Trauma in the Pregnant Female. Luanna Beauchamp, MD, FACOG
|
|
|
- Terence Wilcox
- 7 years ago
- Views:
Transcription
1 Trauma in the Pregnant Female Luanna Beauchamp, MD, FACOG

2
3 Introduction Save the mother, save the fetus
4 The Scenario O The situation: It s Friday night, and as the EMS provider on call, you receive a call. O You go to the scene and find a 25 year old female, restrained passenger in an MVA, with open left tib/fib fracture. O The victim tells you she is 26 weeks pregnant and asks if the baby is OK.
5
6 Second Scenario O Another Friday night call: O You arrive at a residence to find a 30 year old female complaining of abdominal pain and vaginal bleeding. O The police suspect her boyfriend physically assaulted her. O She tells you she is pregnant but does not know how far along she is.
7 Incidence O These two hypothetical cases are actually very common. O Trauma is the leading cause of death in pregnancy O Occurs in 8-10% of all pregnancies O Frequent cause of injury in pregnancy O Accounts for 20% of maternal mortality
8 Incidence O Increases as pregnancy increases O 8% first trimester O 40% in second trimester O 52% in third trimester
9 Types of Trauma O MVA >50% O Falls O Blunt Head Injury O Gunshot Wounds O Stab Wounds O Burns O Drowning
10 Motor Vehicle Accidents O Most common cause of major trauma in pregnancy
11
12

13

14
15 Minor vs Major Trauma O 2-8% of those with trauma will have life threatening injuries O Minor- usually from fall, low speed MVA, minor burns, etc. O Major- MVA, blunt, penetrating trauma,etc. O CAVEAT: Severity of maternal injury may not correlate with risk of adverse pregnancy outcome.
16 Minor vs Major Trauma O Minor- miscarriage in first trimester, placental abruption, fetomaternal hemorrhage O Major- miscarriage in first tri, significant fetal morbidity or fetal/neonatal death
17 Trauma Concepts O Maternal mortality is similar to nonpregnant females in similar situation O Prompt and effective resuscitation is best way to prevent fetal injury and mortality
18 Potential Complications O Maternal death O Fetal or Neonatal death O Maternal Injury O Fetal Injury O Hospitalization
19 Pregnancy Considerations O Gestational age of fetus- viable or not O Anatomic changes O Physiologic changes O Two patients
20 Stratification O Prior to viability: less than weeks. O Viable gestation: 23 weeks and beyond. O In active labor O Critically ill, perimortem state
21
22 Anatomy of a Female
23
24 Female Pelvis
25 Anatomic changes in Pregnancy
26 Reproductive System O Enlargement of uterus O Intra-abdominal organ at 12 weeks O At umbilicus at 20 weeks O Costal margin at 36 weeks O Descends/drops due to fetal engagement around 38 weeks
27
28 Pregnancy
29
30 Reproductive System O Uterus becomes thin-walled. More prone to injury. O Placenta- inelastic. Prone to separation (abruption).
31 Pregnant Female
32 Physiologic changes O Cardiovascular O Hemodynamic O Respiratory O Renal O Gastrointestinal O Hematologic O Musculoskeletal
33 Cardiovascular O Cardiac output -up to 50% increase O Heart rate increases by beats/minute O Pregnant pt can lose 30% ( 2L) of blood volume before vital signs change
34 Hemodynamic O Uterine compression of vena cava: O Causes decreased venous return O Can cause 30% drop in cardiac output O Called Supine Hypotension Syndrome
35 Supine Hypotension Syndrome O Avoid by displacing the uterus O Place in left lateral decubitus position O Manually tilt uterus to side O Towel roll under right hip O Tilt spine immobilization board
36

37 Manbit images
38 Milson I, Forssman L: Factors influencing aortocaval compressionin late pregnancy, Am J Obtst Gynecol 148: , 1984
39
40
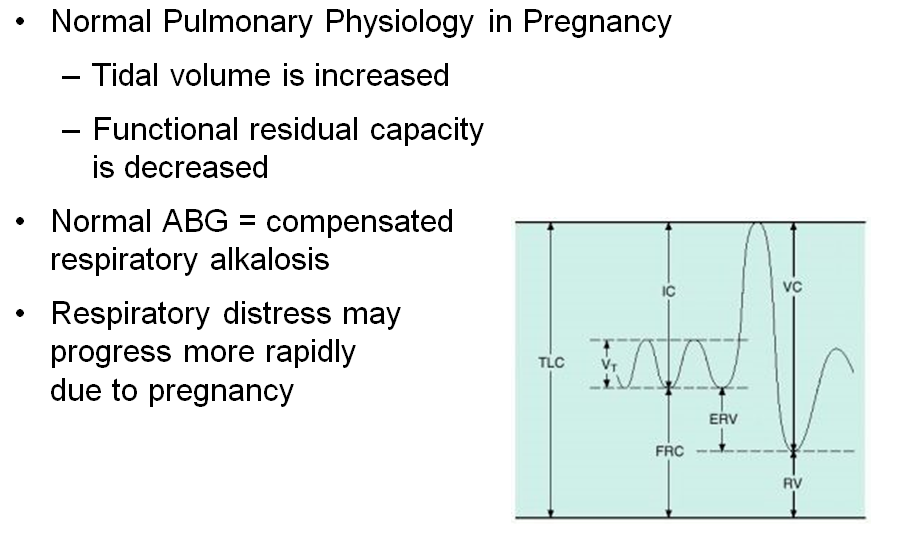
41 Respiratory O Increased O2 consumption O Elevated diaphragm O Tidal volume increased by 30-40% O Minute ventilation increased by 30-40% O Intubation challenging due to airway edema O Increased risk of aspiration
42
43 Respiratory O Maternal-fetal O2 consumption increases 40-50% over non-pregnant state. O Cardiac output increases by 50%. O Functional residual capacity (apneic reserve of O2) decreases by 20% Pregnant patient has diminished capacity to tolerate apnea!
44 Functional residual capacity (FRC) is our air tank for apnea. from Google images
45 Pregnant Mom has a smaller air tank Non-pregnant woman /blog/images/scubaweb.jpg
46 Mom 4 ml O2 / kg / min Feto-placental unit 12 ml O2 / kg / min Mother is consuming and delivering oxygen for two!
47 Respiratory Considerations O At term, respiratory alkalosis with metabolic compensation. Less HCO3- to buffer O At term, lower Hgb concentration to buffer acid load O Less tolerant to both apnea and acidosis
48 Hematologic O 40% increase in blood volume O 25% increase in red cell mass O Results in relative anemia HCT O Mother can lose up to 1500ccs of blood without signs of instability. Fetus cannot tolerate however and will be in shock.
49 Hematologic O WBC increased O Fibrinogen and clotting factors increased O Albumin low
50 Increased coagulopathy
51 Renal O Glomerular filtration rate increased O BUN & Creatinine decrease O Glycosuria common
52 Gastrointestinal O Delayed gastric emptying O Relaxed lower esophageal sphincter O Increases risk for aspiration
53 Musculoskeletal O Joint laxity O Symphysis pubis widens by 7 th month O Sacroiliac joint spaces may increase
54
55 Fetal Blood Supply
56 Fetal Circulation
57 Assessment in the Field O Differences in pregnant females are important, however: O Pregnant patient is still a trauma victim O Should assess the pregnant trauma patient following usual protocols.
58
59 Special considerations O May need to modify evaluation: O Fully evaluate mother O Treat mother O Then assess fetus O Treat fetus
60 Management Protocols OWhat is best for the mother is best for the fetus!!!!!
61 Initial Management O AIRWAY: as per all patients O BREATHING: as per all patients O CIRCULATION: If able, place on left side or left hip tilt
62 Airway Considerations O Assess airway: Can have increased edema which can obscure vocal cords O Mother and fetus both have increased oxygen demands.
