East Midlands Ambulance Service
|
|
|
- Shanon Lambert
- 8 years ago
- Views:
Transcription
1 Appendix 1 East Midlands Ambulance Service New Service Delivery Model Summary Document Trust Executive Board 05 April 2012

2 Contents Introduction The Strategic Context Overview Objectives Next Steps High Level Workforce Transition Plan Year 1 (2012/2013)

3 Introduction The East Midlands Ambulance Service as an aspirational Foundation Trust is embarking upon a significant programme of transformation which will ultimately see a change to the way in which it provides unscheduled health care to the population of the East Midlands. The existing model of service delivery is not clinically led and focussed on the highest standards of clinical excellence and quality as it is designed with the primary focus of achieving performance standards. The Secretary of State announced in December 2010 the introduction of the Clinical Quality Indicators for the ambulance service which came in to effect from April This set of 11 indicators replaced the Category B, 19-minute response time target and supported a move to measure the performance of the ambulance service on what matters most to patients quality and patient outcomes. The existing very traditional model of delivery lacks the required versatility and to continue with the concept of sending any type of resource to an emergency call is not clinically appropriate nor is it affordable with high staff and vehicular costs. Alongside a traditional model of service delivery the divisional management teams are primarily operationally focussed and do not focus sufficiently on clinical leadership or staff welfare. To support a new model of operational delivery the development of an Urgent Care Hub within the Emergency Operations Centre linked through a single point of access is pivotal to the success factor of the transformation programme. Within the Emergency Operations Centre a growth within our clinical assessment ability will support service provision through numbers of patients assessed and discharged over the phone (Hear & Treat) and a significant number of patients referred to alternative care providers (Hear & Refer). The relative reduction in response volumes required will allow the most appropriate resource to be sent to the patient supporting the ethos of Right Care, Right Time, Right Place whilst allowing the Ambulance Service to develop its service model around the requirements of its service users. Critical success factors will need to be achieved to support to new service delivery model including;- Increasing productivity through reduced call cycle times Reducing sickness absence levels Full rota review to create UCA crews and flexibility through 8, 10 &12 hour rota s Benefit realisation of the Resource Management Centre Getting the best leaders that can transact the change Communications and engagement with staff Reviewing the existing estates footprint to develop a new Hub and Spoke model. Reviewing the types and numbers of Trust response vehicles including where appropriate, vehicles which can carry multiple patients. Delivery of performance and quality targets 3

4 1. The Strategic Context 1.1 National Context The Government has embarked on a fundamental reform of the NHS, which will see the responsibility for the commissioning of ambulance services transfer from primary care trusts to GP consortia. These reforms are being introduced at a time when the NHS faces the tightest financial settlement in many years and when the Government aims to deliver up to 20 billion of efficiency savings in the NHS by the end of The ambulance service is expected to play a part in achieving these savings by identifying a minimum of 4 per cent efficiency savings within its budget (around 75 million per year). The ambulance service provides a life-saving service to some patients, is highly regarded by the public, and rightly remains committed to providing a rapid response to urgent and emergency calls at a time of steadily growing call volumes. But, until April 2011, the Department s emphasis on response time as a measure of performance rather than on a more rounded view of clinical outcomes, meant that the incentive structure did not encourage resource optimisation which resulted in little change to the traditional model of service delivery. A number of government plans require the contribution of ambulance services to meet NHS system-wide objectives. Examples include the Government s 10 year NHS Plan published in 2000, the NHS planning and governance framework Standards for Better Health published in July 2004, the Department of Health s National Ambulance Review Taking Healthcare to the Patient: Transforming NHS Ambulance Services published in June 2005 (and 2011) and the Health White Paper Our Health, Our Care, Our Say published in February The follow up review to Taking Healthcare to the Patient National Strategy for Ambulance Services, published in 2011, provided further recommendations, including:- Developing more visible, clinical leadership to support the more complex clinical challenges and an increase in hear and treat and see and treat are supported through high quality clinical leadership and mentoring. Adjusting the Category A target to allow time to gather key patient condition information before dispatching a resource, whilst at the same time protecting existing world class 999 call answering times. Maintaining national compliance with performance measuring whilst ensuring calls to cardiac arrests are singled out to receive the absolute fastest response. On 1 April 2011 new national targets were introduced with the emphasis no longer solely on speed of response. The key national target for Ambulance Trusts remains as maintaining response time performance of reaching 75% of patients with conditions prioritised as Category A within 8 minutes and providing a transport resource to patients within 19 minutes. EMAS must work with their patients and the public to ensure that the services can respond appropriately to all patients. This will require a revised approach to the traditional operational service delivery models. 4

5 1.2 Regional Context The East Midlands Ambulance Service (EMAS) provides emergency and urgent care, patient transport, call handling and clinical assessment services for 4.8 million people in an area covering approximately 6,425 square miles across the six counties of Derbyshire, Nottinghamshire, Lincolnshire, Northamptonshire, Leicestershire and Rutland. EMAS operate a fleet of around 780 vehicles, including emergency ambulances, fast response cars, specialised vehicles and patient transport vehicles. Our overall annual budget is 158 million. Every day, around 2,000 calls from members of the public calling 999 are received. In November, December 2010 and periods within January 2011, the region experienced dramatic and severe weather conditions and a significant increase in demand due to flulike symptoms which affected many people across the region. As a result of these events, and despite urgent management action, EMAS failed to achieve national performance targets for the year. Beyond the Trust s immediate urgent and emergency market exists a wider local health economy, which must be understood not only to realise the Trust s business position in its healthcare market, but also to understand the impact that the local health economy has on demand for Ambulance services. Firstly, in order to establish what encompasses the Trust s local healthcare economy, the Trust s current service provision is considered. The majority of EMAS services are provided for the East Midlands, excluding some mobile healthcare and specialist services which can cross regional boundaries. Therefore, the Trust s local health economy is considered to be the East Midlands, covering the six counties of Derbyshire, Leicestershire, Lincolnshire, Nottinghamshire, Northamptonshire and Rutland. The six East Midlands counties that EMAS serves currently have their healthcare services commissioned by six PCT clusters, made up of eleven PCTs. Whilst these commissioning organisations include NHS Milton Keynes as a member of the Northamptonshire and Milton Keynes Cluster, EMAS does not provide an emergency service to Milton Keynes and so this area is excluded from further regional consideration. Bearing this in mind, healthcare services within the EMAS region are provided by eleven acute trusts, seven mental health trusts and a large number of GP practices and community health providers (eight of these organisations are foundation trusts). Each organisation and the county in which it sits has its own identity and aims to address its own local healthcare agenda. This diversity of agendas adds to the complexity of requirements that EMAS fulfils. At present the Trust s requirements are also very dynamic due to the changing commissioner landscape in the region, and the resultant development of twenty six Clinical Commissioning Groups (CCGs) across the region, including North and North East Lincolnshire PCTs and excluding Milton Keynes PCT. The full impact of these new CCGs is yet to be realised as they are still very much at the development stage. However, the CCGs will bring a great variety of differing perspectives and levels of understanding regarding EMAS services, meaning that the Trust must continue to engage with and educate these new organisations. Furthermore, the CCGs are likely to create a more localised commissioning environment, which may change the way that EMAS promotes its services to increase its market share. To manage the regional commissioning transition and to provide some consistency of engagement with the emerging commissioners, the regional business hub has been replaced with the East Midlands Procurement and Collaborative Transformation team (EMPACT). EMPACT was established in 2010 and serves the East Midlands 11 PCTs. 5

6 This organisation has acted on behalf of the East Midlands commissioners to procure the regional non emergency patient transport services and manage the transactional contract for 999 emergency services. The regional commissioning landscape is also changing further due to the increased role that local authorities will have in terms of public health. The introduction of local health and wellbeing boards will bring together commissioner interests across the NHS, public health and social care. As such, EMAS will have to engage with a wider pool of commissioners and satisfy a broader range of interests. With regards to the population living in the region that the Trust primarily serves, the East Midlands is characterised by a generally poor level of health when compared with the rest of England, based on the most recent relevant health indicators from the UK Public Health Observatories (Reference: Within the East Midlands there are some areas of severe deprivation and significant resultant health needs, which may dictate some of the demand for EMAS services. Aside from the general health profile of the East Midlands population, other factors that will affect EMAS service demand are population growth and age. The East Midlands population is growing and an increasingly greater proportion of that population is of an older age, both of these factors will contribute to urgent and emergency service demand at EMAS. 2.3 Trust Strategic Context East Midlands Ambulance Service failed to achieve national ambulance response targets for the period 2009/10 and 2010/11 for Category A8 and B19 calls. In addition EMAS has also faced significant challenges in meeting clinical quality standards and maintaining a healthy financial balance. In the performance year 2011/12 EMAS is on target to achieve its A8 performance standard but will not achieve its A19 standard. Sub-standard performance is unacceptable to a Trust which aspires to achieve Foundation Trust status and deliver the highest quality care possible. The current service delivery model structure is based upon historic principles of ambulance service delivery. As a result of the higher volume of calls and transformations of NHS services, the current model is no longer offering value for money or achieving performance standards. EMAS recognises that it needs to significantly change its approach to the way in which it serves the region and as such is now commencing a significant programme of transformation starting with a change to its service delivery model. 6

