Compensation Alignment: The Journey to One Dartmouth-Hitchcock. Clifford J. Belden, MD Chief Clinical Officer Dartmouth-Hitchcock
|
|
|
- Lynn McDonald
- 8 years ago
- Views:
Transcription

1 Compensation Alignment: The Journey to One Dartmouth-Hitchcock Clifford J. Belden, MD Chief Clinical Officer Dartmouth-Hitchcock

 40% of contracts with VBP components Don t do well")
2 1200 Physicians (50% AMC) 400 bed AMC + 5 group practices Group Practice AMC Group Practice Group Practice Group Practice Group Practice Multiple compensation models Risk-based 60% (ACO, self pay, employees) 40% of contracts with VBP components Don t do well at FFS
 40% of contracts with VBP components Don t do well")
3 Issues with Old Compensation Plan Providers dissatisfied Multiple plans across system (equity, fairness) Not understandable or transparent Not market competitive Didn t align with our strategic imperatives Disincentive to use Associate Providers Non-productivity measures not included

4 New Compensation Goals Alignment Integration Simplicity

5 Phase 1 Phase 2 Phase 3 Information gathering Goals and guiding principles Basic framework Details of plan 6 Workgroups Allocation Academics Communication Data and tool design Model Design Governance Launch Ongoing governance

6 D-H Guiding Principles Implemented across Dartmouth-Hitchcock (One-DH) Across the Community Group Practices and DH-Lebanon Supporting Service Integration Across D-H Recruiting and Retaining the best Allow us to pay for the type of work that is done Support our Research and Education missions Support important Administrative and Leadership roles Encompass both Physicians & Associate Providers Removing barriers to Team Based Care Appropriate Compensation and Bonus for team based quality success Facilitate our transition from Volume to Value Incorporate and expect achievement and exceeding national and organizational quality measures Transparent and understandable, aligned to strategic goals

7 Physician Compensation Total clinical compensation (100%) includes the following: Productivity Expectations (85%) Value Based Measures (15%)* Access (5%) Quality (5%) Patient Satisfaction (5%) Target Salary, not percent of a percentile Expectation of quality, access and patient satisfaction Not a quality bonus HCAHPS HAC CLABSI CAUTI VBP Readmissions and more

8 Clinical Compensation Models Quality, Access, and Patient Satisfaction (Expectation) 4 Tier Model Applies to physicians in sections measuring wrvus Tier Min Production %ile Max Production %ile Market %ile Pool Calculation 15% Value 85% RVU Physician Clinical Salary (tier) x Clinical FTE = Clinical Pool
 x Clinical FTE =")
9 Clinical Compensation Models Quality, Access, and Patient Satisfaction (Expectation) 15% Value 4 Tier Model Applies to physicians in sections measuring wrvus Tier Min Production %ile Max Production %ile Market %ile Salary Model Family Medicine, Geriatrics, Hospitalists, Pediatric Hospitalists, Internal Medicine, Pediatrics, Palliative Care, Pathology, Anesthesiology, and Emergency Medicine. Pool calculated at the 50 th percentile, regardless of production 85% RVU Pool Calculation Physician Clinical Salary (tier) x Clinical FTE = Clinical Pool
 x Clinical FTE =")
10 Compensation Model Determination Work is shift based? Able to directly control or influence work, productivity and volume? No Work requires in-house on-call presence and/or coverage of necessary services regardless of RVU opportunities? System measures outweigh RVU measures of productivity? Yes Tier Tier Based Model Min Prod %ile Max Prod %ile Market Percentile Salary Model (Market Median) th th th Pool calculated at the 50 th Market Percentile th
 1 0 40 30 th 2 41 60")
11 60% Fee for Service 40% Value Based Contracts How are we paid? Quality, Value and Utilization based Measures CAHPS*, CLABSI, CAUTI, SSI, C. Difficile, Pressure Ulcers, Pneumothorax, DVT/PE, Sepsis, Wound dehiscence, Readmissions, ER Utilization, BP,HA1c, HEDIS OPPE and Others Where do these Quality Performance (Payments and Penalties), show up? ACO Contracts Value Based Purchasing Hospital Readmission Reduction Hospital Acquired Conditions Outpatient Quality Reporting Physicians and Associate Providers are integral to successfully attaining these measures. We want to explicitly link Value, including Quality and Utilization Measures to compensation *Consumer Assessment of Healthcare Providers and Systems

12 Linking Quality and Value Measures to Compensation Quality Measures CAHPS*,CLABSI, CAUTI, SSI, C. Difficile, Pressure Ulcers, Pneumothorax, DVT/PE, Sepsis Wound dehiscence Readmissions ER Utilization, BP, HA1c, HEDIS and others Access Measures 3 rd Available appt % Booked Utilization of OSC and Block Time Local physician engagement in choosing measures is critical Value Domains Quality 5% Access 5% Benchmark Compensation (paid at 100%) 15% Value Patient Based Satisfaction Scores Patient Experience 5% 85% Productivity for Attribution to Compensation, these need to be Applicable, Measurable, Manageable and where appropriate, consistent with how we are Reimbursed *Consumer Assessment of Healthcare Providers and Systems

13 What are some of the reported measures we have 173 of them!

14 Determining the right Value and Quality Measures Local physician engagement in choosing measures is critical Ob-Gyn Radiology General Surgery GI Primary Care Anesth Cards Rheum Hosp Med Cardiac Surgery Access Quality Patient Experience Individual Sectional Regional System ACCESS % Booked 3 rd Available appointment New PCP appointment Reduced ED utilization QUALITY Provider Specific Outcomes Disease specific measures Reportable Metrics Improved Contracting Performance PATIENT EXPERIENCE Provider based experience Sectional satisfaction Service line measures CAHPS Scores *Consumer Assessment of Healthcare Providers and Systems

15 Constructing Value Measures for each area Ob-Gyn Radiology General Surgery GI Primar y Care Anesth Cards Rheum Hosp Med Cardiac Surgery Access Quality Patient Experience General Surgery Primary Care Cardiology Access % Booked Utilization of OR/OSC % Booked New PCP Weekend appts % Booked 3 rd Available External referrals Quality CAUTI, CLABSI, Postop wound dehiscence Handwashing 4W Screening Composite (Pioneer focus) [Ha1c, BP, Colo, BMI], HEDIS measures Mortality and readmission for AMI and HF, BB after MI Handwashing 4E, CVCC Patient Experience Communication with Doctors Satisfaction scores Patient Rating of Doctors Satisfaction Scores Shared Decision Making Communication with Doctors Satisfaction scores *Consumer Assessment of Healthcare Providers and Systems
![Handwashing 4W Screening Composite (Pioneer focus) [Ha1c, BP, Colo, BMI], HEDIS measures Mortality and readmission for AMI and HF, BB after MI Handwashing 4E, CVCC Patient Experience](/docs-images/41/7337378/images/page_15.jpg "Communication with Doctors Satisfaction scores Patient Rating of Doctors Satisfaction Scores Shared Decision Making Communication with Doctors Satisfaction scores *Consumer Assessment of")

