relatively slow process; it takes about 2 years from the initial attack of caries to be clinically evident and be counted as D in the DMFT index.
|
|
|
- Peregrine Gray
- 8 years ago
- Views:
Transcription
1
2 Most childhood tooth decay could be avoided through simple preventive measures such as screening, monitoring, combined use of fluorides and dental sealants and regular professional care. These measures can save children pain, complicated procedures and high dental treatment costs. In order to apply the measures effectively, public health care administrators and decision-makers need the tools, the capacity and the information to assess and monitor oral health needs, choose intervention strategies, design policy options appropriate to their own circumstances and improve the performance of the oral health system [1]. Dental screening data can be used to identify trends and to assist in allocating scarce resources [2] and are an important indicator of a community s health status [3]. One successful model of oral health programmes is school-based screening and education. School-based programmes are increasingly being seen as a strategic way to identify children who need dental care the most and thus improve access to health and social support services for vulnerable populations. Studies show that school dental screening is capable of stimulating dental attendance among children with a treatment need [4,5] and improving the dental health status of schoolchildren [6]. However, there are inherent problems and challenges with school-based screening programmes. Al-Tannir discussed the importance of outreach activities in promoting awareness of a dental screening programme and highlighted the need for personal contact by programme staff to ensure that children get the necessary follow-up [7]. Cooperative relationships between dental practitioners and the schools are required [8]. Furthermore, school-based dental screening programmes can be very time- and labour-intensive [9,10]. Other challenges include developing a standardized screening protocol, including both the establishment of standardized criteria for referral [11] and sufficient training and calibration of screeners [12]. It is important, however, to highlight that training does not fully resolve problems with consistent identification of dental needs between screeners [13]. Another question is who should carry out the screening: dentists and dental hygienists [9] or primary care providers or paediatric dentists [14]. This paper outlines the oral screening programme that has been set up in public schools in 9 governorates in the West Bank region of Palestine, and details the evaluation of the effectiveness of the programme in minimizing oral health diseases, particularly caries. As a global concern, in 1979 The World Health Organization (WHO) announced that by the year 2000, the global average for dental caries was to be no more than 3 decayed, missing or filled teeth (DMFT) at 12 years of age [15] and in 1989 WHO endorsed the promotion of oral health as an integral part of health for all by the year 2000 [1]. To achieve this, WHO urged Member States to establish oral health information systems and offered assistance in efforts to develop these systems and provide them with core standardized methods but with flexibility to expand by adding information relevant to the local situation. To meet national needs and international requests, an oral health screening programme was launched in West Bank public schools of the Palestinian Authority in 1997, aiming to screen schoolchildren

3 in the 3rd, 7th and 10th grades. It is a part of the national school health programme conducted by the Palestinian Ministry of Health (MOH) in collaboration with other international organizations. The programme is carried out and operated by the MOH s 17 dental clinics that are distributed all over the West Bank and report to the central office in Ramallah. The programme started with oral screening, educational seminars and students referrals to oral clinics operated by the MOH. After that, the programme developed into offering some necessary preventive procedures, such as fluoride gel application and fissure sealants for selected schools in school years and The programme uses WHO models and criteria [16] in screening for dental decay using the DMFT index and for gingival health using the CPITN index [community periodontal index of treatment needs]. Later, programme operators added fluorosis and malocclusion assessment to the screening programme. Although the dental screening programme does not have specific objectives, the school health programme aims to improve the general and oral health of school students and increase their access to health services. Programme effectiveness was measured in 2 stages: short-term and long-term. Short-term outcomes can be demonstrated by increasing coverage rate, increasing FT component and care experience index (i.e. more services delivered and more followups made), and increasing the percentage of referred students who actually attended oral clinics (i.e. success in raising awareness of oral health care, increasing follow-up and stimulus for seeking treatment). Long-term outcomes can be demonstrated by lower DMFT values, especially the DT component. This outcome needs more time to be apparent, because caries progression is a relatively slow process; it takes about 2 years from the initial attack of caries to be clinically evident and be counted as D in the DMFT index. Two methods of evaluation were used: quantitative (retrospective analysis of official records) and qualitative (in-depth interviews). Data for the evaluation were drawn from 7 annual oral health reports organized by the central oral health department in the Palestinian Authority MOH (school years until ). These data provide a means for tracking changes in quantifiable behaviours. The oral health offices in the 9 Palestinian governorates send their monthly school oral health screening results to the central office in Ramallah, where they are organized and analysed into the final report. Each school in the designated governorate has the chance to be screened once a year. DMFT data (among other oral health indicators) are collected for each student in the selected grades. The data presented here were derived from routine dental examination conducted by the MOH dentists using visual methods without radiography or fibro-optic transillumination. In school year a grant from the United Nations Children s Fund (UNICEF) supplied all the governorates with WHO standardized examination sets for oral screening. The methods used for the diagnosis and reporting of caries experience followed those published by the WHO for oral epidemiological studies [16]. The dental screening programme targeted public school students in 3rd, 7th and 10th grades in all the 10 governorates. In

4 this evaluation, only data for 7th and 10th grades were used, because for the first 5 years 3rd graders were screened then substituted by 1st graders. The 7th grade (12- year-olds) and 10th grade (15-year-olds) are global monitoring cohorts; this allowed more permanent teeth to be included in the examination, and would facilitate international comparisons [17]. Only 9 governorates were used in this evaluation, because the 10th (Jerusalem) was added only in the last 4 years. Five indicators were used [18]: 1. DMFT index: the mean number of teeth decayed, missing or filled because of decay among schoolchildren. The index may refer to permanent teeth or baby teeth. It is a general indicator of dental health status among children and is felt to be extremely reliable; the lower the index, the better the dental health of the population. The index records past history and is cumulative [19]. To be recorded as decayed, teeth must have evidence of carious cavitations to the level of the dentine. 2. DT index: the number of decayed teeth divided by the number of examined students. This shows the caries experience by population. 3. Care experience index: the number of filled teeth divided by the number of examined students [(FT/DMFT) 100/100]. This indicator assesses the delivery of dental services to the population. 4. Coverage rate: the number of students examined in each governorate divided by the number of students in that governorate. 5. Percentage of MOH oral clinic visits: the percentage of oral clinic visits by referred students (referred by screening teams). This shows the effect of oral school health programmes in stimulating students and their parents to seek dental care and the amount of follow-up by the programme itself. This is a valuable indicator to measure programme effectiveness. Analysis of the data extracted from the MOH s 7 annual reports was carried out using SPSS software package. The second method used in this report was in-depth interviews with programme administrators, dentists who conducted the oral screening and staff involved in interpreting and analysing data. Interviews comprised a series of questions, typically semistructured or unstructured, conducted in person. A trained dentist with dental public health experience prepared and conducted those interviews. The advantages and disadvantages of the programme and other programmes operating in the region, concerns about the implementation of the programme, suggestions and recommendations to improve it and general oral health policy in the Palestinian Authority areas were discussed. The analysis of the data revealed the following outcomes for the 5 indicators. Coverage rate: All governorates showed a steady increase in coverage rates in the first 4 years and a boost in the last 3 years of the evaluation. Overall, the rate increased from 22.8% in 7th grade and 14.5% in 10th grade in to 92.4% and 88.2% respectively in The highest rates were obtained in school year ; coverage rates in 7th grade were consistently higher than 10th grade, as shown in
![comparisons [17]. Only 9 governorates were used in this evaluation, because the 10th (Jerusalem) was added only in the last 4 years. Five indicators were used [18]: 1.](/docs-images/55/8663860/images/page_4.jpg "DMFT index: the mean number of teeth decayed, missing or filled because of decay among schoolchildren. The index may refer to permanent teeth or baby teeth.")
5 Figure 1. A major increase in coverage rates after year occurred after the school oral health administration assigned local dental staff for each region to screen school students, saving time and cost of dentists travelling from one region to another. DMFT index: Trends in DMFT over time demonstrated a slight decrease in DMFT scores for the West Bank in the last 2 years (Figure 2). The mean West Bank DMFT scores for 7th grade ranged from 1.35 in to 2.17 in 2001 and from 1.6 in to 2.9 in for 10th graders. In school year the mean DMFT was 1.49 for 7th grade and 1.9 for 10th grade.
.")