7 2. Overview 2.1 Current The current model offers one level of response to all types of calls, regardless of clinical need. The aim of the current service delivery model is to provide a paramedic on every frontline vehicle, sending the nearest available resource, as fast as possible to deliver patient care. Highly skilled clinical staff are required to deal with routine work which would be more appropriately dealt with by an alternative role which would therefore free up Paramedics to attend only the clinically appropriate calls ensuring that those in need receive the highest level of clinical care. The response includes:- Ambulance that is crewed by a Paramedic and an Ambulance Technician or an Emergency Care Assistant (ECA). Fast Response Vehicles crewed by a Paramedic Fast Response Vehicles crewed by an Emergency Care Practitioner 2.2 Proposed The Trust is proposing a new service delivery model that will be based on three levels of response implemented by 2014 with continued development over the lifetime of the integrated business plan (see table below). Resource Type Skill Level Level 1 Response Urgent Care Ambulance Double Emergency Care Assistant Level 2 Response Level 3 Response Paramedic Fast Response Vehicle Paramedic Ambulance Emergency Care Practitioner Paramedic Paramedic and Emergency Care Assistant/Technician Emergency Care Practitioner The Level 1 response is the Urgent Care Ambulance (UCA) that is crewed by two Emergency Care Assistants (ECA s) and is designed to provide flexible transport for patients who do not require paramedic care but do need transporting to hospital within timescales agreed by a healthcare professional (Doctor, ECP, nurse or paramedic). All UCA s will have a bariatric capability, be able to transport retrieval teams and their equipment and provide an immediate response to life threatening calls. Level 1 vehicles will still have the ability to respond to life threatening category A calls in a first response capacity if they were the nearest available vehicle. 7

8 The Level 2 response has two elements to it, firstly the Paramedic Fast Response Vehicle, which is crewed by a solo Paramedic, providing an immediate response to life threatening calls where the speed of the response is key. The fast response paramedics will assess patients and determine the most appropriate care pathway, which includes See and Treat (SAT), See and Refer (SAR), which includes referral to an Emergency Care Practitioner, and treat and leave at home. It is anticipated that FRV s will primarily respond to Category A calls although as part of an agreed over capacity plan they may be utilised to attend alternative calls. The emphasis of the FRV is to attend the high acuity patients ensuring patients with the greatest need receive a rapid response. The second element is the Paramedic Ambulance, crewed by a paramedic and ECA/Technician, and is designed to respond to 999 calls which require paramedic care. Paramedic ambulances will provide the core response to the majority of 999 calls that are assessed as requiring an immediate response. Paramedics will assess patients and determine the most appropriate care pathway which includes SAT, SAR, and treat and leave at home. The Level 3 response, the Emergency Care Practitioner (ECP), provides a response to calls that have been assessed through the urgent care hub as requiring a response where further clinical assessment is likely, with the intention that patients will be treated at home or appropriately referred to another healthcare professional such as a GP or district nurse. ECP s would still be able to respond to the full range of calls although their primary focus would be around hospital avoidance. The emphasis of mobile healthcare is to send the right resource first time to meet the individual patient s needs with clinical assessment at each stage to determine the most appropriate care pathway and avoid unnecessary attendances at A&E departments and subsequent admissions, with the speed of response and quality of care top priorities. To achieve this staff will have to be matched to the three levels of response. This level of change will require transformation of the existing operational workforce including skill mix ratios of staff to support operational tiers and new operational rotas which are aligned to demand for our services. Technology exists to accurately predict the expected number of calls over a period of time which in conjunction with a unit hour utilisation methodology (UHU) allows the organisation to design a rota system which is flexible to anticipated changes such as seasonal variation. 8

9 Level 2 Response (FRV/DCA) Immediate Response Hear & Treat Hear & Refer Calls (999) Urgent Care Hub Clinical Assement Level 2 Response (FRV/DCA) Call Closed Through DoS Level 3 Response (ECP) Level 1 Response (UCA) 3. Objectives 3.1 Key Objectives The Key objectives of the proposed service delivery model are:- Sending the most appropriate resource to best meet patient needs To deliver against all performance standards. To constantly achieve the highest standards in Ambulance Quality Indicators To improve systems for inter hospital transfers To treat more patients at home - See and Treat. To refer more patients to other health care professionals such as GPs or district nurses or referring patients for admission using the most appropriate care pathway and avoiding attendance at A&E departments See and Refer. To reduce unnecessary conveyances to A&E To use resources more efficiently providing value for money 9

10 4.2 Benefits Trust Wide NHS & Other Stakeholders Public & Patient Flexible and demand responsive It is clinically focussed and clinically led It is affordable It will deliver performance standards More effective use of ECP s Part of an integrated operations model Reduction in handover times Potential reduction in Journey Times Staff development and motivation Delivering on performance targets Delivering on all quality standards More flexible service delivery model Increased cost efficiency Increased non conveyance to A&E departments Lower cost setting for attendance Reduction in Hospital Admissions It will deliver the highest quality of care Improved patient outcomes More timely response More appropriate response Improved patient experience Care closer to home Improved convenience and choice Shorter treatment times More coordinated patient service Care closer to home 3.2 Conclusion EMAS is on track to deliver Category A8 for the performance year 2011/12. A19 is not achievable this year; however planned improvements will have a significant impact during 2012/13. There will still however be a performance gap, and commissioner support to undertake a joint independent county by county review of demand and capacity to establish a baseline for future commissioning. EMAS has seen a year on year increase in both calls and responses over the past ten years; from 2007/2008 to 2010/2011 EMAS has seen a 21% increase in Category A responses alone with a further 12% increase over the past 12 months. It is anticipated through service changes alongside an increase in clinical assessment of calls that although call volume will continue to rise the actual responses will remain fairly static. 10

11 In terms of Category A volumes the Card 33 changes and then the changes to the national targets on 1 st April 2011 when Category B was removed has meant an increase on average of 2,300 more responses per month than prior to this date. EMAS is also seeing a dramatic change to its activity profile, with Saturday and Sunday now been the busiest days of the week for example the average number of Category A responses per day is between 560 and 590 compared to the average weekend day with 650 to 800 responses. There are clear links to 111 activity which significantly increases at weekends, however further analysis is still required. To ensure the changes are successful a full engagement strategy and planner will need to be put in place. This will be both internal and external facing and to do this effectively a full stakeholder mapping exercise will be completed and linked directly to all communications. Using engagement, all key audiences should develop a comprehensive understanding of the reasoning for change and a focus on the objectives we need to achieve. Proactive communications and presenting the change as a priority which affects everybody will ensure that colleagues will actively engage with the process and in turn make the end result a success. Together with this, the narrative used will be in line with the motivations of the different audiences and expressed in a clear manner, according to shared understanding. We will have open and honest communications on the issues we face whilst maintaining a culture of openness and inclusion. 11

12 4. Next Steps A series of scoping sessions will ensure that the project managers from each individual work streams will be supported to deliver against clear timescales. The flowchart below describes how the individual groups will report in and be accountable to the Transformation Delivery Group which will ensure delivery of the whole programme of transformation. TRANSFORMATION DELIVERY GROUP SINGLE POINT OF ACCESS -Pathways -111 URGENT CARE HUB TELEHEALTH NEW MODEL FLEET WORKFORCE -Professionalism of the workforce ESTATES SERVICE LINE MANAGEMENT -Productivity -CIP The programme of change will commence in April 2012 adhering to structured timescales. Quarter 1 - deliver performance standards linking to the Improving Service Delivery plan. 1 It is imperative that the Trust delivers against its key performance indicators whilst undergoing the change programme, this ensures that we provide the highest standards to our service users. Quarter 1 - Commence consultation on rota reviews to support the new service delivery model whilst ensuring that the levels of required resources accurately reflect the demand profiles of the business. Quarter 1 Alignment of all supporting strategies to the new service delivery model including the Estates and Fleet. Quarter 3 - Commence consultation on management structure changes 1 Tabled at Trust Board April 5 th

