Spine. The following case studies relate to injuries to the Spine.
|
|
|
- Sabina Gibbs
- 9 years ago
- Views:
Transcription
1 Spine The following case studies relate to injuries to the Spine. More detailed information regarding the assessment of spinal injuries may be found at Chapter 4 of the MAA s Permanent Impairment Guidelines and Chapter 3.3 of the AMA4 Guidelines. The Motor Accidents Authority of NSW makes no warranties or representation about the accuracy or completeness of the information contained in these Case Studies. It should be noted that the information contained herein is not provided as a substitute for legal advice.

2 Spine Case Study # Brief Description Primary Body System Secondary Body System Spine1 Cervical and thoracic spine injuries Spine Upper Limb Spine2 Thoracic spine fracture Spine Spine3 Pelvic fracture methodology Spine Spine4 Pevis and sacrum fractures Spine Lower Limb Spine5 Cervical spine fracture Spine Spine6 Cervical, thoracic and lumbar spines Spine Spine7 Cervical multilevel structural compromise Spine Upper Limb Spine8 DRE categories Spine Skin Spine9 Thoracic spine fractures Spine Spine10 Thoracic fractures Spine Lower Limb Spine11 Compression Fracture L1 and L2 Spine Spine12 Pre-existing Spinal Surgery Spine Spine13 Multilevel Structural Compromise Spine Upper Limb Spine14 Whiplash Spine Spine15 Spinal Spacing Devices Spine Spine16 Pre-existing Lumbar Impairment Spine Upper Limb Spine17 Sciatica/Psoas muscle Spine Lower Limb Spine18 Pre-existing Spinal Fusion Spine

3 Injuries: Cervical spine soft tissue injury Thoracic spine fracture Right shoulder - AC joint Right knee soft tissue injury The claimant was the driver of a vehicle; another vehicle hit her on the passenger side of their car and she received impact damage to the left side of her body. The momentum from the impact caused her to strike the right-hand side of the car door sustaining injuries to the right-hand side of her body. Current Symptoms Cervical spine pain She describes a central, constant ache; this radiates to the right and left shoulder. She states that it is non-specific and will come on at any time but is particularly worse after she has been looking down for a period of time (e.g. working on a computer). Thoracic spine pain The claimant describes a constant, interscapular ache; it is interspersed with episodes of sharp pain which is localised. The constant ache will invariably radiate to the right shoulder. This back pain is increased by movement especially repetitive lifting, pushing, pulling or attempting to work above her head. The pain is also increased by sitting for 45 minutes. She has problems sleeping at night and needs to us a body pillow. Right shoulder pain The claimant describes an intermittent, sharp pain in the outer aspect of the right shoulder. This radiates to the upper outer arm and can also spread to the right wrist. She will often notice early morning numbness involving both hands (right greater than left) and this is often associated with reduced grip. Her right shoulder pain is aggravated by lifting, working with her arms out in front of her, pushing and pulling and any repetitive movement. Right knee pain She describes an intermittent ache within the joint; this is associated with a tight feeling and she states she invariably experiences a swelling which she notices is in the suprapatellar area. She denies locking or giving way. Clinical Examination On examination she was of average stature and overweight. She walked with a normal gait. She rose steadily using both hands to push herself off the chair. She dressed and undressed slowly but was able to stand independently on each leg without support. She had a normal posture; there was no evidence of pelvic tilt or limb shortening on measurement. Examination of the thoraco-lumbar spine did not reveal any skeletal deformity or abnormality. There was no scoliosis, lumbar tilt or rotational deformity. The kyphotic and lordotic curves were normal. She was specifically tender over the T7 vertebra but

4 this was not associated with any muscle spasm or guarding. I note X-rays performed of the thoracic spine describe a depression in the superior end plate of the mid-thoracic vertebral body which is taken to be T7 on the frontal view; so there is a loss of vertebral height of approximately 20%. No other focal vertebral body abnormality was detected. Examination of the cervical spine showed the neck to be short and thick; the attitude was neutral and normal. There was no evidence of torticollis. There was no specific tenderness over the spinous processes, interspinous ligaments or paraspinous muscles. The trapezii were normal; there was no evidence of muscle spasm and no region acting as a trigger area. Examination of the shoulders showed the bony and soft tissue contours to be equivalent. There was no evidence of rotator cuff or spinate muscle wasting. The AC joint was tender on the right side compared with the left; the SC joints were unremarkable. The following shoulder movements were obtained: Shoulder Measurements (goniometer verified): AMA 4 Figures 38, 41 & 44 (Pages 43, 44 & 45) Measurement RIGHT Measurement LEFT Flexion Extension Adduction Abduction Internal Rotation External Rotation The upper arms were symmetric in dimension and there was no evidence of loss of tone, wasting or tenderness about the triceps or biceps muscles. The grip of the hands was strong and equivalent; there was no evidence of small muscle wasting. Examination of the knees did not demonstrate any condylar or patellar expansion, synovial hypertrophy or effusion (negative swipe test). On repeated flexion extension of both knees there was evidence of some retropatellar crepitus involving the right knee (the Clarke s test was positive). Power throughout the range of movement was strong and equivalent; there were no bursii or cysts associated with the knee joint. There was no medial or lateral joint line tenderness, collateral ligament laxity, increased drawer movement or abnormal tibial rotatory movement. Impairment Evaluation The claimant s cervical spine has been assessed initially from Table 4.1 MAA Permanent Impairment Guidelines; and then from Table 73 of the Fourth Edition of the AMA Guides.

5 There was no evidence of muscle guarding present today. There was no evidence of muscle tenderness over the lower fibres of either trapezius which could have resulted in any neck restriction. There was minimal neck restriction observed at today s examination. There was no evidence of dysmetria noted. Imaging has not shown evidence of pre-existing disease. The claimant s thoracic spine was assessed as a fracture of T7 with less than 25% compression using Table 4.1 MAA Permanent Impairment Guidelines; and then from Table 74 of the Fourth Edition of the AMA Guides. The claimant s right shoulder was assessed using Figures 38, 41 and 44 of AMA4 Guidelines due to loss of range of motion. Examination of the right knee revealed some retropatellar crepitus. I refer to AMA Guides Edition Four, page 83, Table 62 and the sub-caption under this table which states In a patient with a history of direct trauma and complaint of patellofemoral pain and crepitation on physical examination but without joint space narrowing on X- ray, a 2% whole person impairment is given. In my opinion, the claimant s right knee qualifies for a 2% whole person impairment on the basis of this directive. Body Part or System AMA Guides/ MAA Guidelines References (chapter/ page/table) Chapter 3; Table 73 Chapter 3; 1. Cervico-thoracic spine 2. Thoraco-lumbar spine Table Right shoulder Chapter 3; Figures 38, 41 & Right knee Chapter 3; Table 41 & 62 Stabilised (YES/NO) * %WPI = percentage whole person impairment Current %WPI* %WPI* from pre-existing OR subsequent causes Yes Yes Yes Yes %WPI* due to motor accident Determination Regarding the Degree of Whole Person Impairment of the Injured Person as a Result of the Injuries Caused by the Motor Accident The total percentage whole person permanent impairment for assessed injuries caused by the motor accident is 12%.

6 This matter was subject to review by a Medical Review Panel. These are the Review Panel s findings. Claimant s Date of Birth: 7 October 1970 Date of Motor Accident: 28 July 2005 Injuries: Wedge fracture of the T12 vertebra (thoracic spine injury) Panel Findings The report of the X-Ray thoracic and lumbar spine on 9 November 2005 records a healing fracture of the superior end plate of the body of T12 which is virtually complete. There is a residual anterior wedged deformity of approximately 20% There is a mild Tii/12 kyphosis. The Review Panel inspected the plain x-rays of the thoracolumbar spine. Assessor A measured the heights of thoracolumbar vertical bodies (T10, T11, T12, L1) as being 25mm, 24mm, 23mm, 32mm respectively. The corresponding measurements obtained independently by Assessor B were 26.5mm, 24mm, 22mm and 28mm (the variations were within the margins of error of the measurement procedures, and variations in reference point). The radiological parameters clearly indicated significant compression of both T11 and T12 vertebral bodies. Panel Deliberations This is assessable in terms of the DRE criteria, p 106, AMAG4. The panel was in no doubt that the documentation provided clear evidence of a significant thoracic spine injury. There had been unequivocal documentation of a wedge fracture of the T12 vertebra, with associated pain. The panel concluded that examination of the latest films also provided clear evidence of a fracture of T11 (as well as T12) vertebra. The panel now notes that various radiological and clinical entries have raised the possibility that in addition to the T12 fracture there has been a T11 (and/or T10) fracture (vide supra re radiological report from Bankstown Hospital also Liverpool Hospital admission note and subsequent progress notes which refer to possible T11/T12 fractures). The presence of two vertebral body fractures is classified as multi-level structural compromise for purposes of DRE classification (see para 4.33, p28, MAA Permanent Impairment Guidelines). Accordingly, there is a DREIV designation for thoracic spine impairment, and this equates to 20% WPI (see p 106, AMAG4). Panel Decision The whole person permanent impairment of the injuries caused by the accident was calculated as follows:

7 Body Part or System AMA Guides/ MAA Guidelines References (chapter/ page/table) 1. Thoracic spine P106, AMAG4, para 4.33, MAA Guidelines Permanent (YES/NO) * %WPI = percentage whole person impairment Current %WPI* %WPI* from pre-existing OR subsequent causes Yes 20% 0% 20% %WPI* due to motor accident Determination Regarding the Degree of Whole Person Impairment of the Injured Person as a Result of the Injuries Caused by the Motor Accident The total percentage whole person permanent impairment for assessed injuries caused by the motor accident is 20%. Therefore the total whole person impairment is greater than 10%.

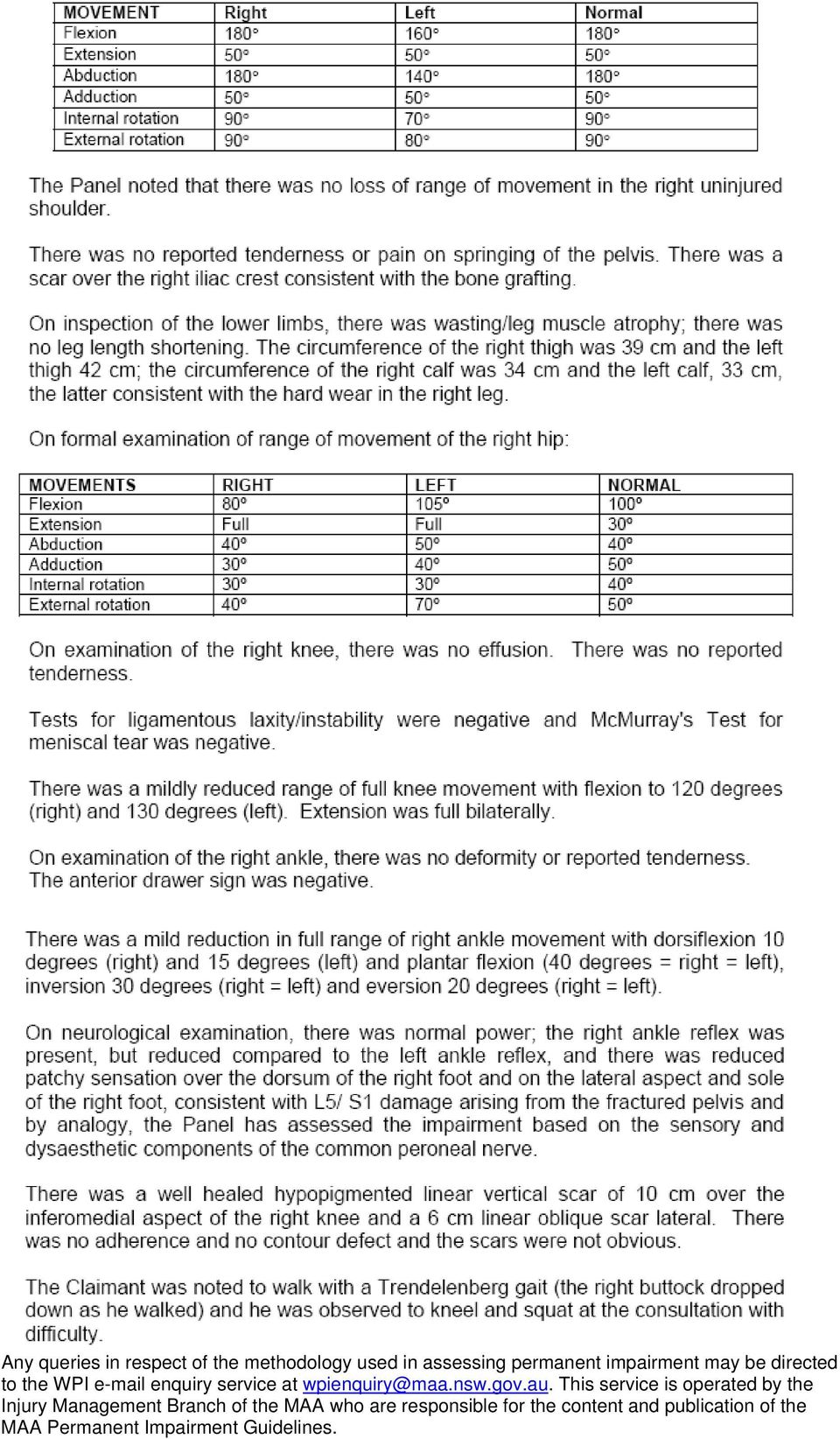
8 This matter was subject to review by a Medical Review Panel. These are the Review Panel s findings. Claimant s Date of Birth: 13 November 1973 Date of Motor Accident: 10 February 2006 Injuries: Pelvis and sacrum multiple fractures Lumbar spine soft tissue injury Clinical Findings The claimant s gait and lower limb functions were all normal. She was able to squat fully and in a normal fashion although with complaint of low back discomfort. Trendelenburg s tests were negative bilaterally. The slump test was positive with complaint of pulling discomfort in the left buttock. On inspection her hands were clean suggesting she had not been performing heavy tasks with the arms. Otherwise joints were held in normal position. There was no joint swelling, no muscle wasting and no changes of complex regional pain syndrome. There was no leg length discrepancy and no mal-alignment of the thoracolumbar spine. On palpation of the lumbar spine there was no allodynia or inflammation of the skin. There was no guarding over the lumbar spine. There was complaint of tenderness over the right and left sacroiliac joint but no true guarding. There was no coccygeal tenderness. There was no tenderness around the left hip joint. There was tenderness over the right anterior superior iliac crest but no guarding. There was no pain on springing the pelvis. Passive movements of the right hip joint were pain free. Passive movements of the left hip joint and external rotation were associated with complaint of pain. There was no hip joint instability. The straight leg raising test was negative bilaterally. Examination of power and reflexes was normal. Tone was normal in the lower limbs. The Babinski response was down going bilaterally. Sensation testing was normal. Range of motion in the lumbar spine was such that extension was two-thirds normal and left rotation two-thirds normal. Other movements were normal. Measurement of the leg lengths was equal. Measurement of the limb circumferences was equal. Range of motion in the hips was as follows: HIP Measurement RIGHT Measurement LEFT Flexion Extension Full Full

