CARE MANAGEMENT FOR LATE LIFE DEPRESSION IN URBAN CHINESE PRIMARY CARE CLINICS
|
|
|
- Mae Chapman
- 8 years ago
- Views:
Transcription

1 CARE MANAGEMENT FOR LATE LIFE DEPRESSION IN URBAN CHINESE PRIMARY CARE CLINICS Dept of Public Health Sciences February 6, 2015 Yeates Conwell, MD Dept of Psychiatry, University of Rochester Shulin Chen, MD, PhD Dept of Psychology, Zhejiang University

2 Shulin Chen, MD, PhD Professor of Psychology Zhejiang University 2

3 3 DISCLOSURES Y. Conwell: NIH Fogarty Center D43 TW05814 China-Rochester Suicide Research Center (ED Caine, PI) S. Chen: NIH Fogarty Center R01 TW Program for New Century Excellent Talents in Universities of China


4 4 DEPRESSION WORLDWIDE Common

5 5 DEPRESSION WORLDWIDE Common Associated with o Greater additive symptom burden o Greater functional impairment o Poorer adherence to tx o Greater utilization of care and cost % higher after controlling for age, gender, severity of medical conditions o Increased mortality

6 6 DEPRESSION IS A CHRONIC ILLNESS Risk of recurrence o 60% after 1 episode o 70% after 2 episodes o 90% after 3 episodes Associated with significant functional impairment Often comorbid with other chronic medical illnesses complicating management 2 nd leading cause of DALYs by 2020 (WHO, 2004)

7 7 LATE LIFE DEPRESSION IN CHINA Common Rarely recognized or treated Chronic disease course Journal of Affective Disorders 141:86-93, 2012

8 LATE LIFE DEPRESSION IN CHINA Journal of Affective Disorders 141:86-93, adults 60 years recruited from a primary care clinic in urban China PHQ-9 screening for all, stratified subsample of 237 administered SCID, followed for 12 months Prevalence of MDD = 11.3% Correlates of MDD = age, female sex, ed, illness burden, living alone, family support, disability. <1% received any treatment 73.2% of those with MDD at baseline remained syndromally depressed a year later 3% had received treatment 8

9 Chen et al, J Affect Disord 141:86-93,

10 10 LATE LIFE DEPRESSION IN CHINA Barriers: o Lack of access to specialty MH care o Access to primary care is good at the community level o BUT, little training in depression dx and treatment for primary care providers o Stigma Opportunities for improvement o 2006: Central gov t emphasizes community-based chronic disease management, including depression.

11
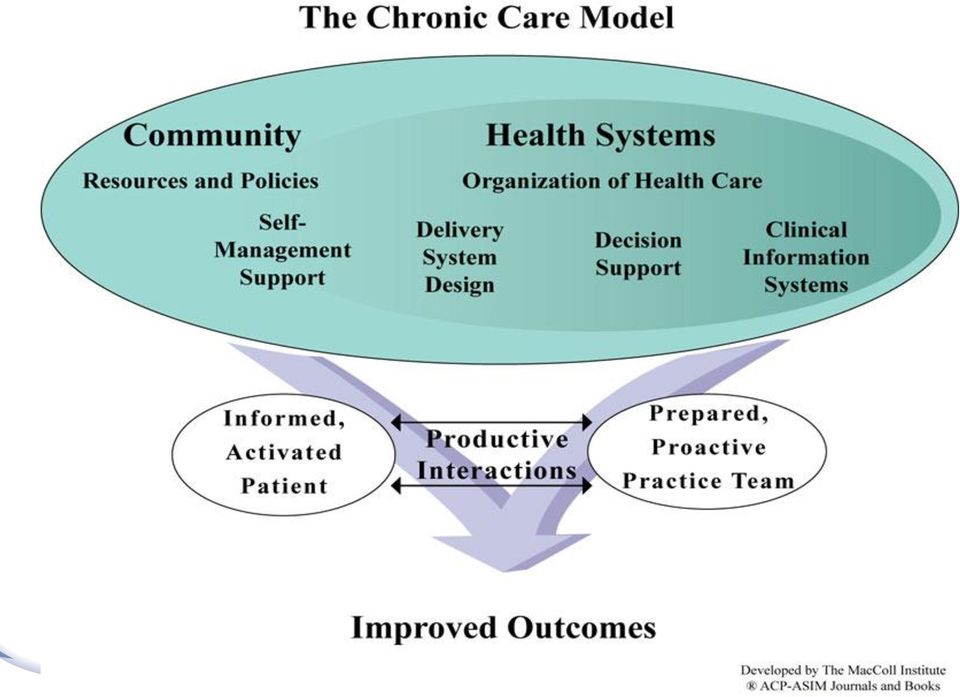
12 Collaborative Care Model CHRONIC DISEASE MANAGEMENT: DEPRESSION o Screening case detection o Regular symptom monitoring o Patient self-management education o Provider education o Evidence-based treatments to remission o Multidisciplinary team o Communications infrastructure o Depression specialists (RN, PhD, SW) embedded in primary care practice o Supervised by psychiatrist
 embedded in primary care practice o")
13 13 COLLABORATIVE CARE FOR DEPRESSION Archer J, Bower P, Gilbody S, et al. Collaborative care for depression and anxiety problems. Cochrane Database Syst Rev 2012; 10: CD RCTs involving 24,308 participants Significantly greater improvement for adults who received collaborative care model in short, medium, and long term f/u Better outcomes also in o quality of life o satisfaction with care o medication use

14 MOST EFFECTIVE COMPONENTS Gilbody S, et al (2006): Archives of Internal Medicine 166: Depression care manager to help PCP o Educate patients o Provide close follow-up o Track depression outcomes, adverse effects and treatment adherence o Facilitate follow-up reassessment Use of practice guidelines Consultation by a psychiatrist

15 15 DEPRESSION CARE MANAGEMENT FOR URBAN CHINESE ELDERS OBJECTIVE: To determine whether care utilizing chronic disease and collaborative care management principles results in better outcomes for older adults with major depression in urban Chinese primary care clinics.


16 16

17 17 Hangzhou City, Zhejiang Province Population: 8.8 million

18 Neighborhood Clinic

19 19 Aims 1. To test whether DCM administered over 12 months would yield greater reductions in depressive symptoms than ecau 2. To examine whether subject groups differed in self-assessments of o o o quality of life satisfaction with their primary care providers perceived stigma regarding depression treatment

20 20 Methods Design o Cluster randomized control trial design o Randomization at the clinic level Intervention sites o Shangcheng District neighborhood PC clinics 16 of 34 clinics randomly selected of which 8 were randomly assigned to deliver DCM, the remainder to ecau

