complexchild.com Understanding Hypoventilation and Its Treatment by Susan Agrawal Most of us have a general understanding of what the term hyperventilation means, since hyperventilation, also called
www.complexchild.com Understanding Hypoventilation and Its Treatment by Susan Agrawal Most of us have a general understanding of what the term hyperventilation means, since hyperventilation, also called
Medical Direction and Practices Board WHITE PAPER
 Medical Direction and Practices Board WHITE PAPER Use of Pressors in Pre-Hospital Medicine: Proper Indication and State of the Science Regarding Proper Choice of Pressor BACKGROUND Shock is caused by a
Medical Direction and Practices Board WHITE PAPER Use of Pressors in Pre-Hospital Medicine: Proper Indication and State of the Science Regarding Proper Choice of Pressor BACKGROUND Shock is caused by a
STAGES OF SHOCK. IRREVERSIBLE SHOCK Heart deteriorates until it can no longer pump and death occurs.
 STAGES OF SHOCK SHOCK : A profound disturbance of circulation and metabolism, which leads to inadequate perfusion of all organs which are needed to maintain life. COMPENSATED NONPROGRESSIVE SHOCK 30 sec
STAGES OF SHOCK SHOCK : A profound disturbance of circulation and metabolism, which leads to inadequate perfusion of all organs which are needed to maintain life. COMPENSATED NONPROGRESSIVE SHOCK 30 sec
Liver Function Essay
 Liver Function Essay Name: Quindoline Ntui Date: April 20, 2009 Professor: Dr. Danil Hammoudi Class: Anatomy and Physiology 2 Liver function The human body consist of many highly organize part working
Liver Function Essay Name: Quindoline Ntui Date: April 20, 2009 Professor: Dr. Danil Hammoudi Class: Anatomy and Physiology 2 Liver function The human body consist of many highly organize part working
Cardiopulmonary Exercise Stress Test (CPET) Archived Medical Policy
 Archived Medical Policy") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Resuscitation in congenital heart disease. Peter C. Laussen MBBS FCICM Department Critical Care Medicine Hospital for Sick Children Toronto
 Resuscitation in congenital heart disease Peter C. Laussen MBBS FCICM Department Critical Care Medicine Hospital for Sick Children Toronto Evolution of Congenital Heart Disease Extraordinary success: Overall
Resuscitation in congenital heart disease Peter C. Laussen MBBS FCICM Department Critical Care Medicine Hospital for Sick Children Toronto Evolution of Congenital Heart Disease Extraordinary success: Overall
Quiz 5 Heart Failure scores (n=163)
") Quiz 5 Heart Failure summary statistics The correct answers to questions are indicated by *. Students were awarded 2 points for question #3 for either selecting spironolactone or eplerenone. However, the
Quiz 5 Heart Failure summary statistics The correct answers to questions are indicated by *. Students were awarded 2 points for question #3 for either selecting spironolactone or eplerenone. However, the
INTRODUCTION TO EECP THERAPY
 INTRODUCTION TO EECP THERAPY is an FDA cleared, Medicare approved, non-invasive medical therapy for the treatment of stable and unstable angina, congestive heart failure, acute myocardial infarction, and
INTRODUCTION TO EECP THERAPY is an FDA cleared, Medicare approved, non-invasive medical therapy for the treatment of stable and unstable angina, congestive heart failure, acute myocardial infarction, and
TACO vs. TRALI: Recognition, Differentiation, and Investigation of Pulmonary Transfusion Reactions
 TACO vs. TRALI: Recognition, Differentiation, and Investigation of Pulmonary Transfusion Reactions Shealynn Harris, M.D. Assistant Medical Director American Red Cross Blood Services Southern Region Case
TACO vs. TRALI: Recognition, Differentiation, and Investigation of Pulmonary Transfusion Reactions Shealynn Harris, M.D. Assistant Medical Director American Red Cross Blood Services Southern Region Case
Inpatient Heart Failure Management: Risks & Benefits
 Inpatient Heart Failure Management: Risks & Benefits Dr. Kenneth L. Baughman Professor of Medicine Harvard Medical School Director, Advanced Heart Disease Section Brigham & Women's Hospital Harvard Medical
Inpatient Heart Failure Management: Risks & Benefits Dr. Kenneth L. Baughman Professor of Medicine Harvard Medical School Director, Advanced Heart Disease Section Brigham & Women's Hospital Harvard Medical
Acute heart failure may be de novo or it may be a decompensation of chronic heart failure.
