Normal and Abnormal Labor and Delivery. Valerie Swiatkowski, MD
|
|
|
- Bethanie Whitehead
- 7 years ago
- Views:
Transcription
1 Normal and Abnormal Labor and Delivery Valerie Swiatkowski, MD

2 Objectives At the end of this lecture, you will be able to: Diagnose labor and define the stages Assess a laboring patient Diagnose abnormal labor Understand the cardinal movements of labor Deliver a baby Understand complications of labor

3 What is Labor? Progressive dilation of the uterine cervix in association with repetitive contractions

4 What is Labor like? Subjectively: Regular contractions getting stronger, longer, closer together Bloody show present Sedation does not stop true labor Objectively: Cervical change occurs Descent of the presenting part

5 What is cervical change?

6 Dilation/ Effacement/Station

7 Fetal Station Williams 2001

8 Bishops Score Dilation (cm) Effacement (%) Station Consistency firm med soft Position post mid ant

9 False Labor is different! Irregular contractions No bloody show No cervical change Head may be ballotable Sedation stops false labor Cervical insufficiency (incompetence): dilation without contractions
:")
10 Taking a Labor History and Physical History: Know 4 facts (at least) (at least): Onset of contractions? Did the water break (ROM)? Vaginal bleeding? Fetal movement (FM)? PMH/ Meds? Last PO intake? Physical: Vitals CV/Pulm/Abd FHT Tocometer (ctx EFW by Leopolds Pelvic exam Fetal position and presentation FHT (fetal heart tracing) ctx tracing)

11 Assessing labor What is normal labor?

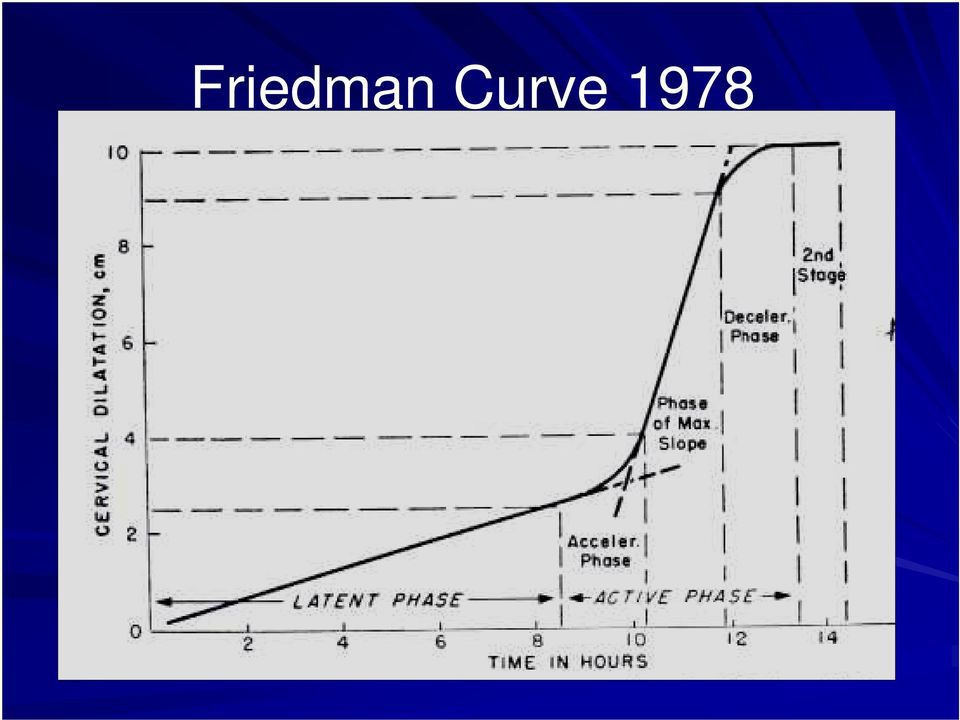
12 Stages of Labor First Stage: Second Stage: Third Stage: Fourth Stage: labor onset to complete dilation complete dilation to delivery of infant delivery of infant to delivery of placenta After delivery of the placenta latent active

13 Friedman Curve 1978
14
15

16 Assessing labor The importance of P sp Power Passage Passenger

17 POWER! Measuring contractions: Palpation: duration, frequency, intensity work intensive External Tocometer: : graphic display no info on strength of contractions Intrauterine pressure catheter (IUPC): accurate feedback in Montevideo units

18 IUPC Adequate contractions are >200 MVU in 10 minutes

19 Up to date. com The Pelvis = Passage

20 Clinical Pelvimetry Obstetrical conjugate anterior symphysis pubis posterior sacral promontory lateral linea terminalis Diagonal conjugate (clinical) inferior border of s.pubis to s.promontory Interspinous/ / Bi-ischial ischial diameter

