EMR Can anyone do this?
|
|
|
- Marcus Dennis Wilcox
- 10 years ago
- Views:
Transcription
1 EMR Can anyone do this? Norio Fukami, MD University of Colorado Piecemeal resection? 1

2 Endoscopic mucosal resection (EMR) and Endoscopic submucosal dissection (ESD) Endoscopic removal of premalignant or malignant gastrointestinal epithelium = Minimally invasive endosurgical treatment of GI tumors = Diagnostic and Therapeutic procedure Can remove certain submucosal tumors e.g. Granular cell tumor, Carcinoid; GIST (?) History of EMR & ESD Simple snare removal (1968) Saline injection and snare resection (1983) Double channel - pinch and cut (1984) Movement to explore Endoscopic removal as an alternative to Surgery Band and resect (1993) EMR cap method (1993) Endoscopic submucosal dissection (mid-late 1990s) Soetikno et al. GIE. 2003(4) 2
 EMR cap method (1993) Endoscopic submucosal dissection (mid-late 1990s) Soetikno et al. GIE. 2003(4) 2")
3 EMR tools Snare injection Cap-EMR Band-EMR ESD knives KD 10Q-1 3

4 EMR/ESD for the cure of cancer Resection of premalignant or malignant lesion as an alternative to surgery Aimed for R0 resection Negative lateral and deep margin = local recurrence Cure = No or very low risk for lymph node metastasis or distant metastasis Preprocedural assessment is mandatory Know when to do it! - Exclude possible non-candidate Weigh risk and benefit Re-assessment after resection: Pathological evaluation Cancer T stage Depth of cancer invasion T1 T2 T3 4

5 Sub-classification of T1 tumor m1: limited within mucosa (HGD) m2: invades into lamina propria m3: invades into muscularis mucosae sm1-3: divide submucosal layer in three even thickness Soetikno et al. GIE. 2003(4) T1 T2 Esophageal cancer AJCC/UICC TNM, 7th edition 5

6 Colon cancer AJCC/UICC TNM, 7th edition Lymph node metastasis risk for T1 tumor varies EMR absolute indication Esophagus SCC m1 0% m2 3% Esophagus Adeno Ca 0% m3 9% 2-3% sm % sm2 sm3 Stomach 13~48% 35~50% ~20% Colon 0-0.4% 0% ~2.5% 10~% Important Factors: lymphovascular invasion, tumor differentiation, tumor budding 6

7 How far can we go? Expanded indications Esophageal cancer (mostly SCC) T1-m1-m2: LN mets 0-3% T1 m3-sm1: LN mets 10-20% But, LN mets 4% if differentiated type & no LV invasion & expansion growth *1 *1 Oyama et al

8 Esophageal cancer (Barrett cancer) sm1 invasion: 9.5% LN mets if LV(-) vs. 20% if LV (+) *1 sm1 invasion with LV(-), differentiated type, expansive growth: - No clinical evidence of metastasis, cancer death during the mean f/u 62 months *2 *1 Badreddine et al. CGH 2010 *2 Manner et al. AJG 2008 Gastric cancer Expanded indication less than 500 μm LN mets; 0-2.5% Gotoda et al. Gastric Cancer % Hirasawa et al. Gastric Cancer 2009 Soetikno et al. J Clin Oncol

9 Colon cancer SM invasion is not considered to be absolute surgical contraindication for endoscopic therapy - no LN mets in the absence of LV invasion less than 3000 μm invasion depth for polypoid less than 1000 μm invasion depth for nonpolypoid lesions *1 *1 Kitajima et al. J Gastroenterol 2004 SM indication for EMR/ESD: less than 1000 μm depth of invasion, differentiated type, no LVI, and no tumor budding. Master s guide for endoscopic diagnosis. Tajiri and Saito Lymph node metastasis risk for T1 tumor EMR absolute indication expanded d indication Esophagus SCC m1 0% m2 3% Esophagus Adeno Ca 0% m3 9% 2-3% sm % sm2 sm3 Stomach 13~48% 35~50% ~20% Colon 0-0.4% 0% 500 μm superficial ~2.5% 1000 μm sm invasion 10~% Important Factors: lymphovascular invasion, tumor differentiation, tumor budding 9

10 Diagnostic or Therapeutic? Basic technique for pathology specimen processing Specimen processing Evaluation of the margins (lateral/deep) requires perpendicular slices Pinnig specimens onto the board before formalin fixation Good! 10

11 Stage/depth assessment Endoscopic assessment of cancer to predict T stage Meticulous evaluation: 85-95% accurate (Tm1-2, 3 vs. sm superficial vs. deep invasion) - superficial type of esophageal SCC (0-IIa-c) and <2cm = m1-2 EUS with HF probe: 80-90% accuracy Paris workshop group. GIE
 - superficial type of esophageal SCC (0-IIa-c) and <2cm =")
12 What to look for? Configuration Fold convergence (thickening, irregularity etc.) Depression Loss of surface patterns or abnormal vessels Stiffness of the wall What to look for as a sign of deep invasion? Master s guide for endoscopic diagnosis. Tajiri and Saito

13 Case study esophagus SCC moderately differentiated, 2.4cm, sm1 no LV invasion 13

14 well differentiated adenocarcinoma, T1a (m2) poorly differentiated adenocarcinoma, T3N1 14

15 Barrett s esophagus with LGD adecarcinoma in Barrett s, T1sm-T2 15

16 Barrett s esophagus with poorly differentiated adenocarcinoma T1sm, N1 at upper paratracheal LN stomach 16

17 well differentiated adenocarcinoma, T1a (m2) 6cm poorly differentiated adenocarcinoma, T1b positive deep margin total gastrectomy no tumor and negative LN 17

18 differentiated adenocarcinoma, T1a (m3), UL + Master s guide for endoscopic diagnosis. Tajiri and Saito poorly differentiated adenocarcinoma, T1a (m3) Master s guide for endoscopic diagnosis. Tajiri and Saito