63 Breathing Considerations O Decreased FRC O Increased O2 consumption O Mother and baby need O2 O Give supplemental O2 via nasal cannula if possible O Consider intubation early
64 Circulation Considerations OPREGNANT PATIENT CAN LOSE A LOT OF BLOOD BEFORE ABNORMAL BP AND PULSE!!
65 Circulation Considerations O Avoid vasopressors O Avoid supine hypotension O Left lateral decubitus
66
67 General Assessment O Initial Assessment O Routine protocol O History O Due date O Pre-existing disease O Pain O Vaginal Bleeding
68 General Assessment O Physical Exam O Routine protocol O Assess uterus and obtain fundal height O Do not perform vaginal exam O Assess fetal heart rate if possible
69 General Assessment O CAVEATS: O Two patients O ABC O Monitor for shock
70 Trauma Management O Follow usual protocols O High flow, high concentration O2 O Large bore IVs O Left lateral tilt O Reassess patient O Monitor fetus
71 Fetal Assessment O Obtain heart rate O Normal heart rate
72
73 Fetal Outcome O Fetal loss occurs in 40% of critically injured pregnant pts O Fetal loss directly related to severity of trauma injury O Overall fetal loss rate 4-5%
74 Fetal Loss Rate O Maternal shock- 80% O Abruption % O Penetrating Abdominal Injury- 70% O CAVEAT: Homicides and MVAs most common cause of fetal death
75 Risk Factors for Fetal Loss O Maternal hypotension O High maternal injury severity score O Ejection from MV O Maternal pelvic fracture O Maternal ETOH use O Motorcycle crash O Uterine rupture
76 Blunt Trauma Concerns O Placental Abruption O Leading cause of fetal death O DIC may occur O Fetal Anemia O Feto-Maternal hemorrhage O Ruptured Uterus O 0.6% of blunt trauma
77 Pattern of Injury O First trimester Blunt Trauma O Uterus in pelvis O Bladder in pelvis O Pattern of injury is similar to nonpregnant O Uterus is protected O Pattern of abd injury unchanged
78
79 Pattern of Injury Blunt Trauma O Second and Third Trimesters O Uterus extrapelvic O Bladder extrapelvic O Stomach, spleen displaced O Increased uteropelvic blood flow O Pattern of injury altered
80 Late Pregnancy Blunt Trauma O Pattern of Injury Altered: O Bladder injuries more common O Small bowel injuries less common O Greater risk of pelvic fractures O Increased uterine rupture O Increased placental abruption
81
82 Placental Abruption O Second most common cause of fetal death in trauma O Incidence ranges from 6-60% in literature O Can result from very minor traumaie fall
83 Placental Abruption O Occurs in 5% of pts with minor injuries O Occurs in 50% of pts with major injuries O Usually occurs within first 24 hrs after injury
84 Etiology of Abruption in Trauma O Uterus has many elastic fibers O Placenta has few elastic fibers O Causes inelastic connection O Susceptible to shearing force
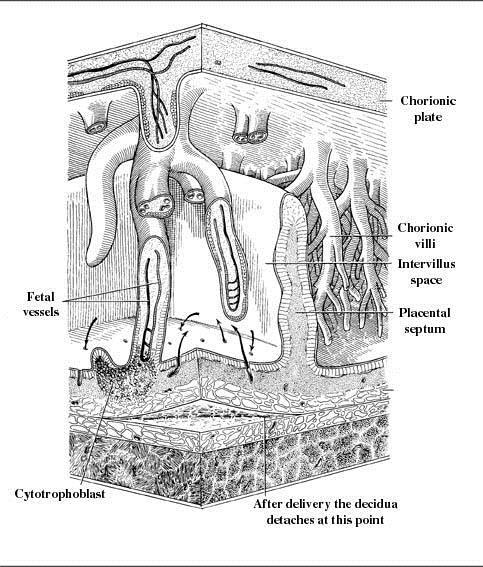
85 Placental abruption Placenta shears off Liquid placenta Elastic myometrium
86 Placental Abruption Bledsoe et al., Essentials of Paramedic Care: Division 1V
87 Placental Abruption O Abdominal pain O Vaginal Bleeding O Uterine tenderness O Contractions O Hard, stiff uterus O Fetal bradycardia
88 What happens if fetus doesn t get enough oxygen? (What is the mammalian diving response?)
89 The mammalian diving reflex shuts down blood flow to all organs except the heart and brain, in order to conserve oxygen. The fetus responds to hypoxia in this manner
90
91 Fetal Hypoxia Response O Fetal O2 uptake is proportional to placental blood flow. O Decrease in FHR due to hypoxia
92 Prevention O Use of seatbelts improves maternal/fetal outcomes in MVA O Incorrect positioning can lead to injuries O If too high- direct injury to uterus and fetus
93
94 Seatbelts O 20% never or rarely use seatbelts O 20% incorrectly use seatbelts O ACOG:..substantial evidence seat belt use in pregnancy protects both the mother and the fetus.
95 Prevention O If only lap belt- increases placental abruption and uterine rupture O Shoulder harnesses decrease likelihood of serious injury in mother, resulting improved fetal outcomes O Airbag deployment not shown to cause harm based on limited data
96 Proper Use of Seatbelts O As low as possible on pregnancy bulge and across pubic symphysis O Placement on uterus causes 3-4X increase in force transmitted to uterus
97 Proper seatbelt position O If too high- direct injury to uterus and fetus O Shoulder harness should be placed between breasts
98
99 Worst Fetal Outcome
100 Proper 3 point harness
101 Best Fetal Outcome
102
103
104 Domestic Violence O Physical abuse can occur O Possibly 10% of pregnant women O Blunt abdominal trauma is common O Need a low index of suspicion
105 Uterine Rupture O Rare in trauma pts % O Can be associated with pelvic fractures O Usually occurs in pts with previous cesarean sections
106 Uterine Rupture O Results from direct abdominal trauma O Maternal mortality 10% O Fetal mortality- almost 100% unless immediately delivered
107 Uterine Rupture O Various degrees- complete with fetus in abdomen to small window in lower uterine segment O 75% of cases involve fundus O With previous C-section, usually occurs in ant LUS
108 Intact Uterus
109 Uterine Rupture
110 Uterine Rupture O Common Findings: O Abdominal tenderness O Uterine irregular shape O Palpable fetal parts
111 OB Complications O Rupture of membranes O Preterm labor O Preterm delivery O Placenta previa O Fetal injury- ICH, etc.
112 Placenta Previa Bledsoe et al., Essentials of Paramedic Care: Division 1V
113 Cardiac Arrest O ABC s O CPR- no difference O Left displacement of uterus O Defibrillator use is OK O If code, delivery by C-section within 5 minutes
114 Perimortem Cesarean Section O No clear guidelines O Best fetal outcomes with delivery within 5 minutes of absent maternal circulation O May result in maternal survival due to increased venous return and elimination of uterine- placental blood flow
115
116 Delivery O Avoid delivery in the field if possible O Try to control the delivery so that the head does not pop out O Double clamp the cord and cut
117 Delivery O Placenta usually detaches and delivers shortly after the baby or up to 30 minutes O Do not pull on cord! Will break!! O Wrap up baby and place on mother s chest if feasible
118 Vertex Delivery
119 Vertex Delivery
120 Vertex Delivery
121 Non-vertex Delivery
122 Breech Presentation
123 Breech Presentation Footling breech
124 Breech Delivery O If at all possible, delay delivery in field O Best outcome is hospital delivery by experienced OB, not ER provider O If unable to delay, obtain maternal assistance if she is able O Place patient on raised surface with pelvis at end of stretcher if possible
125 Wait until presenting part is beyond introitus and gently guide
126 Deliver both legs
127 May need to reach into vagina and grasp leg and pull out
128 Breech Delivery
129 Support body while delivering arms
130 Breech Delivery
131 Support body until head/neck is showing
132 Breech Delivery While supporting baby, let the baby drop downward to deliver the back of the head
133 Breech Delivery Then grasp both legs and pull the body upward to deliver the rest of the head
134
135 Postpartum Hemorrhage O Don t forget that all women who have just delivered are at risk of postpartum hemorrhage
136 Conclusion O Trauma is leading cause of nonobstetric maternal mortality O Follow basic guidelines of trauma evaluation and resuscitation O Be mindful of special considerations in the pregnant trauma victim O Remember that you have TWO victims
137 Goals OSave the mother!! OSave the fetus if possible!
Caring for Mom and Child: Trauma in the Pregnant Patient
 Caring for Mom and Child: Trauma in the Pregnant Patient George Koenig DO, FACS Assistant Professor of Surgery, Division of Trauma & Critical Care Associate Medical Director JeffSTAT Thomas Jefferson University
Caring for Mom and Child: Trauma in the Pregnant Patient George Koenig DO, FACS Assistant Professor of Surgery, Division of Trauma & Critical Care Associate Medical Director JeffSTAT Thomas Jefferson University
Why is prematurity a concern?