16 Department Quality/Financial 16

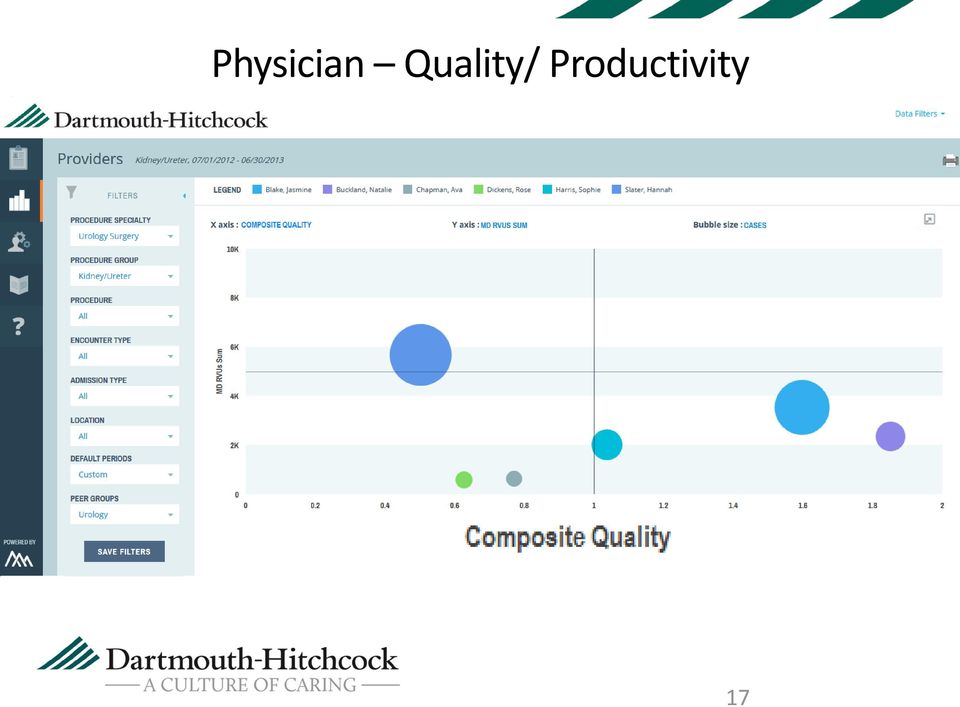
17 Physician Quality/ Productivity 17

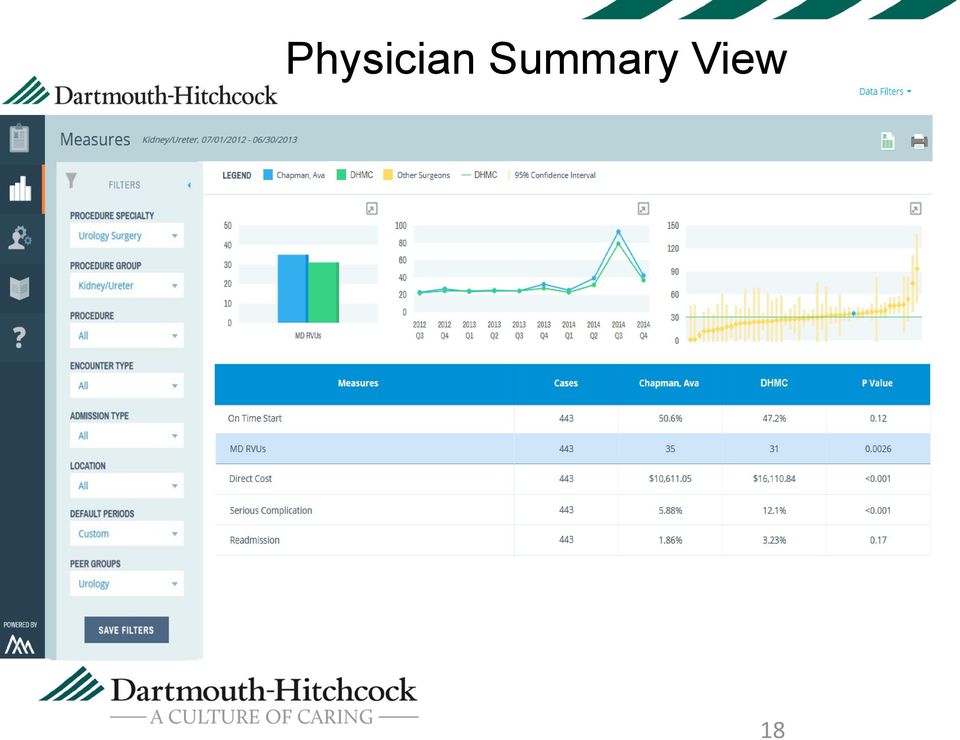
18 Physician Summary View 18
19

20 Transitioning Towards One D-H Individual Locations Academic Medical Center and CGP All Locations Combined Productivity tiers determined by each individual location and sometimes providers. Current Practice Productivity tiers determined by AMC and combined CGP locations Productivity tiers determined by all locations combined based on Service and Specialty (One D-H)

21 Clinical Compensation cfte x salary (based on system tier performance) Modified by patient sat, quality, access Clinical Compensation Pool Physician cfte Measure 1 (50%) Measure 2 (25%) Measure 3 (25%) Weighted Sum A (Manch) B (Manch) C (Leb) D (Leb) E (Leb) F (Keene) G (Keene) TOTAL

22 Sub-allocation of pools Each site receives pool based on relative performance of providers at the location Local input to distribute pool for site Move toward systemwide service lines
23 Tier Physician Clinical Compensation Models Expectations of Quality, Access, and Patient Experience Value Based Measures are 15% of total compensation, reviewed every 6 months Tier Based Model Min Prod %ile Max Prod %ile Market Percentile th th th th Salary Model Typically, Primary Care, Emergency and Hospital based specialties are compensated at a median salary and not a production based Calculated at the 50 th Market Percentile 15% Value 85% Productivity Clinical Compensation Pool Calculation = FTE x Market Rate Individual clinical Performance Determines Local Sub-allocation 0.9 Sub-pool Sub-pool Sub-pool Local Leader Input Keene Manchester Lebanon
24 Physician without an academic role, 100% clinical Clinical Comp Pool cfte x salary based on tier Pool developed across DH Modified by patient sat, quality, access Performance against clinical measures vs. group Individual Compensation What about academic physicians?
25 ? at what level Academic Productivity Academic physician career is different than non-academic Clinical Compensation cfte x salary (based on system tier performance) Modified by patient sat, quality, access Expectation of scholarly output and teaching A percentage of clinical dollars in each section/department in the AMC distributed based on academic performance Accountability framework for academic work at the individual, section and department level being developed Clinical Compensation Pool 10% Faculty 90% of salary distributed based on clinical performance 10% of median salary (using academic cftes) distributed based on academic measures (rank, productivity) Clinical Pool Non-Faculty 100% of salary distributed based on clinical performance
26 Physician with academic role, 100% clinical Clinical Comp Pool cfte x salary based on tier Pool developed across DH Modified by patient sat, quality, access Academic Component 10% x academic cfte x salary based on tier Performance against clinical measures vs. group Academic performance Individual Compensation
27 Physician with academic role, 50% clinical Clinical Comp Academic Component Section Chief, 20% NIH Research 30% cfte x salary based on tier Pool developed across DH Modified by patient sat, quality, access 10% x academic cfte x salary based on tier afte x salary based on tier (clinical role) or admin rate (admin role) Research grant/ contract dollars Performance against clinical measures vs. group Academic performance Modified by performance in role Direct dollars in grant + DH make whole Individual Compensation DH make-whole
28 Activity Reporting Tool A&S Contracts GME Grants Cost- Share Discretion Funds College Support MHMH Grants Dept. Ledger Alloc. Section Ledger Alloc. Authority: Chief Medical Officer Management: Activity Reporting / Provider Services ACTIVITY REPORTING TOOL Compliance Concerns Medicare Part A VA WRJ, VT. Clinical FTE Compensation Plans Per Diems Per Diems & Var. Contracts & Var Operations & Finance Research Management Corporate Accounting NIH Reporting Federal Grant Billing Data Warehouse Output Hires, Terms, & Leaves Transparent Non-Clinical Time Budget & Analyst

29 Name Hidden Name Hidden 29

30 Management Dashboard Monthly View (Red= FTE outside General Surgery. Blue=FTE within General Surgery) Name Hidden 30
31 Clinical Compensation Models Quality, Access, and Patient Satisfaction (Expectation) 15% Value 4 Tier Model Applies to physicians in sections measuring wrvus Tier Min Production %ile Max Production %ile Market %ile Salary Model Family Medicine, Geriatrics, Hospitalists, Pediatric Hospitalists, Internal Medicine, Pediatrics, Palliative Care, Pathology, Anesthesiology, and Emergency Medicine. Pool calculated at the 50 th percentile, regardless of production 85% RVU Pool Calculation Physician Clinical Salary (tier) x Clinical FTE = Clinical Pool
32 Linking Quality and Value Measures to Compensation Quality Measures CAHPS*,CLABSI, CAUTI, SSI, C. Difficile, Pressure Ulcers, Pneumothorax, DVT/PE, Sepsis Wound dehiscence Readmissions ER Utilization, BP, HA1c, HEDIS and others Access Measures 3 rd Available appt % Booked Utilization of OSC and Block Time Patient Based Satisfaction Scores Value Domains Quality 5% Access 5% Patient Experience 5% Benchmark Compensation (paid at 100%) 15% Value 85% Productivity for Attribution to Compensation, these need to be Applicable, Measurable, Manageable and where appropriate, consistent with how we are Reimbursed *Consumer Assessment of Healthcare Providers and Systems
33 Constructing Value Measures for Each Area Ob-Gyn Radiology General Surgery GI Primar y Care Anesth Cards Rheum Hosp Med Cardiac Surgery Access Quality Patient Experience General Surgery Primary Care Cardiology Access % Booked Utilization of OR/OSC % Booked New PCP Weekend appts % Booked 3 rd Available External referrals Quality CAUTI, CLABSI, Postop wound dehiscence Handwashing 4W Screening Composite (Pioneer focus) [Ha1c, BP, Colo, BMI], HEDIS measures Mortality and readmission for AMI and HF, BB after MI Handwashing 4E, CVCC Patient Experience Communication with Doctors Satisfaction scores Patient Rating of Doctors Satisfaction Scores Shared Decision Making Communication with Doctors Satisfaction scores *Consumer Assessment of Healthcare Providers and Systems

