Perioperative Management of External Ventricular (EVD) and Lumbar Drain (LD)
|
|
|
- Amice Burke
- 8 years ago
- Views:
Transcription
1 Perioperative Management of External Ventricular (EVD) and Lumbar Drain (LD) Educational Document from the Society of Neuroscience in Anesthesiology & Critical Care (SNACC) SNACC Task Force for Perioperative Management of Identification Pre-op Assessment Introduction Transporting Intraoperative Management Device Set Up Indications Troubleshooting Patient Preparation Leveling and Zeroing Complications Perioperative Checklist
2 This Presentation is Free of Commercial Bias SNACC does not endorse any particular EVD or LD system manufacturer
3 Perioperative Management of External Ventricular and Lumbar Drain Identification Pre-op Assessment Introduction Transporting Intraoperative Management Device Set Up Indications Troubleshooting Patient Preparation Leveling and Zeroing Complications Perioperative Checklist
4 Introduction to Common Indications for placement of EVD Acute symptomatic hydrocephalus Aneurysmal Subarachnoid Hemorrhage (SAH) Intracerebral and Intraventricular Hemorrhage with decreased level of consciousness Acute ischemic cerebellar stroke in concurrence with decompressive craniectomy ICP monitoring in Traumatic Brain Injury (TBI) TBI with post resuscitation GCS of 3-8, and abnormal computed tomography (CT) scan defined as one with hematomas, contusions, swelling, herniation or compressed basal cisterns Severe TBI with a normal CT scan if two or more of the following features are noted on admission (age over 40 yrs., unilateral or bilateral motor posturing, or SBP < 90 mmhg Management of patients with intracranial hypertension after TBI Malfunctioning or infected ventriculo-peritoneal shunts, and other neurological emergencies occurring due to infective, and neoplastic diseases Facilitation of intraoperative brain relaxation Targeted therapeutic interventions rtissue Plasminogen Activator in patients with IVH (efficacy and safety uncertain) and in patients with SAH Treatment of vasospasm after aneurysmal SAH Antibiotics in management of central nervous system infections Next Pge

 Intracerebral")
 Cerebellar stroke (1)")
5 Introduction to Indications for placement of EVD Subarachnoid Hemorrhage (1) with hydrocephalus (2) Intracerebral hemorrhage (1) with ventricular extension (2) Cerebellar stroke (1) with hydrocephalus (2)
6 Introduction to Indications for placement of LD Acute symptomatic hydrocephalus in SAH Spinal cord protective strategy in open and endovascular thoracic aortic repair for patients at high risk of spinal cord injury Active CSF leak (due to craniofacial trauma) or those at risk for CSF leak during skull base procedures, however lumbar drains do not reduce postoperative CSF leaks Facilitate intraoperative brain relaxation and intraoperative exposure
7 Introduction to Complications associated with placement of Hemorrhage Intracerebral hemorrhage, tract hematoma or tract hemorrhages (0-41%) Neuraxial hematoma (0-3.2%) Neural injury Infection (0-28% EVD, 0-50% LD) Malposition Occlusion and malfunction Over drainage of CSF Subdural or epidural hematoma Re-bleeding from a ruptured cerebral aneurysm Intracranial hypotension Cerebellar tonsillar herniation Paradoxical herniation Pneumocephalus Iatrogenic vascular injury (arteriovenous fistula, cerebral pseudo aneurysm) Fracture of catheters, with retained fragment of catheter Inadvertent injections of drugs Postdural puncture headache





8 Introduction to Complications associated with placement of EVD Tractoma Hemorrhage (1) along EVD (2) track
9 Differences between EVD and LD EVD LD Intracranial pressure monitor Yes No ( Intraspinal pressure) Drainage Leveling Dependent on ICP and EVD setting External auditory meatus Typically drain predetermined amount every hour Phlebostatic axis OR catheter insertion site
10 Perioperative Management of External Ventricular and Lumbar Drain Identification Pre-op Assessment Introduction Transporting Intraoperative Management Device Set Up Indications Troubleshooting Patient Preparation Leveling and Zeroing Complications Perioperative Checklist
")

11 Identify Components of EVD (1) (Type of EVD catheter) Antimicrobial-impregnated EVD Clindamycin and Rifampin Non-antimicrobial impregnated EVD



12 Identify Components of EVD (2) Antibiotic Impregnated EVD 35 cm catheter Tip of EVD



13 Familiarize Yourself with Different EVD Systems Cll ec to n ba g Cll ect on ba g
 for collecting CSF CSF flow from patient 7 7 Stopcock 4 to stop flow of CSF in collection")
14 Identify Components of EVD (3) The Collecting System Stopcock 1 Flushless transducer 3 Stopcock 2 (used to zero) 4 Stopcock 3 clamped to drain 6 5 EVD set at +10 cm H Graduated drip chamber (burette) for collecting CSF CSF flow from patient 7 7 Stopcock 4 to stop flow of CSF in collection bag

15 Identify Components of LD
16 Perioperative Management of External Ventricular and Lumbar Drain Identification Pre-op Assessment Introduction Transporting Intraoperative Management Device Set Up Indications Troubleshooting Patient Preparation Leveling and Zeroing Complications Perioperative Checklist
17 Device Set Up (EVD) EVD systems should be set up by personnel intimately familiar with the devices and demonstrate appropriate clinical competency Devices should be set up observing standards of sterile techniques Only flushless transducer systems are used EVD system is primed with sterile, preservative free saline Setting should be expressed in cm H20 Leveling of EVD should always be made at the external auditory meatus (EAM)
18 Device Set Up Carpenter s Level Bubble Level Laser Level Bubble Laser
")

19 Device Set Up (EVD) Leveling External Auditory Meatus
20 Device Set Up (LD)
21 Device Set Up (LD) LD systems should be set up by personnel intimately familiar with the devices and demonstrate appropriate clinical competency Devices should be set up observing standards of sterile techniques Only flushless transducer systems are used LD system is primed with sterile, preservative free saline Leveling of LD can be made at the external auditory meatus (EAM), level of catheter insertion or at the phlebostatic axis by use of Carpenter s bubble or laser level




22 Device Set Up Carpenter s Level Bubble Level Laser Level Bubble Laser


23 Device Set Up (LD) Leveling Phlebostatic axis Leveling at catheter insertion site
24 Perioperative Management of External Ventricular and Lumbar Drain Identification Pre-op Assessment Introduction Transporting Intraoperative Management Device Set Up Indications Troubleshooting Patient Preparation Leveling and Zeroing Complications Perioperative Checklist


 Open system to air (2) by removing the")

25 Zeroing EVD and LD system Connect ventricular or lumbar catheter under sterile conditions Attach pressure cable to flushless transducer Turn stopcock off to patient by turning it to 3 o clock position (1) Open system to air (2) by removing the red cap Press zero on monitor When monitor indicates 0, return stopcock upright Replace injection cap (3) 2 3 1
26 CAUTION Device Set up



27 Device Set up CAUTION Do not connect EVD or LD system to a high pressure system such as pressure bag used for arterial or central venous catheter
28 Perioperative Management of External Ventricular and Lumbar Drain Identification Pre-op Assessment Introduction Transporting Intraoperative Management Device Set Up Indications Troubleshooting Patient Preparation Leveling and Zeroing Complications Perioperative Checklist
29 Patient Preparation Follow ASRA* guidelines (LD) & NCS **guidelines (EVD) for prompt coagulopathy screening and reversal prior to EVD or LD placement and maintenance Administer antibiotics only prior to placement of EVD or LD, and follow institutional antibiograms in selecting antibiotics Whenever possible use antimicrobial-impregnated EVDs Practice strict aseptic technique based on national and institutional guidelines *ASRA: American Society of Regional Anesthesia **NCS: Neurocritical Care Society
30 Perioperative Management of External Ventricular and Lumbar Drain Identification Pre-op Assessment Introduction Transporting Intraoperative Management Device Set Up Indications Troubleshooting Patient Preparation Leveling and Zeroing Complications Perioperative Checklist
31 Preoperative Assessment Focused history and physical examination CSF color and consistency Hourly and daily CSF output ICP values, ICP waveform analysis, ICP trends, autoregulation indices, CPP and other multimodal monitoring data Clinical and radiological evidence of clamping trial tolerance All pertinent data regarding EVD and LD may be incorporated into a pre-operative handoff between intensive care/ ward providers and anesthesia providers


