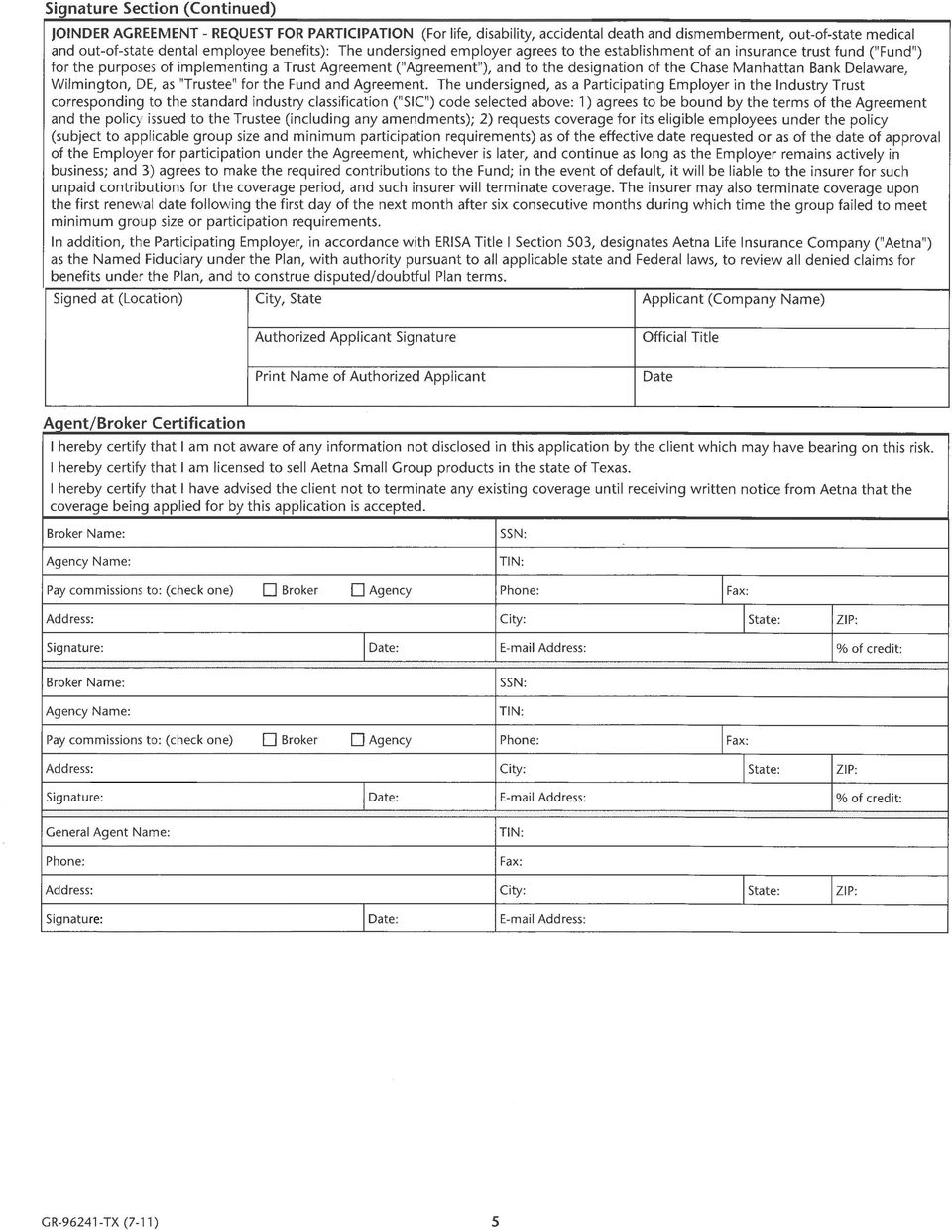
*If a spouse is enrolling, a signature must be included on the enrollment form & medical questionnaire
|
|
|
- Delphia Foster
- 8 years ago
- Views:
Transcription
1 Small Employer Cover Sheet & Checklist New Business Case Information Aetna Small Group Underwriting 4300 Centreway Place, Arlington, TX P.O. Box Arlington, TX Phone (866) Fax (877) Case Name Date Submitted (MM/DD/YY) Broker Name Broker Phone Number ( ) Broker Physical Address City State Zip Code Broker Address Broker Fax Number ( ) Proposed Effective Date (MM/DD/YY) SUBMISSION DATE All new cases with 2 to 50 employees are preferred to be received by Aetna on or before the 5th business day prior to the requested effective date. Cases will be accepted until the last day of the month prior to the effective date. If a cutoff deadline occurs on a weekend, all new cases sold need to be received on the preceding Friday. If incomplete information is provided or if the submission is not complete until after the cut-off date, the case could be assigned a later effective date. REQUIRED FOR NEW BUSINESS Employer Master Application Must be completed, signed and dated by employer Copy of Sold Rates Must be signed by the employer and attached to the new case submission Employer Disclosure Appropriate Disclosure Form based on plan selected for TX must be signed and dated by the employer 50/50 Benefit Description Form 50/50 Benefit Description form signed and dated by the employer Enrollment/Change Form/ Original copy completed & signed byeach employee enrolling for coverage Medical Questionnaire & any continuees.* *If a spouse is enrolling, a signature must be included on the enrollment form & medical questionnaire Employees waiving/declining coverage must complete the waiver section of the Enrollment/Change form. If coverage is being waived due to other coverage, the carrier name, telephone number and group number must be listed. Copy of most recent Quarterly Wage and Tax Statement (QWTS) containing the names, salaries, etc. of all employees of the employer group. The QWTS must be signed and dated by the owner or officer of the company unless filed electronically. If filed electronically, please provide a copy of the electronic validation. Employees who have terminated or work part-time must be noted accordingly on the QWTS. Terminated employees must have the date of termination listed on the QWTS. Newly-hired employees not listed on the QWTS must provide the first and last month s payroll stub and registry/summary for each employee. Sole Proprietor, Partners or Corporate Officers not reported on the Quarterly Wage and Tax form must submit a completed Small Employer (2-50) Proof of Eligibility Form. Also, as identified on the form, additional supporting documentation must be submitted. If group coverage currently exists, a copy of the most recent prior carrier bill must be provided. Individuals contained on the bill should match those listed on the wage and tax statement. If not, please indicate on the bill why they are not on the wage and tax. A check on company check stock for 100% of the first month s medical, dental, STD and life premiums payable to Aetna Health Management, L.L.C. (Aetna s receipt of the check does not guarantee acceptance of the group) Copy of the sold proposal including rates and plan design(s). Verify contribution and participation requirements by product. GENERAL INFORMATION c If applying for PPO or Indemnity medical, please list the prior carrier individual deductible $ d If applying for dental, does dental coverage currently exist? YES NO e If yes and prior plan includes Orthodontia, please provide the prior plan Ortho Max $ f Please note that additional documentation may be required (Common ownership, newly formed business, etc.) BROKER / GENERAL AGENT COMMENTS Broker Signature GA Signature Date (MM/DD/YY) Date (MM/DD/YY) All paperwork is enclosed and my submission is complete. I understand incomplete paperwork could delay the effective date of coverage. Plan Sponsor Signature Date (MM/DD/YY) This submission does not constitute approval. Please do not cancel or change your existing health coverage until you receive formal approval from Aetna SW (3/06)

2 Proof of Eligibility Form Small Employers with 50 or fewer eligible employees Sole Proprietors, Partners or Corporate Officers (To be used for eligible individuals that are not reported on a quarterly wage and tax form) Full Name (First, MI, Last) Phone No. Title Percentage of Ownership in Firm Date of Hire Number of hours worked per week Company Name In order to satisfy the Small Employer Requirements for Proof of Eligibility, the following most recent IRS Tax documents are required. (Anyone eligible must appear on the below documents.) Please check one of the following: Must submit one of the following identified documents : C-Corporation? W2 S-Corporation? IRS Form 1120 S Schedule K-1 along with Schedule E (Form1040) Partnership? IRS Form 1065 schedule K-1; or? IRS Form 1120S Schedule K1 along with Schedule E (Form1040) Limited Liability Company (LLC)? May file as either C Corporation or Partnership Sole Proprietor? IRS Schedule SE and Schedule C filed with Form 1040; or? IRS Form 1040 Schedule F or K1 I attest that while I am not listed on the state quarterly wage and tax statement for this company, the following are true (check applicable boxes): 1. I am a sole proprietor, partner or corporation officer of the company indicated above. 2. I am actively at work at this company on a full time, permanent basis working no less than the minimum number of hours required by the applicable State Laws. 3. I draw wages, compensation, dividends or other distributions from this company on a regular basis and do not derive substantial earned income from any other employment. 4. I have satisfied the designated waiting period before health insurance coverage is to become effective. 5. I am a retiree of the above company and qualify for benefits under their guidelines. (Retiree coverage is only available in states where mandated. Maine and New Hampshire - all groups. Florida and Illinois municipalities only.) I understand this information may be subject to audit and agree to provide Aetna and/or its affiliates, with any and all information and documentation necessary to validate the above statements. I also understand that any misrepresentation by me of my true circumstances may result in the termination of group health coverage from Aetna and/or its affiliates, for me, my enrolled dependents and or this company as Aetna and/or its affiliates may choose. Aetna and/or its affiliates also expressly reserve any other rights and remedies. It is unlawful to knowingly provide false, incomplete, or misleading information to an insurance company for the purpose of defrauding the company. Penalties include imprisonment, fines, and denial of insurance benefits. Signature Date 05/19/06
 Please check one of the following: Must submit one of the following identified documents : C-Corporation?")