 Management of Acute Left Ventricular Failure Acute left ventricular failure presents as pulmonary oedema due to increased pressure in the pulmonary capillaries. It is important to realise though that left
Management of Acute Left Ventricular Failure Acute left ventricular failure presents as pulmonary oedema due to increased pressure in the pulmonary capillaries. It is important to realise though that left
Universitätsklinik für Kardiologie. Test. Thomas M. Suter Akute Herzinsuffizienz Diagnostik und Therapie [email protected] 1
 Test Thomas M. Suter Akute Herzinsuffizienz Diagnostik und Therapie [email protected] 1 Heart Failure - Definition European Heart Journal (2008) 29, 2388 2442 Akute Herzinsuffizienz Diagnostik und
Test Thomas M. Suter Akute Herzinsuffizienz Diagnostik und Therapie [email protected] 1 Heart Failure - Definition European Heart Journal (2008) 29, 2388 2442 Akute Herzinsuffizienz Diagnostik und
CARDIOVASCULAR DYSFUNCTION IN LIVER CIRRHOSIS
 LUCIAN BLAGA UNIVERSITY OF SIBIU VICTOR PAPILIAN FACULTY OF MEDICINE CARDIOVASCULAR DYSFUNCTION IN LIVER CIRRHOSIS Ph.D. THESIS SUMMARY COORDINATOR: PROF.DR. MANIŢIU IOAN Ph.D. STUDENT: LORENA MĂRIEŞ SIBIU
LUCIAN BLAGA UNIVERSITY OF SIBIU VICTOR PAPILIAN FACULTY OF MEDICINE CARDIOVASCULAR DYSFUNCTION IN LIVER CIRRHOSIS Ph.D. THESIS SUMMARY COORDINATOR: PROF.DR. MANIŢIU IOAN Ph.D. STUDENT: LORENA MĂRIEŞ SIBIU
Acknowledgements. PAH in Children: Natural History. The Sildenafil Saga
 The Sildenafil Saga David L. Wessel, MD Executive Vice President Chief Medical Officer Ikaria Distinguished Professor of Critical Care Children s National Medical Center Washington, DC, USA Acknowledgements
The Sildenafil Saga David L. Wessel, MD Executive Vice President Chief Medical Officer Ikaria Distinguished Professor of Critical Care Children s National Medical Center Washington, DC, USA Acknowledgements
ECG may be indicated for patients with cardiovascular risk factors
 eappendix A. Summary for Preoperative ECG American College of Cardiology/ American Heart Association, 2007 A1 2002 A2 European Society of Cardiology and European Society of Anaesthesiology, 2009 A3 Improvement,
eappendix A. Summary for Preoperative ECG American College of Cardiology/ American Heart Association, 2007 A1 2002 A2 European Society of Cardiology and European Society of Anaesthesiology, 2009 A3 Improvement,
Blood Pressure. Blood Pressure (mm Hg) pressure exerted by blood against arterial walls. Blood Pressure. Blood Pressure
 pressure exerted by blood against arterial walls. Blood Pressure. Blood Pressure") Blood Pressure Blood Pressure (mm Hg) pressure exerted by blood against arterial walls Systolic pressure exerted on arteries during systole Diastolic pressure in arteries during diastole 120/80 Borderline
Blood Pressure Blood Pressure (mm Hg) pressure exerted by blood against arterial walls Systolic pressure exerted on arteries during systole Diastolic pressure in arteries during diastole 120/80 Borderline
Treatment of cardiogenic shock
 ACUTE HEART FAILURE AND COMORBIDITY IN THE ELDERLY Treatment of cardiogenic shock Christian J. Wiedermann, M.D., F.A.C.P. Associate Professor of Internal Medicine, Medical University of Innsbruck, Austria
ACUTE HEART FAILURE AND COMORBIDITY IN THE ELDERLY Treatment of cardiogenic shock Christian J. Wiedermann, M.D., F.A.C.P. Associate Professor of Internal Medicine, Medical University of Innsbruck, Austria
Ischemia and Infarction
 Harvard-MIT Division of Health Sciences and Technology HST.035: Principle and Practice of Human Pathology Dr. Badizadegan Ischemia and Infarction HST.035 Spring 2003 In the US: ~50% of deaths are due to
Harvard-MIT Division of Health Sciences and Technology HST.035: Principle and Practice of Human Pathology Dr. Badizadegan Ischemia and Infarction HST.035 Spring 2003 In the US: ~50% of deaths are due to
Oxygen Therapy. Oxygen therapy quick guide V3 July 2012.
 PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
Exchange solutes and water with cells of the body
 Chapter 8 Heart and Blood Vessels Three Types of Blood Vessels Transport Blood Arteries Carry blood away from the heart Transport blood under high pressure Capillaries Exchange solutes and water with cells
Chapter 8 Heart and Blood Vessels Three Types of Blood Vessels Transport Blood Arteries Carry blood away from the heart Transport blood under high pressure Capillaries Exchange solutes and water with cells
Tired, Aching Legs? Swollen Ankles? Varicose Veins? An informative guide for patients
 Tired, Aching Legs? Swollen Ankles? Varicose Veins? An informative guide for patients Are You at Risk? Leg problems are widespread throughout the world, but what most people don t know is that approximately
Tired, Aching Legs? Swollen Ankles? Varicose Veins? An informative guide for patients Are You at Risk? Leg problems are widespread throughout the world, but what most people don t know is that approximately
Interpretation of Laboratory Values
 Interpretation of Laboratory Values Konrad J. Dias PT, DPT, CCS Overview Electrolyte imbalances Renal Function Tests Complete Blood Count Coagulation Profile Fluid imbalance Sodium Electrolyte Imbalances
Interpretation of Laboratory Values Konrad J. Dias PT, DPT, CCS Overview Electrolyte imbalances Renal Function Tests Complete Blood Count Coagulation Profile Fluid imbalance Sodium Electrolyte Imbalances
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL
 Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
How To Understand What You Know
 Heart Disorders Glossary ABG (Arterial Blood Gas) Test: A test that measures how much oxygen and carbon dioxide are in the blood. Anemia: A condition in which there are low levels of red blood cells in
Heart Disorders Glossary ABG (Arterial Blood Gas) Test: A test that measures how much oxygen and carbon dioxide are in the blood. Anemia: A condition in which there are low levels of red blood cells in
The Global Alliance against Chronic Respiratory Diseases
 The Global Alliance against Chronic Respiratory Diseases Pulmonary hypertension Dr Marc Humbert What is the burden of pulmonary hypertension? The true burden of pulmonary hypertension is currently unknown
The Global Alliance against Chronic Respiratory Diseases Pulmonary hypertension Dr Marc Humbert What is the burden of pulmonary hypertension? The true burden of pulmonary hypertension is currently unknown
Low-gradient severe aortic stenosis with normal LVEF: A disturbing clinical entity
 Low-gradient severe aortic stenosis with normal LVEF: A disturbing clinical entity Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Disclosures : None 77-year-old woman, mild dyspnea
Low-gradient severe aortic stenosis with normal LVEF: A disturbing clinical entity Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Disclosures : None 77-year-old woman, mild dyspnea
Inotropes/Vasoactive Agents Hina N. Patel, Pharm.D., BCPS Cathy Lawson, Pharm.D., BCPS
 Inotropes/Vasoactive Agents Hina N. Patel, Pharm.D., BCPS Cathy Lawson, Pharm.D., BCPS 1. Definition -an agent that affects the contractility of the heart -may be positive (increases contractility) or
Inotropes/Vasoactive Agents Hina N. Patel, Pharm.D., BCPS Cathy Lawson, Pharm.D., BCPS 1. Definition -an agent that affects the contractility of the heart -may be positive (increases contractility) or
Milwaukee School of Engineering [email protected]. Case Study: Factors that Affect Blood Pressure Instructor Version
 Case Study: Factors that Affect Blood Pressure Instructor Version Goal This activity (case study and its associated questions) is designed to be a student-centered learning activity relating to the factors