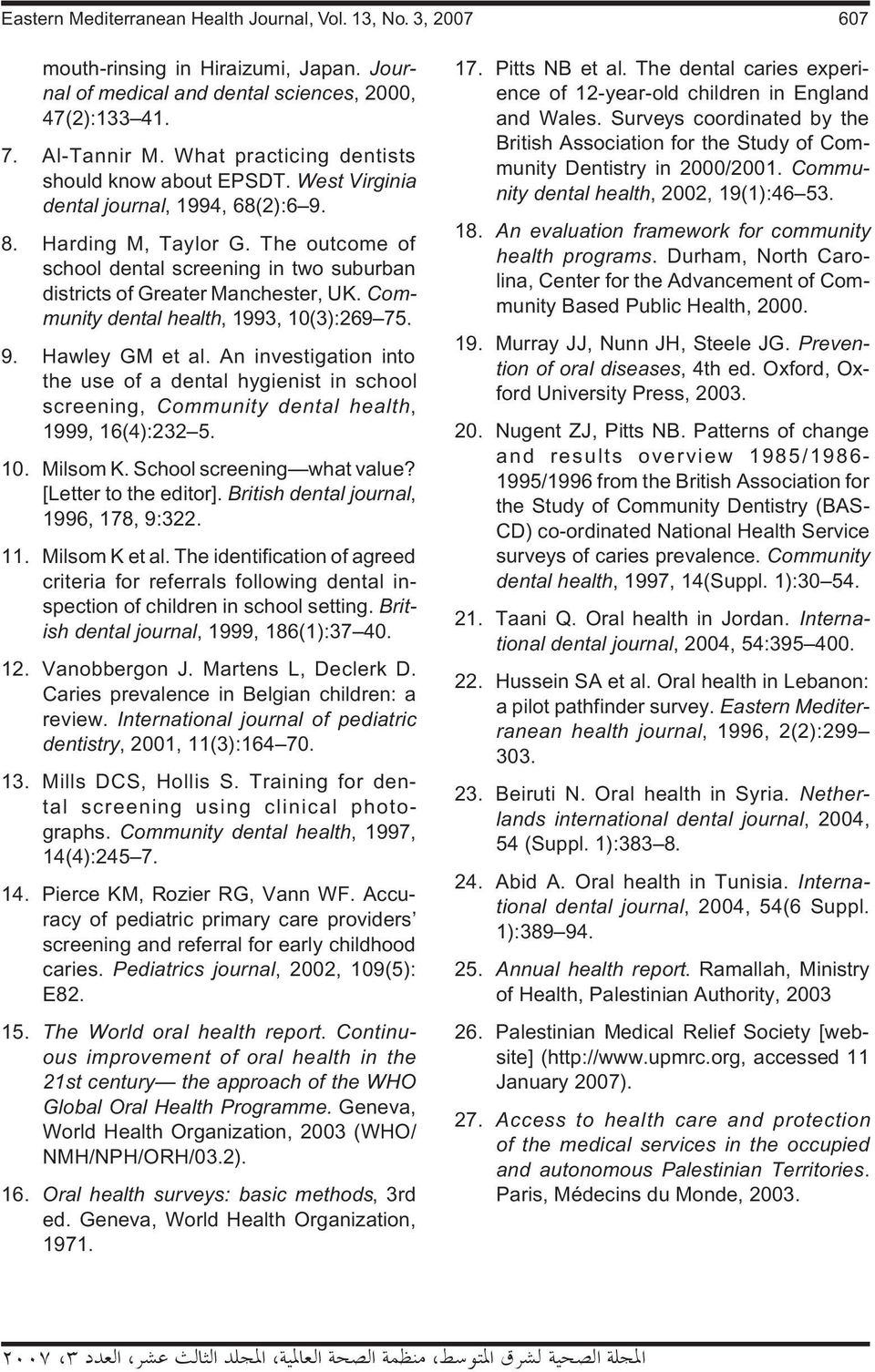
6 The lowest recorded mean DMFT for all areas of the West Bank was 1.35 in 7th grade students and 1.6 in 10th grade in school year The highest DMFT was 2.17 in 7th grade and 2.9 in 10th grade in school year In general, 10th graders had higher DMFT scores than 7th graders. DT index: When the components of DMFT were examined separately, however, we can see that DT was the major contributor to the DMFT scores; FT was the smallest contributor. This was true in both 7th and 10th grades (Figure 3). Thus, although DMFT scores slightly improved over the 7-year period, the DT component had increased while FT and care index remained low. The measure of DT was higher in 10th grade than 7th grade children. Care experience index: The care index ranged from 11.9% to 15.5% for the 7th grade children over the 7-year period of the programme. Care experience indices were higher in 10th grade than 7th grade children (Figure 4). The 7th grade children had a care experience index of 14.8% in school year 2003/04 and 10th graders scored 20% in the same year. Percentage of referred students visiting oral clinics: The analysis showed that a small percentage of referred students attended dental clinics in school years and (Figure 5). The percentage was lowest in Salfit and highest in Jericho. School year had lower values than the preceding year, The mean percentage of students who attended dental clinics increased from 9% in 2002/03 to 11% in 2003/04 school year. Regional variations A wide range of DMFT values were seen across the 9 individual governorates. When analysed by governorate, the highest DMFT was recorded in Salfit (7.8 in 7th grade in school year and 7.0 in 10th grade in school year ), and the lowest DMFT was recorded in Jericho (0.7 in ) and Nablus (0.62 in in 7th grade).
. Thus, although DMFT scores slightly improved over the 7-year period, the DT component had increased while FT and care index remained low.")
7 Comments on the programme performance, administration and equipment extracted from the in-depth interviews with the stakeholders highlighted a number of concerns. These are summarized on Table 1, together with recommendations to address the issues. The 92% coverage rate in the 7th grade cohort (12-years-olds) in 2003/04 could be considered a high figure when compared with an industrialized country such as the United Kingdom (UK). On average, 16% of the total population of children aged 14
 in 2003/04 could be considered a high figure when compared")
8

9

10 years were examined in year , 32% less than in the UK survey [20]. However, the coverage rate in the Palestinian authority MOH s screening programme was calculated from the ratio of examined students to the total number of students. This ratio did not consider the total population in the same age group, which could include children who attend non-public schools or other forms of independent learning. The mean DMFT scores were 1.49 and 1.9 in in 7th and 10th grade respectively. The mean DMFT index compares favourably with some other countries in the region. Jordan scored 3.3 in 1999 [21], Lebanon scored 5.0 in 1996 [22], the Syrian Arab Republic varied between 1.4 and 2.5 in 2004 [23], Egypt scored 1.2 in 1991, and Tunisia scored 1.3 in 1994, Algeria scored 2.3 in 1987, and the Islamic Republic of Iran scored 4.0 in 1992 [24]. However, the West Bank compared less favourably with more developed countries; DMFT ranged from 0.63 to 1.31 in the UK in different regions [17]. Although high DMFT scores indicate high levels of the disease, unchanging DMFT or even a slightly increasing one might indicate a favourable change in care. This is true when all DT components convert to FT components; all the decayed teeth become filled teeth, which points to better treatment services. However, examination of the components of the DMFT index in the 9 governorates of the West Bank did not present this favourable change. DMFT scores in all areas over the 7-year period were largely attributable to the DT components, not the FT. This was also true in the last 2 years when DMFT showed a small reduction. In most of the governorates under study, a slight increase in the DMFT scores after a gradual decrease in the last 3 years was noticed; this could be due to altering the examination strategy in school year Examiners switched from visual inspection to tactile inspection, using mirror and explorer, which is considered more accurate in caries detection. Higher coverage rates demonstrated more representative samples and eventually more accurate DMFT values; this explains the boost in the DMFT index in the 9 governorates in year However, these report results could be more meaningful, if change indicators were weighted according to different coverage rates achieved. There were regional variations in DMFT values across the 9 governorates. The low caries levels in Jericho are likely to be due to the high natural fluoride content in their water resources. Nablus and Ramallah also demonstrated low DMFT and this could be attributed to 3 factors: accessibility: dentists are easier to reach due to the wide availability of public transportation in these urban cities; affordability: these 2 cities are important commercial and political centres in the West Bank, which translates into more job opportunities, and thus higher individual incomes; availability: a high number of dentists work in private practice in these areas. Although the DMF scores of these governorates (Nablus, Ramallah and Jericho) were within normal levels or even lower than WHO recommendations (DMF < 3 for 12-year-olds), the percentage of DT was higher than the FT component in these governorates. This indicates the need to enhance dental care measures among students by increasing awareness of good oral hygiene practices. Meanwhile, the school oral health programme should focus on teeth filling at an early stage of caries and application of fissure sealants.