3

4

5

6
7
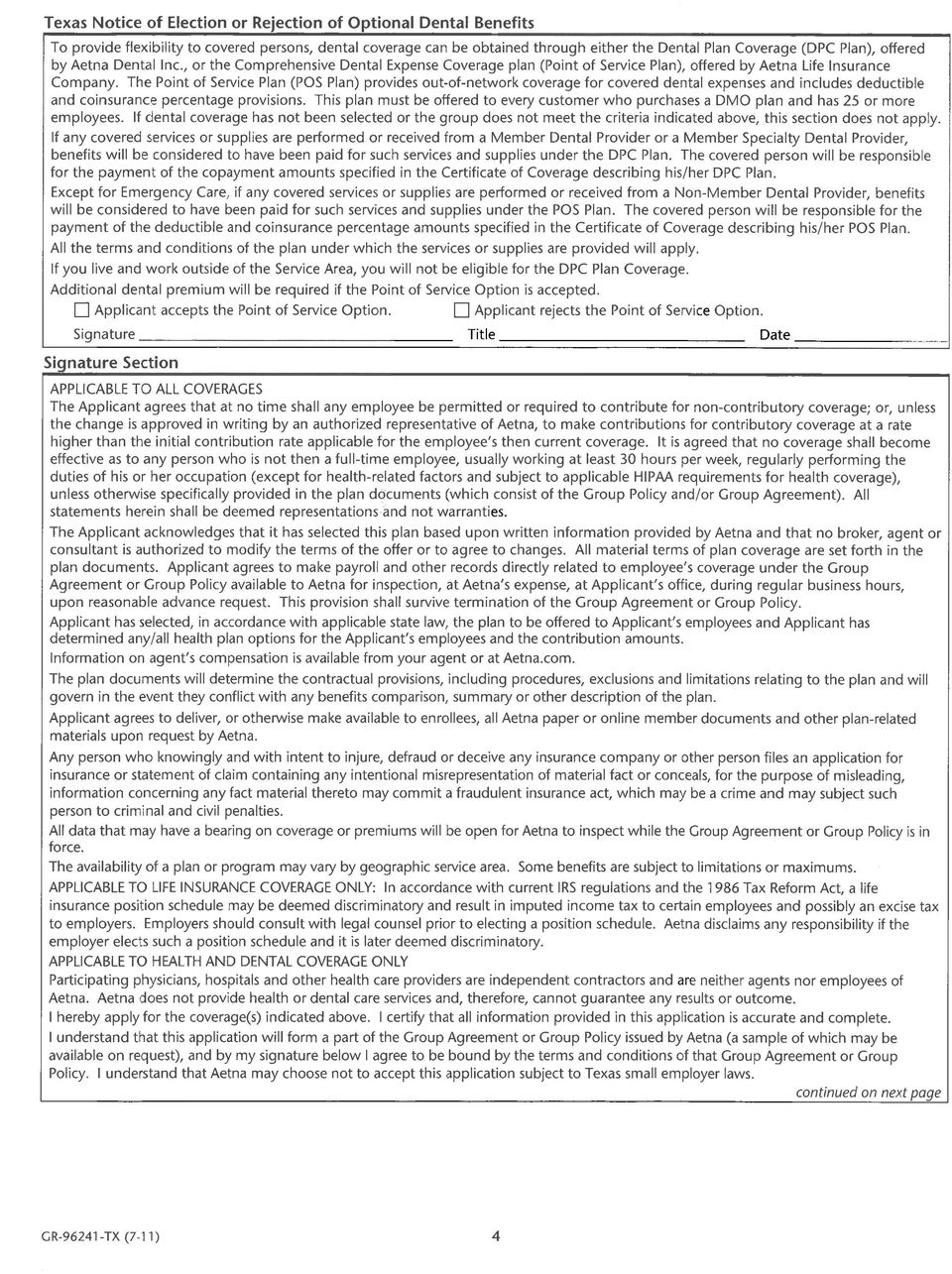
8 Form CCP Figure 1 TEXAS DEPARTMENT OF INSURANCE REQUIRED DISCLOSURE NOTICE FOR ALL EMPLOYER GROUP INDEMNITY CONSUMER CHOICE BENEFIT PLANS ISSUED IN TEXAS As required by 28 TAC , I have been informed that the Consumer Choice Standard Benefit Plan that I am purchasing does not include all state mandated health insurance benefits. I understand that purchase of this plan may limit future coverage options in the event that plan participant's health changes and needed benefits are not covered under the consumer choice health benefit plan. I understand that the following benefits are provided at a reduced level from what is mandated, or are excluded completely from the plan: Mandated Benefit Description IN VITRO FERTILIZATION Article , Section 3A, Texas Insurance Code Unless rejected in writing by the group policyholder, benefits for in-vitro fertilization must be provided to the same extent as benefits provided for other pregnancy-related procedures subject to certain requirements. MENTAL HEALTH Article (F), Texas Insurance Code The insurer must offer and the group policyholder shall have the right to reject benefits for mental or emotional illness. SERIOUS MENTAL ILLNESS Article , Texas Insurance Code Small employer carriers must offer to small employers coverage for serious mental illness that complies with the following: (a) coverage for 45 days of inpatient treatment, and 60 visits for outpatient treatment, including group and individual outpatient treatment in each calendar year; (b) the coverage may NOT include a lifetime limit on the number of days of inpatient treatment or the number of outpatient visits covered under the policy; and (c) the coverage must include the same amount limits, and deductibles and coinsurance factors for serious mental illness as for physical illness. SPEECH AND HEARING - Article (G), Texas Insurance Code Unless rejected by the group policyholder or an alternative level of benefits is negotiated, benefits must be provided for the necessary care and treatment of loss or impairment of speech or hearing that are not less favorable than for physical illness generally. (See also Hearing Screening for Children under section for Mandated Benefits). Benefit Reduced The base medical plan (for groups 2-50) provides coverage for both serious and non-serious mental illness, limited to 14 days inpatient and 20 visits outpatient per member per year. Full benefit per mandate included in medical plans for groups over 50 lives. The base medical plan (for groups 2-50) provides coverage for both serious and non-serious mental illness, limited to 14 days inpatient and 20 visits outpatient per member per year. Full benefit per mandate included in medical plans for groups over 50 lives. Outpatient Speech therapy limited to 20 visits per year. Benefit Excluded Not offered; not covered. Additional benefits not offered or covered Additional benefits not covered or offered. * Note: if additional space is needed, the carrier may add additional lines, or may continue the list on a subsequent page, but must clearly note that an additional page is attached. SMER Lite Disclosure (5/08) For use with Aetna OAMC E1000 and E1500, B500-11, B , B , B , B , B %-11, B %-11, B %-11, Preferred Plans B , B , B , HSA s %, %, %, and PPO s B , B % eff 12/1/11 LHL 254 Rev.05/04

9 Form CCP Figure 1 ** Pursuant to the Federal Patient Protection and Access to Care Act (PPACA), the following are covered at 100% with no Copayments, Deductibles or dollar maximum benefits: Evidence-based items or services that have in effect a rating of "A" or "B" in the current recommendations of the United States Preventative Service Task Force (USPSTF); Routine Adult Physical Examinations (including immunizations, routine vision and hearing screenings); Routine Well Child Care (including immunizations); Routine Cancer Screenings (which include Screening Mammograms; Prostate Specific Antigen (PSA) Tests; Digital-Rectal Exams (DRE); Fecal Occult Blood Tests (FOBT); Sigmoidoscopies; Double Contrast Barium Enemas (DCBE) and Colonoscopies); Routine Eye Examinations, including refraction; Pediatric Preventive Dental; and Routine Gynecological Exams, including routine Pap smears. I understand that I may obtain from the Department of Insurance a consumer brochure with more information on Consumer Choice Health Benefit Plans, either by visiting the TDI website at or by calling By signing this document I affirm that I was offered a benefit plan that contains the state mandated health insurance benefits and that I have elected to purchase this Consumer Choice Benefit Plan. Signature of Applicant Name of Applicant Name of Business (if applicable) Date Address City State Zip Note: This form must be retained by the carrier issuing the policy and must be provided to the Commissioner of Insurance upon request. You have the right to a copy of this written disclosure statement free of charge. A new form must be completed upon each subsequent renewal of this policy. SMER Lite Disclosure (5/08) For use with Aetna OAMC E1000 and E1500, B500-11, B , B , B , B , B %-11, B %-11, B %-11, Preferred Plans B , B , B , HSA s %, %, %, and PPO s B , B % eff 12/1/11 LHL 254 Rev.05/04
 Tests; Digital-Rectal Exams (DRE); Fecal Occult Blood Tests (FOBT); Sigmoidoscopies; Double Contrast Barium Enemas (DCBE) and Colonoscopies); Routine Eye Examinations,")
