Pulmonary Arterial Hypertension (PAH)
|
|
|
- Dwayne Stewart
- 9 years ago
- Views:
Transcription
1 Pulmonary Arterial Hypertension (PAH)

2 Contents 1. Introduction 3 2. What is PAH? 4 3. Classification of PAH 5 4. How is PAH severity classified? 7 5. How common is PAH? 7 6. Why does PAH develop? 8 7. What are the symptoms of PAH? 9 8. Early diagnosis and intervention is crucial 9 9. How is PAH diagnosed? Screening in PAH: key to early diagnosis Echocardiography value as a screening tool Right heart catheterisation the diagnostic gold standard Assessing PAH: 6-minute walk test an evaluation of exercise capacity How is PAH treated? 16

3 1. Introduction Pulmonary arterial hypertension (PAH) is a serious disease of the arteries connecting the heart to the lungs (the pulmonary arteries). As PAH develops, blood flow through the pulmonary arteries is restricted and the right side of the heart is put under increasing strain to pump blood through to the lungs. This leads to the main symptoms of PAH breathlessness, chest tightness limited exercise capacity and fatigue. Untreated, PAH is a disease with a very poor prognosis. The early symptoms of PAH (such as breathlessness, chest tightness and fatigue) can be mild and are common to many other conditions. Reaching the diagnosis can be delayed and as a consequence patients with PAH may first present when the disease has already progressed. This brochure explains how PAH develops, describes the symptoms associated with this disease and outlines how it can be diagnosed and treated. Treatment is aimed at improving symptoms, exercise tolerance, long-term outcomes and quality of life. Until the mid-1980s there were limited treatment options for patients and PAH was associated with poor prognosis. Today, treatment options have improved the prognosis for patients with this condition. 3
 can be mild and are common to many other conditions.")
4 2. What is PAH? Pulmonary Arterial Hypertension (PAH) is a syndrome characterised by a progressive increase in pulmonary vascular resistance leading to right ventricular overload and eventually to right ventricular failure and premature death. 1 The increase in pulmonary vascular resistance is related to a number of progressive changes in the pulmonary arterioles, including: Vasoconstriction Obstructive remodelling of the pulmonary vessel wall through proliferation in the various layers of the blood vessel wall (smooth muscle cell and endothelial cell proliferation) Inflammation In-situ thrombosis The main histological features include medial hypertrophy, intimal thickening, adventitial thickening, plexiform lesions and in-situ thrombosis (Figure 1). The plexifom lesion represents a focal proliferation of endothelial and smooth muscle cells and is pathognomonic of PAH. PAH is defined as a sustained elevation of mean pulmonary arterial pressure to more than 25 mmhg at rest or to more than 30 mmhg while exercising, with a normal pulmonary wedge pressure ( 15 mmhg). 2 In most cases the earliest symptom is dyspnoea on physical exertion. Other symptoms include syncope or near syncope, fatigue and peripheral oedema. 3,4 Chest tightness and pain similar to angina may occur, particularly on physical exertion. Figure 1. 4

5 3. Classification of PAH Pulmonary Arterial Hypertension (PAH) represents Group 1 within the Pulmonary Hypertension WHO clinical classification system (Venice 2003 revision) and is one of five such groups. The groups are divided based on aetiology. 5 Group I. Pulmonary arterial hypertension (PAH) Idiopathic (IPAH) Familial (FPAH) Associated with (APAH): Connective tissue disease Congenital systemic-to-pulmonary shunts Portal hypertension HIV infection Drugs and toxins Other (thyroid disorders, glycogen storage disease, Gaucher s disease, hereditary haemorragic telangiectasia, haemoglobinopathies, myeloproliferative disorders, splenectomy) Associated with significant venous or capillary involvement Pulmonary veno-occlusive disease (PVOD) Pulmonary capillary haemangiomatosis (PCH) Persistent pulmonary hypertension of the newborn (PPHN) Group II. Pulmonary hypertension associated with left heart diseases Group III. Pulmonary hypertension associated with respiratory diseases and/or hypoxemia (including chronic obstructive pulmonary disease) Group IV. Pulmonary hypertension due to chronic thrombotic and/or embolic disease Group V. Miscellaneous group eg. sarcoidosis, histiocytosis X and lymphangiomatosis Idiopathic PAH (IPAH), which by definition has no identifiable underlying cause, is one of the more common types of PAH. Familial PAH (FPAH) accounts for at least 6% of cases of IPAH and mutations in the bone morphogenetic protein receptor 2 (BMPR2) have been identified in the majority of cases of FPAH. 6,7 PAH can also be associated with a number of conditions (Associated Pulmonary Arterial Hypertension APAH), which together account for most other cases of PAH. These conditions include: 1. Connective Tissue Diseases including systemic sclerosis (scleroderma) and systemic lupus erythematosus (SLE) 2. Congenital Heart Disease including Eisenmenger s syndrome 3. Human immunodeficiency virus (HIV) infection 4. Sickle Cell Disease 5
")
6 PAH is also a rare side effect of certain anorexigenic agents, such as fenfluramine and dexfenfluramine. However, the incidence of drug-induced PAH is decreasing as these agents are no longer available. 1. PAH associated with connective tissue disease PAH is a well-recognised complication of connective tissue diseases such as systemic sclerosis and SLE and in affected patients may also occur in association with interstitial lung disease. The prevalence of PAH in patients with systemic sclerosis has been reported to be up to 16% 8 and in systemic sclerosis patients, pulmonary complications, such as interstitial lung disease and PAH, are now the leading causes of death. Patients with PAH associated with systemic sclerosis have a particularly poor prognosis compared to those with systemic sclerosis without PAH PAH associated with congenital heart disease Congenital heart disease is relatively common, affecting around 1% of the population. Within this population 15% will go on to develop PAH. 10 As determined by the level of pulmonary vascular resistance, the most severe form of PAH is Eisenmenger s syndrome, which is associated with the reversal of an initial left to right shunt causing cyanosis and limited exercise capacity PAH associated with HIV infection PAH is a rare (estimated prevalence in patients with HIV: 0.5%) 12 but relatively well-documented complication of HIV infection. With the advent of highly active anti-retroviral therapy (HAART) and markedly improved survival, PAH and other non-infectious manifestations of HIV infection are increasingly responsible for HIV-associated morbidity and poor prognosis. In patients with HIV, the HIV-1 envelope glycoprotein GP120 may stimulate the production of endothelin by macrophages. 13 HIV-associated PAH shows a similar clinical picture to IPAH and seems to be independent of the degree of immunosuppression. 4. PAH associated sickle cell disease Sickle cell disease (SCD) is a genetic disorder of the haemoglobin which results in a chronic haemolytic anaemia. Over time and due to the chronic haemolysis the vasculature becomes damaged and pulmonary hypertension can develop. The prevalence of PAH in sickle cell patients is 20 40%. 14 The two year mortality rate of pulmonary hypertension related to SCD is reported up to 50% and is one of the leading causes of death in SCD. 15 6

7 4. How is PAH severity classified? PAH is usually classified according to a functional class system initially devised by the New York Heart Association (NYHA) for Chronic Heart Failure and then adapted for PAH by the World Health Organisation (WHO). WHO functional class (WHO FC) measures the severity of PAH and reflects the impact on a patient s life in terms of physical activity and symptoms. There are four classes; class I being the least severe and class IV being the most advanced (Table 1). 4 Table 1. Class Class I Class II Class III Class IV Symptomatic profile Patients with pulmonary hypertension but without resulting limitation of physical activity. Ordinary physical activity does not cause dyspnoea or fatigue, chest pain or near syncope. Patients with pulmonary hypertension resulting in slight limitation of physical activity. They are comfortable at rest. Ordinary physical activity causes undue dyspnoea or fatigue, chest pain or near syncope. Patients with pulmonary hypertension resulting in marked limitation of physical activity. They are comfortable at rest. Less than ordinary activity causes undue dyspnoea or fatigue, chest pain or near syncope. Patients with pulmonary hypertension with inability to carry out any physical activity without symptoms. These patients manifest signs of right heart failure. Dyspnoea and/or fatigue may even be present at rest. Discomfort is increased by any physical activity. 5. How common is PAH? Although PAH is a rare disease, with an estimated prevalence of cases per million, 16 the prevalence of PAH in certain at-risk groups is substantially higher. For example, in HIV-infected patients the prevalence is 0.5%, 12 in patients with sickle cell disease the prevalence is 20 40% 14 and in patients with systemic sclerosis the prevalence has been reported to be up to 16%. 8 Idiopathic PAH is more common in young women with a mean age of diagnosis of 36 years. 3 However it can occur at any age. 3 Idiopathic PAH is twice as common in women as in men. 3 Although the true relative prevalence of IPAH, FPAH and APAH are unknown, it is likely that IPAH accounts for at least 40% of cases, and APAH for most of the remaining cases. 17 Due to the non-specific nature of the symptoms, PAH is most frequently diagnosed when patients have reached a more advanced stage of disease (WHO Functional Class III and IV), 17 suggesting that the true prevalence may be higher than documented in the literature. 7
. 4 Table 1.")
