Postoperative management in adults
|
|
|
- Candace Chambers
- 10 years ago
- Views:
Transcription
1 Scottish Intercollegiate Guidelines Net work 77 Postoperative management in adults A practical guide to postoperative care for clinical staff 1 Introduction 1 2 Clinical assessment and monitoring 3 3 Cardiovascular management 11 4 Respiratory management 20 5 Fluid, electrolyte and renal management 28 6 Management of sepsis 34 7 Postoperative nutrition 39 8 Information for discussion with patients and carers 44 9 Development of the guideline 45 Abbreviations 48 Annexes 49 References 52 August 2004 COPIES OF ALL SIGN GUIDELINES ARE AVAILABLE BY CALLING OR ONLINE AT

2 KEY TO CONSENSUS AND EVIDENCE STATEMENTS CONSENSUS STATEMENTS CS Statements developed from structured discussion, informed by any existing evidence and the group s clinical experience, and validated using a formal scoring system. LEVELS OF EVIDENCE 1 ++ High quality meta-analyses, systematic reviews of randomised controlled trials (RCTs), or RCTs with a very low risk of bias 1 + Well conducted meta-analyses, systematic reviews of RCTs, or RCTs with a low risk of bias 1 - Meta-analyses, systematic reviews of RCTs, or RCTs with a high risk of bias 2 ++ High quality systematic reviews of case control or cohort studies High quality case control or cohort studies with a very low risk of confounding or bias and a high probability that the relationship is causal 2 + Well conducted case control or cohort studies with a low risk of confounding or bias and a moderate probability that the relationship is causal 2 - Case control or cohort studies with a high risk of confounding or bias and a significant risk that the relationship is not causal 3 Non-analytic studies, eg case reports, case series 4 Expert opinion GRADES OF RECOMMENDATION Note: The grade of recommendation relates to the strength of the evidence on which the recommendation is based. It does not reflect the clinical importance of the recommendation. A At least one meta-analysis, systematic review of RCTs, or RCT rated as 1 ++ and directly applicable to the target population; or A body of evidence consisting principally of studies rated as 1 +, directly applicable to the target population, and demonstrating overall consistency of results B A body of evidence including studies rated as 2 ++, directly applicable to the target population, and demonstrating overall consistency of results; or Extrapolated evidence from studies rated as 1 ++ or 1 + C A body of evidence including studies rated as 2 +, directly applicable to the target population and demonstrating overall consistency of results; or Extrapolated evidence from studies rated as 2 ++ D Evidence level 3 or 4; or Extrapolated evidence from studies rated as 2 + Scottish Intercollegiate Guidelines Network ISBN First published 2004 SIGN consents to the pho to cop y ing of this guideline for the purpose of implementation in NHSScotland Scottish Intercollegiate Guidelines Network Royal College of Physicians 9 Queen Street, Edinburgh EH2 1JQ SIGN IS FUNDED BY NHS QUALITY IMPROVEMENT SCOTLAND

