Stadards in Abdominoperineal Resection
|
|
|
- Mitchell Harrington
- 10 years ago
- Views:
Transcription
1 Stadards in Abdominoperineal Resection Manuel Francisco T. Roxas, MD, FPCS, FPSCRS, FACS Clinical Associate Professor, University of the Philippines Chief, Section of Colorectal Surgery, Department of Health Jose R Reyes Memorial Medical Center Director, The Medical City Colorectal Clinic and Fellowship Program

2 DISCLOSURES Previous lecturer for Johnson and Johnson Covidien Nestle Novartis Sanofi Unilab


3 Objectives At the end of the session the participants should be able to describe: 1. Historical development of abdominoperineal resection to present standards 2. Technique of extralevator and ischioanal APR


4 Ernest Miles Advocated meticulous removal of Pelvic colon, mesocolon and lymph nodes Wide perineal dissection around anus 1937 Hugh Devine introduced lithotomy position through adjustable leg rests 1938 Lloyd Davis proposed synchronous A-P resection Clinics in Colorectal Surgery Vol 20 N0 3, 2007


5 Claude Dixon Indication for APR APR < 10 cm Easily palpable High grade malignancy, locally advanced Obese patient, small pelvis British Medical Journal May 4, 1968


6 Era of Total Mesorectal Excision Proposed Total Mesorectal Excision in 1982 Sphincter-preservation in majority (> 80%) Pelvic Nerve preservation Local recurrence rates of 3.7% Bill Heald Current Gold Standard for mid to low rectal cancers

7 Worse Outcomes after APR Anterior Resections APR p value 1. Nagtegaal, et al, Survival - Perforations - (+) CRM 57.6% 2.5% 10.7% 38.5% 13.7% 30.4% < Tekkis, et al, (+) CRM 7.5% 16.7% < (OR 3.3) 3. Tilney, et al, (+) CRM 6.7% 17.6% Youssef, et al, (+) CRM 5.0% 26.0% -
 3. Tilney, et al, 2007 - (+) CRM 6.7% 17.6% 0.001 4.")
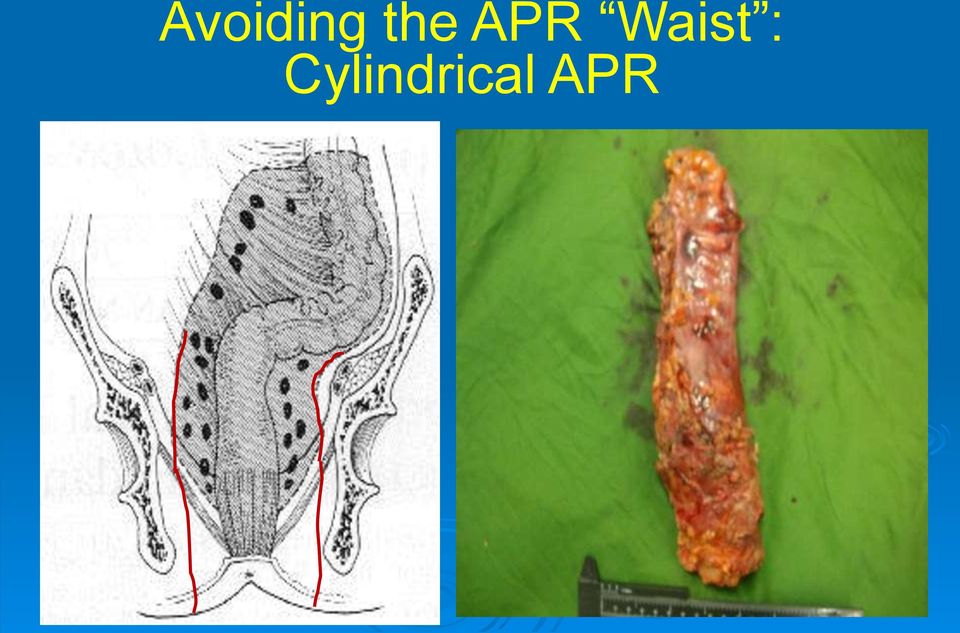
8 Salerno, et al. Sites of Surgical Wasting in the Abdominoperineal Specimen. Br J Surg, 2008 Sep; 95(9): Surgical waist usually between 3.5 and 4.2 cm FAV Smaller amounts of perirectal tissue resected at this level (P < 0.001) Corresponds to puborectalis