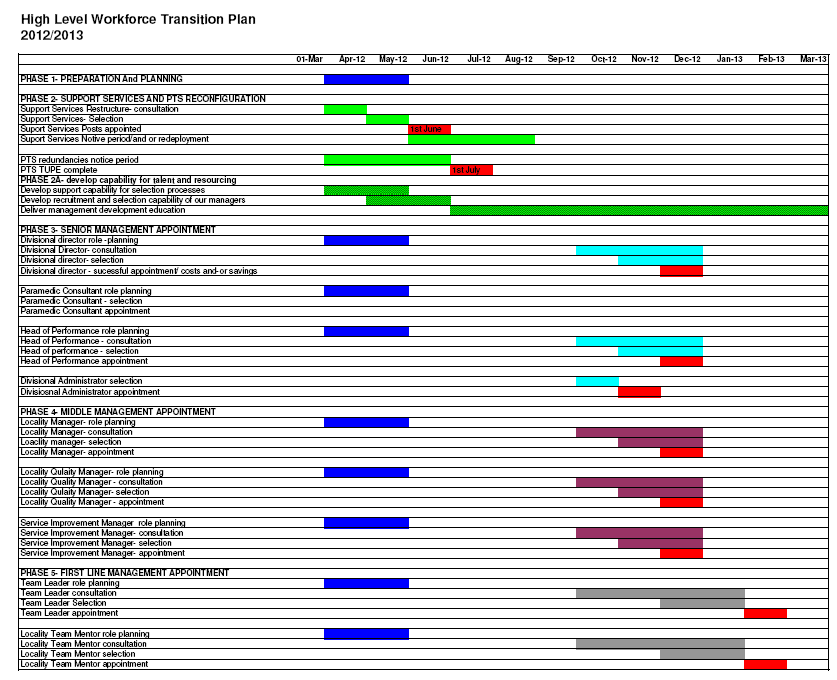
13 5. High Level Workforce Transition Plan Year 1 (2012/2013) The Workforce Transition Plan aims to achieve a full operational management restructure in post by 31 st March The time scale has been proposed to take into account the internal resource capabilities and capacity to deliver change whilst continuing with a management development programme to start to identify talent and embed leadership capabilities across front line and middle manager roles. The scope focuses on the workforce transition that includes: TUPE of PTS staff Reconfiguration of support services in response to the loss of the PTS contract Operational management restructure Operational workforce modelling Key goals of the Work force Strategy are to: Deliver robust and compliant workforce planning to embed a model of organisational development Best practice HRM Excellence in education, training and development Develop talent in our organisation and plan succession into key roles Transformation to a new service model and operational management structure to deliver a culture of staff recognition, supportive management behaviour, positive team working and interpersonal relations; employee involvement and participation, empowered and engaged and well supported staff PHASE ANNUAL PLAN OBJECTIVE WORKFORCE AND FINANCIAL CHANGE April 2012 PHASE 1- PLANNING Deliver a workforce plan to enable transformation to a new service model and operational management structure that ensures business continuity. Commence consultation on operational rota changes which will support the development of 3 tiers of deliver April- 31 st August 2012 PHASE 2- SUPPORT SERVICES AND PTS PHASE 2a- TALENT MANAGEMENT, RESOURCING & EDUCATION TUPE of PTS. Reconfiguration of support service in response to the loss of PTS Develop our people to strengthen our recruitment decision making and ensure that we attract and retain the right people NUMBERS LOSS OF circa 51 support staff TUPE of circa 500 PTS staff FINANCE Financial saving circa 1.5M 13

14 October 2012 PHASE 3 SENIOR MANAGEMENT Consultation Divisional Directors, Paramedic Consultants, Heads of Performance Align the management development education to promote leadership capabilities, staff engagement, talent management and succession planning, increase the quality of appraisal Suggested pool : Existing divisional ADOs, 8b level project managers, other senior level staff. NUMBERS 5 ADO level staff, plus 4 at risk for x3 DD, x3pc, x3 HoP FINANCE Saving circa 140k assuming 5 ADO:3 October 2012 PHASE 4 MIDDLE MANAGEMENT Consultation Locality Managers, Divisional Quality Managers, Service Improvement Manager Align the management development education to promote leadership capabilities, staff engagement, talent management and succession planning, increase the quality of appraisal Suggested pool: Existing SDMs, OSMs NUMBERS 48 staff for 17posts FINANCE saving circa 300k October 2012 PHASE 5 FIRST LINE MANAGER Consultation Team Leaders, Team Mentors Align the management development education to promote leadership capabilities, staff engagement, talent management and succession planning, increase the quality of appraisal Suggested pool: Fall out from phase 4 plus existing PTLs NUMBERS : 31 from phase 4 plus 120 PTLs for 120 posts FINANCE saving circa 1.9m 14

15 Key transition stages showing broad considerations and assumptions PLAN CONSULT SELECTION APPOINTMENT Establish project group and define scope and secure appropriate resources Devise consultation plan Draw up communications plan - internal and external stakeholders Prepare Job Descriptions and indicative bandings Clarify scope of practice/competencies/d ecision making rights required for each role Agree selection pools and processes and anticipate educational requirements by role Take forward consultation process Review and revise job descriptions/ selection criteria/pools as result of consultation Review and /or secure capacity/ resource to deliver (eg assessment centres) Review business continuity plans and risk management Revise and communicate any changes Undertake selection process Confirm successful and unsuccessful appointees Provide support mechanism for displaced staff Confirm suitable alternative arrangements on an individual basis Revise and communicate any changes Transact all employee changes - particular focus for Human Resources, Education and Development Devise individual education plans for new appointees in relation to gaps identified through selection process Revise and communicate any changes Clarification of legal implications Detailed financial modelling Propose what is and is not suitable alternative employment 15
 Review business continuity plans and risk management Revise and communicate any changes Undertake selection")
16