9 Internal Rotation External Rotation Abduction Adduction The most recent x-rays of the pelvis and sacrum, dated 11 January 2007, were carefully reviewed. These x-rays showed that the fractures had united without displacement. Panel Decision The pelvic and sacral fractures are assessed with reference to section 3.4, page 131 AMA4 Guides The injuries to the lumbar spine is assessed with reference to the Diagnosis Based Estimate (DRE) method. The whole person permanent impairment of the injuries caused by the accident was calculated as follows: Pelvis and sacrum multiple fractures The multiple fractures have healed without displacement and without residual signs. The panel noted the asymmetric ranges of movement at the hips and concluded that this was not due to the pelvic fractures because of the nature of these fractures. Therefore, with reference to section 3.4, page 131 AMA4 Guides, the permanent impairment due to these injuries is 0% WPI. Lumbar spine soft tissue injury The lumbar spine injury (injury to the lumbosacral spine) is assessed with reference to the Diagnosis Related Estimate method. The claimant has asymmetric loss of range of motion (dysmetria) with reference to the lumbosacral spine, and therefore DRE Lumbosacral Category II (5% WPI) is the appropriate evaluation. There are no symptoms or signs, that are currently present, that justify assessment of DRE III in this spinal region. Body Part or System 1. Pelvis and sacrum multiple fractures 2. Lumbar spine soft tissue injury: DRE II AMA Guides/ MAA Guidelines References (chapter/ page/table) Chapter 3, section 3.4, page 131 (AMA4) Chapter 3, page 102 (AMA4) Stabilised (YES/NO) * %WPI = percentage whole person impairment Current %WPI* %WPI* from pre-existing OR subsequent causes Yes Yes %WPI* due to motor accident Determination Regarding the Degree of Whole Person Impairment of the Injured Person as a Result of the Injuries Caused by the Motor Accident

10 The total percentage whole person permanent impairment for assessed injuries caused by the motor accident is 5%. Therefore the total whole person impairment is not greater than 10%.

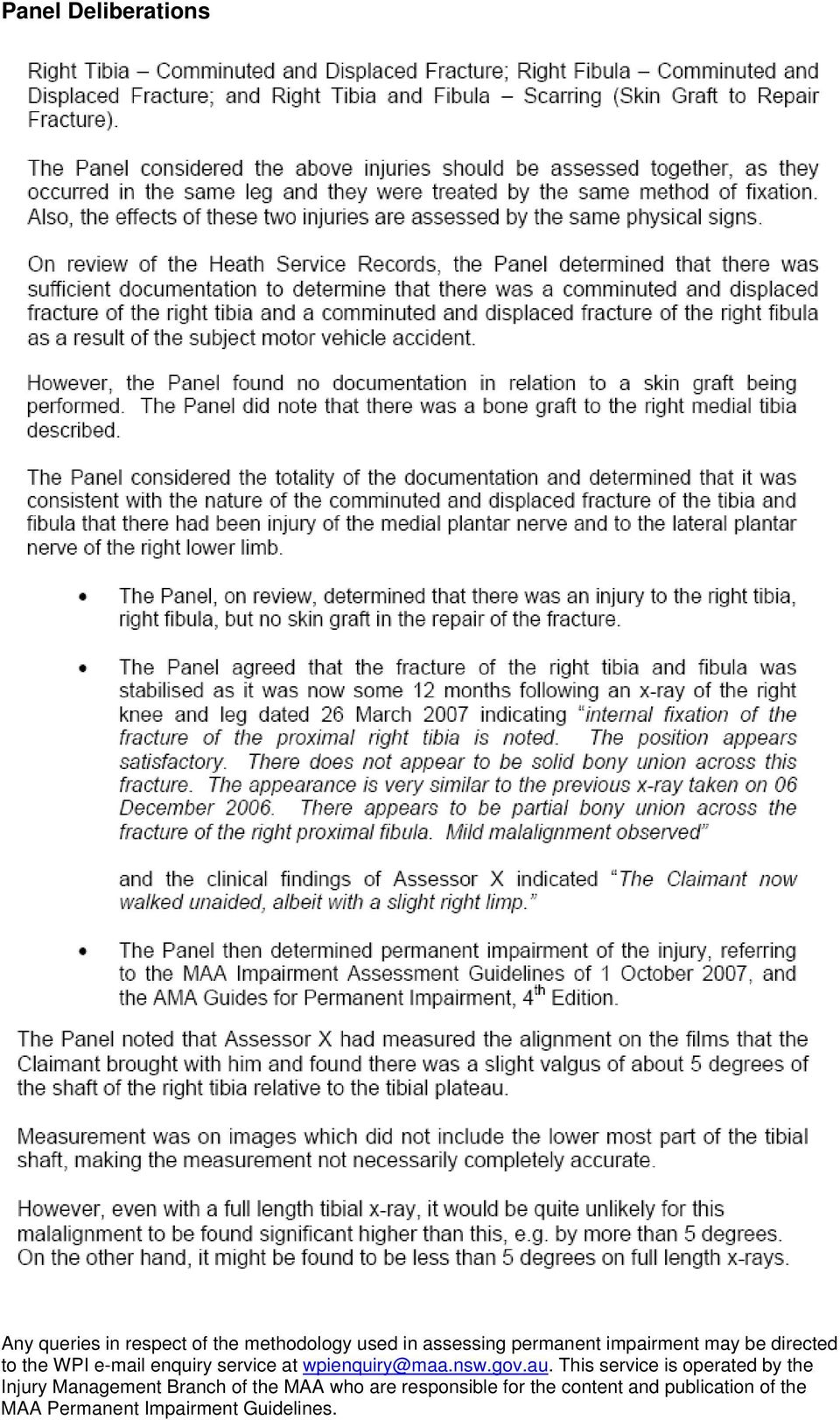
11 This matter was subject to review by a Medical Review Panel. These are the Review Panel s findings. Claimant s Date of Birth: 17 April 1946 Date of Motor Accident: 6 June 2006 Injuries: Clinical Findings

12
13 Panel Deliberations
14

15

16

17 Panel Decision

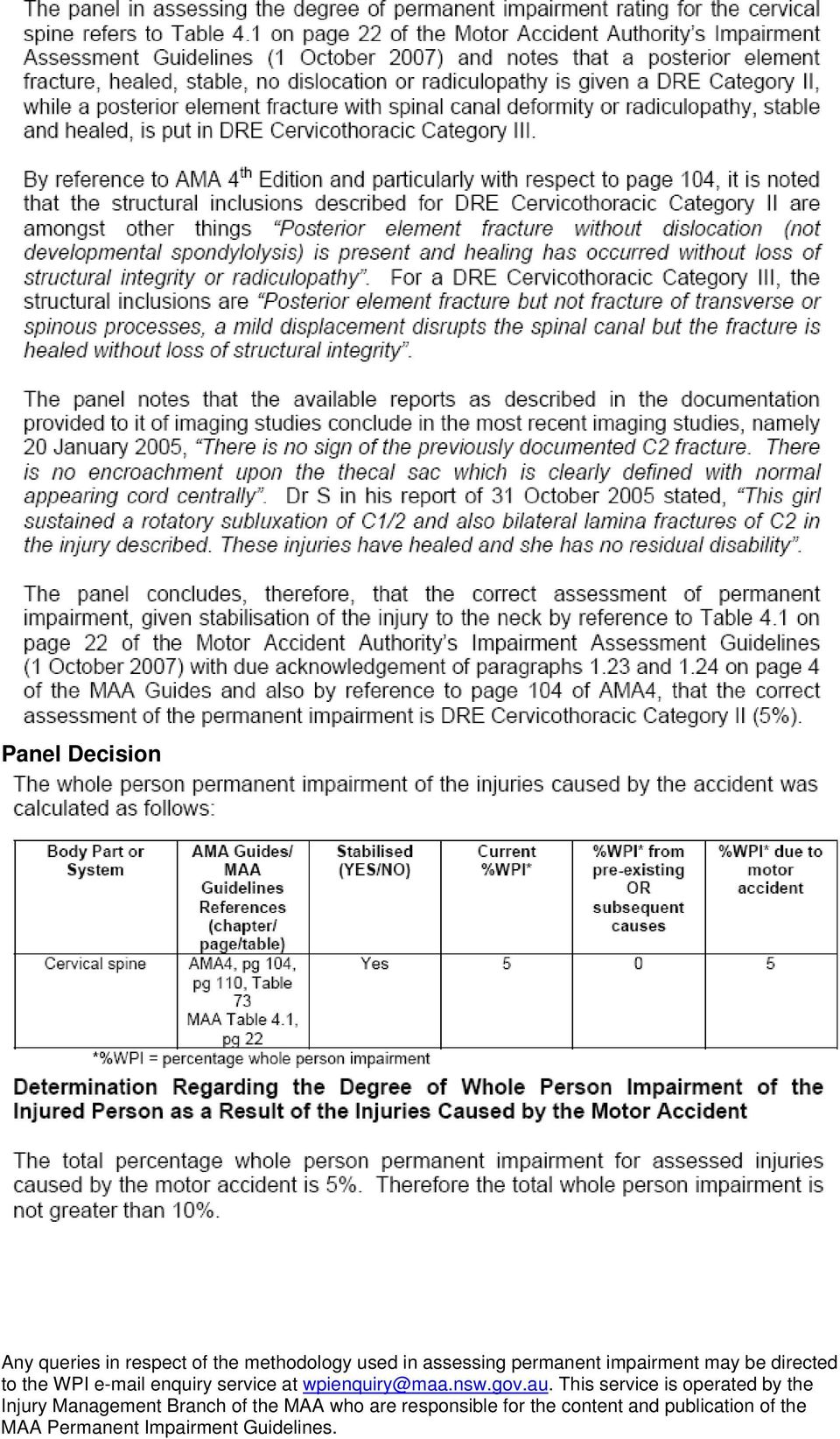
18 This matter was subject to review by a Medical Review Panel. These are the Review Panel s findings. Claimant s Date of Birth: 26 September 1999 Date of Motor Accident: 12 July 2003 Injuries: Cervical spine fracture of spine with displacement Panel Findings

19 Panel Decision
20 This matter was subject to review by a Medical Review Panel. These are the Review Panel s findings. Claimant s Date of Birth: 22 January 1961 Date of Motor Accident: 17 September 2002 Injuries: Cervical spine Thoracic spine Lumbar spine Clinical Findings Cervical spine - disc bulge and protrusion The panel was of the opinion that it would be appropriate to list this injury as Cervical spine soft tissue injury as there was no clear evidence to indicate that a disc bulge and protrusion resulted from the subject accident. The panel noted that the clinical findings reported by Assessor X, namely evidence of asymmetrical neck movement, fulfilled the criteria for Cervicothoracic DRE Category II with 5% whole person impairment. Thoracic spine - disc bulge and protrusion, loss of the anterior height of vertebrae, anterior wedging of T8 vertebral body The panel was of the opinion that it would be appropriate to list this injury as Thoracic Spine anterior wedge compression fracture as there was no clear evidence to indicate that a disc bulge and protrusion resulted from the subject accident. The panel noted that the clinical finding reported by Assessor X, namely evidence of guarding in the right para-thoracic muscles, fulfils the criteria for Thoracolumbar DRE Category II with 5% whole person impairment. The panel also noted that review of the x-rays of the thoracic spine dated 30 January 2004 and 23 June 2004 revealed evidence of a compression fracture of the T8 vertebra with less than 25% compression (according to the method advocated at Item 4.37 of the MAA Guidelines) which also fulfils the criteria for Thoracolumbar DRE Category II with 5% whole person impairment. Lumbar spine - disc bulge and protrusion, fractured vertebrae The panel was of the opinion that it would be appropriate to list this injury as Lumbar spine soft tissue injury as there was no clear evidence to indicate that a disc bulge and protrusion or a vertebral fracture resulted from the subject accident. The panel noted that the clinical findings reported by Assessor X, namely evidence of asymmetrical lower back movement and guarding in the right para-lumbar muscles fulfils the criteria for Lumbosacral DRE Category II.