3

4

5

6
7
8

9

10

11

12

13

14
15

16

17

18

19

20

21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53 DATE Postoperative Monitoring Chart Name Hosp. Number DOB Weight Consultant TIME TEMPERATURE BLOOD 190 PRESSURE ADMISSION 160 BP Plus 30% Less 30% CVP HEART RATE SaO2 FiO2 (l/min or %) Example RESP. RATE URINE Volume NEUROLOGICAL STATE >0.5mls/kg <0.5mls/kg AWAKE VERBAL PAIN UNRESP Pain score BM DR CALLED
54
55
56
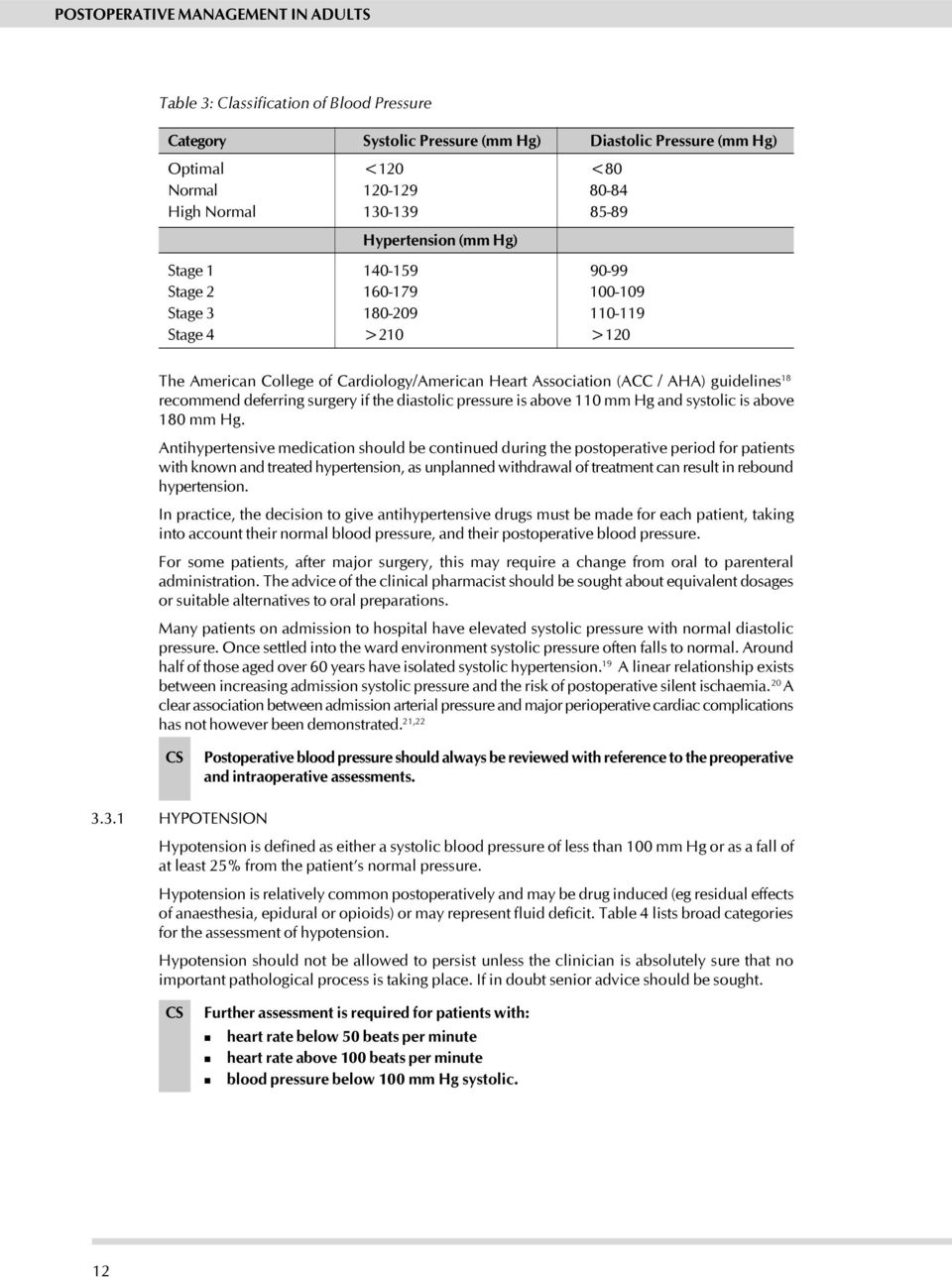
57 RESPIRATORY MANAGEMENT Patients in whom there is a suspicion of postoperative pulmonary complications should have an arterial blood gas analysis, a sputum culture and ECG. Chest X-ray should be performed on suspicion of major collapse, effusions, pneumothorax or haemothorax. Other investigations should be used only if there are specific indications. Oxygen should be given to patients with hypoxaemia using a device that is best tolerated to achieve the necessary SpO 2. In normally hydrated patients humidification is unnecessary. Failure to maintain an SpO 2 >90% or PaO 2 >8.0 kpa is an indication to consider assisted ventilation. Patients developing respiratory failure should be referred to a critical care specialist to be assessed for possible assisted ventilation. The referral should be timely as hypoxia or hypercapnia may lead rapidly to cardiorespiratory arrest. Diagnosis of respiratory infection Any two of the following on two or more days: Pyrexia >38 0 C Positive sputum culture Positive clinical findings Abnormal chest X-ray Atelectasis/infiltrates CARDIOVASCULAR MANAGEMENT ASSESSMENT OF HYPOTENSION Observe if: Seek further advice if: Awake or easily rousable Drowsy or unrousable Comfortable Distressed Normal preoperative BP Hypertensive preoperatively Warm Cold Well perfused (capillary refill <2 seconds) Capillary refill > 2 seconds Heart rate bpm Heart rate >100 or <50 bpm Passing urine (>0.5 ml/kg/hr) Oliguric (<0.5 ml/kg/hr) No obvious bleeding Signs of bleeding (drains, wounds, haematoma) CARDIOVASCULAR MANAGEMENT (Contd.) Postoperative blood pressure should always be reviewed with reference to the preoperative and intraoperative assessments Further assessment is required for patients with: heart rate < 50 and > 100 bpm blood pressure <100 mm Hg systolic. Patients on regular antihypertensive medication should normally be maintained on this medication perioperatively. If the patient becomes hypotensive then it may be appropriate to discontinue some drugs. Beta blockers and IV nitrates may be used safely and effectively in postoperative hypertension. Beta blockers should be continued perioperatively in patients previously taking these drugs for coronary disease, congestive heart failure, hypertension or arrhythmias. Be aware of clinical factors which increase risk to the patient and how these interact with the risks imposed by the surgical procedure. Seek expert help early in the management of serious or potentially serious arrhythmias. Reconsider the level of care. Search for the underlying causes of any supraventricular arrhythmias, eg hypoxia, hypovolaemia, electrolyte abnormality, sepsis or drug toxicity. Where perioperative MI is diagnosed or suspected early specialist medical advice should be sought. Maintain normothermia in the postoperative period. FLUID, ELECTROLYTE & RENAL MANAGEMENT Accurate assessment of fluid and electrolyte status can be difficult and the treatment of a particular patient must be individualised and reviewed frequently in the light of the response to treatment. Volume depletion should be avoided as this can lead to poor perfusion and problems such as anastomotic breakdown, cerebral damage, renal failure and multiple organ failure. Diuretics should not be used to treat oliguria and should be reserved for fluid overload. Hyponatraemia is more commonly due to excess water than sodium deficiency assess volume status. Hypernatraemia most commonly indicates a total body deficiency of water and is an indication for prompt assessment and intervention, especially when levels exceed 155 mmol/l. Hypokalaemia can delay postoperative recovery - magnesium supplementation may also be required. Hyperkalaemia is a medical emergency obtain senior help. Metabolic acidosis is usually due to poor tissue perfusion but can also be caused by excessive administration of saline. SEPSIS Hand washing with soap and water or with alcoholic cleansing agents should be performed before and after patient contact. Early identification and appropriate treatment of sepsis improves outcome. Urine and blood cultures should be obtained whenever there is reason to suspect systemic sepsis. If the cause of sepsis is unknown, treat with broad spectrum antibiotics, guided by local protocols. Results from microbiological specimens should be reviewed regularly and antibiotics changed as necessary. A course of antimicrobial treatment should generally be limited to 5-7 days. Fungi and atypical organisms can contribute to sepsis syndrome, so take cultures and prescribe appropriately. Systemic inflammatory response syndrome (SIRS) is defined as the presence of 2 or more of the following: temperature >38 0 C or <36 0 C heart rate >90 bpm respiratory rate >20 breaths/min or PaCO 2 <4.3kPa white cell count >12,000 cells/mm 3, <4,000 cells/mm 3 or >10% immature forms. When SIRS is present an infective cause should be sought first. NUTRITION Oral intake should be commenced as soon as possible after surgery. Nutritional replacement should be discussed with a dietitian and tailored to the patient's requirements. Enteral nutrition is the preferred method of postoperative nutritional support and should be used if possible. Nutritional and metabolic status should be assessed regularly and the nutritional prescription modified as necessary. Given the lack of a strong evidence base of effective practice for postoperative management this guideline has been developed using a combination of evidenced based and consensus techniques. Initial systematic searches identified any relevant evidence. The critically appraised evidence, together with the clinical experience of the guideline development group, informed the formal consensus methods that were used to develop recommendations. These are presented in the form of consensus statements.
58 Any change in a monitoring regimen should prompt reassessment of the level of care. The doctor completing the initial postoperative assessment should consider the monitoring regimen and appropriate level of care required for the next 24 hours in collaboration with the nursing team. Following specialist surgery it may be necessary to assess additional factors. Pain and adequacy of pain control The monitoring regimen should be reviewed daily so as best to provide data for clinical decision making. Any significant symptoms eg chest pain, breathlessness Postoperative monitoring should be continued on a daily basis. operation out of hours emergency or high risk surgery Trends in the physiological data, rather than absolute numbers, should be reported to assist in the detection of deteriorating patients before a severe physiological compromise occurs. ASA grade 3 Patients with the following risk factors for deterioration should be reassessed within two hours of the first postoperative assessment: Patients requiring the frequent monitoring of multiple variables should be considered for care at level 2 or above. GCS, oxygen saturation and blood glucose Patients at risk of deterioration require frequent assessment. if confusion is present (AMT) MONITORING If abnormal determine: A postoperative assessment should be carried out when the patient returns from theatre. Patient conscious and normally responsive? (AVPU; Alert, Verbal, Painful, Unresponsive) THE