Abnormal LFT s in Asymptomatic Patients
|
|
|
- Eustace Dickerson
- 8 years ago
- Views:
Transcription
1 Abnormal LFT s in Asymptomatic Patients FV Liver Care Pathway Pete Bramley Hepatology/Gastroenterology Forth Valley WSW Event 5 th and 7 th March 2013
2 Overview Liver disease in UK and Scotland Liver function tests - why bother? Liver function tests - the meaning of... Algorithms - explanation and discussion
3

4
5
6 Source:
7
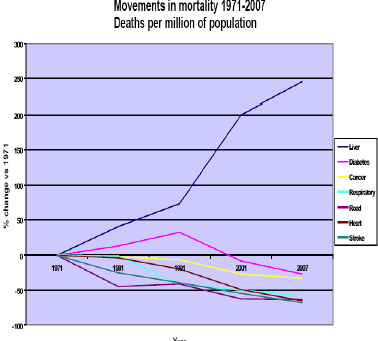
8 Chronic liver disease in Scotland: key points There are a variety of risk factors and diseases that cause chronic liver disease (CLD). The three commonest risk factors for CLD are excessive alcohol consumption; blood borne viruses, in particular Hepatitis B and C, and obesity. Between 1989 and 2010, there has been an approximate three-fold increase in chronic liver disease patient discharge rates in men, and a twofold increase in rates among women. Men living in the most deprived areas are 12 times more likely to die from CLD and for women seven times more likely, than those living in least deprived areas. The CLD mortality rate in Scotland has been increasing steadily over the last 30 yrs which is in contrast to the majority of European countries where CLD death rates have been decreasing. 8
9

10 Increasing deprivation

11 Death rates chronic liver disease per LA

12
13 The liver Superbly designed to maintain body s chemical and metabolic homeostasis
14
15
16
17
18 Acute or Chronic Liver Disease Acute hepatitis usually self-limiting viruses, toxins, drugs Chronic hepatitis if changes persist for over 6 months If continuing damage with cellular destruction leads on to fibrosis and cirrhosis Chronic liver disease
19 The challenge is to diagnose liver disease at an early stage determine aetiology modify disease if possible monitor and treat symptoms proactively deal with complications
20 Liver Function Tests AST/ALT, GGT, Alk Phos Liver injury tests Not a true reflection of hepatic functional reserve / capacity PT, Fibrinogen, Albumin Synthetic function - Bilirubin Excretory function
21 Liver Function Tests
22 Best practice in primary care pathology: interpretation LFT s 2006 In view of the statistical phenomenon of regression to mean, the principle of interval retesting to establish one-off from stable and progressive increases seems sound. There is guidance, but limited evidence, on retesting intervals, although in the asymptomatic context and in view of the slow time course of the potential underlying diseases, the retesting interval of months rather than weeks seems reasonable for minor increases, commonly described as up to 3 5 times the upper limit of normal (ULN). Indications for further investigation of persistent rises commonly refer to 1.5 x ULN. W S A Smellie, J Forth, S Ryder, M J Galloway, A C Wood, I D Watson J Clin Pathol 2006;59:

23 Chronic liver disease with normal LFT s Is the normal range for tests for patients correct? Decrease in AST / ALT during treatment suggesting mild inflammation within normal range of test 23
24 How to determine severity of chronic liver disease Liver biopsy - Gold Standard - tells us as it is? - Bilirubin - Late change hepatocellular- can be normal till cirrhosis- Earlier change cholestatic AST /ALT - not always helpful guide to severity can be normal, intermittently raised or high Alk Phos - as bilirubin - can be normal throughout or early rise Albumin - progressive fall as liver damage more severe PT / Clotting screen - progressive rise as liver deteriorates Platelets - gradual fall as increasing cirrhosis as portal hypertension develops, spleen enlarges, fewer platelets Hb / WCC as spleen continues enlarging - drop in Hb, WCC 24
25 How to determine severity of chronic liver disease Imaging - Ultrasound can show coarse echotexture, fatty change, irregular liver edge, presence of ascites, varices, tumours - liver may be enlarged, normal or small - spleen tends to enlarge - CT / MRI - more information, more detail Fibroscans - measure of stiffness of liver increased values with increasing fibrosis Good at confirming normal liver or significant fibrosis cirrhosis but not as accurate in middle ground - mild to moderate fibrosis - problems if obese Fibrotests in-house or commercial kits - panel of serum markers used to produce an overall value of fibrosis 25 28
26 Jacob Jordaens, Der gefesselte Prometheus, um 1640
27 Investigation of an isolated rise in Bilirubin 1 Isolated increase in Bilirubin >25 (>1.5xULN) Repeat test after 12hr fast And check conjugated / unconjugated split FBC and Film Post fasting if significant increase in Bilirubin (up to 70umol/l ) predominantly unconjugated Diagnosis is Gilberts Syndrome - reassurance and no further Ix needed Post fasting if no increase in Bilirubin But predominantly unconjugated consider haemolysis or haematoma breakdown Check FBC, blood Film Reticulocytes and LDH Post fasting if no increase in Bilirubin but predominantly conjugated Look for other evidence of compensated chronic liver disease If positive for haemolysis refer to haematology Check for potential Drug induced Liver Injury If minor rise < 2xULN (34) recheck all LFT s in 3months If significant rise >2xULN recheck 1 month Abdo-U/S Abnormal Dilated Ducts Abnormal liver mass Urgent referral to GI Medicine * Bilirubin Rising Organise Abdo U/S Check initial Liver screen Bilirubin falling Repeat in 3 months then 6 months Abdo U/S Normal Await rest of results And routine referral to GI Medicine Bilirubin normal No further action
28 Investigation of Isolated Raised Alkaline Phosphatase 2 Rule out pregnancy, young age, post-prandial increase If not already performed -check GGT GGT Normal ALP likely bone origin GGT Increased ALP likely liver origin Test for bone disorders Check for potential Drug induced Liver Injury If minor rise < 2xULN (240) recheck 3months If significant rise >2xULN recheck 1 month ALP static or rising ALP falling Repeat in 3 then 6 months Organise Abdo U/S Check initial liver screen Fluctuating ALP But remains abnormal after 6 months Abdo-U/S Abnormal Dilated Ducts Abnormal liver mass Urgent referral to GI Medicine Abdo U/S Normal Await rest of results, if abnormal perform extended liver screen and sent routine referral to GI Medicine
29 Causes of raised γ GT Hepatobiliary disease (often with other liver enzyme abnormalities). Pancreatic disease. Alcoholism (Sensitivity only 52-92% - low Specificity) Chronic obstructive pulmonary disease. Renal failure. Diabetes. Myocardial infarction. Drugs Enzyme inducers - eg, carbamazepine, phenytoin and barbiturates.