East Midlands Ambulance Service NHS Trust. Service Delivery Model
 East Midlands Ambulance Service NHS Trust Service Delivery Model EXECUTIVE SUMMARY This paper outlines the new service operating model proposed for East Midlands Ambulance Service NHS Trust which has the
East Midlands Ambulance Service NHS Trust Service Delivery Model EXECUTIVE SUMMARY This paper outlines the new service operating model proposed for East Midlands Ambulance Service NHS Trust which has the
A vision for the ambulance service: 2020 and beyond and the steps to its realisation
 A vision for the ambulance service: 2020 and beyond and the steps to its realisation September 2015 Introduction This document outlines the English ambulance sector s vision for 2020 and beyond, and the
A vision for the ambulance service: 2020 and beyond and the steps to its realisation September 2015 Introduction This document outlines the English ambulance sector s vision for 2020 and beyond, and the
South East Coast Ambulance Service NHS Foundation Trust
 South East Coast Ambulance Service NHS Foundation Trust Emergency and Urgent Care in Kent and Medway for Kent HOSC What does SECAmb do? South East Coast Ambulance Service NHS Foundation Trust is an innovative,
South East Coast Ambulance Service NHS Foundation Trust Emergency and Urgent Care in Kent and Medway for Kent HOSC What does SECAmb do? South East Coast Ambulance Service NHS Foundation Trust is an innovative,
Clinical Hubs and UCS
 Clinical Hubs and UCS Clinical Hub Staff Development Traditionally Clinical Hub staff join the Trust as call handlers and progress to dispatcher roles. Recent changes to Hub structure brought about by
Clinical Hubs and UCS Clinical Hub Staff Development Traditionally Clinical Hub staff join the Trust as call handlers and progress to dispatcher roles. Recent changes to Hub structure brought about by
Leicestershire Partnership Trust. Leadership Development Framework
 Leicestershire Partnership Trust Leadership Development Framework 1 Leadership Development Framework Introduction The NHS in England is facing a period of substantial change in light of the recent Government
Leicestershire Partnership Trust Leadership Development Framework 1 Leadership Development Framework Introduction The NHS in England is facing a period of substantial change in light of the recent Government
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Delivering Local Integrated Care Accelerating the Pace of Change WG 17711 Digital ISBN 978 1 0496 0 Crown copyright 2013 2 Contents Joint foreword
Delivering Local Health Care Accelerating the pace of change Delivering Local Integrated Care Accelerating the Pace of Change WG 17711 Digital ISBN 978 1 0496 0 Crown copyright 2013 2 Contents Joint foreword
Changing health and care in West Cheshire The West Cheshire Way
 Changing health and care in West Cheshire The West Cheshire Way Why does the NHS need to change? The NHS is a hugely important service to patients and is highly regarded by the public. It does however
Changing health and care in West Cheshire The West Cheshire Way Why does the NHS need to change? The NHS is a hugely important service to patients and is highly regarded by the public. It does however
Appendix 1 Business Case to Support the Relocation of Mental Health Inpatient Services in Manchester (Clinical Foreword and Executive Summary)
") Appendix 1 Business Case to Support the Relocation of Mental Health Inpatient Services in Manchester (Clinical Foreword and Executive Summary) Together we are better Foreword by the Director of Nursing
Appendix 1 Business Case to Support the Relocation of Mental Health Inpatient Services in Manchester (Clinical Foreword and Executive Summary) Together we are better Foreword by the Director of Nursing
An Introduction to our Services
 An Introduction to our Services Ambulance services are at the front line of the NHS. That s why, at Yorkshire Ambulance Service (YAS), we put patients and their needs at the heart of everything we do.
An Introduction to our Services Ambulance services are at the front line of the NHS. That s why, at Yorkshire Ambulance Service (YAS), we put patients and their needs at the heart of everything we do.
The importance of nurse leadership in securing quality, safety and patient experience in CCGs
 Briefing note: July 2012 The importance of nurse leadership in securing quality, safety and patient experience in CCGs Introduction For the NHS to meet the challenges ahead, decisions about health services
Briefing note: July 2012 The importance of nurse leadership in securing quality, safety and patient experience in CCGs Introduction For the NHS to meet the challenges ahead, decisions about health services
REPORT OF THE VICE-CHAIRMAN OF JOINT CITY AND COUNTY HEALTH SCRUTINY COMMITTEE
 Report to Joint City and County Health Scrutiny Committee 14 January 2013 Agenda Item: REPORT OF THE VICE-CHAIRMAN OF JOINT CITY AND COUNTY HEALTH SCRUTINY COMMITTEE EAST MIDLANDS AMBULANCE SERVICE BETTER
Report to Joint City and County Health Scrutiny Committee 14 January 2013 Agenda Item: REPORT OF THE VICE-CHAIRMAN OF JOINT CITY AND COUNTY HEALTH SCRUTINY COMMITTEE EAST MIDLANDS AMBULANCE SERVICE BETTER
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY COUNCIL OF GOVERNORS 2 ND DECEMBER 2014
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST C EXECUTIVE SUMMARY COUNCIL OF GOVERNORS 2 ND DECEMBER 2014 Subject: Supporting Director: Author: Status 1 NHS England Five Year Forward View A Summary
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST C EXECUTIVE SUMMARY COUNCIL OF GOVERNORS 2 ND DECEMBER 2014 Subject: Supporting Director: Author: Status 1 NHS England Five Year Forward View A Summary
Research is everybody s business
 Research and Development Strategy (DRAFT) 2013-2018 Research is everybody s business 1 Information Reader Box to be inserted for documents six pages and over. (To be inserted in final version, after consultation
Research and Development Strategy (DRAFT) 2013-2018 Research is everybody s business 1 Information Reader Box to be inserted for documents six pages and over. (To be inserted in final version, after consultation
THE QUALITY OF CARE IN. North Lincolnshire. CQC prototype report
 THE QUALITY OF CARE IN North Lincolnshire CQC prototype report February 2016 Quality of care in a place Quality of care in a place The Care Quality Commission is producing a number of prototype documents
THE QUALITY OF CARE IN North Lincolnshire CQC prototype report February 2016 Quality of care in a place Quality of care in a place The Care Quality Commission is producing a number of prototype documents
Review of Non-Emergency Patient Transport Service in Bassetlaw
 BASSETLAW DISTRICT COUNCIL Agenda Item No. HEALTH AND PUBLIC SERVICES SUB-COMMITTEE 10 MARCH 2014 Review of Non-Emergency Patient Transport Service in Bassetlaw The Health & Public Services Sub Committee
BASSETLAW DISTRICT COUNCIL Agenda Item No. HEALTH AND PUBLIC SERVICES SUB-COMMITTEE 10 MARCH 2014 Review of Non-Emergency Patient Transport Service in Bassetlaw The Health & Public Services Sub Committee
A fresh start for the regulation of ambulance services. Working together to change how we regulate ambulance services
 A fresh start for the regulation of ambulance services Working together to change how we regulate ambulance services The Care Quality Commission is the independent regulator of health and adult social
A fresh start for the regulation of ambulance services Working together to change how we regulate ambulance services The Care Quality Commission is the independent regulator of health and adult social
Medway Health and Adult Social Care Overview and Scrutiny Committee. Patient Transport Services
 Medway Health and Adult Social Care Overview and Scrutiny Committee Background Patient Transport Services NHS Kent and Medway agreed to tender the non emergency patient transport services in July 2011,
Medway Health and Adult Social Care Overview and Scrutiny Committee Background Patient Transport Services NHS Kent and Medway agreed to tender the non emergency patient transport services in July 2011,
Children s Trust Board Sponsor: Dr Kate Allen, Consultant in Public Health
 Report to Children s Trust Board 6 th November 2014 Agenda Item: 4 Children s Trust Board Sponsor: Dr Kate Allen, Consultant in Public Health NOTTINGHAMSHIRE SCHOOL NURSING SERVICE REVIEW IMPLICATIONS
Report to Children s Trust Board 6 th November 2014 Agenda Item: 4 Children s Trust Board Sponsor: Dr Kate Allen, Consultant in Public Health NOTTINGHAMSHIRE SCHOOL NURSING SERVICE REVIEW IMPLICATIONS
The Scottish Ambulance Service Improving Care, Reducing Costs. Working together for better patient care
 The Scottish Ambulance Service Improving Care, Reducing Costs Working together for better patient care Key points The Scottish Ambulance Service is seeing more people, faster, and offering better quality
The Scottish Ambulance Service Improving Care, Reducing Costs Working together for better patient care Key points The Scottish Ambulance Service is seeing more people, faster, and offering better quality
How To Write An Emnc Rehabilitation Strategy
 Delivering the Supportive and Palliative Care Improving Outcomes Guidance (IOG) across the East Midlands Priority 8 Rehabilitation Services Rehabilitation Strategy East Midlands Cancer Network 2010 Document
Delivering the Supportive and Palliative Care Improving Outcomes Guidance (IOG) across the East Midlands Priority 8 Rehabilitation Services Rehabilitation Strategy East Midlands Cancer Network 2010 Document
Big Chat 4. Strategy into action. NHS Southport and Formby CCG