21 Up to date. com
22 Bi-ischial Diameter
23 Calwell-Moloy Classification Pelvic Types
24 Gynecoid Pelvis Pelvic brim is a transverse ellipse (nearly a circle) Most favorable for delivery 50 percent of patients
25 Android Pelvis Pelvic brim is triangular Convergent Side Walls (widest posteriorly) Prominent ischial spines Narrow subpubic arch More common in white women
26 Anthropoid Pelvis Pelvic brim is an anteroposterior elipse Gynecoid pelvis turned 90 degrees Narrow ischial spines Much more common in black women
27 Platypelloid Pelvis Pelvic brim is transverse kidney shape Flattened gynecoid shape
28 Don t t forget about the Passenger!
29 Leopolds maneuvers 4 maneuvers to identify fetal landmarks and review feto-maternal relationships
30 Definitions Presentation - the part that lies closest to the pelvic inlet Attitude - relationship of fetal parts to each other (flexion/extension) Lie - relationship between long axis of fetus to mother Position - relationship between fetal denominator and the vertical (a/p) and horizontal (r/l) planes of the birth canal Synclitism
31 Cephalic Presentation and Attitude vertex sinciput brow face Williams 2001
32 Breech Presentation Williams 2001
33 Lie A. Longitudinal: 99% of lie B. Transverse: Associated with multiparity, placentae previa, polyhydraminos, uterine anomaly C. Oblique: Unstable Williams 2001
34 Presentation at Term 3.5% breech 96% vertex 0.3% face Position at Term 66% LOA or LOP 33% ROA or ROP
35 Position Anterior Fontanelle Posterior Fontanelle
36 OA Determining Position OP OT
37 Synclitism A. Anterior asynclitism B. Posterior asynclitism Williams 2001
38 Caput and molding
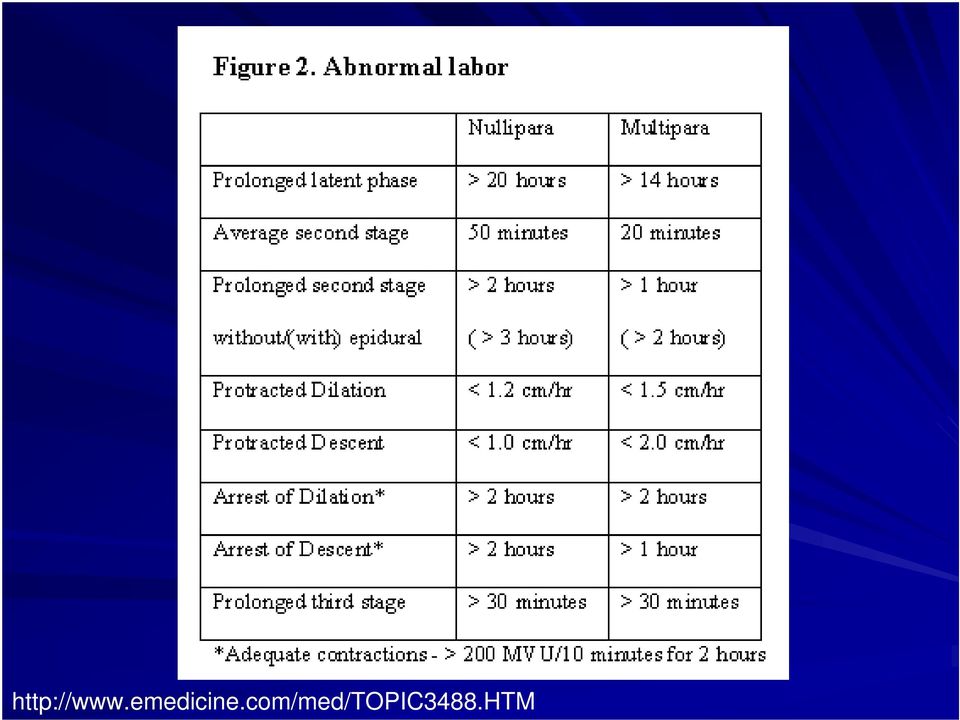
39 Abnormal Labor Prolonged latent phase Treatment: therapeutic rest 85% active, 10% false labor Protraction disorder (primary dysfunctional labor) dilation/descent occur at a slower rate Secondary arrest cessation of a previous normal dilation for 2 hours
40 Maximum Dilation: 10! Finally the Second stage of labor!
41 Cardinal Movement of Labor Engagement Descent Flexion Internal rotation Extension External rotation (restitution) Expulsion
42 Engagement descent of BPD to a level below the plane of the pelvic inlet often occurs before true labor, especially in nulliparous
43 Flexion during descent 9.5cm for vtx / 13.5 cm for brow
44 Williams 2001
45 Stage 1 Stage 2
46 Our job in the delivery room Control extension of the head Protect the perineum Check for Nuchal cord Suction mouth and nose Avoid stimulation if meconium Catch the baby! Clamp the cord
47 Delivery Complications Arrest of descent Nuchal cord Fetal distress Perineal laceration Shoulder dystocia
48 Perineal Lacerations First degree - may involve the vaginal mucosa, perineal skin Second degree - perineal muscles Third degree - external anal sphincter Fourth degree - anterior rectal wall
49 Episiotomy? Easier to repair Decrease length of second stage Decreased trauma to the perineum Increased blood loss Increased trauma
50 Shoulder Dystocia Incidence 0.2-2% 2% of deliveries (Acker 1986) Impingement of bi-acromial diameter of the fetus against the s.pubis and the s.promontory 40-50% occur with birth weight <4000g Risk factors: fetal macrosomia,, diabetes, hx shoulder dystocia,, prolonged second stage
51 Shoulder Dystocia Maternal morbidity - postpartum hemorrhage, 4th degree lacerations Neonatal morbidity - asphyxia, brachial plexus (Erb( palsy, 10-20%, 80-90% recover completely), fracture of humerus/clavicle
52 Shoulder Dystocia Maneuvers Look for turtle sign Avoid excessive traction on shoulders McRoberts: : flattens the lumbosacral curve Suprapubic pressure Ruben/Wood Screw - rotate shoulders to oblique position and pushing posterior shoulder toward fetal back Deliver posterior arm Zavanelli
53
54 Baby s s out! Now What? Stage 3: Placenta
55 Delivery of the Placenta Signs of placenta separation rise in the fundus firm, globular uterus sudden gush of blood umbilical cord lengthening Examine the placenta Delivers within minutes
56 Placenta delivery
57 Care of the Neonate Apgar Scoring System AppearancePale Blue Pink Pulse Absent <100 >100 Grimace Absent Grimace Cry Active Activity Limp Some tone Active Respiration Absent Irregular Reg & Cry
58 Conclusions You will be able to: Diagnose labor and define the stages Assess a laboring patient Diagnose abnormal labor Understand the cardinal movements of labor Deliver a baby Understand complications of labor
59 Thank you! Any questions?
Advanced ICD-10-CM/PCS Coding for OB/Pregnancy
 Advanced ICD-10-CM/PCS Coding for OB/Pregnancy October 14, 2014 Karen Feltner, RHIA, CCS Plan for Today What are we discussing today? What is different in ICD-10-CM for pregnancy? What about ICD-10-PCS
Advanced ICD-10-CM/PCS Coding for OB/Pregnancy October 14, 2014 Karen Feltner, RHIA, CCS Plan for Today What are we discussing today? What is different in ICD-10-CM for pregnancy? What about ICD-10-PCS
Obstetrical Emergencies
 Date: July 18, 2014 Page 1 of 5 Obstetrical Emergencies Purpose: To provide the process for the assessment and management of the patient with an obstetrical related emergency. Pre-Medical Control 1. Follow
Date: July 18, 2014 Page 1 of 5 Obstetrical Emergencies Purpose: To provide the process for the assessment and management of the patient with an obstetrical related emergency. Pre-Medical Control 1. Follow
Examination of the Pregnant Abdomen
 Medical students often find the examination of the pregnant abdomen daunting. This document provides a framework for you to develop a comprehensive understanding of the pregnant abdomen examination at
Medical students often find the examination of the pregnant abdomen daunting. This document provides a framework for you to develop a comprehensive understanding of the pregnant abdomen examination at
Current Claims Issues in Labor, Delivery, and Discharge
 Current Claims Issues in Labor, Delivery, and Discharge Mize Conner, JD, MD, Bellegrove, OB-GYN Current Claims Issues in Labor and Delivery and Discharge OB Emergencies Response Time VBAC Shoulder Dystocia
Current Claims Issues in Labor, Delivery, and Discharge Mize Conner, JD, MD, Bellegrove, OB-GYN Current Claims Issues in Labor and Delivery and Discharge OB Emergencies Response Time VBAC Shoulder Dystocia
ROTATIONAL POSITIONING
 ROTATIONAL POSITIONING A method for rotating posterior babies during labour Problems associated with persistent posterior positioning Prolonged labour 12% for posterior vs. 1.7% Assisted delivery 24.6%
ROTATIONAL POSITIONING A method for rotating posterior babies during labour Problems associated with persistent posterior positioning Prolonged labour 12% for posterior vs. 1.7% Assisted delivery 24.6%
Chapter 17 Preparing for labour July 4th 2011
 Chapter 17 Preparing for labour July 4th 2011 The goats have no midwives, The sheep have no midwives, When the goat is pregnant she is safely delivered, When the sheep is pregnant, she is safely delivered,
Chapter 17 Preparing for labour July 4th 2011 The goats have no midwives, The sheep have no midwives, When the goat is pregnant she is safely delivered, When the sheep is pregnant, she is safely delivered,
Assessment of Fetal Well-Being
 Assessment of Fetal Well-Being Assessment of Fetal Well-Being Fetal Heart Rate (FHR) Fetal Movement- Kick Count Electronic Fetal Monitoring Fetal EKG Biparietal diameter (BPD] Biophysical Profile Fetal