9 Surgical Waisting

10 Cylindrical Technique Removed more tissue Greater distance from sphincters circumferentially Lower CRM involvement and perforations

11 Avoiding the APR Waist : Cylindrical APR
12 West NP, Quirke P, Holm T. et al. Evidence of the Oncologic Superiority of Cylindrical Abdominoperineal Excision for Low Rectal Cancer. J Clin Oncol Jul 20; 26(21): Hypothesis: extended prone perineal dissection results in a more cylindrical specimen and should improve outcomes Retrospective pathologic analysis of 128 APR patients; potentially curable: Stockholm vs Leeds Cylindrical vs. standard technique (+) CRM 14.8% vs 40.6% (p<0.001) Intraop perforation 3.7% vs 22.8% (p=0.255)

13
14

15 Br J Surg Apr;97(4): doi: /bjs.6916.Multicentre experience with extralevator abdominoperineal excision for low rectal cancer 176 extralevator APE from 11 European colorectal surgeons vs 124 standard APR from 1 UK centre Extralevator APR significantly Removed more tissue Reduced CRM involvement Perforations Increased perineal wound complications

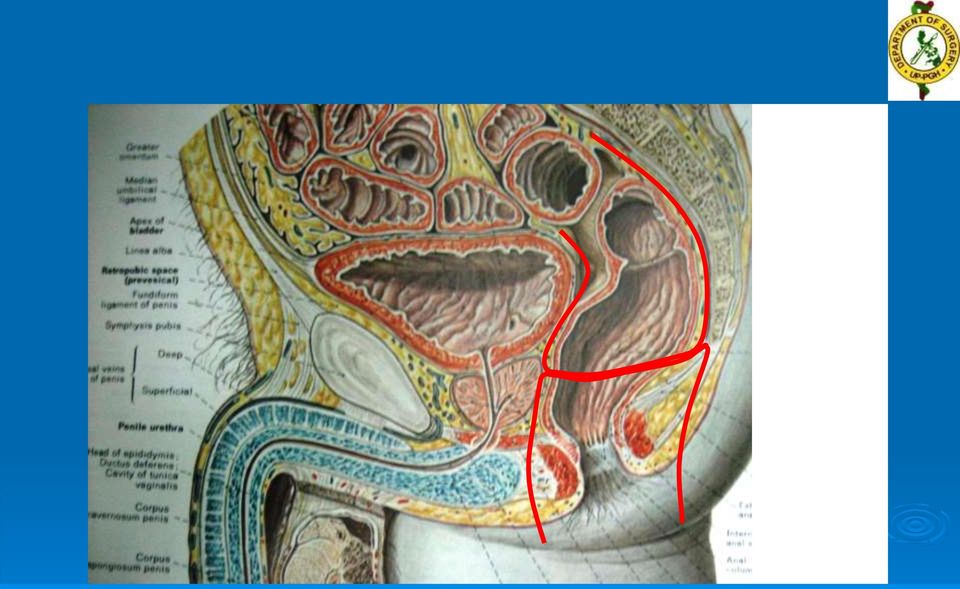
16 Manual of Total Mesorectal Excision, 2013 Torbjorn Holm Intersphincteric APR Extralevator APR Ischioanal APR

