Barrett s Esophagus and Endoscopic Therapy
|
|
|
- Denis Aubrey Franklin
- 10 years ago
- Views:
Transcription
1 Barrett s Esophagus and Endoscopic Therapy John A. Dumot, DO Department of Gastroenterology Cleveland Clinic Foundation Disclosures: Research support from CSA Medical Inc. [email protected]

2 Objectives Relationship of BE, acid reflux and esophageal cancer Screening and surveillance guidelines Management of dysplasia and early cancers

3 Esophagogastric Junction Squamocolumnar junction View on retroflexion

4 Esophagogastric Junction Definitions Squamocolumnar junction (SCJ) = juxtaposition of the squamous and columnar mucosa Esophagogastric junction (EGJ) = dynamic area including the distal esophagus and proximal stomach Hiatal hernia = foreshortened esophagus with proximal stomach herniated into the chest Columnar lined esophagus = SCJ displaced proximal to EGJ

5 Acid Reflux and EGJ Ring during distention Same ring during contraction

6 Hiatal Hernia and Esophagitis Lax LES Small erosions

7 Histology of the EGJ Junction-type epithelium Tortuous, tubular mucus secreting glands without parietal cells 1 to 4 mm in children autopsy study Ormsby, Mod Path 2000 Kilgore, Am J Gastroenterol 1999

8 Histology of the EGJ Alcian blue/pas+ Squamocolumnar Junction

9 Hiatal Hernia and Erosive Esophagitis LA Grade C 1 mucosal breaks bridging the tops of folds but involving <75% of the circumference LA Grade D 1 mucosal breaks bridging the tops of folds and involving >75% of the circumference

10 Healing after Erosive Esophagitis Hiatal hernia with short segment Barrett s Severe peptic stricture

11 Barrett s and Esophageal Cancer Long segment BE with mass lesion Mass lesion is EUS stage T2N1

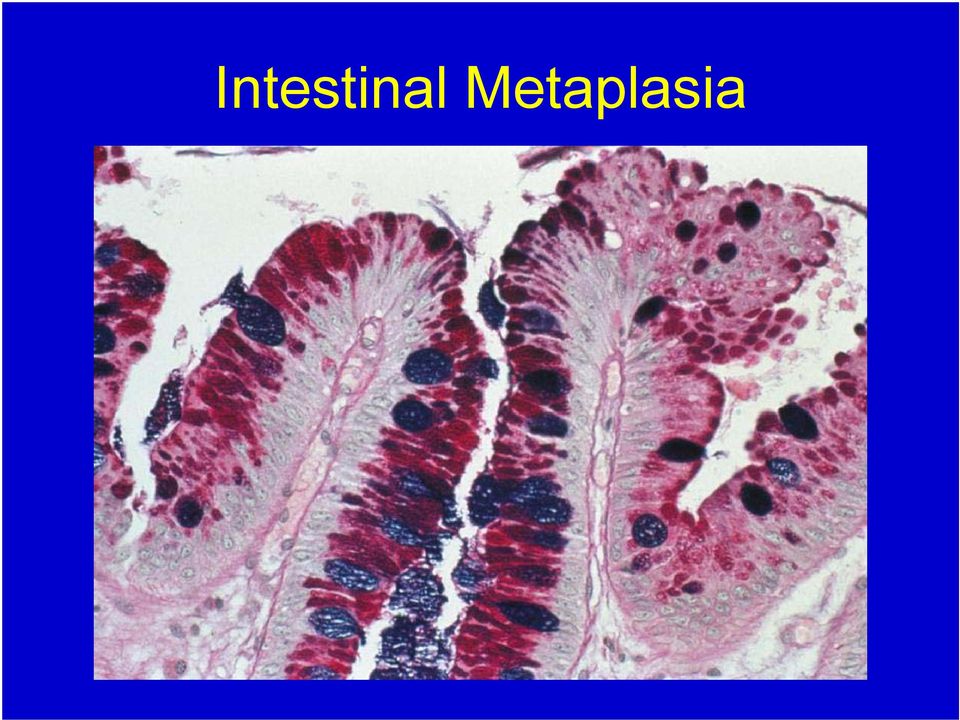
12 Barrett s Esophagus Pathogenesis of Barrett s Repair of injured distal esophageal mucosa Animal model of surgical hiatal hernia with increased acid secretion induces columnar epithelium Cell of origin candidates: esophageal glandular cells gastric cardia mucosa primordial stem cell

13 Intestinal Metaplasia
14 Endoscopic Screening for BE Criteria for Effective Screening Tool High incidence disease High death/disability rate Early treatment decreases mortality Tool easy to apply and acceptable Inexpensive Accurate test BE Screening? BE-yes Ca-no BE-no Ca-yes BE-no Ca-yes No No Yes Subsequent f/u acceptable?

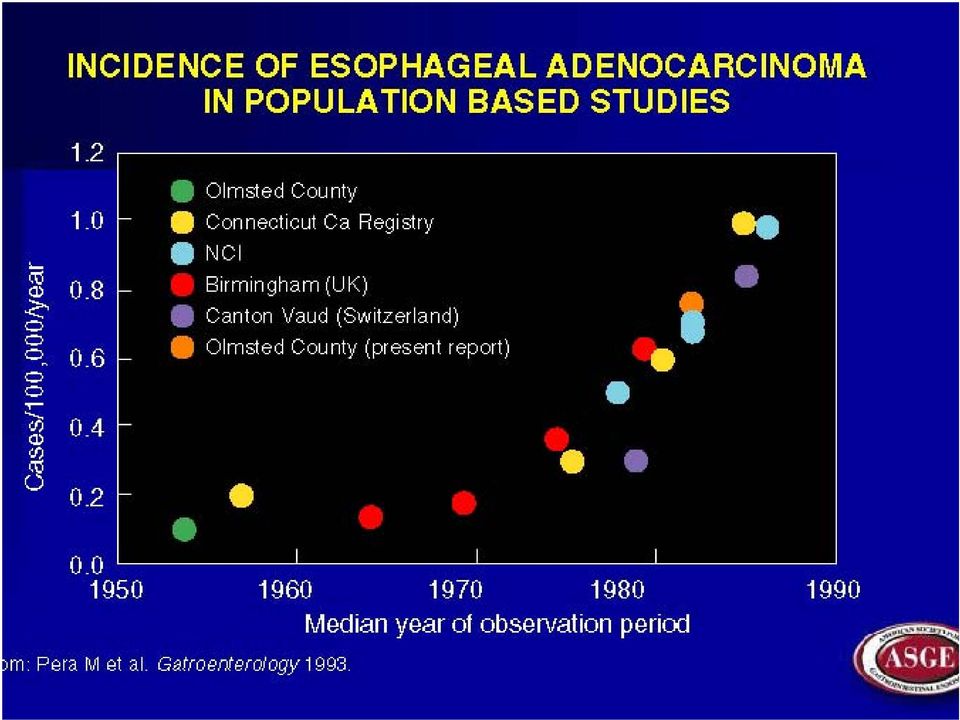
15 Barrett s Screening Rationale 1. Rising incidence of esophageal adenocarcinoma

16 Esophageal Cancer Distal esophageal and GEJ cancer mortality rate increased 4-fold over the last 20 years 5- to 6-fold increase from 1940 to 1989 Esophagus 3.6 / 100,000 (+3.6 APC) Stomach 4.3 / 100,000 (-2.8 APC)
 Stomach 4.")
17 Estimated New Cancer Cases US 2008 Both Men Women igestive system 271, , ,730 Colon & rectum 148,810 77,250 71,560 Pancreas 37,680 18,770 18,910 Stomach 21,500 13,190 8,310 Liver 21,370 15,190 6,180 Esophagus 16,470 12,970 3,500 Small intestine 6,110 3,200 2,910 ACS

18 Estimated Cancer Deaths US 2008 Both Men Women igestive system 135,130 74,850 60,280 Colon & rectum 49,960 24,260 25,700 Pancreas 34,290 17,500 16,790 Liver 18,410 12,570 5,840 Esophagus 14,280 11,250 3,030 Stomach 10,880 6,450 4,430 Small intestine 1, ACS