Assessment of Fetal Well-Being Assessment of Fetal Well-Being Fetal Heart Rate (FHR) Fetal Movement- Kick Count Electronic Fetal Monitoring Fetal EKG Biparietal diameter (BPD] Biophysical Profile Fetal
THE ASSOCIATION BETWEEN FETAL POSITION AT THE ONSET OF LABOUR AND BIRTH OUTCOMES. Aishah Ahmad (Nee Bibi)
") THE ASSOCIATION BETWEEN FETAL POSITION AT THE ONSET OF LABOUR AND BIRTH OUTCOMES by Aishah Ahmad (Nee Bibi) A thesis submitted to: The University of Birmingham For the degree of DOCTOR OF PHILOSOPHY Department
THE ASSOCIATION BETWEEN FETAL POSITION AT THE ONSET OF LABOUR AND BIRTH OUTCOMES by Aishah Ahmad (Nee Bibi) A thesis submitted to: The University of Birmingham For the degree of DOCTOR OF PHILOSOPHY Department
Labor is work, and it is hard work. Labor is an end to pregnancy and a beginning for a new human life in a newly shaped family."
 LABOR AND DELIVERY "The way we give birth to our young is that the muscular organ (the uterus) in which the offspring has been nurtured for nine months begins to contract. The contractions work to open
LABOR AND DELIVERY "The way we give birth to our young is that the muscular organ (the uterus) in which the offspring has been nurtured for nine months begins to contract. The contractions work to open
and mechanism of labour
 Pelvic and fetal cranial anatomy Chapter1 and mechanism of labour Louay S. Louis and Richard Warren Introduction Labour is the series of events whereby the contents of the gravid uterus, the fetus, amniotic
Pelvic and fetal cranial anatomy Chapter1 and mechanism of labour Louay S. Louis and Richard Warren Introduction Labour is the series of events whereby the contents of the gravid uterus, the fetus, amniotic
Guide to Pregnancy and Birth Injury Claims
 Being pregnant, especially for the first time can be a very daunting experience where you often have to put all of your faith in your midwife or doctor. The majority of pregnancies and births occur without
Being pregnant, especially for the first time can be a very daunting experience where you often have to put all of your faith in your midwife or doctor. The majority of pregnancies and births occur without
Registered Nurse Initiated Activities Decision Support Tool No. 8A: Obstetrical Emergencies Cord Prolapse
 Registered Nurse Initiated Activities Decision Support Tool No. 8A: Obstetrical Emergencies Cord Prolapse Decision support tools are evidenced-based documents used to guide the assessment, diagnosis and
Registered Nurse Initiated Activities Decision Support Tool No. 8A: Obstetrical Emergencies Cord Prolapse Decision support tools are evidenced-based documents used to guide the assessment, diagnosis and
COMPLICATIONS OF PREGNANCY, CHILDBIRTH AND THE PUERPERIUM
 COMPLICATIONS OF PREGNANCY, CHILDBIRTH AND THE PUERPERIUM PREGNANCY WITH ABORTIVE OUTCOME (630 639.9) 630 HYDATIDIFORM MOLE 631 OTHER ABNORMAL PRODUCT OF CONCEPTION 632 MISSED ABORTION 633 ECTOPIC PREGNANCY
COMPLICATIONS OF PREGNANCY, CHILDBIRTH AND THE PUERPERIUM PREGNANCY WITH ABORTIVE OUTCOME (630 639.9) 630 HYDATIDIFORM MOLE 631 OTHER ABNORMAL PRODUCT OF CONCEPTION 632 MISSED ABORTION 633 ECTOPIC PREGNANCY
Diagnosis Codes for Pregnancy and Complications of Pregnancy
 This list is for informational purposes only and is not a binding or definitive list of covered conditions. It is not a guarantee of coverage; coverage depends on the available benefits and eligibility
This list is for informational purposes only and is not a binding or definitive list of covered conditions. It is not a guarantee of coverage; coverage depends on the available benefits and eligibility
Guideline for the Use of Oxytocin December 2012
 The following guidelines are intended only as a general educational resource for hospitals and clinicians, and are not intended to reflect or establish a standard of care or to replace individual clinician
The following guidelines are intended only as a general educational resource for hospitals and clinicians, and are not intended to reflect or establish a standard of care or to replace individual clinician
Neonatal Emergencies. Care of the Neonate. Care of the Neonate. Care of the Neonate. Student Objectives. Student Objectives continued.
 Student Objectives Neonatal Emergencies After completing this section the student will be able to: 1. Identify three physiologic and/or anatomic features unique to the newborn 2. List three perinatal factors
Student Objectives Neonatal Emergencies After completing this section the student will be able to: 1. Identify three physiologic and/or anatomic features unique to the newborn 2. List three perinatal factors
Renown Regional Medical Center Department Of Obstetrics and Gynecology. Policies and Procedures Certified Nurse Midwives ( CNM S)
") 1. Overview: Department Of Obstetrics and Gynecology Policies and Procedures Certified Nurse Midwives ( CNM S) supports the practice of Nurse Midwifery and will participate with Certified Nurse Midwives
1. Overview: Department Of Obstetrics and Gynecology Policies and Procedures Certified Nurse Midwives ( CNM S) supports the practice of Nurse Midwifery and will participate with Certified Nurse Midwives
Maternity Care Primary C-Section Rate Specifications 2014 (07/01/2013 to 06/30/2014 Dates of Service)
") Summary of Changes Denominator Changes: Two additions were made to the denominator criteria. The denominator was changed to include patients who had: a vertex position delivery AND a term pregnancy of
Summary of Changes Denominator Changes: Two additions were made to the denominator criteria. The denominator was changed to include patients who had: a vertex position delivery AND a term pregnancy of
Pelvic Anatomy. Robert E. Gutman, MD
 Pelvic Anatomy Robert E. Gutman, MD Objectives Understand pelvic anatomy Organs and structures of the female pelvis Vascular Supply Neurologic supply Pelvic and retroperitoneal contents and spaces Bony
Pelvic Anatomy Robert E. Gutman, MD Objectives Understand pelvic anatomy Organs and structures of the female pelvis Vascular Supply Neurologic supply Pelvic and retroperitoneal contents and spaces Bony
Home Health Agencies. Ante & Postpartum Members
 FIRST PRIORITY HEALTH /FIRST PRIORITY LIFE INSURANCE COMPANY BLUE CROSS OF NORTHEASTERN PENNSYLVANIA CREDENTIALING CRITERIA FOR OBSTETRIC NURSES IN HOME CARE ADMINISTRATIVE PRACTICE GUIDELINE PROVIDER
FIRST PRIORITY HEALTH /FIRST PRIORITY LIFE INSURANCE COMPANY BLUE CROSS OF NORTHEASTERN PENNSYLVANIA CREDENTIALING CRITERIA FOR OBSTETRIC NURSES IN HOME CARE ADMINISTRATIVE PRACTICE GUIDELINE PROVIDER
Shoulder dystocia is one of the
 ALSO SERIES Shoulder Dystocia ELIZABETH G. BAXLEY, M.D., University of South Carolina School of Medicine, Columbia, South Carolina ROBERT W. GOBBO, M.D., University of California at Davis Family Practice
ALSO SERIES Shoulder Dystocia ELIZABETH G. BAXLEY, M.D., University of South Carolina School of Medicine, Columbia, South Carolina ROBERT W. GOBBO, M.D., University of California at Davis Family Practice
Fetal Acid Base Status and Umbilical Cord Sampling. David Acker, MD
 Fetal Acid Base Status and Umbilical Cord Sampling David Acker, MD Part I: Some Background Intra-uterine Event as Causative of CP Cord ph < 7.00 and base excess of > 12 Early onset neonatal encephalopathy
Fetal Acid Base Status and Umbilical Cord Sampling David Acker, MD Part I: Some Background Intra-uterine Event as Causative of CP Cord ph < 7.00 and base excess of > 12 Early onset neonatal encephalopathy