8 6. Why does PAH develop? The exact cause behind the development of PAH remains unknown. However, research has led to a better understanding of the underlying mechanisms. PAH is recognised as a complex, multi-factorial condition involving numerous biochemical pathways and different cell types. Endothelial dysfunction is believed to occur early on in disease pathogenesis, leading to endothelial and smooth muscle cell proliferation and structural changes or remodelling of the pulmonary vascular bed resulting in an increase in pulmonary vascular resistance. Vascular remodeling itself involves all layers of the vessel wall and is characterised by proliferative and obstructive changes involving many cell types, including endothelial, smooth muscle and fibroblasts. Inflammatory cells and platelets may also play a significant role in PAH. Endothelial cell dysfunction results in reduced production of vasodilators,such as nitric oxide (NO) and prostacyclin, and over production of vasoconstrictors, such as thromboxane A2 and endothelin-1 (ET-1). ET-1, NO and prostacyclin have been the principal focus of research into new treatment options for patients with PAH. Endothelin Endothelin is produced by the endothelial cells and is essential for maintenance of normal vascular tone and function. However, high levels of endothelin are seen in patients with PAH due to various aetiologies and correlate with disease severity, 21 resulting in a number of detrimental effects, primarily in the vasculature: 3 Fibrosis Hypertrophy and proliferation of cells, which can lead to thickening, narrowing and occlusion of blood vessels Inflammation Vasoconstriction Endothelin binds to 2 receptors, ET A and ET B. Both receptors are implicated in PAH and mediate the deleterious effects of endothelin. 22 Endothelin receptor antagonism can either mitigate the effects of only one (single ET A antagonist) or both (dual ET A and ET B receptor antagonist) receptor types. Prostacyclin Prostacyclin is a potent vasodilator as well as an inhibitor of platelet activation. It is believed that patients with PAH have low levels of prostacyclin, which could result in vasoconstriction in the pulmonary vasculature and a tendency for smooth muscle cell proliferation and platelet activation, encouraging the formation of thrombi in both the micro-circulation and the pulmonary arteries Therapy with synthetic forms of prostacyclin can help to correct this deficiency, although administering this form of treatment is complex

9 Nitric oxide Nitric oxide is an endothelial-derived substance that, like prostacyclin, is a potent vasodilator and also possesses anti-proliferative properties. PAH patients appear to produce insufficient NO and this may contribute to the development of PAH. 3 The vasodilatory effect of NO is mediated by cgmp, which is rapidly degraded by phosphodiesterases. The inhibition of the degradation of cgmp with phosphodiesterase 5 inhibitors promotes the accumulation of intracellular cgmp, resulting in vasodilatation What are the symptoms of PAH? The changes to the pulmonary vasculature described above lead to the typical symptoms of PAH. The symptoms are caused by the high resistance to blood flow through the lungs and result in increased stress on the heart. This can severely impact the ability to exercise or carry out normal daily activities. Common early symptoms include: 3,4 Breathlessness (dyspnoea), particularly on physical activity Fatigue Dizziness Syncope, also on physical activity (rare) Peripheral oedema Chest pain, again particularly during physical activity The symptoms may not be obvious at first and are often attributed to more common conditions such as asthma, general fatigue, or lack of physical fitness. Over time, however, they can become more severe and begin to limit normal activities. As the disease progresses, some patients may experience constant dyspnoea and fatigue so that even simple tasks such as getting dressed and walking short distances become difficult. 8. Early diagnosis and intervention is crucial Early diagnosis and intervention is important in PAH as without treatment the median survival of patients is 2.8 years, which is comparable with some malignancies However, diagnosis is complex and can be delayed for months or even years as early PAH symptoms are mild and non-specific. This means that PAH is frequently not recognised until the disease is relatively advanced. 3 In fact, the average time from onset to diagnosis is estimated to be approximately 2 years. 17 Although patients progress at different rates, mildly symptomatic PAH patients still have a devastating condition, which can progress rapidly. Recognising and treating PAH early is therefore crucial to changing the course of the disease. Marked improvements in prognosis and survival have been shown for patients who begin targeted therapy in less severe stages of PAH (WHO FCI/II) compared with those in a more severe stage (WHO FCIII/IV). 33 9

10 9. How is PAH diagnosed? The non-specific nature of symptoms associated with PAH means that the diagnosis cannot be made on symptoms alone. A series of investigations is required to make an initial diagnosis, to refine that diagnosis in terms of clinical class of pulmonary hypertension and to evaluate the degree of functional and haemodynamic impairment (Figure 2). Consequently, it can be useful to adopt a four stage approach: 1. Clinical suspicion of pulmonary hypertension Breathlessness (dyspnoea) without overt signs of specific heart or lung disease Screening of patients with associated conditions (Connective Tissue Disease, Congenital Heart Disease, HIV, Sickle Cell Disease) Incidental findings on examination for other clinical reasons 2. Detection of pulmonary hypertension ECG (echocardiogram) Doppler echocardiogram (Figure 2) Chest radiograph, may show evidence of cardiomegaly and enlarged pulmonary arteries (Figure 3) 3. Identify other causes of pulmonary hypertension Pulmonary function tests (PFTs) and arterial blood gas samples Ventilation and perfusion lung scan High resolution computed tomography (HRCT) Pulmonary angiography 4. PAH evaluation and classification (type, functional capacity, haemodynamics) Blood tests and immunology, HIV test, abdominal ultrasound scan 6 minute walk test (6-MWT) and peak VO2 Right heart catheterisation and vasoreactivity testing 10
 without overt signs of specific heart or lung disease Screening of patients with associated conditions (Connective Tissue")
11 Figure 2. Figure 3. 11
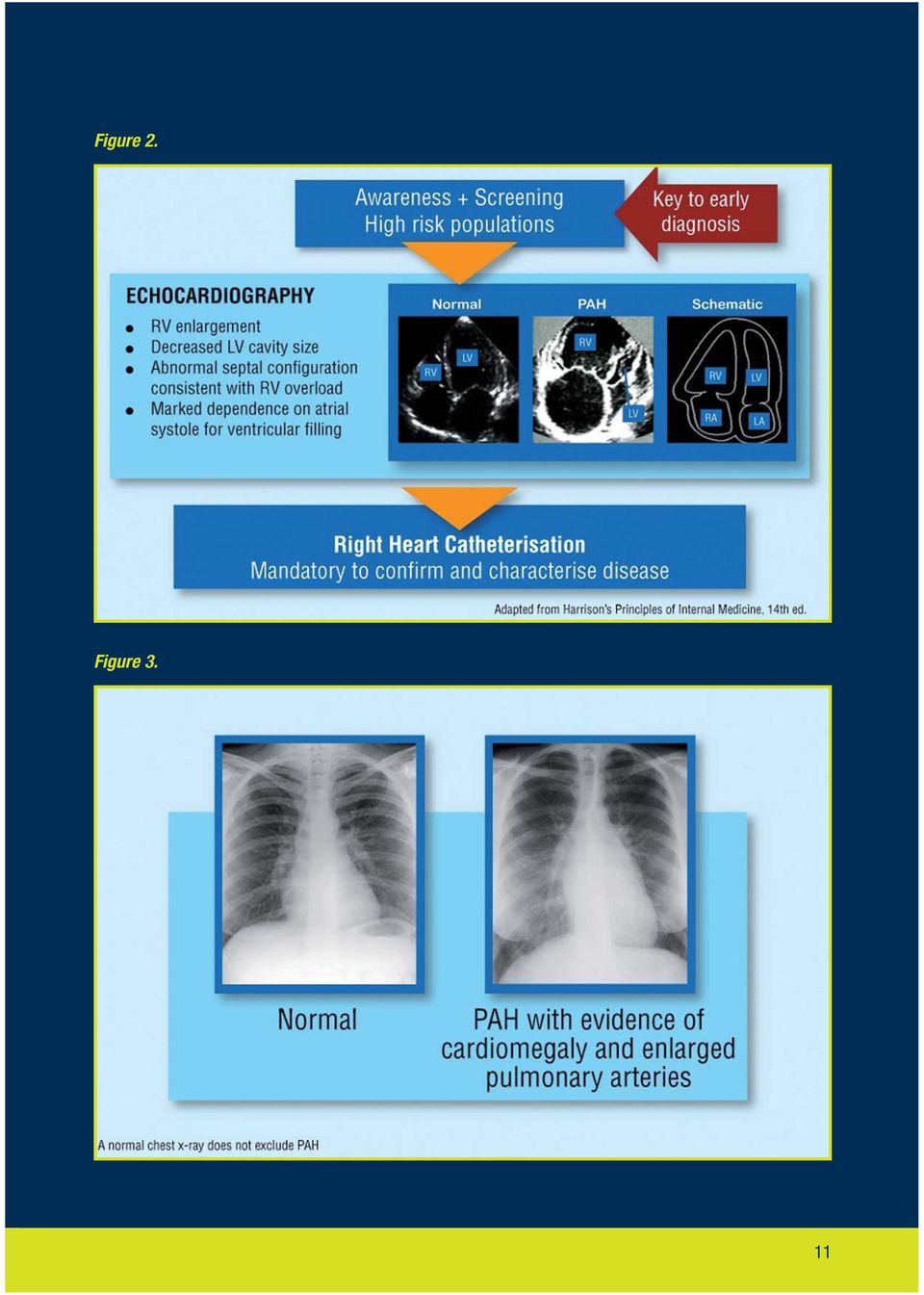