34 Physician Quality/ Productivity 34

35 Transitioning Towards One D-H Individual Locations Academic Medical Center and CGP All Locations Combined Productivity tiers determined by each individual location and sometimes providers. Current Practice Productivity tiers determined by AMC and combined CGP locations Productivity tiers determined by all locations combined based on Service and Specialty (One D-H)
36 Tier Physician Clinical Compensation Models Expectations of Quality, Access, and Patient Experience Value Based Measures are 15% of total compensation, reviewed every 6 months Tier Based Model Min Prod %ile Max Prod %ile Market Percentile th th th th Salary Model Typically, Primary Care, Emergency and Hospital based specialties are compensated at a median salary and not a production based Calculated at the 50 th Market Percentile 15% Value 85% Productivity Clinical Compensation Pool Calculation = FTE x Market Rate Individual clinical Performance Determines Local Sub-allocation 0.9 Sub-pool Sub-pool Sub-pool Local Leader Input Keene Manchester Lebanon
37 ? at what level Academic Productivity Academic physician career is different than non-academic Clinical Compensation cfte x salary (based on system tier performance) Modified by patient sat, quality, access Expectation of scholarly output and teaching A percentage of clinical dollars in each section/department in the AMC distributed based on academic performance Accountability framework for academic work at the individual, section and department level being developed Clinical Compensation Pool 10% Faculty 90% of salary distributed based on clinical performance 10% of median salary (using academic cftes) distributed based on academic measures (rank, productivity) Clinical Pool Non-Faculty 100% of salary distributed based on clinical performance
38 D-H Guiding Principles Implemented across Dartmouth-Hitchcock (One-DH) Across the Community Group Practices and DH-Lebanon Supporting Service Integration Across D-H Recruiting and Retaining the best Allow us to pay for the type of work that is done Support our Research and Education missions Support important Administrative and Leadership roles Encompass both Physicians & Associate Providers Removing barriers to Team Based Care Appropriate Compensation and Bonus for team based quality success Facilitate our transition from Volume to Value Incorporate and expect achievement and exceeding national and organizational quality measures Transparent and understandable, aligned to strategic goals
39 New Compensation Plan Alignment Integration Simplicity
VHA CENTRAL ATLANTIC COMPENSATION PLAN REDESIGN. Karin Chernoff Kaplan, AVA, Director, DGA Partners. January 5, 2012
 VHA CENTRAL ATLANTIC COMPENSATION PLAN REDESIGN Karin Chernoff Kaplan, AVA, Director, DGA Partners January 5, 2012 AGENDA > Introduction and Trends in Physician Compensation > Compensation Plan Design
VHA CENTRAL ATLANTIC COMPENSATION PLAN REDESIGN Karin Chernoff Kaplan, AVA, Director, DGA Partners January 5, 2012 AGENDA > Introduction and Trends in Physician Compensation > Compensation Plan Design
HCAHPS and Value-Based Purchasing Methods and Measurement. Deb Stargardt, Improvement Services Darrel Shanbour, Consulting Services
 HCAHPS and Value-Based Purchasing Methods and Measurement Deb Stargardt, Improvement Services Darrel Shanbour, Consulting Services Today s Learning Objectives Acquire new knowledge pertaining to: A. Hospital
HCAHPS and Value-Based Purchasing Methods and Measurement Deb Stargardt, Improvement Services Darrel Shanbour, Consulting Services Today s Learning Objectives Acquire new knowledge pertaining to: A. Hospital
Value Based Care and Healthcare Reform
 Value Based Care and Healthcare Reform Dimensions in Cardiac Care November, 2014 Jacqueline Matthews, RN, MS Senior Director, Quality Reporting & Reform Quality and Patient Safety Institute Cleveland Clinic
Value Based Care and Healthcare Reform Dimensions in Cardiac Care November, 2014 Jacqueline Matthews, RN, MS Senior Director, Quality Reporting & Reform Quality and Patient Safety Institute Cleveland Clinic
Value-Based Purchasing Program Overview. Maida Soghikian, MD Grand Rounds Scripps Green Hospital November 28, 2012
 Value-Based Purchasing Program Overview Maida Soghikian, MD Grand Rounds Scripps Green Hospital November 28, 2012 Presentation Overview Background and Introduction Inpatient Quality Reporting Program Value-Based
Value-Based Purchasing Program Overview Maida Soghikian, MD Grand Rounds Scripps Green Hospital November 28, 2012 Presentation Overview Background and Introduction Inpatient Quality Reporting Program Value-Based
Compensation 2013: Evolving Models, Emerging Approaches
 Compensation 2013: Evolving Models, Emerging Approaches Results from the AMGA 2013 Medical Group Compensation and Financial Survey By Bradley S.J. Vaudrey, M.B.A., CPA, and Sara Loos, CCP Findings from
Compensation 2013: Evolving Models, Emerging Approaches Results from the AMGA 2013 Medical Group Compensation and Financial Survey By Bradley S.J. Vaudrey, M.B.A., CPA, and Sara Loos, CCP Findings from
Ohio Hospital Association 2015 Annual Meeting. Physician Compensation: Navigating Change from Volume to Value in a Compliant Way
 Ohio Hospital Association 2015 Annual Meeting June 8, 2015 Physician Compensation: Navigating Change from Volume to Value in a Compliant Way Jason Tackett, Sullivan, Cotter and Associates, Inc., jasontackett@sullivancotter.com
Ohio Hospital Association 2015 Annual Meeting June 8, 2015 Physician Compensation: Navigating Change from Volume to Value in a Compliant Way Jason Tackett, Sullivan, Cotter and Associates, Inc., jasontackett@sullivancotter.com
Employed Physicians: Leadership Strategies for a Winning Organization
 Employed Physicians: Leadership Strategies for a Winning Organization Ray Chorey Southeastern Ohio Regional Medical Center President and CEO Thomas Ferkovic SS&G Healthcare Managing Director Practice Comparison
Employed Physicians: Leadership Strategies for a Winning Organization Ray Chorey Southeastern Ohio Regional Medical Center President and CEO Thomas Ferkovic SS&G Healthcare Managing Director Practice Comparison
Unifying Compensation:
 Unifying Compensation: The Lehigh Valley Physicians Group Experience American Medical Group Association Orlando, FL March 15, 2013 Edward Norris, M.D. Chair, Compensation Committee Michael A. Rossi, M.D.,
Unifying Compensation: The Lehigh Valley Physicians Group Experience American Medical Group Association Orlando, FL March 15, 2013 Edward Norris, M.D. Chair, Compensation Committee Michael A. Rossi, M.D.,
Adding Value to. Provider Compensation. June 13, 2016. Healthcare Strategy Group OHA Presentation 2016. Adding Value to. Physician Compensation
 Provider Compensation June 13, 2016 1 Who are We? About (HSG) Hospital-physician integration specialists since 1999 Strategic, best practice approach to employed physician networks and independent physician
Provider Compensation June 13, 2016 1 Who are We? About (HSG) Hospital-physician integration specialists since 1999 Strategic, best practice approach to employed physician networks and independent physician
National Provider Call: Hospital Value-Based Purchasing (VBP) Program
 Program") National Provider Call: Hospital Value-Based Purchasing (VBP) Program Fiscal Year 2016 Overview for Beneficiaries, Providers and Stakeholders Cindy Tourison, MSHI Lead, Hospital Inpatient Quality Reporting
National Provider Call: Hospital Value-Based Purchasing (VBP) Program Fiscal Year 2016 Overview for Beneficiaries, Providers and Stakeholders Cindy Tourison, MSHI Lead, Hospital Inpatient Quality Reporting
How To Pay For Health Care
 Uniting Physicians Through a Common Compensation Structure AMGA 2014 Annual Conference Mercy and Sullivan Cotter Fred Ford, Senior Vice President Ambulatory Care Mercy Fred McQueary, Senior Vice President
Uniting Physicians Through a Common Compensation Structure AMGA 2014 Annual Conference Mercy and Sullivan Cotter Fred Ford, Senior Vice President Ambulatory Care Mercy Fred McQueary, Senior Vice President
NALTO Benchmarking Initiative Fiscal Year 2008. Overview Report for Survey Participants
