Venous Thromboembolism
|
|
|
- William Morrison
- 8 years ago
- Views:
Transcription
1 PREVENTION OF Venous Thromboembolism The Australia & New Zealand Working Party on the Management and Prevention of Venous Thromboembolism. Best Practice Guidelines for Australia & New Zealand 4th Edition

2 The Australia & New Zealand Working Party on the Management and Prevention of Venous Thromboembolism is proud to be affiliated with the International Union of Angiology and the Australasian Society for Thrombosis & Haemostasis. Published By: ABN Health Education & Management Innovations The Australia & New Zealand Working Party on the Management & Prevention of Venous Thromboembolism This book is copyright. Other than for fair dealing for the purposes of private study, research, criticism or review, as permitted under the Copyright Act, no part may be reproduced by any process without written permission. Inquiries should be addressed to the publisher, HEMI. Management and prevention of venous thromboembolism: guidelines for practice in Australia and New Zealand. Bibliography ISBN CONTENTS INTRODUCTION 1 IMPTANCE OF PREVENTION 2 ASSESSMENT F PROPHYLAXIS 3 VTE PROPHYLAXIS 3.1 Duration of Prophylaxis 3.2 Day Surgery & Minor Surgery or Procedures 4 PHARMACOLOGICAL AGENTS 4.1 Out of Hospital & Extended Prophylaxis 4.2 Neuroaxial Block (Epidural/Spinal) 4.3 Bleeding Risk 5 MECHANICAL DEVICES 5.1 Graduated Compression Stockings 5.2 Intermittent Pneumatic Compression 5.3 Pharmacological & Mechanical Combinations 5.4 Precautions 6 ADDITIONAL CONSIDERATIONS 6.1 Pregnancy & Postpartum 6.2 Oestrogen Preparations 6.3 Thrombophilia 7 RISK STRATIFICATION & APPROPRIATE PROPHYLAXIS 7.1 Hip or Knee Arthroplasty and Major Trauma 7.2 Hip Fracture Surgery and Major Surgery 7.3 All other Surgery 7.4 Medical Patients 7.5 Travel Related VTE 8 COST EFFECTIVENESS OF VTE PROPHYLAXIS 9 DIAGNOSIS & TREATMENT OF VTE 10 IMPLEMENTATION OF BEST PRACTICE VTE PROPHYLAXIS GUIDELINES 11 REFERENCES 12 ACKNOWLEDGEMENTS 13 SURGICAL VTE PROPHYLAXIS GUIDE (Centre pages) 14 VTE PROPHYLAXIS GUIDELINES (Back cover tear-off chart)

3 The Australia & New Zealand Working Party on the Prevention of Venous Thromboembolism consists of a group of experts dedicated to promoting best practice in the prevention, treatment and management of venous thromboembolism. They are: Professor John Fletcher (Chairman) Professor of Surgery, University of Sydney, Westmead Hospital, Sydney Assoc Prof Ross Baker Consultant Haematologist, University of Western Australia, Royal Perth Hospital, Perth Dr Charles Fisher Vascular Surgeon, Royal North Shore Hospital, Sydney Professor Alex Gallus Professor of Haematology, Flinders Hospital, Adelaide Dr Geoff Matthews, Vascular Physician, Austin & Repat. Med. Centre, Melbourne Professor Donald MacLellan Director of Surgery, NSW Health, North Sydney Professor Beng Chong Professor of Medicine, University of NSW, St.George Hospital, Sydney Dr Damian Flanagan General Practitioner, Mornington Peninsula, Victoria Assoc Prof Harry Gibbs Vascular Physician, Princess Alexandra Hospital, Brisbane Professor Hatem Salem, Professor of Medicine, Monash University, Alfred Hospital, Melbourne INTRODUCTION These updated guidelines have been developed by the Australia and New Zealand Working Party to assist in the identification and treatment of patients at risk of developing venous thromboembolism (VTE). The recommendations are based on the International Union of Angiology (IUA) and American College of Chest Physicians (ACCP) consensus statements adapted to Australia and New Zealand conditions. The recommendations issue from evidence based practice using the highest level of evidence available. There are many clinical situations where the literature provides little information to direct recommendations for VTE prophylaxis. In these circumstances, the Australia and New Zealand Working Party has applied recommendations based on expert judgement and experience. These recommendations are the combined views of surgeons and physicians expert in thrombosis management and reflect their interpretation of available evidence as well as their subjective opinions about the relative effectiveness, hazard and cost of alternatives. The members of the Australia and New Zealand Working Party hope that this booklet will encourage more appropriate and frequent VTE prophylaxis and treatment and in so doing reduce both patient suffering and health care costs. Professor Michael Stacey, Professor of Surgery, University of Western Australia, Fremantle Hospital, Fremantle Professor Andre Van Rij Professor of Surgery, University of Otago Med School, Dunedin, New Zealand.

4 1 IMPTANCE OF PREVENTION Although there is extensive evidence to guide proper prophylaxis and treatment of VTE, several surveys show that the evidence is not always being followed. One reason for this is that current approaches tend to focus on the acute management of deep venous thrombosis (DVT), rather than on its prevention and chronic sequelae. Symptomatic VTE is a major health problem with an annual incidence of 160 per 100,000 for DVT, 20 per 100,000 for symptomatic non-fatal pulmonary embolism (PE) and 50 per 100,000 for fatal autopsy detected PE. The need for prevention applies regardless of ethnicity. One of the sequelae of VTE is chronic venous insufficiency (CVI), a significant problem throughout the world. CVI decreases quality of life, increases health care costs by causing chronic oedema, cellulitis and recurrent venous ulceration and may cost the Australian Health Care system over $200 million annually. Venous ulcers develop in 300 per 100,000 population and the proportion due to DVT is approximately 25%. DVT occurs in over 50% of some categories of hospitalised patients if prophylaxis is not used (Table 1) although many are asymptomatic. It prolongs the length of hospital stay, increases drug and laboratory costs and causes potentially fatal PE. PE remains the commonest cause of preventable death; 1% of all hospital admissions will die from this. Table 1. Incidence of DVT* without prophylaxis Patient Group Stroke 56% Elective hip replacement 51% Multiple trauma 50% Total knee replacement 47% Hip fracture 45% Spinal cord injury 35% General surgery 25% Myocardial infarction 22% Neurosurgery 22% Gynaecological surgery 14-22% General medicine 17% * DVT detected by screening includes symptomatic & sub-clinical DVT. 2 ASSESSMENT F PROPHYLAXIS For effective VTE prophylaxis of surgical and medical patients, it is important to treat patients according to their individual VTE risk, their clinical condition, the bleeding risk and the appropriateness of the prophylaxis for the individual patient. The assessment for VTE prophylaxis should occur on admission to hospital and prophylaxis should commence without undue delay and be reassessed on a regular basis to ensure prophylaxis remains appropriate. In hospital patients with a prolonged stay prior to surgery, prophylaxis should be commenced during the pre-operative period. Continued encouragement of ambulation and adequate hydration are important principles in all patients regardless of risk category. 3 VTE PROPHYLAXIS 3.1 Duration of Prophylaxis The optimum length of VTE prophylaxis and treatment requires further research. Decisions regarding time of commencement and duration of prophylaxis should be made for each patient individually. However, in most studies, prophylaxis was used for at least 10 days in high-risk patients, 10 days or more in patients with knee replacement and days in patients with hip replacement or hip fracture. In medical patients, prophylaxis should continue until resolution of their acute medical illness or hospital discharge. 3.2 Day Surgery & Minor Surgery or Procedures The risk of developing VTE when undergoing day surgery or minor surgery is considered to be generally low. However, in some day surgery including laparoscopic and arthroscopic surgery, the intra-operative procedures can be relatively prolonged or the patient is already at high risk. In either circumstance, full VTE prophylaxis should be considered. There are also a number of types of trauma or procedures where there is an association with VTE but the risk is low. However, additional factors unique to the patient may increase their risk and emphasise the need for individual assessment for VTE prophylaxis. The following sections include information on common methods of prophylaxis. Section 7 provides recommendations for VTE prophylaxis in a wide variety of clinical situations.
, a significant problem throughout the world.")