12 10. Screening in PAH: key to early diagnosis The key to early diagnosis is introducing screening for high risk patient populations if they are asymptomatic. High risk patient populations include: Family members of a patient with familial Pulmonary Arterial Hypertension (FPAH) Patients with systemic sclerosis (SSc) Patients with HIV Patients with portopulmonary hypertension (PoPH) The results of a disease registry in France indicated that without screening, the majority of patients were diagnosed in a more severe stage of PAH (WHO FC III/IV), and only 25% of patients were in early stage PAH (WHO FC I/II). 17 Furthermore, the results of a French national screening program in a high-risk population indicated that it is possible to detect Pulmonary Arterial Hypertension (PAH) in an earlier stage in a high-risk population 34 (Figure 4). International guidelines now recommend annual screening high-risk groups with Doppler echocardiography. 2,8,35 Doppler echocardiography is currently the most effective method for screening, however, for a definitive diagnosis right heart catheterisation has to be performed. Figure 4. No screening 17 With screening 34 12
.")
13 11. Echocardiography value as a screening tool Transthoracic Doppler-echocardiography (TTE) is a non-invasive screening test for pulmonary arterial hypertension. TTE is able to estimate pulmonary arterial systolic pressure, which is equivalent to right ventricular systolic pressure in the absence of pulmonary outflow obstruction. It can provide additional information about the cause and consequences of PH, including right and left ventricular dimensions and function, heart valve abnormalities, right ventricular ejection and left ventricular filling characteristics and presence of a pericardial effusion. In the initial investigation of patients with PAH it is important to obtain adequate images of the right heart. Pulmonary arterial pressure can be estimated from the tricuspid regurgitant (TR) jet (Figure 5). Figure 5. 13

14 12. Right heart catheterisation the diagnostic gold standard Right heart catheterisation is required for a definitive diagnosis of PAH (Figure 6 and 7) 3,4 to assess the severity of haemodynamic impairment and to test the vasoreactivity of the pulmonary circulation. The following parameters should always be assessed: right atrial pressure (RAP), pulmonary arterial pressure (PAP [systolic, diastolic and mean]), pulmonary capillary wedge pressure (PCWP), cardiac output/index, pulmonary (PVR) and systemic vascular resistance, blood pressure and arterial and mixed venous oxygen saturation. PAH is defined as a sustained elevation of mean pulmonary arterial pressure to >25 mmhg at rest or to >30 mmhg while exercising, with a mean pulmonary wedge pressure or left ventricular end-diastolic pressure of 15 mmhg and pulmonary vascular resistance of 3 woods units. 2 A positive vasoreactive response is defined as a reduction in mean pulmonary artery pressure (mpap) 10 mmhg to reach an absolute value of mpap 40 mmhg with an increase or unchanged cardiac output. A positive response is shown in only 10 15% of patients, and sustained response is shown in even fewer (less than 7%). 1 Figure 6. 14
![The following parameters should always be assessed: right atrial pressure (RAP), pulmonary arterial pressure (PAP [systolic, diastolic and mean]), pulmonary capillary wedge pressure (PCWP), cardiac](/docs-images/49/17590535/images/page_14.jpg "output/index, pulmonary (PVR) and systemic vascular resistance, blood pressure and arterial and mixed venous oxygen saturation.")
15 Figure Assessing PAH: 6-minute walk test an evaluation of exercise capacity In patients with PAH, the 6-MWT to evaluate exercise capacity is reflective of activities of daily living; 36 the distance a PAH patient can walk in 6 minutes is a critical endpoint in studies evaluating the benefit of different therapeutic options. To allow meaningful comparisons, it is important that the 6-MWT be performed under supervision according to a standardised protocol. 37 A 30 m corridor should be available, marked at 3 m intervals The patient should rest for at least 10 minutes prior to the test and should not have performed any rigorous exercise within the previous 2 hours The patient should be asked to rate their baseline dyspnoea The patient should be instructed to walk to their maximum capacity but not to run or jog; they should be permitted to rest as necessary The supervisor should count each lap as the patient finishes it The patient should be asked to rate their dyspnoea at the end of the test The test should be repeated at approximately the same time of day on each occasion 15

16 14. How is PAH treated? There is currently no cure for PAH but advances in understanding how the disease develops (see section: Why does PAH develop?) means that there are now treatments available which have helped to improve prognosis for patients with this disease. Prognosis is influenced by the status of WHO FC when treatment is started patients who start therapy in functional class I or II demonstrate a better prognosis than those whose therapy is started in more severe stages (WHO FC III or IV). 33 Early treatment may delay disease progression By recognising and treating patients as early as possible, disease progression may be delayed. Without treatment, patients in WHO FC II can rapidly deteriorate within 6 months to more advanced Pulmonary Arterial Hypertension (PAH) as evidenced by progression of symptoms. 38 Treatment options have progressed considerably in the last decade, especially those which target the underlying mechanisms of the disease. The main medical treatment options for patients with PAH are: 39 Treatments that are routinely used but with little evidence of a positive impact on the disease progression Anticoagulants, such as warfarin, to address the observed thrombotic changes and potential predisposition in the pulmonary microcirculation for in-situ thrombosis Calcium-channel blockers (CCBs). Less than 10% of IPAH patients benefit from CCB therapy. This figure is even lower in other forms of PAH. If not used in appropriate candidates (patients with demonstrated vasoreactivity during right heart catheterisation), CCBs can decrease cardiac output and systemic vascular resistance without any improvement in PAP and PVR and therefore may be deleterious 1 Diuretics, for treatment of right heart failure Oxygen therapy, to maintain oxygen saturation at >90% at all times 16
. 33 Early treatment may delay disease progression By recognising and treating patients as early as possible, disease progression may be delayed.")