FIRST POSTOPERATIVE ASSESSMENT Drainage from drains, wounds & NG tubes Urine colour and rate of production any specific treatment or prophylaxis required (eg fluids, nutrition, antibiotics, analgesia, anti-emetics, thromboprophylaxis). Jugular venous pressure Conjunctival pallor any specific postoperative instruction concerning possible problems Blood pressure Pulse rate, volume and rhythm any anaesthetic, surgical or intraoperative complications Capillary return <2s or not? Anaesthetic and surgical staff should record the following items in the patient s case notes: Hands - warm or cool, pink or pale? Percussion note DISCHARGE FROM THEATRE AND POSTANAESTHETIC RECOVERY Breath sounds Symmetry of respiration/expansion Trachea central or not? Only accept responsibility appropriate to your training and experience. If in doubt ASK FOR HELP Respiratory rate Effort of breathing/use of accessory muscles Oxygen saturation clinical assessment and monitoring respiratory management cardiovascular management fluid, electrolyte and renal management control of sepsis nutrition Recommended treatment & prophylaxis Postoperative instructions Intraoperative complications Allergies Optimal postoperative care requires: Medications Past medical history PRINCIPLES OF POSTOPERATIVE MANAGEMENT SAMPLE MONITORING REGIMEN FOR FIRST FEW POSTOPERATIVE HOURS CHECKLIST FOR FIRST POSTOPERATIVE ASSESSMENT 77 POSTOPERATIVE MANAGEMENT IN ADULTS: A PRACTICAL GUIDE TO POSTOPERATIVE CARE FOR CLINICAL STAFF
RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND
 RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND Monitor patient on the ward to detect trends in vital signs and to manage accordingly To recognise deteriorating trends and request relevant medical/out
RGN JOY LAUDE WATFORD GENERAL HOSPITAL, ENGLAND Monitor patient on the ward to detect trends in vital signs and to manage accordingly To recognise deteriorating trends and request relevant medical/out
Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi
 Clinical Sessions 2011 By Bhavin Doshi") Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi What is EWS? After qualifying, junior doctors are expected to distinguish between the moderately sick patients who can be managed in the
Early Warning Scores (EWS) Clinical Sessions 2011 By Bhavin Doshi What is EWS? After qualifying, junior doctors are expected to distinguish between the moderately sick patients who can be managed in the
KING FAISAL SPECIALIST HOSPITAL AND RESEARCH CENTRE (GEN. ORG.) NURSING AFFAIRS. Scope of Service PEDIATRIC INTENSIVE CARE UNIT (PICU)
 NURSING AFFAIRS. Scope of Service PEDIATRIC INTENSIVE CARE UNIT (PICU)") PICU-Jan.2012 Page 1 of 7 Number of Beds: 18 Nurse Patient Ratio: 1:1-2 : The Pediatric Intensive Care Unit (PICU) provides 24 hour intensive nursing care for patients aged neonate through adolescence.
PICU-Jan.2012 Page 1 of 7 Number of Beds: 18 Nurse Patient Ratio: 1:1-2 : The Pediatric Intensive Care Unit (PICU) provides 24 hour intensive nursing care for patients aged neonate through adolescence.
Lothian Diabetes Handbook MANAGEMENT OF DIABETIC KETOACIDOSIS
 MANAGEMENT OF DIABETIC KETOACIDOSIS 90 MANAGEMENT OF DIABETIC KETOACIDOSIS Diagnosis elevated plasma and/or urinary ketones metabolic acidosis (raised H + /low serum bicarbonate) Remember that hyperglycaemia,
MANAGEMENT OF DIABETIC KETOACIDOSIS 90 MANAGEMENT OF DIABETIC KETOACIDOSIS Diagnosis elevated plasma and/or urinary ketones metabolic acidosis (raised H + /low serum bicarbonate) Remember that hyperglycaemia,
Levels of Critical Care for Adult Patients
 LEVELS OF CARE 1 Levels of Critical Care for Adult Patients STANDARDS AND GUIDELINES LEVELS OF CARE 2 Intensive Care Society 2009 All rights reserved. No reproduction, copy or transmission of this publication
LEVELS OF CARE 1 Levels of Critical Care for Adult Patients STANDARDS AND GUIDELINES LEVELS OF CARE 2 Intensive Care Society 2009 All rights reserved. No reproduction, copy or transmission of this publication
Oxygen Therapy. Oxygen therapy quick guide V3 July 2012.
 PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
PRESENTATION Oxygen (O 2 ) is a gas provided in a compressed form in a cylinder. It is also available in a liquid form. It is fed via a regulator and flow meter to the patient by means of plastic tubing
Subject: Severe Sepsis/Septic Shock Published Date: August 9, 2013 Scope: Hospital Wide Original Creation Date: August 9, 2013
 Stony Brook Medicine Severe Sepsis/Septic Shock Recognition and Treatment Protocols Subject: Severe Sepsis/Septic Shock Published Date: August 9, 2013 Scope: Hospital Wide Original Creation Date: August
Stony Brook Medicine Severe Sepsis/Septic Shock Recognition and Treatment Protocols Subject: Severe Sepsis/Septic Shock Published Date: August 9, 2013 Scope: Hospital Wide Original Creation Date: August
Recommendations for the Perioperative Care of Patients Selected for Day Care Surgery
 Page 1 of 7 Recommendations for the Perioperative Care of Patients Selected for Day Care Surgery Version Effective Date 1 Feb 1993 (Reviewed Feb 2002) 2 Oct 2012 Document No. HKCA P5 v2 Prepared by College
Page 1 of 7 Recommendations for the Perioperative Care of Patients Selected for Day Care Surgery Version Effective Date 1 Feb 1993 (Reviewed Feb 2002) 2 Oct 2012 Document No. HKCA P5 v2 Prepared by College
CLINICAL SKILLS: THE 'DR ABCDE' ASSESSMENT
 CLINICAL SKILLS: THE 'DR ABCDE' ASSESSMENT The 'DR ABCDE' approach to assessing an acutely unwell patient should be at the front of every junior doctor's mind whenever they get bleeped or asked to see
CLINICAL SKILLS: THE 'DR ABCDE' ASSESSMENT The 'DR ABCDE' approach to assessing an acutely unwell patient should be at the front of every junior doctor's mind whenever they get bleeped or asked to see
Paediatric fluids 13/06/05
 Dr Catharine Wilson Consultant Paediatric Anaesthetist Sheffield Children s Hospital. UK Paediatric fluids 13/06/05 Self assessment: Complete these questions before reading the tutorial. Discuss the answers
Dr Catharine Wilson Consultant Paediatric Anaesthetist Sheffield Children s Hospital. UK Paediatric fluids 13/06/05 Self assessment: Complete these questions before reading the tutorial. Discuss the answers
COPD - Education for Patients and Carers Integrated Care Pathway
 Patient NHS COPD - Education for Patients and Carers Integrated Care Pathway Date ICP completed:. Is the patient following another Integrated Care Pathway[s].. / If yes, record which other Integrated Care
Patient NHS COPD - Education for Patients and Carers Integrated Care Pathway Date ICP completed:. Is the patient following another Integrated Care Pathway[s].. / If yes, record which other Integrated Care
Overview. Geriatric Overview. Chapter 26. Geriatrics 9/11/2012
 Chapter 26 Geriatrics Slide 1 Overview Trauma Common Medical Emergencies Special Considerations in the Elderly Medication Considerations Abuse and Neglect Expanding the Role of EMS Slide 2 Geriatric Overview
Chapter 26 Geriatrics Slide 1 Overview Trauma Common Medical Emergencies Special Considerations in the Elderly Medication Considerations Abuse and Neglect Expanding the Role of EMS Slide 2 Geriatric Overview
CH CONSCIOUS SEDATION
 Summary: CH CONSCIOUS SEDATION It is the policy of Carondelet Health that moderate conscious sedation of patients will be undertaken with appropriate evaluation and monitoring. Effective Date: 9/4/04 Revision
Summary: CH CONSCIOUS SEDATION It is the policy of Carondelet Health that moderate conscious sedation of patients will be undertaken with appropriate evaluation and monitoring. Effective Date: 9/4/04 Revision
Oxygen - update April 2009 OXG
 PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