11 In contrast, Salfit and Qalqiliah presented the highest DMFT scores over the whole programme period; however, due to lack of research, no risk factors have so far been identified in these areas. This great difference in the DMFT values among individual governorates has implications for targeting interventions and services at populations that were identified at risk. The care index results (11.9% to 15.5%) could be considered very low when compared with UK values. The care index mean in the UK was 12% in 1995/96 then improved to 55% in 2002/2003 [17]. Care experience index reflects the restorative care received by those who have suffered disease; it therefore has to be viewed in conjunction with DMFT. These results are of interest in studying the provision of dental services to the age groups under study. Although the mean percentage of students who attended dental clinics increased (from 9% in 2002/03 to 11% in 2003/04), the results are still considered low, when compared with other regions in the world. In Northern Ireland, the school-based dental screening programme stimulated 45% of the screened students to attend dental clinics, in contrast to 27% of the control group [4]. In Davangere, India, the dental screening programme stimulated 31% of screened students to seek dental treatment, compared with only 10% of the control group [5]. In the West Bank, the low percentage of referred students who actually visited dental clinics could be due to the following: Accessibility problems due to difficulties in transportation and checkpoints, curfews and border closures at the Israeli West Bank barrier, especially for students living in rural areas travelling to the city for care. Insufficient oral clinics operated by MOH that offer free treatments (only 17 clinics throughout the West Bank). Oral clinics are clustered in urban areas. Suburbs and rural areas lack this type of service. Inadequate services are provided in those clinics; very little dental specialties are offered. Oral clinics operated by MOH operate only from to hours, the same time period for school attendance. Dentists who carry out curative treatment in the clinics are the same people who are responsible for conducting the school screening; thus they are not always present in the clinics to treat the referred students. Given the political situation in Palestine, the programme operating teams face a number of critical challenges. Like other Palestinians in the West Bank, they suffered from the direct and indirect consequences of military activities and border closures. It is reported that the dental teams and community health workers are prevented from passing through particular Israeli military checkpoints for days or weeks [25]. In addition, checkpoints and road blocks which divide the West Bank into 300 separate clusters cut off 70% of the population from reaching essential health care services for weeks and months [26,27]. Some limitations were also encountered in the data collection process: One of the most important issues that influenced the quality of data collection was the change in examination methods in school year from visual examination only to the use of examination sets which contain probes and mirrors. The percentage of referred students who actually visited oral clinics was available only in the last 2 years. In addition the 10th governorate, Jerusalem, was
![The care index results (11.9% to 15.5%) could be considered very low when compared with UK values. The care index mean in the UK was 12% in 1995/96 then improved to 55% in 2002/2003 [17].](/docs-images/55/8663860/images/page_11.jpg "Care experience index reflects the restorative care received by those who have suffered disease; it therefore has to be viewed in conjunction with DMFT.")
12 added to the screening programme in the last 4 years. The available data from the MOH reports were not always complete because of staff changes and resignations. Finally, continuous change in staff, different training, and lack of commitment to WHO examination criteria [16] make comparability of the data difficult. The existence of the school oral health programme in the Palestinian Authority areas as a database describing school children s oral health represents the commitment of the MOH to improving the school oral health care and services. The slight improvement in DMFT scores in students in some governorates in the last 2 years can be considered progress in caries control. However, maintenance efforts are required to ensure that caries experience at the population level does not rise in disease-stable areas, and an increase in strategic effort is required to address the high caries level in high-risk areas. Many of the problems with delivery of the school oral health programme are symptomatic of the need for substantial improvement in programme management. The programme administrators and operating teams have divergent understandings and expectations of their roles and responsibilities. This is particularly so for observing screening sites, control referrals and followups, and for managing and analysing data. In summary, the MOH strategy for public dental health should use screening data to ensure that priorities for dental health are being properly identified and met, and that responsibilities for policy and operational activities are appropriately assigned and understood between different stakeholders. A national service plan should be developed by the MOH and other collaborators, including a reassessment of the appropriateness of the service planning principles in place, and whether the location and scale of public dental clinics established are meeting the needs of the eligible population. A national oral health promotion strategy should be launched which covers community education, development of an environment supportive of good oral health, facilitation of adequate access to fluoride, support for oral health research and development of a high quality trained workforce.

13
Oral health in Iran. Hamid Reza Pakshir Shiraz, Iran
 International Dental Journal (2004) 54, 367 372 Oral health in Iran Hamid Reza Pakshir Shiraz, Iran The health network in the Islamic Republic (I.R.) of Iran is an integrated public health system with
International Dental Journal (2004) 54, 367 372 Oral health in Iran Hamid Reza Pakshir Shiraz, Iran The health network in the Islamic Republic (I.R.) of Iran is an integrated public health system with
Selecting a School-Based Oral Health Care Program
 Selecting a School-Based Oral Health Care Program Questions and Answers for School Staff Purpose Oral health care delivery within a school setting is a rapidly growing avenue for ensuring that all students
Selecting a School-Based Oral Health Care Program Questions and Answers for School Staff Purpose Oral health care delivery within a school setting is a rapidly growing avenue for ensuring that all students
Dental Health Service in Gezira Locality, Sudan. Abstract
 Dental Health Service in Gezira Locality, Sudan Mogahid Abd El Rahman Yousif DBBS MSc (1), Elhadi Miskeen MRCOG (Part1) (2) (1) Dentist, Deputy Dean Faculty of Dentury, University of Gezira, Sudan (2)
Dental Health Service in Gezira Locality, Sudan Mogahid Abd El Rahman Yousif DBBS MSc (1), Elhadi Miskeen MRCOG (Part1) (2) (1) Dentist, Deputy Dean Faculty of Dentury, University of Gezira, Sudan (2)
State of Mississippi. Oral Health Plan
 State of Mississippi Oral Health Plan 2006 2010 Vision Statement: We envision a Mississippi where every child enjoys optimal oral health; where prevention and health education are emphasized and treatment
State of Mississippi Oral Health Plan 2006 2010 Vision Statement: We envision a Mississippi where every child enjoys optimal oral health; where prevention and health education are emphasized and treatment
Ohio Public Health Association
 Ohio Public Health Association Dental Care Access: A Public Health Issue April 17 th, 2014 Presented by: Audia Ellis, MSN, RN, FNP BC audiaellis@yahoo.com Objectives Evaluate the current state of dental
Ohio Public Health Association Dental Care Access: A Public Health Issue April 17 th, 2014 Presented by: Audia Ellis, MSN, RN, FNP BC audiaellis@yahoo.com Objectives Evaluate the current state of dental
Dental Public Health Activities & Practices
 Dental Public Health Activities & Practices Practice Number: 36001 Submitted By: Oral Health Section, North Carolina Department of Health & Human Services Submission Date: May 2002 Last Updated: January
Dental Public Health Activities & Practices Practice Number: 36001 Submitted By: Oral Health Section, North Carolina Department of Health & Human Services Submission Date: May 2002 Last Updated: January
Nevis Oral Health Survey: Sample of Children Ages 6-8
 Nevis Oral Health Survey: Sample of Children Ages 6-8 Area of Technology and Health Services Delivery Health Services Organization Regional Oral Health Program July 2004 Nevis Oral Health Survey: Sample
Nevis Oral Health Survey: Sample of Children Ages 6-8 Area of Technology and Health Services Delivery Health Services Organization Regional Oral Health Program July 2004 Nevis Oral Health Survey: Sample
Impact of Removing Clinical Preventive Oral Health Services from Ontario Public Health Standards
 STAFF REPORT ACTION REQUIRED Impact of Removing Clinical Preventive Oral Health Services from Ontario Public Health Standards Date: August 1, 2014 To: From: Wards: Board of Health Medical Officer of Health
STAFF REPORT ACTION REQUIRED Impact of Removing Clinical Preventive Oral Health Services from Ontario Public Health Standards Date: August 1, 2014 To: From: Wards: Board of Health Medical Officer of Health
VARNISH! MICHIGAN BABIES TOO!