32 Preoperative Assessment Setting of EVD + 5 cm H cm H cm H20

")
33 Preoperative Assessment Color of CSF Hemorrhagic (Bloody) Xanthochromic Tea-colored

34 Intraoperative Management of P 1 P 2 P 3 Normal ICP waveform P 1 P 2 P 3 Percussion wave ~ reflections off choroid plexus Tidal wave ~ brain compliance Normally P2 wave is 80% of P1 wave Dicrotic wave ~ aortic valve closure

35 Intraoperative Management of Abnormal ICP waveform P 1 P 2 P 3 P2 wave is taller than P1 wave ~reduced cerebral compliance
36 Perioperative Management of External Ventricular and Lumbar Drain Identification Pre-op Assessment Introduction Transporting Intraoperative Management Device Set Up Indications Troubleshooting Patient Preparation Leveling and Zeroing Complications Perioperative Checklist
37 Transporting Patients with EVD or LD Pre-transport screening questionnaire Is EVD continuously draining in the neuro ICU or is it clamped for drainage? What is hourly CSF drainage? What is CSF output over 24 hours? Was an EVD clamp trial conducted in the neuro ICU? What are the results of such clamping trial? What is the baseline ICP ( < 15 mmhg, mmhg, or > 20 mmhg) What is the reason for transporting patient to the anesthesia suite ( Diagnostic vs. therapeutic procedure)

38 Transporting Patients with EVD or LD Open to drain CSF Closed to drain CSF CSF flow from patient CSF flow from patient


 (3) 2 TURN")
39 Transporting Patients with EVD or LD 1 EVD system Mounted on IV Pole (1) EVD Leveled at External Auditory Meatus (2) EVD clamped (distal) (3) 2 TURN UP 3 Next Page
40 Transporting Patients with EVD or LD Monitoring During Transport Continue all pre-transport monitoring and documentation End tidal carbon dioxide Mean and systolic arterial pressures Intracranial pressure, brain tissue oxygenation Cerebral perfusion pressure Use a dedicated intravenous pole to mount EVD and LD Transport personnel be prepared to treat intracranial hypertension during intrahospital transport Individualize decision to transport with EVD open vs. closed to CSF drainage
41 Perioperative Management of External Ventricular and Lumbar Drain Identification Pre-op Assessment Introduction Transporting Intraoperative Management Device Set Up Indications Troubleshooting Patient Preparation Leveling and Zeroing Complications Perioperative Checklist
42 Intraoperative Management of Label EVD and LD

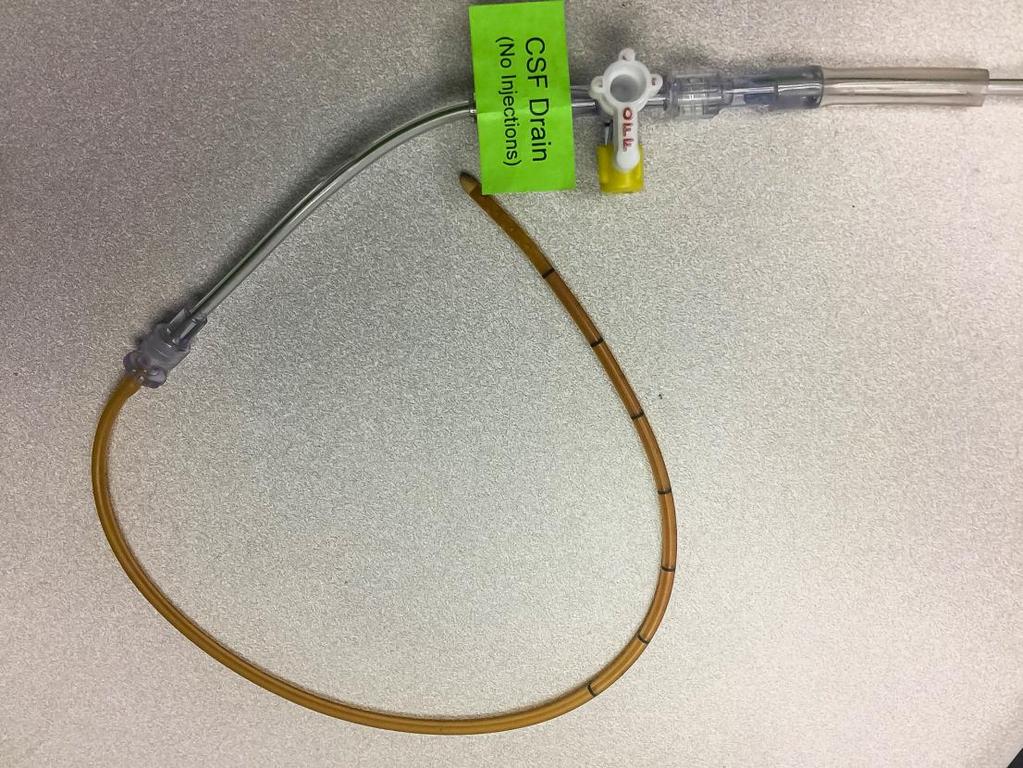

43 Intraoperative Management of
44 Intraoperative Management of Document the following in the anesthetic record at least every hourly or as situation demands Pressure = ICP/CPP or intraspinal pressure (ISP)/ spinal cord perfusion pressure (SCPP), Amount of CSF drainage (expressed in ml), Color of CSF and any change in color of CSF observed during the procedure, Drain height relative to the reference level, and EVD / LD status as set by the stopcocks in the device (i.e. open, clamped) Incorporate all information pertinent to EVD and LD into a standardized intraoperative handoff between anesthesia providers
45 Perioperative Management of External Ventricular and Lumbar Drain Identification Pre-op Assessment Introduction Transporting Intraoperative Management Device Set Up Indications Troubleshooting Patient Preparation Leveling and Zeroing Complications Perioperative Checklist
46 Troubleshooting Promptly recognize any accidental intrathecal injection Lavage of intrathecal space after intrathecal injection is not recommended Routine flushing of the EVD or LD should not be performed EVD or LD tubing that are accidently disconnected should be clamped immediately If EVD or LD system are contaminated by disconnection, all distal parts should be replaced with new sterile tubing



47 Troubleshooting ALERTS SUDDEN CHANGE IN COLOR OF CSF SUDDEN DRAINAGE OF CSF of ML EVD or LD SUDDENLY STOPS DRAINING DAMPENING OF ICP WAVEFORM Call Anesthesiology attending Call Surgeon
48 Perioperative Management of External Ventricular and Lumbar Drain Identification Pre-op Assessment Introduction Transporting Intraoperative Management Device Set Up Indications Troubleshooting Patient Preparation Leveling and Zeroing Complications Perioperative Checklist
49 Perioperative Checklist Preoperative assessment Obtain baseline neurological examination Review EVD (cmh20) & LD setting (in ml/hr of CSF drained) Review hourly CSF output to obtain baseline Review baseline ICP mmhg, ICP trends, and available multimodal monitoring data Review baseline CSF color and consistency Review clamp trials data if available Review coagulopathy profile Review antibiotic plan if anticipating new EVD /LD insertion in the operating room Provide EVD and LD details during pre-operative handoff between intensive care / ward providers and the anesthesia providers. Transporting patients with EVD and LD Confirm decision to travel with EVD or LD clamp vs. open If travelling with EVD clamp, ensure clamping at both proximal port on EVD and distal port on CSF collecting system Confirm HOB status during transport Confirm availability of dedicated intravenous pole for EVD / LD mount Confirm leveling EVD at external auditory meatus & LD at phlebostatic axis or at lumbar catheter insertion site Enable ICP monitoring during transport Confirm availability of medications needed to treat intracranial hypertension during transport Intraoperative management of indwelling drains Prepare transducer cable Identify EVD/ LD tubing by appropriate unique labeling Confirm HOB status during surgical procedure Confirm leveling of EVD at external auditory meatus & LD at phlebostatic axis Obtain ICP waveform & baseline ICP value Record q 1-hour EVD /LD setting Record at least q 1-hour ICP values (recorded with EVD closed to drain) Record at least q 1-hour EVD /LD drain output (expressed in ml) Provide EVD and LD details during intraoperative handoffs between anesthesia providers Inform surgeon if any one or more of the following Sudden decline in CSF drainage or no drainage from EVD or LD, or occlusion of EVD or LD If drain output is greater than ml at any time or in any given hour Sudden change in CSF color Dampening or loss of ICP waveform Next age
50 SNACC QUIZ 1. During pre-operative assessment of patient with indwelling EVD, the anesthesia provider should perform all of the following EXCEPT : A. Perform EVD clamp trial B. Focused neurological examination C. Inspection of EVD system D. Obtain hourly and 24-hour EVD output data Click for answer
51 Perform EVD clamp trial Answer A Question 2
52 2. During transporting a patient to and from the operating room, which of the following is true? A. It is ok to place CSF collecting system horizontal in the patients bed B. It is required to mount CSF collecting system on an intravenous pole C. It is ok not to monitor ICP during transport D. It is ok to connect EVD and LD to a flushable pressure transducer system Click for answer
53 It is required to mount CSF collecting system on an intravenous pole Answer B Question 3
54 3. Which of the following is true? A. Overdrainage complications are common to both EVD and LD B. Ventriculostomy associated hemorrhages occur in only in patients with coagulopathy C. In patients with unsecured ruptured cerebral aneurysm it is ok to open EVD and rapidly drain cerebrospinal fluid D. CSF output of more than 10 ml/hr is considered overdrainage Click for answer
55 Overdrainage complications are common to both EVD and LD Answer A Question 4
56 4. During a neurosurgical procedure, you notice sudden decline in CSF output from external ventricular drain and ICP waveform is lost. All of the following are appropriate in troubleshooting, EXCEPT : A. Examine the system for kinking or obstruction B. Notify neurosurgeon C. Flush the system using preservative free normal saline D. Gently lowering the EVD collecting system Click for answer
57 Flush the system using preservative free normal saline Answer C Question 5

