Improving Weaning Automation (WEAN Study)
|
|
|
- Eric Warner
- 9 years ago
- Views:
Transcription

1 , 2013 Improving Weaning Automation (WEAN Study) François LELLOUCHE, MD, PhD Centre de recherche de l Institut Universitaire de Cardiologie et de Pneumologie de Québec

2 CONFLICTS OF INTEREST - Research contracts with Drager medical (5000can$ for travel expenses for the Canadian study on SmartCare-WEAN study) - Research contracts with Hamilton medical to conduct Intellivent evaluation (Salary of the research assistant) - Program of research on automated ventilation and oxygen therapy: Canadian for Innovation(Fonds des Leaders)/FRSQ grants
/FRSQ")
3 PLAN Too many modes! Evidence-based for new modes? Why automated modes should be promoted? SmartCare: automated weaning with pressure support Clinical evaluation of SmartCare (WEAN study)

4 VPC VAC+ VAPS IPAP PC NAVA Automode BILEVEL ASB VACI VCRP CPAP PAC Autoflow VS AI VPAC VA VAC VC VIV SmartCare PA PACI VS-PPV TC PSV SIMV VAIV VPL PAV PRVC VPS ASV PPS ATC EPAP VACI+ Intellivent MMV VS-AI-Vt mini APRV APV BIPAP VPC SPAP Advanced closed loop during mechanical ventilation. Lellouche&Brochard, Best Pract Res 2009

5 Dual mode within a breath (VAPS) Dual modes breath to breath (VCRP, Autoflow, Volume Assist) Automode Proportionnal Assist Ventilation (PAV) Adaptative Support Ventilation (ASV) Automatic Tube Compensation (ATC) Airway Pressure Release Ventilation (APRV) Respiratory care 2004
 Airway Pressure Release Ventilation (APRV)")
6 ii. Nasogastric tube iii. Amplifier unit NAVA (Sinderby et al., Nature 1999) i. Electrode array iv. Signal processing unit v. Ventilator unit

7 PAV (Younes ARRD 1992) Pressure support ventilation and proportional assist ventilation during weaning from mechanical ventilation. Aguirre-Bermeo H, Bottiroli M, Italiano S, Roche-Campo F, Santos JA, Alonso M, Mancebo J. Med Intensiva Oct 18. [Epub ahead of print]

8 Why automated modes should be promoted? NEJM 2000 ARMA Study 6 vs 12 ml/kg de PIT Health care system under pressure Aging population Failure of the knowledge transfert Weaning/protective ventilatory strategy AUTOMATED KT Machines superiors for simple tasks AUTOMATED SYSTEMS

9 Rationale for weaning automation Weaning protocols are efficient (Ely NEJM 1996, Saura ICM 1996, Kollef CCM 1997, Marelich 2000) and recommended (Mc Intyre Chest 2001, Boles ERJ 2007)..but many obstacles (Ely AJRCCM 1999, Vitacca ICM 2001) to implement weaning protocols trainings on a regular basis required, problems with new protocols and new practices acceptance Great amount of data on weaning (physiological studies & RCT): Esteban, Brochard, Mancebo, Ely, Epstein, Tobin

 Automated adaptation of PSV level 2) Automated weaning protocol automatic decrease of the PSV automatic SBT Message in")
10 Dojat et al. Int J Clin Monit Comput 1992 Automated Weaning: SmartCare Ventilator in PSV 1) Automated adaptation of PSV level 2) Automated weaning protocol automatic decrease of the PSV automatic SBT Message in case of successful SBT Patient Monitor Patient Monitor Alarms Control Control Patient Input Automated pressure support Output Automated Weaning RR, TV, EtCO 2 Automatic Weaning System SmartCare Processing


11 Level of Pressure support (cmh 2O) Example of Weaning with «SmartCare» Minimum level of PS Adaptation Automated reduction of the PSV level Message: «separation from ventilator» PEEP must be 5 cmh 2 O Observation «Automated SBT» Maintain 0:00 0:28 0:57 1:26 1:55 2:24 2:52 E X T U B A T I O N Time (h:min)

 PSV (cmh 2 O) PEEP (cmh 2 O) 43 automated adjustment of the PS level 3 automated SBT Adaptation Observation Message No SBT 1 automated message to consider extubation 2 3 4 5")
12 hours Diagnostic Respiratoire/Niveau with d assistance SmartCare Sur-Assistance AUTOMATED WEANING PHASES SBT# 1 SBT#2 SBT#3 Sous-Assistance 210 automated evaluations of the patient RR (c/min) PSV (cmh 2 O) PEEP (cmh 2 O) 43 automated adjustment of the PS level 3 automated SBT Adaptation Observation Message No SBT 1 automated message to consider extubation CONSIDER SEPARATION Temps (h)

13 INITIAL CLINICAL EVALUATIONS OF SMARTCARE (prototype = NéoGanesh) Dojat et al. AJRCCM 1992 Maintain of the patients in the comfort zone 95% of time 19 patients Dojat et al. AJRCCM 1996 Good performances of the system to predict extubation success/failures 38 patients Dojat et al. AJRCCM 2000 Efficiency of the system to maintain the patients in a comfort zone Reduction of time with high P modifications of PSV/24 hrs vs 1 modification PSV/24 hrs 10 patients Bouadma, Lellouche et al. Intensive Care Med 2005 Possibility to ventilate patients with the system during prolonged periods (up to 12 days)-pilot study for multicenter RCT 42 patients



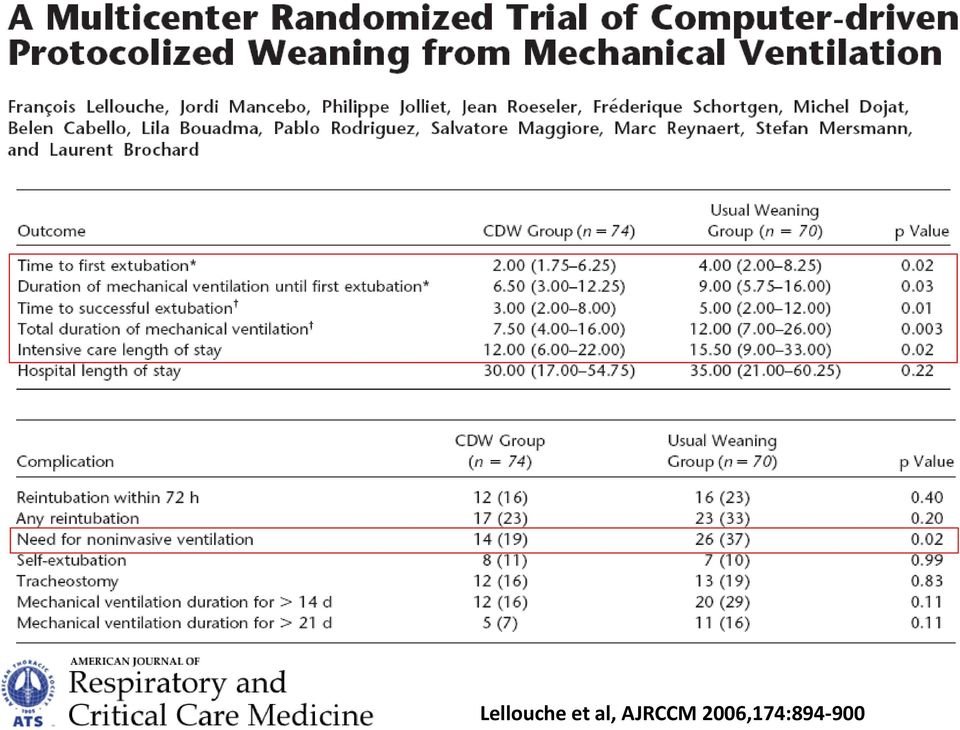
14 YES 1 st Multicenter Randomized Study 144 patients included, 5 centres Mixed population Automated weaning VS Usual protocolized weaning Weaning possible if all following criteria are present: - Improvement of condition having led to intubation - Absence of uncontrolled severe infection - Correction of metabolic disorders - Adequate hemoglobin level - No hemodynamic instability - PaO 2 > 8.5 kpa with FIO and PEEP 5 cmh 2 O Mechanical ventilation Question at least 2 times a day: Weaning possible? YES Initiation of weaning Stop or lowering of sedation Level of Pressure Support : 20 cmh 2 O NO NO PS level 20 cmh 2 O above PEEP > 60 minutes? YES Spontaneous breathing test feasible if after 60' Question at least 2 times a day: with PS 20 cmh Spontaneous breathing test feasible? 2 O, PEEP 5 cmh 2 O (all must be present): Adaptation - Respiratory rate 30/' of PS - Tidal volume 6 ml/kg YES and/or - No hemodynamic instability NO - SpO 2 90% and FIO PEEP level - No other contra-indication Spontaneous breathing test during 30' First choice: Pressure support 10 cmh 2 O, ± PEEP 5 cmh 2 O Extubation criteria (all must be Other choices: - T-piece trial present) - Respiratory rate 30/' - CPAP, flow 30 l/min. PEEP 5 cmh 2 O - Pulse < 120/' Extubation criteria present? - Syst. ABP < 180 and > 90 mmhg - No hemodynamic instability - PaO kpa and FIO ph > 7.30 YES NO Extubation possible? - Level of consciousness Primary end point: OK - Efficient swallowing - Efficient cough NO YES Patient weaned but extubation not possible EXTUBATION Weaning process can begin if: The cause of the respiratory failure is partially or completely controlled, including a SpO2 90% under FIO2 0.5 and PEEP 5 cm H2O Hemodynamic stability (Systolic Blood Pressure between 90 and 160mm Hg + Pulse Weaning time between 60 and 125 /minute + absence of uncontrolled arrhythmias) Temperature < 39 C Haemoglobin 8 g/dl (inclusion first extubation) Absence of significant hydro-electrolytes abnormalities Patients can follow simples orders and there is not need for high dose of sedatives For neurological patients: Glascow Coma Scale > 8, Intra-Cranial Pressure < 20 mmhg, Cerebral Perfusion Pressure > 60 mmhg Those patients who accomplish these criteria will follow a spontaneous breathing test (2 hours T tube or Pressure Support Ventilation with 7 cm H2O of pressure support and Positive End Expiratory Pressure 5 cm H2O). No tolerance to spontaneous breathing test will be considerer if: Respiratory Rate > 35 bpm + clinical manifestation * Hypoxemia (PaO2 < 60 mmhg under O2 flow 4 L/min) Acidosis (ph 7.3) * Clinical manifestations: Systolic Blood Pressure 160 mmhg or 90 mmhg, Heart Rate 140 bpm or augmentation of 25% of baseline, new arrhythmia, lower conscience level, sweating or agitation. 1. Patients will be extubated if they successfully complete the 2 hours spontaneous breathing trial and they have an adequate cough 2. For patients that do not tolerate the spontaneous breathing test, weaning will continue on Pressure Support Ventilation. Pressure Support will be adjusted to achieve a respiratory frequency of bpm and a good clinical adaptation. Pressure Support will be diminished as soon as possible following patient s clinical tolerance. Patients will be extubated if tolerating low Pressure Support levels (next to 10 cm H2O) with low PEEP levels ( 5 cm H2O) if clinical tolerance and cough are adequate.