5 4 PHARMACOLOGICAL AGENTS Studies have confirmed the effectiveness of subcutaneous low-dose unfractionated heparin (LDUH), low molecular weight heparin (LMWH) and the pentasaccharide fondaparinux for preventing VTE. While dosage recommendations have been included in this booklet, there is a requirement for hospital protocols and individual doctors to select the dose, dosage interval and brand of prophylactic agents having referred to full product information. Aspirin may have at best a weak protective effect against DVT in some people and therefore is not recommended for this purpose. Adjusted dose warfarin has a role in some high risk surgical patients but requires regular monitoring of its effect. Newer agents, e.g. oral thrombin or Factor Xa inhibitors, may have a role in prophylaxis in the future. 4.1 Out of Hospital & Extended Prophylaxis Many trials were based on inpatients remaining in hospital for 7-10 days. Increasingly, fewer patients stay as long as 10 days and after discharge may spend a considerable amount of time recuperating at home. They may not be truly ambulant and thus may be at increased risk of VTE. There is no conclusive evidence to form recommendations for ambulatory patients. Nevertheless, it is important to be cautious with early discharge patients as they may still be at risk and may need continued prophylaxis during their convalescence. Patient groups where the value of extended prophylaxis has been demonstrated and where prophylaxis should be continued for days include patients following hip fracture or hip replacement surgery and possibly major curative surgery for cancer. 4.2 Neuraxial Block (Epidural/Spinal) The use of epidural/spinal anaesthesia has been increasing in recent times. While the incidence of DVT may be reduced by neuraxial anaesthesia, the requirement is still high for appropriate prophylaxis. The risk of DVT and the importance of prophylaxis is not diminished with the use of neuraxial anaesthesia. However, anaesthetists have become increasingly concerned about the development of the complication of epidural haematoma in patients who are receiving pharmacoprophylaxis. It is important for the individual patient that the risk of VTE is weighed against the risk of an epidural haematoma and discussions between the anaesthetist and the surgeon should take place early enough for appropriate planning of prophylaxis. While not being able to provide definitive recommendations from the literature, options for the management of such patients would include delaying systemic pharmacological anticoagulants until after the insertion of the epidural catheter or ensuring that pharmacological anticoagulant agents are not administered within 12 hours prior to the insertion or 6 hours following withdrawal of an epidural catheter (see American Society of Regional Anesthesia and Pain Medicine (ASRA) guidelines Bleeding Risk Bleeding is the major complication of anticoagulant treatment and the relative risks for bleeding versus VTE must be considered when commencing anticoagulation. Pharmaceutical interactions must also be considered as they can contribute to unstable anticoagulation and can increase the risk for bleeding. 5 MECHANICAL DEVICES Two main types of mechanical devices are widely used in the prevention of VTE Graduated Compression Stockings (GCS) and Intermittent Pneumatic Compression (IPC). 5.1 Graduated Compression Stockings GCS reduce the incidence of DVT. Studies have generally involved full-length stockings. Although it is anticipated that below knee stockings should also provide a degree of protection against DVT, there are few comparative studies. There are two distinct and non-interchangeable types of GCS, one for DVT prophylaxis and the other for treatment of CVI. In order to achieve optimal benefit from the use of GCS, some general recommendations are provided in Table 2. Table 2. General recommendations for the use of graduated compression stockings for DVT prophylaxis Should be worn continuously during the period of immobility to the return of full ambulation Patient compliance is essential eg. ensuring stockings not rolled down Are contraindicated in critical limb ischaemia Should be measured and fitted for the individual patient

6
7 There are a wide variety of GCS available in Australian and New Zealand. However, there are no Australian standards regulating their manufacture and clinical performance. Ideal characteristics for GCS are set out in Table 3. Table 3. Ideal characteristics for the selection of GCS stockings for DVT prophylaxis Evidence of clinical efficacy Pressure of 16mmHg to 20mmHg at the ankle in the supine position with graduated compression to the knee or above Appropriate and individual sizing for each patient Sizing range should be suitable for a large percentage of the population and the window of coverage should be clearly defined Washing and reuse guidelines should be provided Appropriate manufacturing standards to ensure quality control Independent testing and compression profile of each stocking brand using internationally accepted methods 5.2 Intermittent Pneumatic Compression IPC reduces the incidence of DVT and is more effective than GCS in high risk patients in combination with anticoagulants or when anticoagulants are contraindicated. In Orthopaedic surgery, foot impulse technology (FIT) can be used with GCS if IPC is not possible. The use of IPC devices for DVT prophylaxis is similar to the GCS recommendations in that they should be used during the period of immobility to the return of full ambulation. 5.3 Pharmacological & Mechanical Combinations Combinations of agents (for example, subcutaneous heparin with GCS and/or IPC) may be more effective than single interventions alone. Although studies have generally been too small to draw strong conclusions for prophylaxis in high-risk patients, a combination of pharmacological & mechanical therapy is recommended (see Table 5 & 6). 5.4 Precautions Success in the use of GCS is dependant on proper fitting and continuous use during the VTE risk period. Improper fitting can be due to a limitation in the range of available stocking sizes as well as due to poor limb measurement for sizing. Incorrectly fitting stockings invariably do not provide the graduated compression required for prophylaxis. Reported complications with GCS and IPC are rare but include compartment syndrome, skin ulceration and common peroneal nerve palsy. Importantly, they should not be used in limbs with severe or critical ischaemia. 6 ADDITIONAL CONSIDERATIONS There are a number of other conditions worthy of consideration when determining the risk of VTE. 6.1 Pregnancy & Postpartum Several factors increase the risk of VTE during pregnancy including Caesarean section, obesity, advanced maternal age and thrombophilia. Although there is insufficient data on optimal timing and dosage, LDUH or LMWH are commonly considered for use in pregnant women with a history of idiopathic proximal VTE, thrombophilia or other high-risk factors. In these patients thromboprophylaxis should be continued for four weeks post-partum. Women undergoing Caesarean section should receive thromboprophylaxis as long as there are no contraindications for anticoagulant therapy. 6.2 Oestrogen Preparations It is considered prudent to stop hormone replacement therapy (HRT) and the oral contraceptive pill pre-operatively if the patient is in the high risk category. In the absence of other risk factors, there is insufficient evidence to support routine pre-operative cessation of oral contraceptives or HRT. Appropriate prophylaxis should be used when these agents have not been stopped. Ideally, the oral contraceptive pill should be ceased the cycle before planned surgery and other methods of contraception considered. HRT should cease six weeks before planned surgery. 6.3 Thrombophilia There are many types of thrombophilia (Table 4) but the presence of thrombophilic factors alone does not greatly increase the risk of VTE. However, patients with thrombophilia and a strong family history of VTE, recurrent DVT, or documented unexplained thrombosis before the age of 40 years are at

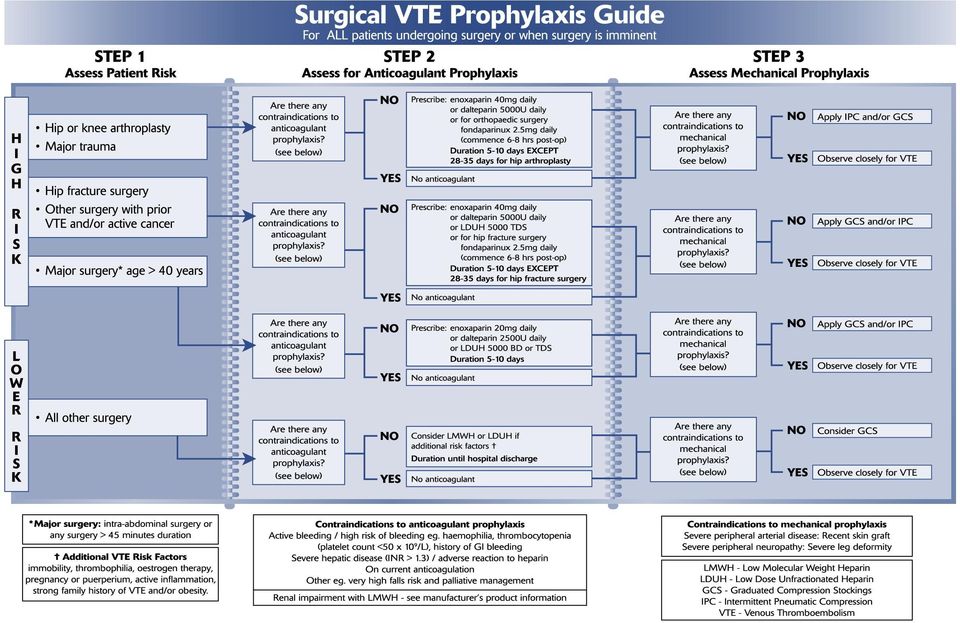
8 increased risk of VTE and should receive prophylaxis during any surgical or medical condition. Screening for thrombophilia before surgery is not required and specialist advice should be sought before screening is considered. Table 4. Causes of thrombophilia Higher Level of Risk: Antithrombin III deficiency Protein S deficiency Protein C deficiency Lower Level Risk: Activated protein C resistance (Factor V Leiden) Prothrombin gene mutation Hyperhomocysteinaemia Lupus anticoagulant Antiphospholipid antibodies Hyperhomocysteinaemia Myeloproliferative disease 7 RISK STRATIFICATION AND APPROPRIATE PROPHYLAXIS This section provides recommendations for VTE prophylaxis in a wide variety of clinical situations. Surgical patients at high risk for VTE are divided into two groups dependant on the recommendations for their prophylaxis. 7.1 Hip or Knee Arthroplasty and Major Trauma Hip or knee arthroplasty and major trauma are high risk for VTE. Recommendations on the management of these patients is summarised in Table 5. Routine ultrasound screening for DVT is not justified in most trauma patients but selective screening might be of benefit in high-risk patients who are unable to receive prophylaxis due to bleeding risk or inability to use mechanical prophylaxis. With the advent of newer technology of retrievable filters and with the option of bedside insertion under ultrasound guidance, there are some who advocate insertion of a prophylactic inferior vena cava filter for trauma patients considered to be at very high risk for VTE and bleeding. However, their routine use is not advised due to lack of evidence of efficacy or cost-effectiveness. Table 5. RISK FEATURES PROPHYLAXIS DURATION DOSAGE HIGH - Hip or knee arthroplasty - Major trauma - LMWH or Fondaparinux* AND - IPC# &/or GCS 5-10 days EXCEPT days for hip arthroplasty * Fondaparinux for orthopaedic surgery only # Foot Impulse Technology (FIT) with GCS may be used if IPC not possible Enoxaparin 40mg/day Dalteparin 5000U day Fondaparinux* 2.5mg/ day (commence 6-8 hours post-op) 7.2 Hip Fracture Surgery, Major Surgery age > 40years and Other Surgery with prior VTE and /or active cancer. In hip fracture surgery and in major surgery in patients over 40 years of age, the duration (>45 minutes) and type of operation (intra-abdominal or intrathoracic versus non-body cavity surgery) are most important and these features constitute a substantial risk for VTE. A prior history of VTE and/or active cancer are significant predictors for the development of VTE post-operatively whether major or other types of surgery. Additional risk factors for VTE development include immobility, the use of oestrogen containing preparations, the presence of thrombophilic factors, pregnancy or puerperium, active inflammation, strong family history of VTE and/or obesity. The risk classification based on international best evidence is shown in Table 6. Table 6. RISK FEATURES PROPHYLAXIS DURATION DOSAGE - Hip fracture surgery HIGH HIGH - Other surgery with prior VTE &/or active cancer - Major surgery* age > 40 years - LMWH or LDUH or Fondaparinux# AND - GCS &/or IPC - LMWH or LDUH AND GCS &/or IPC 5 10 days EXCEPT days for hip fracture surgery Enoxaparin 40mg/day Dalteparin 5000U/day LDUH 5000U TDS Fondaparinux# 2.5mg/day (commence 6-8 hours post-op) 5-10 days Enoxaparin 20mg/day Dalteparin 2500U/day LDUH 5000U BD or TDS # Fondaparinux for orthopaedic surgery only * Major surgery: intra-abdominal surgery or surgery > 45 minutes duration