Case Study: Factors that Affect Blood Pressure Instructor Version Goal This activity (case study and its associated questions) is designed to be a student-centered learning activity relating to the factors
1. Phosphodiesterase Type 5 Enzyme Inhibitors: Sildenafil (Revatio), Tadalafil (Adcirca)
, Tadalafil (Adcirca)") This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutic
This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutic
FVMA 2015: Diagnosis and Management of Pericardial Disease PERICARDIAL EFFUSION Pathophysiology of Cardiac Tamponade
 FVMA 2015: Diagnosis and Management of Pericardial Disease Jonathan A. Abbott, DVM, Dipl. ACVIM (Cardiology) VA-MD College of Veterinary Medicine Virginia Tech, Blacksburg, Virginia Pericardial disease
FVMA 2015: Diagnosis and Management of Pericardial Disease Jonathan A. Abbott, DVM, Dipl. ACVIM (Cardiology) VA-MD College of Veterinary Medicine Virginia Tech, Blacksburg, Virginia Pericardial disease
Recommendations: Other Supportive Therapy of Severe Sepsis*
 Recommendations: Other Supportive Therapy of Severe Sepsis* K. Blood Product Administration 1. Once tissue hypoperfusion has resolved and in the absence of extenuating circumstances, such as myocardial
Recommendations: Other Supportive Therapy of Severe Sepsis* K. Blood Product Administration 1. Once tissue hypoperfusion has resolved and in the absence of extenuating circumstances, such as myocardial
Pharmacy Medical Necessity Guidelines: Pulmonary Hypertension Medications
 Pharmacy Medical Necessity Guidelines: Pulmonary Hypertension Medications Effective: January 1, 2016 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review
Pharmacy Medical Necessity Guidelines: Pulmonary Hypertension Medications Effective: January 1, 2016 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review
STUDY GUIDE 1.1: NURSING DIAGNOSTIC STATEMENTS AND COMPREHENSIVE PLANS OF CARE
 STUDY GUIDE 1.1: NURSING DIAGNOSTIC STATEMENTS AND COMPREHENSIVE PLANS OF CARE WHAT IS A NURSING DIAGNOSIS? A nursing diagnosis is a clinical judgment about individual, family, or community responses to
STUDY GUIDE 1.1: NURSING DIAGNOSTIC STATEMENTS AND COMPREHENSIVE PLANS OF CARE WHAT IS A NURSING DIAGNOSIS? A nursing diagnosis is a clinical judgment about individual, family, or community responses to
Oxygen - update April 2009 OXG
 PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
CONGESTIVE HEART FAILURE PATIENT TEACHING
 CONGESTIVE HEART FAILURE PATIENT TEACHING What is Heart Failure? Congestive Heart Failure occurs when the heart loses its ability to pump enough blood to meet the body s needs. Because the heart is not
CONGESTIVE HEART FAILURE PATIENT TEACHING What is Heart Failure? Congestive Heart Failure occurs when the heart loses its ability to pump enough blood to meet the body s needs. Because the heart is not
Children's Medical Services (CMS) Regional Perinatal Intensive Care Center (RPICC) Neonatal Extracorporeal Life Support (ECLS) Centers Questionnaire
 Regional Perinatal Intensive Care Center (RPICC) Neonatal Extracorporeal Life Support (ECLS) Centers Questionnaire") Children's Medical Services (CMS) Regional Perinatal Intensive Care Center (RPICC) Neonatal Extracorporeal Life Support (ECLS) Centers Questionnaire Date: RPICC Facility: CMS use only Include the following
Children's Medical Services (CMS) Regional Perinatal Intensive Care Center (RPICC) Neonatal Extracorporeal Life Support (ECLS) Centers Questionnaire Date: RPICC Facility: CMS use only Include the following
Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University
 Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University Objectives Define exercise associated collapse (EAC) and exercise-associated postural hypotension
Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University Objectives Define exercise associated collapse (EAC) and exercise-associated postural hypotension