 Stopcock closed to CSF drain b)")
58 5. For accurately measuring ICP, which of the following stopcock position is appropriate? a) Stopcock closed to CSF drain b) Stopcock open to drain CSF Click for answer
59 Stopcock closed to CSF drain Answer A
60 SNACC Task Force Perioperative Management of External Ventricular and Lumbar Drains Abhijit Lele M.B.B.S, M.D., M.S. Amie Hofnagel M.D. Nina Schloemerkemper M.D., Dr.med, FRCA David Wyler M.D. Nophanan Chaikittisilpa M.D. Monica Vavilala M.D. Bhiken Naik M.B.B. Ch. James Williams M.D. Ph.D. Lashmikumar Venkat Raghavan M.B.B.S., M.D., FRCA, FRCPC Ines Koerner M.D., Ph.D.
Section Two: Arterial Pressure Monitoring
 Section Two: Arterial Pressure Monitoring Indications An arterial line is indicated for blood pressure monitoring for the patient with any medical or surgical condition that compromises cardiac output,
Section Two: Arterial Pressure Monitoring Indications An arterial line is indicated for blood pressure monitoring for the patient with any medical or surgical condition that compromises cardiac output,
The Clinical Evaluation of the Comatose Patient in the Emergency Department
 The Clinical Evaluation of the Comatose Patient in the Emergency Department patients with altered mental status (AMS) and coma. treat patients who present to the Emergency Department with altered mental
The Clinical Evaluation of the Comatose Patient in the Emergency Department patients with altered mental status (AMS) and coma. treat patients who present to the Emergency Department with altered mental
Hemodynamic Monitoring: Principles to Practice M. L. Cheatham, MD, FACS, FCCM
 SUMMARY HEMODYNAMIC MONITORING: FROM PRINCIPLES TO PRACTICE Michael L. Cheatham, MD, FACS, FCCM Director, Surgical Intensive Care Units Orlando Regional Medical Center Orlando, Florida Fluid-filled catheters
SUMMARY HEMODYNAMIC MONITORING: FROM PRINCIPLES TO PRACTICE Michael L. Cheatham, MD, FACS, FCCM Director, Surgical Intensive Care Units Orlando Regional Medical Center Orlando, Florida Fluid-filled catheters
INTERDISCIPLINARY CLINICAL MANUAL Policy and Procedure
 INTERDISCIPLINARY CLINICAL MANUAL Policy and Procedure TITLE: Arterial Catheter Blood Sampling/Blood NUMBER: CC 80-005 Pressure Monitoring/Catheter Removal Effective Date: October 2014 Page 1 of 11 Applies
INTERDISCIPLINARY CLINICAL MANUAL Policy and Procedure TITLE: Arterial Catheter Blood Sampling/Blood NUMBER: CC 80-005 Pressure Monitoring/Catheter Removal Effective Date: October 2014 Page 1 of 11 Applies
What You Should Know About Cerebral Aneurysms
 What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Interventions Committee of the American Heart Association Cardiovascular Radiology Council Randall T. Higashida, M.D.,
What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Interventions Committee of the American Heart Association Cardiovascular Radiology Council Randall T. Higashida, M.D.,
What Is an Arteriovenous Malformation (AVM)?
?") What Is an Arteriovenous Malformation (AVM)? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall T. Higashida, M.D., Chair 1 What
What Is an Arteriovenous Malformation (AVM)? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall T. Higashida, M.D., Chair 1 What
Thoracoabdominal aortic aneurysm
 Thoracoabdominal aortic aneurysm Patient (1) - 69 PMH: 2013 - MVP, aortic root replacement with biological valve (Perimount) and subtotal aortic arch replacement Analysis for oppressive chest complaints
Thoracoabdominal aortic aneurysm Patient (1) - 69 PMH: 2013 - MVP, aortic root replacement with biological valve (Perimount) and subtotal aortic arch replacement Analysis for oppressive chest complaints
6.0 Management of Head Injuries for Maxillofacial SHOs
 6.0 Management of Head Injuries for Maxillofacial SHOs As a Maxillofacial SHO you are not required to manage established head injury, however an awareness of the process is essential when dealing with
6.0 Management of Head Injuries for Maxillofacial SHOs As a Maxillofacial SHO you are not required to manage established head injury, however an awareness of the process is essential when dealing with
Using the Pupillometer in Clinical Practice
 Using the Pupillometer in Clinical Practice Claude Hemphill MD M.A.S. [email protected] Kathy Johnson RN, MSN [email protected] Mary Kay Bader RN, MSN, CCNS [email protected] Pupillometry: How It
Using the Pupillometer in Clinical Practice Claude Hemphill MD M.A.S. [email protected] Kathy Johnson RN, MSN [email protected] Mary Kay Bader RN, MSN, CCNS [email protected] Pupillometry: How It
DIAGNOSTIC CRITERIA OF STROKE
 DIAGNOSTIC CRITERIA OF STROKE Diagnostic criteria are used to validate clinical diagnoses. Here below MONICA diagnostic criteria are reported. MONICA - MONItoring trends and determinants of CArdiovascular
DIAGNOSTIC CRITERIA OF STROKE Diagnostic criteria are used to validate clinical diagnoses. Here below MONICA diagnostic criteria are reported. MONICA - MONItoring trends and determinants of CArdiovascular
SERVICE: Neurosurgery - Sinai, PGY 1
 SERVICE: Neurosurgery - Sinai, PGY 1 General description: The Sinai surgical residents will rotate in the Department of Neurosurgery at Sinai Hospital during their intern year. The duration of this rotation
SERVICE: Neurosurgery - Sinai, PGY 1 General description: The Sinai surgical residents will rotate in the Department of Neurosurgery at Sinai Hospital during their intern year. The duration of this rotation
Head Injury. Dr Sally McCarthy Medical Director ECI
 Head Injury Dr Sally McCarthy Medical Director ECI Head injury in the emergency department A common presentation 80% Mild Head Injury = GCS 14 15 10% Moderate Head Injury = GCS 9 13 10% Severe Head Injury
Head Injury Dr Sally McCarthy Medical Director ECI Head injury in the emergency department A common presentation 80% Mild Head Injury = GCS 14 15 10% Moderate Head Injury = GCS 9 13 10% Severe Head Injury
PE finding: Left side extremities mild weakness No traumatic wound No bloody otorrhea, nor rhinorrhea
 Case report A 82-year-old man was suffered from sudden onset spasm of extremities then he fell down to the ground with loss of consciousness. He recovered his consciousness 7-8 mins later but his conscious
Case report A 82-year-old man was suffered from sudden onset spasm of extremities then he fell down to the ground with loss of consciousness. He recovered his consciousness 7-8 mins later but his conscious
Acute Myocardial Infarction (the formulary thrombolytic for AMI at AAMC is TNK, please see the TNK monograph in this manual for information)
") ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Alteplase (Tissue Plasminogen Activator (t-pa)), Activase in the Treatment
ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Alteplase (Tissue Plasminogen Activator (t-pa)), Activase in the Treatment
Measuring central venous pressure
 Elaine Cole Senior lecturer ED/Trauma, City University Barts and the London NHS Trust 1 Learning outcomes That the clinician can: Describe the sites of central venous catheterisation Understand why central
Elaine Cole Senior lecturer ED/Trauma, City University Barts and the London NHS Trust 1 Learning outcomes That the clinician can: Describe the sites of central venous catheterisation Understand why central
NORTH CAROLINA BOARD OF NURSING NURSE AIDE II TRAINING MODULE
 PART A: PREPARING FOR ADMINISTRATION OF IV FLUIDS All four parts of this module, including skills checklists must be successfully completed in order to complete this training module. This activity is a