 Big Chat 4 Strategy into action NHS Southport and Formby CCG Royal Clifton Hotel, Southport, 19 November 2014 Contents What is the Big Chat? 3 About Big Chat 4 4 How the event worked 4 Presentations 5
Big Chat 4 Strategy into action NHS Southport and Formby CCG Royal Clifton Hotel, Southport, 19 November 2014 Contents What is the Big Chat? 3 About Big Chat 4 4 How the event worked 4 Presentations 5
Ambulance Services Commissioning Update
 Joint Health Overview and Scrutiny Committee Great Western Ambulance Service 29 February 2008 Ambulance Services Commissioning Update 1. Purpose To update the Joint Health Overview and Scrutiny Committee
Joint Health Overview and Scrutiny Committee Great Western Ambulance Service 29 February 2008 Ambulance Services Commissioning Update 1. Purpose To update the Joint Health Overview and Scrutiny Committee
AMBULANCE SERVICES PATIENT FOCUSED SUPPORT. THERE WHEN YOU NEED US.
 AMBULANCE SERVICES PATIENT FOCUSED SUPPORT. THERE WHEN YOU NEED US. 2 ST JOHN AMBULANCE AMBULANCE SERVICES EXPERT PROVIDERS OF AMBULANCE SERVICES St John Ambulance is a leading supplier of ambulance services
AMBULANCE SERVICES PATIENT FOCUSED SUPPORT. THERE WHEN YOU NEED US. 2 ST JOHN AMBULANCE AMBULANCE SERVICES EXPERT PROVIDERS OF AMBULANCE SERVICES St John Ambulance is a leading supplier of ambulance services
Welsh Ambulance Services NHS Trust
 Welsh Ambulance Services NHS Trust Financial Support to replace obsolete Ambulance Vehicles 2008/09 BUSINESS JUSTIFICATION CASE Version No: Page 1 of 10 VERSION HISTORY Version Date Brief Summary of Change
Welsh Ambulance Services NHS Trust Financial Support to replace obsolete Ambulance Vehicles 2008/09 BUSINESS JUSTIFICATION CASE Version No: Page 1 of 10 VERSION HISTORY Version Date Brief Summary of Change
Integrating Health and Social Care in England: Lessons from Early Adopters and Implications for Policy
 Knowledge base Integrating Health and Social Care in England: Lessons from Early Adopters and Implications for Policy Chris Ham Professor of Health Policy and Management John Oldham Honorary Senior Fellow
Knowledge base Integrating Health and Social Care in England: Lessons from Early Adopters and Implications for Policy Chris Ham Professor of Health Policy and Management John Oldham Honorary Senior Fellow
Our Quality Account 2012/13
 1 Our Quality Account 2012/13 Contents Page Executive summary 3 A brief overview of our Trust (what we do) 7 Part 1 An introduction to our Quality Account (your definitions of quality) 12 Board Assurance
1 Our Quality Account 2012/13 Contents Page Executive summary 3 A brief overview of our Trust (what we do) 7 Part 1 An introduction to our Quality Account (your definitions of quality) 12 Board Assurance
Summary of Services NSL Non Emergency Patient Transport Service
 Summary of Services NSL n Emergency Patient Transport Service As from 1 st July 2012 for a period of 5 years NSL Care Services one of the UK s largest providers of patient transport services is to run
Summary of Services NSL n Emergency Patient Transport Service As from 1 st July 2012 for a period of 5 years NSL Care Services one of the UK s largest providers of patient transport services is to run
Children s Trust Board Sponsor: Dr Kate Allen, Consultant in Public Health NOTTINGHAMSHIRE SCHOOL NURSING SERVICE PROPOSED REMODELLING PLANS
 Report to Children s Trust Board 23 rd April 2015 Agenda Item: 2 Children s Trust Board Sponsor: Dr Kate Allen, Consultant in Public Health NOTTINGHAMSHIRE SCHOOL NURSING SERVICE PROPOSED REMODELLING PLANS
Report to Children s Trust Board 23 rd April 2015 Agenda Item: 2 Children s Trust Board Sponsor: Dr Kate Allen, Consultant in Public Health NOTTINGHAMSHIRE SCHOOL NURSING SERVICE PROPOSED REMODELLING PLANS
Financial Strategy 5 year strategy 2015/16 2019/20
 Item 4.3 Paper 15 Financial Strategy 5 year strategy 2015/16 2019/20 NHS Guildford and Waverley Clinical Commissioning Group Medium Term Financial Strategy / Finance and Performance Committee May 2015
Item 4.3 Paper 15 Financial Strategy 5 year strategy 2015/16 2019/20 NHS Guildford and Waverley Clinical Commissioning Group Medium Term Financial Strategy / Finance and Performance Committee May 2015
Informatics: The future. An organisational summary
 Informatics: The future An organisational summary DH INFORMATION READER BOX Policy HR/Workforce Management Planning/Performance Clinical Document Purpose Commissioner Development Provider Development Improvement
Informatics: The future An organisational summary DH INFORMATION READER BOX Policy HR/Workforce Management Planning/Performance Clinical Document Purpose Commissioner Development Provider Development Improvement
Supporting the development of ambulance services as out-of-hospital providers
 Supporting the development of ambulance services as out-of-hospital providers Richard Hunt CBE Chair, London Ambulance Service NHS Trust Representing the Association of Ambulance Chief Executives (AACE)
Supporting the development of ambulance services as out-of-hospital providers Richard Hunt CBE Chair, London Ambulance Service NHS Trust Representing the Association of Ambulance Chief Executives (AACE)
Tel: 020 8441 8122 Fax: 020 8447 3890 E: mail@patient-transport.co.uk
 Patient Transport (UK) LTD Leading the Private Ambulance Sector Tel: 020 8441 8122 Fax: 020 8447 3890 E: mail@patient-transport.co.uk Table of Contents Company Statement... 3 Company Values... 3 Services
Patient Transport (UK) LTD Leading the Private Ambulance Sector Tel: 020 8441 8122 Fax: 020 8447 3890 E: mail@patient-transport.co.uk Table of Contents Company Statement... 3 Company Values... 3 Services
A Route Map to the 2020 Vision for Health and Social Care
 A Route Map to the 2020 Vision for Health and Social Care 02 A Route Map to the 2020 Vision for Health and Social Care Introduction This paper sets out a new and accelerated focus on a number of priority
A Route Map to the 2020 Vision for Health and Social Care 02 A Route Map to the 2020 Vision for Health and Social Care Introduction This paper sets out a new and accelerated focus on a number of priority
Improving Emergency Care in England
 Improving Emergency Care in England REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1075 Session 2003-2004: 13 October 2004 LONDON: The Stationery Office 11.25 Ordered by the House of Commons to be printed
Improving Emergency Care in England REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1075 Session 2003-2004: 13 October 2004 LONDON: The Stationery Office 11.25 Ordered by the House of Commons to be printed
93 % c a re Q U a L i t Y c o m m i S S i o n
 W E H A V E O V E R 500 RE G I S T E RE D A M B U L A N C E S, 800 S T A FF M E M B E R S C O M P L E T I N G T E N S O F T H O U S A N D S O F P A T I E N T J O U R N E Y S E V E R Y W E E K, F R O M
W E H A V E O V E R 500 RE G I S T E RE D A M B U L A N C E S, 800 S T A FF M E M B E R S C O M P L E T I N G T E N S O F T H O U S A N D S O F P A T I E N T J O U R N E Y S E V E R Y W E E K, F R O M
RCN policy position. Executive Director of Nursing. RCN survey on PCT Executive Directors of Nursing. Rationale for an Executive Director of Nursing
 RCN Policy Position Executive Director of Nursing Part 1: Part 2: Part 3: Part 4: Part 5: Part 6: Part 7: Part 8: RCN policy position RCN survey on PCT Executive Directors of Nursing Rationale for an Executive
RCN Policy Position Executive Director of Nursing Part 1: Part 2: Part 3: Part 4: Part 5: Part 6: Part 7: Part 8: RCN policy position RCN survey on PCT Executive Directors of Nursing Rationale for an Executive
Supporting information pack
 Supporting information pack The new commissioning system As part of the modernisation of the NHS, a number of changes to how health services are managed came into effect from April 2013. Primary Care Trusts
Supporting information pack The new commissioning system As part of the modernisation of the NHS, a number of changes to how health services are managed came into effect from April 2013. Primary Care Trusts
Lesley MacLeod, Interim Chief Finance Officer. Commercially Sensitive For the Public or Private Agenda To be publically available via the CCG Website
 Subject: Financial Planning 2015-16 Meeting: NHS Milton Keynes CCG Board Date of Meeting: 27 th January 2015 Report of: Lesley MacLeod, Interim Chief Finance Officer Is this document: Commercially Sensitive
Subject: Financial Planning 2015-16 Meeting: NHS Milton Keynes CCG Board Date of Meeting: 27 th January 2015 Report of: Lesley MacLeod, Interim Chief Finance Officer Is this document: Commercially Sensitive
Report by Director of Health and Social Care Commissioning and Interim Director of Joint Commissioning
 Agenda Item No. 5 Policy and Resources Select Committee 21 February 2013 Progress Report on the Joint Commissioning Unit Report by Director of Health and Social Care Commissioning and Interim Director
Agenda Item No. 5 Policy and Resources Select Committee 21 February 2013 Progress Report on the Joint Commissioning Unit Report by Director of Health and Social Care Commissioning and Interim Director
WA Health Patient Transport Strategy 2015-2018
 WA Health Patient Transport Strategy 2015-2018 health.wa.gov.au Table of Contents Executive Summary 2 WA Health Patient Transport Strategy Framework 3 WA Health Patient Transport Strategy Action Plan 4
WA Health Patient Transport Strategy 2015-2018 health.wa.gov.au Table of Contents Executive Summary 2 WA Health Patient Transport Strategy Framework 3 WA Health Patient Transport Strategy Action Plan 4
Patient Choice Strategy