10 Addendum to New Business Input Documents Mandatory Requirement for Health Care Reform Aetna is collecting employee count information to comply with the health care reform law. We are asking you to provide the average number of people you employed in the prior calendar year. We need this information so we can accurately report your data and calculate any potential rebates to which you and your covered subscribers may be entitled under the new medical loss ratio requirements set forth in the Affordable Care Act (ACA). The law defines the number of employees as "the average number of employees employed by the employer's company during the preceding calendar year." An employee is defined as any person for whom the company issues a W-2, including full-time, part-time, and seasonal workers, and regardless of insurance eligibility (sample calculation below). We need the average number of total employees for your company in 2010 to support the 2011 calculations and reports and the payment of any rebates due in How to calculate the average number of total employees* To calculate average number of employees for the year, determine the average number of employees for each month in 2010, add them together and then divide the total by twelve. In the example below, 253 / 12 = 21. Round up or down to the nearest whole number. Jan Feb Mar Apr May June July Aug Sept Oct Nov Dec Average Month Full Time Part Time Seasonal Total *Subject to change based on future regulatory guidance Please enter your calculated average number of employees in the box below. Average Employees in 2010 (whole numbers only; please print legibly) By signing below I certify that: I am an authorized representative of the plan(s) for which this information is being provided. The information I have provided is true and correct. Aetna may rely on the responses I have provided. First Name (Please Print): Last Name (Please Print): Title: Company Name: Address (optional): Signature: Today s Date: Aetna reserves the right to audit all information provided. Providing false, incomplete, or misleading facts or information to an insurance company for the purpose of defrauding or attempting to defraud the company, may violate applicable insurance statutes. GR (7-11)
.")
11
12

13

14

Universal Employer Group Application Package
 Universal Employer Group Application Package Coventry Health and Life Insurance Company, Coventry Health Care of Florida, Inc. (hereinafter referred to as Coventry ). Coventry may be referred to as Plan.
Universal Employer Group Application Package Coventry Health and Life Insurance Company, Coventry Health Care of Florida, Inc. (hereinafter referred to as Coventry ). Coventry may be referred to as Plan.
New York Employer Application For Life, AD&PL, Medical and Dental Coverage
 New York Employer Application For Life, AD&PL, Medical and Dental Coverage Aetna Life Insurance Company 151 Farmington Avenue Hartford, CT 06156 FOR GROUP COVERAGE (51 100) ELIGIBLE EMPLOYEES) Life, Accidental
New York Employer Application For Life, AD&PL, Medical and Dental Coverage Aetna Life Insurance Company 151 Farmington Avenue Hartford, CT 06156 FOR GROUP COVERAGE (51 100) ELIGIBLE EMPLOYEES) Life, Accidental
Employer Application. Texas
 Texas Employer Application FOR GROUP COVERAGE: Large Employer 51 or more employees Small Employer 2 50 employees ** You have the option to choose this Consumer Choice of Benefits Health Insurance Plan
Texas Employer Application FOR GROUP COVERAGE: Large Employer 51 or more employees Small Employer 2 50 employees ** You have the option to choose this Consumer Choice of Benefits Health Insurance Plan
Nevada Employer s Guide to the Affordable Care Act. Nevada Division of Insurance
 Nevada Employer s Guide to the Affordable Care Act Nevada Division of Insurance Nevada Employer s Guide to the Affordable Care Act State of Nevada Department of Business and Industry Division of Insurance
Nevada Employer s Guide to the Affordable Care Act Nevada Division of Insurance Nevada Employer s Guide to the Affordable Care Act State of Nevada Department of Business and Industry Division of Insurance
Employer Application and Joinder Agreement FOR GROUP COVERAGE (2 100 ELIGIBLE EMPLOYEES)
") Illinois Employer Application and Joinder Agreement FOR GROUP COVERAGE (2 100 ELIGIBLE EMPLOYEES) Life, Accidental Death & Personal Loss, Disability, Aetna Managed Choice (Open Access) and Aetna PPO plans
Illinois Employer Application and Joinder Agreement FOR GROUP COVERAGE (2 100 ELIGIBLE EMPLOYEES) Life, Accidental Death & Personal Loss, Disability, Aetna Managed Choice (Open Access) and Aetna PPO plans
Street Address (PO Box not acceptable) City State ZIP. Billing Address (if different than above) City State ZIP
 City State ZIP. Billing Address (if different than above) City State ZIP") Georgia Employer Application FOR GROUP COVERAGE (2-100 ELIGIBLE EMPLOYEES) Life, Accidental Death & Personal Loss, Disability and Aetna PPO, Managed Choice Open Access and Indemnity plans are provided
Georgia Employer Application FOR GROUP COVERAGE (2-100 ELIGIBLE EMPLOYEES) Life, Accidental Death & Personal Loss, Disability and Aetna PPO, Managed Choice Open Access and Indemnity plans are provided
New Jersey Small Employer Certification
 Please Mail To: AmeriHealth Insurance Company of New Jersey AmeriHealth HMO, Inc. 259 Prospect Plains Road, Building M Cranbury, NJ 08512 Tel 215-640-7573 Fax 215-238-7940 Email: NJSEH-Cert@amerihealth.com
Please Mail To: AmeriHealth Insurance Company of New Jersey AmeriHealth HMO, Inc. 259 Prospect Plains Road, Building M Cranbury, NJ 08512 Tel 215-640-7573 Fax 215-238-7940 Email: NJSEH-Cert@amerihealth.com
TIME INSURANCE COMPANY EMPLOYER APPLICATION for Assurant Self-Funded Health Plans
 TIME INSURANCE COMPANY EMPLOYER APPLICATION for Assurant Self-Funded Health Plans Home Office Use Only Group Number: Instructions for completing this agreement: 1) The employer or employer representative
TIME INSURANCE COMPANY EMPLOYER APPLICATION for Assurant Self-Funded Health Plans Home Office Use Only Group Number: Instructions for completing this agreement: 1) The employer or employer representative
Small Employer Group Application Instructions
 Small Employer Group Application Instructions Instructions The attached forms should be completed with the assistance of your authorized Broker or Horizon Blue Cross Blue Shield of New Jersey Sales Representative.
Small Employer Group Application Instructions Instructions The attached forms should be completed with the assistance of your authorized Broker or Horizon Blue Cross Blue Shield of New Jersey Sales Representative.