 NALTO Benchmarking Initiative Fiscal Year 2008 Overview Report for Survey Participants April, 2009 PROPRIETARY DATA, DO NOT DISTRIBUTE OUTSIDE YOUR ORGANIZATION. Your company s license to use this data
NALTO Benchmarking Initiative Fiscal Year 2008 Overview Report for Survey Participants April, 2009 PROPRIETARY DATA, DO NOT DISTRIBUTE OUTSIDE YOUR ORGANIZATION. Your company s license to use this data
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM: FINANCIAL REPORT AND SYSTEM DASHBOARDS May 29, 2013
 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM: FINANCIAL REPORT AND SYSTEM DASHBOARDS May 29, 2013 Office of the Vice President for Health Affairs Board of Trustees Spring Chicago Meeting UI
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM: FINANCIAL REPORT AND SYSTEM DASHBOARDS May 29, 2013 Office of the Vice President for Health Affairs Board of Trustees Spring Chicago Meeting UI
David F. Torchiana, MD Chairman & CEO October 13, 2011
 Overview of the MGPO David F. Torchiana, MD Chairman & CEO October 13, 2011 MGPO Organization and History MGPO: Massachusetts General Physicians Organization MGH 1811 Corporation MGH MGPO Formed in 1994
Overview of the MGPO David F. Torchiana, MD Chairman & CEO October 13, 2011 MGPO Organization and History MGPO: Massachusetts General Physicians Organization MGH 1811 Corporation MGH MGPO Formed in 1994
For trauma, there are some additional attributes that are unique and complex:
 Saving Lives, Reducing Costs of Trauma Care Trauma Center Association of America Model of Value Based Trauma Care to Evaluate, Test and Pilot July 25, 2013 Unique Nature of Trauma Injury and Treatment:
Saving Lives, Reducing Costs of Trauma Care Trauma Center Association of America Model of Value Based Trauma Care to Evaluate, Test and Pilot July 25, 2013 Unique Nature of Trauma Injury and Treatment:
Advance Practice Provider (APP) Compensation Models: Promoting Team Based Care. Wayne M. Hartley, Vice President AMGA Consulting Services
 Compensation Models: Promoting Team Based Care. Wayne M. Hartley, Vice President AMGA Consulting Services") Advance Practice Provider (APP) Compensation Models: Promoting Team Based Care Wayne M. Hartley, Vice President AMGA Consulting Services 1 Presentation Overview AMGA Survey Overview and Demographics APP
Advance Practice Provider (APP) Compensation Models: Promoting Team Based Care Wayne M. Hartley, Vice President AMGA Consulting Services 1 Presentation Overview AMGA Survey Overview and Demographics APP
ADGAP Collective Action Project
 ADGAP Collective Action Project The RVU Model in Academic Geriatric Programs: Benefits, Risks, and Brainstorming the Way Forward Neil M. Resnick, MD Nichole Radulovich, CRA ADGAP/Hartford Leadership Retreat
ADGAP Collective Action Project The RVU Model in Academic Geriatric Programs: Benefits, Risks, and Brainstorming the Way Forward Neil M. Resnick, MD Nichole Radulovich, CRA ADGAP/Hartford Leadership Retreat
Physician Compensation: Where the Market is Going
 Physician Compensation: Where the Market is Going HR Council March 13, 2013 Presented to: 2013 Sullivan, Cotter and Associates, Inc. The material may not be reproduced or copied without written consent
Physician Compensation: Where the Market is Going HR Council March 13, 2013 Presented to: 2013 Sullivan, Cotter and Associates, Inc. The material may not be reproduced or copied without written consent
2009 Nursing Strategic Plan. Atrium Medical Center
 2009 Nursing Strategic Plan Atrium Medical Center Mission Nurses at Atrium Medical Center are empowered to serve our patients by providing personalized, compassionate care with integrity and respect because
2009 Nursing Strategic Plan Atrium Medical Center Mission Nurses at Atrium Medical Center are empowered to serve our patients by providing personalized, compassionate care with integrity and respect because
Physician Compensation Planning: Beyond the Basics. Copyright 2014. Medical Group Management Association (MGMA ). All rights reserved.
. All rights reserved.") Physician Compensation Planning: Beyond the Basics Agenda Introductions/Learning Objectives Compensation Plan Development Process Compensation Planning Step 1: Start Up Step 2: Compensation Plan Options
Physician Compensation Planning: Beyond the Basics Agenda Introductions/Learning Objectives Compensation Plan Development Process Compensation Planning Step 1: Start Up Step 2: Compensation Plan Options
Physician Compensation: Where the Market is Going
 Physician Compensation: Where the Market is Going CFO Council March 13, 2013 Presented to: 2013 Sullivan, Cotter and Associates, Inc. The material may not be reproduced or copied without written consent
Physician Compensation: Where the Market is Going CFO Council March 13, 2013 Presented to: 2013 Sullivan, Cotter and Associates, Inc. The material may not be reproduced or copied without written consent
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT. Norris Vivatrat, MD Associate Medical Director Monarch HealthCare
 PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT
 PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
PIONEER ACO A REVIEW OF THE GRAND EXPERIMENT Norris Vivatrat, MD Associate Medical Director Monarch HealthCare 2 Agenda Pioneer ACO basics, performance and challenges Monarch HealthCare Post-acute network
Sharp HealthCare ACO. Pioneer Introduction to the FSSB November 8, 2012
 Sharp HealthCare ACO Pioneer Introduction to the FSSB November 8, 2012 Sharp HealthCare Not-for-profit serving 3.1 million residents of San Diego County Grew from one hospital in 1955 to an integrated
Sharp HealthCare ACO Pioneer Introduction to the FSSB November 8, 2012 Sharp HealthCare Not-for-profit serving 3.1 million residents of San Diego County Grew from one hospital in 1955 to an integrated
Call-A-Nurse Location
 Call-A-Nurse A 24-hour medical call center, specializing in registered nurse telephone triage, answering service, physician and service referral, and class registration. Call-A-Nurse Location Call-A-Nurse
Call-A-Nurse A 24-hour medical call center, specializing in registered nurse telephone triage, answering service, physician and service referral, and class registration. Call-A-Nurse Location Call-A-Nurse
Value Based Purchasing (VBP) Awareness Brief. FY 2018 Value Based Purchasing Program Domain Weighting
 Awareness Brief. FY 2018 Value Based Purchasing Program Domain Weighting") Value Based Purchasing (VBP) Awareness Brief This Awareness Brief provides a high level summary understanding of value based purchasing. The Hospital Value Based Purchasing (VBP) Program adjusts hospitals
Value Based Purchasing (VBP) Awareness Brief This Awareness Brief provides a high level summary understanding of value based purchasing. The Hospital Value Based Purchasing (VBP) Program adjusts hospitals
Medicare Shared Savings Program
 Medicare Shared Savings Program Eastern Michigan Chapter of HFMA Insurance and Reimbursement Committee April 30, 2015 Presenter: Kenneth B. Lipan, FHFMA Director of Finance: Clinical Integration, Unified
Medicare Shared Savings Program Eastern Michigan Chapter of HFMA Insurance and Reimbursement Committee April 30, 2015 Presenter: Kenneth B. Lipan, FHFMA Director of Finance: Clinical Integration, Unified
Healthcare Reform & Value Based Purchasing: Are You Ready?
 Healthcare Reform & Value Based Purchasing: Are You Ready? Premier, Inc Jan Englert, Director-QUEST Poudre Valley Health System Sonja Wulff, VP Center for Performance Excellence Federal Register Statement:
Healthcare Reform & Value Based Purchasing: Are You Ready? Premier, Inc Jan Englert, Director-QUEST Poudre Valley Health System Sonja Wulff, VP Center for Performance Excellence Federal Register Statement:
INTRODUCTION MEDICAL SCHOOL LANDSCAPE 5/13/2016. Introductions
 Association of Chiefs and Leaders of General Internal Medicine 2016 Leon Hess Management Training and Leadership Institute Medical School Revenues and Budgeting Principles A discussion outlining the revenue
Association of Chiefs and Leaders of General Internal Medicine 2016 Leon Hess Management Training and Leadership Institute Medical School Revenues and Budgeting Principles A discussion outlining the revenue
University of Colorado Health Performance Incentive Compensation Plan Plan Summary Fiscal Year 2014 Staff/Managers/Directors
