PALS Course Outline 2011 Olton/Plainview EMT-P Courses
|
|
|
- Baldric Dickerson
- 7 years ago
- Views:
Transcription
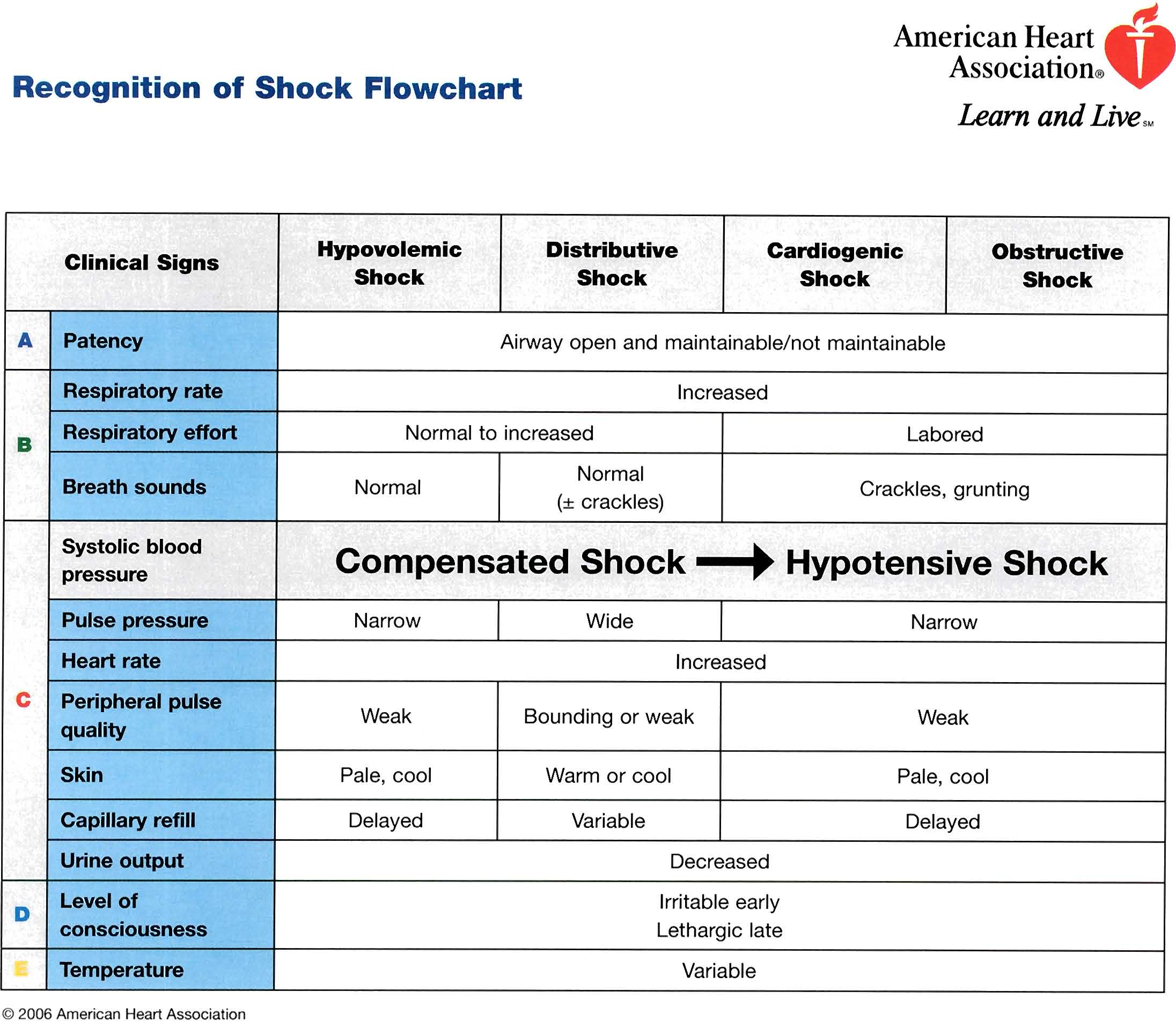
1 PALS Course Outline 2011 Olton/Plainview EMT-P Courses I. PALS Course Overview/Registration II. III. IV. PALS Science Overview Video Child/Infant CPR/AED Review Video Management of Respiratory Emergencies Video V. Review of Respiratory Emergencies Flow Charts Recognition of Respiratory Problems Flow Chart Management of Respiratory Emergencies Flow Chart VI. VII. Review of Rhythm Disturbances/Electrical Therapy Procedures Handouts Vascular Access Video VIII. Resuscitation Team Concept Video IX. Overview of Pediatric Assessment Video X. Review of Pediatric Assessment XI. XII. Review of Shock Handouts Recognition of Shock Flow Chart Management of Shock Flow Chart Review of PALS Cardiac Arrest Priorities CPR Defibrillation IV Access/Medications Advanced Airway Management XIII. Review of Rhythm Treatment Priorities Rate Rhythm Blood Pressure XIV. Review of Cardiac Treatment s AHA Pulseless Arrest SPEMS s a. VF/Pulseless V-Tach (Pediatric) b. Asystole/PEA (Pediatric) AHA Bradycardia SPEMS Pediatric Bradycardia AHA Tachycardia SPEMS s a. SVTs b. V-Tach with a Pulse XV. Putting it all Together Core Case Studies a. Respiratory Cases 1, 2, 3, 4 b. Cardiac Cases 3, 4 c. Shock Cases 1, 2, 3, 4 Pediatric Megacodes (Class) XVI. Written Exam 25 Questions Minimum Passing Grade: 84% XVII. Retesting (As Needed) 1
2 2

3 3
4 American Heart Association Learn and Live Rhythm Disturbances! Electrical Therapy Procedures 2006 American Heart Association 4
5 Procedure for Cardiac Monitoring Introduction Management of any seriously ill or injured patient requires assessment of heart rate and rhythm (cardiac monitoring). Procedure Follow these steps to perform cardiac monitoring. Modify for your specific device. Step Action 1 Power on monitor/defibrillator. 2 Attach ECG leads to patient: White lead-to right shoulder Red lead-to left flank or abdomen Ground (black, green, brown) lead-to left shoulder Note: In units with cardiovascular patients, 5-lead monitoring may be used. For 5-lead monitoring the green lead is placed under the white, lower on the torso. The brown lead is placed in the middle of the chest. Placement of electrodes for ECG monitorin. 3 Adjust device to manual ECG monitoring mode (not AED mode or paddles) to display rhythm in standard limb leads I, II, III. 4 Visually check monitor screen and assess heart rate and rhythm American Heart Association 2 5
6 Emergency Interventions for Tachyarrhythmias Introduction Specific emergency interventions for tachyarrhythmias include vagal maneuvers synchronized cardioversion Vagal Maneuvers Vagal Maneuvers In normal infants and children the heart rate falls with stimulation of the vagus nerve. In patients with supraventricular tachycardia (SVT), vagal stimulation may terminate the tachycardia. Several maneuvers stimulate vagal activity. The success rates of these maneuvers in terminating tachyarrhythmias vary, depending on the child's age, level of cooperation, and underlyill9 condition. If possible, obtain a 12-lead EGG before and after the maneuver; record and monitor the EGG continuously during the maneuver. If the patient is stable and the rhythm does not convert, you may repeat the attempt. If the second attempt fails, select another method or provide pharmacologic therapy. If the patient is unstable, attempt vagal maneuvers only while making preparations for pharmacologic or electrical cardioversion. Do not delay definitive treatment with vagal maneuvers. Maneuver Application of ice to the face Description This is the most effective vagal maneuver in infants and young children. Method One method is to mix crushed ice with water in a plastic bag or glove (Figure 1). While recording the EGG, apply the ice water mixture to the infant's face for only 10 to 15 seconds. Do not obstruct ventilation (ie, cover only the forehead, the eyes, and the bridge of the nose). If this method is successful, SVT will terminate in seconds. ( 2006 American Heart Association 3 6
7 Val salva maneuver Figure 1. Ice water is applied to the infant's face for vagal stimulation in an attempt to terminate SVT. Note that the bag of ice water does not cover the nares or mouth and does not obstruct ventilation. Other vagal maneuvers may be effective and appear to be safe, based on data obtained largely in older children, adolescents, and adults. Older children can be taught to use these maneuvers on their own. Method I nstruct the child to blow through an obstructed straw blow on his thumb as if it were a trumpet without letting any air out while blowing, bear down as if passing a bowel movement hold his breath while ice is laced to the face Do not use the following methods to induce vagal activity: Application of external ocular pressure Carotid massage 2006 American Heart Association 4 7
8 ( \ Synchronized Cardioversion Introduction Synchronized cardioversion is used for children with tachyarrhythmias (SVT, ventricular tachycardia [VT] with pulses, atrial flutter, atrial fibrillation) that are unstable (ie, associated with evidence of cardiovascular compromise, such as poor perfusion, hypotension, or heart failure) requiring immediate cardioversion by an appropriately skilled provider stable-permitting elective cardioversion at the direction of a pediatric cardiologist During synchronized cardioversion electrical therapy is administered through adhesive electrode pads or handheld paddles. You will need to place the defibrillator/monitor in synchronized (sync) mode. The sync mode is designed to deliver energy just after the R wave of the QRS complex. Technique Follow these steps to perform synchronized cardioversion. Modify for your specific device. ( Step Action 1 Consider sedation but do not delay cardioversion in an unstable patient. 2 Power on the monitor/defibrillator (monophasic or biphasic). i 3 Attach monitor leads to the child ("white to right, red to I ribs, what's left over to the left shoulder") and ensure proper display of the child's rhythm. 4 Interpret the heart rhythm. Confirm indication for I synchronized cardioversion. 5 Press the SYNC control button to engage synchronization mode. 6 Look for markers on the R wave indicating sync mode. Adjust monitor gain if necessary until sync markers occur I with each R wave. 7 Select the appropriate energy level. The initial energy dose for synchronized cardioversion is 0.5 to 1 J/kg. If tachyarrhythmia persists after the first attempt, double the dose to 1 to 2 J/kg. 8 Select the largest paddles or pads that will fit on the chest wall without touching. Prepare paddles and J 2006 American Heart Association 5 8
9 i conducting surface for placement. Place paddles/pads correctly. (See steps 2, 3, and 4 in the Procedure for Manual Defibrillation on the student CD.) 9 Announce to team members: "Charging cardioverterstand clear!" 10 Press the CHARGE button. 11 When the cardioverter is fully charged, clear the patient. To ensure the safety of cardioversion, always announce when you are about to deliver a shock (eg, "I am going to shock on three. One, I'm clear. Two, you're clear, oxygen's clear. Three, everybody's clear." Direct oxygen flow away from the patient's chest and consider temporarily disconnecting the bag or the ventilation circuit from the endotracheal tube during shock delivery. 12 Press the DISCHARGE buttons simultaneously on the paddles or the SHOCK button on the cardioverter. 13 Check the monitor to evaluate the rhythm. If the tachyarrhythmia persists, increase the energy level Goules) according to the appropriate algorithm. 14 Activate the sync mode after delivery of each synchronized shock if the patient remains in a tachycardic rhythm. Most defibrillators default back to the unsynchronized mode after delivery of a synchronized shock. This default allows an immediate shock if cardioversion produces VF American Heart Association 6 9