PART A: PREPARING FOR ADMINISTRATION OF IV FLUIDS All four parts of this module, including skills checklists must be successfully completed in order to complete this training module. This activity is a
Severe Headaches in Patients with shunts. Slit Ventricle Syndromes
 Severe Headaches in Patients with shunts Slit Ventricle Syndromes Incidence Of Headaches In Shunted Hydrocephalus Essentially all adolescents and young adults with shunts will have headaches if asked Most
Severe Headaches in Patients with shunts Slit Ventricle Syndromes Incidence Of Headaches In Shunted Hydrocephalus Essentially all adolescents and young adults with shunts will have headaches if asked Most
2. Does the patient have one of the following appropriate indications for placing indwelling urinary catheters?
 A. Decision to Insert a Urinary Catheter: 1. Before placing an indwelling catheter, please consider if these alternatives would be more appropriate: Bladder scanner: to assess and confirm urinary retention,
A. Decision to Insert a Urinary Catheter: 1. Before placing an indwelling catheter, please consider if these alternatives would be more appropriate: Bladder scanner: to assess and confirm urinary retention,
Bleeding in the brain haemorrhagic stroke
 Stroke Helpline: 0303 3033 100 Website: stroke.org.uk Bleeding in the brain haemorrhagic stroke Most strokes are caused by a blockage in an artery leading to the brain an ischaemic stroke. However, about
Stroke Helpline: 0303 3033 100 Website: stroke.org.uk Bleeding in the brain haemorrhagic stroke Most strokes are caused by a blockage in an artery leading to the brain an ischaemic stroke. However, about
Types of Brain Injury
 Types of Brain Injury The bones of your skull are hard and they protect your brain. Your brain is soft, like firm Jell-O. When your head moves, your brain moves inside your skull. When your head is hit
Types of Brain Injury The bones of your skull are hard and they protect your brain. Your brain is soft, like firm Jell-O. When your head moves, your brain moves inside your skull. When your head is hit
Arterial pressure monitoring Direct arterial pressure monitoring permits continuous measurement of systolic, diastolic, and mean pressures and allows
 Arterial pressure monitoring Direct arterial pressure monitoring permits continuous measurement of systolic, diastolic, and mean pressures and allows arterial blood sampling. Because direct measurement
Arterial pressure monitoring Direct arterial pressure monitoring permits continuous measurement of systolic, diastolic, and mean pressures and allows arterial blood sampling. Because direct measurement
Paediatric Intensive Care Unit Nursing Procedure: Care of Arterial Lines.
 Paediatric Intensive Care Unit Nursing Procedure: Care of Arterial Lines. Definition: Arterial Line Placement of an indwelling arterial catheter for the purpose of continuous monitoring of intra arterial
Paediatric Intensive Care Unit Nursing Procedure: Care of Arterial Lines. Definition: Arterial Line Placement of an indwelling arterial catheter for the purpose of continuous monitoring of intra arterial
REMOVAL OF A PICC. Possible Cause Nursing Actions Prevention
 REMOVAL OF A PICC PICC lines are removed following a physician order, when therapy is completed or complications such as line sepsis, thrombosis or phlebitis, require removal. The removal of a PICC line
REMOVAL OF A PICC PICC lines are removed following a physician order, when therapy is completed or complications such as line sepsis, thrombosis or phlebitis, require removal. The removal of a PICC line
Chiari Malformation: Treatment
 Chiari Malformation: Treatment SYMPTOMS DIAGNOSIS LIVING WITH CHIARI TREATMENT Rick Labuda, Executive Director [email protected] 724-940-0116 Disclaimer: This presentation is intended for informational
Chiari Malformation: Treatment SYMPTOMS DIAGNOSIS LIVING WITH CHIARI TREATMENT Rick Labuda, Executive Director [email protected] 724-940-0116 Disclaimer: This presentation is intended for informational
Aspira* Peritoneal Drainage Catheter
 Aspira* Peritoneal Drainage Catheter Instructions For Use Access Systems Product Description: The Aspira* Peritoneal Drainage Catheter is a tunneled, long-term catheter used to drain accumulated fluid
Aspira* Peritoneal Drainage Catheter Instructions For Use Access Systems Product Description: The Aspira* Peritoneal Drainage Catheter is a tunneled, long-term catheter used to drain accumulated fluid
Direct Arterial Blood Pressure Monitoring Angel M. Rivera CVT, VTS (ECC) Animal Emergency Center Glendale, WI March 2003
 Animal Emergency Center Glendale, WI March 2003") Direct Arterial Blood Pressure Monitoring Angel M. Rivera CVT, VTS (ECC) Animal Emergency Center Glendale, WI March 2003 Introduction Direct measurement of arterial blood pressure is obtained via a peripheral
Direct Arterial Blood Pressure Monitoring Angel M. Rivera CVT, VTS (ECC) Animal Emergency Center Glendale, WI March 2003 Introduction Direct measurement of arterial blood pressure is obtained via a peripheral
Pressure reactivity: Relationship between ICP and arterial blood pressure (ABP). Pressure-reactivity index, computational methods. Clinical examples.
. Pressure-reactivity index, computational methods. Clinical examples.") Pressure reactivity: Relationship between ICP and arterial blood pressure (ABP). Pressure-reactivity index, computational methods. Clinical examples. Optimization of cerebral perfusion pressure: Relationship
Pressure reactivity: Relationship between ICP and arterial blood pressure (ABP). Pressure-reactivity index, computational methods. Clinical examples. Optimization of cerebral perfusion pressure: Relationship
TRAUMATIC BRAIN INJURY (TBI)
") Background: Traumatic Brain Injury (TBI) is one of the leading causes of trauma related disability and death in the U.S. TBIs can occur as either blunt, penetrating, or a combination of both depending
Background: Traumatic Brain Injury (TBI) is one of the leading causes of trauma related disability and death in the U.S. TBIs can occur as either blunt, penetrating, or a combination of both depending
Ischaemic stroke 85% (85 in every 100 strokes)
") UNDERSTANDING STROKE DUE TO INTRACEREBRAL HAEMORRHAGE This factsheet provides information for people who have had a stroke due to an intracerebral (bleed in the brain) and for their families and carers.
UNDERSTANDING STROKE DUE TO INTRACEREBRAL HAEMORRHAGE This factsheet provides information for people who have had a stroke due to an intracerebral (bleed in the brain) and for their families and carers.
Australian and New Zealand College of Anaesthetists (ANZCA) Guidelines for the Management of Major Regional Analgesia
 Guidelines for the Management of Major Regional Analgesia") PS03 2014 Australian and New Zealand College of Anaesthetists (ANZCA) Faculty of Pain Medicine Guidelines for the Management of Major Regional Analgesia 1. OVERVIEW This document is intended to apply to
PS03 2014 Australian and New Zealand College of Anaesthetists (ANZCA) Faculty of Pain Medicine Guidelines for the Management of Major Regional Analgesia 1. OVERVIEW This document is intended to apply to
Chiari Malformation: An Overview
 Chiari Malformation: An Overview SYMPTOMS DIAGNOSIS LIVING WITH CHIARI TREATMENT Rick Labuda, Executive Director [email protected] 724-940-0116 Disclaimer: This presentation is intended for informational
Chiari Malformation: An Overview SYMPTOMS DIAGNOSIS LIVING WITH CHIARI TREATMENT Rick Labuda, Executive Director [email protected] 724-940-0116 Disclaimer: This presentation is intended for informational