 Patient Choice Strategy Page 1 of 14 Contents Page 1 Background 4 2 Putting Patients and the Public at the Heart of Health and 5 Healthcare in West Lancashire 3 Where are we now and where do we need to
Patient Choice Strategy Page 1 of 14 Contents Page 1 Background 4 2 Putting Patients and the Public at the Heart of Health and 5 Healthcare in West Lancashire 3 Where are we now and where do we need to
Commissioning Policy (EMSCGP005V2) Defining the boundaries between NHS and Private Healthcare
 Defining the boundaries between NHS and Private Healthcare") Commissioning Policy (EMSCGP005V2) Defining the boundaries between NHS and Private Healthcare Although Primary Care Trusts (PCTs) and East Midlands Specialised Commissioning Group (EMSCG) were abolished
Commissioning Policy (EMSCGP005V2) Defining the boundaries between NHS and Private Healthcare Although Primary Care Trusts (PCTs) and East Midlands Specialised Commissioning Group (EMSCG) were abolished
Medical Services Putting patients first. www.medicalservicesuk.com
 Medical Services Putting patients first We remain the most experienced and longest serving provider of patient transport services. Values In the UK we remain the most experienced and longest serving provider
Medical Services Putting patients first We remain the most experienced and longest serving provider of patient transport services. Values In the UK we remain the most experienced and longest serving provider
Rehabilitation Network Strategy 2014 2017. Final Version 30 th June 2014
 Rehabilitation Network Strategy 2014 2017 Final Version 30 th June 2014 Contents Foreword 3 Introduction Our Strategy 4 Overview of the Cheshire and Merseyside Rehabilitation Network 6 Analysis of our
Rehabilitation Network Strategy 2014 2017 Final Version 30 th June 2014 Contents Foreword 3 Introduction Our Strategy 4 Overview of the Cheshire and Merseyside Rehabilitation Network 6 Analysis of our
(Health Scrutiny Sub-Committee 10 March 2008)
") Somerset County Council Health Scrutiny Sub-Committee 10 March 2008 (Health Scrutiny Sub-Committee 10 March 2008) Non-Emergency Transport for Health Patients in Somerset Lead Officer: Keith Wiggins, Scrutiny
Somerset County Council Health Scrutiny Sub-Committee 10 March 2008 (Health Scrutiny Sub-Committee 10 March 2008) Non-Emergency Transport for Health Patients in Somerset Lead Officer: Keith Wiggins, Scrutiny
NHS continuing healthcare. Detailing what NHS organisations need to know and do. Background
 briefing November 2012 Issue 256 NHS continuing healthcare Detailing what NHS organisations need to know and do Key points From April 2013, CCGs will be legally responsible for commissioning and assessing
briefing November 2012 Issue 256 NHS continuing healthcare Detailing what NHS organisations need to know and do Key points From April 2013, CCGs will be legally responsible for commissioning and assessing
Dual diagnosis: a challenge for the reformed NHS and for Public Health England
 Dual diagnosis: a challenge for the reformed NHS and for Public Health England A discussion paper from Centre for Mental Health, DrugScope and UK Drug Policy Commission The extent and significance of dual
Dual diagnosis: a challenge for the reformed NHS and for Public Health England A discussion paper from Centre for Mental Health, DrugScope and UK Drug Policy Commission The extent and significance of dual
briefing An involving service Ambulance responses in urban and rural areas Background Key points November 2011 Issue 226
 briefing November 2011 Issue 226 An involving service Ambulance responses Key points Patients, rightly, expect a high level of service, wherever they live. Trusts need to address the public s expectation
briefing November 2011 Issue 226 An involving service Ambulance responses Key points Patients, rightly, expect a high level of service, wherever they live. Trusts need to address the public s expectation
Patient Transport Services (PTS) Eligibility Criteria Implementation OVERVIEW AND SCRUTINY COMMITTEE Briefing Paper
 Eligibility Criteria Implementation OVERVIEW AND SCRUTINY COMMITTEE Briefing Paper") 1. Introduction Patient Transport Services (PTS) Eligibility Criteria Implementation OVERVIEW AND SCRUTINY COMMITTEE Briefing Paper This briefing paper seeks to inform Overview and Scrutiny Committees
1. Introduction Patient Transport Services (PTS) Eligibility Criteria Implementation OVERVIEW AND SCRUTINY COMMITTEE Briefing Paper This briefing paper seeks to inform Overview and Scrutiny Committees
STAFFORDSHIRE HEALTH OVERVIEW SCRUTINY MEETING 8 April 2015
 STAFFORDSHIRE HEALTH OVERVIEW SCRUTINY MEETING 8 April 2015 The last year as proved to be a very challenging year for the West Midlands Ambulance Service both regionally and within Staffordshire. Challenges
STAFFORDSHIRE HEALTH OVERVIEW SCRUTINY MEETING 8 April 2015 The last year as proved to be a very challenging year for the West Midlands Ambulance Service both regionally and within Staffordshire. Challenges
Board of Directors Meeting
 Board of Directors Meeting 23 rd July 2014 (BDA/14/26) part Performance Report Monitor Key Indicators Status: A Paper for Information History: Amanda Pritchard Chief Operating Officer Page 1 of 10 Performance
Board of Directors Meeting 23 rd July 2014 (BDA/14/26) part Performance Report Monitor Key Indicators Status: A Paper for Information History: Amanda Pritchard Chief Operating Officer Page 1 of 10 Performance
Strategy & Business Plan 2008-2011
 South Central Ambulance Service NHS Trust Strategy & Business Plan 2008-2011 1 CONTENTS 1.0 Introduction 1.1 Structure Business Plan 2.0 Trust Profile 2.1 Development of the Strategy and Business Plan
South Central Ambulance Service NHS Trust Strategy & Business Plan 2008-2011 1 CONTENTS 1.0 Introduction 1.1 Structure Business Plan 2.0 Trust Profile 2.1 Development of the Strategy and Business Plan
Inspection of Mental Health Division. 4 November 2013
 Inspection of Mental Health Division 4 November 2013 Introduction: The Inspectorate of Mental Health Services had long advocated for the introduction of a HSE Mental Health Directorate with Executive and
Inspection of Mental Health Division 4 November 2013 Introduction: The Inspectorate of Mental Health Services had long advocated for the introduction of a HSE Mental Health Directorate with Executive and
JOB DESCRIPTION. TITLE: Corporate Property Manager SALARY RANGE: 55,000-70,000
 TITLE: Corporate Property Manager SALARY RANGE: 55,000-70,000 JOB DESCRIPTION DEPARTMENT: Property Management Services REGION: North East / North West / Midlands / London / South ACCOUNTABILITIES: The
TITLE: Corporate Property Manager SALARY RANGE: 55,000-70,000 JOB DESCRIPTION DEPARTMENT: Property Management Services REGION: North East / North West / Midlands / London / South ACCOUNTABILITIES: The
People Strategy 2013/17
 D a t a L a b e l : P U B L I C West Lothian Council People Strategy 2013/17 Contents 1 Overview 2 2 Council Priorities 8 3 Strategy Outcomes 10 1 Engaging and motivating our employees 13 2 Recognised
D a t a L a b e l : P U B L I C West Lothian Council People Strategy 2013/17 Contents 1 Overview 2 2 Council Priorities 8 3 Strategy Outcomes 10 1 Engaging and motivating our employees 13 2 Recognised
The Way Forward: Strategic clinical networks
 The Way Forward: Strategic clinical networks The Way Forward Strategic clinical networks First published: 26 July 2012 Prepared by NHS Commissioning Board, a special health authority Contents Foreword...
The Way Forward: Strategic clinical networks The Way Forward Strategic clinical networks First published: 26 July 2012 Prepared by NHS Commissioning Board, a special health authority Contents Foreword...
Advanced Nursing Practice Roles Guidance for NHS Boards
 Advanced Nursing Practice Roles Guidance for NHS Boards NB: Whilst the work has been focused upon Nursing, we are keen to ensure that this initiative reflects frameworks and processes that can be applied
Advanced Nursing Practice Roles Guidance for NHS Boards NB: Whilst the work has been focused upon Nursing, we are keen to ensure that this initiative reflects frameworks and processes that can be applied
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Walsall Healthcare NHS Trust NHS West Midlands Department of Health Introduction
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Walsall Healthcare NHS Trust NHS West Midlands Department of Health Introduction
EAST AYRSHIRE HEALTH AND SOCIAL CARE PARTNERSHIP SHADOW INTEGRATION BOARD 24 APRIL 2014
 EAST AYRSHIRE HEALTH AND SOCIAL CARE PARTNERSHIP SHADOW INTEGRATION BOARD 24 APRIL 2014 PROPOSALS FOR PARTNERSHIP MANAGEMENT AND GOVERNANCE ARRANGEMENTS PURPOSE Report by Director of Health and Social
EAST AYRSHIRE HEALTH AND SOCIAL CARE PARTNERSHIP SHADOW INTEGRATION BOARD 24 APRIL 2014 PROPOSALS FOR PARTNERSHIP MANAGEMENT AND GOVERNANCE ARRANGEMENTS PURPOSE Report by Director of Health and Social
Surrey, North East Hampshire and Farnham and Hounslow. Patient Transport Services Procurement. Patient and Public FAQ Full version.
 Surrey, North East Hampshire and Farnham and Hounslow Patient Transport Services Procurement Patient and Public FAQ Full version December 2016 Clinical Commissioning Groups (CCGs) in Surrey, North East
Surrey, North East Hampshire and Farnham and Hounslow Patient Transport Services Procurement Patient and Public FAQ Full version December 2016 Clinical Commissioning Groups (CCGs) in Surrey, North East
Faversham Network Meeting your community s health and social care needs
 Faversham Network Meeting your community s health and social care needs Your CCG The CCG is the practices and the practices are the CCG. There is no separate CCG to the member practices. - Dame Barbara