17 Treatments that have been specifically studied in PAH Endothelin receptor antagonists endothelin is implicated in the pathogenesis of PAH through actions on the pulmonary vasculature. Endothelin is found to be elevated in patients with PAH and levels of endothelin are directly related to disease severity and prognosis. Endothelin receptor antagonists (ERAs) are oral treatments that either block the ET A receptor alone or both the ET A and ET B receptors 22 Phosphodiesterase 5 inhibitors oral agents which induce relaxation and antiproliferative effects on vascular smooth muscle cells by preventing the reduction in levels of cgmp 29 Prostacyclin analogues may be delivered by continuous intravenous or subcutaneous infusion or via an intermittent nebuliser 39 In very severe cases surgical options may be considered: Balloon atrial septostomy Heart and lung transplantation However, the use of transplantation is constrained by the limited number of donor organs. 17

18 References 1. Sitbon O, Humbert M, Jaïs X et al. Long-term response to calcium channel blockers in idiopathic pulmonary arterial hypertension. Circulation 2005; 111: Galiè N, Torbicki A, Barst RJ, et al. Guidelines on diagnosis and treatment of pulmonary arterial hypertension: The Task Force on Diagnosis and Treatment of Pulmonary Arterial Hypertension of the European Society of Cardiology. Eur Heart J 2004; 25: Gaine SP, Rubin LJ. Primary Pulmonary Hypertension. Lancet 1998; 352: Barst RJ, McGoon M, Torbicki A et al. Diagnosis and differential assessment of pulmonary arterial hypertension. J Am Coll Cardiol 2004; 43(Suppl S): 40S 47S. 5. Simonneau G, Galiè N, Rubin LJ et al. Clinical classification of pulmonary hypertension. J Am Coll Cardiol 2004; 43(Suppl S): 5S 12S. 6. Lane KB, Machado RD, Pauciulo MW et al. Heterozygous germline mutations in BMPR2, encoding a TGFbeta receptor, cause familial primary pulmonary hypertension. The International PPH Consortium. Nat Genet 2000; 26(1): Deng Z, Morse JH, Slager SL et al. Familial primary pulmonary hypertension (gene PPH1) is caused by mutations in the bone morphogenetic protein receptor-ii gene. Am J Hum Genet 2000; 67(3): McGoon M, Gutterman D, Steen V et al. Screening, early detection, and diagnosis of pulmonary arterial hypertension: ACCP evidence-based clinical practice guidelines. Chest 2004; 126(1 Suppl) :14S 34S. 9. Koh ET, Lee P, Gladman DD, Abu-Shakra M. Pulmonary hypertension in systemic sclerosis: an analysis of 17 patients. Br J Rheumatol 1996; 35(10): Beghetti M, Barst RJ, Naeije R, Rubin LJ. Pulmonary arterial hypertension related to congenital heart disease. Elsevier Diller GP, Dimopoulos K, Okonko D et al. Exercise intolerance in adult congenital heart disease: comparative severity, correlates, and prognostic implication. Circulation 2005; 112(6): Sitbon O, Lascoux-Combe C, Delfraissy JF et al. Prevalence of HIV-related pulmonary arterial hypertension in the current antiretroviral therapy era. AJRCCM 2008; 177: Sitbon O, Gressin V, Speich R et al. Bosentan for the treatment of human immunodeficiency virusassociated pulmonary arterial hypertension. Am J Respir Crit Care Med 2004; 170(11): Lin EE, Rodgers GP, Gladwin MT. Hemolytic anemia-associated pulmonary hypertension in sickle cell disease. Curr Hematol Rep. 2005; 4(2): Castro, O. Hoque M, Brown B.D. Pulmonary hypertension in sickle cell disease: cardiac catheterisation results and survival. Blood 2003; 101: Peacock AJ. Treatment of pulmonary hypertension. BMJ 2003; 326: Humbert M, Sitbon O, Chaouat A et al. Pulmonary Arterial Hypertension in France: Results from a National Registry. Am J Respir Crit Care Med 2006; 173(9): Stewart DJ, Levy RD, Cernacek P et al. Increased plasma endothelin-1 in pulmonary hypertension: marker or mediator of disease? Ann Inter Med 1991; 114: Vancheeswaran R, Magoulas T, Efrat G et al. Circulating endothelin-1 levels in systemic sclerosis subsets-a marker of fibrosis or vascular dysfunction? J Rheum 1994; 21: Yoshibayashi M, Nishioka K, Nakao K et al. Plasma endothelin concentrations in patients with pulmonary hypertension associated with congenital heart defects. Evidence for increased production of endothelin in pulmonary circulation. Circulation 1991; 84:
: 40S 47S. 5. Simonneau G, Galiè N, Rubin LJ et al.")
19 21. Galie N, Grigioni F, Bacchi-Reggiani L et al. Relation of endothelin-1 to survival in patients with primary pulmonary hypertension. Eur J Clin Inves 1996; 26: A Channick RN, Simonneau G, Sitbon O et al. Effects of the dual endothelin-receptor antagonist bosentan in patients with pulmonary hypertension: a randomised placebo-controlled study. Lancet 2001; 358: MacGreggor AJ, Canavan R, Knight C et al. Pulmonary hypertension in systemic sclerosis: risk factors for progression and consequences for survival. Rheumatology (Oxford) 2001; 40(4): Loyd JE, Butler MG, Foround TM et al. Genetic anticipation and abnormal gender ratio at birth in familial primary pulmonary hypertension. Am J Respir Crit Care Med 1995; 152: Rubin LJ. Therapy of pulmonary hypertension: the evolution from vasodilators to antiproliferative agents. Am J Respir Crit Care Med 2002; 166: Ono F, Nagaya N, Okamura H et al. Effect of orally active prostacyclin analogue on survival in patients with chronic thromboembolic pulmonary hypertension without major vessel obstruction. Chest 2003; 123: Galie N, Manes A, Branzi A. Emerging medical therapies for pulmonary arterial hypertension. Prog Cardiov Dis 2002: 45: Clapp LH, Finney P, Turcato S et al. Differential effects of stable prostacyclin analogs on smooth muscle proliferation and cyclic AMP generation in human Pulmonary artery. Am J Resp Cell Mol Biol 2002; 26: Galiè N, Ghofrani HA, Torbicki A et al. Sildenafil citrate therapy for pulmonary arterial hypertension. N Engl J Med 2005; 353: D'Alonzo GE, Barst RJ, Ayres SM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. 1991; 115: Kato I, Severson RK and Schwartz AG. Conditional median survival of patients with advanced carcinoma: surveillance, epidemiology, and end results data. Cancer 2001; 92: Bjoraker JA, Ryu JH, Edwin MK, et al. Prognostic significance of histopathologic subsets in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med 1998; 157: Sitbon O, Humbert M, Nunes H, et al. Long-term intravenous epoprostenol infusion in primary pulmonary hypertension: prognostic factors and survival. J Am Coll Cardiol 2002; 40: Hachulla E, Gressin V, Guillevin L, et al. Early detection of pulmonary arterial hypertension in systemic sclerosis: a French nationwide prospective multicenter study. Arthritis Rheum 2005; 52: Hachulla E and Coghlan JG. A new era in the management of pulmonary arterial hypertension related to scleroderma: endothelin receptor antagonism. Ann Rheum Dis 2004; 63: Solway S, Brooks D, Lacasse Y, Thomas S. A qualitative systematic overview of the measurement properties of functional walk tests used in the cardiorespiratory domain. Chest 2001; 119(1): ATS. ATS statement: guidelines for the 6-minute walk test. Am J Respir Crit Care Med 2002; 166: Galiè N, Rubin LJ, Hoeper MM et al. Treatment of patients with mildly symptomatic pulmonary arterial hypertension with bosentan (EARLY study): a double-blind, randomised controlled trial. Lancet 2008; 371: Humbert M, Sitbon O, Simonneau G. Treatment of pulmonary arterial hypertension. N Engl J Med 2004; 351:
 2001; 40(4): 453 459. 24. Loyd JE, Butler MG, Foround TM et al. Genetic anticipation and abnormal gender ratio at birth in familial primary pulmonary hypertension.")
