Practice Protocol. Buprenorphine Guidance Protocol
|
|
|
- Kelley Fowler
- 8 years ago
- Views:
Transcription
1 Practice Protocol Buprenorphine Guidance Protocol Developed by the Arizona Department of Health Services Division of Behavioral Health Services Effective Date: 02/23/11

2 Title Buprenorphine Guidance Protocol Goal/What Do We Want to Achieve Through the Use of this Protocol? The purpose of this document is to provide guidance to Behavioral Health Medical Practitioners within the State of Arizona. This document addresses practice which is consistent with Arizona Department of Health Services (ADHS) Office of Behavioral Health Licensing (OBHL) and Division of Behavioral Health Services (DBHS) standards. This document describes diagnostic requirements, prescribing and dosing strategies, laboratory monitoring strategies and recommendations and physical assessment prior to dosing recommendations. Guidance on psychotherapies that are consistent with buprenorphine treatment, patient selection recommendations, opiate withdrawal assessment protocols and issues relevant to special populations will be reviewed. Additionally, record storage and maintenance, informed consent, patient education, patient residential storage and confidentiality recommendations will be covered in this document. Target Audience Waived buprenorphine providers and OBHL licensed facilities within the State of Arizona. Target Population(s) Tribal and Regional Behavioral Health Authorities (T/RBHA) enrolled individuals above the age of 16 with the diagnosis of opiate dependency. Definitions Buprenorphine (Subutex, Suboxone) Opiate Dependency Opiate Withdrawal. Waived physician prescriber. Informed Consent Background The prevalence of opioid dependency has had a dramatic impact in the U.S. There are 810,000 to 1,000,000 chronic users of heroin in the U.S. (Office of National Drug Control Policy, 2003). The National Survey on Drug Use and Health (NSDUH) indicates that 53% of individuals who abused heroin become dependent. The lifetime use of opioid analgesics reached 29,611,000 in the U.S. in 2002 (NSDUH). Opioid dependency resulted in an increase in emergency room visits from 36,000 to 72,000 between 1991 and 1995 in the U.S. During the same time period, opioid-related 1

3 deaths increased from 2,300 to 4,000 in the U.S. (Substance Abuse and Mental Health Services Administration (SAMHSA) Mortality Data from DAWN, 2002). The prevalence of opioid abuse is increasing. Office-based buprenorphine treatment is intended to make opioid addiction treatment more available and to place the treatment of opioid dependency into mainstream medical practice. Recommended Process/Procedures A. Diagnostic requirements: DSM-IV-TR Criteria for Opioid Dependence: A maladaptive pattern of substance use, leading to clinically significant impairment or distress, as manifested by three (or more) of the DSM-IV-TR criteria occurring over a 12-month period. Examples of drugs which can lead to dependency include: 1. diacetylmorphine (heroin); 2. hydromorphine (Dilaudid), 3. oxycodone (OxyContin, Percodan, Percocet, and Tylox); 4. meperidine (Demerol); 5. hydrocodone (Lortab, Vicodin); 6. morphine (MS Contin, Oramorph), fentanyl (Sublimaze); 7. propoxyphene (Darvon); 8. methadone (Dolophine); 9. codeine and opium. Special Diagnostic Considerations for Individuals released from Corrections: Diagnostic decisions shall be based on the following factors before starting opioid dependency treatment which requires a review of clinical history: 1. length of incarceration; 2. post release addiction patterns and cycles; 3. addiction treatment history; 4. self-help involvement; and 5. reported triggers of illegal drug use and addiction upon release. (SAMHSA s TIP 40) B. Prescribing requirements: DATA 2000 enables qualifying physicians to receive a waiver from the special registration requirements in the Controlled Substances Act for the provision of medication-assisted opioid therapy. This waiver allows qualifying physicians to practice medication-assisted opioid addiction therapy with Schedule III, IV, or V narcotic medications specifically approved by the Food and Drug Administration (FDA). The Drug Enforcement Administration (DEA) assigns the physician a special identification number. DEA regulations require this ID number to be included on all buprenorphine prescriptions for opioid addiction therapy, along with the physician s regular DEA registration number. 2
")
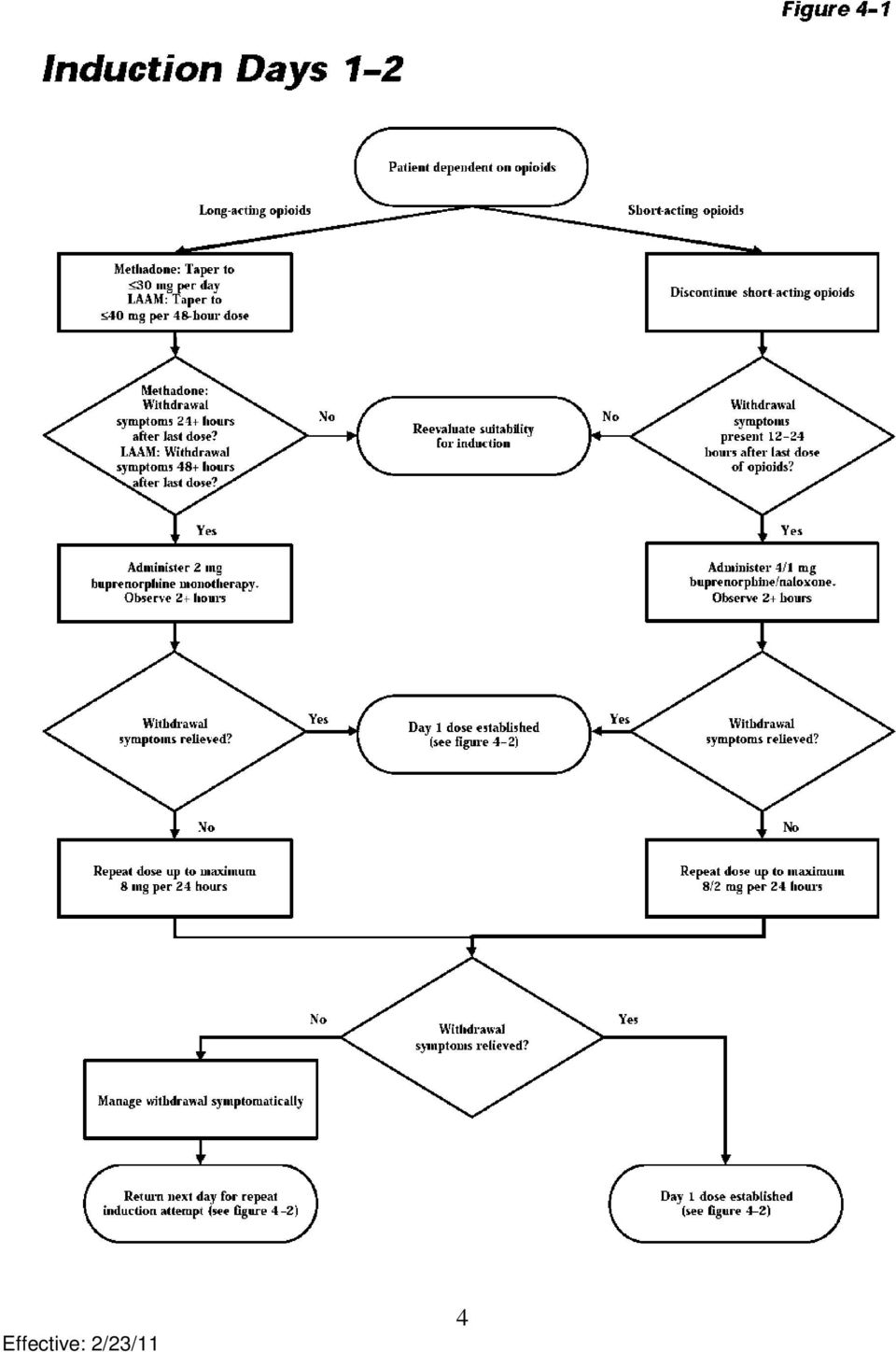
4 To qualify for a waiver under DATA 2000 a licensed physician (MD or DO) must meet any one or more of the following criteria: 1. The physician holds a subspecialty board certification in addiction psychiatry from the American Board of Medical Specialties; 2. The physician holds an addiction certification from the American Society of Addiction Medicine; 3. The physician holds a subspecialty board certification in addiction medicine from the American Osteopathic Association; 4. The physician has, with respect to the treatment and management of opioidaddicted patients, completed not less than eight hours of training (through classroom situations, seminars at professional society meetings, electronic communications, or otherwise) that is provided by the American Society of Addiction Medicine, the American Academy of Addiction Psychiatry, the American Medical Association, the American Osteopathic Association, the American Psychiatric Association, or any other organization that the Secretary determines is appropriate for purposes of this subclause. 5. The physician has participated as an investigator in one or more clinical trials leading to the approval of a narcotic drug in schedule III, IV, or V for maintenance or detoxification treatment, as demonstrated by a statement submitted to the Secretary by the sponsor of such approved drug. 6. The physician has such other training or experience as the State medical licensing board (of the State in which the physician will provide maintenance or detoxification treatment) considers to demonstrate the ability of the physician to treat and manage opioid-addicted patients. 7. The physician has such other training or experience as the Secretary of U.S. Department of Health and Human Services (DHHS) considers to demonstrate the ability of the physician to treat and manage opioid-addicted patients. Any criteria of the Secretary under this subclause shall be established by regulation. Any such criteria are effective only for 3 years after the date on which the criteria are promulgated, but may be extended for such additional discrete 3-year periods as the Secretary considers appropriate for purposes of this subclause. Such an extension of criteria may only be effectuated through a statement published in the Federal Register by the Secretary during the 30-day period preceding the end of the 3-year period involved. C. Clinical observation at critical phases of treatment: Waived buprenorphine providers must consider the entire process of treatment, which includes induction through stabilization, and then maintenance. Below are 1 suggested algorithms developed by Center for Substance Abuse Treatment. 1 Center for Substance Abuse Treatment, Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction. Treatment Improvement Protocol (TIP) Series 40. DHHS Publication No. (SMA) Rockville, MD: Substance Abuse and Mental Health Services Administration,

5 4
6 5

7 6

8 7

9 8