Faversham Network Meeting your community s health and social care needs Your CCG The CCG is the practices and the practices are the CCG. There is no separate CCG to the member practices. - Dame Barbara
Taking Healthcare to the Patient. Transforming NHS Ambulance Services
 Taking Healthcare to the Patient Transforming NHS Ambulance Services Acknowledgements Photos on pages 15, 48 courtesy of Essex Ambulance Service NHS Trust Cover, 10, 12, 18, 24, 34, 40 courtesy of London
Taking Healthcare to the Patient Transforming NHS Ambulance Services Acknowledgements Photos on pages 15, 48 courtesy of Essex Ambulance Service NHS Trust Cover, 10, 12, 18, 24, 34, 40 courtesy of London
Delivering our Vision 5 Year Programme A Performance Management Framework Tier 1: Strategic goals and objectives RIGHT CARE, RIGHT PLACE, RIGHT TIME
 Delivering our Vision 5 Year Programme A Performance Management Framework Tier 1: Strategic goals and objectives RIGHT CARE, RIGHT PLACE, RIGHT TIME To lead in the provision of emergency care; offering
Delivering our Vision 5 Year Programme A Performance Management Framework Tier 1: Strategic goals and objectives RIGHT CARE, RIGHT PLACE, RIGHT TIME To lead in the provision of emergency care; offering
Derbyshire Learning & Development Consortium. Review of Informal Adult & Community Learning
 Derbyshire Learning & Development Consortium Review of Informal Adult & Community Learning October 2011 Lisa Vernon 32 Charnwood Street Derby DE1 2GU Tel: 01332 265960 Fax: 01332 267954 Email: lisa.vernon@consortium.org.uk
Derbyshire Learning & Development Consortium Review of Informal Adult & Community Learning October 2011 Lisa Vernon 32 Charnwood Street Derby DE1 2GU Tel: 01332 265960 Fax: 01332 267954 Email: lisa.vernon@consortium.org.uk
Workforce capacity planning model
 Workforce capacity planning model September 2014 Developed in partnership with 1 Workforce capacity planning helps employers to work out whether or not they have the right mix and numbers of workers with
Workforce capacity planning model September 2014 Developed in partnership with 1 Workforce capacity planning helps employers to work out whether or not they have the right mix and numbers of workers with
HR Corporate Objectives and Strategy Action Plan January 2013
 Reference Objective / Strategy Action Responsibility Target Date (CO1) By 2016 we will be in the top 20% of Acute Trusts as measured by the NHS National Staff Survey Embed the Trust values into reward
Reference Objective / Strategy Action Responsibility Target Date (CO1) By 2016 we will be in the top 20% of Acute Trusts as measured by the NHS National Staff Survey Embed the Trust values into reward
OUTCOME OF 2015/16 GMS CONTRACT NEGOTIATIONS AND REVISIONS TO PMS REVIEW FRAMEWORK
 Gateway Reference 02301 To: Area Team Directors, Regional Heads of Primary Care and Area Team Heads of Primary Care Cc: Regional Directors Commissioning Operations Directorate NHS England Quarry House
Gateway Reference 02301 To: Area Team Directors, Regional Heads of Primary Care and Area Team Heads of Primary Care Cc: Regional Directors Commissioning Operations Directorate NHS England Quarry House
Chairs of the Governing Boards for the CCGs within the collaboration
 Job title: Accountable Officer Clinical Commissioning Groups (CCGs) within the CWHHE collaboration (Central London, West London, Hammersmith & Fulham, Ealing and Hounslow CCGs) Grade: Reports To: Accountable
Job title: Accountable Officer Clinical Commissioning Groups (CCGs) within the CWHHE collaboration (Central London, West London, Hammersmith & Fulham, Ealing and Hounslow CCGs) Grade: Reports To: Accountable
Buckinghamshire, Hampshire and Oxfordshire Health Overview and Scrutiny Joint Review Group
 Buckinghamshire, Hampshire and Oxfordshire Health Overview and Scrutiny Joint Review Group South Central Ambulance Service: Review of Rural Performance February 2010 Contents Page Introduction 1 Methodology
Buckinghamshire, Hampshire and Oxfordshire Health Overview and Scrutiny Joint Review Group South Central Ambulance Service: Review of Rural Performance February 2010 Contents Page Introduction 1 Methodology
Non-Emergency Patient Transport Service Pre-engagement Paper for Oxfordshire Joint Health Overview & Scrutiny Committee Thursday 1 May 2014, 10:00.
 Oxfordshire Clinical Commissioning Group Non-Emergency Patient Transport Service Pre-engagement Paper for Oxfordshire Joint Health Overview & Scrutiny Committee Thursday 1 May 2014, 10:00. Background NHS
Oxfordshire Clinical Commissioning Group Non-Emergency Patient Transport Service Pre-engagement Paper for Oxfordshire Joint Health Overview & Scrutiny Committee Thursday 1 May 2014, 10:00. Background NHS
Middlesbrough Manager Competency Framework. Behaviours Business Skills Middlesbrough Manager
 Middlesbrough Manager Competency Framework + = Behaviours Business Skills Middlesbrough Manager Middlesbrough Manager Competency Framework Background Middlesbrough Council is going through significant
Middlesbrough Manager Competency Framework + = Behaviours Business Skills Middlesbrough Manager Middlesbrough Manager Competency Framework Background Middlesbrough Council is going through significant
Health Policy & Scrutiny Urgency Sub-Committee MINUTES OF PROCEEDINGS
 CITY OF WESTMINSTER MINUTES Health Policy & Scrutiny Urgency Sub-Committee MINUTES OF PROCEEDINGS Minutes of a meeting of the Health Policy & Scrutiny Urgency Sub-Committee Committee held on Thursday 7th
CITY OF WESTMINSTER MINUTES Health Policy & Scrutiny Urgency Sub-Committee MINUTES OF PROCEEDINGS Minutes of a meeting of the Health Policy & Scrutiny Urgency Sub-Committee Committee held on Thursday 7th
UKCPA - A Review of the Current Pharmaceutical Facility
 Modernising Pharmacy Careers Review of Post-Registration Career Development Discussion Paper PRO FORMA FOR CAPTURING RESPONSES TO STAKEHOLDER QUESTIONS Please complete and return to: MPCProgramme@dh.gsi.gov.uk
Modernising Pharmacy Careers Review of Post-Registration Career Development Discussion Paper PRO FORMA FOR CAPTURING RESPONSES TO STAKEHOLDER QUESTIONS Please complete and return to: MPCProgramme@dh.gsi.gov.uk
Ambulance Commissioning Intentions
 Paramedic Emergency Service (PES) Ambulance Commissioning Intentions 2014 / 15 1 P a g e Version Control Version No. Circulated to Date Amended 0.1 11/11/2013 0.2 13/11/2013 0.3 Blackpool Ambulance Commissioning
Paramedic Emergency Service (PES) Ambulance Commissioning Intentions 2014 / 15 1 P a g e Version Control Version No. Circulated to Date Amended 0.1 11/11/2013 0.2 13/11/2013 0.3 Blackpool Ambulance Commissioning
North West Surrey CCG - Head of Ambulance Contracts. Job Description
 North West Surrey CCG - Head of Ambulance Contracts Job Description Job Title: Band: Responsible to: Responsible for: Accountable to: Head of Ambulance Contracts Band 8c Associate Director of Contracts
North West Surrey CCG - Head of Ambulance Contracts Job Description Job Title: Band: Responsible to: Responsible for: Accountable to: Head of Ambulance Contracts Band 8c Associate Director of Contracts
Customer Service Strategy 2010-2013
 Service Strategy 2010-2013 Introduction Our vision for customer service is: Oxfordshire County Council aims to deliver excellent customer service by putting our customers at the heart of everything we
Service Strategy 2010-2013 Introduction Our vision for customer service is: Oxfordshire County Council aims to deliver excellent customer service by putting our customers at the heart of everything we
HR Enabling Strategy 2012-2017
 This document is yet to be put into corporate format but this interim version can be referred to for the time being. Should you have any queries, please refer to Sally Hartley, University Secretary, x
This document is yet to be put into corporate format but this interim version can be referred to for the time being. Should you have any queries, please refer to Sally Hartley, University Secretary, x
Coventry and Warwickshire Repatriation Programme
 NHS Arden Commissioning Support Unit Coventry and Warwickshire Repatriation Programme Large-scale service redesign and innovation to benefit patients Arden Commissioning Support Unit worked with Coventry
NHS Arden Commissioning Support Unit Coventry and Warwickshire Repatriation Programme Large-scale service redesign and innovation to benefit patients Arden Commissioning Support Unit worked with Coventry
PAPER B B - 1 GE/SP/AG. 26 October 2005
 PAPER B St Mary s Hospital Newport Isle of Wight PO30 5TG Tel: 01983 534204 Fax: 01983 822569 Email: graham.elderfield@iow.nhs.uk GE/SP/AG 26 October 2005 Councillor Erica Oulton Commissioner Policy Commission
PAPER B St Mary s Hospital Newport Isle of Wight PO30 5TG Tel: 01983 534204 Fax: 01983 822569 Email: graham.elderfield@iow.nhs.uk GE/SP/AG 26 October 2005 Councillor Erica Oulton Commissioner Policy Commission
(Health Scrutiny Sub-Committee 9 March 2009)
") Somerset County Council Health Scrutiny Sub-Committee 9 March 2009 Drug and Alcohol Treatment Services Author: Amanda Payne Somerset DAAT Co-ordinator Contact Details: Amanda.Payne@somerset.nhs.uk Paper
Somerset County Council Health Scrutiny Sub-Committee 9 March 2009 Drug and Alcohol Treatment Services Author: Amanda Payne Somerset DAAT Co-ordinator Contact Details: Amanda.Payne@somerset.nhs.uk Paper
PSNI Continuous Improvement Program 2014-15 End of Year Report
 PSNI Continuous Improvement Program 2014-15 End of Year Report 1 Contents EXECUTIVE SUMMARY... 5 Project 1: OPERATIONAL POLICING MODEL... 5 Project 2: SCIENTIFIC SUPPORT... 6 Project 3: PPU... 7 Project
