Post-cold war United Nations peacekeeping operations: a review of the case for a hybrid level 2+ medical treatment facility
|
|
|
- Trevor McGee
- 8 years ago
- Views:
Transcription
1 Disaster and Military Medicine This Provisional PDF corresponds to the article as it appeared upon acceptance. Fully formatted PDF and full text (HTML) versions will be made available soon. Post-cold war United Nations peacekeeping operations: a review of the case for a hybrid level 2+ medical treatment facility Disaster and Military Medicine Sample (2015) 1:15 doi: /s z Ralph Jay Johnson (ralph.j.johnson16.mil@mail.mil) Sample ISSN X Article type Review Submission date 3 June 2015 Acceptance date 25 June 2015 Article URL For information about publishing your research in BioMed Central journals, go to Johnson This is an Open Access article distributed under the terms of the Creative Commons Attribution License ( which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited. The Creative Commons Public Domain Dedication waiver ( applies to the data made available in this article, unless otherwise stated.

2 Post-cold war United Nations peacekeeping operations: a review of the case for a hybrid level 2+ medical treatment facility Abstract Ralph Jay Johnson III 1* * Corresponding author ralph.j.johnson16.mil@mail.mil 1 Bravo Branch, 1st BDE, 1 Southern Training Division, 75th Training Command, Aerospace Ave., Houston, TX 77034, USA Post-Cold War, UN peacekeeping operations (UN PKOs) have become larger, more mobile, multi-faceted and conducted over vast areas of remote, rugged, and harsh geography. They have been increasingly involved in dangerous areas with ill-defined boundaries, simmering internecine armed conflict, and disregard on the part of some local parties for peacekeepers security and role. Yet progressively there have been expectations of financial restraint and austerity. Additionally, UN PKOs have become more robust, that is, engaged in preemptive, assertive operations. A statistically positive and significant relationship exists between missions size, complexity, remoteness, and aggressive tenor and a higher probability of trauma or death, especially as a result of hostile actions or disease. Therefore, in the interest of force protection and optimizing operations, a key component of UN PKOs is health care and medical treatment. The expectation is that UN PKO medical support must conform to the general intent and structure of current UN PKOs to become more streamlined, portable, mobile, compartmentalized, and specialized, but also more varied and complex to address the medical aspects of these missions cost-efficiently. This article contends that establishing a hybrid level 2 a level 2 with level 3 modules and components (i.e., level 2+) is a viable course of action when considering trends in the medical aspects of Post-Cold War UN PKOs. A level 2 medical treatment facility has the potential to provide needed forward mobile medical treatment, especially trauma care, for extended, complex, largescale, and comprehensive UN PKOs. This is particularly the case for missions that include humanitarian outreach, preventive medicine, and psychiatry. The level 2 treatment facility is flexible enough to expand into a hybrid level 2+ with augmentation of modules based on changes in mission requirements and variation in medical aspects. Keywords Post-cold war, United Nations, Peacekeeping operations, Peacekeepers, Military medical care, Military medical treatment, Tiers, Echelons, Levels

3 Introduction An essential element of United Nation s peacekeeping operations (UN PKOs) is provision of health services in support of mission personnel in areas of operations [1]. The overall objective of medical support is the physical and mental well-being of deployed personnel, conservation of human resources, preservation of life, and limitation of residual physical and mental disabilities. A nascent understanding suggests that quality health service means that planning, coordination, execution, monitoring, and professional supervision impacts the health and well-being of mission members and ultimately the mission s successful execution [2]. Arguably, peacekeepers operate better when they are healthy and know that high-quality medical treatment is available in case of injury or illness. Nevertheless, UN PKOs are becoming increasingly mobile over wide swaths of rugged/remote geographic areas to meet extensive and varied multi-dimensional mandates all while facing considerable financial constraints [3 5]. Also, UN PKOs are operating in hostile environments with poorly defined boundaries, continued armed conflict, and scant assurance of respect for their safety. To manage and treat sizable numbers of casualties, military medicine, including UN PKOs, uses a planning technique involving echelons ( levels ) of care to reduce the task of providing medical treatment to manageable proportions [6, 7]. Levels of care represent a framework for rational, practical, and efficient deployment of medical resources in support of missions. This framework developed from the premise that casualties occur in places remote from care facilities and these patients must be treated and sheltered at staging points before evacuation. Thus, a medical event or condition is addressed at a level of care that offers the necessary sophistication in skills and complexity in technology and materials. If it cannot be addressed at one level, the patient is moved to a higher level. Thus, a system was instituted for progressive care and five echelons of care were recognized (basic plus levels 1 4). The effectiveness of treatment is enhanced by a division of labor and standardized treatment at each echelon. Minor casualties are preempted early so that serious casualties can receive better treatment. A nagging problem with the system has been a lack of suitable facilities to treat emergencies in forward areas of operations. Casualties are transported long distances with consequent risk. The Medical Support Manual for United Nations Peacekeeping Operations (2nd ed.) notes that levels of medical support have been standardized to ensure the highest standards of peacekeeping medical care come from different countries with varying standards medical support plans must be designed to meet specific operations demands [1]. In this system, the level 2 mobile medical hospital, though mobile, portable, and flexible, is the consequence of deploying a tiered system that evolved from experience in sustaining sizable pre-cold War UN PKOs that were relatively fixed/static and linear. However, reliance on level 2 mobile facilities is also the consequence of a tiered system with increasing complexity that also can rely on the level 3 fixed-facility hospital (or transport out-of-country to such a facility) for extensive diagnostics, trauma surgery, specialist care, and long-term medical care capabilities [8, 9]. In some cases, level 3 facilities have not been deployed and their medical capabilities have rarely been deployed fully. Such care has been obtained from an existing civilian hospital in or near the area of operations or a military hospital in a neighboring stable nation [1]. Previously, UN PKO components had their own basic, level 1, and level 2 medical personnel. Nevertheless, UN PKO missions have attempted to provide a standalone, central level 2 mobile hospital from a troop-contributing nation. These facilities, while relatively

4 fixed/static, can provide mobile care in dynamic operations [10]. However, as the complexity of operations has increased, the need to fix quarters and provide more sophisticated medical capabilities has also increased, thus decreasing mobility. It has always been difficult to balance capabilities and mobility. Smaller mobile medical facilities still need some assets and personnel assigned to larger fixed facilities and remote hospitals despite sacrificing some mobility. That is, to offset any reduction in mobility, the most mobile and mission-essential assets from level 3 augment level 2 and even level 1 [11]. That said, the level 2 mobile hospital remains the standard, mainstay, workhorse, and lynchpin for relatively large-scale UN PKOs in various theaters. The result is lower levels of medical care relying heavily on non-organic transportation personnel to ensure movement and through-put so that care arrives where needed and need is transported to where care can be provided [12, 13]. Movement, in particular patient transport, always incurs risks. Furthermore, UN PKOs are increasingly involved in remote failed states [14]. The local incountry hospitals that could have been used for level 3 care and even remote military hospitals in neighboring so-called stable nations are compromised. Their use for UN personnel is not feasible in that they are poorly equipped and incapable of providing many basic services, medical emergent stabilization services are limited, blood supplies are unavailable, tainted, and even non-existent, and medicines, if even available, are expired, and there is poor sanitation and hygiene [15]. This situation leads to even lengthier and more expensive transports for relatively routine medical procedures as well as catastrophic emergencies needing higher than level 2 care. This then overburdens the transport system; it also affects peacekeeper downtime when peacekeepers cannot return to duty quickly after routine procedures. The situation is even further complicated because UN PKO personnel operate in environments marked by poor sanitation, as well as water- and food-borne vectors and illnesses, and are at high risk for infectious and debilitating diseases [16 20]. Thus, preventive medicine a level 3 commodity is absolutely necessary in remote areas of operation (at level 2 or 1) to advance force protection and civil-military cooperation. The hope is that UN PKOs will become streamlined, faster, more efficient, and more capable so as to be involved in more wide-ranging, multi-faceted operations conducted over large, diverse, and remote geographic areas. Simply put, there are hopes to structure slow and cumbersome processes to quickly respond to emergent crises (cf. [21]). Consequently, medical support is also likely to conform to the larger structure of the UN PKO. Medical support will become smaller, more portable and mobile, more compartmentalized, and more specialized (i.e., modular) to establish itself more quickly in areas of operations. Also, in response to harsh and unforgiving environments, UN PKOs may need to become more selfsufficient and insular (cf. [22]). Therefore, through a review of open sourced research and doctrine, this article contends that a hybrid level 2 medical treatment facility augmented with proper services and modules is the most promising option when accounting for post-cold War trends in the medical aspects of UN PKOs. Risk and trauma have been escalating rapidly, whereas the response has come too late. It is hoped that this report will enable planners and policymakers in more quickly enhancing medical support to UN PKOs and better ensure the health and well-being of UN PKO members, which has increasingly included among the world s militaries. Better health and well-being of UN PKO members is the ideal in medical support ensconced in the UN s medical mission statement.

5 Review Medical aspects Johnson [23 25] reported on the medical aspects of post-cold War UN PKO missions, summarized as follows. (1). UN PKOs are expanded and more robust in post-cold War affairs. They have been and can expect to (1) be conducted in the world s rugged, inhospitable, and inherently dangerous peripheries, primarily on the margins of the Third and Fourth Worlds, (2) involve less benign handovers from unfinished security missions, (3) have questionable consent by belligerents to the peace process and simmering conflicts ready to boil, and (4) draw peacekeepers into hostile action or becoming victims of remote explosive devices. (2). The medical events that UN PKO medical support staff encounters, therefore, will increasingly resemble combat trauma and include exotic and debilitating illnesses. (3). Thus, the conundrum that medical commands face is whether to (1) move medical treatment to patients in the forward area of operations and risk their medical personnel, (2) move patients back to medical treatment with risk to the patients, or (3) strike a practical compromise in between. (4). Additionally, the peripheries in which post-cold War UN PKOs operate have their own locally endemic exotic diseases, other inhospitable and risky features, and wicked flora and fauna. These all pose risks to UN peacekeepers, including medical personnel. This demands preventive medical measures throughout the area of operations. Also, one thing is certain, civil conflict and its ancillary human tragedies are not good for the human psyche. Thus, psychiatric medicine is needed. (5). Furthermore, the demand for civil/military-driven humanitarian medical outreach far into the margins of already risky and dangerous situations adds a new and dangerous dimension to UN PKO missions and their medical components. (6). This creates a need for generalist/family practice medical professionals and medical subspecialties, particularly surgical sub-specialties. As civilians in particular, women and children are caught in the middle of all this, there will be more emphasis on women s and family health issues. So there is an expanded need for women health professionals and family practitioners, in particular in cultures that prohibit cross-gender contact. (7). In addition, as expanded post-cold War UN PKO missions grind on, attrition in medical staffs will require a reserve back-fill system. The downside is that deployed augmentees are at higher risk for psychological morbidities and may be less physically fit for in-thefield austerities. Need for a modified level 2 medical treatment facility The literature on medical aspects of expanded and more robust post-cold War UN PKOs suggests the need for field medical treatment support capable of moving itself, while retaining the ability to deliver varied medical care at different levels. This must be accomplished to provide medical treatment in far forward areas of operations, especially trauma care, which sustains (1) extended and comprehensive operations, (2) maneuvers, and (3) humanitarian outreach. A modified UN PKO level 2 facility can provide the necessary bed capacity for trauma and intermediate care for casualties resulting from hostile action, injuries, and illness [1, 26]. This facility can be variable enough to expand to include
.")