CorCap Cardiac Support Device Patient Information Booklet
 What is Heart Failure? CorCap Cardiac Support Device Patient Information Booklet Heart failure is a condition in which the heart is unable to pump enough blood to meet the needs of the body. To compensate
What is Heart Failure? CorCap Cardiac Support Device Patient Information Booklet Heart failure is a condition in which the heart is unable to pump enough blood to meet the needs of the body. To compensate
Heart Diseases and their Complications
 Heart Diseases and their Complications Health Promotion and Education Program Rev. 2014 2014, MMM Healthcare, Inc. - PMC Medicare Choice, Inc. Reproduction of this material is prohibited. MP-HEP-PPT-252-01-021914-E
Heart Diseases and their Complications Health Promotion and Education Program Rev. 2014 2014, MMM Healthcare, Inc. - PMC Medicare Choice, Inc. Reproduction of this material is prohibited. MP-HEP-PPT-252-01-021914-E
Arterial Blood Gas Case Questions and Answers
 Arterial Blood Gas Case Questions and Answers In the space that follows you will find a series of cases that include arterial blood gases. Each case is then followed by an explanation of the acid-base
Arterial Blood Gas Case Questions and Answers In the space that follows you will find a series of cases that include arterial blood gases. Each case is then followed by an explanation of the acid-base
Common types of congenital heart defects
 Common types of congenital heart defects Congenital heart defects are abnormalities that develop before birth. They can occur in the heart's chambers, valves or blood vessels. A baby may be born with only
Common types of congenital heart defects Congenital heart defects are abnormalities that develop before birth. They can occur in the heart's chambers, valves or blood vessels. A baby may be born with only
Traumatic Cardiac Tamponade. Shane KF Seal 19 November 2003 POS
 Traumatic Cardiac Tamponade Shane KF Seal 19 November 2003 POS Objectives Definition Pathophysiology Diagnosis Treatment Cardiac Tamponade The decompensated phase of cardiac compression resulting from
Traumatic Cardiac Tamponade Shane KF Seal 19 November 2003 POS Objectives Definition Pathophysiology Diagnosis Treatment Cardiac Tamponade The decompensated phase of cardiac compression resulting from
Chapter 16. Learning Objectives. Learning Objectives 9/11/2012. Shock. Explain difference between compensated and uncompensated shock
 Chapter 16 Shock Learning Objectives Explain difference between compensated and uncompensated shock Differentiate among 5 causes and types of shock: Hypovolemic Cardiogenic Neurogenic Septic Anaphylactic
Chapter 16 Shock Learning Objectives Explain difference between compensated and uncompensated shock Differentiate among 5 causes and types of shock: Hypovolemic Cardiogenic Neurogenic Septic Anaphylactic
Heart Failure: Diagnosis and Treatment
 Heart Failure: Diagnosis and Treatment Approximately 5 million people about 2 percent of the U.S. population are affected by heart failure. Diabetes affects 20.8 million Americans and 65 million Americans
Heart Failure: Diagnosis and Treatment Approximately 5 million people about 2 percent of the U.S. population are affected by heart failure. Diabetes affects 20.8 million Americans and 65 million Americans
Oxygenation. Chapter 21. Anatomy and Physiology of Breathing. Anatomy and Physiology of Breathing*
 Oxygenation Chapter 21 Anatomy and Physiology of Breathing Inspiration ~ breathing in Expiration ~ breathing out Ventilation ~ Movement of air in & out of the lungs Respiration ~ exchange of O2 & carbon
Oxygenation Chapter 21 Anatomy and Physiology of Breathing Inspiration ~ breathing in Expiration ~ breathing out Ventilation ~ Movement of air in & out of the lungs Respiration ~ exchange of O2 & carbon
Section 8: Clinical Exercise Testing. a maximal GXT?