 VARNISH! MICHIGAN BABIES TOO! 2012-2013 Annual Report The Varnish! Michigan Babies Too! Program was developed as an incentive for medical providers to have oral health training and begin an oral health
VARNISH! MICHIGAN BABIES TOO! 2012-2013 Annual Report The Varnish! Michigan Babies Too! Program was developed as an incentive for medical providers to have oral health training and begin an oral health
IMPROVING DENTAL CARE AND ORAL HEALTH A CALL TO ACTION EVIDENCE RESOURCE PACK
 IMPROVING DENTAL CARE AND ORAL HEALTH A CALL TO ACTION EVIDENCE RESOURCE PACK NHS England Dental Analytical Team February 2013/14 Gateway reference: 01173 Introduction to this pack This data pack has been
IMPROVING DENTAL CARE AND ORAL HEALTH A CALL TO ACTION EVIDENCE RESOURCE PACK NHS England Dental Analytical Team February 2013/14 Gateway reference: 01173 Introduction to this pack This data pack has been
Promising Practices to Improve Access to Oral Health Care in Rural Communities
 Rural Evaluation Brief February 2013 Y Series - No. 7 NORC WALSH CENTER FOR RURAL HEALTH ANALYSIS http://walshcenter.norc.org Rural Health Research Center UNIVERSITY OF MINNESOTA www.sph.umn.edu/hpm/rhrc/
Rural Evaluation Brief February 2013 Y Series - No. 7 NORC WALSH CENTER FOR RURAL HEALTH ANALYSIS http://walshcenter.norc.org Rural Health Research Center UNIVERSITY OF MINNESOTA www.sph.umn.edu/hpm/rhrc/
Although largely preventable by early examination, identification of
 The Consequences of Untreated Dental Disease in Children Poor oral health in infants and children destroys more than just a smile. Although largely preventable by early examination, identification of individual
The Consequences of Untreated Dental Disease in Children Poor oral health in infants and children destroys more than just a smile. Although largely preventable by early examination, identification of individual
Community Dental Health Coordinator- New Member of the Dental Access to Care Team
 Community Dental Health Coordinator- New Member of the Dental Access to Care Team National Network for Oral Health Access August 2014 Jane Grover DDS MPH- Director Council on Access, Prevention and Interprofessional
Community Dental Health Coordinator- New Member of the Dental Access to Care Team National Network for Oral Health Access August 2014 Jane Grover DDS MPH- Director Council on Access, Prevention and Interprofessional
How To Conduct A Dental Public Health Activity
 Dental Public Health Activities & Practices Practice Number: 49003 Submitted By: Methodist Healthcare Ministries Submission Date: September 2009 Last Updated: September 2009 SECTION I: PRACTICE OVERVIEW
Dental Public Health Activities & Practices Practice Number: 49003 Submitted By: Methodist Healthcare Ministries Submission Date: September 2009 Last Updated: September 2009 SECTION I: PRACTICE OVERVIEW
Oral health and dental care in Australia
 Oral health and dental care in Australia Key facts and figures trends 2014 Oral health and dental care in Australia Key facts and figures trends 2014 Oral health and dental care in Australia: Key facts
Oral health and dental care in Australia Key facts and figures trends 2014 Oral health and dental care in Australia Key facts and figures trends 2014 Oral health and dental care in Australia: Key facts
The State of Oral Health in Europe. Professor Kenneth Eaton Chair of the Platform for Better Oral Health in Europe
 The State of Oral Health in Europe Professor Kenneth Eaton Chair of the Platform for Better Oral Health in Europe 1 TOPICS TO BE COVERED What is the Platform? Its aims and work The report (State of Oral
The State of Oral Health in Europe Professor Kenneth Eaton Chair of the Platform for Better Oral Health in Europe 1 TOPICS TO BE COVERED What is the Platform? Its aims and work The report (State of Oral
Innovative State Practices for Improving The Provision of Medicaid Dental Services:
 Innovative State Practices for Improving The Provision of Medicaid Dental Services: SUMMARY OF EIGHT STATE REPORTS: (Alabama, Arizona, Maryland, Nebraska, North Carolina, Rhode Island, Texas and Virginia)
Innovative State Practices for Improving The Provision of Medicaid Dental Services: SUMMARY OF EIGHT STATE REPORTS: (Alabama, Arizona, Maryland, Nebraska, North Carolina, Rhode Island, Texas and Virginia)
Dental Health Services in Canada
 Dental Health Services in Canada Facts and Figures 2010 Canadian Dental Association Number of Dentists In January 2010, there were 19,563 licensed dentists in Canada. Approximately 89% were in general
Dental Health Services in Canada Facts and Figures 2010 Canadian Dental Association Number of Dentists In January 2010, there were 19,563 licensed dentists in Canada. Approximately 89% were in general
FREQUENTLY ASKED QUESTIONS: ORAL HEALTH IN NEW ZEALAND
 ORAL HEALTH IN NEW ZEALAND What is the oral health status of New Zealand? There are two measures of oral health in New Zealand: The percentage of five-year-olds that are free of dental decay ( caries free
ORAL HEALTH IN NEW ZEALAND What is the oral health status of New Zealand? There are two measures of oral health in New Zealand: The percentage of five-year-olds that are free of dental decay ( caries free
Issue Brief: Expanding Access to Oral Health Care in Idaho
 Issue Brief: Expanding Access to Oral Health Care in Idaho Oral diseases can be attributed to bacterial infections that, if left untreated, can affect other systems of the body. A growing number of studies
Issue Brief: Expanding Access to Oral Health Care in Idaho Oral diseases can be attributed to bacterial infections that, if left untreated, can affect other systems of the body. A growing number of studies
The New Dental Law Schemes in Minnesota - 2008
 Scandrett 1 Minnesota s New Mid-level Dental Practitioner National Academy for State Health Policy Michael Scandrett Minnesota Safety Net Coalition Halleland Health Consulting Scandrett 2 Minnesota s s
Scandrett 1 Minnesota s New Mid-level Dental Practitioner National Academy for State Health Policy Michael Scandrett Minnesota Safety Net Coalition Halleland Health Consulting Scandrett 2 Minnesota s s
Evidence Review: Dental Health Population and Public Health BC Ministry of Health
 Evidence Review: Population and Public Health BC Ministry of Health March 2014 (update from September 2006) This is a review of evidence and best practice that should be seen as a guide to understanding
Evidence Review: Population and Public Health BC Ministry of Health March 2014 (update from September 2006) This is a review of evidence and best practice that should be seen as a guide to understanding
Kansas Dental Project Joint Venture
 Kansas Dental Project Joint Venture Purpose In 2009, the W.K. Kellogg Foundation launched a national initiative to expand access to oral health care through innovative and community-driven solutions to
Kansas Dental Project Joint Venture Purpose In 2009, the W.K. Kellogg Foundation launched a national initiative to expand access to oral health care through innovative and community-driven solutions to
THE PUBLIC HEALTH DENTAL HYGIENE PRACTITIONER ROLE IN MANAGED CARE ORGANIZATIONS. A Fact Sheet Prepared by the PA Dental Hygienists Association
 THE PUBLIC HEALTH DENTAL HYGIENE PRACTITIONER ROLE IN MANAGED CARE ORGANIZATIONS A Fact Sheet Prepared by the PA Dental Hygienists Association Background Bill establishing PHDHPs passed and signed into
THE PUBLIC HEALTH DENTAL HYGIENE PRACTITIONER ROLE IN MANAGED CARE ORGANIZATIONS A Fact Sheet Prepared by the PA Dental Hygienists Association Background Bill establishing PHDHPs passed and signed into
DENTAL AND DENTAL HYGIENE. Chapter 65, Article 1 lists KDB Permanent Administrative Regulations http://www.accesskansas.org/kdb/regulations.
 EXTENDED CARE PERMIT DENTAL AND DENTAL HYGIENE Knowing the laws governing dental hygiene and more specifically dental hygiene services in community settings is essential for all involved in ECP hygiene
EXTENDED CARE PERMIT DENTAL AND DENTAL HYGIENE Knowing the laws governing dental hygiene and more specifically dental hygiene services in community settings is essential for all involved in ECP hygiene
CMS oral Health Initiative an opportunity for Dental Hygienists April 23 rd 2015 Nancy Gurzick, RDH, BSDH, MA
 CMS oral Health Initiative an opportunity for Dental Hygienists April 23 rd 2015 Nancy Gurzick, RDH, BSDH, MA Course objectives Part I Federal and State Oral Health Programs Understanding Medicaid/Federal
CMS oral Health Initiative an opportunity for Dental Hygienists April 23 rd 2015 Nancy Gurzick, RDH, BSDH, MA Course objectives Part I Federal and State Oral Health Programs Understanding Medicaid/Federal
Promoting Oral Health
 Promoting Oral Health Oral diseases are among the most prevalent health problems in the United States. The 198 Surgeon General's Report to the Nation listed dental disease as a critical health problem
Promoting Oral Health Oral diseases are among the most prevalent health problems in the United States. The 198 Surgeon General's Report to the Nation listed dental disease as a critical health problem
 AN ACT RELATING TO DENTISTRY; CHANGING THE LICENSING OF DENTISTS AND DENTAL HYGIENISTS BY CREDENTIAL; EXPANDING THE SCOPE OF PRACTICE OF DENTAL HYGIENISTS. BE IT ENACTED BY THE LEGISLATURE OF THE STATE
AN ACT RELATING TO DENTISTRY; CHANGING THE LICENSING OF DENTISTS AND DENTAL HYGIENISTS BY CREDENTIAL; EXPANDING THE SCOPE OF PRACTICE OF DENTAL HYGIENISTS. BE IT ENACTED BY THE LEGISLATURE OF THE STATE
Dental Public Health Activity Descriptive Report
 Dental Public Health Activity Descriptive Report Practice Number: 04006 Submitted By: Office of Oral Health, Arizona Department of Health Services Submission Date: May 2002 Last Updated: November 2013
Dental Public Health Activity Descriptive Report Practice Number: 04006 Submitted By: Office of Oral Health, Arizona Department of Health Services Submission Date: May 2002 Last Updated: November 2013
Red Lake Nation School Dental Prevention Program
 Red Lake Comprehensive Health Services Red Lake Nation School Dental Prevention Program Cathy Jo Gunvalson School Dental Hygienist Celia Littlecreek School Dental Assistant 24760 Hospital Drive Red Lake,
Red Lake Comprehensive Health Services Red Lake Nation School Dental Prevention Program Cathy Jo Gunvalson School Dental Hygienist Celia Littlecreek School Dental Assistant 24760 Hospital Drive Red Lake,
Michigan Department of Health and Human Services Mobile Dental Program. Erin Suddeth, RDH, BS, MPA Public Health Consultant Oral Health
 Michigan Department of Health and Human Services Mobile Dental Program Erin Suddeth, RDH, BS, MPA Public Health Consultant Oral Health What is PA 100: Mobile Dental Facility? Application For Mobile Dental
Michigan Department of Health and Human Services Mobile Dental Program Erin Suddeth, RDH, BS, MPA Public Health Consultant Oral Health What is PA 100: Mobile Dental Facility? Application For Mobile Dental
2013-2014. Saskatchewan Dental Health Screening Program Report
 2013-2014 Saskatchewan Dental Health Screening Program Report Simran Singh Gill September, 2014 i Saskatchewan Dental Health Screening Program Report 2013-14 ii Table of Contents List of Tables & Figures...