10 D. History and physical assessment prior to induction: The physical assessment must be supported by a comprehensive and accurate clinical history. The history should encompass the types of opioids abused and the history of usage. The provider should review first use, illicit vs. licit use, frequency and amounts, routes of administration, and recent use. The provider should consider tolerance and withdrawal, relapse frequency, and history of non-opioid substance use disorders. Psychiatric and medical histories should be components of the overall history. The physical assessment should evaluate the patient s sensorium and mental status. The medical provider should assess for dilated pupils (opioid withdrawal), constricted pupils (opioid intoxication), unstable vital signs, possible pregnancy, and medical conditions such as chronic pain, renal insufficiency, hepatitis, and HIV/AIDS. The provider should assess the patient for needle marks, cellulitis or dermal abscesses. Laboratory testing should be based on clinical history and the physical examination. Certain high risk medical illnesses should mandate specific laboratory tests. (American Academy of Addiction Psychiatry, 2008) E. Laboratory studies prior to induction and post-induction: The ordered laboratory studies should be based on the findings of the history and physical. The examiner should order pregnancy testing on all women of childbearing years with noted exceptions (i.e., hysterectomy, history of tubal ligation). Urine drug testing enhances treatment outcomes in patients receiving buprenorphine treatment. Urine drug testing is an integral part of on-going evaluation and treatment planning. The provider should consider mechanisms to maintain the validity of the results. In-office buprenorphine practice policies should cover in-office vs. off-site collection, random vs. scheduled, and observed vs. non-observed. Urine drug testing can allow for the monitoring of co-occurring substance use disorders. (American Academy of Addiction Psychiatry, 2008) Practice and prescribing should be based on the patient needs and FDA and State guidelines. F. Each behavioral health recipient has the right to participate in decisions regarding his or her behavioral health care, including the right to refuse treatment. It is important for persons seeking behavioral health services to agree to those services and be made aware of the service options and alternatives available to them as well as specific risks and benefits associated with these services. Providers shall reference ADHS/DBHS Provider Manual Section 3.11, General and Informed Consent to Treatment for additional guidance. G. Storage of records The patient record is: 9

11 1. Maintained on the premises of the behavioral health agency at which the patient is admitted until the patient is discharged; 2. Available and accessible to staff members who provide behavioral health services to the patient; 3. Retained after a patient's discharge: a. For a patient who is an adult, for 7 years after the date of the patient's discharge, unless otherwise provided by law or this chapter (9 A.A.C.20, Article 211 A); b. For a patient who is a child, for 7 years after the date of discharge or for at least 3 years after the date of the patient's 18th birthday, whichever is a longer period of time; and c. Disposed of in a manner that protects patient confidentiality. 4. Storage of Buprenorphine in the physician s office must include being stored under locked conditions and include record keeping tracking information on who received Buprenorphine and the quantity of drug dispensed. Pade (2008) reported the following: DEA record keeping requirements for office-based opioid therapy go beyond the Schedule III record keeping requirements. According to DEA: Practitioners must keep records (including an inventory that accounts for amounts received and amounts dispensed) for all controlled substances dispensed, including Subutex and Suboxone ( 21 CFR Section [c]). In some cases, patients return to the prescribing physician with their filled Subutex or Suboxone prescriptions so that the practitioner can monitor the induction process. While it is acceptable for the patient to return to the practitioner with their filled prescription supplies, practitioners shall not store and dispense controlled substances that are the result of filled patient prescriptions. Practitioners must keep records for controlled substances prescribed and dispensed to patients for maintenance or detoxification treatment (21 CFR Section [c]). Many practitioners comply with this requirement by creating a log that identifies the patient (an ID number may be used instead of name), the name of the drug prescribed or dispensed, as well as the strength and quantity and date of issuance or dispensing. Some physicians comply with this requirement by keeping a copy of the prescription in the patient record. Alternatively, DEA suggests that practitioners could keep separate records for controlled substances prescribed and dispensed for maintenance or detoxification treatment to facilitate the record reviews during physician inspections for DATA compliance. This way, DEA will only review those records related to controlled substances prescribed and dispensed for maintenance or detoxification treatment for physicians maintaining separate records. H. Storage of buprenorphine in the patient s home It is best to store the medication in a location other than where vitamins, aspirin or other over-the-counter medications are stored to avoid any confusion. 10

12 Buprenorphine must be stored in a location that is safe and kept away from children or pets. If buprenorphine is taken by a family member or a person by mistake he or she should be evaluated by a physician immediately. I. Special Treatment Populations The physician should take special considerations when prescribing in the populations below: 1. Pregnant women 2. Adolescents 3. Geriatric Population 4. Persons suffering from pain 5. Persons with a comorbidities (e.g. Hepatitis, HIV, TB, etc) 6. High risk psychiatric patients with suicidal ideation and impaired judgment 7. Under the jurisdiction of the criminal justice system 8. Persons who have a concurrent alcohol or other substance abuse disorders J. Opioid Withdrawal Protocols The physician should consider the use of objective opiate withdrawal assessment instruments (e.g., Clinical Opiate Withdrawal Scale (COWS). Training and Supervision Recommendations Per DATA 2000, training that meets the requirement for a waiver may be provided by the American Academy of Addiction Psychiatry, the American Medical Association, the American Osteopathic Academy of Addiction Medicine, the American Psychiatric Association, the American Society of Addiction Medicine, and other organizations that the Secretary of the Department of Health and Human Services determines are appropriate for this purpose. DATA-qualifying training must include not less than eight hours of instruction on the treatment and management of opioid-addicted patients. Also, as part of training in the treatment of opioid addiction, physicians should at a minimum be a licensed physician to practice medicine in the state of Arizona and obtain some knowledge about the basic principles of brief intervention in case of relapse. Physicians considering providing opioid addiction care should ensure that they are capable and capable of providing psychosocial services. In fact, DATA 2000 stipulates that when physicians submit notification to SAMHSA to obtain the required waiver to practice opioid addiction treatment outside the outpatient treatment program setting, they must attest to their capacity to refer such patients for appropriate counseling and other non-pharmacological therapies. Anticipated Outcomes Maintenance of Office of Behavioral Health Licensing license: A. Measured by office inspections conducted by Office of Behavioral Health Licensing. Avoidance of Critical Events within the office practice: A. Measured by critical incidence reporting by T/RBHA to ADHS/DBHS. 11
