Meaningful Use Stage 1 and 2 Your Survival Guide!
|
|
|
- Sophia Nicholson
- 8 years ago
- Views:
Transcription
1 Meaningful Use Stage 1 and 2 Your Survival Guide! Dr. Gross is on the Vision Expo Conference Advisory Board Dr. Henry and Dr. Gross are affiliated with EHRGURU.NET and have lectured for numerous companies including Topcon, First Insight, and the AOA Jay W. Henry, O.D., M.S. Philip J. Gross, O.D.
2 Thank You to Our Sponsor!
3 Game Plan Meaningful Use Stage 1 and Stage 2: Objective requirements Clinical implications of each objective Objective exemptions Objective compliance How to navigate the different stages
4 Meaningful Use
5 Meaningful Use Meaningful use is the set of standards defined by the Centers for Medicare & Medicaid Services (CMS) Incentive Programs that governs the use of electronic health records and allows eligible providers and hospitals to earn incentive payments by meeting very specific criteria The overall goal of meaningful use is to promote the spread of electronic health records to improve health care in the United States
6 Meaningful Use Specific Goals of Meaningful Use Improve quality of health care Improve safety, efficiency and reduce health disparities Engage patients and families in their care Improve Care Coordination Improve population and public health Ensure adequate privacy and security protections for personal health information
7 Meaningful Use: The Next Stages All providers will complete two years of Stage 1 Meaningful Use (MU) before advancing to the Stage 2 criteria in their 3 rd or 4 th year. Maximum Payment by Start Year Annual Incentive Payment by Stage of Meaningful Use $44,000 $18,000 $12,000 $8,000 $4,000 $2, $44,000 $18,000 $12,000 $8,000 $4,000 $2, $39,000 $15,000 $12,000 $8,000 $4, $24,000 $12,000 $8,000 $4,000
8 Meaningful Use: Reporting Period First year of participation Providers must demonstrate meaningful use for any continuous 90-day reporting period All subsequent years of participation except 2014 Providers must demonstrate meaningful use for a full year EHR reporting period (entire calendar year) For 2014 only (unless it s your first year of participation) All providers regardless of their stage of meaningful use are only required to demonstrate meaningful use for a 3-month EHR reporting period For Medicare EHR incentive program it is fixed to a quarter of the calendar year (1/1 3/31, 4/1-6/30, 7/1 9/30, 10/1 12/31) For Medicaid EHR incentive program the reporting period is not fixed
9 Reporting Periods YEAR 1 All Other Years 2014 Unless it is your first year
10 Meaningful Use Objectives Meaningful use established a core and menu structure for objectives that providers must achieve Core objectives are objectives that all providers must meet Some have exclusions which could exempt you from having to complete that objective (If you exempt from an objective you get credit as if you did it) Menu objectives allow the providers to select from a list a certain number of objectives to meet Some have exclusions which could exempt you from having to complete that objective
11 Stage 1 Changes CMS has announced changes to Stage 1 Meaningful Use objectives Some changes take effect Jan. 1 st, 2013 Some changes take effect in 2014 but are optional for 2013 We will cover all of these changes in the following slides. Fasten your seatbelts!
12 Stage 1 Change on Exclusions to Menu Items Beginning in 2014 You will no longer be permitted to count an exclusion toward the minimum of 5 menu objectives if there are other menu objectives which you can achieve In other words, a provider cannot select a menu objective and claim an exclusion for it if there are other menu objectives they can meet EPs will not be penalized for selecting a menu objective and claiming the exclusion if they would also qualify for the exclusions for all the remaining menu objectives
13 Meaningful Use: Stage 1 vs. Stage 2 Original Stage 1 criteria for Eligible Professionals 15 core objectives 5 of 10 menu objectives (1 must be public health) 20 total objectives Stage 2 criteria for Eligible Professionals 17 core objectives 3 of 6 menu objectives 20 total objectives
14 Stage 1 and Stage 2 Objectives For Stage 1 Information Follow For Stage 2 Information Follow 15 Stage 1 Core Objectives 10 Stage 1 Menu Objectives 17 Stage 2 Core Objectives 6 Stage 2 Menu Objectives
15 Beginning of Stage 1 Core Objectives Beginning of Stage 2 Core Objectives
16 Stage 1 Core Objectives 1. Computerized provider order entry (CPOE) 2. Drug-drug and drug-allergy checks 3. E-Prescribing (erx) 4. Record patient demographics 5. Maintain an up to date problem list of current and active diagnoses 6. Maintain active medication list 7. Maintain active medication allergy list 8. Record and chart changes in vital signs 9. Record smoking status for patients 13 years or older 10. Implement clinical decision support 11. Report ambulatory clinical quality measures to CMS / States 12. Provide patients with an electronic copy of their health information, upon request 13. Provide Clinical summaries for patients for each office visit 14. Capability to exchange key clinical information 15. Protect electronic health information
17 Stage 2 Core Objectives 1. Use computerized provider order entry (CPOE) for medication, laboratory and radiology orders 2. Generate and transmit permissible prescriptions electronically (erx) 3. Record demographic information 4. Record and chart changes in vital signs 5. Record smoking status for patients 13 years old or older 6. Use clinical decision support to improve performance on high-priority health conditions 7. Provide patients the ability to view online, download and transmit their health information 8. Provide clinical summaries for patients for each office visit 9. Protect electronic health information created or maintained by the Certified EHR Technology 10. Incorporate clinical lab-test results into Certified EHR Technology 11. Generate lists of patients by specific conditions to use for quality improvement, reduction of disparities, research, or outreach 12. Use clinically relevant information to identify patients who should receive reminders for preventive/follow-up care 13. Use certified EHR technology to identify patient-specific education resources 14. Perform medication reconciliation 15. Provide summary of care record for each transition of care or referral 16. Submit electronic data to immunization registries 17. Use secure electronic messaging to communicate with patients on relevant health information
18 CPOE: Computerized Provider Order Entry More than 30% of all unique patients seen by the EP with at least one medication in their medication list must have at least one medication order entered using CPOE You can be excluded from meeting this objective if you write fewer than 100 prescriptions during the reporting period More than 60% of medication, 30% of laboratory, and 30% of radiology orders created by the EP during the EHR reporting period must be recorded using CPOE You can be excluded from meeting this objective if you write fewer than 100 prescriptions during the reporting period
19 CPOE Changes Stage 1: > 30% of unique patients with a medication order have at least one medication ordered using CPOE Stage 2: Based on total number of medication, lab, radiology orders not unique patients with a medication order Increases % of medication orders: > 60% of medication orders Adds Lab and Radiology orders: > 30%
20 Stage 1 CPOE Alternate Measure Optional Change 2013 and beyond Beginning in 2013, CMS has added an optional alternate measure for Stage 1 CPOE EPs may select either the original CPOE or the alternate CPOE measure for Stage 1 Alternate Measure More than 30% of all medication orders, created by the EP, during the EHR reporting period are recorded using CPOE
21 Computerized Provider Order Entry Clinical Significance? Directly entering orders into a computer has the benefit of reducing errors by minimizing the ambiguity of hand-written orders, but a much greater benefit is seen with the combination of CPOE and clinical decision support tools Implementation of CPOE is being increasingly encouraged as an important solution to the challenge of reducing medical errors, and improving health care quality and efficiency
22
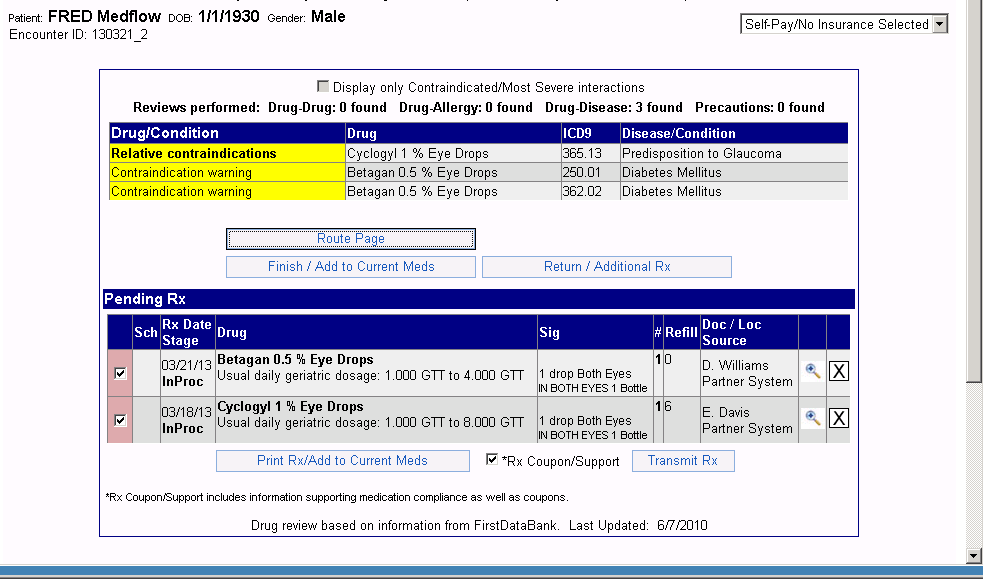
23 Drug-Drug and Drug-Allergy Checks EP has enabled the functionality to automatically check for drug-drug or drugallergy interactions for the entire EHR reporting period There is no exclusion for this objective. No longer a separate objective for Stage 2 It has been incorporated into the Stage 2 Clinical Decision Support measure
24 Drug-Drug and Drug-Allergy Changes Stage 1: EP has enabled the functionality to automatically check for drug-drug or drug-allergy interactions for the entire EHR reporting period Stage 2: No longer an objective has been incorporated and combined into Clinical Decision Support Measure
25 Drug-Drug and Drug-Allergy Checks Clinical Significance? You are responsible for understanding the potential negative interaction a medication you prescribe may have when combined with another medication the patient is already taking Remember this goes back to the importance of keeping an active medication list up to date for each patient Lipitor and Biaxin is there a problem with this combination? Oral antibiotic and Oral contraceptive is there a problem? If we are using a certified EHR with eprescribing, this should occur as part of the ordering of the medications Be sure this feature is turned on and active for you entire reporting period
26
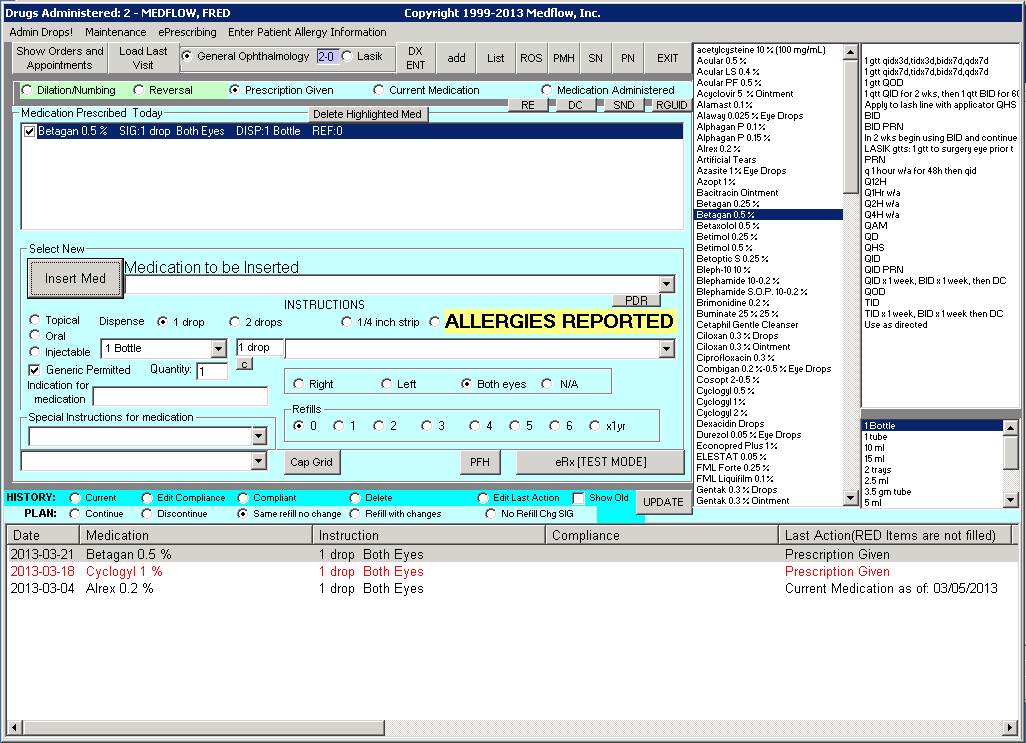
27 Electronic Prescribing More than 40% of all permissible prescriptions written by the EP are transmitted electronically using certified EHR technology You can be excluded from meeting this objective if you write fewer than 100 prescriptions during the reporting period More than 50% of prescriptions are compared to a drug formulary and transmitted electronically You can be excluded from meeting this objective if you write fewer than 100 prescriptions during the reporting period or Do not have a pharmacy within your organization and there are no pharmacies that accept electronic prescriptions within 10 miles of the EP's practice location at the start of his/her EHR reporting period
28 Electronic Prescribing Changes Stage 1: > 40% of permissible prescriptions transmitted electronically Stage 2: Increases % of prescriptions transmitted by erx to > 50% of permissible prescriptions Adds prescriptions are also queried for a drug formulary
29 E-Prescribing Change 2013 and Beyond Beginning Jan 1 st, 2013 new additional exclusion: Any EP who does not have a pharmacy within their organization and there are no pharmacies that accept electronic prescriptions within 10 miles of the EP's practice location at the start of his/her EHR reporting period can take an exclusion on Electronic Prescribing
30 E-Prescribing (erx) Clinical Significance? Improves medication safety Better management of medication costs Improved prescribing accuracy and efficiency Increase practice efficiency Reducing health care costs Reduction of adverse drug events
31
32 Patient Demographics More than 50% of all unique patients seen by the EP have demographics recorded Preferred language, Race, Ethnicity, Gender, Date of Birth No Exclusion More than 80% of all unique patients seen by the EP have demographics recorded. Preferred language, Race, Ethnicity, Gender, Date of Birth No Exclusion
33 Patient Demographics Changes Stage 1: > 50% of unique patients have demographic data stored as structured data Stage 2: Increases percentage to > 80% of unique patients have demographic data stored as structured data
34 Patient Demographics Details Preferred language Ask what is your preferred language and let patient select or write in Ethnicity (federal definition) Hispanic or Latino Not Hispanic or Latino Race (Federal definition, one or more that apply) American Indian or Alaska Native Asian Black or African American White Native Hawaiian or Other Pacific Islander For Race and Ethnicity refuse to specify may be recorded and is a valid response
35 Record demographics Clinical Significance? Many studies indicate that African Americans are 3x more likely to develop POAG, and have an increased risk of hypertensive retinopathy Latinos have an increased risk of diabetes Whites have an increased risk of AMD Patient with central distorted vision --- proper age, race, and gender for central serous?
