Pulmonary Arterial Hypertension. Matt Hegewald, MD FCCP St Charles Medical Center Intermountain Medical Center University of Utah
|
|
|
- Leonard White
- 8 years ago
- Views:
Transcription

1 Pulmonary Arterial Hypertension Matt Hegewald, MD FCCP St Charles Medical Center Intermountain Medical Center University of Utah Intermountain Pulmonary Arterial Hypertension Program

2 Outline Causes of elevated pulmonary artery (PA) pressures Diagnosis of pulmonary hypertension (PH) Classifications of PH Treatment of PAH Meds Rehab

3 Elevated Pulmonary Artery Pressures Pulmonary hypertension (PH) Mean pulmonary artery pressure 25 mmhg

4 Causes of Elevated PA Pressures Ohm s Law: PAP LAP = PVR x CO or PAP = PVR x CO + LAP Pulmonary vascular disease High Cardiac Output Left-sided heart disease

5 Pulmonary Arterial Hypertension (PAH) Right heart catheterization VC RA RV PA PC PV LA LV Aorta Mean pulmonary artery Pressure 25 mmhg Pulmonary capillary Wedge pressure 15 mmhg

6 Pulmonary Arterial Hypertension Pulmonary hypertension (PH) is an elevation of mean pulmonary artery pressure 25 mmhg on right heart catheterization Pulmonary arterial hypertension (group 1 PH) requires that the Mean pulmonary artery pressure 25 mmhg PCWP is < 15 mmhg Pulmonary vascular resistance is > 3 WU

7 PAH Background Rare disease (orphan designation) of the pulmonary microvasculature affecting 15 to 50 people per million inhabitants in the Western world Affects all races Affects all ages; however, most prevalent in 4th and 5th decades of life Higher prevalence in females (80%) Global burden of PAH may be underestimated because of: Underdiagnosis (eg, nondescript symptoms) Misdiagnosis (eg, asthma, left-heart disease) Increasing risk factors (eg, HIV infection, chronic liver disease, stimulant use, schistosomiasis)
 Increasing risk factors (eg, HIV infection, chronic liver disease, stimulant use,")
8 Patients (N) % of PAH patients experienced symptoms for > 2 years before PAH was diagnosed to < to <1 1.0 to < to <2 2.0 to < to <3 3.0 to < to <4 4.0 to < to <5 5.0 to < to <6 6.0 to < to <7 7.0 to < to <8 8.0 to < to <9 9.0 to < to < Time to Diagnosis from Symptom Onset in Years Chest 2010; 137:376

9 Pulmonary Vascular Disease Group 1. Pulmonary arterial hypertension Mean pulmonary artery pressure 25 mmhg Pulmonary capillary wedge pressure 15 mmhg Pulmonary vascular resistance > 3 Wood units Idiopathic PAH Heritable Drug and toxininduced Associated with: Connective tissue disease HIV infection Portal hypertension Congenital heart disease Chronic hemolytic anemia Simonneau G et al. J Am Coll Cardiol. 2009; 54;S43-54.

10 Classifications of Pulmonary Hypertension Group 1: Pulmonary arterial hypertension (PAH) Collagen vascular disease Idiopathic HIV Drugs and toxins Portopulmonary hypertension Congenital heart disease Other Heritable Pulmonary veno-occlusive disease

11 Classifications of Pulmonary Hypertension Group 2. PH due to left heart disease Systolic dysfunction Diastolic dysfunction Valvular disease Group 3. PH due to lung diseases and/or hypoxia COPD Interstitial lung disease Other pulmonary diseases with mixed restrictive and obstructive pattern Sleep-disordered breathing Alveolar hypoventilation disorders Chronic exposure to high altitude Developmental abnormalities Simonneau G et al. J Am Coll Cardiol. 2009; 54;S43-54.

12 Classifications of Pulmonary Hypertension Group 4: Chronic thromboembolic pulmonary hypertension Group 5: Unclear multifactorial mechanisms Sarcoidosis Post-splenectomy Hematologic disorders Metabolic disorders

13 Classification Debates Pulmonary arterial hypertension Out of proportion to: left-sided heart disease lung disease (obstructive lung disease, pulmonary fibrosis)

14 Intrinsic Pulmonary Vascular Disease

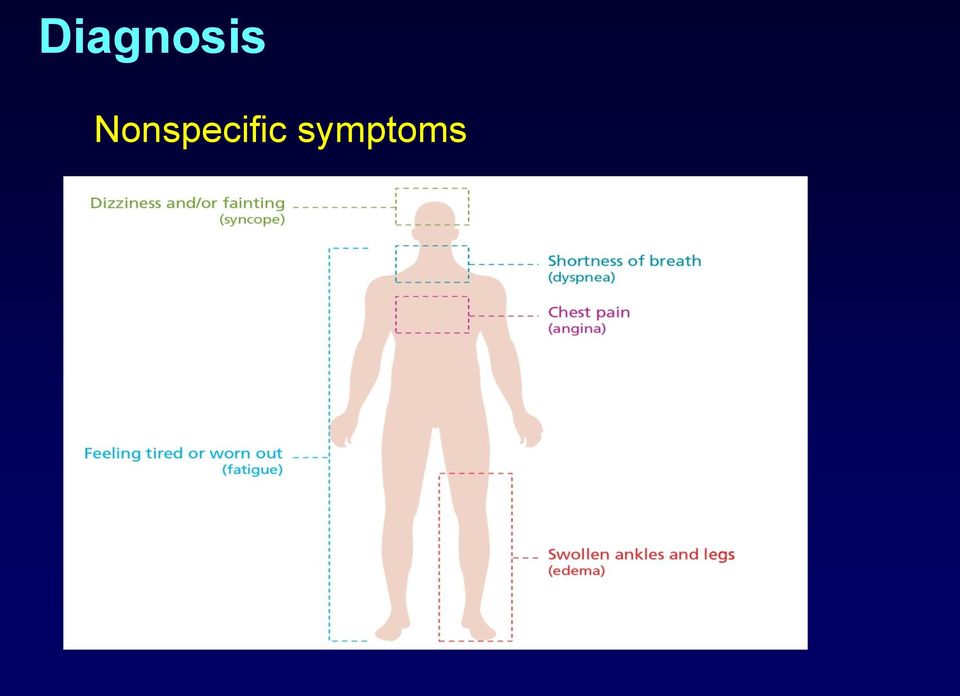
15 Diagnosis Nonspecific symptoms
16 Diagnosis Pulmonary Function Tests Ventilation-Perfusion Scan or Chest CT-Angiogram Obstructive Lung Disease Low DLCO Chronic Pulmonary Embolism Lung Parenchyma Echocardiogram (with agitated saline) Shunt Structural and Functional Changes Laboratory Tests Collagen Vascular Disease Liver disease HIV Sleep Study OSA



17 Common Findings Enlarged cardiac silhouette Enlarged pulmonary arteries Right axis deviation Right atrial enlargement Right ventricular strain

18 Pulmonary Function Tests Decreased DLCO Out of proportion to any restriction % FVC % DLCO 1.6 Spirometry Ref (LLN-ULN) Pre %Ref FVC Liters 2.47 ( ) FEV1 Liters 1.87 ( ) FEV1/FVC % 77 ( ) 81 FEF25-75% L/sec 1.74 ( ) Diffusing Capacity (Hb 13.8) DLCO ml/mmhg/min 20.1 ( ) DL Adj ml/mmhg/min 20.1 ( )
 DLCO ml/mmhg/min 20.1 (14.1-26.1) 9.")
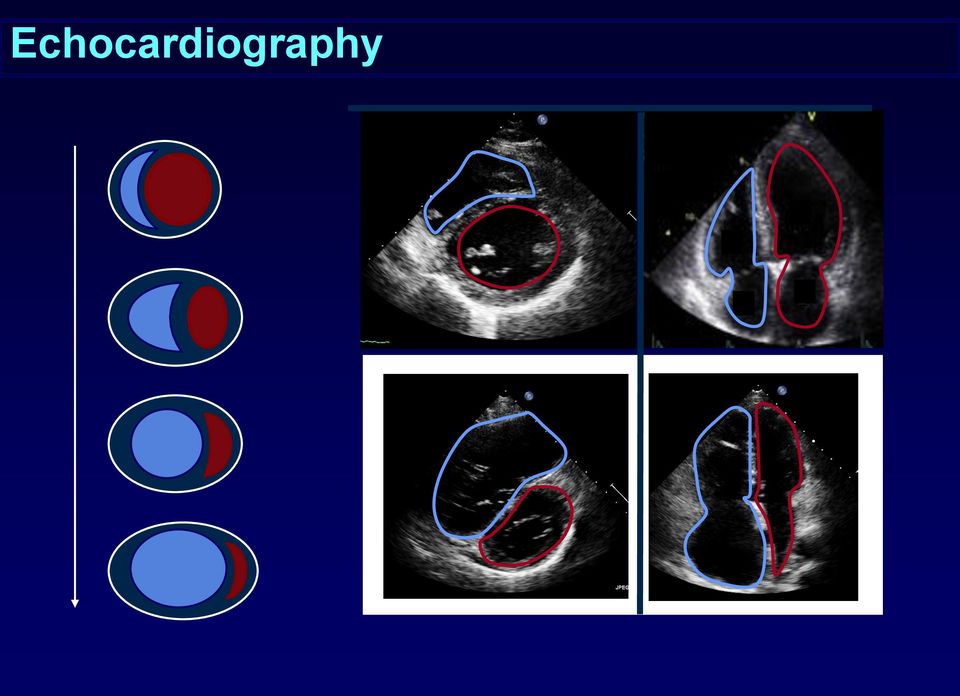
19 Echocardiography Echocardiographic findings concerning for PH Elevated RVSP Right atrial enlargement Right ventricular enlargement Decreased right ventricular systolic function Pericardial effusion Tricuspid jet velocity > 2.8 m/sec 4(TRV) 2 + RAP