 6. High risk psychiatric patients with suicidal ideation and impaired judgment 7.")
13 Resources: American Academy of Addiction Psychiatry (AAAP) Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction: A Treatment Improvement Protocol (TIP) 40 SAMHSA Buprenorphine Information Center at: Suboxone manufacturer s web page at: 12

14 ADHS/DBHS Practice Protocol Buprenorphine Guidance Protocol Desktop Guide Key elements to remember about this best practice: Establishing a maintenance dosage of medications Regulatory issues related to buprenorphine Licensed physicians must be capable and comfortable with opioid addiction Understanding the practice associated with buprenorphine Benefits of using this best practice: Intended to make opioid addiction treatment more available Intended to place the treatment of opioid dependency into mainstream medical practice 13

Ohio Legislative Service Commission
 Ohio Legislative Service Commission Bill Analysis Brian D. Malachowsky H.B. 378 130th General Assembly () Reps. Smith and Sprague BILL SUMMARY Prohibits a physician from prescribing or personally furnishing
Ohio Legislative Service Commission Bill Analysis Brian D. Malachowsky H.B. 378 130th General Assembly () Reps. Smith and Sprague BILL SUMMARY Prohibits a physician from prescribing or personally furnishing
TENNESSEE BOARD OF MEDICAL EXAMINERS POLICY STATEMENT OFFICE-BASED TREATMENT OF OPIOID ADDICTION
 TENNESSEE BOARD OF MEDICAL EXAMINERS POLICY STATEMENT OFFICE-BASED TREATMENT OF OPIOID ADDICTION The Tennessee Board of Medical Examiners has reviewed the Model Policy Guidelines for Opioid Addiction Treatment
TENNESSEE BOARD OF MEDICAL EXAMINERS POLICY STATEMENT OFFICE-BASED TREATMENT OF OPIOID ADDICTION The Tennessee Board of Medical Examiners has reviewed the Model Policy Guidelines for Opioid Addiction Treatment
Information for Pharmacists
 Page 43 by 42 CFR part 2. A general authorization for the release of medical or other information is NOT sufficient for this purpose. Information for Pharmacists SUBOXONE (buprenorphine HCl/naloxone HCl
Page 43 by 42 CFR part 2. A general authorization for the release of medical or other information is NOT sufficient for this purpose. Information for Pharmacists SUBOXONE (buprenorphine HCl/naloxone HCl
Testimony Engrossed House Bill 1101 Department of Human Services Senate Human Services Committee Senator Judy Lee, Chairman February 19, 2013
 Testimony Engrossed House Bill 1101 Department of Human Services Senate Human Services Committee Senator Judy Lee, Chairman February 19, 2013 Chairman Lee, members of the Senate Human Services Committee,
Testimony Engrossed House Bill 1101 Department of Human Services Senate Human Services Committee Senator Judy Lee, Chairman February 19, 2013 Chairman Lee, members of the Senate Human Services Committee,
Buprenorphine/Naloxone Maintenance Treatment for Opioid Dependence
 Buprenorphine/Naloxone Maintenance Treatment for Opioid Dependence Information for Family Members Family members of patients who have been prescribed buprenorphine/naloxone for treatment of opioid addiction
Buprenorphine/Naloxone Maintenance Treatment for Opioid Dependence Information for Family Members Family members of patients who have been prescribed buprenorphine/naloxone for treatment of opioid addiction
Section 303(g)(2)(G) of the Controlled Substances Act (21 U.S.C. 823(g)(2)(G)) is amended. (1) by striking clause (ii) and inserting the following:
(2)(G) of the Controlled Substances Act (21 U.S.C. 823(g)(2)(G)) is amended. (1) by striking clause (ii) and inserting the following:") Section XX. Definitions. Section 303(g)(2)(G) of the Controlled Substances Act (21 U.S.C. 823(g)(2)(G)) is amended (1) by striking clause (ii) and inserting the following: (ii) The term qualifying practitioner
Section XX. Definitions. Section 303(g)(2)(G) of the Controlled Substances Act (21 U.S.C. 823(g)(2)(G)) is amended (1) by striking clause (ii) and inserting the following: (ii) The term qualifying practitioner
Care Management Council submission date: August 2013. Contact Information
 Clinical Practice Approval Form Clinical Practice Title: Acute use of Buprenorphine for the Treatment of Opioid Dependence and Detoxification Type of Review: New Clinical Practice Revisions of Existing
Clinical Practice Approval Form Clinical Practice Title: Acute use of Buprenorphine for the Treatment of Opioid Dependence and Detoxification Type of Review: New Clinical Practice Revisions of Existing
2015 OPSC Annual Convention. syllabus. February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California
 2015 OPSC Annual Convention syllabus February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California FRIDAY, FEBRUARY 6, 2015: 9:30am - 10:30am Opioid Addiction and Buprenorphine Use * Presented by
2015 OPSC Annual Convention syllabus February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California FRIDAY, FEBRUARY 6, 2015: 9:30am - 10:30am Opioid Addiction and Buprenorphine Use * Presented by
Opioid Treatment Services, Office-Based Opioid Treatment
 Optum 1 By United Behavioral Health U.S. Behavioral Health Plan, California Doing Business as OptumHealth Behavioral Solutions of California ( OHBS-CA ) 2015 Level of Care Guidelines Opioid Treatment Services,
Optum 1 By United Behavioral Health U.S. Behavioral Health Plan, California Doing Business as OptumHealth Behavioral Solutions of California ( OHBS-CA ) 2015 Level of Care Guidelines Opioid Treatment Services,
MEDICAL ASSISTANCE BULLETIN
 ISSUE DATE SUBJECT EFFECTIVE DATE MEDICAL ASSISTANCE BULLETIN NUMBER *See below BY Prior Authorization of Opiate Dependence Treatments Pharmacy Service Leesa M. Allen, Deputy Secretary Office of Medical
ISSUE DATE SUBJECT EFFECTIVE DATE MEDICAL ASSISTANCE BULLETIN NUMBER *See below BY Prior Authorization of Opiate Dependence Treatments Pharmacy Service Leesa M. Allen, Deputy Secretary Office of Medical
Physician Information. Answers to Frequently Asked Questions
 Page 31 Physician Information Answers to Frequently Asked Questions Who is qualified to prescribe SUBOXONE or SUBUTEX? Physicians who: Meet one or more of the following training requirements Hold a subspecialty
Page 31 Physician Information Answers to Frequently Asked Questions Who is qualified to prescribe SUBOXONE or SUBUTEX? Physicians who: Meet one or more of the following training requirements Hold a subspecialty
Presentation to Senate Health and Human Services Committee: Prescription Drug Abuse in Texas
 Presentation to Senate Health and Human Services Committee: Prescription Drug Abuse in Texas David Lakey, MD Commissioner, Department of State Health Services Lauren Lacefield Lewis Assistant Commissioner,
Presentation to Senate Health and Human Services Committee: Prescription Drug Abuse in Texas David Lakey, MD Commissioner, Department of State Health Services Lauren Lacefield Lewis Assistant Commissioner,
MEDICAL POLICY Treatment of Opioid Dependence
 POLICY........ PG-0313 EFFECTIVE......11/11/14 LAST REVIEW... 07/14/15 MEDICAL POLICY Treatment of Opioid Dependence GUIDELINES This policy does not certify benefits or authorization of benefits, which
POLICY........ PG-0313 EFFECTIVE......11/11/14 LAST REVIEW... 07/14/15 MEDICAL POLICY Treatment of Opioid Dependence GUIDELINES This policy does not certify benefits or authorization of benefits, which
MEDICAL ASSISTANCE BULLETIN
 ISSUE DATE September 4, 2015 SUBJECT EFFECTIVE DATE September 9, 2015 MEDICAL ASSISTANCE BULLETIN NUMBER *See below BY Prior Authorization of Opiate Dependence Treatments, Oral Buprenorphine Agents - Pharmacy
ISSUE DATE September 4, 2015 SUBJECT EFFECTIVE DATE September 9, 2015 MEDICAL ASSISTANCE BULLETIN NUMBER *See below BY Prior Authorization of Opiate Dependence Treatments, Oral Buprenorphine Agents - Pharmacy
How To Treat Anorexic Addiction With Medication Assisted Treatment