20 For further information visit Actelion Pharmaceuticals Ltd. Gewerbestrasse 16 CH-4123 Allschwil Switzerland

NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Health Technology Appraisal. Drugs for the treatment of pulmonary arterial hypertension
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Drugs for the treatment of Remit / Appraisal objective: Final scope To appraise the clinical and cost effectiveness of
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Drugs for the treatment of Remit / Appraisal objective: Final scope To appraise the clinical and cost effectiveness of
PULMONARY HYPERTENSION. Charles A. Thompson, M.D., FACC, FSCAI Cardiovascular Institute of the South Zachary, Louisiana
 PULMONARY HYPERTENSION Charles A. Thompson, M.D., FACC, FSCAI Cardiovascular Institute of the South Zachary, Louisiana What is Pulmonary Hypertension? What is normal? Pulmonary artery systolic pressure
PULMONARY HYPERTENSION Charles A. Thompson, M.D., FACC, FSCAI Cardiovascular Institute of the South Zachary, Louisiana What is Pulmonary Hypertension? What is normal? Pulmonary artery systolic pressure
Pulmonary Artery Hypertension
 Pulmonary Artery Hypertension Janet M. Pinson, RN, MSN, ACNP Maureen P. Flattery, RN, MS, ANP Virginia Commonwealth University Health System Richmond, VA Pulmonary artery hypertension (PAH) is defined
Pulmonary Artery Hypertension Janet M. Pinson, RN, MSN, ACNP Maureen P. Flattery, RN, MS, ANP Virginia Commonwealth University Health System Richmond, VA Pulmonary artery hypertension (PAH) is defined
PAH has an incidence
 Pulmonary Arterial Hypertension: A Serious Problem Pulmonary arterial hypertension (PAH) is a serious disease with significant morbidity and mortality and no cure. In this article, Dr. Porhownik and Dr.
Pulmonary Arterial Hypertension: A Serious Problem Pulmonary arterial hypertension (PAH) is a serious disease with significant morbidity and mortality and no cure. In this article, Dr. Porhownik and Dr.
Corporate Medical Policy
 Corporate Medical Policy Pulmonary Hypertension, Drug Management File Name: Origination: Last CAP Review: Next CAP Review: Last Review: pulmonary_hypertension_drug_management 06/1998 3/2015 3/2016 3/2015
Corporate Medical Policy Pulmonary Hypertension, Drug Management File Name: Origination: Last CAP Review: Next CAP Review: Last Review: pulmonary_hypertension_drug_management 06/1998 3/2015 3/2016 3/2015
Pulmonary Arterial Hypertension: Review and Updates. Is it Primary vs Secondary Pulmonary Hypertension? No!! Dated Nomenclature. Veronica Franco, MD
 Pulmonary Arterial Hypertension: Review and Updates Veronica Franco, MD Section of Pulmonary Hypertension Section of Heart Failure and Transplantation Ohio State University Is it Primary vs Secondary Pulmonary
Pulmonary Arterial Hypertension: Review and Updates Veronica Franco, MD Section of Pulmonary Hypertension Section of Heart Failure and Transplantation Ohio State University Is it Primary vs Secondary Pulmonary
1. Phosphodiesterase Type 5 Enzyme Inhibitors: Sildenafil (Revatio), Tadalafil (Adcirca)
, Tadalafil (Adcirca)") This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutic
This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutic
Pharmacy Policy Bulletin
 Pharmacy Policy Bulletin Title: Policy #: Pulmonary Arterial Hypertensive (PAH) agents Rx.01.83 Application of pharmacy policy is determined by benefits and contracts. Benefits may vary based on product
Pharmacy Policy Bulletin Title: Policy #: Pulmonary Arterial Hypertensive (PAH) agents Rx.01.83 Application of pharmacy policy is determined by benefits and contracts. Benefits may vary based on product
PULMONARY ARTERIAL HYPERTENSION AGENTS
 Approvable Criteria: PULMONARY ARTERIAL HYPERTENSION AGENTS Brand Name Generic Name Length of Authorization Revatio Sildenafil citrate Calendar Year Adcirca Tadalafil Calendar Year Letairis Ambrisentan
Approvable Criteria: PULMONARY ARTERIAL HYPERTENSION AGENTS Brand Name Generic Name Length of Authorization Revatio Sildenafil citrate Calendar Year Adcirca Tadalafil Calendar Year Letairis Ambrisentan
Riociguat Clinical Trial Program
 Riociguat Clinical Trial Program Riociguat (BAY 63-2521) is an oral agent being investigated as a new approach to treat chronic thromboembolic pulmonary hypertension (CTEPH) and pulmonary arterial hypertension
Riociguat Clinical Trial Program Riociguat (BAY 63-2521) is an oral agent being investigated as a new approach to treat chronic thromboembolic pulmonary hypertension (CTEPH) and pulmonary arterial hypertension
PAH in. Registry to Evaluate Early and Long-Term PAH Disease Management
 PAH in Registry to Evaluate Early and Long-Term PAH Disease Management Ioana R. Preston, MD Co-Director, Pulmonary Hypertension Center Tufts Medical Center, Boston, MA Background What is REVEAL? Multi-center,
PAH in Registry to Evaluate Early and Long-Term PAH Disease Management Ioana R. Preston, MD Co-Director, Pulmonary Hypertension Center Tufts Medical Center, Boston, MA Background What is REVEAL? Multi-center,
Pulmonary Arterial Hypertension. Matt Hegewald, MD FCCP St Charles Medical Center Intermountain Medical Center University of Utah
 Pulmonary Arterial Hypertension Matt Hegewald, MD FCCP St Charles Medical Center Intermountain Medical Center University of Utah Intermountain Pulmonary Arterial Hypertension Program Outline Causes of
Pulmonary Arterial Hypertension Matt Hegewald, MD FCCP St Charles Medical Center Intermountain Medical Center University of Utah Intermountain Pulmonary Arterial Hypertension Program Outline Causes of
The Global Alliance against Chronic Respiratory Diseases
 The Global Alliance against Chronic Respiratory Diseases Pulmonary hypertension Dr Marc Humbert What is the burden of pulmonary hypertension? The true burden of pulmonary hypertension is currently unknown
The Global Alliance against Chronic Respiratory Diseases Pulmonary hypertension Dr Marc Humbert What is the burden of pulmonary hypertension? The true burden of pulmonary hypertension is currently unknown
Pulmonary Arterial Hypertension. Mark Rumbak, MD Professor of Medicine Morsani College of Medicine University of South Florida
 Pulmonary Arterial Hypertension Mark Rumbak, MD Professor of Medicine Morsani College of Medicine University of South Florida PAH Disease State Module Outline Background and definition Clinical classification
Pulmonary Arterial Hypertension Mark Rumbak, MD Professor of Medicine Morsani College of Medicine University of South Florida PAH Disease State Module Outline Background and definition Clinical classification