 University of Colorado Health Performance Incentive Compensation Plan Plan Summary Fiscal Year 2014 Staff/Managers/Directors Plan Purpose The University of Colorado Health provides outstanding patient
University of Colorado Health Performance Incentive Compensation Plan Plan Summary Fiscal Year 2014 Staff/Managers/Directors Plan Purpose The University of Colorado Health provides outstanding patient
Overview of the Hospital Value-Based Purchasing (VBP) Fiscal Year (FY) 2017
 Fiscal Year (FY) 2017") Overview of the Hospital Value-Based Purchasing (VBP) Fiscal Year (FY) 2017 Bethany Wheeler Hospital VBP Program Support Contract Lead HSAG February 17, 2015 2 p.m. ET Purpose This event will provide an
Overview of the Hospital Value-Based Purchasing (VBP) Fiscal Year (FY) 2017 Bethany Wheeler Hospital VBP Program Support Contract Lead HSAG February 17, 2015 2 p.m. ET Purpose This event will provide an
MGMA 2016 Compensation and Production Survey (*Asterisks denote required questions)
") MGMA 2016 Compensation and Production Survey (*Asterisks denote required questions) Time is a valuable thing! We ve created a tiered participation benefit structure to ensure we reward you for the time
MGMA 2016 Compensation and Production Survey (*Asterisks denote required questions) Time is a valuable thing! We ve created a tiered participation benefit structure to ensure we reward you for the time
Benefit Design and ACOs: How Will Private Employers and Health Plans Proceed?
 Benefit Design and ACOs: How Will Private Employers and Health Plans Proceed? Accountable Care Organizations: Implications for Consumers October 14, 2010 Washington, DC Sam Nussbaum, M.D. Executive Vice
Benefit Design and ACOs: How Will Private Employers and Health Plans Proceed? Accountable Care Organizations: Implications for Consumers October 14, 2010 Washington, DC Sam Nussbaum, M.D. Executive Vice
David Ramos, MD, MPH, FACC Managing Physician ColumbiaDoctors of the Hudson Valley
 David Ramos, MD, MPH, FACC Managing Physician ColumbiaDoctors of the Hudson Valley The Changing Landscape of Medicine Changing Culture Demographics Income Terms and definitions RVUs, Restricted Covenants,
David Ramos, MD, MPH, FACC Managing Physician ColumbiaDoctors of the Hudson Valley The Changing Landscape of Medicine Changing Culture Demographics Income Terms and definitions RVUs, Restricted Covenants,
Nurse Credentialing: How to Impact Patient Outcomes in the Marketplace
 Nurse Credentialing: How to Impact Patient Outcomes in the Marketplace Donna King, BSN, MBA, RN, NE-BC, FACHE Vice President, Clinical Operations/Chief Nurse Executive Overview... About Advocate Health
Nurse Credentialing: How to Impact Patient Outcomes in the Marketplace Donna King, BSN, MBA, RN, NE-BC, FACHE Vice President, Clinical Operations/Chief Nurse Executive Overview... About Advocate Health
Patient Experience. The Cleveland Clinic Journey. American Medical Group Association Orlando, Florida March 14, 2013
 Patient Experience The Cleveland Clinic Journey American Medical Group Association Orlando, Florida March 14, 2013 James Merlino, MD Chief Experience Officer Overview How did Cleveland Clinic change their
Patient Experience The Cleveland Clinic Journey American Medical Group Association Orlando, Florida March 14, 2013 James Merlino, MD Chief Experience Officer Overview How did Cleveland Clinic change their
Cornerstone Health Care s ACO Playbook. Grace E. Terrell, MD January 17, 2012
 Cornerstone Health Care s ACO Playbook Grace E. Terrell, MD January 17, 2012 Mission: To be your medical home Vision: To be the model for physician-led health care in America Values: As a physician owned
Cornerstone Health Care s ACO Playbook Grace E. Terrell, MD January 17, 2012 Mission: To be your medical home Vision: To be the model for physician-led health care in America Values: As a physician owned
How Many People Want to Become a Physician Assistant?
 Table of Contents Introduction Purpose... 1 Methods... 1 Demographics Gender Distribution... 2 Age Distribution of Respondents... 2 Number of Years in Practice as a PA... 2 Respondent s Specialties...
Table of Contents Introduction Purpose... 1 Methods... 1 Demographics Gender Distribution... 2 Age Distribution of Respondents... 2 Number of Years in Practice as a PA... 2 Respondent s Specialties...
Contra Cost Health Plan Quality Program Summary November, 2013
 Contra Cost Health Plan Quality Program Summary November, 2013 Mission Statement: Contra Costa Health Plan, along with our community and county health care providers, is committed to ensure our diverse
Contra Cost Health Plan Quality Program Summary November, 2013 Mission Statement: Contra Costa Health Plan, along with our community and county health care providers, is committed to ensure our diverse
Data Infrastructure and Successful Quality Metric Collection: The Last Step in Medicare Shared Savings
 Data Infrastructure and Successful Quality Metric Collection: The Last Step in Medicare Shared Savings Shawn Griffin, MD, Quality Reporting Director Memorial Hermann ACO, and Chief Quality and Informatics
Data Infrastructure and Successful Quality Metric Collection: The Last Step in Medicare Shared Savings Shawn Griffin, MD, Quality Reporting Director Memorial Hermann ACO, and Chief Quality and Informatics
PATIENT EXPERIENCE GRANT PROGRAM SERIES RESEARCH REPORT
 PATIENT EXPERIENCE GRANT PROGRAM SERIES RESEARCH REPORT Impact of a Collaborative Re-structuring of New Hire Hospital Orientation on Employee Engagement Tanya Lott, MSN, RN-BC Winnie Hennessy, PhD, RN,
PATIENT EXPERIENCE GRANT PROGRAM SERIES RESEARCH REPORT Impact of a Collaborative Re-structuring of New Hire Hospital Orientation on Employee Engagement Tanya Lott, MSN, RN-BC Winnie Hennessy, PhD, RN,
Population Health Solutions for Employers MEDIA RESOURCES
 Population Health Solutions for Employers MEDIA RESOURCES ABOUT MISSIONPOINT MissionPoint s mission is to make healthcare more affordable, accessible and improve the quality of care for our members. MissionPoint
Population Health Solutions for Employers MEDIA RESOURCES ABOUT MISSIONPOINT MissionPoint s mission is to make healthcare more affordable, accessible and improve the quality of care for our members. MissionPoint
The Univ ersity o f Texas System Nine Universities. Six Health Institutions. Unlimited Possibilities.
 The Univ ersity o f Texas System Nine Universities. Six Health Institutions. Unlimited Possibilities. System Audit Office 702 Colorado Street, Austin, TX 78701 Phone: 512-499-4390 Fax: 512-499-4426 September
The Univ ersity o f Texas System Nine Universities. Six Health Institutions. Unlimited Possibilities. System Audit Office 702 Colorado Street, Austin, TX 78701 Phone: 512-499-4390 Fax: 512-499-4426 September
Accountable Care Organizations: What Are They and Why Should I Care?
 Accountable Care Organizations: What Are They and Why Should I Care? Adrienne Green, MD Associate Chief Medical Officer, UCSF Medical Center Ami Parekh, MD, JD Med. Director, Health System Innovation,
Accountable Care Organizations: What Are They and Why Should I Care? Adrienne Green, MD Associate Chief Medical Officer, UCSF Medical Center Ami Parekh, MD, JD Med. Director, Health System Innovation,
Value Based Payment Models: What are they and strategies for success
 Value Based Payment Models: What are they and strategies for success Melinda Hancock National Chair Elect Region IV March 2015 Shaping the Curve 2 The Continuum of Risk Source: Hancock, M., Hannah, B.
Value Based Payment Models: What are they and strategies for success Melinda Hancock National Chair Elect Region IV March 2015 Shaping the Curve 2 The Continuum of Risk Source: Hancock, M., Hannah, B.
Utilizing Physician Extenders to Achieve Group Practice Initiatives
 Utilizing Physician Extenders to Achieve Group Practice Initiatives Your presenters Debra Johansen, MBA, CMPE Chief Operating Administrator, HealthFirst Medical Group, Melbourne FL Richard Baney, Jr, MD,
Utilizing Physician Extenders to Achieve Group Practice Initiatives Your presenters Debra Johansen, MBA, CMPE Chief Operating Administrator, HealthFirst Medical Group, Melbourne FL Richard Baney, Jr, MD,
Accountable Care Organizations. Rick Shinto, MD Aveta Health Inc. July 20, 2010
