Pressure reactivity: Relationship between ICP and arterial blood pressure (ABP). Pressure-reactivity index, computational methods. Clinical examples.
|
|
|
- Mildred Phelps
- 9 years ago
- Views:
Transcription
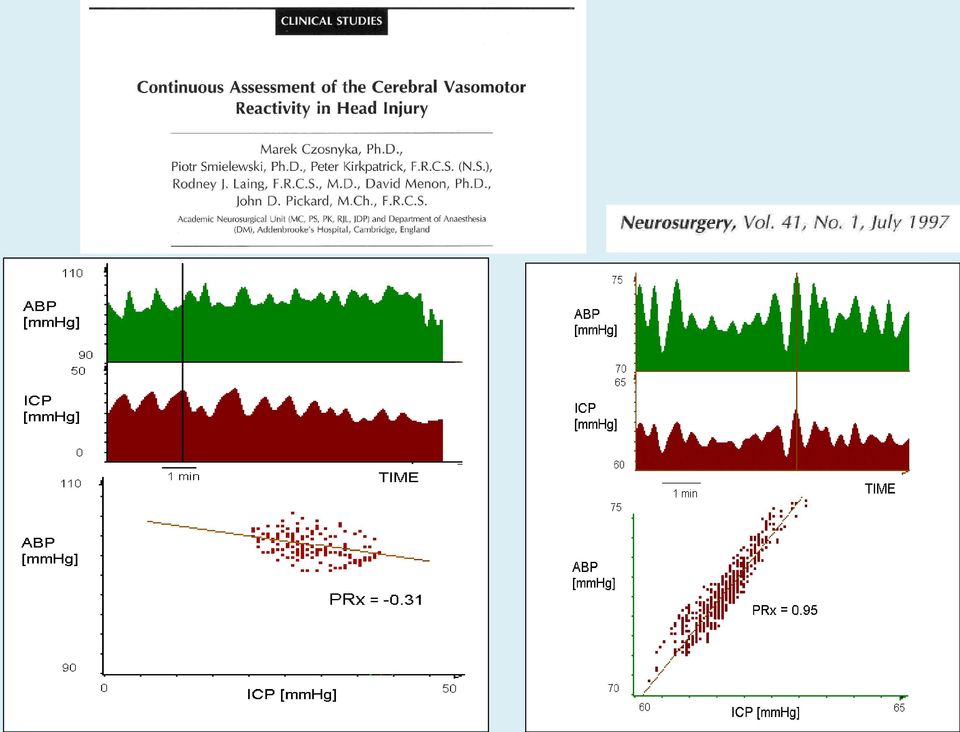
1 Pressure reactivity: Relationship between ICP and arterial blood pressure (ABP). Pressure-reactivity index, computational methods. Clinical examples. Optimization of cerebral perfusion pressure: Relationship between Pressure Reactivity and CPP. Does optimal CPP exist always? Implications on management.

2 Simultaneous analysis of slow changes in arterial pressure and ICP System with disturbed pressurereactivity Pressurereactivity works properly

3

4 Thanks to Dr.P.Smielewski PRx- Calculation principles Input signals ICP, ABP Ouput trend PRx ABP 10 sec window 5 min window MAP Mean(ABP) Mean(ICP) MICP ICP Correlation(MAP, MICP) Primary analysis Final Analysis
 Mean(ICP) MICP ICP")

5 PRx is a rather noisy parameter Some smoothing is required PRx Smoothed PRx Thanks to Dr.P.Smielewski


6 Coherence Unknown origin of micp fluctuations Low coherence between ABP and ICP suggests limited contribution from ABP, however it could also be an evidence of strong nonlinearities MAP MICP Frequency [Hz] 1 Hz Thanks to Dr.P.Smielewski

7 Detrended Thanks to Dr.P.Smielewski Confounding factors: trends MAP MICP MAP_dt MICP_dt MICP PRx = < 0! MAP MICP_dt PRx = 0.54 > 0! MAP_dt

8 Detrending example: raw signals ABP ICP 20 min period Thanks to Dr.P.Smielewski

9 Detrending example: after low pass filter MAP MICP 20 min period Thanks to Dr.P.Smielewski


10 Detrending example: high pass filter method MAP_dt MICP_dt 20 min period Thanks to Dr.P.Smielewski

11 Intracranial Hypertension

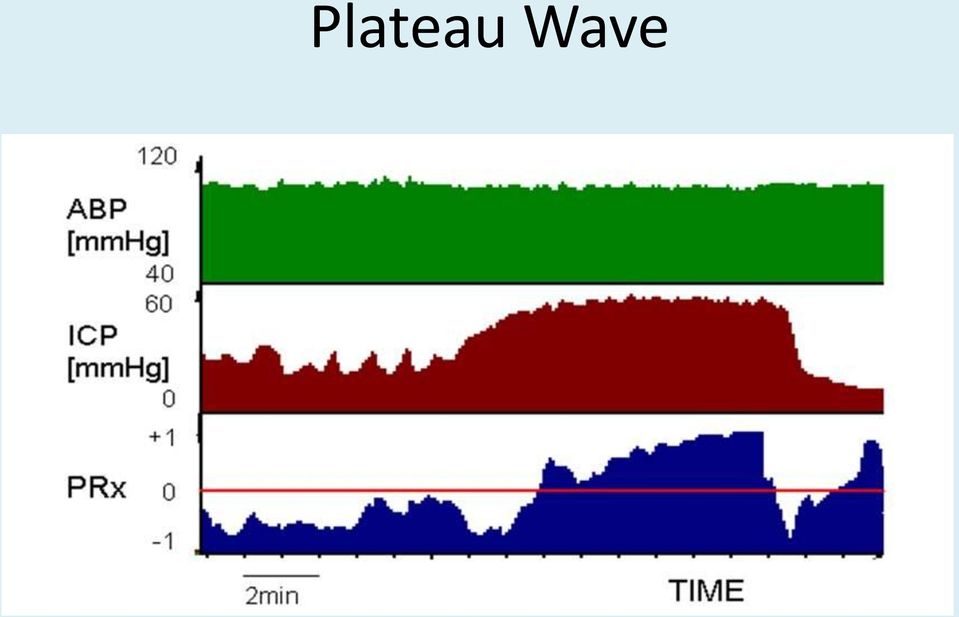
12 Plateau Wave
13 Arterial Hypertension

14 CT Scan 1 Scan 2 SROR (CPP = 74 mmhg) (CPP = 98 mmhg) 5 60% % % 0.4 Figure 5: PET vs. PRx PRx r 2 = 0.32 p = 0.02 (n = 17) PRx correlates with PET-static rate of autoregulation Global SROR PET Steiner LA, Coles JP, Johnston AJ, Chatfield DA, Smielewski P, Fryer TD, Aigbirhio FI, Clark JC, Pickard JD, Menon DK, Czosnyka M. Assessment of Cerebrovascular Autoregulation in Head-Injured Patients. A Validation Study.Stroke :

 -0.")
15 rcbf CMRO 2 OEF 0-30 ml/100g/min m/100g/min 0-75 % r 2 = 0.34 p = r 2 = 0.61 p < PRx 0.2 PRx global CMRO 2 (ml 100g -1 min -1 ) Global oxygen extraction fraction (%)
 -0.")