21 The panel noted that Assessor X had found no objective evidence of radiculopathy in relation to the upper or lower extremities as defined in the MAA Guidelines (Item 4.28 page 27). Panel Decision The whole person permanent impairment of the injuries caused by the accident was calculated as follows: Body Part or System 1. Cervicothoracic spine 2. Thoracolumbar spine 3. Lumbosacral spine AMA Guides/ MAA Guidelines References (chapter/ page/table) AMA4: Para 3.3h, Page 104 MAA: Pages 21 to 29 AMA4: Para 3.3i, Page 106 MAA: Pages 21 to 29 AMA4: Para 3.3g, Page 102 MAA: Pages 21 to 29 Stabilised (YES/NO) Current %WPI* %WPI* from pre-existing OR subsequent causes %WPI* due to motor accident Yes 5% 0% 5% Yes * %WPI = percentage whole person impairment 5% 0% 5% Yes 5% 0% 5% Determination Regarding the Degree of Whole Person Impairment of the Injured Person as a Result of the Injuries Caused by the Motor Accident The total percentage whole person permanent impairment for assessed injuries caused by the motor accident is 15%. Therefore the total whole person impairment is greater than 10%.
22 This matter was subject to review by a Medical Review Panel. These are the Review Panel s findings. Claimant s Date of Birth: 20 March 1972 Date of Motor Accident: 8 February 2006 Injuries: Neck injury C5/6 Left scaphoid fracture Left clavicle fracture Panel Findings Neck
23 Panel Decision
24
25 This matter was subject to review by a Medical Review Panel. These are the Review Panel s findings. Claimant s Date of Birth: 2 April 1985 Date of Motor Accident: 28 December 2003 Injuries: Cervical spine Thoracic spine Lumbar spine Scarring Clinical Findings Cervical Spine: On inspection of the cervical spine, the posture, alignment and contour were normal. There was reported tenderness over the cervical spine centrally and paracentrally on the right and left side and over the shoulder ridges. There was no muscle spasm and no muscle guarding. There was no dysmetria with a symmetric range of neck movements forward flexion and extension, lateral bending to the right and left and rotation to the right and left. Upper Limbs: Examination of the upper limbs was unremarkable. The circumference of the upper arms was 28 cm (right = left) and forearms 23.4 cm (right = left). There were no neurological abnormalities detected in the upper limbs with normal power, tone and deep tendon reflexes. No sensory deficits were elicited. There was a symmetric range of movement of the shoulders. At the extreme ranges of movement of the right shoulder and also the left shoulder, there were reported pains in the neck. The impingement tests were negative and there was no crepitus found in the shoulder joints. On further enquiry at the clinical examination, she did not describe non-verifiable radicular symptomatology in the upper limbs. Back: On inspection of the back, the posture, alignment and contour were normal. There was reported tenderness over the lower lumbar spine but not over the thoracic spine. There was no muscle spasm and no muscle guarding in the thoracic or lumbar spine. There was no dysmetria in the thoracic or lumbar spine with two-thirds normal range of flexion and extension and symmetric lateral bending to the right and left and symmetric rotation. Lower Limbs: There were no neurological abnormalities detected in the lower limbs with normal power, tone and deep tendon reflexes. No sensory deficits were elicited. The circumference of the thighs was 47cm (right) and 46.5cm(left) and calves 34cm (right
26 = left). Straight leg raising was to 80 degrees on each of the right and left side with a negative stretch test. On further enquiry in relation to the nature of her symptomatology in the lower limbs, the symptomatology that she described, was not of a non-verifiable radicular nature. On formal examination of gait, she walked normally and on her heels, toes and heeltoe and made a normal squat. Scarring: On examination of the scarring, there was a well healed hypertrophic scar of 1.5 cm x 0.5 cm with some slight colour difference over the posterior aspect of the right shoulder. There was no adherence and no contour defect. There was a well healed scar of 2.5 cm x 2 mm over the patellar tendon of the right knee. There was no contour defect and no adherence. There was some punctate scarring over the right foot which was not easily distinguishable and she indicated that she was tanned following a holiday. Panel Decision Neck: The Panel confirmed that there was a history of injury and pain in the neck but no clinical differentiators such as muscle spasm, muscle guarding, non-uniform loss of spinal motion (dysmetria) and no non-verifiable radicular complaints (see paragraph 4.17, page 26, of the MAA Impairment Assessment Guidelines of 01 October 2007) and no clinical radiculopathy and concluded that there was a DRE Impairment Category Rating I of the Cervicothoracic Spine which translates to a 0% Whole Person Impairment under Table 73, page 110, of the AMA 4 Guides. Thoracic spine: The Panel considered the examination findings noted above and particularly it was noted that there was no reported symptomatology now in the thoracic spine, no clinical signs of injury such as muscle spasm, muscle guarding and dysmetria and determined that the thoracic spinal injury had resolved. Lumbar Spine: The Panel considered the examination findings noted above and determined that there was a history of injury, pain in the lumbar region but no significant clinical differentiators no muscle spasm, no muscle guarding, no dysmetria, and no nonverifiable radicular symptomatology and no clinical radiculopathy and determined that there was a DRE Impairment Category Rating I of the Lumbosacral Spine which translates to a 0% Whole Person Impairment under Table 72, page 110, of the AMA 4 Guides. Scarring Laceration right leg, laceration left leg, embedded glass right foot: The scars were considered to be well healed but it was noted that the Claimant was conscious of the scars, there was some minor colour contrast with the surrounding skin, and the scars were mildly hypertrophic. The anatomic location was visible with usual clothing and there was minor contour defect but no effect on any activities of daily living and no treatment or intermittent treatment required and no adherence and thus determined a 1% Whole Person Impairment for the scarring under the TEMSKI.
27 The following injuries were found to be resolved and give rise to no assessable impairment: Thoracic spine. The whole person permanent impairment of the injuries caused by the accident was calculated as follows: Body Part or System AMA Guides/ MAA Guidelines References (chapter/ page/table) 1. Cervical spine Chapter 4 MAA Guidelines 1/10/07, Chapter 3.3 AMA 4 Stabilised (YES/NO) Current %WPI* %WPI* from pre-existing OR subsequent causes %WPI* due to motor accident Yes 0% Nil 0% 2. Lumbar spine Chapter 4 MAA Yes Guidelines 0% Nil 0% 1/9/05, Chapter 3.3 AMA 4 3. Scarring TEMSKI Yes 1% Nil 1% * %WPI = percentage whole person impairment Determination Regarding the Degree of Whole Person Impairment of the Injured Person as a Result of the Injuries Caused by the Motor Accident The total percentage whole person permanent impairment for assessed injuries caused by the motor accident is 1%. Therefore the total whole person impairment is not greater than 10%.
28 This matter was subject to review by a Medical Review Panel. These are the Review Panel s findings. Claimant s Date of Birth: 6 October 1988 Date of Motor Accident: 15 November 2004 Injuries: Thoracic spine fractures T11 and T12 Clinical Findings The claimant s plain lumbosacral spine x-ray dated was made available and distributed to each of the panel members. This was only a lateral film. After considerable discussion it was agreed amongst the panel members that the clear cut superior and inferior borders of T11 and T12 and the depressed superior margins of these two vertebrae were consistent with compression fractures and were not consistent with the irregular superior and inferior vertebral body margins and the wedge shape of the vertebral body of lateral view characteristic of Scheuermann s Disease. The panel also considered that the below listed measurements also confirmed compression fractures of T11 and T12 vertebrae:- Vertebra Posterior Height Central Height Anterior Height T11 33cm* 23cm 24cm T12 33cm 25cm 25cm L1 35cm 31cm 33cm *The panel was able to confirm this height by the use of very bright illumination of this area and appeared to be consistent with extrapolation of the more clearly visible parts of superior and posterior border lines. Panel Decision On the basis of the above assessment of the forwarded lateral lumbar spinal x-ray film dated it was the panel s opinion that the claimant had sustained compression fractures of T11 and T12 in the motor accident on the previous day The panel concluded that in the presence of two thoracic vertebral body compression fractures that the claimant was to be assessed as suffering multilevel structural compromise (MAA Impairment Assessment Guidelines, 1 st October, 2007, Item 4.33, Page 28) and that this attracts a thoracolumbar DRE Category IV classification (MAA Impairment Assessment Guidelines, 1 st October, 2007, Item 4.40, Page 28) as there was no evidence of radiculopathy. In accordance with AMA 4, Table 74, Page 3/111, Section 3.3i, Page 3/106 the claimant is assessed as having a permanent 20% whole person impairment.
29 The whole person permanent impairment of the injuries caused by the accident was calculated as follows: Body Part or System 1. Thoracolumbar spine fractures T11 and T12 AMA Guides/ MAA Guidelines References (chapter/ page/table) MAA Impairment Assessment Guidelines, 1 st October, 2007, Items 4.33 and 4.40, Page 28, AMA 4, Table 74, Page 3/111, Section 3.3i, Page 3/106 Stabilised (YES/NO) * %WPI = percentage whole person impairment Current %WPI* %WPI* from pre-existing OR subsequent causes Yes 20% 0% 20% %WPI* due to motor accident Determination Regarding the Degree of Whole Person Impairment of the Injured Person as a Result of the Injuries Caused by the Motor Accident The total percentage whole person permanent impairment for assessed injuries caused by the motor accident is 20%. Therefore the total whole person impairment is greater than 10%.
30 This matter was subject to review by a Medical Review Panel. These are the Review Panel s findings. Claimant s Date of Birth: 11 May 1987 Date of Motor Accident: 13 May 2005 Injuries: Left knee chondromalacia patella Back compression fractures of 5 th, 6 th and 7 th thoracic vertebrae Panel Decision Left Knee The panel noted retro-patella pain and crepitus of the left knee. The panel concluded that the correct assessment for the left knee was 2% whole person impairment from the footnote of Table 62 of the 4 th Edition of the AMA Guides. Thoracic spine The panel noted the chest x-ray report dated 13 May 2005, which stated there is a suggestion of a significant acute compression fracture of the body T7 with loss of height anteriorly in the order of 25 to 30%. There is also the suggestion of bioconvexity and slight anterior depression of the bodies of T5 and T6. The panel had reviewed the subject chest x-ray individually and agreed that there was a 25% compression fracture of the body of a mid thoracic vertebra (presumably T7). The anterior height of the vertebral body was 18mm compared with 24 mm for the vertebrae below. Due to the poor clarity of the x-rays it was not possible to accurately measure the vertebrae above. The panel noted that it was difficult to accurately assess the level of the fracture due to poor clarity of the x-ray view. The panel noted that there was some minor irregularity of the two vertebral bodies above the compression fracture but was not able to confirm fractures at these levels. The panel could see no evidence of significant Scheuermann s disease in the thoracic spine. The panel noted the CT scan of the thoracic spine report dated 19 May The report states there have been compression fractures of the anterior superior end plates of T5, T6 and T7. The most marked compression is in T6. The panel was unable to review the CT scan as it has apparently been lost. The panel noted though that the report supported compression fractures of the mid thoracic spine. The panel could see no reason to dispute the findings of the specialist radiologist. The panel reviewed the thoracic spine x-ray dated 11 October 2006 and agreed that there was a compression fracture in the mid thoracic spine (presumably T7) of 25%. Again it was difficult to confidently ascertain the exact level of the fracture due to the clarity of the x-rays. The panel was not able to confirm fractures to any other thoracic vertebrae even though some irregularity was noted to the vertebral body directly
31 above the fractured level. There was no evidence of significant Scheuermann s disease in the x-rays. The panel considered that on the evidence reviewed that the thoracic spine injury was either DRE III or DRE IV. The compression fracture of 25% at T7 (as a structural inclusion) would give an assessment of DRE III (15% WPI). The panel believed though that the CT report and the subsequent medical report were sufficient to support the probability of compression fractures at 3 levels. In this instance the MAS Permanent Impairment Guidelines (1 October 2007) state in clause 4.33 Multilevel structural compromise is to be interpreted as fractures of more than one vertebra. The panel concluded that the correct assessment of the thoracic spine was DRE IV from Table 74 of the 4 th Edition of the AMA Guides (20% WPI). The panel concluded that the combined permanent impairment assessment of all injuries from the subject motor accident was 22%. The whole person permanent impairment of the injuries caused by the accident was calculated as follows: Body Part or System AMA Guides/ MAA Guidelines References (chapter/ page/table) 1. Thoracic spine Chapter 3, Table 74 (AMA Guides) and clause 4.33 (MAA Guides) 2. Left knee Chapter 3, Footnote Table 62 Stabilised (YES/NO) * %WPI = percentage whole person impairment Current %WPI* %WPI* from pre-existing OR subsequent causes %WPI* due to motor accident Yes Yes Determination Regarding the Degree of Whole Person Impairment of the Injured Person as a Result of the Injuries Caused by the Motor Accident The total percentage whole person permanent impairment for assessed injuries caused by the motor accident is 22%. Therefore the total whole person impairment is greater than 10%.