 Accountable Care Organizations Rick Shinto, MD Aveta Health Inc. July 20, 2010 1 Health Care Reform- New Models of Care Patient Protection and Affordable care Act (PPACA 2010) controlling costs and improving
Accountable Care Organizations Rick Shinto, MD Aveta Health Inc. July 20, 2010 1 Health Care Reform- New Models of Care Patient Protection and Affordable care Act (PPACA 2010) controlling costs and improving
Johns Hopkins University Bloomberg School of Public Health
 Johns Hopkins University Bloomberg School of Public Health Report on Johns Hopkins University School of Medicine Faculty Salary Analysis, 2003-2004 With Additional Comments November 29, 2005 Objectives:
Johns Hopkins University Bloomberg School of Public Health Report on Johns Hopkins University School of Medicine Faculty Salary Analysis, 2003-2004 With Additional Comments November 29, 2005 Objectives:
INDUSTRY PERSPECTIVES
 INDUSTRY PERSPECTIVES Behavioral Health: Staying ahead of the shortage As the demand for behavioral health professionals increases, facilities should consider what implications this may have on facility
INDUSTRY PERSPECTIVES Behavioral Health: Staying ahead of the shortage As the demand for behavioral health professionals increases, facilities should consider what implications this may have on facility
Premium Pay Are you paying too much for your labor? Sandy Yanko HCA Far West Division Vice President Operations
 Premium Pay Are you paying too much for your labor? Sandy Yanko HCA Far West Division Vice President Operations SHS Conference Chicago, IL April 2009 0 Agenda Background Understanding premium pay Analyzing
Premium Pay Are you paying too much for your labor? Sandy Yanko HCA Far West Division Vice President Operations SHS Conference Chicago, IL April 2009 0 Agenda Background Understanding premium pay Analyzing
FY 2016 Inpatient PPS Proposed Rule Quality Issues May 21, 2015
 FY 2016 Inpatient PPS Proposed Rule Quality Issues May 21, 2015 AAMC Staff: Scott Wetzel, swetzel@aamc.org Mary Wheatley, mwheatley@aamc.org Agenda Summary of key quality and payment IPPS provisions Cross-cutting
FY 2016 Inpatient PPS Proposed Rule Quality Issues May 21, 2015 AAMC Staff: Scott Wetzel, swetzel@aamc.org Mary Wheatley, mwheatley@aamc.org Agenda Summary of key quality and payment IPPS provisions Cross-cutting
Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015
 Leveraging the Continuum to Avoid Unnecessary Utilization While Improving Quality Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015 Karim A. Habibi, FHFMA, MPH, MS Senior
Leveraging the Continuum to Avoid Unnecessary Utilization While Improving Quality Leadership Summit for Hospital and Post-Acute Long Term Care Providers May 12, 2015 Karim A. Habibi, FHFMA, MPH, MS Senior
Practice Evaluation Workbook
 Practice name Address: Phone: Email: Web site: Main contact: Fax: Affiliations: Hospital(s): Universitiy: Practice Group (if applicable): Address: Phone: Email: This workbook is intended for the personal
Practice name Address: Phone: Email: Web site: Main contact: Fax: Affiliations: Hospital(s): Universitiy: Practice Group (if applicable): Address: Phone: Email: This workbook is intended for the personal
Title goes here. Performance Management in the Rural Health Clinic. Idaho Bureau of Rural Health & Primary Care November 5, 2014 12:45 p.m. 1:45 p.m.
 Performance Management in the Rural Health Clinic Idaho Bureau of Rural Health & Primary Care November 5, 2014 12:45 p.m. 1:45 p.m. Title goes here Jeff Johnson - CPA, Date Partner or subtitle Wipfli Health
Performance Management in the Rural Health Clinic Idaho Bureau of Rural Health & Primary Care November 5, 2014 12:45 p.m. 1:45 p.m. Title goes here Jeff Johnson - CPA, Date Partner or subtitle Wipfli Health
How To Understand An Accountable Care Organization
 Accountable Care Organizations and Wound Centers No Disclosures Peter F. Lawrence, MD Professor and Chief Division of Vascular Surgery University of California Los Angeles Accountable Care Organization
Accountable Care Organizations and Wound Centers No Disclosures Peter F. Lawrence, MD Professor and Chief Division of Vascular Surgery University of California Los Angeles Accountable Care Organization
Co-management (Service Line Agreement 2007)
") Co-management (Service Line Agreement 2007) Orthopedics Neuroscience Cardiology Cardiovascular Surgery Collaboration on a different level Tactical method of increasing alignment and collaboration Agreement
Co-management (Service Line Agreement 2007) Orthopedics Neuroscience Cardiology Cardiovascular Surgery Collaboration on a different level Tactical method of increasing alignment and collaboration Agreement
Regional Radiology in a Rural State: Implementation and Growth
 Regional Radiology in a Rural State: Implementation and Growth Jocelyn D. Chertoff, MD, MS, MHCDS Chair, Department of Diagnostic Radiology Vice President, Regional Radiology Service Line Dartmouth-Hitchcock
Regional Radiology in a Rural State: Implementation and Growth Jocelyn D. Chertoff, MD, MS, MHCDS Chair, Department of Diagnostic Radiology Vice President, Regional Radiology Service Line Dartmouth-Hitchcock
UNC-Chapel Hill School of Medicine CLINICAL FACULTY COMPENSATION PLAN January 1996
 UNC-Chapel Hill School of Medicine CLINICAL FACULTY COMPENSATION PLAN January 1996 Revised - January 2001, June 2006, July 2008, April, 2009, June 2012, June 2013, June 2014, June 2015 I. Introduction
UNC-Chapel Hill School of Medicine CLINICAL FACULTY COMPENSATION PLAN January 1996 Revised - January 2001, June 2006, July 2008, April, 2009, June 2012, June 2013, June 2014, June 2015 I. Introduction
New York Presbyterian Innovations in Health Care Reform at Academic Medical Centers
 New York Presbyterian Innovations in Health Care Reform at Academic Medical Centers October 28, 2011 Timothy G Ferris, MD, MPH Mass General Physicians Organization, Medical Director Associate Professor,
New York Presbyterian Innovations in Health Care Reform at Academic Medical Centers October 28, 2011 Timothy G Ferris, MD, MPH Mass General Physicians Organization, Medical Director Associate Professor,
Successful Medical Practice Management: Beyond the Beans
 Successful Medical Practice Management: Beyond the Beans Susan Turney, MD, MS, FACMPE, FACP President and CEO MGMA-ACMPE About MGMA-ACMPE The largest, oldest and most respected professional association
Successful Medical Practice Management: Beyond the Beans Susan Turney, MD, MS, FACMPE, FACP President and CEO MGMA-ACMPE About MGMA-ACMPE The largest, oldest and most respected professional association
Medicare Accountable Care Organizations: What it s about
 Medicare Accountable Care Organizations: What it s about Gail Albertson, MD Associate Professor of Medicine Chief Operating Officer, UPI Medicare Accountable Care Under the Medicare Shared Savings Program
Medicare Accountable Care Organizations: What it s about Gail Albertson, MD Associate Professor of Medicine Chief Operating Officer, UPI Medicare Accountable Care Under the Medicare Shared Savings Program
Physician Compensation and
 SHM Roundtable Physician Compensation and Incentive Plans December 9 th, 2010 Dan F ller President & Co Fo nder Dan Fuller President & Co-Founder IN Compass Health Discussion How important is compensation?
SHM Roundtable Physician Compensation and Incentive Plans December 9 th, 2010 Dan F ller President & Co Fo nder Dan Fuller President & Co-Founder IN Compass Health Discussion How important is compensation?
Massachusetts Medical Society
 Massachusetts Medical Society Physician Employment Options Webinar October 10, 2013 Key Questions for Session 1. What market factors are causing an increase in physician employment? Is it all economics?
Massachusetts Medical Society Physician Employment Options Webinar October 10, 2013 Key Questions for Session 1. What market factors are causing an increase in physician employment? Is it all economics?
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION
 Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
Presented by Kathleen S. Wyka, AAS, CRT, THE AFFORDABLE CA ACT AND ITS IMPACT ON THE RESPIRATORY C PROFESSION At the end of this session, you will be able to: Identify ways RT skills can be utilized for
RVU BASED PHYSICIAN COMPENSATION AND PRODUCTIVITY