19 colon Tubular adenoma 19

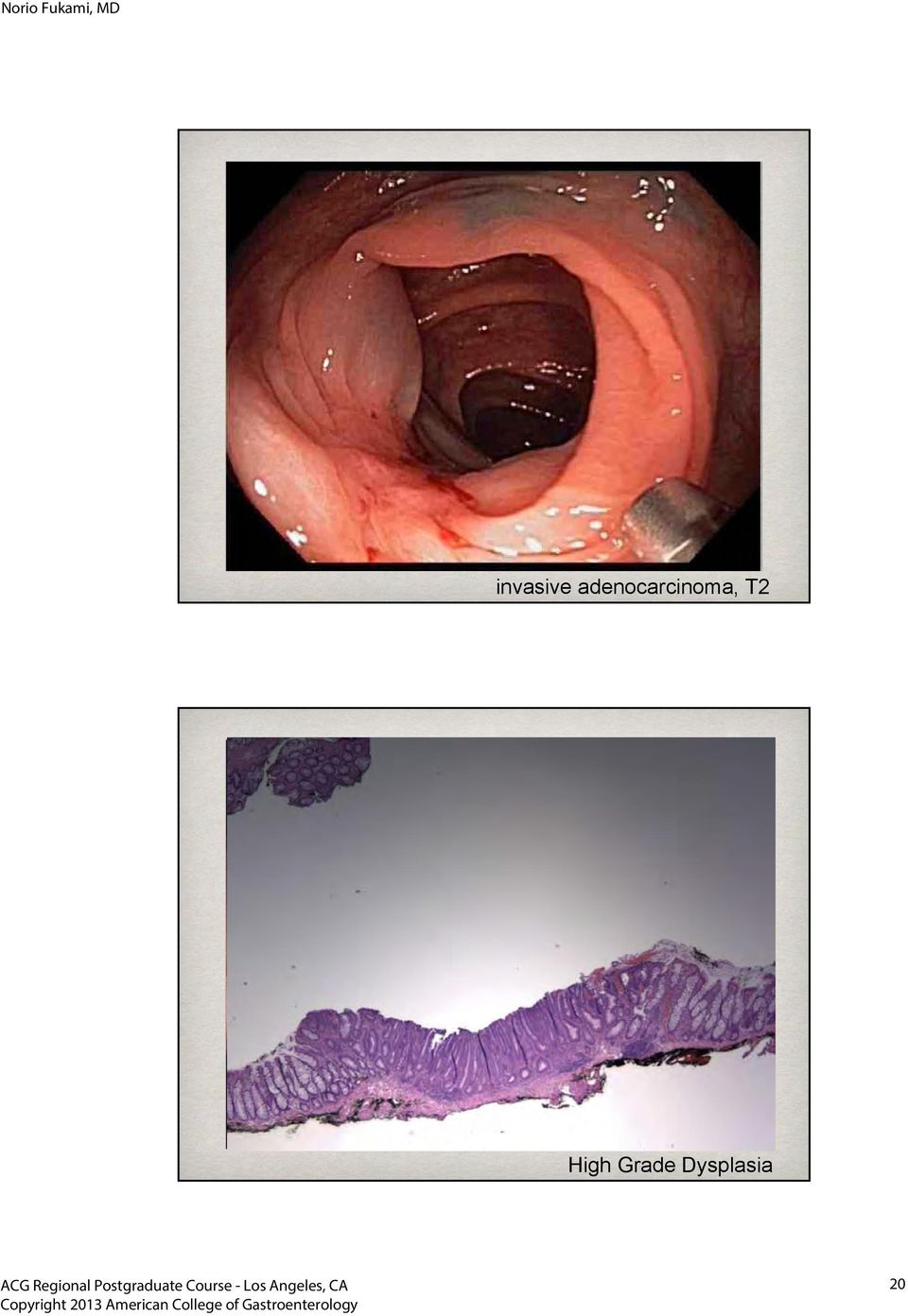
20 invasive adenocarcinoma, T2 High Grade Dysplasia 20
21 8mm moderately differentiated adenocarcinoma, T1sm, 3700 μm Master s guide for endoscopic diagnosis. Tajiri and Saito adenocarcinoma, T2 21
22 adenocarcinoma, Tis (invasive to lp) LST, granular type 5.5cm, Tis 22
23 Conclusions You can do it! - Learn the proper steps Understand the proper indication and the assessment for curative resection Pre-EMR/ESD evaluation is important to select the treatment modality - cut BIG as necessary! Process the specimen properly = prediction of the outcome and risk for recurrence 23
How to report Upper GI EMR/ESD specimens
 Section of Pathology and Tumour Biology How to report Upper GI EMR/ESD specimens Dr.H.Grabsch Warning. Most of the criteria, methodologies, evidence presented in this talk are based on studies in early
Section of Pathology and Tumour Biology How to report Upper GI EMR/ESD specimens Dr.H.Grabsch Warning. Most of the criteria, methodologies, evidence presented in this talk are based on studies in early
Learning Luncheon 7: Endoscopic Mucosal Resection: When, Where and How?
 Endoscopic Mucosal Resection (EMR): When, Where, and Charles J. Lightdale, MD Columbia University New York, NY Endoscopic Mucosal Resection (EMR) EMR developed for removal of sessile or flat neoplasms
Endoscopic Mucosal Resection (EMR): When, Where, and Charles J. Lightdale, MD Columbia University New York, NY Endoscopic Mucosal Resection (EMR) EMR developed for removal of sessile or flat neoplasms
Endoscopic Resection for Barrett s Esophagus and Early Cancer 2014 Masters of Minimally Invasive Surgery
 Endoscopic Resection for Barrett s Esophagus and Early Cancer 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation: Patient ER 51 y/o man with schizophrenia
Endoscopic Resection for Barrett s Esophagus and Early Cancer 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation: Patient ER 51 y/o man with schizophrenia
Endoscopic Therapy for Early Esophageal Cancer: EMR and ESD
 Endoscopic Therapy for Early Esophageal Cancer: EMR and ESD AATS Toronto April 26, 2014 Lorenzo Ferri MD PhD David S. Mulder Chair in Surgery Associate Professor of Surgery and Oncology Disclosures Olympus
Endoscopic Therapy for Early Esophageal Cancer: EMR and ESD AATS Toronto April 26, 2014 Lorenzo Ferri MD PhD David S. Mulder Chair in Surgery Associate Professor of Surgery and Oncology Disclosures Olympus
Captivator EMR Device
 Device Clinical Article and Abstract Summary Endoscopic Mucosal Bergman et al: EMR Training Tips Bergman et al: EMR Learning Curve ASGE: EMR & ESD Guidelines Bergman et al: Captivator EMR vs Cook Duette
Device Clinical Article and Abstract Summary Endoscopic Mucosal Bergman et al: EMR Training Tips Bergman et al: EMR Learning Curve ASGE: EMR & ESD Guidelines Bergman et al: Captivator EMR vs Cook Duette
Cancer of the Cardia/GE Junction: Surgical Options
 Cancer of the Cardia/GE Junction: Surgical Options Michael A Smith, MD Associate Chief Thoracic Surgery Center for Thoracic Disease St Joseph s Hospital and Medical Center Phoenix, AZ Michael Smith, MD
Cancer of the Cardia/GE Junction: Surgical Options Michael A Smith, MD Associate Chief Thoracic Surgery Center for Thoracic Disease St Joseph s Hospital and Medical Center Phoenix, AZ Michael Smith, MD
Endoscopic Submucosal Dissection (E.S.D.) vs. Endoscopic Mucosal Resection (E.M.R.) in Colombia. Advocating E.M.R.
 vs. Endoscopic Mucosal Resection (E.M.R.) in Colombia. Advocating E.M.R.") Controversies in Gastroenterology Endoscopic Submucosal Dissection (E.S.D.) vs. Endoscopic Mucosal Resection (E.M.R.) in Colombia. Advocating E.M.R. Raúl Cañadas Garrido, MD. 1 1 Internist-Gastroenterologist.
Controversies in Gastroenterology Endoscopic Submucosal Dissection (E.S.D.) vs. Endoscopic Mucosal Resection (E.M.R.) in Colombia. Advocating E.M.R. Raúl Cañadas Garrido, MD. 1 1 Internist-Gastroenterologist.
These parameters cannot, at the present time, be determined by non-invasive imaging techniques.
 Endoscopic Mucosal Resection for Upper Gastrointestinal Lesions Kenneth K. Wang, M.D. Chairman, WEO Publication and Guidelines Committee Professor of Medicine, Mayo Clinic Rochester, Minnesota Upper gastrointestinal
Endoscopic Mucosal Resection for Upper Gastrointestinal Lesions Kenneth K. Wang, M.D. Chairman, WEO Publication and Guidelines Committee Professor of Medicine, Mayo Clinic Rochester, Minnesota Upper gastrointestinal
Endoscopic mucosal resection for treatment of early gastric cancer
 Gut 2001;48:225 229 225 Endoscopic mucosal resection for treatment of early gastric cancer H Ono, H Kondo, T Gotoda, K Shirao, H Yamaguchi, D Saito, K Hosokawa, T Shimoda, S Yoshida Department of Endoscopy
Gut 2001;48:225 229 225 Endoscopic mucosal resection for treatment of early gastric cancer H Ono, H Kondo, T Gotoda, K Shirao, H Yamaguchi, D Saito, K Hosokawa, T Shimoda, S Yoshida Department of Endoscopy
Evolution of Barrett s esophagus
 Endoscopic Treatment and Surveillance of Esophageal Cancer: GI Perspective Charles J. Lightdale, MD Columbia University New York, NY Evolution of Barrett s esophagus Squamous esophagus Chronic inflammation