20 Echocardiography
 mmhg 13 mmhg 2.8 L/min 12.")
21 Echocardiography Right atrial pressure Pulmonary artery pressure PCWP Cardiac Output Pulmonary Vascular Resistance 6 mmhg 44/22 (29) mmhg 10 mmhg 5.4 L/min 3.5 Wood units Right atrial pressure Pulmonary artery pressure PCWP Cardiac Output Pulmonary Vascular Resistance 20 mmhg 68/40 (49) mmhg 13 mmhg 2.8 L/min 12.9 Wood units
22 CTPA: Chronic Thromboembolic Disease Courtesy of Bill Auger UCSD

23 Right Heart Catheterization Required to diagnosis pulmonary hypertension Mean pulmonary artery pressure 25 mmhg Pulmonary arterial hypertension Mean pulmonary artery pressure 25 mmhg Normal pulmonary capillary wedge pressure Pulmonary vascular resistance > 3 WU
24 Hemodynamic Variables Normal Abnormal Abnormal Abnormal Right Atrial Pressure < 8 mmhg 9 mmhg 12 mmhg 12 mmhg Mean Pulmonary Artery Pressure < 20 mmhg 40 mmhg 32 mmhg 32 mmhg Pulmonary Capillary Wedge Pressure < 15 mmhg 18 mmhg 29 mmhg 8 mmhg Cardiac Output 5 L/min 13.7 L/min 4.5 L/min 3.2 L/min Pulmonary Vascular Resistance < 3 WU 1.6 WU 1 WU 7.5 WU Liver Disease Left Heart Disease Pulmonary Arterial Hypertension
* Responds to calcium channel blockers (Nifedipine) 20 ppm for 15 minutes Pulmonary hypertension primarily due")
25 Right Heart Catheterization Vasoreactivity Selective vasodilator of the pulmonary vasculature (smooth muscle relaxation) Decrease in mean PA pressure by 10 mmhg to a level < 40 mmhg; no loss of cardiac output ino Pulmonary hypertension primarily due to vasoconstriction (reversible)* Responds to calcium channel blockers (Nifedipine) 20 ppm for 15 minutes Pulmonary hypertension primarily due to cell proliferation (irreversible)
26 Mean pulmonary artery pressure (mmhg) Definition of Vasoreactivity * * 10 mmhg 10
27 Cumulative Survival Survival Based on Vasoreactivity vasoreactive not vasoreactive Years
28 Differential Diagnosis of PAH: Algorithm RVE, RAE, RVSP Left heart disease VHD, CHD COPD ILD thoracic abnl Sleep disorder Echocardiogram Chest x-ray PFTs Sleep study LFTs and clinical evidence of cirrhosis and portal HTN HIV test Autoantibody tests Ventilationperfusion scan, angiography PoPH Functional test RH catheterization Vasodilator test HIV Scleroderma SLE RA Vasculitis Chronic thromboembolism. McLaughlin and McGoon. Circulation. 2006;114:
29 Evaluation of Possible PH Echocardiogram 6-12 month yes Liver disease Collagen vascular disease HIV Abnormal? no Risk Factor? no Routine Follow Up yes Systolic dysfunction Diastolic dysfunction Valvular disease Left Heart Disease? yes Cardiology Consult no Standard PH Work Up
30 Treatment FDA-Approved for PAH Risk stratification is primary determinant of therapy Phosphodiesterase Endothelin Receptor Prostanoids Inhibitors (oral) Antagonists (oral) Sildenafil Bosentan Iloprost (INH) WHO I to IV WHO II, III & IV WHO III & IV Tadalafil Ambrisentan Epoprostenol (IV) WHO I to IV WHO II & III WHO III & IV Treprostinil (IV, SQ, INH) WHO II to IV
31 Determining Therapy Lower Risk Determinants of Risk Higher Risk No Clinical evidence of RV failure Yes Gradual Progression Rapid II, III WHO class IV Longer (>400 m) 6MW distance Shorter (<300 m) Minimally elevated BNP Very elevated Minimal RV dysfunction Normal/near normal RAP and CI Echocardiographic findings Hemodynamics Pericardial effusion, significant RV dysfunction High RAP, low CI McLaughlin VV and McGoon M. Circulation. 2006;114:
32 WHO Functional Classification WHO Class I Class II Class III Definition Patients with PAH but without resulting limitation of physical activity. Ordinary physical activity does not cause undue dyspnea or fatigue, chest pain, or near syncope Patients with PAH resulting in slight limitation of physical activity. They are comfortable at rest. Ordinary physical activity causes undue dyspnea or fatigue, chest pain, or near syncope Patients with PAH resulting in marked limitation of physical activity. They are comfortable at rest. Less than ordinary physical activity causes undue dyspnea or fatigue, chest pain, or near syncope Class IV Patients with PAH with inability to carry out any physical activity without symptoms. These patients manifest signs of right heart failure. Dyspnea or fatigue may even be present at rest. Discomfort is increased by any physical activity
33 % of Newly Diagnosed Patients Functional Class at Diagnosis Class I Class II Class III Class IV Note: Newly diagnosed subjects are those whose diagnostic right heart catheterization (RHC) fell within 90 days prior to enrollment. Patients whose confirmatory diagnostic RHC occurred after consent date will be considered newly diagnosed.
34 Hemodynamic Changes Over Time Pulmonary Vascular Resistance Pulmonary Artery Pressure TIME Cardiac Output
35 Choice of Therapy RHC Vasoreactive? Yes CCB No Sustained Response? Yes Epoprostenol or Treprostinil (IV) Iloprost (INH) ERA, PDE-5 (oral) Treprostinil (SC) High Risk? No Low No Deterioration? ERA, PDE-5 (oral) Epoprostenol or Treprostinil (IV) Iloprost (INH) Treprostinil (SC) Yes Combination Therapy Investigational Protocols Atrial Septostomy Lung Transplant McLaughlin V et al. J. AM Coll Card 2009;30:

:13S-24S. N Engl J Med. 2004;351:1425-1436. Eur Heart J.")
36 Vasoactive Mediators Involved In PAH ABNORMALITIES Nitric oxide deficiency Prostacyclin deficiency Endothelin overexpression PDE-5 inhibitors Block the activity of PDE-5, restoring vasodilation through an increase in cgmp THERAPIES Prostacyclin Supplement the deficiency in PGI 2, resulting in vasodilation and inhibition of platelet aggregation ERAs Block the binding of ET-1 to its receptors, preventing vasoconstrictor effects of ET-1 J Am Coll Cardiol. 2004;43(suppl S):13S-24S. N Engl J Med. 2004;351: Eur Heart J. 2004;25:
37 Parenteral Prostanoids Arachidonic Acid Cyclooxygenases PGH 2 (endoperoxides) PGI 2 Synthase PGI 2 (prostacycline) + camp EPOPROSTENOL TREPROSTINIL +
38 Oral Therapies for PAH Phosphodiesterase-5 inhibitors Nitric Oxide Synthase L-Citrulline O 2 L-Argininine Nitric Oxide SILDENAFIL TADALAFIL + cgmp PDE-5 Degraded cgmp Hypotension Headache GERD
39 Oral Therapies for PAH Endothelin receptor antagonists Pre-Proendothelin Pro-endothelin-1 Endothelin-1
40 Oral Therapies for PAH Endothelin receptor antagonists Pre-Proendothelin Pro-endothelin-1 BOSENTAN AMBRISENTAN Endothelin-1 Fluid Retention Liver Dysfunction Teratogenic