 RVU BASED PHYSICIAN COMPENSATION AND PRODUCTIVITY Ten Recommendations for Determining Physician Compensation/Productivity Through Relative Value Units 2011 Merritt Hawkins 5001 Statesman Drive Irving,
RVU BASED PHYSICIAN COMPENSATION AND PRODUCTIVITY Ten Recommendations for Determining Physician Compensation/Productivity Through Relative Value Units 2011 Merritt Hawkins 5001 Statesman Drive Irving,
Value Based Purchasing and You
 Value Based Purchasing and You David Gourley, RRT, MHA, FAARC Director of Clinical Services and Risk Management Millennium Respiratory Services Whippany, New Jersey Value Based Purchasing and You Overview
Value Based Purchasing and You David Gourley, RRT, MHA, FAARC Director of Clinical Services and Risk Management Millennium Respiratory Services Whippany, New Jersey Value Based Purchasing and You Overview
Incentive Compensation Systems In Community Health Centers. Curt Degenfelder Managing Director curtis.degenfelder@rsmi.com
 Incentive Compensation Systems In Community Health Centers Curt Degenfelder Managing Director curtis.degenfelder@rsmi.com 1 What are the components of successful health centers culture that support an
Incentive Compensation Systems In Community Health Centers Curt Degenfelder Managing Director curtis.degenfelder@rsmi.com 1 What are the components of successful health centers culture that support an
Developing a Sustainable Physician Strategy
 Developing a Sustainable Physician Strategy Chicago, Illinois / April 13, 2010 1 Agenda Introduction Select Industry Trends and Healthcare Reform National Trends Impacting Hospital/ Physician Relationships
Developing a Sustainable Physician Strategy Chicago, Illinois / April 13, 2010 1 Agenda Introduction Select Industry Trends and Healthcare Reform National Trends Impacting Hospital/ Physician Relationships
Value-Based Purchasing An Opportunity for Clinical Nurse Leaders
 Value-Based Purchasing An Opportunity for Clinical Nurse Leaders Marjorie S. Wiggins, DNP, MBA, RN, FAAN, NEA-BC Senior Vice President, Patient Care Services/Chief Nursing Officer AACN-CNL Summit, Long
Value-Based Purchasing An Opportunity for Clinical Nurse Leaders Marjorie S. Wiggins, DNP, MBA, RN, FAAN, NEA-BC Senior Vice President, Patient Care Services/Chief Nursing Officer AACN-CNL Summit, Long
Future of Health Care: How Do You Fit In? Physician Leadership Institute February 28, 2015 Brian M. McCook, CPA
 Future of Health Care: How Do You Fit In? Physician Leadership Institute February 28, 2015 Brian M. McCook, CPA Learning Objectives Industry Transitions Challenges and Changes ACO s Look at the Future
Future of Health Care: How Do You Fit In? Physician Leadership Institute February 28, 2015 Brian M. McCook, CPA Learning Objectives Industry Transitions Challenges and Changes ACO s Look at the Future
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS. Karen Unholz, RN, BSN
 INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
Purchasers Efforts to Promote Better Information Technology
 Purchasers Efforts to Promote Better Information Technology Peter V. Lee Pacific Business Group on Health The Health Information Technology Summit West March 7, 2005 Measuring Provider Quality and Cost-Efficiency
Purchasers Efforts to Promote Better Information Technology Peter V. Lee Pacific Business Group on Health The Health Information Technology Summit West March 7, 2005 Measuring Provider Quality and Cost-Efficiency
Care Coordination. The Embedded Care Manager. Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed
 Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
Care Coordination The Embedded Care Manager Presented by Thomas Decker, MD Mary Finnegan, BSN, M.Ed Goals of Care Management The goals of care Management are consistent with the Triple Aim: Improve population
National Provider Trends & Strategic Considerations Around Value Based Purchasing
 National Provider Trends & Strategic Considerations Around Value Based Purchasing Melinda S. Hancock, FHFMA,CPA Partner, DHG Healthcare 2015-16 Chair, HFMA Southern California HFMA August 2015 Objectives
National Provider Trends & Strategic Considerations Around Value Based Purchasing Melinda S. Hancock, FHFMA,CPA Partner, DHG Healthcare 2015-16 Chair, HFMA Southern California HFMA August 2015 Objectives
Aria Health 111 Years of Caring
 Aria Health 111 Years of Caring Strategic t Plan to Survive the Accountable Care Act (ACA) Andrew DeVoe Chief Financial Officer (CFO) & Treasurer Aria Health Philadelphia, PA Financial Disclaimer Certain
Aria Health 111 Years of Caring Strategic t Plan to Survive the Accountable Care Act (ACA) Andrew DeVoe Chief Financial Officer (CFO) & Treasurer Aria Health Philadelphia, PA Financial Disclaimer Certain
MACRA & APMs: More than Acronyms June 2, 2016
 MACRA & APMs: More than Acronyms June 2, 2016 Agenda 1. Framework 2. CMS Quality Initiatives 3. MACRA - MIPS or APM? 4. Alternative Payment Models 5. Case Study 2 Alternative Payment Models Transitioning
MACRA & APMs: More than Acronyms June 2, 2016 Agenda 1. Framework 2. CMS Quality Initiatives 3. MACRA - MIPS or APM? 4. Alternative Payment Models 5. Case Study 2 Alternative Payment Models Transitioning
Resident Job Search Guide Resources for a Successful Position Search and Interview
 Resident Job Search Guide Resources for a Successful Position Search and Interview Acknowledgements: thank you to Joseph Vitale, M.Ed., Ed.S., J.D., Director of the Cleveland Clinic Office of Physician
Resident Job Search Guide Resources for a Successful Position Search and Interview Acknowledgements: thank you to Joseph Vitale, M.Ed., Ed.S., J.D., Director of the Cleveland Clinic Office of Physician
2009 Emergency Physician Salary & Benefit Survey THIS REPORT: U.S. NATIONAL RESULTS
 2009 Emergency Physician Salary & Benefit Survey THIS REPORT: U.S. TIOL RESULTS 2009 Emergency Physician Salary & Benefit Survey THIS REPORT: U.S. TIOL RESULTS About the Survey Daniel Stern and Associates
2009 Emergency Physician Salary & Benefit Survey THIS REPORT: U.S. TIOL RESULTS 2009 Emergency Physician Salary & Benefit Survey THIS REPORT: U.S. TIOL RESULTS About the Survey Daniel Stern and Associates
INDUSTRY PERSPECTIVES. Chris McDonald, Regional Vice President, Delta Locum Tenens. As many talented physicians adopt locum
 INDUSTRY PERSPECTIVES Locum Tenens Industry Growing; Where do You Stand on the Spectrum? Chris McDonald, Regional Vice President, Delta Locum Tenens the 2nd Quarter 2015 July 14 - June 15 According to
INDUSTRY PERSPECTIVES Locum Tenens Industry Growing; Where do You Stand on the Spectrum? Chris McDonald, Regional Vice President, Delta Locum Tenens the 2nd Quarter 2015 July 14 - June 15 According to
Building an Accountable Care Organization. Jean Malouin, MD MPH University of Michigan Health System September 21, 2012
 Building an Accountable Care Organization Jean Malouin, MD MPH University of Michigan Health System September 21, 2012 Agenda UMHS overview PGP demo ACO precursor Current efforts underway Role of primary
Building an Accountable Care Organization Jean Malouin, MD MPH University of Michigan Health System September 21, 2012 Agenda UMHS overview PGP demo ACO precursor Current efforts underway Role of primary
Diabetes Care 2011-2012
 Clinical Innovations in the Patient Centered Medical Home to Improve Diabetes Care Robert A. Gabbay, MD, PhD, FACP Chief Medical Officer & Senior Vice President Joslin Diabetes Center Harvard Medical School
Clinical Innovations in the Patient Centered Medical Home to Improve Diabetes Care Robert A. Gabbay, MD, PhD, FACP Chief Medical Officer & Senior Vice President Joslin Diabetes Center Harvard Medical School
New Models of Care and Approaches to Payment
 New Models of Care and Approaches to Payment Richard Lopez, MD Chief Medical Officer Richard_Lopez@AtriusHealth.org September 30, 2014 Atrius Health Non-profit alliance of six leading independent medical
New Models of Care and Approaches to Payment Richard Lopez, MD Chief Medical Officer Richard_Lopez@AtriusHealth.org September 30, 2014 Atrius Health Non-profit alliance of six leading independent medical
Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions
 Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions Scott Flinn MD Deborah Schutz RN JD Fritz Steen RN Arch Health Partners A medical foundation formed