30 Serum aminotransferase levels in various liver diseases Acute on chronic Giannini, E. G. et al. CMAJ 2005;172:


31 Non alcoholic fatty liver disease - NAFLD NASH - non-alcoholic steatohepatitis Rapidly becoming disease of 21 st century Metabolic syndrome obesity, diabetes, IHD Normal liver NAFLD Fatty liver NASH Fibrosis 20% cirrhosis
32 Patients with confirmed liver test abnormalities due to known significant alcohol excess, fatty liver or drug induced liver injury (eg statins) provided the appropriate algorithms and investigations detailed above have been followed, can be managed appropriately and safely within primary care. Importance of social / medication history
33 Investigation of Isolated Raised Transaminases 3 Isolated increase in AST/ALT Advise stop alcohol Check for and stop any recently initiated hepatotoxic drugs Advise stop all over the counter herbal /alternative products If BMI > 25 or recent increase in wt - advise loss of 2-5kg Discuss if high risk - current / previous drug misuse /partner of drug misuser / from high prevalence area - check BBV If <2xULN (<80) - recheck in 6 months If >2xULN (>80) - recheck in 3 months If >3xULN (>120) - recheck in 1month Abdo U/S - Abnormal Dilated Ducts Abnormal liver mass Urgent referral to GI Medicine If persisting degree of abnormality or rising values at repeat testing Reinforce above advice Organise Abdo U/S Examine for signs of liver disease Check Initial Liver screen Abdo U/S Normal or fatty liver only Initial liver screen negative - Reinforce advice re stopping alcohol / Drug / herbal meds, losing wt If <2xULN (<80) - recheck in 6 months If >2xULN (>80) - recheck in 3 months If >3xULN (>120) - recheck in 1month if still abnormal - and full compliance with advice above Consider routine referral to GI Medicine See Triage pathway 6 Abdo U/S abnormal texture Initial liver screen negative Send off extended liver screen as appropriate And routine referral to GI Medicine If falling values at repeat test Repeat in 6-12 months Abdo U/S normal or abnormal texture Initial liver screen positive Send off extended liver screen as appropriate to clarify abnormality And routine referral to GI Medicine
34 Investigation of cluster of Abnormal LFT s 4 Predominantly Hepatocellular picture Predominant increase in AST/ALT With raised GGT and +/- minor rise in Bil and ALP Predominantly Cholestatic picture Predominant increase in Alkaline Phosphatase with elevated GGT +/- bilirubin and +/- minor rise in AST/ALT Advise stop alcohol Check for and stop any recently initiated hepatotoxic drugs Advise stop all over the counter herbal /alternative products Discuss if high risk - current / previous drug misuse /partner of drug misuser /from area high prevalence -check for BBV Examine for signs of liver disease If most deranged test <2xULN - recheck in 3 months >2xULN - recheck in 2 months >3xULN - recheck in 1month If pain +/- increased Bilirubin Urgent referral to GI Medicine via the Fast Track Jaundice Service For raid access to U/S and ERCP /MRCP Abdo U/S - Abnormal Dilated Ducts Abnormal liver mass Urgent referral to GI Medicine If persisting degree of abnormality or rising values Request abdo ultrasound and initial liver screen If rapidly deteriorating tests discuss with GI on Call Abdo U/S Normal or fatty liver only Initial liver screen negative - Reinforce advice re stopping alcohol / Drug / herbal meds, losing wt If most deranged test <2xULN - recheck in 6 months If >2xULN - recheck in 3 months If >3xULN - recheck in 1month if still abnormal - and full compliance with advice above Consider routine referral to GI Medicine See Triage pathway 6 Abdo U/S abnormal texture Initial liver screen negative Send off extended liver screen as appropriate And routine referral to GI Medicine If falling values at repeat test Repeat in 3-6 months Abdo U/S normal or abnormal texture Initial liver screen positive Send off extended liver screen as appropriate to clarify abnormality And routine referral to GI Medicine
35 Triage for Forth Valley Liver Care Pathway 5 Follow previous algorithms to classify liver abnormality If concerned about patient or with rapidly deteriorating condition Discuss directly with consultant GI Medicine on Call via Switchboard FVRH Outside office hours in ill patient consider inpatient assessment via CAU Emergency GI clinics for urgent OP referrals held twice week accessed via GI consultant on Call and Sci Gateway If evidence of significant alcohol excess or NAFLD (Fatty liver) and receptive to following lifestyle advice to address health issues. Only refer if adherent to advice with no improvement in LFT s Routine referral via SciGateway to gastroenterology (A9) If significant chronic Alcoholic liver disease or NAFLD (Fatty liver disease) Routine referral via Sci Gateway to gastroenterology (A9) If evidence of Viral Hepatitis, genetic liver disease or autoimmune liver disease Routine referral via Sci Gateway to gastroenterology (A9) If no clear diagnosis but persistent LFT abnormalities and monitored over time interval as per algorithms- Routine referral via Sci Gateway to gastroenterology (A9) If cholestatic jaundice with or without pain in a patient with no evidence of alcohol misuse. Discuss directly with Dr Dalziel s Sec for referral to the FastTrack Jaundice Pathway. For Urgent OP referral for rapid access to U/S and ERCP Patients will be triaged by consultant on call to First available GI consultant routine OP slot Patients will be triaged by consultant on call to First available Hepatology Service routine OP slot. Viral Hepatitis patients will be fast tracked to a Nurse Led assessment and harm reduction clinic Patients will be triaged by consultant on call to First available GI consultant routine OP slot
36 FV Hepatology Service Based at Stirling Community Hospital clinics provided in FVRH, SCH, CCH, SPS, Addictions Previously the FV Hepatitis Service One consultant, three specialist hepatitis nurses, patient pathway co-ordinator, ( + medical secretary in FVRH) Now development of generic Hepatology nurse specialists Nurse led - Virtual Hepatoma screening clinics Administrator led - Varices recall databases Nurse led - Haemochromatosis maintenance clinics Nurse led - outreach HCV / HBV / Hepatology clinics Five consultant clinics per week Tasked to deliver on Government directives Respect and Responsibility / BBV/SH Framework / HIS Hepatitis Standards Sexual Health / HIV integration 36
37 37
38 Screening for significant fibrotic chronic liver disease AST/ALT ratio = AST / ALT When greater than 2.0, it is more likely to be associated with alcoholic hepatitis or hepatocellular carcinoma When greater than 1.0 but less than 2.0, it is likely to be associated with cirrhosis It is normally less than 1.0 with chronic hepatitis C and often becomes greater than 1.0 in cirrhotic HCV However, the AST/ALT ratio is less useful in scenarios where the liver enzymes are not elevated, or where multiple conditions co-exist 38
39 Summary of Recommendations ( BSG Guidelines 2006) 1-Recommendation: Clinicians should be aware that a minority of people with abnormal LFTs will have no liver disease. Evidence grade B. 2-Recommendation: Clinicians should be aware that normal LFTs do not mean an absence of significant liver disease. Evidence grade B. 3-Recommendation: Clinicians should be aware that the majority of asymptomatic patients with abnormal LFT s will have liver disease and a proportion will have significant liver damage (fibrosis or cirrhosis). Evidence grade B. 4-Recommendation: Abnormal LFTs in asymptomatic patients should be investigated in the same way as symptomatic patients as there is no difference in the severity of liver disease found. Evidence grade B. 5-Recommendation: An absence of stigmata of chronic liver disease should not preclude investigation of abnormal LFTs as significant liver damage, including cirrhosis may still be present. Evidence grade B. 6-Recommendation: Any degree of LFT abnormality should be considered for investigation as even minor abnormalities can be associated with significant liver disease. Evidence grade B. 7-Recommendation: Abnormal LFTs in asymptomatic patients should be investigated if the abnormalities have persisted for a minimum of 3-6 months. Evidence grade C. 8-Recommendation: The following tests comprise the initial liver screen and the subsequent more detailed extended liver screen 39
40 Initial liver screen should include Hepatitis Screen (hepatitis B surface antigen, hepatitis C antibody), liver autoantibody screen (anti-mitochondrial antibody, anti-smooth muscle antibody), anti-nuclear antibody (ANF), serum immunoglobulins, serum ferritin, Thyroid function tests (TFT s), full clotting scren. Also request Abdomineal U/S Extended liver screen should includetissue Transglutanimase (TTG) for coeliac disease Anti-Neutrophil Cytotoxic Antibody (ANCA) ceruloplasmin, * α1 antitrypsin level * Alpha Fetoprotein if HBV sag positive - labs should check other HBV markers and Hep B DNA load If Ferritin raised above ULN range check Serum Iron / Total Iron Binding Capacity (Fe/TIBC) = transferrin Sat% If Transferrin Sat% above 55% male or 50% female - check HFE (haemochromatosis) gene assay If Ceruloplasmin below 0.15g/l - on referal Hepatology will organise 24hr urinary copper excretion and ophthalmology review for Kayser Fleischer rings 40
41 Statins and Abnormal Liver function - for info - Not really applicable to protocol as LFT monitoring following introduction of drug 0.5 to 3.0 percent occurrence of persistent elevations in aminotransferases in patients receiving statins. This occurs during the first three months of therapy and is dose-dependent. Several large trials with over 100,000 patient years of exposure have not shown any significant difference in the incidence or severity of persistently raised AST/ALT between statin and placebo treatment. A meta-analysis of 35 randomized trials found an excess risk of aminotransferase elevation with statin therapy versus placebo of 4.2 cases per 1000 patients Rare episodes of more severe liver injury have also been seen, these predominantly occur three to four months after initiation of statin therapy. However, it appears these are sufficiently uncommon that overall the incidence of drug induced liver failure in patients taking statins appears to be no different from the low incidence in the general population. US based knowledge base - UptoDate 2012 recommend changing medications or lowering the statin dose in patients who are found to have an alanine aminotransferase (ALT) level more than three times the upper limit of normal (>120 iu/ml), that is confirmed on a second occasion. The NHS Evidence Clinical Knowledge Summary states that if liver function test s are abnormal while on a statin:if less than three times the upper limit of normal: - Continue the statin, but recheck LFTs within 4 6 weeks to exclude further increases in transaminase levels. - No extra monitoring is required if values are stable. If transaminase levels are three times the upper limit of normal or more:- Stop the statin and recheck LFTs within 4 6 weeks to ensure that values settle (consider re-introducing the statin cautiously at a later date) or Reduce the statin dose and recheck LFTs within 4 6 weeks:stop the statin if transaminase levels continue to be three times the upper limit of normal or more. In Forth Valley we suggest that if there is no improvement to dose modification, then perform an initial liver screen, then if necessary, an extended liver screen should be carried out as per abnormal 41 transaminase pathway above.