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE
 SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: (crc13-nursing) (crc.013-respiratory) Nursing, Special Care Areas Respiratory Care Services Perioperative Services DATE: REVIEWED: PAGES:
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: (crc13-nursing) (crc.013-respiratory) Nursing, Special Care Areas Respiratory Care Services Perioperative Services DATE: REVIEWED: PAGES:
To outline nursing management of patients receiving epidural anesthesia during labor (Includes walking epidurals and combined spinal-epidurals).
.") HOSPITAL NAME INSTITUTIONAL POLICY AND PROCEDURE (IPP) Department: Manual: Section: TITLE/DESCRIPTION POLICY NUMBER LABOR: EPIDURAL EFFECTIVE DATE REVIEW DUE REPLACES NUMBER NO. OF PAGES APPROVED BY APPLIES
HOSPITAL NAME INSTITUTIONAL POLICY AND PROCEDURE (IPP) Department: Manual: Section: TITLE/DESCRIPTION POLICY NUMBER LABOR: EPIDURAL EFFECTIVE DATE REVIEW DUE REPLACES NUMBER NO. OF PAGES APPROVED BY APPLIES
PERIPHERALLY INSERTED CENTRAL CATHETERS (PICC) Fong So Kwan APN, Haematology unit Medical Department, QMH
 Fong So Kwan APN, Haematology unit Medical Department, QMH") PERIPHERALLY INSERTED CENTRAL CATHETERS (PICC) Fong So Kwan APN, Haematology unit Medical Department, QMH 1 What is a PICC catheter? Primary vascular access device since their introduction in the mid-1970s,
PERIPHERALLY INSERTED CENTRAL CATHETERS (PICC) Fong So Kwan APN, Haematology unit Medical Department, QMH 1 What is a PICC catheter? Primary vascular access device since their introduction in the mid-1970s,
PICC & Midline Catheters Patient Information Guide
 PICC & Midline Catheters Patient Information Guide medcompnet.com 1 table of contents Introduction 4 What is a PICC or Midline Catheter? 4 How is the PICC or Midline Catheter Inserted? 6 Catheter Care
PICC & Midline Catheters Patient Information Guide medcompnet.com 1 table of contents Introduction 4 What is a PICC or Midline Catheter? 4 How is the PICC or Midline Catheter Inserted? 6 Catheter Care
EMS Management of Stroke. Deaver Shattuck, M.D. Brian Wiseman, M.D. Keith Woodward, M.D.
 EMS Management of Stroke Deaver Shattuck, M.D. Brian Wiseman, M.D. Keith Woodward, M.D. Financial Disclosure: No relevant financial relationship exists Working Together to End Stroke Formed in 2013 Identified
EMS Management of Stroke Deaver Shattuck, M.D. Brian Wiseman, M.D. Keith Woodward, M.D. Financial Disclosure: No relevant financial relationship exists Working Together to End Stroke Formed in 2013 Identified
Intrathecal Baclofen for CNS Spasticity
 Intrathecal Baclofen for CNS Spasticity Last Review Date: November 13, 2015 Number: MG.MM.ME.31bC5 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or
Intrathecal Baclofen for CNS Spasticity Last Review Date: November 13, 2015 Number: MG.MM.ME.31bC5 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or
Basic Stroke for the New Recruit
 Basic Stroke for the New Recruit Authors Erin Conahan MSN, RN, ACNS-BC, CNRN, SCRN Julie FussnerBSN, RN, CPHQ, SCRN The authors have nothing to disclose. 1 Objectives List causes of small vessel stroke
Basic Stroke for the New Recruit Authors Erin Conahan MSN, RN, ACNS-BC, CNRN, SCRN Julie FussnerBSN, RN, CPHQ, SCRN The authors have nothing to disclose. 1 Objectives List causes of small vessel stroke
THERAPY INTENSITY LEVEL
 THERAPY INTENSITY LEVEL TILBasic = TIL Basic. CDE Variable TILBasic = TIL Basic; Global summary measure of Therapy Intensity Level for control of Intracranial Pressure (ICP).. CDE Definition This summary
THERAPY INTENSITY LEVEL TILBasic = TIL Basic. CDE Variable TILBasic = TIL Basic; Global summary measure of Therapy Intensity Level for control of Intracranial Pressure (ICP).. CDE Definition This summary
PATIENT GUIDE. Understand and care for your peripherally inserted central venous catheter (PICC). MEDICAL
. MEDICAL") PATIENT GUIDE Understand and care for your peripherally inserted central venous catheter (PICC). MEDICAL Introduction The following information is presented as a guideline for your reference. The best
PATIENT GUIDE Understand and care for your peripherally inserted central venous catheter (PICC). MEDICAL Introduction The following information is presented as a guideline for your reference. The best
Policies and Procedures. Related to. IABP Therapy
 Policies and Procedures Related to IABP Therapy Courtesy of Datascope Corp. Clinical Support Services The following policies and procedures are intended to serve as guidelines for developing hospital policy.
Policies and Procedures Related to IABP Therapy Courtesy of Datascope Corp. Clinical Support Services The following policies and procedures are intended to serve as guidelines for developing hospital policy.
Imaging of Thoracic Endovascular Stent-Grafts
 Imaging of Thoracic Endovascular Stent-Grafts Tariq Hameed, M.D. Department of Radiology and Imaging Sciences, Indiana University School of Medicine, Indianapolis, Indiana Disclosures: No relevant financial
Imaging of Thoracic Endovascular Stent-Grafts Tariq Hameed, M.D. Department of Radiology and Imaging Sciences, Indiana University School of Medicine, Indianapolis, Indiana Disclosures: No relevant financial
Constituents within the skull include the brain (80%/1400ml), blood (10%/150ml) and cerebrospinal fluid (CSF 10%/150ml)
, blood (10%/150ml) and cerebrospinal fluid (CSF 10%/150ml)") Cerebral Blood Flow and Intracranial Pressure Dr Lisa Hill, SpR Anaesthesia, Royal Oldham Hospital, UK. Email [email protected] Dr Carl Gwinnutt, Consultant Neuroanaesthetist, Hope Hospital, UK. Part
Cerebral Blood Flow and Intracranial Pressure Dr Lisa Hill, SpR Anaesthesia, Royal Oldham Hospital, UK. Email [email protected] Dr Carl Gwinnutt, Consultant Neuroanaesthetist, Hope Hospital, UK. Part
INR: RUPTURED ANEURYSM: POST EMBOLIZATION Patient Identification Page 1 of 5. Allergies: Weight: kg Diagnosis:
 Page 1 of 5 Allergies: Weight: kg Diagnosis: Service: Admission Admit to Inpatient Admit to Daypatient Place on Outpatient Observation Status Hospital Attending: Attending Physician Attending Provider:
Page 1 of 5 Allergies: Weight: kg Diagnosis: Service: Admission Admit to Inpatient Admit to Daypatient Place on Outpatient Observation Status Hospital Attending: Attending Physician Attending Provider:
N26 Chest Tubes 5/9/2012
 Thoracic cavity, pleural space 1 Conditions requiring chest drainage_1 Air between the pleurae is a pneumothorax Occurs when there is an opening on the surface of the lung or in the airways, y, in the
Thoracic cavity, pleural space 1 Conditions requiring chest drainage_1 Air between the pleurae is a pneumothorax Occurs when there is an opening on the surface of the lung or in the airways, y, in the
Nursing Education and Research
 Melissa Meloche Meloche, RN RN, MSN MSN, CCRN Nursing Education and Research Describe the purpose p of common clinical equipment found in the Intensive Care Unit and how this equipment could impact a patient
Melissa Meloche Meloche, RN RN, MSN MSN, CCRN Nursing Education and Research Describe the purpose p of common clinical equipment found in the Intensive Care Unit and how this equipment could impact a patient
Discovery of an Aneurysm Following a Motorcycle Accident. Maya Babu, MSIII Gillian Lieberman, M.D.
 Discovery of an Aneurysm Following a Motorcycle Accident Maya Babu, MSIII Gillian Lieberman, M.D. Patient CC: July 2004 65 yo male transferred to the BI from an OSH s/p motorcycle crash w/o a helmet CC