16 FLUX ICP ABP PRx and the LLA ABP lowered to zero in piglet LDF vs. CPP to find lower limit of autoregulation PRx compared against LLA Brady K, et al: Stroke 2008 Lee J, et al: Stroke 2009


17 Individual trends are most important



18 Monitoring of Pressure Reactivity Index ICM+ software:


19 Ups and downs... Final was not very optimistic

20 Deterioration of PRx precedes refractory intracranial hypertension?

 ABP mmhg ICP mmhg")
21 Refractory intracranial hypertension (2) ABP mmhg ICP mmhg PRx CPP mmhg

22 Advancing intracranial hypertension- fatal outcome
23 Optimal CPP- oriented therapy PRx PRx Mx Both PRx and Mx show the U-shape relationship with mean CPP (200 patients!). This indicate that for low CPP and CPP above 90 mm Hg both autoregulation and pressure reactivity are defective. There is an optimal CPP from 70 to 90 mm Hg which helps to restore vascular functions after head injury a.) a.) Optimal CPP Cerebral Perfus ion Press ure (mm Hg) Cerebral Perfus ion Press ure (mm Hg) Steiner LA at al. Continuous monitoring of cerebrovascular pressure reactivity allows determination of optimal cerebral perfusion pressure in patients with traumatic brain injury. Crit Care Med Apr;30(4):733-8.
24 New results Thanks to Dr. M.Aries

25 If we can see it in statistical evaluation of big series of patients, can we see it in individual cases? 4 6 hours moving window The chart shows that lowest PRx values corresponding to the strongest autoregulation level fall in the CPP range of mmhg Thanks to Dr. P.Smielewski
26 Optimal CPP in individual cases Thanks to Dr.L.Steiner
27 Optimal CPP oriented therapy? CPPopt ADMISSION TO CRITICAL CARE UNIT START TREATMENT AT CPP 70 MM HG (OR HIGHER IN SEVERLY HEAD INJURED PATIENTS) MONITOR AND AVERAGE PRx FOR 2 HOURS Patient 1 IDENTIFY RANGE OF MINIMAL PRx BY VARYING CPP IN STEPS OF 10 mm Hg OVER 2 HOUR PERIODS CPP OPT IDENTIFIED CALCULATE CPP OPT NO CPP OPT Hours MINIMIZE CPP CPP OPT DURING THE FOLLOWING 2 HOURS MONITOR AND MINIMIZE PRx, POOL DATA AFTER 2 HOURS Steiner LA, Czosnyka M, Piechnik SK, Smielewski P, Chatfield D, Menon DK, Pickard JD. Continuous monitoring of cerebrovascular pressure reactivity allows determination of optimal cerebral perfusion pressure in patients with traumatic brain injury. Crit Care Med Apr;30(4):733-8.
28 CPP OPT and Outcome r = (Spearman rank test) p = Thanks to Dr. L.Steiner
29 What do we know so far about PRx in SAH? (statin trial, placebo branch). PRx agrees with Transient Hyperaemic Response Test and gets worse in vasospasm Tseng MY, Czosnyka M, Richards H, Pickard JD, Kirkpatrick PJ. Effects of acute treatment with pravastatin on cerebral vasospasm, autoregulation, and delayed ischemic deficits after aneurysmal subarachnoid hemorrhage: a phase II randomized placebo-controlled trial. Stroke Aug;36(8):
30 Prx SAH: Effect of Vasospasm CPP [mmhg] Thanks to Dr. P.Biljenga
31 PRx PRx SAH: Effect of Hypertonic Saline 1.0 PRx improvement N= Before HS perfusion During HS perfusion After HS perfusion CPP[mmHg] CPP opt increase N=7 CPP opt [mmhg] Thanks to Dr. P.Biljenga