17 Short-term Outcome of ELAPE for Rectal Cancer. Stelzner S, et al. IJCD 2011 Jul; 26(7) Conventional APE n = 46 ELAPE n = 28 RRR p value Perforation 15.2% 0 p = (+) CRM 4.9% 0 p = Wound infecton 17.4% 10.7% p < 0.518
 CRM 4.")
18 Extended APE vs Standard APE in Rectal Cancer A Systematic Review. Stelzner et al. IJCD 2011 Oct; 26(10) Standard APE N = 4147 Extended APE N = 1097 RRR p value Perforation 10.4% 4.1 % RRR = 60.6% p = (+) CRM 15.4% 9.6% RRR = 37.7% p = Local recurrence 11.9% 6.6% RRR = 44.5% p < 0.001
 CRM 15.4% 9.")
19 RCT of Conventional Vs Cylindrical APR for Locally Advanced Lower Rectal Cancer. Han JG, et al. Am J Surg Sep (204(3) Perineal operating time Total operating time Perineal defect size Conventional APR n = 32 Cylindrical APR n = 35 p value 46 min 32 min p < min 190 min p = cm2 64 cm2 p < Blood loss 300 cc 200 cc p = Total X-sectional tissue area size X-sectional tissue outside IS/MP 1738 mm mm2 p < mm mm2 p < Perineal pain 1 vas 4 vas p < 0.01