PRESENTATION Oxygen (O 2 ) is a gas provided in compressed form in a cylinder. It is also available in liquid form, in a system adapted for ambulance use. It is fed via a regulator and flow meter to the
Hospital Name. Patient Nursing Notes
 PILOT DOCUMENT/ PAC/NCPS DOC /ISSUE/MARCH 4 National Clinical Programme in Surgery PILOT DOCUMENT Hospital Name Patient Nursing Notes FOR DAY CASE ELECTIVE SURGERY PATIENTS UNDERGOING GENERAL OR SPINAL
PILOT DOCUMENT/ PAC/NCPS DOC /ISSUE/MARCH 4 National Clinical Programme in Surgery PILOT DOCUMENT Hospital Name Patient Nursing Notes FOR DAY CASE ELECTIVE SURGERY PATIENTS UNDERGOING GENERAL OR SPINAL
NORTH WALES CRITICAL CARE NETWORK
 NORTH WALES CRITICAL CARE NETWORK LEVELS OF CRITICAL CARE FOR ADULT PATIENTS Throughout the work of the North Wales Critical Care Network reference to Levels of Care for the critically ill are frequently
NORTH WALES CRITICAL CARE NETWORK LEVELS OF CRITICAL CARE FOR ADULT PATIENTS Throughout the work of the North Wales Critical Care Network reference to Levels of Care for the critically ill are frequently
The patient s response to therapy within the first hour in the Emergency Room is one of the most reliable ways to predict need for hospitalization.
 Emergency Room Asthma Management Algorithm The Emergency Room Asthma Management Algorithm is to be used for any patient seen in the Emergency Room with the diagnosis of asthma. (The initial history should
Emergency Room Asthma Management Algorithm The Emergency Room Asthma Management Algorithm is to be used for any patient seen in the Emergency Room with the diagnosis of asthma. (The initial history should
Sepsis Reassess patient Monitor and maintain respiratory/ hemodynamic status
 Patient exhibits two or more of the following SIRS criteria: Temperature greater than 38 o C (100.4 o F) or less SIRS than criteria 36 o C (96.8 o F) Heart Rate greater than 90 beats/minute Respiratory
Patient exhibits two or more of the following SIRS criteria: Temperature greater than 38 o C (100.4 o F) or less SIRS than criteria 36 o C (96.8 o F) Heart Rate greater than 90 beats/minute Respiratory
National Clinical Programme in Surgery (NCPS) Care Pathway for the Management of Day Case Laparoscopic Cholecystectomy
 Care Pathway for the Management of Day Case Laparoscopic Cholecystectomy") National Clinical Programme in Surgery (NCPS) Care Pathway for the Management of Day Case Consultant Surgeon DRAFT VERSION 0.5 090415 Table of Contents 1.0 Purpose... 3 2.0 Scope... 3 3.0 Responsibility...
National Clinical Programme in Surgery (NCPS) Care Pathway for the Management of Day Case Consultant Surgeon DRAFT VERSION 0.5 090415 Table of Contents 1.0 Purpose... 3 2.0 Scope... 3 3.0 Responsibility...
DISCHARGE CRITERIA FOR PHASE I & II- POST ANESTHESIA CARE
 REFERENCES: The Joint Commission Accreditation Manual for Hospitals American Society of Post Anesthesia Nurses: Standards of Post Anesthesia Nursing Practice (1991, 2002). RELATED DOCUMENTS: SHC Administrative
REFERENCES: The Joint Commission Accreditation Manual for Hospitals American Society of Post Anesthesia Nurses: Standards of Post Anesthesia Nursing Practice (1991, 2002). RELATED DOCUMENTS: SHC Administrative
Acute heart failure may be de novo or it may be a decompensation of chronic heart failure.
 Management of Acute Left Ventricular Failure Acute left ventricular failure presents as pulmonary oedema due to increased pressure in the pulmonary capillaries. It is important to realise though that left
Management of Acute Left Ventricular Failure Acute left ventricular failure presents as pulmonary oedema due to increased pressure in the pulmonary capillaries. It is important to realise though that left
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy
 The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
The Sepsis Puzzle: Identification, Monitoring and Early Goal Directed Therapy Cindy Goodrich RN, MS, CCRN Content Description Sepsis is caused by widespread tissue injury and systemic inflammation resulting
STUDY GUIDE 1.1: NURSING DIAGNOSTIC STATEMENTS AND COMPREHENSIVE PLANS OF CARE
 STUDY GUIDE 1.1: NURSING DIAGNOSTIC STATEMENTS AND COMPREHENSIVE PLANS OF CARE WHAT IS A NURSING DIAGNOSIS? A nursing diagnosis is a clinical judgment about individual, family, or community responses to
STUDY GUIDE 1.1: NURSING DIAGNOSTIC STATEMENTS AND COMPREHENSIVE PLANS OF CARE WHAT IS A NURSING DIAGNOSIS? A nursing diagnosis is a clinical judgment about individual, family, or community responses to
PARAMEDIC TRAINING CLINICAL OBJECTIVES
 Page 1 of 21 GENERAL PATIENT UNIT When assigned to the General Patient unit paramedic student should gain knowledge and experience in the following: 1. Appropriate communication with patients and members
Page 1 of 21 GENERAL PATIENT UNIT When assigned to the General Patient unit paramedic student should gain knowledge and experience in the following: 1. Appropriate communication with patients and members
Lynda Richardson, RN, BSN Sepsis/Septic Shock Abstractor. No disclosures
 Lynda Richardson, RN, BSN Sepsis/Septic Shock Abstractor No disclosures 1 2 3 Discuss data requirements -3 hour bundle -6 hour bundle Challenges and compliance issues Success 4 Based on the Surviving Sepsis
Lynda Richardson, RN, BSN Sepsis/Septic Shock Abstractor No disclosures 1 2 3 Discuss data requirements -3 hour bundle -6 hour bundle Challenges and compliance issues Success 4 Based on the Surviving Sepsis
Summary of EWS Policy for NHSP Staff
 Summary of EWS Policy for NHSP Staff For full version see CMFT Intranet Contact Sister Donna Egan outreach coordinator bleep 8742 Tel: 0161 276 8742 Introduction The close monitoring of patients physiological
Summary of EWS Policy for NHSP Staff For full version see CMFT Intranet Contact Sister Donna Egan outreach coordinator bleep 8742 Tel: 0161 276 8742 Introduction The close monitoring of patients physiological
SE5h, Sepsis Education.pdf. Surviving Sepsis
 Surviving Sepsis 1 Scope and Impact of the Problem: Severe sepsis is a major healthcare problem that affects millions of people around the world each year with an extremely high mortality rate of 30 to
Surviving Sepsis 1 Scope and Impact of the Problem: Severe sepsis is a major healthcare problem that affects millions of people around the world each year with an extremely high mortality rate of 30 to
Head Injury. Dr Sally McCarthy Medical Director ECI
 Head Injury Dr Sally McCarthy Medical Director ECI Head injury in the emergency department A common presentation 80% Mild Head Injury = GCS 14 15 10% Moderate Head Injury = GCS 9 13 10% Severe Head Injury
Head Injury Dr Sally McCarthy Medical Director ECI Head injury in the emergency department A common presentation 80% Mild Head Injury = GCS 14 15 10% Moderate Head Injury = GCS 9 13 10% Severe Head Injury
CORONARY ARTERY BYPASS GRAFT & HEART VALVE SURGERY
 CORONARY ARTERY BYPASS GRAFT & HEART VALVE SURGERY www.cpmc.org/learning i learning about your health What to Expect During Your Hospital Stay 1 Our Team: Our cardiac surgery specialty team includes nurses,
CORONARY ARTERY BYPASS GRAFT & HEART VALVE SURGERY www.cpmc.org/learning i learning about your health What to Expect During Your Hospital Stay 1 Our Team: Our cardiac surgery specialty team includes nurses,
Lothian Guideline for Domiciliary Oxygen Therapy Service for COPD
 Lothian Guideline for Domiciliary Oxygen Therapy Service for COPD This document describes the standard for clinical assessment, prescription, optimal management and follow-up of patients receiving domiciliary
Lothian Guideline for Domiciliary Oxygen Therapy Service for COPD This document describes the standard for clinical assessment, prescription, optimal management and follow-up of patients receiving domiciliary
Paediatric Advanced Warning Score (PAWS)