 Medication Assisted Treatment for Opioid Addiction Tanya Hiser, MS, LPC Premier Care of Wisconsin, LLC October 21, 2015 How Did We Get Here? Civil War veterans and women 19th Century physicians cautious
Medication Assisted Treatment for Opioid Addiction Tanya Hiser, MS, LPC Premier Care of Wisconsin, LLC October 21, 2015 How Did We Get Here? Civil War veterans and women 19th Century physicians cautious
Program Assistance Letter
 Program Assistance Letter DOCUMENT NUMBER: 2004-01 DATE: December 5, 2003 DOCUMENT TITLE: Use of Buprenorphine in Health Center Substance Abuse Treatment Programs TO: All Bureau of Primary Health Care
Program Assistance Letter DOCUMENT NUMBER: 2004-01 DATE: December 5, 2003 DOCUMENT TITLE: Use of Buprenorphine in Health Center Substance Abuse Treatment Programs TO: All Bureau of Primary Health Care
The Determinations Report: A Report On the Physician Waiver Program Established by the. Drug Addiction Treatment Act of 2000 ( DATA )
") The Determinations Report: A Report On the Physician Waiver Program Established by the Drug Addiction Treatment Act of 2000 ( DATA ) Submitted by the Center for Substance Abuse Treatment, Substance Abuse
The Determinations Report: A Report On the Physician Waiver Program Established by the Drug Addiction Treatment Act of 2000 ( DATA ) Submitted by the Center for Substance Abuse Treatment, Substance Abuse
Substance Abuse Treatment Admissions Involving Abuse of Pain Relievers: 1998 and 2008
 Treatment Episode Data Set The TEDS Report July 15, 010 Substance Abuse Treatment Admissions Involving Abuse of Pain Relievers: 1998 and 008 In Brief The proportion of all substance abuse treatment admissions
Treatment Episode Data Set The TEDS Report July 15, 010 Substance Abuse Treatment Admissions Involving Abuse of Pain Relievers: 1998 and 008 In Brief The proportion of all substance abuse treatment admissions
INSTRUCTIONS AND PROTOCOLS FOR THE IMPLEMENTATION OF MEDICATION-ASSISTED TREATMENT FOR OPIOID/OPIATE DEPENDENCE
 201 Mulholland Bay City, MI 48708 P 989-497-1344 F 989-497-1348 www.riverhaven-ca.org Title: MAT Protocol Original Date: March 30, 2009 Latest Revision Date: December 16, 2013 Approval/Release Date: January
201 Mulholland Bay City, MI 48708 P 989-497-1344 F 989-497-1348 www.riverhaven-ca.org Title: MAT Protocol Original Date: March 30, 2009 Latest Revision Date: December 16, 2013 Approval/Release Date: January
Treatment of Opioid Dependence: A Randomized Controlled Trial. Karen L. Sees, DO, Kevin L. Delucchi, PhD, Carmen Masson, PhD, Amy
 Category: Heroin Title: Methadone Maintenance vs 180-Day psychosocially Enriched Detoxification for Treatment of Opioid Dependence: A Randomized Controlled Trial Authors: Karen L. Sees, DO, Kevin L. Delucchi,
Category: Heroin Title: Methadone Maintenance vs 180-Day psychosocially Enriched Detoxification for Treatment of Opioid Dependence: A Randomized Controlled Trial Authors: Karen L. Sees, DO, Kevin L. Delucchi,
Prescription drug abuse trends. Minnesota s Prescription Monitoring Program. Minnesota Rural Health Conference June 25, 2013 Duluth
 Prescription drug abuse trends Minnesota s Prescription Monitoring Program Carol Falkowski Drug Abuse Dialogues www.drugabusedialogues.com Barbara Carter, Manager MN Board of Pharmacy www.pmp.pharmacy.state.mn.us
Prescription drug abuse trends Minnesota s Prescription Monitoring Program Carol Falkowski Drug Abuse Dialogues www.drugabusedialogues.com Barbara Carter, Manager MN Board of Pharmacy www.pmp.pharmacy.state.mn.us
Office-based Treatment of Opioid Dependence with Buprenorphine
 Office-based Treatment of Opioid Dependence with Buprenorphine David A. Fiellin, M.D Professor of Medicine, Investigative Medicine and Public Health Yale University School of Medicine Dr. Fiellin s Disclosures
Office-based Treatment of Opioid Dependence with Buprenorphine David A. Fiellin, M.D Professor of Medicine, Investigative Medicine and Public Health Yale University School of Medicine Dr. Fiellin s Disclosures
Opioid/Opiate Dependent Pregnant Women
 Opioid/Opiate Dependent Pregnant Women The epidemic, safety, stigma, and how to help. Presented by Lisa Ramirez MA,LCDC & Kerby Stewart MD The prescription painkiller epidemic is killing more women than
Opioid/Opiate Dependent Pregnant Women The epidemic, safety, stigma, and how to help. Presented by Lisa Ramirez MA,LCDC & Kerby Stewart MD The prescription painkiller epidemic is killing more women than
KENTUCKY ADMINISTRATIVE REGULATIONS TITLE 201. GENERAL GOVERNMENT CABINET CHAPTER 9. BOARD OF MEDICAL LICENSURE
 KENTUCKY ADMINISTRATIVE REGULATIONS TITLE 201. GENERAL GOVERNMENT CABINET CHAPTER 9. BOARD OF MEDICAL LICENSURE 201 KAR 9:260. Professional standards for prescribing and dispensing controlled substances.
KENTUCKY ADMINISTRATIVE REGULATIONS TITLE 201. GENERAL GOVERNMENT CABINET CHAPTER 9. BOARD OF MEDICAL LICENSURE 201 KAR 9:260. Professional standards for prescribing and dispensing controlled substances.
S. ll. To provide access to medication-assisted therapy, and for other purposes. IN THE SENATE OF THE UNITED STATES A BILL
 ALB TH CONGRESS D SESSION S. ll To provide access to medication-assisted therapy, and for other purposes. IN THE SENATE OF THE UNITED STATES llllllllll Mr. MARKEY (for himself, Mrs. FEINSTEIN, Mr. ROCKEFELLER,
ALB TH CONGRESS D SESSION S. ll To provide access to medication-assisted therapy, and for other purposes. IN THE SENATE OF THE UNITED STATES llllllllll Mr. MARKEY (for himself, Mrs. FEINSTEIN, Mr. ROCKEFELLER,
Considerations in Medication Assisted Treatment of Opiate Dependence. Stephen A. Wyatt, D.O. Dept. of Psychiatry Middlesex Hospital Middletown, CT
 Considerations in Medication Assisted Treatment of Opiate Dependence Stephen A. Wyatt, D.O. Dept. of Psychiatry Middlesex Hospital Middletown, CT Disclosures Speaker Panels- None Grant recipient - SAMHSA
Considerations in Medication Assisted Treatment of Opiate Dependence Stephen A. Wyatt, D.O. Dept. of Psychiatry Middlesex Hospital Middletown, CT Disclosures Speaker Panels- None Grant recipient - SAMHSA
ADVISORY OPINION THE USE OF CONTROLLED SUBSTANCES FOR THE TREATMENT OF CHRONIC PAIN
 Doug Ducey Governor Arizona State Board of Nursing 4747 North 7 th Street, Suite 200 Phoenix, AZ 85014-3655 Phone (602) 771-7800 Fax - (602) 771-7888 E-Mail: arizona@azbn.gov Home Page: www.azbn.gov Joey
Doug Ducey Governor Arizona State Board of Nursing 4747 North 7 th Street, Suite 200 Phoenix, AZ 85014-3655 Phone (602) 771-7800 Fax - (602) 771-7888 E-Mail: arizona@azbn.gov Home Page: www.azbn.gov Joey
SUBOXONE /VIVITROL WEBINAR. Educational Training tool concerning the Non-Methadone Medication Assisted Treatment Policy that is Effective on 1/1/12
 SUBOXONE /VIVITROL WEBINAR Educational Training tool concerning the Non-Methadone Medication Assisted Treatment Policy that is Effective on 1/1/12 WEBINAR INTRODUCTIONS Cynthia Parsons- Program Manager
SUBOXONE /VIVITROL WEBINAR Educational Training tool concerning the Non-Methadone Medication Assisted Treatment Policy that is Effective on 1/1/12 WEBINAR INTRODUCTIONS Cynthia Parsons- Program Manager
RULES OF THE ALABAMA BOARD OF MEDICAL EXAMINERS
 RULES OF THE ALABAMA BOARD OF MEDICAL EXAMINERS CHAPTER 540-X-21 POLICY ON DATA 2000: GUIDELINES FOR THE TREATMENT OF OPIOID ADDICTION IN THE MEDICAL OFFICE 1 Table of Contents 540-X-21-.01 Introduction
RULES OF THE ALABAMA BOARD OF MEDICAL EXAMINERS CHAPTER 540-X-21 POLICY ON DATA 2000: GUIDELINES FOR THE TREATMENT OF OPIOID ADDICTION IN THE MEDICAL OFFICE 1 Table of Contents 540-X-21-.01 Introduction
Opiate Abuse and Mental Illness
 visited on Page 1 of 5 LEARN MORE (HTTP://WWW.NAMI.ORG/LEARN-MORE) FIND SUPPORT (HTTP://WWW.NAMI.ORG/FIND-SUPPORT) GET INVOLVED (HTTP://WWW.NAMI.ORG/GET-INVOLVED) DONATE (HTTPS://NAMI360.NAMI.ORG/EWEB/DYNAMICPAGE.ASPX?
visited on Page 1 of 5 LEARN MORE (HTTP://WWW.NAMI.ORG/LEARN-MORE) FIND SUPPORT (HTTP://WWW.NAMI.ORG/FIND-SUPPORT) GET INVOLVED (HTTP://WWW.NAMI.ORG/GET-INVOLVED) DONATE (HTTPS://NAMI360.NAMI.ORG/EWEB/DYNAMICPAGE.ASPX?