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Summary liver function / liver function
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Summary liver function / liver function
Southern Derbyshire. Shared Care Pathology Guidelines. Abnormal Liver Function Tests (LFTs) in Adults
 in Adults") Southern Derbyshire Shared Care Pathology Guidelines Abnormal Liver Function Tests (LFTs) in Adults Purpose of Guideline The management of patients with abnormal liver function test results Scope This
Southern Derbyshire Shared Care Pathology Guidelines Abnormal Liver Function Tests (LFTs) in Adults Purpose of Guideline The management of patients with abnormal liver function test results Scope This
Evaluation of Liver Function tests in Primary Care. Abid Suddle Institute of Liver Studies, KCH
 Evaluation of Liver Function tests in Primary Care Abid Suddle Institute of Liver Studies, KCH Liver Function tests Markers of hepatocellular damage Cholestasis Liver synthetic function Markers of Hepatocellular
Evaluation of Liver Function tests in Primary Care Abid Suddle Institute of Liver Studies, KCH Liver Function tests Markers of hepatocellular damage Cholestasis Liver synthetic function Markers of Hepatocellular
Managing LFT s in General Practice
 Managing LFT s in General Practice Sulleman Moreea FRCP(Edin Edin) ) FRCS(Glasg Glasg) Consultant Gastroenterologist/Hepatologist Bradford Hospitals Trust The normal liver Managing LFT s History and examination
Managing LFT s in General Practice Sulleman Moreea FRCP(Edin Edin) ) FRCS(Glasg Glasg) Consultant Gastroenterologist/Hepatologist Bradford Hospitals Trust The normal liver Managing LFT s History and examination
Alanine aminotransferase (serum, plasma)
") Alanine aminotransferase (serum, plasma) 1 Name and description of analyte 1.1 Name of analyte Alanine aminotransferase (ALT) 1.2 Alternative names Systematic name L alanine:2 oxoglutarate aminotransferase
Alanine aminotransferase (serum, plasma) 1 Name and description of analyte 1.1 Name of analyte Alanine aminotransferase (ALT) 1.2 Alternative names Systematic name L alanine:2 oxoglutarate aminotransferase
Approach to Abnormal Liver Tests
 Approach to Abnormal Liver Tests Naga P. Chalasani, MD, FACG Professor of Medicine and Cellular & Integrative Physiology Director, Division of Gastroenterology and Hepatology Indiana University School
Approach to Abnormal Liver Tests Naga P. Chalasani, MD, FACG Professor of Medicine and Cellular & Integrative Physiology Director, Division of Gastroenterology and Hepatology Indiana University School
The child with abnormal liver function tests
 The child with abnormal liver function tests Dr Jane Hartley Consultant Paediatric Hepatologist Birmingham Children s Hospital, UK 1 st Global Congress CIP, Paris 2011 Contents Over view of liver anatomy,
The child with abnormal liver function tests Dr Jane Hartley Consultant Paediatric Hepatologist Birmingham Children s Hospital, UK 1 st Global Congress CIP, Paris 2011 Contents Over view of liver anatomy,
2.1 AST can be measured in heparin plasma or serum. 3 Summary of clinical applications and limitations of measurements
 Aspartate aminotransferase (serum, plasma) 1 Name and description of analyte 1.1 Name of analyte Aspartate aminotransferase (AST) 1.2 Alternative names Systematic name L aspartate:2 oxoglutarate aminotransferase
Aspartate aminotransferase (serum, plasma) 1 Name and description of analyte 1.1 Name of analyte Aspartate aminotransferase (AST) 1.2 Alternative names Systematic name L aspartate:2 oxoglutarate aminotransferase
What to do with abnormal LFTs? Andrew M Smith Hepatobiliary Surgeon
 What to do with abnormal LFTs? Andrew M Smith Hepatobiliary Surgeon "it looks like there's something wrong.with your television set. Matt Groenig, creator of The Simpsons Probability of an abnormal screening
What to do with abnormal LFTs? Andrew M Smith Hepatobiliary Surgeon "it looks like there's something wrong.with your television set. Matt Groenig, creator of The Simpsons Probability of an abnormal screening
Assessment of some biochemical tests in liver diseases
 Assessment of some biochemical tests in liver diseases By Prof. Mohamed Sharaf-Eldin Prof. of Hepatology & Gastroenterology Faculty of Medicine Tanta University, Egypt. Significant liver damage may occur
Assessment of some biochemical tests in liver diseases By Prof. Mohamed Sharaf-Eldin Prof. of Hepatology & Gastroenterology Faculty of Medicine Tanta University, Egypt. Significant liver damage may occur
Abnormal Liver Function. Dr William Alazawi MA(Cantab) PhD MRCP Senior Lecturer and Consultant in Hepatology Queen Mary, University of London
 PhD MRCP Senior Lecturer and Consultant in Hepatology Queen Mary, University of London") Abnormal Liver Function Dr William Alazawi MA(Cantab) PhD MRCP Senior Lecturer and Consultant in Hepatology Queen Mary, University of London Does Liver Disease Matter? Mortality in England & Wales Liver-related
Abnormal Liver Function Dr William Alazawi MA(Cantab) PhD MRCP Senior Lecturer and Consultant in Hepatology Queen Mary, University of London Does Liver Disease Matter? Mortality in England & Wales Liver-related
Revised Newcastle, North Tyneside and Northumberland Guidelines for the Management of Adults with Asymptomatic Liver Function Abnormalities.
 Clinical Guidelines Revised Newcastle, North Tyneside and Northumberland Guidelines for the Management of Adults with Asymptomatic Liver Function Abnormalities. August 2014 Dr Mark Hudson Dr Stuart McPherson
Clinical Guidelines Revised Newcastle, North Tyneside and Northumberland Guidelines for the Management of Adults with Asymptomatic Liver Function Abnormalities. August 2014 Dr Mark Hudson Dr Stuart McPherson
Evaluation of abnormal LFT in the asymptomatic patient. Son Do, M.D. Advanced Gastroenterology Vancouver, WA
 Evaluation of abnormal LFT in the asymptomatic patient Son Do, M.D. Advanced Gastroenterology Vancouver, WA Definition of chronic, abnormally elevated LFT Elevation of one or more of the following for
Evaluation of abnormal LFT in the asymptomatic patient Son Do, M.D. Advanced Gastroenterology Vancouver, WA Definition of chronic, abnormally elevated LFT Elevation of one or more of the following for
Albumin. Prothrombin time. Total protein
 Hepatitis C Fact Sheet February 2016 www.hepatitis.va.gov Laboratory Tests and Hepatitis If you have hepatitis C, your doctor will use laboratory tests to about learn more about your individual hepatitis
Hepatitis C Fact Sheet February 2016 www.hepatitis.va.gov Laboratory Tests and Hepatitis If you have hepatitis C, your doctor will use laboratory tests to about learn more about your individual hepatitis
Liver Function Tests - The Downside
 KAPIL CHOPRA, MD 1 So I'm going to kickoff this course with the topic of abnormal liver function tests. To be very honest this is a huge topic. I think to do justice I'm going to try and touch on some
KAPIL CHOPRA, MD 1 So I'm going to kickoff this course with the topic of abnormal liver function tests. To be very honest this is a huge topic. I think to do justice I'm going to try and touch on some
Evaluation of a Child with Elevated Transaminases. Linda V. Muir, M.D. April 11, 2008 Northwest Pediatric Liver Disease Symposium
 Evaluation of a Child with Elevated Transaminases Linda V. Muir, M.D. April 11, 2008 Northwest Pediatric Liver Disease Symposium Disclosures I do not have a financial interest, arrangement or affiliation
Evaluation of a Child with Elevated Transaminases Linda V. Muir, M.D. April 11, 2008 Northwest Pediatric Liver Disease Symposium Disclosures I do not have a financial interest, arrangement or affiliation
Transmission of HCV in the United States (CDC estimate)
") Transmission of HCV in the United States (CDC estimate) Past and Future US Incidence and Prevalence of HCV Infection Decline among IDUs Overall incidence Overall prevalence Infected 20+ years Armstrong
Transmission of HCV in the United States (CDC estimate) Past and Future US Incidence and Prevalence of HCV Infection Decline among IDUs Overall incidence Overall prevalence Infected 20+ years Armstrong
Hepatitis C. Laboratory Tests and Hepatitis C
 Hepatitis C Laboratory Tests and Hepatitis C If you have hepatitis C, your doctor will use laboratory tests to check your health. This handout will help you understand what the major tests are and what
Hepatitis C Laboratory Tests and Hepatitis C If you have hepatitis C, your doctor will use laboratory tests to check your health. This handout will help you understand what the major tests are and what
OMG my LFT s! How to Interpret and Use Them. OMG my LFT s! OMG my LFT s!