") Paediatric Advanced Warning Score (PAWS) Prevention is better than cure. Spectrum of critical illness Ward level care HDU Care ICU Care Early admission may improve outcome ICU Outreach teams Medical Emergency
Paediatric Advanced Warning Score (PAWS) Prevention is better than cure. Spectrum of critical illness Ward level care HDU Care ICU Care Early admission may improve outcome ICU Outreach teams Medical Emergency
A National Early Warning Score for the NHS
 A National Early Warning Score for the NHS Professor Gary B Smith FRCA FRCP Centre of Postgraduate Medical Research & Education, School of Health and Social Care, Bournemouth University - from local data
A National Early Warning Score for the NHS Professor Gary B Smith FRCA FRCP Centre of Postgraduate Medical Research & Education, School of Health and Social Care, Bournemouth University - from local data
Cardiac Catheterisation. Cardiology
 Cardiac Catheterisation Cardiology Name: Cardiac catheterisation Version: 1 Page 1 of 7 Contents Page Number(s) 1. Introduction 3 2. Management pre operative 3 3. Management post operative 5 4. Discharge
Cardiac Catheterisation Cardiology Name: Cardiac catheterisation Version: 1 Page 1 of 7 Contents Page Number(s) 1. Introduction 3 2. Management pre operative 3 3. Management post operative 5 4. Discharge
How To Treat A Heart Attack
 13 Resuscitation and preparation for anaesthesia and surgery Key Points 13.1 MANAGEMENT OF EMERGENCIES AND CARDIOPULMONARY RESUSCITATION ESSENTIAL HEALTH TECHNOLOGIES The emergency measures that are familiar
13 Resuscitation and preparation for anaesthesia and surgery Key Points 13.1 MANAGEMENT OF EMERGENCIES AND CARDIOPULMONARY RESUSCITATION ESSENTIAL HEALTH TECHNOLOGIES The emergency measures that are familiar
Acute Care Day Respiratory. SCENARIO The Patient with Acute Asthma
 Acute Care Day Respiratory SCENARIO The Patient with Acute Asthma Notes for the instructor not volunteered to students 30 minutes have been allocated to the running of the scenario with an additional 10
Acute Care Day Respiratory SCENARIO The Patient with Acute Asthma Notes for the instructor not volunteered to students 30 minutes have been allocated to the running of the scenario with an additional 10
S9 Administer thrombolytic treatment in acute ischaemic stroke
 S9 Administer thrombolytic treatment in acute ischaemic Screening and initiating treatment, overseeing competency of treatment About this workforce competence This competence is about the emergency administration
S9 Administer thrombolytic treatment in acute ischaemic Screening and initiating treatment, overseeing competency of treatment About this workforce competence This competence is about the emergency administration
ECG may be indicated for patients with cardiovascular risk factors
 eappendix A. Summary for Preoperative ECG American College of Cardiology/ American Heart Association, 2007 A1 2002 A2 European Society of Cardiology and European Society of Anaesthesiology, 2009 A3 Improvement,
eappendix A. Summary for Preoperative ECG American College of Cardiology/ American Heart Association, 2007 A1 2002 A2 European Society of Cardiology and European Society of Anaesthesiology, 2009 A3 Improvement,
HLTEN609B Practise in the respiratory nursing environment
 HLTEN609B Practise in the respiratory nursing environment Release: 1 HLTEN609B Practise in the respiratory nursing environment Modification History Not Applicable Unit Descriptor Descriptor This unit addresses
HLTEN609B Practise in the respiratory nursing environment Release: 1 HLTEN609B Practise in the respiratory nursing environment Modification History Not Applicable Unit Descriptor Descriptor This unit addresses
Suffolk County Community College School of Nursing NUR 133 ADULT NURSING I
 Suffolk County Community College School of Nursing NUR 133 ADULT NURSING I Page # 1 Instructions for students: Case study # 1 For this lab, you are planning to provide care to the following client: CB
Suffolk County Community College School of Nursing NUR 133 ADULT NURSING I Page # 1 Instructions for students: Case study # 1 For this lab, you are planning to provide care to the following client: CB
Recognizing and Treating Fevers in Children with Complex Medical Issues by Susan Agrawal
 www.complexchild.com Recognizing and Treating Fevers in Children with Complex Medical Issues by Susan Agrawal Fevers can be some of the scariest symptoms we see in our children, but they are also some
www.complexchild.com Recognizing and Treating Fevers in Children with Complex Medical Issues by Susan Agrawal Fevers can be some of the scariest symptoms we see in our children, but they are also some
Sepsis: Identification and Treatment
 Sepsis: Identification and Treatment Daniel Z. Uslan, MD Associate Clinical Professor Division of Infectious Diseases Medical Director, UCLA Sepsis Task Force Severe Sepsis: A Significant Healthcare Challenge
Sepsis: Identification and Treatment Daniel Z. Uslan, MD Associate Clinical Professor Division of Infectious Diseases Medical Director, UCLA Sepsis Task Force Severe Sepsis: A Significant Healthcare Challenge
The new Heart Failure pathway
 The new Heart Failure pathway An integrated and seamless Strategy Dr Sunil Balani Definition of Heart Failure The inability of the heart to pump blood at a rate commensurate with the requirements of metabolising
The new Heart Failure pathway An integrated and seamless Strategy Dr Sunil Balani Definition of Heart Failure The inability of the heart to pump blood at a rate commensurate with the requirements of metabolising
Protocols for Early Extubation After Cardiothoracic Surgery
 Protocols for Early Extubation After Cardiothoracic Surgery AATS / STS CT Critical Care Symposium April 27, 2014 Toronto, Ontario Nevin M. Katz, M.D. Johns Hopkins University Foundation for the Advancement
Protocols for Early Extubation After Cardiothoracic Surgery AATS / STS CT Critical Care Symposium April 27, 2014 Toronto, Ontario Nevin M. Katz, M.D. Johns Hopkins University Foundation for the Advancement
INTRAVENOUS FLUIDS. Acknowledgement. Background. Starship Children s Health Clinical Guideline
 Acknowledgements Background Well child with normal hydration Unwell children (+/- abnormal hydration Maintenance Deficit Ongoing losses (e.g. from drains) Which fluid? Monitoring Special Fluids Post-operative
Acknowledgements Background Well child with normal hydration Unwell children (+/- abnormal hydration Maintenance Deficit Ongoing losses (e.g. from drains) Which fluid? Monitoring Special Fluids Post-operative
Emergency Scenario. Chest Pain
 Emergency Scenario Chest Pain This emergency scenario reviews chest pain in a primary care patient, and is set up for roleplay and case review with your staff. 1) The person facilitating scenarios can
Emergency Scenario Chest Pain This emergency scenario reviews chest pain in a primary care patient, and is set up for roleplay and case review with your staff. 1) The person facilitating scenarios can
Name: Age: Resting BP: Wt. kg: Est. HR max : 85%HR max : Resting HR:
 Bruce Protocol - Submaximal GXT Name: Age: Resting BP: Wt. kg: Est. HR max : 85%HR max : Resting HR: Stage Min. % Grade MPH METs 2min HR 3min HR BP RPE 1 0-3 10 1.7 4.7 2 3-6 12 2.5 7.0 3 6-9 14 3.4 10.1
Bruce Protocol - Submaximal GXT Name: Age: Resting BP: Wt. kg: Est. HR max : 85%HR max : Resting HR: Stage Min. % Grade MPH METs 2min HR 3min HR BP RPE 1 0-3 10 1.7 4.7 2 3-6 12 2.5 7.0 3 6-9 14 3.4 10.1
Trust Guideline for the use of the Modified Early Obstetric Warning Score (MEOWS) in detecting the seriously ill and deteriorating woman.
 in detecting the seriously ill and deteriorating woman.") A clinical guideline recommended for use In: By: For: Key words: Written by: Supported by: Maternity Services. Obstetricians, Midwives and Midwifery Care Assistants. All women receiving care from maternity