INFO Brief. Prescription Opioid Use: Pain Management and Drug Abuse In King County and Washington State
 ADAI-IB 23-3 INFO Brief Prescription Opioid Use: Pain Management and Drug Abuse In King County and Washington State O ctober 23 Caleb Banta-Green (Alcohol and Drug Abuse Institute, University of Washington),
ADAI-IB 23-3 INFO Brief Prescription Opioid Use: Pain Management and Drug Abuse In King County and Washington State O ctober 23 Caleb Banta-Green (Alcohol and Drug Abuse Institute, University of Washington),
Understanding Medication Assisted Treatment (MAT) for Families Affected by Substance Use Disorders
 for Families Affected by Substance Use Disorders") Understanding Medication Assisted Treatment (MAT) for Families Affected by Substance Use Disorders March 20, 2013 Pamela Petersen- Baston, MPA, CAP, CPP 4 9 4 0 I r v i n e B l v d., S u i t e 2 0 2 I
Understanding Medication Assisted Treatment (MAT) for Families Affected by Substance Use Disorders March 20, 2013 Pamela Petersen- Baston, MPA, CAP, CPP 4 9 4 0 I r v i n e B l v d., S u i t e 2 0 2 I
TRENDS IN HEROIN USE IN THE UNITED STATES: 2002 TO 2013
 2013 to 2002 States: United the in Use Heroin in Trends National Survey on Drug Use and Health Short Report April 23, 2015 TRENDS IN HEROIN USE IN THE UNITED STATES: 2002 TO 2013 AUTHORS Rachel N. Lipari,
2013 to 2002 States: United the in Use Heroin in Trends National Survey on Drug Use and Health Short Report April 23, 2015 TRENDS IN HEROIN USE IN THE UNITED STATES: 2002 TO 2013 AUTHORS Rachel N. Lipari,
POLICY AND PROCEDURES FOR PROVIDING NARCOTIC ADDICTION TREATMENT TO PREGNANT OPIOID DEPENDENT INMATES INCARCERATED IN THE COUNTY JAIL
 PURPOSE POLICY AND PROCEDURES FOR PROVIDING NARCOTIC ADDICTION TREATMENT TO PREGNANT OPIOID DEPENDENT INMATES INCARCERATED IN THE COUNTY JAIL To outline the procedures used in recognizing and providing
PURPOSE POLICY AND PROCEDURES FOR PROVIDING NARCOTIC ADDICTION TREATMENT TO PREGNANT OPIOID DEPENDENT INMATES INCARCERATED IN THE COUNTY JAIL To outline the procedures used in recognizing and providing
This module reviews the following: Opioid addiction and the brain Descriptions and definitions of opioid agonists,
 BUPRENORPHINE TREATMENT: A Training For Multidisciplinary Addiction Professionals Module II Opioids 101 Goals for Module II This module reviews the following: Opioid addiction and the brain Descriptions
BUPRENORPHINE TREATMENT: A Training For Multidisciplinary Addiction Professionals Module II Opioids 101 Goals for Module II This module reviews the following: Opioid addiction and the brain Descriptions
Various therapies are used in the
 National Survey of Substance Abuse Treatment Services The N-SSATS Report January 28, 2010 Overview of Opioid Treatment Programs within the United States: 2008 In Brief In 2008, a total of 1,132 (8 of all
National Survey of Substance Abuse Treatment Services The N-SSATS Report January 28, 2010 Overview of Opioid Treatment Programs within the United States: 2008 In Brief In 2008, a total of 1,132 (8 of all
Minimum Insurance Benefits for Patients with Opioid Use Disorder The Opioid Use Disorder Epidemic: The Evidence for Opioid Treatment:
 Minimum Insurance Benefits for Patients with Opioid Use Disorder By David Kan, MD and Tauheed Zaman, MD Adopted by the California Society of Addiction Medicine Committee on Opioids and the California Society
Minimum Insurance Benefits for Patients with Opioid Use Disorder By David Kan, MD and Tauheed Zaman, MD Adopted by the California Society of Addiction Medicine Committee on Opioids and the California Society
The Heroin and Prescription Drug Abuse Prevention and Reduction Act Section by Section
 The Heroin and Prescription Drug Abuse Prevention and Reduction Act Section by Section TITLE I: PREVENTION SUBTITLE A- PRESCRIBER EDUCATION PRACTITIONER EDUCATION This subtitle requires practitioners who
The Heroin and Prescription Drug Abuse Prevention and Reduction Act Section by Section TITLE I: PREVENTION SUBTITLE A- PRESCRIBER EDUCATION PRACTITIONER EDUCATION This subtitle requires practitioners who
American Society of Addiction Medicine
 American Society of Addiction Medicine Public Policy Statement on Office-based Opioid Agonist Treatment (OBOT) BACKGROUND Methadone maintenance treatment of opioid addiction was developed in 1965 and implemented
American Society of Addiction Medicine Public Policy Statement on Office-based Opioid Agonist Treatment (OBOT) BACKGROUND Methadone maintenance treatment of opioid addiction was developed in 1965 and implemented
Medication-Assisted Treatment for Opiate Addiction and the Public Financing of that Treatment
 Medication-Assisted Treatment for Opiate Addiction and the Public Financing of that Treatment Introduction March 3, 2008 By: Suzanne Gelber, MSW, Ph.D., Managing Partner, The Avisa Group Defining Characteristics
Medication-Assisted Treatment for Opiate Addiction and the Public Financing of that Treatment Introduction March 3, 2008 By: Suzanne Gelber, MSW, Ph.D., Managing Partner, The Avisa Group Defining Characteristics
Death in the Suburbs: How Prescription Painkillers and Heroin Have Changed Treatment and Recovery
 Death in the Suburbs: How Prescription Painkillers and Heroin Have Changed Treatment and Recovery Marvin D. Seppala, MD Chief Medical Officer Hazelden Betty Ford Foundation This product is supported by
Death in the Suburbs: How Prescription Painkillers and Heroin Have Changed Treatment and Recovery Marvin D. Seppala, MD Chief Medical Officer Hazelden Betty Ford Foundation This product is supported by
ST. CLAIR COUNTY COMMUNITY MENTAL HEALTH Date Issued: 07/09 Date Revised: 09/11;03/13;06/14;07/15
 ST. CLAIR COUNTY COMMUNITY MENTAL HEALTH Date Issued: 07/09 Date Revised: 09/11;/13;06/14;07/15 WRITTEN BY Jim Johnson Page 1 REVISED BY AUTHORIZED BY Jessica Moeller Debra Johnson I. APPLICATION: THUMB
ST. CLAIR COUNTY COMMUNITY MENTAL HEALTH Date Issued: 07/09 Date Revised: 09/11;/13;06/14;07/15 WRITTEN BY Jim Johnson Page 1 REVISED BY AUTHORIZED BY Jessica Moeller Debra Johnson I. APPLICATION: THUMB
OVERVIEW OF MEDICATION ASSISTED TREATMENT
 Sarah Akerman MD Assistant Professor of Psychiatry Director of Addiction Services Geisel School of Medicine/Dartmouth-Hitchcock Medical Center OVERVIEW OF MEDICATION ASSISTED TREATMENT Conflicts of Interest
Sarah Akerman MD Assistant Professor of Psychiatry Director of Addiction Services Geisel School of Medicine/Dartmouth-Hitchcock Medical Center OVERVIEW OF MEDICATION ASSISTED TREATMENT Conflicts of Interest
Model Policy on DATA 2000 and Treatment of Opioid Addiction in the Medical Office
 Model Policy on DATA 2000 and Treatment of Opioid Addiction in the Medical Office The recommendations contained herein were adopted as policy by the House of Delegates of the Federation of State Medical
Model Policy on DATA 2000 and Treatment of Opioid Addiction in the Medical Office The recommendations contained herein were adopted as policy by the House of Delegates of the Federation of State Medical
MAT Disclosures & Consents 1 of 6. Authorization & Disclosure
 MAT Disclosures & Consents 1 of 6 Authorization & Disclosure ***YOUR INSURANCE MAY NOT PAY FOR ROUTINE SCREENING*** *** APPROPRIATE SCREENING DIAGNOSES MUST BE PROVIDED WHEN INDICATED*** Urine Drug Test
MAT Disclosures & Consents 1 of 6 Authorization & Disclosure ***YOUR INSURANCE MAY NOT PAY FOR ROUTINE SCREENING*** *** APPROPRIATE SCREENING DIAGNOSES MUST BE PROVIDED WHEN INDICATED*** Urine Drug Test
RULES OF THE TENNESSEE DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES
 RULES OF THE TENNESSEE DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES CHAPTER 0940-05-42 MINIMUM PROGRAM REQUIREMENTS FOR NON-RESIDENTIAL OPIOID TREATMENT PROGRAM FACILITIES TABLE OF CONTENTS
RULES OF THE TENNESSEE DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES CHAPTER 0940-05-42 MINIMUM PROGRAM REQUIREMENTS FOR NON-RESIDENTIAL OPIOID TREATMENT PROGRAM FACILITIES TABLE OF CONTENTS
ALABAMA BOARD OF MEDICAL EXAMINERS ADMINISTRATIVE CODE
 Medical Examiners Chapter 540-X-21 ALABAMA BOARD OF MEDICAL EXAMINERS ADMINISTRATIVE CODE CHAPTER 540-X-21 POLICY ON DATA 2000: GUIDELINES FOR THE TREATMENT OF OPIOID ADDICTION IN THE MEDICAL OFFICE 1