Practical Nursing Series: Maternal Newborn Nursing
 This free sample provided by CIMC www. 800.654.4502 Practical Nursing Series: Maternal Newborn Nursing Maternal Newborn Nursing adheres to the revised objectives approved by the Oklahoma Board of Nursing.
This free sample provided by CIMC www. 800.654.4502 Practical Nursing Series: Maternal Newborn Nursing Maternal Newborn Nursing adheres to the revised objectives approved by the Oklahoma Board of Nursing.
What Every Pregnant Woman Needs to Know About Cesarean Section. Be informed. Know your rights. Protect yourself. Protect your baby.
 Be informed. Know your rights. Protect yourself. Protect your baby. What Every Pregnant Woman Needs to Know About Cesarean Section 2012 Childbirth Connection If you re expecting a baby, there s a good
Be informed. Know your rights. Protect yourself. Protect your baby. What Every Pregnant Woman Needs to Know About Cesarean Section 2012 Childbirth Connection If you re expecting a baby, there s a good
Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: OB/GYN Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: OB/GYN Revised: 11/2013 A&P Vagina - known as birth canal. Cervix - head of vagina. Fallopian tubes
Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: OB/GYN Revised: 11/2013 A&P Vagina - known as birth canal. Cervix - head of vagina. Fallopian tubes
General and Objectives Clinical Skills for. Nursing Students in Maternity and Gynecology. Nursing Department
 General and Objectives Clinical Skills for Nursing Students in Maternity and Gynecology Nursing Department Objectives and clinical skills of Antenatal unit Provide antenatal care to woman during normal
General and Objectives Clinical Skills for Nursing Students in Maternity and Gynecology Nursing Department Objectives and clinical skills of Antenatal unit Provide antenatal care to woman during normal
Doppler Ultrasound in the Management of Fetal Growth Restriction Chukwuma I. Onyeije, M.D. Atlanta Perinatal Associates
 Doppler Ultrasound in the Management of Fetal Growth Restriction Chukwuma I. Onyeije, M.D. Atlanta Perinatal Associates 1 For your convenience a copy of this lecture is available for review and download
Doppler Ultrasound in the Management of Fetal Growth Restriction Chukwuma I. Onyeije, M.D. Atlanta Perinatal Associates 1 For your convenience a copy of this lecture is available for review and download
Newborn outcomes after cesarean section for fetal distress in BC
 Newborn outcomes after cesarean section for fetal distress in BC Patricia Janssen, PhD, UBC School of Population and Public Health Scientist, Child and Family Research Institute Kevin Jenniskens, MSc,
Newborn outcomes after cesarean section for fetal distress in BC Patricia Janssen, PhD, UBC School of Population and Public Health Scientist, Child and Family Research Institute Kevin Jenniskens, MSc,
Water Birth Online Course. Women s Services
 Water Birth Online Course Women s Services 1 Water Birth Instructions for Online Class 1. Read through all the slides. 2. Print out the certificate at the end of the slides. 3. Sign and date the certificate.
Water Birth Online Course Women s Services 1 Water Birth Instructions for Online Class 1. Read through all the slides. 2. Print out the certificate at the end of the slides. 3. Sign and date the certificate.
CBT521-EMT11- OB/GYN Emergencies
 Seattle-King County EMS Seattle-King County Emergency Medical Services Division Public Health - Seattle/King County 401 5 th Avenue, Suite 1200 Seattle, WA 98104 (206) 296-4863 January 2011 CBT521-EMT11-
Seattle-King County EMS Seattle-King County Emergency Medical Services Division Public Health - Seattle/King County 401 5 th Avenue, Suite 1200 Seattle, WA 98104 (206) 296-4863 January 2011 CBT521-EMT11-
To outline nursing management of patients receiving epidural anesthesia during labor (Includes walking epidurals and combined spinal-epidurals).
.") HOSPITAL NAME INSTITUTIONAL POLICY AND PROCEDURE (IPP) Department: Manual: Section: TITLE/DESCRIPTION POLICY NUMBER LABOR: EPIDURAL EFFECTIVE DATE REVIEW DUE REPLACES NUMBER NO. OF PAGES APPROVED BY APPLIES
HOSPITAL NAME INSTITUTIONAL POLICY AND PROCEDURE (IPP) Department: Manual: Section: TITLE/DESCRIPTION POLICY NUMBER LABOR: EPIDURAL EFFECTIVE DATE REVIEW DUE REPLACES NUMBER NO. OF PAGES APPROVED BY APPLIES
To provide safe and standardized nursing care for the patient requiring induction or augmentation of labor.
 Policy: Guidelines for the Management of Patients Undergoing Induction or Labor & Delivery Effective Date May 2012 Approval Date May 2012 Supersedes September 2011 Applicable to VUH Children s Hospital
Policy: Guidelines for the Management of Patients Undergoing Induction or Labor & Delivery Effective Date May 2012 Approval Date May 2012 Supersedes September 2011 Applicable to VUH Children s Hospital
LESSON ASSIGNMENT. Normal and Emergency Childbirth. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 2 Normal and Emergency Childbirth. LESSON ASSIGNMENT Paragraphs 2-1 through 2-25. LESSON OBJECTIVES After completing this lesson, you should be able to: 2-1. Define common terms
LESSON ASSIGNMENT LESSON 2 Normal and Emergency Childbirth. LESSON ASSIGNMENT Paragraphs 2-1 through 2-25. LESSON OBJECTIVES After completing this lesson, you should be able to: 2-1. Define common terms
Assessment of Fetal Growth
 Assessment of Fetal Growth Unit / Trust: 1. INTRODUCTION The aim of this guideline template is to outline the methods used to assess fetal growth and the referral pathways utilising customised antenatal
Assessment of Fetal Growth Unit / Trust: 1. INTRODUCTION The aim of this guideline template is to outline the methods used to assess fetal growth and the referral pathways utilising customised antenatal
Normal Pregnancy and Pain Management Case Study
 Normal Pregnancy and Pain Management Case Study Time: 1845 Heather Morris, RN, has just arrived to work her evening shift in Labor & Delivery. This is her 5th year as an RN in the unit. While waiting for
Normal Pregnancy and Pain Management Case Study Time: 1845 Heather Morris, RN, has just arrived to work her evening shift in Labor & Delivery. This is her 5th year as an RN in the unit. While waiting for
This policy outlines the nursing care and management of the labor patient.
 Policy: Nursing Management of the Labor Patient Chapter Labor & Delivery Effective Date December 2012 Approval Date December 2012 Supersedes September 2012 Applicable to VUH Children s Hospital VMG VMG
Policy: Nursing Management of the Labor Patient Chapter Labor & Delivery Effective Date December 2012 Approval Date December 2012 Supersedes September 2012 Applicable to VUH Children s Hospital VMG VMG
Caesarean section and quality of obstetric care
 Caesarean section and quality of obstetric care Gjennombruddsprosjekt for keisersnitt September 2014 Michael Robson The National Maternity Hospital Dublin, Ireland Mrobson@nmh.ie Gjennombruddsprosjekt
Caesarean section and quality of obstetric care Gjennombruddsprosjekt for keisersnitt September 2014 Michael Robson The National Maternity Hospital Dublin, Ireland Mrobson@nmh.ie Gjennombruddsprosjekt
Why is prematurity a concern?
 Prematurity What is prematurity? A baby born before 37 weeks of pregnancy is considered premature. Approximately 12% of all babies are born prematurely. Terms that refer to premature babies are preterm