41 Inhaled Therapies for PAH Candidates Unable to manage parenteral prostanoids Underlying lung disease Treprostinil Nine breaths 4 times daily Iloprost Treatments 6 to 9 times daily Cough Headache Throat Irritation
 PGI 266 (11%) patients were not on PGI, PDE5-Inh, or ETRA CHEST 2010; 137:")
42 PAH Pharmacotherapies ETRA 453 (19%) 290 (12%) (7%) 308 (9%) PDE5-Inh (13%) 417 (17%) N = 2, (12%) PGI 266 (11%) patients were not on PGI, PDE5-Inh, or ETRA CHEST 2010; 137:
43 Pulmonary Rehabilitation in PAH Cardiopulmonary rehab effective for COPD and CHF patients, why not PAH patients? Historically exercise discouraged in PAH patients because of safety concerns Inducing hypoxemia Arrhythmia Precipitous rise in PA pressure resulting in worsening right heart failure ACCP/AACVPR practice guidelines state that rehab may be beneficial in PAH but offers no explicit recommendations
44 Pulmonary Rehabilitation in PAH Study Design Circulation 2006; 114: patients with group I and group IV PH randomly assigned to control or intense training group 15 week program (inpatient for 3 weeks) Primary end points: change in 6-minute walk and quality of life score
45 Pulmonary Rehabilitation in PAH Circulation 2006; 114:
46 Pulmonary Rehabilitation in PAH 111 m increase in 6-minute walking distance between control and primary training group (P< 0.001) Circulation 2006; 114:
47 Pulmonary Rehabilitation in PAH Study Design 22 patients with group I and group IV PH randomly assigned to control or exercise training group 12 week program with 24 1-hour sessions of exercise training Primary end points: change in 6-minute walk and peak VO 2

48 Pulmonary Rehabilitation in PAH
49 Pulmonary Rehabilitation in PAH 58 m increase in 6MWD in exercise group c/w controls (P = 0.003); also significant increase in peak VO 2

50 Pulmonary Rehabilitation in PAH Study Design Chest 2013; 143: patients with group I PAH randomly assigned to education or education/exercise combined 10 week exercise program with sessions of treadmill walking for min per session Primary end points: change in 6-minute walk, peak work rate and quality of life score
51 Pulmonary Rehabilitation in PAH
52 Pulmonary Rehabilitation in PAH 45 m increase in 6 MWD in exercise group c/w education only group; no significant increase in peak VO2 Significant improvement in QOL measures No adverse events Chest 2013; 143:
53 Pulmonary Rehabilitation in PAH Limited evidence but rehab in PAH is safe and effective improvement in exercise capacity generally exceeds that observed in drug trials Optimal patient population and rehab protocol are not well defined