2013-2014 Saskatchewan Dental Health Screening Program Report Simran Singh Gill September, 2014 i Saskatchewan Dental Health Screening Program Report 2013-14 ii Table of Contents List of Tables & Figures...
How To Improve Health Care For Children
 STATE ORAL HEALTH ACTION PLAN (SOHAP) TEMPLATE FOR MEDICAID AND CHIP PROGRAMS STATE: Michigan PROGRAM TYPE ADDRESSED IN TEMPLATE: MEDICAID ONLY X COMBINED MEDICAID AND CHP STATE MEDICAL DENTAL PROGRAM
STATE ORAL HEALTH ACTION PLAN (SOHAP) TEMPLATE FOR MEDICAID AND CHIP PROGRAMS STATE: Michigan PROGRAM TYPE ADDRESSED IN TEMPLATE: MEDICAID ONLY X COMBINED MEDICAID AND CHP STATE MEDICAL DENTAL PROGRAM
Count Your Smiles. Count Your Smiles
 Count Your Smiles 2011-2012 Count Count Your Your Smiles Smiles i ACKNOWLEDGEMENTS State of Michigan Governor Rick Snyder May 2011 Michigan Department of Community Health Director Olga Dazzo Public Health
Count Your Smiles 2011-2012 Count Count Your Your Smiles Smiles i ACKNOWLEDGEMENTS State of Michigan Governor Rick Snyder May 2011 Michigan Department of Community Health Director Olga Dazzo Public Health
Innovative Approaches To The Evaluation and Treatment of Early Childhood Caries
 Innovative Approaches To The Evaluation and Treatment of Early Childhood Caries Terry Yonker, RN MS, FNP Finger Lakes Community Health Telemedicine Clinical Coordinator Penn Yan, NY Learning Outcomes Discuss
Innovative Approaches To The Evaluation and Treatment of Early Childhood Caries Terry Yonker, RN MS, FNP Finger Lakes Community Health Telemedicine Clinical Coordinator Penn Yan, NY Learning Outcomes Discuss
Dental Public Health Activity Descriptive Report
 Dental Public Health Activity Descriptive Report Practice Number: 06005 Submitted By: New York State Department of Health Bureau of Dental Health Submission Date: January 2012 Last Updated: January 2012
Dental Public Health Activity Descriptive Report Practice Number: 06005 Submitted By: New York State Department of Health Bureau of Dental Health Submission Date: January 2012 Last Updated: January 2012
Dental Therapists in New Zealand: What the Evidence Shows
 Issue Brief PROJECT Children s NAME Dental Campaign Dental Therapists in New Zealand: What the Evidence Shows Dental decay remains the most common chronic childhood disease in the United States. 1 More
Issue Brief PROJECT Children s NAME Dental Campaign Dental Therapists in New Zealand: What the Evidence Shows Dental decay remains the most common chronic childhood disease in the United States. 1 More
School-Based Oral Health Care. A Choice for Michigan Children.indd 1
 School-Based Oral Health Care A Choice for Michigan Children School Based Oral Health Care: A Choice for Michigan Children is part of an information set meant to serve as a guideline for school personnel
School-Based Oral Health Care A Choice for Michigan Children School Based Oral Health Care: A Choice for Michigan Children is part of an information set meant to serve as a guideline for school personnel
Children s Dental Health in the United Kingdom, 2003
 Children s Dental Health in the United Kingdom, 2003 Summary Report Deborah Lader Barbara Chadwick Ivor Chestnutt Rachael Harker John Morris Nigel Nuttall Nigel Pitts Jimmy Steele Deborah White Crown copyright
Children s Dental Health in the United Kingdom, 2003 Summary Report Deborah Lader Barbara Chadwick Ivor Chestnutt Rachael Harker John Morris Nigel Nuttall Nigel Pitts Jimmy Steele Deborah White Crown copyright
State of North Carolina. Medicaid Dental Review
 State of North Carolina Medicaid Dental Review October 2010 EXECUTIVE SUMMARY The Centers for Medicare & Medicaid Services (CMS) is committed to improving pediatric dental care in the Medicaid program
State of North Carolina Medicaid Dental Review October 2010 EXECUTIVE SUMMARY The Centers for Medicare & Medicaid Services (CMS) is committed to improving pediatric dental care in the Medicaid program
Dental Hygienist. Dental hygienists help maintain the dental health of their patients and educate them about proper oral hygiene.
 Dental Hygienist At a Glance Dental hygienists help maintain the dental health of their patients and educate them about proper oral hygiene. Search by Cluster Medical & Health Typical Range: 55K - 73K
Dental Hygienist At a Glance Dental hygienists help maintain the dental health of their patients and educate them about proper oral hygiene. Search by Cluster Medical & Health Typical Range: 55K - 73K
Phase I Summary Document: Revising the Fluoride Mouthrinse Program
 Phase I Summary Document: Revising the Fluoride Mouthrinse Program Ad Hoc Committee for the Review of the Nova Scotia Fluoride Mouthrinse (FMR) Program May, 2002 Table of Contents BACKGROUND INFORMATION...
Phase I Summary Document: Revising the Fluoride Mouthrinse Program Ad Hoc Committee for the Review of the Nova Scotia Fluoride Mouthrinse (FMR) Program May, 2002 Table of Contents BACKGROUND INFORMATION...
SmileNet SM Dental Discount Program
 SmileNet SM Dental Discount Program We want to catch you smiling. for Individuals and Families SpecialOffers This program is provided by Anthem Blue Cross Life and Health Insurance Company as a service
SmileNet SM Dental Discount Program We want to catch you smiling. for Individuals and Families SpecialOffers This program is provided by Anthem Blue Cross Life and Health Insurance Company as a service
DERBYSHIRE COUNTY COUNCIL CABINET. 06 May 2014. Report of the Director of Public Health. DENTAL PUBLIC HEALTH IN DERBYSHIRE (Health and Communities)
") PUBLIC Author: Alison Pritchard Agenda Item No.7 (g) DERBYSHIRE COUNTY COUNCIL CABINET 06 May 2014 Report of the Director of Public Health DENTAL PUBLIC HEALTH IN DERBYSHIRE (Health and Communities) 1.
PUBLIC Author: Alison Pritchard Agenda Item No.7 (g) DERBYSHIRE COUNTY COUNCIL CABINET 06 May 2014 Report of the Director of Public Health DENTAL PUBLIC HEALTH IN DERBYSHIRE (Health and Communities) 1.