Discovery of an Aneurysm Following a Motorcycle Accident Maya Babu, MSIII Gillian Lieberman, M.D. Patient CC: July 2004 65 yo male transferred to the BI from an OSH s/p motorcycle crash w/o a helmet CC
Stroke Coding Issues Presentation to: NorthEast Cerebrovascular Consortium
 Stroke Coding Issues Presentation to: NorthEast Cerebrovascular Consortium October 30, 2008 Barry Libman, RHIA, CCS, CCS-P President, Barry Libman Inc. Stroke Coding Issues Outline Medical record documentation
Stroke Coding Issues Presentation to: NorthEast Cerebrovascular Consortium October 30, 2008 Barry Libman, RHIA, CCS, CCS-P President, Barry Libman Inc. Stroke Coding Issues Outline Medical record documentation
31. Lumbar Puncture. PURPOSE: To diagnose central nervous system infections, subarachnoid hemorrhages, and many other neurologic pathologies.
 31. Lumbar Puncture PURPOSE: To diagnose central nervous system infections, subarachnoid hemorrhages, and many other neurologic pathologies. EQUIPMENT NEEDED (FIGURE 31-1): Spinal or lumbar puncture tray
31. Lumbar Puncture PURPOSE: To diagnose central nervous system infections, subarachnoid hemorrhages, and many other neurologic pathologies. EQUIPMENT NEEDED (FIGURE 31-1): Spinal or lumbar puncture tray
CHEST TUBES AND CHEST DRAINAGE SYSTEMS
 CHEST TUBES AND CHEST DRAINAGE SYSTEMS Central Nursing Orientation April 2008 Revised September 2011 OBJECTIVES Describe common tubes and indications for use at LHSC Review indications and contraindications,
CHEST TUBES AND CHEST DRAINAGE SYSTEMS Central Nursing Orientation April 2008 Revised September 2011 OBJECTIVES Describe common tubes and indications for use at LHSC Review indications and contraindications,
Fact Sheet. Shunt Systems for the Management of Hydrocephalus. Overview. Shunt system components. Symptoms of Shunt Malfunction:
 Fact Sheet Shunt Systems for the Management of Hydrocephalus Overview The management of hydrocephalus has challenged neurosurgeons, neurologists, engineers and medical device developers alike because of
Fact Sheet Shunt Systems for the Management of Hydrocephalus Overview The management of hydrocephalus has challenged neurosurgeons, neurologists, engineers and medical device developers alike because of
YALE UNIVERSITY SCHOOL OF MEDICINE: SECTION OF OTOLARYNGOLOGY PATIENT INFORMATION FUNCTIONAL ENDOSCOPIC SINUS SURGERY
 YALE UNIVERSITY SCHOOL OF MEDICINE: SECTION OF OTOLARYNGOLOGY PATIENT INFORMATION FUNCTIONAL ENDOSCOPIC SINUS SURGERY What is functional endoscopic sinus surgery (FESS)? Functional endoscopic sinus surgery
YALE UNIVERSITY SCHOOL OF MEDICINE: SECTION OF OTOLARYNGOLOGY PATIENT INFORMATION FUNCTIONAL ENDOSCOPIC SINUS SURGERY What is functional endoscopic sinus surgery (FESS)? Functional endoscopic sinus surgery
How To Monitor Csp For A Patient
 ICM plus - a Versatile Software for Assessment of CSF Dynamics Zofia Czosnyka MD; Angelos G. Kolias MSc, MRCS; Peter Smielewski; Marek Czosnyka; John Douglas Pickard Addenbrooke s Hospital & University
ICM plus - a Versatile Software for Assessment of CSF Dynamics Zofia Czosnyka MD; Angelos G. Kolias MSc, MRCS; Peter Smielewski; Marek Czosnyka; John Douglas Pickard Addenbrooke s Hospital & University
Within the Scope of Practice/Role of APRN RN _ X_LPN CNA
 Wyoming State Board of Nursing 130 Hobbs Avenue, Suite B Cheyenne, WY 82002 Phone (307) 777-7601 Fax (307) 777-3519 E-Mail: [email protected] Home Page: https://nursing-online.state.wy.us/ OPINION:
Wyoming State Board of Nursing 130 Hobbs Avenue, Suite B Cheyenne, WY 82002 Phone (307) 777-7601 Fax (307) 777-3519 E-Mail: [email protected] Home Page: https://nursing-online.state.wy.us/ OPINION:
CUESTA COLLEGE REGISTERED NURSING PROGRAM CRITICAL ELEMENTS
 CUESTA COLLEGE REGISTERED NURSING PROGRAM CRITICAL ELEMENTS LEVELS I through IV A. OVERRIDING CRITICAL ELEMENTS Violation of an overriding area will result in termination and failure of the particular
CUESTA COLLEGE REGISTERED NURSING PROGRAM CRITICAL ELEMENTS LEVELS I through IV A. OVERRIDING CRITICAL ELEMENTS Violation of an overriding area will result in termination and failure of the particular
Collaboration Anesthesia
 HPC hpcconnection.ca Nursing Neuro - axial Analgesia cross sector Pharmacists Intractable patient centered Opioids Interventional Consensus Collaboration Anesthesia Physicians epidural evidence based Intraspinal
HPC hpcconnection.ca Nursing Neuro - axial Analgesia cross sector Pharmacists Intractable patient centered Opioids Interventional Consensus Collaboration Anesthesia Physicians epidural evidence based Intraspinal
Vascular Access. Chapter 3
 Vascular Access Chapter 3 Vascular Access Introduction Obtaining vascular access in infants and children can be difficult even under optimal conditions. Attempting emergent access in a hypotensive, struggling
Vascular Access Chapter 3 Vascular Access Introduction Obtaining vascular access in infants and children can be difficult even under optimal conditions. Attempting emergent access in a hypotensive, struggling
ON-Q * Catheters and Introducers
 Instructions For Use ON-Q * Catheters and Introducers MANUFACTURED BY: Kimberly-Clark 1400 Holcomb Bridge Road Roswell, GA 30076 USA Kimberly-Clark N.V. Da Vincilaan 1 1935 Zaventem, Belgium Figure 1 4
Instructions For Use ON-Q * Catheters and Introducers MANUFACTURED BY: Kimberly-Clark 1400 Holcomb Bridge Road Roswell, GA 30076 USA Kimberly-Clark N.V. Da Vincilaan 1 1935 Zaventem, Belgium Figure 1 4
Your anaesthetist may suggest that you have a spinal or epidural injection. These
 Risks associated with your anaesthetic Section 11: Nerve damage associated with a spinal or epidural injection Your anaesthetist may suggest that you have a spinal or epidural injection. These injections
Risks associated with your anaesthetic Section 11: Nerve damage associated with a spinal or epidural injection Your anaesthetist may suggest that you have a spinal or epidural injection. These injections
PATIENT INFORMATION BOOKLET
 PATIENT INFORMATION BOOKLET Wingspan Stent System with Gateway PTA Balloon Catheter TABLE OF CONTENTS Definitions... 2 What is the Purpose of This Booklet?... 3 What is an Intracranial Lesion?... 3 Who
PATIENT INFORMATION BOOKLET Wingspan Stent System with Gateway PTA Balloon Catheter TABLE OF CONTENTS Definitions... 2 What is the Purpose of This Booklet?... 3 What is an Intracranial Lesion?... 3 Who
STROKE OCCURRENCE SYMPTOMS OF STROKE
 STROKE OCCURRENCE SYMPTOMS OF STROKE The symptoms of stroke depend on what part of the brain is affected and how large an area is involved. A stroke is a sudden event accompanied by one or more of the
STROKE OCCURRENCE SYMPTOMS OF STROKE The symptoms of stroke depend on what part of the brain is affected and how large an area is involved. A stroke is a sudden event accompanied by one or more of the
Traumatic Head Injuries
 Traumatic Brain Injury (TBI) Traumatic Head Injuries Major contributing cause of trauma deaths Many survivors have permanent disability Commonly occurs in young adults (mostly males) Spokane County EMS
Traumatic Brain Injury (TBI) Traumatic Head Injuries Major contributing cause of trauma deaths Many survivors have permanent disability Commonly occurs in young adults (mostly males) Spokane County EMS
Ultrasound in Vascular Surgery. Torbjørn Dahl
 Ultrasound in Vascular Surgery Torbjørn Dahl 1 The field of vascular surgery Veins dilatation and obstruction (varicose veins and valve dysfunction) Arteries dilatation and narrowing (aneurysms and atherosclerosis)
Ultrasound in Vascular Surgery Torbjørn Dahl 1 The field of vascular surgery Veins dilatation and obstruction (varicose veins and valve dysfunction) Arteries dilatation and narrowing (aneurysms and atherosclerosis)