Medical Examiners Chapter 540-X-21 ALABAMA BOARD OF MEDICAL EXAMINERS ADMINISTRATIVE CODE CHAPTER 540-X-21 POLICY ON DATA 2000: GUIDELINES FOR THE TREATMENT OF OPIOID ADDICTION IN THE MEDICAL OFFICE 1
Substance Abuse During Pregnancy: Moms on Meds. Jennifer Anderson Maddron, M.D LeConte Womens Healthcare Associates
 Substance Abuse During Pregnancy: Moms on Meds Jennifer Anderson Maddron, M.D LeConte Womens Healthcare Associates 2010 National Survey on Drug Use and Health An estimated 4.4% of pregnant women reported
Substance Abuse During Pregnancy: Moms on Meds Jennifer Anderson Maddron, M.D LeConte Womens Healthcare Associates 2010 National Survey on Drug Use and Health An estimated 4.4% of pregnant women reported
Treatment Approaches for Drug Addiction
 Treatment Approaches for Drug Addiction [NOTE: This is a fact sheet covering research findings on effective treatment approaches for drug abuse and addiction. If you are seeking treatment, please call
Treatment Approaches for Drug Addiction [NOTE: This is a fact sheet covering research findings on effective treatment approaches for drug abuse and addiction. If you are seeking treatment, please call
ADVISORY OPINION THE USE OF CONTROLLED SUBSTANCES FOR THE TREATMENT OF CHRONIC PAIN
 Janice K. Brewer Governor Arizona State Board of Nursing 4747 North 7 th Street, Suite 200 Phoenix, AZ 85014-3655 Phone (602) 889-5150 Fax - (602) 889-5155 E-Mail: arizona@azbn.gov Home Page: http://www.azbn.gov
Janice K. Brewer Governor Arizona State Board of Nursing 4747 North 7 th Street, Suite 200 Phoenix, AZ 85014-3655 Phone (602) 889-5150 Fax - (602) 889-5155 E-Mail: arizona@azbn.gov Home Page: http://www.azbn.gov
The ABCs of Medication Assisted Treatment
 The ABCs of Medication Assisted Treatment J E F F R E Y Q U A M M E, E X E C U T I V E D I R E C T O R C O N N E C T I C U T C E R T I F I C A T I O N B O A R D The ABCs of Medication Assisted Treatment
The ABCs of Medication Assisted Treatment J E F F R E Y Q U A M M E, E X E C U T I V E D I R E C T O R C O N N E C T I C U T C E R T I F I C A T I O N B O A R D The ABCs of Medication Assisted Treatment
Treatment Approaches for Drug Addiction
 Treatment Approaches for Drug Addiction NOTE: This is a fact sheet covering research findings on effective treatment approaches for drug abuse and addiction. If you are seeking treatment, please call 1-800-662-HELP(4357)
Treatment Approaches for Drug Addiction NOTE: This is a fact sheet covering research findings on effective treatment approaches for drug abuse and addiction. If you are seeking treatment, please call 1-800-662-HELP(4357)
Web-Based Resources. Locating Treatment
 Web-Based Resources Locating Treatment http://dpt2.samhsa.gov/treatment/ -- This is the Substance Abuse and Mental Health Services Administration s (SAMHSA) page for locating both public and private opiate
Web-Based Resources Locating Treatment http://dpt2.samhsa.gov/treatment/ -- This is the Substance Abuse and Mental Health Services Administration s (SAMHSA) page for locating both public and private opiate
Southlake Psychiatry. Suboxone Contract
 Suboxone Contract Thank you for considering Southlake Psychiatry for your Suboxone treatment. Opiate Addiction is a serious condition for which you may find relief with Suboxone treatment. In order to
Suboxone Contract Thank you for considering Southlake Psychiatry for your Suboxone treatment. Opiate Addiction is a serious condition for which you may find relief with Suboxone treatment. In order to
Opioid Prescribing for Chronic Pain: Guidelines for Marin County Clinicians
 Opioid Prescribing for Chronic Pain: Guidelines for Marin County Clinicians Although prescription pain medications are intended to improve the lives of people with pain, their increased use and misuse
Opioid Prescribing for Chronic Pain: Guidelines for Marin County Clinicians Although prescription pain medications are intended to improve the lives of people with pain, their increased use and misuse
Neurobiology and Treatment of Opioid Dependence. Nebraska MAT Training September 29, 2011
 Neurobiology and Treatment of Opioid Dependence Nebraska MAT Training September 29, 2011 Top 5 primary illegal drugs for persons age 18 29 entering treatment, % 30 25 20 15 10 Heroin or Prescription Opioids
Neurobiology and Treatment of Opioid Dependence Nebraska MAT Training September 29, 2011 Top 5 primary illegal drugs for persons age 18 29 entering treatment, % 30 25 20 15 10 Heroin or Prescription Opioids
Increasing Access to Opioid Addiction Treatment
 Report to The Vermont Legislature Increasing Access to Opioid Addiction Treatment In Accordance with Act 75, 2013, Section 14b An Act Relating to Strengthening Vermont s Response to Opioid Addiction and
Report to The Vermont Legislature Increasing Access to Opioid Addiction Treatment In Accordance with Act 75, 2013, Section 14b An Act Relating to Strengthening Vermont s Response to Opioid Addiction and
STATISTICS. Opiate Substitution Therapy for Opiate Dependence. Alan Shein, M.D.
 Opiate Substitution Therapy for Opiate Dependence Alan Shein, M.D. OH #1-1 STATISTICS Prevalence of Specific Drug Abuse and Vulnerability to Develop Addictions National Household Survey and Related Surveys
Opiate Substitution Therapy for Opiate Dependence Alan Shein, M.D. OH #1-1 STATISTICS Prevalence of Specific Drug Abuse and Vulnerability to Develop Addictions National Household Survey and Related Surveys
Performance Standards
 Performance Standards Co-Occurring Disorder Competency Performance Standards are intended to provide a foundation and serve as a tool to promote continuous quality improvement and progression toward best
Performance Standards Co-Occurring Disorder Competency Performance Standards are intended to provide a foundation and serve as a tool to promote continuous quality improvement and progression toward best
The Federation of State Medical Boards 2013 Model Guidelines for Opioid Addiction Treatment in the Medical Office
 The Federation of State Medical Boards 2013 Model Guidelines for Opioid Addiction Treatment in the Medical Office Adopted April 2013 for Consideration by State Medical Boards 2002 FSMB Model Guidelines
The Federation of State Medical Boards 2013 Model Guidelines for Opioid Addiction Treatment in the Medical Office Adopted April 2013 for Consideration by State Medical Boards 2002 FSMB Model Guidelines
Appendices to Interim Report on the Baltimore Buprenorphine Initiative. Managed Care Organization Information Pages
 Appendices to Interim Report on the Baltimore Buprenorphine Initiative Appendix A Managed Care Organization Information Pages Appendix B Buprenorphine Online Physician Training Information Packet Appendix
Appendices to Interim Report on the Baltimore Buprenorphine Initiative Appendix A Managed Care Organization Information Pages Appendix B Buprenorphine Online Physician Training Information Packet Appendix
10/19/15. Stephen Loyd, M.D., F.A.C.P Healthy Kingsport Meadowview Convention Center Kingsport, Tennessee October 17, 2015
 Stephen Loyd, M.D., F.A.C.P Healthy Kingsport Meadowview Convention Center Kingsport, Tennessee October 17, 2015 Receives no commercial support, in any form, from pharmaceutical companies or anyone else
Stephen Loyd, M.D., F.A.C.P Healthy Kingsport Meadowview Convention Center Kingsport, Tennessee October 17, 2015 Receives no commercial support, in any form, from pharmaceutical companies or anyone else
Frequently Asked Questions (FAQ s): Medication-Assisted Treatment for Opiate Addiction
: Medication-Assisted Treatment for Opiate Addiction") Frequently Asked Questions (FAQ s): Medication-Assisted Treatment for Opiate Addiction March 3, 2008 By: David Rinaldo, Ph.D., Managing Partner, The Avisa Group In this FAQ What medications are currently
Frequently Asked Questions (FAQ s): Medication-Assisted Treatment for Opiate Addiction March 3, 2008 By: David Rinaldo, Ph.D., Managing Partner, The Avisa Group In this FAQ What medications are currently
Treatment of opioid use disorders