Prematurity What is prematurity? A baby born before 37 weeks of pregnancy is considered premature. Approximately 12% of all babies are born prematurely. Terms that refer to premature babies are preterm
KENTUCKY BOARD OF NURSING 312 Whittington Parkway, Suite 300 Louisville, Kentucky 40222-5172 http://kbn.ky.gov ADVISORY OPINION STATEMENT
 (Revised 4/2016) KENTUCKY BOARD OF NURSING 312 Whittington Parkway, Suite 300 Louisville, Kentucky 40222-5172 http://kbn.ky.gov ADVISORY OPINION STATEMENT ROLES OF NURSES IN THE CARE OF PRENATAL AND INTRAPARTUM
(Revised 4/2016) KENTUCKY BOARD OF NURSING 312 Whittington Parkway, Suite 300 Louisville, Kentucky 40222-5172 http://kbn.ky.gov ADVISORY OPINION STATEMENT ROLES OF NURSES IN THE CARE OF PRENATAL AND INTRAPARTUM
Birth Injury Exploring Legal Options. By Patrick Malone
 Birth Injury Exploring Legal Options The joyous process of childbirth occasionally ends in tragedy: a serious injury to the baby, or even death of mother or child. Children who suffer injuries during or
Birth Injury Exploring Legal Options The joyous process of childbirth occasionally ends in tragedy: a serious injury to the baby, or even death of mother or child. Children who suffer injuries during or
How To Choose Between A Vaginal Birth Or A Cesarean Section
 Be informed. Know your rights. Protect yourself. Protect your baby. What Every Pregnant Woman Needs to Know About Cesarean Section 2012 Childbirth Connection If you re expecting a baby, there s a good
Be informed. Know your rights. Protect yourself. Protect your baby. What Every Pregnant Woman Needs to Know About Cesarean Section 2012 Childbirth Connection If you re expecting a baby, there s a good
Fairview Health Services CERTIFIED NURSE MIDWIFE Delineation of Privileges CROSSWALK FOR REQUESTING FAIRVIEW PRIVILEGES
 PAGE 1 OF 4 Fairview Health Services CERTIFIED NURSE MIDWIFE Delineation of Privileges Applicant s Name (please print): CROSSWALK FOR REQUESTING FAIRVIEW PRIVILEGES I Want to Work at the Following Fairview
PAGE 1 OF 4 Fairview Health Services CERTIFIED NURSE MIDWIFE Delineation of Privileges Applicant s Name (please print): CROSSWALK FOR REQUESTING FAIRVIEW PRIVILEGES I Want to Work at the Following Fairview
Certified Professional Midwives Caring for Mothers and Babies in Virginia
 Certified Professional Midwives Caring for Mothers and Babies in Virginia Commonwealth Midwives Alliance Certified Professional Midwives in VA Licensed by the BOM since January 2006 5 member Midwifery
Certified Professional Midwives Caring for Mothers and Babies in Virginia Commonwealth Midwives Alliance Certified Professional Midwives in VA Licensed by the BOM since January 2006 5 member Midwifery
Maj Alison Baum. R3, Nellis FMR
 Maj Alison Baum R3, Nellis FMR What are some of your thoughts about birth plans? http://www.youtube.com/watch?v=hh62v0c xf04 Labor: Pain management wishes Doulas Episiotomy Intermittent fetal monitoring
Maj Alison Baum R3, Nellis FMR What are some of your thoughts about birth plans? http://www.youtube.com/watch?v=hh62v0c xf04 Labor: Pain management wishes Doulas Episiotomy Intermittent fetal monitoring
AHA/AAP Neonatal Resuscitation Guidelines 2010: Summary of Major Changes and Comment on its Utility in Resource-Limited Settings
 AHA/AAP Neonatal Resuscitation Guidelines 2010: Summary of Major Changes and Comment on its Utility in Resource-Limited Settings Resuscitation step Recommendations (2005) Recommendations (2010) Comments/LOE
AHA/AAP Neonatal Resuscitation Guidelines 2010: Summary of Major Changes and Comment on its Utility in Resource-Limited Settings Resuscitation step Recommendations (2005) Recommendations (2010) Comments/LOE
Patient information on soft markers
 Patient information on soft markers Before you read this section remember the following important points. The vast majority of babies with soft markers are normal. Soft markers are frequently seen in healthy
Patient information on soft markers Before you read this section remember the following important points. The vast majority of babies with soft markers are normal. Soft markers are frequently seen in healthy
Cord Blood Erythropoietin and Markers of Fetal Hypoxia
 July 21, 2011 By NeedsFixing [1] To investigating the relationship between cord blood erythropoietin and clinical markers of fetal hypoxia. Abstract Objective: To investigating the relationship between
July 21, 2011 By NeedsFixing [1] To investigating the relationship between cord blood erythropoietin and clinical markers of fetal hypoxia. Abstract Objective: To investigating the relationship between
Lectures of Human Anatomy
 Lectures of Human Anatomy Vertebral Column-I By DR. ABDEL-MONEM AWAD HEGAZY M.B. with honor 1983, Dipl."Gynecology and Obstetrics "1989, Master "Anatomy and Embryology" 1994, M.D. "Anatomy and Embryology"
Lectures of Human Anatomy Vertebral Column-I By DR. ABDEL-MONEM AWAD HEGAZY M.B. with honor 1983, Dipl."Gynecology and Obstetrics "1989, Master "Anatomy and Embryology" 1994, M.D. "Anatomy and Embryology"
A 28 year old woman, gravida 2, para 1, at 16 weeks gestation informs you that her cat, which she has owned for several years, has toxoplasmosis, as
 A 28 year old woman, gravida 2, para 1, at 16 weeks gestation informs you that her cat, which she has owned for several years, has toxoplasmosis, as diagnosed from a stool sample. She is concerned about
A 28 year old woman, gravida 2, para 1, at 16 weeks gestation informs you that her cat, which she has owned for several years, has toxoplasmosis, as diagnosed from a stool sample. She is concerned about
C. P. Noel McCarthy, MD 1936 1936--2009 2009 Risk Reduction Strategies in Risk Obstetrics & Gynecology
 C. P. Noel McCarthy, MD 1936-2009 Risk Reduction Strategies in Obstetrics & Gynecology John F. Rodis, MD Professor of Clinical Obstetrics & Gynecology Columbia University College of Physicians & Surgeons
C. P. Noel McCarthy, MD 1936-2009 Risk Reduction Strategies in Obstetrics & Gynecology John F. Rodis, MD Professor of Clinical Obstetrics & Gynecology Columbia University College of Physicians & Surgeons
Human Anatomy & Physiology
 PowerPoint Lecture Slides prepared by Barbara Heard, Atlantic Cape Community College Ninth Edition Human Anatomy & Physiology C H A P T E R 7 The Skeleton: Part B Annie Leibovitz/Contact Press Images Vertebral
PowerPoint Lecture Slides prepared by Barbara Heard, Atlantic Cape Community College Ninth Edition Human Anatomy & Physiology C H A P T E R 7 The Skeleton: Part B Annie Leibovitz/Contact Press Images Vertebral
Vanderbilt University Medical Center Policy Manual
 Key Words: OB, Obstetric, L&D, Labor and Delivery, Triage Applicable to VUH Children s VMG VMG Off-site locations VPH VUSN VUSM Sandra Smith, RN Manager, Labor and Delivery Approved by Robin Mutz, RNC,
Key Words: OB, Obstetric, L&D, Labor and Delivery, Triage Applicable to VUH Children s VMG VMG Off-site locations VPH VUSN VUSM Sandra Smith, RN Manager, Labor and Delivery Approved by Robin Mutz, RNC,
Fetal Blood Sampling Guideline
 This is an official Northern Trust policy and should not be edited in any way Fetal Blood Sampling Guideline Reference Number: NHSCT/11/423 Target audience: This policy is directed to all obstetricians
This is an official Northern Trust policy and should not be edited in any way Fetal Blood Sampling Guideline Reference Number: NHSCT/11/423 Target audience: This policy is directed to all obstetricians
Implementing Maternity Bundled Payment To Reduce Low-risk First-birth Cesarean Births: A Multi-Stakeholder Initiative