21 Neighborhood Clinic
22 22 Methods Subjects o 60 years, independent living, registered residents o Stage 1 screen: PHQ-9 total score 10 o Stage 2: SCID dx of major depressive episode, MMSE score >18, with capacity to consent, without psychosis or significant risk for suicide. o Consent to participate given the treatment arm to which their clinic was assigned Research assessments at o Baseline, 3-, 6-, 9-, and 12-mths.
23 23 Intervention: ecau Status quo: little or no training for PCPs in MH Rarely diagnosed or treated No established transfer mechanism to MH specialists Provided copy of depression practice guidelines Informed of subject s PHQ-9 score and dx -- Hence enhanced CAU --
24 24 Intervention: Depression Care Management Based on Three Component Model (MacArthur Foundation. Depression Management Tool Kit ) Primary care physician --Treatment Guidelines Figure 1. The Depression Care Management Model Care manager --Psychoeducation --Monitoring treatment --Adherence support --Communication Patients with late life depression Psychiatrist --Psychiatric consultation --Supervision (Key: Adapted from MacArthur Foundation s Initiative on Depression & Primary Care)
25 25 Intervention: Depression Care Management Depression practice guidelines o Antidepressant medications: STAGED guidelines China Treatment and Prevention Guidelines for Depression (CTPGD) Sertraline -> augmentation with buproprion XR o Referral to Hangzhou MH Center if improvement <50% in 16 weeks Care Manager Psychiatric supervision and consultation
26 26 Intervention: Depression Care Management Care Manager o 1 nurse from each PCC (receive 3 yrs post high school education, no MH training) o 3 hrs training, monthly supervision and continuing education from study psychiatrist o Responsibilities: Pt/family education Facilitate communications with PCP Support adherence Outreach to pt q2 weeks, monitor PHQ-9 score
27 27 Intervention: Depression Care Management Psychiatric supervision and consultation o Monthly visit to each PCC Support collaborative team fxn Continuing education re: depression management Consult re: care of non-responding patients or those with consultation No direct pt contact
28 28 Measures Demographics Primary outcome o Hamilton Depression Rating Scale (HAMD) o Response: 50% decrease in HAMD from baseline o Remission: HAMD<7 Secondary outcomes o 12-item Short Form Health Survey (SF-12) o 3-item Treatment Stigma Scale (TSS) o 8-item Client Satisfaction Questionnaire (CSQ)
29 29 Results 4397 pts screened, yielding 162 in ecau and 164 in DCM. SCREENI NG MDD/SCI D BASELINE 12-M FOLLOW-UP DCM CAU
30 Baseline demographic and clinical characteristics Table 1. Demographic and clinical characteristics of participants in the DCM and ecau groups at baseline 30 DCM group ecau group (n=164) (n=162) T value (p value) Age-years (mean ± SD) 7 1 7± ± (0 95) Gender-Female % 63.4% 63 6% 0 10 (0 97) Education % 0.17 (0 92) 8 years 72 0% 72 3% >8 years 28 0% 27 7% Living % 0 21 (0 83) Alone 9 1% 9 6% With spouse 49 4% 49 3% With children 41 5% 41 1% Marriage % 0 27 (0 75) Married 78 7% 79 9% Single, separated, or divorced 21 3% 20 1% Physical illnesses number 4 74± ± (0 62) HAMD score (mean ± SD) 18 7± ± (0 31) DCM, Depression Care Management; ecau, enhance Care-as-usual; HAMD, Hamilton Depression Rating Scale
31 31! Depression measures, by group Table 2. Depression response and remission over time in the DCM and ecau groups DCM group (n=164) ecau group (n=162) Estimated Between Group Difference (95% CI) Effect Size (Cohen s d or Odds ratio, 95%CI) P value HDRS (mean ± SD) -6 5 (-7 1, -5.9) 0 8 (0 7, 0 9) <0 001 Baseline 18 7± ±3 5 3 months 9 3± ±4 3 6 months 8 0± ± months 6 1± ±5 2 Response rates (%) (n) 32 8 (24 5, 43 9) 4 3 (3 1, 5 9) < months 51 2% (54/134) 4 8% (7/145) 6 months 58 1% (71/122) 12 0% (14/117) 12 months 66 3% (73/110) 21 2% (22/104) Remission rates (%) (n) 15 3 (11 6, 20 2) 12 7 (9 5, 17) < months 19 4%(26/134) 0 7% (1/145) 6 months 31 1% (38/122) 3 4% (4/117) 12 months 57 4% (63/110) 8 7% (9/104)
32 32 QoL, Stigma, Tx Satisfaction, by group Table 2. Depression response and remission over time in the DCM and ecau groups DCM group (n=164) ecau group (n=162) Estimated Between Group Difference (95% CI) Effect Size (Cohen s d or Odds ratio, 95%CI) P value SF-12 (mean ± SD) 9 6 (8 1, 11 1) 0 7 (0 6, 0 8) <0 001 Baseline 31 8± ± months 49 0± ±8 7 TSS (mean ± SD) -1 4 (-1 5, -1 2) 0 9 (0 7, 1 1) <0 001 Baseline 2 5± ± months 0 6± ±0 8 CSQ-8 (mean ± SD) 4 8 (3 7, 5 9) 0 6 (0 5, 0 7) <0 001 Baseline 14 6± ± months 22 3± ±5 8
33 33 Summary Treatment delivery (solely medications) far more likely in DCM o DCM: 164/164 at entry; 82% continue at 3 mths. o ecau: 7/162 at entry, 5/162 at 3 mths DCM had better outcomes at all time points in o depression sx severity, response, remission o satisfaction with depression care o quality of life o perceived stigma
34 34 Summary Differences between groups pronounced at 3 months and remained through 12 mths Not accounted for by referral to MH care No differences in rates of hospitalization (17 in DCM vs. 26 in ecau; all medical) No psychiatric admissions No suicidal behavior or deaths in either group
35 35 Commentary Large effect size o At 12 mths, DCM subjects had remission rate 6.6 times greater than ecau (57.4% versus 8.7%) o Compare Cochrane meta-analysis showing overall 12-month depression remission rate 1.3 times greater than usual care. * o Highest rate for any single study reporting 3.3 times greater remission. * Why? * Archer J, Bower P, Gilbody S, et al. Collaborative care for depression and anxiety problems. The Cochrane database of systematic reviews 2012;10:CD
36 36 Commentary Stigma as barrier to care. Satisfaction adherence, response QoL reflecting wide range of pt/family centered care values. Limitations o Urban, wealthy o Not blinded o Traditional Chinese medicine effects not tracked o No option of psychosocial intervention o 12 mth duration
37 37 FUTURE DIRECTIONS Adapt to rural China Testing in other LMICs Incorporate o psychosocial intervention option o traditional medical practices o use of information technologies (telehealth visits) Training of providers in collab & team based care Combine with management of other chronic conditions (physical and mental)
38 Hangzhou -- Qiantang River 谢 谢 -- THANK YOU
Elizabeth A. Crocco, MD Assistant Clinical Professor Chief, Division of Geriatric Psychiatry Department of Psychiatry and Behavioral Sciences Miller
 Elizabeth A. Crocco, MD Assistant Clinical Professor Chief, Division of Geriatric Psychiatry Department of Psychiatry and Behavioral Sciences Miller School of Medicine/University of Miami Question 1 You
Elizabeth A. Crocco, MD Assistant Clinical Professor Chief, Division of Geriatric Psychiatry Department of Psychiatry and Behavioral Sciences Miller School of Medicine/University of Miami Question 1 You
Dr. Anna M. Acee, EdD, ANP-BC, PMHNP-BC Long Island University, Heilbrunn School of Nursing
 Dr. Anna M. Acee, EdD, ANP-BC, PMHNP-BC Long Island University, Heilbrunn School of Nursing Overview Depression is significantly higher among elderly adults receiving home healthcare, particularly among
Dr. Anna M. Acee, EdD, ANP-BC, PMHNP-BC Long Island University, Heilbrunn School of Nursing Overview Depression is significantly higher among elderly adults receiving home healthcare, particularly among
Lessons on the Integration of Medicine and Psychiatry
 Lessons on the Integration of Medicine and Psychiatry Edward Post, MD, PhD Associate Professor of Internal Medicine, University of Michigan VA Health Services Research & Development Center of Excellence,
Lessons on the Integration of Medicine and Psychiatry Edward Post, MD, PhD Associate Professor of Internal Medicine, University of Michigan VA Health Services Research & Development Center of Excellence,