 Section 8: Clinical Exercise Testing Maximal GXT ACSM Guidelines: Chapter 5 ACSM Manual: Chapter 8 HPHE 4450 Dr. Cheatham Outline What is the purpose of a maximal GXT? Who should have a maximal GXT (and
Section 8: Clinical Exercise Testing Maximal GXT ACSM Guidelines: Chapter 5 ACSM Manual: Chapter 8 HPHE 4450 Dr. Cheatham Outline What is the purpose of a maximal GXT? Who should have a maximal GXT (and
CONTENTS. Note to the Reader 00. Acknowledgments 00. About the Author 00. Preface 00. Introduction 00
 Natural Therapies for Emphysema By Robert J. Green Jr., N.D. CONTENTS Note to the Reader 00 Acknowledgments 00 About the Author 00 Preface 00 Introduction 00 1 Essential Respiratory Anatomy and Physiology
Natural Therapies for Emphysema By Robert J. Green Jr., N.D. CONTENTS Note to the Reader 00 Acknowledgments 00 About the Author 00 Preface 00 Introduction 00 1 Essential Respiratory Anatomy and Physiology
PERIPHERAL STEM CELL TRANSPLANT INTRODUCTION
 PERIPHERAL STEM CELL TRANSPLANT INTRODUCTION This booklet was designed to help you and the important people in your life understand the treatment of high dose chemotherapy with stem cell support: a procedure
PERIPHERAL STEM CELL TRANSPLANT INTRODUCTION This booklet was designed to help you and the important people in your life understand the treatment of high dose chemotherapy with stem cell support: a procedure
She was 39 years old, gravida 4, para 2. She had an Idiopathic Pulmonary. Arterial Hypertension (PAH) revealed during pregnancy by a New York Heart
 revealed during pregnancy by a New York Heart") Case #1 (year 1992): She was 39 years old, gravida 4, para 2. She had an Idiopathic Pulmonary Arterial Hypertension (PAH) revealed during pregnancy by a New York Heart Association (NYHA) functional class
Case #1 (year 1992): She was 39 years old, gravida 4, para 2. She had an Idiopathic Pulmonary Arterial Hypertension (PAH) revealed during pregnancy by a New York Heart Association (NYHA) functional class
Management of the Patient with Aortic Stenosis undergoing Non-cardiac Surgery
 Management of the Patient with Aortic Stenosis undergoing Non-cardiac Surgery Srinivasan Rajagopal M.D. Assistant Professor Division of Cardiothoracic Anesthesia Objectives Describe the pathophysiology
Management of the Patient with Aortic Stenosis undergoing Non-cardiac Surgery Srinivasan Rajagopal M.D. Assistant Professor Division of Cardiothoracic Anesthesia Objectives Describe the pathophysiology
Update on Small Animal Cardiopulmonary Resuscitation (CPR)- is anything new?
- is anything new?") Update on Small Animal Cardiopulmonary Resuscitation (CPR)- is anything new? DVM, DACVA Objective: Update on the new Small animal guidelines for CPR and a discussion of the 2012 Reassessment Campaign on
Update on Small Animal Cardiopulmonary Resuscitation (CPR)- is anything new? DVM, DACVA Objective: Update on the new Small animal guidelines for CPR and a discussion of the 2012 Reassessment Campaign on
Objectives. The ECG in Pulmonary and Congenital Heart Disease. Lead II P-Wave Amplitude during COPD Exacerbation and after Treatment (50 pts.