2. Background This drug had not previously been considered by the PBAC.
 PUBLIC SUMMARY DOCUMENT Product: Ambrisentan, tablets, 5 mg and 10 mg, Volibris Sponsor: GlaxoSmithKline Australia Pty Ltd Date of PBAC Consideration: July 2009 1. Purpose of Application The submission
PUBLIC SUMMARY DOCUMENT Product: Ambrisentan, tablets, 5 mg and 10 mg, Volibris Sponsor: GlaxoSmithKline Australia Pty Ltd Date of PBAC Consideration: July 2009 1. Purpose of Application The submission
Statement on Disability: Pulmonary Hypertension
 Statement on Disability: Pulmonary Hypertension Ronald J. Oudiz, MD and Robyn J. Barst, MD on behalf of Pulmonary Hypertension Association The Scientific Leadership Council of the Pulmonary Hypertension
Statement on Disability: Pulmonary Hypertension Ronald J. Oudiz, MD and Robyn J. Barst, MD on behalf of Pulmonary Hypertension Association The Scientific Leadership Council of the Pulmonary Hypertension
Pulmonary Arterial Hypertension: Assessment of disease s severity
 Pulmonary Arterial Hypertension: Assessment of disease s severity Carmine Dario Vizza Dept. Cardiovascular and Respiratory Diseases La Sapienza University of Rome e-mail : [email protected] Pulmonary
Pulmonary Arterial Hypertension: Assessment of disease s severity Carmine Dario Vizza Dept. Cardiovascular and Respiratory Diseases La Sapienza University of Rome e-mail : [email protected] Pulmonary
Type II Pulmonary Hypertension: Pulmonary Hypertension due to Left Heart Disease
 Heart Failure Center Hadassah University Hospital Type II Pulmonary Hypertension: Pulmonary Hypertension due to Left Heart Disease Israel Gotsman MD The Heart Failure Center, Heart Institute Hadassah University
Heart Failure Center Hadassah University Hospital Type II Pulmonary Hypertension: Pulmonary Hypertension due to Left Heart Disease Israel Gotsman MD The Heart Failure Center, Heart Institute Hadassah University
Acknowledgements. PAH in Children: Natural History. The Sildenafil Saga
 The Sildenafil Saga David L. Wessel, MD Executive Vice President Chief Medical Officer Ikaria Distinguished Professor of Critical Care Children s National Medical Center Washington, DC, USA Acknowledgements
The Sildenafil Saga David L. Wessel, MD Executive Vice President Chief Medical Officer Ikaria Distinguished Professor of Critical Care Children s National Medical Center Washington, DC, USA Acknowledgements
Guidelines on diagnosis and treatment of pulmonary arterial hypertension
 European Heart Journal (2004) 25, 2243 2278 ESC Guidelines Guidelines on diagnosis and treatment of pulmonary arterial hypertension The Task Force on Diagnosis and Treatment of Pulmonary Arterial Hypertension
European Heart Journal (2004) 25, 2243 2278 ESC Guidelines Guidelines on diagnosis and treatment of pulmonary arterial hypertension The Task Force on Diagnosis and Treatment of Pulmonary Arterial Hypertension
FREEDOM C: A 16-Week, International, Multicenter, Double-Blind, Randomized, Placebo-Controlled Comparison of the Efficacy and Safety of Oral UT-15C
 FREEDOM C: A 16-Week, International, Multicenter, Double-Blind, Randomized, Placebo-Controlled Comparison of the Efficacy and Safety of Oral UT-15C SR in Combination with an ERA and/or a PDE-5 Inhibitor
FREEDOM C: A 16-Week, International, Multicenter, Double-Blind, Randomized, Placebo-Controlled Comparison of the Efficacy and Safety of Oral UT-15C SR in Combination with an ERA and/or a PDE-5 Inhibitor
Liver Function Essay
 Liver Function Essay Name: Quindoline Ntui Date: April 20, 2009 Professor: Dr. Danil Hammoudi Class: Anatomy and Physiology 2 Liver function The human body consist of many highly organize part working
Liver Function Essay Name: Quindoline Ntui Date: April 20, 2009 Professor: Dr. Danil Hammoudi Class: Anatomy and Physiology 2 Liver function The human body consist of many highly organize part working
CLINICAL POLICY Department: Medical Management Document Name: Pulmonary Arterial Hypertension Therapies
 Page: 1 of 15 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
Page: 1 of 15 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
Pharmacy Medical Necessity Guidelines: Pulmonary Hypertension Medications
 Pharmacy Medical Necessity Guidelines: Pulmonary Hypertension Medications Effective: January 1, 2016 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review
Pharmacy Medical Necessity Guidelines: Pulmonary Hypertension Medications Effective: January 1, 2016 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review
ECG may be indicated for patients with cardiovascular risk factors
 eappendix A. Summary for Preoperative ECG American College of Cardiology/ American Heart Association, 2007 A1 2002 A2 European Society of Cardiology and European Society of Anaesthesiology, 2009 A3 Improvement,
eappendix A. Summary for Preoperative ECG American College of Cardiology/ American Heart Association, 2007 A1 2002 A2 European Society of Cardiology and European Society of Anaesthesiology, 2009 A3 Improvement,
She was 39 years old, gravida 4, para 2. She had an Idiopathic Pulmonary. Arterial Hypertension (PAH) revealed during pregnancy by a New York Heart
 revealed during pregnancy by a New York Heart") Case #1 (year 1992): She was 39 years old, gravida 4, para 2. She had an Idiopathic Pulmonary Arterial Hypertension (PAH) revealed during pregnancy by a New York Heart Association (NYHA) functional class
Case #1 (year 1992): She was 39 years old, gravida 4, para 2. She had an Idiopathic Pulmonary Arterial Hypertension (PAH) revealed during pregnancy by a New York Heart Association (NYHA) functional class
1p36 and the Heart. John Lynn Jefferies, MD, MPH, FACC, FAHA
 1p36 and the Heart John Lynn Jefferies, MD, MPH, FACC, FAHA Director, Advanced Heart Failure and Cardiomyopathy Services Associate Professor, Pediatric Cardiology and Adult Cardiovascular Diseases Associate
1p36 and the Heart John Lynn Jefferies, MD, MPH, FACC, FAHA Director, Advanced Heart Failure and Cardiomyopathy Services Associate Professor, Pediatric Cardiology and Adult Cardiovascular Diseases Associate
Atrial Fibrillation An update on diagnosis and management
 Dr Arvind Vasudeva Consultant Cardiologist Atrial Fibrillation An update on diagnosis and management Atrial fibrillation (AF) remains the commonest disturbance of cardiac rhythm seen in clinical practice.
Dr Arvind Vasudeva Consultant Cardiologist Atrial Fibrillation An update on diagnosis and management Atrial fibrillation (AF) remains the commonest disturbance of cardiac rhythm seen in clinical practice.
Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations.
 INTRODUCTION Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations. Although decrease in cardiovascular mortality still major cause of morbidity & burden of disease.
INTRODUCTION Coronary Artery Disease leading cause of morbidity & mortality in industrialised nations. Although decrease in cardiovascular mortality still major cause of morbidity & burden of disease.
Acute heart failure may be de novo or it may be a decompensation of chronic heart failure.