9 7.3 All Other Surgery The requirement for prophylaxis for all other surgery is dependant on any additional VTE risk factors that the patient may carry including immobility, thrombophilia, oestrogen therapy, pregnancy or puerperium, active inflammation, strong family history of VTE and/or obesity. These factors if present will require consideration for prophylaxis. Otherwise, there are no specific recommendations regarding prophylaxis other than the option of GCS use (Table 7). Table 7. RISK FEATURES PROPHYLAXIS DURATION DOSAGE LOWER All other surgery - Consider GCS - Consider LMWH or LDUH if additional risk factors Until hospital discharge If additional risk factors: Enoxaparin 20mg/day Dalteparin 2500U/day LDUH 5000U BD or TDS Additional VTE risk factors: immobility, thrombophilia, oestrogen therapy, pregnancy or puerperium, active inflammation, strong family history of VTE and/or obesity. 7.4 Medical Patients Up to 75% of fatal PE in general hospitals occur in non-surgical patients immobilised by medical illness, yet there are fewer trials on VTE prophylaxis for hospitalised medical patients compared to surgical patients. Available data suggest that prophylaxis can prevent approximately two thirds of VTE in medical patients, a reduction rate similar to prophylaxis in surgical patients. Patients suffering an acute stroke with paralysis of a lower limb, a history of VTE, active cancer, decompensated cardiac failure, acute on chronic lung disease, acute on chronic inflammatory disorders or age over 60 years are at highest risk of VTE (Table 8). Medical patients with additional risk factors should also be considered for prophylaxis. Table 8. RISK FEATURES PROPHYLAXIS DURATION DOSAGE HIGH LOW - Ischaemic stroke# - History of VTE - Active cancer - Decompensated cardiac failure - Acute on chronic lung disease* - Acute on chronic inflammatory disease - Age >60 years* None of above features LMWH or LDUH Until resolution of acute medical illness or until hospital discharge Nil Enoxaparin 40mg/day Dalteparin 5000U/day LDUH 5000U BD or TDS # Favour LMWH over LDUH *While patients aged over 60 years are currently classified as high risk, those who are otherwise well and ambulant and younger patients with acute on chronic lung disease may may not be at high risk for VTE in the absence of other risk factors. 7.5 Travel Related VTE The risk of travel related DVT is not confined to air travel. There is little information available in the literature with recent studies indicating that the incidence of travel related PE appears to be small and is estimated to be about 1:1 million arrivals although possibly increasing to 1:70,000 arrivals for flights longer than 12 hours. Further studies are required to fully define the risk of travel related VTE. However, based on current information and knowledge, the majority of the travelling public are at low risk of developing a DVT and some common sense suggestions should be followed: Ensure adequate hydration by drinking sufficient fluids Regularly mobilise ankles, massage the calves and exercise leg muscles when seated for prolonged periods Avoid combining sedatives with excess alcohol Wear non-restrictive clothing Exercise eg. walking, before and after travel and during stop-overs. Considered at high risk are those travellers with a history of previous VTE, those with known pro-thrombotic states, recent surgery, significant medical illness or with multiple risk factors. In these patients the administration of prophylactic LMWH and use of properly measured and fitted GCS (20-25mmHg) is suggested. Lower compression (e.g 16-20mmHg) does not offer adequate

10 protection when the legs are in a dependent position. Non-graduated stockings are not recommended. Aspirin is not likely to be appropriate as at best it may have a weak protective effect and in some people excess bleeding may negate any benefit. 8 COST EFFECTIVENESS OF VTE PROPHYLAXIS Currently recommended prophylactic methods have been demonstrated to be cost effective in patients at high risk of VTE due to the high cost of diagnosis and treatment of VTE in these patients. There are no data on the cost effectiveness of prophylaxis in low risk groups. Effective VTE prophylaxis and treatment should also reduce the costs of managing the post-thrombotic syndrome and its consequences, especially chronic venous leg ulcers. 9 DIAGNOSIS AND TREATMENT OF VTE Best Practice Guidelines for the diagnosis and treatment of VTE have been published in booklet form by the Australia and New Zealand Working Party. In summary, the clinical diagnosis of DVT and PE is inaccurate and if suspected, should be confirmed by objective investigations although treatment may be commenced in the meantime. The current recommendation is to perform venous duplex ultrasound scanning for suspected DVT. For the diagnosis of suspected PE, ventilation perfusion scanning, CT angiography or pulmonary angiography is recommended according to local practice. Reliance on D-Dimer without pre-test probability assessment is not recommended. Swift and effective diagnosis and treatment of active VTE helps to prevent thrombus extension, leg swelling, potentially fatal PE and the development of the post-thrombotic syndrome. Therapeutic heparin is required (usually low molecular weight heparin). Oral anticoagulants should overlap heparin therapy for at least 2 days. Thrombolysis, thrombectomy or insertion of an IVC filter may be required in selected patients. Following a DVT, consideration should be given for the use of long term GCS (>20mmHg). Several studies have shown that GCS can reduce the incidence of post-thrombotic syndrome by up to 50%, yet many patients do not receive GCS. 10 IMPLEMENTATION OF BEST PRACTICE VTE PROPHYLAXIS GUIDELINES There are a number of studies in the literature that suggest inpatient VTE prophylaxis is sub-optimal. A major challenge, therefore, is to implement appropriate systems and policies in hospitals that ensure compliance with best practice guidelines. Further recommendations include: VTE prophylaxis should be used routinely Hospital policies should include VTE prophylaxis guidelines VTE prophylaxis guidelines should be included in clinical pathways, ward and specialist unit guidelines and staff manuals. Hospitals should undertake regular audit of the extent and quality of VTE prophylaxis Clinicians should ensure that individual patients have a VTE risk assessment documented in the case notes The application and use of mechanical methods of prophylaxis should be recorded Familiarisation of VTE prophylaxis guidelines should be included in senior and junior medical staff orientation, hospital grand rounds and hospital newsletters Liaison should occur with community care physicians particularly for patients receiving extended prophylaxis out of hospital 11 REFERENCES The recommendations for the prevention of VTE are based on the internationally accepted guidelines. The full lists of references supporting these recommendations are to be found in the following articles: Nicolaides AN, Fareed J, Kakkar AK, Breddin HK, Goldhaber SZ, HullR, Kakkar VV, Michiels JJ, Myers K, Samana M, Sasahara, Kalodiki E.. Prevention of venous thromboembolism. International Consensus Statement. (Guidelines according to scientific evidence). Int Angiol 2006; 25: Geerts, WH, Pineo, GF, Heit, JA, Bergqvist, D, Lassen, MR, Colwell, CW, Ray, JG. Prevention of Venous Thromboembolism. The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004; 126:338S 400S. 12 ACKNOWLEDGEMENTS The Working Party members wish to acknowledge the support of the medical industry through their provision of non-directed educational grants. The opinions expressed in this booklet are entirely those of the expert clinicians on the Working Party.

11 NOTES
DISCLAIMER ARTHROPLASTY SOCIETY VTE INFORMATION
 DISCLAIMER ARTHROPLASTY SOCIETY VTE INFORMATION Venous thromboembolism is the most common complication after total hip and total knee arthroplasty. In recent times members of the Australian Orthopaedic
DISCLAIMER ARTHROPLASTY SOCIETY VTE INFORMATION Venous thromboembolism is the most common complication after total hip and total knee arthroplasty. In recent times members of the Australian Orthopaedic
Trust Guideline for Thromboprophylaxis in Trauma and Orthopaedic Inpatients
 A clinical guideline recommended for use In: By: For: Key words: Department of Orthopaedics, NNUHT Medical staff Trauma & Orthopaedic Inpatients Deep vein thrombosis, Thromboprophylaxis, Orthopaedic Surgery
A clinical guideline recommended for use In: By: For: Key words: Department of Orthopaedics, NNUHT Medical staff Trauma & Orthopaedic Inpatients Deep vein thrombosis, Thromboprophylaxis, Orthopaedic Surgery
6/19/2012. Update on Venous Thromboembolism Prophylaxis. Disclosure. Learning Objectives. No conflicts of interest to declare
 Update on Venous Thromboembolism Prophylaxis Disclosure No conflicts of interest to declare Learning Objectives After completion of this presentation, participants should be able to: Define venous thromboembolism,
Update on Venous Thromboembolism Prophylaxis Disclosure No conflicts of interest to declare Learning Objectives After completion of this presentation, participants should be able to: Define venous thromboembolism,
Clinical practice guideline for the prevention of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to
 in patients admitted to") Clinical practice guideline for the prevention of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to Australian hospitals DRAFT FOR PUBLIC CONSULTATION 2009 Commonwealth
Clinical practice guideline for the prevention of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to Australian hospitals DRAFT FOR PUBLIC CONSULTATION 2009 Commonwealth
Published 2011 by the American Academy of Orthopaedic Surgeons 6300 North River Road Rosemont, IL 60018. AAOS Clinical Practice Guidelines Unit
 Volume 4. AAOS Clinical Guideline on Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty Comparison with Other Guidelines Disclaimer This clinical guideline
Volume 4. AAOS Clinical Guideline on Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty Comparison with Other Guidelines Disclaimer This clinical guideline
Venous Thromboembolic Treatment Guidelines
 Venous Thromboembolic Treatment Guidelines About the NYU Venous Thromboembolic Center (VTEC) The center s mission is to deliver advanced screening, detection, care, and management services for patients
Venous Thromboembolic Treatment Guidelines About the NYU Venous Thromboembolic Center (VTEC) The center s mission is to deliver advanced screening, detection, care, and management services for patients
Clinical Practice Guideline
 Clinical Practice Guideline For the Prevention of Venous Thromboembolism in Patients Admitted to Australian Hospitals Working to build a healthy Australia Commonwealth of Australia 2009 Paper-based publication
Clinical Practice Guideline For the Prevention of Venous Thromboembolism in Patients Admitted to Australian Hospitals Working to build a healthy Australia Commonwealth of Australia 2009 Paper-based publication
What Does Pregnancy Have to Do With Blood Clots in a Woman s Legs?