15 Lellouche et al, AJRCCM 2006,174:

16 Randomized Controlled Trial Monocentric, medical patients 102 patients included High levels of PEEP... Rose, Intensive Care Medicine 2008

 9 centres Interventions: Automated Weaning (SmartCare ) vs.")

17 Population: Critically ill adults requiring MV> 24 h - Early stage of the weaning process - When patients first tolerate PS (PS Trial) - Patients who are not already weaned (SBT successfully completed) 9 centres Interventions: Automated Weaning (SmartCare ) vs. Protocolized Weaning (paper-based protocol) Common features: PS mode, opportunities for SBTs, PEEP/FiO 2 chart, sedation protocol, extubation/reintubation criteria, criteria for NIV for post-extubation respiratory distress. Primary Outcome: Compliance and acceptance with the weaning & sedation protocols Secondary Outcomes: weaning and mechanical ventilation duration, mechanical ventilation complications Burns et al., AJRCCM 2013

18 Baseline Characteristics Automated Weaning (n=49) Protocolized Weaning (n=43) p-value Age (year), mean (std) 62.0 (13.8) 65.9 (13.6) 0.18 Female, n (%) 18 (36.7%) 20 (46.5%) 0.34 Duration of MV before randomization (days), median (IQT) 6 (3-10) 5 (2-8) 0.14 Apache II, mean (std) 23.5 (6.3) 23.9 (8.3) 0.78 MODS, mean (std) 5.0 (2.6) 5.0 (2.2) 0.93 COPD, n (%) 10 (20.4%) 13 (30.2%) 0.28 Central neurologic disorder, n (%) 7 (14.3%) 5 (11.6%) 0.71 Classification, n (%) non operative 36 (73.5%) 30 (69.8%) emergent post-op 8 (18.0%) 5 (11.6%) 0.51 elective postop 5 (10.0%) 7 (16.3%) Cointerventions at randomization, n (%) Continuous/intermittent sedation 32 (66.7%) 33 (76.7%) 0.29 Continuous/intermittent narcotics 35 (72.9%) 29 (67.4%) 0.57 Inotropes or vasopressors 9 (18.8%) 4 (9.3%) 0.24 Enteral/parenteral nutrition 43 (89.6%) 36 (83.7%) 0.41 Antibiotics 37 (77.1%) 32 (74.4%) 0.77 Pulmonary artery catheter 0 1 (2.3%) 0.47 Dialysis (intermittent or continuous) 3 (6.3%) 4 (9.3%) 0.70 Neuroleptic medications 5 (10.4%) 6 (14.0%) 0.61
 7 (16.3%) Cointerventions at randomization, n (%) Continuous/intermittent sedation 32 (66.7%) 33 (76.7%) 0.29 Continuous/intermittent narcotics 35 (72.9%) 29 (67.4%) 0.")
19 Peri-randomization mechanical ventilation setting Automated Weaning (n=49) Protocolized Weaning (n=43) p-value Mode of ventilation before PST, n (%) PC 2 (4.1%) 5 (11.6%) 0.25 SIMV + PS 1 (2.0%) 3 (7.0%) 0.34 PRVC 6 (12.2%) PS 34 (67.3%) 25 (58.1%) 0.36 AC 7 (14.3%) 10 (23.3%) 0.27 PST duration (min), mean (std) (86.6) (131.7) 0.98 Ventilator settings after successful PST PS (above PEEP) cm H 2 O, mean (std) 15.9 (4.1) 16.0 (4.1) 0.93 Set PEEP, mean (std) 6.5 (1.7) 6.4 (1.6) 0.70 FiO 2, mean (std) 0.40 (0.07) 0.44 (0.09) 0.02
 cm H 2 O, mean (std) 15.9 (4.1) 16.0 (4.1) 0.93 Set PEEP, mean (std) 6.5 (1.")
20 PRIMARY OUTCOME Compliance and Acceptance Weaning and Sedation Protocols Automated Weaning (n=49) Protocolized Weaning (n=43) P Value COMPLIANCE - Weaning Protocol Days with protocol violations (%) Average hours off protocol (median, IQR) Proportion of hours with protocol violation (%) 29.0 (8.6) 21.3 (± 9.9) 2.2 (± 5.6) 18.0 (3.5) 17.8 (± 7.4) 2.6 (±1.1) COMPLIANCE - Sedation Protocol Total missing SAS or RASS scores, n (%) Missing SAS or RASS on weaning protocol Extreme SAS or RASS scores Extreme SAS or RASS scores on protocol 302 (14.7) 69 (22.8%) 66 (4.1%) 29 (3.3%) 467 (14.9) 184 (39.4%) 120 (4.7%) 69 (3.9%) 0.86 < Weaning Protocol Acceptance (0-10 scale) Physician acceptance score (mean, std) RT acceptance scores (mean, std) 7.4 (± 2.5) 7.2 (± 2.6) 8.1 (± 2.3) 8.1 (± 1.8) 0.01 < Sedation Protocols Acceptance (0-10 scale) RN acceptance score - SAS (mean, std) RN acceptance score - RASS (mean, std) 7.9 (± 1.9) 8.0 (± 1.7) 7.6 (± 2.4) 8.4 (± 1.9)
 66 (4.1%) 29 (3.3%) 467 (14.9) 184 (39.4%) 120 (4.7%) 69 (3.9%) 0.86 <0.0001 0.36 0.")
21 SECONDARY OUTCOMES Automated Weaning (n=49) Protocolized Weaning (n=43) p-value Time to first extubation, days, mean (sd) 3.9 (3.3) 8.1 (9.2) 0.02 Time to successful ext., days, mean (sd) 4.8 (3.4) 10.5 (11.1) 0.01 Total duration of MV, days, mean (sd) 11.5 (5.8) 15.4 (12.0) 0.13 ICU length of stay, days, mean (sd) 9.7 (7.8) 15.3 (12.8) 0.04 Hospital length of stay, days, mean (sd) 28.0 (26.0) 31.3 (18.1) 0.54 Nosocomial pneumonia, n (%) 5 (10%) 6 (14.0%) 0.56 Reintubation, n (%) 9 (18%) 11 (25.6%) 0.38 Requirement for NIV, n (%) 4 (8.2%) 6 (14%) 0.50 Self extubation, n (%) 0 1 (2.6%) 0.48 ICU mortality, n (%) 9 (18.4%) 9 (20.9%) 0.80
22 Burns et al., AJRCCM 2013
23 RT acceptance (0-10 scale) median (IQR) Physician acceptance (0-10 scale) median (IQR) Time to first extubation, median (IQR) Time to successful ext., median (IQR) Time to successful completion of an SBT median (IQR) Total duration of mechanical ventilation, median (IQR) ICU length of stay, median (IQR) Tracheostomy, count (%) Prolonged mechanical ventilation at 21 days, n (%) AW n=20 7 (5, 8) 8 (5, 9) 4 (2, 10) 4 (3, 10) 0 (0, 2) 10 (8, 20) 10 (5, 16) 4 (20.0) 1 (6.7) HH p-value HME p-value PW n=17 8 (8, 10) 8 (7, 9) 4 (2, 6) 4 (2, 4) 2.5 (1.5, 4) 9 (6, 17) 6 (5, 9) 1 (5.9) AW PW n=29 n=26 < (7, 9) (8, 9) Sub-study Impact of humidification (7, 10) (8, 10) device 9 on (i) (2, 5) acceptance (3,16) 0.25 (ii) 4 outcome (2, 7) (3, 22) < (0, 3) CLUSTERS: (2, 10) centres 18.5used HH (8, 17) in both (11, 29) groups (5, 12) 3 centres (6, 28) used HME in both 14groups (13.8) (53.9) (28.6) Burns et al., AJRCCM 2013, Appendix E11
 118±165 hours (Protocols) (P=0.")
24 Automated weaning (SmartCare) vs local weaning protocols in post-surgical patients Randomized Controlled Trial Post-op patients with MV > 9 hours 300 patients included 94±144 hours (SmartCare) 118±165 hours (Protocols) (P=0.18) Schadler, AJRCCM 2012
25 Randomized controlled trial 48 patients who failed SBT Mixed population Monocentric Liu, Chinese Med J 2013
26 Lellouche et al., AJRCCM 2006 Rose et al., Intensive Care Medicine 2008 Liu et al., Chinese med J 2013 Schadler et al., AJRCCM 2012 Burns et al., AJRCCM 2013 In the context of increasing gap between needs and supply to manage patients on MV, All these studies can be considered «positive» : = better (or same outcome) with less human interventions
27 Evidence-Based Meta-analysis SmartCare versus Non-automated Weaning Strategies for Critically Ill Adults: A Systematic Review and Meta-analysis. Karen EA Burns, Francois Lellouche, Rosane Nisenbaum, Martin Lessard and Jan O. Friedrich Automated versus non-automated weaning for reducing the duration of mechanical ventilation for critically ill adults and children. Rose L, Schultz MJ, Cardwell CR, Jouvet P, McAuley DF, Blackwood B. Cochrane Database Syst Rev Jun 6;6:CD doi:0.1002/ cd pub2.
28 Why automated modes should be promoted? Mai 2000 NEJM ARMA Study 6 vs 12 ml/kg de PIT Health care system under pressure Aging population Failure of the knowledge transfert Weaning/protective ventilatory strategy AUTOMATED KT Machines superiors for simple tasks AUTOMATED SYSTEMS EVIDENCE from RCTs +++
29 LIMITATIONS OF SMARTCARE -Limitations of pressure support ventilation: In specific populations (Neuro/cardiac): T-Tube > PSV Patient-ventilator asynchronies in COPD patients -Only one parameter automatically set (PSV level) next generation = Fully Automated Ventilators Intellivent (Arnal ICM 2012, Lellouche ICM 2013), EWS (Schadler J Monit Comput 2013) -Use of HH with Smartcare can lead to EtCO 2 sensor errors -Specific features should be avoided (night rest option) -Only one manufacturer provides this «mode» (but accessible to all. no patent )
30 Conclusions: - Many reasons to use automated weaning - Evidence favoring Automated weaning: => Smartcare > to protocolized weaning with PSV => WEAN study: SmartCare VS. protocolized weaning with HIGH compliance rate -> promising results for clinically important outcomes - Larger RCT are needed.. automated weaning&ventilation will become standard of care - The next generation of ventilators will be (are) Fully Automated (Intellivent, Evita Weaning Systems)