36
37 Maintain an Up-to-Date Problem List More than 80% of all unique patients seen by the EP have at least one entry or an indication that no problems are known for the patient recorded as structured data There is no exclusion for this objective No longer a separate objective for Stage 2 It has been incorporated into the Stage 2 Summary of Care Document at Transitions of Care and Referrals
38 Maintain an up-to-date list of current and active diagnosis (problem list) Clinical Significance? This is an ongoing list of active problems or diagnosis Creating this list will allow you to immediately understand your patient's overall health The problem lists states the most important health problems facing a patient You will know they are diabetic and you need to do additional clinical testing for diabetic retinopathy, or that they have POAG and need additional clinical testing done We typically already record problems or diagnosis just be sure to list them in the proper fields in your EHR
39
40 Maintain Active Medication List More than 80% of all unique patients seen by the EP have at least one medication recorded or an indication that the patient is not currently prescribed any medication recorded There is no exclusion for this objective. No longer a separate objective for Stage 2 It has been incorporated into the Stage 2 Summary of Care Document at Transitions of Care and Referrals
41 Maintain active medication list Clinical Significance? We should be checking all patients medication list at each visit because many of the meds have ocular side effects If they tell you they are on a diabetic medication that will alert you to the need for additional testing for retinopathy or macular edema as well We now need to indicate a negative if no prescribed medications exist In other words, we have to make sure that the record shows no prescribed medications
42
43 Maintain Active Medication Allergy List More than 80% of all unique patients seen by the EP have at least one medication allergy recorded or an indication that the patient has no known medication allergies recorded. There is no exclusion for this objective No longer a separate objective for Stage 2 It has been incorporated into the Stage 2 Summary of Care Document at Transitions of Care and Referrals
44 Maintain active medication allergy list Clinical Significance? We should be checking all patients allergy status at each visit so we don t prescribe a medication that could cause an allergic or anaphylactic reaction We now need to indicate a negative if no medication allergies exist In other words, we have to make sure that the record shows no active medication allergies
45
46 Record and Chart Changes in Vital Signs For more than 50% of all unique patients age 2 and over seen by the EP, height, weight and blood pressure are recorded as structured data BMI should be calculated and displayed Plot and display growth and BMI charts for 2-20 years You can be excluded if: You don t see any patients 2 years or older or You believe all 3 of these vital signs are NOT relevant to your scope of practice For more than 80% of all unique patients seen by the EP, blood pressure (for patients age 3 and over only) and height and weight (for all ages) are recorded as structured data. BMI should be calculated and displayed, Plot and display growth and BMI charts for 0-20 years You may be excluded if you: See no patients 3 years or older Believe that all 3 vital signs of height/length, weight, and blood pressure have no relevance to your scope of practice You are excluded from recording blood pressure if you believe that height/length and weight are relevant to your scope of practice, but blood pressure is not You are excluded from recording height/length and weight if you believe that blood pressure is relevant to your scope of practice, but height/length and weight are not
47 Vital Signs Changes Stage 1: Vital signs must be recorded for more than 50% of all unique patients age 2 and over Plot and display growth and BMI charges for 2-20 years Stage 2: Increases percentage to > 80% of unique patients Increases age on blood pressure to age >3 Plot and display growth and BMI charts for 0-20 years Reduces age on height and weight to birth (all ages) New exclusion for height/weight only New exclusion for blood pressure only
48 Stage 1 Vital Signs Changes Optional 2013 / Required 2014 The measure amends the age limit for vital signs to: Blood pressure for patients ages 3 and over Height and weight for patients of all ages
49 Stage 1 Vital Signs Changes Optional 2013 / Required 2014 The measure amends the exclusions as well: If you see no patients 3 years or older you are excluded from recording blood pressure If you believe that all three vital signs of height, weight, and blood pressure have no relevance to your scope of practice you are excluded from recording all three of them If you believe that height and weight are relevant to your scope of practice, but blood pressure is not, you are excluded from recording blood pressure If you believe that blood pressure is relevant to your scope of practice, but height and weight are not, you are excluded from recording height and weight
50 Record and chart changes in vital signs Clinical Significance? Many clinical studies have shown an increased risk of AMD, glaucoma, and Cataracts in overweight patients BMI is calculated as weight (lbs) / height 2 (inches) x 703 BMI of is normal, > 25 is overweight, >30 is Obese Height/weight/BMI: Can add height and weight to patient questionnaire Suggest starting with patient attestation for height and weight but move to actually measuring it The BMI is a function of the software Blood pressure: We should be doing this on all patients Helps in the diagnosis of hypertensive retinopathy You will be surprised how many patients have significantly elevated BP and you may be the one to prevent them from having a stroke
51 Record and chart changes in vital signs Clinical Significance? Recent study found that after 6 years of age, the probability of obesity in adulthood exceeded 50% for obese children Recent study found that atherosclerosis starts in childhood and the presence of obesity is highly correlated Large prospective study found Obese men has 1.46 to 2.40 times the risk of death Obese women had 1.51 to 2.76 times the risk of death According to the World Health Organization 51% of cerebrovascular disease deaths are attributable to high systolic blood pressure, 45% of ischemic heart disease deaths are attributable to high systolic blood pressure, The leading cause of cardiovascular death worldwide is high blood pressure
52
53 Record Smoking Status for Patients 13 Years or Older More than 50% of all unique patients 13 years old or older seen by the EP have smoking status recorded as structured data You can be excluded from this objective if you do not see any patients who are age 13 years or older More than 80% of all unique patients 13 years old or older seen by the EP have smoking status recorded as structured data You can be excluded from this objective if you do not see any patients who are age 13 years or older
54 Smoking Status Changes Stage 1: > 50% of unique patients 13 years or older have smoking status recorded as structured data Stage 2: Increases % to > 80% of unique patients 13 years or older have smoking status recorded as structured data
55 Record smoking status for patients 13 years or older Clinical Significance? We know and should advise any patients who are smoking that they have an increased risk for AMD as well as glaucoma, and cataracts Consider adding questions to the patient registration form to get the information on status Have this information recorded during history taking This must be recorded in the EHR as structured data and it will be tracked by the EHR for compliance
56 Record smoking status for patients 13 years or older Clinical Significance? Tobacco is the single greatest cause of disease and premature death in America today and is responsible for: More than 435,000 deaths annually $96 billion annually in medical expenses $97 billion annually in lost productivity When compared with non-smokers, smoking is estimated to increase the risk of: Coronary heart disease by 2 to 4 times Stroke by 2 to 4 times Men developing lung cancer by 23 times Women developing lung cancer by 13 times Death from chronic obstructive lung diseases by 12 to 13 times
57
58 Clinical Decision Support Rule Implement one clinical decision support rule that will trigger alerts for providers when they have patients with certain diagnosis or conditions No exclusion Measure 1: Implement five clinical decision support interventions related to four or more clinical quality measures for the entire EHR reporting period Measure 2: The EP has enabled and implemented the functionality for drug-drug and drug-allergy interaction checks for the entire EHR reporting period For Measure 2, you can be excluded if you write fewer than 100 medication orders during the reporting period
59 Clinical Decision Support Changes Stage 1: One clinical decision support rule enabled related to your specialty Stage 2: 5 Rules are now required based on four clinical quality measures (to be covered next) plus drug-drug and drug-allergy interaction checks If there are not four clinical quality measures related to your scope of practice or patient population, the clinical decision support interventions must be related to high-priority health conditions
60 Clinical Decision Support Details Clinical Decision Support: Functionality that builds upon the foundation of an EHR to provide persons involved in care processes with general and person-specific information, intelligently filtered and organized, at appropriate times, to enhance health and health care
61 Implement clinical decision support Clinical Significance? These are rules designed to help us meet the standard of care in terms of testing and follow up care Examples: If a patient has an active medication of Plaquenil listed, has a macular visual field, color vision testing, and a SD OCT been ordered? When an IOP is above a specific level, a warning of possible glaucoma is triggered If a diagnosis of glaucoma is entered, is the patient scheduled or have they had a VF or a scanning laser within the last 6-12months
62
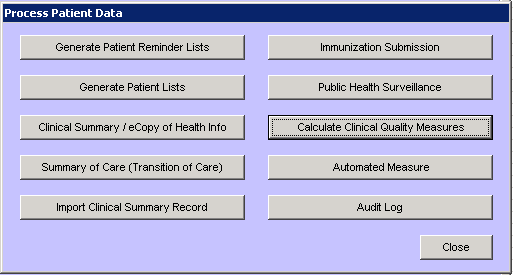
63 Report Clinical Quality Measures Beginning in 2013 no longer a separate objective Has been incorporated into the definition of a Meaningful EHR user You still must provide aggregate numerator, denominator, and exclusions through attestation or be part of the PQRS Electronic Reporting Pilot No longer a separate objective but providers must still submit CQM s to achieve meaningful use Starting in 2014, all CQMs will be submitted electronically to CMS
64 Clinical Quality Measures 2013 and Beyond Clinical quality measures, or CQMs, are tools that help us measure and track the quality of healthcare services provided by eligible professionals CQMs measure many aspects of patient care including: outcomes clinical processes, patient safety efficient use of healthcare resources, care coordination patient engagements, population and public health clinical guidelines
65 Clinical Quality Measures 2013 and Beyond Although clinical quality measure (CQM) reporting has been removed as a core objective for EPs, all providers are required to report on CQMs in order to demonstrate meaningful use Beginning in 2014, all providers regardless of their stage of meaningful use will report on CQMs in the same way
66 Report ambulatory clinical quality measures to CMS for 2013 Only Every EP must report on clinical quality measures to demonstrate Meaningful Use Your certified EHR will track and produce a report with your clinical quality measures data (numerators and denominators). You will utilize this report when you complete your attestation There are no thresholds or percentages that you must meet. You just need to report the data exactly as it is contained in your EHR report
67 Report ambulatory clinical quality measures to CMS for 2013 Only You must report on: 3 Core measures (If you don t collect data on one or more of the 3 core measures, you can use a measure from the alternate core list as a replacement) AND 3 measures that are relevant to Optometry from an additional Menu list of 38 items
68 Report ambulatory clinical quality measures to CMS for 2013 Only The 3 core clinical quality measures are: Core Clinical Quality Measure National Quality Forum (NQF) and / or PQRS Measure Number Hypertension: Blood Pressure Measurement Preventive Care and Screening Measure Pair: a. Tobacco Use Assessment b. Tobacco Cessation Intervention NQF 0013 NQF 0028 Adult Weight Screening and Follow-up NQF 0421 PQRS 128
69 Report ambulatory clinical quality measures to CMS for 2013 Only The 3 alternate core clinical quality measures are: Alternate Core Clinical Quality Measure National Quality Forum (NQF) and / or PQRS Measure Number Weight Assessment and Counseling for Children and Adolescents Preventive Care and Screening: Influenza Immunization for Patients 50 Years Old NQF 0024 NQF 0041 PQRS 110 Childhood Immunization Status NQF 00038
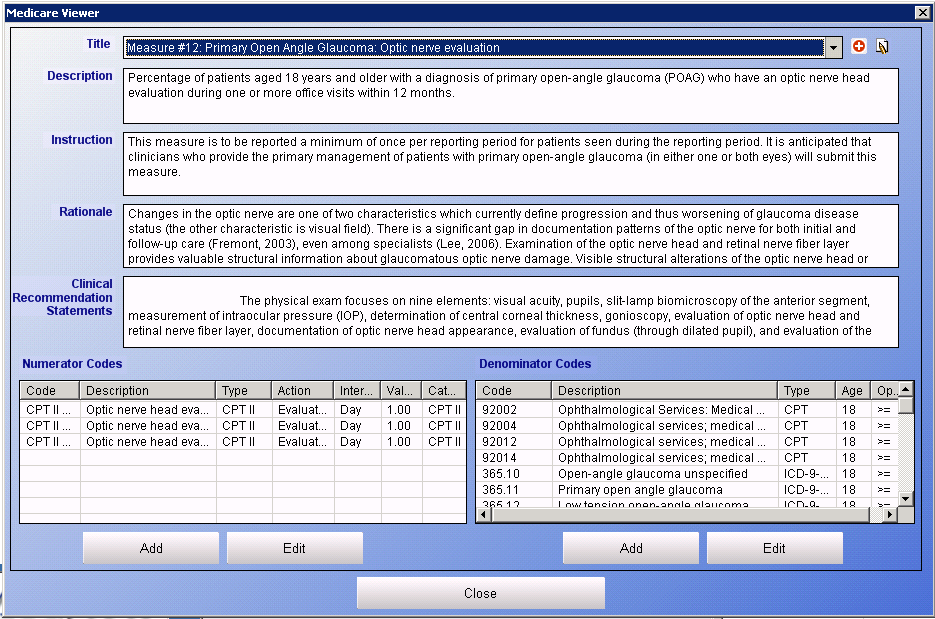