54 Change in 6MWD (m) Walk Distance (meters) Median Change (meters) Mean (± SEM) absolute change vs baseline (m) 30 min. post inhalation 6MWD with Approved Drugs Median Change from Baseline in 6-Minute Walk Exercise Test at Week *P Inhaled Iloprost - AIR Iloprost Placebo Epoprostenol Treatment: Barst RJ et al. NEJM 334: , Epoprostenol Baseline = 315 m FDA-Approved Bosentan: Conventional Baseline = 270 m 6-min Walk Test (ITT) 62 Change From Baseline to Week Placebo (n = 69) Bosentan 125 or 250 mg BID (n = 144) Walk Distance Phase III Trials: Change in 6MWD -40 Baseline Week 4 Week 8 Week 16 As a Function of Dose 1 Treprostinil mg/bid 125 or 250 mg/bid p = Mean ± SEM Baseline 4 weeks 8 weeks 12 weeks ARIES 1: Primary Endpoint 75 Change in 6MWD at Week 12 placebo-adjusted 10 mg = 51.4 m (p = ) 5 mg = 30.6 m (p = ) Sildenafil m Ambrisentan m -7.8 m -25 Week 0 Week 4 Week 8 Week 12 Wilcoxon rank-sum test compared to placebo Error bars = standard error of the mean Placebo 5 mg 10 mg Oudiz RJ. Chest. 2006;130 (Suppl 1):121S.
55 Summary Pulmonary hypertension (PH) is an elevation of mean PA pressure to 25 mmhg on right heart catheterization PAH (group 1 PH) requires that the PCWP is < 15 mmhg and the pulmonary vascular resistance is > 3 WU Symptoms of pulmonary hypertension are nonspecific Dyspnea Fatigue Echocardiogram is the best screening tool Oral and parenteral therapies are available Exercise training and pulmonary rehabilitation is beneficial
PULMONARY HYPERTENSION. Charles A. Thompson, M.D., FACC, FSCAI Cardiovascular Institute of the South Zachary, Louisiana
 PULMONARY HYPERTENSION Charles A. Thompson, M.D., FACC, FSCAI Cardiovascular Institute of the South Zachary, Louisiana What is Pulmonary Hypertension? What is normal? Pulmonary artery systolic pressure
PULMONARY HYPERTENSION Charles A. Thompson, M.D., FACC, FSCAI Cardiovascular Institute of the South Zachary, Louisiana What is Pulmonary Hypertension? What is normal? Pulmonary artery systolic pressure
Pulmonary Arterial Hypertension: Review and Updates. Is it Primary vs Secondary Pulmonary Hypertension? No!! Dated Nomenclature. Veronica Franco, MD
 Pulmonary Arterial Hypertension: Review and Updates Veronica Franco, MD Section of Pulmonary Hypertension Section of Heart Failure and Transplantation Ohio State University Is it Primary vs Secondary Pulmonary
Pulmonary Arterial Hypertension: Review and Updates Veronica Franco, MD Section of Pulmonary Hypertension Section of Heart Failure and Transplantation Ohio State University Is it Primary vs Secondary Pulmonary
ELIGIBILITY CRITERIA FOR PULMONARY ARTERIAL HYPERTENSION THERAPY
 ELIGIBILITY CRITERIA FOR PULMONARY ARTERIAL HYPERTENSION THERAPY Contents ELIGIBILITY CRITERIA FOR INITIATION OF PULMONARY ARTERIAL HYPERTENSION THERAPY... 2 Initial Application for Funding of Pulmonary
ELIGIBILITY CRITERIA FOR PULMONARY ARTERIAL HYPERTENSION THERAPY Contents ELIGIBILITY CRITERIA FOR INITIATION OF PULMONARY ARTERIAL HYPERTENSION THERAPY... 2 Initial Application for Funding of Pulmonary
Pulmonary Artery Hypertension
 Pulmonary Artery Hypertension Janet M. Pinson, RN, MSN, ACNP Maureen P. Flattery, RN, MS, ANP Virginia Commonwealth University Health System Richmond, VA Pulmonary artery hypertension (PAH) is defined
Pulmonary Artery Hypertension Janet M. Pinson, RN, MSN, ACNP Maureen P. Flattery, RN, MS, ANP Virginia Commonwealth University Health System Richmond, VA Pulmonary artery hypertension (PAH) is defined
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Health Technology Appraisal. Drugs for the treatment of pulmonary arterial hypertension
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Drugs for the treatment of Remit / Appraisal objective: Final scope To appraise the clinical and cost effectiveness of
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Drugs for the treatment of Remit / Appraisal objective: Final scope To appraise the clinical and cost effectiveness of
1. Phosphodiesterase Type 5 Enzyme Inhibitors: Sildenafil (Revatio), Tadalafil (Adcirca)
, Tadalafil (Adcirca)") This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutic
This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutic
Pulmonary Hypertension in Sickle Cell Disease. Jorge Ramos Hematology Fellows Conference June 28, 2013
 Pulmonary Hypertension in Sickle Cell Disease Jorge Ramos Hematology Fellows Conference June 28, 2013 Patient Presentation 28F with SCD, genotype SS. Presented to UWMC ER with 1 month progressive DOE and
Pulmonary Hypertension in Sickle Cell Disease Jorge Ramos Hematology Fellows Conference June 28, 2013 Patient Presentation 28F with SCD, genotype SS. Presented to UWMC ER with 1 month progressive DOE and
Pulmonary Arterial Hypertension. Mark Rumbak, MD Professor of Medicine Morsani College of Medicine University of South Florida
 Pulmonary Arterial Hypertension Mark Rumbak, MD Professor of Medicine Morsani College of Medicine University of South Florida PAH Disease State Module Outline Background and definition Clinical classification
Pulmonary Arterial Hypertension Mark Rumbak, MD Professor of Medicine Morsani College of Medicine University of South Florida PAH Disease State Module Outline Background and definition Clinical classification
PULMONARY ARTERIAL HYPERTENSION AGENTS
 Approvable Criteria: PULMONARY ARTERIAL HYPERTENSION AGENTS Brand Name Generic Name Length of Authorization Revatio Sildenafil citrate Calendar Year Adcirca Tadalafil Calendar Year Letairis Ambrisentan
Approvable Criteria: PULMONARY ARTERIAL HYPERTENSION AGENTS Brand Name Generic Name Length of Authorization Revatio Sildenafil citrate Calendar Year Adcirca Tadalafil Calendar Year Letairis Ambrisentan
Type II Pulmonary Hypertension: Pulmonary Hypertension due to Left Heart Disease
 Heart Failure Center Hadassah University Hospital Type II Pulmonary Hypertension: Pulmonary Hypertension due to Left Heart Disease Israel Gotsman MD The Heart Failure Center, Heart Institute Hadassah University
Heart Failure Center Hadassah University Hospital Type II Pulmonary Hypertension: Pulmonary Hypertension due to Left Heart Disease Israel Gotsman MD The Heart Failure Center, Heart Institute Hadassah University
Hope in 2011 Clinical Advances Where is the road taking us?
 Hope in 2011 Clinical Advances Where is the road taking us? Richard Channick, MD Arlene Schiro, NP Disclosures Arlene Schiro no relevant financial and/or commercial relationships to disclose Hope is like
Hope in 2011 Clinical Advances Where is the road taking us? Richard Channick, MD Arlene Schiro, NP Disclosures Arlene Schiro no relevant financial and/or commercial relationships to disclose Hope is like
FREEDOM C: A 16-Week, International, Multicenter, Double-Blind, Randomized, Placebo-Controlled Comparison of the Efficacy and Safety of Oral UT-15C
 FREEDOM C: A 16-Week, International, Multicenter, Double-Blind, Randomized, Placebo-Controlled Comparison of the Efficacy and Safety of Oral UT-15C SR in Combination with an ERA and/or a PDE-5 Inhibitor
FREEDOM C: A 16-Week, International, Multicenter, Double-Blind, Randomized, Placebo-Controlled Comparison of the Efficacy and Safety of Oral UT-15C SR in Combination with an ERA and/or a PDE-5 Inhibitor
PAH has an incidence
 Pulmonary Arterial Hypertension: A Serious Problem Pulmonary arterial hypertension (PAH) is a serious disease with significant morbidity and mortality and no cure. In this article, Dr. Porhownik and Dr.
Pulmonary Arterial Hypertension: A Serious Problem Pulmonary arterial hypertension (PAH) is a serious disease with significant morbidity and mortality and no cure. In this article, Dr. Porhownik and Dr.
Corporate Medical Policy
 Corporate Medical Policy Pulmonary Hypertension, Drug Management File Name: Origination: Last CAP Review: Next CAP Review: Last Review: pulmonary_hypertension_drug_management 06/1998 3/2015 3/2016 3/2015
Corporate Medical Policy Pulmonary Hypertension, Drug Management File Name: Origination: Last CAP Review: Next CAP Review: Last Review: pulmonary_hypertension_drug_management 06/1998 3/2015 3/2016 3/2015
Clinical Commissioning Policy: Targeted Therapies for Pulmonary Hypertension Functional Class II. April 2013. Reference : NHSCB/A11/P/a
 Clinical Commissioning Policy: Targeted Therapies for Pulmonary Hypertension Functional Class II April 2013 Reference : NHS Commissioning Board Clinical Commissioning Policy: Amendment to National Policy
Clinical Commissioning Policy: Targeted Therapies for Pulmonary Hypertension Functional Class II April 2013 Reference : NHS Commissioning Board Clinical Commissioning Policy: Amendment to National Policy
Statement on Disability: Pulmonary Hypertension
 Statement on Disability: Pulmonary Hypertension Ronald J. Oudiz, MD and Robyn J. Barst, MD on behalf of Pulmonary Hypertension Association The Scientific Leadership Council of the Pulmonary Hypertension
Statement on Disability: Pulmonary Hypertension Ronald J. Oudiz, MD and Robyn J. Barst, MD on behalf of Pulmonary Hypertension Association The Scientific Leadership Council of the Pulmonary Hypertension
The Global Alliance against Chronic Respiratory Diseases
 The Global Alliance against Chronic Respiratory Diseases Pulmonary hypertension Dr Marc Humbert What is the burden of pulmonary hypertension? The true burden of pulmonary hypertension is currently unknown