20 RCT of Conventional Vs Cylindrical APR for Locally Advanced Lower Rectal Cancer. Han JG, et al. Am J Surg Sep (204(3) Over-all Survival Conventional APR n = 32 Disease-free Survival Cylindrical APRn = 35 p value (+) CRM 9 2 p = 0.13 Perforation 5 2 p = Local recurrence 4 1 p = 0.48
 CRM 9 2 p = 0.")
21 Results of extralevator APR for low rectal ca including quality of life and long term wound complications. Welsch T, et al. Int J Colorectal Dis 2013 pr; 28(4) Retrospective review; 30 pts (+) CRM in 2 cases (^>&%) No bowel perforation No local recurrence after 28.3 months Perineal wound complications in 46.6%; managed conservatively Persistent perineal pain in 50% Quality of life levels are maintained, though genitourinary functions are impaired
22
23 Factors associated with oncologic outcomes after APR compared with restorative resection for low rectal ca: patient- and tumor-related or technical factors only?.. Reshef A, et al. DCR 2012 Jan; 55(1) Retrospective review APR = 413; Restorative resection = 993 APR pts : older, higher ASA; worse tumor differentiation; higher stage (p<0.001) Local recurrence: APR 7% vs RR 3% (p=0.02) Overall survival: APR 56% vs.rr 71% (p<0.001) DFS: APR 54% VS RR 70% (p<0.001)
24 Factors associated with oncologic outcomes after APR compared with restorative resection for low rectal ca: patient- and tumor-related or technical factors only?.. Reshef A, et al. DCR 2012 Jan; 55(1) Conclusions: Technical factors alone are unlikely to be responsible for the worse outcomes after abdominoperineal resection A combination of patient- and tumor-related factors that may have indicated the choice of the procedure also probably contribute to the worse outcomes.
25 Focus on extralevator perineal dissection in supine position (sppd) for low rectal ca has led to better quality of surgery and oncologic outcome. Martijnse IS, et al. Ann Surg Onco 2012 Mar; 19(3) 246 pts; (112 traditional vs.134 sppd; 101 of which were perineal first) (+) CRM overall = 10% R1 specimen before and after sppd: ct0-3: 6.8% down to 2.2% ct4: 30.2% down to 5.7% (p=0.001) Decreased local recurrence: ct4: 25% down to 2.4%; ypt4: 34% down to 5.6% Over-all survival improvement: 83% up to 92%
26 Focus on extralevator perineal dissection in supine position (sppd) for low rectal ca has led to better quality of surgery and oncologic outcome. Martijnse IS, et al. Ann Surg Onco 2012 Mar; 19(3) Conclusions: Focus on perineal dissection improves quality of surgery and oncologic outcomes Not all pts require more radical resection
27 Anterior-entry APR: a variation in the method of perineal dissection.. Simunovic M et al. Ann Surg Onco 2012 Mar; 19(3) 10 cases Quality of surgical specimens was high 1 (+) CRM 1 perforation Conclusion: Anterior entry is feasible and may minimize rates of (+) radial margins
28 Outcome of extralevator APE compared with standard surgery: results from a single centre. Asplund D, et al. Colorectal Dis 2012 Oct; 14(10) Standard APE N = 79 Extralevator APE n = 79 p value (+) CRM 20% 17% No difference Perforation 10% 13% No difference Local recurrence 8.9% 8.9% No difference Perineal wound infection Perineal wound revision 28% 46% p < % 22% p< 0.05 Hospital stay 11 days 12 days p < 0.05
29 A comparison of published rates of resection margin involvement and intra-operative perforation between standard and cylindrical APE for low rectal cancer. Krishna A,,, et al. Colorectal Dis Jan: 15(1) Review of 6 independent hospital and population based patient series no evidence that extralevator APE significantly lowered CRM and perforation compared with standard APE Conclusion: Need for RCT