32
33 Temporal profiles of cerebrovascular pressure reactivity in children with traumatic brain injury Prospective observational study, commenced 2006 Undertaken at the state of Victoria s tertiary paediatric hospital, the Royal Children s Hospital (RCH) Aims: Establish monitoring of PRx in children with TBI at the RCH Investigate PRx vs time PRx vs CPP PRx vs outcome Thanks to Mr. P.Lewis
34 Patients / Data n=23 patients Age range 4-16 years All severe TBI (GCS 3-8) on admission All received ICP monitoring via parenchymal or fluidcoupled monitoring (EVD) Continuous recording of ABP, ICP, EtCO2 from admission until removal of ICP monitor Range: 1-11 days Median recording length: 3 days Not all monitored days able to be analysed Continuous drainage from EVD ICM+ Codman Thanks to Mr. P.Lewis
35 PRx vs CPP (pooled) Thanks to Mr. P.Lewis
36 Summary Simple analysis of ABP-ICP interaction (low bandwidth) Positive association with outcome Detection of optimal CPP Good agreement with other more expensive methods Promising value of PRx after SAH
perfusion pressure: Definitions. Implication on management protocols. What happens when CPP is too low, and when it is too high? Non-invasive CPP?
 7. Cerebral perfusion pressure: Definitions. Implication on management protocols. What happens when CPP is too low, and when it is too high? Non-invasive CPP? Definitions of CPP Thanks to Dr. E. Schmidt
7. Cerebral perfusion pressure: Definitions. Implication on management protocols. What happens when CPP is too low, and when it is too high? Non-invasive CPP? Definitions of CPP Thanks to Dr. E. Schmidt
13. Volume-pressure infusion tests: Typical patterns of infusion studies in different forms of CSF circulatory disorders.
 13. Volume-pressure infusion tests: Typical patterns of infusion studies in different forms of CSF circulatory disorders. Hydrocephalus is far more complex than disorder of CSF circulation CSF circulation
13. Volume-pressure infusion tests: Typical patterns of infusion studies in different forms of CSF circulatory disorders. Hydrocephalus is far more complex than disorder of CSF circulation CSF circulation
10. Monitoring of pressure-volume compensation- VPR and RAP
 10. Monitoring of pressure-volume compensation- VPR and RAP Various shapes of Pressure-Volume curves J.Neurosurg 1975, Vol 42 Volume pressure response is proportional to mean ICP but not always Avezaat
10. Monitoring of pressure-volume compensation- VPR and RAP Various shapes of Pressure-Volume curves J.Neurosurg 1975, Vol 42 Volume pressure response is proportional to mean ICP but not always Avezaat
Monitoring of Cerebral Blood Flow. Transcranial Doppler Laser Doppler Flowmetry Thermal dilution method (Hemedex)
") Monitoring of Cerebral Blood Flow Transcranial Doppler Laser Doppler Flowmetry Thermal dilution method (Hemedex) Ultrasound in Tissue Some Facts: blood cell tissue probe ultrasound travels at a constant
Monitoring of Cerebral Blood Flow Transcranial Doppler Laser Doppler Flowmetry Thermal dilution method (Hemedex) Ultrasound in Tissue Some Facts: blood cell tissue probe ultrasound travels at a constant
20. Cerebral Compartmental Compliances
 20. Cerebral Compartmental Compliances CBF a (t) Cerebral arterial inflow Cerebral arterial blood volume (C a BV) mean CBF a 0 CBF v (t) Cerebral venous outflow CBV(t) mean CBV + - t t ΔCBV (CBF (t) CBF
20. Cerebral Compartmental Compliances CBF a (t) Cerebral arterial inflow Cerebral arterial blood volume (C a BV) mean CBF a 0 CBF v (t) Cerebral venous outflow CBV(t) mean CBV + - t t ΔCBV (CBF (t) CBF
Statistical Analysis of Arterial Blood Pressure (ABP), Central Venous. Pressure (CVP), and Intracranial Pressure (ICP)
, Central Venous. Pressure (CVP), and Intracranial Pressure (ICP)") Statistical Analysis of Arterial Blood Pressure (ABP), Central Venous Pressure (CVP), and Intracranial Pressure (ICP) Heechang Kim, Member, IEEE Portland State University E-mail: [email protected] This
Statistical Analysis of Arterial Blood Pressure (ABP), Central Venous Pressure (CVP), and Intracranial Pressure (ICP) Heechang Kim, Member, IEEE Portland State University E-mail: [email protected] This
Clinical Research Software for Intensive Care Monitoring
 The past, the present and the future Clinical Research Software for Intensive Care Monitoring Dr Peter Smielewski Dept of Clinical Neurosciences University of Cambridge Disclosure ICM+ software is licensed
The past, the present and the future Clinical Research Software for Intensive Care Monitoring Dr Peter Smielewski Dept of Clinical Neurosciences University of Cambridge Disclosure ICM+ software is licensed
Cerebral blood flow (CBF) is dependent on a number of factors that can broadly be divided into:
 is dependent on a number of factors that can broadly be divided into:") Cerebral Blood Flow and Intracranial Pressure Dr Lisa Hill, SpR Anaesthesia, Royal Oldham Hospital, UK. Email [email protected] Dr Carl Gwinnutt, Consultant Neuroanaesthetist, Hope Hospital, UK. The
Cerebral Blood Flow and Intracranial Pressure Dr Lisa Hill, SpR Anaesthesia, Royal Oldham Hospital, UK. Email [email protected] Dr Carl Gwinnutt, Consultant Neuroanaesthetist, Hope Hospital, UK. The
THERAPY INTENSITY LEVEL
 THERAPY INTENSITY LEVEL TILBasic = TIL Basic. CDE Variable TILBasic = TIL Basic; Global summary measure of Therapy Intensity Level for control of Intracranial Pressure (ICP).. CDE Definition This summary
THERAPY INTENSITY LEVEL TILBasic = TIL Basic. CDE Variable TILBasic = TIL Basic; Global summary measure of Therapy Intensity Level for control of Intracranial Pressure (ICP).. CDE Definition This summary
Using the Pupillometer in Clinical Practice
 Using the Pupillometer in Clinical Practice Claude Hemphill MD M.A.S. [email protected] Kathy Johnson RN, MSN [email protected] Mary Kay Bader RN, MSN, CCNS [email protected] Pupillometry: How It
Using the Pupillometer in Clinical Practice Claude Hemphill MD M.A.S. [email protected] Kathy Johnson RN, MSN [email protected] Mary Kay Bader RN, MSN, CCNS [email protected] Pupillometry: How It
TCD in Intensive Care
 TCD in Intensive Care Background: Transcranial Doppler (TCD) ultrasonography is a technique that uses a hand-held Doppler transducer (placed on the surface of the cranial skin) to measure the velocity
TCD in Intensive Care Background: Transcranial Doppler (TCD) ultrasonography is a technique that uses a hand-held Doppler transducer (placed on the surface of the cranial skin) to measure the velocity