Nebraska Oral Health State Plan. DRAFT September 7, 2011
 Nebraska Oral Health State Plan DRAFT September 7, 2011 Letter to Stakeholders/ Public Acknowledgements List of Stakeholders and Contributors Table of Contents Process and Purpose of Plan A State Oral
Nebraska Oral Health State Plan DRAFT September 7, 2011 Letter to Stakeholders/ Public Acknowledgements List of Stakeholders and Contributors Table of Contents Process and Purpose of Plan A State Oral
Non-carious dental conditions
 Non-carious dental conditions Children s Dental Health in the United Kingdom, 2003 Barbara Chadwick, Liz Pendry October 2004 Crown copyright 2004 Office for National Statistics 1 Drummond Gate London SW1V
Non-carious dental conditions Children s Dental Health in the United Kingdom, 2003 Barbara Chadwick, Liz Pendry October 2004 Crown copyright 2004 Office for National Statistics 1 Drummond Gate London SW1V
Position Paper on Access to Oral Health Care for Canadians
 Position Paper on Access to Oral Health Care for Canadians Approved CDA Board of Directors May 2010 Preamble A daily regimen of brushing and flossing is an important part of good oral health while equitable
Position Paper on Access to Oral Health Care for Canadians Approved CDA Board of Directors May 2010 Preamble A daily regimen of brushing and flossing is an important part of good oral health while equitable
Public insurance for dental care for chidren
 Public insurance for dental care for chidren Country: Israel Partner Institute: The Myers-JDC-Brookdale Institute, Jerusalem Survey no: (16)2010 Author(s): Nir Kaidar, Tuvia Horev and Bruce Rosen Health
Public insurance for dental care for chidren Country: Israel Partner Institute: The Myers-JDC-Brookdale Institute, Jerusalem Survey no: (16)2010 Author(s): Nir Kaidar, Tuvia Horev and Bruce Rosen Health
Aurora Health Access to Dental Services For Senior Citizens
 2016 GUIDE TO SENIOR ORAL HEALTH RESOURCES IN AURORA The Aurora Health Access Senior Circle, working together with the Aurora Commission for Seniors, compiled the following guide to senior oral health
2016 GUIDE TO SENIOR ORAL HEALTH RESOURCES IN AURORA The Aurora Health Access Senior Circle, working together with the Aurora Commission for Seniors, compiled the following guide to senior oral health
HEALTH MASTER PLAN SRI LANKA HEALTH & SHINING ISLAND IN THE 21 ST CENTURY PROJECT PROFILES. Other Units FEBRUARY 2009 MINISTRY OF HEALTH & NUTRITION
 HEALTH MASTER PLAN SRI LANKA HEALTH & SHINING ISLAND IN THE 21 ST CENTURY PROJECT PROFILES Other Units FEBRUARY 2009 MINISTRY OF HEALTH & NUTRITION Reporting Directors DDG/BES Project No Programme or Project
HEALTH MASTER PLAN SRI LANKA HEALTH & SHINING ISLAND IN THE 21 ST CENTURY PROJECT PROFILES Other Units FEBRUARY 2009 MINISTRY OF HEALTH & NUTRITION Reporting Directors DDG/BES Project No Programme or Project
California HealthCare Foundation. Emergency Department Visits and Hospitalizations for Preventable Dental Conditions. Projects in Oral Health
 Emergency Department Visits and Hospitalizations for Preventable Dental Conditions California HealthCare Foundation April 2009 Lisa Maiuro, Ph.D., Health Management Associates Len Finocchio, Dr.P.H. California
Emergency Department Visits and Hospitalizations for Preventable Dental Conditions California HealthCare Foundation April 2009 Lisa Maiuro, Ph.D., Health Management Associates Len Finocchio, Dr.P.H. California
Fluoridation Position Statement
 Fluoridation Position Statement Part B of the Oral Health Strategy relates to a separate document on a detailed Oral Health Strategy for the CDHB 1 PART A Fluoridation position statement 2 TABLE OF CONTENTS
Fluoridation Position Statement Part B of the Oral Health Strategy relates to a separate document on a detailed Oral Health Strategy for the CDHB 1 PART A Fluoridation position statement 2 TABLE OF CONTENTS
Executive Summary: Adult Dental Health Survey 2009
 Executive Summary: Adult Dental Health Survey 2009 Copyright 2011, The Health and Social Care Information Centre. All Rights Reserved. 1 The NHS Information Centre is England s central, authoritative source
Executive Summary: Adult Dental Health Survey 2009 Copyright 2011, The Health and Social Care Information Centre. All Rights Reserved. 1 The NHS Information Centre is England s central, authoritative source
Vermont Oral Health Plan 2014
 Vermont Oral Health Plan 2014 Table of Contents INTRODUCTION TO VERMONT ORAL HEALTH PLAN 2013... 3 THE BURDEN OF ORAL DISEASE IN VERMONT... 6 Children... 6 Adults... 8 Older Adults... 10 Disparities...
Vermont Oral Health Plan 2014 Table of Contents INTRODUCTION TO VERMONT ORAL HEALTH PLAN 2013... 3 THE BURDEN OF ORAL DISEASE IN VERMONT... 6 Children... 6 Adults... 8 Older Adults... 10 Disparities...
Oral Health Coding Fact Sheet for Primary Care Physicians
 2015 Oral Health Coding Fact Sheet for Primary Care Physicians CPT Codes: Current Procedural Terminology (CPT) codes are developed and maintained by the American Medical Association. The codes consist
2015 Oral Health Coding Fact Sheet for Primary Care Physicians CPT Codes: Current Procedural Terminology (CPT) codes are developed and maintained by the American Medical Association. The codes consist
Dual Degree Programs in Dental Education: Exploring Benefits and Challenges
 Dual Degree Programs in Dental Education: Exploring Benefits and Challenges SESSION OBJECTIVES Describe how existing dual degree program models can be implemented in dental schools. Identify how a dual
Dual Degree Programs in Dental Education: Exploring Benefits and Challenges SESSION OBJECTIVES Describe how existing dual degree program models can be implemented in dental schools. Identify how a dual
Dental Public Health Activities & Practices
 Dental Public Health Activities & Practices Practice Number: 15001 Submitted By: Oral Health Program, Idaho Department of Health and Welfare Submission Date: April 2002 Last Updated: April 2002 Name of
Dental Public Health Activities & Practices Practice Number: 15001 Submitted By: Oral Health Program, Idaho Department of Health and Welfare Submission Date: April 2002 Last Updated: April 2002 Name of
kaiser medicaid and the uninsured commission on June 2012 Children and Oral Health: Assessing Needs, Coverage, and Access
 P O L I C Y B R I E F kaiser commission on medicaid and the uninsured Children and Oral Health: Assessing Needs, Coverage, and Access 1330 G S T R E E T NW, W A S H I N G T O N, DC 20005 P H O N E: (202)
P O L I C Y B R I E F kaiser commission on medicaid and the uninsured Children and Oral Health: Assessing Needs, Coverage, and Access 1330 G S T R E E T NW, W A S H I N G T O N, DC 20005 P H O N E: (202)
www.ochaopt.org United Nations Office for the Coordination of Humanitarian Affairs occupied Palestinian territory
 In the Spotlight opt AREA C Vulnerability Profile The Vulnerability Profile Project (VPP), launched in 013, is an inter-agency exercise designed to identify vulnerabilities in Area C 1. This feature provides
In the Spotlight opt AREA C Vulnerability Profile The Vulnerability Profile Project (VPP), launched in 013, is an inter-agency exercise designed to identify vulnerabilities in Area C 1. This feature provides
AWARENESS OF THE ORAL HEALTH OF PEDIATRIC PATIENTS AMONG THE PEDIATRICIANS IN AHMEDABAD CITY- AN EPIDEMIOLOGICAL RESEARCH
 ORIGINAL ARTICLE AWARENESS OF THE ORAL HEALTH OF PEDIATRIC PATIENTS AMONG THE PEDIATRICIANS IN AHMEDABAD CITY- AN EPIDEMIOLOGICAL RESEARCH Maithilee Jani 1, Anshul Shah 1, Ajay Pala 2 B.D.S, 1 Ahmedabad
ORIGINAL ARTICLE AWARENESS OF THE ORAL HEALTH OF PEDIATRIC PATIENTS AMONG THE PEDIATRICIANS IN AHMEDABAD CITY- AN EPIDEMIOLOGICAL RESEARCH Maithilee Jani 1, Anshul Shah 1, Ajay Pala 2 B.D.S, 1 Ahmedabad
the virtual dental home Improving the oral health of vulnerable and underserved populations using geographically distributed telehealth-enabled teams
 policy brief the virtual dental home Improving the oral health of vulnerable and underserved populations using geographically distributed telehealth-enabled teams May, 2013 Pacific Center for Special Care
policy brief the virtual dental home Improving the oral health of vulnerable and underserved populations using geographically distributed telehealth-enabled teams May, 2013 Pacific Center for Special Care
Health Priority: Access to Primary and Preventive Health Services Objective 4: Access to Oral Health Services
 Health Priority: Access to Primary and Preventive Health Services Objective 4: Access to Oral Health Services Long Term (2010) Subcommittee Outcome Objective: By 2010, increase by 10 percentage points
Health Priority: Access to Primary and Preventive Health Services Objective 4: Access to Oral Health Services Long Term (2010) Subcommittee Outcome Objective: By 2010, increase by 10 percentage points
Oral health and dental care in Australia
 Oral health and dental care in Australia Key facts and figures 2011 Sergio Chrisopoulos Research Associate Katie Beckwith Research Officer Jane Harford Research Fellow Australian Research Centre for Population
Oral health and dental care in Australia Key facts and figures 2011 Sergio Chrisopoulos Research Associate Katie Beckwith Research Officer Jane Harford Research Fellow Australian Research Centre for Population
California s State Oral Health Infrastructure: Opportunities for Improvement and Funding
 California s State Oral Health Infrastructure: Opportunities for Improvement and Funding joel diringer, jd, mph, and kathy r. phipps, drph, rdh abstract California has virtually no statewide dental public
California s State Oral Health Infrastructure: Opportunities for Improvement and Funding joel diringer, jd, mph, and kathy r. phipps, drph, rdh abstract California has virtually no statewide dental public
The New Providers WA State. Important State Document. Hospital ER Visits: Washington State
 The New Providers WA State Professor Rebecca L. Stolberg, RDH, BSDH, MSDH Important State Document Washington State s Oral Health Workforce (December 2009) http://www.ws-ohc.org/plan/chws_fr130_skillman.pdf
The New Providers WA State Professor Rebecca L. Stolberg, RDH, BSDH, MSDH Important State Document Washington State s Oral Health Workforce (December 2009) http://www.ws-ohc.org/plan/chws_fr130_skillman.pdf
By Jane Meredith Adams
 Schooll s sttrrugglle tto prro safety viide netdenttall healltt March 31st, 2013 Add a Comment By Jane Meredith Adams Like 3 Share Share Students learn how to care for their teeth and receive preventive
Schooll s sttrrugglle tto prro safety viide netdenttall healltt March 31st, 2013 Add a Comment By Jane Meredith Adams Like 3 Share Share Students learn how to care for their teeth and receive preventive
WMI Mutual Insurance Company
 Dental Policy WMI Mutual Insurance Company PO Box 572450 Salt Lake City, UT 84157 (801) 263-8000 & (800) 748-5340 Fax: (801) 263-1247 DENTAL POLICY A. Schedule of Benefits: Annual Maximum Dental Benefit
Dental Policy WMI Mutual Insurance Company PO Box 572450 Salt Lake City, UT 84157 (801) 263-8000 & (800) 748-5340 Fax: (801) 263-1247 DENTAL POLICY A. Schedule of Benefits: Annual Maximum Dental Benefit
Career paths and opportunities for the Dental Assistant
 Career paths and opportunities for the Dental Assistant Ms Eleanor Schroeder Program Coordinator Dental Assistant Programs Session overview Career pathways for the qualified Dental Assistant (Certificate
Career paths and opportunities for the Dental Assistant Ms Eleanor Schroeder Program Coordinator Dental Assistant Programs Session overview Career pathways for the qualified Dental Assistant (Certificate
CHAPTER 5 BEST PRACTICES IN ORAL HEALTH POLICIES
 CHAPTER 5 BEST PRACTICES IN ORAL HEALTH POLICIES 5.1 FINDINGS 5.1.1 POLICY LEVEL BEST PRACTICES A research team from University of Mississippi attempted to identify sustainable programs and policies with
CHAPTER 5 BEST PRACTICES IN ORAL HEALTH POLICIES 5.1 FINDINGS 5.1.1 POLICY LEVEL BEST PRACTICES A research team from University of Mississippi attempted to identify sustainable programs and policies with
Impact and Opportunities for Integrated Medical and Dental Care Management under the Affordable Care Act
 Impact and Opportunities for Integrated Medical and Dental Care Management under the Affordable Care Act A Federal Perspective David Williams, Ph.D. Objective of this presentation: To share the Federal
Impact and Opportunities for Integrated Medical and Dental Care Management under the Affordable Care Act A Federal Perspective David Williams, Ph.D. Objective of this presentation: To share the Federal
Financing. Objective 1: Comprehensive dental benefits are available to low-income Kansans through an expansion of KanCare benefits.