31 Thank you!
Importance of Protocols in the Decision to Use Noninvasive Ventilation
 Importance of Protocols in the Decision to Use Noninvasive Ventilation Janice L. Zimmerman, M.D. Weill Cornell Medical College The Methodist Hospital Houston, Texas Objectives Review application of protocols
Importance of Protocols in the Decision to Use Noninvasive Ventilation Janice L. Zimmerman, M.D. Weill Cornell Medical College The Methodist Hospital Houston, Texas Objectives Review application of protocols
Mechanical Ventilation for Dummies Keep It Simple Stupid
 Mechanical Ventilation for Dummies Keep It Simple Stupid Indications Airway Ventilation failure (CO2) Hypoxia Combination Airway obstruction Inability to protect airway Hypoxia (PaO 2 < 50) Hypercapnia
Mechanical Ventilation for Dummies Keep It Simple Stupid Indications Airway Ventilation failure (CO2) Hypoxia Combination Airway obstruction Inability to protect airway Hypoxia (PaO 2 < 50) Hypercapnia
Year in review: mechanical ventilation
 Year in review: mechanical ventilation Leo Heunks, MD, PhD Pulmonary and Critical Care Physician Dept of Critical Care Intensivisten dagen 2013 Disclosures Maquet (NAVA catheters, travel fee, speakers
Year in review: mechanical ventilation Leo Heunks, MD, PhD Pulmonary and Critical Care Physician Dept of Critical Care Intensivisten dagen 2013 Disclosures Maquet (NAVA catheters, travel fee, speakers
From AARC Protocol Committee; Subcommittee Adult Critical Care Version 1.0a (Sept., 2003), Subcommittee Chair, Susan P. Pilbeam
, Subcommittee Chair, Susan P. Pilbeam") AARC - ADULT MECHANICAL VENTILATOR PROTOCOLS 1. Guidelines for Using Ventilator Protocols 2. Definition of Modes and Suggestions for Use of Modes 3. Adult Respiratory Ventilator Protocol - Guidelines for
AARC - ADULT MECHANICAL VENTILATOR PROTOCOLS 1. Guidelines for Using Ventilator Protocols 2. Definition of Modes and Suggestions for Use of Modes 3. Adult Respiratory Ventilator Protocol - Guidelines for
Protocols for Early Extubation After Cardiothoracic Surgery
 Protocols for Early Extubation After Cardiothoracic Surgery AATS / STS CT Critical Care Symposium April 27, 2014 Toronto, Ontario Nevin M. Katz, M.D. Johns Hopkins University Foundation for the Advancement
Protocols for Early Extubation After Cardiothoracic Surgery AATS / STS CT Critical Care Symposium April 27, 2014 Toronto, Ontario Nevin M. Katz, M.D. Johns Hopkins University Foundation for the Advancement
RES Non-Invasive Positive Pressure Ventilation Guideline Page 1 of 9
 Page 1 of 9 Scope: Respiratory Care Department, Physicians, Advanced Nurse Practitioners (APRN), Physician Assistants (PA) Population: Patients receiving rescue or non-rescue non-invasive positive pressure
Page 1 of 9 Scope: Respiratory Care Department, Physicians, Advanced Nurse Practitioners (APRN), Physician Assistants (PA) Population: Patients receiving rescue or non-rescue non-invasive positive pressure
Non-Invasive Positive Pressure Ventilation in Heart Failure Patients: For Who, Wy & When?
 REUNIÃO CONJUNTA DOS GRUPOS DE ESTUDO DE CUIDADOS INTENSIVOS CARDÍACOS E DE FISIOPATOLOGIA DO ESFORÇO E REABILITAÇÃO CARDÍACA O L H Ã O 2 7 e 2 8 d e J a n e i r o 2 0 1 2 Non-Invasive Positive Pressure
REUNIÃO CONJUNTA DOS GRUPOS DE ESTUDO DE CUIDADOS INTENSIVOS CARDÍACOS E DE FISIOPATOLOGIA DO ESFORÇO E REABILITAÇÃO CARDÍACA O L H Ã O 2 7 e 2 8 d e J a n e i r o 2 0 1 2 Non-Invasive Positive Pressure
Neurally Adjusted Ventilatory Assist: NAVA for Neonates
 Neurally Adjusted Ventilatory Assist: NAVA for Neonates Robert L. Chatburn, MHHS, RRT-NPS, FAARC Research Manager Respiratory Institute Cleveland Clinic Professor Department of Medicine Lerner College
Neurally Adjusted Ventilatory Assist: NAVA for Neonates Robert L. Chatburn, MHHS, RRT-NPS, FAARC Research Manager Respiratory Institute Cleveland Clinic Professor Department of Medicine Lerner College
Airway Pressure Release Ventilation
 Page: 1 Policy #: 25.01.153 Issued: 4-1-2006 Reviewed/ Revised: Section: 10-11-2006 Respiratory Care Airway Pressure Release Ventilation Description/Definition Airway Pressure Release Ventilation (APRV)
Page: 1 Policy #: 25.01.153 Issued: 4-1-2006 Reviewed/ Revised: Section: 10-11-2006 Respiratory Care Airway Pressure Release Ventilation Description/Definition Airway Pressure Release Ventilation (APRV)
Weaning the Unweanable
 Weaning the Unweanable Gerald W. Staton, Jr, MD Professor of Medicine Pulmonary & Critical Care Medicine Emory University School of Medicine Atlanta, GA [email protected] Disclosures Pulmonary Program
Weaning the Unweanable Gerald W. Staton, Jr, MD Professor of Medicine Pulmonary & Critical Care Medicine Emory University School of Medicine Atlanta, GA [email protected] Disclosures Pulmonary Program
MECHINICAL VENTILATION S. Kache, MD
 MECHINICAL VENTILATION S. Kache, MD Spontaneous respiration vs. Mechanical ventilation Natural spontaneous ventilation occurs when the respiratory muscles, diaphragm and intercostal muscles pull on the
MECHINICAL VENTILATION S. Kache, MD Spontaneous respiration vs. Mechanical ventilation Natural spontaneous ventilation occurs when the respiratory muscles, diaphragm and intercostal muscles pull on the
BIPAP Synchrony TM AVAPS
 BIPAP Synchrony TM AVAPS Product Presentation V1.6 Contents Home NIV Solution introduction BiPAP Technology and Auto-Trak algorithm Consensus conference, Chest 1999 The AVAPS algorithm The AVAPS settings
BIPAP Synchrony TM AVAPS Product Presentation V1.6 Contents Home NIV Solution introduction BiPAP Technology and Auto-Trak algorithm Consensus conference, Chest 1999 The AVAPS algorithm The AVAPS settings
Recommendations: Other Supportive Therapy of Severe Sepsis*
 Recommendations: Other Supportive Therapy of Severe Sepsis* K. Blood Product Administration 1. Once tissue hypoperfusion has resolved and in the absence of extenuating circumstances, such as myocardial
Recommendations: Other Supportive Therapy of Severe Sepsis* K. Blood Product Administration 1. Once tissue hypoperfusion has resolved and in the absence of extenuating circumstances, such as myocardial
Common Ventilator Management Issues
 Common Ventilator Management Issues William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center You have just admitted a 28 year-old
Common Ventilator Management Issues William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center You have just admitted a 28 year-old
What s s Happening in Canada
 Nurses Role in Mechanical Ventilation: an International Perspective Louise Rose Lawrence S. Bloomberg Professor in Critical Care Nursing University of Toronto Adjunct Scientist Li Ka Shing Institute, St
Nurses Role in Mechanical Ventilation: an International Perspective Louise Rose Lawrence S. Bloomberg Professor in Critical Care Nursing University of Toronto Adjunct Scientist Li Ka Shing Institute, St
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy
 The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
NURSING SERVICES DEPARTMENT