Preferred Risk Administrators EMPLOYER APPLICATION For Self-Funded Health Plans HOME OFFICE USE ONLY: Group Number:
 Preferred Risk Administrators EMPLOYER APPLICATION For Self-Funded Health Plans HOME OFFICE USE ONLY: Group Number: Instructions for completing this agreement: 1) The employer or employer representative
Preferred Risk Administrators EMPLOYER APPLICATION For Self-Funded Health Plans HOME OFFICE USE ONLY: Group Number: Instructions for completing this agreement: 1) The employer or employer representative
New Group Application East Region New business effective Jan. 1, 2011
 New Group Application East Region New business effective Jan. 1, 2011 2-50 Eligible employees PriorityHMO SM PriorityPOS SM PriorityPPO SM Revised 10/10 Life just got a little easier. This comprehensive
New Group Application East Region New business effective Jan. 1, 2011 2-50 Eligible employees PriorityHMO SM PriorityPOS SM PriorityPPO SM Revised 10/10 Life just got a little easier. This comprehensive
Employer Group Benefits Data Form 2-100 Eligible Employees
 Employer Group Benefits Data Form 2-100 Eligible Employees INSTRUCTIONS FOR COMPLETION 1. Answer all questions completely and accurately. 2. Do not cancel your existing coverage until you receive written
Employer Group Benefits Data Form 2-100 Eligible Employees INSTRUCTIONS FOR COMPLETION 1. Answer all questions completely and accurately. 2. Do not cancel your existing coverage until you receive written
SMALL EMPLOYER GROUP APPLICATION INSTRUCTIONS
 SMALL EMPLOYER GROUP APPLICATION INSTRUCTIONS This form should be completed with the assistance of your authorized Broker or Horizon Healthcare of New York Sales Representative. Please be sure that all
SMALL EMPLOYER GROUP APPLICATION INSTRUCTIONS This form should be completed with the assistance of your authorized Broker or Horizon Healthcare of New York Sales Representative. Please be sure that all
Employee Enrollment Application EmployeeElect for 1 50 Employee Small Groups. California
 Employee Enrollment Application EmployeeElect for 1 50 Employee Small Groups California Health care plans offered by Anthem Blue Cross. Insurance plans offered by Anthem Blue Cross Life and Health Insurance
Employee Enrollment Application EmployeeElect for 1 50 Employee Small Groups California Health care plans offered by Anthem Blue Cross. Insurance plans offered by Anthem Blue Cross Life and Health Insurance
Street Address (PO Box not acceptable) City State ZIP. Billing Address (if different than above) City State ZIP
 City State ZIP. Billing Address (if different than above) City State ZIP") Florida Employer Application FOR GROUPS OF 100 or FEWER ELIGIBLE EMPLOYEES Life, Accidental Death & Personal Loss, Disability, Aetna Managed Choice, and Aetna PPO plans are underwritten by Aetna Life Insurance
Florida Employer Application FOR GROUPS OF 100 or FEWER ELIGIBLE EMPLOYEES Life, Accidental Death & Personal Loss, Disability, Aetna Managed Choice, and Aetna PPO plans are underwritten by Aetna Life Insurance
Small Employer Group Application Instructions
 Small Employer Group Application Instructions Instructions The attached forms should be completed with the assistance of your authorized Broker or Horizon Blue Cross Blue Shield of New Jersey Sales Representative.
Small Employer Group Application Instructions Instructions The attached forms should be completed with the assistance of your authorized Broker or Horizon Blue Cross Blue Shield of New Jersey Sales Representative.
New Group Submission Checklist HARVARD PILGRIM HEALTH CARE Best Buy HSA PPO Plans
 hsainsurance.com New Group Submission Checklist HARVARD PILGRIM HEALTH CARE Best Buy HSA PPO Plans To ensure your application is processed as quickly and accurately as possible, follow these steps: 1.
hsainsurance.com New Group Submission Checklist HARVARD PILGRIM HEALTH CARE Best Buy HSA PPO Plans To ensure your application is processed as quickly and accurately as possible, follow these steps: 1.
2016 employer application for small groups
 SMALL BUSINESS GROUP 2016 employer application for small groups For coverage effective on or after Jan. 1, 2016 1 APPLICATION CHECKLIST Please make sure your application package includes: Signed employer
SMALL BUSINESS GROUP 2016 employer application for small groups For coverage effective on or after Jan. 1, 2016 1 APPLICATION CHECKLIST Please make sure your application package includes: Signed employer
UNDERWRITING QUICK REFERENCE GUIDE SMALL BUSINESS GROUP. What works for you?
 Healthcare UnitedHealthcare UnitedHealthcare UnitedHealthcare UnitedHealthcare UnitedHealthcare UnitedHealthcare UnitedHealthcare UnitedHealthcare UnitedHealthcare UnitedHealthc edhealthcare UnitedHealthcare
Healthcare UnitedHealthcare UnitedHealthcare UnitedHealthcare UnitedHealthcare UnitedHealthcare UnitedHealthcare UnitedHealthcare UnitedHealthcare UnitedHealthcare UnitedHealthc edhealthcare UnitedHealthcare
EMBLEMHEALTH FOR SMALL GROUPS
 Print In Ink EMBLEMHEALTH FOR SMALL GROUPS EmblemHealth insurance programs are underwritten by Group Health Incorporated (GHI), HIP Health Plan of Greater New York (HIP) and HIP Insurance Company of New
Print In Ink EMBLEMHEALTH FOR SMALL GROUPS EmblemHealth insurance programs are underwritten by Group Health Incorporated (GHI), HIP Health Plan of Greater New York (HIP) and HIP Insurance Company of New
PLAN DESIGN AND BENEFITS HMO Open Access Plan 912
 PLAN FEATURES Deductible (per calendar year) $1,000 Individual $2,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. Member cost sharing for certain services
PLAN FEATURES Deductible (per calendar year) $1,000 Individual $2,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. Member cost sharing for certain services
Important Effective Dates for Employers and Health Plans
 Brought to you by Krempa Associates, Inc. Important Effective Dates for Employers and Health Plans On March 23, 2010, President Obama signed the health care reform bill, or Affordable Care Act (ACA), into
Brought to you by Krempa Associates, Inc. Important Effective Dates for Employers and Health Plans On March 23, 2010, President Obama signed the health care reform bill, or Affordable Care Act (ACA), into
Important Effective Dates for Employers and Health Plans
 Brought to you by Sullivan Benefits Important Effective Dates for Employers and Health Plans On March 23, 2010, President Obama signed the health care reform bill, or Affordable Care Act (ACA), into law.
Brought to you by Sullivan Benefits Important Effective Dates for Employers and Health Plans On March 23, 2010, President Obama signed the health care reform bill, or Affordable Care Act (ACA), into law.
New York Small Group Indemnity Aetna Life Insurance Company Plan Effective Date: 10/01/2010. PLAN DESIGN AND BENEFITS - NY Indemnity 1-10/10*
 PLAN FEATURES Deductible (per calendar year) $2,500 Individual $7,500 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. Member cost sharing for certain services,
PLAN FEATURES Deductible (per calendar year) $2,500 Individual $7,500 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. Member cost sharing for certain services,
Important Effective Dates for Employers and Health Plans
 Brought to you by Hipskind Seyfarth Risk Solutions Important Effective Dates for Employers and Health Plans On March 23, 2010, President Obama signed the health care reform bill, or Affordable Care Act
Brought to you by Hipskind Seyfarth Risk Solutions Important Effective Dates for Employers and Health Plans On March 23, 2010, President Obama signed the health care reform bill, or Affordable Care Act
Employer Group Application
 Employer Group Application Please complete entire application using dark blue or black ink. 1515 North Saint Joseph Avenue PO Box 8000 Marshfield, WI 54449-8000 1-800-472-2363 or 715-221-9555 TTY 1-877-727-2232
Employer Group Application Please complete entire application using dark blue or black ink. 1515 North Saint Joseph Avenue PO Box 8000 Marshfield, WI 54449-8000 1-800-472-2363 or 715-221-9555 TTY 1-877-727-2232
Section A: Company Information Employer tax ID no. (required) City County State ZIP code
 City County State ZIP code") Employer Enrollment Application For 20-100 Anthem Balanced Funding California Insurance plans offered by Anthem Blue Cross Life and Health Insurance Company (Anthem). You, the employer, must complete this
Employer Enrollment Application For 20-100 Anthem Balanced Funding California Insurance plans offered by Anthem Blue Cross Life and Health Insurance Company (Anthem). You, the employer, must complete this
PART A. I,, in my capacity as Corporate Secretary or LLC Manager Name of Corporate Secretary or LLC Manager
 COLORADO DEPARTMENT OF LABOR AND EMPLOYMENT DIVISION OF WORKERS COMPENSATION REJECTION OF COVERAGE BY CORPORATE OFFICERS OR MEMBERS OF A LIMITED LIABILITY COMPANY (LLC) PART A 1. Type of Entity Corporation
COLORADO DEPARTMENT OF LABOR AND EMPLOYMENT DIVISION OF WORKERS COMPENSATION REJECTION OF COVERAGE BY CORPORATE OFFICERS OR MEMBERS OF A LIMITED LIABILITY COMPANY (LLC) PART A 1. Type of Entity Corporation
PLAN DESIGN AND BENEFITS - Tx OAMC 2500 08 PREFERRED CARE
 PLAN FEATURES Deductible (per calendar year) $2,500 Individual $5,000 Individual $7,500 3 Individuals per $15,000 3 Individuals per Unless otherwise indicated, the Deductible must be met prior to benefits
PLAN FEATURES Deductible (per calendar year) $2,500 Individual $5,000 Individual $7,500 3 Individuals per $15,000 3 Individuals per Unless otherwise indicated, the Deductible must be met prior to benefits
Colorado Employer Application For employer groups with 1-50 employees
 Colorado Employer Application For employer groups with 1-50 employees P.O. Box 14326 Reading, PA 19612 www.seechangehealth.com Main: 866-340-7182 Fax: 610-374-6986 Enroll@SeeChangeHealth.com 1. Company
Colorado Employer Application For employer groups with 1-50 employees P.O. Box 14326 Reading, PA 19612 www.seechangehealth.com Main: 866-340-7182 Fax: 610-374-6986 Enroll@SeeChangeHealth.com 1. Company
Small Group Application/Change Form 2 50 Eligible Employees
 Small Group Application/Change Form 2 50 Eligible Employees Thank you for choosing Empire. Please fill out all items in order for us to quickly and accurately process your application. Once you ve completed
Small Group Application/Change Form 2 50 Eligible Employees Thank you for choosing Empire. Please fill out all items in order for us to quickly and accurately process your application. Once you ve completed
Fax this request to the Regional Sales Office: (610) 524-5289. Request an Assurant Insurance Company small group quote.