10 Procedure for Manual Defibrillation Introduction Defibrillation shocks are indicated for ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT). To treat VF/pulseless VT effectively, you need to know how to operate a manual defibrillator and perform manual defibrillation. Procedure Follow these steps to operate a manual monitor/defibrillator (either biphasic or monophasic) and attempt manual defibrillation. Modify for your specific device. Step Action 1 Power on monitor/defibrillator. 2 Select the proper pads or paddles. Attach adhesive electrode pads. Select largest paddles or pads that will fit on the chest wall without touching. i Weight/Age Paddle/Pad Size 10 kg Large adult paddles (8 to 13 cm) ( approximately 1 Adult pads year old) <10 kg Small infant paddles (4.5 cm) «1 year old) Pediatric pads 3 Prepare paddles/pads for rhythm identification and shock delivery. If using paddles, apply electrode cream or paste to them. Placing paddles directly on the child's bare skin decreases the delivered current. Note: Do not use saline-soaked gauze pads or sonographic gels. Do not use alcohol pads because they may pose a fire hazard and produce chest burns. If using adhesive electrode pads, peel the backing away. 4 Position paddles or pads so that the heart is between them. Place one paddle or pad on the upper right side of the chest below the clavicle, along the patient's right upper sternal border. Place the other paddle/pad lateral to the left nipple in the anterior axillary line (positioned under and to the left of the nipple and between the nipple and the axilla). Make sure paddles do not touch. Do not overlap pads American Heart Association 7 10
11 \ An alternative method is to place the paddles/pads in an anterior-posterior position with one just to the left of the sternum and the other over the back. Anterior-posterior placement may be necessary if the child is an infant and only large paddles or pads are available. In dextrocardia, position pads in a mirror image of the standard placement. Adjust device to manual mode (not AED mode). If necessary, adjust LEAD button to display rhythm in standard limb leads I, II, or III (if EGG leads are used) paddles (if paddles are used instead of pads) Interpret heart rhythm. Confirm indication for defibrillation. Adjust ENERGY button to select appropriate energy dose. An initial dose of 2 J/kg (biphasic or monophasic waveform) is recommended. If this dose does not terminate VF or pulseless VT, deliver subsequent doses of 4 J/kg. Apply firm pressure to paddles to create good contact between the paddle and the skin. Ensure good contact between the skin and the adhesive electrode pad. If a large amount of hair on the chest prevents good skin-electrode contact, quickly shave the area and reapply the paddle/pad. Modifications may be required in special situations. i Special Situation Standing water Implanted defibrillator or pacemaker Transdermal medication patch Modification Remove the victim 'from the water and quickly wipe the chest. Do not place an electrode pad directly over the implanted device because the device may reduce delivery of current to the heart. Place the pad at least 1 inch (2.5 cm) to the side of the implanted device. Do not place an electrode pad directly over a medication patch. If the patch is in the way, remove it and wipe the child's skin before attaching the pad. 10 Press the CHARGE button to charge the defibrillator. The CHARGE button is located either on the defibrillator or 2006 American Heart Association 8 11
12 on one or both paddles. If the device requires more that 10 seconds to charge, rescuers may resume chest compression until the device is charged and ready for shock delivery. 11 "Clear" the patient when the defibrillator is fully charged. To ensure the safety of defibrillation, always announce when you are about to deliver a shock. State a "warning" firmly and in a forceful voice before delivering each shock (this entire sequence should take less than 5 seconds). You may use a warning like this: "I am going to shock on three. One, I'm clear." Check to make sure you are clear of contact with the patient, the stretcher, or other equipment. "Two, you're clear." Make a visual check to ensure that no one is touching the patient or stretcher. In particular, check the person providing ventilations. That person's hands should not be touching the ventilatory adjuncts, including an advanced airway. Be sure oxygen is not flowing across the patient's chest. Direct flow away from the patient's chest and consider temporarily disconnecting the bag or the ventilation circuit from the endotracheal tube during shock delivery. "Three, everybody is clear." Check yourself one more time before pressing the SHOCK button(s). You need not use these exact words, but you must warn others that you are about to deliver shocks and that everyone must stand clear. 12 Press SHOCK button(s) to deliver current. Press either a Single SHOCK button located on the defibrillator both SHOCK buttons on paddles simultaneously 13 Immediately resume CPR starting with chest compressions for about 2 minutes American Heart Association 9 12
13 Pediatric Assessment Flowchart American Heart ~ Association ~ Learn and Live '" General Assessment Appearance... Work of Breathing'" Circulation O Primary Assessment Airway Breathing Circulation Disability Exposure Secondary Assessment (SAMPLE history, focused physical exam, bedside glucose) Tertiary Assessment (laboratory studies, x-rays, other tests) Categorize illness by type and severity Respiratory Circulatory Respiratory distress or Respiratory failure Upper airway obstruction Lower airway obstruction Lung tissue disease Disordered control of breathing Compensated shock or Hypotensive shock Hypovolemic shock Distributive shock Cardiogenic shock Obstructive shock Respiratory + Circulatory including cardiopulmonary failure If at any time during the assessment and categorization process you identify a life-threatening condition Immediately initiate life-saving interventions and activate the emergency response system 2006 American Heart Association 13
14 14

15 PALS Management of Shock Emergencies Flowchart American Heart ~ Associatioll ~ Learn and Live SM Management of Shock Emergencies Flowchart Nonhemorrhagic 20 mukg NS/LR bolus, repeat as needed Consider colloid after 3rd NS/LR bolus Management : Septic Shock Oxygen Pulse oximetry ECG monitor IV/IO access BLS as indicated Bedside glucose Hypovolemic Shock Specific Management for Selected Conditions Hemorrhagic Control external bleeding 20 mukg NS/LR bolus repeat 2 or 3x as needed Transfuse PRBCs as indicated Distributive Shock Specific Management for Selected Conditions Septic Anaphylactic Neurogenic 1M epinephrine (or auto-injector) Antihistamines Corticosteroids Epinephrine infusion Albuterol BradyarrhythmialTachyarrhythmia Management s: Bradycardia Tachycardia with poor perfusion Cardiogenic Shock Specific Management for Selected Conditions 20 mukg NS/LR bolus, repeat PRN Vasopressor Other (eg, CHD, Myocarditis, Cardiomyopathy, Poisoning) 5 to 10 mukg NS/LR bolus, repeat PRN Vasoactive infusion Consider expert consultation Obstructive Shock Specific Management for Selected Conditions Ductal-Dependent (LV Outflow Obstruction) Tension Pneumothorax Cardiac Tamponade Pulmonary Embolism Prostaglandin E, Expert consultation Needle decom pression Tube thoracostomy Pericardiocentesis 20 mukg NS/LR bolus 20 mukg NS/LR bolus, repeat PRN Consider thrombolytics, anticoagulants Expert consultation 2006 American Heart Association 15

16 16
17 VENTRICULAR FIBRILLATION, or PULSELESS VENTRICULAR TACHYCARDIA* - PEDIATRIC EMT- Paramedic 1. ABCs 2. CPR (2005 Guidelines)** 3. Ventilate with Oxygen (Insert OPA/NPA) 4. Use ResQPOD if the patient has reached puberty 5. Attach Defibrillator 6. 2 Joules/kg or Biphasic Equivalent 7. Resume CPR ***A Fluid Challange of 20cc/kg Should be Administered Over 10 Minutes in All Cardiac Arrest Situations. May Repeat Once. Rhythm Change? *Patients > 1 YOA In all witnessed or known short duration (<4-5 minutes) cardiac arrest where defibrillation is indicated immediate defibrillation should be performed. In all other arrest situations where defibrillation is indicated the provider should perform 5 cycles (2 minutes) of CPR prior to defibrillation. 1. Resume CPR 2. IV, NS, TKO*** 3. Intubate Patient 4. Epinephrine: Repeat Every 3 to 5 Minutes IV/IO: 0.01mg/kg to a max of 1mg per single dose(1:10,000, 0.1mL/kg) ET: 0.1mg/kg (1:1,000, 0.1mL/kg) to a max of 1mg per single dose Joules/kg, to a max of 360 Joules or Biphasic Equivalent 6. Resume CPR Rhythm Change? 1. Resume CPR 2. Amiodarone, 5mg/kg to a max of 300mg. May repeat once in 3-5 minutes at 2.5mg/kg to a max of 150mg.**** 3. 4 Joules/kg, to a max of 360 Joules or Biphasic Equivalent 4. Resume CPR Continue to Treat, Monitor & Transport Rhythm Change? Check Pulse *** If IV or IO access unavailable administer Lidocaine 2mg/kg, ET. If V-Tach not suppressed repeat Lidocaine 2mg/kg, ET, every 3-5 minutes to a max of 6mg/kg, ET Once an antiarrhythmic is administered DO T administer a different antiarrhythmic. If IV or IO access is obtained after ET Lidocaine was administered, administer Lidocaine 1mg/kg, IV, may repeat every 3-5 minutes to a max of 3mg/kg, IV (Should not administer more than 3 total doses whether IV/IO or ET) The Administration of Lidocaine during IO placement for pain control ONLY does not contraindicate the administration of Amiodarone if indicated Refer to Appropriate 02/01/2011 ** Ideally chest compressions should be interrupted only for rhythm checks and actual defibrillations. The 2005 guidelines state that when CPR is indicated the provider should perform 5 cycles (2 Minutes) of chest compressions. Continue CPR while drugs are prepared/administered and the defibrillator is charging. Providers must organize care to ensure that chest compressions, initial and subsequent defibrillations are not delayed in order to administer drugs, place advanced airways or obtain vascular access. 17 Page 18