Maximizing Limited Care Management Resources to Improve Clinical Quality and Ensure Safe Transitions Scott Flinn MD Deborah Schutz RN JD Fritz Steen RN Arch Health Partners A medical foundation formed
Accountable Care Organization
 Accountable Care Organization April 13, 2011 The Indianapolis Association of Health Underwriters Drivers of Payment Reform Increased attention to regional variation in costs and quality Payment for care
Accountable Care Organization April 13, 2011 The Indianapolis Association of Health Underwriters Drivers of Payment Reform Increased attention to regional variation in costs and quality Payment for care
Decoding Medicare Spending Per Beneficiary (MSPB) Management and Physician Opportunities Together
 Management and Physician Opportunities Together") Decoding Medicare Spending Per Beneficiary (MSPB) Management and Physician Opportunities Together Dale N. Schumacher THE TRANSFORMATION TO CONSUMER-DRIVEN HEALTHCARE Decoding Medicare Spending Per Beneficiary
Decoding Medicare Spending Per Beneficiary (MSPB) Management and Physician Opportunities Together Dale N. Schumacher THE TRANSFORMATION TO CONSUMER-DRIVEN HEALTHCARE Decoding Medicare Spending Per Beneficiary
Engage Connect Influence
 Engage Connect Influence 2013 CAP Policy Meeting Pathology s Experience with Care Coordination Blair Childs Premier Healthcare Alliance Blair Childs SVP, Public Affairs THE NATION S LARGEST HEALTHCARE
Engage Connect Influence 2013 CAP Policy Meeting Pathology s Experience with Care Coordination Blair Childs Premier Healthcare Alliance Blair Childs SVP, Public Affairs THE NATION S LARGEST HEALTHCARE
Faculty Compensation Plan. Department of Family Medicine and Community Health. UMass Memorial Health Care/University of Massachusetts Medical School
 Faculty Compensation Plan Department of Family Medicine and Community Health UMass Memorial Health Care/University of Massachusetts Medical School Faculty Compensation Plan Department of Family Medicine
Faculty Compensation Plan Department of Family Medicine and Community Health UMass Memorial Health Care/University of Massachusetts Medical School Faculty Compensation Plan Department of Family Medicine
Hospital Value-based Purchasing Specifications 2016 Updated August 2015
 Description Methodology Measurement Period Allowable Exclusions Total Performance Score Individual measures CMS incentive program for PPS hospitals. The purpose is to achieve value by tying payment to
Description Methodology Measurement Period Allowable Exclusions Total Performance Score Individual measures CMS incentive program for PPS hospitals. The purpose is to achieve value by tying payment to
Evaluating Your Hospitalist Program: Key Questions and Considerations
 Evaluating Your Hospitalist Program: Key Questions and Considerations Evaluating Your Hospitalist Program: Key Questions and Considerations By Vinnie Sharma, MBA, MPH Manager, Physician Advisory Services
Evaluating Your Hospitalist Program: Key Questions and Considerations Evaluating Your Hospitalist Program: Key Questions and Considerations By Vinnie Sharma, MBA, MPH Manager, Physician Advisory Services
Predicting What Matters Using Predictive Analytics to Reduce Suffering, Save Lives, and Optimize the Cost of Care
 Predicting What Matters Using Predictive Analytics to Reduce Suffering, Save Lives, and Optimize the Cost of Care Predictive Analytics for Population Health Management NCHICA Learning Objectives By the
Predicting What Matters Using Predictive Analytics to Reduce Suffering, Save Lives, and Optimize the Cost of Care Predictive Analytics for Population Health Management NCHICA Learning Objectives By the
Subcommittee on PCCM improvement
 Subcommittee on PCCM improvement Principles of Care Coordination Comprehensive services linked by an "integrator." Payments reflect patient complexity Current PCCM PCP office serves as care coordinator
Subcommittee on PCCM improvement Principles of Care Coordination Comprehensive services linked by an "integrator." Payments reflect patient complexity Current PCCM PCP office serves as care coordinator
CAREER PATHS IN QUALITY
 CAREER PATHS IN QUALITY Evan Benjamin, MD, FACP Assistant Professor of Medicine Vice-President Baystate Medical Center Tufts University School of Medicine BAYSTATE MEDICAL CENTER 601 bed tertiary care
CAREER PATHS IN QUALITY Evan Benjamin, MD, FACP Assistant Professor of Medicine Vice-President Baystate Medical Center Tufts University School of Medicine BAYSTATE MEDICAL CENTER 601 bed tertiary care
Physician Compensation Models for the Current Environment
 Physician Compensation Models for the Current Environment February 8, 2012 The Maine Chapter of HFMA Susan Stowell Presentation Agenda Physician market trends Health reform Impact on physician compensation
Physician Compensation Models for the Current Environment February 8, 2012 The Maine Chapter of HFMA Susan Stowell Presentation Agenda Physician market trends Health reform Impact on physician compensation
Value-Based Purchasing
 Emerging Topics in Healthcare Reform Value-Based Purchasing Janssen Pharmaceuticals, Inc. Value-Based Purchasing The Patient Protection and Affordable Care Act (ACA) established the Hospital Value-Based
Emerging Topics in Healthcare Reform Value-Based Purchasing Janssen Pharmaceuticals, Inc. Value-Based Purchasing The Patient Protection and Affordable Care Act (ACA) established the Hospital Value-Based
About MGMA. Our mission To continually improve the performance of medical group practice professionals and the organizations they represent
 About MGMA Our mission To continually improve the performance of medical group practice professionals and the organizations they represent Impact of Healthcare Reform on Pediatric Practices William F.
About MGMA Our mission To continually improve the performance of medical group practice professionals and the organizations they represent Impact of Healthcare Reform on Pediatric Practices William F.
Southwestern Vermont Medical Center Operating Budget Fiscal Year 2016
 Southwestern Vermont Medical Center Operating Budget Fiscal Year 2016 Southwestern Vermont Medical Center s (hereafter SVMC or Medical Center ) Operating Budget for Fiscal Year (hereafter FY ) 2016 has
Southwestern Vermont Medical Center Operating Budget Fiscal Year 2016 Southwestern Vermont Medical Center s (hereafter SVMC or Medical Center ) Operating Budget for Fiscal Year (hereafter FY ) 2016 has
Leveraging Big Data Improving Performance. University of Missouri Thomas J. Selva, M.D. - CMIO
 Leveraging Big Data Improving Performance University of Missouri Thomas J. Selva, M.D. - CMIO University Hospital and Clinics Ellis Fischel Cancer Center Women s and Children s Hospital Missouri Orthopaedic
Leveraging Big Data Improving Performance University of Missouri Thomas J. Selva, M.D. - CMIO University Hospital and Clinics Ellis Fischel Cancer Center Women s and Children s Hospital Missouri Orthopaedic
Southwest Medical Associates
 Southwest Medical Associates Introduction Nine medical centers + five SMA Convenient Care clinics 60% primary care (IM/FP, Peds, Ob/Gyn) Eight medical sub-specialties Adult and pediatric hospitalist groups
Southwest Medical Associates Introduction Nine medical centers + five SMA Convenient Care clinics 60% primary care (IM/FP, Peds, Ob/Gyn) Eight medical sub-specialties Adult and pediatric hospitalist groups
AASA PHYSICIAN RECRUITING AND COMPENSATION TRENDS
 AASA PHYSICIAN RECRUITING AND COMPENSATION TRENDS OUR AGENDA 1. The state of the physician workforce 2. Physician recruiting incentives and trends OUR FRAGILE, FRAGMENTED PHYSICIAN WORKFORCE PART 1 HOW
AASA PHYSICIAN RECRUITING AND COMPENSATION TRENDS OUR AGENDA 1. The state of the physician workforce 2. Physician recruiting incentives and trends OUR FRAGILE, FRAGMENTED PHYSICIAN WORKFORCE PART 1 HOW
11/24/2015. State of In-House Physician Recruitment
 State of In-House Physician Recruitment Fall 2015 1 Industry Reports Overview Recruitment Processes Report Recruitment Benchmarking Report Physician Compensation, Benefits and Recruitment Incentives Report
State of In-House Physician Recruitment Fall 2015 1 Industry Reports Overview Recruitment Processes Report Recruitment Benchmarking Report Physician Compensation, Benefits and Recruitment Incentives Report