 524-5289. Request an Assurant Insurance Company small group quote.") Fax this request to the Regional Sales Office: (610) 524-5289 Request an Assurant Insurance Company small group quote. 1. Completion of Part 1 (Group and Plan Data). 2. Completion of Part 2 (Employee Data)
Fax this request to the Regional Sales Office: (610) 524-5289 Request an Assurant Insurance Company small group quote. 1. Completion of Part 1 (Group and Plan Data). 2. Completion of Part 2 (Employee Data)
PLAN DESIGN AND BENEFITS POS Open Access Plan 1944
 PLAN FEATURES PARTICIPATING Deductible (per calendar year) $3,000 Individual $9,000 Family $4,000 Individual $12,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being
PLAN FEATURES PARTICIPATING Deductible (per calendar year) $3,000 Individual $9,000 Family $4,000 Individual $12,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being
PROFESSIONAL GROUP PLANS, INC.
 PROFESSIONAL GROUP PLANS, INC. Specializing in Employee Benefits Horizon Healthcare of New York New Business Submission Checklist Small Group Sold Case Checklist Employer Application Copy of Sold Proposal
PROFESSIONAL GROUP PLANS, INC. Specializing in Employee Benefits Horizon Healthcare of New York New Business Submission Checklist Small Group Sold Case Checklist Employer Application Copy of Sold Proposal
PRODUCERS QUICK REFERENCE GUIDE Agent Marketing Support Toll Free: 866-280-0766 In Columbia: 803-382-5976 www.bluechoicesc.com
 PRODUCERS QUICK REFERENCE GUIDE Agent Marketing Support Toll Free: 866-280-0766 In Columbia: 803-382-5976 www.bluechoicesc.com Group Size and Proposal Rating: BusinessADVANTAGE Plans 1/1/2014 2 50 Adjusted
PRODUCERS QUICK REFERENCE GUIDE Agent Marketing Support Toll Free: 866-280-0766 In Columbia: 803-382-5976 www.bluechoicesc.com Group Size and Proposal Rating: BusinessADVANTAGE Plans 1/1/2014 2 50 Adjusted
New York Small Group Application OHI I. GENERAL INFORMATION
 New York Small Group Application OHI Oxford Health Insurance Inc. www.oxfordhealth.com Mailing Address: Group Enrollment Department, 14 Central Park Drive, Hooksett, NH 03106 I. GENERAL INFORMATION Freedom
New York Small Group Application OHI Oxford Health Insurance Inc. www.oxfordhealth.com Mailing Address: Group Enrollment Department, 14 Central Park Drive, Hooksett, NH 03106 I. GENERAL INFORMATION Freedom
PLAN DESIGN AND BENEFITS Basic HMO Copay Plan 1-10
 PLAN FEATURES Deductible (per calendar year) Member Coinsurance Not Applicable Not Applicable Out-of-Pocket Maximum $5,000 Individual (per calendar year) $10,000 Family Once the Family Out-of-Pocket Maximum
PLAN FEATURES Deductible (per calendar year) Member Coinsurance Not Applicable Not Applicable Out-of-Pocket Maximum $5,000 Individual (per calendar year) $10,000 Family Once the Family Out-of-Pocket Maximum
EMPLOYER GROUP APPLICATION Segment 2: Small Group Bundled with Medical; Size 2 100
 The HIPAA Certification must be included with the Employer Group Application in order for this application to be considered complete. Incomplete applications may be returned. EMPLOYER GROUP APPLICATION
The HIPAA Certification must be included with the Employer Group Application in order for this application to be considered complete. Incomplete applications may be returned. EMPLOYER GROUP APPLICATION
Small Business Application
 Small Business Application for Group Enrollment Agreement/Group Policy Medical and Life/AD&D plans are provided by Health Net of Arizona, Inc. and/or Health Net Life Insurance Company (together, Health
Small Business Application for Group Enrollment Agreement/Group Policy Medical and Life/AD&D plans are provided by Health Net of Arizona, Inc. and/or Health Net Life Insurance Company (together, Health
How To Get A Life Insurance Policy In Gorgonia
 Employee Enrollment Application For 51+ Employee s Georgia You, the employee, must complete this application. You are solely responsible for its accuracy and completeness. To avoid the possibility of delay,
Employee Enrollment Application For 51+ Employee s Georgia You, the employee, must complete this application. You are solely responsible for its accuracy and completeness. To avoid the possibility of delay,
PLAN DESIGN AND BENEFITS - New York Open Access EPO 1-10/10
 PLAN FEATURES Deductible (per calendar year) $1,000 Individual $3,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. Member cost sharing for certain services,
PLAN FEATURES Deductible (per calendar year) $1,000 Individual $3,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. Member cost sharing for certain services,
COLORADO Assurant Health Individual Medical Metallic Plans Enrollment Packet
 Client Tip Sheet COLORADO Assurant Health Individual Medical Metallic Plans Enrollment Packet Thank you for applying for an Assurant Health Individual Medical Metallic plan. Please review the product materials
Client Tip Sheet COLORADO Assurant Health Individual Medical Metallic Plans Enrollment Packet Thank you for applying for an Assurant Health Individual Medical Metallic plan. Please review the product materials
How To Get A Group Insurance Plan From Tufts Health Plan
 MASSACHUSETTS NEW CASE SUBMISSION CHECKLIST To help you set up your Tufts Health Plan coverage, simply submit the items listed below. Tufts Health Plan must receive all proposed sold account paperwork
MASSACHUSETTS NEW CASE SUBMISSION CHECKLIST To help you set up your Tufts Health Plan coverage, simply submit the items listed below. Tufts Health Plan must receive all proposed sold account paperwork
How To Get Disability Insurance In New York
 NEW YORK DISABILITY BENEFITS LAW (DBL) State-mandated, non-occupational disability coverage for your employees WHILE EMPLOYEES RECOVER PROVIDE THEM PEACE OF MIND RATES EFFECTIVE 10/1/2014 GROUPROTECTOR
NEW YORK DISABILITY BENEFITS LAW (DBL) State-mandated, non-occupational disability coverage for your employees WHILE EMPLOYEES RECOVER PROVIDE THEM PEACE OF MIND RATES EFFECTIVE 10/1/2014 GROUPROTECTOR
SMALL GROUP PLAN DESIGN AND BENEFITS OPEN CHOICE OUT-OF-STATE PPO PLAN - $1,000
 PLAN FEATURES PREFERRED CARE NON-PREFERRED CARE Deductible (per calendar year; applies to all covered services) $1,000 Individual $3,000 Family $2,000 Individual $6,000 Family Plan Coinsurance ** 80% 60%
PLAN FEATURES PREFERRED CARE NON-PREFERRED CARE Deductible (per calendar year; applies to all covered services) $1,000 Individual $3,000 Family $2,000 Individual $6,000 Family Plan Coinsurance ** 80% 60%
PLAN DESIGN AND BENEFITS - Tx OAMC Basic 2500-10 PREFERRED CARE
 PLAN FEATURES Deductible (per calendar year) $2,500 Individual $4,000 Individual $7,500 Family $12,000 Family 3 Individuals per Family 3 Individuals per Family Unless otherwise indicated, the Deductible
PLAN FEATURES Deductible (per calendar year) $2,500 Individual $4,000 Individual $7,500 Family $12,000 Family 3 Individuals per Family 3 Individuals per Family Unless otherwise indicated, the Deductible
Employer/Group Enrollment Application & Change Form
 Employer/Group Enrollment Application & Change Form MMO 1-99 Eligible Employees Employer Group Enrollment Application/Change Form MMO 1-99 Eligible Employees initial enrollment change 1. Group/Company
Employer/Group Enrollment Application & Change Form MMO 1-99 Eligible Employees Employer Group Enrollment Application/Change Form MMO 1-99 Eligible Employees initial enrollment change 1. Group/Company
EMPLOYER GROUP APPLICATION Segment 2: Small Group Bundled with Medical; Size 2 100
 The HIPAA Certification must be included with the Employer Group Application in order for this application to be considered complete. Incomplete applications may be returned. EMPLOYER GROUP APPLICATION
The HIPAA Certification must be included with the Employer Group Application in order for this application to be considered complete. Incomplete applications may be returned. EMPLOYER GROUP APPLICATION
Rocky Mountain Health Plans Individual Application
 Plans underwritten by Rocky Mountain HMO (RMHMO) 1A Rocky Mountain Health Plans Individual Application Thank you for choosing Rocky Mountain Health Plans (RMHP) for your health care coverage. Here are
Plans underwritten by Rocky Mountain HMO (RMHMO) 1A Rocky Mountain Health Plans Individual Application Thank you for choosing Rocky Mountain Health Plans (RMHP) for your health care coverage. Here are
Underwriting Guidelines For Specialty Benefit Solutions (SBS) & Oxford Benefit Management (OBM)
 & Oxford Benefit Management (OBM)") Underwriting Guidelines For Specialty Benefit Solutions (SBS) & Oxford Benefit Management (OBM) July, 2012 Version 1.0 Prepared by UnitedHealthcare Specialty Benefits 1 10/16/2012 The following document
Underwriting Guidelines For Specialty Benefit Solutions (SBS) & Oxford Benefit Management (OBM) July, 2012 Version 1.0 Prepared by UnitedHealthcare Specialty Benefits 1 10/16/2012 The following document
Please complete in blue or black ink only. Section A: Employee Information Last name First name M.I. Social Security no.