Endoscopic Treatment and Surveillance of Esophageal Cancer: GI Perspective Charles J. Lightdale, MD Columbia University New York, NY Evolution of Barrett s esophagus Squamous esophagus Chronic inflammation
How to treat early gastric cancer. Surgery
 How to treat early gastric cancer Surgery Mark I. van Berge Henegouwen Department of Surgery, AMC, Amsterdam Director upper GI surgical unit Academic Medical Center Upper GI surgery at AMC 100 oesophagectomies
How to treat early gastric cancer Surgery Mark I. van Berge Henegouwen Department of Surgery, AMC, Amsterdam Director upper GI surgical unit Academic Medical Center Upper GI surgery at AMC 100 oesophagectomies
Bridging Techniques. What s between EMR and Traditional Surgery? Elisabeth C. McLemore, MD, FACS, FASCRS
 Bridging Techniques What s between EMR and Traditional Surgery? Elisabeth C. McLemore, MD, FACS, FASCRS Associate Professor of Surgery Assistant Program Director, General Surgery Residency Disclosures
Bridging Techniques What s between EMR and Traditional Surgery? Elisabeth C. McLemore, MD, FACS, FASCRS Associate Professor of Surgery Assistant Program Director, General Surgery Residency Disclosures
Endoscopic submucosal dissection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline
 Guideline") Guideline 829 Endoscopic submucosal dissection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline Authors Institutions Pedro Pimentel-Nunes 1, Mário Dinis-Ribeiro 1, Thierry Ponchon 2, Alessandro
Guideline 829 Endoscopic submucosal dissection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline Authors Institutions Pedro Pimentel-Nunes 1, Mário Dinis-Ribeiro 1, Thierry Ponchon 2, Alessandro
ESD for colorectal lesions I am in favour. Alessandro Repici, MD Digestive Endoscopy Unit IRCCS Istituto Clinico Humanitas Milano, Italy
 ESD for colorectal lesions I am in favour Alessandro Repici, MD Digestive Endoscopy Unit IRCCS Istituto Clinico Humanitas Milano, Italy Surgery for early colonic lesions 51 pts referred for lap colectomy
ESD for colorectal lesions I am in favour Alessandro Repici, MD Digestive Endoscopy Unit IRCCS Istituto Clinico Humanitas Milano, Italy Surgery for early colonic lesions 51 pts referred for lap colectomy
Barrett s oesophagus: specimen handling and reporting
 Barrett s oesophagus: specimen handling and reporting Professor Neil A Shepherd Gloucester and Cheltenham, UK The role of the pathologist in Barrett s oesophagus 1. Diagnosis 2. Typing 3. Assessing response
Barrett s oesophagus: specimen handling and reporting Professor Neil A Shepherd Gloucester and Cheltenham, UK The role of the pathologist in Barrett s oesophagus 1. Diagnosis 2. Typing 3. Assessing response
Success rate of curative endoscopic mucosal resection with circumferential mucosal incision assisted by submucosal injection of sodium hyaluronate
 Success rate of curative endoscopic mucosal resection with circumferential mucosal incision assisted by submucosal injection of sodium hyaluronate Hironori Yamamoto, MD, Hiroshi Kawata, MD, Keijiro Sunada,
Success rate of curative endoscopic mucosal resection with circumferential mucosal incision assisted by submucosal injection of sodium hyaluronate Hironori Yamamoto, MD, Hiroshi Kawata, MD, Keijiro Sunada,
Challenges in gastric, appendiceal and rectal NETs Leuven, 29.11.2014
 Challenges in gastric, appendiceal and rectal NETs Leuven, 29.11.2014 Prof. Dr. Chris Verslype, Leuven Prof. Dr. Aurel Perren, Bern Menue Challenges: 1. Gastric NET 2. Appendiceal NET 3. Rectal NET SEER,
Challenges in gastric, appendiceal and rectal NETs Leuven, 29.11.2014 Prof. Dr. Chris Verslype, Leuven Prof. Dr. Aurel Perren, Bern Menue Challenges: 1. Gastric NET 2. Appendiceal NET 3. Rectal NET SEER,
Endoscopic Management of Barrett s High-Grade Dysplasia and Early Stage Esophageal Cancer
 VOLUME 10, ISSUE 2, YEAR 2011 Endoscopic Management of Barrett s High-Grade Dysplasia and Early Stage Esophageal Cancer James L. Wise, MD Duluth, MN. Introduction: In recent years there has been intense
VOLUME 10, ISSUE 2, YEAR 2011 Endoscopic Management of Barrett s High-Grade Dysplasia and Early Stage Esophageal Cancer James L. Wise, MD Duluth, MN. Introduction: In recent years there has been intense
HOW I DO IT Endoscopic mucosal resection (EMR) in the esophagus
 in the esophagus") HOW I DO IT (EMR) in the esophagus AUTHORSHIP How I do it: Horst Neuhaus, MD Department of Internal Medicine Evangelisches Krankenhaus Düsseldorf Germany Comment Hiroyasu Makuuchi, MD Professor and Chairman
HOW I DO IT (EMR) in the esophagus AUTHORSHIP How I do it: Horst Neuhaus, MD Department of Internal Medicine Evangelisches Krankenhaus Düsseldorf Germany Comment Hiroyasu Makuuchi, MD Professor and Chairman
Endo Conference: Large Polypectomy & EMR
 Endo Conference: Large Polypectomy & EMR Dr. Whang Feb 3, 2015 VOGELGRAM: genetic pathway of colorectal cancer & genes affected by point mutations Outline I. Baseline Colonoscopy II. Colon Polyps III.
Endo Conference: Large Polypectomy & EMR Dr. Whang Feb 3, 2015 VOGELGRAM: genetic pathway of colorectal cancer & genes affected by point mutations Outline I. Baseline Colonoscopy II. Colon Polyps III.