18 ASYSTOLE or PULSELESS ELECTRICAL ACTIVITY - PEDIATRIC EMT- Paramedic ***IV Fluids Should be Infused at a Rate to Obtain a Fluid Bolus of 20cc/kg Over 10 Minutes. May Repeat Once if Needed. 1. ABCs 2. CPR (2005 Guidelines)* 3. Ventilate with Oxygen (Insert OPA/NPA) 4. Use ResQPOD if the patient has reached puberty 5. Attach Defibrillator** 6. IV, NS*** 7. Intubate Patient 8. Resume CPR Rhythm Change or Pulse Present? **** Consider Whether One of the Following may be Involved and Treat Appropriately: Hypovolemia (Infuse Volume) Hypoxia (Ventilate) Hypo/Hyperkalemia Hydrogen Ion (Acidosis) Hypoglycemia (D50) Hypothermia Toxins/OD Tamponade (Cardiac) Tension Pneumothorax (Decompress Chest) Thrombosis (Pulmonary, Coronary) Trauma 1. Resume CPR 2. Epinephrine: Repeat Every 3 to 5 Minutes IV/IO: 0.01mg/kg up to a max of 1mg per single dose. (1:10,000, 0.1mL/kg) or ET: 0.1mg/kg up to a max of 1mg per single dose. (1:1,000, 0.1mL/kg) Rhythm Change or Pulse Present? Resume CPR Treat Possible Contributing Factors**** Refer to Appropriate Continue to Treat, Monitor & Transport **Asystole should be confirmed in 2 leads. If rhythm is unclear and possibly Ventricular Fibrillation, go to Ventricular Fibrillation. * Ideally chest compressions should be interrupted only for rhythm check. The 2005 guidelines state that when CPR is indicated the provider should perform 5 cycles (2 minutes) of chest compressions. Continue CPR while drugs are prepared/administered. Providers must organize care to minimize interruption in chest compressions for rhythm checks, advance airway insertion, or vascular access. 02/01/2011 Page 8 18

19 19
20 BRADYARRHYTHMIA - PEDIATRIC EMT- Paramedic 1. ABCs 2. Oxygen 3. Assist Ventilations if Respirations Inadequate (Insert OPA/NPA if needed) 4. Intubate Patient if Unable to Maintain Airway 5. IV, NS, TKO (Use IO Access if Necessary) 6. Assess Vital Signs & Perfusion Patient has any of the Following: Signs/Symptoms of Hypoperfusion? Hypotension? Respiratory Difficulty? Perform Chest Compressions if, Despite Oxygenation & Ventilation, Heart Rate: <80/min in an Infant (<1 year old) <60/min in a Child (1-12 years old) Pulse >60 (>80 in Infant), or Signs/Symptoms Resolve? Epinephrine: IV/IO: 0.01mg/kg (1:10,000, 0.1mL/kg) to a max of 5cc per single dose. or ET: 0.1mg/kg (1:1,000, 0.1mL/kg) to a max of 0.5cc per single dose. Repeat Every 3-5 Minutes at Same Dose Pulse >60 (>80 in Infant), or Signs/Symptoms Resolve? Atropine, 0.02mg/kg, IV Minimum Dose 0.1mg Maximum Single Dose 0.5mg May Repeat every 3-5 Minutes (In children 0-8 years of age to a max of 1mg) (In Adolescence 9-15 years of age to a max of 2mg) Continue to Treat, Monitor & Transport 02/01/2011 Page 10 20

21 21
22 1. Oxygen 2. IV, NS, TKO Patient Conscious? SUPRAVENTRICULAR TACHYCARDIA (>150) 1. Synchronized 100 Joules 2. Synchronized 200 Joules* 3. Synchronized 300 Joules* 4. Synchronized 360 Joules* EMT- Paramedic *Repeated Cardioversions Are Done Only if There is Rhythm Change. Rhythm Change? Refer to Appropriate Valsalva Maneuver Rhythm Change? Adenosine, 12mg, IV Rhythm Change? Refer to Appropriate Refer to Appropriate Adenosine, 12mg, IV Rhythm Change? Refer to Appropriate If Systolic BP >90mmHg and patient is conscious give Versed, 5mg, IVP (2.5mg if > 60 years old) Altered Mental Status, Chest Pain, Hypotension, or Other Signs of Shock Continue to Treat, Monitor & Transport 1. Synchronized 100 Joules 2. Synchronized 200 Joules* 3. Synchronized 300 Joules* 4. Synchronized 360 Joules* Rhythm Change? **Amiodarone, 150mg IV Over 10 minutes. May Repeat Once if Needed. (may mix into 100cc of D5W) Rhythm Change? Refer to Appropriate Continue to Treat, Monitor & Transport Refer to Appropriate PEDIATRIC DOSES Sync. 1Joule/kg to a max of 100 J Sync. 2Joules/kg to a max of 360 J* Adenosine, 0.1mg/kg to a max of 12mg Versed, 0.1mg/kg, IV, to a max of 2.5mg Amiodarone 5mg/kg, IV, over 20 minutes, to a max single dose of 150mg. May be repeated X 2 (Do not mix into 100cc of D5W) 02/01/2011 PEDIATRIC SVT RATES In Infants Heart rate > 220 In Children Heart Rate > 180 ** The Administration of Lidocaine during IO placement for pain control ONLY does not contraindicate the administration of Amiodarone if indicated Page 16 22
23 VENTRICULAR TACHYCARDIA WITH A PULSE EMT- Paramedic 1. Oxygen 2. IV, NS, TKO Patient Experiencing Any of the Following: Systolic BP <90mmHG? Chest Pain? Dyspnea? Signs/Symptoms of CHF? Other Signs/Symptoms of Hypoperfusion? Continued on Following Page C Amiodarone 150mg, IV, over 10 minutes. If patient remains without above signs and symptoms. Amiodarone may be repeated every 10 minutes as needed to a max of 450mg. (May mix into 100cc of D5W) Ventricular Tachycardia Suppressed? Class I or II Cardiac Rhythm (P-11) with stable vital signs? Refer to Appropriate Does Patient Have any Signs and Symptoms Listed Above? Continue to Treat, Monitor & Transport Continue to Treat, Monitor & Transport * * If at any time the patient starts to experience any of the signs and symptoms noted above, go directly to Cardioversion.( Pg 20) PEDIATRIC DOSE Amiodarone 5mg/kg, IV, over 20 minutes, to a max single dose of 150mg. May be repeated X 2 (Do not mix into 100cc of D5W) 02/01/ Page 19
24 VENTRICULAR TACHYCARDIA WITH A PULSE (CONTINUED) EMT- Paramedic C If systolic BP >90mmHg consider Versed, 5 mg, IV (2.5 mg if >60 years old) 1. Synchronized 100 Joules 2. Synchronized 200 Joules** 3. Synchronized 300 Joules** 4. Synchronized 360 Joules** **Repeated Cardioversions Are Done Only if There is Rhythm Change. Ventricular Tachycardia Suppressed? Class I or II Cardiac Rhythm (P-11) with stable vital signs? Refer to Appropriate Refer to Post Resuscitation Management (pg-13) Intubate Patient If Needed*** 1. Amiodarone 150mg, IV, over 10 minutes. Amiodarone may be repeated every 10 minutes as needed to max of 450mg. (May mix into 100cc of D5W) 2. Synchronized 360 Joules,** or Energy Setting Previously Successful, Following Each Dose of Amiodarone. Ventricular Tachycardia Suppressed? Class I or II Cardiac Rhythm (P-11) with stable vital signs? Refer to Appropriate Continue to Treat, Monitor & Transport Continue to Treat, Monitor & Transport PEDIATRIC CARDIOVERSION Infant- 1J/kg up to a max of 100J Child- 2J/kg up to a max of 360J *** If IV or IO access unavailable administer Lidocaine 2mg/kg, ET. If V-Tach not suppressed repeat Lidocaine 2mg/kg, ET, every 3-5 minutes to a max of 6mg/kg, ET Once an antiarrhythmic is administered DO T administer a different antiarrhythmic. If IV or IO access is obtained after ET Lidocaine was administered, administer Lidocaine 1mg/kg, IV, may repeat every 3-5 minutes to a max of 3mg/kg, IV (Should not administer more than 3 total doses whether IV/IO or ET) The Administration of Lidocaine during IO placement for pain control ONLY does not contraindicate the administration of Amiodarone if indicated PEDIATRIC DOSE Amiodarone 5mg/kg, IV, over 20 minutes, to a max single dose of 150mg. May be repeated X 2 (Do not mix into 100cc of D5W) Versed, 0.1mg/kg, IV, to a max of 2.5mg Lidocaine 2mg/kg, ET, every 3-5 minutes, to max of 6mg/kg. If IV or IO access is obtained after ET Lidocaine was administered, administer Lidocaine 1mg/kg, IV, may repeat every 3-5 minutes to a max of 3mg/kg, IV (Should not administer more than 3 total doses whether IV/IO or ET) Once an antiarrhythmic is administered DO T administer a different antiarrhythmic. 02/01/ Page 20
Community Ambulance Service of Minot ALS Standing Orders Legend
 Legend Indicates General Information and Guidelines Indicates Procedures Indicates Medication Administration Indicates Referral to Other Protocol Indicates Referral to Online Medical Direction Pediatric
Legend Indicates General Information and Guidelines Indicates Procedures Indicates Medication Administration Indicates Referral to Other Protocol Indicates Referral to Online Medical Direction Pediatric
Cardiac Arrest VF/Pulseless VT Learning Station Checklist
 Cardiac Arrest VF/Pulseless VT Learning Station Checklist VF/VT 00 American Heart Association Adult Cardiac Arrest Shout for Help/Activate Emergency Response Epinephrine every - min Amiodarone Start CPR
Cardiac Arrest VF/Pulseless VT Learning Station Checklist VF/VT 00 American Heart Association Adult Cardiac Arrest Shout for Help/Activate Emergency Response Epinephrine every - min Amiodarone Start CPR