Appropriate Urinary Catheter Use and Management
 Appropriate Urinary Catheter Use and Management Nursing Education Material Mohamad Fakih, MD, MPH 1 This presentation This presentation targets all nurses with patient care responsibilities including the
Appropriate Urinary Catheter Use and Management Nursing Education Material Mohamad Fakih, MD, MPH 1 This presentation This presentation targets all nurses with patient care responsibilities including the
6/3/2011. High Prevalence and Incidence. Low back pain is 5 th most common reason for all physician office visits in the U.S.
 High Prevalence and Incidence Prevalence 85% of Americans will experience low back pain at some time in their life. Incidence 5% annual Timothy C. Shen, M.D. Physical Medicine and Rehabilitation Sub-specialty
High Prevalence and Incidence Prevalence 85% of Americans will experience low back pain at some time in their life. Incidence 5% annual Timothy C. Shen, M.D. Physical Medicine and Rehabilitation Sub-specialty
MISSISSIPPI BOARD OF NURSING IV THERAPY COURSE FOR THE EXPANDED ROLE LICENSED PRACTICAL NURSE COURSE OUTLINE
 THEORY MINIMUM 40 HOURS COURSE OUTLINE UNIT TOPIC HOURS* I LEGAL ASPECTS AND PRACTICE OF IV THERAPY 1 II REVIEW OF ANATOMY AND PHYSIOLOGY 6 III FLUID AND ELECTROLYTE BALANCE 10 IV EQUIPMENT AND PROCEDURES
THEORY MINIMUM 40 HOURS COURSE OUTLINE UNIT TOPIC HOURS* I LEGAL ASPECTS AND PRACTICE OF IV THERAPY 1 II REVIEW OF ANATOMY AND PHYSIOLOGY 6 III FLUID AND ELECTROLYTE BALANCE 10 IV EQUIPMENT AND PROCEDURES
Aspira* Pleural Drainage Catheter
 Aspira* Pleural Drainage Catheter Instructions For Use Access Systems Product Description: The Aspira* Pleural Drainage Catheter is a tunneled, long-term catheter used to drain accumulated fluid from the
Aspira* Pleural Drainage Catheter Instructions For Use Access Systems Product Description: The Aspira* Pleural Drainage Catheter is a tunneled, long-term catheter used to drain accumulated fluid from the
SECTION 12.1 URINARY CATHETERS
 SECTION 12.1 URINARY CATHETERS Introduction Summary of Recommendations taken from Guidelines for the Prevention of Catheter-associated Urinary Tract Infection, Published on behalf of SARI by HSE Health
SECTION 12.1 URINARY CATHETERS Introduction Summary of Recommendations taken from Guidelines for the Prevention of Catheter-associated Urinary Tract Infection, Published on behalf of SARI by HSE Health
Vaxcel PICCs Valved and Non-Valved. A Patient s Guide
 Vaxcel PICCs Valved and Non-Valved A Patient s Guide Information about your Vaxcel PICC is available by calling the Navilyst Medical Vascular Access Information Line 800.513.6876 Vaxcel Peripherally Inserted
Vaxcel PICCs Valved and Non-Valved A Patient s Guide Information about your Vaxcel PICC is available by calling the Navilyst Medical Vascular Access Information Line 800.513.6876 Vaxcel Peripherally Inserted
Perioperative Management of Patients with Obstructive Sleep Apnea. Kalpesh Ganatra,MD Diplomate, American Board of Sleep Medicine
 Perioperative Management of Patients with Obstructive Sleep Apnea Kalpesh Ganatra,MD Diplomate, American Board of Sleep Medicine Disclosures. This activity is supported by an education grant from Trivalley
Perioperative Management of Patients with Obstructive Sleep Apnea Kalpesh Ganatra,MD Diplomate, American Board of Sleep Medicine Disclosures. This activity is supported by an education grant from Trivalley
FERNE / EMRA 2009 Mid-Atlantic Emergency Medicine Medical Student Symposium: ABCs of Head CT Interpretation; Heather M. Prendergast MD, MPH.
 ABCs of Head CT Interpretation in the Emergency Department: CT Interpretation Workshop Guide Heather M. Prendergast, MD, MPH, FACEP Associate Professor Department of Emergency Medicine University of Illinois
ABCs of Head CT Interpretation in the Emergency Department: CT Interpretation Workshop Guide Heather M. Prendergast, MD, MPH, FACEP Associate Professor Department of Emergency Medicine University of Illinois
www.backandspinefl.com Back and Spine Center 509 Riverside Dr., Suite 203 Stuart, FL 34994 Phone: (772) 288-5862
 288-5862") Non-Profit ORG. U.S. Postage PAID West Palm BCH. FL. PERMIT NO. 4709 www.backandspinefl.com Back and Spine Center 509 Riverside Dr., Suite 203 Stuart, FL 34994 Phone: (772) 288-5862 The evolution of neurosurgery
Non-Profit ORG. U.S. Postage PAID West Palm BCH. FL. PERMIT NO. 4709 www.backandspinefl.com Back and Spine Center 509 Riverside Dr., Suite 203 Stuart, FL 34994 Phone: (772) 288-5862 The evolution of neurosurgery
Head and Spinal Cord Injury: Diagnosis and Management
 Head and Spinal Cord Injury: Diagnosis and Management Prashant Chittiboina, MD, MPH a, Hugo Cuellar-Saenz, MD b, Christina Notarianni, MD a, Raul Cardenas, MD c, Bharat Guthikonda, MD a, * KEYWORDS Traumatic
Head and Spinal Cord Injury: Diagnosis and Management Prashant Chittiboina, MD, MPH a, Hugo Cuellar-Saenz, MD b, Christina Notarianni, MD a, Raul Cardenas, MD c, Bharat Guthikonda, MD a, * KEYWORDS Traumatic
Patient Information Guide Morpheus CT Peripherally Inserted Central Catheter
 Patient Information Guide Morpheus CT Peripherally Inserted Central Catheter IC 192 Rev C A measure of flexibility and strength. Table of Contents 1. Introduction 2. What is the Morpheus CT PICC? 3. What
Patient Information Guide Morpheus CT Peripherally Inserted Central Catheter IC 192 Rev C A measure of flexibility and strength. Table of Contents 1. Introduction 2. What is the Morpheus CT PICC? 3. What
Chiari malformations
 A fact sheet for patients and carers Chiari malformations This fact sheet provides information on Chiari malformations. It focuses on Chiari malformations in adults. Our fact sheets are designed as general
A fact sheet for patients and carers Chiari malformations This fact sheet provides information on Chiari malformations. It focuses on Chiari malformations in adults. Our fact sheets are designed as general
APPENDIX B SAMPLE PEDIATRIC CRITICAL CARE NURSE PRACTITIONER GOALS AND OBJECTIVES
 APPENDIX B SAMPLE PEDIATRIC CRITICAL CARE NURSE PRACTITIONER GOALS AND OBJECTIVES The critical care nurse practitioner orientation is an individualized process based on one s previous experiences and should
APPENDIX B SAMPLE PEDIATRIC CRITICAL CARE NURSE PRACTITIONER GOALS AND OBJECTIVES The critical care nurse practitioner orientation is an individualized process based on one s previous experiences and should
The Electronic Medical Record in its entirety can be found on pages 39-54. The EMR is the reading tool that students will use as they complete The
 The Electronic Medical Record in its entirety can be found on pages 39-54. The EMR is the reading tool that students will use as they complete The Virtual Stroke Lab. The idea of the EMR was that students
The Electronic Medical Record in its entirety can be found on pages 39-54. The EMR is the reading tool that students will use as they complete The Virtual Stroke Lab. The idea of the EMR was that students
TCD in Intensive Care
 TCD in Intensive Care Background: Transcranial Doppler (TCD) ultrasonography is a technique that uses a hand-held Doppler transducer (placed on the surface of the cranial skin) to measure the velocity
TCD in Intensive Care Background: Transcranial Doppler (TCD) ultrasonography is a technique that uses a hand-held Doppler transducer (placed on the surface of the cranial skin) to measure the velocity
URINARY CATHETER CARE