 NURSING SERVICES DEPARTMENT TITLE: Mechanical Ventilation PATIENT CARE PLAN DIAGNOSIS: DISCHARGE CRITERIA: 1 The patient will: Maintain adequate mechanics of PERTINENT INFORMATION:. ventilation as demonstrated
NURSING SERVICES DEPARTMENT TITLE: Mechanical Ventilation PATIENT CARE PLAN DIAGNOSIS: DISCHARGE CRITERIA: 1 The patient will: Maintain adequate mechanics of PERTINENT INFORMATION:. ventilation as demonstrated
Chronic Critical Illness: Can it be prevented? Carmen C Polito, MD Pulmonary & Critical Care Medicine Emory University Atlanta, GA cpolito@emory.
 Chronic Critical Illness: Can it be prevented? Carmen C Polito, MD Pulmonary & Critical Care Medicine Emory University Atlanta, GA [email protected] Data free zone Disclosures A (Very) Old Case 65 year-old
Chronic Critical Illness: Can it be prevented? Carmen C Polito, MD Pulmonary & Critical Care Medicine Emory University Atlanta, GA [email protected] Data free zone Disclosures A (Very) Old Case 65 year-old
Nursing Education and Research
 Melissa Meloche Meloche, RN RN, MSN MSN, CCRN Nursing Education and Research Describe the purpose p of common clinical equipment found in the Intensive Care Unit and how this equipment could impact a patient
Melissa Meloche Meloche, RN RN, MSN MSN, CCRN Nursing Education and Research Describe the purpose p of common clinical equipment found in the Intensive Care Unit and how this equipment could impact a patient
James F. Kravec, M.D., F.A.C.P
 James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
James F. Kravec, M.D., F.A.C.P Chairman, Department of Internal Medicine, St. Elizabeth Health Center Chair, General Internal Medicine, Northeast Ohio Medical University Associate Medical Director, Hospice
KING FAISAL SPECIALIST HOSPITAL AND RESEARCH CENTRE (GEN. ORG.) NURSING AFFAIRS. Scope of Service PEDIATRIC INTENSIVE CARE UNIT (PICU)
 NURSING AFFAIRS. Scope of Service PEDIATRIC INTENSIVE CARE UNIT (PICU)") PICU-Jan.2012 Page 1 of 7 Number of Beds: 18 Nurse Patient Ratio: 1:1-2 : The Pediatric Intensive Care Unit (PICU) provides 24 hour intensive nursing care for patients aged neonate through adolescence.
PICU-Jan.2012 Page 1 of 7 Number of Beds: 18 Nurse Patient Ratio: 1:1-2 : The Pediatric Intensive Care Unit (PICU) provides 24 hour intensive nursing care for patients aged neonate through adolescence.
Nurses Competencies in Caring for Mechanically Ventilated Patients, What does the Evidence Say? Dr. Samah Anwar Dr. Noha El-Baz
 Nurses Competencies in Caring for Mechanically Ventilated Patients, What does the Evidence Say? Dr. Samah Anwar Dr. Noha El-Baz The mechanically ventilated patient presents many challenges for the intensive
Nurses Competencies in Caring for Mechanically Ventilated Patients, What does the Evidence Say? Dr. Samah Anwar Dr. Noha El-Baz The mechanically ventilated patient presents many challenges for the intensive
Levels of Critical Care for Adult Patients
 LEVELS OF CARE 1 Levels of Critical Care for Adult Patients STANDARDS AND GUIDELINES LEVELS OF CARE 2 Intensive Care Society 2009 All rights reserved. No reproduction, copy or transmission of this publication
LEVELS OF CARE 1 Levels of Critical Care for Adult Patients STANDARDS AND GUIDELINES LEVELS OF CARE 2 Intensive Care Society 2009 All rights reserved. No reproduction, copy or transmission of this publication
MECHANICAL VENTILATION: AN OVERVIEW
 MECHANICAL VENTILATION: AN OVERVIEW by Kevin T. Martin BVE, RRT, RCP V7117 HC 04 RC Educational Consulting Services, Inc. P.O. Box 1930, Brockton, MA 02303-1930 (800) 441-LUNG / (877) 367-NURS www.rcecs.com
MECHANICAL VENTILATION: AN OVERVIEW by Kevin T. Martin BVE, RRT, RCP V7117 HC 04 RC Educational Consulting Services, Inc. P.O. Box 1930, Brockton, MA 02303-1930 (800) 441-LUNG / (877) 367-NURS www.rcecs.com
Ventilator Application of the Passy-Muir Valve David A. Muir Course Outline Benefits Review of the Biased Closed Position No Leak Passy-Muir Valves
 Ventilator Application of the Passy-Muir Valve Michael S. Harrell, B.S., RRT Director of Clinical Education-Respiratory [email protected] (949) 833-8255 David A. Muir 23 year-old ventilator dependent
Ventilator Application of the Passy-Muir Valve Michael S. Harrell, B.S., RRT Director of Clinical Education-Respiratory [email protected] (949) 833-8255 David A. Muir 23 year-old ventilator dependent
INTRODUCING RESMED S. Home NIV Solutions. S9 VPAP ST-A with ivaps S9 VPAP ST. Why choose average when you can choose intelligent?
 INTRODUCING RESMED S Home NIV Solutions S9 VPAP ST-A with ivaps S9 VPAP ST Why choose average when you can choose intelligent? Now you can provide intelligent air through ResMed s intelligent Volume-Assured
INTRODUCING RESMED S Home NIV Solutions S9 VPAP ST-A with ivaps S9 VPAP ST Why choose average when you can choose intelligent? Now you can provide intelligent air through ResMed s intelligent Volume-Assured
3100B Clinical Training Program. 3100B HFOV VIASYS Healthcare
 3100B Clinical Training Program 3100B HFOV VIASYS Healthcare HFOV at Alveolar Level Nieman,, G, SUNY 1999 Who DO We Treat? Only Pathology studied to date has been ARDS Questions about management of adults
3100B Clinical Training Program 3100B HFOV VIASYS Healthcare HFOV at Alveolar Level Nieman,, G, SUNY 1999 Who DO We Treat? Only Pathology studied to date has been ARDS Questions about management of adults
How To Treat A Patient With A Lung Condition
 NHS FORTH VALLEY BIPAP Guideline Date of First Issue 27 / 10 / 2010 Approved 27 / 10 / 2010 Current Issue Date 27 / 10 / 2010 Review Date 27 / 10 / 2012 Version Version 1.00 EQIA Yes 27 / 10 / 2010 Author
NHS FORTH VALLEY BIPAP Guideline Date of First Issue 27 / 10 / 2010 Approved 27 / 10 / 2010 Current Issue Date 27 / 10 / 2010 Review Date 27 / 10 / 2012 Version Version 1.00 EQIA Yes 27 / 10 / 2010 Author
POCKET GUIDE. NAVA and NIV NAVA in neonatal settings
 POCKET GUIDE NAVA and NIV NAVA in neonatal settings Table of contents EMPTY 1 2 3 4 Introduction and background facts Invasive ventilation with NAVA Non invasive ventilation with NAVA NAVA and NIV NAVA
POCKET GUIDE NAVA and NIV NAVA in neonatal settings Table of contents EMPTY 1 2 3 4 Introduction and background facts Invasive ventilation with NAVA Non invasive ventilation with NAVA NAVA and NIV NAVA
High Impact Intervention Care bundle to reduce ventilation-association pneumonia
 High Impact Intervention Care bundle to reduce ventilation-association pneumonia Aim To reduce the incidence of ventilation-associated pneumonia (VAP). Context The aim of the care bundle, as set out in
High Impact Intervention Care bundle to reduce ventilation-association pneumonia Aim To reduce the incidence of ventilation-associated pneumonia (VAP). Context The aim of the care bundle, as set out in
MECHANICAL VENTILATION
 MECHANICAL VENTILATION INDICATIONS: Respiratory Failure Cardiopulmonary arrest Trauma (especially head, neck, and chest) Cardiovascular impairment (strokes, tumors, infection, emboli, trauma) Neurological
MECHANICAL VENTILATION INDICATIONS: Respiratory Failure Cardiopulmonary arrest Trauma (especially head, neck, and chest) Cardiovascular impairment (strokes, tumors, infection, emboli, trauma) Neurological