PRO-CPR. 2015 Guidelines: PALS Algorithm Overview. (Non-AHA supplementary precourse material)
") PRO-CPR 2015 Guidelines: PALS Algorithm Overview (Non-AHA supplementary precourse material) Please reference Circulation (from our website), the ECC Handbook, or the 2015 ACLS Course Manual for correct
PRO-CPR 2015 Guidelines: PALS Algorithm Overview (Non-AHA supplementary precourse material) Please reference Circulation (from our website), the ECC Handbook, or the 2015 ACLS Course Manual for correct
Cardiac Arrest Pediatric Ventricular Fibrillation / Pulseless Ventricular Tachycardia Protocol revised October 2008
 Cardiac Arrest Pediatric Ventricular Fibrillation / Pulseless Ventricular Tachycardia Protocol revised October 2008 Preamble In contrast to cardiac arrest in adults, cardiopulmonary arrest in pediatric
Cardiac Arrest Pediatric Ventricular Fibrillation / Pulseless Ventricular Tachycardia Protocol revised October 2008 Preamble In contrast to cardiac arrest in adults, cardiopulmonary arrest in pediatric
PEDIATRIC TREATMENT GUIDELINES
 P1 Pediatric Patient Care P2 Cardiac Arrest Initial Care and CPR P3 Neonatal Resuscitation P4 Ventricular Fibrillation / Ventricular Tachycardia P5 PEA / Asystole P6 Symptomatic Bradycardia P7 Tachycardia
P1 Pediatric Patient Care P2 Cardiac Arrest Initial Care and CPR P3 Neonatal Resuscitation P4 Ventricular Fibrillation / Ventricular Tachycardia P5 PEA / Asystole P6 Symptomatic Bradycardia P7 Tachycardia
ACLS Study Guide BLS Overview CAB
 ACLS Study Guide The ACLS Provider exam is 50-mutiple choice questions. Passing score is 84%. Student may miss 8 questions. For students taking ACLS for the first time or renewing students with a current
ACLS Study Guide The ACLS Provider exam is 50-mutiple choice questions. Passing score is 84%. Student may miss 8 questions. For students taking ACLS for the first time or renewing students with a current
ACLS Provider Manual Comparison Sheet Based on 2010 AHA Guidelines for CPR and ECC. BLS Changes
 ACLS Provider Manual Comparison Sheet Based on 2010 AHA Guidelines for CPR and ECC CPR Chest compressions, Airway, Breathing (C-A-B) BLS Changes New Old Rationale New science indicates the following order:
ACLS Provider Manual Comparison Sheet Based on 2010 AHA Guidelines for CPR and ECC CPR Chest compressions, Airway, Breathing (C-A-B) BLS Changes New Old Rationale New science indicates the following order:
Pediatric Advanced Life Support (PALS) Recertification Preparatory Materials
 Recertification Preparatory Materials") Pediatric Advanced Life Support (PALS) Recertification Preparatory Materials 1 PEDIATRIC ADVANCED LIFE SUPPORT (PALS) RECERTIFICATION TABLE OF CONTENTS CYCLIC APPROACH 03 PEDIATRIC ASSESSMENT FLOWCHART
Pediatric Advanced Life Support (PALS) Recertification Preparatory Materials 1 PEDIATRIC ADVANCED LIFE SUPPORT (PALS) RECERTIFICATION TABLE OF CONTENTS CYCLIC APPROACH 03 PEDIATRIC ASSESSMENT FLOWCHART
Procedure 17: Cardiopulmonary Resuscitation
 Cardiopulmonary Resuscitation 349 Procedure 17: Cardiopulmonary Resuscitation Introduction Cardiopulmonary arrest (CPA) occurs when a patient s heart and lungs stop functioning. In children, CPA usually
Cardiopulmonary Resuscitation 349 Procedure 17: Cardiopulmonary Resuscitation Introduction Cardiopulmonary arrest (CPA) occurs when a patient s heart and lungs stop functioning. In children, CPA usually
IU Health ACLS Study Guide
 IU Health ACLS Study Guide Preparing for your upcoming ACLS Class REVISED SEPTEMBER 2011 ON APRIL 1, 2011 WE BEGAN TEACHING THE 2010 AHA GUIDELINES. WE HIGHLY RECOMMEND REVIEWING THE NEW ALGORYHMS FOUND
IU Health ACLS Study Guide Preparing for your upcoming ACLS Class REVISED SEPTEMBER 2011 ON APRIL 1, 2011 WE BEGAN TEACHING THE 2010 AHA GUIDELINES. WE HIGHLY RECOMMEND REVIEWING THE NEW ALGORYHMS FOUND
Official Online ACLS Exam
 \ Official Online ACLS Exam Please fill out this form before you take the exam. Name : Email : Phone : 1. Hypovolemia initially produces which arrhythmia? A. PEA B. Sinus tachycardia C. Symptomatic bradyarrhythmia
\ Official Online ACLS Exam Please fill out this form before you take the exam. Name : Email : Phone : 1. Hypovolemia initially produces which arrhythmia? A. PEA B. Sinus tachycardia C. Symptomatic bradyarrhythmia
If you do not wish to print the entire pre-test you may print Page 2 only to write your answers, score your test, and turn in to your instructor.
 This is a SAMPLE of the pretest you can access with your AHA PALS Course Manual at Heart.org/Eccstudent using your personal code that comes with your PALS Course Manual The American Heart Association strongly
This is a SAMPLE of the pretest you can access with your AHA PALS Course Manual at Heart.org/Eccstudent using your personal code that comes with your PALS Course Manual The American Heart Association strongly
ACLS PRE-TEST ANNOTATED ANSWER KEY
 ACLS PRE-TEST ANNOTATED ANSWER KEY June, 2011 Question 1: Question 2: There is no pulse with this rhythm. Question 3: Question 4: Question 5: Question 6: Question 7: Question 8: Question 9: Question 10:
ACLS PRE-TEST ANNOTATED ANSWER KEY June, 2011 Question 1: Question 2: There is no pulse with this rhythm. Question 3: Question 4: Question 5: Question 6: Question 7: Question 8: Question 9: Question 10:
American Heart Association ACLS Pre-Course Self Assessment Dec., 2006. ECG Analysis. Name the following rhythms from the list below:
 American Heart Association ACLS Pre-Course Self Assessment Dec., 2006 ECG Analysis This pre-test is exactly the same as the pretest on the ACLS Provider manual CD. This paper version can be completed in
American Heart Association ACLS Pre-Course Self Assessment Dec., 2006 ECG Analysis This pre-test is exactly the same as the pretest on the ACLS Provider manual CD. This paper version can be completed in
Present : PGY 王 淳 峻 Supervisor: F1 王 德 皓 991109
 Present : PGY 王 淳 峻 Supervisor: F1 王 德 皓 991109 Interventions to prevent cardiac arrest + Airway management + Ventilation support + Treatment of bradyarrhythmias & Tachyarrhythmias Treat cardiac arrest
Present : PGY 王 淳 峻 Supervisor: F1 王 德 皓 991109 Interventions to prevent cardiac arrest + Airway management + Ventilation support + Treatment of bradyarrhythmias & Tachyarrhythmias Treat cardiac arrest
Wilson County Emergency Management Agency Protocol Manual Protocols
 Asystole No pulse or respirations Confirm cardiac rhythm with combo pads or electrodes Record in two leads to confirm Asystole and to rule out fine V-Fib. Basic assessment and management (up to your scope
Asystole No pulse or respirations Confirm cardiac rhythm with combo pads or electrodes Record in two leads to confirm Asystole and to rule out fine V-Fib. Basic assessment and management (up to your scope
Crash Cart Drugs Drugs used in CPR. Dr. Layla Borham Professor of Clinical Pharmacology Umm Al Qura University
 Crash Cart Drugs Drugs used in CPR Dr. Layla Borham Professor of Clinical Pharmacology Umm Al Qura University Introduction A list of the drugs kept in the crash carts. This list has been approved by the
Crash Cart Drugs Drugs used in CPR Dr. Layla Borham Professor of Clinical Pharmacology Umm Al Qura University Introduction A list of the drugs kept in the crash carts. This list has been approved by the
PALS Interim Study Guide
 PALS Interim Study Guide 2006 Bulletin: New resuscitation science and American Heart Association treatment guidelines were released November 28, 2005! The new AHA Handbook of Emergency Cardiac Care (ECC)
PALS Interim Study Guide 2006 Bulletin: New resuscitation science and American Heart Association treatment guidelines were released November 28, 2005! The new AHA Handbook of Emergency Cardiac Care (ECC)
Michigan Adult Cardiac Protocols CARDIAC ARREST GENERAL. Date: May 31, 2012 Page 1 of 5
 Date: May 31, 2012 Page 1 of 5 Cardiac Arrest General This protocol should be followed for all adult cardiac arrests. Medical cardiac arrest patients undergoing attempted resuscitation should not be transported
Date: May 31, 2012 Page 1 of 5 Cardiac Arrest General This protocol should be followed for all adult cardiac arrests. Medical cardiac arrest patients undergoing attempted resuscitation should not be transported
EMS SKILL CARDIAC EMERGENCY: AUTOMATED EXTERNAL DEFIBRILLATION (AED)
") EMS SKILL CARDIAC EMERGENCY: AUTOMATED EXTERNAL DEFIBRILLATION (AED) PERFORMANCE OBJECTIVE Demonstrate competency in assessing signs of cardiopulmonary arrest and performing defibrillation using a semi-automated
EMS SKILL CARDIAC EMERGENCY: AUTOMATED EXTERNAL DEFIBRILLATION (AED) PERFORMANCE OBJECTIVE Demonstrate competency in assessing signs of cardiopulmonary arrest and performing defibrillation using a semi-automated
Update on Small Animal Cardiopulmonary Resuscitation (CPR)- is anything new?