 How to Interpret and Use Them René Romero, M.D. Clinical Director, Pediatric Hepatology CPG Gastroenterology, Hepatology and Nutrition Emory University School of Medicine Objectives Understand the anatomy
How to Interpret and Use Them René Romero, M.D. Clinical Director, Pediatric Hepatology CPG Gastroenterology, Hepatology and Nutrition Emory University School of Medicine Objectives Understand the anatomy
NP/PA Clinical Hepatology Fellowship Summary of Year-Long Curriculum
 OVERVIEW OF THE FELLOWSHIP The goal of the AASLD NP/PA Fellowship is to provide a 1-year postgraduate hepatology training program for nurse practitioners and physician assistants in a clinical outpatient
OVERVIEW OF THE FELLOWSHIP The goal of the AASLD NP/PA Fellowship is to provide a 1-year postgraduate hepatology training program for nurse practitioners and physician assistants in a clinical outpatient
LIVER FUNCTION TESTS AND STATINS
 LIVER FUNCTION TESTS AND STATINS Philippe J. Zamor and Mark W. Russo Current Opinion in Cardiology 2011,26:338 341 SUMMARY Purpose of review: To discuss recent data on statins in patients with elevated
LIVER FUNCTION TESTS AND STATINS Philippe J. Zamor and Mark W. Russo Current Opinion in Cardiology 2011,26:338 341 SUMMARY Purpose of review: To discuss recent data on statins in patients with elevated
Review: How to work up your patient with Hepatitis C
 Review: How to work up your patient with Hepatitis C You screened your patient, and now the HCV antibody test is positive. What do you do next? The antibody test only means they have been exposed to HCV.
Review: How to work up your patient with Hepatitis C You screened your patient, and now the HCV antibody test is positive. What do you do next? The antibody test only means they have been exposed to HCV.
What to Do with the Patient With Abnormal Liver Enzymes? Nizar N. Zein, M.D. The Cleveland Clinic
 What to Do with the Patient With Abnormal Liver Enzymes? Nizar N. Zein, M.D. The Cleveland Clinic Introduction Elevated liver enzymes is often not a clinical problem by itself. However it is a warning
What to Do with the Patient With Abnormal Liver Enzymes? Nizar N. Zein, M.D. The Cleveland Clinic Introduction Elevated liver enzymes is often not a clinical problem by itself. However it is a warning
Session 11: The ABCs of LFTs Learning Objectives
 Session 11: The ABCs of LFTs Learning Objectives 1. Define 3 key components of the patient history that should be further evaluated when liver function testing reveals elevated aminotransferases. 2. Identify
Session 11: The ABCs of LFTs Learning Objectives 1. Define 3 key components of the patient history that should be further evaluated when liver function testing reveals elevated aminotransferases. 2. Identify
Hepatology Guidelines for Primary Care November 2011
 Common requests for hepatology opinion/advice 1. Abnormal LFTs (is this fatty liver?) 2. Fatty Liver Disease (is this serious liver disease?) 3. Abnormal liver ultrasound 4. Alcohol related liver disease
Common requests for hepatology opinion/advice 1. Abnormal LFTs (is this fatty liver?) 2. Fatty Liver Disease (is this serious liver disease?) 3. Abnormal liver ultrasound 4. Alcohol related liver disease
Asymptomatic Elevated Liver Function Tests: Physiology, Chemistry, and Workup
 Asymptomatic Elevated Liver Function Tests: Physiology, Chemistry, and Workup James T. Sing, Jr., D.O., FACG, AGAF Scott & White Clinic Assistant Professor Department of Internal Medicine Division of Gastroenterology
Asymptomatic Elevated Liver Function Tests: Physiology, Chemistry, and Workup James T. Sing, Jr., D.O., FACG, AGAF Scott & White Clinic Assistant Professor Department of Internal Medicine Division of Gastroenterology
Comparative Levels of ALT, AST, ALP and GGT in Liver associated Diseases
 Available online at wwwpelagiaresearchlibrarycom European Journal of Experimental Biology, 2013, 3(2):280-284 ISSN: 2248 9215 CODEN (USA): EJEBAU Comparative Levels of ALT, AST, ALP and GGT in Liver associated
Available online at wwwpelagiaresearchlibrarycom European Journal of Experimental Biology, 2013, 3(2):280-284 ISSN: 2248 9215 CODEN (USA): EJEBAU Comparative Levels of ALT, AST, ALP and GGT in Liver associated
Disclosures. Interpreting Liver Tests: What Do They Mean? Liver Function Tests. Objectives. Common Tests. Case 1
 Disclosures Interpreting Liver Tests: What Do They Mean? I have no financial disclosures to make. Roman Perri, MD Vanderbilt University Medical Center Nashville, TN Objectives Discuss tests commonly used
Disclosures Interpreting Liver Tests: What Do They Mean? I have no financial disclosures to make. Roman Perri, MD Vanderbilt University Medical Center Nashville, TN Objectives Discuss tests commonly used
Non-alcoholic fatty liver disease: Prognosis and Treatment
 Non-alcoholic fatty liver disease: Prognosis and Treatment Zachary Henry, M.D. Assistant Professor UVA Gastroenterology & Hepatology October 28, 2015 Overview Case Presentation Prognosis Effects of fibrosis
Non-alcoholic fatty liver disease: Prognosis and Treatment Zachary Henry, M.D. Assistant Professor UVA Gastroenterology & Hepatology October 28, 2015 Overview Case Presentation Prognosis Effects of fibrosis
HOW TO EVALUATE ELEVATED LIVER ENZYMES
 HOW TO EVALUATE ELEVATED LIVER ENZYMES Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine LABORATORY TESTS OF
HOW TO EVALUATE ELEVATED LIVER ENZYMES Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine LABORATORY TESTS OF
Liver Diseases. An Essential Guide for Nurses and Health Care Professionals
 Brochure More information from http://www.researchandmarkets.com/reports/1047385/ Liver Diseases. An Essential Guide for Nurses and Health Care Professionals Description: Liver disease is a rapidly growing
Brochure More information from http://www.researchandmarkets.com/reports/1047385/ Liver Diseases. An Essential Guide for Nurses and Health Care Professionals Description: Liver disease is a rapidly growing
GUIDELINES & PROTOCOLS
 GUIDELINES & PROTOCOLS ADVISORY COMMITTEE Effective Date: August 1, 2011 Scope This guideline provides recommendations for the evaluation and interpretation of abnormal liver test results in adults ( 19
GUIDELINES & PROTOCOLS ADVISORY COMMITTEE Effective Date: August 1, 2011 Scope This guideline provides recommendations for the evaluation and interpretation of abnormal liver test results in adults ( 19
Liver Function Tests. Dr Stephen Butler Paediatric Advance Trainee TDHB
 Liver Function Tests Dr Stephen Butler Paediatric Advance Trainee TDHB Introduction Case presentation What is the liver? Overview of tests used to measure liver function RJ 10 month old European girl
Liver Function Tests Dr Stephen Butler Paediatric Advance Trainee TDHB Introduction Case presentation What is the liver? Overview of tests used to measure liver function RJ 10 month old European girl
LIVER FUNCTION TESTS
 MODULE Liver Function Tests 17 LIVER FUNCTION TESTS 17.1 INTRODUCTION Liver function tests are a group of tests done to assess the functional capacity of the liver as well as any cellular damage to the