 Financing Kansans have a way to pay for high-quality, affordable dental services. Dental parity and consumer understanding of insurance policies are essential elements of success. Objective 1: Comprehensive
Financing Kansans have a way to pay for high-quality, affordable dental services. Dental parity and consumer understanding of insurance policies are essential elements of success. Objective 1: Comprehensive
Ann A. Stueck, MSN,RN
 Integrating Bright Futures into Public Health at the State and Local Levels Oral Health Theme Murray L. Katcher, MD, PhD, FAAP Moderator Chief Medical Officer for Community Health Promotion State MCH Medical
Integrating Bright Futures into Public Health at the State and Local Levels Oral Health Theme Murray L. Katcher, MD, PhD, FAAP Moderator Chief Medical Officer for Community Health Promotion State MCH Medical
Curriculum Vitae Ahmed Abdel Rhman Mohamed Ali. Ahmed Abdel Rahman Mohamed Ali Beirut Arab University. (961) 1 300110 ext: 2715
 1 300110 ext: 2715") PERSONAL INFORMATION Curriculum Vitae Ahmed Abdel Rhman Mohamed Ali Ahmed Abdel Rahman Mohamed Ali Beirut Arab University (961) 1 300110 ext: 2715 abdelrahman@bau.edu.lb Gender Male Date of birth 27/08/1949
PERSONAL INFORMATION Curriculum Vitae Ahmed Abdel Rhman Mohamed Ali Ahmed Abdel Rahman Mohamed Ali Beirut Arab University (961) 1 300110 ext: 2715 abdelrahman@bau.edu.lb Gender Male Date of birth 27/08/1949
Region of Waterloo Public Health Dental Health Program Report 2011-2014. April 2015
 Region of Waterloo Public Health Dental Health Program Report 2011-2014 April 2015 Authors: Grace Bermingham, Chris Harold, Jan Herbison, Dr. Robert Hawkins and Meghan Randall Contributors: Kerri Hutchinson
Region of Waterloo Public Health Dental Health Program Report 2011-2014 April 2015 Authors: Grace Bermingham, Chris Harold, Jan Herbison, Dr. Robert Hawkins and Meghan Randall Contributors: Kerri Hutchinson
Improving oral health in England: Piloting Dental Care. The English experience
 Improving oral health in England: Piloting Dental Care The English experience Jimmy Steele Newcastle University Sue Gregory Deputy CDO: Department of Health The case for change 1. The changing population
Improving oral health in England: Piloting Dental Care The English experience Jimmy Steele Newcastle University Sue Gregory Deputy CDO: Department of Health The case for change 1. The changing population
A Review of Indonesia s Dental Health - Past, Present and Future
 Review Article Int J Clin Prev Dent 2014;10(3):121-126ㆍhttp://dx.doi.org/10.15236/ijcpd.2014.10.3.121 ISSN (Print) 1738-8546ㆍISSN (Online) 2287-6197 A Review of Indonesia s Dental Health - Past, Present
Review Article Int J Clin Prev Dent 2014;10(3):121-126ㆍhttp://dx.doi.org/10.15236/ijcpd.2014.10.3.121 ISSN (Print) 1738-8546ㆍISSN (Online) 2287-6197 A Review of Indonesia s Dental Health - Past, Present
Oral Health Program. Strategic Plan. U.S. Department of Health and Human Services Centers for Disease Control and Prevention
 Oral Health Program Strategic Plan 2011 2014 U.S. Department of Health and Human Services Centers for Disease Control and Prevention Centers for Disease Control and Prevention National Center for Chronic
Oral Health Program Strategic Plan 2011 2014 U.S. Department of Health and Human Services Centers for Disease Control and Prevention Centers for Disease Control and Prevention National Center for Chronic
Frequently Asked Questions (FAQs)
") Cisco Systems LifeConnections Dental Center Frequently Asked Questions (FAQs) December 2013 Contents General 1. What is Cisco s LifeConnections Health Center?... 3 2. What dental care services are available
Cisco Systems LifeConnections Dental Center Frequently Asked Questions (FAQs) December 2013 Contents General 1. What is Cisco s LifeConnections Health Center?... 3 2. What dental care services are available
DESCRIPTION of the ORAL HEALTH CARE in ROMANIA
 OVIDIUS UNIVERSITY CONSTANTA FACULTY OF DENTAL MEDICINE EADPH 2010 15 th Annual Meeting// September 9-11 // Constanta, ROMANIA DESCRIPTION of the ORAL HEALTH CARE in ROMANIA Corneliu AMARIEI, Cristina
OVIDIUS UNIVERSITY CONSTANTA FACULTY OF DENTAL MEDICINE EADPH 2010 15 th Annual Meeting// September 9-11 // Constanta, ROMANIA DESCRIPTION of the ORAL HEALTH CARE in ROMANIA Corneliu AMARIEI, Cristina
Semester I Dental Anatomy (Basic Orofacial Anatomy)
") Dental Assisting Curriculum Example The dentalcare.com CE library offers over 150 courses that can be used in conjunction with your dental assisting curriculum. The guide below recommends courses to assign,
Dental Assisting Curriculum Example The dentalcare.com CE library offers over 150 courses that can be used in conjunction with your dental assisting curriculum. The guide below recommends courses to assign,
Index of clinical consequences of untreated dental caries (pufa) in primary dentition of children from north-east Poland
 in primary dentition of children from north-east Poland") Advances in Medical Sciences Vol. 58(2) 2013 pp 442-447 DOI: 10.2478/v10039-012-0075-x Medical University of Bialystok, Poland Index of clinical consequences of untreated dental caries (pufa) in primary
Advances in Medical Sciences Vol. 58(2) 2013 pp 442-447 DOI: 10.2478/v10039-012-0075-x Medical University of Bialystok, Poland Index of clinical consequences of untreated dental caries (pufa) in primary
NC History. Access Problems. The Partnership. Funding. Into the Mouths of Babes. Kelly Haupt, RDH, MHA Project Coordinator.