- is anything new?") Update on Small Animal Cardiopulmonary Resuscitation (CPR)- is anything new? DVM, DACVA Objective: Update on the new Small animal guidelines for CPR and a discussion of the 2012 Reassessment Campaign on
Update on Small Animal Cardiopulmonary Resuscitation (CPR)- is anything new? DVM, DACVA Objective: Update on the new Small animal guidelines for CPR and a discussion of the 2012 Reassessment Campaign on
Management of Adult Cardiac Arrest
 73991_CH27_page68-73.qxd 6/6/11 3:54 PM Page 68 27.68 Section 5 Medical Guidelines for Performing a 12-Lead ECG The only way to learn how to obtain a 12-lead ECG is to practice with the equipment itself.
73991_CH27_page68-73.qxd 6/6/11 3:54 PM Page 68 27.68 Section 5 Medical Guidelines for Performing a 12-Lead ECG The only way to learn how to obtain a 12-lead ECG is to practice with the equipment itself.
Cardiac Arrest - Ventricular Fibrillation / Pulseless Ventricular Tachycardia Protocol revised October 2008
 Cardiac Arrest - Ventricular Fibrillation / Pulseless Ventricular Tachycardia Protocol revised October 2008 Preamble Survival from cardiorespiratory arrest for patients who present with ventricular fibrillation
Cardiac Arrest - Ventricular Fibrillation / Pulseless Ventricular Tachycardia Protocol revised October 2008 Preamble Survival from cardiorespiratory arrest for patients who present with ventricular fibrillation
The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010.
 ACLS Study Guide The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. Please read the below information carefully This letter is to confirm your
ACLS Study Guide The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. Please read the below information carefully This letter is to confirm your
CRNA ACLS, PALS, & BLS REFRESHER
 Attn: Certified Nurse Anesthetists (CRNA) CPR Consultants, Inc. 7404 G Chapel Hill Road, Raleigh, NC, 27607 CRNA ACLS, PALS, & BLS REFRESHER CRNA American Heart Association Triple Certification (BLS, ACLS,
Attn: Certified Nurse Anesthetists (CRNA) CPR Consultants, Inc. 7404 G Chapel Hill Road, Raleigh, NC, 27607 CRNA ACLS, PALS, & BLS REFRESHER CRNA American Heart Association Triple Certification (BLS, ACLS,
DEBRIEFING GUIDE. The key components of an optimal code response: 1. Early recognition that the patient is deteriorating or has become unresponsive.
 DEBRIEFING GUIDE I N T R O D U C T I O N Debriefing has been shown to improve clinical behavior during cardiac resuscitation and, as such, has become a recommended procedure in the 2010 American Heart
DEBRIEFING GUIDE I N T R O D U C T I O N Debriefing has been shown to improve clinical behavior during cardiac resuscitation and, as such, has become a recommended procedure in the 2010 American Heart
Team Leader. Ensures high-quality CPR at all times Assigns team member roles Ensures that team members perform well. Bradycardia Management
 ACLS Megacode Case 1: Sinus Bradycardia (Bradycardia VF/Pulseless VT Asystole Out-of-Hospital Scenario You are a paramedic and arrive on the scene to find a 57-year-old woman complaining of indigestion.
ACLS Megacode Case 1: Sinus Bradycardia (Bradycardia VF/Pulseless VT Asystole Out-of-Hospital Scenario You are a paramedic and arrive on the scene to find a 57-year-old woman complaining of indigestion.
E C C. American Heart Association. Advanced Cardiovascular Life Support. Written Exams. May 2011
 E C C American Heart Association Advanced Cardiovascular Life Support Written Exams Contents: Exam Memo Student Answer Sheet Version A Exam Version A Answer Key Version A Reference Sheet Version B Exam
E C C American Heart Association Advanced Cardiovascular Life Support Written Exams Contents: Exam Memo Student Answer Sheet Version A Exam Version A Answer Key Version A Reference Sheet Version B Exam
E C C. American Heart Association. Advanced Cardiovascular Life Support. Written Precourse Self-Assessment. May 2011. 2011 American Heart Association
 E C C American Heart Association Advanced Cardiovascular Life Support Written Precourse Self-Assessment May 2011 2011 American Heart Association 2011 ACLS Written Precourse Self-Assessment 1. Ten minutes
E C C American Heart Association Advanced Cardiovascular Life Support Written Precourse Self-Assessment May 2011 2011 American Heart Association 2011 ACLS Written Precourse Self-Assessment 1. Ten minutes
It is recommended that the reader review each medical directive presented in this presentation along with the actual PCP Core medical directive.
 It is recommended that the reader review each medical directive presented in this presentation along with the actual PCP Core medical directive. This presentation will highlight the changes and any new
It is recommended that the reader review each medical directive presented in this presentation along with the actual PCP Core medical directive. This presentation will highlight the changes and any new
www.cprtrainingfast.com
 ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION 1. Ten minutes after an 85 year old woman collapses, paramedics arrive and start CPR for the first time. The monitor shows fine (low amplitude)
ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION 1. Ten minutes after an 85 year old woman collapses, paramedics arrive and start CPR for the first time. The monitor shows fine (low amplitude)
Megacode Testing Checklist 1/2 Bradycardia VF/Pulseless VT Asystole ROSC
 Megacode Testing Checklist 1/2 Bradycardia VF/Pulseless VT Asystole ROSC Student Name: Test Bradycardia Management Recognizes symptomatic bradycardia Administers correct dose of atropine Prepares for second-line
Megacode Testing Checklist 1/2 Bradycardia VF/Pulseless VT Asystole ROSC Student Name: Test Bradycardia Management Recognizes symptomatic bradycardia Administers correct dose of atropine Prepares for second-line
CPR/AED for Professional Rescuers and Health Care Providers HANDBOOK
 CPR/AED for Professional Rescuers and Health Care Providers HANDBOOK TABLE OF CONTENTS SECTION 1: THE PROFESSIONAL RESCUER The Duty to Respond 2 Preventing the Spread of Bloodborne Pathogens 3 Taking Action
CPR/AED for Professional Rescuers and Health Care Providers HANDBOOK TABLE OF CONTENTS SECTION 1: THE PROFESSIONAL RESCUER The Duty to Respond 2 Preventing the Spread of Bloodborne Pathogens 3 Taking Action
American Heart Association. Pediatric Advanced Life Support. Written Precourse Self-Assessment. Questions and Answer Key for Students.
 E C C American Heart Association Pediatric Advanced Life Support Written Precourse Self-Assessment Questions and Answer Key for Students January 2012 PALS Written 2011 Precourse Self-Assessment ECG Rhythm
E C C American Heart Association Pediatric Advanced Life Support Written Precourse Self-Assessment Questions and Answer Key for Students January 2012 PALS Written 2011 Precourse Self-Assessment ECG Rhythm
ROC CONTINUOUS CHEST COMPRESSIONS STUDY (CCC): MEDICAL CARDIAC ARREST MEDICAL DIRECTIVE
: MEDICAL CARDIAC ARREST MEDICAL DIRECTIVE") ROC CONTINUOUS CHEST COMPRESSIONS STUDY (CCC): MEDICAL CARDIAC ARREST MEDICAL DIRECTIVE An Advanced Care Paramedic will provide the treatment based on the randomization scheme and as prescribed in this
ROC CONTINUOUS CHEST COMPRESSIONS STUDY (CCC): MEDICAL CARDIAC ARREST MEDICAL DIRECTIVE An Advanced Care Paramedic will provide the treatment based on the randomization scheme and as prescribed in this
2015 Interim Resources for BLS
 2015 Interim Resources for BLS Original Release: November 25, 2015 Starting in 2016, new versions of American Heart Association online courses will be released to reflect the changes published in the 2015
2015 Interim Resources for BLS Original Release: November 25, 2015 Starting in 2016, new versions of American Heart Association online courses will be released to reflect the changes published in the 2015
Question-and-Answer Document 2010 AHA Guidelines for CPR & ECC As of October 18, 2010
 Question-and-Answer Document 2010 AHA Guidelines for CPR & ECC As of October 18, 2010 Q: What are the most significant changes in the 2010 AHA Guidelines for CPR & ECC? A: Major changes for all rescuers,
Question-and-Answer Document 2010 AHA Guidelines for CPR & ECC As of October 18, 2010 Q: What are the most significant changes in the 2010 AHA Guidelines for CPR & ECC? A: Major changes for all rescuers,
ACLS PHARMACOLOGY 2011 Guidelines
 ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
ACLS PHARMACOLOGY 2011 Guidelines ADENOSINE Narrow complex tachycardias or wide complex tachycardias that may be supraventricular in nature. It is effective in treating 90% of the reentry arrhythmias.
Cardiac Arrest: General Considerations
 Andrea Gabrielli, MD, FCCM Cardiac Arrest: General Considerations Cardiopulmonary resuscitation (CPR) is described as a series of assessments and interventions performed during a variety of acute medical
Andrea Gabrielli, MD, FCCM Cardiac Arrest: General Considerations Cardiopulmonary resuscitation (CPR) is described as a series of assessments and interventions performed during a variety of acute medical
Purpose To guide registered nurses who may manage clients experiencing sudden or unexpected life-threatening cardiac emergencies.