A clinical guideline recommended for use In: By: For: Key words: Written by: Supported by: Maternity Services. Obstetricians, Midwives and Midwifery Care Assistants. All women receiving care from maternity
The Newcastle upon Tyne Hospitals NHS Foundation Trust. National Early Warning Score (NEWS) Policy
 Policy") The Newcastle upon Tyne Hospitals NHS Foundation Trust National Early Warning Score (NEWS) Policy Version.: 1.0 Effective From: 3 December 2014 Expiry Date: 3 December 2016 Date Ratified: 1 September 2014
The Newcastle upon Tyne Hospitals NHS Foundation Trust National Early Warning Score (NEWS) Policy Version.: 1.0 Effective From: 3 December 2014 Expiry Date: 3 December 2016 Date Ratified: 1 September 2014
Preoperative Laboratory and Diagnostic Studies
 Preoperative Laboratory and Diagnostic Studies Preoperative Labratorey and Diagnostic Studies The concept of standardized testing in all presurgical patients regardless of age or medical condition is no
Preoperative Laboratory and Diagnostic Studies Preoperative Labratorey and Diagnostic Studies The concept of standardized testing in all presurgical patients regardless of age or medical condition is no
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL
 Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
Marilyn Borkgren-Okonek, APN, CCNS, RN, MS Suburban Lung Associates, S.C. Elk Grove Village, IL www.goldcopd.com GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT
Documentation Guidelines for Physicians Interventional Pain Services
 Documentation Guidelines for Physicians Interventional Pain Services Pamela Gibson, CPC Assistant Director, VMG Coding Anesthesia and Surgical Divisions 343.8791 1 General Principles of Medical Record
Documentation Guidelines for Physicians Interventional Pain Services Pamela Gibson, CPC Assistant Director, VMG Coding Anesthesia and Surgical Divisions 343.8791 1 General Principles of Medical Record
F.E.E.A. FONDATION EUROPEENNE D'ENSEIGNEMENT EN ANESTHESIOLOGIE FOUNDATION FOR EUROPEAN EDUCATION IN ANAESTHESIOLOGY
 créée sous le Patronage de l'union Européenne Detailed plan of the program of six courses 1. RESPIRATORY 1. ESPIRATORY AND THORAX 1.1 Physics and principles of measurement 1.1.1 Physical laws 1.1.2 Vaporizers
créée sous le Patronage de l'union Européenne Detailed plan of the program of six courses 1. RESPIRATORY 1. ESPIRATORY AND THORAX 1.1 Physics and principles of measurement 1.1.1 Physical laws 1.1.2 Vaporizers
ST. ROSE HOSPITAL EMERGENCY SERVICES THERAPEUTIC HYPOTHERMIA AFTER CARDIAC ARREST PROTOCOL PURPOSE
 PURPOSE To outline the management of therapeutic hypothermia for the patient following cardiac arrest. LEVEL SUPPORTIVE DATA EFFECTS OF THERAPEUTIC HYPOTHERMIA Interdependent. Requires MD order. Cardiac
PURPOSE To outline the management of therapeutic hypothermia for the patient following cardiac arrest. LEVEL SUPPORTIVE DATA EFFECTS OF THERAPEUTIC HYPOTHERMIA Interdependent. Requires MD order. Cardiac
CorCap Cardiac Support Device Patient Information Booklet
 What is Heart Failure? CorCap Cardiac Support Device Patient Information Booklet Heart failure is a condition in which the heart is unable to pump enough blood to meet the needs of the body. To compensate
What is Heart Failure? CorCap Cardiac Support Device Patient Information Booklet Heart failure is a condition in which the heart is unable to pump enough blood to meet the needs of the body. To compensate
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF)
 MANAGEMENT of Atrial Fibrillation (AF)") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF) Key priorities Identification and diagnosis Treatment for persistent AF Treatment for permanent AF Antithrombotic
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT of Atrial Fibrillation (AF) Key priorities Identification and diagnosis Treatment for persistent AF Treatment for permanent AF Antithrombotic
APPENDIX B SAMPLE PEDIATRIC CRITICAL CARE NURSE PRACTITIONER GOALS AND OBJECTIVES
 APPENDIX B SAMPLE PEDIATRIC CRITICAL CARE NURSE PRACTITIONER GOALS AND OBJECTIVES The critical care nurse practitioner orientation is an individualized process based on one s previous experiences and should
APPENDIX B SAMPLE PEDIATRIC CRITICAL CARE NURSE PRACTITIONER GOALS AND OBJECTIVES The critical care nurse practitioner orientation is an individualized process based on one s previous experiences and should
RESPONDING TO ANESTHETIC COMPLICATIONS
 RESPONDING TO ANESTHETIC COMPLICATIONS General anesthesia poses minimal risk to most patients when performed by a capable anesthetist using appropriate protocols and proper monitoring. However, it is vitally
RESPONDING TO ANESTHETIC COMPLICATIONS General anesthesia poses minimal risk to most patients when performed by a capable anesthetist using appropriate protocols and proper monitoring. However, it is vitally
NICE Pathways bring together all NICE guidance, quality standards and other NICE information on a specific topic.
 Diabetic ketoacidosis in children and young people bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They
Diabetic ketoacidosis in children and young people bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They
ELSO GUIDELINES FOR TRAINING AND CONTINUING EDUCATION OF ECMO SPECIALISTS
 ELSO GUIDELINES FOR TRAINING AND CONTINUING EDUCATION OF ECMO SPECIALISTS PURPOSE The "" is a document developed by the Extracorporeal Life Support Organization (ELSO) as a reference for current and future
ELSO GUIDELINES FOR TRAINING AND CONTINUING EDUCATION OF ECMO SPECIALISTS PURPOSE The "" is a document developed by the Extracorporeal Life Support Organization (ELSO) as a reference for current and future
KIH Cardiac Rehabilitation Program
 KIH Cardiac Rehabilitation Program For any further information Contact: +92-51-2870361-3, 2271154 [email protected] What is Cardiac Rehabilitation Cardiac rehabilitation describes all measures used to
KIH Cardiac Rehabilitation Program For any further information Contact: +92-51-2870361-3, 2271154 [email protected] What is Cardiac Rehabilitation Cardiac rehabilitation describes all measures used to
SIGN. Management of hip fracture in older people. June 2009. A national clinical guideline. Scottish Intercollegiate Guidelines Network
 SIGN Scottish Intercollegiate Guidelines Network Part of NHS Quality Improvement Scotland Help us to improve SIGN guidelines - click here to complete our survey 111 Management of hip fracture in older
SIGN Scottish Intercollegiate Guidelines Network Part of NHS Quality Improvement Scotland Help us to improve SIGN guidelines - click here to complete our survey 111 Management of hip fracture in older
2002 burns responsible for 322,000 deaths world wide. aboriginal community in NA Most burns occur in the urban environment
 Burn Injuries: The Problem 2002 burns responsible for 322,000 deaths world wide 4 th as cause of unintentional child injury death in the USA 3 rd leading cause of unintentional death in aboriginal community
Burn Injuries: The Problem 2002 burns responsible for 322,000 deaths world wide 4 th as cause of unintentional child injury death in the USA 3 rd leading cause of unintentional death in aboriginal community
Gloucestershire Hospitals
 Gloucestershire Hospitals NHS Foundation Trust TRUST GUIDELINE EPILEPSY AND STATUS EPILEPTICUS MANAGEMENT 1. INTRODUCTION The aim of this guideline is to ensure safe management of Status Epilepticus in
Gloucestershire Hospitals NHS Foundation Trust TRUST GUIDELINE EPILEPSY AND STATUS EPILEPTICUS MANAGEMENT 1. INTRODUCTION The aim of this guideline is to ensure safe management of Status Epilepticus in
Board of Directors. 28 January 2015