NORTH WALES CRITICAL CARE NETWORK
 NORTH WALES CRITICAL CARE NETWORK LEVELS OF CRITICAL CARE FOR ADULT PATIENTS Throughout the work of the North Wales Critical Care Network reference to Levels of Care for the critically ill are frequently
NORTH WALES CRITICAL CARE NETWORK LEVELS OF CRITICAL CARE FOR ADULT PATIENTS Throughout the work of the North Wales Critical Care Network reference to Levels of Care for the critically ill are frequently
Mechanical Ventilators
 University of Washington Academic Medical Center Copyright 2000 Disclaimer Children's Hospital and Regional Medical Center Copyright 2002 Disclaimer Mechanical Ventilators Authors Created 07/31/95 Reviewed
University of Washington Academic Medical Center Copyright 2000 Disclaimer Children's Hospital and Regional Medical Center Copyright 2002 Disclaimer Mechanical Ventilators Authors Created 07/31/95 Reviewed
ETCO2 Monitoring: Riding the Wave! Disclosure 4/11/2013
 ETCO2 Monitoring: Riding the Wave! Debbie Fox, MBA, RRT-NPS, FAARC Director, Respiratory Care Wesley Medical Center Disclosure I have no financial conflicts to disclose. I have participated in focus groups
ETCO2 Monitoring: Riding the Wave! Debbie Fox, MBA, RRT-NPS, FAARC Director, Respiratory Care Wesley Medical Center Disclosure I have no financial conflicts to disclose. I have participated in focus groups
Airway Pressure Release Ventilation (APRV) for the Treatment of Severe Life-Threatening ARDS in a Morbidly Obese Patient
 for the Treatment of Severe Life-Threatening ARDS in a Morbidly Obese Patient") Review Crit Care & Shock (2008) 11 : 132-136 Airway Pressure Release Ventilation (APRV) for the Treatment of Severe Life-Threatening ARDS in a Morbidly Obese Patient Amyn Hirani, Rodrigo Cavallazzi, Anastasia
Review Crit Care & Shock (2008) 11 : 132-136 Airway Pressure Release Ventilation (APRV) for the Treatment of Severe Life-Threatening ARDS in a Morbidly Obese Patient Amyn Hirani, Rodrigo Cavallazzi, Anastasia
Mean Duration (days) ± SD b. n = 587 n = 587
 ± SD b. n = 587 n = 587") Online Table 1. Length of stay in matched cohorts of patients with VA and patients without VA a MS-DRG opulation (Code) ECMO or tracheostomy with mechanical ventilation 96 hours or principal diagnosis
Online Table 1. Length of stay in matched cohorts of patients with VA and patients without VA a MS-DRG opulation (Code) ECMO or tracheostomy with mechanical ventilation 96 hours or principal diagnosis
SARASOTA MEMORIAL HOSPITAL DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL DEPARTMENT POLICY TITLE: NON-INVASIVE POSITIVE PRESSURE (NPPV) VENTILATION (CPAP/BIPAP) Job Title of Reviewer: EFFECTIVE DATE: REVISED DATE: POLICY TYPE: Director, Respiratory
PS1006 SARASOTA MEMORIAL HOSPITAL DEPARTMENT POLICY TITLE: NON-INVASIVE POSITIVE PRESSURE (NPPV) VENTILATION (CPAP/BIPAP) Job Title of Reviewer: EFFECTIVE DATE: REVISED DATE: POLICY TYPE: Director, Respiratory
Introduction Hypothesis Methods Results Conclusions Figure 11-1: Format for scientific abstract preparation
 ABSTRACT AND MANUSCRIPT PREPARATION / 69 CHAPTER ELEVEN ABSTRACT AND MANUSCRIPT PREPARATION Once data analysis is complete, the natural progression of medical research is to publish the conclusions of
ABSTRACT AND MANUSCRIPT PREPARATION / 69 CHAPTER ELEVEN ABSTRACT AND MANUSCRIPT PREPARATION Once data analysis is complete, the natural progression of medical research is to publish the conclusions of
Ruchika D. Husa, MD, MS Assistant t Professor of Medicine in the Division of Cardiology The Ohio State University Wexner Medical Center
 Modified Early Warning Score (MEWS) Ruchika D. Husa, MD, MS Assistant t Professor of Medicine i in the Division of Cardiology The Ohio State University Wexner Medical Center MEWS Simple physiological scoring
Modified Early Warning Score (MEWS) Ruchika D. Husa, MD, MS Assistant t Professor of Medicine i in the Division of Cardiology The Ohio State University Wexner Medical Center MEWS Simple physiological scoring
Perioperative Management of Patients with Obstructive Sleep Apnea. Kalpesh Ganatra,MD Diplomate, American Board of Sleep Medicine
 Perioperative Management of Patients with Obstructive Sleep Apnea Kalpesh Ganatra,MD Diplomate, American Board of Sleep Medicine Disclosures. This activity is supported by an education grant from Trivalley
Perioperative Management of Patients with Obstructive Sleep Apnea Kalpesh Ganatra,MD Diplomate, American Board of Sleep Medicine Disclosures. This activity is supported by an education grant from Trivalley
CHEST VOLUME 120 / NUMBER 6 / DECEMBER, 2001 Supplement
 CHEST VOLUME 120 / NUMBER 6 / DECEMBER, 2001 Supplement Section I: Guidelines Evidence-Based Guidelines for Weaning and Discontinuing Ventilatory Support* A Collective Task Force Facilitated by the American
CHEST VOLUME 120 / NUMBER 6 / DECEMBER, 2001 Supplement Section I: Guidelines Evidence-Based Guidelines for Weaning and Discontinuing Ventilatory Support* A Collective Task Force Facilitated by the American
INTERDISCIPLINARY CLINICAL MANUAL Policy/ Procedure
 INTERDISCIPLINARY CLINICAL MANUAL Policy/ Procedure TITLE: Non Invasive Positive NUMBER: CC 45-072 Pressure Ventilation Date Issued: October 2011 Page 1 of 13 Applies To: Respiratory Therapy and Nursing
INTERDISCIPLINARY CLINICAL MANUAL Policy/ Procedure TITLE: Non Invasive Positive NUMBER: CC 45-072 Pressure Ventilation Date Issued: October 2011 Page 1 of 13 Applies To: Respiratory Therapy and Nursing
For every breath he takes. Trilogy200 ventilator s added sensitivity lets you breathe easier knowing your patients are where they belong home.
 For every breath he takes Trilogy200 ventilator s added sensitivity lets you breathe easier knowing your patients are where they belong home. Sensitive to your patients needs Trilogy200, a portable life-support
For every breath he takes Trilogy200 ventilator s added sensitivity lets you breathe easier knowing your patients are where they belong home. Sensitive to your patients needs Trilogy200, a portable life-support
Critical Care Therapy and Respiratory Care Section
 Critical Care Therapy and Respiratory Care Section Category: Clinical Section: Special Procedures Title: Transport of Critically Ill Patients Policy #: 05 Revised: 04/00 1.0 DESCRIPTION 1.1 Definition:
Critical Care Therapy and Respiratory Care Section Category: Clinical Section: Special Procedures Title: Transport of Critically Ill Patients Policy #: 05 Revised: 04/00 1.0 DESCRIPTION 1.1 Definition:
Titration protocol reference guide
 Titration protocol reference guide Description Page Titration protocol goals 4 CPAP protocol CPAP protocol 6 CPAP titration protocol 7 CPAP reimbursement criteria 8 BiPAP S protocol BiPAP S protocol 10
Titration protocol reference guide Description Page Titration protocol goals 4 CPAP protocol CPAP protocol 6 CPAP titration protocol 7 CPAP reimbursement criteria 8 BiPAP S protocol BiPAP S protocol 10
Guidelines for Standards of Care for Patients with Acute Respiratory Failure on Mechanical Ventilatory Support