The Global Alliance against Chronic Respiratory Diseases Pulmonary hypertension Dr Marc Humbert What is the burden of pulmonary hypertension? The true burden of pulmonary hypertension is currently unknown
Scottish Medicines Consortium
 Scottish Medicines Consortium sildenafil citrate 20mg tablets (Revatio ) No. (235/06) Pfizer New indication 6 January 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the above
Scottish Medicines Consortium sildenafil citrate 20mg tablets (Revatio ) No. (235/06) Pfizer New indication 6 January 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the above
PAH in. Registry to Evaluate Early and Long-Term PAH Disease Management
 PAH in Registry to Evaluate Early and Long-Term PAH Disease Management Ioana R. Preston, MD Co-Director, Pulmonary Hypertension Center Tufts Medical Center, Boston, MA Background What is REVEAL? Multi-center,
PAH in Registry to Evaluate Early and Long-Term PAH Disease Management Ioana R. Preston, MD Co-Director, Pulmonary Hypertension Center Tufts Medical Center, Boston, MA Background What is REVEAL? Multi-center,
OVERVIEW FDA-APPROVED INDICATIONS
 Tufts Health Together Tufts Health Direct Pharmacy Medical Necessity Guidelines Pulmonary Hypertension Effective: December 9, 2014 Clinical documentation and prior authorization required Not covered Pharmacy
Tufts Health Together Tufts Health Direct Pharmacy Medical Necessity Guidelines Pulmonary Hypertension Effective: December 9, 2014 Clinical documentation and prior authorization required Not covered Pharmacy
Copyright 2012 Oregon State University. All Rights Reserved
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Riociguat Clinical Trial Program
 Riociguat Clinical Trial Program Riociguat (BAY 63-2521) is an oral agent being investigated as a new approach to treat chronic thromboembolic pulmonary hypertension (CTEPH) and pulmonary arterial hypertension
Riociguat Clinical Trial Program Riociguat (BAY 63-2521) is an oral agent being investigated as a new approach to treat chronic thromboembolic pulmonary hypertension (CTEPH) and pulmonary arterial hypertension
Pharmacy Policy Bulletin
 Pharmacy Policy Bulletin Title: Policy #: Pulmonary Arterial Hypertensive (PAH) agents Rx.01.83 Application of pharmacy policy is determined by benefits and contracts. Benefits may vary based on product
Pharmacy Policy Bulletin Title: Policy #: Pulmonary Arterial Hypertensive (PAH) agents Rx.01.83 Application of pharmacy policy is determined by benefits and contracts. Benefits may vary based on product
Target therapies for the treatment of pulmonary arterial hypertension in Adults
 Paper K2 National Specialised Commissioning Group Commissioning Policy Target therapies for the treatment of pulmonary arterial hypertension in Adults POLICY PUBLISHED: 1 JULY 2008 POLICY REVISED: 14 JANUARY
Paper K2 National Specialised Commissioning Group Commissioning Policy Target therapies for the treatment of pulmonary arterial hypertension in Adults POLICY PUBLISHED: 1 JULY 2008 POLICY REVISED: 14 JANUARY
Pharmacy Medical Necessity Guidelines: Pulmonary Hypertension Medications
 Pharmacy Medical Necessity Guidelines: Pulmonary Hypertension Medications Effective: January 1, 2016 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review
Pharmacy Medical Necessity Guidelines: Pulmonary Hypertension Medications Effective: January 1, 2016 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review
Recently approved drugs offer significant improvements for treatment options in pulmonary arterial hypertension
 DISEASE MANAGEMENT Recently approved drugs offer significant improvements for treatment options in pulmonary arterial hypertension Treatment of pulmonary arterial hypertension (PAH) Class I. PAH without
DISEASE MANAGEMENT Recently approved drugs offer significant improvements for treatment options in pulmonary arterial hypertension Treatment of pulmonary arterial hypertension (PAH) Class I. PAH without
CLINICAL POLICY Department: Medical Management Document Name: Pulmonary Arterial Hypertension Therapies
 Page: 1 of 15 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
Page: 1 of 15 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
Chronic Thromboembolic Disease. Chronic Thromboembolic Disease Definition. Diagnosis Prevention Treatment Surgical Nonsurgical
 Chronic Thromboembolic Disease Diagnosis Prevention Treatment Surgical Nonsurgical Chronic Thromboembolic Disease Definition Pulmonary Hypertension due to chronic thromboembolism 6 months post acute PE:
Chronic Thromboembolic Disease Diagnosis Prevention Treatment Surgical Nonsurgical Chronic Thromboembolic Disease Definition Pulmonary Hypertension due to chronic thromboembolism 6 months post acute PE:
*Documentation of pretreatment results from right heart catheterization and PEA required, as applicable
 DRUG POLICY BENEFIT APPLICATION Pulmonary Arterial Hypertension Benefit determinations are based on the applicable contract language in effect at the time the services were rendered. Exclusions, limitations
DRUG POLICY BENEFIT APPLICATION Pulmonary Arterial Hypertension Benefit determinations are based on the applicable contract language in effect at the time the services were rendered. Exclusions, limitations
Pulmonary Arterial Hypertension: Assessment of disease s severity
 Pulmonary Arterial Hypertension: Assessment of disease s severity Carmine Dario Vizza Dept. Cardiovascular and Respiratory Diseases La Sapienza University of Rome e-mail : dario.vizza@uniroma1.it Pulmonary
Pulmonary Arterial Hypertension: Assessment of disease s severity Carmine Dario Vizza Dept. Cardiovascular and Respiratory Diseases La Sapienza University of Rome e-mail : dario.vizza@uniroma1.it Pulmonary
CADTH CANADIAN DRUG EXPERT REVIEW COMMITTEE FINAL RECOMMENDATION
 CADTH CANADIAN DRUG EXPERT REVIEW COMMITTEE FINAL RECOMMENDATION RIOCIGUAT (Adempas Bayer HealthCare Inc.) Indication: Pulmonary Arterial Hypertension Recommendation: The CADTH Canadian Drug Expert Review
CADTH CANADIAN DRUG EXPERT REVIEW COMMITTEE FINAL RECOMMENDATION RIOCIGUAT (Adempas Bayer HealthCare Inc.) Indication: Pulmonary Arterial Hypertension Recommendation: The CADTH Canadian Drug Expert Review
PAH. Salman Bin AbdulAziz University College Of Pharmacy 22/01/35
 Salman Bin AbdulAziz University College Of Pharmacy PAH Therapeutics II PHCL 430 Ahmed A AlAmer PharmD R.W. is a 38-year-old obese woman who presents with increasing symptoms of fatigue and shortness of
Salman Bin AbdulAziz University College Of Pharmacy PAH Therapeutics II PHCL 430 Ahmed A AlAmer PharmD R.W. is a 38-year-old obese woman who presents with increasing symptoms of fatigue and shortness of
Idiopathic Pulmonary Fibrosis (IPF) Research
 Research") Idiopathic Pulmonary Fibrosis (IPF): Why Early Referral is Critical Even if Your Patient is Not Eligible for a Clinical Trial Idiopathic Pulmonary Fibrosis (IPF) Research Management of IPF requires a confident
Idiopathic Pulmonary Fibrosis (IPF): Why Early Referral is Critical Even if Your Patient is Not Eligible for a Clinical Trial Idiopathic Pulmonary Fibrosis (IPF) Research Management of IPF requires a confident
Non-Invasive Risk Predictors in (Children with) Pulmonary Hypertension
 Pulmonary Hypertension") Ideal risk prognosticator Easy to acquire Non-Invasive Risk Predictors in (Children with) Pulmonary Hypertension Safe -- Non-invasive Robust Gerhard-Paul Diller Astrid Lammers Division of Adult Congenital
Ideal risk prognosticator Easy to acquire Non-Invasive Risk Predictors in (Children with) Pulmonary Hypertension Safe -- Non-invasive Robust Gerhard-Paul Diller Astrid Lammers Division of Adult Congenital
2. Background This drug had not previously been considered by the PBAC.
 PUBLIC SUMMARY DOCUMENT Product: Ambrisentan, tablets, 5 mg and 10 mg, Volibris Sponsor: GlaxoSmithKline Australia Pty Ltd Date of PBAC Consideration: July 2009 1. Purpose of Application The submission
PUBLIC SUMMARY DOCUMENT Product: Ambrisentan, tablets, 5 mg and 10 mg, Volibris Sponsor: GlaxoSmithKline Australia Pty Ltd Date of PBAC Consideration: July 2009 1. Purpose of Application The submission
Advanced Therapies for Pharmacological Treatment of Pulmonary Hypertension
 Advanced Therapies for Pharmacological Treatment of Pulmonary Hypertension Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana,
Advanced Therapies for Pharmacological Treatment of Pulmonary Hypertension Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana,
Research Review EDUCATIONAL SERIES. Pulmonary Arterial Hypertension
 Research Review EDUCATIONAL SERIES About the Reviewers Dr Ken Whyte is a Respiratory Physician at Auckland DHB Respiratory Services and Honorary Associate Professor of Medicine at the University of Auckland.
Research Review EDUCATIONAL SERIES About the Reviewers Dr Ken Whyte is a Respiratory Physician at Auckland DHB Respiratory Services and Honorary Associate Professor of Medicine at the University of Auckland.
Diagnosis and Management of Pulmonary Arterial Hypertension: Implications for Respiratory Care
 Diagnosis and Management of Pulmonary Arterial Hypertension: Implications for Respiratory Care Deborah Jo Levine MD Introduction Definition Normal Physiology Pathophysiology Pathogenesis Classification
Diagnosis and Management of Pulmonary Arterial Hypertension: Implications for Respiratory Care Deborah Jo Levine MD Introduction Definition Normal Physiology Pathophysiology Pathogenesis Classification
We can learn a lot from you...