6 augmentation by medical detachments in response to changing mission requirements. Additionally, this component s far forward medical care should be upgraded consistent with U.S. and British models with medics who are (1) assigned to patient transport and other medical duties and (2) trained and certified as emergency medical technicians and paramedics or emergency practical nurses [9, 27]. For forward area units, designated squad-level military personnel should be trained and certified as combat life savers or in basic first aid. The objective is to enhance and push medical/trauma care knowledge and skills down to the forward areas of operations to improve responsiveness closer to medical emergencies. Mobility is important as medical support must move in tandem with forward area of operations peacekeepers. The level 2 facility technically is mobile and provides fundamental trauma care as a base on which modules can be plugged in for play (i.e., modularity). Specifically, this allows other specialty components to be added or subtracted as needed to offer augmentation tailored to the mission and its changing nature [28, 29]. Thus, the next generation of medical care for UN PKOs can have the flexibility to expand (or contract) to support needed medical detachments, while retaining mobility and the ability to provide comprehensive medical care, including trauma care. Note, modularity has been used and incorporated in US Armed Forces and NATO/UE procedures and doctrine and it cannot be over-emphasized that modularity of medical support is not a new concept and has been developed by US Armed Forces and NATO/UE to meet the challenges of their missions that bear striking similarity to the challenges UN PKOs have been increasingly facing in the Post- Cold War [1, 30 34]. Rather, what is relatively innovative is advocating modularity s adoption, adaptation to and expanded and practical use for medical support on UN PKOs to overcome new challenges regarding the health nuances of Post-Cold War UN PKOs. (Note: UN PKOs have never been restricted from using modular medical support either.) Level 2 facilities are in areas of operations where medical personnel are best able to intervene medically to alter what might otherwise be debilitating or fatal medical outcomes [28, 29]. They also can be augmented with health providers to care for common and endemic diseases and psychological stressors encountered in operations [9]. Level 1 components are primarily designed to treat life-threatening conditions and evacuate to level 2, possibly even level 3 or out of the country [1]. Note that under the changing conditions of UN PKO missions, level 1 medical facilities are insufficient to provide the level of care necessary to avoid out-ofcountry medical evacuation and repatriation [5, 15]. Level 2 can provide trauma care and basic medical treatment, as well as hold patients who can return to duty, and surgical teams, preventive medicine teams, and psychiatric providers alone or in combinations can be plugged into the level 2 facility depending on operations, although maintaining them at a level 3 facility is more traditional. Level 2 has no intensive care, medical supply, or extensive formulary capability [1]. However, through augmentation, level 2 can provide limited specialty care and limited pharmacy, blood, medical supply, and equipment capability. Level 2 also lacks effective operations planning, patient administration, and signal support components that only a level 3 facility provides. It can also accommodate components to address humanitarian outreach and women s healthcare. An ad hoc/hybrid level 2 facility can provide care comparable to a level 3 but cannot supplant the level 3 entirely. Future operations mission structures, such as the post-cold War expanded structures, will require basic and level 1 / 2 augmented support and need to be farther forward and nearer field units. Level 2 should acquire medical care aspects of level 3 such as preventive medicine and psychological care providers. A condensed level 3 can then concentrate on medical command for overall operations. Mission operations needs support
![nurses [9, 27]. For forward area units, designated squad-level military personnel should be trained and certified as combat life savers or in basic first aid.](/docs-images/46/321122/images/page_6.jpg "The objective is to enhance and push medical/trauma care knowledge and skills down to the forward areas of operations to improve responsiveness closer to medical emergencies.")
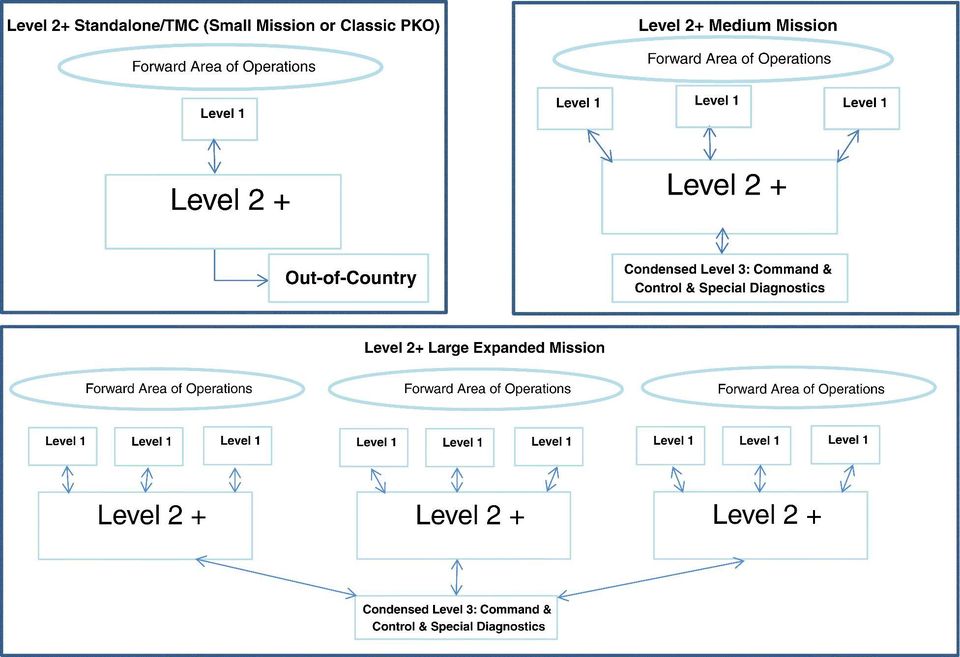
7 from a level 3 facility to provide administration and coordination. Therefore, one level 3 facility but a condensed level 3 should be assigned per mission at the command level. In future post-cold War expanded UN PKOs, the level 2 facility should be modular with the ability to expand with add-on level 3 components. This aligns with the provision of medical treatment and specialized care based on operations exigencies, hostilities, patients, terrain, and civil-military concerns. To support such UN PKOs, the unit must be tactical. Therefore, it must have the maneuverability to rapidly travel over some distance in tandem with peacekeepers. The level 2 facility arguably is the center of gravity for medical support for UN PKOs. In field operations, this component of care provides seriously hurt and ill patients with lifesaving medical intervention. It is also where patients are stabilized for evacuation out-ofoperations and even out-of-country. Thus, ground and air Medevac capabilities with highly trained medical personnel for en-route life support must still be emphasized. The UN PKO medical literature regarding PKO medical aspects suggests that future medical support should be able to move quickly over large distances and provide comprehensive coverage farther forward in tandem with mobile forward area peacekeepers. Augmented level 2 facilities provide the level of care to do this effectively. Recent operations have demonstrated that the focus of level 2 can be trauma care, followed by non-hostile injuries and then illness (if augmented by preventive medicine teams) (cf. [9, 28, 29]). Level 3 can continue to offer specialized surgical capabilities. It can also have the commandstaff and extensive medical logistics and maintenance capabilities required for sustained long-term care. Its drawback is that it lacks modular flexibility. Therefore, given the expected direction of future UN PKOs, emphasis on medical support for operations must be at the level 2 facility that also incorporates (1) preventive and psychological medicine, (2) portability and mobility, (3) medical sustainment pushed as far forward as possible, and (4) accommodation for expanded specialized care responsive to operational contingencies (e.g., humanitarian outreach and women s healthcare). This also permits modular expansion of bed capacity for larger treatment, holding, and evacuation. The mobile modular level 2+ In UN PKOs, personnel and material are available for level 2+ as attachments and augmentation building blocks for the current level 2. Level 2+ should have trauma and medical clinic (general practice) services, nursing services with psychiatric nursing resources (i.e., dual hats ), expanded pharmacy, blood supply, and expanded medical stock. Preventive medicine teams should be attached but dispatched and roving throughout the theater to address field sanitation issues, potable water acquisition, disease prevention, and non-hostile action injury reduction (cf. [16]). The command structure should retain the rank-and-staff structure of the level 2 facility with slight elevation due to its add-ons from level 3. The level 2 facility should retain the capability to expand and exceed normal bed and sub-specialty capability through modularity. It should have a commander, deputy for clinical services, director for nursing care, and administrative officer [1]. This facility should not be an amalgamation from different troopsupplying nations. Rather, it should be a unified, cohesive entity from one troop-supplying nation, capable of maintaining its own vehicles, generators, and equipment and conducting basic medical maintenance. Also, this unit must be able to communicate with field units,

8 aviation, and ground transportation and lower and higher elements. Logically, clinical services should be organized around trauma, resuscitation, and life-and-limb and eyesight sustainment with the intent to support continuous operations. There should be a provision for general and orthopedic practice as well but not extensive diagnostic capabilities, which can be maintained at level 3. At the level 2 facility, the need for trauma care is obvious, as is the need to treat most illnesses encountered in operations. This includes emergency medical treatment. Nursing services should include bed care and patient specialists. Service and supply should allow the organization to increase in size threefold. That way, if the level 2 cannot address a particular challenge, it can be expanded modularly by adding on those capabilities. It must be underscored that Post-Cold War US and NATO/EU missions and operations clearly have shown multi-nationality and sharing medical assets and appropriate practitioners combined through modularity is included in their doctrine and has contributed to the outstanding, successful medical support on their missions [30 36]. To address personnel turnover, back-fill from individual augmentees (e.g., reservists and Home Guard) may be necessary. The troop-contributing nation should manage training and pre-deployment readiness. Detachments should be from either the troop-supplying nation of the level 2+ facility or modules representing one troop-supplying nation [13]. This ensures the cohesion that develops from training and working together over time and avoids communication difficulties related to multi-national amalgamations. These modules would be capable of relatively rapid deployment. Expansion of the level 2+ would also give level 2+ leaders opportunities to develop leadership skills, work on tactical field problems, and meet operational challenges in the field [9]. Additional non-unit equipment should be available from the level 3 to the level 2+ depending on mission needs. Detachments such as humanitarian medical aid could be organized within the level 2+ and/or drawn on from the level 3. This system can facilitate a modular push forward. This would improve adaptability necessary for future UN PKOs that might have different and more particular requirements, for example: those with specific hinterland family medicine humanitarian outreach mobile clinics as described by Milosevic [37]; or, preventive medicine taskings in the peripheries as described by Hazra [16]. These modules would require fewer personnel and less equipment and be interchangeable. Ideally, several level 2 + s could be fielded in large-scale missions and coordinated by the condensed but refocused level 3 (see Fig. 1). Figure 1 Possible Level 2 + Medical Treatment Facility PK Mission Configurations Supporting this shift in medical treatment facilities, and furthering rapid deployment, will require pre-positioning, depot, cache, tracking and management, maintenance of equipment, and contracting and finance specialists. As the Liberian (ECOWAS) mission reported, every contingent, including medical units and treatment facilities, must be insular and selfsufficient such that it includes laundry, catering, accommodations, office, communications, explosive ordinance disposal (EOD), and observation [38]. This means they must be equipped to support whatever type of medical care mission they encounter. This might require extra inventory or specialized inventory for plug-in-and-play, depending on operational requirements. This also would create a redundancy of material that has proved useful in previous and prolonged operations that resulted in the need for replacement and maintenance of worn and broken equipment.