 Prematurity What is prematurity? A baby born before 37 weeks of pregnancy is considered premature. Approximately 12% of all babies are born prematurely. Terms that refer to premature babies are preterm
Prematurity What is prematurity? A baby born before 37 weeks of pregnancy is considered premature. Approximately 12% of all babies are born prematurely. Terms that refer to premature babies are preterm
BLS TREATMENT GUIDELINES - CARDIAC
 BLS TREATMENT GUIDELINES - CARDIAC CARDIOPULMONARY ARREST - NON-TRAUMATIC (SJ-B101) effective 07/01/99 Defibrillation CPR Apply S-AED and assess rhythm as trained. Defib as indicated Simultaneous OXYGEN:
BLS TREATMENT GUIDELINES - CARDIAC CARDIOPULMONARY ARREST - NON-TRAUMATIC (SJ-B101) effective 07/01/99 Defibrillation CPR Apply S-AED and assess rhythm as trained. Defib as indicated Simultaneous OXYGEN:
United States Department of Transportation National Highway Traffic Safety Administration Paramedic: National Standard Curriculum 1
 UNIT TERMINAL OBJECTIVE 4-8 At the completion of this unit, the paramedic student will be able to integrate pathophysiologic principles and the assessment findings to formulate a field impression and implement
UNIT TERMINAL OBJECTIVE 4-8 At the completion of this unit, the paramedic student will be able to integrate pathophysiologic principles and the assessment findings to formulate a field impression and implement
What is ACLS Maternal Focus?
 Carla Rider, MBA, BSN, RNC-LRN, Administrative Director Women s Services Meredith Green, MSN Candidate, BSN, RN, Clinical Educator Women s Services What is? ACLS Component 1 American Heart Association
Carla Rider, MBA, BSN, RNC-LRN, Administrative Director Women s Services Meredith Green, MSN Candidate, BSN, RN, Clinical Educator Women s Services What is? ACLS Component 1 American Heart Association
Chapter 31 Obstetrics and Neonatal Care 1137. Scene Size-up. Primary Assessment
 Chapter 31 Obstetrics and Neonatal Care 1137 Scene Size-up Scene Safety Mechanism of Injury (MOI)/ Nature of Illness (NOI) Ensure scene safety and safe access to the patient. Standard precautions should
Chapter 31 Obstetrics and Neonatal Care 1137 Scene Size-up Scene Safety Mechanism of Injury (MOI)/ Nature of Illness (NOI) Ensure scene safety and safe access to the patient. Standard precautions should
Aehlert: Paramedic Practice Today PowerPoint Lecture Notes Chapter 50: Abdominal Trauma
 Aehlert: Paramedic Practice Today PowerPoint Lecture Notes Chapter 50: Abdominal Trauma Chapter 50 Abdominal Trauma 1 Describe the epidemiology, including morbidity, mortality rates, and prevention strategies,
Aehlert: Paramedic Practice Today PowerPoint Lecture Notes Chapter 50: Abdominal Trauma Chapter 50 Abdominal Trauma 1 Describe the epidemiology, including morbidity, mortality rates, and prevention strategies,
Southern Stone County Fire Protection District Emergency Medical Protocols
 TITLE Pediatric Medical Assessment PM 2.4 Confirm scene safety Appropriate body substance isolation procedures Number of patients Nature of illness Evaluate the need for assistance B.L.S ABC s & LOC Focused
TITLE Pediatric Medical Assessment PM 2.4 Confirm scene safety Appropriate body substance isolation procedures Number of patients Nature of illness Evaluate the need for assistance B.L.S ABC s & LOC Focused
Obstetrical Emergencies
 Date: July 18, 2014 Page 1 of 5 Obstetrical Emergencies Purpose: To provide the process for the assessment and management of the patient with an obstetrical related emergency. Pre-Medical Control 1. Follow
Date: July 18, 2014 Page 1 of 5 Obstetrical Emergencies Purpose: To provide the process for the assessment and management of the patient with an obstetrical related emergency. Pre-Medical Control 1. Follow
Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: OB/GYN Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: OB/GYN Revised: 11/2013 A&P Vagina - known as birth canal. Cervix - head of vagina. Fallopian tubes
Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: OB/GYN Revised: 11/2013 A&P Vagina - known as birth canal. Cervix - head of vagina. Fallopian tubes
Overview. Geriatric Overview. Chapter 26. Geriatrics 9/11/2012
 Chapter 26 Geriatrics Slide 1 Overview Trauma Common Medical Emergencies Special Considerations in the Elderly Medication Considerations Abuse and Neglect Expanding the Role of EMS Slide 2 Geriatric Overview
Chapter 26 Geriatrics Slide 1 Overview Trauma Common Medical Emergencies Special Considerations in the Elderly Medication Considerations Abuse and Neglect Expanding the Role of EMS Slide 2 Geriatric Overview
FEMALE ANATOMY. the Functions of the Female Organs
 FEMALE ANATOMY the Functions of the Female Organs An educational video for every woman who is told she needs pelvic surgery, including exploratory surgery or removal of the uterus, fallopian tubes, or
FEMALE ANATOMY the Functions of the Female Organs An educational video for every woman who is told she needs pelvic surgery, including exploratory surgery or removal of the uterus, fallopian tubes, or
First Responder (FR) and Emergency Medical Responder (EMR) Progress Log
 and Emergency Medical Responder (EMR) Progress Log") First Responder (FR) and Emergency Medical Responder (EMR) Progress Log Note: Those competencies that are for EMR only are denoted by boldface type. For further details on the National Occupational Competencies
First Responder (FR) and Emergency Medical Responder (EMR) Progress Log Note: Those competencies that are for EMR only are denoted by boldface type. For further details on the National Occupational Competencies
404 Section 5 Shock and Resuscitation. Scene Size-up. Primary Assessment. History Taking
 404 Section 5 and Resuscitation Scene Size-up Scene Safety Mechanism of Injury (MOI)/ Nature of Illness (NOI) Ensure scene safety and address hazards. Standard precautions should include a minimum of gloves
404 Section 5 and Resuscitation Scene Size-up Scene Safety Mechanism of Injury (MOI)/ Nature of Illness (NOI) Ensure scene safety and address hazards. Standard precautions should include a minimum of gloves
Oxygen Therapy. Oxygen therapy quick guide V3 July 2012.
 PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
Oxygen - update April 2009 OXG
 PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
1st Responder to Emergency Medical Responder Transition Course
 1st Responder to Emergency Medical Responder Transition Course Mandatory Training July 5, 2011 Authored by: Eddie Manley, Education Coordinator OSDH - EMS 1 st Responder to EMR Recommended Transition Course
1st Responder to Emergency Medical Responder Transition Course Mandatory Training July 5, 2011 Authored by: Eddie Manley, Education Coordinator OSDH - EMS 1 st Responder to EMR Recommended Transition Course
To outline nursing management of patients receiving epidural anesthesia during labor (Includes walking epidurals and combined spinal-epidurals).
.") HOSPITAL NAME INSTITUTIONAL POLICY AND PROCEDURE (IPP) Department: Manual: Section: TITLE/DESCRIPTION POLICY NUMBER LABOR: EPIDURAL EFFECTIVE DATE REVIEW DUE REPLACES NUMBER NO. OF PAGES APPROVED BY APPLIES
HOSPITAL NAME INSTITUTIONAL POLICY AND PROCEDURE (IPP) Department: Manual: Section: TITLE/DESCRIPTION POLICY NUMBER LABOR: EPIDURAL EFFECTIVE DATE REVIEW DUE REPLACES NUMBER NO. OF PAGES APPROVED BY APPLIES
Anatomical and Physiological Changes in Pregnancy Relevant to Anaesthesia
 Anatomical and Physiological Changes in Pregnancy Relevant to Anaesthesia Dr. A. Calzolari Specialist Registrar in Anaesthesia Dr. D. J. Dalgleish Consultant Anaesthetist Royal Bournemouth Hospital Dorset,
Anatomical and Physiological Changes in Pregnancy Relevant to Anaesthesia Dr. A. Calzolari Specialist Registrar in Anaesthesia Dr. D. J. Dalgleish Consultant Anaesthetist Royal Bournemouth Hospital Dorset,
Neonatal Emergencies. Care of the Neonate. Care of the Neonate. Care of the Neonate. Student Objectives. Student Objectives continued.