MODULE Liver Function Tests 17 LIVER FUNCTION TESTS 17.1 INTRODUCTION Liver function tests are a group of tests done to assess the functional capacity of the liver as well as any cellular damage to the
BACKGROUND MEDIA INFORMATION Fast facts about liver disease
 BACKGROUND MEDIA INFORMATION Fast facts about liver disease Liver, or hepatic, disease comprises a wide range of complex conditions that affect the liver. Liver diseases are extremely costly in terms of
BACKGROUND MEDIA INFORMATION Fast facts about liver disease Liver, or hepatic, disease comprises a wide range of complex conditions that affect the liver. Liver diseases are extremely costly in terms of
GT-020 Phase 1 Clinical Trial: Results of Second Cohort
 GT-020 Phase 1 Clinical Trial: Results of Second Cohort July 29, 2014 NASDAQ: GALT www.galectintherapeutics.com 2014 Galectin Therapeutics inc. Forward-Looking Statement This presentation contains, in
GT-020 Phase 1 Clinical Trial: Results of Second Cohort July 29, 2014 NASDAQ: GALT www.galectintherapeutics.com 2014 Galectin Therapeutics inc. Forward-Looking Statement This presentation contains, in
LIVER FUNCTION TESTS AND LIVER DISEASES. Prof. Fang Zheng Department of Laboratory Medicine School of Medicine, Wuhan University
 LIVER FUNCTION TESTS AND LIVER DISEASES Prof. Fang Zheng Department of Laboratory Medicine School of Medicine, Wuhan University Content the Anatomy of Liver the Function of Liver Tests of Liver Function
LIVER FUNCTION TESTS AND LIVER DISEASES Prof. Fang Zheng Department of Laboratory Medicine School of Medicine, Wuhan University Content the Anatomy of Liver the Function of Liver Tests of Liver Function
HIV and Hepatitis Co-infection. Martin Fisher Brighton and Sussex University Hospitals, UK
 HIV and Hepatitis Co-infection Martin Fisher Brighton and Sussex University Hospitals, UK Useful References British HIV Association 2010 http://www.bhiva.org/documents/guidelines/hepbc/2010/ hiv_781.pdf
HIV and Hepatitis Co-infection Martin Fisher Brighton and Sussex University Hospitals, UK Useful References British HIV Association 2010 http://www.bhiva.org/documents/guidelines/hepbc/2010/ hiv_781.pdf
Recommendations for the Identification of Chronic Hepatitis C virus infection Among Persons Born During 1945-1965
 Recommendations for the Identification of Chronic Hepatitis C virus infection Among Persons Born During 1945-1965 MMWR August 17, 2012 Prepared by : The National Viral Hepatitis Technical Assistance Center
Recommendations for the Identification of Chronic Hepatitis C virus infection Among Persons Born During 1945-1965 MMWR August 17, 2012 Prepared by : The National Viral Hepatitis Technical Assistance Center
HEPATITIS WEB STUDY Acute Hepatitis C Virus Infection: Epidemiology, Clinical Features, and Diagnosis
 HEPATITIS WEB STUDY Acute C Virus Infection: Epidemiology, Clinical Features, and Diagnosis H. Nina Kim, MD Assistant Professor of Medicine Division of Infectious Diseases University of Washington School
HEPATITIS WEB STUDY Acute C Virus Infection: Epidemiology, Clinical Features, and Diagnosis H. Nina Kim, MD Assistant Professor of Medicine Division of Infectious Diseases University of Washington School
Routine Investigations for Liver Disease a guide
 fighting childhood liver disease Routine Investigations for Liver Disease a guide Medical Information Series Welcome This leaflet has been written specifically for: Parents/carers of a child with a liver
fighting childhood liver disease Routine Investigations for Liver Disease a guide Medical Information Series Welcome This leaflet has been written specifically for: Parents/carers of a child with a liver
Update on Hepatitis C. Sally Williams MD
 Update on Hepatitis C Sally Williams MD Hep C is Everywhere! Hepatitis C Magnitude of the Infection Probably 8 to 10 million people in the U.S. are infected with Hep C 30,000 new cases are diagnosed annually;
Update on Hepatitis C Sally Williams MD Hep C is Everywhere! Hepatitis C Magnitude of the Infection Probably 8 to 10 million people in the U.S. are infected with Hep C 30,000 new cases are diagnosed annually;
Laboratory Monitoring of Adult Hospital Patients Receiving Parenteral Nutrition
 Laboratory Monitoring of Adult Hospital Patients Receiving Parenteral Nutrition Copy 1 Location of copies Web based only The following guideline is for use by medical staff caring for the patient and members
Laboratory Monitoring of Adult Hospital Patients Receiving Parenteral Nutrition Copy 1 Location of copies Web based only The following guideline is for use by medical staff caring for the patient and members
MANAGEMENT OF COMMON SIDE EFFECTS of INH (Isoniazid), RIF (Rifampin), PZA (Pyrazinamide), and EMB (Ethambutol)
, RIF (Rifampin), PZA (Pyrazinamide), and EMB (Ethambutol)") MANAGEMENT OF COMMON SIDE EFFECTS of INH (Isoniazid), RIF (Rifampin), PZA (Pyrazinamide), and EMB (Ethambutol) 1. Hepatotoxicity: In Active TB Disease a. Background: 1. Among the 4 standard anti-tb drugs,
MANAGEMENT OF COMMON SIDE EFFECTS of INH (Isoniazid), RIF (Rifampin), PZA (Pyrazinamide), and EMB (Ethambutol) 1. Hepatotoxicity: In Active TB Disease a. Background: 1. Among the 4 standard anti-tb drugs,
HEPATOLOGY CLERKSHIP
 College of Osteopathic Medicine HEPATOLOGY CLERKSHIP Office for Clinical Affairs 515-271-1629 FAX 515-271-1727 Elective Rotation General Description This elective rotation is a four (4) week introductory,
College of Osteopathic Medicine HEPATOLOGY CLERKSHIP Office for Clinical Affairs 515-271-1629 FAX 515-271-1727 Elective Rotation General Description This elective rotation is a four (4) week introductory,
The most serious symptoms of this stage are:
 The Natural Progression of Hepatitis C The natural history of hepatitis C looks at the likely outcomes for people infected with the virus if there is no medical intervention. However, the process of trying
The Natural Progression of Hepatitis C The natural history of hepatitis C looks at the likely outcomes for people infected with the virus if there is no medical intervention. However, the process of trying
NAFLD/NASH: Criteri diagnostici e prognostici
 Monotematica AISF Personalizzazione della Cura in Epatologia NAFLD/NASH: Criteri diagnostici e prognostici Pisa 17-19 ottobre 2013 Elisabetta Bugianesi MD, PhD Division of Gastro-Hepatology, University
Monotematica AISF Personalizzazione della Cura in Epatologia NAFLD/NASH: Criteri diagnostici e prognostici Pisa 17-19 ottobre 2013 Elisabetta Bugianesi MD, PhD Division of Gastro-Hepatology, University
Viral Hepatitis Case Report
 Page 1 of 9 Viral Hepatitis Case Report Perinatal Hepatitis B Virus Infection Michigan Department of Community Health Communicable Disease Division Investigation Information Investigation ID Onset Date
Page 1 of 9 Viral Hepatitis Case Report Perinatal Hepatitis B Virus Infection Michigan Department of Community Health Communicable Disease Division Investigation Information Investigation ID Onset Date
Hepatitis C Treatment Expansion Initiative Multi-Site Conference Call. March 16, 2011