 Employee Enrollment Application For 2 50 Employee Small s Virginia care plans offered by Anthem Blue Cross and Blue Shield and Keepers, Inc. PPO health care plans are insurance products offered by Anthem
Employee Enrollment Application For 2 50 Employee Small s Virginia care plans offered by Anthem Blue Cross and Blue Shield and Keepers, Inc. PPO health care plans are insurance products offered by Anthem
Health Care Reform 101 for June 3, 2013
 Commercial & Personal Insurance Employee Benefits Retirement Plan Services Wealth Management Health Care Reform 101 for June 3, 2013 Requirements: Pre-HCR vs. Post-HCR Offering/Maintaining Health Insurance
Commercial & Personal Insurance Employee Benefits Retirement Plan Services Wealth Management Health Care Reform 101 for June 3, 2013 Requirements: Pre-HCR vs. Post-HCR Offering/Maintaining Health Insurance
New Jersey Small Employer Certification
 Oxford Health Insurance, Inc. New Jersey Small Employer Certification Mailing Address: NJ Small Group Enrollment Dept. 14 Central Park Drive Hookset, NH 03106 800-385-9088 For a Group Health Benefits Plan
Oxford Health Insurance, Inc. New Jersey Small Employer Certification Mailing Address: NJ Small Group Enrollment Dept. 14 Central Park Drive Hookset, NH 03106 800-385-9088 For a Group Health Benefits Plan
STATE OF OKLAHOMA. 1st Session of the 49th Legislature (2003) AS INTRODUCED
 AS INTRODUCED") STATE OF OKLAHOMA 1st Session of the 49th Legislature (2003) HOUSE BILL HB1152 By: Pettigrew AS INTRODUCED An Act relating to insurance; creating the Oklahoma Health Insurance Consumer Choice Act; defining
STATE OF OKLAHOMA 1st Session of the 49th Legislature (2003) HOUSE BILL HB1152 By: Pettigrew AS INTRODUCED An Act relating to insurance; creating the Oklahoma Health Insurance Consumer Choice Act; defining
HEALTH CARE REFORM: FREQUENTLY ASKED QUESTIONS (Group, Individual, Seasonal)
") Group Health Insurance Q & A HEALTH CARE REFORM: FREQUENTLY ASKED QUESTIONS (Group, Individual, Seasonal) 1. Will small employers continue to have 12 month rates as they exist today? a. Yes. Employer groups
Group Health Insurance Q & A HEALTH CARE REFORM: FREQUENTLY ASKED QUESTIONS (Group, Individual, Seasonal) 1. Will small employers continue to have 12 month rates as they exist today? a. Yes. Employer groups
Additional Information Provided by Aetna Life Insurance Company
 Additional Information Provided by Aetna Life Insurance Company Inquiry Procedure The plan of benefits described in the Booklet-Certificate is underwritten by: Aetna Life Insurance Company (Aetna) 151
Additional Information Provided by Aetna Life Insurance Company Inquiry Procedure The plan of benefits described in the Booklet-Certificate is underwritten by: Aetna Life Insurance Company (Aetna) 151
2015 Small group new business application
 2015 Small group new business application PLEASE COMPLETE AND RETURN ALL PAGES IN THIS APPLICATION OR PROCESSING COULD BE DELAYED. 1-50 eligible employees New group checklist Use this checklist to expedite
2015 Small group new business application PLEASE COMPLETE AND RETURN ALL PAGES IN THIS APPLICATION OR PROCESSING COULD BE DELAYED. 1-50 eligible employees New group checklist Use this checklist to expedite
Aetna Life Insurance Company Hartford, Connecticut 06156
 Aetna Life Insurance Company Hartford, Connecticut 06156 Extraterritorial Certificate Rider (GR-9N-CR1) Policyholder: The TLC Companies Group Policy No.: GP-811431 Rider: West Virginia ET Medical Issue
Aetna Life Insurance Company Hartford, Connecticut 06156 Extraterritorial Certificate Rider (GR-9N-CR1) Policyholder: The TLC Companies Group Policy No.: GP-811431 Rider: West Virginia ET Medical Issue
Affordable Care Act (ACA) Frequently Asked Questions
 Frequently Asked Questions") Grandfathered policies Q1: What is grandfathered health plan coverage? A: The interim final rule on grandfathering under ACA generally defines grandfathered health plan coverage as coverage provided by
Grandfathered policies Q1: What is grandfathered health plan coverage? A: The interim final rule on grandfathering under ACA generally defines grandfathered health plan coverage as coverage provided by
Small Group Checklist
 Small Group Checklist required documents Please use the checklist below for enrolling a small group with Health Republic Insurance The more complete and thorough you are with these documents, the more
Small Group Checklist required documents Please use the checklist below for enrolling a small group with Health Republic Insurance The more complete and thorough you are with these documents, the more
Deadline 11/30/2013 Medical Plan BC/BS PPO Plan 1 Dental Plan EBS Benefit Solutions
 Employee Name: Date of birth: 2014 Carrols Corporation Employee Benefits Open Enrollment Form Only Complete if you are changing or adding benefits Effective Date: EmpID/POS ID 01/01/2014 Complete Address:
Employee Name: Date of birth: 2014 Carrols Corporation Employee Benefits Open Enrollment Form Only Complete if you are changing or adding benefits Effective Date: EmpID/POS ID 01/01/2014 Complete Address:
Individual Health Plan Contract Change Form (For ACA plans)
") Individual Health Plan Contract Change Form (For ACA plans) Instructions: Use a ballpoint pen to complete the form and follow guidelines listed below: GUIDELINES Complete checked section if you are using
Individual Health Plan Contract Change Form (For ACA plans) Instructions: Use a ballpoint pen to complete the form and follow guidelines listed below: GUIDELINES Complete checked section if you are using
VOLUNTARY GROUP TERM LIFE INSURANCE:
 VOLUNTARY GROUP TERM LIFE INSURANCE: This plan offers you and your dependents an excellent opportunity to purchase affordable group term life insurance on a payroll deduction basis. The important plan
VOLUNTARY GROUP TERM LIFE INSURANCE: This plan offers you and your dependents an excellent opportunity to purchase affordable group term life insurance on a payroll deduction basis. The important plan
Please be aware that rates are subject to change based on final information and census.