 Student Objectives Neonatal Emergencies After completing this section the student will be able to: 1. Identify three physiologic and/or anatomic features unique to the newborn 2. List three perinatal factors
Student Objectives Neonatal Emergencies After completing this section the student will be able to: 1. Identify three physiologic and/or anatomic features unique to the newborn 2. List three perinatal factors
Rural Health Advisory Committee s Rural Obstetric Services Work Group
 Rural Health Advisory Committee s Rural Obstetric Services Work Group March 15 th webinar topic: Rural Obstetric Patient and Community Issues Audio: 888-742-5095, conference code 6054760826 Rural Obstetric
Rural Health Advisory Committee s Rural Obstetric Services Work Group March 15 th webinar topic: Rural Obstetric Patient and Community Issues Audio: 888-742-5095, conference code 6054760826 Rural Obstetric
Emergency Medical Technician - Basic
 Washington State Specific Objectives for Emergency Medical Technician - Basic OFFICE OF EMERGENCY MEDICAL AND TRAUMA PREVENTION September 1996 Emergency Medical Technician - Basic Definition: Emergency
Washington State Specific Objectives for Emergency Medical Technician - Basic OFFICE OF EMERGENCY MEDICAL AND TRAUMA PREVENTION September 1996 Emergency Medical Technician - Basic Definition: Emergency
Nursing. Management of Spinal Trauma. Content. Objectives. Objectives
 7 cervical vertebrae Content 12 thoracic vertebrae Nursing 5 sacral vertebrae Management of Spinal Trauma Kwai Fung Betty Siu Ward Manager O&T Dept TKOH Date : 22nd April 2007 5 lumbar vertebrae 4 coccygeal
7 cervical vertebrae Content 12 thoracic vertebrae Nursing 5 sacral vertebrae Management of Spinal Trauma Kwai Fung Betty Siu Ward Manager O&T Dept TKOH Date : 22nd April 2007 5 lumbar vertebrae 4 coccygeal
Northwestern Health Sciences University. Basic Life Support for Healthcare Providers
 Northwestern Health Sciences University Basic Life Support for Healthcare Providers Pretest May 2005 This examination to be used only as a PRECOURSE TEST for BLS for Healthcare Providers Courses Based
Northwestern Health Sciences University Basic Life Support for Healthcare Providers Pretest May 2005 This examination to be used only as a PRECOURSE TEST for BLS for Healthcare Providers Courses Based
EMERGENCY MEDICAL RESPONDER (EMR) PRACTICAL SKILLS EXAMINATION REPORT State Form 54407 (R / 5-13)
 PRACTICAL SKILLS EXAMINATION REPORT State Form 54407 (R / 5-13)") EMERGENCY MEDICAL RESPONDER (EMR) PRACTICAL SKILLS EXAMINATION REPT State Form 54407 (R / 5-3) INDIANA DEPARTMENT OF HOMELAND SECURITY EMERGENCY MEDICAL SERVICES CERTIFICATION 302 West Washington Street,
EMERGENCY MEDICAL RESPONDER (EMR) PRACTICAL SKILLS EXAMINATION REPT State Form 54407 (R / 5-3) INDIANA DEPARTMENT OF HOMELAND SECURITY EMERGENCY MEDICAL SERVICES CERTIFICATION 302 West Washington Street,
General and Objectives Clinical Skills for. Nursing Students in Maternity and Gynecology. Nursing Department
 General and Objectives Clinical Skills for Nursing Students in Maternity and Gynecology Nursing Department Objectives and clinical skills of Antenatal unit Provide antenatal care to woman during normal
General and Objectives Clinical Skills for Nursing Students in Maternity and Gynecology Nursing Department Objectives and clinical skills of Antenatal unit Provide antenatal care to woman during normal
(a) Glasgow coma scale less than or equal to thirteen; (b) Loss of consciousness greater than five minutes;
 Glasgow coma scale less than or equal to thirteen; (b) Loss of consciousness greater than five minutes;") ACTION: Original DATE: 09/11/2014 3:19 PM 4765-14-02 Determination of a trauma victim. Emergency medical service personnel shall use the criteria in this rule, consistent with their certification, to evaluate
ACTION: Original DATE: 09/11/2014 3:19 PM 4765-14-02 Determination of a trauma victim. Emergency medical service personnel shall use the criteria in this rule, consistent with their certification, to evaluate
Uterine fibroids (Leiomyoma)
") Uterine fibroids (Leiomyoma) What are uterine fibroids? Uterine fibroids are fairly common benign (not cancer) growths in the uterus. They occur in about 25 50% of all women. Many women who have fibroids
Uterine fibroids (Leiomyoma) What are uterine fibroids? Uterine fibroids are fairly common benign (not cancer) growths in the uterus. They occur in about 25 50% of all women. Many women who have fibroids
Red Flags that should not be ignored
 Pregnancy that should not be ignored If a pregnant woman tells you she is experiencing any of the following symptoms during pregnancy, assist her to contact her emergency care professional right away.
Pregnancy that should not be ignored If a pregnant woman tells you she is experiencing any of the following symptoms during pregnancy, assist her to contact her emergency care professional right away.
BLUNT TORSO INJURY FROM IMPACT OR DECELERATION HAS ABDOMINAL SOLID ORGAN TRAUMA UNTIL PROVEN OTHERWISE
 Abdominal and Pelvic Trauma In the primary survey, the circulation part includes thinking about the abdomen as a source of occult hemorrhage The OBVIOUS THING is a penetrating abdominal injury Generally
Abdominal and Pelvic Trauma In the primary survey, the circulation part includes thinking about the abdomen as a source of occult hemorrhage The OBVIOUS THING is a penetrating abdominal injury Generally
Spinal Cord Injury Education. An Overview for Patients, Families, and Caregivers
 Spinal Cord Injury Education An Overview for Patients, Families, and Caregivers Spinal Cord Anatomy A major component of the Central Nervous System (CNS) It is 15 to 16 inches long, and weighs 1 to 2 ounces
Spinal Cord Injury Education An Overview for Patients, Families, and Caregivers Spinal Cord Anatomy A major component of the Central Nervous System (CNS) It is 15 to 16 inches long, and weighs 1 to 2 ounces
Examination of the Pregnant Abdomen
 Medical students often find the examination of the pregnant abdomen daunting. This document provides a framework for you to develop a comprehensive understanding of the pregnant abdomen examination at
Medical students often find the examination of the pregnant abdomen daunting. This document provides a framework for you to develop a comprehensive understanding of the pregnant abdomen examination at
ROTATIONAL POSITIONING
 ROTATIONAL POSITIONING A method for rotating posterior babies during labour Problems associated with persistent posterior positioning Prolonged labour 12% for posterior vs. 1.7% Assisted delivery 24.6%
ROTATIONAL POSITIONING A method for rotating posterior babies during labour Problems associated with persistent posterior positioning Prolonged labour 12% for posterior vs. 1.7% Assisted delivery 24.6%
Birth after Caesarean Choices for delivery
 Birth after Caesarean Choices for delivery page 2 What are my choices for birth after a Caesarean? Currently, approximately 1 in 4 women (25%) in England give birth by Caesarean delivery. Some women have
Birth after Caesarean Choices for delivery page 2 What are my choices for birth after a Caesarean? Currently, approximately 1 in 4 women (25%) in England give birth by Caesarean delivery. Some women have
Pediatric Airway Management
 Pediatric Airway Management Dec 2003 Dr. Shapiro I., PICU Adult Chain of Survival EMS CPR ALS Early Defibrillation Pediatric Chain of Survival Prevention CPR EMS ALS Out-of-Hospital Cardiac Arrest SIDS
Pediatric Airway Management Dec 2003 Dr. Shapiro I., PICU Adult Chain of Survival EMS CPR ALS Early Defibrillation Pediatric Chain of Survival Prevention CPR EMS ALS Out-of-Hospital Cardiac Arrest SIDS
National Registry of Emergency Medical Technicians Emergency Medical Technician Psychomotor Examination BLEEDING CONTROL/SHOCK MANAGEMENT
 BLEEDING CONTROL/SHOCK MANAGEMENT Candidate: Examiner: Date: Signature: Possible Applies direct pressure to the wound 1 NOTE: The examiner must now inform the candidate that the wound continues to bleed.