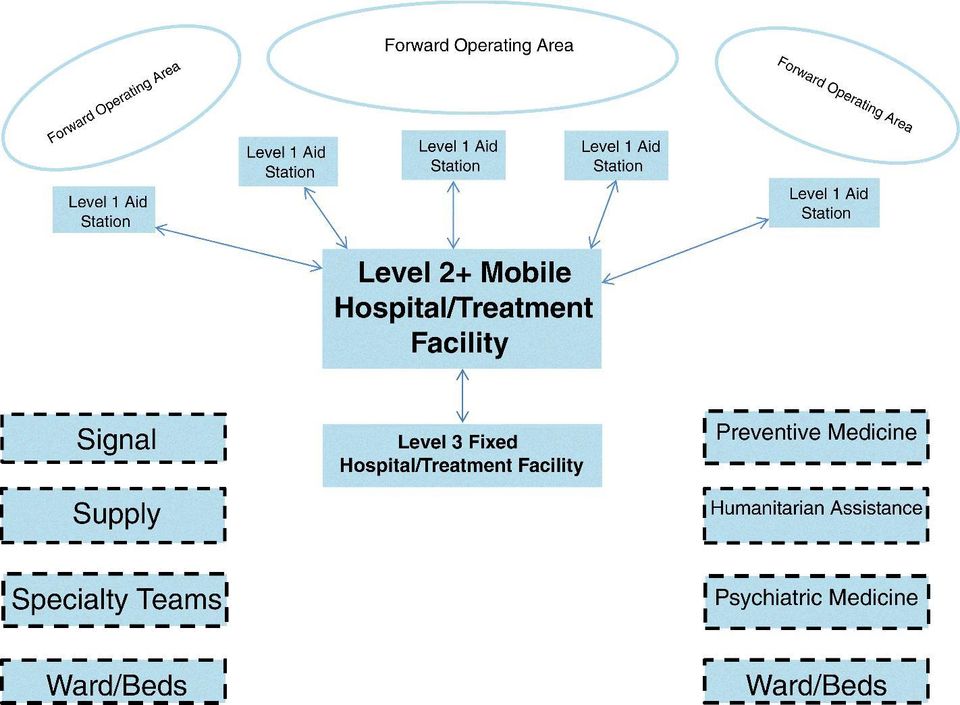
9 Conclusions Predicting the future is precarious. Nevertheless, the evidence-based work reported here suggests that a hybrid level 2+ medical facility augmented with proper services and modules is optimal and best-practices for addressing trends and medical aspects of future UN PKOs (see Fig. 2). Figure 2 Possible Theater Level 2 + Medical Treatment Facility for PK Mission(s) with Modules for Attachment or Plug-in-and-Play Figure 2 basic and level 1 medical care is a critical capability required for all UN PKOs. Level 2 is where wounded, injured, or ill patients are collected, stabilized, and treated prior to return to duty or evacuation. If past experience predicts future experience, future UN PKOs medical support will be mobile across large distances into dangerous, remote, and rugged areas. Medical care will be close-in to facilitate rapid treatment and evacuation from basic and level 1 facilities. In previous operations, it was unrealistic to rely on aero-evacuation entirely, in particular with (1) constant disruption due to inclement weather, (2) a lack of landing areas and night vision devices, and (3) even hostile anti-aircraft fire. The requirement will be a more complex and larger level 2 facility capable of moving closer to field operations. A consideration for planners will be security for medical treatment facilities in areas where conflict resolution is indeed robust. This is because the level 2 facility is a potentially vulnerable, high-value target. Another consideration is that additional modules will reduce mobility even with more transportation components. Thus, the level 2 must have more of its own transportation with the inclusion of additional modules. The recommendations discussed here have the potential to provide medical care capable of supporting UN PKOs with more mobile medical capabilities, but without the footprint of a level 3 or the need for expensive out-of-country facilities. The facility will have an appropriate size to support ad hoc small contingency operations and humanitarian outreach or special operations. The level 2+ should be an element of a troop-lending nation, train as a unit, and deploy and function intact to avoid language barriers and communication issues. [12, 13]. To interface with other personnel/units on the mission who speak a different language, interpreters may be needed. These smaller hospitals will be more easily deployed and enhanced through modularity. Modularity is achievable by implementing a system of detachments for requirements and specialties. These can come from the level 2+ s trooplending nation or self-contained detachment modules from other troop-lending nations. The point is that standards of care must be comparable and personnel must train and work together in the modules. More importantly, this provides the mission commander with flexibility in planning for particular and varied missions or in responding to mission changes. The lessons reported here convey the importance of medical care to UN PKOs. They suggest courses of action that include use of modular augmentation in the level 2 medical care for UN PKOs. This system could significantly enhance the provision of military medical care on UN PKO missions in ways that are capabilities-based and efficiently achieved with flexibility, mobility, adaptability, and expediency to accommodate particular, varied, and evolving UN PKOs. Given the direction of post-cold War UN PKO trends, the recommendations in this report should be incorporated across the spectrum of medical aspects of expanded, post-cold War-type missions. The operational component of the level 2 hospital can be modularly augmented with detachments and teams, which can be plugged in for play. At its core, it will
 with Modules for Attachment or Plug-in-and-Play Figure 2 basic and level 1 medical care is a critical capability")
10 still provide needed trauma and general practice care. The importance of the work reported here is that it provides a general conceptual approach to considerations of medical aspects across the spectrum of UN PKO missions, specifically the iterative identification of relevant medical and health aspects to UN PKO missions and planning for medical controls accordingly. In light of the changed in the nature of Post-Cold War PKOs, the argument for a change in terms of policy revision and adoption for PKO medical support described herein is a natural logical extension. The next logical extension in terms of what is to be done are steps to marshal this along. The following are possible generic steps, in a general sequential order but conducted iteratively, that at minimum can be aimed to mobilize policy and opinion. Study the requirements/standards that need to be in policy. Conduct and take into account a needs/risk assessment. Align the policy with previous policy and discard or revise un-useful policy with new policy. Involve others, especially stakeholders, in drafting of policy for maximum buy-in and to catch things in error or unworkable. Get the policy approval from the high-ranking stakeholders. Train and manage expectations on the necessity and benefit of the policy. Take care to modify and update continuously as the policy is piloted, vetted and implemented [2, 11, 39 45]. Also, there must be an assessment to the extent that recommendations grab the attention of policy makers. One lesson learned is that UN PKO medical support planning is complex; it requires more than a simple fix of additional mobility or closer proximity or the addition of this or that facet or module. Therefore, medical support plans must be purpose built for each operation. Plans (and planners) must be capable of speedy initial reaction and sufficiently flexible to manage rapidly changing demands (cf. [2]). Thus, given the experience of past UN PKOs, in addition to fundamental structural modifications, future UN PKOs will need to adopt a medical support planning mind-set that is informed by continuously updated research and aims to achieve best practices (cf. [12, 13]). The mind-set adopted for medical planning must consider and seek to strike a delicate balance in the trinity of proximity to medical care, time involved in transporting, and security given the nature of UN PKOs. Medical capabilities must correspond to the mission, strength, and composition of the force they support and the assessed environmental hazards they face. Finally, the paucity of research on which to base an evidence-based review of structural and procedural modifications for UN PKOs and non-war military interventions literally cries for the need for more open-sourced, peer-reviewed work in this arena. Not only does the peerreview process add credibility to findings and patina to the finished product, but incorporation into and citations in other research and critical response are indicators of the extent to which the recommendations actually have engaged policy makers.

11 Competing interests The author reports no conflicts of interest. The author gratefully thanks the University of the Texas Health Science Center Medical School and U.S. Army Reserves for material support. Neither institution or agency had any involvement in study design; collection, analysis, and interpretation of data; writing the report; and the decision to submit the report for publication. Acknowledgements The work and opinions expressed herein are solely those of the author. The author thanks Mr. (COL) Karl Farris and Mr. (COL) George Oliver for their advice and guidance and encouragement on that project that culminated in this manuscript. The author gratefully acknowledges LTC SC Neesen for his work that provided the basis to test the ideas of his hypothesis on UN peacekeeping missions. References 1. United Nations Department of Peace Keeping Operations. Medical support manual for United Nations peacekeeping operations. 2nd ed. New York: UN; p Balanzino S. Lessons learned in peacekeeping operations. Brussels: NATO; p Osmancavusoglu E. Challenges to United Nations peacekeeping operations in the postcold War era. Percept. J Int Aff. 2000;4: United Nations. Report of the special committee on peacekeeping operations: 2012 substantive session (New York, 21 february-16 march and 11 September 2012), General assembly official records sixty-sixth session supplement No. 19. New York: UN; p Seet B, Burnham GM. Fatality trends in United Nations peacekeeping operations, JAMA. 2000;284(5): Hacon WS. Echelons of medical care. JCMA. 1962;87: Beebe GW, DeBakey ME. Battle casualties: Incidence, mortality, and logistic considerations. Springfield: Charles C. Thomas, inc; Seet B. Increased humanitarian deaths may not mean higher risks of dying. Comment BMJ. 2001;322(7281): Reade MC. Medical support for British peacekeeping operations in Kosovo (UNMIK/KFOR). ADF Health. 2002;3: Seet B. Levels of medical support for United Nations peacekeeping operations. Mil Med. 1999;164:451 6.
 George Oliver for their advice and guidance and encouragement on that project that culminated in this manuscript.")
12 11. Frechette L, Kristensen A. UN Peacekeeping: 20 Years of Reform. Ontario: CIGI Papers; Smadi RM, Smadi BY. Medical aspects of United Nations peace keeping missions: a Sixmonth-experience in eriteria. JRMS. 2004;11(1): Joshi VV, Wg CDR. United Nations mission in sierra Leone (UNAMSIL): medical deployment and experiences. Ind J Aerospace Med. 2003;47(1): Holt VK, Kelly M. Protecting civilians in the context of UN peacekeeping operations: successes, setbacks and remaining challenges. New York: Department of Peacekeeping Operations; Chulkov N. Review of the medical service in the United Nations system. Geneva: Joint Inspection Unit; p Hazra A. Challenges of setting up a potable water supply system in a United Nations peacekeeping mission: the south Sudan experience. Int J Hygiene Environ Health. 2013;216: Ledgerwood JL. Asia pacific issues: UN peacekeeping missions: the lessons from Cambodia. Anal East West Ctr. 1994;11: Schwartz E, Paul F, Pener H, Almog S, Rotenberg M, et al. Malaria antibodies and Mefloquine levels among United Nations troops in Angola. J Trvl Med. 2001;8: Cali G. The Italian army medical corps in the United Nations peace-keeping operations: Somalia and Mozambique, December 1992 December Med Trop (Mars). 1996;56(4): Craig SC, Pittman PR, Lewis TE, Rossi CA, Henchal EA, et al. An accelerated schedule for tick-borne encephalitis vaccine: the American military experience in Bosnia. Am J Trop Med Hygiene. 1999;61: Onuorah M. How policy, funding issues clog Nigeria s UN peace-keeping operations. South African Foreign Policy Iinitiative Ministry of Foreign Affairs of Japan. Current Issues Surrounding UN Peace-keeping Operations and Japanese Perspective Johnson RJ. Medical aspects of UN peacekeeping operations: trends, courses of action, and recommendations, Thesis report presented in partial fulfillment of the COTIPSO program Johnson RJ. A literature review of medical aspects of Post-Cold War UN peacekeeping operations: Trends, lessons learnt, courses of action, and recommendations. J R Army Med Corps. 2015;17:1 6.