32 Injuries: Compression fractures L1 and L2 At time of the accident the male claimant was in his mid thirties and had no history of problems of his lumbar spine. He was travelling on his motor bike and was hit from behind by another vehicle. The claimant recalls being thrown in the air and landing on the ground. The claimant stated he temporarily lost consciousness. He complained that he experienced low back pain. Pain persisted and a few days after the accident he saw his GP who arranged X-rays of the lumbar region. He was initially advised that there was no fracture. The claimant had continuing pain in the lumbar region for which he took regular strong pain relief. The claimant then underwent a CT scan of the lumbar spine in which revealed compression fractures of L1 and L2. Clinical Examination The assessor confirmed that the CT scan of the lumbar spine dated November 2007 showed an old healing wedge compression fracture of the L1 and L2 vertebral body without complication. A CT scan of the lumbar spine taken in June 2008 also confirmed the compression fractures at L1 and L2. There were no plain films available for review. The measurements of the vertebral bodies, measured on the CT scan dated June 2008 were as follows:- Vertebra Anterior Posterior Border- Height Saggital view T12 8mm 8mm L1 6mm 8mm L2 7mm 8mm L3 8mm 8mm This results in a compression fracture of 25% at L1 and 13% at L2 (rounding). Impairment Evaluation The assessor determined that the Lumbar spine - compression fractures of L1 and L2 was caused by the MVA of August He also noted that the compression fractures of L1 and L2 had stabilised. The fractures had united and there had been no change in the claimant s clinical condition in the past 3 months. The assessor determined that the claimant had sustained a multilevel structural compromise due to the compression fractures at L1 and L2. The assessor assessed the claimant as being in a lumbosacral category 4 in the diagnosis related estimate category (DRE) (reference Table 4.1, Chapter 4, page 22 in the Permanent Impairment Guidelines 1/10/2007).
33 A DRE Lumbosacral Category 4 results in a 20% WPI (reference Chapter 3, page 102 in AMA4). If the claimant had only suffered one compression fracture of 25% to the L1 vertebrae then he would have been placed in lumbosacral category 3 in the DRE category for which a descriptor is vertebral body compression fracture 25 50% (reference Table 4.1, Chapter 4 page 22 in the Permanent Impairment Guidelines 1/10/2007). A DRE Lumbosacral Category 3 results in a 10% WPI (reference Chapter 3, page 102 in AMA4).
34 This matter was subject to a review by a Medical Review Panel. These are the Review Panel s findings. Injuries: Neck severe strain Lower Back severe strain Right Wrist severe strain The claimant was involved in a MVA when the motor vehicle he was driving was struck from behind by another car and was written off as a result. The claimant was taken by ambulance to Hospital where he was kept under observation for a week. X- Rays were carried out and concern was expressed about possible spinal damage. Clinical Findings: On re-examination the claimant was observed to move somewhat awkwardly when sitting and when getting up from a sitting position but to be able to walk without difficulty. On formal examination of his active ranges of lumbar spinal motion all of these ranges were noted to be quite markedly restricted and it was particularly noted that trunk tilting and trunk rotation to the left was significantly more restricted than the right. Straight leg raising was restricted by pain in his back when prone to 35 in the right lower limb and 30 in the left lower limb. Whilst confirming the claimant s history and current symptoms he was noted to have very much freer ranges of neck motion in all directions than when subsequently formally examined at which time on repeated assessment he had very variable degrees of restrictions to all of these ranges of active motion. Panel Deliberations Neck Severe Strain After examining the claimant s range of movements and examining the medical evidence the Panel agreed that the claimant had a DRE Cervicothoracic Impairment Category 1 with a permanent 0% whole person impairment. Right Wrist Severe Strain The Panel considered that there was no abnormal physical findings on examination of his right wrist as his uninjured left wrist had identical ranges of motion. He was therefore assessed as having a permanent 0% whole person impairment with respect to the injury to the right wrist. Lower Back Severe Strain The Panel determined that as the claimant identified pain and numbness in his left leg associated with his back pain and that there was no contemporaneous evidence of a discrete injury to his left leg that the listed injury to the left leg required to be assessed in conjunction with his back injury. At the re-examination of the claimant there was evidence of asymmetrical restriction to the ranges of motion in his lumbar spine, somewhat variable restriction to the range of the straight leg raising in both his
35 lower limbs, absence of his left ankle jerk, muscle wasting in both his left thigh and left calf and sensory alteration in a distribution in the left lower limb which was predominantly in the distribution of L5 and S1 dermatome. On the basis of these findings it was the Panel s determination that the claimant had a DRE Lumbosacral impairment category III (due to radiculopathy) with a permanent 10% whole person impairment. WPI related to previous injury (10% - 5% = 5%) The Panel also determined that the observed lower lumbar midline surgical scar confirmed the history of previously having undergone discectomy but without any evidence of subsequent radiculopathy and, as such, the claimant had a pre-existing DRE Lumbosacral Impairment Category II with a permanent 5% whole person impairment. Subtracting the level of pre-existing whole person impairment from his current level of permanent impairment the Panel determined the claimant to have an overall permanent 5% whole person impairment for lumbosacral impairment caused by the MVA. Panel Decision The degree of permanent impairment of the injured person as a result of the injury to the neck severe strain, lower back severe strain to incorporate left leg severe strain, right wrist severe strain, caused by the accident, is not greater than 10%.
36 This matter was subject to a review by a Medical Review Panel. These are the Review Panel s findings. Injuries: Neck injury C5/6 Sternum fracture Ribs fracture Left Scaphoid fracture Left Clavicle and collar bone dislocation History The claimant was involved in a MVA on his way home from work when he had a head-on collision with another vehicle which had lost control. He was told that he had a fractured sternum and a fractured scaphoid in his wrist. He had problems with his left clavicular joint and also his neck. He required physiotherapy for the injury to his neck and needed a C5/6 fusion in August He had left arm numbness which continued following the fusion. He had previously undergone a C5/C6 disc replacement back in 2002 but claims he had no numbness following that surgery until after the MVA. Clinical Findings With reference to the neck injury the Panel noted that the claimant had a C5/C6 disc replacement in 2002 and recovered well. As a result of the subject MVA he had an anterior cervical fusion at the same level in August The Panel concluded that the original Assessor was correct in assessing the claimant s pre-existing impairment related to the neck injury at 25% WPI. The Panel however disagreed with the findings that the claimant s current injuries were classified as DRE IV. They noted that the original Assessor found neurological abnormalities in the claimant s left upper extremity at the time of examination which included sensory loss in an appropriate spinal nerve root distribution and asymmetry of reflexes. The Panel determined that these findings are consistent with radiculopathy as defined in clause 4.28, page 27 MAA Guidelines. Furthermore the Panel noted that clause 4.40 of the Guidelines state that multilevel structural compromise with radiculopathy is classed as DRE V which is equivalent to 35% WPI. Therefore the Panel determined that the WPI related to the neck injury sustained in the subject MVA was 35% minus 25% for pre-existing injury which equals 10% WPI. Panel Decision The Whole Person Impairment of the injuries caused by the accident was calculated as follows: Neck Injury C5/6: For the reasons outlined above, 35% - 25% = 10%
37 Sternum and Ribs Fracture: These injuries had completely resolved and gave rise to no assessable WPI. Left Scaphoid Fracture: The Panel accepted the original Assessor s assessment of 1% WPI related to this injury, based on a reduced range of movement. Left Clavicle Fracture: The Panel accepted the original Assessor s assessment of 0% WPI related to this injury. The Panel determined the WPI for assessed injuries caused by the subject MVA was 11%.
38 Injury: Whiplash In 2003, the claimant was a 39 year old passenger of a vehicle that was stationary at traffic lights and who sustained a whiplash injury when his vehicle was struck from behind. The claimant initially consulted his GP and was later seen by a specialist who recommended conservative treatment by way of physiotherapy and hydrotherapy whilst undertaking exercises at home. This continued for a little less than one year and he now only continues to take medication. Clinical Examination The claimant s range of movements were limited by voluntary muscle control but the painful tender muscles in the upper right shoulder girdle, in the Assessor s opinion, were significant and were considered as evidence of muscle guarding. Range of motion measurements were recorded as follows: Cervical Spine Flexion 30 Extension 0 Lateral Flexion 5 Rotation Rt 30 Rotation Lt 30 Examination of the thoracic spine revealed no tenderness. There was symmetrical range of movement in the thoracic spine with the thoracic movements being approximately half normal range but without muscle guarding or spasm. This is consistent with degenerative change. The movements are all symmetrical. The chest expansion is reduced but symmetrical and there was very minimal thoracic spinal extension on full inspiration, being consistent with the absence of muscle guarding or spasm noted clinically. The claimant presented with x-ray appearances which were consistent with a constitutional and degenerative condition and which do not carry features which would normally be present in traumatic fractures of the vertebral bodies. Diagnosis and Causation The Assessor determined that the claimant sustained a soft tissue injury to the cervical spine (with aggravation of previously asymptomatic degenerative change) and a soft tissue injury to the thoracic spine (with aggravation of a previously symptomatic degenerative/developmental condition) due to the subject motor vehicle accident.
39 Impairment Evaluation The Assessor found at the cervical spine there was no asymmetric loss of range of motion, but muscle guarding was deemed to be present, particularly on the lateral aspect of the neck and upper right shoulder girdle. There were no neurological changes in the upper extremities and therefore no evidence of radiculopathy. The claimant was assessed according to Tables 70 and 73, pages 108 and 110 in the AMA 4 Guides, as DRE Cervico thoracic Category ll. This equates to 5% PI. At the thoracic spine there was no asymmetric loss of range of motion and no muscle guarding or spasm detectable on examination. The claimant did not describe radicular symptoms in the trunk or lower extremities. There was no evidence of nerve root damage, therefore no detectable radiculopathy. The claimant was assessed according to Tables 70 and 74, pages 108 and 111 in the AMA 4 Guides, as DRE Thoraco-lumbar Category l. This equates to 0% PI. The total permanent impairment was 5%.
40 This matter was subject to a review by a Medical Review Panel. These are the Review Panel s findings. This case study provides a practical example of how a Review Panel dealt with the assessment of spinal spacing devices, and specifically whether this equated to spinal stabilisation and therefore multilevel structural compromise. Injury: Lumbar Spine A 36 year old man was driving a truck that hit a bump in the road that threw him up, and as he came down the truck hit another bump and he forcibly made contact with the seat as the vehicle came up to meet him. A CT scan revealed a large central and right sided disc protrusion at L5/S1 and a mild bulge at L4/5 level. He eventually had surgery, which led to resolution of the right leg pain. However, back pain continued, radiating to the left buttock and left testicle and down the left leg. The MAS Assessment At the assessment, the claimant reported his current symptoms were constant pain radiating from the low back to the left buttock, thigh, calf and foot. He reported weakness in the left leg with occasions when the leg gave way. He still had some hesitancy initiating urination. He occasionally used a walking stick. Examination revealed some loss of lumbar extension (arching the back backwards), no evidence of spasm, normal power but some sensory impairment in the left lower leg and foot, no muscle wasting and absent left ankle jerk. Nerve tension tests were normal. The Medical Assessor determined the L5/S1 disc prolapse with radiculopathy was caused by the motor accident. The Medical Assessor noted the claimant underwent decompression of the L5/S1 disc as well as some surgery at the L4/5 with posterior stabilisation at L4/5/S1, but not an interbody fusion. The Medical Assessor determined DRE IV in accordance with clause and Table 4.1, noting surgery at two levels with radiculopathy. The total assessed WPI was therefore 20%. The Review Panel The Panel considered all the available evidence and decided that further information was necessary to clarify the nature of the posterior stabilisation device used in the operation and how it impacted upon the anatomy of the spine. They requested the operation report for the spinal surgery, the associated nurse s operating report containing the details specifically identifying the product used as the stabilisation device (including the sticky labels attached to the notes as product identification data), and all available imaging studies of the lumbar spine.
41 The information requested was received and the Panel reconvened. The Panel noted the spacing devices used between L4/5 and L5/S1 were called X- Stop. The Panel s research on this device shows that it is a distraction device which allows limited extension but allows normal flexion and has no significant effect on rotation or lateral motion of the spine. The literature reviewed supported the common thinking of the Panel that this does not constitute a spinal fusion. The product advisory information regarding X-Stop indicates that it is not considered as a spinal fusion device. The Panel noted the injury to the lumbar spine was associated with asymmetry of reflexes and reproducible sensory loss anatomically localised to an appropriate spinal nerve root. As there were two signs of radiculopathy, the Panel concluded radiculopathy was present, in accordance with clause 4.28 of the MAA Guidelines (p.27). The Panel assessed the injury to the lumbar spine impairment at DRE Lumbosacral Category III, Radiculopathy (Table 72, page 3/110 and page 3/102 of the AMA 4 Guides). This equates to 10% WPI.
42 This matter was subject to a review by a Medical Review Panel. These are the Review Panel s findings. Injuries: Lumbar spine aggravation of pre-existing condition Cervical spine soft tissue injury Left shoulder rotator cuff strain Panel Deliberations
43 Panel Decision