Bipolar Disorder and Substance Abuse Joseph Goldberg, MD
 Diabetes and Depression in Older Adults: A Telehealth Intervention Julie E. Malphurs, PhD Asst. Professor of Psychiatry and Behavioral Science Miller School of Medicine, University of Miami Research Coordinator,
Diabetes and Depression in Older Adults: A Telehealth Intervention Julie E. Malphurs, PhD Asst. Professor of Psychiatry and Behavioral Science Miller School of Medicine, University of Miami Research Coordinator,
Major Depressive Disorders Questions submitted for consideration by workshop participants
 Major Depressive Disorders Questions submitted for consideration by workshop participants Prioritizing Comparative Effectiveness Research Questions: PCORI Stakeholder Workshops June 9, 2015 Patient-Centered
Major Depressive Disorders Questions submitted for consideration by workshop participants Prioritizing Comparative Effectiveness Research Questions: PCORI Stakeholder Workshops June 9, 2015 Patient-Centered
Viability and Impact of Telehealth-Based Depression Care in Home Care
 Viability and Impact of Telehealth-Based Depression Care in Home Care Thomas Sheeran, PhD, ME Rhode Island Hospital Alpert Medical School of Brown University Funding: NIMH K01MH08757 Disclosures: None
Viability and Impact of Telehealth-Based Depression Care in Home Care Thomas Sheeran, PhD, ME Rhode Island Hospital Alpert Medical School of Brown University Funding: NIMH K01MH08757 Disclosures: None
CLINICAL PRACTICE GUIDELINES Treatment of Schizophrenia
 CLINICAL PRACTICE GUIDELINES Treatment of Schizophrenia V. Service Delivery Service Delivery and the Treatment System General Principles 1. All patients should have access to a comprehensive continuum
CLINICAL PRACTICE GUIDELINES Treatment of Schizophrenia V. Service Delivery Service Delivery and the Treatment System General Principles 1. All patients should have access to a comprehensive continuum
Elderly males, especially white males, are the people at highest risk for suicide in America.
 Statement of Ira R. Katz, MD, PhD Professor of Psychiatry Director, Section of Geriatric Psychiatry University of Pennsylvania Director, Mental Illness Research Education and Clinical Center Philadelphia
Statement of Ira R. Katz, MD, PhD Professor of Psychiatry Director, Section of Geriatric Psychiatry University of Pennsylvania Director, Mental Illness Research Education and Clinical Center Philadelphia
DEPRESSION Depression Assessment PHQ-9 Screening tool Depression treatment Treatment flow chart Medications Patient Resource
 E-Resource March, 2015 DEPRESSION Depression Assessment PHQ-9 Screening tool Depression treatment Treatment flow chart Medications Patient Resource Depression affects approximately 20% of the general population
E-Resource March, 2015 DEPRESSION Depression Assessment PHQ-9 Screening tool Depression treatment Treatment flow chart Medications Patient Resource Depression affects approximately 20% of the general population
Managing depression after stroke. Presented by Maree Hackett
 Managing depression after stroke Presented by Maree Hackett After stroke Physical changes We can see these Depression Emotionalism Anxiety Confusion Communication problems What is depression? Category
Managing depression after stroke Presented by Maree Hackett After stroke Physical changes We can see these Depression Emotionalism Anxiety Confusion Communication problems What is depression? Category
Do Patients of Racial/Ethnic Minority and Lower SES Use Depression Care Management Differently?
 Do Patients of Racial/Ethnic Minority and Lower SES Use Depression Care Management Differently? Yuhua Bao, Ph.D. Division of Health Policy, Department of Public Health Weill Cornell Medical College 2009
Do Patients of Racial/Ethnic Minority and Lower SES Use Depression Care Management Differently? Yuhua Bao, Ph.D. Division of Health Policy, Department of Public Health Weill Cornell Medical College 2009
Major Depressive Disorder (MDD) Guideline Diagnostic Nomenclature for Clinical Depressive Conditions
 Guideline Diagnostic Nomenclature for Clinical Depressive Conditions") Major Depressive Disorder Major Depressive Disorder (MDD) Guideline Diagnostic omenclature for Clinical Depressive Conditions Conditions Diagnostic Criteria Duration Major Depression 5 of the following
Major Depressive Disorder Major Depressive Disorder (MDD) Guideline Diagnostic omenclature for Clinical Depressive Conditions Conditions Diagnostic Criteria Duration Major Depression 5 of the following
Integrating Primary Care and Behavioral Health Services: A Compass and A Horizon
 Integrating Primary Care and Behavioral Health Services: A Compass and A Horizon A curriculum for community health centers Developed for the Bureau of Primary Health Care Managed Care Technical Assistance
Integrating Primary Care and Behavioral Health Services: A Compass and A Horizon A curriculum for community health centers Developed for the Bureau of Primary Health Care Managed Care Technical Assistance
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA MAJOR DEPRESSION IN ADULTS IN PRIMARY CARE HEALTH CARE GUIDELINE (ICSI) Health Care Guideline Twelfth Edition May 2009. The guideline was reviewed and adopted by the Molina
MOLINA HEALTHCARE OF CALIFORNIA MAJOR DEPRESSION IN ADULTS IN PRIMARY CARE HEALTH CARE GUIDELINE (ICSI) Health Care Guideline Twelfth Edition May 2009. The guideline was reviewed and adopted by the Molina
Kaiser Permanente Southern California Depression Care Program
 Kaiser Permanente Southern California Depression Care Program Abstract In 2001, Kaiser Permanente of Southern California (KPSC) adopted the IMPACT model of collaborative care for depression, developed
Kaiser Permanente Southern California Depression Care Program Abstract In 2001, Kaiser Permanente of Southern California (KPSC) adopted the IMPACT model of collaborative care for depression, developed
Professional Reference Series Depression and Anxiety, Volume 1. Depression and Anxiety Prevention for Older Adults
 Professional Reference Series Depression and Anxiety, Volume 1 Depression and Anxiety Prevention for Older Adults TA C M I S S I O N The mission of the Older Americans Substance Abuse and Mental Health
Professional Reference Series Depression and Anxiety, Volume 1 Depression and Anxiety Prevention for Older Adults TA C M I S S I O N The mission of the Older Americans Substance Abuse and Mental Health
Effective Care Management for Behavioral Health Integration
 Effective Care Management for Behavioral Health Integration Title: Effective Care Management for Behavioral Health Integration A process improvement initiative focused on improving mental health outcomes
Effective Care Management for Behavioral Health Integration Title: Effective Care Management for Behavioral Health Integration A process improvement initiative focused on improving mental health outcomes
What happens to depressed adolescents? A beyondblue funded 3 9 year follow up study
 What happens to depressed adolescents? A beyondblue funded 3 9 year follow up study Amanda Dudley, Bruce Tonge, Sarah Ford, Glenn Melvin, & Michael Gordon Centre for Developmental Psychiatry & Psychology
What happens to depressed adolescents? A beyondblue funded 3 9 year follow up study Amanda Dudley, Bruce Tonge, Sarah Ford, Glenn Melvin, & Michael Gordon Centre for Developmental Psychiatry & Psychology
Evaluations. Viewer Call-In. www.t2b2.org. Phone: 800-452-0662 Fax: 518-426-0696. Geriatric Mental Health. Thanks to our Sponsors: Guest Speaker
 Geriatric Mental Health June 1, 7 Guest Speaker Michael B. Friedman, LMSW Chairperson Geriatric Mental Health Alliance of New York Thanks to our Sponsors: School of Public Health, University at Albany
Geriatric Mental Health June 1, 7 Guest Speaker Michael B. Friedman, LMSW Chairperson Geriatric Mental Health Alliance of New York Thanks to our Sponsors: School of Public Health, University at Albany