13 25. Johnson RJ. A review of supplementary medical aspects of Post-Cold War UN peacekeeping operations: Trends, lessons learned, courses of action, and recommendations. J Peacekeeping In press. 26. Leslie D. Operational logistical support of UN peacekeeping missions: intermediate logistics course. Williamsburg: Peace Operations Training Institute; p Sokhin A. Unified principles, requirements and standards of armed forces medical support: the impact of NATO/multinational military missions on health care management, Kraine armed forces: research institute of military medicine Rosenfeld JV. Neurosurgery in Rwanda during a United Nations peace-keeping mission. Mil Med. 1997;162(5): Farrow GB, Rosenfeld JV, Crozier JA, Wheatley P, Warfe P. Military surgery in Rwanda. Aust N Z J Surg. 1997;67(10): Dailey J, Ijames VL. Evolution of the combat and operational stress control detachment, US army medical journal p Rentas F, Lincoln D, Harding A, Maas P, Giglio J, Fryar R, et al. The armed services blood program: blood support to combat casualty care 2001 to J Trauma Acute Care Surg. 2012;73(6 Suppl 5):S Reilly CD, Waller SG, Flynn WJ, Montalvo MA, Ward JB. U.S. Air force mobile ophthalmic surgery team. Mil Med. 2004;169(12): Rozin R, Klausner JM, Dolev E. New concepts of forward combat surgery. Injury. 1988;19(3): European Defense Agency. Multinational modular medical units: capability gap. Brussels: European Union; p Col BR, Maj HP, Kao R, McAlister V, Po J, Stiegelmar R, et al. The role 3 multinational medical unit at Kandahar airfield Can J Surg. 2011;54(6 Suppl):S Nessen SC. The mobile modular surgical hospital: the army medical Department s future unit of action, Thesis presented to the U.S. Army command and staff college Milosevic M. Challenges of women s participation in Serbian peacekeeping missions, Brigade cetre for security policy p UNDPKO. Rehatting ECOWAS forces as UN peacekeepers: lessons learned. Workshop on lessons from ECOWAS peacekeeping operations : towards an action agenda for implementation. Accra: Kofi Annan International Peacekeeping Training Centre; p Harrel-bond B. Africa s dependency and the remedies: the 4th international congress of African studies. Am Univ Field Staff Rep Africa. 1979;39:1 8.
:311 4. 29.")
14 40. Secretary-General. Report of the secretary-general: civilian capacity in the aftermath of conflict. New York: United Nations; Special Committee on Peacekeeping Operations. Dangerous peacekeeping deployment areas demand adherence to founding principles, focus on performance, impartiality, 239th & 240th Meetings. New York: United Nations; p Vielra M. The UN and its peacekeeping dilemma. New York: United Nations; p Suthaniraraj K, Quinn M, Mendez J. Standing for change in peacekeeping operations, UNEPS Secretariate. New York: United Nations; p Rhomberg L. Strategies to protect health of U.S. Forces; Analytical processes for assessing risks. Washington, D.C.: National Academies Press; Ladsous H, Haq A, Lute JH. Performance peacekeeping. New York: United Nations; 2014.

15
16
THE LEVEL OF MEDICAL SUPPORT IMPORTANT INDICATOR IN THE COMPLETION OF INTERNATIONAL ARMY MISSIONS
 THE LEVEL OF MEDICAL SUPPORT IMPORTANT INDICATOR IN THE COMPLETION OF INTERNATIONAL ARMY MISSIONS Locotenent colonel dr. Eugen Preda Spitalul Clinic de Urgenţă Militar Dr. Ştefan Odobleja Craiova Abstract
THE LEVEL OF MEDICAL SUPPORT IMPORTANT INDICATOR IN THE COMPLETION OF INTERNATIONAL ARMY MISSIONS Locotenent colonel dr. Eugen Preda Spitalul Clinic de Urgenţă Militar Dr. Ştefan Odobleja Craiova Abstract
Department of Defense INSTRUCTION
 Department of Defense INSTRUCTION NUMBER 1322.24 October 6, 2011 ASD(HA) SUBJECT: Reference: Medical Readiness Training (a) DoD Directive 5124.02, Under Secretary of Defense for Personnel and Readiness
Department of Defense INSTRUCTION NUMBER 1322.24 October 6, 2011 ASD(HA) SUBJECT: Reference: Medical Readiness Training (a) DoD Directive 5124.02, Under Secretary of Defense for Personnel and Readiness
Department of Veterans Affairs VHA DIRECTIVE 2010-010 Veterans Health Administration Washington, DC 20420 March 2, 2010
 Department of Veterans Affairs VHA DIRECTIVE 2010-010 Veterans Health Administration Washington, DC 20420 STANDARDS FOR EMERGENCY DEPARTMENT AND URGENT CARE CLINIC STAFFING NEEDS IN VHA FACILITIES 1. PURPOSE:
Department of Veterans Affairs VHA DIRECTIVE 2010-010 Veterans Health Administration Washington, DC 20420 STANDARDS FOR EMERGENCY DEPARTMENT AND URGENT CARE CLINIC STAFFING NEEDS IN VHA FACILITIES 1. PURPOSE:
COJUMA s. Legal Considerations for Defense Support to Civil Authorities. U.S. Southern Command Miami, Florida Draft
 COJUMA s Legal Considerations for Defense Support to Civil Authorities U.S. Southern Command 28 Miami, Florida Miami, Florida Draft Table of Contents Legal Considerations for Defense Support to Civil Authorities.....10
COJUMA s Legal Considerations for Defense Support to Civil Authorities U.S. Southern Command 28 Miami, Florida Miami, Florida Draft Table of Contents Legal Considerations for Defense Support to Civil Authorities.....10
LESSON SEVEN CAMPAIGN PLANNING FOR MILITARY OPERATIONS OTHER THAN WAR MQS MANUAL TASKS: 01-9019.00-0001 OVERVIEW
 TASK DESCRIPTION: LESSON SEVEN CAMPAIGN PLANNING FOR MILITARY OPERATIONS OTHER THAN WAR MQS MANUAL TASKS: 01-9019.00-0001 OVERVIEW Learn the differences between planning for a campaign in war and planning
TASK DESCRIPTION: LESSON SEVEN CAMPAIGN PLANNING FOR MILITARY OPERATIONS OTHER THAN WAR MQS MANUAL TASKS: 01-9019.00-0001 OVERVIEW Learn the differences between planning for a campaign in war and planning
CO-CHAIR S SUMMARY REPORT OF THE 3 rd ARF PEACEKEEPING EXPERTS MEETING SIEM REAP, CAMBODIA 24-26 June 2009
 CO-CHAIR S SUMMARY REPORT OF THE 3 rd ARF PEACEKEEPING EXPERTS MEETING SIEM REAP, CAMBODIA 24-26 June 2009 1. Pursuant to the decision of the 15 th ASEAN Regional Forum (ARF) Ministerial Meeting in July
CO-CHAIR S SUMMARY REPORT OF THE 3 rd ARF PEACEKEEPING EXPERTS MEETING SIEM REAP, CAMBODIA 24-26 June 2009 1. Pursuant to the decision of the 15 th ASEAN Regional Forum (ARF) Ministerial Meeting in July
Managing Ballistic Injury in the Military Environment: The Concept of Forward Surgical Support
 27 Managing Ballistic Injury in the Military Environment: The Concept of Forward Surgical Support Donald Jenkins, Paul Dougherty, and James M. Ryan Introduction In this chapter, the emphasis is on surgical
27 Managing Ballistic Injury in the Military Environment: The Concept of Forward Surgical Support Donald Jenkins, Paul Dougherty, and James M. Ryan Introduction In this chapter, the emphasis is on surgical
Militarism and HIV/AIDS: The Deadly Consequences for Women. Background paper by Women's International League for Peace and Freedom
 Militarism and HIV/AIDS: The Deadly Consequences for Women Background paper by Women's International League for Peace and Freedom UN General Assembly Special Session on HIV/AIDS June, 2001 It is known
Militarism and HIV/AIDS: The Deadly Consequences for Women Background paper by Women's International League for Peace and Freedom UN General Assembly Special Session on HIV/AIDS June, 2001 It is known
Department of Defense INSTRUCTION
 Department of Defense INSTRUCTION NUMBER 6000.11 May 4, 2012 USD(P&R) SUBJECT: Patient Movement (PM) References: See Enclosure 1 1. PURPOSE. This Instruction: a. Reissues DoD Instruction (DoDI) 6000.11
Department of Defense INSTRUCTION NUMBER 6000.11 May 4, 2012 USD(P&R) SUBJECT: Patient Movement (PM) References: See Enclosure 1 1. PURPOSE. This Instruction: a. Reissues DoD Instruction (DoDI) 6000.11
Conflict management Funmi Olonisaki King s College London
 Conflict management Funmi Olonisaki King s College London 1 Key messages conveyed by conflict and conflict management trends in Africa Regional and sub-regional organisations are an integral part of the
Conflict management Funmi Olonisaki King s College London 1 Key messages conveyed by conflict and conflict management trends in Africa Regional and sub-regional organisations are an integral part of the
Roles of Medical Care (United States)
") Roles of Medical Care (United States) Chapter 2 Roles of Medical Care (United States) Introduction Military doctrine supports an integrated health services support system to triage, treat, evacuate, and
Roles of Medical Care (United States) Chapter 2 Roles of Medical Care (United States) Introduction Military doctrine supports an integrated health services support system to triage, treat, evacuate, and
THE HONORABLE WILLIAM WINKENWERDER, JR. M.D., M.B.A. ASSISTANT SECRETARY OF DEFENSE FOR HEALTH AFFAIRS BEFORE THE SUBCOMMITTEE ON MILITARY PERSONNEL
 THE HONORABLE WILLIAM WINKENWERDER, JR. M.D., M.B.A. ASSISTANT SECRETARY OF DEFENSE FOR HEALTH AFFAIRS BEFORE THE SUBCOMMITTEE ON MILITARY PERSONNEL ARMED SERVICES COMMITTEE U.S. HOUSE OF REPRESENTATIVES
THE HONORABLE WILLIAM WINKENWERDER, JR. M.D., M.B.A. ASSISTANT SECRETARY OF DEFENSE FOR HEALTH AFFAIRS BEFORE THE SUBCOMMITTEE ON MILITARY PERSONNEL ARMED SERVICES COMMITTEE U.S. HOUSE OF REPRESENTATIVES
Adopted by the Security Council at its 7268th meeting, on 18 September 2014
 United Nations S/RES/2177 (2014) Security Council Distr.: General 18 September 2014 Resolution 2177 (2014) Adopted by the Security Council at its 7268th meeting, on 18 September 2014 The Security Council,
United Nations S/RES/2177 (2014) Security Council Distr.: General 18 September 2014 Resolution 2177 (2014) Adopted by the Security Council at its 7268th meeting, on 18 September 2014 The Security Council,
Support to Civil Administration
 Chapter 11 Support to Civil Administration Support to civil administration is the most specialized CA supporting mission. CA commands and brigades are organized to support civil administration in support
Chapter 11 Support to Civil Administration Support to civil administration is the most specialized CA supporting mission. CA commands and brigades are organized to support civil administration in support
Position Classification Flysheet for Logistics Management Series, GS-0346
 Position Classification Flysheet for Logistics Management Series, GS-0346 Table of Contents SERIES DEFINITION... 2 SERIES COVERAGE... 2 EXCLUSIONS... 4 DISTINGUISHING BETWEEN LOGISTICS MANAGEMENT AND OTHER