 Hepatitis C Treatment Expansion Initiative Multi-Site Conference Call March 16, 2011 Case Presentations Kansas City Free Health Clinic Carilion Clinic Didactic Session Challenges in Determining HCV Treatment
Hepatitis C Treatment Expansion Initiative Multi-Site Conference Call March 16, 2011 Case Presentations Kansas City Free Health Clinic Carilion Clinic Didactic Session Challenges in Determining HCV Treatment
Liver means Life. Why this manifesto? We are eager to ensure. that we can contribute. to society as much. as possible, and we. are equally keen to
 Manifesto by the European Liver Patients Association (ELPA) on policy measures against chronic liver disease 2014 to 2019 Why this manifesto? Every five years European voters get the opportunity to have
Manifesto by the European Liver Patients Association (ELPA) on policy measures against chronic liver disease 2014 to 2019 Why this manifesto? Every five years European voters get the opportunity to have
New IDSA/AASLD Guidelines for Hepatitis C
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER New IDSA/AASLD Guidelines for Hepatitis C John Scott, MD, MSc Associate Professor, UW SoM Asst Director, Liver Clinic, Harborview Medical Center Presentation
NORTHWEST AIDS EDUCATION AND TRAINING CENTER New IDSA/AASLD Guidelines for Hepatitis C John Scott, MD, MSc Associate Professor, UW SoM Asst Director, Liver Clinic, Harborview Medical Center Presentation
Approach to Abnormal Liver Tests
 This Morning s Presentation Approach to Abnormal Liver Tests Hal F. Yee, Jr., M.D., Ph.D. Rice Distinguished Professor, UCSF Chief of Gastroenterology, SFGH hyee@medsfgh.ucsf.edu Clinical vignettes representing
This Morning s Presentation Approach to Abnormal Liver Tests Hal F. Yee, Jr., M.D., Ph.D. Rice Distinguished Professor, UCSF Chief of Gastroenterology, SFGH hyee@medsfgh.ucsf.edu Clinical vignettes representing
Hepatitis C Infections in Oregon September 2014
 Public Health Division Hepatitis C Infections in Oregon September 214 Chronic HCV in Oregon Since 25, when positive laboratory results for HCV infection became reportable in Oregon, 47,252 persons with
Public Health Division Hepatitis C Infections in Oregon September 214 Chronic HCV in Oregon Since 25, when positive laboratory results for HCV infection became reportable in Oregon, 47,252 persons with
The following should be current within the past 6 months:
 EVALUATION Baseline Labs Obtain at time or prior to initial evaluation CBC with diff PT/INR CMP HCV Genotype (obtained PRIOR TO consult visit) HCV RNA (obtained PRIOR TO consult visit) Hep A IgG Hep BsAg,
EVALUATION Baseline Labs Obtain at time or prior to initial evaluation CBC with diff PT/INR CMP HCV Genotype (obtained PRIOR TO consult visit) HCV RNA (obtained PRIOR TO consult visit) Hep A IgG Hep BsAg,
Update on hepatitis C: treatment and care and future directions
 Update on hepatitis C: treatment and care and future directions Professor Greg Dore Viral Hepatitis Clinical Research Program, National Centre in HIV Epidemiology and Clinical Research, University of New
Update on hepatitis C: treatment and care and future directions Professor Greg Dore Viral Hepatitis Clinical Research Program, National Centre in HIV Epidemiology and Clinical Research, University of New
INITIATING ORAL AUBAGIO (teriflunomide) THERAPY
 THERAPY") FOR YOUR PATIENTS WITH RELAPSING FORMS OF MS INITIATING ORAL AUBAGIO (teriflunomide) THERAPY WARNING: HEPATOTOXICITY AND RISK OF TERATOGENICITY Severe liver injury including fatal liver failure has been
FOR YOUR PATIENTS WITH RELAPSING FORMS OF MS INITIATING ORAL AUBAGIO (teriflunomide) THERAPY WARNING: HEPATOTOXICITY AND RISK OF TERATOGENICITY Severe liver injury including fatal liver failure has been
Interpretation of abnormal liver function tests. Dr Rania Bakry, MD
 Interpretation of abnormal liver function tests Dr Rania Bakry, MD Liver function tests Noninvasive method of screening for the presence of liver dysfunction Pattern of lab test abnormality allows recognition
Interpretation of abnormal liver function tests Dr Rania Bakry, MD Liver function tests Noninvasive method of screening for the presence of liver dysfunction Pattern of lab test abnormality allows recognition
MANAGEMENT OF LIVER CIRRHOSIS
 MANAGEMENT OF LIVER CIRRHOSIS Information Leaflet Your Health. Our Priority. Page 2 of 6 What is cirrhosis? Cirrhosis is a result of long-term, continuous damage to the liver and may be due to many different
MANAGEMENT OF LIVER CIRRHOSIS Information Leaflet Your Health. Our Priority. Page 2 of 6 What is cirrhosis? Cirrhosis is a result of long-term, continuous damage to the liver and may be due to many different
Abnormal Liver Tests. Dr David Scott Gastroenterologist
 Abnormal Liver Tests Dr David Scott Gastroenterologist Talk Outline Understanding Liver Tests Examples of Liver Diseases Case Studies Blood Tests for the Liver LFTs = Liver Function tests Hepatocyte damage
Abnormal Liver Tests Dr David Scott Gastroenterologist Talk Outline Understanding Liver Tests Examples of Liver Diseases Case Studies Blood Tests for the Liver LFTs = Liver Function tests Hepatocyte damage
A.P. Chen, MD Director, Developmental Therapeutics Clinic Division of Cancer Treatment and Diagnosis National Cancer Institute
 A.P. Chen, MD Director, Developmental Therapeutics Clinic Division of Cancer Treatment and Diagnosis National Cancer Institute Click to view Biosketch and Presentation Abstract or page down to review presentation
A.P. Chen, MD Director, Developmental Therapeutics Clinic Division of Cancer Treatment and Diagnosis National Cancer Institute Click to view Biosketch and Presentation Abstract or page down to review presentation
PREVENTION OF HCC BY HEPATITIS C TREATMENT. Morris Sherman University of Toronto
 PREVENTION OF HCC BY HEPATITIS C TREATMENT Morris Sherman University of Toronto Pathogenesis of HCC in chronic hepatitis C Injury cirrhosis HCC Injury cirrhosis HCC Time The Ideal Study Prospective randomized
PREVENTION OF HCC BY HEPATITIS C TREATMENT Morris Sherman University of Toronto Pathogenesis of HCC in chronic hepatitis C Injury cirrhosis HCC Injury cirrhosis HCC Time The Ideal Study Prospective randomized
Liver, Gallbladder and Pancreas diseases. Premed 2 Pathophysiology
 Liver, Gallbladder and Pancreas diseases Premed 2 Pathophysiology Pancreas Pancreatitis Acute Pancreatitis Autodigestion of the pancreas due to activation of the enzymes Hemorrhagic fat necrosis, calcium
Liver, Gallbladder and Pancreas diseases Premed 2 Pathophysiology Pancreas Pancreatitis Acute Pancreatitis Autodigestion of the pancreas due to activation of the enzymes Hemorrhagic fat necrosis, calcium
LIVER FUNCTION TESTS
 LIVER FUNCTION TESTS University of PNG School of Medicine and Health Sciences, Division of Basic Medical Sciences, Discipline of Biochemistry & Molecular Biology VJ Temple 1 What are some of the functions
LIVER FUNCTION TESTS University of PNG School of Medicine and Health Sciences, Division of Basic Medical Sciences, Discipline of Biochemistry & Molecular Biology VJ Temple 1 What are some of the functions
Cirrhosis and HCV. Jonathan Israel M.D.