70 Report ambulatory clinical quality measures to CMS for 2013 Only Additional Clinical Quality Measures You must pick 3 from the list of 38. Optometry relevant shown below Additional Clinical Quality Measures Primary Open Angle Glaucoma: Optic Nerve Evaluation Diabetic Retinopathy: Documentation of presence or absence of macular edema and level of severity of retinopathy Diabetic Retinopathy: Communication with the physician managing ongoing diabetes care National Quality Forum (NQF) and / or PQRS Measure Number PQRS 12 PQRS 18 PQRS 19 Diabetes: Eye exam PQRS 117
71 Report ambulatory clinical quality measures to CMS for 2013 Only Clinical Significance? Again these remind us of the clinical importance of blood pressure measurement, tobacco use assessment and cessation advice, as well as weight and BMI calculations This information is important because it is being utilized as a measure of quality of clinical care for your patients Your certified EHR does the work! It will track and calculate the measures as you enter clinical data You must report these numbers when you attest If you have a zero in the denominator on one or more of the core clinical quality measures replace it with one (or more) measures from the alternate list Choose 3 measures from the additional list that are relevant to Optometry Remember there are no minimum values that you must obtain you just report the numbers from your certified EHR report
72 Report ambulatory clinical quality measures to CMS for 2013 Only Need help understanding CQMs for 2013?? CQM webpage easures.asp#topofpage User guide o_cqms.pdf You tube video
73 Report ambulatory clinical quality measures to CMS for 2014 Beginning in 2014, all providers regardless of their stage of meaningful use will report on CQMs in the same way For 2014, CMS is not requiring the submission of a core set of CQMs Instead CMS has identified two recommended core sets of CQMs, one for adults and one for children CMS encourages eligible professionals to report from the recommended core set to the extent those CQMs are applicable to your scope of practice and patient population
74 Report ambulatory clinical quality measures to CMS for 2014 CMS selected the recommended core set of CQMs for EPs based on analysis of several factors: Conditions that contribute to the morbidity and mortality of the most Medicare and Medicaid beneficiaries Conditions that represent national public health priorities Conditions that are common to health disparities Conditions that disproportionately drive healthcare costs and could improve with better quality measurement Measures that would enable CMS, States, and the provider community to measure quality of care in new dimensions, with a stronger focus on parsimonious measurement Measures that include patient and/or caregiver engagement
75 Report ambulatory clinical quality measures to CMS for 2014 EPs must report on 9 out of 64 total CQMs Providers must select CQMs from at least 3 of the 6 key health care policy domains (listed below) recommended by the Department of Health and Human Services National Quality Strategy 1. Patient and Family Engagement 2. Patient Safety 3. Care Coordination 4. Population and Public Health 5. Efficient Use of Healthcare Resources 6. Clinical Processes/Effectiveness
76 Report ambulatory clinical quality measures to CMS for 2014 Adult Recommended Core Measures Controlling High Blood Pressure Use of High-Risk Medications in the Elderly Preventive Care and Screening: Tobacco Use: Screening and Cessation Intervention Use of Imaging Studies for Low Back Pain Preventive Care and Screening: Screening for Clinical Depression and Follow-Up Plan Documentation of Current Medications in the Medical Record Preventive Care and Screening: Body Mass Index (BMI) Screening and Follow-Up Closing the referral loop: receipt of specialist report Functional status assessment for complex chronic conditions
77 Report ambulatory clinical quality measures to CMS for 2014 Pediatric Recommended Core Measures Appropriate Testing for Children with Pharyngitis Weight Assessment and Counseling for Nutrition and Physical Activity for Children and Adolescents Chlamydia Screening for Women Use of Appropriate Medications for Asthma Childhood Immunization Status Appropriate Treatment for Children with Upper Respiratory Infection (URI) ADHD: Follow-Up Care for Children Prescribed Attention- Deficit/Hyperactivity Disorder (ADHD) Medication Preventive Care and Screening: Screening for Clinical Depression and Follow-Up Plan Children who have dental decay or cavities
78 Report ambulatory clinical quality measures to CMS for 2014 Beginning in 2014, all Medicare-eligible providers beyond their first year of demonstrating meaningful use must electronically report their CQM data to CMS EPs can electronically report with the following methods: Physician Quality Reporting System (PQRS) Electronic submission of samples of patient-level data. EPs can also report as group using the PQRS GPRO tool. EPs who electronically report using this PQRS option will meet both their EHR Incentive Program and PQRS reporting requirements CMS-designated transmission method Electronic submission of aggregate-level data
79 Report ambulatory clinical quality measures to CMS for 2014 Need help understanding CQMs for 2014?? CQM webpage Guidance/Legislation/EHRIncentivePrograms/20 14_ClinicalQualityMeasures.html
80
81
82
83 Patient Electronic Copy and Access More than 50% of all patients who request an electronic copy of their health information are provided the electronic copy within 3 business days. You may be excluded if none of your patients requests an electronic copy of their health information Measure 1: More than 50% of all unique patients are provided timely (within 4 business days after the info is available to the EP) online access to their health information Measure 2: More than 5% of all unique patients view, download, or transmit to a 3rd party their health information You can be excluded if you neither order nor create any of the info listed for inclusion (see next slide) You can be excluded if you conduct 50% or more of encounters in a county that does not have 50% or more housing units with 3Mbps broadband availability
84 Patient Electronic Copy and Electronic Access Changes Stage 1: Only required for patients who request and electronic copy Stage 2: Must be done for > 50% of unique patients Now being held accountable for the patients to utilize the information: More than 5% of all unique patients (or authorized representative) view, download, or transmit to a 3rd party their health information You must provide: patient name, provider's name and office contact information, current and past problem list, procedures. laboratory test results, current medication list and medication history, current medication allergy list and medication allergy history, vital signs, smoking status, demographic information care plan field(s), including goals and instructions, and any known care team members including the primary care provider (PCP) of record You may be excluded if you don t create any of the above listed information (except patient name, provider name and office info)
85 Stage 1 Electronic Copy and Electronic Access to Health Information Changes Required 2014 Original Stage 1 core objective replaced Provide patients with electronic copy of health info upon request Original Stage 1 menu objective replaced Provide patients with timely electronic access to their health information within 4 business days 2014 New stage 1 objective: More than 50% of unique patients are provided timely (within 4 business days) online access to their health information
86 Patient Electronic Copy and Electronic Access Clinical Significance for Stage 1? This reinforces the importance of involving your patients in their own healthcare For stage 1 when a patient makes a request, EPs must provide the patient with all of the health information they have available electronically within 3 business days At a minimum includes: diagnostic test results, problem list, medication lists, medication allergies Certified software will generate this report The media could be any electronic form such as patient portal, PHR, CD, USB fob, etc. EPs are expected to make reasonable accommodations for patient preference Per HIPAA rules, you may charge a fee for this service
87 Patient Electronic Copy and Electronic Access Clinical Significance for Stage 2? Patient access will allow patients to understand what clinical testing was completed during an encounter as well as the results of those tests Online electronic access through either a patient portal or personal health record (PHR) will satisfy this objective The minimal information to be included is: Lab test results, problem list, medication list, and medication allergy list You may withhold information from the electronic copy in accordance with HIPAA

88
89
90 Provide Clinical Summaries for Patients for Each Office Visit Clinical summaries must be provided to patients within 3 business days of visit for more than 50% of all office visits You may be excluded if you have no office visits Clinical summaries must be provided to patients or authorized representatives within 1 business days for more than 50% of all office visits You may be excluded if you have no office visits
91 Provide Clinical Summaries Changes Stage 1: You have 3 business days to provide summary Stage 2: You have 1 business day to provide summary
92 Provide clinical summaries for patients for each office visit Clinical Significance? At completion of the exam, the EHR would take the key clinical data elements from the electronic record and create a summary of the findings which can be given to the patient to help them better understand their overall health The clinical summary can be provided through a personal health record, patient portal on the web site, secure , electronic media such as CD or USB fob, or printed copy. If the EP chooses an electronic media, they would be required to provide the patient a paper copy upon request
93 Provide clinical summaries for patients for each office visit Clinical Significance? Enhances the ability of patients to remember and, if necessary, convey to family members, the content of interactions with their care team Supports greater patient engagement in making good choices about healthy behaviors Summaries should include items such as: updated medication list, vital signs, reason for visit, problem list, medications / immunizations, lab tests ordered / results, and follow up appointments An EP may choose to withhold particular information if they believe substantial harm may arise from disclosure
94
95
96 Capability to Exchange Key Clinical Information This objective is eliminated from Stage 1 in 2013 and is no longer an objective This objective is not required for Stage 2
97 Protect Electronic Health Information Conduct or review a security risk analysis and implement security updates as needed and correct identified security deficiencies as part of the process No exclusion Conduct or review a security risk analysis including addressing the encryption/security of data at rest and implement security updates as needed and correct identified security deficiencies as part of the process No exclusion
98 Protect electronic health information A major goal of the Security Rule is to protect the privacy of individuals health information while allowing covered entities to adopt new technologies to improve the quality and efficiency of patient care This is similar to the current HIPAA security rules You must conduct or review a security risk analysis and implement updates as necessary Should be done once prior to end of reporting period Your software vendor should be able to provide you with tools to complete the risk analysis
99 Protect electronic health information HIPAA protects the privacy of individually identifiable health information, called protected health information (PHI) Security Rule protects a subset of information covered by the Privacy Rule, which is all individually identifiable health information a covered entity creates, receives, maintains or transmits in electronic form. The Security Rule calls this information electronic protected health information (e-phi)
100 Protect electronic health information The Security Rule requires covered entities to maintain reasonable and appropriate administrative, technical, and physical safeguards for protecting e-phi Specifically, covered entities must: Ensure the confidentiality, integrity, and availability of all e- PHI they create, receive, maintain or transmit; Identify and protect against reasonably anticipated threats to the security or integrity of the information; Protect against reasonably anticipated, impermissible uses or disclosures; and Ensure compliance by their workforce
101 Protect electronic health information The Security Rule require covered entities to perform risk analysis as part of their security management processes A risk analysis process includes, but is not limited to, the following activities: Evaluate the likelihood and impact of potential risks to e- PHI; Implement appropriate security measures to address the risks identified in the risk analysis; Document the chosen security measures and, where required, the rationale for adopting those measures; 10 and Maintain continuous, reasonable, and appropriate security protections