 Guidelines for Standards of Care for Patients with Acute Respiratory Failure on Mechanical Ventilatory Support Copyright by the SOCIETY OF CRITICAL CARE MEDICINE These guidelines can also be found in the
Guidelines for Standards of Care for Patients with Acute Respiratory Failure on Mechanical Ventilatory Support Copyright by the SOCIETY OF CRITICAL CARE MEDICINE These guidelines can also be found in the
Benjamin M. Marlin Department of Computer Science University of Massachusetts Amherst [email protected] January 21, 2011
 Modeling and Prediction With ICU Electronic Health Records Data Department of Computer Science University of Massachusetts Amherst [email protected] January 21, 2011 The Big Picture: History of Medical
Modeling and Prediction With ICU Electronic Health Records Data Department of Computer Science University of Massachusetts Amherst [email protected] January 21, 2011 The Big Picture: History of Medical
Nurses and Respiratory Therapists Working Together for Safe Alarm Systems Management
 Nurses and Respiratory Therapists Working Together for Safe Alarm Systems Management May 11, 2015 9/25/2013 1 AAMI Foundation Vision: To drive the safe adoption and use of healthcare technology Visit our
Nurses and Respiratory Therapists Working Together for Safe Alarm Systems Management May 11, 2015 9/25/2013 1 AAMI Foundation Vision: To drive the safe adoption and use of healthcare technology Visit our
Long Term Acute Care Hospital: Criteria for Admission
 Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. M issouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. M issouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
D-370-2010. Non-Invasive Ventilation (NIV) with the Oxylog 2000 plus and Oxylog 3000 plus
 with the Oxylog 2000 plus and Oxylog 3000 plus") D-370-2010 Non-Invasive Ventilation (NIV) with the Oxylog 2000 plus and Oxylog 3000 plus 02 NON INVASIVE VENTILATION WARNING This booklet is not a substitute for the Instructions for Use of the Oxylog
D-370-2010 Non-Invasive Ventilation (NIV) with the Oxylog 2000 plus and Oxylog 3000 plus 02 NON INVASIVE VENTILATION WARNING This booklet is not a substitute for the Instructions for Use of the Oxylog
PULMONARY PHYSIOLOGY
 I. Lung volumes PULMONARY PHYSIOLOGY American College of Surgeons SCC Review Course Christopher P. Michetti, MD, FACS and Forrest O. Moore, MD, FACS A. Tidal volume (TV) is the volume of air entering and
I. Lung volumes PULMONARY PHYSIOLOGY American College of Surgeons SCC Review Course Christopher P. Michetti, MD, FACS and Forrest O. Moore, MD, FACS A. Tidal volume (TV) is the volume of air entering and
NIV in non CPE, non-copd, non-neuromuscular patients
 NIV in non CPE, non-copd, non-neuromuscular patients Giorgio Iotti Anestesia e Rianimazione 2 Pavia Italia Missioni ECMOteam Pavia 2009/2011 18 4 2 Trasporto con ECMO senza ECMO ALI/ARDS Immunocompetent
NIV in non CPE, non-copd, non-neuromuscular patients Giorgio Iotti Anestesia e Rianimazione 2 Pavia Italia Missioni ECMOteam Pavia 2009/2011 18 4 2 Trasporto con ECMO senza ECMO ALI/ARDS Immunocompetent
DATA SHEET. Capnography option. www.airliquidemedicalsystems.com. November 2013 V2.2
 November 2013 V2.2 DATA SHEET www.airliquidemedicalsystems.com [1] Monnal T75 (CO 2 )/ Air Liquide Medical Systems APPLICATION AREA OPERATING CONDITIONS Application: Patient categories: Weight: Intensive
November 2013 V2.2 DATA SHEET www.airliquidemedicalsystems.com [1] Monnal T75 (CO 2 )/ Air Liquide Medical Systems APPLICATION AREA OPERATING CONDITIONS Application: Patient categories: Weight: Intensive
Implementation of a high volume, complex clinical pathway for cardiothoracic surgery patients in the intensive care unit.
 Implementation of a high volume, complex clinical pathway for cardiothoracic surgery patients in the intensive care unit. Marion van der Kolk Surgeon/Intensivist UMC St Radboud, Nijmegen The Netherlands
Implementation of a high volume, complex clinical pathway for cardiothoracic surgery patients in the intensive care unit. Marion van der Kolk Surgeon/Intensivist UMC St Radboud, Nijmegen The Netherlands
DRG 475 Respiratory System Diagnosis with Ventilator Support. ICD-9-CM Coding Guidelines
 DRG 475 Respiratory System Diagnosis with Ventilator Support ICD-9-CM Coding G The below listed g are not inclusive. The coder should refer to the applicable Coding Clinic g for additional information.
DRG 475 Respiratory System Diagnosis with Ventilator Support ICD-9-CM Coding G The below listed g are not inclusive. The coder should refer to the applicable Coding Clinic g for additional information.
Pain Management in the Critically ill Patient
 Pain Management in the Critically ill Patient Jim Ducharme MD CM, FRCP President-Elect, IFEM Clinical Professor of Medicine, McMaster University Adjunct Professor of Family Medicine, Queens University
Pain Management in the Critically ill Patient Jim Ducharme MD CM, FRCP President-Elect, IFEM Clinical Professor of Medicine, McMaster University Adjunct Professor of Family Medicine, Queens University
High-Frequency Oscillatory Ventilation
 High-Frequency Oscillatory Ventilation Arthur Jones EdD, RRT Learning Objectives Describe the indications and rationale and monitoring for HFOV. Identify HFOV settings and describe the effects of their
High-Frequency Oscillatory Ventilation Arthur Jones EdD, RRT Learning Objectives Describe the indications and rationale and monitoring for HFOV. Identify HFOV settings and describe the effects of their
Extracorporeal Life Support Organization (ELSO) Guidelines for Neonatal Respiratory Failure
 Guidelines for Neonatal Respiratory Failure") Extracorporeal Life Support Organization (ELSO) Guidelines for Neonatal Respiratory Failure Introduction This neonatal respiratory failure guideline is a supplement to ELSO s General Guidelines for all
Extracorporeal Life Support Organization (ELSO) Guidelines for Neonatal Respiratory Failure Introduction This neonatal respiratory failure guideline is a supplement to ELSO s General Guidelines for all
Non-invasive ventilation in acute respiratory failure
 192 BTS GUIDELINE Non-invasive ventilation in acute respiratory failure British Thoracic Society Standards of Care Committee... Thorax 2002;57:192 211 Members of BTS Standards of Care Committee: S Baudouin,
192 BTS GUIDELINE Non-invasive ventilation in acute respiratory failure British Thoracic Society Standards of Care Committee... Thorax 2002;57:192 211 Members of BTS Standards of Care Committee: S Baudouin,
Rehabilitation and Lung Cancer Resection. Roberto Benzo MD MS Mindful Breathing Laboratory Division of Pulmonary & CCM Mayo Clinic
 Rehabilitation and Lung Cancer Resection Roberto Benzo MD MS Mindful Breathing Laboratory Division of Pulmonary & CCM Mayo Clinic Disclosure Funded by the National Cancer Institute NIH for Preoperative
Rehabilitation and Lung Cancer Resection Roberto Benzo MD MS Mindful Breathing Laboratory Division of Pulmonary & CCM Mayo Clinic Disclosure Funded by the National Cancer Institute NIH for Preoperative