 The ECG in Pulmonary and Congenital Heart Disease Gabriel Gregoratos, MD Objectives Review the pathophysiology and ECG signs of pulmonary dysfunction Review the ECG findings in patients with: COPD (chronic
The ECG in Pulmonary and Congenital Heart Disease Gabriel Gregoratos, MD Objectives Review the pathophysiology and ECG signs of pulmonary dysfunction Review the ECG findings in patients with: COPD (chronic
Safe Zone: CV PIP < 26; HFOV: MAP < 16; HFJV: MAP < 16 Dopamine infusion up to 20 mcg/kg/min Epinephrine infusion up to 0.1 mcg /kg/min.
 Congenital Diaphragmatic Hernia: Management Guidelines 5-2006 Issued By: Division of Neonatology Reviewed: Effective Date: Categories: Chronicity Document Congenital Diaphragmatic Hernia: Management Guidelines
Congenital Diaphragmatic Hernia: Management Guidelines 5-2006 Issued By: Division of Neonatology Reviewed: Effective Date: Categories: Chronicity Document Congenital Diaphragmatic Hernia: Management Guidelines
Overview. Geriatric Overview. Chapter 26. Geriatrics 9/11/2012
 Chapter 26 Geriatrics Slide 1 Overview Trauma Common Medical Emergencies Special Considerations in the Elderly Medication Considerations Abuse and Neglect Expanding the Role of EMS Slide 2 Geriatric Overview
Chapter 26 Geriatrics Slide 1 Overview Trauma Common Medical Emergencies Special Considerations in the Elderly Medication Considerations Abuse and Neglect Expanding the Role of EMS Slide 2 Geriatric Overview
ACLS PHARMACOLOGY 2011 Guidelines
 ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
Guidelines for diagnosis and management of acute pulmonary embolism
 Guidelines for diagnosis and management of acute pulmonary embolism By Dr. Ahmed Zaghloul M.D. Anesthesia & Critical Care 2014 Predisposing factors for VTE Predisposing factor Strong predisposing factors
Guidelines for diagnosis and management of acute pulmonary embolism By Dr. Ahmed Zaghloul M.D. Anesthesia & Critical Care 2014 Predisposing factors for VTE Predisposing factor Strong predisposing factors
The State of the Liver in the Adult Patient after Fontan Palliation
 The State of the Liver in the Adult Patient after Fontan Palliation Fred Wu, M.D. Boston Adult Congenital Heart Service Boston Children s Hospital/Brigham & Women s Hospital 7 th National Adult Congenital
The State of the Liver in the Adult Patient after Fontan Palliation Fred Wu, M.D. Boston Adult Congenital Heart Service Boston Children s Hospital/Brigham & Women s Hospital 7 th National Adult Congenital
Ventilation Perfusion Relationships
 Ventilation Perfusion Relationships VENTILATION PERFUSION RATIO Ideally, each alveolus in the lungs would receive the same amount of ventilation and pulmonary capillary blood flow (perfusion). In reality,
Ventilation Perfusion Relationships VENTILATION PERFUSION RATIO Ideally, each alveolus in the lungs would receive the same amount of ventilation and pulmonary capillary blood flow (perfusion). In reality,
PULMONARY ARTERIAL HYPERTENSION AGENTS
 Approvable Criteria: PULMONARY ARTERIAL HYPERTENSION AGENTS Brand Name Generic Name Length of Authorization Revatio Sildenafil citrate Calendar Year Adcirca Tadalafil Calendar Year Letairis Ambrisentan
Approvable Criteria: PULMONARY ARTERIAL HYPERTENSION AGENTS Brand Name Generic Name Length of Authorization Revatio Sildenafil citrate Calendar Year Adcirca Tadalafil Calendar Year Letairis Ambrisentan
Sepsis: Identification and Treatment
 Sepsis: Identification and Treatment Daniel Z. Uslan, MD Associate Clinical Professor Division of Infectious Diseases Medical Director, UCLA Sepsis Task Force Severe Sepsis: A Significant Healthcare Challenge