 Emergency Cardiac Care: Decision Support Tool #1 RN-Initiated Emergency Cardiac Care Without Cardiac Monitoring/Manual Defibrillator or Emergency Cardiac Drugs Decision support tools are evidence-based
Emergency Cardiac Care: Decision Support Tool #1 RN-Initiated Emergency Cardiac Care Without Cardiac Monitoring/Manual Defibrillator or Emergency Cardiac Drugs Decision support tools are evidence-based
10. An infant with a history of vomiting and diarrhea arrives by ambulance. During your primary assessment the infant responds only to painful stimula
 1. You are called to help resuscitate an infant with severe symptomatic bradycardia associated with respiratory distress. The bradycardia persists despite establishment of an effective airway, oxygenation,
1. You are called to help resuscitate an infant with severe symptomatic bradycardia associated with respiratory distress. The bradycardia persists despite establishment of an effective airway, oxygenation,
New resuscitation science and American Heart Association treatment guidelines were released October 28, 2010!
 ACLS Study Guide 2010 Bulletin: New resuscitation science and American Heart Association treatment guidelines were released October 28, 2010! The new AHA Handbook of Emergency Cardiac Care (ECC) contains
ACLS Study Guide 2010 Bulletin: New resuscitation science and American Heart Association treatment guidelines were released October 28, 2010! The new AHA Handbook of Emergency Cardiac Care (ECC) contains
table of contents drug reference
 table of contents drug reference ADULT DRUG REFERENCE...155 161 PEDIATRIC DRUG REFERENCE...162 164 PEDIATRIC WEIGHT-BASED DOSING CHARTS...165 180 Adenosine...165 Amiodarone...166 Atropine...167 Defibrillation...168
table of contents drug reference ADULT DRUG REFERENCE...155 161 PEDIATRIC DRUG REFERENCE...162 164 PEDIATRIC WEIGHT-BASED DOSING CHARTS...165 180 Adenosine...165 Amiodarone...166 Atropine...167 Defibrillation...168
2015 Interim Resources for HeartCode ACLS
 2015 Interim Resources for HeartCode ACLS Original Release: November 25, 2015 Starting in 2016, new versions of American Heart Association online courses will be released to reflect the changes published
2015 Interim Resources for HeartCode ACLS Original Release: November 25, 2015 Starting in 2016, new versions of American Heart Association online courses will be released to reflect the changes published
Department of Emergency and Disaster Medicine Medical University of LODZ
 Electrotherapy in emergency states Department of Emergency and Disaster Medicine Medical University of LODZ defibrillation defibrillation The purpous of defibrillation is to deliver a randomly timed high-energy
Electrotherapy in emergency states Department of Emergency and Disaster Medicine Medical University of LODZ defibrillation defibrillation The purpous of defibrillation is to deliver a randomly timed high-energy
Adult Drug Reference. Dopamine Drip Chart. Pediatric Drug Reference. Pediatric Drug Dosage Charts DRUG REFERENCES
 Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
If you do not wish to print the entire pre-test you may print Page 2 only to write your answers, score your test, and turn in to your instructor.
 This is a SAMPLE of the pretest you can access with your AHA PALS Course Manual at Heart.org/Eccstudent using your personal code that comes with your PALS Course Manual The American Heart Association strongly
This is a SAMPLE of the pretest you can access with your AHA PALS Course Manual at Heart.org/Eccstudent using your personal code that comes with your PALS Course Manual The American Heart Association strongly
Advanced Cardiac Life Support
 Advanced Cardiac Life Support Dr Teo Wee Siong NATIONAL RESUSCITATION COUNCIL Singapore Guidelines 2006 Prof Anantharaman A/Prof Lim Swee Han Dr Chee Tek Siong A/Prof Peter Manning A/Prof Eillyne Seow
Advanced Cardiac Life Support Dr Teo Wee Siong NATIONAL RESUSCITATION COUNCIL Singapore Guidelines 2006 Prof Anantharaman A/Prof Lim Swee Han Dr Chee Tek Siong A/Prof Peter Manning A/Prof Eillyne Seow
PALS Study Guide. PALS Study Guide Revised August 2010, Page 1 [TCL]
![PALS Study Guide. PALS Study Guide Revised August 2010, Page 1 [TCL]](/thumbs/26/7254148.jpg "PALS Study Guide. PALS Study Guide Revised August 2010, Page 1 [TCL]") PALS Study Guide Course Overview This Study Guide is an extensive outline of content that will be taught in the American Heart Association Accredited Pediatric Advanced Life Support (PALS) Course. It is
PALS Study Guide Course Overview This Study Guide is an extensive outline of content that will be taught in the American Heart Association Accredited Pediatric Advanced Life Support (PALS) Course. It is
TENNESSEE EMERGENCY MEDICAL SERVICES PROTOCOL GUIDELINES. Index
 Introduction Definitions Index Cardiac Emergency (Adult & Pediatric) 101 Automatic External Defibrillator 102 New Onset Atrial Fibrillation and Flutter 103 Bradycardia 104 Acute Coronary Syndrome/STEMI
Introduction Definitions Index Cardiac Emergency (Adult & Pediatric) 101 Automatic External Defibrillator 102 New Onset Atrial Fibrillation and Flutter 103 Bradycardia 104 Acute Coronary Syndrome/STEMI
ACLS Cardiac Arrest Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767
 ACLS Cardiac Arrest Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767 Copyright 2010 American Heart Association ACLS Cardiac Arrest Circular Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767
ACLS Cardiac Arrest Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767 Copyright 2010 American Heart Association ACLS Cardiac Arrest Circular Algorithm Neumar, R. W. et al. Circulation 2010;122:S729-S767
The American Heart Association Guidelines Including Pediatric Resuscitation
 Lesson 3 The American Heart Association Guidelines Including Pediatric Resuscitation Sharon E. Mace, MD, FACEP, FAAP Objectives On completion of this lesson, you should be able to: 1. List the correct
Lesson 3 The American Heart Association Guidelines Including Pediatric Resuscitation Sharon E. Mace, MD, FACEP, FAAP Objectives On completion of this lesson, you should be able to: 1. List the correct
Atrial & Junctional Dysrhythmias
 Atrial & Junctional Dysrhythmias Atrial & Junctional Dysrhythmias Atrial Premature Atrial Complex Wandering Atrial Pacemaker Atrial Tachycardia (ectopic) Multifocal Atrial Tachycardia Atrial Flutter Atrial
Atrial & Junctional Dysrhythmias Atrial & Junctional Dysrhythmias Atrial Premature Atrial Complex Wandering Atrial Pacemaker Atrial Tachycardia (ectopic) Multifocal Atrial Tachycardia Atrial Flutter Atrial
Southern Stone County Fire Protection District Emergency Medical Protocols
 TITLE Pediatric Medical Assessment PM 2.4 Confirm scene safety Appropriate body substance isolation procedures Number of patients Nature of illness Evaluate the need for assistance B.L.S ABC s & LOC Focused
TITLE Pediatric Medical Assessment PM 2.4 Confirm scene safety Appropriate body substance isolation procedures Number of patients Nature of illness Evaluate the need for assistance B.L.S ABC s & LOC Focused
Summary of State Emergency Medical Control Committee (SEMCC) Approved Protocol Revisions September 1, 2015 NALOXONE
 Approved Protocol Revisions September 1, 2015 NALOXONE") October 22, 2015 Summary of State Emergency Medical Control Committee (SEMCC) Approved Protocol Revisions September 1, 2015 NALOXONE Summary: Expand Naloxone down to the Emergency Medical Technician (EMT)
October 22, 2015 Summary of State Emergency Medical Control Committee (SEMCC) Approved Protocol Revisions September 1, 2015 NALOXONE Summary: Expand Naloxone down to the Emergency Medical Technician (EMT)
The management of cardiac arrest
 CHAPTER 6 The management of cardiac arrest LEARNING OBJECTIVES In this chapter you will learn: How to assess the cardiac arrest rhythm and perform advanced life support 6.1. INTRODUCTION Cardiac arrest
CHAPTER 6 The management of cardiac arrest LEARNING OBJECTIVES In this chapter you will learn: How to assess the cardiac arrest rhythm and perform advanced life support 6.1. INTRODUCTION Cardiac arrest
Success Manual and Cheat Sheet Notes to Pass Your Basic Life Support (BLS) Course
 Course") Success Manual and Cheat Sheet Notes to Pass Your Basic Life Support (BLS) Course Written by: Jay Snaric, MS And Kimberly Hickman, RN CPR St. Louis 44 Meramec Valley Plaza St. Louis MO 63088 www.stlcpr.com
Success Manual and Cheat Sheet Notes to Pass Your Basic Life Support (BLS) Course Written by: Jay Snaric, MS And Kimberly Hickman, RN CPR St. Louis 44 Meramec Valley Plaza St. Louis MO 63088 www.stlcpr.com
New Approaches for Prehospital Cardiac Arrest Management 2010 NCEMSF Conference
 New Approaches for Prehospital Cardiac Arrest Management 2010 NCEMSF Conference Mark E. Pinchalk, MS, EMT-P Paramedic Crew Chief City of Pittsburgh EMS Out of Hospital Cardiac Arrest Poor outcomes: Arizona
New Approaches for Prehospital Cardiac Arrest Management 2010 NCEMSF Conference Mark E. Pinchalk, MS, EMT-P Paramedic Crew Chief City of Pittsburgh EMS Out of Hospital Cardiac Arrest Poor outcomes: Arizona
HOW TO USE THE LIFEPAK 1000 DEFIBRILLATOR 3
 3 How to Use the LIFEPAK 1000 Defibrillator HOW TO USE THE LIFEPAK 1000 DEFIBRILLATOR 3 This section provides an overview of information and instructions for using the LIFEPAK 1000 defibrillator. Modes