102 Protect electronic health information Administrative Safeguards Are Required Security Management Process: Must identify and analyze potential risks to e-phi, and implement security measures that reduce risks and vulnerabilities to a reasonable and appropriate level Security Personnel: Must designate a security official who is responsible for developing and implementing its security policies and procedures Information Access Management: Implement policies and procedures for authorizing access to e-phi only when such access is appropriate based on the user or recipient's role (role-based access) Workforce Training and Management: Must provide for appropriate authorization and supervision of workforce members who work with e- PHI. You must train all workforce members regarding security policies and procedures, and you must have and apply appropriate sanctions against workforce members who violate policies and procedures Evaluation: Must perform a periodic assessment of how well your security policies and procedures meet the requirements of the Security Rule
103 Protect electronic health information Physical Safeguards Are Required Facility Access and Control: Must limit physical access to facilities while ensuring that authorized access is allowed Workstation and Device Security: Must implement policies and procedures to specify proper use of and access to workstations and electronic media. Must have in place policies and procedures regarding the transfer, removal, disposal, and re-use of electronic media, to ensure appropriate protection of electronic protected health information (e-phi)
104 Protect electronic health information Technical Safeguards Are Required Access Control: Must implement technical policies and procedures that allow only authorized persons to access electronic protected health information (e-phi) Audit Controls: Must implement hardware, software, and/or procedural mechanisms to record and examine access and other activity in information systems that contain or use e-phi Integrity Controls: Must implement policies and procedures to ensure that e-phi is not improperly altered or destroyed. Electronic measures must be put in place to confirm that e-phi has not been improperly altered or destroyed Transmission Security: Must implement technical security measures that guard against unauthorized access to e-phi that is being transmitted over an electronic network
105 Protect electronic health information Required and Addressable Implementation Specifications The "required" implementation specifications must be implemented. The "addressable" designation does not mean that an implementation specification is optional it permits covered entities to determine whether the addressable implementation specification is reasonable and appropriate for that covered entity If it is not, the Security Rule allows the covered entity to adopt an alternative measure that achieves the purpose of the standard, if the alternative measure is reasonable and appropriate
106 Protect electronic health information Organizational Requirements Covered Entity Responsibilities: If a covered entity knows of an activity or practice of a business associate that constitutes a material breach or violation of the business associate s obligation, the covered entity must take reasonable steps to cure the breach or end the violation. Violations include the failure to implement safeguards that reasonably and appropriately protect e-phi
107 Protect electronic health information Policies and Procedures and Documentation Requirements Must adopt reasonable and appropriate policies and procedures to comply with the provisions of the Security Rule. Must maintain, until six years after the later of the date of their creation or last effective date, written security policies and procedures and written records of required actions, activities or assessments Updates: Must periodically review and update your documentation in response to environmental or organizational changes that affect the security of electronic protected health information (e-phi)
108 Protect electronic health information Enforcement and Penalties for Noncompliance Compliance: The Security Rule establishes a set of national standards for confidentiality, integrity and availability of e-phi. The Department of Health and Human Services (HHS), Office for Civil Rights (OCR) is responsible for administering and enforcing these standards, in concert with its enforcement of the Privacy Rule, and may conduct complaint investigations and compliance reviews
109 End of Stage 1 Core Objectives Continued Stage 2 Core Objectives Beginning of Stage 1 Menu Objectives
110 Stage 1 Menu Objectives 1. Drug formulary checks 2. Incorporate clinical lab-test results 3. Generate lists of patients by specific conditions 4. Send reminders to patients for preventive / follow-up care 5. Electronic access to health information for patients 6. Patient specific education resources 7. Medication reconciliation 8. Summary of care record for transitions of care 9. Submit electronic data to immunization registries 10. Submit electronic syndromic surveillance data to public health agencies
111 Drug Formulary Checks EP has enabled functionality for a drug formulary checks and has access to at least one internal or external formulary for the entire reporting period You can be excluded from meeting this objective if you write fewer than 100 prescriptions during the reporting period No longer a separate objective for Stage 2 It has been incorporated into the Stage 2 e-prescribing measure
112 Drug Formulary Changes Stage 1: Menu Item Stage 2: Removed as an objective Incorporated into the e-prescribing measure for Stage 2
113 Drug Formulary Checks Clinical Significance? When you prescribe a medication you will now need to consider if that medication is the best choice both for the condition and for the patient s medication formulary For example would it be best to prescribe Vigamox if it is nonformulary or would it make more sense to utilize Zymar instead if it is on the formulary? For each clinical condition there may be multiple medications that work This is a function of your certified EHR software e- prescribing system Be sure the functionality is turned on and active for your entire reporting period
114
115 Incorporate Clinical Lab-Test Results More than 40% of all clinical lab test results ordered by the EP during the reporting period (whose results are in a +/- or numerical format) are incorporated in the EHR as structured data You can be excluded from this objective if you did not order any lab tests during the reporting period or if none of the lab tests ordered have results in a positive / negative or numerical format More than 55% of all clinical lab test results ordered by the EP during the reporting period (whose results are in a +/- or numerical format) are incorporated in the EHR as structured data You can be excluded from this objective if you did not order any lab tests during the reporting period or if none of the lab tests ordered have results in a positive / negative or numerical format
116 Clinical Lab-Test Results Changes Stage 1: Menu objective Requires > 40% of discrete lab test results to be stored as structured data Stage 2: Core objective Increased the percentage to > 55% of discrete lab test results to be stored as structured data
117 Incorporate clinical lab-test results Clinical Significance? This allows us to order lab tests directly from our EHR to a lab It will allow quicker lab orders and the results will be returned electronically Easier for us to order lab tests for conditions like recurring uveitis, diabetics, Graves disease This applies to lab results ordered by you during the reporting period whose results are either positive/negative or numerical format Typically blood, urine, path reports Many of us could take the exemption for not ordering any lab tests whose results are either in a positive/negative or numeric format during the EHR reporting period
118
119 Generate Lists of Patients by Specific Conditions Generate at least one report listing patients of the EP with a specific condition No exclusion Generate at least one report listing patients of the EP with a specific condition No exclusion
120 Patient Lists Changes Stage 1: Menu Objective Stage 2: Core Objective No other changes
121 Generate lists of patients by specific conditions Clinical Significance? There may be times when you need to know every patient in your office that has a certain condition to offer them a new best treatment that becomes available New glaucoma medication or treatment option New contact lens material or type of lens All certified EHRs can generate a list of patients based on certain conditions The objective does not dictate the reports which must be generated An EP can determine which reports are most useful to their care efforts
122
123 Patient Reminders (Stage 1) Preventive Care (Stage 2) More than 20% of all patients 65 years or older or 5 years or younger were sent the appropriate reminder during the reporting period You can be excluded from this objective if you have no patients 65 years or older or 5 years old or younger More than 10% of all unique patients who have had 2 or more office visits within the 24 months before the beginning of the reporting period were sent a reminder, per pt. preference when available You can be excluded if you have no office visits in the 24 months before the EHR reporting period
124 Patient Reminders / Preventive Care Changes Stage 1: Menu objective Required 20% of all patients 65 years or older or 5 years or younger to be sent reminder Stage 2: Core Measure Lowered the percentage to 10% but now includes all unique patients who have had 2 or more office visits within the 24 months before the beginning of the reporting period
125 Send Reminders to Patients for Preventive / Follow Up Care Clinical Significance? This allows us to properly follow up with our patients who need further care Do some of your patients with POAG need to follow up for an OCT or VF Do a group of your diabetic patients need to return for a DFE This is fairly easy to do in all certified EHR software There is no specific requirements for the reminders You have the discretion to determine the frequency, means of transmission and form of the reminder limited only by the requirements of HIPAA
126
127
128 Electronic Access to Health Information for Patients At least 10% of all unique patients seen by the EP are provided timely (within 4 business days of being updated in the EHR) electronic access to their health information. You can be excluded from this objective if you do not order or create any of the following: Lab results, Problem list, Medication list, Medication allergy list This objective is no longer a measure for Stage 2
129 Stage 1 Electronic Access to Health Information for Patients Changes Required 2014 This objective will be eliminated from Stage 1 in 2014 New 2014 Measure: More than 50% of all unique patients seen by the EP during the EHR reporting period are provided timely (within 4 business days after the information is available to the EP) online access to their health information subject to the EP's discretion to withhold certain information
130
131
132 Patient Specific Education Resources More than 10% of all unique patients seen by the EP are provided patient specific education resources No exclusion Patient-specific education resources identified by the EHR are provided to patients for more than 10% of all unique patients with office visits You can be excluded if you have no office visits during the reporting period
133 Patient Specific Educational Resources Changes Stage 1: Menu Objective Percentage required is 10% of all unique patients seen are given educational resources Stage 2: Core Objective Percentage remains at 10% but now is all unique patients with office visits Exclusion now available for EPs with no office visits
134 Patient specific education resources Clinical Significance? It is our job as a doctor to properly educate our patients on all of their clinical findings and diagnosis as well as risks and benefits of each treatment option Certified EHRs have the ability to identify patient specific educational resources based on the problem list, medication list, or lab test results The EHR technology should be used to suggest the patient educational resources The resources do not have to be stored within or generated by the EHR. AMD or ERM = Amsler Grid AMD = AREDS information as well
135

136
Meaningful Use Stage 1 and 2 Your Survival Guide!
 Where to go for Help, Handouts, and Future Updates Meaningful Use Stage 1 and 2 Your Survival Guide! Dr. Henry and Dr. Gross are affiliated with www.ehrguru.net and have lectured for numerous companies
Where to go for Help, Handouts, and Future Updates Meaningful Use Stage 1 and 2 Your Survival Guide! Dr. Henry and Dr. Gross are affiliated with www.ehrguru.net and have lectured for numerous companies
MEANINGFUL USE STAGE 2 2015 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 MEANINGFUL USE STAGE 2 2015 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives EPs must meet 3 of the 6 menu measures.
MEANINGFUL USE STAGE 2 2015 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives EPs must meet 3 of the 6 menu measures.