 Implementing Maternity Bundled Payment To Reduce Low-risk First-birth Cesarean Births: A Multi-Stakeholder Initiative Elliott Main MD, CMQCC Brynn Rubinstein, PBGH Agenda 1. Pilot Overview (Brynn) 2. Quality
Implementing Maternity Bundled Payment To Reduce Low-risk First-birth Cesarean Births: A Multi-Stakeholder Initiative Elliott Main MD, CMQCC Brynn Rubinstein, PBGH Agenda 1. Pilot Overview (Brynn) 2. Quality
Obstetrical Hemorrhage and Obstetric Laceration Workgroup
 Obstetrical Hemorrhage and Obstetric Laceration Workgroup Purpose To develop standard clinical definitions on select diagnoses & categories to be used consistently across all hospitals in Maryland Definitions
Obstetrical Hemorrhage and Obstetric Laceration Workgroup Purpose To develop standard clinical definitions on select diagnoses & categories to be used consistently across all hospitals in Maryland Definitions
Medical Negligence. Standard of Care 2/25/2014. Medico Legal Risk Reduction in Obstetrics
 Medico Legal Risk Reduction in Obstetrics James E. Looper, Jr. Hall Booth Smith, PC JLooper@hallboothsmith.com 615 313 9911 Medical Negligence To prevail on a medical-malpractice claim, a plaintiff must
Medico Legal Risk Reduction in Obstetrics James E. Looper, Jr. Hall Booth Smith, PC JLooper@hallboothsmith.com 615 313 9911 Medical Negligence To prevail on a medical-malpractice claim, a plaintiff must
Women's Circle Nurse-Midwife Services Inc. Angela Kreider CNM, MSN 1003 Plumas Street Yuba City, CA 95991 (530)751-2273 FAX (530)751-2274
751-2273 FAX (530)751-2274") Women's Circle Nurse-Midwife Services Inc. Angela Kreider CNM, MSN 1003 Plumas Street Yuba City, CA 95991 (530)751-2273 FAX (530)751-2274 Informed Disclosure and Consent The following consent explains
Women's Circle Nurse-Midwife Services Inc. Angela Kreider CNM, MSN 1003 Plumas Street Yuba City, CA 95991 (530)751-2273 FAX (530)751-2274 Informed Disclosure and Consent The following consent explains
Normal Child Birth- How to assist in delivery of a newborn. By: Louis Durkin MD. Objectives:
 Normal Child Birth- How to assist in delivery of a newborn. By: Louis Durkin MD Objectives: 1. Describe the evaluation of the pregnant patient. 2. Recognize signs and symptoms of imminent delivery. 3.
Normal Child Birth- How to assist in delivery of a newborn. By: Louis Durkin MD Objectives: 1. Describe the evaluation of the pregnant patient. 2. Recognize signs and symptoms of imminent delivery. 3.
THE SUPREME COURT OF APPEAL OF SOUTH AFRICA JUDGMENT. Mrs Nondumiso Sindiswe Sibisi NO
 THE SUPREME COURT OF APPEAL OF SOUTH AFRICA JUDGMENT Reportable Case No: 311/2013 In the matter between: Mrs Nondumiso Sindiswe Sibisi NO Appellant and Dr D P Maitin Respondent Neutral Citation: Sibisi
THE SUPREME COURT OF APPEAL OF SOUTH AFRICA JUDGMENT Reportable Case No: 311/2013 In the matter between: Mrs Nondumiso Sindiswe Sibisi NO Appellant and Dr D P Maitin Respondent Neutral Citation: Sibisi
Chapter 31 Obstetrics and Neonatal Care 1137. Scene Size-up. Primary Assessment
 Chapter 31 Obstetrics and Neonatal Care 1137 Scene Size-up Scene Safety Mechanism of Injury (MOI)/ Nature of Illness (NOI) Ensure scene safety and safe access to the patient. Standard precautions should
Chapter 31 Obstetrics and Neonatal Care 1137 Scene Size-up Scene Safety Mechanism of Injury (MOI)/ Nature of Illness (NOI) Ensure scene safety and safe access to the patient. Standard precautions should
Beverly E Hashimoto, M.D. Virginia Mason Medical Center, Seattle, WA
 Pelvic Floor Relaxation Beverly E Hashimoto, M.D. Virginia Mason Medical Center, Seattle, WA Disclosures Beverly Hashimoto: GE Medical Systems: research support and consultant (all fees given to Virginia
Pelvic Floor Relaxation Beverly E Hashimoto, M.D. Virginia Mason Medical Center, Seattle, WA Disclosures Beverly Hashimoto: GE Medical Systems: research support and consultant (all fees given to Virginia
Giving birth in Bronovo. Welcome! Presentatie Verloskunde en Gynaecologie
 Giving birth in Bronovo Welcome! Welcome to Bronovo Content of presentation Preparation The birth When it doesn't go to plan Pain relief Practical information Preparation Medical care from the midwife
Giving birth in Bronovo Welcome! Welcome to Bronovo Content of presentation Preparation The birth When it doesn't go to plan Pain relief Practical information Preparation Medical care from the midwife
Refer to Specialist. The Diagnosis and Management of Shoulder Pain 1. SLAP lesions, types 1 through 4
 The Diagnosis Management of Shoulder Pain 1 Significant Hisry -Age -Extremity Dominance -Hisry of trauma, dislocation, subluxation -Weakness, numbness, paresthesias -Sports participation -Past medical
The Diagnosis Management of Shoulder Pain 1 Significant Hisry -Age -Extremity Dominance -Hisry of trauma, dislocation, subluxation -Weakness, numbness, paresthesias -Sports participation -Past medical
Cerebral Palsy. 1995-2014, The Patient Education Institute, Inc. www.x-plain.com nr200105 Last reviewed: 06/17/2014 1
 Cerebral Palsy Introduction Cerebral palsy, or CP, can cause serious neurological symptoms in children. Thousands of children are diagnosed with cerebral palsy every year. This reference summary explains
Cerebral Palsy Introduction Cerebral palsy, or CP, can cause serious neurological symptoms in children. Thousands of children are diagnosed with cerebral palsy every year. This reference summary explains
Registered Midwife Clinical Privileges REAPPOINTMENT 2015-2016 Effective from July 1, 2015 to June 30, 2016
 Name: Initial privileges (initial appointment) Renewal of privileges (reappointment) All new applicants must meet the following requirements as approved by the governing body, effective: 04/Jun/2013. Applicant:
Name: Initial privileges (initial appointment) Renewal of privileges (reappointment) All new applicants must meet the following requirements as approved by the governing body, effective: 04/Jun/2013. Applicant:
Kathryn DeVault, RHIA, CCS, CCS-P Director, HIM Solutions, AHIMA
 ICD-10-CM: Let s Code, Part II Kathryn DeVault, RHIA, CCS, CCS-P Director, HIM Solutions, AHIMA Agenda Coding questions answered Review of ICD-10-CM coding scenarios ICD-10-CM Coding Questions Coding Questions...
ICD-10-CM: Let s Code, Part II Kathryn DeVault, RHIA, CCS, CCS-P Director, HIM Solutions, AHIMA Agenda Coding questions answered Review of ICD-10-CM coding scenarios ICD-10-CM Coding Questions Coding Questions...
Inpatient Obstetric Nursing
 NCC believes the individual certified nurse is the best person to determine the specialty code for their CE, as they have the specific content of the CE program. Inpatient Obstetric Nursing NCC Maintenance
NCC believes the individual certified nurse is the best person to determine the specialty code for their CE, as they have the specific content of the CE program. Inpatient Obstetric Nursing NCC Maintenance
Cerebral Palsy. In order to function, the brain needs a continuous supply of oxygen.
 Cerebral Palsy Introduction Cerebral palsy, or CP, can cause serious neurological symptoms in children. Up to 5000 children in the United States are diagnosed with cerebral palsy every year. This reference
Cerebral Palsy Introduction Cerebral palsy, or CP, can cause serious neurological symptoms in children. Up to 5000 children in the United States are diagnosed with cerebral palsy every year. This reference
Breakout 2 - OMT for the Lumbar Spine and Sacrum Gretta A. Gross, DO