 Patient s Guide to Prevention of Blood Clots During Pregnancy: Use of Blood-Thinning A Patient s Guide to Prevention of Blood Clots During Pregnancy: Use of Blood-Thinning Drugs to Prevent Abnormal Blood
Patient s Guide to Prevention of Blood Clots During Pregnancy: Use of Blood-Thinning A Patient s Guide to Prevention of Blood Clots During Pregnancy: Use of Blood-Thinning Drugs to Prevent Abnormal Blood
Position Statement: The Use of VTED Prophylaxis in Foot and Ankle Surgery
 Position Statement: The Use of VTED Prophylaxis in Foot and Ankle Surgery Position Statement There is currently insufficient data for the (AOFAS) to recommend for or against routine VTED prophylaxis for
Position Statement: The Use of VTED Prophylaxis in Foot and Ankle Surgery Position Statement There is currently insufficient data for the (AOFAS) to recommend for or against routine VTED prophylaxis for
Venous thromboembolism: reducing the risk. Quick reference guide. Issue date: January 2010
 Issue date: January 2010 Venous thromboembolism: reducing the risk Reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital This guideline
Issue date: January 2010 Venous thromboembolism: reducing the risk Reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital This guideline
Confirmed Deep Vein Thrombosis (DVT)
") Confirmed Deep Vein Thrombosis (DVT) Information for patients What is deep vein thrombosis? Blood clotting provides us with essential protection against severe loss of blood from an injury to a vein or
Confirmed Deep Vein Thrombosis (DVT) Information for patients What is deep vein thrombosis? Blood clotting provides us with essential protection against severe loss of blood from an injury to a vein or
New Oral Anticoagulants. How safe are they outside the trials?
 New Oral Anticoagulants How safe are they outside the trials? Objectives The need for anticoagulant therapy Indications for anticoagulation Traditional anticoagulant therapies Properties of new oral anticoagulants
New Oral Anticoagulants How safe are they outside the trials? Objectives The need for anticoagulant therapy Indications for anticoagulation Traditional anticoagulant therapies Properties of new oral anticoagulants
Preventing Blood Clots in Adult Patients. Information For Patients
 Preventing Blood Clots in Adult Patients Information For Patients 1 This leaflet will give you information on how to reduce the risk of developing blood clots during and after your stay in hospital. If
Preventing Blood Clots in Adult Patients Information For Patients 1 This leaflet will give you information on how to reduce the risk of developing blood clots during and after your stay in hospital. If
Use of Antithrombotic Agents In The Presence Of Neuraxial Anesthesia
 Use of Antithrombotic Agents In The Presence Of Neuraxial Anesthesia Insertion, removal or presence of a catheter in selected sites can place a patient who is antithrombotic agent at risk for a local bleeding
Use of Antithrombotic Agents In The Presence Of Neuraxial Anesthesia Insertion, removal or presence of a catheter in selected sites can place a patient who is antithrombotic agent at risk for a local bleeding
Dabigatran etexilate for the treatment and secondary prevention of deep vein thrombosis and/or pulmonary embolism ERRATUM
 Dabigatran etexilate for the treatment and secondary prevention of deep vein thrombosis and/or pulmonary embolism ERRATUM This report was commissioned by the NIHR HTA Programme as project number 12/78
Dabigatran etexilate for the treatment and secondary prevention of deep vein thrombosis and/or pulmonary embolism ERRATUM This report was commissioned by the NIHR HTA Programme as project number 12/78
Low Molecular Weight Heparin. All Wales Medicines Strategy Group (AWMSG) Recommendations and advice
 Recommendations and advice") Low Molecular Weight Heparin All Wales Medicines Strategy Group (AWMSG) Recommendations and advice Starting Point Low Molecular Weight Heparin (LMWH): Inhibits factor Xa and factor IIa (thrombin) Small
Low Molecular Weight Heparin All Wales Medicines Strategy Group (AWMSG) Recommendations and advice Starting Point Low Molecular Weight Heparin (LMWH): Inhibits factor Xa and factor IIa (thrombin) Small
PARTICULAR ASPECTS OF ANTI-THROMBOTIC TREATMENT IN HIP ARTHROPLASTY
 1 UNIVERSITY OF MEDICINE AND PHARMACY CRAIOVA PARTICULAR ASPECTS OF ANTI-THROMBOTIC TREATMENT IN HIP ARTHROPLASTY ABSTRACT Ph.D student DR. TRUŞCĂ PAUL TIBERIU SCIENTIFIC COORDONATOR PROF. DR.VALENTIN
1 UNIVERSITY OF MEDICINE AND PHARMACY CRAIOVA PARTICULAR ASPECTS OF ANTI-THROMBOTIC TREATMENT IN HIP ARTHROPLASTY ABSTRACT Ph.D student DR. TRUŞCĂ PAUL TIBERIU SCIENTIFIC COORDONATOR PROF. DR.VALENTIN
Overview of the TJC/CMS VTE Core Measures
 Overview of the TJC/CMS VTE Core Measures CMS Specification Manual 4.2 January 1, 2013 June 30, 2013 Victoria Agramonte, RN, MSN Project Manager, IPRO VTE Regional Learning Sessions NYS Partnership for
Overview of the TJC/CMS VTE Core Measures CMS Specification Manual 4.2 January 1, 2013 June 30, 2013 Victoria Agramonte, RN, MSN Project Manager, IPRO VTE Regional Learning Sessions NYS Partnership for
To provide an evidenced-based approach to treatment of patients presenting with deep vein thrombosis.
 DEEP VEIN THROMBOSIS: TREATMENT TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To provide an evidenced-based approach to treatment of patients presenting with deep vein thrombosis.
DEEP VEIN THROMBOSIS: TREATMENT TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To provide an evidenced-based approach to treatment of patients presenting with deep vein thrombosis.
NIMC VTE Prophylaxis Section Audit and Reporting Tool User Guide
 NIMC VTE Prophylaxis Section Audit and Reporting Tool User Guide November 2013 Commonwealth of Australia 2013 This work is copyright. It may be reproduced in whole or in part for study or training purposes
NIMC VTE Prophylaxis Section Audit and Reporting Tool User Guide November 2013 Commonwealth of Australia 2013 This work is copyright. It may be reproduced in whole or in part for study or training purposes
DATE: 06 May 2013 CONTEXT AND POLICY ISSUES
 TITLE: Low Molecular Weight Heparins versus New Oral Anticoagulants for Long-Term Thrombosis Prophylaxis and Long-Term Treatment of DVT and PE: A Review of the Clinical and Cost-Effectiveness DATE: 06
TITLE: Low Molecular Weight Heparins versus New Oral Anticoagulants for Long-Term Thrombosis Prophylaxis and Long-Term Treatment of DVT and PE: A Review of the Clinical and Cost-Effectiveness DATE: 06
Backgrounder. Current anticoagulant therapies
 Backgrounder Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Current anticoagulant therapies Anticoagulant drugs have significantly reduced the risk of thromboembolic events
Backgrounder Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Current anticoagulant therapies Anticoagulant drugs have significantly reduced the risk of thromboembolic events
East Kent Prescribing Group
 East Kent Prescribing Group Rivaroxaban (Xarelto ) Safety Information Approved by the East Kent Prescribing Group. Approved by: East Kent Prescribing Group (Representing Ashford CCG, Canterbury and Coastal
East Kent Prescribing Group Rivaroxaban (Xarelto ) Safety Information Approved by the East Kent Prescribing Group. Approved by: East Kent Prescribing Group (Representing Ashford CCG, Canterbury and Coastal
NHS FIFE WIDE POLICY - HAEMATOLOGY MANAGEMENT OF ANTICOAGULATION THERAPY DURING MAJOR AND MINOR ELECTIVE SURGERY
 MANAGEMENT OF ANTICOAGULATION THERAPY DURING MAJOR AND MINOR ELECTIVE SURGERY The scope of this guideline is to simplify the management of patients on oral anticoagulation undergoing major and minor surgery.
MANAGEMENT OF ANTICOAGULATION THERAPY DURING MAJOR AND MINOR ELECTIVE SURGERY The scope of this guideline is to simplify the management of patients on oral anticoagulation undergoing major and minor surgery.