30 Multicentre study of CRM positivity and outcomes following APE for rectal ca. Kennelly RP, et al. Br J Surg Jan; 100(1) 5 hospital databases; 302 pts Neoadjuvant CRT in 50% T3 T 4 = 62.9% (+) N = 42.1% (+) CRM = 13.9 % Multivariate analysis: Risk factors for (+) CRM pt4 (OR =19.92, 95% CI ) (+) N (OR = 3.04; 95% CI ) (+) CRM was a risk factor for local recurrene ( p = 0.022) and decreased survival (p = 0.001)
31 Multicentre study of CRM positivity and outcomes following APE for rectal ca. Kennelly RP,, et al. Br J Surg Jan; 100(1) Conclusion: (+) CRM was dictated by tumor stage, not by center or surgeon. Wide extralevator APE is probably required only for very advanced tumors
32 A 12-year experience of the Trendelenberg perineal approach for APR. Toshniwal S, et al. ANZ J Surg Apr 17 Retrospective review 53 pts; 87% received neoadjuvant therapy 11% morbidity Local recurrence = 4% at 5 years 5 year survival = 66% Conclusion: APR in lithotomy position can be done with acceptable perineal morbidity and oncologic safety, achieving (-) CRM in a cylindrical specimen
33 Analysis of outcome using a levator sparing technique of APE of rectum and anus. Cylindrical ELAPE is not necessary in all patients. Ramsay G., et al. Eur J Surg Oncol Nov; 39 (11) Retrospective review from APE in 43 out of 361 rectal cancers Neoadjuvant CRT in 98% 38 month follow up: 4.6% local recurrence 18.6% mortality Conclusion: With neoadjuvant CRT, levator sparing excision of the rectum is safe, with less morbidity and perioperative complications
34 Is the jury out?
35 Laparoscopic APR Study Method Patients Results 1. Ng et al 2009 RCT 99 (51 lap) Earlier BM and ambulation Less analgesia 2. Iroatulum, et al 1998 Case control 15 (8 lap) Shorter hospital stay by 50% 3. Araulo et al 2003 RCT 28 (13 lap) Shorter OR and anesthesia time 4. Fleshman et al Wong et al 2006 Retros review Prospective cohort 194 (42 lap) Shorter hospital stay Higher rate of perineal infections 102 (71 lap) Less bloos loss and BT Less abdominal wound and chest infections Better survival
36 Laparoscopic APR Similar outcomes compared to open Specimen retrieval Nodes Margins Cancer Outcomes Local recurrence Survival But did not mention extralevator or cylindrical
37 Laparoscopic extralevator APE of the rectum: shortterm outcomes of a prospective case series. Kiplinf AL., et al. Tech Coloproctol 2013 Oct (EPUB) 28 pts Conversion rate 18% (+) CRM in 3 (10.8%) No perforations Mean length of stay = 7 days Perinal wound complications in 25% 38 month follow up Local recurrence of 11% Overall survival = 75% Disease-free survival = 71%
 Robotic Marecik, SJ, et al. DCR. 2011 Oct; 54 (10) Kang Cy, et al. Am Surg.")
38 Transabdominal Levator Transection Laparoscopic Chi Pi, et al. Ann Surg Oncol May: 20 (5) Robotic Marecik, SJ, et al. DCR Oct; 54 (10) Kang Cy, et al. Am Surg Oct; 78 (10)
39 DIVISION OF COLORECTAL SURGERY UP PHILIPPINE GENERAL HOSPITAL Initiated MDT, TME and Extralevator APR in APR pts APR rate = 27.8% Mean distance = 1.5 cm Pre-op RT = 67.5% Long course CRT = 50.4% Short course RT = 17.1%
40 DIVISION OF COLORECTAL SURGERY UP PHILIPPINE GENERAL HOSPITAL Operations done: Residents 64.1% vs Consultants 35.9% Open 72.7% vs Lap 27.4% Lithotomy 54.7% vs prone 45.3% Multivisceral resections = 29.1% THBSO, posterior vaginectomy, pprostatectomy Stage II or III = 64.1% Pathologic complete response = 6.8%
41 DIVISION OF COLORECTAL SURGERY UP PHILIPPINE GENERAL HOSPITAL Results: waisting = 36.11% Perforations = 15.4% (+) CRM = 16.5% Significant factors associated with (+) CRM Males (OR 5.26; 95% CI ) Radiotherapy (OR = 7.87; 95% CI )
42 DIVISION OF COLORECTAL SURGERY UP PHILIPPINE GENERAL HOSPITAL Results: Factors with trends towards lower adverse pathologic outcomes (waisting, perforations and CRM positivity), though not statistically significant: Prone (vs lithotomy) Lap (vs. open) Consultant (vs. resident) Long course CRT (vs Short course RT)