The Berlin definition of Severe ARDS includes assessment of which of the following?
 2013 ACS Critical Care Update ARDS, Ventilators MCQs August, 2013 (Berlin Definition of ARDS Question 1) The Berlin definition of Severe ARDS includes assessment of which of the following? A. Oxygenation:
2013 ACS Critical Care Update ARDS, Ventilators MCQs August, 2013 (Berlin Definition of ARDS Question 1) The Berlin definition of Severe ARDS includes assessment of which of the following? A. Oxygenation:
Weaning of the Patient with ARDS
 Weaning of the Patient with ARDS William E. Hurford, MD Associate Professor of Anesthesia Harvard Medical School Director, Critical Care Department of Anesthesia and Critical Care Massachusetts General
Weaning of the Patient with ARDS William E. Hurford, MD Associate Professor of Anesthesia Harvard Medical School Director, Critical Care Department of Anesthesia and Critical Care Massachusetts General
ESCMID Online Lecture Library. by author
 Do statins improve outcomes of patients with sepsis and pneumonia? Jordi Carratalà Department of Infectious Diseases Statins for sepsis & community-acquired pneumonia Sepsis and CAP are major healthcare
Do statins improve outcomes of patients with sepsis and pneumonia? Jordi Carratalà Department of Infectious Diseases Statins for sepsis & community-acquired pneumonia Sepsis and CAP are major healthcare
VENTILATION SERVO-s EASY AND RELIABLE PATIENT CARE
 VENTILATION SERVO-s EASY AND RELIABLE PATIENT CARE Critical Care SERVO-s 3 SERVO-s SIMPLY MAKES SENSE MAQUET THE GOLD STANDARD Leading the way: MAQUET is a premier international provider of medical products
VENTILATION SERVO-s EASY AND RELIABLE PATIENT CARE Critical Care SERVO-s 3 SERVO-s SIMPLY MAKES SENSE MAQUET THE GOLD STANDARD Leading the way: MAQUET is a premier international provider of medical products
Subject: Severe Sepsis/Septic Shock Published Date: August 9, 2013 Scope: Hospital Wide Original Creation Date: August 9, 2013
 Stony Brook Medicine Severe Sepsis/Septic Shock Recognition and Treatment Protocols Subject: Severe Sepsis/Septic Shock Published Date: August 9, 2013 Scope: Hospital Wide Original Creation Date: August
Stony Brook Medicine Severe Sepsis/Septic Shock Recognition and Treatment Protocols Subject: Severe Sepsis/Septic Shock Published Date: August 9, 2013 Scope: Hospital Wide Original Creation Date: August
Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi
 Clinical Sessions 2011 By Bhavin Doshi") Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi What is EWS? After qualifying, junior doctors are expected to distinguish between the moderately sick patients who can be managed in the
Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi What is EWS? After qualifying, junior doctors are expected to distinguish between the moderately sick patients who can be managed in the
Oxygenation. Chapter 21. Anatomy and Physiology of Breathing. Anatomy and Physiology of Breathing*
 Oxygenation Chapter 21 Anatomy and Physiology of Breathing Inspiration ~ breathing in Expiration ~ breathing out Ventilation ~ Movement of air in & out of the lungs Respiration ~ exchange of O2 & carbon
Oxygenation Chapter 21 Anatomy and Physiology of Breathing Inspiration ~ breathing in Expiration ~ breathing out Ventilation ~ Movement of air in & out of the lungs Respiration ~ exchange of O2 & carbon
Comparison of the Rate of Improvement in Gas Exchange between Two High Frequency Ventilators in a Newborn Piglet Lung Injury Model
 Comparison of the Rate of Improvement in Gas Exchange between Two High Frequency Ventilators in a Newborn Piglet Lung Injury Model Kurt Gillette, MD, San Antonio Military Medical Center Background: High
Comparison of the Rate of Improvement in Gas Exchange between Two High Frequency Ventilators in a Newborn Piglet Lung Injury Model Kurt Gillette, MD, San Antonio Military Medical Center Background: High
MECHANICAL VENTILATION IN THE NEONATE
 Supplemental Resources for the PICU/NICU MECHANICAL VENTILATION IN THE NEONATE I. GENERAL PRINCIPLES A. NEONATAL VENTILATORS We use three types of neonatal ventilators in the NICU: 1. SIMV (Synchronized
Supplemental Resources for the PICU/NICU MECHANICAL VENTILATION IN THE NEONATE I. GENERAL PRINCIPLES A. NEONATAL VENTILATORS We use three types of neonatal ventilators in the NICU: 1. SIMV (Synchronized
MODULE. POSITIVE AIRWAY PRESSURE (PAP) Titrations
 Titrations") MODULE POSITIVE AIRWAY PRESSURE (PAP) Titrations POSITIVE AIRWAY PRESSURE (PAP) TITRATIONS OBJECTIVES At the end of this module the student must be able to: Identify the standards of practice for administering
MODULE POSITIVE AIRWAY PRESSURE (PAP) Titrations POSITIVE AIRWAY PRESSURE (PAP) TITRATIONS OBJECTIVES At the end of this module the student must be able to: Identify the standards of practice for administering
Edwards FloTrac Sensor & Edwards Vigileo Monitor. Understanding Stroke Volume Variation and Its Clinical Application
 Edwards FloTrac Sensor & Edwards Vigileo Monitor Understanding Stroke Volume Variation and Its Clinical Application 1 Topics System Configuration Pulsus Paradoxes Reversed Pulsus Paradoxus What is Stroke
Edwards FloTrac Sensor & Edwards Vigileo Monitor Understanding Stroke Volume Variation and Its Clinical Application 1 Topics System Configuration Pulsus Paradoxes Reversed Pulsus Paradoxus What is Stroke
DISCHARGE CRITERIA FOR PHASE I & II- POST ANESTHESIA CARE
 REFERENCES: The Joint Commission Accreditation Manual for Hospitals American Society of Post Anesthesia Nurses: Standards of Post Anesthesia Nursing Practice (1991, 2002). RELATED DOCUMENTS: SHC Administrative
REFERENCES: The Joint Commission Accreditation Manual for Hospitals American Society of Post Anesthesia Nurses: Standards of Post Anesthesia Nursing Practice (1991, 2002). RELATED DOCUMENTS: SHC Administrative
5/30/2014 OBJECTIVES THE ROLE OF A RESPIRATORY THERAPIST IN THE DELIVERY ROOM. Disclosure
 THE ROLE OF A RESPIRATORY THERAPIST IN THE DELIVERY ROOM Ona Fofah, MD FAAP Assistant Professor of Pediatrics Director, Division of Neonatology Department of Pediatrics Rutgers- NJMS, Newark OBJECTIVES
THE ROLE OF A RESPIRATORY THERAPIST IN THE DELIVERY ROOM Ona Fofah, MD FAAP Assistant Professor of Pediatrics Director, Division of Neonatology Department of Pediatrics Rutgers- NJMS, Newark OBJECTIVES
NON-INVASIVE VENTILATION. Jason C. Brainard, MD Assistant Professor Department of Anesthesiology
 NON-INVASIVE VENTILATION Jason C. Brainard, MD Assistant Professor Department of Anesthesiology Objectives Overview of Non-Invasive Ventilation Discuss Specific Indications for Non-Invasive Ventilation
NON-INVASIVE VENTILATION Jason C. Brainard, MD Assistant Professor Department of Anesthesiology Objectives Overview of Non-Invasive Ventilation Discuss Specific Indications for Non-Invasive Ventilation
AT HOME DR. D. K. PILLAI MUG @ UOM
 NON - INVASIVE VENTILATION AT HOME DR. D. K. PILLAI 07.09.2011 MUG @ UOM In the beginning came. OSA (HS) 1. CPAP for OSAHS (Obstructive Sleep Apnoea Hypopnoea Syndrome) 2 NIPPV 2. NIPPV (Non