 Educational program by Material endorsed by We can learn a lot from you... When it comes to pulmonary arterial hypertension (PAH), the members of your specialist healthcare team are experts on the best
Educational program by Material endorsed by We can learn a lot from you... When it comes to pulmonary arterial hypertension (PAH), the members of your specialist healthcare team are experts on the best
Pulmonary Diseases. Lung Disease: Pathophysiology, Medical and Exercise Programming. Overview of Pathophysiology
 Lung Disease: Pathophysiology, Medical and Exercise Programming Overview of Pathophysiology Ventilatory Impairments Increased airway resistance Reduced compliance Increased work of breathing Ventilatory
Lung Disease: Pathophysiology, Medical and Exercise Programming Overview of Pathophysiology Ventilatory Impairments Increased airway resistance Reduced compliance Increased work of breathing Ventilatory
Medicare C/D Medical Coverage Policy
 Nebulizer Medications Origination: June 17, 2009 Review Date: October 21, 2015 Next Review: October, 2017 Medicare C/D Medical Coverage Policy DESCRIPTION Nebulizer medications are used to prevent and
Nebulizer Medications Origination: June 17, 2009 Review Date: October 21, 2015 Next Review: October, 2017 Medicare C/D Medical Coverage Policy DESCRIPTION Nebulizer medications are used to prevent and
Acknowledgements. PAH in Children: Natural History. The Sildenafil Saga
 The Sildenafil Saga David L. Wessel, MD Executive Vice President Chief Medical Officer Ikaria Distinguished Professor of Critical Care Children s National Medical Center Washington, DC, USA Acknowledgements
The Sildenafil Saga David L. Wessel, MD Executive Vice President Chief Medical Officer Ikaria Distinguished Professor of Critical Care Children s National Medical Center Washington, DC, USA Acknowledgements
Pulmonary Arterial Hypertension (PAH) Agents 12/01/2009
 Agents 12/01/2009") Pulmonary Arterial Hypertension (PAH) Agents 12/01/2009 Copyright 2006-2009 by Provider Synergies, L.L.C. All rights reserved. Printed in the United States of America. All rights reserved. No part of this
Pulmonary Arterial Hypertension (PAH) Agents 12/01/2009 Copyright 2006-2009 by Provider Synergies, L.L.C. All rights reserved. Printed in the United States of America. All rights reserved. No part of this
P pulmonary Hypertension and Its Importance to the Body
 Cardiol Clin 22 (2004) 441 452 Diagnosis and treatment of pulmonary arterial hypertension Richard Channick, MD a, *, Timothy L. Williamson, MD b a Division of Pulmonary and Critical Care, University of
Cardiol Clin 22 (2004) 441 452 Diagnosis and treatment of pulmonary arterial hypertension Richard Channick, MD a, *, Timothy L. Williamson, MD b a Division of Pulmonary and Critical Care, University of
James F. Kravec, M.D., F.A.C.P
 James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
Pulmonal hypertensjon. Arne K. Andreassen Kardiologisk avdeling Oslo Universitetssykehus Rikshospitalet
 Pulmonal hypertensjon Arne K. Andreassen Kardiologisk avdeling Oslo Universitetssykehus Rikshospitalet Clinical classification of pulmonary hypertension 1. Pulmonary arterial hypertension (PAH) 2. Pulmonary
Pulmonal hypertensjon Arne K. Andreassen Kardiologisk avdeling Oslo Universitetssykehus Rikshospitalet Clinical classification of pulmonary hypertension 1. Pulmonary arterial hypertension (PAH) 2. Pulmonary
Inpatient Heart Failure Management: Risks & Benefits
 Inpatient Heart Failure Management: Risks & Benefits Dr. Kenneth L. Baughman Professor of Medicine Harvard Medical School Director, Advanced Heart Disease Section Brigham & Women's Hospital Harvard Medical
Inpatient Heart Failure Management: Risks & Benefits Dr. Kenneth L. Baughman Professor of Medicine Harvard Medical School Director, Advanced Heart Disease Section Brigham & Women's Hospital Harvard Medical
A Review of Sitaxsentan Sodium in Patients with Pulmonary Arterial Hypertension
 A Review of Sitaxsentan Sodium in Patients with Pulmonary Arterial Hypertension The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters.
A Review of Sitaxsentan Sodium in Patients with Pulmonary Arterial Hypertension The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters.
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL
 Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
Therapeutic Class Overview Pulmonary Arterial Hypertension Agents
 Therapeutic Class Overview Pulmonary Arterial Hypertension Agents Therapeutic Class Overview/Summary: The oral pulmonary hypertension agents are Food Drug Administration (FDA)-approved for the treatment
Therapeutic Class Overview Pulmonary Arterial Hypertension Agents Therapeutic Class Overview/Summary: The oral pulmonary hypertension agents are Food Drug Administration (FDA)-approved for the treatment
April 2015 CALGARY ZONE CLINICAL REFERENCE PULMONARY CENTRAL ACCESS & TRIAGE
 April 2015 CALGARY ZONE CLINICAL REFERENCE CENTRAL ACCESS & TRIAGE Introduction Pulmonary consulting services are organized through the Calgary Zone Pulmonary Central Access and Triage (PCAT). Working
April 2015 CALGARY ZONE CLINICAL REFERENCE CENTRAL ACCESS & TRIAGE Introduction Pulmonary consulting services are organized through the Calgary Zone Pulmonary Central Access and Triage (PCAT). Working
CADTH Therapeutic Review Report
 Canadian Agency for Drugs and Technologies in Health Agence canadienne des médicaments et des technologies de la santé CADTH Therapeutic Review Report March 2015 Drugs for Pulmonary Arterial Hypertension:
Canadian Agency for Drugs and Technologies in Health Agence canadienne des médicaments et des technologies de la santé CADTH Therapeutic Review Report March 2015 Drugs for Pulmonary Arterial Hypertension:
Pulmonary Arterial Hypertension
 Chapter 27 Pulmonary Arterial Hypertension Gandharba Ray, L Ravi Kumar INTRODUCTION ABSTRACT Pulmonary arterial hypertension (PAH) is a syndrome resulting from decreased flow of blood in the pulmonary
Chapter 27 Pulmonary Arterial Hypertension Gandharba Ray, L Ravi Kumar INTRODUCTION ABSTRACT Pulmonary arterial hypertension (PAH) is a syndrome resulting from decreased flow of blood in the pulmonary
Pulmonary Arterial Hypertension (PAH)
") Pulmonary Arterial Hypertension (PAH) Contents 1. Introduction 3 2. What is PAH? 4 3. Classification of PAH 5 4. How is PAH severity classified? 7 5. How common is PAH? 7 6. Why does PAH develop? 8 7.
Pulmonary Arterial Hypertension (PAH) Contents 1. Introduction 3 2. What is PAH? 4 3. Classification of PAH 5 4. How is PAH severity classified? 7 5. How common is PAH? 7 6. Why does PAH develop? 8 7.
Medical management of CHF: A New Class of Medication. Al Timothy, M.D. Cardiovascular Institute of the South
 Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
Meta-Analysis of Randomized Controlled Trials on Treatment of Pulmonary Arterial Hypertension
 Circulation Journal Official Journal of the Japanese Circulation Society http://www.j-circ.or.jp Meta-Analysis of Randomized Controlled Trials on Treatment of Pulmonary Arterial Hypertension Bing He, BSc;
Circulation Journal Official Journal of the Japanese Circulation Society http://www.j-circ.or.jp Meta-Analysis of Randomized Controlled Trials on Treatment of Pulmonary Arterial Hypertension Bing He, BSc;
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF)
 MANAGEMENT of Atrial Fibrillation (AF)") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF) Key priorities Identification and diagnosis Treatment for persistent AF Treatment for permanent AF Antithrombotic
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF) Key priorities Identification and diagnosis Treatment for persistent AF Treatment for permanent AF Antithrombotic
Tests. Pulmonary Functions
 Pulmonary Functions Tests Static lung functions volumes Dynamic lung functions volume and velocity Dynamic Tests Velocity dependent on Airway resistance Resistance of lung tissue to change in shape Dynamic
Pulmonary Functions Tests Static lung functions volumes Dynamic lung functions volume and velocity Dynamic Tests Velocity dependent on Airway resistance Resistance of lung tissue to change in shape Dynamic
Evidence briefing on drug treatments for functional class II pulmonary hypertension
 Evidence briefing on drug treatments for functional class II pulmonary hypertension The North of England Specialised Commissioning Group is the lead organisation charged with commissioning targeted therapies
Evidence briefing on drug treatments for functional class II pulmonary hypertension The North of England Specialised Commissioning Group is the lead organisation charged with commissioning targeted therapies
240- PROBLEM SET INSERTION OF SWAN-GANZ SYSTEMIC VASCULAR RESISTANCE. Blood pressure = f(cardiac output and peripheral resistance)
") 240- PROBLEM SET INSERTION OF SWAN-GANZ 50 kg Pig Rt Jugular 0 cm Rt Atrium 10 cm Rt ventricle 15 cm Wedge 20-25 cm SYSTEMIC VASCULAR RESISTANCE Blood pressure = f(cardiac output and peripheral resistance)
240- PROBLEM SET INSERTION OF SWAN-GANZ 50 kg Pig Rt Jugular 0 cm Rt Atrium 10 cm Rt ventricle 15 cm Wedge 20-25 cm SYSTEMIC VASCULAR RESISTANCE Blood pressure = f(cardiac output and peripheral resistance)
Universitätsklinik für Kardiologie. Test. Thomas M. Suter Akute Herzinsuffizienz Diagnostik und Therapie thomas.suter@insel.ch 1