 New Small Group Checklist Group : Effective Date: Please be aware that rates are subject to change based on final information and census. Completed Group Application & Eligibility Provisions Plan Selection(s)
New Small Group Checklist Group : Effective Date: Please be aware that rates are subject to change based on final information and census. Completed Group Application & Eligibility Provisions Plan Selection(s)
or my newly adopted/placed for adoption child(ren): placement date)
: placement date)") Washington Individual Enrollment Application Effective January 1, 2016 This application is for health care coverage purchased directly from Premera Blue Cross (Premera). For timely and proper processing,
Washington Individual Enrollment Application Effective January 1, 2016 This application is for health care coverage purchased directly from Premera Blue Cross (Premera). For timely and proper processing,
IC 27-8-15 Chapter 15. Small Employer Group Health Insurance
 IC 27-8-15 Chapter 15. Small Employer Group Health Insurance IC 27-8-15-0.1 Application of certain amendments to chapter Sec. 0.1. The following amendments to this chapter apply as follows: (1) The addition
IC 27-8-15 Chapter 15. Small Employer Group Health Insurance IC 27-8-15-0.1 Application of certain amendments to chapter Sec. 0.1. The following amendments to this chapter apply as follows: (1) The addition
CHANGES FOR GROUPS RENEWING INTO OXFORD NEW YORK AND NEW JERSEY SMALL GROUP PRODUCTS
 CHANGES FOR GROUPS RENEWING INTO OXFORD NEW YORK AND NEW JERSEY SMALL GROUP PRODUCTS Last year, we communicated planned changes to our online enrollment tool, IDEA Management System SM (IDEA) as part of
CHANGES FOR GROUPS RENEWING INTO OXFORD NEW YORK AND NEW JERSEY SMALL GROUP PRODUCTS Last year, we communicated planned changes to our online enrollment tool, IDEA Management System SM (IDEA) as part of
Chapter 91. Regulation 68 Patient Rights under Health Insurance Coverage in Louisiana
 D. A copy of the certification form shall be maintained by the insurer and by the producing agent or broker in the policyholder's record for a period of five years from the date of issuance of the insurance
D. A copy of the certification form shall be maintained by the insurer and by the producing agent or broker in the policyholder's record for a period of five years from the date of issuance of the insurance
Employer s guide to health care reform requirements
 Employer s guide to health care reform requirements June 2015 edition As the Affordable Care Act (ACA) continues to be implemented, you ll need to remain aware of the policies and provisions that affect
Employer s guide to health care reform requirements June 2015 edition As the Affordable Care Act (ACA) continues to be implemented, you ll need to remain aware of the policies and provisions that affect
Name change (Complete sections A, B, C ) Address (complete sections A, C)
 Address (complete sections A, C)") Please review entire form; print or type in black ink only. Retain pink copy for your records and use as a temporary ID after the effective date. Page 1 of 3 Southern Colorado Group Enrollment/Change Form
Please review entire form; print or type in black ink only. Retain pink copy for your records and use as a temporary ID after the effective date. Page 1 of 3 Southern Colorado Group Enrollment/Change Form
New Jersey Large Group Application
 New Jersey Large Group Application Oxford Health Insurance, Inc. Corporate Address: 48 Monroe Turnpike, Trumbull, CT 06611 800-444-6222 www.oxfordhealth.com I. G E N E R A L I N F O R M A T I O N 1. Full
New Jersey Large Group Application Oxford Health Insurance, Inc. Corporate Address: 48 Monroe Turnpike, Trumbull, CT 06611 800-444-6222 www.oxfordhealth.com I. G E N E R A L I N F O R M A T I O N 1. Full
Employer s Guide To Health Care Reform
 Employer s Guide To Health Care Reform A nonprofit independent licensee of the Blue Cross Blue Shield Association National strength. Local focus. Individual care. SM As part of our commitment to being
Employer s Guide To Health Care Reform A nonprofit independent licensee of the Blue Cross Blue Shield Association National strength. Local focus. Individual care. SM As part of our commitment to being
HMO $10 100% 1 HMO $25 100% 1 Classic $20 HMO 1 Classic $30 HMO 1 Classic $40 HMO 1 Saver $20 HMO 1 Saver $30 HMO 1 Saver $40 HMO 1
 Employee Addition/Change of Coverage Application 2 50 Existing Small Group For adding new/existing employees and eligible dependents to existing coverage. Health care plans offered by Anthem Blue Cross.
Employee Addition/Change of Coverage Application 2 50 Existing Small Group For adding new/existing employees and eligible dependents to existing coverage. Health care plans offered by Anthem Blue Cross.
California Small Group MC Aetna Life Insurance Company
 PLAN FEATURES Deductible (per calendar year) $3,000 Individual $6,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All covered expenses accumulate separately
PLAN FEATURES Deductible (per calendar year) $3,000 Individual $6,000 Family Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All covered expenses accumulate separately
New Business Transmittal Checklist
 New Business Transmittal Checklist 1. New Business Submission Form Form # CLIC NBSF (02/2012) 2. Employer Application (must be completed by agent with employer s original signature on the 2 nd page): a.
New Business Transmittal Checklist 1. New Business Submission Form Form # CLIC NBSF (02/2012) 2. Employer Application (must be completed by agent with employer s original signature on the 2 nd page): a.
Small Group Underwriting Guidelines 1
 Small Group Underwriting Guidelines 1 New York FOR BUSINESSES WITH 2-50 EMPLOYEES Small Group Underwriting Guidelines EmblemHealth s community-rated plans are available for purchase by qualified small
Small Group Underwriting Guidelines 1 New York FOR BUSINESSES WITH 2-50 EMPLOYEES Small Group Underwriting Guidelines EmblemHealth s community-rated plans are available for purchase by qualified small
Sandy Wood, CEBS (Certified Employee Benefit Specialist) Healthcare Consultant sandy@thebenefitsacademy.com 206-669-3345
 Healthcare Consultant sandy@thebenefitsacademy.com 206-669-3345") 1 Sandy Wood, CEBS (Certified Employee Benefit Specialist) Healthcare Consultant sandy@thebenefitsacademy.com 206-669-3345 2 Terms you need to know Required Notices 2014 Plan Requirements The Grandfathered
1 Sandy Wood, CEBS (Certified Employee Benefit Specialist) Healthcare Consultant sandy@thebenefitsacademy.com 206-669-3345 2 Terms you need to know Required Notices 2014 Plan Requirements The Grandfathered
Name change (Complete sections A, B, C ) Address (complete sections A, C)
 Address (complete sections A, C)") Please review entire form; print or type in black ink only. Retain pink copy for your records and use as a temporary ID after the effective date. Page 1 of 3 Denver/Boulder/Longmont EMPLOYEE LAST NAME
Please review entire form; print or type in black ink only. Retain pink copy for your records and use as a temporary ID after the effective date. Page 1 of 3 Denver/Boulder/Longmont EMPLOYEE LAST NAME
SMALL EMPLOYER GROUP APPLICATION
 SMALL EMPLOYER GROUP APPLICATION EmblemHealth insurance programs are underwritten by (GHI)Group Health Incorporated and (HIP) HIP Health Plan of New York. PRINT IN INK SECTION I: GROUP INFORMATION Company
SMALL EMPLOYER GROUP APPLICATION EmblemHealth insurance programs are underwritten by (GHI)Group Health Incorporated and (HIP) HIP Health Plan of New York. PRINT IN INK SECTION I: GROUP INFORMATION Company
Please complete in blue or black ink only. Section A: Employee Information Last name First name M.I. Social Security no.