Position Classification Flysheet for Logistics Management Series, GS-0346 Table of Contents SERIES DEFINITION... 2 SERIES COVERAGE... 2 EXCLUSIONS... 4 DISTINGUISHING BETWEEN LOGISTICS MANAGEMENT AND OTHER
International Relations Networking of the Austrian Armed Forces
 International Relations Networking of the Austrian Armed Forces Address given by General Roland ERTL Chief of General Staff, Austrian Armed Forces Ladies and Gentlemen, distinguished guests, The Austrian
International Relations Networking of the Austrian Armed Forces Address given by General Roland ERTL Chief of General Staff, Austrian Armed Forces Ladies and Gentlemen, distinguished guests, The Austrian
Health Solutions. Mission-Critical Support Across the Health Spectrum
 Health Solutions Mission-Critical Support Across the Health Spectrum IT Experts Who Know Health, Health Experts Who Know IT Today s healthcare challenges are formidable: an aging population, lack of interoperability
Health Solutions Mission-Critical Support Across the Health Spectrum IT Experts Who Know Health, Health Experts Who Know IT Today s healthcare challenges are formidable: an aging population, lack of interoperability
OPERATIONAL RISK MANAGEMENT B130786 STUDENT HANDOUT
 UNITED STATES MARINE CORPS THE BASIC SCHOOL MARINE CORPS TRAINING COMMAND CAMP BARRETT, VIRGINIA 22134-5019 OPERATIONAL RISK MANAGEMENT B130786 STUDENT HANDOUT Basic Officer Course (ORM) Introduction Importance
UNITED STATES MARINE CORPS THE BASIC SCHOOL MARINE CORPS TRAINING COMMAND CAMP BARRETT, VIRGINIA 22134-5019 OPERATIONAL RISK MANAGEMENT B130786 STUDENT HANDOUT Basic Officer Course (ORM) Introduction Importance
2014 Florida Governors Hurricane Conference. National Disaster Medical System. Disaster Medical Assistance Team. Overview
 United States Department of Health & Human Services Office of The Assistant Secretary for Preparedness and Response 2014 Florida Governors Hurricane Conference National Disaster Medical System Disaster
United States Department of Health & Human Services Office of The Assistant Secretary for Preparedness and Response 2014 Florida Governors Hurricane Conference National Disaster Medical System Disaster
Dilemmas in Emergency Management & Response. Bruria Adini Wiesel, PhD Emergency & Disaster Management Division Israeli Ministry of Health
 Dilemmas in Emergency Management & Response Bruria Adini Wiesel, PhD Emergency & Disaster Management Division Israeli Ministry of Health 1 Dilemmas in disaster preparedness Provision of medical services
Dilemmas in Emergency Management & Response Bruria Adini Wiesel, PhD Emergency & Disaster Management Division Israeli Ministry of Health 1 Dilemmas in disaster preparedness Provision of medical services
The Role of Military Public Health and Healthcare Providers in National Bioterrorism Event Consequence Management
 The Role of Military Public Health and Healthcare Providers in National Bioterrorism Event Consequence Management COL (Ret) Zygmunt F. Dembek, PhD, MS, MPH, LHD EpiMilitaris Conference Hotel Zamek Ryn
The Role of Military Public Health and Healthcare Providers in National Bioterrorism Event Consequence Management COL (Ret) Zygmunt F. Dembek, PhD, MS, MPH, LHD EpiMilitaris Conference Hotel Zamek Ryn
Impact of Transition on Health Care Delivery
 Agency Coordinating Body for Afghan Relief & Development Impact of Transition on Health Care Delivery The security transition in Afghanistan is entering its final phase in 2014, with partial withdrawal
Agency Coordinating Body for Afghan Relief & Development Impact of Transition on Health Care Delivery The security transition in Afghanistan is entering its final phase in 2014, with partial withdrawal
The challenges of the military-medical service in the 21 st century, focusing on the support of NATO s medical transformation
 ZRÍNYI MIKLÓS NATIONAL DEFENSE UNIVERSITY KOSSUTH LAJOS FACULTY OF MILITARY SCIENCE Military Science PhD School Col. István Kopcsó M.D. The challenges of the military-medical service in the 21 st century,
ZRÍNYI MIKLÓS NATIONAL DEFENSE UNIVERSITY KOSSUTH LAJOS FACULTY OF MILITARY SCIENCE Military Science PhD School Col. István Kopcsó M.D. The challenges of the military-medical service in the 21 st century,
December 23, 2010. Dr. David Blumenthal National Coordinator for Health Information Technology Department of Health and Human Services
 December 23, 2010 Dr. David Blumenthal National Coordinator for Health Information Technology Department of Health and Human Services RE: Prioritized measurement concepts Dear Dr. Blumenthal: Thank you
December 23, 2010 Dr. David Blumenthal National Coordinator for Health Information Technology Department of Health and Human Services RE: Prioritized measurement concepts Dear Dr. Blumenthal: Thank you
Summary 1. Module scope and objectives 2. Terms, definitions and abbreviations 3. Introduction 4. The military component
 4.40 UN Military Roles and Responsibilities Contents Summary... 1 1. Module scope and objectives... 1 2. Terms, definitions and abbreviations... 2 3. Introduction... 2 4. The military component... 2 4.1.
4.40 UN Military Roles and Responsibilities Contents Summary... 1 1. Module scope and objectives... 1 2. Terms, definitions and abbreviations... 2 3. Introduction... 2 4. The military component... 2 4.1.
ONE FEDERAL COORDINATING CENTER S PLAN FOR AIRHEAD MANAGEMENT
 ONE FEDERAL COORDINATING CENTER S PLAN FOR AIRHEAD MANAGEMENT by Walter G. Green III, Ph.D., CFAAMA, FACCP Associate Professor of Emergency Management University of Richmond A Paper Presented at the American
ONE FEDERAL COORDINATING CENTER S PLAN FOR AIRHEAD MANAGEMENT by Walter G. Green III, Ph.D., CFAAMA, FACCP Associate Professor of Emergency Management University of Richmond A Paper Presented at the American
Expert Seminar. Engagement with Non-State Armed Groups in Peace Processes
 Expert Seminar Engagement with Non-State Armed Groups in Peace Processes Sept. 14 th and 15 th, 2010, Berlin Background: Non-state armed groups (NSAG) conflict regions. By exercising armed violence and
Expert Seminar Engagement with Non-State Armed Groups in Peace Processes Sept. 14 th and 15 th, 2010, Berlin Background: Non-state armed groups (NSAG) conflict regions. By exercising armed violence and
CYBER SECURITY AND CYBER DEFENCE IN THE EUROPEAN UNION OPPORTUNITIES, SYNERGIES AND CHALLENGES
 CYBER SECURITY AND CYBER DEFENCE IN THE EUROPEAN UNION OPPORTUNITIES, SYNERGIES AND CHALLENGES By Wolfgang Röhrig, Programme Manager Cyber Defence at EDA and Wg Cdr Rob Smeaton, Cyber Defence Staff Officer
CYBER SECURITY AND CYBER DEFENCE IN THE EUROPEAN UNION OPPORTUNITIES, SYNERGIES AND CHALLENGES By Wolfgang Röhrig, Programme Manager Cyber Defence at EDA and Wg Cdr Rob Smeaton, Cyber Defence Staff Officer
NPWJ International Criminal Justice Policy Series No. 1. Prosecuting Violations of International Criminal Law: Who should be tried?
 Prosecuting Violations of International Criminal Law: Who should be tried? Preliminary edition for distribution during the Third Session of the ICC Assembly of States Parties, The Hague, September 2004
Prosecuting Violations of International Criminal Law: Who should be tried? Preliminary edition for distribution during the Third Session of the ICC Assembly of States Parties, The Hague, September 2004
JOINT STATEMENT COMMISSION ON WARTIME CONTRACTING
 JOINT STATEMENT COMMISSION ON WARTIME CONTRACTING TOTAL FORCE POLICY, THE QDR, AND OTHER DEFENSE OPERATIONAL PLANNING: WHY DOES PLANNING FOR CONTRACTORS CONTINUE TO LAG? JULY 12, 2010 Chairman Thibault,
JOINT STATEMENT COMMISSION ON WARTIME CONTRACTING TOTAL FORCE POLICY, THE QDR, AND OTHER DEFENSE OPERATIONAL PLANNING: WHY DOES PLANNING FOR CONTRACTORS CONTINUE TO LAG? JULY 12, 2010 Chairman Thibault,
While interagency education and training have long been staples of the intelligence and
 Navigating Interagency Education and Training Courses by John Dyson While interagency education and training have long been staples of the intelligence and law enforcement communities, such efforts are
Navigating Interagency Education and Training Courses by John Dyson While interagency education and training have long been staples of the intelligence and law enforcement communities, such efforts are
Assisted Living Facilities & Adult Care Comprehensive Emergency Management Plans
 Assisted Living Facilities & Adult Care Comprehensive Emergency Management Plans STATUTORY REFERENCE GUIDANCE CRITERIA The Henrico County Division of Fire s Office of Emergency Management provides this
Assisted Living Facilities & Adult Care Comprehensive Emergency Management Plans STATUTORY REFERENCE GUIDANCE CRITERIA The Henrico County Division of Fire s Office of Emergency Management provides this
Madam Chairwoman, Ranking Member Michaud, and Members of the Subcommittee:
 STATEMENT OF JOY J. ILEM DEPUTY NATIONAL LEGISLATIVE DIRECTOR OF THE DISABLED AMERICAN VETERANS BEFORE THE COMMITTEE ON VETERANS AFFAIRS SUBCOMMITTEE ON HEALTH UNITED STATES HOUSE OF REPRESENTATIVES JULY
STATEMENT OF JOY J. ILEM DEPUTY NATIONAL LEGISLATIVE DIRECTOR OF THE DISABLED AMERICAN VETERANS BEFORE THE COMMITTEE ON VETERANS AFFAIRS SUBCOMMITTEE ON HEALTH UNITED STATES HOUSE OF REPRESENTATIVES JULY
Introduction. Catastrophic Incident Annex. Cooperating Agencies: Coordinating Agency: Department of Homeland Security
 Catastrophic Incident Annex Coordinating Agency: Department of Homeland Security Cooperating Agencies: All Federal departments and agencies (and other organizations) with assigned primary or supporting
Catastrophic Incident Annex Coordinating Agency: Department of Homeland Security Cooperating Agencies: All Federal departments and agencies (and other organizations) with assigned primary or supporting
DEPARTMENT OF THE AIR FORCE PRESENTATION TO THE SUBCOMMITTEE ON MILITARY PERSONNEL COMMITTEE ON ARMED SERVICES UNITED STATES HOUSE OF REPRESENTATIVES
 DEPARTMENT OF THE AIR FORCE PRESENTATION TO THE SUBCOMMITTEE ON MILITARY PERSONNEL COMMITTEE ON ARMED SERVICES UNITED STATES HOUSE OF REPRESENTATIVES SUBJECT: SUICIDE PREVENTION STATEMENT OF: LIEUTENANT
DEPARTMENT OF THE AIR FORCE PRESENTATION TO THE SUBCOMMITTEE ON MILITARY PERSONNEL COMMITTEE ON ARMED SERVICES UNITED STATES HOUSE OF REPRESENTATIVES SUBJECT: SUICIDE PREVENTION STATEMENT OF: LIEUTENANT
NHS Trusts and the UK International Emergency Trauma Register.