NON - INVASIVE VENTILATION AT HOME DR. D. K. PILLAI 07.09.2011 MUG @ UOM In the beginning came. OSA (HS) 1. CPAP for OSAHS (Obstructive Sleep Apnoea Hypopnoea Syndrome) 2 NIPPV 2. NIPPV (Non
La Ventilazione non-invasiva: questioni aperte... Andrea Bellone UOC di Pronto Soccorso-OBI-Medicina per Acuti Azienda Ospedaliera Sant'Anna Como
 La Ventilazione non-invasiva: questioni aperte... Andrea Bellone UOC di Pronto Soccorso-OBI-Medicina per Acuti Azienda Ospedaliera Sant'Anna Como Ruolo del medico di PS 1) Diagnostica differenziale 2)
La Ventilazione non-invasiva: questioni aperte... Andrea Bellone UOC di Pronto Soccorso-OBI-Medicina per Acuti Azienda Ospedaliera Sant'Anna Como Ruolo del medico di PS 1) Diagnostica differenziale 2)
Postoperative management in adults
 Scottish Intercollegiate Guidelines Net work 77 Postoperative management in adults A practical guide to postoperative care for clinical staff 1 Introduction 1 2 Clinical assessment and monitoring 3 3 Cardiovascular
Scottish Intercollegiate Guidelines Net work 77 Postoperative management in adults A practical guide to postoperative care for clinical staff 1 Introduction 1 2 Clinical assessment and monitoring 3 3 Cardiovascular
Oxygenation and Oxygen Therapy Michael Billow, D.O.
 Oxygenation and Oxygen Therapy Michael Billow, D.O. The delivery of oxygen to all body tissues is the essence of critical care. Patients in respiratory distress/failure come easily to mind as the ones
Oxygenation and Oxygen Therapy Michael Billow, D.O. The delivery of oxygen to all body tissues is the essence of critical care. Patients in respiratory distress/failure come easily to mind as the ones
CENTER FOR DRUG EVALUATION AND RESEARCH
 CENTER FOR DRUG EVALUATION AND RESEARCH APPLICATION NUMBER: 205029Orig1s000 SUMMARY REVIEW Cross Discipline Team Leader Review 4. Nonclinical Pharmacology/Toxicology In their review of the original application,
CENTER FOR DRUG EVALUATION AND RESEARCH APPLICATION NUMBER: 205029Orig1s000 SUMMARY REVIEW Cross Discipline Team Leader Review 4. Nonclinical Pharmacology/Toxicology In their review of the original application,
Critical Care Therapy and Respiratory Care Section
 Category: Section: Title: Critical Care Therapy and Respiratory Care Section Policy #: 03 Revised: 5/02 1.0 DESCRIPTION Clinical Ventilator Management Invasive and Noninvasive Positive Pressure Ventilation
Category: Section: Title: Critical Care Therapy and Respiratory Care Section Policy #: 03 Revised: 5/02 1.0 DESCRIPTION Clinical Ventilator Management Invasive and Noninvasive Positive Pressure Ventilation
Trilogy200. Proximal pressure line. Exhalation valve line. Quick start guide. Overview. Circuit set-up. Set-up screen. Prescription set-up
 Trilogy200 Proximal pressure line Exhalation valve line Quick start guide 1 2 3 4 Overview Circuit set-up Set-up screen Prescription set-up 1 Overview 4 Porting block Detachable battery Air inlet and grey
Trilogy200 Proximal pressure line Exhalation valve line Quick start guide 1 2 3 4 Overview Circuit set-up Set-up screen Prescription set-up 1 Overview 4 Porting block Detachable battery Air inlet and grey
AVAPS-AE Auto-titration Mode of Noninvasive Ventilation. Monique Hom Sr. Clinical Education Manager HHS
 AVAPS-AE Auto-titration Mode of Noninvasive Ventilation Monique Hom Sr. Clinical Education Manager HHS AVAPS-AE: Why do we need it? 3 AVAPS-AE AVAPS-AE is an Auto-titration Mode of Noninvasive ventilation
AVAPS-AE Auto-titration Mode of Noninvasive Ventilation Monique Hom Sr. Clinical Education Manager HHS AVAPS-AE: Why do we need it? 3 AVAPS-AE AVAPS-AE is an Auto-titration Mode of Noninvasive ventilation
Boaray 700 Anesthesia Machine
 Boaray 700 Anesthesia Machine Features CE certification. 15 inch colored LCD, touch screen setting, big font display, free changeable angles of views. Various ventilation modes - VCV, PCV, SIMV+VCV, SIMV+PCV.
Boaray 700 Anesthesia Machine Features CE certification. 15 inch colored LCD, touch screen setting, big font display, free changeable angles of views. Various ventilation modes - VCV, PCV, SIMV+VCV, SIMV+PCV.
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) S. Agarwal, MD, S. Kache MD
 S. Agarwal, MD, S. Kache MD") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) S. Agarwal, MD, S. Kache MD Definition ARDS is a clinical syndrome of lung injury with hypoxic respiratory failure caused by intense pulmonary inflammation that
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) S. Agarwal, MD, S. Kache MD Definition ARDS is a clinical syndrome of lung injury with hypoxic respiratory failure caused by intense pulmonary inflammation that
Title/Description: Admission Criteria, Discharge Criteria, and Standards of Operation of the Pediatric Intensive Care Unit.
 University of Kentucky / UK HealthCare Policy and Procedure Policy # CH02-02 Title/Description: Admission Criteria, Discharge Criteria, and Standards of Operation of the Pediatric Intensive Care Unit.
University of Kentucky / UK HealthCare Policy and Procedure Policy # CH02-02 Title/Description: Admission Criteria, Discharge Criteria, and Standards of Operation of the Pediatric Intensive Care Unit.
Principles of Mechanical Ventilation
 Principles of Mechanical Ventilation The Basics Presented by WANG, Tzong-Luen Professor, Medical School, FJU Director, ED, SKH President, SECCM, Taiwan Origins of mechanical ventilation The era of intensive
Principles of Mechanical Ventilation The Basics Presented by WANG, Tzong-Luen Professor, Medical School, FJU Director, ED, SKH President, SECCM, Taiwan Origins of mechanical ventilation The era of intensive
Fisiología Respiratoria, Hipercapnia Permisiva e Injuria Pulmonar. Wally A. Carlo, M.D. University of Alabama at Birmingham
 Fisiología Respiratoria, Hipercapnia Permisiva e Injuria Pulmonar Wally A. Carlo, M.D. University of Alabama at Birmingham Randomized Trial of Oxygen Saturation Targets in Premature Infants - the SUPPORT
Fisiología Respiratoria, Hipercapnia Permisiva e Injuria Pulmonar Wally A. Carlo, M.D. University of Alabama at Birmingham Randomized Trial of Oxygen Saturation Targets in Premature Infants - the SUPPORT
Paediatric Advanced Warning Score (PAWS)
") Paediatric Advanced Warning Score (PAWS) Prevention is better than cure. Spectrum of critical illness Ward level care HDU Care ICU Care Early admission may improve outcome ICU Outreach teams Medical Emergency
Paediatric Advanced Warning Score (PAWS) Prevention is better than cure. Spectrum of critical illness Ward level care HDU Care ICU Care Early admission may improve outcome ICU Outreach teams Medical Emergency
Evidence-Based Ventilator Weaning and Discontinuation
 Evidence-Based Ventilator Weaning and Discontinuation Neil R MacIntyre MD FAARC Introduction Assessing Ventilator-Discontinuation Potential Extubation Managing the Patient Who Fails SBT Protocols Implemented
Evidence-Based Ventilator Weaning and Discontinuation Neil R MacIntyre MD FAARC Introduction Assessing Ventilator-Discontinuation Potential Extubation Managing the Patient Who Fails SBT Protocols Implemented