CLINICAL PRACTICE GUIDELINE: MOBILITY WITH A DEEP VEIN THROMBOSIS (DVT) Page 1 of 10
 Page 1 of 10") Page 1 of 10 1.0 FOCUS: Mobilization with a Deep Vein Thrombosis (DVT). The purpose of this clinical practice guideline (CPG) is to ensure that new knowledge is integrated across Fraser Health and to standardize
Page 1 of 10 1.0 FOCUS: Mobilization with a Deep Vein Thrombosis (DVT). The purpose of this clinical practice guideline (CPG) is to ensure that new knowledge is integrated across Fraser Health and to standardize
XARELTO (rivaroxaban tablets) in Knee and Hip Replacement Surgery
 in Knee and Hip Replacement Surgery") XARELTO (rivaroxaban tablets) in Knee and Hip Replacement Surgery Fast Facts: XARELTO is a novel, once-daily, oral anticoagulant recently approved in the United States for the prevention (prophylaxis)
XARELTO (rivaroxaban tablets) in Knee and Hip Replacement Surgery Fast Facts: XARELTO is a novel, once-daily, oral anticoagulant recently approved in the United States for the prevention (prophylaxis)
Venous and Lymphatic Disorders
 Venous and Lymphatic Disorders. ก. Venous and Lymphatic Disorders Varicose Veins Deep Vein Thrombosis (DVT) Lymphedema What Is Varicose Veins? Latin: Varicose = Varix = twisted Abnormal venous dilatation
Venous and Lymphatic Disorders. ก. Venous and Lymphatic Disorders Varicose Veins Deep Vein Thrombosis (DVT) Lymphedema What Is Varicose Veins? Latin: Varicose = Varix = twisted Abnormal venous dilatation
Venous Thromboembolic Disease Prophylaxis Following Foot & Ankle Surgery: A Randomized Controlled Comparative Trial
 Venous Thromboembolic Disease Prophylaxis Following Foot & Ankle Surgery: A Randomized Controlled Comparative Trial Study background: Venous thromboembolic disease (VTED) is a pathological process that
Venous Thromboembolic Disease Prophylaxis Following Foot & Ankle Surgery: A Randomized Controlled Comparative Trial Study background: Venous thromboembolic disease (VTED) is a pathological process that
Using CDS (Clinical Decision Support) for Quality Initiatives at a Community Hospital
 for Quality Initiatives at a Community Hospital") Using CDS (Clinical Decision Support) for Quality Initiatives at a Community Hospital Jonathan Sykes MD, CMIO Jacalyn Liebowitz RN, MBA,NEA-BCFACHE VP Care Continuum Allegiance Health - Jackson, MI DISCLAIMER:
Using CDS (Clinical Decision Support) for Quality Initiatives at a Community Hospital Jonathan Sykes MD, CMIO Jacalyn Liebowitz RN, MBA,NEA-BCFACHE VP Care Continuum Allegiance Health - Jackson, MI DISCLAIMER:
DVT/PE Management with Rivaroxaban (Xarelto)
") DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
DVT/PE Management with Rivaroxaban (Xarelto) Rivaroxaban is FDA approved for the acute treatment of DVT and PE and reduction in risk of recurrence of DVT and PE. FDA approved indications: Non valvular
A Prospective, Controlled Trial of a Pharmacy-Driven Alert System to Increase. Thromboprophylaxis Rates in Medical Inpatients
 1 A Prospective, Controlled Trial of a Pharmacy-Driven Alert System to Increase Thromboprophylaxis Rates in Medical Inpatients David A. Garcia, MD, Jessica Highfill, Katie Finnerty, Keith Hutchinson, MD
1 A Prospective, Controlled Trial of a Pharmacy-Driven Alert System to Increase Thromboprophylaxis Rates in Medical Inpatients David A. Garcia, MD, Jessica Highfill, Katie Finnerty, Keith Hutchinson, MD
Information for you Treatment of venous thrombosis in pregnancy and after birth. What are the symptoms of a DVT during pregnancy?
 Information for you Treatment of venous thrombosis in pregnancy and after birth Published in September 2011 What is venous thrombosis? Thrombosis is a blood clot in a blood vessel (a vein or an artery).
Information for you Treatment of venous thrombosis in pregnancy and after birth Published in September 2011 What is venous thrombosis? Thrombosis is a blood clot in a blood vessel (a vein or an artery).
National Guidance and New Protocols
 National Guidance and New Protocols Dr Jane Strong Consultant Haematologist DVT clinical lead Acute VTE chair DAWN AC Twentieth User Group Meeting 8 th October 2012 DVT patient pathway Assessment Diagnosis
National Guidance and New Protocols Dr Jane Strong Consultant Haematologist DVT clinical lead Acute VTE chair DAWN AC Twentieth User Group Meeting 8 th October 2012 DVT patient pathway Assessment Diagnosis
Traveller s Thrombosis. Dr. Peter Verhamme Vascular Medicine and Haemostasis UZ Leuven
 Traveller s Thrombosis Dr. Peter Verhamme Vascular Medicine and Haemostasis UZ Leuven Case 1: To thromboprophylaxe or not Women, aged 49, BMI 29, Combined Oral Contraceptives. Family history of provoked
Traveller s Thrombosis Dr. Peter Verhamme Vascular Medicine and Haemostasis UZ Leuven Case 1: To thromboprophylaxe or not Women, aged 49, BMI 29, Combined Oral Contraceptives. Family history of provoked
ABOUT XARELTO CLINICAL STUDIES
 ABOUT XARELTO CLINICAL STUDIES FAST FACTS Xarelto (rivaroxaban) is a novel, oral direct Factor Xa inhibitor. On September 30, 2008, the European Commission granted marketing approval for Xarelto for the
ABOUT XARELTO CLINICAL STUDIES FAST FACTS Xarelto (rivaroxaban) is a novel, oral direct Factor Xa inhibitor. On September 30, 2008, the European Commission granted marketing approval for Xarelto for the
National Guidance and New Protocols
 National Guidance and New Protocols Dr Jane Strong Consultant Haematologist DVT clinical lead Acute VTE chair DAWN AC Twentieth User Group Meeting 8 th October 2012 Autumn dawn Restless geese take flight
National Guidance and New Protocols Dr Jane Strong Consultant Haematologist DVT clinical lead Acute VTE chair DAWN AC Twentieth User Group Meeting 8 th October 2012 Autumn dawn Restless geese take flight
How To Take Xarelto
 A patient's guide Your clinic's contact details are: Name: Contact number: Contents 2 Why have I been prescribed Xarelto? 2 What is Xarelto? 3 How do I take Xarelto? 3 What should I do if I miss a dose
A patient's guide Your clinic's contact details are: Name: Contact number: Contents 2 Why have I been prescribed Xarelto? 2 What is Xarelto? 3 How do I take Xarelto? 3 What should I do if I miss a dose
Prevention of Venous Thromboembolism
 Policy Directive Prevention of Venous Thromboembolism Document Number PD2010_077 Publication date 22-Dec-2010 Functional Sub group Corporate Administration - Governance Clinical/ Patient Services - Surgical
Policy Directive Prevention of Venous Thromboembolism Document Number PD2010_077 Publication date 22-Dec-2010 Functional Sub group Corporate Administration - Governance Clinical/ Patient Services - Surgical
2.5mg SC daily. INR target 2-3 30 mg SC q 12 hr or 40mg daily. 10 mg PO q day (CrCl 30 ml/min). Avoid if < 30 ml/min. 2.