 NHS Trusts and the UK International Emergency Trauma Register. The ultimate beneficiaries from UK professional health workers gaining international experience are NHS patients in the UK Liam Donaldson,
NHS Trusts and the UK International Emergency Trauma Register. The ultimate beneficiaries from UK professional health workers gaining international experience are NHS patients in the UK Liam Donaldson,
MEDICAL READINESS AND OPERATIONAL MEDICINE
 Chapter Four MEDICAL READINESS AND OPERATIONAL MEDICINE The readiness mission of the MHS makes the system unique among U.S. health-care organizations. Its stated mission to provide, and to maintain readiness
Chapter Four MEDICAL READINESS AND OPERATIONAL MEDICINE The readiness mission of the MHS makes the system unique among U.S. health-care organizations. Its stated mission to provide, and to maintain readiness
ECONOMICS OF PEACE AND SECURITY Global and Regional Security Alliances - Carlos Seiglie and Sylvie Matelly UNESCO EOLSS
 GLOBAL AND REGIONAL SECURITY ALLIANCES Carlos Seiglie Rutgers University, NJ, USA Sylvie Matelly Université Pierre Mendes France, Grenoble, France Keywords: collective action, public good, regional security
GLOBAL AND REGIONAL SECURITY ALLIANCES Carlos Seiglie Rutgers University, NJ, USA Sylvie Matelly Université Pierre Mendes France, Grenoble, France Keywords: collective action, public good, regional security
Danish lessons learned: The comprehensive/integrated approach after Iraq and Afghanistan
 Military Studies Magazine Danish lessons learned: The comprehensive/integrated approach after Iraq and Afghanistan by Peter Viggo Jakobsen Photo: Forsvaret ISSUE 01, VOLUME 02, 2014 1 Subcribe at fak.dk/eng/magazine
Military Studies Magazine Danish lessons learned: The comprehensive/integrated approach after Iraq and Afghanistan by Peter Viggo Jakobsen Photo: Forsvaret ISSUE 01, VOLUME 02, 2014 1 Subcribe at fak.dk/eng/magazine
How To Determine The Entitlement To Healthcare In The Nhs
 Journal of Public Health Medicine Vol. 21, No. 3, pp. 325 330 Printed in Great Britain Entitlement to military healthcare limitations of the NHS model Major Martin C. M. Bricknell Summary The Defence Medical
Journal of Public Health Medicine Vol. 21, No. 3, pp. 325 330 Printed in Great Britain Entitlement to military healthcare limitations of the NHS model Major Martin C. M. Bricknell Summary The Defence Medical
How To Write The Who Disability And Rehabilitation Guidelines
 WORLD HEALTH ORGANIZATION CONCEPT PAPER WHO Guidelines on Health-Related Rehabilitation (Rehabilitation Guidelines) MANDATE The World Health Assembly Resolution on "Disability, including prevention, management
WORLD HEALTH ORGANIZATION CONCEPT PAPER WHO Guidelines on Health-Related Rehabilitation (Rehabilitation Guidelines) MANDATE The World Health Assembly Resolution on "Disability, including prevention, management
Template 7.1. Core Functions of Hospital Facilities and Providers in the Implementation of CSC Plans
 Template 7.1. Core Functions of Hospital Facilities and Providers in the Implementation of CSC Plans Hospital Facilities Function 1. Alerting Health care facility is able to receive and manage alerts from
Template 7.1. Core Functions of Hospital Facilities and Providers in the Implementation of CSC Plans Hospital Facilities Function 1. Alerting Health care facility is able to receive and manage alerts from
East Midlands Ambulance Service NHS Trust. Service Delivery Model
 East Midlands Ambulance Service NHS Trust Service Delivery Model EXECUTIVE SUMMARY This paper outlines the new service operating model proposed for East Midlands Ambulance Service NHS Trust which has the
East Midlands Ambulance Service NHS Trust Service Delivery Model EXECUTIVE SUMMARY This paper outlines the new service operating model proposed for East Midlands Ambulance Service NHS Trust which has the
CHALLENGES AND BARRIERS ALONG THE IN-COUNTRY SUPPLY CHAIN
 UN Commission on Life-Saving Commodities for Women and Children CHALLENGES AND BARRIERS ALONG THE IN-COUNTRY SUPPLY CHAIN To increase access to life-saving commodities for women and children, barriers
UN Commission on Life-Saving Commodities for Women and Children CHALLENGES AND BARRIERS ALONG THE IN-COUNTRY SUPPLY CHAIN To increase access to life-saving commodities for women and children, barriers
Followup Audit: Enterprise Blood Management System Not Ready for Full Deployment
 Inspector General U.S. Department of Defense Report No. DODIG 2015 008 OCTOBER 23, 2014 Followup Audit: Enterprise Blood Management System Not Ready for Full Deployment INTEGRITY EFFICIENCY ACCOUNTABILITY
Inspector General U.S. Department of Defense Report No. DODIG 2015 008 OCTOBER 23, 2014 Followup Audit: Enterprise Blood Management System Not Ready for Full Deployment INTEGRITY EFFICIENCY ACCOUNTABILITY
Typed Resource Definitions Emergency Medical Services Resources
 Typed Resource Definitions Emergency Medical Services Resources FEMA 508-3 (March 2009) Background Resource Typing Web Site Supersedure Changes The National Mutual Aid and Resource Management Initiative
Typed Resource Definitions Emergency Medical Services Resources FEMA 508-3 (March 2009) Background Resource Typing Web Site Supersedure Changes The National Mutual Aid and Resource Management Initiative
Active Engagement, Modern Defence - Strategic Concept for the Defence and Security of the Members of the North Atlantic Treaty Organization, 1010
 1 Modern security environment contains a broad and evolving set of challenges to the security of NATO s territory and populations. In order to assure their security, the Alliance must and will continue
1 Modern security environment contains a broad and evolving set of challenges to the security of NATO s territory and populations. In order to assure their security, the Alliance must and will continue
Part 1: The Origins of the Responsibility to Protect and the R2PCS Project
 Part 1: The Origins of the Responsibility to Protect and the R2PCS Project What is the Responsibility to Protect (R2P)? R2P is an emerging international norm which sets forth that states have the primary
Part 1: The Origins of the Responsibility to Protect and the R2PCS Project What is the Responsibility to Protect (R2P)? R2P is an emerging international norm which sets forth that states have the primary
Analysis of VA Health Care Utilization among Operation Enduring Freedom (OEF), Operation Iraqi Freedom (OIF), and Operation New Dawn (OND) Veterans
, Operation Iraqi Freedom (OIF), and Operation New Dawn (OND) Veterans") Analysis of VA Health Care Utilization among Operation Enduring Freedom (OEF), Operation Iraqi Freedom (OIF), and Operation New Dawn (OND) Veterans Cumulative from 1 st Qtr FY 2002 through 4th Qtr FY 2011
Analysis of VA Health Care Utilization among Operation Enduring Freedom (OEF), Operation Iraqi Freedom (OIF), and Operation New Dawn (OND) Veterans Cumulative from 1 st Qtr FY 2002 through 4th Qtr FY 2011
Statement at the Fourth Committee Opening Debate. Under Secretary-General for Field Support, Ms. Ameerah Haq. 28 October 2014
 As Delivered Statement at the Fourth Committee Opening Debate Under Secretary-General for Field Support, Ms. Ameerah Haq 28 October 2014 I appreciate this opportunity to meet with you, once again, with
As Delivered Statement at the Fourth Committee Opening Debate Under Secretary-General for Field Support, Ms. Ameerah Haq 28 October 2014 I appreciate this opportunity to meet with you, once again, with
"The European Union's Security Architecture and its role to strengthen Peace and Security"
 Chairman EU Military Committee General Patrick de Rousiers at the 29 th Asia Pacific Round Table in Kuala Lumpur 02 June 2015 "The European Union's Security Architecture and its role to strengthen Peace
Chairman EU Military Committee General Patrick de Rousiers at the 29 th Asia Pacific Round Table in Kuala Lumpur 02 June 2015 "The European Union's Security Architecture and its role to strengthen Peace
ort Office of the Inspector General Department of Defense YEAR 2000 COMPLIANCE OF THE STANDARD ARMY MAINTENANCE SYSTEM-REHOST Report Number 99-165
 it ort YEAR 2000 COMPLIANCE OF THE STANDARD ARMY MAINTENANCE SYSTEM-REHOST Report Number 99-165 May 24, 1999 Office of the Inspector General Department of Defense Additional Copies To obtain additional
it ort YEAR 2000 COMPLIANCE OF THE STANDARD ARMY MAINTENANCE SYSTEM-REHOST Report Number 99-165 May 24, 1999 Office of the Inspector General Department of Defense Additional Copies To obtain additional
Peace operations 2010 reform strategy (excerpts from the report of the Secretary-General)
") Peace operations 2010 reform strategy (excerpts from the report of the Secretary-General) Reporting to the General Assembly on 24 February 2006 on the financing of the United Nations peacekeeping operations
Peace operations 2010 reform strategy (excerpts from the report of the Secretary-General) Reporting to the General Assembly on 24 February 2006 on the financing of the United Nations peacekeeping operations
ST/SGB/2004/8. Secretariat. United Nations. Secretary-General s bulletin Organization of the Office of Human Resources Management.
 United Nations Secretariat 7 April 2004 ST/SGB/2004/8 Secretary-General s bulletin Organization of the Office of Human Resources Management The Secretary-General, pursuant to the Secretary-General s bulletin
United Nations Secretariat 7 April 2004 ST/SGB/2004/8 Secretary-General s bulletin Organization of the Office of Human Resources Management The Secretary-General, pursuant to the Secretary-General s bulletin
ORIGINAL: ENGLISH 11th May, 1967 DOCUMENT DPC/D(67)23. DEFENCE PLANNING COMMITTEE Decisions of Defence Planning Committee in Ministerial Session
23. DEFENCE PLANNING COMMITTEE Decisions of Defence Planning Committee in Ministerial Session") ORIGINAL: ENGLISH 11th May, 1967 DOCUMENT DEFENCE PLANNING COMMITTEE Decisions of Defence Planning Committee in Ministerial Session Note by the Chairman I attach for your information a list of the decisions
ORIGINAL: ENGLISH 11th May, 1967 DOCUMENT DEFENCE PLANNING COMMITTEE Decisions of Defence Planning Committee in Ministerial Session Note by the Chairman I attach for your information a list of the decisions
AEROMEDICAL EVACUATION IN NATO LED MILITARY OPERATIONS
 Review of the Air Force Academy No 2 (26) 2014 AEROMEDICAL EVACUATION IN NATO LED MILITARY OPERATIONS 1. INTRODUCTION One of factors that significantly determine military operations is logistic support.
Review of the Air Force Academy No 2 (26) 2014 AEROMEDICAL EVACUATION IN NATO LED MILITARY OPERATIONS 1. INTRODUCTION One of factors that significantly determine military operations is logistic support.