19 Male Cancer Deaths Lung & bronchus 90,810 (31%) 2. Prostate 28,660 (10%) 3. Colon & rectum 24,260 (8%) 4. Pancreas 17,500 (6%) 5. Liver & intrahep bile duct 12,570 (4%) 6. Leukemia 12,460 (4%) 7. Esophagus 11,250 (4%) 8. Urinary bladder 9,950 (3%) 9. Non-Hodgkin lymphoma 9,790 (3%) 10.Kidney & renal pelvis 8,100 (3%)
 8. Urinary bladder 9,950 (3%) 9.")
20
21 Esophageal Adenocarcinoma and Colon Cancer Screening Esophageal adenocarcinoma incidence 3 per 100,000 Colon cancer incidence 58 per 100,000
22 Barrett s Screening Rationale 1. Rising incidence of esophageal adenocarcinoma 2. Reflux symptoms are a risk factor for BE and esophageal cancer
23 Barrett s Esophagus How common is BE? < 1% of unselected autopsies < 1% of patients without GERD symptoms 6% - 12% of symptomatic GERD patients
24 GERD Symptoms and BE Barrett s (N=79) GERD (N=94) P-value Severe symptoms 85% 59% <0.02 Duration (yr) <0.05 Age of onset (yr) 35.3 ± ± 13 <0.05 Eisen Am J Gastroenterol 1997;92
25 Barrett s Esophagus Who develops Barrett s? Clearly associated with severe GERD Male:female ratio 9:1 Hiatal hernia Low LES pressures
26 BE & Duration of GERD Symptoms Symptom Duration OR < 1 Yr 1-5 Yr 5-10 Yr > 10 Yr Lieberman Am J Gastroenterol 1997;92:1
27 GERD and Esophageal Cancer Odds Ratio Recurrent reflux (1 / wk) 7 Frequent reflux (>3 / wk) 16 Severity & duration (>20 yr.) 43 Lagergeren NEJM 199
28 Barrett s Screening Rationale 1. Rising incidence of esophageal adenocarcinoma 2. Reflux symptoms are a risk factor for BE and esophageal cancer 3. Barrett s esophagus is the only known intermediate stage
29 Rising Incidence of BE in Olmstead County Conio Gut 2001
30 North America Estimates of Barrett s and Esophageal Cancer 4,500,000 4,290,000 4,000,000 3,500,000 Population Size 3,000,000 2,500,000 2,000,000 1,500,000 1,980,000 1,000, , ,000 SIM LGD HGD CA Barrett's Esophagus Disease State 20,513
31 Barrett s and Esophageal Cancer Mean annual incidence of cancer in long- and short- segment BE is ~0.5% 30-fold increase over the general population Short segment BE Elevated lesion < 20mm diameter
32 Short-Segment Barrett s Dilemmas of the expanded definition of BE Differentiation from gastric metaplasia Differentiation from cardia intestinal metaplasia Natural history of ultra-short segment BE
33
34 Barrett s Screening Rationale 1. Rising incidence of esophageal adenocarcinoma 2. Reflux symptoms are a risk factor for BE and esophageal cancer 3. Barrett s esophagus is the only known intermediate stage 4. Early detection provides better survival
35 Barrett s Screening Rationale Only 5% of esophageal adenocarcinoma cases occur in patients with known Barrett s esophagus
36 Five-Year Relative Survival Rates by Stage at Diagnosis Local Regional Distant Esophagus Colon & rectum Breast (female) Pancreas Stomach Ries SEER Cancer Statistics Review,
37 Impact of Surveillance in Barrett s Associated Cancers Corley Gastroenterol 200
38 Impact of Surveillance in Barrett s Associated Cancers Corley Gastroenterol 200
39
40
41 Screening for BE GERD symptoms for > 10 years Endoscopic biopsy: Columnar epithelium Intestinal metaplasia Any length
42 Endoscopic Surveillance of Barrett s Falk Techniques in GI Endoscopy 2000;2:
43 Endoscopic Surveillance of Barrett s Levine Gastrointest Endosc 1991;37:3
44 Distribution of Dysplasia and Cancer in Resection Specimens SCJ SCJ Barrett s, no dysplasia Low - grade dysplasia High - grade dysplasia Cancer Cameron Am J Gastroenterol 1997;92:58
45
46 Endoscopic Surveillance of Barrett s ysplasia one ndefinite ow-grade igh-grade Focal Multi-focal Interval 3 years* 3 to 6 months after PPI 12 months 3 months Intervention or observation? *After 2 exams are negative for dysplasia 1 yr apart *Requires 4-quadrant biopsies every 1 to 2 cm
47
48 Staging Esophageal Cancer
49
50 EGJ Cancer Extrinsic compression from infiltrative gastric cardia mass Prosthetic stent required to maintain lumen
51 Screening for Barrett s Barriers to screening Cost Screening tool not universally accepted Compliance with follow-up Future plans for screening Small bore endoscopes Capsule endoscopy Genetic testing
52 Capsule Endoscopy Screening for BE Capsule Recorder Lower Sphincter with Short Segment BE
53 Endoscopic Therapy for BE with Dysplasia? ASSUMPTIONS Esophagectomy may not be in the best interest of all patients Observation without intervention may not be the best option in some patients Successful eradication of dysplasia and early cancers is possible in some patients
54 Endoscopic Therapy Ablation vs. Mucosectomy Ablation EMR Pathologic Staging Pain Strictures Bleeding Cancer cover-up Strictures
55 Photodynamic Therapy (PDT) ed Light Cell Death O 2 P P* 3 O 2
56 PDT for Barrett s and Early Cancer Barrett s segment with IMCa Cylindrical laser fiber and light
57 PDT for Barrett s and Early Cancer Severe esophagitis 48 hrs Follow up surveillance 1 yr
58 PDT Long Term Follow-up Two year follow-up reveals ongoing esophagitis due to unremitting reflux.
59 PDT for Barrett s and Early Cancer Photofrin only FDA approved therapy 70% - 80% effective Up to 3 treatment sessions required Complications Photosensitivity for days per session Universal chest pain 30% patients stricture
60 PDT for Barrett s and Early Cancer 100 patients (13 with T1 lesions) Light dose 100 to 250 J/cm Treatment failures 3 of 13 cancers progressed Complications strictures in 34% pain Follow up 19 months (4 to 84) Centering balloons Overholt Gastrointest Endosc 1
61 PDT for Barrett s HGD Multicenter trial 208 patients (2:1) PDT vs. omeprazole Complete ablation HGD 77% (106/138) PDT compared to 39% (27/70) omeprazole group Multiple treatments 68% PDT patients required 2 treatments 47% PDT patients required 3 treatments Overholt Gastrointest Endosc 2005;62
62 PDT for Barrett s HGD Multicenter trial 5 year follow up 208 patients (2:1) PDT vs. omeprazole Progression to cancer 15% PDT compared to 29% omeprazole group Overholt Gastrointest Endosc 2007;66:
63 PDT Stricture Short inflammatory 5 mm stricture Balloon dilation to 16 mm
64 Barrett s Esophagus after PDT Residual islands of dysplasia BICAP ablation
65 Cleveland Clinic Experience with PDT 17 patients (12 IMCA / 5 HGD) Follow up 2.3 (±1.7) years Age 78.9 (±5.1) BE length 5.8 (±2.2) cm 29% PDT alone 42% PDT + other endoscopic treatments Non-responders 29%
66 RFA - HALO 360 System Circumferential balloon-ablation Controlled depth energy density, electrode geometry
67 RFA - HALO 90 System Scope-mounted ablation Primary therapy short segment Barrett s touch-up residual disease
68 AIM II Complete Response Complete response to SIM in 98% patients (n = 70) 2.5-year follow-up after stepwise circumferential and focal ablation Fleischer Gastrointest Endosc 2008
69 RFA Advantages Limited depth of injury Limits strictures Immediate effect No restrictions on surgical anatomy or complex hiatal hernias
70 RFA Limitations Limited depth of injury Inadequate for nodular areas Requires contact with mucosa Skip areas and residual disease
71 RFA Limitations EGJ most like area for failure
72 RFA Summary 85-98% Complete response IM and dysplasia Elimination of abnormal genetic markers Preservation of esophageal function Safety profile high with low incidence strictures Pain significant and requires management Requires contact with the mucosa Difficult to treat in strictures or angulated lumen Inadequate response with nodular mucosa
73 LN CryoSpray Ablation (CSA)
74 LN Cryotherapy he freeze-thaw cycle Mechanism of Injury Ice crystals disrupt lipids and cytoskeleton Ischemia and vascular stasis Reperfusion injury with cellular leakage and submucosal hemorrhage Inflammatory response Immune stimulation Apoptosis