 Executive Summary Purpose: Board of Directors 28 January 2015 Briefing on the requirements for the Trust to comply with Hard Truths Commitments Regarding the Publishing of Staffing Data Director of Nursing
Executive Summary Purpose: Board of Directors 28 January 2015 Briefing on the requirements for the Trust to comply with Hard Truths Commitments Regarding the Publishing of Staffing Data Director of Nursing
Leeds Teaching Hospital Ward Healthcheck Metrics Programme
 Ward Healthcheck paper - Appendix 2 Appen Leeds Teaching Hospital Ward Healthcheck Metrics Programme Metrics Information Introduction The nursing care Metrics were initially developed in the north west
Ward Healthcheck paper - Appendix 2 Appen Leeds Teaching Hospital Ward Healthcheck Metrics Programme Metrics Information Introduction The nursing care Metrics were initially developed in the north west
Procedure for Inotrope Administration in the home
 Procedure for Inotrope Administration in the home Purpose This purpose of this procedure is to define the care used when administering inotropic agents intravenously in the home This includes: A. Practice
Procedure for Inotrope Administration in the home Purpose This purpose of this procedure is to define the care used when administering inotropic agents intravenously in the home This includes: A. Practice
Oxygenation. Chapter 21. Anatomy and Physiology of Breathing. Anatomy and Physiology of Breathing*
 Oxygenation Chapter 21 Anatomy and Physiology of Breathing Inspiration ~ breathing in Expiration ~ breathing out Ventilation ~ Movement of air in & out of the lungs Respiration ~ exchange of O2 & carbon
Oxygenation Chapter 21 Anatomy and Physiology of Breathing Inspiration ~ breathing in Expiration ~ breathing out Ventilation ~ Movement of air in & out of the lungs Respiration ~ exchange of O2 & carbon
IN-HOME QUALITY IMPROVEMENT BEST PRACTICE: PHYSICIAN RELATIONSHIPS NURSE TRACK
 IN-HOME QUALITY IMPROVEMENT BEST PRACTICE: PHYSICIAN RELATIONSHIPS NURSE TRACK Best Practice Intervention Packages were designed for use by any In-Home Provider Agency to support reducing avoidable hospitalizations
IN-HOME QUALITY IMPROVEMENT BEST PRACTICE: PHYSICIAN RELATIONSHIPS NURSE TRACK Best Practice Intervention Packages were designed for use by any In-Home Provider Agency to support reducing avoidable hospitalizations
Nurses Competencies in Caring for Mechanically Ventilated Patients, What does the Evidence Say? Dr. Samah Anwar Dr. Noha El-Baz
 Nurses Competencies in Caring for Mechanically Ventilated Patients, What does the Evidence Say? Dr. Samah Anwar Dr. Noha El-Baz The mechanically ventilated patient presents many challenges for the intensive
Nurses Competencies in Caring for Mechanically Ventilated Patients, What does the Evidence Say? Dr. Samah Anwar Dr. Noha El-Baz The mechanically ventilated patient presents many challenges for the intensive
Epidural Continuous Infusion. Patient information Leaflet
 Epidural Continuous Infusion Patient information Leaflet April 2015 Introduction You may already know that epidural s are often used to treat pain during childbirth. This same technique can also used as
Epidural Continuous Infusion Patient information Leaflet April 2015 Introduction You may already know that epidural s are often used to treat pain during childbirth. This same technique can also used as
240- PROBLEM SET INSERTION OF SWAN-GANZ SYSTEMIC VASCULAR RESISTANCE. Blood pressure = f(cardiac output and peripheral resistance)
") 240- PROBLEM SET INSERTION OF SWAN-GANZ 50 kg Pig Rt Jugular 0 cm Rt Atrium 10 cm Rt ventricle 15 cm Wedge 20-25 cm SYSTEMIC VASCULAR RESISTANCE Blood pressure = f(cardiac output and peripheral resistance)
240- PROBLEM SET INSERTION OF SWAN-GANZ 50 kg Pig Rt Jugular 0 cm Rt Atrium 10 cm Rt ventricle 15 cm Wedge 20-25 cm SYSTEMIC VASCULAR RESISTANCE Blood pressure = f(cardiac output and peripheral resistance)
Purpose To guide registered nurses who may manage clients experiencing sudden or unexpected life-threatening cardiac emergencies.
 Emergency Cardiac Care: Decision Support Tool #1 RN-Initiated Emergency Cardiac Care Without Cardiac Monitoring/Manual Defibrillator or Emergency Cardiac Drugs Decision support tools are evidence-based
Emergency Cardiac Care: Decision Support Tool #1 RN-Initiated Emergency Cardiac Care Without Cardiac Monitoring/Manual Defibrillator or Emergency Cardiac Drugs Decision support tools are evidence-based
Pulmonary Rehabilitation in Newark and Sherwood
 Pulmonary Rehabilitation in Newark and Sherwood With exception of smoking cessation pulmonary rehabilitation is the single most effective intervention for any patient with COPD. A Cochrane review published
Pulmonary Rehabilitation in Newark and Sherwood With exception of smoking cessation pulmonary rehabilitation is the single most effective intervention for any patient with COPD. A Cochrane review published
Lifestyle-based Adrenal Dysfunction
 Assessing Adrenal Function Primary FDM Testing Glandular vs. Lifestyle Adrenal problems Glandular-based Adrenal Problems Lifestyle-based Adrenal Dysfunction http://www.fmtown.com 1 Causes of Adrenal Dysfunction
Assessing Adrenal Function Primary FDM Testing Glandular vs. Lifestyle Adrenal problems Glandular-based Adrenal Problems Lifestyle-based Adrenal Dysfunction http://www.fmtown.com 1 Causes of Adrenal Dysfunction
Risk estimation and the prevention of cardiovascular disease. A national clinical guideline
 SIGN Scottish Intercollegiate Guidelines Network Help us to improve SIGN guidelines - click here to complete our survey 97 Risk estimation and the prevention of cardiovascular disease A national clinical
SIGN Scottish Intercollegiate Guidelines Network Help us to improve SIGN guidelines - click here to complete our survey 97 Risk estimation and the prevention of cardiovascular disease A national clinical
Hyperosmolar Non-Ketotic Diabetic State (HONK)
") Hyperosmolar Non-Ketotic Diabetic State (HONK) University Hospitals of Leicester NHS Trust Guidelines for Management of Acute Medical Emergencies Management is largely the same as for diabetic ketoacidosis
Hyperosmolar Non-Ketotic Diabetic State (HONK) University Hospitals of Leicester NHS Trust Guidelines for Management of Acute Medical Emergencies Management is largely the same as for diabetic ketoacidosis
Acutely ill patients in hospital. Recognition of and response to acute illness in adults in hospital
 Issue date: July 2007 Acutely ill patients in hospital Recognition of and response to acute illness in adults in hospital NICE clinical guideline 50 Developed by the Centre for Clinical Practice at NICE
Issue date: July 2007 Acutely ill patients in hospital Recognition of and response to acute illness in adults in hospital NICE clinical guideline 50 Developed by the Centre for Clinical Practice at NICE
Scope and Standards for Nurse Anesthesia Practice
 Scope and Standards for Nurse Anesthesia Practice Copyright 2013 222 South Prospect Ave. Park Ridge, IL 60068 www.aana.com Scope and Standards for Nurse Anesthesia Practice The AANA Scope and Standards
Scope and Standards for Nurse Anesthesia Practice Copyright 2013 222 South Prospect Ave. Park Ridge, IL 60068 www.aana.com Scope and Standards for Nurse Anesthesia Practice The AANA Scope and Standards
Flexible sigmoidoscopy the procedure explained Please bring this booklet with you
 Flexible sigmoidoscopy the procedure explained Please bring this booklet with you Exceptional healthcare, personally delivered Introduction You have been advised by your GP or hospital doctor to have an
Flexible sigmoidoscopy the procedure explained Please bring this booklet with you Exceptional healthcare, personally delivered Introduction You have been advised by your GP or hospital doctor to have an