3 How to Use the LIFEPAK 1000 Defibrillator HOW TO USE THE LIFEPAK 1000 DEFIBRILLATOR 3 This section provides an overview of information and instructions for using the LIFEPAK 1000 defibrillator. Modes
TO GET PAST THE 2 HARDEST STATIONS AT STATE PARAMEDIC BOARDS
 A REVIEW OF THE 2 CARDIOLOGY STATIONS: WHAT TO SAY & WHAT TO DO TO GET PAST THE 2 HARDEST STATIONS AT STATE PARAMEDIC BOARDS VERSION 8 AHA ECC 2005 STANDARD---BY JAMES ROFF PARAMEDIC GRADUATE PREPARATION
A REVIEW OF THE 2 CARDIOLOGY STATIONS: WHAT TO SAY & WHAT TO DO TO GET PAST THE 2 HARDEST STATIONS AT STATE PARAMEDIC BOARDS VERSION 8 AHA ECC 2005 STANDARD---BY JAMES ROFF PARAMEDIC GRADUATE PREPARATION
Percent pulseless cardiac events monitored or witnessed (pediatric patients): Percent of pulseless cardiac events monitored or witnessed
: Percent of pulseless cardiac events monitored or witnessed") RESUSCITATION RFACT SHEET Get With The Guidelines -Resuscitation is the American Heart Association s collaborative quality improvement program demonstrated to improve adherence to evidence-based care of
RESUSCITATION RFACT SHEET Get With The Guidelines -Resuscitation is the American Heart Association s collaborative quality improvement program demonstrated to improve adherence to evidence-based care of
Advanced Cardiovascular Life Support Case Scenarios
 Advanced Cardiovascular Life Support Case Scenarios ACLS Respiratory Arrest Case Out-of-Hospital Scenario You are a paramedic and respond to the scene of a possible cardiac arrest. A young man lies motionless
Advanced Cardiovascular Life Support Case Scenarios ACLS Respiratory Arrest Case Out-of-Hospital Scenario You are a paramedic and respond to the scene of a possible cardiac arrest. A young man lies motionless
Adult, Child, and Infant Written Exam CPR Pro for the Professional Rescuer
 Adult, Child, and Infant Written Exam CPR Pro for the Professional Rescuer Instructions: Read each of the following questions carefully and then place an X over the correct answer on the separate answer
Adult, Child, and Infant Written Exam CPR Pro for the Professional Rescuer Instructions: Read each of the following questions carefully and then place an X over the correct answer on the separate answer
AMERICAN HEART ASSOCIATION 2010 ACLS GUIDELINES: WHAT EVERY CLINICIAN NEEDS TO KNOW
 AMERICAN HEART ASSOCIATION 2010 ACLS GUIDELINES: WHAT EVERY CLINICIAN NEEDS TO KNOW Joseph Heidenreich, MD Texas A&M Health Science Center Scott & White Memorial Hospital Scott & White Memorial Hospital
AMERICAN HEART ASSOCIATION 2010 ACLS GUIDELINES: WHAT EVERY CLINICIAN NEEDS TO KNOW Joseph Heidenreich, MD Texas A&M Health Science Center Scott & White Memorial Hospital Scott & White Memorial Hospital
404 Section 5 Shock and Resuscitation. Scene Size-up. Primary Assessment. History Taking
 404 Section 5 and Resuscitation Scene Size-up Scene Safety Mechanism of Injury (MOI)/ Nature of Illness (NOI) Ensure scene safety and address hazards. Standard precautions should include a minimum of gloves
404 Section 5 and Resuscitation Scene Size-up Scene Safety Mechanism of Injury (MOI)/ Nature of Illness (NOI) Ensure scene safety and address hazards. Standard precautions should include a minimum of gloves
8 Peri-arrest arrhythmias
 8 Peri-arrest arrhythmias Introduction Cardiac arrhythmias are relatively common in the peri-arrest period. They are common in the setting of acute myocardial infarction and may precipitate ventricular
8 Peri-arrest arrhythmias Introduction Cardiac arrhythmias are relatively common in the peri-arrest period. They are common in the setting of acute myocardial infarction and may precipitate ventricular
BLS: basic cardiac life support. ACLS: advanced cardiac life support. PALS: paediatric advanced life support. VF: ventricular fibrillation
 RN-Initiated Emergency Cardiac Care: Decision Support Tool #2 Emergency Cardiac Care in Areas Using Cardiac Monitoring, Defibrillation and Emergency Cardiac Drugs Decision support tools are evidenced-based
RN-Initiated Emergency Cardiac Care: Decision Support Tool #2 Emergency Cardiac Care in Areas Using Cardiac Monitoring, Defibrillation and Emergency Cardiac Drugs Decision support tools are evidenced-based
How you can help save lives
 How you can help save lives Through Life Support Training Courses with THE INTERNATIONAL LIFE SUPPORT TRAINING CENTER (ILSTC) TABLE OF CONTENTS Introduction Page 3 Basic Life Support for Healthcare Provider
How you can help save lives Through Life Support Training Courses with THE INTERNATIONAL LIFE SUPPORT TRAINING CENTER (ILSTC) TABLE OF CONTENTS Introduction Page 3 Basic Life Support for Healthcare Provider
Emergency Medical Services Advanced Level Competency Checklist
 Emergency Services Advanced Level Competency Checklist EMS Service: Current License in State of Nebraska: # (Copy of license kept in file at station) Date of joining EMS Service: EMS Service Member Name:
Emergency Services Advanced Level Competency Checklist EMS Service: Current License in State of Nebraska: # (Copy of license kept in file at station) Date of joining EMS Service: EMS Service Member Name:
BLS for Healthcare Providers Study Guide and Pretest
 BLS for Healthcare Providers Study Guide and Pretest Adult CPR 1-Rescuer CPR Sequence check for responsiveness if no response, activate 911 and get the AED open the airway look, listen, & feel for breathing
BLS for Healthcare Providers Study Guide and Pretest Adult CPR 1-Rescuer CPR Sequence check for responsiveness if no response, activate 911 and get the AED open the airway look, listen, & feel for breathing
American Heart Association
 American Heart Association Basic Life Support for Healthcare Providers Pretest April 2006 This examination to be used only as a PRECOURSE TEST For BLS for Healthcare Providers Courses 2006 American Heart
American Heart Association Basic Life Support for Healthcare Providers Pretest April 2006 This examination to be used only as a PRECOURSE TEST For BLS for Healthcare Providers Courses 2006 American Heart
EMBARGOED FOR RELEASE
 Systems of Care and Continuous Quality Improvement Universal elements of a system of care have been identified to provide stakeholders with a common framework with which to assemble an integrated resuscitation
Systems of Care and Continuous Quality Improvement Universal elements of a system of care have been identified to provide stakeholders with a common framework with which to assemble an integrated resuscitation
Procedure -8. Intraosseous Infusion Adult and Pediatric EZIO. Page 1 of 7 APPROVED:
 Page 1 of 7 Intraosseous Infusion Adult and Pediatric APPROVED: EMS Medical Director EMS Administrator 1. Goals/Introduction: 1.1 Intraosseous (IO) infusion provides an effective alternative means of providing
Page 1 of 7 Intraosseous Infusion Adult and Pediatric APPROVED: EMS Medical Director EMS Administrator 1. Goals/Introduction: 1.1 Intraosseous (IO) infusion provides an effective alternative means of providing
R Series Quick Reference Guide
 R Series Quick Reference Guide 2010 ZOLL Medical Corporation. All rights reserved. CPR Index, OneStep, R Series, Real CPR Help, See-Thru CPR, statpadz, and ZOLL are trademarks or registered trademarks
R Series Quick Reference Guide 2010 ZOLL Medical Corporation. All rights reserved. CPR Index, OneStep, R Series, Real CPR Help, See-Thru CPR, statpadz, and ZOLL are trademarks or registered trademarks
PEDIATRIC GUIDELINES
 PEDIATRIC GUIDELINES Southwest CT EMS,coord. Rev. 4/07 5-01 Guidelines For Pediatric Care Page 1 of 1 5-01 GUIDELINES FOR PEDIATRIC CARE I. Cardiac arrest in children is not a sudden event. It is almost
PEDIATRIC GUIDELINES Southwest CT EMS,coord. Rev. 4/07 5-01 Guidelines For Pediatric Care Page 1 of 1 5-01 GUIDELINES FOR PEDIATRIC CARE I. Cardiac arrest in children is not a sudden event. It is almost
Chapter 16. Learning Objectives. Learning Objectives 9/11/2012. Shock. Explain difference between compensated and uncompensated shock
 Chapter 16 Shock Learning Objectives Explain difference between compensated and uncompensated shock Differentiate among 5 causes and types of shock: Hypovolemic Cardiogenic Neurogenic Septic Anaphylactic
Chapter 16 Shock Learning Objectives Explain difference between compensated and uncompensated shock Differentiate among 5 causes and types of shock: Hypovolemic Cardiogenic Neurogenic Septic Anaphylactic
2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Presenter Name Disclosures
2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Presenter Name Disclosures
Oxygen - update April 2009 OXG
 PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
Paediatric Advanced Life Support
 Paediatric Advanced Life Support Introduction There is concern that resuscitation from cardiac arrest is not performed as well as it might because the variations in guidelines for different age groups
Paediatric Advanced Life Support Introduction There is concern that resuscitation from cardiac arrest is not performed as well as it might because the variations in guidelines for different age groups
AEC: INTERMEDIATE to PARAMEDIC PROGRAM MONDAY/WEDNESDAY @ AEC TRAINING CENTER OCTOBER 22, 2015 through JULY 23, 2016
 AEC: INTERMEDIATE to PARAMEDIC PROGRAM MONDAY/WEDNESDAY @ AEC TRAINING CENTER OCTOBER 22, 2015 through JULY 23, 2016 Thursday 10/22/15 9a-4p 10/24/15 Orientation/Introduction Ground Ambulance Operations
AEC: INTERMEDIATE to PARAMEDIC PROGRAM MONDAY/WEDNESDAY @ AEC TRAINING CENTER OCTOBER 22, 2015 through JULY 23, 2016 Thursday 10/22/15 9a-4p 10/24/15 Orientation/Introduction Ground Ambulance Operations