Center for Endoscopic Research & Therapeutics
 Center for Endoscopic Research & Therapeutics 5758 South Maryland Avenue (MC9028) Chicago, Illinois 60637 (773) 702-1459 www.uchospitals.edu Center for Endoscopic Research & Therapeutics To refer a patient
Center for Endoscopic Research & Therapeutics 5758 South Maryland Avenue (MC9028) Chicago, Illinois 60637 (773) 702-1459 www.uchospitals.edu Center for Endoscopic Research & Therapeutics To refer a patient
Endoscopic mucosal resection (EMR) of colorectal neoplasms ENDOSCOPY CORNER
 of colorectal neoplasms ENDOSCOPY CORNER") CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:22 26 ENDOSCOPY CORNER Efficacy of Endoscopic Mucosal Resection With Circumferential Incision for Patients With Large Colorectal Tumors TAKU SAKAMOTO, TAKAHISA
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:22 26 ENDOSCOPY CORNER Efficacy of Endoscopic Mucosal Resection With Circumferential Incision for Patients With Large Colorectal Tumors TAKU SAKAMOTO, TAKAHISA
9. Discuss guidelines for follow-up post-thyroidectomy for cancer (labs/tests) HH
 HH") 9. Discuss guidelines for follow-up post-thyroidectomy for cancer (labs/tests) HH Differentiated thyroid cancer expresses the TSH receptor on the cell membrane and responds to TSH stimulation by increasing
9. Discuss guidelines for follow-up post-thyroidectomy for cancer (labs/tests) HH Differentiated thyroid cancer expresses the TSH receptor on the cell membrane and responds to TSH stimulation by increasing
POEM Procedure for. Esophageal Achalasia
 POEM Procedure for Esophageal Achalasia POEM (Per-Oral endoscopic myotomy) is an incisionless procedure to treat esophageal achalasia, totally performed by endoscopy, without cutting the surface of the
POEM Procedure for Esophageal Achalasia POEM (Per-Oral endoscopic myotomy) is an incisionless procedure to treat esophageal achalasia, totally performed by endoscopy, without cutting the surface of the
Use of stents in esophageal cancer" Hans Gerdes, M.D. Director, GI Endoscopy Unit Memorial Sloan-Kettering Cancer Center
 Use of stents in esophageal cancer" Hans Gerdes, M.D. Director, GI Endoscopy Unit Memorial Sloan-Kettering Cancer Center Features of esophageal cancer Esophageal cancer is an abnormal growth that arises
Use of stents in esophageal cancer" Hans Gerdes, M.D. Director, GI Endoscopy Unit Memorial Sloan-Kettering Cancer Center Features of esophageal cancer Esophageal cancer is an abnormal growth that arises
Recurrent & Persistent Papillary Thyroid Cancer Central Nodal Dissection vs. Node-Picking Patterns of Nodal Metastases Recurrent Laryngeal Nerve,
 Recurrent & Persistent Papillary Thyroid Cancer Central Nodal Dissection vs. Node-Picking Patterns of Nodal Metastases Recurrent Laryngeal Nerve, Larynx, Trachea, & Esophageal Management Robert C. Wang,
Recurrent & Persistent Papillary Thyroid Cancer Central Nodal Dissection vs. Node-Picking Patterns of Nodal Metastases Recurrent Laryngeal Nerve, Larynx, Trachea, & Esophageal Management Robert C. Wang,
ERBEJET 2. The versatility of waterjet surgery: ERBEJET 2 with hybrid instruments WATERJET SURGERY
 ERBEJET 2 The versatility of waterjet surgery: ERBEJET 2 with hybrid instruments WATERJET SURGERY Gentle interventions in surgery and endoscopy Waterjet surgery with hybrid technology Waterjet surgery
ERBEJET 2 The versatility of waterjet surgery: ERBEJET 2 with hybrid instruments WATERJET SURGERY Gentle interventions in surgery and endoscopy Waterjet surgery with hybrid technology Waterjet surgery
Post-DDW OAG Course - Therapeutic Endoscopy
 Post-DDW OAG Course - Therapeutic Endoscopy June 13, 2015 Jeffrey Mosko Division of Gastroenterology St. Michael's Hospital University of Toronto [email protected] Program Name: Post-DDW OAG course CanMEDS
Post-DDW OAG Course - Therapeutic Endoscopy June 13, 2015 Jeffrey Mosko Division of Gastroenterology St. Michael's Hospital University of Toronto [email protected] Program Name: Post-DDW OAG course CanMEDS
Endoscopic Diagnosis and Treatment for Colorectal Cancer
 17 Endoscopic Diagnosis and Treatment for Colorectal Cancer Hiroyuki Kato, Teruhiko Sakamoto, Hiroko Otsuka, Rieko Yamada and Kiyo Watanabe Tokyo Women s Medical University, Medical Center East, Department
17 Endoscopic Diagnosis and Treatment for Colorectal Cancer Hiroyuki Kato, Teruhiko Sakamoto, Hiroko Otsuka, Rieko Yamada and Kiyo Watanabe Tokyo Women s Medical University, Medical Center East, Department
Endotherapy for high grade dysplasia & early oesophageal neoplasia in Barrett s oesophagus: A single centre retrospective audit
 Endotherapy for high grade dysplasia & early oesophageal neoplasia in Barrett s oesophagus: A single centre retrospective audit U Duffy, K Gowland, AI Morris, HL Smart Department of Gastroenterology, Royal
Endotherapy for high grade dysplasia & early oesophageal neoplasia in Barrett s oesophagus: A single centre retrospective audit U Duffy, K Gowland, AI Morris, HL Smart Department of Gastroenterology, Royal
Thursday, November 3, 2005
 Thursday, November 3, 2005 8:30-10:30 a. m. Gastric Tumors, Session 1 Chairman: P. Ruszniewski, Clichy, France 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders: G. Rindi, Parma,