Best Principles for Integration of Child Psychiatry into the Pediatric Health Home
 Best Principles for Integration of Child Psychiatry into the Pediatric Health Home Approved by AACAP Council June 2012 These guidelines were developed by: Richard Martini, M.D., co-chair, Committee on
Best Principles for Integration of Child Psychiatry into the Pediatric Health Home Approved by AACAP Council June 2012 These guidelines were developed by: Richard Martini, M.D., co-chair, Committee on
Screening Tools and Interventions for Common Behavioral Health Disorders TXPEC-0772-13
 Screening Tools and Interventions for Common Behavioral Health Disorders TXPEC-0772-13 Screening Tools and Interventions for Common Behavioral Health Disorders Depression Depression is a potentially life-threatening
Screening Tools and Interventions for Common Behavioral Health Disorders TXPEC-0772-13 Screening Tools and Interventions for Common Behavioral Health Disorders Depression Depression is a potentially life-threatening
Pennsylvania Depression Quality Improvement Collaborative
 Pennsylvania Depression Quality Improvement Collaborative Carol Hann, RN, MSN, CPHQ, Collaborative Manager Southeastern Pennsylvania Association for Healthcare Quality (SPAHQ) David Payne, Psy.D., Senior
Pennsylvania Depression Quality Improvement Collaborative Carol Hann, RN, MSN, CPHQ, Collaborative Manager Southeastern Pennsylvania Association for Healthcare Quality (SPAHQ) David Payne, Psy.D., Senior
Depression Remission at Six Months Specifications 2014 (Follow-up Visits for 07/01/2012 to 06/30/2013 Index Contact Dates)
") Description Methodology Rationale Measurement Period A measure of the percentage of adults patients who have reached remission at six months (+/- 30 days) after being identified as having an initial PHQ-9
Description Methodology Rationale Measurement Period A measure of the percentage of adults patients who have reached remission at six months (+/- 30 days) after being identified as having an initial PHQ-9
Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination of care for both services.
 Domain 3 Projects 3.a.i Integration of Primary Care and Behavioral Health Services Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination
Domain 3 Projects 3.a.i Integration of Primary Care and Behavioral Health Services Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination
TECHNICAL/CLINICAL TOOLS BEST PRACTICE 7: Depression Screening and Management
 TECHNICAL/CLINICAL TOOLS BEST PRACTICE 7: Depression Screening and Management WHY IS THIS IMPORTANT? Depression causes fluctuations in mood, low self esteem and loss of interest or pleasure in normally
TECHNICAL/CLINICAL TOOLS BEST PRACTICE 7: Depression Screening and Management WHY IS THIS IMPORTANT? Depression causes fluctuations in mood, low self esteem and loss of interest or pleasure in normally
Collaborative care and psychiatric consultation models in primary care
 Collaborative care and psychiatric consultation models in primary care C Van der Feltz-Cornelis Prof Primary Care Psychiatry Invitational Conference Nijmegen, 2 oktober 2013 Psychiatrist, Epidemiologist
Collaborative care and psychiatric consultation models in primary care C Van der Feltz-Cornelis Prof Primary Care Psychiatry Invitational Conference Nijmegen, 2 oktober 2013 Psychiatrist, Epidemiologist
TREATING ASPD IN THE COMMUNITY: FURTHERING THE PD OFFENDER STRATEGY. Jessica Yakeley Portman Clinic Tavistock and Portman NHS Foundation Trust
 TREATING ASPD IN THE COMMUNITY: FURTHERING THE PD OFFENDER STRATEGY Jessica Yakeley Portman Clinic Tavistock and Portman NHS Foundation Trust Treating the untreatable? Lack of evidence base for ASPD Only
TREATING ASPD IN THE COMMUNITY: FURTHERING THE PD OFFENDER STRATEGY Jessica Yakeley Portman Clinic Tavistock and Portman NHS Foundation Trust Treating the untreatable? Lack of evidence base for ASPD Only
MS an Mental Health. Alison Carolan MS Mental Health Nurse Kings College Hospital. IMPARTS December 2013
 MS an Mental Health Alison Carolan MS Mental Health Nurse Kings College Hospital IMPARTS December 2013 MS and Mental Health MS is an autoimmune disease MS carries high risk of common mental disorders and
MS an Mental Health Alison Carolan MS Mental Health Nurse Kings College Hospital IMPARTS December 2013 MS and Mental Health MS is an autoimmune disease MS carries high risk of common mental disorders and
How To Help Veterans With A Mental Health Diagnosis
 RIGHT CARE RIGHT TIME RIGHT PLACE DEBORAH HARRIS-COBBINAH RN, MSN, CNS, NP, BC Faculty Disclosure Deborah Harris-Cobbinah, MSN, ANP,MHCNS,BC Conflict of Interest: None Employer: Dept. of Veterans Affairs
RIGHT CARE RIGHT TIME RIGHT PLACE DEBORAH HARRIS-COBBINAH RN, MSN, CNS, NP, BC Faculty Disclosure Deborah Harris-Cobbinah, MSN, ANP,MHCNS,BC Conflict of Interest: None Employer: Dept. of Veterans Affairs
Collaborative Care: Evidence-Based Mental Health Care in Primary Care Settings
 Collaborative Care: Evidence-Based Mental Health Care in Primary Care Settings Anna Ratzliff, MD, PhD Assistant Professor Associate Director for Education, Division of Integrated Care & Public Health Department
Collaborative Care: Evidence-Based Mental Health Care in Primary Care Settings Anna Ratzliff, MD, PhD Assistant Professor Associate Director for Education, Division of Integrated Care & Public Health Department
UW Medicine Integrated Mental Health Care. Laura Collins MSW, Darcy Jaffe ARNP Jürgen Unützer, MD, MPH, MA
 UW Medicine Integrated Mental Health Care Laura Collins MSW, Darcy Jaffe ARNP Jürgen Unützer, MD, MPH, MA Why Behavioral Health Care in Primary Care? 1. Access to care: Serve patients where they are 2.
UW Medicine Integrated Mental Health Care Laura Collins MSW, Darcy Jaffe ARNP Jürgen Unützer, MD, MPH, MA Why Behavioral Health Care in Primary Care? 1. Access to care: Serve patients where they are 2.
Service delivery interventions
 Service delivery interventions S A S H A S H E P P E R D D E P A R T M E N T O F P U B L I C H E A L T H, U N I V E R S I T Y O F O X F O R D CO- C O O R D I N A T I N G E D I T O R C O C H R A N E E P
Service delivery interventions S A S H A S H E P P E R D D E P A R T M E N T O F P U B L I C H E A L T H, U N I V E R S I T Y O F O X F O R D CO- C O O R D I N A T I N G E D I T O R C O C H R A N E E P
Telemedicine in Physical Health and Behavioral Health
 Telemedicine in Physical Health and Behavioral Health Collaborative Care Summit April 16, 2015 Shabana Khan, MD Assistant Professor of Psychiatry Western Psychiatric Institute and Clinic University of
Telemedicine in Physical Health and Behavioral Health Collaborative Care Summit April 16, 2015 Shabana Khan, MD Assistant Professor of Psychiatry Western Psychiatric Institute and Clinic University of
Mental Health Needs Assessment Personality Disorder Prevalence and models of care
 Mental Health Needs Assessment Personality Disorder Prevalence and models of care Introduction and definitions Personality disorders are a complex group of conditions identified through how an individual
Mental Health Needs Assessment Personality Disorder Prevalence and models of care Introduction and definitions Personality disorders are a complex group of conditions identified through how an individual
Challenges to Detection and Management of PTSD in Primary Care
 Challenges to Detection and Management of PTSD in Primary Care Karen H. Seal, MD, MPH University of California, San Francisco San Francisco VA Medical Center General Internal Medicine Section PTSD is Prevalent
Challenges to Detection and Management of PTSD in Primary Care Karen H. Seal, MD, MPH University of California, San Francisco San Francisco VA Medical Center General Internal Medicine Section PTSD is Prevalent