75 LN Cryotherapy Depth of Injury 1 hour: minimal inflammation 48 hours: marked inflammation Johnston Gastrointest Endosc 2001 A3448
76 LN Cryotherapy Advantages High patient tolerance Minimal chest pain Familiarity with concept Able to treat uneven surfaces Possible to treat submucosal lesions Greenwald DDW 2007
77 Dosimetry Spray duration (10 20 seconds) Spray cycles (2 4) LN Cryotherapy
78 LN Cryotherapy Risks Liquid nitrogen conversion to gas 20 second spray releases 7 8 liters Perforation 3 of 116 patients; 365 cases 2 Gastric rents from over distention 1 Pneumoperitoneum
79 Strictures 4% LN Cryotherapy Risks Appears limited to those with prior narrowing or therapy Lip ulcer Pain usually mild 0 to 5 days
80 Johnston Gastrointest Endosc 2005
81 Dumot Gastrointest Endosc 2009
82 LN Cryotherapy with EMR Dumot Gastrointest Endosc 2009
83 LN Cryotherapy and Squamous Cell Cancer SSC case series (n = 6) 74 years median age (IQR 65 82) 2 Tsm1 and 4 Tm 20 mm median size (IQR 14-26) Cricopharyngeus (3), diverticulum (1), stricture (3), varices (1) and prior radiation therapy (3) Uniform response 5 of 6 local complete response Dumot DDW 2009
84 Invasive SCC PET positive 3 rd head / neck ca LN Cryotherapy and Squamous Cell Cancer
85 Future Goals Improve decompression Safety Increase dosimetry (depth of injury) Reduce treatment times Improve visibility
86 LN Cryotherapy Summary Unique mechanism Noncontact technique effective for lesions in difficult topography Depth of injury capable of treating early cancers High patient acceptance Low incidence of pain and strictures Patient familiarity
87 Cap-fitted Technique Crescent-type snare Friction fit caps Disposable injection needle
88 Cap-fitted EMR Technique Submucosal injection is made in standard fashion Crescent-shaped snare is pre-looped into the cap rim Cap sucks lesion into cap and strangulates lesion Snare is closed and suction is released then cut tissue Cap is used to aspirate the resected lesion Inoue Gastrointest Endosc 1993;39:5 Tada Gastrointest Endosc 1996;44:6
89 Band-Ligation Technique Standard E.V.L. device or Duette Deploy rubber band around lesion Hexagon-type snare Suzuki et al. GE 1999;49:192- Ell et al. Gastro 2000;119:670-
90 EMR-Ligation vs. EMR-Cap: Early Esophageal CA 100 endoscopic resections (72 patients) 50 EMR-L (w/o SM lift) 50 EMR-C (w/ SM lift: diluted epinephrine and saline) Specimen (max. dia. / mm) (max. area / mm 2 ) EMR-L 16.4 x EMR-C 15.5 x Site at 24 hr EMR-L 20.6 x EMR-C 18.9 x Failure rate: 1/50 (2%) EMR-L (due to scarring from prior procedures) 6/50 (12%) EMR-C (technical difficulties) May Gastrointest Endosc 2003;57
91 Short Segment Barrett s and Esophageal Cancer hort segment BE ith TisN0 mass 1 month after EMR Surveillance at 6 years
92 Endoscopic Therapy for Early Cancers in BE: Mayo Clinic Experience Surgery EMR/PDT (n=64) (n=24) Sex (M/F) 58 / 6 21 / 3 Age (mean±se) 67 ± 1 68 ± 2 BE length (cm±se) 6.5 ± ±.8 Follow up (mo.±se) 19 ± 3 12 ± 2 Pacifico Clin Gastroenterol 200
93 Endoscopic Therapy for Early Cancers in BE: Mayo Clinic Experience Surgery EMR/PDT (n=64) (%) (n=24) (%) Photosensitivity 0 2 (8) Strictures 10 (16) 2 (8) Anastomotic leak 5 (8) 0 Wound infections 5 (8) 0 Dumping syndrome 3 (5) 0 Other* 8 (13) 0 Empyema, blood transfusions, atrial fib., aspiration, chylothorax)
94 Endoscopic Therapy for Early Cancers in BE: Mayo Clinic Experience Surgery EMR/PDT (n=64) (%) (n=24) (%) Death due to therapy 1 0 Unrelated death 1 2 Failed therapy 0 4* - Ca on 1st F/U Bx 1 - surgery 1 - CRT 2 - died
95 Ablation Risks All methods Failure to continue surveillance Remember squamous overgrowth occurs in treatment naïve patients
96 Endoscopic Mucosal Resection Provides pathological specimen Margins Peripheral and deep Tumor grade Lymphatic and vascular involvement Immediate effect Most complications readily apparent Well tolerated
97 EGJ Cancer Staging with EMR Thick proximal gastric fold Submucosal saline injection Cap-fitted EMR site
98 EMR Specimen of EGJ Adenocarcinoma Polypoid specimen with invasive cancer into the deep submucosal layer
99 Barrett s and Esophageal Cancer 100 patients 36.7 month mean follow up Ell Gastrointest Endosc 20
100 Squamous Cell Cancer Esophagus EMR 5-year survival data for early lesions 84 vs. 77% Shimizu Gastrointest Endosc 2002;56
101 Late Failures Long term follow up imperative Direct surveillance yourself Treat recurrences aggressively
102
103
104
105
106
107 Conclusions Endoscopic therapy is effective for dysplasia and some early cancers Well and moderately differentiated cancer Limited to the mucosal layer Mucosectomy provides accurate pathologic staging and therapy in some cases Ablation is appropriate for treating large areas of highgrade dysplasia Surgical resection provides the only durable cure Endoscopic therapy requires intense life-long surveillance
Evolution of Barrett s esophagus
 Endoscopic Treatment and Surveillance of Esophageal Cancer: GI Perspective Charles J. Lightdale, MD Columbia University New York, NY Evolution of Barrett s esophagus Squamous esophagus Chronic inflammation
Endoscopic Treatment and Surveillance of Esophageal Cancer: GI Perspective Charles J. Lightdale, MD Columbia University New York, NY Evolution of Barrett s esophagus Squamous esophagus Chronic inflammation
Learning Luncheon 7: Endoscopic Mucosal Resection: When, Where and How?
 Endoscopic Mucosal Resection (EMR): When, Where, and Charles J. Lightdale, MD Columbia University New York, NY Endoscopic Mucosal Resection (EMR) EMR developed for removal of sessile or flat neoplasms
Endoscopic Mucosal Resection (EMR): When, Where, and Charles J. Lightdale, MD Columbia University New York, NY Endoscopic Mucosal Resection (EMR) EMR developed for removal of sessile or flat neoplasms
Cancer of the Cardia/GE Junction: Surgical Options
 Cancer of the Cardia/GE Junction: Surgical Options Michael A Smith, MD Associate Chief Thoracic Surgery Center for Thoracic Disease St Joseph s Hospital and Medical Center Phoenix, AZ Michael Smith, MD
Cancer of the Cardia/GE Junction: Surgical Options Michael A Smith, MD Associate Chief Thoracic Surgery Center for Thoracic Disease St Joseph s Hospital and Medical Center Phoenix, AZ Michael Smith, MD
What is Barrett s esophagus? How does Barrett s esophagus develop?
 Barrett s Esophagus What is Barrett s esophagus? Barrett s esophagus is a pre-cancerous condition affecting the lining of the esophagus, the swallowing tube that carries foods and liquids from the mouth
Barrett s Esophagus What is Barrett s esophagus? Barrett s esophagus is a pre-cancerous condition affecting the lining of the esophagus, the swallowing tube that carries foods and liquids from the mouth
Endoscopic Resection for Barrett s Esophagus and Early Cancer 2014 Masters of Minimally Invasive Surgery
 Endoscopic Resection for Barrett s Esophagus and Early Cancer 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation: Patient ER 51 y/o man with schizophrenia
Endoscopic Resection for Barrett s Esophagus and Early Cancer 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation: Patient ER 51 y/o man with schizophrenia
EMR Can anyone do this?
 EMR Can anyone do this? Norio Fukami, MD University of Colorado Piecemeal resection? 1 Endoscopic mucosal resection (EMR) and Endoscopic submucosal dissection (ESD) Endoscopic removal of premalignant or
EMR Can anyone do this? Norio Fukami, MD University of Colorado Piecemeal resection? 1 Endoscopic mucosal resection (EMR) and Endoscopic submucosal dissection (ESD) Endoscopic removal of premalignant or