. Avoid if < 30 ml/min. 2.") Anticoagulation dosing at UCDMC (SC=subcutaneously; CI=continuous infusion) Indication Agent Dose Comments Prophylaxis Any or No bleeding risk factors see adult heparin (VTE prophylaxis) IV infusion order
Anticoagulation dosing at UCDMC (SC=subcutaneously; CI=continuous infusion) Indication Agent Dose Comments Prophylaxis Any or No bleeding risk factors see adult heparin (VTE prophylaxis) IV infusion order
Rivaroxaban (Xarelto) for preventing venous thromboembolism after hip or knee replacement surgery
 for preventing venous thromboembolism after hip or knee replacement surgery") for preventing venous thromboembolism after hip or knee replacement surgery (riv-ah-rocks-ah-ban) Summary Rivaroxaban is an oral anticoagulant and the first direct factor Xa inhibitor. Rivaroxaban has
for preventing venous thromboembolism after hip or knee replacement surgery (riv-ah-rocks-ah-ban) Summary Rivaroxaban is an oral anticoagulant and the first direct factor Xa inhibitor. Rivaroxaban has
Thrombosis and Hemostasis
 Thrombosis and Hemostasis Wendy Lim, MD, MSc, FRCPC Associate Professor, Department of Medicine McMaster University, Hamilton, ON Overview To review the important developments in venous thromboembolism
Thrombosis and Hemostasis Wendy Lim, MD, MSc, FRCPC Associate Professor, Department of Medicine McMaster University, Hamilton, ON Overview To review the important developments in venous thromboembolism
Anticoagulant therapy
 Anticoagulation: The risks Anticoagulant therapy 1990 2002: 600 incidents reported 120 resulted in death of patient 92 deaths related to warfarin usage 28 reports related to heparin usage Incidents in
Anticoagulation: The risks Anticoagulant therapy 1990 2002: 600 incidents reported 120 resulted in death of patient 92 deaths related to warfarin usage 28 reports related to heparin usage Incidents in
ACUTE DVT MANAGEMENT Richard J. DeMasi, MD April 26, 2014
 ACUTE DVT MANAGEMENT Richard J. DeMasi, MD April 26, 2014 Thromboembolism epidemiology 5 million DVT s 900,000 PE s 290,000 fatalities Heit J. Blood. 2005;106:910. 10 VTE events Since this talk began DVT
ACUTE DVT MANAGEMENT Richard J. DeMasi, MD April 26, 2014 Thromboembolism epidemiology 5 million DVT s 900,000 PE s 290,000 fatalities Heit J. Blood. 2005;106:910. 10 VTE events Since this talk began DVT
Paul G. Lee. 2 ND YEAR RESEARCH ELECTIVE RESIDENT S JOURNAL Volume III, 1998-1999. A. Objective
 A comparison of six months of anticoagulation with extended anticoagulation for a first episode of venous thromboembolism in patients with thrombophilia Paul G. Lee A. Objective a. To evaluate the risk
A comparison of six months of anticoagulation with extended anticoagulation for a first episode of venous thromboembolism in patients with thrombophilia Paul G. Lee A. Objective a. To evaluate the risk
ANTICOAGULATION USE FOR THE PREVENTION AND TREATMENT OF THROMBOEMBOLIC DISEASE
 ANTICOAGULATION USE FOR THE PREVENTION AND TREATMENT OF THROMBOEMBOLIC DISEASE Jamie N. Nadler, M.D. Assistant Professor of Medicine State University of New York at Buffalo Department of medicine Division
ANTICOAGULATION USE FOR THE PREVENTION AND TREATMENT OF THROMBOEMBOLIC DISEASE Jamie N. Nadler, M.D. Assistant Professor of Medicine State University of New York at Buffalo Department of medicine Division
Anticoagulation at the end of life. Rhona Maclean Rhona.maclean@sth.nhs.uk
 Anticoagulation at the end of life Rhona Maclean Rhona.maclean@sth.nhs.uk Content Anticoagulant Therapies Indications for anticoagulation Venous thromboembolism (VTE) Atrial Fibrillation Mechnical Heart
Anticoagulation at the end of life Rhona Maclean Rhona.maclean@sth.nhs.uk Content Anticoagulant Therapies Indications for anticoagulation Venous thromboembolism (VTE) Atrial Fibrillation Mechnical Heart
SIGN. Prevention and management of venous thromboembolism. Quick Reference Guide. December 2010. Scottish Intercollegiate Guidelines Network
 SIGN Scottish Intercollegiate Guidelines Network Part of NHS Quality Improvement Scotland 122 Prevention and management of venous thromboembolism Quick Reference Guide ecember 2010 This Quick Reference
SIGN Scottish Intercollegiate Guidelines Network Part of NHS Quality Improvement Scotland 122 Prevention and management of venous thromboembolism Quick Reference Guide ecember 2010 This Quick Reference
Prevention of stroke and systemic embolism in adult patients with non-valvular atrial fibrillation (AF) with one or more risk factors
 with one or more risk factors") News Release For use outside the US and UK only Bayer Pharma AG 13342 Berlin Germany Tel. +49 30 468-1111 www.bayerpharma.com Bayer s Xarelto Approved in the EU for the Prevention of Stroke in Patients
News Release For use outside the US and UK only Bayer Pharma AG 13342 Berlin Germany Tel. +49 30 468-1111 www.bayerpharma.com Bayer s Xarelto Approved in the EU for the Prevention of Stroke in Patients
Enoxaparin for long term anticoagulation in patients unsuitable for oral anticoagulants
 Enoxaparin for long term anticoagulation in patients unsuitable for oral anticoagulants Traffic light classification- Amber 2 Information sheet for Primary Care Prescribers Relevant Licensed Indications
Enoxaparin for long term anticoagulation in patients unsuitable for oral anticoagulants Traffic light classification- Amber 2 Information sheet for Primary Care Prescribers Relevant Licensed Indications
INTRODUCTION Thrombophilia deep vein thrombosis DVT pulmonary embolism PE inherited thrombophilia
 INTRODUCTION Thrombophilia (Hypercoagulability) is a condition in which a person forms blood clots more than normal. Blood clots may occur in the arms or legs (e.g., deep vein thrombosis DVT), the lungs
INTRODUCTION Thrombophilia (Hypercoagulability) is a condition in which a person forms blood clots more than normal. Blood clots may occur in the arms or legs (e.g., deep vein thrombosis DVT), the lungs
APSR RESPIRATORY UPDATES
 APSR RESPIRATORY UPDATES Volume 6, Issue 1 Newsletter Date: January 2014 APSR EDUCATION PUBLICATION Inside this issue: Venous thromboembolism Pulmonary embolism and deep vein thrombosis. 2 Outpatient versus
APSR RESPIRATORY UPDATES Volume 6, Issue 1 Newsletter Date: January 2014 APSR EDUCATION PUBLICATION Inside this issue: Venous thromboembolism Pulmonary embolism and deep vein thrombosis. 2 Outpatient versus
INTRODUCTION Thrombophilia deep vein thrombosis DVT pulmonary embolism PE inherited thrombophilia
 INTRODUCTION Thrombophilia (Hypercoagulability) is a condition in which a person forms blood clots more than normal. Blood clots may occur in the arms or legs (e.g., deep vein thrombosis DVT), the lungs
INTRODUCTION Thrombophilia (Hypercoagulability) is a condition in which a person forms blood clots more than normal. Blood clots may occur in the arms or legs (e.g., deep vein thrombosis DVT), the lungs
Rivaroxaban to prevent blood clots for patients who have a lower limb plaster cast. Information for patients Pharmacy
 Rivaroxaban to prevent blood clots for patients who have a lower limb plaster cast Information for patients Pharmacy Your doctor has prescribed a tablet called rivaroxaban. This leaflet tells you about
Rivaroxaban to prevent blood clots for patients who have a lower limb plaster cast Information for patients Pharmacy Your doctor has prescribed a tablet called rivaroxaban. This leaflet tells you about
La Profilassi del Tromboembolismo Venoso in Medicina
 La Profilassi del Tromboembolismo Venoso in Medicina Claudio Cimminiello U.O. Medicina Interna Azienda Ospedaliera di Vimercate Decisions regarding prophylaxis in nonsurgical patients should be made after
La Profilassi del Tromboembolismo Venoso in Medicina Claudio Cimminiello U.O. Medicina Interna Azienda Ospedaliera di Vimercate Decisions regarding prophylaxis in nonsurgical patients should be made after
Randomized, double-blind, parallel-group, multicenter, doubledummy
 ABOUT RECORD STUDIES FAST FACTS RECORD is a global program of four trials in more than 12,500 patients, comparing Xarelto (rivaroxaban) and enoxaparin in the prevention of venous thromboembolism (VTE)
ABOUT RECORD STUDIES FAST FACTS RECORD is a global program of four trials in more than 12,500 patients, comparing Xarelto (rivaroxaban) and enoxaparin in the prevention of venous thromboembolism (VTE)
Investor News. Not intended for U.S. and UK media
 Investor News Not intended for U.S. and UK media Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Bayer s Xarelto (Rivaroxaban) Approved for the Treatment of Pulmonary Embolism
Investor News Not intended for U.S. and UK media Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Bayer s Xarelto (Rivaroxaban) Approved for the Treatment of Pulmonary Embolism
How To Get A Dose Of Bayer Healthcare'S Oral Anticoagulant, Xarelto
 News Release FOR UK HEALTHCARE MEDIA ONLY Bayer HealthCare Bayer plc Bayer House Strawberry Hill Newbury Berkshire, RG14 1JA www.bayer.co.uk Bayer s Xarelto (rivaroxaban) Recommended by CHMP for EU Approval
News Release FOR UK HEALTHCARE MEDIA ONLY Bayer HealthCare Bayer plc Bayer House Strawberry Hill Newbury Berkshire, RG14 1JA www.bayer.co.uk Bayer s Xarelto (rivaroxaban) Recommended by CHMP for EU Approval
Thrombophilia. Steven R. Lentz, M.D. Ph.D. Carver College of Medicine The University of Iowa May 2003
 Thrombophilia Steven R. Lentz, M.D. Ph.D. Carver College of Medicine The University of Iowa May 2003 Thrombophilia Hereditary and acquired risk factors for thrombosis Venous thromboembolism Arterial thromboembolism
Thrombophilia Steven R. Lentz, M.D. Ph.D. Carver College of Medicine The University of Iowa May 2003 Thrombophilia Hereditary and acquired risk factors for thrombosis Venous thromboembolism Arterial thromboembolism
Uncontrolled when printed. Version 1.1. Acute Sector. Lead Author/Co-ordinator: Mr Simon Barker Consultant Orthopaedic Surgeon Julie Fraser
 Acute Sector NHS Grampian Staff Local Treatment Protocol For Venous Thromoboembolic Prophylaxis Using Rivaroxaban 10mg Tablets In Adult Patients Undergoing Elective Hip Or Knee Replacement Surgery. Lead
Acute Sector NHS Grampian Staff Local Treatment Protocol For Venous Thromoboembolic Prophylaxis Using Rivaroxaban 10mg Tablets In Adult Patients Undergoing Elective Hip Or Knee Replacement Surgery. Lead
45 yo fall from ladder
 DVT and PE Prophylaxis in Lower Extremity Trauma Daniel T. Altman, MD Associate Professor of Orthopaedic Surgery Drexel University College of Medicine Temple University School of Medicine Allegheny General
DVT and PE Prophylaxis in Lower Extremity Trauma Daniel T. Altman, MD Associate Professor of Orthopaedic Surgery Drexel University College of Medicine Temple University School of Medicine Allegheny General
Anti-Coagulation Therapies: A Review of Best Practices for Managing Risk
 Volume 20 No. 1 Spring 2012 Anti-Coagulation Therapies: A Review of Best Practices for Managing Risk Dear Colleague: This first newsletter of 2012 deals with an important aspect of patient care the monitoring
Volume 20 No. 1 Spring 2012 Anti-Coagulation Therapies: A Review of Best Practices for Managing Risk Dear Colleague: This first newsletter of 2012 deals with an important aspect of patient care the monitoring
Failure or significant adverse effects to all of the alternatives: Eliquis and Xarelto
 This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutics
This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutics
Anticoagulation Dosing at UCDMC Indication Agent Standard Dose Comments and Dose Adjustments VTE Prophylaxis All Services UFH 5,000 units SC q 8 h
 Indication Agent Standard Dose Comments and Dose Adjustments VTE Prophylaxis All Services UFH 5,000 units SC q 8 h See EMR adult VTE prophylaxis CI order set Enoxaparin See service specific dosing Assess
Indication Agent Standard Dose Comments and Dose Adjustments VTE Prophylaxis All Services UFH 5,000 units SC q 8 h See EMR adult VTE prophylaxis CI order set Enoxaparin See service specific dosing Assess
ADVICE ON TRAVEL-RELATED DEEP VEIN THROMBOSIS
 ADVICE ON TRAVEL-RELATED DEEP VEIN THROMBOSIS Introduction 1. A possible link between deep vein thrombosis (DVT) and long haul air travel was first suggested by reports in medical journals in the 1950s.