Depression, anxiety and long term conditions. Linda Gask Professor of Primary Care Psychiatry University of Manchester
 Depression, anxiety and long term conditions Linda Gask Professor of Primary Care Psychiatry University of Manchester Depression and LTCs People with LTCs are twice as likely than other adults to suffer
Depression, anxiety and long term conditions Linda Gask Professor of Primary Care Psychiatry University of Manchester Depression and LTCs People with LTCs are twice as likely than other adults to suffer
Mental Health Service Delivery In Nursing Homes
 Mental Health Service Delivery In Nursing Homes Steve Bartels, MD, MS Professor of Psychiatry and Community & Family Medicine Director, Dartmouth Centers for Health and Aging Overview Prevalence of mental
Mental Health Service Delivery In Nursing Homes Steve Bartels, MD, MS Professor of Psychiatry and Community & Family Medicine Director, Dartmouth Centers for Health and Aging Overview Prevalence of mental
Worksite Depression Screening and Treatment: An Innovative, Integrated Program
 Photos placed in horizontal position with even amount of white space between photos and header Photos placed in horizontal position with even amount of white space between photos and header Worksite Depression
Photos placed in horizontal position with even amount of white space between photos and header Photos placed in horizontal position with even amount of white space between photos and header Worksite Depression
Practice Redesign for Dementia: The UCLA Alzheimer's and Dementia Care Program
 Practice Redesign for Dementia: The UCLA Alzheimer's and Dementia Care Program Zaldy S. Tan, MD, MPH Medical Director, UCLA Alzheimer s and Dementia Care Program Director, California Geriatric Education
Practice Redesign for Dementia: The UCLA Alzheimer's and Dementia Care Program Zaldy S. Tan, MD, MPH Medical Director, UCLA Alzheimer s and Dementia Care Program Director, California Geriatric Education
BACKGROUND. ADA and the European Association recently issued a consensus algorithm for management of type 2 diabetes
 BACKGROUND More than 25% of people with diabetes take insulin ADA and the European Association recently issued a consensus algorithm for management of type 2 diabetes Insulin identified as the most effective
BACKGROUND More than 25% of people with diabetes take insulin ADA and the European Association recently issued a consensus algorithm for management of type 2 diabetes Insulin identified as the most effective
Telehealth interventions for mood disorders: What? Who? How?
 Telehealth interventions for mood disorders: What? Who? How? Gregory Simon MD MPH Group Health Center for Health Studies, Seattle, WA Public Health Impact Depression: Lifetime prevalence of 16%, One-year
Telehealth interventions for mood disorders: What? Who? How? Gregory Simon MD MPH Group Health Center for Health Studies, Seattle, WA Public Health Impact Depression: Lifetime prevalence of 16%, One-year
The use of alcohol and drugs and HIV treatment compliance in Brazil
 The use of alcohol and drugs and HIV treatment compliance in Brazil André Malbergier, MD, PhD Hospital das Clínicas Medical School University of São Paulo Brasil The Casa da AIDS offers specialized integral
The use of alcohol and drugs and HIV treatment compliance in Brazil André Malbergier, MD, PhD Hospital das Clínicas Medical School University of São Paulo Brasil The Casa da AIDS offers specialized integral
DEPRESSION CARE PROCESS STEP EXPECTATIONS RATIONALE
 1 DEPRESSION CARE PROCESS STEP EXPECTATIONS RATIONALE ASSESSMENT/PROBLEM RECOGNITION 1. Did the staff and physician seek and document risk factors for depression and any history of depression? 2. Did staff
1 DEPRESSION CARE PROCESS STEP EXPECTATIONS RATIONALE ASSESSMENT/PROBLEM RECOGNITION 1. Did the staff and physician seek and document risk factors for depression and any history of depression? 2. Did staff
The Future Is Now: Psychiatric Mental Health Nursing Graduate Preparation for Integrated Care
 The Future Is Now: Psychiatric Mental Health Nursing Graduate Preparation for Integrated Care Beth Phoenix, PhD, RN Health Sciences Clinical Professor UCSF School of Nursing beth.phoenix@nursing.ucsf.edu
The Future Is Now: Psychiatric Mental Health Nursing Graduate Preparation for Integrated Care Beth Phoenix, PhD, RN Health Sciences Clinical Professor UCSF School of Nursing beth.phoenix@nursing.ucsf.edu
Healthy Coping in Diabetes Self Management
 Healthy Coping in Diabetes Self Management Support for this product was provided by a grant from the Robert Wood Johnson Foundation in Princeton, New Jersey, 2009 Objectives Describe the relationship among
Healthy Coping in Diabetes Self Management Support for this product was provided by a grant from the Robert Wood Johnson Foundation in Princeton, New Jersey, 2009 Objectives Describe the relationship among
Comparison of Two Dual Diagnosis Tracks: Enhanced Dual Diagnosis versus Standard Dual Diagnosis Treatment Report Date: July 17, 2003
 Comparison of Two Dual Diagnosis Tracks: Enhanced Dual Diagnosis versus Standard Dual Diagnosis Treatment Report Date: July 17, 2003 Objective: To compare treatment outcomes and treatment costs for four
Comparison of Two Dual Diagnosis Tracks: Enhanced Dual Diagnosis versus Standard Dual Diagnosis Treatment Report Date: July 17, 2003 Objective: To compare treatment outcomes and treatment costs for four
Mental Health. Health Equity Highlight: Women
 Mental Health Background A person s ability to carry on productive activities and live a rewarding life is affected not only by physical health but by mental health. In addition, mental well-being can
Mental Health Background A person s ability to carry on productive activities and live a rewarding life is affected not only by physical health but by mental health. In addition, mental well-being can
Improving primary care management of depression in adults with comorbid chronic illnesses
 Executive summary of current research Improving primary care management of depression in adults with comorbid chronic illnesses Principal Investigator Jane McCusker, MD DrPH Co-Investigators Martin Cole,
Executive summary of current research Improving primary care management of depression in adults with comorbid chronic illnesses Principal Investigator Jane McCusker, MD DrPH Co-Investigators Martin Cole,
Approved: New Requirements for Residential and Outpatient Eating Disorders Programs
 Approved: New Requirements for Residential and Outpatient Eating Disorders Programs Effective July 1, 2016, for Behavioral Health Care Accreditation Program The Joint Commission added several new requirements
Approved: New Requirements for Residential and Outpatient Eating Disorders Programs Effective July 1, 2016, for Behavioral Health Care Accreditation Program The Joint Commission added several new requirements
Using web-based videoconferencing to deliver both standard and intensified levels of substance abuse counseling treatment. Van L.
 Using web-based videoconferencing to deliver both standard and intensified levels of substance abuse counseling treatment Van L. King, MD Addiction Treatment Services Johns Hopkins Bayview Medical Center
Using web-based videoconferencing to deliver both standard and intensified levels of substance abuse counseling treatment Van L. King, MD Addiction Treatment Services Johns Hopkins Bayview Medical Center
October 22, 2014 Jill M. Gregoire RN, MSN Quality Assurance/Clinical Operations Director Indian Stream Health Center Colebrook, NH
 October 22, 2014 Jill M. Gregoire RN, MSN Quality Assurance/Clinical Operations Director Indian Stream Health Center Colebrook, NH Why Stratify Risk for Your Patients? NCQA s Patient-Centered Medical Home
October 22, 2014 Jill M. Gregoire RN, MSN Quality Assurance/Clinical Operations Director Indian Stream Health Center Colebrook, NH Why Stratify Risk for Your Patients? NCQA s Patient-Centered Medical Home