 Breakout 2 - OMT for the Lumbar Spine and Sacrum Gretta A. Gross, DO Osteopathic Diagnosis and Treatment of the Lumbar Spine and Sacrum Gretta A. Gross, DO, MMedEd, FACOFP DOME/PD Houston Healthcare Family
Breakout 2 - OMT for the Lumbar Spine and Sacrum Gretta A. Gross, DO Osteopathic Diagnosis and Treatment of the Lumbar Spine and Sacrum Gretta A. Gross, DO, MMedEd, FACOFP DOME/PD Houston Healthcare Family
IDPH ESF-8 Plan: Pediatric and Neonatal Surge Annex Obstetrical Care Guidelines 2015
 Purpose: To provide guidance to practitioners caring for pregnant women and newborn patients during a disaster Disclaimer: This guideline are not meant to be all inclusive, replace an existing policy and
Purpose: To provide guidance to practitioners caring for pregnant women and newborn patients during a disaster Disclaimer: This guideline are not meant to be all inclusive, replace an existing policy and
Birth injury. Amy J. Gagnon, M.D. Maternal-Fetal Medicine. Colorado Perinatal Care Council November 18, 2011
 Birth injury Amy J. Gagnon, M.D. Maternal-Fetal Medicine Colorado Perinatal Care Council November 18, 2011 Birth injury: overview Cephalohematoma Subgaleal hemorrhage Retinal hemorrhage Facial nerve palsy
Birth injury Amy J. Gagnon, M.D. Maternal-Fetal Medicine Colorado Perinatal Care Council November 18, 2011 Birth injury: overview Cephalohematoma Subgaleal hemorrhage Retinal hemorrhage Facial nerve palsy
How To Test For Fetal Blood
 Fetal (FBS) / paired cord blood sampling guideline (GL839) Approval Approval Group Job Title, Chair of Committee Date Maternity & Children s Services Clinical Governance Committee Mr Mark Selinger, Consultant
Fetal (FBS) / paired cord blood sampling guideline (GL839) Approval Approval Group Job Title, Chair of Committee Date Maternity & Children s Services Clinical Governance Committee Mr Mark Selinger, Consultant
Applications of Doppler Ultrasound in Fetal Growth Assessment. David Cole
 Applications of Doppler Ultrasound in Fetal Growth Assessment David Cole Aims The aim of this presentation is to consider the use of Doppler ultrasound to investigate and monitor those pregnancies at risk
Applications of Doppler Ultrasound in Fetal Growth Assessment David Cole Aims The aim of this presentation is to consider the use of Doppler ultrasound to investigate and monitor those pregnancies at risk
How To Treat A Pregnant Woman With A Miscarriage
 Special Patient Populations Obstetrics EMR Education Standard Recognizes and manages life threats based on simple assessment findings for a patient with special needs while awaiting additional emergency
Special Patient Populations Obstetrics EMR Education Standard Recognizes and manages life threats based on simple assessment findings for a patient with special needs while awaiting additional emergency
Chapter 14. Board of Certified Direct-Entry Midwives.
 Chapter 14. Board of Certified Direct-Entry Midwives. (Words in boldface and underlined indicate language being added; words [CAPITALIZED AND BRACKETED] indicate language being deleted. Complete new sections
Chapter 14. Board of Certified Direct-Entry Midwives. (Words in boldface and underlined indicate language being added; words [CAPITALIZED AND BRACKETED] indicate language being deleted. Complete new sections
FAMILY PLANNING AND PREGNANCY
 FAMILY PLANNING AND PREGNANCY Decisions about family planning can be difficult and very emotional when one of the prospective parents has a genetic disorder, such as Marfan syndrome. Before making any
FAMILY PLANNING AND PREGNANCY Decisions about family planning can be difficult and very emotional when one of the prospective parents has a genetic disorder, such as Marfan syndrome. Before making any
Caring for your perineum and pelvic floor after a 3rd or 4th degree tear
 Caring for your perineum and pelvic floor after a 3rd or 4th degree tear Most women, up to nine in ten (90%), tear to some extent during childbirth. Most tears occur in the perineum, the area between the
Caring for your perineum and pelvic floor after a 3rd or 4th degree tear Most women, up to nine in ten (90%), tear to some extent during childbirth. Most tears occur in the perineum, the area between the
EmONC Training Curricula Comparison
 EmONC Training Curricula Comparison The purpose of this guide is to provide a quick resource for trainers and course administrators to decide which EmONC curriculum is most applicable to their training
EmONC Training Curricula Comparison The purpose of this guide is to provide a quick resource for trainers and course administrators to decide which EmONC curriculum is most applicable to their training
Document Classification
 Document Classification Document Title Document Type Unique Identifier Function(s) (see table) Scope (see table) Target Audience Key words Author(s) Owner (see table) Date first published 2004 Date this
Document Classification Document Title Document Type Unique Identifier Function(s) (see table) Scope (see table) Target Audience Key words Author(s) Owner (see table) Date first published 2004 Date this
AvMA Annual Clinical Negligence Conference 27-28 June 2014, Hilton Brighton. Mr Duncan Irons Senior Consultant University Hospital Durham
 AvMA Annual Clinical Negligence Conference 27-28 June 2014, Hilton Brighton Mr Duncan Irons Senior Consultant University Hospital Durham CTG s common errors Uterine rupture Caesarean complications Episiotomy
AvMA Annual Clinical Negligence Conference 27-28 June 2014, Hilton Brighton Mr Duncan Irons Senior Consultant University Hospital Durham CTG s common errors Uterine rupture Caesarean complications Episiotomy
Regions Hospital Delineation of Privileges Certified Nurse Midwife
 Regions Hospital Delineation of Privileges Certified Nurse Midwife Applicant s Name: Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting. Review education
Regions Hospital Delineation of Privileges Certified Nurse Midwife Applicant s Name: Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting. Review education
ICD-10 OVERVIEW Coding Guidelines For OB/GYN
 ICD-10 OVERVIEW Coding Guidelines For OB/GYN ICD-10 Chapter 15 Pregnancy, Childbirth and the Puerperium (O00-O9A) Note: Codes from this chapter are for use only on maternal records, NEVER on newborn records.
ICD-10 OVERVIEW Coding Guidelines For OB/GYN ICD-10 Chapter 15 Pregnancy, Childbirth and the Puerperium (O00-O9A) Note: Codes from this chapter are for use only on maternal records, NEVER on newborn records.
Major roles of neurocognitive developmental center are as follows:
 Major roles of neurocognitive developmental center are as follows: 1. Fine developmental assessment of infant and toddler by Bayley Scales of Infant Development 2. Assessment of infant development by age
Major roles of neurocognitive developmental center are as follows: 1. Fine developmental assessment of infant and toddler by Bayley Scales of Infant Development 2. Assessment of infant development by age
CONFIDENT CODING FOR OB/GYN CONFIDENT CODING FOR OB/GYN
 Arlene J. Smith, CPC AAPC National Advisory Board 2007-2009 1 So when exactly does the global period start? Unraveling the confusion in antepartum care coding Correct coding for multiple gestations! Vaginal
Arlene J. Smith, CPC AAPC National Advisory Board 2007-2009 1 So when exactly does the global period start? Unraveling the confusion in antepartum care coding Correct coding for multiple gestations! Vaginal