ADVICE ON TRAVEL-RELATED DEEP VEIN THROMBOSIS Introduction 1. A possible link between deep vein thrombosis (DVT) and long haul air travel was first suggested by reports in medical journals in the 1950s.
Deep Vein Thrombosis (DVT) AUTHORS: Nancy Skinner, RN, C, CCM Peter Moran, RN, C, BSN, MS, CCM
 AUTHORS: Nancy Skinner, RN, C, CCM Peter Moran, RN, C, BSN, MS, CCM") Deep Vein Thrombosis (DVT) AUTHORS: Nancy Skinner, RN, C, CCM Peter Moran, RN, C, BSN, MS, CCM CMAG CASE MANAGEMENT ADHERENCE GUIDELINES VERSION 1.0 DEEP VEIN THROMBOSIS (DVT) Guidelines from the Case
Deep Vein Thrombosis (DVT) AUTHORS: Nancy Skinner, RN, C, CCM Peter Moran, RN, C, BSN, MS, CCM CMAG CASE MANAGEMENT ADHERENCE GUIDELINES VERSION 1.0 DEEP VEIN THROMBOSIS (DVT) Guidelines from the Case
Inpatient Anticoagulation Safety. To provide safe and effective anticoagulation therapy through a collaborative approach.
 Inpatient Anticoagulation Safety Purpose: Policy: To provide safe and effective anticoagulation therapy through a collaborative approach. Upon the written order of a physician, Heparin, Low Molecular Weight
Inpatient Anticoagulation Safety Purpose: Policy: To provide safe and effective anticoagulation therapy through a collaborative approach. Upon the written order of a physician, Heparin, Low Molecular Weight
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2013
 Clinical Practice Guideline August 2013") Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2013 General Principles: There is compelling data in the medical literature to support
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2013 General Principles: There is compelling data in the medical literature to support
Prescriber Guide. 20mg. 15mg. Simply Protecting More Patients. Simply Protecting More Patients
 Prescriber Guide 20mg Simply Protecting More Patients 15mg Simply Protecting More Patients 1 Dear Doctor, This prescriber guide was produced by Bayer Israel in cooperation with the Ministry of Health as
Prescriber Guide 20mg Simply Protecting More Patients 15mg Simply Protecting More Patients 1 Dear Doctor, This prescriber guide was produced by Bayer Israel in cooperation with the Ministry of Health as
Hypercoagulability How to Expect the Unexpected. Beth Saft, DO VOMA Conference 2012
 Hypercoagulability How to Expect the Unexpected Beth Saft, DO VOMA Conference 2012 Who is at Risk Most Common Hypercoagulability Objectives + When to Test What to do with the Test Results Who gets a DVT
Hypercoagulability How to Expect the Unexpected Beth Saft, DO VOMA Conference 2012 Who is at Risk Most Common Hypercoagulability Objectives + When to Test What to do with the Test Results Who gets a DVT
2. Background This indication of rivaroxaban had not previously been considered by the PBAC.
 PUBLIC SUMMARY DOCUMENT Product: Rivaroxaban, tablets, 15mg and 20mg, Xarelto Sponsor: Bayer Australia Ltd Date of PBAC Consideration: March 2013 1. Purpose of Application The application requested the
PUBLIC SUMMARY DOCUMENT Product: Rivaroxaban, tablets, 15mg and 20mg, Xarelto Sponsor: Bayer Australia Ltd Date of PBAC Consideration: March 2013 1. Purpose of Application The application requested the
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 10 March 2010
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 10 March 2010 ARIXTRA 1.5 mg/0.3 ml, solution for injection in pre-filled syringe Box of 2 (CIP: 363 500-6) Box of
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 10 March 2010 ARIXTRA 1.5 mg/0.3 ml, solution for injection in pre-filled syringe Box of 2 (CIP: 363 500-6) Box of
Bayer Initiates Rivaroxaban Phase III Study to Support Dose Selection According to Individual Benefit-Risk Profile in Long- Term VTE Prevention
 Investor News Not intended for U.S. and UK Media Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Long-term prevention of venous blood clots (VTE): Bayer Initiates Rivaroxaban
Investor News Not intended for U.S. and UK Media Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com Long-term prevention of venous blood clots (VTE): Bayer Initiates Rivaroxaban
Sign up to receive ATOTW weekly - email worldanaesthesia@mac.com
 THROMBOPROPHYLAXIS PART 2 ANAESTHESIA TUTORIAL OF THE WEEK 244 12 TH DECEMBER 2011 Nicola Ross, anaesthetic registrar Huddersfield Royal Infirmary Nicholas Freeman, anaesthetic registrar Harrogate District
THROMBOPROPHYLAXIS PART 2 ANAESTHESIA TUTORIAL OF THE WEEK 244 12 TH DECEMBER 2011 Nicola Ross, anaesthetic registrar Huddersfield Royal Infirmary Nicholas Freeman, anaesthetic registrar Harrogate District
rivaroxaban 15 and 20mg film-coated tablets (Xarelto ) SMC No. (755/12) Bayer PLC
 SMC No. (755/12) Bayer PLC") rivaroxaban 15 and 20mg film-coated tablets (Xarelto ) SMC No. (755/12) Bayer PLC 13 January 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS
rivaroxaban 15 and 20mg film-coated tablets (Xarelto ) SMC No. (755/12) Bayer PLC 13 January 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS
rivaroxaban 15mg and 20mg film-coated tablets (Xarelto ) SMC No. (852/13) Bayer plc
 SMC No. (852/13) Bayer plc") rivaroxaban 15mg and 20mg film-coated tablets (Xarelto ) SMC No. (852/13) Bayer plc 08 February 2013 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises
rivaroxaban 15mg and 20mg film-coated tablets (Xarelto ) SMC No. (852/13) Bayer plc 08 February 2013 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises
UHS CLINICAL CARE COLLABORATION: Outpatient & Inpatient
 Guidelines for Anticoagulation Initiation and Management Y2014 UHS CLINICAL CARE COLLABORATION: Outpatient & Inpatient Topic Page Number MEDICATION FLOW AND PATIENT FLOW... 2 AND 3 PARENTERAL ANTICOAGULANTS...
Guidelines for Anticoagulation Initiation and Management Y2014 UHS CLINICAL CARE COLLABORATION: Outpatient & Inpatient Topic Page Number MEDICATION FLOW AND PATIENT FLOW... 2 AND 3 PARENTERAL ANTICOAGULANTS...
Pulmonary Embolism Treatment Update
 UC SF Pulmonary Embolism Treatment Update Jeffrey Tabas, MD Professor UCSF School of Medicine Emergency Department San Francisco General Hospital sf g h Disclosure No Financial Relationships to Disclose
UC SF Pulmonary Embolism Treatment Update Jeffrey Tabas, MD Professor UCSF School of Medicine Emergency Department San Francisco General Hospital sf g h Disclosure No Financial Relationships to Disclose
Preventing Blood Clots After Hip or Knee Replacement Surgery or Surgery for a Broken Hip. A Review of the Research for Adults
 Preventing Blood Clots After Hip or Knee Replacement Surgery or Surgery for a Broken Hip A Review of the Research for Adults Is This Information Right for Me? Yes, if: You are considering or planning to
Preventing Blood Clots After Hip or Knee Replacement Surgery or Surgery for a Broken Hip A Review of the Research for Adults Is This Information Right for Me? Yes, if: You are considering or planning to
CDEC FINAL RECOMMENDATION
 CDEC FINAL RECOMMENDATION RIVAROXABAN (Xarelto Bayer Inc.) New Indication: Pulmonary Embolism Note: The Canadian Drug Expert Committee (CDEC) previously reviewed rivaroxaban for the treatment of deep vein
CDEC FINAL RECOMMENDATION RIVAROXABAN (Xarelto Bayer Inc.) New Indication: Pulmonary Embolism Note: The Canadian Drug Expert Committee (CDEC) previously reviewed rivaroxaban for the treatment of deep vein
A PATIENT S GUIDE TO PULMONARY EMBOLISM TREATMENT
 A PATIENT S GUIDE TO PULMONARY EMBOLISM TREATMENT This medicine is subject to additional monitoring. This will allow quick identification of new safety information. If you get any side effects, talk to
A PATIENT S GUIDE TO PULMONARY EMBOLISM TREATMENT This medicine is subject to additional monitoring. This will allow quick identification of new safety information. If you get any side effects, talk to
Title Use of rivaroxaban in suspected DVT in the Emergency Department Standard Operating Procedure. Author s job title. Pharmacist.