These parameters cannot, at the present time, be determined by non-invasive imaging techniques.
 Endoscopic Mucosal Resection for Upper Gastrointestinal Lesions Kenneth K. Wang, M.D. Chairman, WEO Publication and Guidelines Committee Professor of Medicine, Mayo Clinic Rochester, Minnesota Upper gastrointestinal
Endoscopic Mucosal Resection for Upper Gastrointestinal Lesions Kenneth K. Wang, M.D. Chairman, WEO Publication and Guidelines Committee Professor of Medicine, Mayo Clinic Rochester, Minnesota Upper gastrointestinal
Endotherapy for high grade dysplasia & early oesophageal neoplasia in Barrett s oesophagus: A single centre retrospective audit
 Endotherapy for high grade dysplasia & early oesophageal neoplasia in Barrett s oesophagus: A single centre retrospective audit U Duffy, K Gowland, AI Morris, HL Smart Department of Gastroenterology, Royal
Endotherapy for high grade dysplasia & early oesophageal neoplasia in Barrett s oesophagus: A single centre retrospective audit U Duffy, K Gowland, AI Morris, HL Smart Department of Gastroenterology, Royal
Horizon Scanning in Surgery: Application to Surgical Education and Practice
 Horizon Scanning in Surgery: Application to Surgical Education and Practice Cryotherapy for Esophageal Cancer May 2012 American College of Surgeons Division of Education Prepared by the Australian Safety
Horizon Scanning in Surgery: Application to Surgical Education and Practice Cryotherapy for Esophageal Cancer May 2012 American College of Surgeons Division of Education Prepared by the Australian Safety
Endoscopic Therapy for Early Esophageal Cancer: EMR and ESD
 Endoscopic Therapy for Early Esophageal Cancer: EMR and ESD AATS Toronto April 26, 2014 Lorenzo Ferri MD PhD David S. Mulder Chair in Surgery Associate Professor of Surgery and Oncology Disclosures Olympus
Endoscopic Therapy for Early Esophageal Cancer: EMR and ESD AATS Toronto April 26, 2014 Lorenzo Ferri MD PhD David S. Mulder Chair in Surgery Associate Professor of Surgery and Oncology Disclosures Olympus
Use of stents in esophageal cancer" Hans Gerdes, M.D. Director, GI Endoscopy Unit Memorial Sloan-Kettering Cancer Center
 Use of stents in esophageal cancer" Hans Gerdes, M.D. Director, GI Endoscopy Unit Memorial Sloan-Kettering Cancer Center Features of esophageal cancer Esophageal cancer is an abnormal growth that arises
Use of stents in esophageal cancer" Hans Gerdes, M.D. Director, GI Endoscopy Unit Memorial Sloan-Kettering Cancer Center Features of esophageal cancer Esophageal cancer is an abnormal growth that arises
Photodynamic Therapy for the Treatment of Barrett s Esophagus: A Systematic Review and Economic Evaluation
 Health Technology & Policy Series; 29:1 Photodynamic Therapy for the Treatment of Barrett s Esophagus: A Systematic Review and Economic Evaluation FINAL REPORT August 29 Submitted to: The Alberta Health
Health Technology & Policy Series; 29:1 Photodynamic Therapy for the Treatment of Barrett s Esophagus: A Systematic Review and Economic Evaluation FINAL REPORT August 29 Submitted to: The Alberta Health
HOW I DO IT Endoscopic mucosal resection (EMR) in the esophagus
 in the esophagus") HOW I DO IT (EMR) in the esophagus AUTHORSHIP How I do it: Horst Neuhaus, MD Department of Internal Medicine Evangelisches Krankenhaus Düsseldorf Germany Comment Hiroyasu Makuuchi, MD Professor and Chairman
HOW I DO IT (EMR) in the esophagus AUTHORSHIP How I do it: Horst Neuhaus, MD Department of Internal Medicine Evangelisches Krankenhaus Düsseldorf Germany Comment Hiroyasu Makuuchi, MD Professor and Chairman
Endoscopic treatment of Common Esophageal disorders
 Endoscopic treatment of Common Esophageal disorders November 7, 2015 Shivangi T. Kothari, MD Assistant Professor, Medicine Associate Director of Endoscopy Co-Director Developmental Endoscopy Lab at UR
Endoscopic treatment of Common Esophageal disorders November 7, 2015 Shivangi T. Kothari, MD Assistant Professor, Medicine Associate Director of Endoscopy Co-Director Developmental Endoscopy Lab at UR
How to report Upper GI EMR/ESD specimens
 Section of Pathology and Tumour Biology How to report Upper GI EMR/ESD specimens Dr.H.Grabsch Warning. Most of the criteria, methodologies, evidence presented in this talk are based on studies in early
Section of Pathology and Tumour Biology How to report Upper GI EMR/ESD specimens Dr.H.Grabsch Warning. Most of the criteria, methodologies, evidence presented in this talk are based on studies in early
Gastroesophageal Reflux Disease (GERD) and Barrett s Esophagus (BE)
 and Barrett s Esophagus (BE)") Gastroesophageal Reflux Disease (GERD) and Barrett s Esophagus (BE) Hashem El-Serag, M.D., M.P.H. Dan L. Duncan Professor of Medicine Chief, Gastroenterology and Hepatology Baylor College of Medicine Houston,
Gastroesophageal Reflux Disease (GERD) and Barrett s Esophagus (BE) Hashem El-Serag, M.D., M.P.H. Dan L. Duncan Professor of Medicine Chief, Gastroenterology and Hepatology Baylor College of Medicine Houston,
This is a prospective study that analyzed the factors associated with cancer progression after
 Sample Peer-Review of a Fictitious Manuscript Reviewer A s Comments to Authors: This is a prospective study that analyzed the factors associated with cancer progression after EMR of Barrett s esophagus
Sample Peer-Review of a Fictitious Manuscript Reviewer A s Comments to Authors: This is a prospective study that analyzed the factors associated with cancer progression after EMR of Barrett s esophagus
National Digestive Diseases Information Clearinghouse
 Barrett s Esophagus National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is Barrett s esophagus? Barrett s esophagus is
Barrett s Esophagus National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is Barrett s esophagus? Barrett s esophagus is
Captivator EMR Device
 Device Clinical Article and Abstract Summary Endoscopic Mucosal Bergman et al: EMR Training Tips Bergman et al: EMR Learning Curve ASGE: EMR & ESD Guidelines Bergman et al: Captivator EMR vs Cook Duette
Device Clinical Article and Abstract Summary Endoscopic Mucosal Bergman et al: EMR Training Tips Bergman et al: EMR Learning Curve ASGE: EMR & ESD Guidelines Bergman et al: Captivator EMR vs Cook Duette
Gastrointestinal Bleeding
 Gastrointestinal Bleeding Introduction Gastrointestinal bleeding is a symptom of many diseases rather than a disease itself. A number of different conditions can cause gastrointestinal bleeding. Some causes
Gastrointestinal Bleeding Introduction Gastrointestinal bleeding is a symptom of many diseases rather than a disease itself. A number of different conditions can cause gastrointestinal bleeding. Some causes
Endoscopic Submucosal Dissection (E.S.D.) vs. Endoscopic Mucosal Resection (E.M.R.) in Colombia. Advocating E.M.R.
 vs. Endoscopic Mucosal Resection (E.M.R.) in Colombia. Advocating E.M.R.") Controversies in Gastroenterology Endoscopic Submucosal Dissection (E.S.D.) vs. Endoscopic Mucosal Resection (E.M.R.) in Colombia. Advocating E.M.R. Raúl Cañadas Garrido, MD. 1 1 Internist-Gastroenterologist.
Controversies in Gastroenterology Endoscopic Submucosal Dissection (E.S.D.) vs. Endoscopic Mucosal Resection (E.M.R.) in Colombia. Advocating E.M.R. Raúl Cañadas Garrido, MD. 1 1 Internist-Gastroenterologist.
Post-DDW OAG Course - Therapeutic Endoscopy
 Post-DDW OAG Course - Therapeutic Endoscopy June 13, 2015 Jeffrey Mosko Division of Gastroenterology St. Michael's Hospital University of Toronto [email protected] Program Name: Post-DDW OAG course CanMEDS