Thursday, November 3, 2005 8:30-10:30 a. m. Gastric Tumors, Session 1 Chairman: P. Ruszniewski, Clichy, France 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders: G. Rindi, Parma,
The digestive system. Medicine and technology. Normal structure and function Diagnostic methods Example diseases and therapies
 The digestive system Medicine and technology Normal structure and function Diagnostic methods Example diseases and therapies The digestive system An overview (1) Oesophagus Liver (hepar) Biliary system
The digestive system Medicine and technology Normal structure and function Diagnostic methods Example diseases and therapies The digestive system An overview (1) Oesophagus Liver (hepar) Biliary system
National Program of Cancer Registries Education and Training Series. How to Collect High Quality Cancer Surveillance Data
 National Program of Cancer Registries Education and Training Series How to Collect High Quality Cancer Surveillance Data 1 NAACCR Administers NPCR-Education Contract for the Centers for Disease Control
National Program of Cancer Registries Education and Training Series How to Collect High Quality Cancer Surveillance Data 1 NAACCR Administers NPCR-Education Contract for the Centers for Disease Control
Magnetic Anchor for More Effective Endoscopic Mucosal Resection
 Jpn J Clin Oncol 2004;34(3)118 123 Magnetic Anchor for More Effective Endoscopic Mucosal Resection Toshiaki Kobayashi 1, Takushi Gotohda 1, Katsunori Tamakawa 2, Hirohisa Ueda 3 and Tadao Kakizoe 1 1 National
Jpn J Clin Oncol 2004;34(3)118 123 Magnetic Anchor for More Effective Endoscopic Mucosal Resection Toshiaki Kobayashi 1, Takushi Gotohda 1, Katsunori Tamakawa 2, Hirohisa Ueda 3 and Tadao Kakizoe 1 1 National
Changes in Breast Cancer Reports After Second Opinion. Dr. Vicente Marco Department of Pathology Hospital Quiron Barcelona. Spain
 Changes in Breast Cancer Reports After Second Opinion Dr. Vicente Marco Department of Pathology Hospital Quiron Barcelona. Spain Second Opinion in Breast Pathology Usually requested when a patient is referred
Changes in Breast Cancer Reports After Second Opinion Dr. Vicente Marco Department of Pathology Hospital Quiron Barcelona. Spain Second Opinion in Breast Pathology Usually requested when a patient is referred
The New International Staging System Lung Cancer
 The New International Staging System Lung Cancer Valerie W. Rusch, MD Chief, Thoracic Surgery Memorial Sloan-Kettering Cancer Center Chair, Lung and Esophagus Task Force, American Joint Commission on Cancer
The New International Staging System Lung Cancer Valerie W. Rusch, MD Chief, Thoracic Surgery Memorial Sloan-Kettering Cancer Center Chair, Lung and Esophagus Task Force, American Joint Commission on Cancer
Current Status and Perspectives of Radiation Therapy for Breast Cancer
 Breast Cancer Current Status and Perspectives of Radiation Therapy for Breast Cancer JMAJ 45(10): 434 439, 2002 Masahiro HIRAOKA, Masaki KOKUBO, Chikako YAMAMOTO and Michihide MITSUMORI Department of Therapeutic
Breast Cancer Current Status and Perspectives of Radiation Therapy for Breast Cancer JMAJ 45(10): 434 439, 2002 Masahiro HIRAOKA, Masaki KOKUBO, Chikako YAMAMOTO and Michihide MITSUMORI Department of Therapeutic
E L E C T R O S U R G E R G Y / W A T E R J E T S U R G E R Y. Endoscopic Submucosal Dissec tion
 E L E C T R O S U R G E R G Y / W A T E R J E T S U R G E R Y E S D W o r k s t a t i o n w i t h H y b r i d K n i f e Endoscopic Submucosal Dissec tion fast, safe and easy with the HybridKnife. introduc
E L E C T R O S U R G E R G Y / W A T E R J E T S U R G E R Y E S D W o r k s t a t i o n w i t h H y b r i d K n i f e Endoscopic Submucosal Dissec tion fast, safe and easy with the HybridKnife. introduc
Captivator II. Single-Use Snares
 Captivator II Single-Use Snares Captivator II Snares are the first line of stiff and rounded snares available in multiple sizes with both a hot and cold snaring indication. The Captivator II Snare line
Captivator II Single-Use Snares Captivator II Snares are the first line of stiff and rounded snares available in multiple sizes with both a hot and cold snaring indication. The Captivator II Snare line
OBJECTIVES By the end of this segment, the community participant will be able to:
 Cancer 101: Cancer Diagnosis and Staging Linda U. Krebs, RN, PhD, AOCN, FAAN OCEAN Native Navigators and the Cancer Continuum (NNACC) (NCMHD R24MD002811) Cancer 101: Diagnosis & Staging (Watanabe-Galloway
Cancer 101: Cancer Diagnosis and Staging Linda U. Krebs, RN, PhD, AOCN, FAAN OCEAN Native Navigators and the Cancer Continuum (NNACC) (NCMHD R24MD002811) Cancer 101: Diagnosis & Staging (Watanabe-Galloway
ENDOSCOPY IN GASTRIC CANCER: NEW IMAGING TECHNIQUES, NEW TREATMENT MODALITIES (EMR, ESD)
") ENDOSCOPY IN GASTRIC CANCER: NEW IMAGING TECHNIQUES, NEW TREATMENT MODALITIES (EMR, ESD) Fabrice Caillol Paoli Calmettes Institute, Marseille, France June 10th, Prague, Czech Republic EUS AND STAGING 1980:
ENDOSCOPY IN GASTRIC CANCER: NEW IMAGING TECHNIQUES, NEW TREATMENT MODALITIES (EMR, ESD) Fabrice Caillol Paoli Calmettes Institute, Marseille, France June 10th, Prague, Czech Republic EUS AND STAGING 1980:
GENERAL CODING. When you review old cases that were coded to unknown, make corrections based on guidelines in effect at the time of diagnosis.
 GENERAL CODING When you review old cases that were coded to unknown, make corrections based on guidelines in effect at the time of diagnosis. Exception: You must review and revise EOD coding for prostate
GENERAL CODING When you review old cases that were coded to unknown, make corrections based on guidelines in effect at the time of diagnosis. Exception: You must review and revise EOD coding for prostate
MRI in Rectal Cancer. Kartik S Jhaveri, MD,FRCPC Director, Abdominal MRI Director, CME Program
 MRI in Rectal Cancer Kartik S Jhaveri, MD,FRCPC Director, Abdominal MRI Director, CME Program DISCLOSURES No Relevant Disclosures 2 OBJECTIVES Imaging of Rectal Cancer Why MRI? MR Protocol MR Anatomy Preoperative
MRI in Rectal Cancer Kartik S Jhaveri, MD,FRCPC Director, Abdominal MRI Director, CME Program DISCLOSURES No Relevant Disclosures 2 OBJECTIVES Imaging of Rectal Cancer Why MRI? MR Protocol MR Anatomy Preoperative
The Diagnosis of Cancer in the Pathology Laboratory
 The Diagnosis of Cancer in the Pathology Laboratory Dr Edward Sheffield Christmas Select 74 Meeting, Queen s Hotel Cheltenham, 3 rd December 2014 Agenda Overview of the pathology of cancer How specimens
The Diagnosis of Cancer in the Pathology Laboratory Dr Edward Sheffield Christmas Select 74 Meeting, Queen s Hotel Cheltenham, 3 rd December 2014 Agenda Overview of the pathology of cancer How specimens
The Captivator II Snares are the first line of stiff and rounded snares available in multiple sizes with both a hot and cold snaring indication.
 Captivator II Single-Use Snares The Captivator II Snares are the first line of stiff and rounded snares available in multiple sizes with both a hot and cold snaring indication. The Captivator II Snare
Captivator II Single-Use Snares The Captivator II Snares are the first line of stiff and rounded snares available in multiple sizes with both a hot and cold snaring indication. The Captivator II Snare
Barrett s Esophagus and Endoscopic Therapy
 Barrett s Esophagus and Endoscopic Therapy John A. Dumot, DO Department of Gastroenterology Cleveland Clinic Foundation Disclosures: Research support from CSA Medical Inc. [email protected] Objectives Relationship
Barrett s Esophagus and Endoscopic Therapy John A. Dumot, DO Department of Gastroenterology Cleveland Clinic Foundation Disclosures: Research support from CSA Medical Inc. [email protected] Objectives Relationship
The Royal Marsden. Surgery for Gastric and GE Junction Cancer: primary palliative where and when? William Allum
 The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative where and when? William Allum Any surgeon can cure Surgeon - dependent No surgeon can cure EMR D2 GASTRECTOMY H N SN. WEDGE
The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative where and when? William Allum Any surgeon can cure Surgeon - dependent No surgeon can cure EMR D2 GASTRECTOMY H N SN. WEDGE
PROTOCOL OF THE RITA DATA QUALITY STUDY
 PROTOCOL OF THE RITA DATA QUALITY STUDY INTRODUCTION The RITA project is aimed at estimating the burden of rare malignant tumours in Italy using the population based cancer registries (CRs) data. One of
PROTOCOL OF THE RITA DATA QUALITY STUDY INTRODUCTION The RITA project is aimed at estimating the burden of rare malignant tumours in Italy using the population based cancer registries (CRs) data. One of
The Whipple Operation for Pancreatic Cancer: Optimism vs. Reality. Franklin Wright UCHSC Department of Surgery Grand Rounds September 11, 2006
 The Whipple Operation for Pancreatic Cancer: Optimism vs. Reality Franklin Wright UCHSC Department of Surgery Grand Rounds September 11, 2006 Overview Pancreatic ductal adenocarcinoma Pancreaticoduodenectomy
The Whipple Operation for Pancreatic Cancer: Optimism vs. Reality Franklin Wright UCHSC Department of Surgery Grand Rounds September 11, 2006 Overview Pancreatic ductal adenocarcinoma Pancreaticoduodenectomy
Photodynamic Therapy for the Treatment of Barrett s Esophagus: A Systematic Review and Economic Evaluation
 Health Technology & Policy Series; 29:1 Photodynamic Therapy for the Treatment of Barrett s Esophagus: A Systematic Review and Economic Evaluation FINAL REPORT August 29 Submitted to: The Alberta Health
Health Technology & Policy Series; 29:1 Photodynamic Therapy for the Treatment of Barrett s Esophagus: A Systematic Review and Economic Evaluation FINAL REPORT August 29 Submitted to: The Alberta Health
On Gastric Cancer. Jun Haeng Lee, M.D. Department of Medicine,Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
 On Gastric Cancer Jun Haeng Lee, M.D. Department of Medicine,Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea AGC Borrmann IV - initial endoscopic examination Fold thickening
On Gastric Cancer Jun Haeng Lee, M.D. Department of Medicine,Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea AGC Borrmann IV - initial endoscopic examination Fold thickening
New strategies in anticancer therapy