Depression often coexists with other chronic conditions
 Depression A treatable disease PROPORTION OF PATIENTS WHO ARE DEPRESSED, BY CHRONIC CONDITION Diabetes 33% Parkinson s Disease % Recent Stroke % Hospitalized with Cancer 42% Recent Heart Attack 45% SOURCE:
Depression A treatable disease PROPORTION OF PATIENTS WHO ARE DEPRESSED, BY CHRONIC CONDITION Diabetes 33% Parkinson s Disease % Recent Stroke % Hospitalized with Cancer 42% Recent Heart Attack 45% SOURCE:
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Best Practices Managing Patients with Multiple Chronic Conditions Advocate Medical Group Case Study Organization Profile Advocate Medical Group is part of Advocate Health Care, a large, integrated, not-for-profit
Preferred Practice Guidelines Bipolar Disorder in Children and Adolescents
 These Guidelines are based in part on the following: American Academy of Child and Adolescent Psychiatry s Practice Parameter for the Assessment and Treatment of Children and Adolescents With Bipolar Disorder,
These Guidelines are based in part on the following: American Academy of Child and Adolescent Psychiatry s Practice Parameter for the Assessment and Treatment of Children and Adolescents With Bipolar Disorder,
Improving the Measurement Properties of Depressive Symptom Instruments for Use after SCI
 Improving the Measurement Properties of Depressive Symptom Instruments for Use after SCI Allen Heinemann, PhD Ryan Williams, PhD Charles Bombardier, PhD Martin Forchheimer, MPP Jesse Fann, MD Holly Neumann,
Improving the Measurement Properties of Depressive Symptom Instruments for Use after SCI Allen Heinemann, PhD Ryan Williams, PhD Charles Bombardier, PhD Martin Forchheimer, MPP Jesse Fann, MD Holly Neumann,
Profile: Incorporating Routine Behavioral Health Screenings Into the Patient-Centered Medical Home
 104 A LOOK TO THE FUTURE Profile: Incorporating Routine Behavioral Health Screenings Into the Patient-Centered Medical Home Background Management of chronic diseases can be challenging in primary care,
104 A LOOK TO THE FUTURE Profile: Incorporating Routine Behavioral Health Screenings Into the Patient-Centered Medical Home Background Management of chronic diseases can be challenging in primary care,
The NYU Caregiver Intervention
 The NYU Caregiver Intervention Translating an Evidence-based Intervention for Spouse-Caregivers into Community Settings Mary S. Mittelman, DrPH Center of Excellence for Brain Aging and Dementia NYU Langone
The NYU Caregiver Intervention Translating an Evidence-based Intervention for Spouse-Caregivers into Community Settings Mary S. Mittelman, DrPH Center of Excellence for Brain Aging and Dementia NYU Langone
(4) To characterize the course of illness after adequate response to and continuation on the treatments found effective for individual participants.
 To characterize the course of illness after adequate response to and continuation on the treatments found effective for individual participants.") I. Specific Aims/Objectives STAR*D has several main objectives and is powered to assess the effectiveness of a sequence of treatments at various levels of treatment. Most of these objectives entail evaluating
I. Specific Aims/Objectives STAR*D has several main objectives and is powered to assess the effectiveness of a sequence of treatments at various levels of treatment. Most of these objectives entail evaluating
Psychiatric Comorbidity in Methamphetamine-Dependent Patients
 Psychiatric Comorbidity in Methamphetamine-Dependent Patients Suzette Glasner-Edwards, Ph.D. UCLA Integrated Substance Abuse Programs August11 th, 2010 Overview Comorbidity in substance users Risk factors
Psychiatric Comorbidity in Methamphetamine-Dependent Patients Suzette Glasner-Edwards, Ph.D. UCLA Integrated Substance Abuse Programs August11 th, 2010 Overview Comorbidity in substance users Risk factors
Developmental. SBIRT Substance Abuse (AUDIT & DAST Scales)
") s Tools Developmental 96110 Developmental testing; limited (e.g., Pediatric Symptom Checklist, Vanderbilt AD/HD, Developmental Screening Test II, Early Language Milestone Screen), with interpretation and
s Tools Developmental 96110 Developmental testing; limited (e.g., Pediatric Symptom Checklist, Vanderbilt AD/HD, Developmental Screening Test II, Early Language Milestone Screen), with interpretation and
Disease Management Identifications and Stratification Health Risk Assessment Level 1: Level 2: Level 3: Stratification
 Disease Management UnitedHealthcare Disease Management (DM) programs are part of our innovative Care Management Program. Our Disease Management (DM) program is guided by the principles of the UnitedHealthcare
Disease Management UnitedHealthcare Disease Management (DM) programs are part of our innovative Care Management Program. Our Disease Management (DM) program is guided by the principles of the UnitedHealthcare
Population Health Management For Behavioral Health. MHA s 2015 Annual Conference June 3, 2015
 Population Health Management For Behavioral Health MHA s 2015 Annual Conference June 3, 2015 Goals of the Affordable Care Act Improve the health of populations Lower per capita costs Improve the patient
Population Health Management For Behavioral Health MHA s 2015 Annual Conference June 3, 2015 Goals of the Affordable Care Act Improve the health of populations Lower per capita costs Improve the patient
Disclosure. I have the following relationships with commercial interests:
 Disclosure Electra Paskett, Ph.D., MPH I have the following relationships with commercial interests: Merck Research grant, in-kind donation Pfizer Stock ownership Meridian Bioscience Stock ownership A
Disclosure Electra Paskett, Ph.D., MPH I have the following relationships with commercial interests: Merck Research grant, in-kind donation Pfizer Stock ownership Meridian Bioscience Stock ownership A
Integrated Health Care Models and Practices
 Integrated Health Care Models and Practices The Greater Houston Behav io r al Health Affordable Care Act Initiative S e c o n d C o m m u n i t y E d u c a t i o n E v e n t I n t e g r a t e d H e a l
Integrated Health Care Models and Practices The Greater Houston Behav io r al Health Affordable Care Act Initiative S e c o n d C o m m u n i t y E d u c a t i o n E v e n t I n t e g r a t e d H e a l
The Relationship Between Empowerment Care and Quality of Life Among Members of Assisted Living Facilities
 The Relationship Between Empowerment Care and Quality of Life Among Members of Assisted Living Facilities Kirsten Kranz Faculty Sponsor: Dung Ngo, Department of Psychology ABSTRACT The purpose of this
The Relationship Between Empowerment Care and Quality of Life Among Members of Assisted Living Facilities Kirsten Kranz Faculty Sponsor: Dung Ngo, Department of Psychology ABSTRACT The purpose of this
PAYMENT INNOVATIONS SUPPORTING BEHAVIORAL HEALTHCARE DELIVERY IMPROVEMENT. NGA July 2015
 PAYMENT INNOVATIONS SUPPORTING BEHAVIORAL HEALTHCARE DELIVERY IMPROVEMENT NGA July 2015 My Background Medicaid Director Previously DMH Medical Director 20 years Practicing Psychiatrist CMHCs 10 years FQHC
PAYMENT INNOVATIONS SUPPORTING BEHAVIORAL HEALTHCARE DELIVERY IMPROVEMENT NGA July 2015 My Background Medicaid Director Previously DMH Medical Director 20 years Practicing Psychiatrist CMHCs 10 years FQHC
Licensed Mental Health Counselors and the Military Health System
 Licensed Mental Health Counselors and the Military Health System LT Rick Schobitz, Ph.D., USPHS Deputy Director, Behavioral Medicine Division Office of the Chief Medical Officer TRICARE Management Activity
Licensed Mental Health Counselors and the Military Health System LT Rick Schobitz, Ph.D., USPHS Deputy Director, Behavioral Medicine Division Office of the Chief Medical Officer TRICARE Management Activity