Post-DDW OAG Course - Therapeutic Endoscopy June 13, 2015 Jeffrey Mosko Division of Gastroenterology St. Michael's Hospital University of Toronto [email protected] Program Name: Post-DDW OAG course CanMEDS
Endoscopic eradication of Barrett s esophagus
 TECHNICAL REVIEW Endoscopic eradication of Barrett s esophagus Sachin Wani, MD, Hari Sayana, MD, Prateek Sharma, MD Kansas City, Missouri, USA Barrett s esophagus (BE) is the premalignant lesion of esophageal
TECHNICAL REVIEW Endoscopic eradication of Barrett s esophagus Sachin Wani, MD, Hari Sayana, MD, Prateek Sharma, MD Kansas City, Missouri, USA Barrett s esophagus (BE) is the premalignant lesion of esophageal
Billing Guideline. Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/2012 Last Update Effective: 4/16
 Effective Date: 1/1/2012 Last Update Effective: 4/16") Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/2012 Last Update Effective: 4/16 Billing Guideline Background Health First administers benefit packages with full coverage
Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/2012 Last Update Effective: 4/16 Billing Guideline Background Health First administers benefit packages with full coverage
Cancer is the leading cause of death for Canadians aged 35 to 64 and is also the leading cause of critical illness claims in Canada.
 Underwriting cancer In this issue of the Decision, we provide an overview of Canadian cancer statistics and the information we use to make an underwriting decision. The next few issues will deal with specific
Underwriting cancer In this issue of the Decision, we provide an overview of Canadian cancer statistics and the information we use to make an underwriting decision. The next few issues will deal with specific
Barrett s oesophagus: specimen handling and reporting
 Barrett s oesophagus: specimen handling and reporting Professor Neil A Shepherd Gloucester and Cheltenham, UK The role of the pathologist in Barrett s oesophagus 1. Diagnosis 2. Typing 3. Assessing response
Barrett s oesophagus: specimen handling and reporting Professor Neil A Shepherd Gloucester and Cheltenham, UK The role of the pathologist in Barrett s oesophagus 1. Diagnosis 2. Typing 3. Assessing response
The digestive system. Medicine and technology. Normal structure and function Diagnostic methods Example diseases and therapies
 The digestive system Medicine and technology Normal structure and function Diagnostic methods Example diseases and therapies The digestive system An overview (1) Oesophagus Liver (hepar) Biliary system
The digestive system Medicine and technology Normal structure and function Diagnostic methods Example diseases and therapies The digestive system An overview (1) Oesophagus Liver (hepar) Biliary system
POEM Procedure for. Esophageal Achalasia
 POEM Procedure for Esophageal Achalasia POEM (Per-Oral endoscopic myotomy) is an incisionless procedure to treat esophageal achalasia, totally performed by endoscopy, without cutting the surface of the
POEM Procedure for Esophageal Achalasia POEM (Per-Oral endoscopic myotomy) is an incisionless procedure to treat esophageal achalasia, totally performed by endoscopy, without cutting the surface of the
11/10/2014. I have nothing to Disclose. Covered Stents discussed are NOT FDA approved for the indications covered in my presentation
 I have nothing to Disclose Ramsey Dallal, MD, FACS Vice Chair Department of Surgery Chief Bariatric i and Minimally i Invasive Surgery Einstein Healthcare Network Nemacolin, PA 2014 Covered Stents discussed
I have nothing to Disclose Ramsey Dallal, MD, FACS Vice Chair Department of Surgery Chief Bariatric i and Minimally i Invasive Surgery Einstein Healthcare Network Nemacolin, PA 2014 Covered Stents discussed
ORIGINAL ARTICLE: Clinical Endoscopy
 ORIGINAL ARTICLE: Clinical Endoscopy Endotherapy for superficial adenocarcinoma of the esophagus: an American experience Shreyas Saligram, MD, MRCP, 1 Jennifer Chennat, MD, 1 Huankai Hu, MD, 2 Jon M. Davison,
ORIGINAL ARTICLE: Clinical Endoscopy Endotherapy for superficial adenocarcinoma of the esophagus: an American experience Shreyas Saligram, MD, MRCP, 1 Jennifer Chennat, MD, 1 Huankai Hu, MD, 2 Jon M. Davison,
Cancer Screening and Early Detection Guidelines
 Cancer Screening and Early Detection Guidelines Guillermo Tortolero Luna, MD, PhD Director Cancer Control and Population Sciences Program University of Puerto Rico Comprehensive Cancer Center ASPPR Clinical
Cancer Screening and Early Detection Guidelines Guillermo Tortolero Luna, MD, PhD Director Cancer Control and Population Sciences Program University of Puerto Rico Comprehensive Cancer Center ASPPR Clinical
Acute Abdominal Pain following Bariatric Surgery. Disclosure. Objectives 8/17/2015. I have nothing to disclose
 Acute Abdominal Pain following Bariatric Surgery Kathy J. Morris, DNP, APRN, FNP C, FAANP University of Nebraska Medical Center College of Nursing Disclosure I have nothing to disclose Objectives Pathophysiology
Acute Abdominal Pain following Bariatric Surgery Kathy J. Morris, DNP, APRN, FNP C, FAANP University of Nebraska Medical Center College of Nursing Disclosure I have nothing to disclose Objectives Pathophysiology
CPT COD1NG UPDATES Gastroenterology CPT Advisors
 2014 CPT COD1NG UPDATES Gastroenterology CPT Advisors Joel V. Brill, MD, AGA CPT Advisor Daniel C. DeMarco, MD, ACG CPT Advisor Glenn D. Littenberg, MD, ASGE CPT Advisor The American College of Gastroenterology
2014 CPT COD1NG UPDATES Gastroenterology CPT Advisors Joel V. Brill, MD, AGA CPT Advisor Daniel C. DeMarco, MD, ACG CPT Advisor Glenn D. Littenberg, MD, ASGE CPT Advisor The American College of Gastroenterology
Core curriculum for EMR and ablative techniques
 Communication from the ASGE Training Committee CORE CURRICULUM Core curriculum for EMR and ablative techniques This document was prepared by the American Society for Gastrointestinal Endoscopy (ASGE) Training
Communication from the ASGE Training Committee CORE CURRICULUM Core curriculum for EMR and ablative techniques This document was prepared by the American Society for Gastrointestinal Endoscopy (ASGE) Training
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 PRACTICE GUIDELINES nature publishing group 1 ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nichol as J. Sha he e n, M D, M PH, FAC G 1, Gary W. Falk, MD, MS, FACG 2, Prasad G.
PRACTICE GUIDELINES nature publishing group 1 ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nichol as J. Sha he e n, M D, M PH, FAC G 1, Gary W. Falk, MD, MS, FACG 2, Prasad G.
Safety of Endoscopic Mucosal Resection for Barrett s Esophagus
 1440 ORIGINAL CONTRIBUTIONS nature publishing group see CMErelated editorial on page x Safety of Endoscopic Mucosal Resection for Barrett s Esophagus Yutaka Tomizawa, MD 1, Prasad G. Iyer, MD 1, Louis
1440 ORIGINAL CONTRIBUTIONS nature publishing group see CMErelated editorial on page x Safety of Endoscopic Mucosal Resection for Barrett s Esophagus Yutaka Tomizawa, MD 1, Prasad G. Iyer, MD 1, Louis
Cervical Cancer The Importance of Cervical Screening and Vaccination
 Cervical Cancer The Importance of Cervical Screening and Vaccination Cancer Cells Cancer begins in cells, the building blocks that make up tissues. Tissues make up the organs of the body. Sometimes, this
Cervical Cancer The Importance of Cervical Screening and Vaccination Cancer Cells Cancer begins in cells, the building blocks that make up tissues. Tissues make up the organs of the body. Sometimes, this
Esophageal cancer. Dr. med. Henrik Csaba Horváth
 Esophageal cancer Dr. med. Henrik Csaba Horváth Epidemiology 8th most common cancer worldwide Male/Female ratio: 3,5-4 Mean age at Dx 64 yrs Epidemiology in Switzerland 500-550 new cases/yr 400-450 deaths/yr