 Cirrhosis and HCV Jonathan Israel M.D. Outline Relationship of fibrosis and cirrhosisprevalence and epidemiology. Sequelae of cirrhosis Diagnosis of cirrhosis Effect of cirrhosis on efficacy of treatment
Cirrhosis and HCV Jonathan Israel M.D. Outline Relationship of fibrosis and cirrhosisprevalence and epidemiology. Sequelae of cirrhosis Diagnosis of cirrhosis Effect of cirrhosis on efficacy of treatment
LIVER CANCER AND TUMOURS
 LIVER CANCER AND TUMOURS LIVER CANCER AND TUMOURS Healthy Liver Cirrhotic Liver Tumour What causes liver cancer? Many factors may play a role in the development of cancer. Because the liver filters blood
LIVER CANCER AND TUMOURS LIVER CANCER AND TUMOURS Healthy Liver Cirrhotic Liver Tumour What causes liver cancer? Many factors may play a role in the development of cancer. Because the liver filters blood
Information about hepatitis C for patients and carers
 Information about hepatitis C for patients and carers What is hepatitis C? Hepatitis C is an illness caused by a virus which can be passed through blood from one person to another. It mainly affects the
Information about hepatitis C for patients and carers What is hepatitis C? Hepatitis C is an illness caused by a virus which can be passed through blood from one person to another. It mainly affects the
PRIOR AUTHORIZATION PROTOCOL FOR HEPATITIS C TREATMENT
 PRIOR AUTHORIZATION PROTOCOL FOR HEPATITIS C TREATMENT HARVONI (90mg ledipasvir/400mg sofosbuvir): tablet (PREFERRED AGENT) SOVALDI (sofosbuvir ): 400mg tablets (PREFERRED AGENT ) OLYSIO (simeprivir) PEG-INTRON
PRIOR AUTHORIZATION PROTOCOL FOR HEPATITIS C TREATMENT HARVONI (90mg ledipasvir/400mg sofosbuvir): tablet (PREFERRED AGENT) SOVALDI (sofosbuvir ): 400mg tablets (PREFERRED AGENT ) OLYSIO (simeprivir) PEG-INTRON
Rivaroxaban: Prescribing Guidance for the treatment of provoked venous thromboembolism (VTE)
") Rivaroxaban: Prescribing Guidance for the treatment of provoked venous thromboembolism (VTE) Amber Drug Level 2 Leeds We have started your patient on rivaroxaban for the treatment of provoked VTE (deep
Rivaroxaban: Prescribing Guidance for the treatment of provoked venous thromboembolism (VTE) Amber Drug Level 2 Leeds We have started your patient on rivaroxaban for the treatment of provoked VTE (deep
New Development in Treating Liver Disorders: Approaches to liver function test from mild to fulminant disorders
 Research and Reviews New Development in Treating Liver Disorders: Approaches to liver function test from mild to fulminant disorders JMAJ 53(4): 218 223, 2010 Hirohito TSUBOUCHI,* 1 Akio IDO,* 2 Seiichi
Research and Reviews New Development in Treating Liver Disorders: Approaches to liver function test from mild to fulminant disorders JMAJ 53(4): 218 223, 2010 Hirohito TSUBOUCHI,* 1 Akio IDO,* 2 Seiichi
Preface. TTY: (888) 232-6348 or cdcinfo@cdc.gov. Hepatitis C Counseling and Testing, contact: 800-CDC-INFO (800-232-4636)
 232-6348 or cdcinfo@cdc.gov. Hepatitis C Counseling and Testing, contact: 800-CDC-INFO (800-232-4636)") Preface The purpose of this CDC Hepatitis C Counseling and Testing manual is to provide guidance for hepatitis C counseling and testing of individuals born during 1945 1965. The guide was used in draft
Preface The purpose of this CDC Hepatitis C Counseling and Testing manual is to provide guidance for hepatitis C counseling and testing of individuals born during 1945 1965. The guide was used in draft
www.australiandoctor.com.au Table 1: Pathology of liver abnormalities 50 (may be normal, or very high with complete biliary obstruction
 How to Treat PULL-OUT SECTION Complete How to Treat quizzes online /cpd to earn CPD or PDP points. INSIDE Non-hepatic causes Underestimated severity of liver disease Rare diagnoses Drug-induced liver damage
How to Treat PULL-OUT SECTION Complete How to Treat quizzes online /cpd to earn CPD or PDP points. INSIDE Non-hepatic causes Underestimated severity of liver disease Rare diagnoses Drug-induced liver damage
HCV/HIVCo-infection A case study by. Dominic Côté, Nurse Clinician B.Sc Chronic Viral Illness Services McGill University Health Centre
 HCV/HIVCo-infection A case study by Dominic Côté, Nurse Clinician B.Sc Chronic Viral Illness Services McGill University Health Centre Objectives By sharing a case study of a patient co-infected with HIV/HCV
HCV/HIVCo-infection A case study by Dominic Côté, Nurse Clinician B.Sc Chronic Viral Illness Services McGill University Health Centre Objectives By sharing a case study of a patient co-infected with HIV/HCV
Liver Transplantation for Hepatocellular Carcinoma. John P. Roberts, MD Chief, Division of Transplant Service University of California, San Francisco
 Liver Transplantation for Hepatocellular Carcinoma John P. Roberts, MD Chief, Division of Transplant Service University of California, San Francisco Hepatocellular Carcinoma HCC is the 5th most common
Liver Transplantation for Hepatocellular Carcinoma John P. Roberts, MD Chief, Division of Transplant Service University of California, San Francisco Hepatocellular Carcinoma HCC is the 5th most common
After the Cure: Long-Term Management of HCV Liver Disease Norah A. Terrault, MD, MPH
 After the Cure: Long-Term Management of HCV Liver Disease Norah A. Terrault, MD, MPH Professor of Medicine Department of Gastroenterology Director, Viral Hepatitis Center University of California San Francisco
After the Cure: Long-Term Management of HCV Liver Disease Norah A. Terrault, MD, MPH Professor of Medicine Department of Gastroenterology Director, Viral Hepatitis Center University of California San Francisco
Primary Care Guidance Program: Non-Alcohol related Fatty Liver Disease (NAFLD) Guidance on Management in Primary Care
 Guidance on Management in Primary Care") Primary Care Guidance Program: Non-Alcohol related Fatty Liver Disease (NAFLD) Guidance on Management in Primary Care This advice has been developed to help GPs with shared care of patients with Non- Alcohol
Primary Care Guidance Program: Non-Alcohol related Fatty Liver Disease (NAFLD) Guidance on Management in Primary Care This advice has been developed to help GPs with shared care of patients with Non- Alcohol
2015 Outpatient Chronic Hepatitis B Management
 2015 Outpatient Chronic Hepatitis B Management Hepatitis B Hepatitis B Info 70% of acute infections are subclinical More severe symptoms when in addition to other liver disease Fulminant Hepatitis
2015 Outpatient Chronic Hepatitis B Management Hepatitis B Hepatitis B Info 70% of acute infections are subclinical More severe symptoms when in addition to other liver disease Fulminant Hepatitis
Indications in Hepatology and Liver Diseases
 exclusively working in Health Care sananet GmbH Tilo Stolzke Breite Str. 6-8 23562 Lübeck Germany Telefon : +49 451 400 8301 Telefax : +49 451 400 8302 E-Mail : stolzke@sananet.com Internet : www.sananet.com
exclusively working in Health Care sananet GmbH Tilo Stolzke Breite Str. 6-8 23562 Lübeck Germany Telefon : +49 451 400 8301 Telefax : +49 451 400 8302 E-Mail : stolzke@sananet.com Internet : www.sananet.com
Lamivudine for Patients with hronic Hepatitis B and Advanced Liver Disease. From : New England Journal of Medicine
 Lamivudine for Patients with hronic Hepatitis B and Advanced Liver Disease From : New England Journal of Medicine Volume 351:1521-1531, Number 15, Oct 7, 2004 馬 偕 紀 念 醫 院 一 般 內 科, 肝 膽 腸 胃 科 新 竹 分 院 陳 重
Lamivudine for Patients with hronic Hepatitis B and Advanced Liver Disease From : New England Journal of Medicine Volume 351:1521-1531, Number 15, Oct 7, 2004 馬 偕 紀 念 醫 院 一 般 內 科, 肝 膽 腸 胃 科 新 竹 分 院 陳 重
Prof. of Tropical Medicine Faculty of Medicine Alexandria University
 prof. Dr. Ali El-Kady (MD) Prof. of Tropical Medicine Faculty of Medicine Alexandria University DRUGS THAT MAY CAUSE LIVER DYSFUNCTION DAMAGE The liver is the principal organ that is capable of converting
prof. Dr. Ali El-Kady (MD) Prof. of Tropical Medicine Faculty of Medicine Alexandria University DRUGS THAT MAY CAUSE LIVER DYSFUNCTION DAMAGE The liver is the principal organ that is capable of converting
Evaluation and Prognosis of Patients with Cirrhosis
 Evaluation and Prognosis of Patients with Cirrhosis Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded
Evaluation and Prognosis of Patients with Cirrhosis Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded
Unexplained Hepatic, Neurologic or Psychiatric Symptoms?