Impact of Brief Intervention on Problem Drug Use in Public Hospital Based Primary Care Settings
 Impact of Brief Intervention on Problem Drug Use in Public Hospital Based Primary Care Settings Antoinette Krupski, PhD University of Washington at Harborview Medical Center Seattle, Washington USA Coauthors
Impact of Brief Intervention on Problem Drug Use in Public Hospital Based Primary Care Settings Antoinette Krupski, PhD University of Washington at Harborview Medical Center Seattle, Washington USA Coauthors
Antidepressants and suicidal thoughts and behaviour. Pharmacovigilance Working Party. January 2008
 Antidepressants and suicidal thoughts and behaviour Pharmacovigilance Working Party January 2008 PhVWP PAR January 2008 Page 1/15 1. Introduction The Pharmacovigilance Working Party has on a number of
Antidepressants and suicidal thoughts and behaviour Pharmacovigilance Working Party January 2008 PhVWP PAR January 2008 Page 1/15 1. Introduction The Pharmacovigilance Working Party has on a number of
The family physician system reform in small cities in I.R. Iran
 Evaluating Impact: Turning Promises into Evidence The family physician system reform in small cities in I.R. Iran Masoud Abolhallaj, Abbas Vosoogh, Arash Rashidian, Alireza Delavari Cairo, January 2008
Evaluating Impact: Turning Promises into Evidence The family physician system reform in small cities in I.R. Iran Masoud Abolhallaj, Abbas Vosoogh, Arash Rashidian, Alireza Delavari Cairo, January 2008
With Depression Without Depression 8.0% 1.8% Alcohol Disorder Drug Disorder Alcohol or Drug Disorder
 Minnesota Adults with Co-Occurring Substance Use and Mental Health Disorders By Eunkyung Park, Ph.D. Performance Measurement and Quality Improvement May 2006 In Brief Approximately 16% of Minnesota adults
Minnesota Adults with Co-Occurring Substance Use and Mental Health Disorders By Eunkyung Park, Ph.D. Performance Measurement and Quality Improvement May 2006 In Brief Approximately 16% of Minnesota adults
Assessment of depression in adults in primary care
 Assessment of depression in adults in primary care Adapted from: Identification of Common Mental Disorders and Management of Depression in Primary care. New Zealand Guidelines Group 1 The questions and
Assessment of depression in adults in primary care Adapted from: Identification of Common Mental Disorders and Management of Depression in Primary care. New Zealand Guidelines Group 1 The questions and
Integrated Care: The Behavioral Health Primary Care Model. M. Hunter Hansen, PsyD, MP
 Integrated Care: The Behavioral Health Primary Care Model M. Hunter Hansen, PsyD, MP Objectives Brief Review of the History of Mental Health Care The State of Mental Healthcare The Role of Primary Care
Integrated Care: The Behavioral Health Primary Care Model M. Hunter Hansen, PsyD, MP Objectives Brief Review of the History of Mental Health Care The State of Mental Healthcare The Role of Primary Care
Medication Management of Depressive Disorders in Children and Adolescents. Satya Tata, M.D. Kansas University Medical Center
 Medication Management of Depressive Disorders in Children and Adolescents Satya Tata, M.D. Kansas University Medical Center First Line Medications SSRIs Prozac (Fluoxetine): 5-605 mg Zoloft (Sertraline):
Medication Management of Depressive Disorders in Children and Adolescents Satya Tata, M.D. Kansas University Medical Center First Line Medications SSRIs Prozac (Fluoxetine): 5-605 mg Zoloft (Sertraline):
Psychosocial treatment of late-life depression with comorbid anxiety
 Psychosocial treatment of late-life depression with comorbid anxiety Viviana Wuthrich Centre for Emotional Health Macquarie University, Sydney, Australia Why Comorbidity? Comorbidity is Common Common disorders,
Psychosocial treatment of late-life depression with comorbid anxiety Viviana Wuthrich Centre for Emotional Health Macquarie University, Sydney, Australia Why Comorbidity? Comorbidity is Common Common disorders,
Depression Screening in Primary Care
 Depression Screening in Primary Care Toni Johnson, MD Kristen Palcisco, BA, MSN, APRN MetroHealth System Our Vision Make Greater Cleveland a healthier place to live and a better place to do business. 2
Depression Screening in Primary Care Toni Johnson, MD Kristen Palcisco, BA, MSN, APRN MetroHealth System Our Vision Make Greater Cleveland a healthier place to live and a better place to do business. 2
Primary Care-Mental Health Integration (PC-MHI) Functional Tool
 Functional Tool") Primary Care-Mental Health Integration (PC-MHI) Functional Tool The purpose of this tool is to outline the essential elements of a fully functional Primary Care-Mental Health Integration (PC-MHI) program
Primary Care-Mental Health Integration (PC-MHI) Functional Tool The purpose of this tool is to outline the essential elements of a fully functional Primary Care-Mental Health Integration (PC-MHI) program
MOH CLINICAL PRACTICE GUIDELINES 6/2011 DEPRESSION
 MOH CLINICAL PRACTICE GUIDELINES 6/2011 DEPRESSION Executive summary of recommendations Details of recommendations can be found in the main text at the pages indicated. Clinical evaluation D The basic
MOH CLINICAL PRACTICE GUIDELINES 6/2011 DEPRESSION Executive summary of recommendations Details of recommendations can be found in the main text at the pages indicated. Clinical evaluation D The basic
Depression Support Resources: Telephonic/Care Management Follow-up
 Depression Support Resources: Telephonic/Care Management Follow-up Depression Support Resources: Telephonic/Care Management Follow-up Primary Care Toolkit September 2015 Page 29 Role of the Phone Clinician
Depression Support Resources: Telephonic/Care Management Follow-up Depression Support Resources: Telephonic/Care Management Follow-up Primary Care Toolkit September 2015 Page 29 Role of the Phone Clinician
HealthCare Partners of Nevada. Heart Failure
 HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
HealthCare Partners of Nevada Heart Failure Disease Management Program 2010 HF DISEASE MANAGEMENT PROGRAM The HealthCare Partners of Nevada (HCPNV) offers a Disease Management program for members with
How To Understand The Effectiveness Of Case Management
 Effect of Case Management on Time to Return to Work: A Systematic Review and Meta-Analysis IWH Plenary; March 29, 2011 J.W. Busse, DC, PhD Background In an effort to optimize disability management practices,
Effect of Case Management on Time to Return to Work: A Systematic Review and Meta-Analysis IWH Plenary; March 29, 2011 J.W. Busse, DC, PhD Background In an effort to optimize disability management practices,
The State of Mental Health and Aging in America
 Issue Brief #2: Addressing Depression in Older Adults: Selected Evidence-Based Programs In recognition of the essential role mental health plays in overall health, the Healthy Aging Program at the Centers
Issue Brief #2: Addressing Depression in Older Adults: Selected Evidence-Based Programs In recognition of the essential role mental health plays in overall health, the Healthy Aging Program at the Centers
Integrating mental health with other NCDs
 Integrating mental health with other NCDs Inge Petersen, PhD. programme for improving mental health care Outline of presentation Why integrate mental health with other NCDs? Example of integration using
Integrating mental health with other NCDs Inge Petersen, PhD. programme for improving mental health care Outline of presentation Why integrate mental health with other NCDs? Example of integration using
echat: Screening & intervening for mental health & lifestyle issues
 echat: Screening & intervening for mental health & lifestyle issues Felicity Goodyear-Smith Professor & Academic Head Dept of General Practice & Primary Health Care Faculty of Medicine & Health Science