Sepsis: Identification and Treatment Daniel Z. Uslan, MD Associate Clinical Professor Division of Infectious Diseases Medical Director, UCLA Sepsis Task Force Severe Sepsis: A Significant Healthcare Challenge
The new Heart Failure pathway
 The new Heart Failure pathway An integrated and seamless Strategy Dr Sunil Balani Definition of Heart Failure The inability of the heart to pump blood at a rate commensurate with the requirements of metabolising
The new Heart Failure pathway An integrated and seamless Strategy Dr Sunil Balani Definition of Heart Failure The inability of the heart to pump blood at a rate commensurate with the requirements of metabolising
Adult Congenital Heart Disease and Pulmonary Arterial Hypertension. Patient Information
 Adult Congenital Heart Disease and Pulmonary Arterial Hypertension Patient Information WHAT IS CONGENITAL HEART DISEASE? Congenital heart disease (CHD) refers to a defect of the heart or major blood vessels
Adult Congenital Heart Disease and Pulmonary Arterial Hypertension Patient Information WHAT IS CONGENITAL HEART DISEASE? Congenital heart disease (CHD) refers to a defect of the heart or major blood vessels
ACID- BASE and ELECTROLYTE BALANCE. MGHS School of EMT-Paramedic Program 2011
 ACID- BASE and ELECTROLYTE BALANCE MGHS School of EMT-Paramedic Program 2011 ACID- BASE BALANCE Ions balance themselves like a see-saw. Solutions turn into acids when concentration of hydrogen ions rises
ACID- BASE and ELECTROLYTE BALANCE MGHS School of EMT-Paramedic Program 2011 ACID- BASE BALANCE Ions balance themselves like a see-saw. Solutions turn into acids when concentration of hydrogen ions rises
V: Infusion Therapy. College of Licensed Practical Nurses of Alberta, Competency Profile for LPNs, 3rd Ed. 181
 V: Infusion Therapy College of Licensed Practical Nurses of Alberta, Competency Profile for LPNs, 3rd Ed. 181 Competency: V-1 Principles of V-1-1 V-1-2 V-1-3 V-1-4 V-1-5 Demonstrate knowledge and ability
V: Infusion Therapy College of Licensed Practical Nurses of Alberta, Competency Profile for LPNs, 3rd Ed. 181 Competency: V-1 Principles of V-1-1 V-1-2 V-1-3 V-1-4 V-1-5 Demonstrate knowledge and ability
DISCLOSURES RISK ASSESSMENT. Stroke and Heart Disease -Is there a Link Beyond Risk Factors? Daniel Lackland, MD
 STROKE AND HEART DISEASE IS THERE A LINK BEYOND RISK FACTORS? D AN IE L T. L AC K L AN D DISCLOSURES Member of NHLBI Risk Assessment Workgroup RISK ASSESSMENT Count major risk factors For patients with
STROKE AND HEART DISEASE IS THERE A LINK BEYOND RISK FACTORS? D AN IE L T. L AC K L AN D DISCLOSURES Member of NHLBI Risk Assessment Workgroup RISK ASSESSMENT Count major risk factors For patients with
Tired, Aching Legs? Swollen Ankles? Varicose Veins?
 Tired, Aching Legs? Swollen Ankles? Varicose Veins? Healthy Legs 2006 http://healthylegs.com Page 1 Venous disorders are widespread Leg problems are widespread throughout the world, but what most people
Tired, Aching Legs? Swollen Ankles? Varicose Veins? Healthy Legs 2006 http://healthylegs.com Page 1 Venous disorders are widespread Leg problems are widespread throughout the world, but what most people
Vtial sign #1: PULSE. Vital Signs: Assessment and Interpretation. Factors that influence pulse rate: Importance of Vital Signs
 Vital Signs: Assessment and Interpretation Elma I. LeDoux, MD, FACP, FACC Associate Professor of Medicine Vtial sign #1: PULSE Reflects heart rate (resting 60-90/min) Should be strong and regular Use 2
Vital Signs: Assessment and Interpretation Elma I. LeDoux, MD, FACP, FACC Associate Professor of Medicine Vtial sign #1: PULSE Reflects heart rate (resting 60-90/min) Should be strong and regular Use 2