Ophthalmology Meaningful Use Attestation Guide Stage 1 2013 Edition
 Ophthalmology Meaningful Use Attestation Guide Stage 1 2013 Edition Ophthalmologists can register for the Medicare electronic health record (EHR) incentive program on the CMS website: https://ehrincentives.cms.gov
Ophthalmology Meaningful Use Attestation Guide Stage 1 2013 Edition Ophthalmologists can register for the Medicare electronic health record (EHR) incentive program on the CMS website: https://ehrincentives.cms.gov
DEMONSTRATING MEANINGFUL USE STAGE 1 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EHR TECHNOLOGY IN 2014
 DEMONSTRATING MEANINGFUL USE STAGE 1 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EHR TECHNOLOGY IN 2014 The chart below lists the measures (and specialty exclusions) that eligible providers must
DEMONSTRATING MEANINGFUL USE STAGE 1 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EHR TECHNOLOGY IN 2014 The chart below lists the measures (and specialty exclusions) that eligible providers must
MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY On August 24, the Centers for Medicare & Medicaid Services (CMS) posted the much anticipated final rule for Stage
MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY On August 24, the Centers for Medicare & Medicaid Services (CMS) posted the much anticipated final rule for Stage
DEMONSTRATING MEANINGFUL USE STAGE 1 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EHR TECHNOLOGY IN 2015
 DEMONSTRATING MEANINGFUL USE STAGE 1 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EHR TECHNOLOGY IN 2015 The chart below lists the measures (and specialty exclusions) that eligible providers must
DEMONSTRATING MEANINGFUL USE STAGE 1 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EHR TECHNOLOGY IN 2015 The chart below lists the measures (and specialty exclusions) that eligible providers must
EHR Incentive Program Focus on Stage One Meaningful Use. Kim Davis-Allen, Outreach Coordinator Kim.davis@ahca.myflorida.com October 16, 2014
 EHR Incentive Program Focus on Stage One Meaningful Use Kim Davis-Allen, Outreach Coordinator Kim.davis@ahca.myflorida.com October 16, 2014 Checklist Participation Explanation Program Updates Stage One
EHR Incentive Program Focus on Stage One Meaningful Use Kim Davis-Allen, Outreach Coordinator Kim.davis@ahca.myflorida.com October 16, 2014 Checklist Participation Explanation Program Updates Stage One
Stage 1 vs. Stage 2 Comparison for Eligible Professionals
 Stage 1 vs. Comparison for Eligible Professionals CORE OBJECTIVES (17 Total) Stage 1 Objective Stage 1 Measure Objective Measure Use CPOE for Medication orders directly entered by any licensed healthcare
Stage 1 vs. Comparison for Eligible Professionals CORE OBJECTIVES (17 Total) Stage 1 Objective Stage 1 Measure Objective Measure Use CPOE for Medication orders directly entered by any licensed healthcare
Meaningful Use 2014: Stage 2 MU Overview. Scott A. Jens, OD, FAAO October 16, 2013
 Meaningful Use 2014: Stage 2 MU Overview Scott A. Jens, OD, FAAO October 16, 2013 Overview General Overview of Stage 2 MU in 2014 Core Objectives for Stage 2 Menu Objectives for Stage 2 Complete summary
Meaningful Use 2014: Stage 2 MU Overview Scott A. Jens, OD, FAAO October 16, 2013 Overview General Overview of Stage 2 MU in 2014 Core Objectives for Stage 2 Menu Objectives for Stage 2 Complete summary
Stage 1 vs. Stage 2 Comparison Table for Eligible Professionals Last Updated: August, 2012
 Stage 1 vs. Stage 2 Comparison Table for Eligible Professionals Last Updated: August, 2012 CORE OBJECTIVES (17 total) Stage 1 Objective Stage 1 Measure Stage 2 Objective Stage 2 Measure Use CPOE for medication
Stage 1 vs. Stage 2 Comparison Table for Eligible Professionals Last Updated: August, 2012 CORE OBJECTIVES (17 total) Stage 1 Objective Stage 1 Measure Stage 2 Objective Stage 2 Measure Use CPOE for medication
STAGES 1 AND 2 REQUIREMENTS FOR MEETING MEANINGFUL USE OF EHRs 1
 STAGES 1 AND 2 REQUIREMENTS FOR MEETING MEANINGFUL USE OF EHRs 1 Requirement CPOE Use CPOE for medication orders directly entered by any licensed health care professional who can enter orders into the
STAGES 1 AND 2 REQUIREMENTS FOR MEETING MEANINGFUL USE OF EHRs 1 Requirement CPOE Use CPOE for medication orders directly entered by any licensed health care professional who can enter orders into the
Demonstrating Meaningful Use Stage 1 Requirements for Eligible Providers Using Certified EMR Technology
 Demonstrating Meaningful Use Stage 1 Requirements for Eligible Providers Using Certified EMR Technology The chart below lists the measures (and specialty exclusions) that eligible providers must demonstrate
Demonstrating Meaningful Use Stage 1 Requirements for Eligible Providers Using Certified EMR Technology The chart below lists the measures (and specialty exclusions) that eligible providers must demonstrate
Presented by. Terri Gonzalez Director of Practice Improvement North Carolina Medical Society
 Presented by Terri Gonzalez Director of Practice Improvement North Carolina Medical Society Meaningful Use is using certified EHR technology to: Improve quality, safety, efficiency, and reduce errors Engage
Presented by Terri Gonzalez Director of Practice Improvement North Carolina Medical Society Meaningful Use is using certified EHR technology to: Improve quality, safety, efficiency, and reduce errors Engage
Meaningful Use Objectives
 Meaningful Use Objectives The purpose of the electronic health records (EHR) incentive program is not so much the adoption of health information technology (HIT), but rather how HIT can further the goals
Meaningful Use Objectives The purpose of the electronic health records (EHR) incentive program is not so much the adoption of health information technology (HIT), but rather how HIT can further the goals
Meaningful Use Stage 2 Implementation Guide
 Meaningful Use Stage 2 Implementation Guide Copyright 2014 Kareo, Inc. All rights reserved. Updated October 2014 Table of Contents Get Ready... 1 Task List: Meaningful Use Stage 2... 2 Basic Training...
Meaningful Use Stage 2 Implementation Guide Copyright 2014 Kareo, Inc. All rights reserved. Updated October 2014 Table of Contents Get Ready... 1 Task List: Meaningful Use Stage 2... 2 Basic Training...
Medicaid EHR Incentive Program. Focus on Stage 2. Kim Davis-Allen, Outreach Coordinator Kim.davis@ahca.myflorida.com
 Medicaid EHR Incentive Program Focus on Stage 2 Kim Davis-Allen, Outreach Coordinator Kim.davis@ahca.myflorida.com Understanding Participation Program Year Program Year January 1 st - December 31st. Year
Medicaid EHR Incentive Program Focus on Stage 2 Kim Davis-Allen, Outreach Coordinator Kim.davis@ahca.myflorida.com Understanding Participation Program Year Program Year January 1 st - December 31st. Year
STAGE 2 of the EHR Incentive Programs
 EHR Incentive Programs A program administered by the Centers for Medicare & Medicaid Services (CMS) Eligible Professional s Guide to STAGE 2 of the EHR Incentive Programs September 2013 TABLE OF CONTENTS...
EHR Incentive Programs A program administered by the Centers for Medicare & Medicaid Services (CMS) Eligible Professional s Guide to STAGE 2 of the EHR Incentive Programs September 2013 TABLE OF CONTENTS...
Medicaid EHR Incentive Program Dentists as Eligible Professionals. Kim Davis-Allen, Outreach Coordinator Kim.davis@ahca.myflorida.
 Medicaid EHR Incentive Program Dentists as Eligible Professionals Kim Davis-Allen, Outreach Coordinator Kim.davis@ahca.myflorida.com Considerations Must begin participation by Program Year 2016 Not required
Medicaid EHR Incentive Program Dentists as Eligible Professionals Kim Davis-Allen, Outreach Coordinator Kim.davis@ahca.myflorida.com Considerations Must begin participation by Program Year 2016 Not required
STAGE 2 MEANINGFUL USE CORE AND MENU MEASURES FOR ELIGIBLE PROFESSIONALS
 STAGE 2 MEANINGFUL USE CORE AND MENU MEASURES FOR ELIGIBLE PROFESSIONALS CORE MEASURES must meet all CPOE for Medication, Laboratory and Radiology Orders Objective: Use computerized provider order entry
STAGE 2 MEANINGFUL USE CORE AND MENU MEASURES FOR ELIGIBLE PROFESSIONALS CORE MEASURES must meet all CPOE for Medication, Laboratory and Radiology Orders Objective: Use computerized provider order entry
Meaningful Use - The Basics
 Meaningful Use - The Basics Presented by PaperFree Florida 1 Topics Meaningful Use Stage 1 Meaningful Use Barriers: Observations from the field Help and Questions 2 What is Meaningful Use Meaningful Use
Meaningful Use - The Basics Presented by PaperFree Florida 1 Topics Meaningful Use Stage 1 Meaningful Use Barriers: Observations from the field Help and Questions 2 What is Meaningful Use Meaningful Use
Stage 1 vs. Stage 2 Comparison Table for Eligible Hospitals and CAHs Last Updated: August, 2012
 CORE OBJECTIVES (16 total) Stage 1 vs. Stage 2 Comparison Table for Eligible Hospitals and CAHs Last Updated: August, 2012 Stage 1 Objective Use CPOE for medication orders directly entered by any licensed
CORE OBJECTIVES (16 total) Stage 1 vs. Stage 2 Comparison Table for Eligible Hospitals and CAHs Last Updated: August, 2012 Stage 1 Objective Use CPOE for medication orders directly entered by any licensed
EHR Incentive Program Stage 2 Objectives Summary CORE OBJECTIVES (You must meet all objectives unless exclusion applies.)
") EHR Incentive Program Stage 2 Objectives Summary CORE OBJECTIVES (You must meet all objectives unless exclusion applies.) TARGETING CANCER CARE Objective Objective Description Measure/Attestation Requirement
EHR Incentive Program Stage 2 Objectives Summary CORE OBJECTIVES (You must meet all objectives unless exclusion applies.) TARGETING CANCER CARE Objective Objective Description Measure/Attestation Requirement
Stage 1 Meaningful Use for Specialists. NYC REACH Primary Care Information Project NYC Department of Health & Mental Hygiene
 Stage 1 Meaningful Use for Specialists NYC REACH Primary Care Information Project NYC Department of Health & Mental Hygiene 1 Today s Agenda Meaningful Use Overview Meaningful Use Measures Resources Primary
Stage 1 Meaningful Use for Specialists NYC REACH Primary Care Information Project NYC Department of Health & Mental Hygiene 1 Today s Agenda Meaningful Use Overview Meaningful Use Measures Resources Primary
6/26/2013. Continuing Medical Education Disclaimer
 Meaningful Use Stage 2: Understanding the Requirements and Changes June 26, 2013 12:30 1:30 p.m., EDT Marnivia Spencer, CCME EHR Consultant 2013 The Carolinas Center for Medical Excellence All Rights Reserved
Meaningful Use Stage 2: Understanding the Requirements and Changes June 26, 2013 12:30 1:30 p.m., EDT Marnivia Spencer, CCME EHR Consultant 2013 The Carolinas Center for Medical Excellence All Rights Reserved
Meaningful Use Criteria for Eligible Hospitals and Eligible Professionals (EPs)
") Meaningful Use Criteria for Eligible and Eligible Professionals (EPs) Under the Electronic Health Record (EHR) meaningful use final rules established by the Centers for Medicare and Medicaid Services (CMS),
Meaningful Use Criteria for Eligible and Eligible Professionals (EPs) Under the Electronic Health Record (EHR) meaningful use final rules established by the Centers for Medicare and Medicaid Services (CMS),
Agenda. What is Meaningful Use? Stage 2 - Meaningful Use Core Set. Stage 2 - Menu Set. Clinical Quality Measures (CQM) Clinical Considerations
 Clinical Considerations") AQAF Health Information Technology Forum Meaningful Use Stage 2 Clinical Considerations Marla Clinkscales & Mike Bice Alabama Regional Extension Center (ALREC) August 13, 2013 0 Agenda What is Meaningful
AQAF Health Information Technology Forum Meaningful Use Stage 2 Clinical Considerations Marla Clinkscales & Mike Bice Alabama Regional Extension Center (ALREC) August 13, 2013 0 Agenda What is Meaningful
Core Set of Objectives and Measures Must Meet All 15 Measures Stage 1 Objectives Stage 1 Measures Reporting Method
 Core Set of Objectives and Measures Must Meet All 15 Measures Stage 1 Objectives Stage 1 Measures Reporting Method Use Computerized Provider Order Entry (CPOE) for medication orders directly entered by
Core Set of Objectives and Measures Must Meet All 15 Measures Stage 1 Objectives Stage 1 Measures Reporting Method Use Computerized Provider Order Entry (CPOE) for medication orders directly entered by
Meaningful Use. Medicare and Medicaid EHR Incentive Programs
 Meaningful Use Medicare and Medicaid Table of Contents What is Meaningful Use?... 1 Table 1: Patient Benefits... 2 What is an EP?... 4 How are Registration and Attestation Being Handled?... 5 What are
Meaningful Use Medicare and Medicaid Table of Contents What is Meaningful Use?... 1 Table 1: Patient Benefits... 2 What is an EP?... 4 How are Registration and Attestation Being Handled?... 5 What are
Meaningful Use Updates Stage 2 and 3. Julia Moore, Business Analyst SMC Partners, LLC July 8, 2015
 Meaningful Use Updates Stage 2 and 3 Julia Moore, Business Analyst SMC Partners, LLC July 8, 2015 Stage 2 Requirements 2015 EPs beyond 1st year of MU must report on a full year of data EPs in 1 st year
Meaningful Use Updates Stage 2 and 3 Julia Moore, Business Analyst SMC Partners, LLC July 8, 2015 Stage 2 Requirements 2015 EPs beyond 1st year of MU must report on a full year of data EPs in 1 st year
Ophthalmology Meaningful Use Attestation Guide Stage 2 2014 Edition
 Ophthalmology Meaningful Use Attestation Guide Stage 2 2014 Edition Physicians who first participated in meaningful use in 2011 or 2012 must move on to Stage 2 in 2014. For 2014 only, physicians will attest
Ophthalmology Meaningful Use Attestation Guide Stage 2 2014 Edition Physicians who first participated in meaningful use in 2011 or 2012 must move on to Stage 2 in 2014. For 2014 only, physicians will attest
Meaningful Use 2014 Changes
 Meaningful Use 2014 Changes Lisa Sagwitz HIT Workflow & Implementation Coordinator September 4, 2014 1 PA Reach Who are we? Designated by ONC as the PA East and PA West Regional Extension Center We have
Meaningful Use 2014 Changes Lisa Sagwitz HIT Workflow & Implementation Coordinator September 4, 2014 1 PA Reach Who are we? Designated by ONC as the PA East and PA West Regional Extension Center We have
Meaningful Use Stage 2: Important Implications for Pediatrics
 Meaningful Use Stage 2: Important Implications for Pediatrics Glossary of Acronyms MU CQM EHR CEHRT EPs CAHs e-rx CPOE emar ONC CMS HHS Meaningful Use Clinical quality measure Electronic health record
Meaningful Use Stage 2: Important Implications for Pediatrics Glossary of Acronyms MU CQM EHR CEHRT EPs CAHs e-rx CPOE emar ONC CMS HHS Meaningful Use Clinical quality measure Electronic health record
Meaningful Use Qualification Plan
 Meaningful Use Qualification Plan Overview Certified EHR technology used in a meaningful way is one piece of a broader Health Information Technology infrastructure intended to reform the health care system
Meaningful Use Qualification Plan Overview Certified EHR technology used in a meaningful way is one piece of a broader Health Information Technology infrastructure intended to reform the health care system
Meaningful Use: Stage 1 and 2 Hospitals (EH) and Providers (EP) Lindsey Mongold, MHA HIT Practice Advisor Oklahoma Foundation for Medical Quality
 and Providers (EP) Lindsey Mongold, MHA HIT Practice Advisor Oklahoma Foundation for Medical Quality") Meaningful Use: Stage 1 and 2 Hospitals (EH) and Providers (EP) Lindsey Mongold, MHA HIT Practice Advisor Oklahoma Foundation for Medical Quality Meaningful Use Stage 1 Focuses on Functional & Interoperability
Meaningful Use: Stage 1 and 2 Hospitals (EH) and Providers (EP) Lindsey Mongold, MHA HIT Practice Advisor Oklahoma Foundation for Medical Quality Meaningful Use Stage 1 Focuses on Functional & Interoperability
Meaningful Use Stage 1:
 Whitepaper Meaningful Use Stage 1: EHR Incentive Program Information -------------------------------------------------------------- Daw Systems, Inc. UPDATED: November 2012 This document is designed to
Whitepaper Meaningful Use Stage 1: EHR Incentive Program Information -------------------------------------------------------------- Daw Systems, Inc. UPDATED: November 2012 This document is designed to
Stage 2 Meaningful Use What the Future Holds. Lindsey Wiley, MHA HIT Manager Oklahoma Foundation for Medical Quality
 Stage 2 Meaningful Use What the Future Holds Lindsey Wiley, MHA HIT Manager Oklahoma Foundation for Medical Quality An Important Reminder For audio, you must use your phone: Step 1: Call (866) 906-0123.