echat: Screening & intervening for mental health & lifestyle issues Felicity Goodyear-Smith Professor & Academic Head Dept of General Practice & Primary Health Care Faculty of Medicine & Health Science
IN 2004, THE Japanese government announced a. Development of a clinical pathway for long-term inpatients with schizophreniapcn_2040 99..
 Psychiatry and Clinical Neurosciences 2010; 64: 99 103 doi:10.1111/j.1440-1819.2009.02040.x Short Communication Development of a clinical pathway for long-term inpatients with schizophreniapcn_2040 99..103
Psychiatry and Clinical Neurosciences 2010; 64: 99 103 doi:10.1111/j.1440-1819.2009.02040.x Short Communication Development of a clinical pathway for long-term inpatients with schizophreniapcn_2040 99..103
GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services
 GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services Aged, Blind and Disabled Stakeholder Presentation Indiana Family and Social Services Administration August
GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services Aged, Blind and Disabled Stakeholder Presentation Indiana Family and Social Services Administration August
Suicide & Older Adults Julie E. Malphurs, PhD
 Suicide & Older Adults Julie E. Malphurs, PhD Lead Program Analyst, Mental Health Service Miami VA Healthcare System & Asst. Professor of Research Department of Psychiatry and Behavioral Science Center
Suicide & Older Adults Julie E. Malphurs, PhD Lead Program Analyst, Mental Health Service Miami VA Healthcare System & Asst. Professor of Research Department of Psychiatry and Behavioral Science Center
An Integrated Approach to Treating Depression in the Adult Primary Care Setting
 An Integrated Approach to Treating Depression in the Adult Primary Care Setting February 5, 2014 Alexander Blount, EdD Director, Center for Integrated Primary Care Lily Awad, MD Associate Medical Director,
An Integrated Approach to Treating Depression in the Adult Primary Care Setting February 5, 2014 Alexander Blount, EdD Director, Center for Integrated Primary Care Lily Awad, MD Associate Medical Director,
Henriëtte van der Horst VUmc Head of Department of General Practice and Elderly Care Medicine
 MUS and psychiatry in primary care Henriëtte van der Horst VUmc Head of Department of General Practice and Elderly Care Medicine Double Dutch: two topics Major changes in the mental health care organisation
MUS and psychiatry in primary care Henriëtte van der Horst VUmc Head of Department of General Practice and Elderly Care Medicine Double Dutch: two topics Major changes in the mental health care organisation
Fixing Mental Health Care in America
 Fixing Mental Health Care in America A National Call for Measurement Based Care in Behavioral Health and Primary Care An Issue Brief Released by The Kennedy Forum Prepared by: John Fortney PhD, Rebecca
Fixing Mental Health Care in America A National Call for Measurement Based Care in Behavioral Health and Primary Care An Issue Brief Released by The Kennedy Forum Prepared by: John Fortney PhD, Rebecca
Oncology Nursing Society Annual Progress Report: 2008 Formula Grant
 Oncology Nursing Society Annual Progress Report: 2008 Formula Grant Reporting Period July 1, 2009 June 30, 2010 Formula Grant Overview The Oncology Nursing Society received $12,473 in formula funds for
Oncology Nursing Society Annual Progress Report: 2008 Formula Grant Reporting Period July 1, 2009 June 30, 2010 Formula Grant Overview The Oncology Nursing Society received $12,473 in formula funds for
Co-Occurring Disorder-Related Quick Facts: ELDERLY
 Co-Occurring Disorder-Related Quick Facts: ELDERLY Elderly: In 2004, persons over the age of 65 reached a total of 36.3 million in the United States, an increase of approximately nine percent over the
Co-Occurring Disorder-Related Quick Facts: ELDERLY Elderly: In 2004, persons over the age of 65 reached a total of 36.3 million in the United States, an increase of approximately nine percent over the
Breathe With Ease. Asthma Disease Management Program
 Breathe With Ease Asthma Disease Management Program MOLINA Breathe With Ease Pediatric and Adult Asthma Disease Management Program Background According to the National Asthma Education and Prevention Program
Breathe With Ease Asthma Disease Management Program MOLINA Breathe With Ease Pediatric and Adult Asthma Disease Management Program Background According to the National Asthma Education and Prevention Program
Quality of Life and Illness Perception in Adult EB Clinic Patients
 Quality of Life and Illness Perception in Adult EB Clinic Patients Diane Beattie, Psychologist in Clinical Training Jacinta Kennedy, Principal Clinical Psychologist Katherine Sweeney, Clinical Nurse Specialist
Quality of Life and Illness Perception in Adult EB Clinic Patients Diane Beattie, Psychologist in Clinical Training Jacinta Kennedy, Principal Clinical Psychologist Katherine Sweeney, Clinical Nurse Specialist
Provider Training. Behavioral Health Screening, Referral, and Coding Requirements
 Provider Training Behavioral Health Screening, Referral, and Coding Requirements Training Outline I. Behavioral Health Screening Requirements and Referrals II. Healthy Behaviors Substance and Alcohol Abuse
Provider Training Behavioral Health Screening, Referral, and Coding Requirements Training Outline I. Behavioral Health Screening Requirements and Referrals II. Healthy Behaviors Substance and Alcohol Abuse
Mental Health Services for Children and Youth in Nova Scotia
 Mental Health Services for Children and Youth in Nova Scotia Presentation to the Standing Committee on Community Services - June 1, 2010 Patricia Murray, Director of Children s Services Mental Health,
Mental Health Services for Children and Youth in Nova Scotia Presentation to the Standing Committee on Community Services - June 1, 2010 Patricia Murray, Director of Children s Services Mental Health,
Depression, Mental Health and Native American Youth
 Depression, Mental Health and Native American Youth Aisha Mays, MD UCSF Department of Family And Community Medicine Native American Health Center Oakland, CA July 8, 2015 Presenter Disclosures No relationships
Depression, Mental Health and Native American Youth Aisha Mays, MD UCSF Department of Family And Community Medicine Native American Health Center Oakland, CA July 8, 2015 Presenter Disclosures No relationships
Frequent headache is defined as headaches 15 days/month and daily. Course of Frequent/Daily Headache in the General Population and in Medical Practice
 DISEASE STATE REVIEW Course of Frequent/Daily Headache in the General Population and in Medical Practice Egilius L.H. Spierings, MD, PhD, Willem K.P. Mutsaerts, MSc Department of Neurology, Brigham and
DISEASE STATE REVIEW Course of Frequent/Daily Headache in the General Population and in Medical Practice Egilius L.H. Spierings, MD, PhD, Willem K.P. Mutsaerts, MSc Department of Neurology, Brigham and
Running Head: INTERNET USE IN A COLLEGE SAMPLE. TITLE: Internet Use and Associated Risks in a College Sample
 Running Head: INTERNET USE IN A COLLEGE SAMPLE TITLE: Internet Use and Associated Risks in a College Sample AUTHORS: Katherine Derbyshire, B.S. Jon Grant, J.D., M.D., M.P.H. Katherine Lust, Ph.D., M.P.H.
Running Head: INTERNET USE IN A COLLEGE SAMPLE TITLE: Internet Use and Associated Risks in a College Sample AUTHORS: Katherine Derbyshire, B.S. Jon Grant, J.D., M.D., M.P.H. Katherine Lust, Ph.D., M.P.H.
Integrating Primary Care and Behavioral Health
 Integrating Primary Care and Behavioral Health IMPACT MODIFIED Presenters Bridget Harrison, MD, MPH Interim Chair, Dept. of Family Medicine Santa Clara Valley Medical Center (SCVMC) San Jose, CA Elena
Integrating Primary Care and Behavioral Health IMPACT MODIFIED Presenters Bridget Harrison, MD, MPH Interim Chair, Dept. of Family Medicine Santa Clara Valley Medical Center (SCVMC) San Jose, CA Elena