44 This matter was subject to a review by a Medical Review Panel. These are the Review Panel s findings. Injuries: Back musculoligamentous damage Neck musculoligamentous damage Right hip fracture, incorporating right leg fracture Right knee musculoligamentous damage Right psoas muscle tear to muscle and resultant atrophy Sciatic nerve right sided sciatic neurapraxia Clinical Findings The claimant had continuing complaints of pain which was constant and affected the right lateral thigh and posterior right calf; and was present intermittently in the right shin and he had a bruising type pain in the right gluteal muscles. He also noticed intermittent pain in the medial left thigh like a prick of needles going in but he said that he had never mentioned this before so he was informed that it could not be assessed. He said when walking, the ball of his right foot felt like he was walking on a rock or a bunched up sock in his shoe and interfered with walking. He had partial numbness around the scar in the proximal lateral thigh and irritation across the front of the right ankle. He has difficulty lifting his right leg to go up steps and he tends to trip over his toes and he has to lift his right leg with his hands in and out of the car. He can t run without hanging onto something because of thigh weakness. He can t lie on his right side because of discomfort. He can no longer ride distances on his motorbike and can t polish and do mechanical work on his motorbike. He was taking Nurofen Plus and Panadeine Forte. Examination His height was 175 cms and weight 99.2 kilos. Cervical spine: no guarding or spasm and no tenderness. The grip was strong in both hands and neurology of the upper limbs was normal. Flexion 40 Extension 40 Rotation to the right 60 Rotation to the left 60 Lateral bending to the right 35 Lateral bending to the left 35 Lumbar spine: lordosis was preserved and there was no muscle guarding or spasm. There was no tenderness. He stood erect with normal alignment of the lower extremities. Reflexes, power and sensation in the lower limbs were normal. Straight leg raising whilst supine was 90 on the left and 45 on the right with complaint of right hip pain whilst sitting straight leg raising was 90 bilaterally with negative flip test. It was concluded that limitation of straight leg raising whilst supine was caused
45 by the complaint of right hip pain rather than being a response indicating sciatica. He was able to stand on his toes and heels, complaining of hip discomfort, however he showed normal strength on these movements. Flexion 85 fingertips 17 cm from floor Extension 30 Rotation to the right 40 Rotation to the left 40 Lateral bending to the right 30 Lateral bending to the left 30 Right and left hips: Hip Movements Active ROM Measured RIGHT Flexion Extension 0 10 Abduction Adduction Internal Rotation External Rotation Active ROM Measured LEFT There was significant right psoas weakness. There was no weakness elsewhere in the sciatic nerve distribution. The right and left knees showed full range of movement. There was a well healed scar 16 cms in length on the lateral proximal two-thirds of the right thigh. Thigh girths: right equals 48.5, left equals 48 cms. Leg girths: right equals 40.5, left equals 39.5 cms. Sensation testing showed partial decreased sensation around the scar on the lateral right thigh and partial decreased sensation lateral right leg distal to the fibular head with normal sensation in the mid leg and then further partial decreased sensation in the distal one-third of the right posterior leg. Sensation was normal in the ball of the foot but there was hyperaesthesia under the right heel. Radiology was reviewed consisting of ultrasound Doppler scan of the right leg checking for deep vein thrombosis, MRI scan of the lumbar spine, x-ray of the hip, MRI of the hip, CT scan of the hip and an x-ray of the right leg and femur. A nerve conduction study concluded there was electrophysiological evidence of a high right sciatic neuropathy proximal to hamstring innervation that affects the peroneal component predominantly and is axonal in nature rather than a lumbar plexopathy or L5 radiculopathy. Panel Deliberations Based on the examination findings, the Panel assigned DRE Category 1 to the Lumbosacral Spine symptoms of injury present but no guarding descriptors present - and found that the neck and right knee injuries had resolved with no assessable impairment. There was impaired psoas motor function with Grade 4 motor weakness of hip flexion giving 2% Whole Person Impairment from Table 39 from psoas weakness. There was no motor weakness demonstrable elsewhere in
46 the sciatic nerve innervated muscles of the right lower extremity. Flexion of 70 in the right hip gave 4% Whole Person Impairment from AMA 4 Table 40, page 78 and was the greatest impairment from loss of active range of motion in the hip (MAA Chapter 3, clause 3.18, page 15) Referring to Table 68 there was not uniform reduction of sensation in the entire sciatic nerve distribution. There was partial sensory loss in the common peroneal nerve distribution graded as 2 from Table 11a, that is 25% sensory deficit. 25% of 2% maximum sensory loss from common peroneal nerve from Table 68 is 0.5% rounded to 1% WPI. There was also Grade 2 or 25% sensory deficit in the medial calcaneal nerve territory in the right foot which is part of the tibial nerve and 25% of 5% from Clause 3.35 MAA Guides Chapter 3 page 17 gives 1% Whole Person Impairment. Alternatively, as there were aspects of both common peroneal and tibial nerve territories affected by partial sensory loss, an equivalent is to use the sciatic nerve sensory component to calculate the loss and one-quarter (25%) of 7% representing total sensory loss of the sciatic nerve is 1.75% rounded to 2% WPI. There was no motor deficit in the sciatic nerve distribution. Combining 4% x 2% x 2% using the Combined Values Chart gives a total of 8% whole person impairment. The discomfort noted in the ball of the foot by the claimant did not attract a rating for sensory impairment as sensation was normal in this part of the right foot. The sensory impairment associated with the scar was not widespread enough to be attributable to peripheral nerve injury and it has been assessed by another Assessor. Panel Decision The degree of whole person permanent impairment of the injuries caused by the accident was calculated as follows: Body Part or System AMA Guides/ MAA Guidelines References (chapter/ page/table) 1. Back MAA Chapter 4, Table 4.1, page 22; AMA 4, Chapter 3, Table 72, page 110 DRE I 2. Neck No assessable permanent impairment Permanent (YES/NO) Current %WPI* %WPI* from pre-existing OR subsequent causes Yes %WPI* due to motor accident
47 3. Right hip/leg MAA Chapter 3, clause 3.18, page 15; AMA 4, table 40, page Right knee No assessable permanent 5. Right psoas muscle 6. Sciatic nerve neurapraxia impairment AMA 4 Chapter 3, Table 39, page 77 Grade 4 AMA 4 Chapter 3, Table 11a grade 2, page 48, Table 68, page 89 * %WPI = percentage whole person impairment Yes Yes Yes Determination Regarding the Degree of Whole Person Impairment of the Injured Person as a Result of the Injuries Caused by the Motor Accident The total percentage whole person permanent impairment for assessed injuries caused by the motor accident is 8%.
48 This matter was subject to a review by a Medical Review Panel. These are the Review Panel s findings. Injuries: Neck musculoligamentous injury Back and left leg failed fusion at L4/5 requiring re-fusion The claimant had a history of low back injury after falling down steps many years ago, culminating in lumbar spine fusion in approximately It was noted that her condition had significantly improved post surgery to the level of playing tennis and running with children. Before the subject accident she was almost completely pain free. Following the motor accident, the claimant was immobilized and reliant upon a wheelchair for several weeks due to concurrent fractures involving the right foot and left wrist. She developed increased back pain some 6-8 weeks post accident once she became ambulant. Her backache did not improve. She was eventually referred to an orthopaedic surgeon who diagnosed damage to the fusion area caused by the accident. She came to further lumbar (L4-S1) fusion in Clinical Evidence The Panel noted that the Assessor s examination findings of the cervical spine were consistent with Cervicothoracic DRE I or 0% WPI. The Panel also agreed with the Assessor that the present WPI of the lumbar spine is 25% (incorporating lumbar fusion and radiculopathy i.e. Lumbosacral DRE V categorization). However, the Panel noted that the Assessor made no deduction for pre-existing Lumbar fusion. In regard to the deduction issue for the lower back, the Panel noted extensive evidence on file of treatment for pre-existing low back pain as follows: GP records in 2001 indicate chronic symptoms in the lower back for which she was taking strong analgesia such as Oxycontin and Celebrex. A Centrelink Treating Doctor s Report dated 11/4/02 noted severe pain needing long-term medication and injections. Treatment to date had included Oxycontin, Sacro Iliac joint injections, other joint blocks and consultation with the Pain Specialist. The claimant was regularly receiving spinal injections (mainly left Sacro-Iliac [SI] joint blocks with local anaesthetic and steroid) for low back pain from Just 2-3 months before the subject motor accident, she had
49 received an injection to the left SI joint, authorized a Pain Physician whom she had been consulting since 2001 for neck and low back pain. The Panel noted specific relevant comments made within various medical reports in relation to the claimant s lower back symptoms prior to the subject motor accident. On the basis of the above information, the Panel concluded that the available documentation provides ample objective evidence of pre-existing symptomatic permanent impairment in the same region (i.e. Lumbar spine) at the time of the accident as mandated by instructions given in Paragraph 1.33 page 6 of the MAA Permanent Impairment Guidelines. More specifically, the claimant was clearly experiencing symptoms in the lower back for which she was receiving injections to the SI joint during the 12 months preceding the subject motor accident. The Panel also discussed whether the treatment interventions received by the claimant (left SI [sacro iliac] joint injections) between 2001 and 2006 was causally related to the initial spinal fusion in approximately The Panel concluded that the serial SI joint injections given during this period were related to symptoms stemming from the initial 1992 lumbar fusion procedure. The Panel noted that injection of pain-relieving medication to the SI joint could provide symptomatic relief of adjacent low back pain by diffusion of medication. It was also noted that the original fusion had permanently altered the lumbar spine biomechanics, placing stress upon adjacent joints including the Sacroiliac which could in turn become pain generators. The Panel noted too that the bone scan performed in 2007 did not demonstrate findings consistent with sacro-iliitis. Essentially, the Lumbosacral spine and pelvis (including the SI joints) function as a single unit due to their close anatomical proximity. Panel Deliberations The Panel agreed that there is 0% WPI of the neck representing DRE I of the Cervicothoracic Spine. The Assessor noted no non-verifiable radicular complaints. His clinical findings did not include dysmetria, muscle guarding, muscle spasm or neurological abnormalities to indicate radiculopathy. The Panel found that DRE I categorization of the Cervicothoracic spine with 0% WPI is appropriate. In regard to WPI of the Lumbar spine: The Panel refers to the instructions given in paragraphs on page 6 of the MAA Guides to Permanent Impairment: If there is objective evidence of pre-existing symptomatic impairment in the same region at the time of the accident, then its value should be calculated and subtracted from the current whole person value. If there is no objective evidence of pre-existing symptomatic permanent impairment, then its possible presence should be ignored...in apportioning spine impairment, first the current spine impairment would be estimated, and then impairment from any preexisting spine problem would be estimated. The estimate for pre-existing impairment
50 would be subtracted from that for the present impairment to account for the effects of the former..pre-existing impairments should not be assessed if they are unrelated or not relevant to the impairments arising from the motor accident. As noted above, the Panel has determined that there is objective evidence of preexisting symptomatic impairment in the lower back at the time of the accident. In this case, WPI for pre-existing symptomatic impairment of the lower back is 20% representing Lumbosacral DRE IV for the initial lumbar fusion procedure in the absence of radiculopathy (paragraphs pages of the MAA Permanent Impairment Guides). There is presently 25% WPI (DRE V) of Lumbosacral Spine due to history of lumbar fusion and addition of persistent left-sided L5 radiculopathy since the subject motor accident (paragraphs pages of the MAA Permanent Impairment Guides). 20% WPI (representing pre-existing symptomatic impairment) is subtracted from the present 25% WPI with residual 5% WPI due to the subject motor accident. Panel Decision There is 0% WPI for the Cervicothoracic spine (neck). There is 5% WPI for the Lumbosacral spine (back) due to the subject motor accident. In summary, there is 5% WPI due to the subject accident. Body Part or System Neck Musculoligamentous injury AMA Guides/ MAA Guidelines References (chapter/ page/table) Permanent (YES/NO) Current %WPI* %WPI* from pre-existing OR subsequent causes Yes 0% Not applicable %WPI* due to motor accident 0% 2 2 Back and left leg- failed fusion at L4-5 requiring refusion Paragraphs page 6 Table 4.1, page 22, paragraphs 4.34 and 4.40 page 28 MAA Guides Yes 25% 20% 5% * %WPI = percentage whole person impairment
51 Determination Regarding the Degree of Whole Person Impairment of the Injured Person as a Result of the Injuries Caused by the Motor Accident The total percentage whole person permanent impairment for assessed injuries caused by the motor accident is 5%. Therefore the total whole person impairment is not greater than 10%.
Upper Limb. The following case studies relate to injuries to the Upper Limb.
 Upper Limb The following case studies relate to injuries to the Upper Limb. More detailed information regarding the assessment of injuries to the upper limb may be found at Chapter 2 of the MAA s Permanent
Upper Limb The following case studies relate to injuries to the Upper Limb. More detailed information regarding the assessment of injuries to the upper limb may be found at Chapter 2 of the MAA s Permanent
SPINE. Postural Malalignments 4/9/2015. Cervical Spine Evaluation. Thoracic Spine Evaluation. Observations. Assess position of head and neck
 SPINE Observations Body type Postural alignments and asymmetries should be observed from all views Assess height differences between anatomical landmarks Figure 25-9 Figure 25-10 Figure 25-11 & 12 Postural
SPINE Observations Body type Postural alignments and asymmetries should be observed from all views Assess height differences between anatomical landmarks Figure 25-9 Figure 25-10 Figure 25-11 & 12 Postural
Closed Automobile Insurance Third Party Liability Bodily Injury Claim Study in Ontario