 癌 症 診 療 指 引 簡 介 及 臨 床 應 用 New strategies in anticancer therapy 中 山 醫 學 大 學 附 設 醫 院 腫 瘤 內 科 蔡 明 宏 醫 師 2014/3/29 Anti-Cancer Therapy Surgical Treatment Radiotherapy Chemotherapy Target Therapy Supportive
癌 症 診 療 指 引 簡 介 及 臨 床 應 用 New strategies in anticancer therapy 中 山 醫 學 大 學 附 設 醫 院 腫 瘤 內 科 蔡 明 宏 醫 師 2014/3/29 Anti-Cancer Therapy Surgical Treatment Radiotherapy Chemotherapy Target Therapy Supportive
Treatment and Surveillance of Non- Muscle Invasive Bladder Cancer
 Treatment and Surveillance of Non- Muscle Invasive Bladder Cancer David Josephson, MD FACS Fellowship Director, Urologic Oncology and Robotic Surgery Program Staging Most important in risk assessment and
Treatment and Surveillance of Non- Muscle Invasive Bladder Cancer David Josephson, MD FACS Fellowship Director, Urologic Oncology and Robotic Surgery Program Staging Most important in risk assessment and
CPT COD1NG UPDATES Gastroenterology CPT Advisors
 2014 CPT COD1NG UPDATES Gastroenterology CPT Advisors Joel V. Brill, MD, AGA CPT Advisor Daniel C. DeMarco, MD, ACG CPT Advisor Glenn D. Littenberg, MD, ASGE CPT Advisor The American College of Gastroenterology
2014 CPT COD1NG UPDATES Gastroenterology CPT Advisors Joel V. Brill, MD, AGA CPT Advisor Daniel C. DeMarco, MD, ACG CPT Advisor Glenn D. Littenberg, MD, ASGE CPT Advisor The American College of Gastroenterology
Pathologic Assessment Of The Breast And Axilla After Preoperative Therapy
 Pathologic Assessment Of The Breast And Axilla After Preoperative Therapy W. Fraser Symmans, M.D. Associate Professor of Pathology UT M.D. Anderson Cancer Center Pathologic Complete Response (pcr) Proof
Pathologic Assessment Of The Breast And Axilla After Preoperative Therapy W. Fraser Symmans, M.D. Associate Professor of Pathology UT M.D. Anderson Cancer Center Pathologic Complete Response (pcr) Proof
SAGES 2015 Flexible Endoscopy Course for Fellows
 Goals and Objectives: At the end of the course, the MIS fellow will be familiar with GI endoscopes, towers, and the instruments used for endoscopy and endoscopic surgery. The fellow will also be able to
Goals and Objectives: At the end of the course, the MIS fellow will be familiar with GI endoscopes, towers, and the instruments used for endoscopy and endoscopic surgery. The fellow will also be able to
Core curriculum for EMR and ablative techniques
 Communication from the ASGE Training Committee CORE CURRICULUM Core curriculum for EMR and ablative techniques This document was prepared by the American Society for Gastrointestinal Endoscopy (ASGE) Training
Communication from the ASGE Training Committee CORE CURRICULUM Core curriculum for EMR and ablative techniques This document was prepared by the American Society for Gastrointestinal Endoscopy (ASGE) Training
Esophagus Cancer. What is cancer?
 What is cancer? Esophagus Cancer The body is made up of trillions of living cells. Normal body cells grow, divide to make new cells, and die in an orderly way. During the early years of a person s life,
What is cancer? Esophagus Cancer The body is made up of trillions of living cells. Normal body cells grow, divide to make new cells, and die in an orderly way. During the early years of a person s life,
Metastatic Cervical Cancer s/p Radiation Therapy, Radical Hysterectomy and Attempted Modified Internal Hemipelvectomy
 Metastatic Cervical Cancer s/p Radiation Therapy, Radical Hysterectomy and Attempted Modified Internal Hemipelvectomy Sarah Hutto,, MSIV Marc Underhill, M.D. January 27, 2009 Past History 45 yo female
Metastatic Cervical Cancer s/p Radiation Therapy, Radical Hysterectomy and Attempted Modified Internal Hemipelvectomy Sarah Hutto,, MSIV Marc Underhill, M.D. January 27, 2009 Past History 45 yo female
Cervical Cancer The Importance of Cervical Screening and Vaccination
 Cervical Cancer The Importance of Cervical Screening and Vaccination Cancer Cells Cancer begins in cells, the building blocks that make up tissues. Tissues make up the organs of the body. Sometimes, this
Cervical Cancer The Importance of Cervical Screening and Vaccination Cancer Cells Cancer begins in cells, the building blocks that make up tissues. Tissues make up the organs of the body. Sometimes, this
LOWER GI ENDOSCOPIES So why is CMS yanking our chain? General Concepts for all GI Endoscopy Procedures
 LOWER GI ENDOSCOPIES We have lots of changes to lower GI coding for 2015 to talk about. Code definitions have been revised and many new codes have been added to this chapter. First the good news: All these
LOWER GI ENDOSCOPIES We have lots of changes to lower GI coding for 2015 to talk about. Code definitions have been revised and many new codes have been added to this chapter. First the good news: All these
This is a prospective study that analyzed the factors associated with cancer progression after
 Sample Peer-Review of a Fictitious Manuscript Reviewer A s Comments to Authors: This is a prospective study that analyzed the factors associated with cancer progression after EMR of Barrett s esophagus
Sample Peer-Review of a Fictitious Manuscript Reviewer A s Comments to Authors: This is a prospective study that analyzed the factors associated with cancer progression after EMR of Barrett s esophagus