BLEEDING CONTROL/SHOCK MANAGEMENT Candidate: Examiner: Date: Signature: Possible Applies direct pressure to the wound 1 NOTE: The examiner must now inform the candidate that the wound continues to bleed.
PARAMEDIC TRAINING CLINICAL OBJECTIVES
 Page 1 of 21 GENERAL PATIENT UNIT When assigned to the General Patient unit paramedic student should gain knowledge and experience in the following: 1. Appropriate communication with patients and members
Page 1 of 21 GENERAL PATIENT UNIT When assigned to the General Patient unit paramedic student should gain knowledge and experience in the following: 1. Appropriate communication with patients and members
American Heart Association. Basic Life Support for Healthcare Providers
 American Heart Association Basic Life Support for Healthcare Providers Pretest February 2001 This examination to be used only as a PRECOURSE TEST for BLS for Healthcare Providers Courses 2001 American
American Heart Association Basic Life Support for Healthcare Providers Pretest February 2001 This examination to be used only as a PRECOURSE TEST for BLS for Healthcare Providers Courses 2001 American
Certified Athletic trainers should follow a 10-step process of evaluation for orthopedic injuries, which includes but is not limited to:
 Acute Care Policy Acute Care Policy and Procedures Athletic training students within Winona State University s Athletic Training Education Program have the opportunity to evaluate acute athletic injuries
Acute Care Policy Acute Care Policy and Procedures Athletic training students within Winona State University s Athletic Training Education Program have the opportunity to evaluate acute athletic injuries
What Every Pregnant Woman Needs to Know About Cesarean Section. Be informed. Know your rights. Protect yourself. Protect your baby.
 Be informed. Know your rights. Protect yourself. Protect your baby. What Every Pregnant Woman Needs to Know About Cesarean Section 2012 Childbirth Connection If you re expecting a baby, there s a good
Be informed. Know your rights. Protect yourself. Protect your baby. What Every Pregnant Woman Needs to Know About Cesarean Section 2012 Childbirth Connection If you re expecting a baby, there s a good
Delayed Cord Clamping
 ICEA Position Paper Delayed Cord Clamping Position The International Childbirth Education Association recognizes that the first minutes after birth are crucial to both mother and newborn. Optimal care
ICEA Position Paper Delayed Cord Clamping Position The International Childbirth Education Association recognizes that the first minutes after birth are crucial to both mother and newborn. Optimal care
Developing Human Fetus
 Period Date LAB. DEVELOPMENT OF A HUMAN FETUS After a human egg is fertilized with human sperm, the most amazing changes happen that allow a baby to develop. This amazing process, called development, normally
Period Date LAB. DEVELOPMENT OF A HUMAN FETUS After a human egg is fertilized with human sperm, the most amazing changes happen that allow a baby to develop. This amazing process, called development, normally
Anatomy and Physiology: Understanding the Importance of CPR
 Anatomy and Physiology: Understanding the Importance of CPR Overview This document gives you more information about the body s structure (anatomy) and function (physiology). This information will help
Anatomy and Physiology: Understanding the Importance of CPR Overview This document gives you more information about the body s structure (anatomy) and function (physiology). This information will help
STATE OF MAINE DEPARTMENT OF PUBLIC SAFETY MAINE EMERGENCY MEDICAL SERVICES 152 STATE HOUSE STATION AUGUSTA, MAINE 04333
 STATE OF MAINE DEPARTMENT OF PUBLIC SAFETY MAINE EMERGENCY MEDICAL SERVICES 152 STATE HOUSE STATION AUGUSTA, MAINE 04333 PAUL R. LEPAGE GOVERNOR JOHN E. MORRIS COMMISSIONER SHAUN A. ST. GERMAIN DIRECTOR
STATE OF MAINE DEPARTMENT OF PUBLIC SAFETY MAINE EMERGENCY MEDICAL SERVICES 152 STATE HOUSE STATION AUGUSTA, MAINE 04333 PAUL R. LEPAGE GOVERNOR JOHN E. MORRIS COMMISSIONER SHAUN A. ST. GERMAIN DIRECTOR
Fetal Acid Base Status and Umbilical Cord Sampling. David Acker, MD
 Fetal Acid Base Status and Umbilical Cord Sampling David Acker, MD Part I: Some Background Intra-uterine Event as Causative of CP Cord ph < 7.00 and base excess of > 12 Early onset neonatal encephalopathy
Fetal Acid Base Status and Umbilical Cord Sampling David Acker, MD Part I: Some Background Intra-uterine Event as Causative of CP Cord ph < 7.00 and base excess of > 12 Early onset neonatal encephalopathy
Contents. 1. What types of car restraints are available? 3. 2. Buying a car child seat- checklist 5. 3. Tips for fitting car seats 6
 Child Car Safety Contents 1. What types of car restraints are available? 3 2. Buying a car child seat- checklist 5 3. Tips for fitting car seats 6 4. How to use car seats 6 5. Legislation for child safety
Child Car Safety Contents 1. What types of car restraints are available? 3 2. Buying a car child seat- checklist 5 3. Tips for fitting car seats 6 4. How to use car seats 6 5. Legislation for child safety
School of Diagnostic Medical Sonography Course Catalog
 School of Diagnostic Medical Sonography Course Catalog 2 School of Diagnostic Medical Sonography Course Schedule Our program provides a broad base of education and performance- based clinical experience
School of Diagnostic Medical Sonography Course Catalog 2 School of Diagnostic Medical Sonography Course Schedule Our program provides a broad base of education and performance- based clinical experience
Applications of Doppler Ultrasound in Fetal Growth Assessment. David Cole
 Applications of Doppler Ultrasound in Fetal Growth Assessment David Cole Aims The aim of this presentation is to consider the use of Doppler ultrasound to investigate and monitor those pregnancies at risk
Applications of Doppler Ultrasound in Fetal Growth Assessment David Cole Aims The aim of this presentation is to consider the use of Doppler ultrasound to investigate and monitor those pregnancies at risk
Guide to Pregnancy and Birth Injury Claims
 Being pregnant, especially for the first time can be a very daunting experience where you often have to put all of your faith in your midwife or doctor. The majority of pregnancies and births occur without
Being pregnant, especially for the first time can be a very daunting experience where you often have to put all of your faith in your midwife or doctor. The majority of pregnancies and births occur without
CHLAMYDIA SCREENING IN WOMEN
 CHLAMYDIA SCREENING IN WOMEN APPLICATIONS OBJECTIVE Purpose of Measure: ELIGIBLE POPULATION Which members are included? STANDARD OF CARE What screening should be done? NCQA ACCEPTED CODES DOCUMENTATION
CHLAMYDIA SCREENING IN WOMEN APPLICATIONS OBJECTIVE Purpose of Measure: ELIGIBLE POPULATION Which members are included? STANDARD OF CARE What screening should be done? NCQA ACCEPTED CODES DOCUMENTATION
Emergency Scenarios with Case Review. Hemorrhage. 1) The person facilitating scenarios can print out the pages below.
 The person facilitating scenarios can print out the pages below.") Emergency Scenarios with Case Review Hemorrhage This emergency scenario is about patient with hemorrhage following an abortion, and is set up for role-play and case review with your staff. 1) The person
Emergency Scenarios with Case Review Hemorrhage This emergency scenario is about patient with hemorrhage following an abortion, and is set up for role-play and case review with your staff. 1) The person
How To Choose Between A Vaginal Birth Or A Cesarean Section
 Be informed. Know your rights. Protect yourself. Protect your baby. What Every Pregnant Woman Needs to Know About Cesarean Section 2012 Childbirth Connection If you re expecting a baby, there s a good
Be informed. Know your rights. Protect yourself. Protect your baby. What Every Pregnant Woman Needs to Know About Cesarean Section 2012 Childbirth Connection If you re expecting a baby, there s a good
Homeostasis. The body must maintain a delicate balance of acids and bases.