 Employee Enrollment Application For 2 50 Employee Small s Virginia care plans offered by Anthem Blue Cross and Blue Shield and Keepers, Inc. PPO health care plans are insurance products offered by Anthem
Employee Enrollment Application For 2 50 Employee Small s Virginia care plans offered by Anthem Blue Cross and Blue Shield and Keepers, Inc. PPO health care plans are insurance products offered by Anthem
PLAN DESIGN AND BENEFITS - Tx OAMC 1500-10 PREFERRED CARE
 PLAN FEATURES Deductible (per calendar year) $1,500 Individual $3,000 Individual $4,500 Family $9,000 Family 3 Individuals per Family 3 Individuals per Family Unless otherwise indicated, the Deductible
PLAN FEATURES Deductible (per calendar year) $1,500 Individual $3,000 Individual $4,500 Family $9,000 Family 3 Individuals per Family 3 Individuals per Family Unless otherwise indicated, the Deductible
DVH PLUS with Coverage Schedule CSA58PP
 Medico Insurance Company Dental, Vision & Hearing Plan Form A58 DVH PLUS with Coverage Schedule CSA58PP Premium Rates by Mode Monthly Automatic Bank Withdrawal Quarterly Automatic Bank Withdrawal Issue
Medico Insurance Company Dental, Vision & Hearing Plan Form A58 DVH PLUS with Coverage Schedule CSA58PP Premium Rates by Mode Monthly Automatic Bank Withdrawal Quarterly Automatic Bank Withdrawal Issue
Please make a choice between agebanded and composite rates for your group. Age-Banded Composite
 Benefit Schedule for Employer Groups SIGNATURE SHEET Anniversary Group No.: AE: Benefit & Premium Modification Broker: This Agreement, consisting of the Benefit Schedule(s) and other related documents,
Benefit Schedule for Employer Groups SIGNATURE SHEET Anniversary Group No.: AE: Benefit & Premium Modification Broker: This Agreement, consisting of the Benefit Schedule(s) and other related documents,
TIPS. for Submitting New Regulated Small Groups (groups with 2 50 employees)
") TIPS for Submitting New Regulated Small Groups (groups with 2 50 employees) Blue Cross and Blue Shield of Texas (BCBSTX) is committed to providing excellent service. These tips should be helpful as you
TIPS for Submitting New Regulated Small Groups (groups with 2 50 employees) Blue Cross and Blue Shield of Texas (BCBSTX) is committed to providing excellent service. These tips should be helpful as you
California Small Group MC Aetna Life Insurance Company
 PLAN FEATURES Deductible (per calendar year) $1,000 per member $1,000 per member Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All covered expenses accumulate
PLAN FEATURES Deductible (per calendar year) $1,000 per member $1,000 per member Unless otherwise indicated, the Deductible must be met prior to benefits being payable. All covered expenses accumulate
Health Plans Coverage Summary
 www.hr.msu.edu/openenrollment Faculty & Staff Health Plans Coverage Summary PREVENTIVE SERVICES Health Maintenance Exam (1) Annual Gynecological Exam Pap Smear Screening (lab services only) Mammography
www.hr.msu.edu/openenrollment Faculty & Staff Health Plans Coverage Summary PREVENTIVE SERVICES Health Maintenance Exam (1) Annual Gynecological Exam Pap Smear Screening (lab services only) Mammography
Utah Renewal Instructions
 Utah Renewal Instructions For 2 50 Eligible Employees Effective August 1, 2009 Easy steps to renew your coverage 14.02.138.1-UT A (5/09) Aetna is the brand name used for products and services provided
Utah Renewal Instructions For 2 50 Eligible Employees Effective August 1, 2009 Easy steps to renew your coverage 14.02.138.1-UT A (5/09) Aetna is the brand name used for products and services provided
Companion Life Insurance Company. Administrative Guide
 Companion Life Insurance Company Administrative Guide Contents Section.Title About Your Companion Life Administrative Guide I. Online Services II. New Enrollments Who is Eligible for insurance? Processing
Companion Life Insurance Company Administrative Guide Contents Section.Title About Your Companion Life Administrative Guide I. Online Services II. New Enrollments Who is Eligible for insurance? Processing
Individual Health Plan Contract Change Form (For Grandfathered Plans and pre-aca Non-Grandfathered Plans)
") Individual Health Plan Contract Change Form (For Grandfathered Plans and pre-aca Non-Grandfathered Plans) GUIDELINES Instructions: Use a ballpoint pen to complete the form and follow guidelines listed
Individual Health Plan Contract Change Form (For Grandfathered Plans and pre-aca Non-Grandfathered Plans) GUIDELINES Instructions: Use a ballpoint pen to complete the form and follow guidelines listed
Employer Application for Small Business
 General Information Group s Legal Name Group Name to appear on ID card (maximum 30 characters) (DO NOT STAPLE) Employer Application for Small Business To avoid processing delays, please make sure you:
General Information Group s Legal Name Group Name to appear on ID card (maximum 30 characters) (DO NOT STAPLE) Employer Application for Small Business To avoid processing delays, please make sure you:
Reporting Requirements for Employers and Health Plans
 Brought to you by Cross Employee Benefits Reporting Requirements for Employers and Health Plans The Affordable Care Act (ACA) created a number of federal reporting requirements for employers and health
Brought to you by Cross Employee Benefits Reporting Requirements for Employers and Health Plans The Affordable Care Act (ACA) created a number of federal reporting requirements for employers and health
Application for Individual Health & Dental Insurance
 Application for Individual Health & Dental Insurance (For plans effective 1/1/2015 and after) PO Box 14527 Des Moines, Iowa 50306-3527 DIRECTIONS If you are applying for a new policy during Open Enrollment,
Application for Individual Health & Dental Insurance (For plans effective 1/1/2015 and after) PO Box 14527 Des Moines, Iowa 50306-3527 DIRECTIONS If you are applying for a new policy during Open Enrollment,
Employer Reporting of Health Coverage Code Sections 6055 & 6056
 Brought to you by Hickok & Boardman HR Intelligence Employer Reporting of Health Coverage Code Sections 6055 & 6056 The Affordable Care Act (ACA) created new reporting requirements under Internal Revenue
Brought to you by Hickok & Boardman HR Intelligence Employer Reporting of Health Coverage Code Sections 6055 & 6056 The Affordable Care Act (ACA) created new reporting requirements under Internal Revenue
How many Highly-Compensated employees have a dependent care need?
 Flexible Benefit Plan Pre-Qualifying Checklist & Quote Request For review and evaluation of your current benefit program complete the following information. We can then determine if the implementation
Flexible Benefit Plan Pre-Qualifying Checklist & Quote Request For review and evaluation of your current benefit program complete the following information. We can then determine if the implementation
Health Care Administrators
 Health Care Administrators January 21, 2005 Depend on HCA to be your resource for news and information. Page 1 of 2 1 Important Clarifications Related to Health Savings Accounts You ve asked for more information
Health Care Administrators January 21, 2005 Depend on HCA to be your resource for news and information. Page 1 of 2 1 Important Clarifications Related to Health Savings Accounts You ve asked for more information
UNDERWRITING GUIDELINES FOR PRODUCERS ID0224-0115. mynmhc.org
 UNDERWRITING GUIDELINES FOR PRODUCERS ID0224-0115 mynmhc.org Table of Contents Purpose and Overview I. Group and Employee Eligibility Requirements 1. Employer Eligibility 2. Ineligible Groups 3. Eligible
UNDERWRITING GUIDELINES FOR PRODUCERS ID0224-0115 mynmhc.org Table of Contents Purpose and Overview I. Group and Employee Eligibility Requirements 1. Employer Eligibility 2. Ineligible Groups 3. Eligible
NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY NATIONWIDE SPECIALTY INSURANCE CLAIM FORM
 NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY NATIONWIDE SPECIALTY INSURANCE CLAIM FORM THIS CLAIM CANNOT BE PROCESSED WITHOUT ALL OF THE BELOW INFORMATION AND STATEMENTS OF PAYMENTS FROM
NATIONWIDE LIFE INSURANCE COMPANY NATIONAL CASUALTY COMPANY NATIONWIDE SPECIALTY INSURANCE CLAIM FORM THIS CLAIM CANNOT BE PROCESSED WITHOUT ALL OF THE BELOW INFORMATION AND STATEMENTS OF PAYMENTS FROM
Health Care Reform 2015 Update
 Health Care Reform 2015 Update Presented to: Employee Health Benefits Committee Presented by: Pamela A. Boyer Information is current as of time of presentation: Oct. 15, 2015 1 Overview of Presentation
Health Care Reform 2015 Update Presented to: Employee Health Benefits Committee Presented by: Pamela A. Boyer Information is current as of time of presentation: Oct. 15, 2015 1 Overview of Presentation
PENNSYLVANIA Assurant Health Individual Medical Metallic Plans Enrollment Packet
 Client Tip Sheet PENNSYLVANIA Assurant Health Individual Medical Metallic Plans Enrollment Packet Thank you for applying for an Assurant Health Individual Medical Metallic plan. Please review the product
Client Tip Sheet PENNSYLVANIA Assurant Health Individual Medical Metallic Plans Enrollment Packet Thank you for applying for an Assurant Health Individual Medical Metallic plan. Please review the product
Accidental Dismemberment Insurance Claim Form
 State of Florida Account Participating Agencies and Departments Payroll Deduction Code 262 Mail To: Cigna P.O. Box 22328 Pittsburgh, PA 15222-0328 1-800-238-2125 Toll Free Claims administered by Cigna
State of Florida Account Participating Agencies and Departments Payroll Deduction Code 262 Mail To: Cigna P.O. Box 22328 Pittsburgh, PA 15222-0328 1-800-238-2125 Toll Free Claims administered by Cigna