 Page 1 Closed Automobile Insurance Third Party Liability Bodily Injury Claim Study in Ontario Injury Descriptions Developed from Newfoundland claim study injury definitions No injury Death Psychological
Page 1 Closed Automobile Insurance Third Party Liability Bodily Injury Claim Study in Ontario Injury Descriptions Developed from Newfoundland claim study injury definitions No injury Death Psychological
Gilbert Varela, M.D., Inc 5232 E. Beverly Boulevard Los Angeles, California 90022 Phone: (323) 724-6911 Fax: (323) 724-6915
 724-6911 Fax: (323) 724-6915") Gilbert Varela, M.D., Inc 5232 E. Beverly Boulevard Los Angeles, California 90022 Phone: (323) 724-6911 Fax: (323) 724-6915 September 10, 2007 Law offices of xxxxxxxxx Santa Monica, CA 90405 REGARDING:
Gilbert Varela, M.D., Inc 5232 E. Beverly Boulevard Los Angeles, California 90022 Phone: (323) 724-6911 Fax: (323) 724-6915 September 10, 2007 Law offices of xxxxxxxxx Santa Monica, CA 90405 REGARDING:
IMPAIRMENT RATING 5 TH EDITION MODULE II
 IMPAIRMENT RATING 5 TH EDITION MODULE II THE SPINE AND ALTERATION OF MOTION SEGMENT INTEGRITY (AOMSI) PRESENTED BY: RONALD J. WELLIKOFF, D.C., FACC, FICC In conjuction with: The chapter on the spine includes
IMPAIRMENT RATING 5 TH EDITION MODULE II THE SPINE AND ALTERATION OF MOTION SEGMENT INTEGRITY (AOMSI) PRESENTED BY: RONALD J. WELLIKOFF, D.C., FACC, FICC In conjuction with: The chapter on the spine includes
If you or a loved one have suffered because of a negligent error during spinal surgery, you will be going through a difficult time.
 If you or a loved one have suffered because of a negligent error during spinal surgery, you will be going through a difficult time. You may be worried about your future, both in respect of finances and
If you or a loved one have suffered because of a negligent error during spinal surgery, you will be going through a difficult time. You may be worried about your future, both in respect of finances and
Low Back Injury in the Industrial Athlete: An Anatomic Approach
 Low Back Injury in the Industrial Athlete: An Anatomic Approach Earl J. Craig, M.D. Assistant Professor Indiana University School of Medicine Department of Physical Medicine and Rehabilitation Epidemiology
Low Back Injury in the Industrial Athlete: An Anatomic Approach Earl J. Craig, M.D. Assistant Professor Indiana University School of Medicine Department of Physical Medicine and Rehabilitation Epidemiology
WORKCOVER DIVISION Case No.C12401789 --- S GARNETT MELBOURNE REASONS FOR DECISION ---
 !Undefined Bookmark, I IN THE MAGISTRATES COURT OF VICTORIA AT MELBOURNE WORKCOVER DIVISION Case No.C12401789 ZIVKA SAPAZOVSKI Plaintiff v ONE FORCE GROUP AUSTRALIA PTY LTD Defendant --- MAGISTRATE: S
!Undefined Bookmark, I IN THE MAGISTRATES COURT OF VICTORIA AT MELBOURNE WORKCOVER DIVISION Case No.C12401789 ZIVKA SAPAZOVSKI Plaintiff v ONE FORCE GROUP AUSTRALIA PTY LTD Defendant --- MAGISTRATE: S
A Syndrome (Pattern) Approach to Low Back Pain. History
 Approach to Low Back Pain. History") A Syndrome (Pattern) Approach to Low Back Pain Hamilton Hall MD FRCSC Professor, Department of Surgery, University of Toronto Medical Director, CBI Health Group Executive Director, Canadian Spine Society
A Syndrome (Pattern) Approach to Low Back Pain Hamilton Hall MD FRCSC Professor, Department of Surgery, University of Toronto Medical Director, CBI Health Group Executive Director, Canadian Spine Society
Information on the Chiropractic Care of Lower Back Pain
 Chiropractic Care of Lower Back Pain Lower back pain is probably the most common condition seen the the Chiropractic office. Each month it is estimated that up to one third of persons experience some type
Chiropractic Care of Lower Back Pain Lower back pain is probably the most common condition seen the the Chiropractic office. Each month it is estimated that up to one third of persons experience some type
1 REVISOR 5223.0070. (4) Pain associated with rigidity (loss of motion or postural abnormality) or
 Pain associated with rigidity (loss of motion or postural abnormality) or") 1 REVISOR 5223.0070 5223.0070 MUSCULOSKELETAL SCHEDULE; BACK. Subpart 1. Lumbar spine. The spine rating is inclusive of leg symptoms except for gross motor weakness, bladder or bowel dysfunction, or sexual
1 REVISOR 5223.0070 5223.0070 MUSCULOSKELETAL SCHEDULE; BACK. Subpart 1. Lumbar spine. The spine rating is inclusive of leg symptoms except for gross motor weakness, bladder or bowel dysfunction, or sexual
Avoid The Dreaded Back Injury by Proper Lifting Techniques
 Avoid The Dreaded Back Injury by Proper Lifting Techniques If you ve ever strained your back while lifting something, you ll know the importance of lifting safely. Agenda Introduction About the Back The
Avoid The Dreaded Back Injury by Proper Lifting Techniques If you ve ever strained your back while lifting something, you ll know the importance of lifting safely. Agenda Introduction About the Back The
BACK PAIN: WHAT YOU SHOULD KNOW
 BACK PAIN: WHAT YOU SHOULD KNOW Diane Metzer LOWER BACK PAIN Nearly everyone at some point has back pain that interferes with work, recreation and routine daily activities. Four out of five adults experience
BACK PAIN: WHAT YOU SHOULD KNOW Diane Metzer LOWER BACK PAIN Nearly everyone at some point has back pain that interferes with work, recreation and routine daily activities. Four out of five adults experience
AMA Guides 6 th Edition AADEP SPINE EXAMPLES
 AMA Guides 6 th Edition AADEP SPINE EXAMPLES 1 Questions? James B. Talmage MD, Occupational Health Center, 315 N. Washington Ave, Suite 165 Cookeville, TN 38501 Phone 931-526-1604 (Fax 526-7378) [email protected]
AMA Guides 6 th Edition AADEP SPINE EXAMPLES 1 Questions? James B. Talmage MD, Occupational Health Center, 315 N. Washington Ave, Suite 165 Cookeville, TN 38501 Phone 931-526-1604 (Fax 526-7378) [email protected]
Contact your Doctor or Nurse for more information.
 A spinal cord injury is damage to your spinal cord that affects your movement, feeling, or the way your organs work. The injury can happen by cutting, stretching, or swelling of the spinal cord. Injury
A spinal cord injury is damage to your spinal cord that affects your movement, feeling, or the way your organs work. The injury can happen by cutting, stretching, or swelling of the spinal cord. Injury
Case Studies Updated 10.24.11
 S O L U T I O N S Case Studies Updated 10.24.11 Hill DT Solutions Cervical Decompression Case Study An 18-year-old male involved in a motor vehicle accident in which his SUV was totaled suffering from
S O L U T I O N S Case Studies Updated 10.24.11 Hill DT Solutions Cervical Decompression Case Study An 18-year-old male involved in a motor vehicle accident in which his SUV was totaled suffering from
NETWORK FITNESS FACTS THE HIP
 NETWORK FITNESS FACTS THE HIP The Hip Joint ANATOMY OF THE HIP The hip bones are divided into 5 areas, which are: Image: www.health.com/health/static/hw/media/medical/hw/ hwkb17_042.jpg The hip joint is
NETWORK FITNESS FACTS THE HIP The Hip Joint ANATOMY OF THE HIP The hip bones are divided into 5 areas, which are: Image: www.health.com/health/static/hw/media/medical/hw/ hwkb17_042.jpg The hip joint is
POST SURGICAL RETURN OF RIGHT LEG PAIN. TREATED SUCCESSFULLY WITH COX FLEXION DISTRACTION DECOMPRESSION ADJUSTING
 POST SURGICAL RETURN OF RIGHT LEG PAIN. TREATED SUCCESSFULLY WITH COX FLEXION DISTRACTION DECOMPRESSION ADJUSTING A 47 year old white married female was seen for the chief complaint of low back and right
POST SURGICAL RETURN OF RIGHT LEG PAIN. TREATED SUCCESSFULLY WITH COX FLEXION DISTRACTION DECOMPRESSION ADJUSTING A 47 year old white married female was seen for the chief complaint of low back and right
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH)
") A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) Introduction Diffuse Idiopathic Skeletal Hyperostosis (DISH) is a phenomenon that more commonly affects older males. It is associated
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) Introduction Diffuse Idiopathic Skeletal Hyperostosis (DISH) is a phenomenon that more commonly affects older males. It is associated
THE LUMBAR SPINE (BACK)
") THE LUMBAR SPINE (BACK) At a glance Chronic back pain, especially in the area of the lumbar spine (lower back), is a widespread condition. It can be assumed that 75 % of all people have it sometimes or
THE LUMBAR SPINE (BACK) At a glance Chronic back pain, especially in the area of the lumbar spine (lower back), is a widespread condition. It can be assumed that 75 % of all people have it sometimes or
Notice of Independent Review Decision DESCRIPTION OF THE SERVICE OR SERVICES IN DISPUTE:
 Notice of Independent Review Decision DATE OF REVIEW: 08/15/08 IRO CASE #: NAME: DESCRIPTION OF THE SERVICE OR SERVICES IN DISPUTE: Determine the appropriateness of the previously denied request for physical
Notice of Independent Review Decision DATE OF REVIEW: 08/15/08 IRO CASE #: NAME: DESCRIPTION OF THE SERVICE OR SERVICES IN DISPUTE: Determine the appropriateness of the previously denied request for physical
Guidelines for the table of injuries. For injuries on or after 2 November 2005
 For injuries on or after 2 November 2005 Background Changes to the Table of injuries (TOI) were made in 2005 and are now adopted by the Medical Assessment Tribunal at Q-COMP. The major differences between
For injuries on or after 2 November 2005 Background Changes to the Table of injuries (TOI) were made in 2005 and are now adopted by the Medical Assessment Tribunal at Q-COMP. The major differences between
Neck Injuries and Disorders
 Neck Injuries and Disorders Introduction Any part of your neck can be affected by neck problems. These affect the muscles, bones, joints, tendons, ligaments or nerves in the neck. There are many common
Neck Injuries and Disorders Introduction Any part of your neck can be affected by neck problems. These affect the muscles, bones, joints, tendons, ligaments or nerves in the neck. There are many common
.org. Fractures of the Thoracic and Lumbar Spine. Cause. Description
 Fractures of the Thoracic and Lumbar Spine Page ( 1 ) Spinal fractures can vary widely in severity. While some fractures are very serious injuries that require emergency treatment, other fractures can
Fractures of the Thoracic and Lumbar Spine Page ( 1 ) Spinal fractures can vary widely in severity. While some fractures are very serious injuries that require emergency treatment, other fractures can
The opinions expressed in the report are solely those of the physician performing the examination.
 401 Second Avenue South, Suite 110 Seattle, WA 98104 Telephone: 206.324.6622 Toll Free: 1.800.331.6622 Fax: 206.726.8605 Medical Examination of Employer: : of Exam: of Birth: of Injury: Location of Exam:
401 Second Avenue South, Suite 110 Seattle, WA 98104 Telephone: 206.324.6622 Toll Free: 1.800.331.6622 Fax: 206.726.8605 Medical Examination of Employer: : of Exam: of Birth: of Injury: Location of Exam:
L5 S1 Extruded Disc Relieved with Cox Technic Decompression Spinal Adjusting
 1 L5 S1 Extruded Disc Relieved with Cox Technic Decompression Spinal Adjusting submitted by Joseph d'angiolillo DC 11 Clyde Road, Suite 103 Somerset, NJ 08873 (732) 873 2222 This is a case study of a patient
1 L5 S1 Extruded Disc Relieved with Cox Technic Decompression Spinal Adjusting submitted by Joseph d'angiolillo DC 11 Clyde Road, Suite 103 Somerset, NJ 08873 (732) 873 2222 This is a case study of a patient
Clinical guidance for MRI referral
 MRI for cervical radiculopathy Referral by a medical practitioner (excluding a specialist or consultant physician) for a scan of spine for a patient 16 years or older for suspected: cervical radiculopathy
MRI for cervical radiculopathy Referral by a medical practitioner (excluding a specialist or consultant physician) for a scan of spine for a patient 16 years or older for suspected: cervical radiculopathy
HELPFUL HINTS FOR A HEALTHY BACK
 HELPFUL HINTS FOR A HEALTHY BACK 1. Standing and Walking For correct posture, balance your head above your shoulders, eyes straight ahead, everything else falls into place. Try to point toes straight ahead
HELPFUL HINTS FOR A HEALTHY BACK 1. Standing and Walking For correct posture, balance your head above your shoulders, eyes straight ahead, everything else falls into place. Try to point toes straight ahead
The Petrylaw Lawsuits Settlements and Injury Settlement Report
 The Petrylaw Lawsuits Settlements and Injury Settlement Report BACK INJURIES How Minnesota Juries Decide the Value of Pain and Suffering in Back Injury Cases The Petrylaw Lawsuits Settlements and Injury
The Petrylaw Lawsuits Settlements and Injury Settlement Report BACK INJURIES How Minnesota Juries Decide the Value of Pain and Suffering in Back Injury Cases The Petrylaw Lawsuits Settlements and Injury
Neck Pain Overview Causes, Diagnosis and Treatment Options
 Neck Pain Overview Causes, Diagnosis and Treatment Options Neck pain is one of the most common forms of pain for which people seek treatment. Most individuals experience neck pain at some point during
Neck Pain Overview Causes, Diagnosis and Treatment Options Neck pain is one of the most common forms of pain for which people seek treatment. Most individuals experience neck pain at some point during
Rehabilitation after shoulder dislocation
 Physiotherapy Department Rehabilitation after shoulder dislocation Information for patients This information leaflet gives you advice on rehabilitation after your shoulder dislocation. It is not a substitute
Physiotherapy Department Rehabilitation after shoulder dislocation Information for patients This information leaflet gives you advice on rehabilitation after your shoulder dislocation. It is not a substitute
Large L5 S1 Disc Protrusion Treated Successfully With Cox Technic
 Cox Technic Email Case #77 October 2009 by Dr. Greenwood 1 Large L5 S1 Disc Protrusion Treated Successfully With Cox Technic A case study presented to the Part III Hospital Based Training Course for Cox
Cox Technic Email Case #77 October 2009 by Dr. Greenwood 1 Large L5 S1 Disc Protrusion Treated Successfully With Cox Technic A case study presented to the Part III Hospital Based Training Course for Cox
For Deep Pressure Massage
 T H E R A C A N E O W N E R S M A N U A L For Deep Pressure Massage Thera Cane is a self massager used to apply pressure to sore muscles. The unique design of the Thera Cane lets you apply deep pressure
T H E R A C A N E O W N E R S M A N U A L For Deep Pressure Massage Thera Cane is a self massager used to apply pressure to sore muscles. The unique design of the Thera Cane lets you apply deep pressure
Spine Anatomy and Spine General The purpose of the spine is to help us stand and sit straight, move, and provide protection to the spinal cord.
 Spine Anatomy and Spine General The purpose of the spine is to help us stand and sit straight, move, and provide protection to the spinal cord. Normal List Kyphosis The human spine has 7 Cervical vertebra
Spine Anatomy and Spine General The purpose of the spine is to help us stand and sit straight, move, and provide protection to the spinal cord. Normal List Kyphosis The human spine has 7 Cervical vertebra
Colossus Important Diagnoses. Instructions for How to List Diagnoses
 1 Colossus Important Diagnoses Instructions for How to List Diagnoses 1. Only list diagnoses on HCFA-1500 or CMS-1500 billing forms 2. Use as many billing forms/pages as necessary (4 diagnoses per billing