 Management of Acute Left Ventricular Failure Acute left ventricular failure presents as pulmonary oedema due to increased pressure in the pulmonary capillaries. It is important to realise though that left
Management of Acute Left Ventricular Failure Acute left ventricular failure presents as pulmonary oedema due to increased pressure in the pulmonary capillaries. It is important to realise though that left
Idiopathic Pulmonary Fibrosis (IPF) Research
 Research") Idiopathic Pulmonary Fibrosis (IPF): Why Early Referral is Critical Even if Your Patient is Not Eligible for a Clinical Trial Idiopathic Pulmonary Fibrosis (IPF) Research Management of IPF requires a confident
Idiopathic Pulmonary Fibrosis (IPF): Why Early Referral is Critical Even if Your Patient is Not Eligible for a Clinical Trial Idiopathic Pulmonary Fibrosis (IPF) Research Management of IPF requires a confident
INTRODUCTION TO EECP THERAPY
 INTRODUCTION TO EECP THERAPY is an FDA cleared, Medicare approved, non-invasive medical therapy for the treatment of stable and unstable angina, congestive heart failure, acute myocardial infarction, and
INTRODUCTION TO EECP THERAPY is an FDA cleared, Medicare approved, non-invasive medical therapy for the treatment of stable and unstable angina, congestive heart failure, acute myocardial infarction, and
Milwaukee School of Engineering [email protected]. Case Study: Factors that Affect Blood Pressure Instructor Version
 Case Study: Factors that Affect Blood Pressure Instructor Version Goal This activity (case study and its associated questions) is designed to be a student-centered learning activity relating to the factors
Case Study: Factors that Affect Blood Pressure Instructor Version Goal This activity (case study and its associated questions) is designed to be a student-centered learning activity relating to the factors
Version 1 2015. Module guide. Preliminary document. International Master Program Cardiovascular Science University of Göttingen
 Version 1 2015 Module guide International Master Program Cardiovascular Science University of Göttingen Part 1 Theoretical modules Synopsis The Master program Cardiovascular Science contains four theoretical
Version 1 2015 Module guide International Master Program Cardiovascular Science University of Göttingen Part 1 Theoretical modules Synopsis The Master program Cardiovascular Science contains four theoretical
HEART HEALTH WEEK 3 SUPPLEMENT. A Beginner s Guide to Cardiovascular Disease HEART FAILURE. Relatively mild, symptoms with intense exercise
 WEEK 3 SUPPLEMENT HEART HEALTH A Beginner s Guide to Cardiovascular Disease HEART FAILURE Heart failure can be defined as the failing (insufficiency) of the heart as a mechanical pump due to either acute
WEEK 3 SUPPLEMENT HEART HEALTH A Beginner s Guide to Cardiovascular Disease HEART FAILURE Heart failure can be defined as the failing (insufficiency) of the heart as a mechanical pump due to either acute
Medical management of CHF: A New Class of Medication. Al Timothy, M.D. Cardiovascular Institute of the South
 Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
Medical management of CHF: A New Class of Medication Al Timothy, M.D. Cardiovascular Institute of the South Disclosures Speakers Bureau for Amgen Background Chronic systolic congestive heart failure remains
HYPERTROPHIC CARDIOMYOPATHY
 HYPERTROPHIC CARDIOMYOPATHY Most often diagnosed during infancy or adolescence, hypertrophic cardiomyopathy (HCM) is the second most common form of heart muscle disease, is usually genetically transmitted,
HYPERTROPHIC CARDIOMYOPATHY Most often diagnosed during infancy or adolescence, hypertrophic cardiomyopathy (HCM) is the second most common form of heart muscle disease, is usually genetically transmitted,
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL
 Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
Requirements for Provision of Outreach Paediatric Cardiology Service
 Requirements for Provision of Outreach Paediatric Cardiology Service Dr Shakeel A Qureshi, Consultant Paediatric Cardiologist, Evelina Children s Hospital, London, UK On behalf of British Congenital Cardiac
Requirements for Provision of Outreach Paediatric Cardiology Service Dr Shakeel A Qureshi, Consultant Paediatric Cardiologist, Evelina Children s Hospital, London, UK On behalf of British Congenital Cardiac
James F. Kravec, M.D., F.A.C.P
 James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
The new Heart Failure pathway
 The new Heart Failure pathway An integrated and seamless Strategy Dr Sunil Balani Definition of Heart Failure The inability of the heart to pump blood at a rate commensurate with the requirements of metabolising
The new Heart Failure pathway An integrated and seamless Strategy Dr Sunil Balani Definition of Heart Failure The inability of the heart to pump blood at a rate commensurate with the requirements of metabolising
Potential Causes of Sudden Cardiac Arrest in Children
 Potential Causes of Sudden Cardiac Arrest in Children Project S.A.V.E. When sudden death occurs in children, adolescents and younger adults, heart abnormalities are likely causes. These conditions are
Potential Causes of Sudden Cardiac Arrest in Children Project S.A.V.E. When sudden death occurs in children, adolescents and younger adults, heart abnormalities are likely causes. These conditions are
The heart then repolarises (or refills) in time for the next stimulus and contraction.
 in time for the next stimulus and contraction.") Atrial Fibrillation BRIEFLY, HOW DOES THE HEART PUMP? The heart has four chambers. The upper chambers are called atria. One chamber is called an atrium, and the lower chambers are called ventricles. In
Atrial Fibrillation BRIEFLY, HOW DOES THE HEART PUMP? The heart has four chambers. The upper chambers are called atria. One chamber is called an atrium, and the lower chambers are called ventricles. In
5. Management of rheumatic heart disease
 5. Management of rheumatic heart disease The fundamental goal in the long-term management of RHD is to prevent ARF recurrences, and therefore, prevent the progression of RHD, and in many cases allow for
5. Management of rheumatic heart disease The fundamental goal in the long-term management of RHD is to prevent ARF recurrences, and therefore, prevent the progression of RHD, and in many cases allow for
Pulmonary Diseases. Lung Disease: Pathophysiology, Medical and Exercise Programming. Overview of Pathophysiology
 Lung Disease: Pathophysiology, Medical and Exercise Programming Overview of Pathophysiology Ventilatory Impairments Increased airway resistance Reduced compliance Increased work of breathing Ventilatory
Lung Disease: Pathophysiology, Medical and Exercise Programming Overview of Pathophysiology Ventilatory Impairments Increased airway resistance Reduced compliance Increased work of breathing Ventilatory
The largest clinical study of Bayer's Xarelto (rivaroxaban) Wednesday, 14 November 2012 07:38
 Wednesday, 14 November 2012 07:38") Bayer HealthCare has announced the initiation of the COMPASS study, the largest clinical study of its oral anticoagulant Xarelto (rivaroxaban) to date, investigating the prevention of major adverse cardiac
Bayer HealthCare has announced the initiation of the COMPASS study, the largest clinical study of its oral anticoagulant Xarelto (rivaroxaban) to date, investigating the prevention of major adverse cardiac
Exchange solutes and water with cells of the body
 Chapter 8 Heart and Blood Vessels Three Types of Blood Vessels Transport Blood Arteries Carry blood away from the heart Transport blood under high pressure Capillaries Exchange solutes and water with cells
Chapter 8 Heart and Blood Vessels Three Types of Blood Vessels Transport Blood Arteries Carry blood away from the heart Transport blood under high pressure Capillaries Exchange solutes and water with cells
INTRODUCTION Thrombophilia deep vein thrombosis DVT pulmonary embolism PE inherited thrombophilia
 INTRODUCTION Thrombophilia (Hypercoagulability) is a condition in which a person forms blood clots more than normal. Blood clots may occur in the arms or legs (e.g., deep vein thrombosis DVT), the lungs
INTRODUCTION Thrombophilia (Hypercoagulability) is a condition in which a person forms blood clots more than normal. Blood clots may occur in the arms or legs (e.g., deep vein thrombosis DVT), the lungs