 Homeostasis The body must maintain a delicate balance of acids and bases. Metabolic and respiratory processes must work together to keep hydrogen ion (H+) levels normal and stable. ph of Blood The ph of
Homeostasis The body must maintain a delicate balance of acids and bases. Metabolic and respiratory processes must work together to keep hydrogen ion (H+) levels normal and stable. ph of Blood The ph of
9/1/2009. Lemons 2001
 TRAUMA IN PREGNANCY Fifth leading cause of death worldwide Death rate of women from unintentional injury is 24/100,000 000 Most frequent form is motor vehicle accidents US 1.6 deaths per 10 6 miles Accidents:
TRAUMA IN PREGNANCY Fifth leading cause of death worldwide Death rate of women from unintentional injury is 24/100,000 000 Most frequent form is motor vehicle accidents US 1.6 deaths per 10 6 miles Accidents:
EMERGENCY MEDICAL RESPONDER (EMR) PRACTICAL SKILLS EXAMINATION REPORT
 PRACTICAL SKILLS EXAMINATION REPORT") Reset Form EMERGENCY MEDICAL RESPONDER (EMR) PRACTICAL SKILLS EXAMINATION REPT INDIANA DEPARTMENT OF HOMELAND SECURITY EMERGENCY MEDICAL SERVICES CERTIFICATION 302 West Washington Street, Room E239 Indianapolis,
Reset Form EMERGENCY MEDICAL RESPONDER (EMR) PRACTICAL SKILLS EXAMINATION REPT INDIANA DEPARTMENT OF HOMELAND SECURITY EMERGENCY MEDICAL SERVICES CERTIFICATION 302 West Washington Street, Room E239 Indianapolis,
CPR/AED for Professional Rescuers and Health Care Providers HANDBOOK
 CPR/AED for Professional Rescuers and Health Care Providers HANDBOOK TABLE OF CONTENTS SECTION 1: THE PROFESSIONAL RESCUER The Duty to Respond 2 Preventing the Spread of Bloodborne Pathogens 3 Taking Action
CPR/AED for Professional Rescuers and Health Care Providers HANDBOOK TABLE OF CONTENTS SECTION 1: THE PROFESSIONAL RESCUER The Duty to Respond 2 Preventing the Spread of Bloodborne Pathogens 3 Taking Action
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy
 The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
School of Diagnostic Medical Sonography
 Semester 1 Orientation - 101 This class is an introduction to sonography which includes a basic anatomy review, introduction to sonographic scanning techniques and physical principles. This curriculum
Semester 1 Orientation - 101 This class is an introduction to sonography which includes a basic anatomy review, introduction to sonographic scanning techniques and physical principles. This curriculum
Newborn outcomes after cesarean section for fetal distress in BC
 Newborn outcomes after cesarean section for fetal distress in BC Patricia Janssen, PhD, UBC School of Population and Public Health Scientist, Child and Family Research Institute Kevin Jenniskens, MSc,
Newborn outcomes after cesarean section for fetal distress in BC Patricia Janssen, PhD, UBC School of Population and Public Health Scientist, Child and Family Research Institute Kevin Jenniskens, MSc,
PERINATAL NUTRITION. Nutrition during pregnancy and lactation. Nutrition during infancy.
 PERINATAL NUTRITION Nutrition during pregnancy and lactation Nutrition during infancy. Rama Bhat, MD. Department of Pediatrics, University of Illinois Hospital Chicago, Illinois. Nutrition During Pregnancy
PERINATAL NUTRITION Nutrition during pregnancy and lactation Nutrition during infancy. Rama Bhat, MD. Department of Pediatrics, University of Illinois Hospital Chicago, Illinois. Nutrition During Pregnancy
2012 Mississippi EMT Transitional Refresher Curriculum EMT Refresher Training- Curriculum Transition: EMT-Basic EMT Timeline: February 2012-March 2015
 2012 Mississippi EMT Transitional Refresher Curriculum EMT Refresher Training- Curriculum Transition: EMT-Basic EMT Timeline: February 2012-March 2015 Introduction This document provides the statewide
2012 Mississippi EMT Transitional Refresher Curriculum EMT Refresher Training- Curriculum Transition: EMT-Basic EMT Timeline: February 2012-March 2015 Introduction This document provides the statewide
Cornual ruptured pregnancy with placenta increta CORNUAL RUPTURED PREGNANCY WITH PLACENTA INCRETA A RARE CASE
 142 CORNUAL RUPTURED PREGNANCY WITH PLACENTA INCRETA A RARE CASE Agarwal NR 1, Rani A 1 *, Batra S 1 1. Department of Obststetrics and Gynaecology, Institute of Medical Sciences, Banares Hindu Univarsity.
142 CORNUAL RUPTURED PREGNANCY WITH PLACENTA INCRETA A RARE CASE Agarwal NR 1, Rani A 1 *, Batra S 1 1. Department of Obststetrics and Gynaecology, Institute of Medical Sciences, Banares Hindu Univarsity.
CLINICAL GUIDELINE FOR VAGINAL BIRTH AFTER CAESAREAN SECTION (VBAC)
") CLINICAL GUIDELINE FOR VAGINAL BIRTH AFTER CAESAREAN SECTION (VBAC) 1. Aim/Purpose of this Guideline 1.1. Due to a rise in the caesarean section rate there are increasing numbers of pregnant women who
CLINICAL GUIDELINE FOR VAGINAL BIRTH AFTER CAESAREAN SECTION (VBAC) 1. Aim/Purpose of this Guideline 1.1. Due to a rise in the caesarean section rate there are increasing numbers of pregnant women who
TITLE 836 INDIANA EMERGENCY MEDICAL SERVICES COMMISSION. ARTICLE 1.5 Trauma Field Triage and Transport Destination Requirements
 TITLE 836 INDIANA EMERGENCY MEDICAL SERVICES COMMISSION ARTICLE 1.5 Trauma Field Triage and Transport Destination Requirements 836 IAC 1.5-1 Purpose Affected: [IC 10-14-3-12; IC 16-18; IC 16-21-2; IC 16-31-2-9;
TITLE 836 INDIANA EMERGENCY MEDICAL SERVICES COMMISSION ARTICLE 1.5 Trauma Field Triage and Transport Destination Requirements 836 IAC 1.5-1 Purpose Affected: [IC 10-14-3-12; IC 16-18; IC 16-21-2; IC 16-31-2-9;
Why your weight matters during pregnancy and after birth
 Information for you Published in November 2011 (next review date: 2015) Why your weight matters during pregnancy and after birth Most women who are overweight have a straightforward pregnancy and birth
Information for you Published in November 2011 (next review date: 2015) Why your weight matters during pregnancy and after birth Most women who are overweight have a straightforward pregnancy and birth
EMR EMERGENCY MEDICAL RESPONDER Course Syllabus
 6111 E. Skelly Drive P. O. Box 477200 Tulsa, OK 74147-7200 EMR EMERGENCY MEDICAL RESPONDER Course Syllabus Course Number: HLTH-0009 OHLAP Credit: No OCAS Code: 9373 Course Length: 66 Hours Career Cluster:
6111 E. Skelly Drive P. O. Box 477200 Tulsa, OK 74147-7200 EMR EMERGENCY MEDICAL RESPONDER Course Syllabus Course Number: HLTH-0009 OHLAP Credit: No OCAS Code: 9373 Course Length: 66 Hours Career Cluster:
Chapter 7. Ideally, educational preparation for childbirth begins prior to conception
 Chapter 7 Nursing Management of Pain During Labor and Birth Key Terms Cleansing breath Effleurage Endorphins Pain threshold Focal point Pain tolerance Education for Childbearing Ideally, educational preparation
Chapter 7 Nursing Management of Pain During Labor and Birth Key Terms Cleansing breath Effleurage Endorphins Pain threshold Focal point Pain tolerance Education for Childbearing Ideally, educational preparation
Registered Nurse Initiated Activities Decision Support Tool No. 8A: Obstetrical Emergencies Cord Prolapse
 Registered Nurse Initiated Activities Decision Support Tool No. 8A: Obstetrical Emergencies Cord Prolapse Decision support tools are evidenced-based documents used to guide the assessment, diagnosis and
Registered Nurse Initiated Activities Decision Support Tool No. 8A: Obstetrical Emergencies Cord Prolapse Decision support tools are evidenced-based documents used to guide the assessment, diagnosis and
It is recommended that the reader review each medical directive presented in this presentation along with the actual PCP Core medical directive.