Threshold-based Use of Brain Oxygen Monitor and Seizure Detection
 Threshold-based Use of Brain Oxygen Monitor and Seizure Detection Alex Roederer, Jonathan Tannen, Soojin Park M.D. University of Pennsylvania {a1,a2,a3,a4}@seas.upenn.edu July 13, 2010 Abstract Brain tissue
Threshold-based Use of Brain Oxygen Monitor and Seizure Detection Alex Roederer, Jonathan Tannen, Soojin Park M.D. University of Pennsylvania {a1,a2,a3,a4}@seas.upenn.edu July 13, 2010 Abstract Brain tissue
King County EMS Stroke Quality Improvement Program
 King County EMS Stroke Quality Improvement Program A Report from the King County EMS Medical QI Section March 2012 Prepared by Sofia Husain, Jim Duren, and Norm Nedell OBJECTIVE The goal of the King County
King County EMS Stroke Quality Improvement Program A Report from the King County EMS Medical QI Section March 2012 Prepared by Sofia Husain, Jim Duren, and Norm Nedell OBJECTIVE The goal of the King County
The Clinical Evaluation of the Comatose Patient in the Emergency Department
 The Clinical Evaluation of the Comatose Patient in the Emergency Department patients with altered mental status (AMS) and coma. treat patients who present to the Emergency Department with altered mental
The Clinical Evaluation of the Comatose Patient in the Emergency Department patients with altered mental status (AMS) and coma. treat patients who present to the Emergency Department with altered mental
THE INTERNET STROKE CENTER PRESENTATIONS AND DISCUSSIONS ON STROKE MANAGEMENT
 THE INTERNET STROKE CENTER PRESENTATIONS AND DISCUSSIONS ON STROKE MANAGEMENT Stroke Prevention in Atrial Fibrillation Gregory Albers, M.D. Director Stanford Stroke Center Professor of Neurology and Neurological
THE INTERNET STROKE CENTER PRESENTATIONS AND DISCUSSIONS ON STROKE MANAGEMENT Stroke Prevention in Atrial Fibrillation Gregory Albers, M.D. Director Stanford Stroke Center Professor of Neurology and Neurological
Clinical Medical Policy Cognitive Rehabilitation
 Benefit Coverage Outpatient cognitive rehabilitation is considered to be the most appropriate setting for members who have sustained a traumatic brain injury or an acute brain insult. Covered Benefit for
Benefit Coverage Outpatient cognitive rehabilitation is considered to be the most appropriate setting for members who have sustained a traumatic brain injury or an acute brain insult. Covered Benefit for
2.2 Elimination of Trend and Seasonality
 26 CHAPTER 2. TREND AND SEASONAL COMPONENTS 2.2 Elimination of Trend and Seasonality Here we assume that the TS model is additive and there exist both trend and seasonal components, that is X t = m t +
26 CHAPTER 2. TREND AND SEASONAL COMPONENTS 2.2 Elimination of Trend and Seasonality Here we assume that the TS model is additive and there exist both trend and seasonal components, that is X t = m t +
Head Injury. Dr Sally McCarthy Medical Director ECI
 Head Injury Dr Sally McCarthy Medical Director ECI Head injury in the emergency department A common presentation 80% Mild Head Injury = GCS 14 15 10% Moderate Head Injury = GCS 9 13 10% Severe Head Injury
Head Injury Dr Sally McCarthy Medical Director ECI Head injury in the emergency department A common presentation 80% Mild Head Injury = GCS 14 15 10% Moderate Head Injury = GCS 9 13 10% Severe Head Injury
Plumbing 101:! TXA and EMS! Jay H. Reich, MD FACEP! EMS Medical Director! City of Kansas City, Missouri/Kansas City Fire Department!
 Plumbing 101:! TXA and EMS! Jay H. Reich, MD FACEP! EMS Medical Director! City of Kansas City, Missouri/Kansas City Fire Department! EMS Section Chief! Department of Emergency Medicine! University of Missouri-Kansas
Plumbing 101:! TXA and EMS! Jay H. Reich, MD FACEP! EMS Medical Director! City of Kansas City, Missouri/Kansas City Fire Department! EMS Section Chief! Department of Emergency Medicine! University of Missouri-Kansas
1. Cerebrospainal Fluid (CSF) circulation in brain: Sites and mechanisms of CSF secretion, circulation and reabsorption. Physiological and modelling
 circulation in brain: Sites and mechanisms of CSF secretion, circulation and reabsorption. Physiological and modelling") 1. Cerebrospainal Fluid (CSF) circulation in brain: Sites and mechanisms of CSF secretion, circulation and reabsorption. Physiological and modelling description. Cerebrospinal space Brain lump in a box?
1. Cerebrospainal Fluid (CSF) circulation in brain: Sites and mechanisms of CSF secretion, circulation and reabsorption. Physiological and modelling description. Cerebrospinal space Brain lump in a box?
Imaging of Acute Stroke. Noam Eshkar, M.D New Jersey Neuroscience Institute JFK Medical Center Edison Radiology Group
 Imaging of Acute Stroke Noam Eshkar, M.D New Jersey Neuroscience Institute JFK Medical Center Edison Radiology Group Modalities Non Contrast CT (NCCT) Contrast CT Angiography MRI MR Angiography Perfusion
Imaging of Acute Stroke Noam Eshkar, M.D New Jersey Neuroscience Institute JFK Medical Center Edison Radiology Group Modalities Non Contrast CT (NCCT) Contrast CT Angiography MRI MR Angiography Perfusion
Making the Case for CPG s Jean Luciano, MSN, RN, CNRN, SCRN, CRNP, FAHA Claranne Mathiesen, MSN, RN, CNRN, SCRN, FAHA
 Making the Case for CPG s Jean Luciano, MSN, RN, CNRN, SCRN, CRNP, FAHA Claranne Mathiesen, MSN, RN, CNRN, SCRN, FAHA Disclosures Jeanie Luciano Genentech speakers bureau Claranne Mathiesen - none 1 Objective
Making the Case for CPG s Jean Luciano, MSN, RN, CNRN, SCRN, CRNP, FAHA Claranne Mathiesen, MSN, RN, CNRN, SCRN, FAHA Disclosures Jeanie Luciano Genentech speakers bureau Claranne Mathiesen - none 1 Objective
Medical Management of Ischemic Stroke: An Update. Siddharth Sehgal, MD Medical Director, TMH Neuroscience Center
 Medical Management of Ischemic Stroke: An Update Siddharth Sehgal, MD Medical Director, TMH Neuroscience Center Objectives Diagnostic evaluation and management of acute ischemic stroke. Inpatient management
Medical Management of Ischemic Stroke: An Update Siddharth Sehgal, MD Medical Director, TMH Neuroscience Center Objectives Diagnostic evaluation and management of acute ischemic stroke. Inpatient management
ROLE OF LDL CHOLESTEROL, HDL CHOLESTEROL AND TRIGLYCERIDES IN THE PREVENTION OF CORONARY HEART DISEASE AND STROKE
 ROLE OF LDL CHOLESTEROL, HDL CHOLESTEROL AND TRIGLYCERIDES IN THE PREVENTION OF CORONARY HEART DISEASE AND STROKE I- BACKGROUND: Coronary artery disease and stoke are the major killers in the United States.
ROLE OF LDL CHOLESTEROL, HDL CHOLESTEROL AND TRIGLYCERIDES IN THE PREVENTION OF CORONARY HEART DISEASE AND STROKE I- BACKGROUND: Coronary artery disease and stoke are the major killers in the United States.
Accreditation and Certification Guidelines
 Accreditation and Certification Guidelines MARTIN GIZZI, MD, PHD, FAHA CHAIR, NJ NEUROSCIENCE INSTITUTE AT JFK CHAIR, NORTH EAST CEREBROVASCULAR CONSORTIUM (NECC) CHAIR, STROKE ADVISORY PANEL, NJDOH MEMBER,
Accreditation and Certification Guidelines MARTIN GIZZI, MD, PHD, FAHA CHAIR, NJ NEUROSCIENCE INSTITUTE AT JFK CHAIR, NORTH EAST CEREBROVASCULAR CONSORTIUM (NECC) CHAIR, STROKE ADVISORY PANEL, NJDOH MEMBER,
New Treatments for Stroke Prevention in Atrial Fibrillation. John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013
 New Treatments for Stroke Prevention in Atrial Fibrillation John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013 Classification Paroxysmal atrial fibrillation (AF) Last < 7
New Treatments for Stroke Prevention in Atrial Fibrillation John C. Andrefsky, MD, FAHA NEOMED Internal Medicine Review course May 5 th, 2013 Classification Paroxysmal atrial fibrillation (AF) Last < 7
Epinephrine in CPR. The 5 Most Important EMS Articles EAGLES 2014. Epi vs No-Epi Take Homes 2/28/2014. VF/VT (1990 Pairs) Epi vs No-Epi
 Epi vs No-Epi") The 5 Most Important EMS Articles EAGLES 214 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN nephrine in CPR VF/VT
The 5 Most Important EMS Articles EAGLES 214 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN nephrine in CPR VF/VT
How To Monitor Csp For A Patient
 ICM plus - a Versatile Software for Assessment of CSF Dynamics Zofia Czosnyka MD; Angelos G. Kolias MSc, MRCS; Peter Smielewski; Marek Czosnyka; John Douglas Pickard Addenbrooke s Hospital & University
ICM plus - a Versatile Software for Assessment of CSF Dynamics Zofia Czosnyka MD; Angelos G. Kolias MSc, MRCS; Peter Smielewski; Marek Czosnyka; John Douglas Pickard Addenbrooke s Hospital & University
APPENDIX A NEUROLOGIST S GUIDE TO USING ICD-9-CM CODES FOR CEREBROVASCULAR DISEASES INTRODUCTION
 APPENDIX A NEUROLOGIST S GUIDE TO USING ICD-9-CM CODES FOR CEREBROVASCULAR DISEASES INTRODUCTION ICD-9-CM codes for cerebrovascular diseases is not user friendly. This presentation is designed to assist
APPENDIX A NEUROLOGIST S GUIDE TO USING ICD-9-CM CODES FOR CEREBROVASCULAR DISEASES INTRODUCTION ICD-9-CM codes for cerebrovascular diseases is not user friendly. This presentation is designed to assist
The 5 Most Important EMS Articles EAGLES 2014
 The 5 Most Important EMS Articles EAGLES 2014 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
The 5 Most Important EMS Articles EAGLES 2014 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
GP workshop. Maria Fitzpatrick Nurse Consultant Kings College Stroke Centre
 GP workshop Maria Fitzpatrick Nurse Consultant Kings College Stroke Centre Stroke: the Facts Stroke: the Facts Every 5 minutes someone in the UK has a stroke 1 in 4 men and 1 in 5 women will have a stroke
GP workshop Maria Fitzpatrick Nurse Consultant Kings College Stroke Centre Stroke: the Facts Stroke: the Facts Every 5 minutes someone in the UK has a stroke 1 in 4 men and 1 in 5 women will have a stroke
Hummi Micro Draw Blood Transfer Device. The Next Generation System for Closed Micro Blood Sampling in the Neonate
 Hummi Micro Draw Blood Transfer Device The Next Generation System for Closed Micro Blood Sampling in the Neonate Current Methods for Umbilical Blood Sampling Current Methods for Umbilical Blood Sampling
Hummi Micro Draw Blood Transfer Device The Next Generation System for Closed Micro Blood Sampling in the Neonate Current Methods for Umbilical Blood Sampling Current Methods for Umbilical Blood Sampling
Malmö Preventive Project. Cardiovascular Endpoints
 Malmö Preventive Project Department of Clinical Sciences Malmö University Hospital Lund University Malmö Preventive Project Cardiovascular Endpoints End of follow-up: 31 Dec 2008 * Report: 21 June 2010
Malmö Preventive Project Department of Clinical Sciences Malmö University Hospital Lund University Malmö Preventive Project Cardiovascular Endpoints End of follow-up: 31 Dec 2008 * Report: 21 June 2010
What is the Future of Epinephrine in Cardiac Arrest? Pros and Cons
 What is the Future of Epinephrine in Cardiac Arrest? Pros and Cons Melissa L. Thompson Bastin, PharmD., BCPS Komal A. Pandya, PharmD., BCPS 0 Presenter Disclosure Information Melissa L. Thompson Bastin,
What is the Future of Epinephrine in Cardiac Arrest? Pros and Cons Melissa L. Thompson Bastin, PharmD., BCPS Komal A. Pandya, PharmD., BCPS 0 Presenter Disclosure Information Melissa L. Thompson Bastin,
Acute Myocardial Infarction (the formulary thrombolytic for AMI at AAMC is TNK, please see the TNK monograph in this manual for information)
") ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Alteplase (Tissue Plasminogen Activator (t-pa)), Activase in the Treatment
ANNE ARUNDEL MEDICAL CENTER CRITICAL CARE MEDICATION MANUAL DEPARTMENT OF NURSING AND PHARMACY Guidelines for Use of Intravenous Alteplase (Tissue Plasminogen Activator (t-pa)), Activase in the Treatment
Functional neuroimaging. Imaging brain function in real time (not just the structure of the brain).
.") Functional neuroimaging Imaging brain function in real time (not just the structure of the brain). The brain is bloody & electric Blood increase in neuronal activity increase in metabolic demand for glucose
Functional neuroimaging Imaging brain function in real time (not just the structure of the brain). The brain is bloody & electric Blood increase in neuronal activity increase in metabolic demand for glucose
ADVANCE: a factorial randomised trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 ADVANCE: a factorial randomised trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Effects of a fixed combination of the ACE inhibitor, perindopril,
ADVANCE: a factorial randomised trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Effects of a fixed combination of the ACE inhibitor, perindopril,
TIME LOST IS BRAIN LOST. TARGET: STROKE CAMPAIGN MANUAL
 TIME LOST IS BRAIN LOST. TARGET: STROKE CAMPAIGN MANUAL 2010, American Heart Association TARGET: STROKE CAMPAIGN MANUAL 01 INTRODUCTION Welcome to the Target: Stroke. The purpose of this manual is to provide
TIME LOST IS BRAIN LOST. TARGET: STROKE CAMPAIGN MANUAL 2010, American Heart Association TARGET: STROKE CAMPAIGN MANUAL 01 INTRODUCTION Welcome to the Target: Stroke. The purpose of this manual is to provide
Malmö Preventive Project. Cardiovascular Endpoints
 Malmö Preventive Project Department of Clinical Sciences Skåne University Hospital, Malmö Lund University Malmö Preventive Project Cardiovascular Endpoints End of follow-up: 30 June 2009 Report: 7 October
Malmö Preventive Project Department of Clinical Sciences Skåne University Hospital, Malmö Lund University Malmö Preventive Project Cardiovascular Endpoints End of follow-up: 30 June 2009 Report: 7 October
Medical Direction and Practices Board WHITE PAPER
 Medical Direction and Practices Board WHITE PAPER Use of Pressors in Pre-Hospital Medicine: Proper Indication and State of the Science Regarding Proper Choice of Pressor BACKGROUND Shock is caused by a
Medical Direction and Practices Board WHITE PAPER Use of Pressors in Pre-Hospital Medicine: Proper Indication and State of the Science Regarding Proper Choice of Pressor BACKGROUND Shock is caused by a
DIAGNOSTIC CRITERIA OF STROKE
 DIAGNOSTIC CRITERIA OF STROKE Diagnostic criteria are used to validate clinical diagnoses. Here below MONICA diagnostic criteria are reported. MONICA - MONItoring trends and determinants of CArdiovascular
DIAGNOSTIC CRITERIA OF STROKE Diagnostic criteria are used to validate clinical diagnoses. Here below MONICA diagnostic criteria are reported. MONICA - MONItoring trends and determinants of CArdiovascular
Extracorporeal Life Support Organization (ELSO) Guidelines for Neonatal Respiratory Failure
 Guidelines for Neonatal Respiratory Failure") Extracorporeal Life Support Organization (ELSO) Guidelines for Neonatal Respiratory Failure Introduction This neonatal respiratory failure guideline is a supplement to ELSO s General Guidelines for all
Extracorporeal Life Support Organization (ELSO) Guidelines for Neonatal Respiratory Failure Introduction This neonatal respiratory failure guideline is a supplement to ELSO s General Guidelines for all
Diabetic Ketoacidosis
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Diabetic Ketoacidosis Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Diabetic Ketoacidosis Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
ALBERTA PROVINCIAL STROKE STRATEGY (APSS)
") ALBERTA PROVINCIAL STROKE STRATEGY (APSS) Stroke Systems of Care Key Components APSS Pillar Recommendations March 28, 2007 1 The following is a summary of the key components and APSS Pillar recommendations
ALBERTA PROVINCIAL STROKE STRATEGY (APSS) Stroke Systems of Care Key Components APSS Pillar Recommendations March 28, 2007 1 The following is a summary of the key components and APSS Pillar recommendations
Lothian Diabetes Handbook MANAGEMENT OF DIABETIC KETOACIDOSIS
 MANAGEMENT OF DIABETIC KETOACIDOSIS 90 MANAGEMENT OF DIABETIC KETOACIDOSIS Diagnosis elevated plasma and/or urinary ketones metabolic acidosis (raised H + /low serum bicarbonate) Remember that hyperglycaemia,
MANAGEMENT OF DIABETIC KETOACIDOSIS 90 MANAGEMENT OF DIABETIC KETOACIDOSIS Diagnosis elevated plasma and/or urinary ketones metabolic acidosis (raised H + /low serum bicarbonate) Remember that hyperglycaemia,
Cardiovascular Endpoints
 The Malmö Diet and Cancer Study Department of Clinical Sciences Malmö University Hospital Lund University The Malmö Diet and Cancer Study CV-cohort Cardiovascular Endpoints End of follow-up: 31 Dec * Report:
The Malmö Diet and Cancer Study Department of Clinical Sciences Malmö University Hospital Lund University The Malmö Diet and Cancer Study CV-cohort Cardiovascular Endpoints End of follow-up: 31 Dec * Report:
Inclusion of Biological Information in Treatment Planning Optimization Dag Rune Olsen
 Inclusion of Biological Information in Treatment Planning Optimization Dag Rune Olsen Institute for Cancer Research, Norwegian Radium Hospital, University of Oslo Theragnostics biological conformality
Inclusion of Biological Information in Treatment Planning Optimization Dag Rune Olsen Institute for Cancer Research, Norwegian Radium Hospital, University of Oslo Theragnostics biological conformality
2016 International Stroke Conference Hot Topics Lori M. Massaro, MSN, CRNP Kari Moore, MSN, AGACNP-BC
 2016 International Stroke Conference Hot Topics Lori M. Massaro, MSN, CRNP Kari Moore, MSN, AGACNP-BC Disclosures Lori M. Massaro, MSN,CRNP speakers bureau Genentech Kari Moore, MSN, AGACNP-BC -none 1
2016 International Stroke Conference Hot Topics Lori M. Massaro, MSN, CRNP Kari Moore, MSN, AGACNP-BC Disclosures Lori M. Massaro, MSN,CRNP speakers bureau Genentech Kari Moore, MSN, AGACNP-BC -none 1
Physiological Basis of the BOLD Signal. Kerstin Preuschoff Social and Neural systems Lab University of Zurich
 Physiological Basis of the BOLD Signal Kerstin Preuschoff Social and Neural systems Lab University of Zurich Source: Arthurs & Boniface, 2002 From Stimulus to Bold Overview Physics of BOLD signal - Magnetic
Physiological Basis of the BOLD Signal Kerstin Preuschoff Social and Neural systems Lab University of Zurich Source: Arthurs & Boniface, 2002 From Stimulus to Bold Overview Physics of BOLD signal - Magnetic
Discovery of an Aneurysm Following a Motorcycle Accident. Maya Babu, MSIII Gillian Lieberman, M.D.
 Discovery of an Aneurysm Following a Motorcycle Accident Maya Babu, MSIII Gillian Lieberman, M.D. Patient CC: July 2004 65 yo male transferred to the BI from an OSH s/p motorcycle crash w/o a helmet CC
Discovery of an Aneurysm Following a Motorcycle Accident Maya Babu, MSIII Gillian Lieberman, M.D. Patient CC: July 2004 65 yo male transferred to the BI from an OSH s/p motorcycle crash w/o a helmet CC
STROKE OCCURRENCE SYMPTOMS OF STROKE
 STROKE OCCURRENCE SYMPTOMS OF STROKE The symptoms of stroke depend on what part of the brain is affected and how large an area is involved. A stroke is a sudden event accompanied by one or more of the
STROKE OCCURRENCE SYMPTOMS OF STROKE The symptoms of stroke depend on what part of the brain is affected and how large an area is involved. A stroke is a sudden event accompanied by one or more of the
Copyright March 1, 2016 by AAPM. All rights reserved.
 DISCLAIMER: TO THE EXTENT ALLOWED BY LOCAL LAW, THIS INFORMATION IS PROVIDED TO YOU BY THE AMERICAN ASSOCIATION OF PHYSICISTS IN MEDICINE, A NON-PROFIT ORGANIZATION ORGANIZED TO PROMOTE THE APPLICATION
DISCLAIMER: TO THE EXTENT ALLOWED BY LOCAL LAW, THIS INFORMATION IS PROVIDED TO YOU BY THE AMERICAN ASSOCIATION OF PHYSICISTS IN MEDICINE, A NON-PROFIT ORGANIZATION ORGANIZED TO PROMOTE THE APPLICATION
EMS Management of Stroke. Deaver Shattuck, M.D. Brian Wiseman, M.D. Keith Woodward, M.D.
 EMS Management of Stroke Deaver Shattuck, M.D. Brian Wiseman, M.D. Keith Woodward, M.D. Financial Disclosure: No relevant financial relationship exists Working Together to End Stroke Formed in 2013 Identified
EMS Management of Stroke Deaver Shattuck, M.D. Brian Wiseman, M.D. Keith Woodward, M.D. Financial Disclosure: No relevant financial relationship exists Working Together to End Stroke Formed in 2013 Identified
Making Sense of the New Statin guidelines. They are more than just lowering your cholesterol!
 Making Sense of the New Statin guidelines They are more than just lowering your cholesterol! No Disclosures Margaret (Peg) O Donnell DNPs, FNP, ANP B-C, FAANP Senior Nurse Practitioner South Nassau Communities
Making Sense of the New Statin guidelines They are more than just lowering your cholesterol! No Disclosures Margaret (Peg) O Donnell DNPs, FNP, ANP B-C, FAANP Senior Nurse Practitioner South Nassau Communities
Level III Stroke Center Data Collection Requirements
 Who? Level III Stroke Center Data Collection Requirements All LERN Level III Stroke Centers. LERN Level I and II Stroke Centers have reporting requirements to The Joint Commission or other Board approved
Who? Level III Stroke Center Data Collection Requirements All LERN Level III Stroke Centers. LERN Level I and II Stroke Centers have reporting requirements to The Joint Commission or other Board approved
Brain Cooling in Traumatic Brain Injury and Stroke
 Brain Cooling in Traumatic Brain Injury and Stroke Bridget Harris, PhD, RGN Clinical Research Specialist, NHS Lothian Research Fellow, University of Edinburgh Content Therapeutic temperature reduction
Brain Cooling in Traumatic Brain Injury and Stroke Bridget Harris, PhD, RGN Clinical Research Specialist, NHS Lothian Research Fellow, University of Edinburgh Content Therapeutic temperature reduction
Chapter 4 Physiological Therapeutics. 1 Cryotherapy
 Chapter 4 Physiological Therapeutics 1 Cryotherapy CRYOTHERAPY PHYSIOLOGIC EFFECTS OF ICE APPLICATION 1. Decreased circulation 5. Increased tissue stiffness 2. Local vasoconstriction 6. Decreased muscle
Chapter 4 Physiological Therapeutics 1 Cryotherapy CRYOTHERAPY PHYSIOLOGIC EFFECTS OF ICE APPLICATION 1. Decreased circulation 5. Increased tissue stiffness 2. Local vasoconstriction 6. Decreased muscle
Therapeutic Management Options for. Acute Ischemic Stroke Anna Rosenbaum, MD
 Therapeutic Management Options for Acute Ischemic Stroke Anna Rosenbaum, MD Epidemiology Epidemiology 4 th leading cause of death in the United States 1 Leading cause of disability Increase in projected
Therapeutic Management Options for Acute Ischemic Stroke Anna Rosenbaum, MD Epidemiology Epidemiology 4 th leading cause of death in the United States 1 Leading cause of disability Increase in projected
E x p l a i n i n g Stroke
 Explaining Stroke Introduction Explaining Stroke is a practical step-by-step booklet that explains how a stroke happens, different types of stroke and how to prevent a stroke. Many people think a stroke
Explaining Stroke Introduction Explaining Stroke is a practical step-by-step booklet that explains how a stroke happens, different types of stroke and how to prevent a stroke. Many people think a stroke
Substandard Underwriting Structured Settlements
 Substandard Underwriting Structured Settlements Structures 101-Back to Basics February 20-22, 2013 Las Vegas, Nevada Rosemary Brindamour BSN CSSC Chief Medical Underwriter Structured Settlement Underwriting
Substandard Underwriting Structured Settlements Structures 101-Back to Basics February 20-22, 2013 Las Vegas, Nevada Rosemary Brindamour BSN CSSC Chief Medical Underwriter Structured Settlement Underwriting
Traumatic Brain Injury (1.2.3) Management of severe TBI (1.2.3.1) Learning Objectives
 Management of severe TBI (1.2.3.1) Learning Objectives") Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
PHYSICIAN SIGNATURE DATE TIME DRUG ALLERGIES WT: KG
 MED Hospitalist Stroke-TIA Vital Signs Vital Signs Q4H (DEF)* Q2H Q1H Vital Signs Orthostatic Activity Activity Bedrest, for 12 hours then Up ad lib (DEF)* Bedrest, for 24 hours then Up ad lib Up Ad Lib
MED Hospitalist Stroke-TIA Vital Signs Vital Signs Q4H (DEF)* Q2H Q1H Vital Signs Orthostatic Activity Activity Bedrest, for 12 hours then Up ad lib (DEF)* Bedrest, for 24 hours then Up ad lib Up Ad Lib
What Is an Arteriovenous Malformation (AVM)?
?") What Is an Arteriovenous Malformation (AVM)? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall T. Higashida, M.D., Chair 1 What
What Is an Arteriovenous Malformation (AVM)? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall T. Higashida, M.D., Chair 1 What
Guidelines for diagnosis and management of acute pulmonary embolism
 Guidelines for diagnosis and management of acute pulmonary embolism By Dr. Ahmed Zaghloul M.D. Anesthesia & Critical Care 2014 Predisposing factors for VTE Predisposing factor Strong predisposing factors
Guidelines for diagnosis and management of acute pulmonary embolism By Dr. Ahmed Zaghloul M.D. Anesthesia & Critical Care 2014 Predisposing factors for VTE Predisposing factor Strong predisposing factors
The practice of lowering blood pressure (BP)
") Original Paper Treatment of Hypertension in the Inpatient Setting: Use of Intravenous Labetalol and Hydralazine Alan B. Weder, MD; 1 Steven Erickson, PharmD 2 Acute blood pressure elevations are commonly
Original Paper Treatment of Hypertension in the Inpatient Setting: Use of Intravenous Labetalol and Hydralazine Alan B. Weder, MD; 1 Steven Erickson, PharmD 2 Acute blood pressure elevations are commonly
Acknowledgements. PAH in Children: Natural History. The Sildenafil Saga
 The Sildenafil Saga David L. Wessel, MD Executive Vice President Chief Medical Officer Ikaria Distinguished Professor of Critical Care Children s National Medical Center Washington, DC, USA Acknowledgements
The Sildenafil Saga David L. Wessel, MD Executive Vice President Chief Medical Officer Ikaria Distinguished Professor of Critical Care Children s National Medical Center Washington, DC, USA Acknowledgements
Effective Services for People Living with Brain Injury
 Effective Services for People Living with Brain Injury Jean Capler, MSW, LCSW Local Support Network Leader The Rehabilitation Hospital of Indiana Resource Facilitation Plan for Today Brain Injury 101 Challenges
Effective Services for People Living with Brain Injury Jean Capler, MSW, LCSW Local Support Network Leader The Rehabilitation Hospital of Indiana Resource Facilitation Plan for Today Brain Injury 101 Challenges
Stroke Coding Issues Presentation to: NorthEast Cerebrovascular Consortium
 Stroke Coding Issues Presentation to: NorthEast Cerebrovascular Consortium October 30, 2008 Barry Libman, RHIA, CCS, CCS-P President, Barry Libman Inc. Stroke Coding Issues Outline Medical record documentation
Stroke Coding Issues Presentation to: NorthEast Cerebrovascular Consortium October 30, 2008 Barry Libman, RHIA, CCS, CCS-P President, Barry Libman Inc. Stroke Coding Issues Outline Medical record documentation
VASOPRESSOR AGENTS IN SEPTIC SHOCK
 VASOPRESSOR AGENTS IN SEPTIC SHOCK Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles President European Society of Intensive
VASOPRESSOR AGENTS IN SEPTIC SHOCK Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles President European Society of Intensive
JNC-8 Blood Pressure and ACC/AHA Cholesterol Guideline Updates. January 30, 2014
 JNC-8 Blood Pressure and ACC/AHA Cholesterol Guideline Updates January 30, 2014 GOALS Review key recommendations from recently published guidelines on blood pressure and cholesterol management Discuss
JNC-8 Blood Pressure and ACC/AHA Cholesterol Guideline Updates January 30, 2014 GOALS Review key recommendations from recently published guidelines on blood pressure and cholesterol management Discuss
Cardiovascular Endpoints
 The Malmö Diet and Cancer Study Department of Clinical Sciences Skåne University Hospital, Malmö Lund University The Malmö Diet and Cancer Study CV-cohort Cardiovascular Endpoints End of follow-up: 30
The Malmö Diet and Cancer Study Department of Clinical Sciences Skåne University Hospital, Malmö Lund University The Malmö Diet and Cancer Study CV-cohort Cardiovascular Endpoints End of follow-up: 30
Traumatic Head Injuries
 Traumatic Brain Injury (TBI) Traumatic Head Injuries Major contributing cause of trauma deaths Many survivors have permanent disability Commonly occurs in young adults (mostly males) Spokane County EMS
Traumatic Brain Injury (TBI) Traumatic Head Injuries Major contributing cause of trauma deaths Many survivors have permanent disability Commonly occurs in young adults (mostly males) Spokane County EMS
Guidelines and Protocols
 TITLE: HEAD TRAUMA PURPOSE: To provide guidelines for rapid, accurate assessment of the head and intracranial structures for traumatic injury and to plan and implement appropriate interventions for identified
TITLE: HEAD TRAUMA PURPOSE: To provide guidelines for rapid, accurate assessment of the head and intracranial structures for traumatic injury and to plan and implement appropriate interventions for identified
TRAUMATIC BRAIN INJURY (TBI)
") Background: Traumatic Brain Injury (TBI) is one of the leading causes of trauma related disability and death in the U.S. TBIs can occur as either blunt, penetrating, or a combination of both depending
Background: Traumatic Brain Injury (TBI) is one of the leading causes of trauma related disability and death in the U.S. TBIs can occur as either blunt, penetrating, or a combination of both depending
STROKE PREVENTION AND TREATMENT MARK FISHER, MD PROFESSOR OF NEUROLOGY UC IRVINE
 STROKE PREVENTION AND TREATMENT MARK FISHER, MD PROFESSOR OF NEUROLOGY UC IRVINE CASE REPORT: ACUTE STROKE MANAGEMENT 90 YEAR OLD WOMAN, PREVIOUSLY ACTIVE AND INDEPENDENT, CHRONIC ATRIAL FIBRILLATION,
STROKE PREVENTION AND TREATMENT MARK FISHER, MD PROFESSOR OF NEUROLOGY UC IRVINE CASE REPORT: ACUTE STROKE MANAGEMENT 90 YEAR OLD WOMAN, PREVIOUSLY ACTIVE AND INDEPENDENT, CHRONIC ATRIAL FIBRILLATION,
Evaluating ED Patients with Transient Ischemic Attack: Inpatient vs. Outpatient Strategies
 Evaluating ED Patients with Transient Ischemic Attack: Inpatient vs. Outpatient Strategies Michael A. Ross MD FACEP Associate Professor of Emergency Medicine Wayne State University School of Medicine Detroit
Evaluating ED Patients with Transient Ischemic Attack: Inpatient vs. Outpatient Strategies Michael A. Ross MD FACEP Associate Professor of Emergency Medicine Wayne State University School of Medicine Detroit
MANAGEMENT OF LIPID DISORDERS: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF LIPID DISORDERS: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING
MANAGEMENT OF LIPID DISORDERS: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING
Lifecheque Basic Critical Illness Insurance
 Lifecheque Basic Critical Illness Insurance Strong. Reliable. Trustworthy. Forward-thinking. Extra help on the road to recovery Surviving a critical illness can be very challenging financially Few of us
Lifecheque Basic Critical Illness Insurance Strong. Reliable. Trustworthy. Forward-thinking. Extra help on the road to recovery Surviving a critical illness can be very challenging financially Few of us
Inpatient Heart Failure Management: Risks & Benefits
 Inpatient Heart Failure Management: Risks & Benefits Dr. Kenneth L. Baughman Professor of Medicine Harvard Medical School Director, Advanced Heart Disease Section Brigham & Women's Hospital Harvard Medical
Inpatient Heart Failure Management: Risks & Benefits Dr. Kenneth L. Baughman Professor of Medicine Harvard Medical School Director, Advanced Heart Disease Section Brigham & Women's Hospital Harvard Medical
ESCMID Online Lecture Library. by author
 Do statins improve outcomes of patients with sepsis and pneumonia? Jordi Carratalà Department of Infectious Diseases Statins for sepsis & community-acquired pneumonia Sepsis and CAP are major healthcare
Do statins improve outcomes of patients with sepsis and pneumonia? Jordi Carratalà Department of Infectious Diseases Statins for sepsis & community-acquired pneumonia Sepsis and CAP are major healthcare
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy
 The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
doi: 10.1016/j.jocn.2010.10.005
 doi: 10.1016/j.jocn.2010.10.005 A remote desktop-based telemedicine system Yasushi Shibata, MD, PhD Department of Neurosurgery, Mito Medical Center, University of Tsukuba Mito, Ibaraki, 310-0015, Japan
doi: 10.1016/j.jocn.2010.10.005 A remote desktop-based telemedicine system Yasushi Shibata, MD, PhD Department of Neurosurgery, Mito Medical Center, University of Tsukuba Mito, Ibaraki, 310-0015, Japan
 STROKE April 2011 Dr Amer Jafar A delay in recognizing early warning signs (WS) and risk factors (RF) of ischemic stroke causes a delay in treatment Evaluated: knowledge of RF and WS and the impact of
STROKE April 2011 Dr Amer Jafar A delay in recognizing early warning signs (WS) and risk factors (RF) of ischemic stroke causes a delay in treatment Evaluated: knowledge of RF and WS and the impact of