43 CONCLUSION Achieve better pathologic and oncologic outcomes with APR through: focused perineal phase Irrespective of: perineal phase position or abdominal phase procedure Aiming for a cylindrical or lollipop shaped specimen with negative margins and perforations more experienced surgeons after long course chemoradiotherapy if warranted
44 THANK YOU
Neoadjuvant therapy are we doing it right? Short course and chemoradiation
 Neoadjuvant therapy are we doing it right? Short course and chemoradiation Rob Glynne-Jones Mount Vernon Cancer Centre Relevant Endpoints in rectal cancer Local recurrence Disease-free survival Overall
Neoadjuvant therapy are we doing it right? Short course and chemoradiation Rob Glynne-Jones Mount Vernon Cancer Centre Relevant Endpoints in rectal cancer Local recurrence Disease-free survival Overall
Bridging Techniques. What s between EMR and Traditional Surgery? Elisabeth C. McLemore, MD, FACS, FASCRS
 Bridging Techniques What s between EMR and Traditional Surgery? Elisabeth C. McLemore, MD, FACS, FASCRS Associate Professor of Surgery Assistant Program Director, General Surgery Residency Disclosures
Bridging Techniques What s between EMR and Traditional Surgery? Elisabeth C. McLemore, MD, FACS, FASCRS Associate Professor of Surgery Assistant Program Director, General Surgery Residency Disclosures
National Bowel Cancer Audit Report 2008 Public and Executive Summary
 National Bowel Cancer Audit Report 2008 Public and Executive Summary Prepared in association with: Healthcare Quality Improvement Partnership HQIP Association of Coloproctology of Great Britain and Ireland
National Bowel Cancer Audit Report 2008 Public and Executive Summary Prepared in association with: Healthcare Quality Improvement Partnership HQIP Association of Coloproctology of Great Britain and Ireland
Approccio multidisciplinare nei tumori del retto
 Approccio multidisciplinare nei tumori del retto F. Muñoz Radiation Oncology Department University of Torino, Italy RECENT CHANGES IN RECTAL CANCER DIAGNOSIS AND THERAPY Optimal staging by EUS and MRI
Approccio multidisciplinare nei tumori del retto F. Muñoz Radiation Oncology Department University of Torino, Italy RECENT CHANGES IN RECTAL CANCER DIAGNOSIS AND THERAPY Optimal staging by EUS and MRI
Principles of Radiation Therapy A Bapsi Chakravarthy, MD Associate e P rofessor Professor Radiation Oncology
 Principles of Radiation Therapy A Bapsi Chakravarthy, MD Associate Professor Radiation Oncology Disclosure Information I have no financial relationships to disclose relevant to the conten of this presentation.
Principles of Radiation Therapy A Bapsi Chakravarthy, MD Associate Professor Radiation Oncology Disclosure Information I have no financial relationships to disclose relevant to the conten of this presentation.
GENERAL SUMMARY AND DISCUSSION
 GENERAL SUMMARY AND DISCUSSION In the last 30 years, abdominal surgery has progressed from the standard open approach to less invasive techniques such as laparoscopy and natural orifice translumenal endoscopic
GENERAL SUMMARY AND DISCUSSION In the last 30 years, abdominal surgery has progressed from the standard open approach to less invasive techniques such as laparoscopy and natural orifice translumenal endoscopic
Facing Prostate Cancer Surgery? Learn about minimally invasive da Vinci Surgery
 Facing Prostate Cancer Surgery? Learn about minimally invasive da Vinci Surgery The Condition: Prostate Cancer Your prostate is a walnut-sized gland that is part of the male reproductive system. The prostate
Facing Prostate Cancer Surgery? Learn about minimally invasive da Vinci Surgery The Condition: Prostate Cancer Your prostate is a walnut-sized gland that is part of the male reproductive system. The prostate
Chapter 5. Eur J Cancer 2009; 45: 1175-1183
 Chapter 5 The abdominoperineal resection itself is associated with an adverse outcome: the European experience based on a pooled analysis of five European randomised clinical trials on rectal cancer Marcel
Chapter 5 The abdominoperineal resection itself is associated with an adverse outcome: the European experience based on a pooled analysis of five European randomised clinical trials on rectal cancer Marcel
Facing a Hysterectomy? If you ve been diagnosed with early stage gynecologic cancer, learn about minimally invasive da Vinci Surgery
 Facing a Hysterectomy? If you ve been diagnosed with early stage gynecologic cancer, learn about minimally invasive da Vinci Surgery The Condition: Early Stage Gynecologic Cancer A variety of gynecologic