PSNI Continuous Improvement Program 2014-15 End of Year Report 1 Contents EXECUTIVE SUMMARY... 5 Project 1: OPERATIONAL POLICING MODEL... 5 Project 2: SCIENTIFIC SUPPORT... 6 Project 3: PPU... 7 Project
Delivering Appropriate Emergency Care Services - Protocol Development and Design
 Delivering Appropriate Emergency Care Services - Protocol Development and Design Sherrill Evans, Karen Evans, Peter Huxley, Helen Snooks, Ian Russell et al Mental Health Research Team, College of Human
Delivering Appropriate Emergency Care Services - Protocol Development and Design Sherrill Evans, Karen Evans, Peter Huxley, Helen Snooks, Ian Russell et al Mental Health Research Team, College of Human
Developing commissioning support. Towards service excellence
 Developing commissioning support Towards service excellence 1 Developing commissioning support Towards service excellence First published: 2 February 2012 1 Contents Overview 3 Chapter 1: Context and vision
Developing commissioning support Towards service excellence 1 Developing commissioning support Towards service excellence First published: 2 February 2012 1 Contents Overview 3 Chapter 1: Context and vision
Performance Evaluation Report 2013 14. The City of Cardiff Council Social Services
 Performance Evaluation Report 2013 14 The City of Cardiff Council Social Services October 2014 This report sets out the key areas of progress and areas for improvement in The City of Cardiff Council Social
Performance Evaluation Report 2013 14 The City of Cardiff Council Social Services October 2014 This report sets out the key areas of progress and areas for improvement in The City of Cardiff Council Social
Wiltshire Wide Capacity Management and System Resilience 2015/16 Briefing for Wiltshire Health and Wellbeing Board November 2015
 Wiltshire Wide Capacity Management and System Resilience 2015/16 Briefing for Wiltshire Health and Wellbeing Board November 2015 1.0 Overview The aim of the document is to provide an update on the approaches
Wiltshire Wide Capacity Management and System Resilience 2015/16 Briefing for Wiltshire Health and Wellbeing Board November 2015 1.0 Overview The aim of the document is to provide an update on the approaches
IMPROVING DENTAL CARE AND ORAL HEALTH A CALL TO ACTION. February 2014 Gateway reference: 01173
 1 IMPROVING DENTAL CARE AND ORAL HEALTH A CALL TO ACTION February 2014 Gateway reference: 01173 2 Background NHS dental services are provided in primary care and community settings, and in hospitals for
1 IMPROVING DENTAL CARE AND ORAL HEALTH A CALL TO ACTION February 2014 Gateway reference: 01173 2 Background NHS dental services are provided in primary care and community settings, and in hospitals for
Shropshire Highways Draft Asset Management and Communications Strategy and Implications of Department for Transport Incentivised funding
 Committee and Date Cabinet 14 th October 2015 Shropshire Highways Draft Asset Management and Communications Strategy and Implications of Department for Transport Incentivised funding Responsible Officer
Committee and Date Cabinet 14 th October 2015 Shropshire Highways Draft Asset Management and Communications Strategy and Implications of Department for Transport Incentivised funding Responsible Officer
Managed Clinical Neuromuscular Networks
 Managed Clinical Neuromuscular Networks Registered Charity No. 205395 and Scottish Registered Charity No. SC039445 The case for Managed Clinical Neuromuscular Networks 1. Executive summary Muscular Dystrophy
Managed Clinical Neuromuscular Networks Registered Charity No. 205395 and Scottish Registered Charity No. SC039445 The case for Managed Clinical Neuromuscular Networks 1. Executive summary Muscular Dystrophy
Attached is the 2015-16 business plan for Transport Services for consideration by OPCC. (Please see attached)
") Financial Performance Programme 2014-15 Report to: the Office of the Police and Crime Commissioner for Essex Report from: Essex Police Meeting Date: 21 st May 2015 Topic: Transport Services 15-16 Business
Financial Performance Programme 2014-15 Report to: the Office of the Police and Crime Commissioner for Essex Report from: Essex Police Meeting Date: 21 st May 2015 Topic: Transport Services 15-16 Business
NHS Scotland Wheelchair Modernisation Delivery Group
 SCOTTISH GOVERNMENT HEALTH AND SOCIAL CARE DIRECTORATES THE QUALITY UNIT HEALTHCARE PLANNING DIVISION NHS Scotland Wheelchair Modernisation Delivery Group WHEELCHAIR & SEATING SERVICES QUALITY IMPROVEMENT
SCOTTISH GOVERNMENT HEALTH AND SOCIAL CARE DIRECTORATES THE QUALITY UNIT HEALTHCARE PLANNING DIVISION NHS Scotland Wheelchair Modernisation Delivery Group WHEELCHAIR & SEATING SERVICES QUALITY IMPROVEMENT
Worcestershire Patient Transport Service (PTS)
") Worcestershire Patient Transport Service (PTS) Have your say 2014 Patient Transport Service (PTS) Background In Worcestershire we have a Non-Emergency Transport Service and an Urgent Unplanned Transport
Worcestershire Patient Transport Service (PTS) Have your say 2014 Patient Transport Service (PTS) Background In Worcestershire we have a Non-Emergency Transport Service and an Urgent Unplanned Transport
Surrey, North East Hampshire and Farnham and Hounslow Patient Transport Services Procurement. Patient and Public FAQ Full version
 Surrey, North East Hampshire and Farnham and Hounslow Patient Transport Services Procurement Patient and Public FAQ Full version July 2015 1 Clinical Commissioning Groups (CCGs) in Surrey, North East Hampshire
Surrey, North East Hampshire and Farnham and Hounslow Patient Transport Services Procurement Patient and Public FAQ Full version July 2015 1 Clinical Commissioning Groups (CCGs) in Surrey, North East Hampshire
Not just a matter of time A review of urgent and emergency care services in England
 Inspecting Informing Improving Not just a matter of time A review of urgent and emergency care services in England Service review September 2008 Commission for Healthcare Audit and Inspection This document
Inspecting Informing Improving Not just a matter of time A review of urgent and emergency care services in England Service review September 2008 Commission for Healthcare Audit and Inspection This document
Newly Qualified Social Worker (NQSW) Fixed Term Post
 Fixed Term Post") Newly Qualified Social Worker (NQSW) Fixed Term Post ROLE PROFILE Role Title: Service: Accountable to: Grade: JE Code: Social Worker (NQ) Children and Families Team Manager F JE1043 Purpose of Role To
Newly Qualified Social Worker (NQSW) Fixed Term Post ROLE PROFILE Role Title: Service: Accountable to: Grade: JE Code: Social Worker (NQ) Children and Families Team Manager F JE1043 Purpose of Role To
Job Description. Applications Development Manager Band 8b
 Job Description Applications Development Manager Band 8b Job Title: Team / Directorate: Band: Responsible to: Accountable to: Application Development Manager (Hub) Commissioning Intelligence, Commercial
Job Description Applications Development Manager Band 8b Job Title: Team / Directorate: Band: Responsible to: Accountable to: Application Development Manager (Hub) Commissioning Intelligence, Commercial
Prime Minister s Challenge Fund (PMCF): Improving Access to General Practice. Innovation Showcase Series Using Technology to Improve Access
: Improving Access to General Practice. Innovation Showcase Series Using Technology to Improve Access") Prime Minister s Challenge Fund (PMCF): Improving Access to General Practice Innovation Showcase Series Using Technology to Improve Access February 2015: Showcase Two About PMCF In October 2013, the Prime
Prime Minister s Challenge Fund (PMCF): Improving Access to General Practice Innovation Showcase Series Using Technology to Improve Access February 2015: Showcase Two About PMCF In October 2013, the Prime
Public Service Commission. Government Sector Employment Act 2013
 Public Service Commission Government Sector Employment Act 2013 Contents Foreword...3 The NSW government sector workforce: what is changing?...4 Key features of the GSE Act 2013...6 The government sector...
Public Service Commission Government Sector Employment Act 2013 Contents Foreword...3 The NSW government sector workforce: what is changing?...4 Key features of the GSE Act 2013...6 The government sector...
Hub and Spoke Policy for Undergraduate Nursing and Midwifery Programmes
 Hub and Spoke Policy for Undergraduate Nursing and Midwifery Programmes 1 1.0 Introduction 1.1 The three Higher Education Institutions (HEIs) are committed to providing practice placements which maximise
Hub and Spoke Policy for Undergraduate Nursing and Midwifery Programmes 1 1.0 Introduction 1.1 The three Higher Education Institutions (HEIs) are committed to providing practice placements which maximise
Care, Fairness & Housing Policy Development Panel 21 November 2005
 Agenda Item No: 6 Developing a Corporate Health & Well-being Strategy Head of Environmental Services Summary: This report proposes the development of a health & well-being strategy for the Council, which
Agenda Item No: 6 Developing a Corporate Health & Well-being Strategy Head of Environmental Services Summary: This report proposes the development of a health & well-being strategy for the Council, which
Future National Clinical Priorities for Ambulance Services in England
 Background Future National Clinical Priorities for Ambulance Services in England National Ambulance Service Medical Directors (NASMeD) April 2014 Ambulance services have delivered significant improvements
Background Future National Clinical Priorities for Ambulance Services in England National Ambulance Service Medical Directors (NASMeD) April 2014 Ambulance services have delivered significant improvements