Esophageal cancer Dr. med. Henrik Csaba Horváth Epidemiology 8th most common cancer worldwide Male/Female ratio: 3,5-4 Mean age at Dx 64 yrs Epidemiology in Switzerland 500-550 new cases/yr 400-450 deaths/yr
Chapter I Overview Chapter Contents
 Chapter I Overview Chapter Contents Table Number Contents I-1 Estimated New Cancer Cases and Deaths for 2005 I-2 53-Year Trends in US Cancer Death Rates I-3 Summary of Changes in Cancer Incidence and Mortality
Chapter I Overview Chapter Contents Table Number Contents I-1 Estimated New Cancer Cases and Deaths for 2005 I-2 53-Year Trends in US Cancer Death Rates I-3 Summary of Changes in Cancer Incidence and Mortality
PATIENT CONSENT TO PROCEDURE - ROUX-EN-Y GASTRIC BYPASS
 As a patient you must be adequately informed about your condition and the recommended surgical procedure. Please read this document carefully and ask about anything you do not understand. Please initial
As a patient you must be adequately informed about your condition and the recommended surgical procedure. Please read this document carefully and ask about anything you do not understand. Please initial
A PATIENT S GUIDE TO ABLATION THERAPY
 A PATIENT S GUIDE TO ABLATION THERAPY THE DIVISION OF VASCULAR/INTERVENTIONAL RADIOLOGY THE ROBERT WOOD JOHNSON UNIVERSITY HOSPITAL Treatment options for patients with cancer continue to expand, providing
A PATIENT S GUIDE TO ABLATION THERAPY THE DIVISION OF VASCULAR/INTERVENTIONAL RADIOLOGY THE ROBERT WOOD JOHNSON UNIVERSITY HOSPITAL Treatment options for patients with cancer continue to expand, providing
2016 Quick Reference Coding Chart
 43197 Trans nasal esophagoscopy 43198 Biospy Trans Nasal Esophagoscopy Esophagoscopy 43200 Esophagoscopy Includes collection of specimen(s) by brushing or washing, when performed. 43201 Submucosal injection
43197 Trans nasal esophagoscopy 43198 Biospy Trans Nasal Esophagoscopy Esophagoscopy 43200 Esophagoscopy Includes collection of specimen(s) by brushing or washing, when performed. 43201 Submucosal injection
Medical Nutrition Therapy for Upper Gastrointestinal Tract Disorders. By: Jalal Hejazi PhD, MSc.
 Medical Nutrition Therapy for Upper Gastrointestinal Tract Disorders By: Jalal Hejazi PhD, MSc. Digestive Disorders Common problem; more than 50 million outpatient visits per year Dietary habits and nutrition
Medical Nutrition Therapy for Upper Gastrointestinal Tract Disorders By: Jalal Hejazi PhD, MSc. Digestive Disorders Common problem; more than 50 million outpatient visits per year Dietary habits and nutrition
Center for Endoscopic Research & Therapeutics
 Center for Endoscopic Research & Therapeutics 5758 South Maryland Avenue (MC9028) Chicago, Illinois 60637 (773) 702-1459 www.uchospitals.edu Center for Endoscopic Research & Therapeutics To refer a patient
Center for Endoscopic Research & Therapeutics 5758 South Maryland Avenue (MC9028) Chicago, Illinois 60637 (773) 702-1459 www.uchospitals.edu Center for Endoscopic Research & Therapeutics To refer a patient
Endoscopic therapy for obesity and complications of bariatric surgery
 Endoscopic therapy for obesity and complications of bariatric surgery Jacques Devière, MD, PhD Erasme University Hospital Brussels Belgium [email protected] Obesity Affects 300 millions
Endoscopic therapy for obesity and complications of bariatric surgery Jacques Devière, MD, PhD Erasme University Hospital Brussels Belgium [email protected] Obesity Affects 300 millions
Endoscopic mucosal resection for treatment of early gastric cancer
 Gut 2001;48:225 229 225 Endoscopic mucosal resection for treatment of early gastric cancer H Ono, H Kondo, T Gotoda, K Shirao, H Yamaguchi, D Saito, K Hosokawa, T Shimoda, S Yoshida Department of Endoscopy
Gut 2001;48:225 229 225 Endoscopic mucosal resection for treatment of early gastric cancer H Ono, H Kondo, T Gotoda, K Shirao, H Yamaguchi, D Saito, K Hosokawa, T Shimoda, S Yoshida Department of Endoscopy
FAQ About Prostate Cancer Treatment and SpaceOAR System
 FAQ About Prostate Cancer Treatment and SpaceOAR System P. 4 Prostate Cancer Background SpaceOAR Frequently Asked Questions (FAQ) 1. What is prostate cancer? The vast majority of prostate cancers develop
FAQ About Prostate Cancer Treatment and SpaceOAR System P. 4 Prostate Cancer Background SpaceOAR Frequently Asked Questions (FAQ) 1. What is prostate cancer? The vast majority of prostate cancers develop
PSA Screening for Prostate Cancer Information for Care Providers
 All men should know they are having a PSA test and be informed of the implications prior to testing. This booklet was created to help primary care providers offer men information about the risks and benefits
All men should know they are having a PSA test and be informed of the implications prior to testing. This booklet was created to help primary care providers offer men information about the risks and benefits
HER2 Status: What is the Difference Between Breast and Gastric Cancer?
 Ask the Experts HER2 Status: What is the Difference Between Breast and Gastric Cancer? Bharat Jasani MBChB, PhD, FRCPath Marco Novelli MBChB, PhD, FRCPath Josef Rüschoff, MD Robert Y. Osamura, MD, FIAC
Ask the Experts HER2 Status: What is the Difference Between Breast and Gastric Cancer? Bharat Jasani MBChB, PhD, FRCPath Marco Novelli MBChB, PhD, FRCPath Josef Rüschoff, MD Robert Y. Osamura, MD, FIAC
Surgery for oesophageal cancer
 Surgery for oesophageal cancer This information is an extract from the booklet Understanding oesophageal cancer (cancer of the gullet). You may find the full booklet helpful. We can send you a free copy
Surgery for oesophageal cancer This information is an extract from the booklet Understanding oesophageal cancer (cancer of the gullet). You may find the full booklet helpful. We can send you a free copy
ERBEJET 2. The versatility of waterjet surgery: ERBEJET 2 with hybrid instruments WATERJET SURGERY
 ERBEJET 2 The versatility of waterjet surgery: ERBEJET 2 with hybrid instruments WATERJET SURGERY Gentle interventions in surgery and endoscopy Waterjet surgery with hybrid technology Waterjet surgery
ERBEJET 2 The versatility of waterjet surgery: ERBEJET 2 with hybrid instruments WATERJET SURGERY Gentle interventions in surgery and endoscopy Waterjet surgery with hybrid technology Waterjet surgery
Lung Cancer: More than meets the eye
 Lung Cancer Education Program November 23, 2013 Lung Cancer: More than meets the eye Shantanu Banerji MD, FRCPC Presenter Disclosure Faculty: Shantanu Banerji Relationships with commercial interests: Grants/Research
Lung Cancer Education Program November 23, 2013 Lung Cancer: More than meets the eye Shantanu Banerji MD, FRCPC Presenter Disclosure Faculty: Shantanu Banerji Relationships with commercial interests: Grants/Research
GASTROESOPHAGEAL REFLUX DISEASE (GERD)
") GASTROESOPHAGEAL REFLUX DISEASE (GERD) Gastroesophageal reflux disease is a clinical scenario where the gastric or duodenal contents reflux back up into the esophagus. Reflux esophagitis, however, is a
GASTROESOPHAGEAL REFLUX DISEASE (GERD) Gastroesophageal reflux disease is a clinical scenario where the gastric or duodenal contents reflux back up into the esophagus. Reflux esophagitis, however, is a
Bridging Techniques. What s between EMR and Traditional Surgery? Elisabeth C. McLemore, MD, FACS, FASCRS
 Bridging Techniques What s between EMR and Traditional Surgery? Elisabeth C. McLemore, MD, FACS, FASCRS Associate Professor of Surgery Assistant Program Director, General Surgery Residency Disclosures
Bridging Techniques What s between EMR and Traditional Surgery? Elisabeth C. McLemore, MD, FACS, FASCRS Associate Professor of Surgery Assistant Program Director, General Surgery Residency Disclosures