404 Section 5 Shock and Resuscitation. Scene Size-up. Primary Assessment. History Taking
 404 Section 5 and Resuscitation Scene Size-up Scene Safety Mechanism of Injury (MOI)/ Nature of Illness (NOI) Ensure scene safety and address hazards. Standard precautions should include a minimum of gloves
404 Section 5 and Resuscitation Scene Size-up Scene Safety Mechanism of Injury (MOI)/ Nature of Illness (NOI) Ensure scene safety and address hazards. Standard precautions should include a minimum of gloves
Understanding Hypoventilation and Its Treatment by Susan Agrawal
 www.complexchild.com Understanding Hypoventilation and Its Treatment by Susan Agrawal Most of us have a general understanding of what the term hyperventilation means, since hyperventilation, also called
www.complexchild.com Understanding Hypoventilation and Its Treatment by Susan Agrawal Most of us have a general understanding of what the term hyperventilation means, since hyperventilation, also called
URN: Family name: Given name(s): Address:
: Address:") The State of Queensland (Queensland Health) 2012 Contact [email protected] Facility: Clinical Pathways Never Replace Clinical Judgement Care Outlined In This Pathway Must be Altered If It Is Not Clinically
The State of Queensland (Queensland Health) 2012 Contact [email protected] Facility: Clinical Pathways Never Replace Clinical Judgement Care Outlined In This Pathway Must be Altered If It Is Not Clinically
CROSS HEALTH CARE BOUNDARIES MATERNITY CLINICAL GUIDELINE
 CROSS HEALTH CARE BOUNDARIES MATERNITY CLINICAL GUIDELINE Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Obstetric Early Warning Score Guideline Implementation
CROSS HEALTH CARE BOUNDARIES MATERNITY CLINICAL GUIDELINE Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Obstetric Early Warning Score Guideline Implementation
Chapter 16. Learning Objectives. Learning Objectives 9/11/2012. Shock. Explain difference between compensated and uncompensated shock
 Chapter 16 Shock Learning Objectives Explain difference between compensated and uncompensated shock Differentiate among 5 causes and types of shock: Hypovolemic Cardiogenic Neurogenic Septic Anaphylactic
Chapter 16 Shock Learning Objectives Explain difference between compensated and uncompensated shock Differentiate among 5 causes and types of shock: Hypovolemic Cardiogenic Neurogenic Septic Anaphylactic
BUNDLES IN 2013: SURVIVING SEPSIS CAMPAIGN
 BUNDLES IN 2013: SURVIVING SEPSIS CAMPAIGN R. Phillip Dellinger MD, MSc, MCCM Professor of Medicine Cooper Medical School of Rowan University Professor of Medicine University Medicine and Dentistry of
BUNDLES IN 2013: SURVIVING SEPSIS CAMPAIGN R. Phillip Dellinger MD, MSc, MCCM Professor of Medicine Cooper Medical School of Rowan University Professor of Medicine University Medicine and Dentistry of
STAGES OF SHOCK. IRREVERSIBLE SHOCK Heart deteriorates until it can no longer pump and death occurs.
 STAGES OF SHOCK SHOCK : A profound disturbance of circulation and metabolism, which leads to inadequate perfusion of all organs which are needed to maintain life. COMPENSATED NONPROGRESSIVE SHOCK 30 sec
STAGES OF SHOCK SHOCK : A profound disturbance of circulation and metabolism, which leads to inadequate perfusion of all organs which are needed to maintain life. COMPENSATED NONPROGRESSIVE SHOCK 30 sec
ACCIDENT AND EMERGENCY DEPARTMENT/CARDIOLOGY
 Care Pathway Triage category ATRIAL FIBRILLATION PATHWAY ACCIDENT AND EMERGENCY DEPARTMENT/CARDIOLOGY AF/ FLUTTER IS PRIMARY REASON FOR PRESENTATION YES NO ONSET SYMPTOMS OF AF./../ TIME DURATION OF AF
Care Pathway Triage category ATRIAL FIBRILLATION PATHWAY ACCIDENT AND EMERGENCY DEPARTMENT/CARDIOLOGY AF/ FLUTTER IS PRIMARY REASON FOR PRESENTATION YES NO ONSET SYMPTOMS OF AF./../ TIME DURATION OF AF
Document Details Title. Early Warning Score Protocol for Community Hospitals and Prisons to detect the Deteriorating Patient
 Document Details Title Early warning Score Protocol for community Hospitals and Prisons to Detect the Deteriorating Patient Trust Ref No 1558-29748 Local Ref (optional) Main points the document This protocol
Document Details Title Early warning Score Protocol for community Hospitals and Prisons to Detect the Deteriorating Patient Trust Ref No 1558-29748 Local Ref (optional) Main points the document This protocol
Introduction. Definition
 DIRECTIVES FOR PRIVATE AMBULATORY SURGICAL CENTRES PROVIDING AMBULATORY SURGERY: REGULATION 4(1) OF THE PRIVATE HOSPITALS AND MEDICAL CLINICS REGULATIONS [CAP 248, Rg 1] I Introduction 1 These directives
DIRECTIVES FOR PRIVATE AMBULATORY SURGICAL CENTRES PROVIDING AMBULATORY SURGERY: REGULATION 4(1) OF THE PRIVATE HOSPITALS AND MEDICAL CLINICS REGULATIONS [CAP 248, Rg 1] I Introduction 1 These directives
Adult Home Oxygen Therapy. Purpose To provide guidance on the requirements for and procedures relating to domiciliary oxygen therapy.
 Contents Purpose... 1 Scope/Audience... 1 Categories for Home Oxygen Therapy... 2 Assessment for Home Oxygen Therapy... 3 Investigations... 3 Requests for home oxygen... 3 Provision of Home Oxygen... 4
Contents Purpose... 1 Scope/Audience... 1 Categories for Home Oxygen Therapy... 2 Assessment for Home Oxygen Therapy... 3 Investigations... 3 Requests for home oxygen... 3 Provision of Home Oxygen... 4
Pulmonary Diseases. Lung Disease: Pathophysiology, Medical and Exercise Programming. Overview of Pathophysiology
 Lung Disease: Pathophysiology, Medical and Exercise Programming Overview of Pathophysiology Ventilatory Impairments Increased airway resistance Reduced compliance Increased work of breathing Ventilatory
Lung Disease: Pathophysiology, Medical and Exercise Programming Overview of Pathophysiology Ventilatory Impairments Increased airway resistance Reduced compliance Increased work of breathing Ventilatory
National Early Warning Score. National Clinical Guideline No. 1
 National Early Warning Score National Clinical Guideline No. 1 February 2013 The National Early Warning Score and COMPASS Education programme project is a work stream of the National Acute Medicine Programme,
National Early Warning Score National Clinical Guideline No. 1 February 2013 The National Early Warning Score and COMPASS Education programme project is a work stream of the National Acute Medicine Programme,
Diabetic nephropathy is detected clinically by the presence of persistent microalbuminuria or proteinuria.
 Kidney Complications Diabetic Nephropathy Diabetic nephropathy is detected clinically by the presence of persistent microalbuminuria or proteinuria. The peak incidence of nephropathy is usually 15-25 years
Kidney Complications Diabetic Nephropathy Diabetic nephropathy is detected clinically by the presence of persistent microalbuminuria or proteinuria. The peak incidence of nephropathy is usually 15-25 years
Atrial Fibrillation Management Across the Spectrum of Illness
 Disclosures Atrial Fibrillation Management Across the Spectrum of Illness NONE Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University Objectives AF Discuss the pathophysiology, diagnosis,
Disclosures Atrial Fibrillation Management Across the Spectrum of Illness NONE Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University Objectives AF Discuss the pathophysiology, diagnosis,
Laparoscopic Colectomy. What do I need to know about my laparoscopic colorectal surgery?
 Laparoscopic Colectomy What do I need to know about my laparoscopic colorectal surgery? Traditionally, colon & rectal surgery requires a large, abdominal and/or pelvic incision, which often requires a
Laparoscopic Colectomy What do I need to know about my laparoscopic colorectal surgery? Traditionally, colon & rectal surgery requires a large, abdominal and/or pelvic incision, which often requires a