Stage 2 Meaningful Use What the Future Holds Lindsey Wiley, MHA HIT Manager Oklahoma Foundation for Medical Quality An Important Reminder For audio, you must use your phone: Step 1: Call (866) 906-0123.
MEANINGFUL USE. Community Center Readiness Guide Additional Resource #13 Meaningful Use Implementation Tracking Tool (Template) CONTENTS:
 CONTENTS:") Community Center Readiness Guide Additional Resource #13 Meaningful Use Implementation Tracking Tool (Template) MEANINGFUL USE HITECH s goal is not adoption alone but meaningful use of EHRs that is, their
Community Center Readiness Guide Additional Resource #13 Meaningful Use Implementation Tracking Tool (Template) MEANINGFUL USE HITECH s goal is not adoption alone but meaningful use of EHRs that is, their
Stage Two Meaningful Use Measures for Eligible Professionals
 Stage Two Meaningful Use Measures for Eligible Professionals GENERAL REQUIREMENT FOR ELIGIBLE PROFESSIONALS Objective Measure Numerator, Denominator, & Exclusion Application Tips Required by the Final
Stage Two Meaningful Use Measures for Eligible Professionals GENERAL REQUIREMENT FOR ELIGIBLE PROFESSIONALS Objective Measure Numerator, Denominator, & Exclusion Application Tips Required by the Final
Meaningful Use Stage 2
 Meaningful Use Stage 2 Presented by: Sarah Leake, HTS Consultant HTS, a division of Mountain Pacific Quality Health Foundation 1 HTS Who We Are Stage 2 MU Overview Learning Objectives 2014 CEHRT Certification
Meaningful Use Stage 2 Presented by: Sarah Leake, HTS Consultant HTS, a division of Mountain Pacific Quality Health Foundation 1 HTS Who We Are Stage 2 MU Overview Learning Objectives 2014 CEHRT Certification
TABLE 4: STAGE 2 MEANINGFUL USE OBJECTIVES AND ASSOCIATED MEASURES SORTED BY CORE AND MENU SET
 CMS-0044-P 156 TABLE 4: STAGE 2 MEANINGFUL USE OBJECTIVES AND ASSOCIATED MEASURES SORTED BY CORE AND MENU SET Improving quality, safety, efficiency, and reducing health disparities Use computerized provider
CMS-0044-P 156 TABLE 4: STAGE 2 MEANINGFUL USE OBJECTIVES AND ASSOCIATED MEASURES SORTED BY CORE AND MENU SET Improving quality, safety, efficiency, and reducing health disparities Use computerized provider
Meaningful Use Stage 2 Administrator Training
 Meaningful Use Stage 2 Administrator Training 1 During the call please mute your line to reduce background noise. 2 Agenda Review of the EHR Incentive Programs for Stage 2 Meaningful Use Measures and Corresponding
Meaningful Use Stage 2 Administrator Training 1 During the call please mute your line to reduce background noise. 2 Agenda Review of the EHR Incentive Programs for Stage 2 Meaningful Use Measures and Corresponding
Stage 1 Meaningful Use - Attestation Worksheet: Core Measures
 Stage 1 Meaningful Use - Attestation Worksheet: Core Measures Core Measures Objective # Objective Title / Explanation Goal Attestation Response - Values below reflect reponses of most radiologists Explanation
Stage 1 Meaningful Use - Attestation Worksheet: Core Measures Core Measures Objective # Objective Title / Explanation Goal Attestation Response - Values below reflect reponses of most radiologists Explanation
Eligible Professionals (EPs) Purdue Research Foundation
 Purdue Research Foundation") Understanding STAGE 2 Meaningful Use and the Incentive Program Eligible Professionals (EPs) About Incentives Eligible Professionals report during a calendar year Eligible Professionals can only attest
Understanding STAGE 2 Meaningful Use and the Incentive Program Eligible Professionals (EPs) About Incentives Eligible Professionals report during a calendar year Eligible Professionals can only attest
MEETING MEANINGFUL USE IN MICROMD -STAGE TWO- Presented by: Anna Mrvelj EMR Training Specialist
 MEETING MEANINGFUL USE IN MICROMD -STAGE TWO- Presented by: Anna Mrvelj EMR Training Specialist 1 Proposed Rule On April 15, 2015 CMS Issued a new proposal rule for the Medicare and Medicaid EHR Incentive
MEETING MEANINGFUL USE IN MICROMD -STAGE TWO- Presented by: Anna Mrvelj EMR Training Specialist 1 Proposed Rule On April 15, 2015 CMS Issued a new proposal rule for the Medicare and Medicaid EHR Incentive
EHR Reporting Period In 2015
 Meaningful Use: It s Not Too Late For 2015! Jeffrey D. Lehrman, DPM, FACFAS, FASPS, FAPWH APMA Coding Committee Expert Panelist, Codingline.com Fellow, American Academy of Podiatric Practice Management
Meaningful Use: It s Not Too Late For 2015! Jeffrey D. Lehrman, DPM, FACFAS, FASPS, FAPWH APMA Coding Committee Expert Panelist, Codingline.com Fellow, American Academy of Podiatric Practice Management
E Z BIS ELECTRONIC HEALTH RECORDS
 E Z BIS ELECTRONIC HEALTH RECORDS CERTIFICATION AND THE HITECH INCENTIVE PROGRAM The Incentives On July 13, 2010, the U.S. Department of Health and Human Services finalized the Electronic Health Record
E Z BIS ELECTRONIC HEALTH RECORDS CERTIFICATION AND THE HITECH INCENTIVE PROGRAM The Incentives On July 13, 2010, the U.S. Department of Health and Human Services finalized the Electronic Health Record
Attachment 1 Stage 1 Meaningful Use Criteria
 Core Set of Objectives and Measures Must Meet All 15 Measures Stage 1 Objectives Stage 1 Measures Reporting Method Use Computerized Provider Order Entry (CPOE) for medication orders directly entered by
Core Set of Objectives and Measures Must Meet All 15 Measures Stage 1 Objectives Stage 1 Measures Reporting Method Use Computerized Provider Order Entry (CPOE) for medication orders directly entered by
Thank You to Our Sponsors! CMS EHR Incentive Requirements. CMS EHR Incentive Programs. CMS EHR Incentive Programs. Steps to Get Started 3/15/2012
 Thank You to Our Sponsors! AOA EHR Preparedness Program EHR Incentive Programs and Meaningful Use Update Jay W. Henry, O.D., M.S. Philip J. Gross, O.D. CMS EHR Incentive Programs Provide incentive payments
Thank You to Our Sponsors! AOA EHR Preparedness Program EHR Incentive Programs and Meaningful Use Update Jay W. Henry, O.D., M.S. Philip J. Gross, O.D. CMS EHR Incentive Programs Provide incentive payments
Meaningful Use 2015 and beyond. Presented by: Anna Mrvelj EMR Training Specialist
 Meaningful Use 2015 and beyond Presented by: Anna Mrvelj EMR Training Specialist 1 Agenda A look at the CMS Website Finding your EMR version Certification Number Proposed Rule by the Centers for Medicare
Meaningful Use 2015 and beyond Presented by: Anna Mrvelj EMR Training Specialist 1 Agenda A look at the CMS Website Finding your EMR version Certification Number Proposed Rule by the Centers for Medicare
Understanding Meaningful Use Stage 2
 Understanding Meaningful Use Stage 2 Miranda Ladue, Manager, Product Management Adam Plotts, Manager, Product Management Copyright 2011 Allscripts Healthcare Solutions, Inc. Agenda Review MU Timeline MU
Understanding Meaningful Use Stage 2 Miranda Ladue, Manager, Product Management Adam Plotts, Manager, Product Management Copyright 2011 Allscripts Healthcare Solutions, Inc. Agenda Review MU Timeline MU
Electronic Health Record (EHR) Incentive Program. Stage 2 Final Rule Update Part 2
 Incentive Program. Stage 2 Final Rule Update Part 2") Office of Medical Assistance Programs Electronic Health Record (EHR) Incentive Program Stage 2 Final Rule Update Part 2 November 7, 2012 Medical Assistance HIT Initiative 1 Office of Medical Assistance
Office of Medical Assistance Programs Electronic Health Record (EHR) Incentive Program Stage 2 Final Rule Update Part 2 November 7, 2012 Medical Assistance HIT Initiative 1 Office of Medical Assistance
Meaningful Use Cheat Sheet CORE MEASURES: ALL REQUIRED # Measure Exclusions How to Meet in WEBeDoctor
 Meaningful Use Cheat Sheet CORE MEASURES: ALL REQUIRED # Measure Exclusions How to Meet in WEBeDoctor 1 CPOE (Computerized Physician Order Entry) More than 30 percent of all unique patients with at least
Meaningful Use Cheat Sheet CORE MEASURES: ALL REQUIRED # Measure Exclusions How to Meet in WEBeDoctor 1 CPOE (Computerized Physician Order Entry) More than 30 percent of all unique patients with at least
Contact Information: West Texas Health Information Technology Regional Extension Center 3601 4 th Street MS 6232 Lubbock, Texas 79424 806-743-1338
 Contact Information: West Texas Health Information Technology Regional Extension Center 3601 4 th Street MS 6232 Lubbock, Texas 79424 806-743-1338 http://www.wtxhitrec.org/ Grant award - $6.6m Total number
Contact Information: West Texas Health Information Technology Regional Extension Center 3601 4 th Street MS 6232 Lubbock, Texas 79424 806-743-1338 http://www.wtxhitrec.org/ Grant award - $6.6m Total number
Meaningful Use Stage 2: Summary of Proposed Rule for Eligible Professionals (EPs) Wyatt Packer HIT Regional Extension Center (REC) HealthInsight