 It is recommended that the reader review each medical directive presented in this presentation along with the actual PCP Core medical directive. This presentation will highlight the changes and any new
It is recommended that the reader review each medical directive presented in this presentation along with the actual PCP Core medical directive. This presentation will highlight the changes and any new
35-40% of GBS disease occurs in the elderly or in adults with chronic medical conditions.
 What is Group B Strep (GBS)? Group B Streptococcus (GBS) is a type of bacteria that is found in the lower intestine of 10-35% of all healthy adults and in the vagina and/or lower intestine of 10-35% of
What is Group B Strep (GBS)? Group B Streptococcus (GBS) is a type of bacteria that is found in the lower intestine of 10-35% of all healthy adults and in the vagina and/or lower intestine of 10-35% of
Premature Infant Care
 Premature Infant Care Introduction A premature baby is born before the 37th week of pregnancy. Premature babies are also called preemies. Premature babies may have health problems because their organs
Premature Infant Care Introduction A premature baby is born before the 37th week of pregnancy. Premature babies are also called preemies. Premature babies may have health problems because their organs
Cardiovascular Disease and Maternal Mortality what do we know and what are the key questions?
 Cardiovascular Disease and Maternal Mortality what do we know and what are the key questions? AFSHAN HAMEED, MD, FACOG, FACC Associate Clinical Professor Maternal Fetal Medicine and Cardiology University
Cardiovascular Disease and Maternal Mortality what do we know and what are the key questions? AFSHAN HAMEED, MD, FACOG, FACC Associate Clinical Professor Maternal Fetal Medicine and Cardiology University
National Registry Skill Sheets
 Bleeding Control/Shock Management BVM Ventilation of an Apneic Adult Patient Cardiac Arrest Management/AED Joint Immobilization Long Bone Immobilization Oxygen Administration By Non-Rebreather Mask Patient
Bleeding Control/Shock Management BVM Ventilation of an Apneic Adult Patient Cardiac Arrest Management/AED Joint Immobilization Long Bone Immobilization Oxygen Administration By Non-Rebreather Mask Patient
A 28 year old woman, gravida 2, para 1, at 16 weeks gestation informs you that her cat, which she has owned for several years, has toxoplasmosis, as
 A 28 year old woman, gravida 2, para 1, at 16 weeks gestation informs you that her cat, which she has owned for several years, has toxoplasmosis, as diagnosed from a stool sample. She is concerned about
A 28 year old woman, gravida 2, para 1, at 16 weeks gestation informs you that her cat, which she has owned for several years, has toxoplasmosis, as diagnosed from a stool sample. She is concerned about
TN Emergency Medical Services
 TN Emergency edical ODULES AND UNITS ES System ES Providers: ER and ET Safety and Wellness Body echanics System Communication Documentation Therapeutic Communication Legal and Ethical Issues Intro to Respiratory
TN Emergency edical ODULES AND UNITS ES System ES Providers: ER and ET Safety and Wellness Body echanics System Communication Documentation Therapeutic Communication Legal and Ethical Issues Intro to Respiratory
STATE OF CONNECTICUT
 STATE OF CONNECTICUT DEPARTMENT OF PUBLIC HEALTH June 7, 2010 The Following Will Be Policy For Emergency Medical Service Care Providers: GUIDELINES FOR EMR, EMT, AEMT, and Paramedic DETERMINATION OF DEATH/DISCONTINUATION
STATE OF CONNECTICUT DEPARTMENT OF PUBLIC HEALTH June 7, 2010 The Following Will Be Policy For Emergency Medical Service Care Providers: GUIDELINES FOR EMR, EMT, AEMT, and Paramedic DETERMINATION OF DEATH/DISCONTINUATION
Claiming Compensation for Birth Injuries.
 Clinical Negligence: Claiming Compensation for Birth Injuries. T H O M P S O N S F A C T S H E E T About birth injury Compensation Types of birth injury cases where compensation may be possible How to
Clinical Negligence: Claiming Compensation for Birth Injuries. T H O M P S O N S F A C T S H E E T About birth injury Compensation Types of birth injury cases where compensation may be possible How to
National Registry of Emergency Medical Technicians Emergency Medical Responder Psychomotor Examination PATIENT ASSESSMENT/MANAGEMENT TRAUMA
 PATIENT ASSESSMENT/MANAGEMENT TRAUMA Scenario # Note: Areas denoted by ** may be integrated within sequence of Primary Survey/Resuscitation SCENE SIZE-UP Determines the mechanism of injury/nature of illness
PATIENT ASSESSMENT/MANAGEMENT TRAUMA Scenario # Note: Areas denoted by ** may be integrated within sequence of Primary Survey/Resuscitation SCENE SIZE-UP Determines the mechanism of injury/nature of illness
What Does Pregnancy Have to Do With Blood Clots in a Woman s Legs?
 Patient s Guide to Prevention of Blood Clots During Pregnancy: Use of Blood-Thinning A Patient s Guide to Prevention of Blood Clots During Pregnancy: Use of Blood-Thinning Drugs to Prevent Abnormal Blood
Patient s Guide to Prevention of Blood Clots During Pregnancy: Use of Blood-Thinning A Patient s Guide to Prevention of Blood Clots During Pregnancy: Use of Blood-Thinning Drugs to Prevent Abnormal Blood
Assessment of Fetal Growth
 Assessment of Fetal Growth Unit / Trust: 1. INTRODUCTION The aim of this guideline template is to outline the methods used to assess fetal growth and the referral pathways utilising customised antenatal
Assessment of Fetal Growth Unit / Trust: 1. INTRODUCTION The aim of this guideline template is to outline the methods used to assess fetal growth and the referral pathways utilising customised antenatal
The Rh Factor: How It Can Affect Your Pregnancy
 The American College of Obstetricians and Gynecologists f AQ FREQUENTLY ASKED QUESTIONS FAQ027 PREGNANCY The Rh Factor: How It Can Affect Your Pregnancy What is the Rh factor? How does a person get the
The American College of Obstetricians and Gynecologists f AQ FREQUENTLY ASKED QUESTIONS FAQ027 PREGNANCY The Rh Factor: How It Can Affect Your Pregnancy What is the Rh factor? How does a person get the
Guidelines for the Management of a Pregnant Trauma Patient
 SOGC CLINICAL PRACTICE GUIDELINE No. 325, June 2015 Guidelines for the Management of a Pregnant Trauma Patient This clinical practice guideline has been prepared by the Maternal Fetal Medicine Committee,
SOGC CLINICAL PRACTICE GUIDELINE No. 325, June 2015 Guidelines for the Management of a Pregnant Trauma Patient This clinical practice guideline has been prepared by the Maternal Fetal Medicine Committee,
The Developing Person Through the Life Span 8e by Kathleen Stassen Berger
 The Developing Person Through the Life Span 8e by Kathleen Stassen Berger Chapter 4 Prenatal Development and Birth PowerPoint Slides developed by Martin Wolfger and Michael James Ivy Tech Community College-Bloomington
The Developing Person Through the Life Span 8e by Kathleen Stassen Berger Chapter 4 Prenatal Development and Birth PowerPoint Slides developed by Martin Wolfger and Michael James Ivy Tech Community College-Bloomington
PATIENT CONSENT TO PROCEDURE - ROUX-EN-Y GASTRIC BYPASS
 As a patient you must be adequately informed about your condition and the recommended surgical procedure. Please read this document carefully and ask about anything you do not understand. Please initial
As a patient you must be adequately informed about your condition and the recommended surgical procedure. Please read this document carefully and ask about anything you do not understand. Please initial
National Registry of Emergency Medical Technicians Emergency Medical Responder Psychomotor Examination BVM VENTILATION OF AN APNEIC ADULT PATIENT