 Treatment of opioid use disorders Gerardo Gonzalez, MD Associate Professor of Psychiatry Director, Division of Addiction Psychiatry Disclosures I have no financial conflicts to disclose I will review evidence
Treatment of opioid use disorders Gerardo Gonzalez, MD Associate Professor of Psychiatry Director, Division of Addiction Psychiatry Disclosures I have no financial conflicts to disclose I will review evidence
Suboxone Programs: Treating Opioid Dependence in CHCs Andrew Putney, MD Medical Director SSTAR ATS and CHC, Fall River, Massachusetts
 Suboxone Programs: Treating Opioid Dependence in CHCs Andrew Putney, MD Medical Director SSTAR ATS and CHC, Fall River, Massachusetts Educational Objectives: Review epidemiology of opioid addiction in
Suboxone Programs: Treating Opioid Dependence in CHCs Andrew Putney, MD Medical Director SSTAR ATS and CHC, Fall River, Massachusetts Educational Objectives: Review epidemiology of opioid addiction in
BUPRENORPHINE TREATMENT
 BUPRENORPHINE TREATMENT Curriculum Infusion Package (CIP) Based on the Work of Dr. Thomas Freese of the Pacific Southwest ATTC Drug Addiction Treatment Act of 2000 (DATA 2000) Developed by Mountain West
BUPRENORPHINE TREATMENT Curriculum Infusion Package (CIP) Based on the Work of Dr. Thomas Freese of the Pacific Southwest ATTC Drug Addiction Treatment Act of 2000 (DATA 2000) Developed by Mountain West
8/1/2014. Who We Are. BHG s Medical Mission. BHG Company Overview
 Who We Are BHG s Medical Mission BHG Company Overview Behavioral Health Group (BHG) is a leading provider of opioid addiction treatment services. Our treatment centers provide pharmacotherapeutic maintenance
Who We Are BHG s Medical Mission BHG Company Overview Behavioral Health Group (BHG) is a leading provider of opioid addiction treatment services. Our treatment centers provide pharmacotherapeutic maintenance
Model Policy on DATA 2000 and Treatment of Opioid Addiction in the Medical Office
 Model Policy on DATA 2000 and Treatment of Opioid Addiction in the Medical Office April 2013 The recommendations contained herein were adopted as policy by the House of Delegates of the Federation of State
Model Policy on DATA 2000 and Treatment of Opioid Addiction in the Medical Office April 2013 The recommendations contained herein were adopted as policy by the House of Delegates of the Federation of State
Policy on DATA 2000 and Treatment of Opioid Addiction in the Medical Office
 Vermont Board of Medical Practice Policy on DATA 2000 and Treatment of Opioid Addiction in the Medical Office Background and Introduction The Vermont Board of Medical Practice (the Board) is committed
Vermont Board of Medical Practice Policy on DATA 2000 and Treatment of Opioid Addiction in the Medical Office Background and Introduction The Vermont Board of Medical Practice (the Board) is committed
MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION
 MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION Mark Fisher Program Administrator State Opioid Treatment Adminstrator Kentucky Division of Behavioral Health OBJECTIVES Learn about types of opioids and
MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION Mark Fisher Program Administrator State Opioid Treatment Adminstrator Kentucky Division of Behavioral Health OBJECTIVES Learn about types of opioids and
Beyond SBIRT: Integrating Addiction Medicine into Primary Care
 Beyond SBIRT: Integrating Addiction Medicine into Primary Care Community Clinic Association of Los Angeles County 14 th Annual Health Care Symposium March 6, 2015 Keith Heinzerling MD, Karen Lamp MD; Allison
Beyond SBIRT: Integrating Addiction Medicine into Primary Care Community Clinic Association of Los Angeles County 14 th Annual Health Care Symposium March 6, 2015 Keith Heinzerling MD, Karen Lamp MD; Allison
Table of Contents. I. Introduction... 2. II. Summary... 3. A. Total Drug Intoxication Deaths... 5. B. Opioid-Related Deaths... 9
 Table of Contents I. Introduction... 2 II. Summary... 3 III. Charts A. Total Drug Intoxication Deaths... 5 B. Opioid-Related Deaths... 9 C. Heroin-Related Deaths... 11 D. Prescription Opioid-Related Deaths...
Table of Contents I. Introduction... 2 II. Summary... 3 III. Charts A. Total Drug Intoxication Deaths... 5 B. Opioid-Related Deaths... 9 C. Heroin-Related Deaths... 11 D. Prescription Opioid-Related Deaths...
Prescriber Behavior, Pain Treatment and Addiction Treatment
 Prescriber Behavior, Pain Treatment and Addiction Treatment Mary Fleming, M.S. Director, Office of Policy, Planning, and Innovation Substance Abuse and Mental Health Services Administration NGA Policy
Prescriber Behavior, Pain Treatment and Addiction Treatment Mary Fleming, M.S. Director, Office of Policy, Planning, and Innovation Substance Abuse and Mental Health Services Administration NGA Policy
Using Buprenorphine in an Opioid Treatment Program
 Using Buprenorphine in an Opioid Treatment Program Thomas E. Freese, PhD Director of Training, UCLA Integrated Substance Abuse Programs Director, Pacific Southwest Addiction Technology Transfer Center
Using Buprenorphine in an Opioid Treatment Program Thomas E. Freese, PhD Director of Training, UCLA Integrated Substance Abuse Programs Director, Pacific Southwest Addiction Technology Transfer Center
An integrated approach to addressing opiate abuse in Maine. Debra L. Brucker, MPA, PhD State of Maine Office of Substance Abuse October 2009
 An integrated approach to addressing opiate abuse in Maine Debra L. Brucker, MPA, PhD State of Maine Office of Substance Abuse October 2009 Background Defining the problem: Opiates pain relievers (OxyContin,
An integrated approach to addressing opiate abuse in Maine Debra L. Brucker, MPA, PhD State of Maine Office of Substance Abuse October 2009 Background Defining the problem: Opiates pain relievers (OxyContin,
Federal Regulations For Prescribing Scheduled Controlled Substances
 Federal Regulations For Prescribing Scheduled Controlled Substances HEIT TEMPLATE.PPT 1 Central Principle of Balance With the Use of Controlled Substances Dual imperative of government Establish a system
Federal Regulations For Prescribing Scheduled Controlled Substances HEIT TEMPLATE.PPT 1 Central Principle of Balance With the Use of Controlled Substances Dual imperative of government Establish a system
IN THE GENERAL ASSEMBLY STATE OF. Ensuring Access to Medication Assisted Treatment Act
 IN THE GENERAL ASSEMBLY STATE OF Ensuring Access to Medication Assisted Treatment Act 1 Be it enacted by the People of the State of Assembly:, represented in the General 1 1 1 1 Section 1. Title. This
IN THE GENERAL ASSEMBLY STATE OF Ensuring Access to Medication Assisted Treatment Act 1 Be it enacted by the People of the State of Assembly:, represented in the General 1 1 1 1 Section 1. Title. This
TREATMENT MODALITIES. May, 2013
 TREATMENT MODALITIES May, 2013 Treatment Modalities New York State Office of Alcoholism and Substance Abuse Services (NYS OASAS) regulates the addiction treatment modalities offered in New York State.
TREATMENT MODALITIES May, 2013 Treatment Modalities New York State Office of Alcoholism and Substance Abuse Services (NYS OASAS) regulates the addiction treatment modalities offered in New York State.
Outcomes for Opiate Users at FRN Facilities. FRN Research Report September 2014
 Outcomes for Opiate Users at FRN Facilities FRN Research Report September 2014 Introduction The illicit use of opioids has reached epidemic proportions in the United States (Alford, 2007; Meges et al,
Outcomes for Opiate Users at FRN Facilities FRN Research Report September 2014 Introduction The illicit use of opioids has reached epidemic proportions in the United States (Alford, 2007; Meges et al,
Dependence and Addiction. Marek C. Chawarski, Ph.D. Yale University David Metzger, Ph.D. University of Pennsylvania
 Dependence and Addiction Marek C. Chawarski, Ph.D. Yale University David Metzger, Ph.D. University of Pennsylvania Overview Heroin and other opiates The disease of heroin addiction or dependence Effective
Dependence and Addiction Marek C. Chawarski, Ph.D. Yale University David Metzger, Ph.D. University of Pennsylvania Overview Heroin and other opiates The disease of heroin addiction or dependence Effective
Medication is not a part of treatment.