 Wyatt Packer HIT Regional Extension Center (REC) HealthInsight") Meaningful Use Stage 2: Summary of Proposed Rule for Eligible Professionals (EPs) Wyatt Packer HIT Regional Extension Center (REC) HealthInsight Notice of Proposed Rule Making (NPRM) Stage 2 proposed rule
Meaningful Use Stage 2: Summary of Proposed Rule for Eligible Professionals (EPs) Wyatt Packer HIT Regional Extension Center (REC) HealthInsight Notice of Proposed Rule Making (NPRM) Stage 2 proposed rule
Psychiatrists and Reporting on Meaningful Use Stage 1. August 6, 2012
 Psychiatrists and Reporting on Meaningful Use Stage 1 August 6, 2012 Quick Overview Functional Measures Providers (tracked by NPI) must report on 15 core objectives and associated measures and 5 objectives
Psychiatrists and Reporting on Meaningful Use Stage 1 August 6, 2012 Quick Overview Functional Measures Providers (tracked by NPI) must report on 15 core objectives and associated measures and 5 objectives
CQMs. Clinical Quality Measures 101
 CQMs Clinical Quality Measures 101 BASICS AND GOALS In the past 10 years, clinical quality measures (CQMs) have become an integral component in the Centers for Medicare & Medicaid Services (CMS) drive
CQMs Clinical Quality Measures 101 BASICS AND GOALS In the past 10 years, clinical quality measures (CQMs) have become an integral component in the Centers for Medicare & Medicaid Services (CMS) drive
Meaningful Use of Certified EHR Technology with My Vision Express*
 Insight Software, LLC 3050 Universal Blvd Ste 120 Weston FL 33331-3528 Tel. 877-882-7456 www.myvisionexpress.com Meaningful Use of Certified EHR Technology with My Vision Express* Eligible Professional
Insight Software, LLC 3050 Universal Blvd Ste 120 Weston FL 33331-3528 Tel. 877-882-7456 www.myvisionexpress.com Meaningful Use of Certified EHR Technology with My Vision Express* Eligible Professional
AAP Meaningful Use: Certified EHR Technology Criteria
 AAP Meaningful Use: Certified EHR Technology Criteria On July 13, 2010, the US Centers for Medicare and Medicaid Services (CMS) released a Final Rule establishing the criteria with which eligible pediatricians,
AAP Meaningful Use: Certified EHR Technology Criteria On July 13, 2010, the US Centers for Medicare and Medicaid Services (CMS) released a Final Rule establishing the criteria with which eligible pediatricians,
Meaningful Use Stage 2. Presenter: Linda Wise, EMR Training Specialist
 Meaningful Use Stage 2 Presenter: Linda Wise, EMR Training Specialist 1 AGENDA 2 Agenda Meaningful Use in Review Moving Into Stage 2 Meaningful Use Learning the Requirements Understanding the Measures
Meaningful Use Stage 2 Presenter: Linda Wise, EMR Training Specialist 1 AGENDA 2 Agenda Meaningful Use in Review Moving Into Stage 2 Meaningful Use Learning the Requirements Understanding the Measures
EMR Name/ Model. meridianemr 4.2 CCHIT 2011 certified
 EMR Name/ Model EMR Vendor meridianemr 4.2 CCHIT 2011 certified meridianemr, Inc Core Set of Measures Objective Stage 1 Objectives Stage 1 Measures EMR Module/ Feature 1 Use CPOE for medication orders
EMR Name/ Model EMR Vendor meridianemr 4.2 CCHIT 2011 certified meridianemr, Inc Core Set of Measures Objective Stage 1 Objectives Stage 1 Measures EMR Module/ Feature 1 Use CPOE for medication orders
Meaningful Use Guidelines: Radiologists
 Meaningful Use Meaningful Use (MU) criteria allows providers to demonstrate that they are using certified EHR technology in ways that can be measured significantly in quality and in quantity. Many assume
Meaningful Use Meaningful Use (MU) criteria allows providers to demonstrate that they are using certified EHR technology in ways that can be measured significantly in quality and in quantity. Many assume
VIII. Dentist Crosswalk
 Page 27 VIII. Dentist Crosswalk Overview The final rule on meaningful use requires that an Eligible Professional (EP) report on both clinical quality measures and functional objectives and measures. While
Page 27 VIII. Dentist Crosswalk Overview The final rule on meaningful use requires that an Eligible Professional (EP) report on both clinical quality measures and functional objectives and measures. While
Medicare & Medicaid EHR Incentive Programs
 Medicare & Medicaid EHR Incentive Programs Stage 2 NPRM Overview Robert Anthony Office of E-Health Standards and Services Marsha Smith Office of Clinical Standards and Quality March 21, 2012 Proposed Rule
Medicare & Medicaid EHR Incentive Programs Stage 2 NPRM Overview Robert Anthony Office of E-Health Standards and Services Marsha Smith Office of Clinical Standards and Quality March 21, 2012 Proposed Rule
STAGE 2 MEANINGFUL USE FOR ELIGIBLE HOSPITALS AND CRITICAL ACCESS HOSPITALS (CAHS)
") STAGE 2 MEANINGFUL USE FOR ELIGIBLE HOSPITALS AND CRITICAL ACCESS HOSPITALS (CAHS) CORE MEASURES must meet all CPOE for Medication, Laboratory and Radiology Orders Objective: Use computerized provider
STAGE 2 MEANINGFUL USE FOR ELIGIBLE HOSPITALS AND CRITICAL ACCESS HOSPITALS (CAHS) CORE MEASURES must meet all CPOE for Medication, Laboratory and Radiology Orders Objective: Use computerized provider
Incentives to Accelerate EHR Adoption
 Incentives to Accelerate EHR Adoption The passage of the American Recovery and Reinvestment Act (ARRA) of 2009 provides incentives for eligible professionals (EPs) to adopt and use electronic health records
Incentives to Accelerate EHR Adoption The passage of the American Recovery and Reinvestment Act (ARRA) of 2009 provides incentives for eligible professionals (EPs) to adopt and use electronic health records
Lunch and Learn IFAF 09/24/11. Michael L. Brody, DPM
 Lunch and Learn IFAF 09/24/11 Michael L. Brody, DPM Disclaimers Sammy Sponsor of this presentation PICA Biomedix All Pro Imaging The Brave New World of HIT Today s Topics: PQRS E-Rx EMR Health Information
Lunch and Learn IFAF 09/24/11 Michael L. Brody, DPM Disclaimers Sammy Sponsor of this presentation PICA Biomedix All Pro Imaging The Brave New World of HIT Today s Topics: PQRS E-Rx EMR Health Information
MICROMD EMR VERSION 9.0 2014 OBJECTIVE MEASURE CALCULATIONS
 MICROMD EMR VERSION 9.0 2014 OBJECTIVE MEASURE CALCULATIONS TABLE OF CONTENTS PREFACE Welcome to MicroMD EMR... i How This Guide is Organized... i Understanding Typographical Conventions... i Cross-References...
MICROMD EMR VERSION 9.0 2014 OBJECTIVE MEASURE CALCULATIONS TABLE OF CONTENTS PREFACE Welcome to MicroMD EMR... i How This Guide is Organized... i Understanding Typographical Conventions... i Cross-References...
EMR Name/ Model. Cerner PowerChart Ambulatory (PowerWorks ASP)
") EMR Name/ Model EMR Vendor Cerner PowerChart Ambulatory (PowerWorks ASP) Cerner Corporation Core Set of Measures 1 Use CPOE for medication orders directly entered by any licensed healthcare professional
EMR Name/ Model EMR Vendor Cerner PowerChart Ambulatory (PowerWorks ASP) Cerner Corporation Core Set of Measures 1 Use CPOE for medication orders directly entered by any licensed healthcare professional
Quest to Attest 2014 Stage 1 Meaningful Use. Brett M. Paepke, OD Advisor, Stage 1 Meaningful Use
 Quest to Attest 2014 Stage 1 Meaningful Use Brett M. Paepke, OD Advisor, Stage 1 Meaningful Use Goals Discussion of MU and the Incentive Program Analysis of Stage 1 Objectives Summary of RevolutionEHR
Quest to Attest 2014 Stage 1 Meaningful Use Brett M. Paepke, OD Advisor, Stage 1 Meaningful Use Goals Discussion of MU and the Incentive Program Analysis of Stage 1 Objectives Summary of RevolutionEHR
hospital s or CAH s inpatient or professional guidelines
 EMR Name/ Model EMR Vendor XLEMR/XLEMR-2011-MU XLEMR Objective 1 Core Set of Measures Use CPOE for medication orders Use CPOE for medication orders More than 30% of unique patients directly entered by
EMR Name/ Model EMR Vendor XLEMR/XLEMR-2011-MU XLEMR Objective 1 Core Set of Measures Use CPOE for medication orders Use CPOE for medication orders More than 30% of unique patients directly entered by
Overview of the EHR Incentive Program
 Overview of the EHR Incentive Program presented by Meaningful Use Stages 1 & 2 1 P Automated coding P Chief-complaint-driven P AnticiPlate Technology P Point-and-Click Functionality P erx through Surescripts
Overview of the EHR Incentive Program presented by Meaningful Use Stages 1 & 2 1 P Automated coding P Chief-complaint-driven P AnticiPlate Technology P Point-and-Click Functionality P erx through Surescripts
Stage 2 of Meaningful Use Summary of Proposed Rule
 Stage 2 of Meaningful Use Summary of Proposed Rule Background In order to receive incentives for the adoption of electronic health records (EHRs) under either the Medicare or Medicaid (Medi-Cal) incentive
Stage 2 of Meaningful Use Summary of Proposed Rule Background In order to receive incentives for the adoption of electronic health records (EHRs) under either the Medicare or Medicaid (Medi-Cal) incentive
Reporting Period: For Stage 2, the reporting period must be the entire Federal Fiscal Year.