 Test Thomas M. Suter Akute Herzinsuffizienz Diagnostik und Therapie thomas.suter@insel.ch 1 Heart Failure - Definition European Heart Journal (2008) 29, 2388 2442 Akute Herzinsuffizienz Diagnostik und
Test Thomas M. Suter Akute Herzinsuffizienz Diagnostik und Therapie thomas.suter@insel.ch 1 Heart Failure - Definition European Heart Journal (2008) 29, 2388 2442 Akute Herzinsuffizienz Diagnostik und
2/20/2015. Cardiac Evaluation of Potential Solid Organ Transplant Recipients. Issues Specific to Transplantation. Kidney Transplantation.
 DISCLOSURES I have no relevant financial relationships to disclose. Cardiac Evaluation of Potential Solid Organ Transplant Recipients Michele Hamilton, MD Director, Heart Failure Program Cedars Sinai Heart
DISCLOSURES I have no relevant financial relationships to disclose. Cardiac Evaluation of Potential Solid Organ Transplant Recipients Michele Hamilton, MD Director, Heart Failure Program Cedars Sinai Heart
Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations.
 INTRODUCTION Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations. Although decrease in cardiovascular mortality still major cause of morbidity & burden of disease.
INTRODUCTION Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations. Although decrease in cardiovascular mortality still major cause of morbidity & burden of disease.
Summary Review for Regulatory Action
 Summary Review for Regulatory Action Date (electronic stamp) From Norman Stockbridge Subject Division Director Summary Review NDA/BLA # Supplement # NDA 21-290 Applicant Name Actelion Date of Submission
Summary Review for Regulatory Action Date (electronic stamp) From Norman Stockbridge Subject Division Director Summary Review NDA/BLA # Supplement # NDA 21-290 Applicant Name Actelion Date of Submission
Low-gradient severe aortic stenosis with normal LVEF: A disturbing clinical entity
 Low-gradient severe aortic stenosis with normal LVEF: A disturbing clinical entity Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Disclosures : None 77-year-old woman, mild dyspnea
Low-gradient severe aortic stenosis with normal LVEF: A disturbing clinical entity Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Disclosures : None 77-year-old woman, mild dyspnea
Atrial Fibrillation Management Across the Spectrum of Illness
 Disclosures Atrial Fibrillation Management Across the Spectrum of Illness NONE Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University Objectives AF Discuss the pathophysiology, diagnosis,
Disclosures Atrial Fibrillation Management Across the Spectrum of Illness NONE Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University Objectives AF Discuss the pathophysiology, diagnosis,
Atrial Fibrillation 2014 How to Treat How to Anticoagulate. Allan Anderson, MD, FACC, FAHA Division of Cardiology
 Atrial Fibrillation 2014 How to Treat How to Anticoagulate Allan Anderson, MD, FACC, FAHA Division of Cardiology Projection for Prevalence of Atrial Fibrillation: 5.6 Million by 2050 Projected number of
Atrial Fibrillation 2014 How to Treat How to Anticoagulate Allan Anderson, MD, FACC, FAHA Division of Cardiology Projection for Prevalence of Atrial Fibrillation: 5.6 Million by 2050 Projected number of
Pharmacology of the Respiratory Tract: COPD and Steroids
 Pharmacology of the Respiratory Tract: COPD and Steroids Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Head, Centre of Heart
Pharmacology of the Respiratory Tract: COPD and Steroids Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Head, Centre of Heart
RATE VERSUS RHYTHM CONTROL OF ATRIAL FIBRILLATION: SPECIAL CONSIDERATION IN ELDERLY. Charles Jazra
 RATE VERSUS RHYTHM CONTROL OF ATRIAL FIBRILLATION: SPECIAL CONSIDERATION IN ELDERLY Charles Jazra NO CONFLICT OF INTEREST TO DECLARE Relationship Between Atrial Fibrillation and Age Prevalence, percent
RATE VERSUS RHYTHM CONTROL OF ATRIAL FIBRILLATION: SPECIAL CONSIDERATION IN ELDERLY Charles Jazra NO CONFLICT OF INTEREST TO DECLARE Relationship Between Atrial Fibrillation and Age Prevalence, percent
ATRIAL FIBRILLATION (RATE VS RHYTHM CONTROL)
") ATRIAL FIBRILLATION (RATE VS RHYTHM CONTROL) By Prof. Dr. Helmy A. Bakr Mansoura Universirty 2014 AF Classification: Mechanisms of AF : Selected Risk Factors and Biomarkers for AF: WHY AF? 1. Atrial fibrillation
ATRIAL FIBRILLATION (RATE VS RHYTHM CONTROL) By Prof. Dr. Helmy A. Bakr Mansoura Universirty 2014 AF Classification: Mechanisms of AF : Selected Risk Factors and Biomarkers for AF: WHY AF? 1. Atrial fibrillation
Pulmonary arterial hypertension (PAH) is a
 is a") Eur Respir Rev 2010; 19: 118, 279 287 DOI: 10.1183/09059180.00008010 CopyrightßERS 2010 REVIEW Management of severe pulmonary arterial hypertension J-L. Vachiéry* and G. Simonneau # ABSTRACT: Pulmonary
Eur Respir Rev 2010; 19: 118, 279 287 DOI: 10.1183/09059180.00008010 CopyrightßERS 2010 REVIEW Management of severe pulmonary arterial hypertension J-L. Vachiéry* and G. Simonneau # ABSTRACT: Pulmonary
ANAESTHESIA FOR THE PATIENT WITH PULMONARY HYPERTENSION ANAESTHESIA TUTORIAL OF THE WEEK 228
 ANAESTHESIA FOR THE PATIENT WITH PULMONARY HYPERTENSION ANAESTHESIA TUTORIAL OF THE WEEK 228 20 TH JUNE 2011 Dr Sarah Thomas, Senior Anaesthetic Registrar Royal Hobart Hospital Correspondence to sarah.thomas@dhhs.tas.gov.au
ANAESTHESIA FOR THE PATIENT WITH PULMONARY HYPERTENSION ANAESTHESIA TUTORIAL OF THE WEEK 228 20 TH JUNE 2011 Dr Sarah Thomas, Senior Anaesthetic Registrar Royal Hobart Hospital Correspondence to sarah.thomas@dhhs.tas.gov.au
National Learning Objectives for COPD Educators
 National Learning Objectives for COPD Educators National Learning Objectives for COPD Educators The COPD Educator will be able to achieve the following objectives. Performance objectives, denoted by the
National Learning Objectives for COPD Educators National Learning Objectives for COPD Educators The COPD Educator will be able to achieve the following objectives. Performance objectives, denoted by the
Electronic version is available on the following websites: www.moh.gov.my
 STATEMENT OF INTENT These guidelines were developed to be guides for clinical practice, based on the best available evidence at the time of development. Adherence to these guidelines may not necessarily
STATEMENT OF INTENT These guidelines were developed to be guides for clinical practice, based on the best available evidence at the time of development. Adherence to these guidelines may not necessarily
1p36 and the Heart. John Lynn Jefferies, MD, MPH, FACC, FAHA
 1p36 and the Heart John Lynn Jefferies, MD, MPH, FACC, FAHA Director, Advanced Heart Failure and Cardiomyopathy Services Associate Professor, Pediatric Cardiology and Adult Cardiovascular Diseases Associate
1p36 and the Heart John Lynn Jefferies, MD, MPH, FACC, FAHA Director, Advanced Heart Failure and Cardiomyopathy Services Associate Professor, Pediatric Cardiology and Adult Cardiovascular Diseases Associate
Pulmonary Arterial Hypertension (PAH) Agents, Oral and Inhaled Therapeutic Class Review (TCR) March 30, 2015
 Agents, Oral and Inhaled Therapeutic Class Review (TCR) March 30, 2015") Pulmonary Arterial Hypertension (PAH) Agents, Oral and Inhaled Therapeutic Class Review (TCR) March 30, 2015 No part of this publication may be reproduced or transmitted in any form or by any means, electronic
Pulmonary Arterial Hypertension (PAH) Agents, Oral and Inhaled Therapeutic Class Review (TCR) March 30, 2015 No part of this publication may be reproduced or transmitted in any form or by any means, electronic
Functional Class Improvement and 3-Year Survival Outcomes in Patients With Pulmonary Arterial Hypertension in the REVEAL Registry
 CHEST Original Research PULMONARY VASCULAR DISEASE Functional Class Improvement and 3-Year Survival Outcomes in Patients With Pulmonary Arterial Hypertension in the REVEAL Registry Robyn J. Barst, MD ;
CHEST Original Research PULMONARY VASCULAR DISEASE Functional Class Improvement and 3-Year Survival Outcomes in Patients With Pulmonary Arterial Hypertension in the REVEAL Registry Robyn J. Barst, MD ;
Atrial Fibrillation An update on diagnosis and management
 Dr Arvind Vasudeva Consultant Cardiologist Atrial Fibrillation An update on diagnosis and management Atrial fibrillation (AF) remains the commonest disturbance of cardiac rhythm seen in clinical practice.
Dr Arvind Vasudeva Consultant Cardiologist Atrial Fibrillation An update on diagnosis and management Atrial fibrillation (AF) remains the commonest disturbance of cardiac rhythm seen in clinical practice.
She was 39 years old, gravida 4, para 2. She had an Idiopathic Pulmonary. Arterial Hypertension (PAH) revealed during pregnancy by a New York Heart
 revealed during pregnancy by a New York Heart") Case #1 (year 1992): She was 39 years old, gravida 4, para 2. She had an Idiopathic Pulmonary Arterial Hypertension (PAH) revealed during pregnancy by a New York Heart Association (NYHA) functional class
Case #1 (year 1992): She was 39 years old, gravida 4, para 2. She had an Idiopathic Pulmonary Arterial Hypertension (PAH) revealed during pregnancy by a New York Heart Association (NYHA) functional class
Liver Function Essay
 Liver Function Essay Name: Quindoline Ntui Date: April 20, 2009 Professor: Dr. Danil Hammoudi Class: Anatomy and Physiology 2 Liver function The human body consist of many highly organize part working
Liver Function Essay Name: Quindoline Ntui Date: April 20, 2009 Professor: Dr. Danil Hammoudi Class: Anatomy and Physiology 2 Liver function The human body consist of many highly organize part working