Designed by Endoscopists, Refined by Nurses & Techs An Intuitive Endoscopic Electrosurgical Platform
 Designed by Endoscopists, Refined by Nurses & Techs An Intuitive Endoscopic Electrosurgical Platform Energizing Therapeutic Endoscopy For Over 20 Years From the 1988 introduction of Argon and through a
Designed by Endoscopists, Refined by Nurses & Techs An Intuitive Endoscopic Electrosurgical Platform Energizing Therapeutic Endoscopy For Over 20 Years From the 1988 introduction of Argon and through a
Breast Cancer: from bedside and grossing room to diagnoses and beyond. Adriana Corben, M.D.
 Breast Cancer: from bedside and grossing room to diagnoses and beyond Adriana Corben, M.D. About breast anatomy Breasts are special organs that develop in women during puberty when female hormones are
Breast Cancer: from bedside and grossing room to diagnoses and beyond Adriana Corben, M.D. About breast anatomy Breasts are special organs that develop in women during puberty when female hormones are
ORIGINAL ARTICLE: Clinical Endoscopy
 ORIGINAL ARTICLE: Clinical Endoscopy Large refractory colonic polyps: is it time to change our practice? A prospective study of the clinical and economic impact of a tertiary referral colonic mucosal resection
ORIGINAL ARTICLE: Clinical Endoscopy Large refractory colonic polyps: is it time to change our practice? A prospective study of the clinical and economic impact of a tertiary referral colonic mucosal resection
HAVE YOU BEEN NEWLY DIAGNOSED with DCIS?
 HAVE YOU BEEN NEWLY DIAGNOSED with DCIS? Jen D. Mother and volunteer. Diagnosed with DCIS breast cancer in 2012. An educational guide prepared by Genomic Health This guide is designed to educate women
HAVE YOU BEEN NEWLY DIAGNOSED with DCIS? Jen D. Mother and volunteer. Diagnosed with DCIS breast cancer in 2012. An educational guide prepared by Genomic Health This guide is designed to educate women
Avastin: Glossary of key terms
 Avastin: Glossary of key terms Adenocarcinoma Adenoma Adjuvant therapy Angiogenesis Anti-angiogenics Antibody Antigen Avastin (bevacizumab) Benign A form of carcinoma that originates in glandular tissue.
Avastin: Glossary of key terms Adenocarcinoma Adenoma Adjuvant therapy Angiogenesis Anti-angiogenics Antibody Antigen Avastin (bevacizumab) Benign A form of carcinoma that originates in glandular tissue.
Safety of Endoscopic Mucosal Resection for Barrett s Esophagus
 1440 ORIGINAL CONTRIBUTIONS nature publishing group see CMErelated editorial on page x Safety of Endoscopic Mucosal Resection for Barrett s Esophagus Yutaka Tomizawa, MD 1, Prasad G. Iyer, MD 1, Louis
1440 ORIGINAL CONTRIBUTIONS nature publishing group see CMErelated editorial on page x Safety of Endoscopic Mucosal Resection for Barrett s Esophagus Yutaka Tomizawa, MD 1, Prasad G. Iyer, MD 1, Louis
Luis D. Carcorze Soto, MD PGY-3
 Luis D. Carcorze Soto, MD PGY-3 Peritoneal Surface Malignancies Peritoneum Patient Selection Operative Technique HIPEC EPIC Primary: Primary Peritoneal Carcinoma Malignant Peritoneal Mesothelioma Metastatic:
Luis D. Carcorze Soto, MD PGY-3 Peritoneal Surface Malignancies Peritoneum Patient Selection Operative Technique HIPEC EPIC Primary: Primary Peritoneal Carcinoma Malignant Peritoneal Mesothelioma Metastatic:
A918: Prostate: adenocarcinoma
 A918: Prostate: adenocarcinoma General facts of prostate cancer The prostate is about the size of a walnut. It is just below the bladder and in front of the rectum. The tube that carries urine (the urethra)
A918: Prostate: adenocarcinoma General facts of prostate cancer The prostate is about the size of a walnut. It is just below the bladder and in front of the rectum. The tube that carries urine (the urethra)
Billing Guideline. Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/2012 Last Update Effective: 4/16
 Effective Date: 1/1/2012 Last Update Effective: 4/16") Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/2012 Last Update Effective: 4/16 Billing Guideline Background Health First administers benefit packages with full coverage
Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/2012 Last Update Effective: 4/16 Billing Guideline Background Health First administers benefit packages with full coverage
Targeted Therapy What the Surgeon Needs to Know
 Targeted Therapy What the Surgeon Needs to Know AATS Focus in Thoracic Surgery 2014 David R. Jones, M.D. Professor & Chief, Thoracic Surgery Memorial Sloan Kettering Cancer Center I have no disclosures
Targeted Therapy What the Surgeon Needs to Know AATS Focus in Thoracic Surgery 2014 David R. Jones, M.D. Professor & Chief, Thoracic Surgery Memorial Sloan Kettering Cancer Center I have no disclosures
Stomach (Gastric) Cancer. Prof. M K Mahajan ACDT & RC Bathinda
 Cancer. Prof. M K Mahajan ACDT & RC Bathinda") Stomach (Gastric) Cancer Prof. M K Mahajan ACDT & RC Bathinda Gastric Cancer Role of Radiation Layers of the Stomach Mucosa Submucosa Muscularis Serosa Stomach and Regional Lymph Nodes Stomach and Regional
Stomach (Gastric) Cancer Prof. M K Mahajan ACDT & RC Bathinda Gastric Cancer Role of Radiation Layers of the Stomach Mucosa Submucosa Muscularis Serosa Stomach and Regional Lymph Nodes Stomach and Regional