 A Diagnostic Tool for Physicians Unexplained Hepatic, Neurologic or Psychiatric Symptoms? Think WILSON DISEASE ALGORITHMS FOR ASSESSMENT OF WILSON DISEASE Table 1. Clinical Features in Patients with Wilson
A Diagnostic Tool for Physicians Unexplained Hepatic, Neurologic or Psychiatric Symptoms? Think WILSON DISEASE ALGORITHMS FOR ASSESSMENT OF WILSON DISEASE Table 1. Clinical Features in Patients with Wilson
LCD for Viral Hepatitis Serology Tests
 LCD for Viral Hepatitis Serology Tests Applicable CPT Code(s): 86692 Antibody; Hepatitis, Delta Agent 86704 Hepatitis B Core Antibody (HBcAb); Total 86705 Hepatitis B Core Antibody (HBcAb); IgM Antibody
LCD for Viral Hepatitis Serology Tests Applicable CPT Code(s): 86692 Antibody; Hepatitis, Delta Agent 86704 Hepatitis B Core Antibody (HBcAb); Total 86705 Hepatitis B Core Antibody (HBcAb); IgM Antibody
Surveillance for Hepatocellular Carcinoma
 Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
ELEMENTS FOR A PUBLIC SUMMARY. Overview of disease epidemiology. Summary of treatment benefits
 VI: 2 ELEMENTS FOR A PUBLIC SUMMARY Bicalutamide (CASODEX 1 ) is a hormonal therapy anticancer agent, used for the treatment of prostate cancer. Hormones are chemical messengers that help to control the
VI: 2 ELEMENTS FOR A PUBLIC SUMMARY Bicalutamide (CASODEX 1 ) is a hormonal therapy anticancer agent, used for the treatment of prostate cancer. Hormones are chemical messengers that help to control the
Assessment of Liver Function and Diagnostic Studies. Disclosures
 Assessment of Liver Function and Diagnostic Studies 2011 Joseph Ahn, M.D., M.S. Assistant Professor of Medicine Medical Director, Liver Transplantation v.3 Disclosures Absolute Autopsy Key Points 1. Review
Assessment of Liver Function and Diagnostic Studies 2011 Joseph Ahn, M.D., M.S. Assistant Professor of Medicine Medical Director, Liver Transplantation v.3 Disclosures Absolute Autopsy Key Points 1. Review
Recommendations 8/14/2014. Hepatitis C Clinical Approach Primary Care. Purpose of Presentation. HCV Prevalence Year of Birth
 Hepatitis C Clinical Approach Primary Care Dr. Vicki L. MIt McIntyre, FNP Tucson Gastroenterology Specialists Tucson, Arizona University of Phoenix Lead Faculty, Department of Nursing Tucson, Arizona Purpose
Hepatitis C Clinical Approach Primary Care Dr. Vicki L. MIt McIntyre, FNP Tucson Gastroenterology Specialists Tucson, Arizona University of Phoenix Lead Faculty, Department of Nursing Tucson, Arizona Purpose
Beginner's guide to Hepatitis C testing and immunisation against hepatitis A+B in general practice
 Beginner's guide to Hepatitis C testing and immunisation against hepatitis A+B in general practice Dr Chris Ford GP & SMMGP Clinical Lead Kate Halliday Telford & Wrekin Shared Care Coordinator Aims Discuss:
Beginner's guide to Hepatitis C testing and immunisation against hepatitis A+B in general practice Dr Chris Ford GP & SMMGP Clinical Lead Kate Halliday Telford & Wrekin Shared Care Coordinator Aims Discuss:
POST EXPOSURE PROPHYLAXI S
 Departments of Infectious Diseases & Emergency Medicine POST EXPOSURE PROPHYLAXI S QUI CK GUI DE FOR EMERGENCY DEPT Adapted from Irish National PEP Guidelines and St James s Hospital GUIDE Clinic/Emergency
Departments of Infectious Diseases & Emergency Medicine POST EXPOSURE PROPHYLAXI S QUI CK GUI DE FOR EMERGENCY DEPT Adapted from Irish National PEP Guidelines and St James s Hospital GUIDE Clinic/Emergency
Novartis Gilenya FDO Program Clinical Protocol and Highlights from Prescribing Information (PI)
") Novartis Gilenya FDO Program Clinical Protocol and Highlights from Prescribing Information (PI) Highlights from Prescribing Information - the link to the full text PI is as follows: http://www.pharma.us.novartis.com/product/pi/pdf/gilenya.pdf
Novartis Gilenya FDO Program Clinical Protocol and Highlights from Prescribing Information (PI) Highlights from Prescribing Information - the link to the full text PI is as follows: http://www.pharma.us.novartis.com/product/pi/pdf/gilenya.pdf
NASH: It is not JUST a Fatty Liver. Karen F. Murray, M.D. Director of Hepatobiliary Program Children s Hospital and Regional Medical Center
 NASH: It is not JUST a Fatty Liver Karen F. Murray, M.D. Director of Hepatobiliary Program Children s Hospital and Regional Medical Center Stages of Fatty Liver Disorders Fatty Liver 16-35% of Western
NASH: It is not JUST a Fatty Liver Karen F. Murray, M.D. Director of Hepatobiliary Program Children s Hospital and Regional Medical Center Stages of Fatty Liver Disorders Fatty Liver 16-35% of Western
Service Definition with all Clinical Terms Service: Laprascopic Cholecystectomy Clinic (No Gallstones in bile duct)
") Service Definition with all Clinical Terms Service: Laprascopic Cholecystectomy Clinic (No Gallstones in bile duct) Section 1 Service Details Service ID: 7540540 Service Comments: Referrer Alert: Service
Service Definition with all Clinical Terms Service: Laprascopic Cholecystectomy Clinic (No Gallstones in bile duct) Section 1 Service Details Service ID: 7540540 Service Comments: Referrer Alert: Service
Management of non response or relapse following HCV therapy. Greg Dore Darrell Crawford
 Management of non response or relapse following HCV therapy Greg Dore Darrell Crawford Learning objectives To understand importance of characterisation of prior HCV therapy response To explore options
Management of non response or relapse following HCV therapy Greg Dore Darrell Crawford Learning objectives To understand importance of characterisation of prior HCV therapy response To explore options
North of Tyne Area Prescribing Committee
 North of Tyne Area Prescribing Committee ANTIPSYCHOTICS IN PSYCHOSIS, BIPOLAR DISORDER AND AUGMENTATION THERAPY IN TREATMENT RESISTANT DEPRESSION Information for Primary Care Updated November 2013 This
North of Tyne Area Prescribing Committee ANTIPSYCHOTICS IN PSYCHOSIS, BIPOLAR DISORDER AND AUGMENTATION THERAPY IN TREATMENT RESISTANT DEPRESSION Information for Primary Care Updated November 2013 This
Bilirubin (serum, plasma)
") Bilirubin (serum, plasma) 1 Analyte 1.1 Name of analyte Bilirubin 1.2 Alternative names None 1.3 NLMC code 1.4 Description of analyte Bilirubin is a linear tetrapyrrole (MW 585 Da), the final product of
Bilirubin (serum, plasma) 1 Analyte 1.1 Name of analyte Bilirubin 1.2 Alternative names None 1.3 NLMC code 1.4 Description of analyte Bilirubin is a linear tetrapyrrole (MW 585 Da), the final product of
Canadian Association of Gastroenterology (CAG) Practice Guidelines: Evaluation of abnormal liver enzyme tests
 Practice Guidelines: Evaluation of abnormal liver enzyme tests") CAG PRACTICE GUIDELINES Canadian Association of Gastroenterology Practice Guidelines: Evaluation of abnormal liver enzyme tests Approximately one in 10 Canadians has at least one abnormal liver biochemical
CAG PRACTICE GUIDELINES Canadian Association of Gastroenterology Practice Guidelines: Evaluation of abnormal liver enzyme tests Approximately one in 10 Canadians has at least one abnormal liver biochemical
better medicin Liver Function Testing in primary care
 bpac nz better medicin e Liver Function Testing in primary care Liver Function Testing in primary care P o i n t s t o c o n s i d e r While reading this document, you may like to consider the following
bpac nz better medicin e Liver Function Testing in primary care Liver Function Testing in primary care P o i n t s t o c o n s i d e r While reading this document, you may like to consider the following
Recruitment Start date: April 2010 End date: Recruitment will continue until enrolment is fully completed
 Apitope study The study drug (ATX-MS-1467) is a new investigational drug being tested as a potential treatment for relapsing forms of multiple sclerosis (RMS). The term investigational drug means it has
Apitope study The study drug (ATX-MS-1467) is a new investigational drug being tested as a potential treatment for relapsing forms of multiple sclerosis (RMS). The term investigational drug means it has
Commonly Asked Questions About Chronic Hepatitis C
 Commonly Asked Questions About Chronic Hepatitis C From the American College of Gastroenterology 1. How common is the hepatitis C virus? The hepatitis C virus is the most common cause of chronic viral
Commonly Asked Questions About Chronic Hepatitis C From the American College of Gastroenterology 1. How common is the hepatitis C virus? The hepatitis C virus is the most common cause of chronic viral
EMEA PUBLIC STATEMENT ON LEFLUNOMIDE (ARAVA) - SEVERE AND SERIOUS HEPATIC REACTIONS -
 - SEVERE AND SERIOUS HEPATIC REACTIONS -") The European Agency for the Evaluation of Medicinal Products Post-authorisation evaluation of medicines for human use London, 12 March 2001 Doc. Ref: EMEA/H/5611/01/en EMEA PUBLIC STATEMENT ON LEFLUNOMIDE
The European Agency for the Evaluation of Medicinal Products Post-authorisation evaluation of medicines for human use London, 12 March 2001 Doc. Ref: EMEA/H/5611/01/en EMEA PUBLIC STATEMENT ON LEFLUNOMIDE
Hepatitis B and C Co-infection. Mark Hull MHSc, FRCPC Clinical Assistant Professor Division of AIDS
 Hepatitis B and C Co-infection Mark Hull MHSc, FRCPC Clinical Assistant Professor Division of AIDS Objectives Review natural history of hepatitis coinfection Brief overview of treatment indications for
Hepatitis B and C Co-infection Mark Hull MHSc, FRCPC Clinical Assistant Professor Division of AIDS Objectives Review natural history of hepatitis coinfection Brief overview of treatment indications for