Figure 3: Dysphagia. 14 meets. esophageal. esophageal manometry +/- +/- impedance measurement. structural lesion? no. 19 yes
 Figure 3: Dysphagia 1 patient with dysphagia 2 history and physical exam. suggestive of nesophageal etiology? 3 evaluate and treat as as indicated 4 upper GI GI endoscopy with biopsies 15 achalasia, absent
Figure 3: Dysphagia 1 patient with dysphagia 2 history and physical exam. suggestive of nesophageal etiology? 3 evaluate and treat as as indicated 4 upper GI GI endoscopy with biopsies 15 achalasia, absent
Types of Bariatric Procedures. Tejal Brahmbhatt, MD General Surgery Teaching Conference April 18, 2012
 Types of Bariatric Procedures Tejal Brahmbhatt, MD General Surgery Teaching Conference April 18, 2012 A Brief History of Bariatric Surgery First seen in pts with short bowel syndrome weight loss First
Types of Bariatric Procedures Tejal Brahmbhatt, MD General Surgery Teaching Conference April 18, 2012 A Brief History of Bariatric Surgery First seen in pts with short bowel syndrome weight loss First
Endoscopic Management of Barrett s High-Grade Dysplasia and Early Stage Esophageal Cancer
 VOLUME 10, ISSUE 2, YEAR 2011 Endoscopic Management of Barrett s High-Grade Dysplasia and Early Stage Esophageal Cancer James L. Wise, MD Duluth, MN. Introduction: In recent years there has been intense
VOLUME 10, ISSUE 2, YEAR 2011 Endoscopic Management of Barrett s High-Grade Dysplasia and Early Stage Esophageal Cancer James L. Wise, MD Duluth, MN. Introduction: In recent years there has been intense
Figure 2: Recurrent chest pain of suspected esophageal origin
 Figure 2: Recurrent chest pain of suspected esophageal origin 1 patient with chest pain of suspected esophageal origin 2 history and physical exam. suggestive of n-esophageal etiology? 3 evaluate and treat
Figure 2: Recurrent chest pain of suspected esophageal origin 1 patient with chest pain of suspected esophageal origin 2 history and physical exam. suggestive of n-esophageal etiology? 3 evaluate and treat
Science Highlights. To PSA or not to PSA: That is the Question.
 Science Highlights June 2012 by Ann A. Kiessling, PhD at the To PSA or not to PSA: That is the Question. The current raucous debate over the commonly used PSA blood test to screen for prostate cancer,
Science Highlights June 2012 by Ann A. Kiessling, PhD at the To PSA or not to PSA: That is the Question. The current raucous debate over the commonly used PSA blood test to screen for prostate cancer,
Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy. Patient Name
 Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy Patient Name Please read this form carefully and ask about anything you may not understand. I consent to have a laparoscopic Vertical Sleeve
Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy Patient Name Please read this form carefully and ask about anything you may not understand. I consent to have a laparoscopic Vertical Sleeve
How to Effectively Code for Endoscopic Procedures in Gastroenterology
 How to Effectively Code for Endoscopic Procedures in Gastroenterology Ariwan Rakvit, MD Associate Professor Interim Chief, Division of Gastroenterology Texas Tech University Health Science Center All rights
How to Effectively Code for Endoscopic Procedures in Gastroenterology Ariwan Rakvit, MD Associate Professor Interim Chief, Division of Gastroenterology Texas Tech University Health Science Center All rights
C a nc e r C e nter. Annual Registry Report
 C a nc e r C e nter Annual Registry Report 214 214 Cancer Registry Report Larraine A. Tooker, CTR Please note that the 214 Cancer Registry Annual Report is created in 214, but it reflects data on cases
C a nc e r C e nter Annual Registry Report 214 214 Cancer Registry Report Larraine A. Tooker, CTR Please note that the 214 Cancer Registry Annual Report is created in 214, but it reflects data on cases
Esophageal Cancer. Understanding your diagnosis
 Esophageal Cancer Understanding your diagnosis Esophageal Cancer Understanding your diagnosis When you first hear that you have cancer, you may feel alone and afraid. You may be overwhelmed by the large
Esophageal Cancer Understanding your diagnosis Esophageal Cancer Understanding your diagnosis When you first hear that you have cancer, you may feel alone and afraid. You may be overwhelmed by the large
Cryosurgery in Cancer Treatment: Questions and Answers. Key Points
 CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Cryosurgery in Cancer
CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Cryosurgery in Cancer
Radiation Therapy for Prostate Cancer
 Radiation Therapy for Prostate Cancer Introduction Cancer of the prostate is the most common form of cancer that affects men. About 240,000 American men are diagnosed with prostate cancer every year. Your
Radiation Therapy for Prostate Cancer Introduction Cancer of the prostate is the most common form of cancer that affects men. About 240,000 American men are diagnosed with prostate cancer every year. Your
ESD for colorectal lesions I am in favour. Alessandro Repici, MD Digestive Endoscopy Unit IRCCS Istituto Clinico Humanitas Milano, Italy
 ESD for colorectal lesions I am in favour Alessandro Repici, MD Digestive Endoscopy Unit IRCCS Istituto Clinico Humanitas Milano, Italy Surgery for early colonic lesions 51 pts referred for lap colectomy
ESD for colorectal lesions I am in favour Alessandro Repici, MD Digestive Endoscopy Unit IRCCS Istituto Clinico Humanitas Milano, Italy Surgery for early colonic lesions 51 pts referred for lap colectomy
Early Prostate Cancer: Questions and Answers. Key Points
 CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Early Prostate Cancer:
CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Early Prostate Cancer:
Overview of Bariatric Surgery
 Overview of Bariatric Surgery To better understand how weight loss surgery works, it is helpful to know how the normal digestive process works. As food moves along the digestive tract, special digestive
Overview of Bariatric Surgery To better understand how weight loss surgery works, it is helpful to know how the normal digestive process works. As food moves along the digestive tract, special digestive
How to treat early gastric cancer. Surgery
 How to treat early gastric cancer Surgery Mark I. van Berge Henegouwen Department of Surgery, AMC, Amsterdam Director upper GI surgical unit Academic Medical Center Upper GI surgery at AMC 100 oesophagectomies
How to treat early gastric cancer Surgery Mark I. van Berge Henegouwen Department of Surgery, AMC, Amsterdam Director upper GI surgical unit Academic Medical Center Upper GI surgery at AMC 100 oesophagectomies
SAGES 2015 Flexible Endoscopy Course for Fellows
 Goals and Objectives: At the end of the course, the MIS fellow will be familiar with GI endoscopes, towers, and the instruments used for endoscopy and endoscopic surgery. The fellow will also be able to
Goals and Objectives: At the end of the course, the MIS fellow will be familiar with GI endoscopes, towers, and the instruments used for endoscopy and endoscopic surgery. The fellow will also be able to
Number. Source: Vital Records, M CDPH
 Epidemiology of Cancer in Department of Public Health Revised April 212 Introduction The general public is very concerned about cancer in the community. Many residents believe that cancer rates are high
Epidemiology of Cancer in Department of Public Health Revised April 212 Introduction The general public is very concerned about cancer in the community. Many residents believe that cancer rates are high