 Document Control Title Use of rivaroxaban in suspected DVT in the Emergency Department Author Pharmacist Directorate Clinical Support Services Version Date Issued Status 0.1 Oct Draft 2015 1.0 Dec Final
Document Control Title Use of rivaroxaban in suspected DVT in the Emergency Department Author Pharmacist Directorate Clinical Support Services Version Date Issued Status 0.1 Oct Draft 2015 1.0 Dec Final
What is the appropriate duration of treatment for VTE? Any advances in predicting recurrence?
 What is the appropriate duration of treatment for VTE? Any advances in predicting recurrence? Beverley Hunt Thrombosis & Haemostasis, King s College Guy s & St Thomas Trust Medical Director of Lifeblood:
What is the appropriate duration of treatment for VTE? Any advances in predicting recurrence? Beverley Hunt Thrombosis & Haemostasis, King s College Guy s & St Thomas Trust Medical Director of Lifeblood:
ASHP Therapeutic Position Statement on the Role of Pharmacotherapy in Preventing Venous Thromboembolism in Hospitalized Patients
 ASHP Therapeutic Position Statements 545 ASHP Therapeutic Position Statement on the Role of Pharmacotherapy in Preventing Venous Thromboembolism in Hospitalized Patients Position Hospitals should develop
ASHP Therapeutic Position Statements 545 ASHP Therapeutic Position Statement on the Role of Pharmacotherapy in Preventing Venous Thromboembolism in Hospitalized Patients Position Hospitals should develop
HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below
 RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below") Name: generic (trade) Rivaroxaban (Xarelto ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below What it is Indications
Name: generic (trade) Rivaroxaban (Xarelto ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) RIVAROXABAN RECOMMENDED see specific recommendations for licensed indications below What it is Indications
Thromboprophylaxis Guidelines for Adult Patients in:
 Once printed this document is uncontrolled. Please refer to the Trusts intranet site for the most up to date version. Thromboprophylaxis Guidelines for Adult Patients in: Critical Care General Surgery
Once printed this document is uncontrolled. Please refer to the Trusts intranet site for the most up to date version. Thromboprophylaxis Guidelines for Adult Patients in: Critical Care General Surgery
Eliquis. Policy. covered: Eliquis is. indicated to. reduce the. therapy. Eliquis is. superior to. of 32 to. Eliquis is AMPLIFY. nonfatal. physicians.
 Eliquis (apixaban) Policy Number: 5.01.573 Origination: 06/2014 Last Review: 07/2015 Next Review: 07/2016 Policy BCBSKC will provide coverage for Eliquis when it is determined to be medically necessary
Eliquis (apixaban) Policy Number: 5.01.573 Origination: 06/2014 Last Review: 07/2015 Next Review: 07/2016 Policy BCBSKC will provide coverage for Eliquis when it is determined to be medically necessary
Deep Vein Thrombosis (DVT) in pregnancy
 in pregnancy") Deep Vein Thrombosis (DVT) in pregnancy Information and advice for women and families Maternity What is a deep vein thrombosis (DVT)? A deep vein thrombosis (DVT) is a blood clot that forms in a deep leg
Deep Vein Thrombosis (DVT) in pregnancy Information and advice for women and families Maternity What is a deep vein thrombosis (DVT)? A deep vein thrombosis (DVT) is a blood clot that forms in a deep leg
Prior Authorization Guideline
 Guideline Guideline Name Formulary Xarelto (rivaroxaban) UnitedHealthcare Community & State Approval Date 0/0/203 Revision Date 8//204 Technician Note: CPS Approval Date: /5/20; CPS Revision Date: 8/20/204
Guideline Guideline Name Formulary Xarelto (rivaroxaban) UnitedHealthcare Community & State Approval Date 0/0/203 Revision Date 8//204 Technician Note: CPS Approval Date: /5/20; CPS Revision Date: 8/20/204
Cardiovascular Disease
 Cardiovascular Disease 1 Cardiovascular Disease 1. More target specific oral anticoagulants (TSOAC) 2. Vorapaxar (Zonivity) 3. Continued noise about a polypill 4. WATCHMAN 3 1 2 3 4 Left Atrial Appendage
Cardiovascular Disease 1 Cardiovascular Disease 1. More target specific oral anticoagulants (TSOAC) 2. Vorapaxar (Zonivity) 3. Continued noise about a polypill 4. WATCHMAN 3 1 2 3 4 Left Atrial Appendage
*** Drug Safety Alert ***
 *** Drug Safety Alert *** Xarelto (Rivaroxaban) Tablets FDA MedWatch - August 2013 Safety Labeling Changes with revisions to Prescribing Information [Posted 09/13/2013] The MedWatch August 2013 Safety
*** Drug Safety Alert *** Xarelto (Rivaroxaban) Tablets FDA MedWatch - August 2013 Safety Labeling Changes with revisions to Prescribing Information [Posted 09/13/2013] The MedWatch August 2013 Safety
Haematology for GP s Part 2. Anticoagulation in DVT and PE VTE. Introduction. DVT Principles of diagnosis. VTE in Bradford
 Haematology for GP s Part 2 Anticoagulation in DVT and PE Introduction NICE guidelines DVT and PE diagnosis and treatment Warfarin New anticoagulants Cases VTE VTE is an important cause of morbidity and
Haematology for GP s Part 2 Anticoagulation in DVT and PE Introduction NICE guidelines DVT and PE diagnosis and treatment Warfarin New anticoagulants Cases VTE VTE is an important cause of morbidity and
VTE Virtual Learning Series #1: Preventing VTE: Evidence and Execution
 VTE Virtual Learning Series #1: Preventing VTE: Evidence and Execution Hosted by: Shari McKeown, RRT, FCSRT, MA Quality Leader, BC Patient Safety & Quality Council smckeown@bcpsqc.ca www.clinicalcaremanagement.ca
VTE Virtual Learning Series #1: Preventing VTE: Evidence and Execution Hosted by: Shari McKeown, RRT, FCSRT, MA Quality Leader, BC Patient Safety & Quality Council smckeown@bcpsqc.ca www.clinicalcaremanagement.ca
Antithrombotic therapy
 Orthogeriatrics Clinical Summary Document Antithrombotic therapy Topics Preexisting anticoagulation and timing of surgery Reversal of anticoagulation Perioperative thromboprophylaxis When should we be
Orthogeriatrics Clinical Summary Document Antithrombotic therapy Topics Preexisting anticoagulation and timing of surgery Reversal of anticoagulation Perioperative thromboprophylaxis When should we be
Joseph A. Caprini, MD, MS, FACS, RVT
 Joseph A. Caprini, MD, MS, FACS, RVT Louis W. Biegler Chair of Surgery NorthShore University HealthSystem, Evanston, IL Clinical Professor of Surgery University of Chicago Pritzker School of Medicine,
Joseph A. Caprini, MD, MS, FACS, RVT Louis W. Biegler Chair of Surgery NorthShore University HealthSystem, Evanston, IL Clinical Professor of Surgery University of Chicago Pritzker School of Medicine,
NHS FORTH VALLEY RIVAROXABAN AS TREATMENT FOR DEEP VEIN THROMBOSIS AND PULMONARY EMBOLISM IN ADULTS
 NHS FORTH VALLEY RIVAROXABAN AS TREATMENT FOR DEEP VEIN THROMBOSIS AND PULMONARY EMBOLISM IN ADULTS Date of First Issue 01/12/ 2012 Approved 15/11/2012 Current Issue Date 29/10/2014 Review Date 29/10/2016
NHS FORTH VALLEY RIVAROXABAN AS TREATMENT FOR DEEP VEIN THROMBOSIS AND PULMONARY EMBOLISM IN ADULTS Date of First Issue 01/12/ 2012 Approved 15/11/2012 Current Issue Date 29/10/2014 Review Date 29/10/2016
Cost Effectiveness of Apixaban (Eliquis ) for the Prevention of Venous Thromboembolic Events in Adult Patients who have Undergone Elective Total Hip
 for the Prevention of Venous Thromboembolic Events in Adult Patients who have Undergone Elective Total Hip") Cost Effectiveness of Apixaban (Eliquis ) for the Prevention of Venous Thromboembolic Events in Adult Patients who have Undergone Elective Total Hip Replacement or Total Knee Replacement National Centre
Cost Effectiveness of Apixaban (Eliquis ) for the Prevention of Venous Thromboembolic Events in Adult Patients who have Undergone Elective Total Hip Replacement or Total Knee Replacement National Centre
Service Specification Template Department of Health, updated June 2015
 Service Specification Template Department of Health, updated June 2015 Service Specification No. : 2 Service: Commissioner Lead: Provider Lead: Period: Anti-coagulation monitoring Date of Review: 31 st
Service Specification Template Department of Health, updated June 2015 Service Specification No. : 2 Service: Commissioner Lead: Provider Lead: Period: Anti-coagulation monitoring Date of Review: 31 st
The new oral anticoagulants & the future of haemostasis laboratory testing. Alcohol: the good, the bad and the ugly
 The new oral anticoagulants & the future of haemostasis laboratory testing Emmanuel J Favaloro Diagnostic Haemostasis Laboratory, Institute of Clinical Pathology & Medical Research, ICPMR, Pathology West,
The new oral anticoagulants & the future of haemostasis laboratory testing Emmanuel J Favaloro Diagnostic Haemostasis Laboratory, Institute of Clinical Pathology & Medical Research, ICPMR, Pathology West,