1 Colossus Important Diagnoses Instructions for How to List Diagnoses 1. Only list diagnoses on HCFA-1500 or CMS-1500 billing forms 2. Use as many billing forms/pages as necessary (4 diagnoses per billing
Medical Report Prepared for The Court on
 Medical Report Prepared for The Court on Mr Sample Report Claimant's Address Claimant's Date of Birth Instructing Party Instructing Party Address Instructing Party Ref Solicitors Ref Corex Ref 1 The Lane
Medical Report Prepared for The Court on Mr Sample Report Claimant's Address Claimant's Date of Birth Instructing Party Instructing Party Address Instructing Party Ref Solicitors Ref Corex Ref 1 The Lane
Workplace Health, Safety & Compensation Review Division
 Workplace Health, Safety & Compensation Review Division WHSCRD Case No: 14152-06 WHSCC Claim No: 606499 and 791748 Decision Number: 14147 Lloyd Piercey Review Commissioner The Review Proceedings 1. The
Workplace Health, Safety & Compensation Review Division WHSCRD Case No: 14152-06 WHSCC Claim No: 606499 and 791748 Decision Number: 14147 Lloyd Piercey Review Commissioner The Review Proceedings 1. The
Temple Physical Therapy
 Temple Physical Therapy A General Overview of Common Neck Injuries For current information on Temple Physical Therapy related news and for a healthy and safe return to work, sport and recreation Like Us
Temple Physical Therapy A General Overview of Common Neck Injuries For current information on Temple Physical Therapy related news and for a healthy and safe return to work, sport and recreation Like Us
Spinal Surgery 2. Teaching Aims. Common Spinal Pathologies. Disc Degeneration. Disc Degeneration. Causes of LBP 8/2/13. Common Spinal Conditions
 Teaching Aims Spinal Surgery 2 Mr Mushtaque A. Ishaque BSc(Hons) BChir(Cantab) DM FRCS FRCS(Ed) FRCS(Orth) Hunterian Professor at The Royal College of Surgeons of England Consultant Orthopaedic Spinal
Teaching Aims Spinal Surgery 2 Mr Mushtaque A. Ishaque BSc(Hons) BChir(Cantab) DM FRCS FRCS(Ed) FRCS(Orth) Hunterian Professor at The Royal College of Surgeons of England Consultant Orthopaedic Spinal
ICD-10 Cheat Sheet Frequently Used ICD-10 Codes for Musculoskeletal Conditions *
 ICD-10 Cheat Sheet Frequently Used ICD-10 Codes for Musculoskeletal Conditions * Finding the ICD-10 equivalent for an ICD-9 code can be a challenge. This resource of frequently used codes can help when
ICD-10 Cheat Sheet Frequently Used ICD-10 Codes for Musculoskeletal Conditions * Finding the ICD-10 equivalent for an ICD-9 code can be a challenge. This resource of frequently used codes can help when
Screening Examination of the Lower Extremities BUY THIS BOOK! Lower Extremity Screening Exam
 Screening Examination of the Lower Extremities Melvyn Harrington, MD Department of Orthopaedic Surgery & Rehabilitation Loyola University Medical Center BUY THIS BOOK! Essentials of Musculoskeletal Care
Screening Examination of the Lower Extremities Melvyn Harrington, MD Department of Orthopaedic Surgery & Rehabilitation Loyola University Medical Center BUY THIS BOOK! Essentials of Musculoskeletal Care
Pre - Operative Rehabilitation Program for Anterior Cruciate Ligament Reconstruction
 Pre - Operative Rehabilitation Program for Anterior Cruciate Ligament Reconstruction This protocol is designed to assist you with your preparation for surgery and should be followed under the direction
Pre - Operative Rehabilitation Program for Anterior Cruciate Ligament Reconstruction This protocol is designed to assist you with your preparation for surgery and should be followed under the direction
Mike s Top Ten Tips for Reducing Back Pain
 Mike s Top Ten Tips for Reducing Back Pain The following article explains ways of preventing, reducing or eliminating back pain. I have found them to be very useful to myself, my clients and my patients.
Mike s Top Ten Tips for Reducing Back Pain The following article explains ways of preventing, reducing or eliminating back pain. I have found them to be very useful to myself, my clients and my patients.
Whiplash and Whiplash- Associated Disorders
 Whiplash and Whiplash- Associated Disorders North American Spine Society Public Education Series What Is Whiplash? The term whiplash might be confusing because it describes both a mechanism of injury and
Whiplash and Whiplash- Associated Disorders North American Spine Society Public Education Series What Is Whiplash? The term whiplash might be confusing because it describes both a mechanism of injury and
.org. Herniated Disk in the Lower Back. Anatomy. Description
 Herniated Disk in the Lower Back Page ( 1 ) Sometimes called a slipped or ruptured disk, a herniated disk most often occurs in your lower back. It is one of the most common causes of low back pain, as
Herniated Disk in the Lower Back Page ( 1 ) Sometimes called a slipped or ruptured disk, a herniated disk most often occurs in your lower back. It is one of the most common causes of low back pain, as
Body Mechanics for Mammography Technologists
 Body Mechanics for Mammography Technologists Diane Rinella RT(R)(M)(BD)RDMS(BR)CDT Objectives Recognize causes and risk factors for Musculoskeletal Disorders (MSDs) for mammography technologists Understand
Body Mechanics for Mammography Technologists Diane Rinella RT(R)(M)(BD)RDMS(BR)CDT Objectives Recognize causes and risk factors for Musculoskeletal Disorders (MSDs) for mammography technologists Understand
Today s session. Common Problems in Rehab. www.physiofitness.com.au/filex.htm LOWER BODY REHAB ESSENTIALS TIM KEELEY FILEX 2012
 Tim Keeley B.Phty, Cred.MDT, APA Principal Physiotherapist physiofitness.com.au facebook.com/physiofitness Today s session Essential list for the lower body Rehab starting point Focussing on activation,
Tim Keeley B.Phty, Cred.MDT, APA Principal Physiotherapist physiofitness.com.au facebook.com/physiofitness Today s session Essential list for the lower body Rehab starting point Focussing on activation,
Lower Back Pain An Educational Guide
 Lower Back Pain An Educational Guide A publication from the Center of Pain Medicine and Physiatric Rehabilitation 2002 Medical Parkway Ste 150 1630 Main St Ste 215 Annapolis, MD 21401 Chester, MD 21619
Lower Back Pain An Educational Guide A publication from the Center of Pain Medicine and Physiatric Rehabilitation 2002 Medical Parkway Ste 150 1630 Main St Ste 215 Annapolis, MD 21401 Chester, MD 21619
Diagnostic Imaging Exams
 Guide for Chiropractors Diagnostic Imaging Exams CREATED FOR OUR CHIROPRACTIC PARTNERS This document has been prepared by the specialized, board-certified radiologists who interpret patient exams for Center
Guide for Chiropractors Diagnostic Imaging Exams CREATED FOR OUR CHIROPRACTIC PARTNERS This document has been prepared by the specialized, board-certified radiologists who interpret patient exams for Center
CERVICAL DISC HERNIATION
 CERVICAL DISC HERNIATION Most frequent at C 5/6 level but also occur at C 6 7 & to a lesser extent at C4 5 & other levels In relatively younger persons soft disk protrusion is more common than hard disk
CERVICAL DISC HERNIATION Most frequent at C 5/6 level but also occur at C 6 7 & to a lesser extent at C4 5 & other levels In relatively younger persons soft disk protrusion is more common than hard disk
Injury Prevention for the Back and Neck
 Injury Prevention for the Back and Neck www.csmr.org We have created this brochure to provide you with information regarding: Common Causes of Back and Neck Injuries and Pain Tips for Avoiding Neck and
Injury Prevention for the Back and Neck www.csmr.org We have created this brochure to provide you with information regarding: Common Causes of Back and Neck Injuries and Pain Tips for Avoiding Neck and
Return to same game if sx s resolve within 15 minutes. Return to next game if sx s resolve within one week Return to Competition
 Assessment Skills of the Spine on the Field and in the Clinic Ron Burke, MD Cervical Spine Injuries Sprains and strains Stingers Transient quadriparesis Cervical Spine Injuries Result in critical loss
Assessment Skills of the Spine on the Field and in the Clinic Ron Burke, MD Cervical Spine Injuries Sprains and strains Stingers Transient quadriparesis Cervical Spine Injuries Result in critical loss
.org. Shoulder Pain and Common Shoulder Problems. Anatomy. Cause
 Shoulder Pain and Common Shoulder Problems Page ( 1 ) What most people call the shoulder is really several joints that combine with tendons and muscles to allow a wide range of motion in the arm from scratching
Shoulder Pain and Common Shoulder Problems Page ( 1 ) What most people call the shoulder is really several joints that combine with tendons and muscles to allow a wide range of motion in the arm from scratching
How to Get and Keep a Healthy Back. Amy Eisenson, B.S. Exercise Physiologist
 How to Get and Keep a Healthy Back Amy Eisenson, B.S. Exercise Physiologist Lesson Objectives Statistics of Back Pain Anatomy of the Spine Causes of Back Pain Four Work Factors Core Muscles Connection
How to Get and Keep a Healthy Back Amy Eisenson, B.S. Exercise Physiologist Lesson Objectives Statistics of Back Pain Anatomy of the Spine Causes of Back Pain Four Work Factors Core Muscles Connection
LOW BACK PAIN EXAMINATION
 LOW BACK PAIN EXAMINATION John Petty, M.D. Medical Director Department of Physical Medicine & Rehabilitation Kettering Medical Center February 8, 2014 PRE-TEST QUESTION What part of the low back physical
LOW BACK PAIN EXAMINATION John Petty, M.D. Medical Director Department of Physical Medicine & Rehabilitation Kettering Medical Center February 8, 2014 PRE-TEST QUESTION What part of the low back physical
The Effects of Cox Decompression Technic in the Treatment of Low Back Pain and Sciatica in a Golf Professional
 Cox Technic Email Case Report 72, June 2009, James Schantz DC 1 The Effects of Cox Decompression Technic in the Treatment of Low Back Pain and Sciatica in a Golf Professional James E. Schantz, D.C. Leading
Cox Technic Email Case Report 72, June 2009, James Schantz DC 1 The Effects of Cox Decompression Technic in the Treatment of Low Back Pain and Sciatica in a Golf Professional James E. Schantz, D.C. Leading
THE BENJAMIN INSTITUTE PRESENTS. Excerpt from Listen To Your Pain. Assessment & Treatment of. Low Back Pain. Ben E. Benjamin, Ph.D.
 THE BENJAMIN INSTITUTE PRESENTS Excerpt from Listen To Your Pain Assessment & Treatment of Low Back Pain A B E N J A M I N I N S T I T U T E E B O O K Ben E. Benjamin, Ph.D. 2 THERAPIST/CLIENT MANUAL The
THE BENJAMIN INSTITUTE PRESENTS Excerpt from Listen To Your Pain Assessment & Treatment of Low Back Pain A B E N J A M I N I N S T I T U T E E B O O K Ben E. Benjamin, Ph.D. 2 THERAPIST/CLIENT MANUAL The
Hand and Upper Extremity Injuries in Outdoor Activities. John A. Schneider, M.D.
 Hand and Upper Extremity Injuries in Outdoor Activities John A. Schneider, M.D. Biographical Sketch Dr. Schneider is an orthopedic surgeon that specializes in the treatment of hand and upper extremity
Hand and Upper Extremity Injuries in Outdoor Activities John A. Schneider, M.D. Biographical Sketch Dr. Schneider is an orthopedic surgeon that specializes in the treatment of hand and upper extremity
Orthopaedic Spine Center. Anterior Cervical Discectomy and Fusion (ACDF) Normal Discs
 Normal Discs") Orthopaedic Spine Center Graham Calvert MD James Woodall MD PhD Anterior Cervical Discectomy and Fusion (ACDF) Normal Discs The cervical spine consists of the bony vertebrae, discs, nerves and other structures.
Orthopaedic Spine Center Graham Calvert MD James Woodall MD PhD Anterior Cervical Discectomy and Fusion (ACDF) Normal Discs The cervical spine consists of the bony vertebrae, discs, nerves and other structures.
Information for the Patient About Surgical
 Information for the Patient About Surgical Decompression and Stabilization of the Spine Aging and the Spine Daily wear and tear, along with disc degeneration due to aging and injury, are common causes
Information for the Patient About Surgical Decompression and Stabilization of the Spine Aging and the Spine Daily wear and tear, along with disc degeneration due to aging and injury, are common causes
The Essential Lower Back Exam
 STFM National Convention 2011 New Orleans The Essential Lower Back Exam Judith A. Furlong, M.D., Cathee McGonigle, D.O. & Rob Rutherford, MD Objectives Brief review of the anatomy of the back, (hip and
STFM National Convention 2011 New Orleans The Essential Lower Back Exam Judith A. Furlong, M.D., Cathee McGonigle, D.O. & Rob Rutherford, MD Objectives Brief review of the anatomy of the back, (hip and
Neck Pain HealthshareHull Information for Guided Patient Management
 HealthshareHull Information for Guided Patient Management Index Introduction 2 The neck (cervical spine) anatomy 2 What are the common types of neck pain? 3 What are the common symptoms associated with
HealthshareHull Information for Guided Patient Management Index Introduction 2 The neck (cervical spine) anatomy 2 What are the common types of neck pain? 3 What are the common symptoms associated with
Lower Back Pain HealthshareHull Information for Guided Patient Management
 HealthshareHull Information for Guided Patient Management Index Introduction 2 Lumbar spine anatomy 2 What is lower back pain? 3 Conditions that may be causing your back pain 3 When should I see my doctor?
HealthshareHull Information for Guided Patient Management Index Introduction 2 Lumbar spine anatomy 2 What is lower back pain? 3 Conditions that may be causing your back pain 3 When should I see my doctor?
ENTITLEMENT ELIGIBILITY GUIDELINES SPONDYLOLISTHESIS AND SPONDYLOLYSIS
 ENTITLEMENT ELIGIBILITY GUIDELINES SPONDYLOLISTHESIS AND SPONDYLOLYSIS MPC 01414 ICD-9 756.12; 738.41; 756.11 DEFINITION Spondylolisthesis is generally defined as an anterior or posterior slipping or displacement
ENTITLEMENT ELIGIBILITY GUIDELINES SPONDYLOLISTHESIS AND SPONDYLOLYSIS MPC 01414 ICD-9 756.12; 738.41; 756.11 DEFINITION Spondylolisthesis is generally defined as an anterior or posterior slipping or displacement
Pelvic Girdle Pain (PGP) Fact Sheet
 Fact Sheet") Pelvic Girdle Pain (PGP) Fact Sheet Physiotherapy PGP describes pain that is experienced in the front (symphysis pubis joint) and/or back (sacroiliac joints) of your pelvis. This is a common problem, affecting
Pelvic Girdle Pain (PGP) Fact Sheet Physiotherapy PGP describes pain that is experienced in the front (symphysis pubis joint) and/or back (sacroiliac joints) of your pelvis. This is a common problem, affecting
SPINE SURGERY - LUMBAR DECOMPRESSION
 SPINE SURGERY - LUMBAR DECOMPRESSION Information Leaflet Your Health. Our Priority. Page 2 of 7 Introduction This booklet has been compiled by the physiotherapy department to help you understand lumbar
SPINE SURGERY - LUMBAR DECOMPRESSION Information Leaflet Your Health. Our Priority. Page 2 of 7 Introduction This booklet has been compiled by the physiotherapy department to help you understand lumbar
Pilates for the Rehabilitation of Iliopsoas Tendonitis and Low Back Pain
 Pilates for the Rehabilitation of Iliopsoas Tendonitis and Low Back Pain Bruce Manuel November 30, 2015 CAP Standard 2015 Pilates Denver Greenwood Village, CO Abstract Iliopsoas Tendonitis is irritation
Pilates for the Rehabilitation of Iliopsoas Tendonitis and Low Back Pain Bruce Manuel November 30, 2015 CAP Standard 2015 Pilates Denver Greenwood Village, CO Abstract Iliopsoas Tendonitis is irritation