Cardiovascular diseases. pathology
 Cardiovascular diseases pathology Atherosclerosis Vascular diseases A disease that results in arterial wall thickens as a result of build- up of fatty materials such cholesterol, resulting in acute and
Cardiovascular diseases pathology Atherosclerosis Vascular diseases A disease that results in arterial wall thickens as a result of build- up of fatty materials such cholesterol, resulting in acute and
Section Four: Pulmonary Artery Waveform Interpretation
 Section Four: Pulmonary Artery Waveform Interpretation All hemodynamic pressures and waveforms are generated by pressure changes in the heart caused by myocardial contraction (systole) and relaxation/filling
Section Four: Pulmonary Artery Waveform Interpretation All hemodynamic pressures and waveforms are generated by pressure changes in the heart caused by myocardial contraction (systole) and relaxation/filling
RATE VERSUS RHYTHM CONTROL OF ATRIAL FIBRILLATION: SPECIAL CONSIDERATION IN ELDERLY. Charles Jazra
 RATE VERSUS RHYTHM CONTROL OF ATRIAL FIBRILLATION: SPECIAL CONSIDERATION IN ELDERLY Charles Jazra NO CONFLICT OF INTEREST TO DECLARE Relationship Between Atrial Fibrillation and Age Prevalence, percent
RATE VERSUS RHYTHM CONTROL OF ATRIAL FIBRILLATION: SPECIAL CONSIDERATION IN ELDERLY Charles Jazra NO CONFLICT OF INTEREST TO DECLARE Relationship Between Atrial Fibrillation and Age Prevalence, percent
Treating AF: The Newest Recommendations. CardioCase presentation. Ethel s Case. Wayne Warnica, MD, FACC, FACP, FRCPC
 Treating AF: The Newest Recommendations Wayne Warnica, MD, FACC, FACP, FRCPC CardioCase presentation Ethel s Case Ethel, 73, presents with rapid heart beating and mild chest discomfort. In the ED, ECG
Treating AF: The Newest Recommendations Wayne Warnica, MD, FACC, FACP, FRCPC CardioCase presentation Ethel s Case Ethel, 73, presents with rapid heart beating and mild chest discomfort. In the ED, ECG
Congenital Diaphragmatic Hernia. Manuel A. Molina, M.D. University Hospital at Brooklyn SUNY Downstate
 Congenital Diaphragmatic Hernia Manuel A. Molina, M.D. University Hospital at Brooklyn SUNY Downstate Congenital Diaphragmatic Hernias Incidence 1 in 2000 to 5000 live births. 80% in the left side, 20%
Congenital Diaphragmatic Hernia Manuel A. Molina, M.D. University Hospital at Brooklyn SUNY Downstate Congenital Diaphragmatic Hernias Incidence 1 in 2000 to 5000 live births. 80% in the left side, 20%
Preoperative Laboratory and Diagnostic Studies
 Preoperative Laboratory and Diagnostic Studies Preoperative Labratorey and Diagnostic Studies The concept of standardized testing in all presurgical patients regardless of age or medical condition is no
Preoperative Laboratory and Diagnostic Studies Preoperative Labratorey and Diagnostic Studies The concept of standardized testing in all presurgical patients regardless of age or medical condition is no
Management in the pre-hospital setting
 Management in the pre-hospital setting Inflammation of the joints Two main types: Osteoarthritis - cartilage loss from wear and tear Rheumatoid arthritis - autoimmune disorder Affects all age groups,
Management in the pre-hospital setting Inflammation of the joints Two main types: Osteoarthritis - cartilage loss from wear and tear Rheumatoid arthritis - autoimmune disorder Affects all age groups,
Medicare C/D Medical Coverage Policy
 Nebulizer Medications Origination: June 17, 2009 Review Date: October 21, 2015 Next Review: October, 2017 Medicare C/D Medical Coverage Policy DESCRIPTION Nebulizer medications are used to prevent and
Nebulizer Medications Origination: June 17, 2009 Review Date: October 21, 2015 Next Review: October, 2017 Medicare C/D Medical Coverage Policy DESCRIPTION Nebulizer medications are used to prevent and
Antiplatelet and anticoagulation treatment of patients undergoing carotid and peripheral artery angioplasty
 Round Table: Antithrombotic therapy beyond ACS Antiplatelet and anticoagulation treatment of patients undergoing carotid and peripheral artery angioplasty M. Matsagkas, MD, PhD, EBSQ-Vasc Associate Professor
Round Table: Antithrombotic therapy beyond ACS Antiplatelet and anticoagulation treatment of patients undergoing carotid and peripheral artery angioplasty M. Matsagkas, MD, PhD, EBSQ-Vasc Associate Professor
Collagen Vascular Lung Disease
 6 Collagen Vascular Lung Disease Collagen vascular or connective tissue disorders are a group of autoimmune diseases in which antibodies attack the body s own organs and systems. Among the many targets
6 Collagen Vascular Lung Disease Collagen vascular or connective tissue disorders are a group of autoimmune diseases in which antibodies attack the body s own organs and systems. Among the many targets
HYPERTENSION ASSOCIATED WITH RENAL DISEASES
 RENAL DISEASE v Patients with renal insufficiency should be encouraged to reduce dietary salt and protein intake. v Target blood pressure is less than 135-130/85 mmhg. If patients have urinary protein
RENAL DISEASE v Patients with renal insufficiency should be encouraged to reduce dietary salt and protein intake. v Target blood pressure is less than 135-130/85 mmhg. If patients have urinary protein
Diabetes mellitus. Lecture Outline
 Diabetes mellitus Lecture Outline I. Diagnosis II. Epidemiology III. Causes of diabetes IV. Health Problems and Diabetes V. Treating Diabetes VI. Physical activity and diabetes 1 Diabetes Disorder characterized
Diabetes mellitus Lecture Outline I. Diagnosis II. Epidemiology III. Causes of diabetes IV. Health Problems and Diabetes V. Treating Diabetes VI. Physical activity and diabetes 1 Diabetes Disorder characterized
DISCLOSURES RISK ASSESSMENT. Stroke and Heart Disease -Is there a Link Beyond Risk Factors? Daniel Lackland, MD
 STROKE AND HEART DISEASE IS THERE A LINK BEYOND RISK FACTORS? D AN IE L T. L AC K L AN D DISCLOSURES Member of NHLBI Risk Assessment Workgroup RISK ASSESSMENT Count major risk factors For patients with
STROKE AND HEART DISEASE IS THERE A LINK BEYOND RISK FACTORS? D AN IE L T. L AC K L AN D DISCLOSURES Member of NHLBI Risk Assessment Workgroup RISK ASSESSMENT Count major risk factors For patients with
Cardiovascular disease physiology. Linda Lowe-Krentz Bioscience in the 21 st Century October 14, 2011
 Cardiovascular disease physiology Linda Lowe-Krentz Bioscience in the 21 st Century October 14, 2011 Content Introduction The number 1 killer in America Some statistics Recommendations The disease process
Cardiovascular disease physiology Linda Lowe-Krentz Bioscience in the 21 st Century October 14, 2011 Content Introduction The number 1 killer in America Some statistics Recommendations The disease process
Prevention of stroke and systemic embolism in adult patients with non-valvular atrial fibrillation (AF) with one or more risk factors
 with one or more risk factors") News Release For use outside the US and UK only Bayer Pharma AG 13342 Berlin Germany Tel. +49 30 468-1111 www.bayerpharma.com Bayer s Xarelto Approved in the EU for the Prevention of Stroke in Patients
News Release For use outside the US and UK only Bayer Pharma AG 13342 Berlin Germany Tel. +49 30 468-1111 www.bayerpharma.com Bayer s Xarelto Approved in the EU for the Prevention of Stroke in Patients
Francine Lortie-Monette, MD, MSc, CSPQ, MBA Department of Epidemiology and Biostatistics University of Western Ontario 2003
 ASBESTOS Francine Lortie-Monette, MD, MSc, CSPQ, MBA Department of Epidemiology and Biostatistics University of Western Ontario 2003 Asbestosis Asbestosis is a model for other dust diseases as well as
ASBESTOS Francine Lortie-Monette, MD, MSc, CSPQ, MBA Department of Epidemiology and Biostatistics University of Western Ontario 2003 Asbestosis Asbestosis is a model for other dust diseases as well as
Inotropes/Vasoactive Agents Hina N. Patel, Pharm.D., BCPS Cathy Lawson, Pharm.D., BCPS
 Inotropes/Vasoactive Agents Hina N. Patel, Pharm.D., BCPS Cathy Lawson, Pharm.D., BCPS 1. Definition -an agent that affects the contractility of the heart -may be positive (increases contractility) or
Inotropes/Vasoactive Agents Hina N. Patel, Pharm.D., BCPS Cathy Lawson, Pharm.D., BCPS 1. Definition -an agent that affects the contractility of the heart -may be positive (increases contractility) or
DVT/PE Management with Rivaroxaban (Xarelto)
") DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular