Retrospective Denials Management
|
|
|
- Verity Scott
- 10 years ago
- Views:
Transcription


1 Retrospective Denials Management Weaving together the Clinical, Technical, and Legal Components Glen Reiner, RN, BSN, VP of Clinical Operations Nicole Guido, VP Business Development

2 Our goals for our time today An overview of effective Denials Management approach Key Performance Indicators MAP Keys Description of team composition Review of possible Denials Management processes and workflows The importance of accurate data collection and analysis Specific Denials Management challenges 2

3 Revenue Cycle Imperatives How ACCA is Affecting the Revenue Cycle The complexities of today s coverage and reimbursement landscape demands a level of focus and expertise unparalleled in the past * Expanded Coverage Payment Cuts Improve Performance and Efficiency Patient Access - Eligibility Processes Denials Management/ Denials Prevention * Illustration adapted from hfmap Revenue Cycle Excellence presentation on Reform impacts 3

4 Define a Denial What is a denial? ANY CLAIM PAID LESS THAN EXPECTED How do you calculate the dollar impact of a denial? THE DELTA 4

5 Some of the keys to success include: Systems that collect data and processes that translate that data into information Front end processes to ensure eligibility, notification and authorization Ongoing and timely clinical review and communication with payors Contract management & IT systems that accurately calculate expected payments using complex reimbursement formulas Integrated denials management for both technical and clinical 5

6 Overview of Denials Management Process Role of the Denials Management Team Take responsibility for an assigned portion of a hospital s accounts receivable, beginning with the identification of a clinical, technical or legal denial The process should include: Initial Review Clinical Review Clinical & Technical Appeals Preparation & Referral to Legal Joint Operating Committees with Payors Follow up 6

7 Seamless integration of business office and clinical audit operations is imperative A process must be in place between AR staff and clinical staff The Hand-off Delivery of clinical denials to clinical staff (paper vs. electronic) Nurse Audit request (explanation of problem) RAs/EOBs/UBs Medical records Clinical audit inventory must be managed Distribution to clinical staff - Prioritization methodologies Productivity measurements Clinical outcome reports 7

8 Denials Management Team Composition Diverse team of experts comprised of: Project Management Nurses & Medical Directors Accounts Receivable/Billing Specialists Inpatient/Outpatient Coders Clerical Support Specialists Legal Support Considerations when building the team Existing resources, reporting relationships Corporate Partners 8



9 Denials Management Work Flow Model A/R Rep. Review Accept Adjust Close Technical Action Accept Denials Occurs Referral A/R Rep. Review Reconsideration, Appeal, Grievance * Follow Up Payment Close Clinical Legal Action Nurse Audit Accept Adjust Close * Referral to Legal as needed at any point 9

10 Denials Management Work Flow Status 10

11 Denials Management Data The data that is generated from the Denials Management process is almost as valuable as the additional revenue This information can be used by the facility to focus concurrent CM and UR efforts as well as improve clinical and PFS functions 11

12 HFMA s MAP Keys Sets a national standard for revenue cycle excellence Define the critical indicators of revenue cycle performance in clear, unbiased terms Ensure consistent reporting Each Key has a Purpose, Value and Calculation 12

13 Initial Denial Rate Zero Pay Purpose: Trending indicator of percentage claims not paid Value: Indicates providers ability to comply with payer requirements and payer s ability to accurately pay the claim Number of zero paid claims denied Number of total claims remitted 13

14 Initial Denial Rate Partial Pay Purpose: Trending indicator of percentage claims partially paid Value: Indicates providers ability to comply with payer requirements and payer s ability to accurately pay the claim Number of partially paid claims denied Number of total claims remitted 14

15 Denials Overturned by Appeal Purpose: Trending indicator of hospital s success in managing the appeal process Value: Indicates opportunities for payer and provider process improvement and improves cash flow Number of appealed claims paid Total number of claims appealed and finalized or closed 15

16 Denial Write-Offs as a Percent of Net Revenue Purpose: Trending indicator of final disposition of lost reimbursement, where all efforts of appeal have been exhausted or provider chooses to write off expected payment amount Value: Indicates provider s ability to comply with payer requirement and payers ability to accurately pay the claim Net dollars written off as denials Net patient services revenue 16

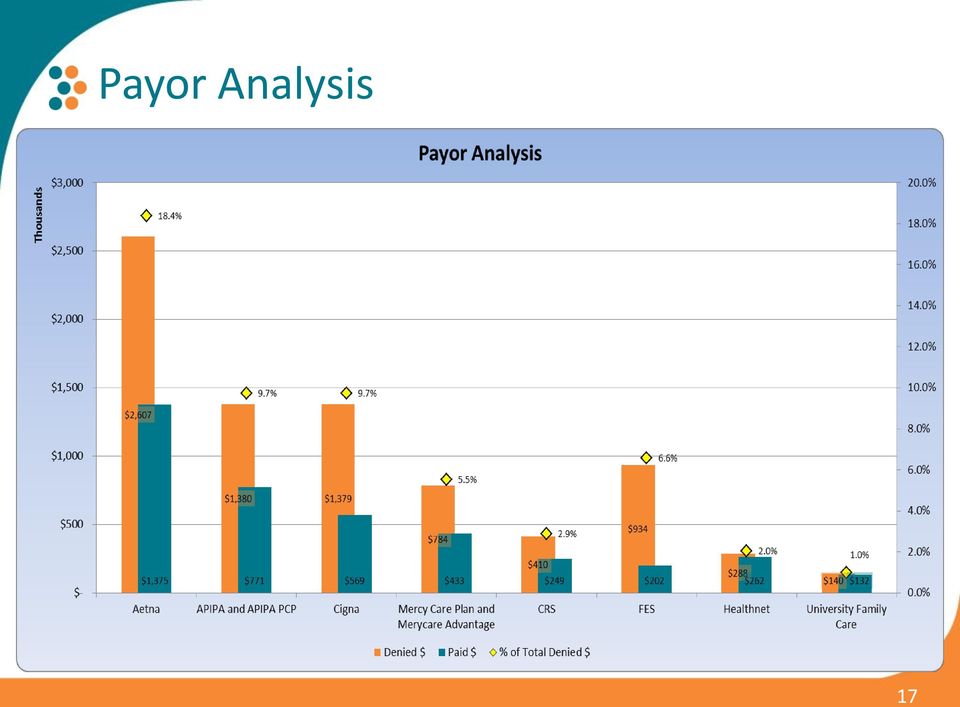
17 Payor Analysis 17
18 Denial Area Summary 18

19 Ideally, data from denials should directly feed continuous improvement efforts Conducting a root cause analysis for denials can identify opportunities for improvement and education ultimately preventing future denials for the same reason 19

20 Illustration of Cause and Effect Analysis Outcomes 20

21 Analysis of Denials Management root causes often reveal issues in multiple areas Technical Prior Auth Billing error Wrong Insurance Contract Coverage Eligibility Technical Prior Auth Denials Hospital Issues Legal Clinical/ Medical Payment less than expected Non-covered services Concurrent denials Grievance/appeal Process Denials Health Plan Issues Clinical/ Medical Onsite review Medical Director LOS/Delay days Not medically necessary Non covered service 21
22 Sample Denials Management Analysis System wide, the areas not under the Hospital System s immediate influence (Physician, Health Plan, and Patient) represented nearly 73% of the resolved denied claims: $6.5M of the total $8.6M Front End and Back End combined represented just under 10% of the total number of resolved denied claims, and just under 9% of the dollars The team had the most success appealing claims from the Health Plan Denial Area at 67% of total recovered dollars. The Physician Denial Area was a significant challenge with only 7% of total recovered dollars on all resolved claims The Physician Denial Area had the largest number of resolved denied claims at each hospital 22
23 Sample Denials Management Analysis At one hospital system an in-depth review demonstrated that the hospital had specific clinical issues Physician delay in discharge Patients no longer meeting inpatient criteria and documentation insufficient to support continued stay In cases where the patient is waiting for skilled nursing facility placement, roughly 40% of denied dollars were recovered on appeal/reconsideration Overutilization of ICU Short pays by health plans where the ICU level is not supported by documentation On appeal 32% of denied dollars in this category related to Physician use of ICU were recovered 23
24 Sample Denials Management Data Client Product Status Denial Reason Number Of Accounts DENIED Dollar Amount Denied # of accounts disputed APPEALED Percentage Of Accounts Appealed Dollar Amount Appealed Percentage Of Dollars Appealed ABC ZB AHCCCS/Health Plan Issue 7 $ 1, % $ % ABC ZB Delay days or Delay in care 0 $ - 0 0% $ - 0% ABC ZB Denied days meet SNF(sub-acute) level of care 0 $ - 0 0% $ - 0% ABC ZB Disallowed charges 2 $ 36, % $ 36, % ABC ZB Documentation does not support expected tier 12 $ 7, % $ 7, % ABC ZB ESP or Dialysis days only 1 $ % $ - 0% ABC ZB FES/Emergent criteria or Stabilization 49 $ 17, % $ 13, % ABC ZB Mental health plan responsible for denied days 1 $ % $ % ABC ZB OBS. V. Inpatient 1 $ 1, % $ - 0% ABC ZB Other 2 $ 3, % $ 3, % ABC ZB Technical Issue 22 $ 7, % $ 7, % TOTAL ZERO BALANCE 97 $ 76, % $ 69, % 24
25 $5,000,000 $4,000,000 $3,000,000 $2,000,000 $1,000,000 Tracking of short pays over time will identify unwanted trends, not always reasons $0 Short Pay Dollars Short Pay Claims 25
26 Sample Denials Management Results $26,170,509 in denied charges with a recovery rate of 54.05% Financial Class Denied Charges Recovery Rate Medicaid $13,172, % Commercial $5,094, % Medicare-Risk $2,069, % BCBS $4,116, % Medicare $1,711, % 26


27 Closing The Loop By using the data to focus concurrent processes and drive educational efforts the Denials Management Team and the hospital were able to produce the following results: After a concentrated education and document improvement effort the overall recoveries from the Physician Denial area showed a dramatic increase (40%) Revise Process/Educate Review Results The fact that the recovery rate increased while the denial rate remained stagnant is an indication that the documentation improved, but the plan s behavior is lagging behind Recommend Root Cause 27
28 Specific Denials Management Challenges Emergency Department denials Observation versus Inpatient Inpatient cases where documentation does not support inpatient level of care Many times are being paid $0.00 Very difficult to appeal retrospectively with a valid inpatient order Best place to catch these denials is at the time of admit Denials Management data can be used to focus these efforts 28
29 Specific Denials Management Challenges Elective Surgery denials Scheduled and authorized as outpatient, but made inpatient after the procedure The chart contains an outpatient authorization, an inpatient order and the documentation supports outpatient level of care These claims are either being short paid or paid at $0.00 Very difficult to argue on appeal with out excellent documentation of complications Addressing these denials concurrently will require excellent communication with the Clinicians, Scheduling and Case Management Documentation improvement program is also a possibility 29
30 Specific Denials Management Challenges Discharge to a lower level of care Awaiting bed availability or placement Possibility of partnering with appropriate alternative care facilities Risk-sharing Readmission Denials The same or similar diagnosis Can be technical and/or clinical issue 30
31 Clinical Denials Management is an Essential Component of the Revenue Cycle Prevents money from being left on the table Provides great insight into process improvement opportunities Requires specific, detailed processes and resource allocation Systems for data analysis and comparison are crucial Strong clinical integration is imperative 31
32 Thank you for your time! Questions? 32
33 Adreima Contact Information Glen R. Reiner Vice President of Clinical Operations Phone: (602) Cell: (602) [email protected] Nicole Guido Vice President of Business Development Cell: (619) [email protected] 33
Leveraging Predictive Analytic and Artificial Intelligence Technology for Financial and Clinical Performance
 Leveraging Predictive Analytic and Artificial Intelligence Technology for Financial and Clinical Performance Matt Seefeld CEO & Co-Founder [email protected] www.interpointpartners.com (404)446-0051
Leveraging Predictive Analytic and Artificial Intelligence Technology for Financial and Clinical Performance Matt Seefeld CEO & Co-Founder [email protected] www.interpointpartners.com (404)446-0051
Rejection Prevention. How Actionable Data Can Drive Results in Your Revenue Cycle
 Rejection Prevention How Actionable Data Can Drive Results in Your Revenue Cycle Objectives Build a data collection strategy in denials and rejections that drives action and ultimately improved results
Rejection Prevention How Actionable Data Can Drive Results in Your Revenue Cycle Objectives Build a data collection strategy in denials and rejections that drives action and ultimately improved results
HFMA MAP Keys Patient Access Measure:
 HFMA MAP Keys Patient Access Pre-Registration Rate Trending indicator that patient access processes are timely, accurate, and efficient Indicates revenue cycle efficiency and effectiveness N: number of
HFMA MAP Keys Patient Access Pre-Registration Rate Trending indicator that patient access processes are timely, accurate, and efficient Indicates revenue cycle efficiency and effectiveness N: number of
CHANGING YOUR CASE MANAGEMENT MODEL OF CARE. Jan Lear, RN, CMC Director of Case Management MedStar Franklin Square Medical Center
 CHANGING YOUR CASE MANAGEMENT MODEL OF CARE Jan Lear, RN, CMC Director of Case Management MedStar Franklin Square Medical Center 1 Program Objectives To be able to describe the compliance and regulatory
CHANGING YOUR CASE MANAGEMENT MODEL OF CARE Jan Lear, RN, CMC Director of Case Management MedStar Franklin Square Medical Center 1 Program Objectives To be able to describe the compliance and regulatory
Functions: The UM Program consists of the following components:
 1.0 Introduction Alameda County Behavioral Health Care Services (ACBHCS) includes a Utilization Management (UM) Program and Behavioral Health Managed Care Plan (MCP). They are dedicated to delivering cost
1.0 Introduction Alameda County Behavioral Health Care Services (ACBHCS) includes a Utilization Management (UM) Program and Behavioral Health Managed Care Plan (MCP). They are dedicated to delivering cost
MEDICAL MANAGEMENT OVERVIEW MEDICAL NECESSITY CRITERIA RESPONSIBILITY FOR UTILIZATION REVIEWS MEDICAL DIRECTOR AVAILABILITY
 4 MEDICAL MANAGEMENT OVERVIEW Our medical management philosophy and approach focus on providing both high quality and cost-effective healthcare services to our members. Our Medical Management Department
4 MEDICAL MANAGEMENT OVERVIEW Our medical management philosophy and approach focus on providing both high quality and cost-effective healthcare services to our members. Our Medical Management Department
Concurrent Utilization Review: Getting It Right By Olakunle Olaniyan, MD, MBA, Iskla L. Brown RN, and Kayode Williams, MD, MBA, FFARCSI
 Utilization Concurrent Utilization Review: Getting It Right By Olakunle Olaniyan, MD, MBA, Iskla L. Brown RN, and Kayode Williams, MD, MBA, FFARCSI In this article Take advantage of ways to improve your
Utilization Concurrent Utilization Review: Getting It Right By Olakunle Olaniyan, MD, MBA, Iskla L. Brown RN, and Kayode Williams, MD, MBA, FFARCSI In this article Take advantage of ways to improve your
POLICY #1571.00 SUBJECT: INPATIENT CERTIFICATION AND AUTHORIZATION
 Effective Date: 9/13/2007; 7/13/2005 Revised Date: 11/7/07 Review Date: North Sound Mental Health Administration Section 1500 Clinical: Inpatient Certification and Authorization Authorizing Source: WAC
Effective Date: 9/13/2007; 7/13/2005 Revised Date: 11/7/07 Review Date: North Sound Mental Health Administration Section 1500 Clinical: Inpatient Certification and Authorization Authorizing Source: WAC
Care Management Can We Do It Better?
 Care Management Can We Do It Better? Wilma Acosta, Associate Director Protiviti, Inc. Alex Robison, Managing Director Protiviti, Inc. Agenda I. Care Management Challenges II. Compliance Case Studies Intermittently
Care Management Can We Do It Better? Wilma Acosta, Associate Director Protiviti, Inc. Alex Robison, Managing Director Protiviti, Inc. Agenda I. Care Management Challenges II. Compliance Case Studies Intermittently
CHAPTER 5 SERVICE DESCRIPTIONS. Inpatient Hospital Psychiatric Services. Service Coverage
 CHAPTER 5 SERVICE DESCRIPTIONS Inpatient Hospital Psychiatric Services Service Coverage Inpatient psychiatric care involves skilled psychiatric services in a hospital setting. The care delivered includes
CHAPTER 5 SERVICE DESCRIPTIONS Inpatient Hospital Psychiatric Services Service Coverage Inpatient psychiatric care involves skilled psychiatric services in a hospital setting. The care delivered includes
Exploring the Impact of the RAC Program on Hospitals Nationwide. Results of AHA RACTRAC Survey, 4 th Quarter 2012
 Exploring the Impact of the RAC Program on Hospitals Nationwide Results of AHA RACTRAC Survey, 4 th Quarter 2012 March 8, 2013 RAC 101 Centers for Medicare & Medicaid Services (CMS) Recovery Audit Contractors
Exploring the Impact of the RAC Program on Hospitals Nationwide Results of AHA RACTRAC Survey, 4 th Quarter 2012 March 8, 2013 RAC 101 Centers for Medicare & Medicaid Services (CMS) Recovery Audit Contractors
The Changing Face of Medical Necessity under ICD-10
 The Changing Face of Medical Necessity under ICD-0 Sponsored by 95 N. Fine Ave #04 Fresno CA 93720-565 Phone: (559) 25-5038 Fax: (559) 25-5836 www.californiahia.org Program Handouts Monday, June 8, 205
The Changing Face of Medical Necessity under ICD-0 Sponsored by 95 N. Fine Ave #04 Fresno CA 93720-565 Phone: (559) 25-5038 Fax: (559) 25-5836 www.californiahia.org Program Handouts Monday, June 8, 205
IPPS Observation vs. Inpatient Admissions Training Questions and Answers
 IPPS Observation vs. Inpatient Admissions Training Questions and Answers The following questions and answers are from the Part A IPPS Observation vs. Inpatient Admissions web-based trainings conducted
IPPS Observation vs. Inpatient Admissions Training Questions and Answers The following questions and answers are from the Part A IPPS Observation vs. Inpatient Admissions web-based trainings conducted
Utilization Review and Denial Management
 September 2014 Clinical Resource Management Series Part 3 of 10 Utilization Review and Denial Management Part 3 in our Clinical Resource Management (CRM) series is focused on utilization review and denial
September 2014 Clinical Resource Management Series Part 3 of 10 Utilization Review and Denial Management Part 3 in our Clinical Resource Management (CRM) series is focused on utilization review and denial
Overview of Hospital Utilization Review
 Overview of Hospital Utilization Review Legal Authority The Inspector General (IG) hospital utilization review function operates under guidelines and regulations contained in: Texas Administrative Code
Overview of Hospital Utilization Review Legal Authority The Inspector General (IG) hospital utilization review function operates under guidelines and regulations contained in: Texas Administrative Code
Transformational Data-Driven Solutions for Healthcare
 Transformational Data-Driven Solutions for Healthcare Transformational Data-Driven Solutions for Healthcare Today s healthcare providers face increasing pressure to improve operational performance while
Transformational Data-Driven Solutions for Healthcare Transformational Data-Driven Solutions for Healthcare Today s healthcare providers face increasing pressure to improve operational performance while
Medical Necessity & Charting Guidelines
 Medical Necessity & Charting Guidelines 1 In most cases we are told the rules up front - or will be told if we ask Like most games, the one who knows the rules the best WINS 4 2 Nationally Recognized Industry
Medical Necessity & Charting Guidelines 1 In most cases we are told the rules up front - or will be told if we ask Like most games, the one who knows the rules the best WINS 4 2 Nationally Recognized Industry
CHAPTER 17 CREDIT AND COLLECTION
 CHAPTER 17 CREDIT AND COLLECTION 17101. Credit and Collection Section 17102. Purpose 17103. Policy 17104. Procedures NOTE: Rule making authority cited for the formulation of regulations for the Credit
CHAPTER 17 CREDIT AND COLLECTION 17101. Credit and Collection Section 17102. Purpose 17103. Policy 17104. Procedures NOTE: Rule making authority cited for the formulation of regulations for the Credit
CARE MANAGEMENT SERIES Part 6 Developing a Staffing Model That Works
 CARE MANAGEMENT SERIES Part 6 Developing a Staffing Model That Works We will get to staffing but let s start by reviewing core functions. Care Management As we have discussed previously, Care Management
CARE MANAGEMENT SERIES Part 6 Developing a Staffing Model That Works We will get to staffing but let s start by reviewing core functions. Care Management As we have discussed previously, Care Management
Capacity Management: Patient Throughput and Case Management Improvement. February 25, 2015
 Capacity Management: Patient Throughput and Case Management Improvement February 25, 2015 Agenda Introduction Impetus for Change Approach to Improving Case and Capacity Management Client Case Study Key
Capacity Management: Patient Throughput and Case Management Improvement February 25, 2015 Agenda Introduction Impetus for Change Approach to Improving Case and Capacity Management Client Case Study Key
Keeping the Reimbursement Train on Track
 EXECUTIVE BRIEFING Keeping the Reimbursement Train on Track By Kelley Blair MA, vice president at Craneware Professional Services and Linda Corley, MBA, CPC, corporate compliance officer, Dell Services
EXECUTIVE BRIEFING Keeping the Reimbursement Train on Track By Kelley Blair MA, vice president at Craneware Professional Services and Linda Corley, MBA, CPC, corporate compliance officer, Dell Services
The University of Texas Southwestern Medical Center Denials Management Audit University Hospitals. Internal Audit Report 14:10B
 Office of Internal Audit The University of Texas Southwestern Medical Center Denials Management Audit University Hospitals Internal Audit Report 14:10B November 19, 2014 Table of Contents I. Executive
Office of Internal Audit The University of Texas Southwestern Medical Center Denials Management Audit University Hospitals Internal Audit Report 14:10B November 19, 2014 Table of Contents I. Executive
Residential Substance Abuse Treatment: Impact of Concurrent Utilization Review
 Report to The Vermont Legislature Residential Substance Abuse Treatment: Impact of Concurrent Utilization Review In Accordance with Act 179 (2014), Section E.300.2, An Act Relating to Making Appropriations
Report to The Vermont Legislature Residential Substance Abuse Treatment: Impact of Concurrent Utilization Review In Accordance with Act 179 (2014), Section E.300.2, An Act Relating to Making Appropriations
How to Prepare a Winning RAC Appeal
 How to Prepare a Winning RAC Appeal Craneware InSight Consulting Copyright 2011, CRANEWARE INSIGHT. All rights reserved. www.cranewareinsight.com p.1 Introduction Introductions Karen Bowden, RHIA, Senior
How to Prepare a Winning RAC Appeal Craneware InSight Consulting Copyright 2011, CRANEWARE INSIGHT. All rights reserved. www.cranewareinsight.com p.1 Introduction Introductions Karen Bowden, RHIA, Senior
Beyond the Basics: Accelerating the Revenue Cycle Through Advanced KPI s
 Optimizing the business of healthcare Beyond the Basics: Table of Contents Overview 1 The Importance of Metrics 1 Taking the Next Step 1 Baseline KPI s 2 Why Advanced KPI s 2 Advanced KPI s In Action 3
Optimizing the business of healthcare Beyond the Basics: Table of Contents Overview 1 The Importance of Metrics 1 Taking the Next Step 1 Baseline KPI s 2 Why Advanced KPI s 2 Advanced KPI s In Action 3
EHR Client Bulletin: Answers to Your Most Frequently Asked Condition Code 44 Questions
 EHR Client Bulletin: Answers to Your Most Frequently Asked Condition Code 44 Questions Originally Issued On: February 25, 2010 Last Update: February 20, 2013 UPDATE: The following EHR Client Bulletin was
EHR Client Bulletin: Answers to Your Most Frequently Asked Condition Code 44 Questions Originally Issued On: February 25, 2010 Last Update: February 20, 2013 UPDATE: The following EHR Client Bulletin was
EISENHOWER MEDICAL CENTER Financial Assistance Program Full Charity Care and Discount Partial Charity Care Policies
 EISENHOWER MEDICAL CENTER Financial Assistance Program Full Charity Care and Discount Partial Charity Care Policies PURPOSE Eisenhower Medical Center (EMC) serves all persons within Rancho Mirage and the
EISENHOWER MEDICAL CENTER Financial Assistance Program Full Charity Care and Discount Partial Charity Care Policies PURPOSE Eisenhower Medical Center (EMC) serves all persons within Rancho Mirage and the
Revenue Cycle Objectives Challenges Management Goals and Expected Benefits Sample Metrics Opportunities Summary Solution Steps
 Common Findings Revealed: Revenue Cycle Review John Bartell, RN, BSN, Partner Tina Nazier, MBA, Director Wipfli LLP Topics for Discussion Revenue Cycle Objectives Challenges Management Goals and Expected
Common Findings Revealed: Revenue Cycle Review John Bartell, RN, BSN, Partner Tina Nazier, MBA, Director Wipfli LLP Topics for Discussion Revenue Cycle Objectives Challenges Management Goals and Expected
Ten Overlooked Opportunities For Significant Performance Improvement and Cost Savings
 Ten Overlooked Opportunities For Significant Performance Improvement and Cost Savings Ten Overlooked Opportunities For Significant Performance Improvement and Cost Savings Huron Healthcare s Performance
Ten Overlooked Opportunities For Significant Performance Improvement and Cost Savings Ten Overlooked Opportunities For Significant Performance Improvement and Cost Savings Huron Healthcare s Performance
RAC Preparation 7 Key Steps and Best Practices
 McGuireWoods Health Care practice is ranked 6th largest in the country by the American Health Lawyers Association. RAC Preparation 7 Key Steps and Best Practices Elissa K. Moore, Associate 704.343.2218
McGuireWoods Health Care practice is ranked 6th largest in the country by the American Health Lawyers Association. RAC Preparation 7 Key Steps and Best Practices Elissa K. Moore, Associate 704.343.2218
Provider Manual. Utilization Management
 Provider Manual Utilization Management Utilization Management This section of the Manual was created to help guide you and your staff in working with Kaiser Permanente s Utilization Management (UM) policies
Provider Manual Utilization Management Utilization Management This section of the Manual was created to help guide you and your staff in working with Kaiser Permanente s Utilization Management (UM) policies
Engaging Touch Free Practices Carolinas HealthCare System - A Case Study on Automation in the Revenue Cycle
 Engaging Touch Free Practices Carolinas HealthCare System - A Case Study on Automation in the Revenue Cycle Elizabeth P. Staas, Recondo Technology Katie Davis, Carolinas HealthCare System Who we are Elizabeth
Engaging Touch Free Practices Carolinas HealthCare System - A Case Study on Automation in the Revenue Cycle Elizabeth P. Staas, Recondo Technology Katie Davis, Carolinas HealthCare System Who we are Elizabeth
RAC Audits. RAC audits. RAC Audits 1/31/2014. What you need to know By Angie Cameron and Maggie Lester Johnston Barton Proctor & Rose
 RAC Audits What you need to know By Angie Cameron and Maggie Lester Johnston Barton Proctor & Rose RAC audits In early January 2013, Medicaid rolled out its plan for Recovery Audit Contractor Reviews of
RAC Audits What you need to know By Angie Cameron and Maggie Lester Johnston Barton Proctor & Rose RAC audits In early January 2013, Medicaid rolled out its plan for Recovery Audit Contractor Reviews of
Revenue Cycle Management Practice
 Revenue Cycle Management Practice W h i t e p a p e r By William Malm, ND, RN Practice Director, Revenue Cycle Management, HCPro, Inc. Recovery audit contractors Recovery Audit Contractors Strategic planning
Revenue Cycle Management Practice W h i t e p a p e r By William Malm, ND, RN Practice Director, Revenue Cycle Management, HCPro, Inc. Recovery audit contractors Recovery Audit Contractors Strategic planning
Conifer Health Solutions Tenet Investor Webinar
 Conifer Health Solutions Tenet Investor Webinar May 16, 2012 Stephen Mooney President, Conifer Health Solutions 1 2012 Conifer Health Solutions, LLC. All Rights Reserved. Forward Looking Statements Certain
Conifer Health Solutions Tenet Investor Webinar May 16, 2012 Stephen Mooney President, Conifer Health Solutions 1 2012 Conifer Health Solutions, LLC. All Rights Reserved. Forward Looking Statements Certain
Revenue Cycle Management
 Revenue Cycle Management 2007 Edition Copyright 2007 Revenue Integrity Specialist Team University of Arkansas for Medical Sciences All rights reserved INTRODUCTION Welcome! The program is facilitated by
Revenue Cycle Management 2007 Edition Copyright 2007 Revenue Integrity Specialist Team University of Arkansas for Medical Sciences All rights reserved INTRODUCTION Welcome! The program is facilitated by
6 Critical Impact Factors of Health Reform on Revenue Cycle Management Pyramid Healthcare Solutions Thought Leadership Series
 6 Critical Impact Factors of Health Reform on Revenue Cycle Management Pyramid Healthcare Solutions Thought Leadership Series The healthcare industry is undergoing significant change in the face of the
6 Critical Impact Factors of Health Reform on Revenue Cycle Management Pyramid Healthcare Solutions Thought Leadership Series The healthcare industry is undergoing significant change in the face of the
University Healthcare Administrative Policy
 Page 1 of 6 APPROVED BY: Signatures on File FINANCIAL POLICY (UH) is a not-for profit teaching hospital committed to providing quality health care services. In order to provide necessary medical services
Page 1 of 6 APPROVED BY: Signatures on File FINANCIAL POLICY (UH) is a not-for profit teaching hospital committed to providing quality health care services. In order to provide necessary medical services
Regulatory Compliance Policy No. COMP-RCC 4.52 Title:
 I. SCOPE: Regulatory Compliance Policy No. COMP-RCC 4.52 Page: 1 of 19 This policy applies to (1) Tenet Healthcare Corporation and its wholly-owned subsidiaries and affiliates (each, an Affiliate ); (2)
I. SCOPE: Regulatory Compliance Policy No. COMP-RCC 4.52 Page: 1 of 19 This policy applies to (1) Tenet Healthcare Corporation and its wholly-owned subsidiaries and affiliates (each, an Affiliate ); (2)
Certain exceptions apply to Hospital Inpatient Confinement for childbirth as described below.
 Tennessee Applicable Policies PRECERTIFICATION Benefits payable for Hospital Inpatient Confinement Charges and confinement charges for services provided in an inpatient confinement facility will be reduced
Tennessee Applicable Policies PRECERTIFICATION Benefits payable for Hospital Inpatient Confinement Charges and confinement charges for services provided in an inpatient confinement facility will be reduced
The following online training module will provide a general overview of the Vanderbilt University Medical Center s (VUMC) technical revenue cycle.
 technical revenue cycle.") The following online training module will provide a general overview of the Vanderbilt University Medical Center s (VUMC) technical revenue cycle. This Revenue Cycle Overview training will establish a
The following online training module will provide a general overview of the Vanderbilt University Medical Center s (VUMC) technical revenue cycle. This Revenue Cycle Overview training will establish a
6 Critical Impact Factors of Health Reform on Revenue Cycle Management
 6 Critical Impact Factors of Health Reform on Revenue Cycle Management Pyramid Healthcare Solutions Thought Leadership Series The healthcare industry is undergoing significant change in the face of the
6 Critical Impact Factors of Health Reform on Revenue Cycle Management Pyramid Healthcare Solutions Thought Leadership Series The healthcare industry is undergoing significant change in the face of the
Top Ten Questions. Time and Energy. Robin Bradbury 800-355-0410 [email protected]
 Robin Bradbury 800-355-0410 [email protected] Top Ten Questions 1. What are the key measures for the Revenue Cycle? 2. How do you document and share this information with the Revenue Cycle staff? 3. What
Robin Bradbury 800-355-0410 [email protected] Top Ten Questions 1. What are the key measures for the Revenue Cycle? 2. How do you document and share this information with the Revenue Cycle staff? 3. What
HOSPITAL-ISSUED NOTICE OF NONCOVERAGE
 HOSPITAL-ISSUED NOTICE OF NONCOVERAGE Citations and Authority for Hospital-Issued Notice of Noncoverage (HINNs) The statutory authorities applicable to your review of a Hospital-Issued Notice of Noncoverage
HOSPITAL-ISSUED NOTICE OF NONCOVERAGE Citations and Authority for Hospital-Issued Notice of Noncoverage (HINNs) The statutory authorities applicable to your review of a Hospital-Issued Notice of Noncoverage
Transfer DRGs: Approaches to Revenue Recovery. A BESLER White Paper
 Transfer DRGs: Approaches to Revenue Recovery A BESLER White Paper June 2014 Copyright 2014 BESLER Consulting. All rights reserved. *HFMA staff and volunteers determined that Transfer DRG Revenue Recovery
Transfer DRGs: Approaches to Revenue Recovery A BESLER White Paper June 2014 Copyright 2014 BESLER Consulting. All rights reserved. *HFMA staff and volunteers determined that Transfer DRG Revenue Recovery
Frequently Asked Questions About Your Hospital Bills
 Frequently Asked Questions About Your Hospital Bills The Registration Process Why do I have to verify my address each time? Though address and telephone numbers remain constant for approximately 70% of
Frequently Asked Questions About Your Hospital Bills The Registration Process Why do I have to verify my address each time? Though address and telephone numbers remain constant for approximately 70% of
5 KPIs That Require Revenue Cycle Managers' Attention. Devendra Saharia FEATURE STORY. healthcare financial management association www.hfma.
 SEPTEMBER 2014 healthcare financial management association www.hfma.org FEATURE STORY 5 KPIs That Require Revenue Cycle Managers' Attention Devendra Saharia Devendra Saharia REPRINT September 2014 healthcare
SEPTEMBER 2014 healthcare financial management association www.hfma.org FEATURE STORY 5 KPIs That Require Revenue Cycle Managers' Attention Devendra Saharia Devendra Saharia REPRINT September 2014 healthcare
6 Critical Impact Factors of Health Reform on Revenue Cycle Management
 6 Critical Impact Factors of Health Reform on Revenue Cycle Management Pyramid Healthcare Solutions Thought Leadership Series The healthcare industry is undergoing significant change in the face of the
6 Critical Impact Factors of Health Reform on Revenue Cycle Management Pyramid Healthcare Solutions Thought Leadership Series The healthcare industry is undergoing significant change in the face of the
Hospital Denials Management In-source, Outsource or Both?
 Page 1 Hospital Denials Management In-source, Outsource or Both? by Holly Pelaia Summary A strong revenue stream case is made for intelligent outsourcing of hospital denials up to 20% more effective in
Page 1 Hospital Denials Management In-source, Outsource or Both? by Holly Pelaia Summary A strong revenue stream case is made for intelligent outsourcing of hospital denials up to 20% more effective in
CHAPTER 7: UTILIZATION MANAGEMENT
 OVERVIEW The Plan s Utilization Management (UM) program is collaboration with providers to promote and document the appropriate use of health care resources. The program reflects the most current utilization
OVERVIEW The Plan s Utilization Management (UM) program is collaboration with providers to promote and document the appropriate use of health care resources. The program reflects the most current utilization
Health Insurance SMART NC
 Health Insurance SMART NC ANNUAL REPORT ON EXTERNAL REVIEW ACTIVITY 202 North Carolina Department of Insurance Wayne Goodwin, Commissioner A REPORT ON EXTERNAL REVIEW REQUESTS IN NORTH CAROLINA Health
Health Insurance SMART NC ANNUAL REPORT ON EXTERNAL REVIEW ACTIVITY 202 North Carolina Department of Insurance Wayne Goodwin, Commissioner A REPORT ON EXTERNAL REVIEW REQUESTS IN NORTH CAROLINA Health
Premera Blue Cross Medicare Advantage Provider Reference Manual
 Premera Blue Cross Medicare Advantage Provider Reference Manual Introduction to Premera Blue Cross Medicare Advantage Plans Premera Blue Cross offers Medicare Advantage (MA) plans in King, Pierce, Snohomish,
Premera Blue Cross Medicare Advantage Provider Reference Manual Introduction to Premera Blue Cross Medicare Advantage Plans Premera Blue Cross offers Medicare Advantage (MA) plans in King, Pierce, Snohomish,
PREPARING FOR ICD-10 IDENTIFYING THE STEPS TO BE TAKEN AND THE TIMELINE MAY 2014
 PREPARING FOR ICD-10 IDENTIFYING THE STEPS TO BE TAKEN AND THE TIMELINE MAY 2014 Diane Taylor, BSN, RN Selman-Holman & Associates LLC, Senior Associate Selman-Holman & Associates, LLC Diane Taylor, BSN,
PREPARING FOR ICD-10 IDENTIFYING THE STEPS TO BE TAKEN AND THE TIMELINE MAY 2014 Diane Taylor, BSN, RN Selman-Holman & Associates LLC, Senior Associate Selman-Holman & Associates, LLC Diane Taylor, BSN,
Understanding Revenue Cycle Strategy How to Optimize Process and Performance
 Understanding Revenue Cycle Strategy How to Optimize Process and Performance White Paper 1.800.4BEACON BeaconPartners.com BOSTON CLEVELAND SAN FRANCISCO TORONTO The revenue cycle can no longer be seen
Understanding Revenue Cycle Strategy How to Optimize Process and Performance White Paper 1.800.4BEACON BeaconPartners.com BOSTON CLEVELAND SAN FRANCISCO TORONTO The revenue cycle can no longer be seen
What is the prior authorization process for Skilled Nursing Facility Admission?
 MyCare Long Term Care (LTC) Nursing Facility FAQs The nursing facility network is an essential part of the health care delivery system and we value your partnership. We appreciate the compassion you offer
MyCare Long Term Care (LTC) Nursing Facility FAQs The nursing facility network is an essential part of the health care delivery system and we value your partnership. We appreciate the compassion you offer
OBJECTIVES. Session 115 How to Manage Accounts Receivable & Cash Flow. M. Aaron Little, CPA. Melinda A. Gaboury, COS-C.
 Session 115 How to Manage Accounts Receivable & Cash Flow Melinda A. Gaboury, COS-C Healthcare CPAs Provider & ADVISORS Solutions, Inc. Chief Executive Officer [email protected]
Session 115 How to Manage Accounts Receivable & Cash Flow Melinda A. Gaboury, COS-C Healthcare CPAs Provider & ADVISORS Solutions, Inc. Chief Executive Officer [email protected]
NRH Medical Rehabilitation Network Adding Life to Years
 NRH Medical Rehabilitation Network Adding Life to Years Paul R. Rao Ph.D. CCC CPHQ FACHE Vice President, Clinical Services, Quality & Compliance National Rehabilitation Hospital 102 Irving Street NW Washington
NRH Medical Rehabilitation Network Adding Life to Years Paul R. Rao Ph.D. CCC CPHQ FACHE Vice President, Clinical Services, Quality & Compliance National Rehabilitation Hospital 102 Irving Street NW Washington
Frequently Asked Billing Questions
 Frequently Asked Billing Questions How will I be billed? Mayo Clinic Health System will send you a billing statement with your charges. Provider charges for clinic and hospital services will be billed
Frequently Asked Billing Questions How will I be billed? Mayo Clinic Health System will send you a billing statement with your charges. Provider charges for clinic and hospital services will be billed
Patient Access. The Big Opportunity
 Patient Access The Big Opportunity Evolution of the Revenue Cycle Over the last 10 15 years the industry has Increased Awareness Understanding Recognition Leading to.. Use of Key Performance Indicators
Patient Access The Big Opportunity Evolution of the Revenue Cycle Over the last 10 15 years the industry has Increased Awareness Understanding Recognition Leading to.. Use of Key Performance Indicators
Catch 22: The Case of Utilization Management s Return on Investment Evaluation
 14 Catch 22: The Case of Utilization Management s Return on Investment Evaluation Fern FitzHenry I ve just identified about $200,000 in charges that don t meet the medical necessity requirements, John
14 Catch 22: The Case of Utilization Management s Return on Investment Evaluation Fern FitzHenry I ve just identified about $200,000 in charges that don t meet the medical necessity requirements, John
Protect and Improve Profitability in Your Practice. Positioning Your Organization for a RAC Audit
 Protect and Improve Profitability in Your Practice Positioning Your Organization for a RAC Audit 2011 Annual Educational Seminar March 9, 2011 Presented By: Cindy Tipton-Cain, Exec. Director Physician
Protect and Improve Profitability in Your Practice Positioning Your Organization for a RAC Audit 2011 Annual Educational Seminar March 9, 2011 Presented By: Cindy Tipton-Cain, Exec. Director Physician
Behavioral Health (MAPSI) Utilization Management Program Components
 Utilization Management Program Components") Behavioral Health (MAPSI) Utilization Management Program Components Payer Name: Printed Name of Payer Representative: Phone: Is this document applicable to all groups? Yes No If no, please indicate specific
Behavioral Health (MAPSI) Utilization Management Program Components Payer Name: Printed Name of Payer Representative: Phone: Is this document applicable to all groups? Yes No If no, please indicate specific
8.470 HOSPITAL BACK UP LEVEL OF CARE PAGE 1 OF 10. Complex wound care means that the client meets the following criteria:
 8.470 HOSPITAL BACK UP LEVEL OF CARE PAGE 1 OF 10 8.470 HOSPITAL BACK UP LEVEL OF CARE 8.470.1 DEFINITIONS Complex wound care means that the client meets the following criteria: 1. Has at least one of
8.470 HOSPITAL BACK UP LEVEL OF CARE PAGE 1 OF 10 8.470 HOSPITAL BACK UP LEVEL OF CARE 8.470.1 DEFINITIONS Complex wound care means that the client meets the following criteria: 1. Has at least one of
CLAIM FORM REQUIREMENTS
 CLAIM FORM REQUIREMENTS When billing for services, please pay attention to the following points: Submit claims on a current CMS 1500 or UB04 form. Please include the following information: 1. Patient s
CLAIM FORM REQUIREMENTS When billing for services, please pay attention to the following points: Submit claims on a current CMS 1500 or UB04 form. Please include the following information: 1. Patient s
NORTH COUNTRY COMMUNITY MENTAL HEALTH NORTHERN AFFILIATION UTILIZATION MANAGEMENT PLAN November 1, 2001. Revised January 2013
 NORTH COUNTRY COMMUNITY MENTAL HEALTH NORTHERN AFFILIATION UTILIZATION MANAGEMENT PLAN November 1, 2001 Revised January 2013 I. Mission II. III. IV. Scope Philosophy Authority V. Utilization Management
NORTH COUNTRY COMMUNITY MENTAL HEALTH NORTHERN AFFILIATION UTILIZATION MANAGEMENT PLAN November 1, 2001 Revised January 2013 I. Mission II. III. IV. Scope Philosophy Authority V. Utilization Management
Exhibit 2.9 Utilization Management Program
 Exhibit 2.9 Utilization Management Program Access HealthSource, Inc. Utilization Management Company is licensed as a Utilization Review Agent with the Texas Department of Insurance. The Access HealthSource,
Exhibit 2.9 Utilization Management Program Access HealthSource, Inc. Utilization Management Company is licensed as a Utilization Review Agent with the Texas Department of Insurance. The Access HealthSource,
Denials Management: Key Assessment Steps to Prevent and Recover Repetitive Revenue Leakage
 Industry Landscape An aging U.S. population is fueling increased demand for hospital beds and healthcare services. However, with several years of shrinking margins and falling bond ratings for many hospitals,
Industry Landscape An aging U.S. population is fueling increased demand for hospital beds and healthcare services. However, with several years of shrinking margins and falling bond ratings for many hospitals,
West Penn Allegheny Health System
 West Penn Allegheny Health System System Compliance Department Medical Necessity and Billing for Inpatient Rehabilitation Lessons Learned from an Inpatient Rehab Unit Billing Audit 2006 HCCA Compliance
West Penn Allegheny Health System System Compliance Department Medical Necessity and Billing for Inpatient Rehabilitation Lessons Learned from an Inpatient Rehab Unit Billing Audit 2006 HCCA Compliance
Shellie Sulzberger, LPN, CPC, ICDCT-CM. Coding & Compliance Initiatives, Inc.
 Shellie Sulzberger, LPN, CPC, ICDCT-CM Coding & Compliance Initiatives, Inc. My connection to coding and documentation My connection to clinical processes My connection to ICD-10 My connection to YOU Coding
Shellie Sulzberger, LPN, CPC, ICDCT-CM Coding & Compliance Initiatives, Inc. My connection to coding and documentation My connection to clinical processes My connection to ICD-10 My connection to YOU Coding
Granville Health System
 Approved by: Granville Health System FINANCIAL POLICY Effective Date: Revised Date(s): FINANCIAL POLICY - DRAFT 09-16-2014 Granville Health System is a not-for profit hospital committed to providing quality
Approved by: Granville Health System FINANCIAL POLICY Effective Date: Revised Date(s): FINANCIAL POLICY - DRAFT 09-16-2014 Granville Health System is a not-for profit hospital committed to providing quality
Chapter 16 Restricted Recipient Program
 Chapter 16 Restricted Recipient Program Program Overview The Restricted Recipient Program (RRP) is a program developed by the Minnesota Department of Human Services for recipients who have failed to comply
Chapter 16 Restricted Recipient Program Program Overview The Restricted Recipient Program (RRP) is a program developed by the Minnesota Department of Human Services for recipients who have failed to comply
HEALTH INSURANCE UTILIZATION REVIEW, APPEALS AND GRIEVANCES YOUR RIGHTS AS A HEALTH INSURANCE CONSUMER
 CONSUMER'SGUIDE A Consumer s Guide to HEALTH INSURANCE UTILIZATION REVIEW, APPEALS AND GRIEVANCES YOUR RIGHTS AS A HEALTH INSURANCE CONSUMER from your North Carolina Department of Insurance A MESSAGE
CONSUMER'SGUIDE A Consumer s Guide to HEALTH INSURANCE UTILIZATION REVIEW, APPEALS AND GRIEVANCES YOUR RIGHTS AS A HEALTH INSURANCE CONSUMER from your North Carolina Department of Insurance A MESSAGE
The Power of Metrics Part Two. By Rob Borchert, CPAM Altarum Institute: Revenue Cycle Management Practice
 The Power of Metrics Part Two By Rob Borchert, CPAM July 2009 The Power of Metrics Part Two By Rob Borchert, CPAM Altarum Institute: Revenue Cycle Management Practice July 2009 THE POWER OF METRICS PART
The Power of Metrics Part Two By Rob Borchert, CPAM July 2009 The Power of Metrics Part Two By Rob Borchert, CPAM Altarum Institute: Revenue Cycle Management Practice July 2009 THE POWER OF METRICS PART
REIMBURSEMENT CODING SERIES
 REIMBURSEMENT CODING SERIES Occ. Work Prob. Effective Last Code No. Class Title Area Area Period Date Action 4839 Reimbursement Coder 02 445 6 mo. 00/00/00 Rev. 4840 Reimbursement Coding Specialist 02
REIMBURSEMENT CODING SERIES Occ. Work Prob. Effective Last Code No. Class Title Area Area Period Date Action 4839 Reimbursement Coder 02 445 6 mo. 00/00/00 Rev. 4840 Reimbursement Coding Specialist 02
Appeals Provider Manual 15
 Table of Contents Overview... 15.1 Commercial Member appeals... 15.1 Self-insured groups... 15.1 Traditional/CMM Members... 15.1 Who may appeal... 15.1 How to file an internal appeal on behalf of the Member...
Table of Contents Overview... 15.1 Commercial Member appeals... 15.1 Self-insured groups... 15.1 Traditional/CMM Members... 15.1 Who may appeal... 15.1 How to file an internal appeal on behalf of the Member...
UB-04, Inpatient / Outpatient
 UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
Using Six Sigma Concepts to Improve Revenue Cycle
 Using Six Sigma Concepts to Improve Revenue Cycle Presented by Joseph Koons, MHSA, FHFMA, CRCE-I Managing Director, Revenue Cycle Centra Health Lynchburg Virginia March 4, 2014 Agenda Introduction to
Using Six Sigma Concepts to Improve Revenue Cycle Presented by Joseph Koons, MHSA, FHFMA, CRCE-I Managing Director, Revenue Cycle Centra Health Lynchburg Virginia March 4, 2014 Agenda Introduction to
Online Provider/Pharmacy Directory: New Guidelines and Requirements
 Vol. 3, No. 3 PROVIDER PULSE October - 2015 In This Issue New Guidelines... page 1 Provider Portal...page 2 Part D...page 2 Medical Services... page 3 Quality...page 4 Claims/New Rep...page 5 Online Provider/Pharmacy
Vol. 3, No. 3 PROVIDER PULSE October - 2015 In This Issue New Guidelines... page 1 Provider Portal...page 2 Part D...page 2 Medical Services... page 3 Quality...page 4 Claims/New Rep...page 5 Online Provider/Pharmacy
HEALTH CARE AUDITING & MONITORING TOOLS
 HEALTH CARE AUDITING & MONITORING TOOLS TABLE OF CONTENTS ABOUT THIS MANUAL SUGGESTIONS INTRODUCTION LIST OF CONTRIBUTORS MONITORING & AUDITING PRACTICES FOR EFFECTIVE COMPLIANCE PLANNING AND CONDUCTING
HEALTH CARE AUDITING & MONITORING TOOLS TABLE OF CONTENTS ABOUT THIS MANUAL SUGGESTIONS INTRODUCTION LIST OF CONTRIBUTORS MONITORING & AUDITING PRACTICES FOR EFFECTIVE COMPLIANCE PLANNING AND CONDUCTING
Revenue Cycle Responsibilities. Revenue Cycle. Objectives 4/9/2013
 Revenue Cycle Kathryn DeVault, RHIA, CCS, CCS-P AHIMA 2013 Objectives Identify responsibilities within the Revenue Cycle Focus on management of the revenue cycle process Discuss the revenue cycle process
Revenue Cycle Kathryn DeVault, RHIA, CCS, CCS-P AHIMA 2013 Objectives Identify responsibilities within the Revenue Cycle Focus on management of the revenue cycle process Discuss the revenue cycle process
MINIMUM STANDARDS FOR UTILIZATION REVIEW AGENTS
 MINIMUM STANDARDS FOR UTILIZATION REVIEW AGENTS Title 15: Mississippi State Department of Health Part 3: Office of Health Protection Subpart 1: Health Facilities Licensure and Certification Post Office
MINIMUM STANDARDS FOR UTILIZATION REVIEW AGENTS Title 15: Mississippi State Department of Health Part 3: Office of Health Protection Subpart 1: Health Facilities Licensure and Certification Post Office
Compensation and Claims Processing
 Compensation and Claims Processing Compensation The network rate for eligible outpatient visits is reimbursed to you at the lesser of (1) your customary charge, less any applicable co-payments, coinsurance
Compensation and Claims Processing Compensation The network rate for eligible outpatient visits is reimbursed to you at the lesser of (1) your customary charge, less any applicable co-payments, coinsurance
Riverside Physician Network Utilization Management
 Subject: Program Riverside Physician Network Author: Candis Kliewer, RN Department: Product: Commercial, Senior Revised by: Linda McKevitt, RN Approved by: Effective Date January 1997 Revision Date 1/21/15
Subject: Program Riverside Physician Network Author: Candis Kliewer, RN Department: Product: Commercial, Senior Revised by: Linda McKevitt, RN Approved by: Effective Date January 1997 Revision Date 1/21/15
Denial Management: Best Practices and Evaluation
 Denial Management: Best Practices and Evaluation Presented by Principal Auditor Susan M. Walker University of California, San Francisco April 9, 2015 Internal Audit Webinar Series Webinar Agenda Project
Denial Management: Best Practices and Evaluation Presented by Principal Auditor Susan M. Walker University of California, San Francisco April 9, 2015 Internal Audit Webinar Series Webinar Agenda Project
Revenue Cycle. An operational overview and some ideas of how to negotiate the complex roads ahead. HFMA ROAD SHOW SUTTER CENTER FOR HEALTH PROFESSIONS
 HFMA ROAD SHOW SUTTER CENTER FOR HEALTH PROFESSIONS Presented by: Steve Thompson and the PFS Revenue Cycle Committee January 7, 2008 Revenue Cycle An operational overview and some ideas of how to negotiate
HFMA ROAD SHOW SUTTER CENTER FOR HEALTH PROFESSIONS Presented by: Steve Thompson and the PFS Revenue Cycle Committee January 7, 2008 Revenue Cycle An operational overview and some ideas of how to negotiate
Appeals and Provider Dispute Resolution
 Appeals and Provider Dispute Resolution There are two distinct processes related to Non-Coverage (Adverse) Determinations (NCD) regarding requests for services or payment: (1) Appeals and (2) Provider
Appeals and Provider Dispute Resolution There are two distinct processes related to Non-Coverage (Adverse) Determinations (NCD) regarding requests for services or payment: (1) Appeals and (2) Provider
Session Name Objectives Suggested Attendees
 Cerner Demonstration Sesion Descriptions Cerner Demonstration Session Descriptions Thursday, November 12 th Session Name Objectives Suggested Attendees Day in the Life - Care Across the Continuum An overview
Cerner Demonstration Sesion Descriptions Cerner Demonstration Session Descriptions Thursday, November 12 th Session Name Objectives Suggested Attendees Day in the Life - Care Across the Continuum An overview
BILLING COMPANY STANDARDS
 BILLING COMPANY STANDARDS ASSESSING PRACTICE VALUE OF OUTSOURCING Cost Saving Efficiencies gained Improved collections Compliance Once a decision to out source is made the following due diligence should
BILLING COMPANY STANDARDS ASSESSING PRACTICE VALUE OF OUTSOURCING Cost Saving Efficiencies gained Improved collections Compliance Once a decision to out source is made the following due diligence should
Westchester Medical Center. 2014 Operating Budget
 Westchester Medical Center 2014 Operating Budget December 4, 2013 WESTCHESTER COUNTY HEALTH CARE CORPORATION Operating Budget 2014 Table of Contents Page Executive Summary 1 Detailed Discussion of Revenue
Westchester Medical Center 2014 Operating Budget December 4, 2013 WESTCHESTER COUNTY HEALTH CARE CORPORATION Operating Budget 2014 Table of Contents Page Executive Summary 1 Detailed Discussion of Revenue
SECTION 7: APPEALS TEXAS MEDICAID PROVIDER PROCEDURES MANUAL: VOL. 1
 TEXAS MEDICAID PROVIDER PROCEDURES MANUAL: VOL. 1 SECTION 7: APPEALS 7.1 Appeal Methods................................................................. 7-2 7.1.1 Electronic Appeal Submission.......................................................
TEXAS MEDICAID PROVIDER PROCEDURES MANUAL: VOL. 1 SECTION 7: APPEALS 7.1 Appeal Methods................................................................. 7-2 7.1.1 Electronic Appeal Submission.......................................................
What Happens When Your Health Insurance Carrier Says NO
 * What Happens When Your Health Insurance Carrier Says NO Most health carriers today carefully evaluate requests to see a specialist or have certain medical procedures performed. A medical professional
* What Happens When Your Health Insurance Carrier Says NO Most health carriers today carefully evaluate requests to see a specialist or have certain medical procedures performed. A medical professional