 BVM VENTILATION OF AN APNEIC ADULT PATIENT Candidate: Examiner: Date: Signature: Possible Points Checks responsiveness NOTE: After checking responsiveness and breathing for at least 5 but no 1 Checks breathing
BVM VENTILATION OF AN APNEIC ADULT PATIENT Candidate: Examiner: Date: Signature: Possible Points Checks responsiveness NOTE: After checking responsiveness and breathing for at least 5 but no 1 Checks breathing
CBT521-EMT11- OB/GYN Emergencies
 Seattle-King County EMS Seattle-King County Emergency Medical Services Division Public Health - Seattle/King County 401 5 th Avenue, Suite 1200 Seattle, WA 98104 (206) 296-4863 January 2011 CBT521-EMT11-
Seattle-King County EMS Seattle-King County Emergency Medical Services Division Public Health - Seattle/King County 401 5 th Avenue, Suite 1200 Seattle, WA 98104 (206) 296-4863 January 2011 CBT521-EMT11-
Objectives. Burn Assessment and Management. Questions Regarding the Case Study. Case Study. Patient Assessment. Patient Assessment
 Objectives Burn Assessment and Management Discuss the mechanisms and complications of a thermal burn, electrical burn and an inhalation burn Explain the factors to consider when determining the severity
Objectives Burn Assessment and Management Discuss the mechanisms and complications of a thermal burn, electrical burn and an inhalation burn Explain the factors to consider when determining the severity
EMS POLICIES AND PROCEDURES
 EMS POLICIES AND PROCEDURES POLICY #: 13 EFFECT DATE: xx/xx/05 PAGE: 1 of 4 *** DRAFT *** SUBJECT: TRIAGE OF TRAUMA PATIENTS *** DRAFT *** APPROVED BY: I. PURPOSE Art Lathrop, EMS Director Joseph A. Barger,
EMS POLICIES AND PROCEDURES POLICY #: 13 EFFECT DATE: xx/xx/05 PAGE: 1 of 4 *** DRAFT *** SUBJECT: TRIAGE OF TRAUMA PATIENTS *** DRAFT *** APPROVED BY: I. PURPOSE Art Lathrop, EMS Director Joseph A. Barger,
Training Bulletin. June 2014. Emergency Health Services Branch Ministry of Health and Long-Term Care. Issue Number 113 version 1.0
 Training Bulletin Field Trauma Triage and Air Ambulance Utilization Standards June 2014 Issue Number 113 version 1.0 Emergency Health Services Branch Ministry of Health and Long-Term Care Training Bulletin,
Training Bulletin Field Trauma Triage and Air Ambulance Utilization Standards June 2014 Issue Number 113 version 1.0 Emergency Health Services Branch Ministry of Health and Long-Term Care Training Bulletin,
Diagnosis Codes for Pregnancy and Complications of Pregnancy
 This list is for informational purposes only and is not a binding or definitive list of covered conditions. It is not a guarantee of coverage; coverage depends on the available benefits and eligibility
This list is for informational purposes only and is not a binding or definitive list of covered conditions. It is not a guarantee of coverage; coverage depends on the available benefits and eligibility
Question-and-Answer Document 2010 AHA Guidelines for CPR & ECC As of October 18, 2010
 Question-and-Answer Document 2010 AHA Guidelines for CPR & ECC As of October 18, 2010 Q: What are the most significant changes in the 2010 AHA Guidelines for CPR & ECC? A: Major changes for all rescuers,
Question-and-Answer Document 2010 AHA Guidelines for CPR & ECC As of October 18, 2010 Q: What are the most significant changes in the 2010 AHA Guidelines for CPR & ECC? A: Major changes for all rescuers,
Home Health Agencies. Ante & Postpartum Members
 FIRST PRIORITY HEALTH /FIRST PRIORITY LIFE INSURANCE COMPANY BLUE CROSS OF NORTHEASTERN PENNSYLVANIA CREDENTIALING CRITERIA FOR OBSTETRIC NURSES IN HOME CARE ADMINISTRATIVE PRACTICE GUIDELINE PROVIDER
FIRST PRIORITY HEALTH /FIRST PRIORITY LIFE INSURANCE COMPANY BLUE CROSS OF NORTHEASTERN PENNSYLVANIA CREDENTIALING CRITERIA FOR OBSTETRIC NURSES IN HOME CARE ADMINISTRATIVE PRACTICE GUIDELINE PROVIDER
Labor is work, and it is hard work. Labor is an end to pregnancy and a beginning for a new human life in a newly shaped family."
 LABOR AND DELIVERY "The way we give birth to our young is that the muscular organ (the uterus) in which the offspring has been nurtured for nine months begins to contract. The contractions work to open
LABOR AND DELIVERY "The way we give birth to our young is that the muscular organ (the uterus) in which the offspring has been nurtured for nine months begins to contract. The contractions work to open
Obstetric Emergencies
 Obstetric Emergencies Dr. Si Lay Khaing Senior Lecturer/ O&G Specialist Faculty of Medicine University of Malaya 15 th March 2014 Abstract Life Saving, The obstetric patient is unique in medicine as two
Obstetric Emergencies Dr. Si Lay Khaing Senior Lecturer/ O&G Specialist Faculty of Medicine University of Malaya 15 th March 2014 Abstract Life Saving, The obstetric patient is unique in medicine as two
Sepsis: Identification and Treatment
 Sepsis: Identification and Treatment Daniel Z. Uslan, MD Associate Clinical Professor Division of Infectious Diseases Medical Director, UCLA Sepsis Task Force Severe Sepsis: A Significant Healthcare Challenge
Sepsis: Identification and Treatment Daniel Z. Uslan, MD Associate Clinical Professor Division of Infectious Diseases Medical Director, UCLA Sepsis Task Force Severe Sepsis: A Significant Healthcare Challenge
Carry out vaginal examinations at least once every 4 hours in the first stage of labour and plot the findings on the partograph.
 First stage: Diagnosis of Labour Latent phase - Cervix less than 4 cm dilated. Active phase - Cervix between 4 cm and 10 cm dilated - Rate of cervical dilatation at least 1 cm/hour - Effacement is usually
First stage: Diagnosis of Labour Latent phase - Cervix less than 4 cm dilated. Active phase - Cervix between 4 cm and 10 cm dilated - Rate of cervical dilatation at least 1 cm/hour - Effacement is usually
.org. Fractures of the Thoracic and Lumbar Spine. Cause. Description
 Fractures of the Thoracic and Lumbar Spine Page ( 1 ) Spinal fractures can vary widely in severity. While some fractures are very serious injuries that require emergency treatment, other fractures can
Fractures of the Thoracic and Lumbar Spine Page ( 1 ) Spinal fractures can vary widely in severity. While some fractures are very serious injuries that require emergency treatment, other fractures can
X-Plain Abdominal Aortic Aneurysm Vascular Surgery Reference Summary
 X-Plain Abdominal Aortic Aneurysm Vascular Surgery Reference Summary Ballooning of the aorta, also known as an "abdominal aortic aneurysm," can lead to life threatening bleeding. Doctors may recommend
X-Plain Abdominal Aortic Aneurysm Vascular Surgery Reference Summary Ballooning of the aorta, also known as an "abdominal aortic aneurysm," can lead to life threatening bleeding. Doctors may recommend
January-February 2008 Volume 27 Number 1. Case Study Peer Reviewed Perimortem cesarean section in the helicopter EMS setting: A case report
 January-February 2008 Volume 27 Number 1 Case Study Peer Reviewed Perimortem cesarean section in the helicopter EMS setting: A case report http://www2.us.elsevierhealth.com/inst/serve?retrieve=pii/s1067-991x(07)00164-2&arttype=full#head1
January-February 2008 Volume 27 Number 1 Case Study Peer Reviewed Perimortem cesarean section in the helicopter EMS setting: A case report http://www2.us.elsevierhealth.com/inst/serve?retrieve=pii/s1067-991x(07)00164-2&arttype=full#head1
SAMPLE. UK Obstetric Surveillance System. Management of Pregnancy following Laparoscopic Adjustable Gastric Band Surgery.
 ID Number: UK Obstetric Surveillance System Management of Pregnancy following Laparoscopic Adjustable Gastric Band Surgery Case Definition: Study 04/11 Data Collection Form - Please report any woman delivering
ID Number: UK Obstetric Surveillance System Management of Pregnancy following Laparoscopic Adjustable Gastric Band Surgery Case Definition: Study 04/11 Data Collection Form - Please report any woman delivering