SECRETARY OF THE ARMY WASHINGTON
 SECRETARY OF THE ARMY WASHINGTON 2 2 JUN 2016 MEMORANDUM FOR SEE DISTRIBUTION SUBJECT: Army Directive 2016-18 (Divesting Legacy Information Technology Hardware, Software, and Services in Support of the
SECRETARY OF THE ARMY WASHINGTON 2 2 JUN 2016 MEMORANDUM FOR SEE DISTRIBUTION SUBJECT: Army Directive 2016-18 (Divesting Legacy Information Technology Hardware, Software, and Services in Support of the
Security Council. United Nations S/2008/434
 United Nations S/2008/434 Security Council Distr.: General 3 July 2008 Original: English Special report of the Secretary-General pursuant to Security Council resolution 1806 (2008) on the United Nations
United Nations S/2008/434 Security Council Distr.: General 3 July 2008 Original: English Special report of the Secretary-General pursuant to Security Council resolution 1806 (2008) on the United Nations
Meaningful Use and Engaging Patients: Beyond Checking the Box
 RelayHealth Clinical Solutions Executive Brief Meaningful Use and Engaging Patients: Beyond Checking the Box Contents Contents Introduction The term patient engagement has become entrenched in the healthcare
RelayHealth Clinical Solutions Executive Brief Meaningful Use and Engaging Patients: Beyond Checking the Box Contents Contents Introduction The term patient engagement has become entrenched in the healthcare
How To Improve Safety Of A Vehicle
 Humanav operational benefits May 2010 White paper 2 Table of Contents A. Introduction - Vehicle Tracking...3 B. Good Practice...4 1. Security for staff, vehicles and cargo...6 2. Safety for staff and other
Humanav operational benefits May 2010 White paper 2 Table of Contents A. Introduction - Vehicle Tracking...3 B. Good Practice...4 1. Security for staff, vehicles and cargo...6 2. Safety for staff and other
Training and Evaluation Outline Report
 Training and Evaluation Outline Report Task Number: 71-9-8600 Task Title: Establish Civil Security (Division Echelon and Above [Operational]) Distribution Restriction: for public release; distribution
Training and Evaluation Outline Report Task Number: 71-9-8600 Task Title: Establish Civil Security (Division Echelon and Above [Operational]) Distribution Restriction: for public release; distribution
SIGIR AGENCIES NEED IMPROVED FINANCIAL DATA REPORTING FOR PRIVATE SECURITY CONTRACTORS. October 30, 2008. What SIGIR Found. Why SIGIR Did This Study
 OFFICE OF THE SPECIAL INSPECTOR GENERAL FOR IRAQ RECONSTRUCTION AGENCIES NEED IMPROVED FINANCIAL DATA REPORTING FOR PRIVATE SECURITY CONTRACTORS SIIGIIR--09--005 OCTOBER 30,, 2008 SIGIR Special Inspector
OFFICE OF THE SPECIAL INSPECTOR GENERAL FOR IRAQ RECONSTRUCTION AGENCIES NEED IMPROVED FINANCIAL DATA REPORTING FOR PRIVATE SECURITY CONTRACTORS SIIGIIR--09--005 OCTOBER 30,, 2008 SIGIR Special Inspector
Having undertaken a general discussion on the basis of Report IV, Small and medium-sized enterprises and decent and productive employment creation,
 International Labour Conference Provisional Record 104th Session, Geneva, June 2015 11-1 Fourth item on the agenda: Small and medium-sized enterprises and decent and productive employment creation Reports
International Labour Conference Provisional Record 104th Session, Geneva, June 2015 11-1 Fourth item on the agenda: Small and medium-sized enterprises and decent and productive employment creation Reports
GUIDELINE STATEMENT REGARDING POSSIBLE EBOLA DEPLOYMENT BY PHS STAFF/VOLUNTEERS
 September 15, 2014 RE: Ebola Outbreak West Africa 2014 > GUIDELINES TO ALL STAFF RE DEPLOYMENTS IMPORTANCE: WARNING ALERT SENSITIVITY: NO RESTRICTIONS/FULL DISTRIBUTION RESPONSE: PERSONAL ACTION REQUIRED
September 15, 2014 RE: Ebola Outbreak West Africa 2014 > GUIDELINES TO ALL STAFF RE DEPLOYMENTS IMPORTANCE: WARNING ALERT SENSITIVITY: NO RESTRICTIONS/FULL DISTRIBUTION RESPONSE: PERSONAL ACTION REQUIRED
Ensuring WHO s capacity to prepare for and respond to future large-scale and sustained outbreaks and emergencies
 EXECUTIVE BOARD Special session on Ebola Provisional agenda item 3 EBSS/3/3 EXECUTIVE BOARD 136th session 9 January 2015 Provisional agenda item 9.4 Ensuring WHO s capacity to prepare for and respond to
EXECUTIVE BOARD Special session on Ebola Provisional agenda item 3 EBSS/3/3 EXECUTIVE BOARD 136th session 9 January 2015 Provisional agenda item 9.4 Ensuring WHO s capacity to prepare for and respond to
OPNAVINST 3000.15A USFF/CNO N3/N5 10 Nov 2014
 DEPARTMENT OF THE NAVY OFFICE OF THE CHIEF OF NAVAL OPERATIONS 2000 NAVY PENTAGON WASHINGTON, DC 20350-2000 OPNAVINST 3000.15A USFF/CNO N3/N5 OPNAV INSTRUCTION 3000.15A From: Chief of Naval Operations
DEPARTMENT OF THE NAVY OFFICE OF THE CHIEF OF NAVAL OPERATIONS 2000 NAVY PENTAGON WASHINGTON, DC 20350-2000 OPNAVINST 3000.15A USFF/CNO N3/N5 OPNAV INSTRUCTION 3000.15A From: Chief of Naval Operations
HEALTH CARE IN DANGER
 VIOLENCE AGAINST HEALTH CARE MUST END HEALTH CARE IN DANGER. A SIXTEEN-COUNTRY STUDY VIOLENT INCIDENTS AFFECTING HEALTH CARE HEALTH CARE IN DANGER JANUARY TO DECEMBER 2012 i VIOLENT INCIDENTS AFFECTING
VIOLENCE AGAINST HEALTH CARE MUST END HEALTH CARE IN DANGER. A SIXTEEN-COUNTRY STUDY VIOLENT INCIDENTS AFFECTING HEALTH CARE HEALTH CARE IN DANGER JANUARY TO DECEMBER 2012 i VIOLENT INCIDENTS AFFECTING
ITMF Disaster Recovery and Business Continuity Committee Report for the UGA IT Master Plan
 ITMF Disaster Recovery and Business Continuity Committee Report for the UGA IT Master Plan I. Executive Summary Planning for continued operation during unforeseen catastrophic events, and for returning
ITMF Disaster Recovery and Business Continuity Committee Report for the UGA IT Master Plan I. Executive Summary Planning for continued operation during unforeseen catastrophic events, and for returning
Giving you peace of mind 24 hours a day Wherever you operate
 Giving you peace of mind 24 hours a day Wherever you operate Contents Contents Introduction - Medilink International 2 Your Business in Safe Hands 10 Our People 11 Our Services 11 Health & Safety 12 Audit
Giving you peace of mind 24 hours a day Wherever you operate Contents Contents Introduction - Medilink International 2 Your Business in Safe Hands 10 Our People 11 Our Services 11 Health & Safety 12 Audit
EMS Subspecialty Certification Review Course. Learning Objectives 2. Medical Oversight of EMS Systems 2.1 Medical Oversight
 EMS Subspecialty Certification Review Course Medical Oversight of EMS Systems 2.1 Medical Oversight Version Date: 7.31.15 Learning Objectives 1 Upon the completion of this program participants will be
EMS Subspecialty Certification Review Course Medical Oversight of EMS Systems 2.1 Medical Oversight Version Date: 7.31.15 Learning Objectives 1 Upon the completion of this program participants will be
Hank Christen 02/09/01. The DMAT Safety Officer By Hank Christen, Fl-1 DMAT
 Hank Christen 02/09/01 The DMAT Safety Officer By Hank Christen, Fl-1 DMAT Introduction: The DMAT Safety Officer is a member of the Command Staff, and is directly supervised by the DMAT Unit Commander
Hank Christen 02/09/01 The DMAT Safety Officer By Hank Christen, Fl-1 DMAT Introduction: The DMAT Safety Officer is a member of the Command Staff, and is directly supervised by the DMAT Unit Commander
STATEMENT. RE: Telemedicine. May 1, 2014. of the. American Medical Association. to the
 STATEMENT of the American Medical Association to the House Committee on Energy and Commerce Subcommittee on Health United States House of Representatives RE: Telemedicine May 1, 2014 Division of Legislative
STATEMENT of the American Medical Association to the House Committee on Energy and Commerce Subcommittee on Health United States House of Representatives RE: Telemedicine May 1, 2014 Division of Legislative
How To Write An Interim Report On A Disaster In Australia
 REPORTING Second Draft Post-Disaster Damage Assessment and Need Analysis PO Box 4, Klong Luang Pathumthani 12120 Thailand www.adpc.ait.ac.th TABLE OF CONTENTS Page 1. Introduction 2 2. Types of Assessment
REPORTING Second Draft Post-Disaster Damage Assessment and Need Analysis PO Box 4, Klong Luang Pathumthani 12120 Thailand www.adpc.ait.ac.th TABLE OF CONTENTS Page 1. Introduction 2 2. Types of Assessment
Occupational Outlook Handbook, 2004-05 Edition
 Occupational Outlook Handbook, 2004-05 Edition U.S. Department of Labor Bureau of Labor Statistics Bulletin 2540 Registered Nurses + Chris is pleased with the favorable job outlook. Job security is important
Occupational Outlook Handbook, 2004-05 Edition U.S. Department of Labor Bureau of Labor Statistics Bulletin 2540 Registered Nurses + Chris is pleased with the favorable job outlook. Job security is important
Letter dated 27 August 2015 from the Secretary-General to the President of the Security Council
 United Nations S/2015/669 Security Council Distr.: General 27 August 2015 Original: English Letter dated 27 August 2015 from the Secretary-General to the President of the Security Council On 7 August 2015,
United Nations S/2015/669 Security Council Distr.: General 27 August 2015 Original: English Letter dated 27 August 2015 from the Secretary-General to the President of the Security Council On 7 August 2015,
The future of application outsourcing: making the move from tactical to strategic
 IBM Global Business Services White Paper The future of application outsourcing: making the move from tactical to strategic Application Services Page 2 Contents 2 Introduction 2 Success brings new challenges
IBM Global Business Services White Paper The future of application outsourcing: making the move from tactical to strategic Application Services Page 2 Contents 2 Introduction 2 Success brings new challenges
Appendix D Logistics Support Element MISSION ORGANIZATION
 Logistics Support Element Effective force projection logistics require a seamless logistics system operating across the strategic, operational, and tactical levels. Elements from CONUS and the theater
Logistics Support Element Effective force projection logistics require a seamless logistics system operating across the strategic, operational, and tactical levels. Elements from CONUS and the theater
DOD DIRECTIVE 4715.21 CLIMATE CHANGE ADAPTATION AND RESILIENCE
 DOD DIRECTIVE 4715.21 CLIMATE CHANGE ADAPTATION AND RESILIENCE Originating Component: Office of the Under Secretary of Defense for Acquisition, Technology, and Logistics Effective: January 14, 2016 Releasability:
DOD DIRECTIVE 4715.21 CLIMATE CHANGE ADAPTATION AND RESILIENCE Originating Component: Office of the Under Secretary of Defense for Acquisition, Technology, and Logistics Effective: January 14, 2016 Releasability:
Prepared by: Kate Tarrant Prepared February 3, 2015