 Eligible Hospital and Critical Access Hospital (CAH) Attestation Worksheet for Stage 2 of the Medicare Electronic Health Record (EHR) Incentive Program The Eligible Hospital and CAH Attestation Worksheet
Eligible Hospital and Critical Access Hospital (CAH) Attestation Worksheet for Stage 2 of the Medicare Electronic Health Record (EHR) Incentive Program The Eligible Hospital and CAH Attestation Worksheet
2 Final Rule for EPs. Meaningful Use Stage 2. October 18, 2012
 Meaningful Use Stage 2 Final Rule for EPs October 18, 2012 Ivy Baer ibaer@aamc.org 202-828-0499 Mary Wheatley mwheatley@aamc.org 202-862-6297 Meaningful Use Stage 2 CMS final rule was released in the Federal
Meaningful Use Stage 2 Final Rule for EPs October 18, 2012 Ivy Baer ibaer@aamc.org 202-828-0499 Mary Wheatley mwheatley@aamc.org 202-862-6297 Meaningful Use Stage 2 CMS final rule was released in the Federal
An Introduction to the Medicaid EHR Incentive Program for Eligible Professionals
 EHR Incentive Programs A program administered by the Centers for Medicare & Medicaid Services (CMS) An Introduction to the Medicaid EHR Incentive Program for Eligible Professionals cms.gov/ehrincentiveprograms
EHR Incentive Programs A program administered by the Centers for Medicare & Medicaid Services (CMS) An Introduction to the Medicaid EHR Incentive Program for Eligible Professionals cms.gov/ehrincentiveprograms
Appendix 2. PCMH 2014 and CMS Stage 2 Meaningful Use Requirements
 Appendix 2 PCMH 2014 and CMS Stage 2 Meaningful Use Requirements Appendix 2 PCMH 2014 and CMS Stage 2 Meaningful Use Requirements 2-1 APPENDIX 2 PCMH 2014 AND CMS STAGE 2 MEANINGFUL USE REQUIREMENTS Medicare
Appendix 2 PCMH 2014 and CMS Stage 2 Meaningful Use Requirements Appendix 2 PCMH 2014 and CMS Stage 2 Meaningful Use Requirements 2-1 APPENDIX 2 PCMH 2014 AND CMS STAGE 2 MEANINGFUL USE REQUIREMENTS Medicare
Qualifying for Medicare Incentive Payments with Crystal Practice Management. Version 4.1.25
 Qualifying for Medicare Incentive Payments with Crystal Practice Management Version 4.1.25 01/01/ Table of Contents Qualifying for Medicare Incentive Payments with... 1 General Information... 3 Links to
Qualifying for Medicare Incentive Payments with Crystal Practice Management Version 4.1.25 01/01/ Table of Contents Qualifying for Medicare Incentive Payments with... 1 General Information... 3 Links to
MDeverywhere, Inc. Presents 2014 CMS EHR Incentive Program Requirements: What Providers Need To Know
 MDeverywhere, Inc. Presents 2014 CMS EHR Incentive Program Requirements: What Providers Need To Know Presented by: Kristen Heffernan Director Product Management & Marketing, Henry Schein MicroMD Agenda
MDeverywhere, Inc. Presents 2014 CMS EHR Incentive Program Requirements: What Providers Need To Know Presented by: Kristen Heffernan Director Product Management & Marketing, Henry Schein MicroMD Agenda
MEANINGFUL USE STAGE 2 Summary of Proposed Rule (EP)
") MEANINGFUL USE STAGE 2 Summary of Proposed Rule (EP) The Meaningful Use Stage 2 Notice of Proposed Rule Making (NPRM) has been released and entered a 60-day comment period (March 7-May 6, 2012). HealthInsight
MEANINGFUL USE STAGE 2 Summary of Proposed Rule (EP) The Meaningful Use Stage 2 Notice of Proposed Rule Making (NPRM) has been released and entered a 60-day comment period (March 7-May 6, 2012). HealthInsight
Achieving Meaningful Use Training Manual
 Achieving Meaningful Use Training Manual Terms EP Eligible Professional Medicare Eligible Professional o Doctor of Medicine or Osteopathy o Doctor of Dental Surgery or Dental Medicine o Doctor of Podiatric
Achieving Meaningful Use Training Manual Terms EP Eligible Professional Medicare Eligible Professional o Doctor of Medicine or Osteopathy o Doctor of Dental Surgery or Dental Medicine o Doctor of Podiatric
Attesting for Meaningful Use Stage 2 in 2014 Customer Help Guide
 Attesting for Meaningful Use Stage 2 in 2014 Customer Help Guide Table of Contents PURPOSE OF THIS DOCUMENT 4 MEANINGFUL USE STAGE 2 OVERVIEW 4 ATTESTING FOR CORE OBJECTIVES 5 CORE OBJECTIVE #1: CPOE 7
Attesting for Meaningful Use Stage 2 in 2014 Customer Help Guide Table of Contents PURPOSE OF THIS DOCUMENT 4 MEANINGFUL USE STAGE 2 OVERVIEW 4 ATTESTING FOR CORE OBJECTIVES 5 CORE OBJECTIVE #1: CPOE 7
EHR Meaningful Use Guide
 EHR Meaningful Use Guide for Stage I (2011) HITECH Attestation Version 2.0 Updated May/June 2014 in partnership with 1-866-866-6778 platinum@medicfusion.com www.medicfusion.com/platinum Medicfusion EMR
EHR Meaningful Use Guide for Stage I (2011) HITECH Attestation Version 2.0 Updated May/June 2014 in partnership with 1-866-866-6778 platinum@medicfusion.com www.medicfusion.com/platinum Medicfusion EMR
2013 Meaningful Use Dashboard Calculation Guide
 2013 Meaningful Use Dashboard Calculation Guide Learn how to use Practice Fusion s Meaningful Use Dashboard to help you achieve Meaningful Use. For more information, visit the Meaningful Use Center. General
2013 Meaningful Use Dashboard Calculation Guide Learn how to use Practice Fusion s Meaningful Use Dashboard to help you achieve Meaningful Use. For more information, visit the Meaningful Use Center. General
A Guide to Understanding and Qualifying for Meaningful Use Incentives
 A Guide to Understanding and Qualifying for Meaningful Use Incentives A White Paper by DrFirst Copyright 2000-2012 DrFirst All Rights Reserved. 1 Table of Contents Understanding and Qualifying for Meaningful
A Guide to Understanding and Qualifying for Meaningful Use Incentives A White Paper by DrFirst Copyright 2000-2012 DrFirst All Rights Reserved. 1 Table of Contents Understanding and Qualifying for Meaningful
NY Medicaid EHR Incentive Program. Eligible Professionals Meaningful Use Stage 2 (MU2) Webinar www.emedny.org/meipass
 Webinar www.emedny.org/meipass") Eligible Professionals Meaningful Use Stage 2 (MU2) Webinar www.emedny.org/meipass May 2015 2 Meaningful Use Stage 2 Overview of EHR Introduction to Meaningful Use Meaningful Use Stage 2 Objectives Clinical
Eligible Professionals Meaningful Use Stage 2 (MU2) Webinar www.emedny.org/meipass May 2015 2 Meaningful Use Stage 2 Overview of EHR Introduction to Meaningful Use Meaningful Use Stage 2 Objectives Clinical
Achieving Meaningful Use with Centricity EMR
 GE Healthcare Achieving Meaningful Use with Centricity EMR Are you Ready to Report? GE Healthcare EMR Consulting CHUG Fall Conference October 2010 Achieving Meaningful Use with Centricity EMR The EMR Consulting
GE Healthcare Achieving Meaningful Use with Centricity EMR Are you Ready to Report? GE Healthcare EMR Consulting CHUG Fall Conference October 2010 Achieving Meaningful Use with Centricity EMR The EMR Consulting
Are you ready? Meaningful Use Stage 2 HIT Summit July 26, 2014
 Are you ready? Meaningful Use Stage 2 HIT Summit July 26, 2014 Meaningful Use Stage 2 Are you Ready? Speakers: Robyn Polinar, BA, MBA, AMB & Community EMR Supervisor Hawai i Pacific Health Nadine Owen,
Are you ready? Meaningful Use Stage 2 HIT Summit July 26, 2014 Meaningful Use Stage 2 Are you Ready? Speakers: Robyn Polinar, BA, MBA, AMB & Community EMR Supervisor Hawai i Pacific Health Nadine Owen,
Meaningful Use - Stage 1. And. Practice Maximus
 Meaningful Use - Stage 1 And Practice Maximus The following explains how Practice Maximus certified EHR module allows user to achieve meaningful use objectives for Stage 1. Eligible Professionals (EP)
Meaningful Use - Stage 1 And Practice Maximus The following explains how Practice Maximus certified EHR module allows user to achieve meaningful use objectives for Stage 1. Eligible Professionals (EP)
Stage 2 Overview Tipsheet Last Updated: August, 2012
 Stage 2 Overview Tipsheet Last Updated: August, 2012 Overview CMS recently published a final rule that specifies the Stage 2 criteria that eligible professionals (EPs), eligible hospitals, and critical
Stage 2 Overview Tipsheet Last Updated: August, 2012 Overview CMS recently published a final rule that specifies the Stage 2 criteria that eligible professionals (EPs), eligible hospitals, and critical
Meaningful Use Stage 2
 Meaningful Use Stage 2 Shannon Vogel Director, Health Information Technology Electronic Health Record Boost ARRA passed on Feb. 13, 2009. Health Information Technology for Economic and Clinical Health
Meaningful Use Stage 2 Shannon Vogel Director, Health Information Technology Electronic Health Record Boost ARRA passed on Feb. 13, 2009. Health Information Technology for Economic and Clinical Health
Meaningful Use Stage 2 MU Audits
 Meaningful Use Stage 2 MU Audits Presented by: Deb Anderson, CPHIMS HTS Consultant HTS, a division of Mountain Pacific Quality Health Foundation 1 CEHRT Certified Electronic Health Record Technology (EHR)
Meaningful Use Stage 2 MU Audits Presented by: Deb Anderson, CPHIMS HTS Consultant HTS, a division of Mountain Pacific Quality Health Foundation 1 CEHRT Certified Electronic Health Record Technology (EHR)
Stage 2 Meaningful Use
 Stage 2 Meaningful Use Stage 2 Topics Overview 2014 Reporting Changes Medicaid Provider Eligibility Measures Overview Core Objectives Comparison Menu Objectives Comparison Clinical Quality Measures 2 High
Stage 2 Meaningful Use Stage 2 Topics Overview 2014 Reporting Changes Medicaid Provider Eligibility Measures Overview Core Objectives Comparison Menu Objectives Comparison Clinical Quality Measures 2 High
We're Ready for MU2...Are You?
 Meaningful Use Are you considering purchasing an Electronic Health Record (EHR) or moving from your current vendor? Is your goal to attain Meaningful Use status in order to receive EHR incentive dollars?
Meaningful Use Are you considering purchasing an Electronic Health Record (EHR) or moving from your current vendor? Is your goal to attain Meaningful Use status in order to receive EHR incentive dollars?
Stage 2 of Meaningful Use: Ten Points of Interest
 November 8, 2012 Practice Group: Health Care Stage 2 of Meaningful Use: Ten Points of Interest By Patricia C. Shea On September 4, 2012, the Department of Health and Human Services, Centers for Medicare
November 8, 2012 Practice Group: Health Care Stage 2 of Meaningful Use: Ten Points of Interest By Patricia C. Shea On September 4, 2012, the Department of Health and Human Services, Centers for Medicare
Modified Stage 2 Final Rule 2015-2017
 Modified Stage 2 Final Rule 2015-2017 Illinois Health Information Technology Regional Extension Center (ILHITREC) SUPPORT PROVIDED BY ILHITREC: The Illinois Health Information Technology Regional Extension
Modified Stage 2 Final Rule 2015-2017 Illinois Health Information Technology Regional Extension Center (ILHITREC) SUPPORT PROVIDED BY ILHITREC: The Illinois Health Information Technology Regional Extension
TABLE B5: STAGE 2 OBJECTIVES AND MEASURES
 294 TABLE B5: STAGE 2 OBJECTIVES AND MEASURES CORE SET Improving quality, safety, efficiency, and reducing health disparities Use computerized provider order entry (CPOE) for medication, laboratory and
294 TABLE B5: STAGE 2 OBJECTIVES AND MEASURES CORE SET Improving quality, safety, efficiency, and reducing health disparities Use computerized provider order entry (CPOE) for medication, laboratory and
Meaningful Use in 2015 and Beyond Changes for Stage 2
 Meaningful Use in 2015 and Beyond Changes for Stage 2 Jennifer Boaz Transformation Support Specialist Proprietary 1 Definitions AIU = Adopt, Implement or Upgrade EP = Eligible Professional API = Application
Meaningful Use in 2015 and Beyond Changes for Stage 2 Jennifer Boaz Transformation Support Specialist Proprietary 1 Definitions AIU = Adopt, Implement or Upgrade EP = Eligible Professional API = Application
0 What is Meaningful Use and where are we? 0 What is the Physician Quality Reporting System and where stage are we on?
 Outline 0 What is Meaningful Use and where are we? 0 What is the Physician Quality Reporting System and where stage are we on? 0 How can we leverage the EMR to demonstrate the quality of our care? Meaningful
Outline 0 What is Meaningful Use and where are we? 0 What is the Physician Quality Reporting System and where stage are we on? 0 How can we leverage the EMR to demonstrate the quality of our care? Meaningful
Medicare & Medicaid EHR Incentive Program Meaningful Use Stage 1 Requirements Summary. http://www.cms.gov/ehrincentiveprograms/
 Medicare & Medicaid EHR Incentive Program Meaningful Use Stage 1 Requirements Summary 2010 What are the Requirements of Stage 1 Meaningful Use? Basic Overview of Stage 1 Meaningful Use: Reporting period
Medicare & Medicaid EHR Incentive Program Meaningful Use Stage 1 Requirements Summary 2010 What are the Requirements of Stage 1 Meaningful Use? Basic Overview of Stage 1 Meaningful Use: Reporting period
BEGINNER MEDICAID EHR INCENTIVE PROGRAM FOR ELIGIBLE PROFESSIONALS. » An Introduction to: Last Updated: April 2014
 01 BEGINNER» An Introduction to: MEDICAID EHR INCENTIVE PROGRAM FOR ELIGIBLE PROFESSIONALS Last Updated: April 2014 Table of contents How to use this guide... 2 1. Program basics... 5 What is the Medicaid
01 BEGINNER» An Introduction to: MEDICAID EHR INCENTIVE PROGRAM FOR ELIGIBLE PROFESSIONALS Last Updated: April 2014 Table of contents How to use this guide... 2 1. Program basics... 5 What is the Medicaid