Endoscopy and infection: Prevention of infection during endoscopy Treatment of infection by endoscopy. M. Arvanitakis SRBG June 2009
 Endoscopy and infection: Prevention of infection during endoscopy Treatment of infection by endoscopy M. Arvanitakis SRBG June 2009 Outline Antibiotic prophylaxis during endoscopy Upper GI endoscopy Lower
Endoscopy and infection: Prevention of infection during endoscopy Treatment of infection by endoscopy M. Arvanitakis SRBG June 2009 Outline Antibiotic prophylaxis during endoscopy Upper GI endoscopy Lower
Investigating Community Cancer Concerns--Deer Park Community Advisory Council, 2008
 Investigating Community Cancer Concerns--Deer Park Community Advisory Council, 2008 David R. Risser, M.P.H., Ph.D. [email protected] Epidemiologist Cancer Epidemiology and Surveillance Branch
Investigating Community Cancer Concerns--Deer Park Community Advisory Council, 2008 David R. Risser, M.P.H., Ph.D. [email protected] Epidemiologist Cancer Epidemiology and Surveillance Branch
Colonoscopy Data Collection Form
 Identifier: Sociodemographic Information Type: Zip Code: Gender: Height: (inches) Race: Ethnicity Inpatient Outpatient Male Female Birth Date: Weight: (pounds) American Indian (Native American) or Alaska
Identifier: Sociodemographic Information Type: Zip Code: Gender: Height: (inches) Race: Ethnicity Inpatient Outpatient Male Female Birth Date: Weight: (pounds) American Indian (Native American) or Alaska
Challenges in gastric, appendiceal and rectal NETs Leuven, 29.11.2014
 Challenges in gastric, appendiceal and rectal NETs Leuven, 29.11.2014 Prof. Dr. Chris Verslype, Leuven Prof. Dr. Aurel Perren, Bern Menue Challenges: 1. Gastric NET 2. Appendiceal NET 3. Rectal NET SEER,
Challenges in gastric, appendiceal and rectal NETs Leuven, 29.11.2014 Prof. Dr. Chris Verslype, Leuven Prof. Dr. Aurel Perren, Bern Menue Challenges: 1. Gastric NET 2. Appendiceal NET 3. Rectal NET SEER,
Understanding. Pancreatic Cancer
 Understanding Pancreatic Cancer Understanding Pancreatic Cancer The Pancreas The pancreas is an organ that is about 6 inches long. It s located deep in your belly between your stomach and backbone. Your
Understanding Pancreatic Cancer Understanding Pancreatic Cancer The Pancreas The pancreas is an organ that is about 6 inches long. It s located deep in your belly between your stomach and backbone. Your
Endoscopic submucosal dissection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline
 Guideline") Guideline 829 Endoscopic submucosal dissection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline Authors Institutions Pedro Pimentel-Nunes 1, Mário Dinis-Ribeiro 1, Thierry Ponchon 2, Alessandro
Guideline 829 Endoscopic submucosal dissection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline Authors Institutions Pedro Pimentel-Nunes 1, Mário Dinis-Ribeiro 1, Thierry Ponchon 2, Alessandro
1400 Telegraph Bloomfield Hills, MI 48302 248-334-6877-Phone number/248-334-6877-fax Number CANCER TREATMENT
 1400 Telegraph Bloomfield Hills, MI 48302 248-334-6877-Phone number/248-334-6877-fax Number CANCER TREATMENT Learning that your pet has a diagnosis of cancer can be overwhelming. We realize that your pet
1400 Telegraph Bloomfield Hills, MI 48302 248-334-6877-Phone number/248-334-6877-fax Number CANCER TREATMENT Learning that your pet has a diagnosis of cancer can be overwhelming. We realize that your pet
Informed Consent for Laparoscopic Roux en Y Gastric Bypass. Patient Name
 Informed Consent for Laparoscopic Roux en Y Gastric Bypass Patient Name Please read this form carefully and ask about anything you may not understand. I consent to have a laparoscopic Roux en Y Gastric
Informed Consent for Laparoscopic Roux en Y Gastric Bypass Patient Name Please read this form carefully and ask about anything you may not understand. I consent to have a laparoscopic Roux en Y Gastric
Frequently Asked Questions About Ovarian Cancer
 Media Contact: Gerri Gomez Howard Cell: 303-748-3933 [email protected] Frequently Asked Questions About Ovarian Cancer What is ovarian cancer? Ovarian cancer is a cancer that forms in tissues
Media Contact: Gerri Gomez Howard Cell: 303-748-3933 [email protected] Frequently Asked Questions About Ovarian Cancer What is ovarian cancer? Ovarian cancer is a cancer that forms in tissues
Cystic Neoplasms of the Pancreas: A multidisciplinary approach to the prevention and early detection of invasive pancreatic cancer.
 This lecture is drawn from the continuing medical education program Finding Hope: Prevention, Early Detection and Treatment of Pancreatic Cancer, Nov, 2011. Robert P. Jury, MD Cystic Neoplasms of the Pancreas:
This lecture is drawn from the continuing medical education program Finding Hope: Prevention, Early Detection and Treatment of Pancreatic Cancer, Nov, 2011. Robert P. Jury, MD Cystic Neoplasms of the Pancreas:
1. What is the prostate-specific antigen (PSA) test?
 test?") 1. What is the prostate-specific antigen (PSA) test? Prostate-specific antigen (PSA) is a protein produced by the cells of the prostate gland. The PSA test measures the level of PSA in the blood. The doctor
1. What is the prostate-specific antigen (PSA) test? Prostate-specific antigen (PSA) is a protein produced by the cells of the prostate gland. The PSA test measures the level of PSA in the blood. The doctor
Esophagus Cancer. What is cancer?
 What is cancer? Esophagus Cancer The body is made up of trillions of living cells. Normal body cells grow, divide to make new cells, and die in an orderly way. During the early years of a person s life,
What is cancer? Esophagus Cancer The body is made up of trillions of living cells. Normal body cells grow, divide to make new cells, and die in an orderly way. During the early years of a person s life,
Treatment of Dysplasia in Barrett Esophagus
 FOCUSED REVIEW SERIES: Endoscopic and Molecular Imaging of Premalignant GI Lesions, Part II Clin Endosc 2014;47:55-64 Print ISSN 2234-2400 / On-line ISSN 2234-2443 http://dx.doi.org/10.5946/ce.2014.47.1.55
FOCUSED REVIEW SERIES: Endoscopic and Molecular Imaging of Premalignant GI Lesions, Part II Clin Endosc 2014;47:55-64 Print ISSN 2234-2400 / On-line ISSN 2234-2443 http://dx.doi.org/10.5946/ce.2014.47.1.55
The Need for Accurate Lung Cancer Staging
 The Need for Accurate Lung Cancer Staging Peter Baik, DO Thoracic Surgery Cancer Treatment Centers of America Oklahoma Osteopathic Association 115th Annual Convention Financial Disclosures: None 2 Objectives
The Need for Accurate Lung Cancer Staging Peter Baik, DO Thoracic Surgery Cancer Treatment Centers of America Oklahoma Osteopathic Association 115th Annual Convention Financial Disclosures: None 2 Objectives
Prostate Cancer Screening. A Decision Guide for African Americans
 Prostate Cancer Screening A Decision Guide for African Americans This booklet was developed by the U.S. Department of Health and Human Services, Centers for Disease Control and Prevention (CDC). Published
Prostate Cancer Screening A Decision Guide for African Americans This booklet was developed by the U.S. Department of Health and Human Services, Centers for Disease Control and Prevention (CDC). Published
Treatments for Barrett s Oesophagus
 Treatments for Barrett s Oesophagus Introduction This leaflet describes the various ways in which Barrett s Oesophagus is treated. It has been produced in association with Heartburn Cancer UK (HCUK), a
Treatments for Barrett s Oesophagus Introduction This leaflet describes the various ways in which Barrett s Oesophagus is treated. It has been produced in association with Heartburn Cancer UK (HCUK), a