Resuscitation Patient Management Tool May 2015 CPA Event
 OPTIONAL: Local Event ID: Did pt. receive chest compressions and/or defibrillation during this event? criteria) (does NOT meet inclusion Date/Time the need for chest compressions ( or defibrillation when
OPTIONAL: Local Event ID: Did pt. receive chest compressions and/or defibrillation during this event? criteria) (does NOT meet inclusion Date/Time the need for chest compressions ( or defibrillation when
THE REGIONAL EMERGENCY MEDICAL ADVISORY COMMITTEE NEW YORK CITY PREHOSPITAL TREATMENT PROTOCOLS ADVANCED LIFE SUPPORT (PARAMEDIC) PROTOCOLS
 PROTOCOLS") THE REGIONAL EMERGENCY MEDICAL ADVISORY COMMITTEE NEW YORK CITY PREHOSPITAL TREATMENT PROTOCOLS ADVANCED LIFE SUPPORT (PARAMEDIC) PROTOCOLS July 2012 Version 07012012 The Regional Emergency Medical Services
THE REGIONAL EMERGENCY MEDICAL ADVISORY COMMITTEE NEW YORK CITY PREHOSPITAL TREATMENT PROTOCOLS ADVANCED LIFE SUPPORT (PARAMEDIC) PROTOCOLS July 2012 Version 07012012 The Regional Emergency Medical Services
Alabama Medications. Christopher J. Colvin January 2010
 Alabama Medications Christopher J. Colvin p January 2010 Activated Charcoal Used to absorb toxins ingested before they can be absorbed in the GI system. Contraindicated in AMS patients who cannot control
Alabama Medications Christopher J. Colvin p January 2010 Activated Charcoal Used to absorb toxins ingested before they can be absorbed in the GI system. Contraindicated in AMS patients who cannot control
Paramedic Pediatric Medical Math Test
 Paramedic Pediatric Medical Math Test Name: Date: Problem 1 Your 4 year old pediatric patient weighs 40 pounds. She is febrile. You need to administer acetaminophen (Tylenol) 15mg/kg. How many mg will
Paramedic Pediatric Medical Math Test Name: Date: Problem 1 Your 4 year old pediatric patient weighs 40 pounds. She is febrile. You need to administer acetaminophen (Tylenol) 15mg/kg. How many mg will
Canine Tactical Combat Casualty Care
 Canine Tactical Combat Casualty Care The following C-TCC guidelines are based on human C-TCCC guidelines and the limited data available on combat injuries and field treatment of working dogs. These guideline
Canine Tactical Combat Casualty Care The following C-TCC guidelines are based on human C-TCCC guidelines and the limited data available on combat injuries and field treatment of working dogs. These guideline
Tachyarrhythmias (fast heart rhythms)
") Patient information factsheet Tachyarrhythmias (fast heart rhythms) The normal electrical system of the heart The heart has its own electrical conduction system. The conduction system sends signals throughout
Patient information factsheet Tachyarrhythmias (fast heart rhythms) The normal electrical system of the heart The heart has its own electrical conduction system. The conduction system sends signals throughout
Practical ACLS Megacode Testing and Training Scenario Set for SimPad. Consolidated Instructor Manual. Frances Wickham Lee, DBA
 Practical ACLS Megacode Testing and Training Scenario Set for SimPad Consolidated Instructor Manual Frances Wickham Lee, DBA Scenario Authors: Frances Wickham Lee, DBA John Walker, BHS John Schaefer, MD
Practical ACLS Megacode Testing and Training Scenario Set for SimPad Consolidated Instructor Manual Frances Wickham Lee, DBA Scenario Authors: Frances Wickham Lee, DBA John Walker, BHS John Schaefer, MD
PARAMEDIC TRAINING CLINICAL OBJECTIVES
 Page 1 of 21 GENERAL PATIENT UNIT When assigned to the General Patient unit paramedic student should gain knowledge and experience in the following: 1. Appropriate communication with patients and members
Page 1 of 21 GENERAL PATIENT UNIT When assigned to the General Patient unit paramedic student should gain knowledge and experience in the following: 1. Appropriate communication with patients and members
BASIC LIFE SUPPORT - ADULT
 BASIC LIFE SUPPORT - ADULT First Issued by/date BKW PCT May 2003 Issue Version Purpose of Issue/Description of Change 3 Policy reviewed. No changes in procedure or legislation since policy revised 12 months
BASIC LIFE SUPPORT - ADULT First Issued by/date BKW PCT May 2003 Issue Version Purpose of Issue/Description of Change 3 Policy reviewed. No changes in procedure or legislation since policy revised 12 months
Airway and Breathing Skills Levels Interpretive Guidelines
 Office of Emergency Medical Services and Trauma INDEX EFFECTIVE LAST REVIEW PAGES VERSION R-P11A 7/1/2011 7/1/2011 5 2011 Scope of Practice for EMS Personnel Emergency Medical Personnel are permitted to
Office of Emergency Medical Services and Trauma INDEX EFFECTIVE LAST REVIEW PAGES VERSION R-P11A 7/1/2011 7/1/2011 5 2011 Scope of Practice for EMS Personnel Emergency Medical Personnel are permitted to
Oxygen Therapy. Oxygen therapy quick guide V3 July 2012.
 PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
EMS Course Requirements
 EMS Course Requirements The following outlines should be followed when creating your course syllabi. The minimum course hours must be met, but they can be exceeded depending on the needs of your class.
EMS Course Requirements The following outlines should be followed when creating your course syllabi. The minimum course hours must be met, but they can be exceeded depending on the needs of your class.
Inotropes/Vasoactive Agents Hina N. Patel, Pharm.D., BCPS Cathy Lawson, Pharm.D., BCPS
 Inotropes/Vasoactive Agents Hina N. Patel, Pharm.D., BCPS Cathy Lawson, Pharm.D., BCPS 1. Definition -an agent that affects the contractility of the heart -may be positive (increases contractility) or
Inotropes/Vasoactive Agents Hina N. Patel, Pharm.D., BCPS Cathy Lawson, Pharm.D., BCPS 1. Definition -an agent that affects the contractility of the heart -may be positive (increases contractility) or
ANZCOR Guideline 12.4 Medications and Fluids in Paediatric Advanced Life Support
 ANZCOR Guideline 12. Medications and Fluids in Paediatric Advanced Life Support Who does this guideline apply to? This guideline applies to infants and children. Summary Who is the audience for this guideline?
ANZCOR Guideline 12. Medications and Fluids in Paediatric Advanced Life Support Who does this guideline apply to? This guideline applies to infants and children. Summary Who is the audience for this guideline?
American Heart Association. BLS Instructor Course. Written Examination. July 2003
 American Heart Association BLS Instructor Course Written Examination July 2003 Basic Life Support Instructor Exam Part I Please do not mark on this examination. Record the best answer on the separate answer
American Heart Association BLS Instructor Course Written Examination July 2003 Basic Life Support Instructor Exam Part I Please do not mark on this examination. Record the best answer on the separate answer
Cardiac arrest management Connie J. Mattera, NWC EMSS
 Stayin alive Contemporary Cardiac Arrest Management Connie J. Mattera, M.S., R.N., EMT-P CMATTERA@nch.org www.nwcemss.org Upon completion the participant will identify priorities of care for pts in cardiac
Stayin alive Contemporary Cardiac Arrest Management Connie J. Mattera, M.S., R.N., EMT-P CMATTERA@nch.org www.nwcemss.org Upon completion the participant will identify priorities of care for pts in cardiac
GUIDELINE 11.9 MANAGING ACUTE DYSRHYTHMIAS. (To be read in conjunction with Guideline 11.7 Post-Resuscitation Therapy in Adult Advanced Life Support)
") AUSTRALIAN RESUSCITATION COUNCIL GUIDELINE 11.9 MANAGING ACUTE DYSRHYTHMIAS (To be read in conjunction with Guideline 11.7 Post-Resuscitation Therapy in Adult Advanced Life Support) The term cardiac arrhythmia
AUSTRALIAN RESUSCITATION COUNCIL GUIDELINE 11.9 MANAGING ACUTE DYSRHYTHMIAS (To be read in conjunction with Guideline 11.7 Post-Resuscitation Therapy in Adult Advanced Life Support) The term cardiac arrhythmia
ACLS Defibrillation Protocols With the ZOLL Rectilinear Biphasic Waveform AHA/ERC Guidelines 2005
 ACLS Defibrillation Protocols With the ZOLL Rectilinear Biphasic Waveform AHA/ERC Guidelines 2005 Introduction: The purpose of this document is to outline the equivalent biphasic protocols specific to
ACLS Defibrillation Protocols With the ZOLL Rectilinear Biphasic Waveform AHA/ERC Guidelines 2005 Introduction: The purpose of this document is to outline the equivalent biphasic protocols specific to
Adding IV Amiodarone to the EMS Algorithm for Cardiac Arrest Due to VF/Pulseless VT
 Adding IV Amiodarone to the EMS Algorithm for Cardiac Arrest Due to VF/Pulseless VT Introduction Before the year 2000, the traditional antiarrhythmic agents (lidocaine, bretylium, magnesium sulfate, procainamide,
Adding IV Amiodarone to the EMS Algorithm for Cardiac Arrest Due to VF/Pulseless VT Introduction Before the year 2000, the traditional antiarrhythmic agents (lidocaine, bretylium, magnesium sulfate, procainamide,
National Registry of Emergency Medical Technicians Emergency Medical Technician Psychomotor Examination BLEEDING CONTROL/SHOCK MANAGEMENT
 BLEEDING CONTROL/SHOCK MANAGEMENT Candidate: Examiner: Date: Signature: Possible Applies direct pressure to the wound 1 NOTE: The examiner must now inform the candidate that the wound continues to bleed.
BLEEDING CONTROL/SHOCK MANAGEMENT Candidate: Examiner: Date: Signature: Possible Applies direct pressure to the wound 1 NOTE: The examiner must now inform the candidate that the wound continues to bleed.