SPINE ANATOMY AND PROCEDURES. Tulsa Spine & Specialty Hospital 6901 S. Olympia Avenue Tulsa, Oklahoma 74132
 SPINE ANATOMY AND PROCEDURES Tulsa Spine & Specialty Hospital 6901 S. Olympia Avenue Tulsa, Oklahoma 74132 SPINE ANATOMY The spine consists of 33 bones called vertebrae. The top 7 are cervical, or neck
SPINE ANATOMY AND PROCEDURES Tulsa Spine & Specialty Hospital 6901 S. Olympia Avenue Tulsa, Oklahoma 74132 SPINE ANATOMY The spine consists of 33 bones called vertebrae. The top 7 are cervical, or neck
Chiropractic ICD-10 Common Codes List
 Chiropractic ICD-10 Common Codes List This is a preliminary list of common ICD-10 codes for chiropractic diagnoses. This is a common code list to be used as a guide for coding and is not intended to represent
Chiropractic ICD-10 Common Codes List This is a preliminary list of common ICD-10 codes for chiropractic diagnoses. This is a common code list to be used as a guide for coding and is not intended to represent
A Patient s Guide to Artificial Cervical Disc Replacement
 A Patient s Guide to Artificial Cervical Disc Replacement Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine condition that can cause pain and numbness
A Patient s Guide to Artificial Cervical Disc Replacement Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine condition that can cause pain and numbness
KNEE EXERCISE PROGRAM
 KNEE PROGRAM INTRODUCT ION Welcome to your knee exercise program. The exercises in the program are designed to improve your knee stability and strength of the muscles around your knee and hip. The strength
KNEE PROGRAM INTRODUCT ION Welcome to your knee exercise program. The exercises in the program are designed to improve your knee stability and strength of the muscles around your knee and hip. The strength
Objectives. Spinal Fractures: Classification Diagnosis and Treatment. Level of Fracture. Neuro exam Muscle Grading
 Objectives Spinal Fractures: Classification Diagnosis and Treatment Johannes Bernbeck,, MD Review and apply the understanding of incidence and etiology of VCF. Examine conservative and operative management
Objectives Spinal Fractures: Classification Diagnosis and Treatment Johannes Bernbeck,, MD Review and apply the understanding of incidence and etiology of VCF. Examine conservative and operative management
Pain Management Top Diagnosis Codes (Crosswalk)
") Pain Management Top s (Crosswalk) 274.00 Gout arthropathy, M1000 Idiopathic gout, unspecified site unspecified M10011 Idiopathic gout, right shoulder M10012 Idiopathic gout, left shoulder M10019 Idiopathic
Pain Management Top s (Crosswalk) 274.00 Gout arthropathy, M1000 Idiopathic gout, unspecified site unspecified M10011 Idiopathic gout, right shoulder M10012 Idiopathic gout, left shoulder M10019 Idiopathic
Options for Cervical Disc Degeneration A Guide to the Fusion Arm of the M6 -C Artificial Disc Study
 Options for Cervical Disc Degeneration A Guide to the Fusion Arm of the M6 -C Artificial Disc Study Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine
Options for Cervical Disc Degeneration A Guide to the Fusion Arm of the M6 -C Artificial Disc Study Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine
Lumbar Disc Herniation/Bulge Protocol
 Lumbar Disc Herniation/Bulge Protocol Anatomy and Biomechanics The lumbar spine is made up of 5 load transferring bones called vertebrae. They are stacked in a column with an intervertebral disc sandwiched
Lumbar Disc Herniation/Bulge Protocol Anatomy and Biomechanics The lumbar spine is made up of 5 load transferring bones called vertebrae. They are stacked in a column with an intervertebral disc sandwiched
INDEPENDENT MEDICAL EVALUATION
 Claimant: Requested by: Date of Injury: February 3, 2003 Date of Examination: April 22, 2008 Claim #: INDEPENDENT MEDICAL EVALUATION All information contained herein is from medical records provided to
Claimant: Requested by: Date of Injury: February 3, 2003 Date of Examination: April 22, 2008 Claim #: INDEPENDENT MEDICAL EVALUATION All information contained herein is from medical records provided to
Range of Motion. A guide for you after spinal cord injury. Spinal Cord Injury Rehabilitation Program
 Range of Motion A guide for you after spinal cord injury Spinal Cord Injury Rehabilitation Program This booklet has been written by the health care providers who provide care to people who have a spinal
Range of Motion A guide for you after spinal cord injury Spinal Cord Injury Rehabilitation Program This booklet has been written by the health care providers who provide care to people who have a spinal
Patient Guide. Sacroiliac Joint Pain
 Patient Guide Sacroiliac Joint Pain Anatomy Where is the Sacroiliac Joint? The sacroiliac joint (SIJ) is located at the bottom end of your spine, where the "tailbone" (sacrum) joins the pelvis (ilium).
Patient Guide Sacroiliac Joint Pain Anatomy Where is the Sacroiliac Joint? The sacroiliac joint (SIJ) is located at the bottom end of your spine, where the "tailbone" (sacrum) joins the pelvis (ilium).
TWO CONTRASTING CASES OF SCIATIC RADICULOPATHY: ONE WITH NORMAL MRI AND ONE WITH A FREE FRAGMENT. WHAT S A CHIROPRACTOR TO DO?
 Cox Case Report #59 by Dr. James Cox published 4/08 1 TWO CONTRASTING CASES OF SCIATIC RADICULOPATHY: ONE WITH NORMAL MRI AND ONE WITH A FREE FRAGMENT. WHAT S A CHIROPRACTOR TO DO? A 26-year-old, white,
Cox Case Report #59 by Dr. James Cox published 4/08 1 TWO CONTRASTING CASES OF SCIATIC RADICULOPATHY: ONE WITH NORMAL MRI AND ONE WITH A FREE FRAGMENT. WHAT S A CHIROPRACTOR TO DO? A 26-year-old, white,
FD: ACN=235 ACC=R FD: DT:D DN: 1290/87 STY: PANEL: Bradbury; Beattie; Apsey DDATE: 180188 ACT: 40(2) KEYW: Temporary total disability; Temporary
 KEYW: Temporary total disability; Temporary") FD: ACN=235 ACC=R FD: DT:D DN: 1290/87 STY: PANEL: Bradbury; Beattie; Apsey DDATE: 180188 ACT: 40(2) KEYW: Temporary total disability; Temporary partial disability. SUM: - Tribunal found that worker was
FD: ACN=235 ACC=R FD: DT:D DN: 1290/87 STY: PANEL: Bradbury; Beattie; Apsey DDATE: 180188 ACT: 40(2) KEYW: Temporary total disability; Temporary partial disability. SUM: - Tribunal found that worker was
COMPUTER-RELATED MUSCLE, TENDON, AND JOINT INJURIES
 CHAPTER ELEVEN COMPUTER-RELATED MUSCLE, TENDON, AND JOINT INJURIES To reduce the risk of pain in your neck and shoulders, stay within these recommended ranges of movement: Neck Flexion: 0 o -15 o (bending
CHAPTER ELEVEN COMPUTER-RELATED MUSCLE, TENDON, AND JOINT INJURIES To reduce the risk of pain in your neck and shoulders, stay within these recommended ranges of movement: Neck Flexion: 0 o -15 o (bending
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 2515/11
 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 2515/11 BEFORE: R. McClellan : Vice-Chair M. Christie : Member Representative of Employers A. Signoroni : Member Representative of Workers HEARING:
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 2515/11 BEFORE: R. McClellan : Vice-Chair M. Christie : Member Representative of Employers A. Signoroni : Member Representative of Workers HEARING:
Physiotherapy Database Exercises for people with Spinal Cord Injury
 Physiotherapy Database Exercises for people with Spinal Cord Injury Compiled by the physiotherapists associated with the following Sydney (Australian) spinal units : Last Generated on Mon Mar 29 16:57:20
Physiotherapy Database Exercises for people with Spinal Cord Injury Compiled by the physiotherapists associated with the following Sydney (Australian) spinal units : Last Generated on Mon Mar 29 16:57:20
Sciatica Yuliya Mutsa PTA 236
 Sciatica Yuliya Mutsa PTA 236 Sciatica is a common type of pain affecting the sciatic nerve, which extends from the lower back all the way through the back of the thigh and down through the leg. Depending
Sciatica Yuliya Mutsa PTA 236 Sciatica is a common type of pain affecting the sciatic nerve, which extends from the lower back all the way through the back of the thigh and down through the leg. Depending
WORKERS COMPENSATION BOARD APPEAL TRIBUNAL. [Personal information] CASE I.D. #[personal information]
![WORKERS COMPENSATION BOARD APPEAL TRIBUNAL. [Personal information] CASE I.D. #[personal information]](/thumbs/25/6156167.jpg "WORKERS COMPENSATION BOARD APPEAL TRIBUNAL. [Personal information] CASE I.D. #[personal information]") WORKERS COMPENSATION BOARD APPEAL TRIBUNAL BETWEEN: [personal information] CASE I.D. #[personal information] PLAINTIFF AND: WORKERS COMPENSATION BOARD OF PRINCE EDWARD ISLAND DEFENDANT DECISION #41 [Personal
WORKERS COMPENSATION BOARD APPEAL TRIBUNAL BETWEEN: [personal information] CASE I.D. #[personal information] PLAINTIFF AND: WORKERS COMPENSATION BOARD OF PRINCE EDWARD ISLAND DEFENDANT DECISION #41 [Personal
OVERVIEW. NEUROSURGICAL ASSESSMENT CERVICAL PROBLEMS Dirk G. Franzen, M.D. WHAT IS THE MOST IMPORTANT PART OF THE PHYSICAL EXAM?
 NEUROSURGICAL ASSESSMENT CERVICAL PROBLEMS Dirk G. Franzen, M.D. Neurological Surgery Bluegrass Orthopaedics and Hand Care OVERVIEW SCOPE OF THE PROBLEM PREVALENCE PATHOLOGY ANATOMIC CONSIDERATIONS ASSESSMENT
NEUROSURGICAL ASSESSMENT CERVICAL PROBLEMS Dirk G. Franzen, M.D. Neurological Surgery Bluegrass Orthopaedics and Hand Care OVERVIEW SCOPE OF THE PROBLEM PREVALENCE PATHOLOGY ANATOMIC CONSIDERATIONS ASSESSMENT
Spine Evaluation. Copyright 2004, Yoshiyuki Shiratori. All right reserved.
 Spine Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling? Mechanism:
Spine Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling? Mechanism:
DIFFERENTIAL DIAGNOSIS OF LOW BACK PAIN. Arnold J. Weil, M.D., M.B.A. Non-Surgical Orthopaedics, P.C. Atlanta, GA
 DIFFERENTIAL DIAGNOSIS OF LOW BACK PAIN Arnold J. Weil, M.D., M.B.A. Non-Surgical Orthopaedics, P.C. Atlanta, GA MEDICAL ALGORITHM OF REALITY LOWER BACK PAIN Yes Patient will never get better until case
DIFFERENTIAL DIAGNOSIS OF LOW BACK PAIN Arnold J. Weil, M.D., M.B.A. Non-Surgical Orthopaedics, P.C. Atlanta, GA MEDICAL ALGORITHM OF REALITY LOWER BACK PAIN Yes Patient will never get better until case
Thoracolumbar Fratures R1: 胡 家 瑞 指 导 老 师 : 吴 轲 主 任
 Thoracolumbar Fratures R1: 胡 家 瑞 指 导 老 师 : 吴 轲 主 任 Patient Data Name: 苏 XX Gender: Female Age:47 years old Admission date: 2010.06.09 Chief complaint Fell down from 4-54 5 meter tree and lead to lumbosacral
Thoracolumbar Fratures R1: 胡 家 瑞 指 导 老 师 : 吴 轲 主 任 Patient Data Name: 苏 XX Gender: Female Age:47 years old Admission date: 2010.06.09 Chief complaint Fell down from 4-54 5 meter tree and lead to lumbosacral
Degenerative Lumbar Scoliosis with Stenosis Successfully Treated with Cox Distraction Manipulation
 Cox Technic Case Report #92 (sent February 2011 2/8/11 ) 1 Degenerative Lumbar Scoliosis with Stenosis Successfully Treated with Cox Distraction Manipulation Presented By Robert E. Patterson Jr., D.C.
Cox Technic Case Report #92 (sent February 2011 2/8/11 ) 1 Degenerative Lumbar Scoliosis with Stenosis Successfully Treated with Cox Distraction Manipulation Presented By Robert E. Patterson Jr., D.C.
Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, The Cervical Spine. What is the Cervical Spine?
 Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine condition that can cause pain and numbness in the neck, shoulders, arms, and even hands. This patient
Each year, hundreds of thousands of adults are diagnosed with Cervical Disc Degeneration, an upper spine condition that can cause pain and numbness in the neck, shoulders, arms, and even hands. This patient
Soft-tissue injuries of the neck in automobile accidents: Factors influencing prognosis
 Soft-tissue injuries of the neck in automobile accidents: Factors influencing prognosis 1 Mason Hohl, MD FROM ABSTRACT: Journal of Bone and Joint Surgery (American) December 1974;56(8):1675-1682 Five years
Soft-tissue injuries of the neck in automobile accidents: Factors influencing prognosis 1 Mason Hohl, MD FROM ABSTRACT: Journal of Bone and Joint Surgery (American) December 1974;56(8):1675-1682 Five years
PERFORMANCE RUNNING. Piriformis Syndrome
 Piriformis Syndrome Have you started to experience pain in your hip or down your leg while beginning or advancing your fitness program? This pain may be stemming from the piriformis muscle in your hip.
Piriformis Syndrome Have you started to experience pain in your hip or down your leg while beginning or advancing your fitness program? This pain may be stemming from the piriformis muscle in your hip.
Patient Information. Lateral Lumbar Interbody Fusion Surgery (LLIF).
.") Patient Information. Lateral Lumbar Interbody Fusion Surgery (LLIF). Understanding your spine Disc Between each pair of vertebrae there is a disc that acts as a cushion to protect the vertebra, allows
Patient Information. Lateral Lumbar Interbody Fusion Surgery (LLIF). Understanding your spine Disc Between each pair of vertebrae there is a disc that acts as a cushion to protect the vertebra, allows
Cervical Whiplash: Considerations in the Rehabilitation of Cervical Myofascial Injury. Canadian Family Physician
 Cervical Whiplash: Considerations in the Rehabilitation of Cervical Myofascial Injury 1 Canadian Family Physician Volume 32, September 1986 Arthur Ameis, MD Dr. Ames practices physical medicine and rehabilitation,
Cervical Whiplash: Considerations in the Rehabilitation of Cervical Myofascial Injury 1 Canadian Family Physician Volume 32, September 1986 Arthur Ameis, MD Dr. Ames practices physical medicine and rehabilitation,
MET: Posterior (backward) Rotation of the Innominate Bone.
 Rotation of the Innominate Bone.") MET: Posterior (backward) Rotation of the Innominate Bone. Purpose: To reduce an anterior rotation of the innominate bone at the SI joint. To increase posterior (backward) rotation of the SI joint. Precautions:
MET: Posterior (backward) Rotation of the Innominate Bone. Purpose: To reduce an anterior rotation of the innominate bone at the SI joint. To increase posterior (backward) rotation of the SI joint. Precautions:
Surgery for cervical disc prolapse or cervical osteophyte
 Mr Paul S. D Urso MBBS(Hons), PhD, FRACS Neurosurgeon Provider Nº: 081161DY Epworth Centre Suite 6.1 32 Erin Street Richmond 3121 Tel: 03 9421 5844 Fax: 03 9421 4186 AH: 03 9483 4040 email: [email protected]
Mr Paul S. D Urso MBBS(Hons), PhD, FRACS Neurosurgeon Provider Nº: 081161DY Epworth Centre Suite 6.1 32 Erin Street Richmond 3121 Tel: 03 9421 5844 Fax: 03 9421 4186 AH: 03 9483 4040 email: [email protected]
Runner's Injury Prevention
 JEN DAVIS DPT Runner's Injury Prevention Jen Davis DPT Orthopedic Physical Therapy Foot Traffic 7718 SE 13th Ave Portland, OR 97202 (503) 482-7232 [email protected] www.runfastpt.com!1 THE AMAZING RUNNER
JEN DAVIS DPT Runner's Injury Prevention Jen Davis DPT Orthopedic Physical Therapy Foot Traffic 7718 SE 13th Ave Portland, OR 97202 (503) 482-7232 [email protected] www.runfastpt.com!1 THE AMAZING RUNNER
SPINE, LOWER EXTREMITY, AND PELVIC IMPAIRMENT SECTION
 SPINE, LOWER EXTREMITY, AND PELVIC IMPAIRMENT SECTION Lev.II Curriculum Rev. 6/09 99 OBJECTIVES FOR SPINAL, LOWER EXTREMITY, AND PELVIC IMPAIRMENT RATING SECTION 1. Demonstrate ability to properly measure
SPINE, LOWER EXTREMITY, AND PELVIC IMPAIRMENT SECTION Lev.II Curriculum Rev. 6/09 99 OBJECTIVES FOR SPINAL, LOWER EXTREMITY, AND PELVIC IMPAIRMENT RATING SECTION 1. Demonstrate ability to properly measure