 STATE POLICY TO PROMOTE EFFECTIVE TEACHING AND LEARNING Discussion Guide: In What Ways do Teaching Condition Support Effective Teachers? Prepared by: Kate Tarrant Prepared February 3, 2015 Please note
STATE POLICY TO PROMOTE EFFECTIVE TEACHING AND LEARNING Discussion Guide: In What Ways do Teaching Condition Support Effective Teachers? Prepared by: Kate Tarrant Prepared February 3, 2015 Please note
Community Policing. Defined
 Community Policing Defined The Primary Elements of Community Policing Nonprof its / Service Providers Using the Crime Triangle Community policing is a philosophy that promotes organizational strategies
Community Policing Defined The Primary Elements of Community Policing Nonprof its / Service Providers Using the Crime Triangle Community policing is a philosophy that promotes organizational strategies
Department of Defense INSTRUCTION
 Department of Defense INSTRUCTION NUMBER 6490.05 November 22, 2011 Incorporating Change 1, Effective October 2, 2013 USD(P&R) SUBJECT: Maintenance of Psychological Health in Military Operations References:
Department of Defense INSTRUCTION NUMBER 6490.05 November 22, 2011 Incorporating Change 1, Effective October 2, 2013 USD(P&R) SUBJECT: Maintenance of Psychological Health in Military Operations References:
ESCAMBIA COUNTY FIRE-RESCUE 3105.005
 Patrick T Grace, Fire Chief Page 1 of 13 PURPOSE: Escambia County Fire-Rescue responds to a wide range of emergency incidents. In order to effectively manage personnel and resources and to provide for
Patrick T Grace, Fire Chief Page 1 of 13 PURPOSE: Escambia County Fire-Rescue responds to a wide range of emergency incidents. In order to effectively manage personnel and resources and to provide for
Accreditation Program: Hospital. Emergency Management
 ccreditation Program: Hospital Emergency Management ccreditation of Healthcare Organizations ccreditation Program: Hospital Chapter: Emergency Management Standard EM.01.01.01 The [organization] engages
ccreditation Program: Hospital Emergency Management ccreditation of Healthcare Organizations ccreditation Program: Hospital Chapter: Emergency Management Standard EM.01.01.01 The [organization] engages
Health in the 2030 Agenda for Sustainable Development
 EXECUTIVE BOARD EB138/CONF./8 138th session 27 January 2016 Agenda item 7.2 Health in the 2030 Agenda for Sustainable Development Draft resolution proposed by Japan, Panama, South Africa, Thailand, United
EXECUTIVE BOARD EB138/CONF./8 138th session 27 January 2016 Agenda item 7.2 Health in the 2030 Agenda for Sustainable Development Draft resolution proposed by Japan, Panama, South Africa, Thailand, United
NCDs POLICY BRIEF - INDIA
 Age group Age group NCDs POLICY BRIEF - INDIA February 2011 The World Bank, South Asia Human Development, Health Nutrition, and Population NON-COMMUNICABLE DISEASES (NCDS) 1 INDIA S NEXT MAJOR HEALTH CHALLENGE
Age group Age group NCDs POLICY BRIEF - INDIA February 2011 The World Bank, South Asia Human Development, Health Nutrition, and Population NON-COMMUNICABLE DISEASES (NCDS) 1 INDIA S NEXT MAJOR HEALTH CHALLENGE
NGO security coordination and other sources of support WITHIN FIRST 1-2 WEEKS. Office/compound/ facility security
 3 Risk assessment tool BEFORE DEPLOYMENT OR STARTING PROGRAMME Context analysis and actor mapping Risk assessment Security strategies Acceptance, protection and deterrence What is the context and who are
3 Risk assessment tool BEFORE DEPLOYMENT OR STARTING PROGRAMME Context analysis and actor mapping Risk assessment Security strategies Acceptance, protection and deterrence What is the context and who are
The Challenges and Recommendations of Accessing to Affected Population for Humanitarian Assistance: A Narrative Review
 Global Journal of Health Science; Vol. 7, No. 3; 2015 ISSN 1916-9736 E-ISSN 1916-9744 Published by Canadian Center of Science and Education The Challenges and Recommendations of Accessing to Affected Population
Global Journal of Health Science; Vol. 7, No. 3; 2015 ISSN 1916-9736 E-ISSN 1916-9744 Published by Canadian Center of Science and Education The Challenges and Recommendations of Accessing to Affected Population
ER24 GLOBAL CARE SERVICES
 ER24 GLOBAL CARE SERVICES 1. ER24 SERVICES OVERVIEW Training Academy Global Care Services Occupational Healthcare Site Based Medical Services Fleet and Procurement Road Ambulance Services Corporate & Value
ER24 GLOBAL CARE SERVICES 1. ER24 SERVICES OVERVIEW Training Academy Global Care Services Occupational Healthcare Site Based Medical Services Fleet and Procurement Road Ambulance Services Corporate & Value
Aiding recovery?: a few thoughts on post-conflict rehabilitation
 Aiding recovery?: a few thoughts on post-conflict rehabilitation Speaking notes for the meeting Living with the megapower: implications of the war on terrorism Royal Institute of International Affairs,
Aiding recovery?: a few thoughts on post-conflict rehabilitation Speaking notes for the meeting Living with the megapower: implications of the war on terrorism Royal Institute of International Affairs,
Flexible, Life-Cycle Support for Unique Mission Requirements
 Flexible, Life-Cycle Support for Unique Mission Requirements We Meet the Need Anytime, Anywhere, Any Mission The customers we serve are diverse and so are their requirements. Transformational logistics
Flexible, Life-Cycle Support for Unique Mission Requirements We Meet the Need Anytime, Anywhere, Any Mission The customers we serve are diverse and so are their requirements. Transformational logistics
Quarterly Afghanistan UK Patient Treatment Statistics: RCDM and DMRC Headley Court 8 October 2007-30 June 2015
 Quarterly Afghanistan UK Patient Treatment Statistics: RCDM and DMRC Headley Court 8 October 2007-30 June 2015 Published 30 July 2015 This report provides statistical information on United Kingdom (UK)
Quarterly Afghanistan UK Patient Treatment Statistics: RCDM and DMRC Headley Court 8 October 2007-30 June 2015 Published 30 July 2015 This report provides statistical information on United Kingdom (UK)
Case Studies in Systems Engineering Central to the Success of Applied Systems Engineering Education Programs
 Complexity Case Studies in Systems Engineering Central to the Success of Applied Systems Engineering Education Programs Carlee A. Bishop Principal Research Engineer, Georgia Tech Research Institute Georgia
Complexity Case Studies in Systems Engineering Central to the Success of Applied Systems Engineering Education Programs Carlee A. Bishop Principal Research Engineer, Georgia Tech Research Institute Georgia
DEPARTMENT OF THE NAVY BUREAU OF MEDICNE AND SURGERY 2300 E STREET mi WASHINGTON DC 20372-5300
 DEPARTMENT OF THE NAVY BUREAU OF MEDICNE AND SURGERY 2300 E STREET mi WASHINGTON DC 20372-5300 IN REPlY REFER TO BUMEDINST 5450. 167A BUMED-MI2 BUMED INSTRUCTION 5450.167A Subj: MISSION, FUNCTIONS, AND
DEPARTMENT OF THE NAVY BUREAU OF MEDICNE AND SURGERY 2300 E STREET mi WASHINGTON DC 20372-5300 IN REPlY REFER TO BUMEDINST 5450. 167A BUMED-MI2 BUMED INSTRUCTION 5450.167A Subj: MISSION, FUNCTIONS, AND
*****IMPORTANT SUBMITTAL INFORMATION*****
 The following minimum criteria are to be used when developing Comprehensive Emergency Management Plans (CEMP) for all Nursing Homes. The criteria serve as the required plan format for the CEMP, and will
The following minimum criteria are to be used when developing Comprehensive Emergency Management Plans (CEMP) for all Nursing Homes. The criteria serve as the required plan format for the CEMP, and will
pm4dev, 2007 management for development series Project Management Organizational Structures PROJECT MANAGEMENT FOR DEVELOPMENT ORGANIZATIONS
 pm4dev, 2007 management for development series Project Management Organizational Structures PROJECT MANAGEMENT FOR DEVELOPMENT ORGANIZATIONS PROJECT MANAGEMENT FOR DEVELOPMENT ORGANIZATIONS A methodology
pm4dev, 2007 management for development series Project Management Organizational Structures PROJECT MANAGEMENT FOR DEVELOPMENT ORGANIZATIONS PROJECT MANAGEMENT FOR DEVELOPMENT ORGANIZATIONS A methodology
The Healthy Asia Pacific 2020 Roadmap INTRODUCTION: THE HEALTHY ASIA PACIFIC 2020 INITIATIVE
 The Healthy Asia Pacific 2020 Roadmap INTRODUCTION: THE HEALTHY ASIA PACIFIC 2020 INITIATIVE In the 2014 APEC Leader s Declaration and Joint Ministerial Statement, it is recognized that the prospect of
The Healthy Asia Pacific 2020 Roadmap INTRODUCTION: THE HEALTHY ASIA PACIFIC 2020 INITIATIVE In the 2014 APEC Leader s Declaration and Joint Ministerial Statement, it is recognized that the prospect of
WHO Consultation on the Zero Draft Global Mental Health Action Plan 2013-2020 International Diabetes Federation (IDF) Submission
 Submission") WHO Consultation on the Zero Draft Global Mental Health Action Plan 2013-2020 International Diabetes Federation (IDF) Submission The International Diabetes Federation (IDF), an umbrella organisation of
WHO Consultation on the Zero Draft Global Mental Health Action Plan 2013-2020 International Diabetes Federation (IDF) Submission The International Diabetes Federation (IDF), an umbrella organisation of
Before The President s Task Force on 21st Century Policing. February 23, 2015 The Newseum Washington, D.C.
 Written Testimony of Lieutenant Alexander L. Eastman, MD, MPH, FACS Dallas Police Department The Trauma Center at Parkland The University of Texas Southwestern Medical Center Before The President s Task
Written Testimony of Lieutenant Alexander L. Eastman, MD, MPH, FACS Dallas Police Department The Trauma Center at Parkland The University of Texas Southwestern Medical Center Before The President s Task
Cybersecurity: Mission integration to protect your assets
 Cybersecurity: Mission integration to protect your assets C Y B E R S O L U T I O N S P O L I C Y O P E R AT I O N S P E O P L E T E C H N O L O G Y M A N A G E M E N T Ready for what s next Cyber solutions
Cybersecurity: Mission integration to protect your assets C Y B E R S O L U T I O N S P O L I C Y O P E R AT I O N S P E O P L E T E C H N O L O G Y M A N A G E M E N T Ready for what s next Cyber solutions
Department of Defense INSTRUCTION. SUBJECT: Information Assurance (IA) in the Defense Acquisition System
 in the Defense Acquisition System") Department of Defense INSTRUCTION NUMBER 8580.1 July 9, 2004 SUBJECT: Information Assurance (IA) in the Defense Acquisition System ASD(NII) References: (a) Chapter 25 of title 40, United States Code (b)
Department of Defense INSTRUCTION NUMBER 8580.1 July 9, 2004 SUBJECT: Information Assurance (IA) in the Defense Acquisition System ASD(NII) References: (a) Chapter 25 of title 40, United States Code (b)