 Into the Mouths of Babes NC Oral Screening and Varnish Project Kelly Haupt, RDH, MHA Project Coordinator NC History 25% of ALL children entering kindergarten have visible, untreated decay 20% of indigent
Into the Mouths of Babes NC Oral Screening and Varnish Project Kelly Haupt, RDH, MHA Project Coordinator NC History 25% of ALL children entering kindergarten have visible, untreated decay 20% of indigent
CHILDREN S ORAL HEALTH RECENT RESEARCH & BEST PRACTICE RECOMMENDATIONS. brought to you by:
 CHILDREN S ORAL HEALTH RECENT RESEARCH & BEST PRACTICE RECOMMENDATIONS brought to you by: February 2015 ABOUT COHAT: This toolkit is brought to you by the Children s Oral Health Action Team (COHAT), created
CHILDREN S ORAL HEALTH RECENT RESEARCH & BEST PRACTICE RECOMMENDATIONS brought to you by: February 2015 ABOUT COHAT: This toolkit is brought to you by the Children s Oral Health Action Team (COHAT), created
4: Complexity and maintenance - a report from the Adult Dental Health Survey 2009
 4: Complexity and maintenance - a report from the Adult Dental Health Survey 2009 Copyright 2011, The Health and Social Care Information Centre. All Rights Reserved. 1 The NHS Information Centre is England
4: Complexity and maintenance - a report from the Adult Dental Health Survey 2009 Copyright 2011, The Health and Social Care Information Centre. All Rights Reserved. 1 The NHS Information Centre is England
A Message. Dear Colleague:
 A Message Dear Colleague: I am pleased to present the New York State Oral Health Plan. This plan addresses the burden of oral disease in New York State and was developed by the New York State Department
A Message Dear Colleague: I am pleased to present the New York State Oral Health Plan. This plan addresses the burden of oral disease in New York State and was developed by the New York State Department
Guidelines for Providing Dental Services in Skilled Nursing Facilities
 Guidelines for Providing Dental Services in Skilled Nursing Facilities March 2013 The following information was adapted from a publication of the Center for Oral Health 1. It was compiled to assist skilled
Guidelines for Providing Dental Services in Skilled Nursing Facilities March 2013 The following information was adapted from a publication of the Center for Oral Health 1. It was compiled to assist skilled
Dental Quality Metrics Workgroup. Recommendations for the Metrics and Scoring Committee December 2013
 Dental Quality Metrics Workgroup Recommendations for the Metrics and Scoring Committee Introduction In 2012, Oregon Senate Bill 1580, Section 21, established the nine-member Metrics and Scoring Committee,
Dental Quality Metrics Workgroup Recommendations for the Metrics and Scoring Committee Introduction In 2012, Oregon Senate Bill 1580, Section 21, established the nine-member Metrics and Scoring Committee,
Oral Health Care: Dental Insurance Program
 Oral Health Care: Dental Insurance Program Approved: November 2009 Oral Health Care includes diagnostic, preventive, and therapeutic services provided by general dental practitioners, dental specialists,
Oral Health Care: Dental Insurance Program Approved: November 2009 Oral Health Care includes diagnostic, preventive, and therapeutic services provided by general dental practitioners, dental specialists,
Promoting and Enhancing the Oral Health of the Public HHS ORAL HEALTH INITIATIVE 2010
 Promoting and Enhancing the Oral Health of the Public HHS ORAL HEALTH INITIATIVE 2010 Table of Contents ADMINISTRATION FOR CHILDREN AND FAMILIES... 4 Head Start Dental Home Initiative... 4 CENTERS FOR
Promoting and Enhancing the Oral Health of the Public HHS ORAL HEALTH INITIATIVE 2010 Table of Contents ADMINISTRATION FOR CHILDREN AND FAMILIES... 4 Head Start Dental Home Initiative... 4 CENTERS FOR
Fluoride and Dental Health in Europe
 Fluoride and Dental Health in Europe Dental Health in Europe - A Problem for Disadvataged Groups Report of an EU-funded Conference A conference of dental and public health experts drawn from every Member
Fluoride and Dental Health in Europe Dental Health in Europe - A Problem for Disadvataged Groups Report of an EU-funded Conference A conference of dental and public health experts drawn from every Member
STEP. Workplans: A Program Management Tool. René Lavinghouze MA Kathleen Heiden RDH, MSPH. Step 2: Describing the Program
 STEP C Workplans: A Program Management Tool René Lavinghouze MA Kathleen Heiden RDH, MSPH 2C_1 STEP C Workplans: A Program Management Tool Contents How to Use This Packet 4 Tip Sheets at a Glance 5 Case
STEP C Workplans: A Program Management Tool René Lavinghouze MA Kathleen Heiden RDH, MSPH 2C_1 STEP C Workplans: A Program Management Tool Contents How to Use This Packet 4 Tip Sheets at a Glance 5 Case
PROPOSED REGULATION OF THE BOARD OF DENTAL EXAMINERS OF NEVADA. LCB File No. R086-16
 PROPOSED REGULATION OF THE BOARD OF DENTAL EXAMINERS OF NEVADA LCB File No. R086-16 PROPOSED REGULATION CHANGES (NAC 631.033, NAC 631.175, and NAC 631.210) NAC 631.033 Use of laser radiation, administration
PROPOSED REGULATION OF THE BOARD OF DENTAL EXAMINERS OF NEVADA LCB File No. R086-16 PROPOSED REGULATION CHANGES (NAC 631.033, NAC 631.175, and NAC 631.210) NAC 631.033 Use of laser radiation, administration
Dental hygiene Undergraduate
 Dental hygiene Undergraduate The supportive and enthusiastic staff really help to make this challenging course rewarding and enjoyable. Stephanie DCP student The programme is well organised and delivered
Dental hygiene Undergraduate The supportive and enthusiastic staff really help to make this challenging course rewarding and enjoyable. Stephanie DCP student The programme is well organised and delivered
SENATE BILL 1419 AN ACT
 House Engrossed Senate Bill State of Arizona Senate Forty-ninth Legislature Second Regular Session SENATE BILL AN ACT AMENDING TITLE, CHAPTER, ARTICLE, ARIZONA REVISED STATUTES, BY ADDING SECTION -; AMENDING
House Engrossed Senate Bill State of Arizona Senate Forty-ninth Legislature Second Regular Session SENATE BILL AN ACT AMENDING TITLE, CHAPTER, ARTICLE, ARIZONA REVISED STATUTES, BY ADDING SECTION -; AMENDING
Importance of Access to and Utilization of Oral Health Care in Pennsylvania
 Importance of Access to and Utilization of Oral Health Care in Pennsylvania Ed Franchi Special Projects Coordinator Cheryl Bumgardner Clinical Coordinator Updated, March 2013 1 Contents Introduction 3
Importance of Access to and Utilization of Oral Health Care in Pennsylvania Ed Franchi Special Projects Coordinator Cheryl Bumgardner Clinical Coordinator Updated, March 2013 1 Contents Introduction 3
Budget Submission. January 2012. January 23, 2012 Authored by: Sara Harrup
 Budget Submission January 2012 January 23, 2012 Authored by: Sara Harrup BUDGET SUBMISSION January 2012 Introduction The Australian Dental Prosthetists Association Ltd (ADPA Ltd) is the peak professional
Budget Submission January 2012 January 23, 2012 Authored by: Sara Harrup BUDGET SUBMISSION January 2012 Introduction The Australian Dental Prosthetists Association Ltd (ADPA Ltd) is the peak professional
Department of Human Services Health Services Committee Senator Judy Lee, Chair August 18, 2015
 Department of Human Services Health Services Committee Senator Judy Lee, Chair August 18, 2015 Chairman Lee, members of the Health Services Committee, I am Maggie Anderson, Executive Director of the Department
Department of Human Services Health Services Committee Senator Judy Lee, Chair August 18, 2015 Chairman Lee, members of the Health Services Committee, I am Maggie Anderson, Executive Director of the Department
May 2013 Prepared by: Frances M. Kim, DDS, DrPH for Community Catalyst
 Economic Viability of Dental Therapists May 2013 Prepared by: Frances M. Kim, DDS, DrPH for Community Catalyst Economic Viability of Dental Therapists Prepared by: Frances M. Kim, DDS, DrPH for Community
Economic Viability of Dental Therapists May 2013 Prepared by: Frances M. Kim, DDS, DrPH for Community Catalyst Economic Viability of Dental Therapists Prepared by: Frances M. Kim, DDS, DrPH for Community
Dr. Cindi Sherwood, DDS, Independence House Committee on Health and Human Services (HB 2079)
") Dr. Cindi Sherwood, DDS, Independence House Committee on Health and Human Services (HB 2079) My name is Cindi Sherwood and I am speaking in opposition to House Bill 2079. My background is that I was trained
Dr. Cindi Sherwood, DDS, Independence House Committee on Health and Human Services (HB 2079) My name is Cindi Sherwood and I am speaking in opposition to House Bill 2079. My background is that I was trained
Bonitas Medical Scheme Dental Benefit Table
 Bonitas Medical Dental Benefit Table 2015 PRIMARY DENTAL BENEFIT TABLE 2015 BONSAVE DENTAL BENEFIT TABLE 2015 STANDARD DENTAL BENEFIT TABLE 2015 BONCOM DENTAL BENEFIT TABLE 2015 Dental benefits are paid
Bonitas Medical Dental Benefit Table 2015 PRIMARY DENTAL BENEFIT TABLE 2015 BONSAVE DENTAL BENEFIT TABLE 2015 STANDARD DENTAL BENEFIT TABLE 2015 BONCOM DENTAL BENEFIT TABLE 2015 Dental benefits are paid