The webinar will begin shortly
 Important Information for receiving your CE Certificate You will receive an email within 3-5 business days providing a LINK to the CE Certificate, the webinar recording and the presentation slides. This
Important Information for receiving your CE Certificate You will receive an email within 3-5 business days providing a LINK to the CE Certificate, the webinar recording and the presentation slides. This
Labor & Delivery Nursing Assessment Checklist
 Labor & Delivery Nursing Assessment Checklist NAME: DATE LEVEL OF COMPETENCE 1. No experience Never or observed only 3. Performs Independently Consistently practices 2. Needs Assistance Occasionally practices
Labor & Delivery Nursing Assessment Checklist NAME: DATE LEVEL OF COMPETENCE 1. No experience Never or observed only 3. Performs Independently Consistently practices 2. Needs Assistance Occasionally practices
Determining the Posture, Shape and Mobility of the Spine
 Determining the Posture, Shape and Mobility of the Spine The World of Biomechanics Assessment of the Mobility Function Using a special Triple Cervical marker set comprising miniature ultrasound transmitters,
Determining the Posture, Shape and Mobility of the Spine The World of Biomechanics Assessment of the Mobility Function Using a special Triple Cervical marker set comprising miniature ultrasound transmitters,
Evaluation of cardiotocographic and cord blood changes in induced labor with dinoprostone and misoprostol
 International Journal of Reproduction, Contraception, Obstetrics and Gynecology Pandey K et al. Int J Reprod Contracept Obstet Gynecol. 2014 Mar;3(1):199-203 www.ijrcog.org pissn 2320-1770 eissn 2320-1789
International Journal of Reproduction, Contraception, Obstetrics and Gynecology Pandey K et al. Int J Reprod Contracept Obstet Gynecol. 2014 Mar;3(1):199-203 www.ijrcog.org pissn 2320-1770 eissn 2320-1789
Assessment M EDIAL INK
 lon23944_ch18.qxd 2/14/06 4:45 PM Page 420 CHAPTER Intrapartal 18 Nursing Assessment It was strange. After months of waiting for my baby s birth, labor took me by surprise. I wasn t quite ready to move
lon23944_ch18.qxd 2/14/06 4:45 PM Page 420 CHAPTER Intrapartal 18 Nursing Assessment It was strange. After months of waiting for my baby s birth, labor took me by surprise. I wasn t quite ready to move
How To Know If A Delivery Is Complicated By Shoulder Dystocia
 Deconstructing A permanent brachial plexus injury is devastating to a child. It affects not only what the child can and can t do, but also his or her self-image. This injury rarely occurs in the absence
Deconstructing A permanent brachial plexus injury is devastating to a child. It affects not only what the child can and can t do, but also his or her self-image. This injury rarely occurs in the absence
PELVIS. 2007 Lippincott Williams & Wilkins S59 BONE: PELVIS (6) Location: Pelvic ring (61)
 Location: Pelvic ring (61)") PELVIS BONE: PELVIS (6) Location: Pelvic ring (61) Types: A. Lesion sparing (or with no displacement of) posterior arch (61-A) B. Incomplete disruption of posterior arch, partially stable (61-B) C. Complete
PELVIS BONE: PELVIS (6) Location: Pelvic ring (61) Types: A. Lesion sparing (or with no displacement of) posterior arch (61-A) B. Incomplete disruption of posterior arch, partially stable (61-B) C. Complete
What is ACLS Maternal Focus?
 Carla Rider, MBA, BSN, RNC-LRN, Administrative Director Women s Services Meredith Green, MSN Candidate, BSN, RN, Clinical Educator Women s Services What is? ACLS Component 1 American Heart Association
Carla Rider, MBA, BSN, RNC-LRN, Administrative Director Women s Services Meredith Green, MSN Candidate, BSN, RN, Clinical Educator Women s Services What is? ACLS Component 1 American Heart Association
Birth Injury Odyssey: Observations from Both Sides
 Birth Injury Odyssey: Observations from Both Sides By: Daniel J. Huff, Esq. Huff, Powell & Bailey, LLC 999 Peachtree Street, Suite 950 Atlanta, Georgia 30309 Taylor Tribble, Esq. Huff, Powell & Bailey,
Birth Injury Odyssey: Observations from Both Sides By: Daniel J. Huff, Esq. Huff, Powell & Bailey, LLC 999 Peachtree Street, Suite 950 Atlanta, Georgia 30309 Taylor Tribble, Esq. Huff, Powell & Bailey,
Structure and Function of the Hip
 Structure and Function of the Hip Objectives Identify the bones and bony landmarks of the hip and pelvis Identify and describe the supporting structures of the hip joint Describe the kinematics of the
Structure and Function of the Hip Objectives Identify the bones and bony landmarks of the hip and pelvis Identify and describe the supporting structures of the hip joint Describe the kinematics of the
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE
 SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: MAGNESIUM SULFATE ADMINISTRATION FOR ANTEPARTUM AND INTRAPARTUM PATIENTS WITH PRE-TERM LABOR DATE: REVIEWED: PAGES: 6/92 08/11 1 of 6 ISSUED FOR: Nursing
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: MAGNESIUM SULFATE ADMINISTRATION FOR ANTEPARTUM AND INTRAPARTUM PATIENTS WITH PRE-TERM LABOR DATE: REVIEWED: PAGES: 6/92 08/11 1 of 6 ISSUED FOR: Nursing
Claiming Compensation for Birth Injuries.
 Clinical Negligence: Claiming Compensation for Birth Injuries. T H O M P S O N S F A C T S H E E T About birth injury Compensation Types of birth injury cases where compensation may be possible How to
Clinical Negligence: Claiming Compensation for Birth Injuries. T H O M P S O N S F A C T S H E E T About birth injury Compensation Types of birth injury cases where compensation may be possible How to
Research. Shoulder dystocia is an uncommon
 Research www.ajog.org OBSTETRICS Effects of shoulder dystocia training on the incidence of brachial plexus injury Steven R. Inglis, MD; Nikolaus Feier, MD; Jyothi B. Chetiyaar, MD; Margaret H. Naylor,
Research www.ajog.org OBSTETRICS Effects of shoulder dystocia training on the incidence of brachial plexus injury Steven R. Inglis, MD; Nikolaus Feier, MD; Jyothi B. Chetiyaar, MD; Margaret H. Naylor,
Prognosis of Very Large First-Trimester Hematomas
 Case Series Prognosis of Very Large First-Trimester Hematomas Juliana Leite, MD, Pamela Ross, RDMS, RDCS, A. Cristina Rossi, MD, Philippe Jeanty, MD, PhD Objective. The aim of this study was to evaluate
Case Series Prognosis of Very Large First-Trimester Hematomas Juliana Leite, MD, Pamela Ross, RDMS, RDCS, A. Cristina Rossi, MD, Philippe Jeanty, MD, PhD Objective. The aim of this study was to evaluate
BEST- Practice Management Guidelines B: BEST Decision E: Evidence-Based S: Simple & Safe T: Team Focused
 OB Excellence: Postpartum Hemorrhage [PPH]-DATA ANALYSIS Perinatal University Speaker/Master Instructor: Carol A. Curran RNC, MS, OGNP CEO & Founder: Clinical Specialists Consulting & Perinatal University
OB Excellence: Postpartum Hemorrhage [PPH]-DATA ANALYSIS Perinatal University Speaker/Master Instructor: Carol A. Curran RNC, MS, OGNP CEO & Founder: Clinical Specialists Consulting & Perinatal University
Nursing Management During Labor and Birth. KeyTERMS. LearningOBJECTIVES
 chapter 14 Nursing Management During Labor and Birth KeyTERMS accelerations artifact baseline fetal heart rate baseline variability crowning deceleration electronic fetal monitoring episiotomy Leopold
chapter 14 Nursing Management During Labor and Birth KeyTERMS accelerations artifact baseline fetal heart rate baseline variability crowning deceleration electronic fetal monitoring episiotomy Leopold