 URINARY CATHETER CARE INTRODUCTION Urinary catheter care is a very important skill, and it is a skill that many certified nursing assistants (CNAs) must know. Competence at providing urinary catheter care
URINARY CATHETER CARE INTRODUCTION Urinary catheter care is a very important skill, and it is a skill that many certified nursing assistants (CNAs) must know. Competence at providing urinary catheter care
Minimally Invasive Spine Surgery For Your Patients
 Minimally Invasive Spine Surgery For Your Patients Lukas P. Zebala, M.D. Assistant Professor Orthopaedic and Neurological Spine Surgery Department of Orthopaedic Surgery Washington University School of
Minimally Invasive Spine Surgery For Your Patients Lukas P. Zebala, M.D. Assistant Professor Orthopaedic and Neurological Spine Surgery Department of Orthopaedic Surgery Washington University School of
1-1 THE NERVOUS SYSTEM
 C A S E S T U D Y 1 : N e w b o r n Adapted from Thomson Delmar Learning s Case Study Series: Pediatrics, by Bonita E. Broyles, RN, BSN, MA, PhD. Copyright 2006 Thomson Delmar Learning, Clifton Park, NY.
C A S E S T U D Y 1 : N e w b o r n Adapted from Thomson Delmar Learning s Case Study Series: Pediatrics, by Bonita E. Broyles, RN, BSN, MA, PhD. Copyright 2006 Thomson Delmar Learning, Clifton Park, NY.
Emerging therapies for Intracerebral Hemorrhage
 Emerging therapies for Intracerebral Hemorrhage Chitra Venkat, MBBS, MD, MSc. Associate Professor of Neurology and Neurological Sciences Stroke and Neurocritical Care. Stanford University Learning objectives
Emerging therapies for Intracerebral Hemorrhage Chitra Venkat, MBBS, MD, MSc. Associate Professor of Neurology and Neurological Sciences Stroke and Neurocritical Care. Stanford University Learning objectives
About Normal Pressure Hydrocephalus (NPH) A Book for Adults and Their Families
 A Book for Adults and Their Families") About Normal Pressure Hydrocephalus (NPH) A Book for Adults and Their Families About Normal Pressure Hydrocephalus A Book for Adults and Their Families was written for adults with NPH, their families,
About Normal Pressure Hydrocephalus (NPH) A Book for Adults and Their Families About Normal Pressure Hydrocephalus A Book for Adults and Their Families was written for adults with NPH, their families,
Common Regional Nerve Blocks Quick Guide developed by UWHC Acute Pain Service Jan 2011
 Common Regional Nerve Blocks Quick Guide developed by UWHC Acute Pain Service Jan 2011 A single shot nerve block is the injection of local anesthetic to block a specific nerve distribution. It can be placed
Common Regional Nerve Blocks Quick Guide developed by UWHC Acute Pain Service Jan 2011 A single shot nerve block is the injection of local anesthetic to block a specific nerve distribution. It can be placed
Endovascular Repair of an Axillary Artery Aneurysm: A Novel Approach
 Endovascular Repair of an Axillary Artery Aneurysm: A Novel Approach Bao- Thuy D. Hoang, MD 1, Jonathan- Hien Vu, MD 2, Jerry Matteo, MD 3 1 Department of Surgery, University of Florida College of Medicine,
Endovascular Repair of an Axillary Artery Aneurysm: A Novel Approach Bao- Thuy D. Hoang, MD 1, Jonathan- Hien Vu, MD 2, Jerry Matteo, MD 3 1 Department of Surgery, University of Florida College of Medicine,
Ward 29 guide to the safe preparation and administration of intravenous (IV) antibiotics at home
 antibiotics at home") Ward 29 guide to the safe preparation and administration of intravenous (IV) antibiotics at home Contents Page Important contact numbers 1 General information on preparing and administering IV antibiotics
Ward 29 guide to the safe preparation and administration of intravenous (IV) antibiotics at home Contents Page Important contact numbers 1 General information on preparing and administering IV antibiotics
Minimally Invasive Spine Surgery
 Chapter 1 Minimally Invasive Spine Surgery 1 H.M. Mayer Primum non nocere First do no harm In the long history of surgery it always has been a basic principle to restrict the iatrogenic trauma done to
Chapter 1 Minimally Invasive Spine Surgery 1 H.M. Mayer Primum non nocere First do no harm In the long history of surgery it always has been a basic principle to restrict the iatrogenic trauma done to
DISCHARGE CRITERIA FOR PHASE I & II- POST ANESTHESIA CARE
 REFERENCES: The Joint Commission Accreditation Manual for Hospitals American Society of Post Anesthesia Nurses: Standards of Post Anesthesia Nursing Practice (1991, 2002). RELATED DOCUMENTS: SHC Administrative
REFERENCES: The Joint Commission Accreditation Manual for Hospitals American Society of Post Anesthesia Nurses: Standards of Post Anesthesia Nursing Practice (1991, 2002). RELATED DOCUMENTS: SHC Administrative
Liau DW : Injuries and Liability Related to Peripheral Catheters: A Closed Claims Analysis. ASA Newsletter 70(6): 11-13 & 16, 2006.
: 11-13 & 16, 2006.") Citation Liau DW : Injuries and Liability Related to Peripheral Catheters: A Closed Claims Analysis. ASA Newsletter 70(6): 11-13 & 16, 2006. Full Text An anesthesiologist inserted a 14-gauge peripheral
Citation Liau DW : Injuries and Liability Related to Peripheral Catheters: A Closed Claims Analysis. ASA Newsletter 70(6): 11-13 & 16, 2006. Full Text An anesthesiologist inserted a 14-gauge peripheral
Neuroimaging of Headache. Kenneth D. Williams, MD
 Neuroimaging of Headache Kenneth D. Williams, MD Disclosures Financial: None Off Label Usage: None Key Points Headache is an extremely common symptom. Structural abnormalities (Primary HA) are rare. Clinical
Neuroimaging of Headache Kenneth D. Williams, MD Disclosures Financial: None Off Label Usage: None Key Points Headache is an extremely common symptom. Structural abnormalities (Primary HA) are rare. Clinical
20. Cerebral Compartmental Compliances
 20. Cerebral Compartmental Compliances CBF a (t) Cerebral arterial inflow Cerebral arterial blood volume (C a BV) mean CBF a 0 CBF v (t) Cerebral venous outflow CBV(t) mean CBV + - t t ΔCBV (CBF (t) CBF
20. Cerebral Compartmental Compliances CBF a (t) Cerebral arterial inflow Cerebral arterial blood volume (C a BV) mean CBF a 0 CBF v (t) Cerebral venous outflow CBV(t) mean CBV + - t t ΔCBV (CBF (t) CBF
Corporate Medical Policy
 File Name: anesthesia_services Origination: 8/2007 Last CAP Review: 1/2016 Next CAP Review: 1/2017 Last Review: 1/2016 Corporate Medical Policy Description of Procedure or Service There are three main
File Name: anesthesia_services Origination: 8/2007 Last CAP Review: 1/2016 Next CAP Review: 1/2017 Last Review: 1/2016 Corporate Medical Policy Description of Procedure or Service There are three main
Anesthesia Billing: 101. Presented by: Medi-Corp, Inc www.medi-corp.com
 Anesthesia Billing: 101 Presented by: Medi-Corp, Inc www.medi-corp.com Disclaimer Statement The material enclosed is based on information that is in effect at the time of this presentation. This presentation
Anesthesia Billing: 101 Presented by: Medi-Corp, Inc www.medi-corp.com Disclaimer Statement The material enclosed is based on information that is in effect at the time of this presentation. This presentation
Advances In Spine Care. James D. Bruffey M.D. Scripps Clinic Division of Orthopaedic Surgery Section of Spinal Surgery
 Advances In Spine Care James D. Bruffey M.D. Scripps Clinic Division of Orthopaedic Surgery Section of Spinal Surgery Introduction The Spine - A common source of problems Back pain is the #2 presenting
Advances In Spine Care James D. Bruffey M.D. Scripps Clinic Division of Orthopaedic Surgery Section of Spinal Surgery Introduction The Spine - A common source of problems Back pain is the #2 presenting