 Medication is not a part of treatment. Medication can be an effective part of treatment. Medication is used in the treatment of many diseases, including addiction. Medical decisions must be made by trained
Medication is not a part of treatment. Medication can be an effective part of treatment. Medication is used in the treatment of many diseases, including addiction. Medical decisions must be made by trained
TREATMENT POLICY #05. Criteria for Using Methadone for Medication-Assisted Treatment and Recovery
 Michigan Department of Community Health, Behavioral Health and Developmental Disabilities Administration BUREAU OF SUBSTANCE ABUSE AND ADDICTION SERVICES TREATMENT POLICY #05 SUBJECT: Criteria for Using
Michigan Department of Community Health, Behavioral Health and Developmental Disabilities Administration BUREAU OF SUBSTANCE ABUSE AND ADDICTION SERVICES TREATMENT POLICY #05 SUBJECT: Criteria for Using
Addiction Psychiatry Fellowship Rotation Goals & Objectives
 Addiction Psychiatry Fellowship Rotation Goals & Objectives Table of Contents University Neuropsychiatric Institute (UNI) Training Site 2 Inpatient addiction psychiatry rotation.....2 Outpatient addiction
Addiction Psychiatry Fellowship Rotation Goals & Objectives Table of Contents University Neuropsychiatric Institute (UNI) Training Site 2 Inpatient addiction psychiatry rotation.....2 Outpatient addiction
Medication-Assisted Treatment for Opioid Addiction
 Medication-Assisted Treatment for Opioid Addiction This document contains a general discussion of medications approved by the U.S. Food and Drug Administration (FDA) for use in the treatment of opioid
Medication-Assisted Treatment for Opioid Addiction This document contains a general discussion of medications approved by the U.S. Food and Drug Administration (FDA) for use in the treatment of opioid
Behavioral Health Barometer. Mississippi, 2014
 Behavioral Health Barometer Mississippi, 2014 Acknowledgments This report was prepared for the Substance Abuse and Mental Health Services Administration (SAMHSA) by RTI International under contract No.
Behavioral Health Barometer Mississippi, 2014 Acknowledgments This report was prepared for the Substance Abuse and Mental Health Services Administration (SAMHSA) by RTI International under contract No.
Update on Buprenorphine: Induction and Ongoing Care
 Update on Buprenorphine: Induction and Ongoing Care Elizabeth F. Howell, M.D., DFAPA, FASAM Department of Psychiatry, University of Utah School of Medicine North Carolina Addiction Medicine Conference
Update on Buprenorphine: Induction and Ongoing Care Elizabeth F. Howell, M.D., DFAPA, FASAM Department of Psychiatry, University of Utah School of Medicine North Carolina Addiction Medicine Conference
Opioids for Pain Treatment. Opioids for Chronic Pain and Addiction Treatment. Outline for Today. Opioids for pain treatment
 Opioids for Chronic Pain and Addiction Treatment Joseph Merrill M.D., M.P.H. University of Washington February 24, 2012 Outline for Today Opioids for pain treatment Trends Problems High dose prescribing
Opioids for Chronic Pain and Addiction Treatment Joseph Merrill M.D., M.P.H. University of Washington February 24, 2012 Outline for Today Opioids for pain treatment Trends Problems High dose prescribing
Resources for the Prevention and Treatment of Substance Use Disorders
 Resources for the Prevention and Treatment of Substance Use Disorders Table of Contents Age-standardized DALYs, alcohol and drug use disorders, per 100 000 Age-standardized death rates, alcohol and drug
Resources for the Prevention and Treatment of Substance Use Disorders Table of Contents Age-standardized DALYs, alcohol and drug use disorders, per 100 000 Age-standardized death rates, alcohol and drug
Outpatient Detoxification
 Opioid dependence is a challenging and complicated condition, but it can be treated. If you re working to overcome opioid dependence, you know the experience can sometimes be overwhelming. That s why the
Opioid dependence is a challenging and complicated condition, but it can be treated. If you re working to overcome opioid dependence, you know the experience can sometimes be overwhelming. That s why the
Opiate Addiction in Ohio: An Update on Scope of Problem Ashland Ohio
 Governor s Cabinet Opiate Action Team Promoting Wellness and Recovery John R. Kasich, Governor Tracy J. Plouck, Director Opiate Addiction in Ohio: An Update on Scope of Problem Ashland Ohio November 14,
Governor s Cabinet Opiate Action Team Promoting Wellness and Recovery John R. Kasich, Governor Tracy J. Plouck, Director Opiate Addiction in Ohio: An Update on Scope of Problem Ashland Ohio November 14,
Michigan Guidelines for the Use of Controlled Substances for the Treatment of Pain
 Michigan Guidelines for the Use of Controlled Substances for the Treatment of Pain Section I: Preamble The Michigan Boards of Medicine and Osteopathic Medicine & Surgery recognize that principles of quality
Michigan Guidelines for the Use of Controlled Substances for the Treatment of Pain Section I: Preamble The Michigan Boards of Medicine and Osteopathic Medicine & Surgery recognize that principles of quality
Visit www.takebackmylife.org to hear more of my story or call 211 for help and treatment options
 In high school, I experimented with alcohol and pot. Then I moved on to narcotics and cocaine, which landed me in jail several times. By 25, I was a daily heroin user with a long-term prison sentence.
In high school, I experimented with alcohol and pot. Then I moved on to narcotics and cocaine, which landed me in jail several times. By 25, I was a daily heroin user with a long-term prison sentence.
Medication treatments for opioid use disorders
 Medication treatments for opioid use disorders Summary for counties JUDITH MARTIN, Medical Director of Substance Use Services, San Francisco Department of Public Health Brief history of Methadone and Buprenorphine
Medication treatments for opioid use disorders Summary for counties JUDITH MARTIN, Medical Director of Substance Use Services, San Francisco Department of Public Health Brief history of Methadone and Buprenorphine
Use of Buprenorphine in the Treatment of Opioid Addiction
 Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary Which of the following is an
Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary Which of the following is an
Quick Guide. For Physicians. Based on TIP 40 Clinical Guidelines for the Use of Buprenorphine in the Treatment. of Opioid Addiction TIP
 Buprenorphine Clinical Guide Quick Guide For Physicians Based on TIP 40 Clinical Guidelines for the Use of Buprenorphine in the Treatment Clinical Guidelines for the Use of Buprenorphine in the Treatment
Buprenorphine Clinical Guide Quick Guide For Physicians Based on TIP 40 Clinical Guidelines for the Use of Buprenorphine in the Treatment Clinical Guidelines for the Use of Buprenorphine in the Treatment
American Society of Addiction Medicine
 American Society of Addiction Medicine Public Policy Statement on Treatment for Alcohol and Other Drug Addiction 1 I. General Definitions of Addiction Treatment Addiction Treatment is the use of any planned,
American Society of Addiction Medicine Public Policy Statement on Treatment for Alcohol and Other Drug Addiction 1 I. General Definitions of Addiction Treatment Addiction Treatment is the use of any planned,
Behavioral Health Barometer. Virginia, 2014
 Behavioral Health Barometer Virginia, 2014 Acknowledgments This report was prepared for the Substance Abuse and Mental Health Services Administration (SAMHSA) by RTI International under contract No. 283
Behavioral Health Barometer Virginia, 2014 Acknowledgments This report was prepared for the Substance Abuse and Mental Health Services Administration (SAMHSA) by RTI International under contract No. 283
MAD-MR: 12-13 SPECIALTY SERVICES EFF: 9-1-12 MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION INDEX
 INDEX 8.325.11 8.325.11.1 ISSUING AGENCY...1 8.325.11.2 SCOPE...1 8.325.11.3 STATUTORY AUTHORITY...1 8.325.11.4 DURATION...1 8.325.11.5 EFFECTIVE DATE...1 8.325.11.6 OBJECTIVE...1 8.325.11.7 DEFINITIONS...1
INDEX 8.325.11 8.325.11.1 ISSUING AGENCY...1 8.325.11.2 SCOPE...1 8.325.11.3 STATUTORY AUTHORITY...1 8.325.11.4 DURATION...1 8.325.11.5 EFFECTIVE DATE...1 8.325.11.6 OBJECTIVE...1 8.325.11.7 DEFINITIONS...1
John R. Kasich, Governor Orman Hall, Director
 John R. Kasich, Governor Orman Hall, Director 2 3 Epidemics of unintentional drug overdoses in Ohio, 1979-2011 1,2,3 1800 1600 1400 1200 1000 800 Prescription drugs are causing a larger overdose epidemic
John R. Kasich, Governor Orman Hall, Director 2 3 Epidemics of unintentional drug overdoses in Ohio, 1979-2011 1,2,3 1800 1600 1400 1200 1000 800 Prescription drugs are causing a larger overdose epidemic