Pulmonary Vascular Disease: Pulmonary Hypertension and Pulmonary Embolism
 Pulmonary Vascular Disease: Pulmonary Hypertension and Pulmonary Embolism Selim M. Arcasoy, M.D. Selim M. Arcasoy, M.D. Professor of Clinical Medicine Medical Program Director Lung Transplantation Program
Pulmonary Vascular Disease: Pulmonary Hypertension and Pulmonary Embolism Selim M. Arcasoy, M.D. Selim M. Arcasoy, M.D. Professor of Clinical Medicine Medical Program Director Lung Transplantation Program
Pulmonary Arterial Hypertension Special Issues and Current Therapeutic Approaches: Part Two
 The online version of this article, along with access to discussion threads on NATF s eforum, is available at: www.natfonline.org/ethrombosis.php (January, 2010) Pulmonary Arterial Hypertension Special
The online version of this article, along with access to discussion threads on NATF s eforum, is available at: www.natfonline.org/ethrombosis.php (January, 2010) Pulmonary Arterial Hypertension Special
Diagnosis and Management of Life Threatening Cardiac Emergencies
 Diagnosis and Management of Life Threatening Cardiac Emergencies Carley Saelinger,VMD, DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian.
Diagnosis and Management of Life Threatening Cardiac Emergencies Carley Saelinger,VMD, DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian.
Treating AF: The Newest Recommendations. CardioCase presentation. Ethel s Case. Wayne Warnica, MD, FACC, FACP, FRCPC
 Treating AF: The Newest Recommendations Wayne Warnica, MD, FACC, FACP, FRCPC CardioCase presentation Ethel s Case Ethel, 73, presents with rapid heart beating and mild chest discomfort. In the ED, ECG
Treating AF: The Newest Recommendations Wayne Warnica, MD, FACC, FACP, FRCPC CardioCase presentation Ethel s Case Ethel, 73, presents with rapid heart beating and mild chest discomfort. In the ED, ECG
Online supplements are not copyedited prior to posting.
 Functional Impact of a Spectrum of Interstitial Lung Abnormalities in Rheumatoid Arthritis Tracy J. Doyle, MD, MPH; Paul F. Dellaripa, MD; Kerri Batra, MD; Michelle L. Frits, BA; Christine K. Iannaccone,
Functional Impact of a Spectrum of Interstitial Lung Abnormalities in Rheumatoid Arthritis Tracy J. Doyle, MD, MPH; Paul F. Dellaripa, MD; Kerri Batra, MD; Michelle L. Frits, BA; Christine K. Iannaccone,
Objectives. The ECG in Pulmonary and Congenital Heart Disease. Lead II P-Wave Amplitude during COPD Exacerbation and after Treatment (50 pts.
 The ECG in Pulmonary and Congenital Heart Disease Gabriel Gregoratos, MD Objectives Review the pathophysiology and ECG signs of pulmonary dysfunction Review the ECG findings in patients with: COPD (chronic
The ECG in Pulmonary and Congenital Heart Disease Gabriel Gregoratos, MD Objectives Review the pathophysiology and ECG signs of pulmonary dysfunction Review the ECG findings in patients with: COPD (chronic
PAH: Standard of Care
 PAH: Standard of Care Nazzareno Galiè Istituto di Cardiologia Università di Bologna nazzareno.galie@unibo.it TF 7 Therapy Standard of Care Questions A. Do we have additional information on the role of
PAH: Standard of Care Nazzareno Galiè Istituto di Cardiologia Università di Bologna nazzareno.galie@unibo.it TF 7 Therapy Standard of Care Questions A. Do we have additional information on the role of
ECG may be indicated for patients with cardiovascular risk factors
 eappendix A. Summary for Preoperative ECG American College of Cardiology/ American Heart Association, 2007 A1 2002 A2 European Society of Cardiology and European Society of Anaesthesiology, 2009 A3 Improvement,
eappendix A. Summary for Preoperative ECG American College of Cardiology/ American Heart Association, 2007 A1 2002 A2 European Society of Cardiology and European Society of Anaesthesiology, 2009 A3 Improvement,
Pulmonary Arterial Hypertension (PAH)
") Pulmonary Arterial Hypertension (PAH) Contents Introduction 2 What is PAH? 3 Classifi cation of PAH 5 How common is PAH? 8 Why does PAH develop? 9 What are the symptoms of PAH? 12 How is PAH diagnosed?
Pulmonary Arterial Hypertension (PAH) Contents Introduction 2 What is PAH? 3 Classifi cation of PAH 5 How common is PAH? 8 Why does PAH develop? 9 What are the symptoms of PAH? 12 How is PAH diagnosed?
Normal Intracardiac Pressures. Lancashire & South Cumbria Cardiac Network
 Normal Intracardiac Pressures Lancashire & South Cumbria Cardiac Network Principle Pressures recorded from catheter tip Electrical transducer - wheatstone bridge mechanical to electrical waveform display
Normal Intracardiac Pressures Lancashire & South Cumbria Cardiac Network Principle Pressures recorded from catheter tip Electrical transducer - wheatstone bridge mechanical to electrical waveform display
Inotropes/Vasoactive Agents Hina N. Patel, Pharm.D., BCPS Cathy Lawson, Pharm.D., BCPS
 Inotropes/Vasoactive Agents Hina N. Patel, Pharm.D., BCPS Cathy Lawson, Pharm.D., BCPS 1. Definition -an agent that affects the contractility of the heart -may be positive (increases contractility) or
Inotropes/Vasoactive Agents Hina N. Patel, Pharm.D., BCPS Cathy Lawson, Pharm.D., BCPS 1. Definition -an agent that affects the contractility of the heart -may be positive (increases contractility) or
STAGES OF SHOCK. IRREVERSIBLE SHOCK Heart deteriorates until it can no longer pump and death occurs.
 STAGES OF SHOCK SHOCK : A profound disturbance of circulation and metabolism, which leads to inadequate perfusion of all organs which are needed to maintain life. COMPENSATED NONPROGRESSIVE SHOCK 30 sec
STAGES OF SHOCK SHOCK : A profound disturbance of circulation and metabolism, which leads to inadequate perfusion of all organs which are needed to maintain life. COMPENSATED NONPROGRESSIVE SHOCK 30 sec
Rehabilitation and Lung Cancer Resection. Roberto Benzo MD MS Mindful Breathing Laboratory Division of Pulmonary & CCM Mayo Clinic
 Rehabilitation and Lung Cancer Resection Roberto Benzo MD MS Mindful Breathing Laboratory Division of Pulmonary & CCM Mayo Clinic Disclosure Funded by the National Cancer Institute NIH for Preoperative
Rehabilitation and Lung Cancer Resection Roberto Benzo MD MS Mindful Breathing Laboratory Division of Pulmonary & CCM Mayo Clinic Disclosure Funded by the National Cancer Institute NIH for Preoperative
Section Four: Pulmonary Artery Waveform Interpretation
 Section Four: Pulmonary Artery Waveform Interpretation All hemodynamic pressures and waveforms are generated by pressure changes in the heart caused by myocardial contraction (systole) and relaxation/filling
Section Four: Pulmonary Artery Waveform Interpretation All hemodynamic pressures and waveforms are generated by pressure changes in the heart caused by myocardial contraction (systole) and relaxation/filling
Ambulatory Rehabilitation Improves Exercise Capacity in Patients With Pulmonary Hypertension
 Journal of Cardiac Failure Vol. 17 No. 3 2011 Ambulatory Rehabilitation Improves Exercise Capacity in Patients With Pulmonary Hypertension BENJAMIN D. FOX, MB, BS, 1,2 MICHAEL KASSIRER, MD, 1 ISRAELA WEISS,
Journal of Cardiac Failure Vol. 17 No. 3 2011 Ambulatory Rehabilitation Improves Exercise Capacity in Patients With Pulmonary Hypertension BENJAMIN D. FOX, MB, BS, 1,2 MICHAEL KASSIRER, MD, 1 ISRAELA WEISS,
Anticoagulants in Atrial Fibrillation
 Anticoagulants in Atrial Fibrillation Starting and Stopping Them Safely Carmine D Amico, D.O. Overview Learning objectives Introduction Basic concepts Treatment strategy & options Summary 1 Learning objectives
Anticoagulants in Atrial Fibrillation Starting and Stopping Them Safely Carmine D Amico, D.O. Overview Learning objectives Introduction Basic concepts Treatment strategy & options Summary 1 Learning objectives
DVT/PE Management with Rivaroxaban (Xarelto)
") DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
New Treatments for Stroke Prevention in Atrial Fibrillation. John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013
 New Treatments for Stroke Prevention in Atrial Fibrillation John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013 Classification Paroxysmal atrial fibrillation (AF) Last < 7
New Treatments for Stroke Prevention in Atrial Fibrillation John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013 Classification Paroxysmal atrial fibrillation (AF) Last < 7
HEART HEALTH WEEK 3 SUPPLEMENT. A Beginner s Guide to Cardiovascular Disease HEART FAILURE. Relatively mild, symptoms with intense exercise
 WEEK 3 SUPPLEMENT HEART HEALTH A Beginner s Guide to Cardiovascular Disease HEART FAILURE Heart failure can be defined as the failing (insufficiency) of the heart as a mechanical pump due to either acute
WEEK 3 SUPPLEMENT HEART HEALTH A Beginner s Guide to Cardiovascular Disease HEART FAILURE Heart failure can be defined as the failing (insufficiency) of the heart as a mechanical pump due to either acute
Cardiovascular Disease and Maternal Mortality what do we know and what are the key questions?
 Cardiovascular Disease and Maternal Mortality what do we know and what are the key questions? AFSHAN HAMEED, MD, FACOG, FACC Associate Clinical Professor Maternal Fetal Medicine and Cardiology University
Cardiovascular Disease and Maternal Mortality what do we know and what are the key questions? AFSHAN HAMEED, MD, FACOG, FACC Associate Clinical Professor Maternal Fetal Medicine and Cardiology University