Facing a Hysterectomy? If you ve been diagnosed with early stage gynecologic cancer, learn about minimally invasive da Vinci Surgery The Condition: Early Stage Gynecologic Cancer A variety of gynecologic
MRI in Rectal Cancer. Kartik S Jhaveri, MD,FRCPC Director, Abdominal MRI Director, CME Program
 MRI in Rectal Cancer Kartik S Jhaveri, MD,FRCPC Director, Abdominal MRI Director, CME Program DISCLOSURES No Relevant Disclosures 2 OBJECTIVES Imaging of Rectal Cancer Why MRI? MR Protocol MR Anatomy Preoperative
MRI in Rectal Cancer Kartik S Jhaveri, MD,FRCPC Director, Abdominal MRI Director, CME Program DISCLOSURES No Relevant Disclosures 2 OBJECTIVES Imaging of Rectal Cancer Why MRI? MR Protocol MR Anatomy Preoperative
Laparoscopic Repair of Incisional Hernia. Maria B. ALBUJA-CRUZ, MD University of Colorado Department of Surgery-Grand Rounds
 Laparoscopic Repair of Incisional Hernia Maria B. ALBUJA-CRUZ, MD University of Colorado Department of Surgery-Grand Rounds Overview Definition Advantages of Laparoscopic Repair Disadvantages of Open Repair
Laparoscopic Repair of Incisional Hernia Maria B. ALBUJA-CRUZ, MD University of Colorado Department of Surgery-Grand Rounds Overview Definition Advantages of Laparoscopic Repair Disadvantages of Open Repair
Rectal Cancer. To Radiate or not to radiate? Q: Should rectal cancer RT/CRT decisions be based solely on stage? 11/09/2014
 Rectal Cancer To Radiate or not to radiate?? Dr. Corinne Doll Radiation Oncologist Tom Baker Cancer Centre Calgary, Alberta Q: Should rectal cancer RT/CRT decisions be based solely on stage? 1 Q: Can RT/CRT
Rectal Cancer To Radiate or not to radiate?? Dr. Corinne Doll Radiation Oncologist Tom Baker Cancer Centre Calgary, Alberta Q: Should rectal cancer RT/CRT decisions be based solely on stage? 1 Q: Can RT/CRT
How To Teach A Patient To Live With A Tumour
 RECTAL CANCER WHEN TO OPERATE Operative Treatment Strategies... From Minimal to Maximal Champalimaud Foundation Lisbon, Portugal 7 th - 8 th November 2014 Organisation - Champalimaud Foundation Amjad Parvaiz
RECTAL CANCER WHEN TO OPERATE Operative Treatment Strategies... From Minimal to Maximal Champalimaud Foundation Lisbon, Portugal 7 th - 8 th November 2014 Organisation - Champalimaud Foundation Amjad Parvaiz
Clinical Practice Assessment Robotic surgery
 Clinical Practice Assessment Robotic surgery Background: Surgery is by nature invasive. Efforts have been made over time to reduce complications and the trauma inherently associated with surgery through
Clinical Practice Assessment Robotic surgery Background: Surgery is by nature invasive. Efforts have been made over time to reduce complications and the trauma inherently associated with surgery through
Thomas A. Kollmorgen, M.D. Oregon Urology Institute
 Thomas A. Kollmorgen, M.D. Oregon Urology Institute None 240,000 new diagnosis per year, and an estimated 28,100 deaths (2012) 2 nd leading cause of death from cancer in U.S.A. Approximately 1 in 6 men
Thomas A. Kollmorgen, M.D. Oregon Urology Institute None 240,000 new diagnosis per year, and an estimated 28,100 deaths (2012) 2 nd leading cause of death from cancer in U.S.A. Approximately 1 in 6 men
How to treat early gastric cancer. Surgery
 How to treat early gastric cancer Surgery Mark I. van Berge Henegouwen Department of Surgery, AMC, Amsterdam Director upper GI surgical unit Academic Medical Center Upper GI surgery at AMC 100 oesophagectomies
How to treat early gastric cancer Surgery Mark I. van Berge Henegouwen Department of Surgery, AMC, Amsterdam Director upper GI surgical unit Academic Medical Center Upper GI surgery at AMC 100 oesophagectomies
Stomach (Gastric) Cancer. Prof. M K Mahajan ACDT & RC Bathinda
 Cancer. Prof. M K Mahajan ACDT & RC Bathinda") Stomach (Gastric) Cancer Prof. M K Mahajan ACDT & RC Bathinda Gastric Cancer Role of Radiation Layers of the Stomach Mucosa Submucosa Muscularis Serosa Stomach and Regional Lymph Nodes Stomach and Regional
Stomach (Gastric) Cancer Prof. M K Mahajan ACDT & RC Bathinda Gastric Cancer Role of Radiation Layers of the Stomach Mucosa Submucosa Muscularis Serosa Stomach and Regional Lymph Nodes Stomach and Regional
Bowel Preparation for Colon Resection. Eric Klein, M.D. SUNY Downstate Department of Surgery
 Bowel Preparation for Colon Resection Eric Klein, M.D. SUNY Downstate Department of Surgery Historical Perspective During World War II, failure to treat penetrating colon injuries with diversion could
Bowel Preparation for Colon Resection Eric Klein, M.D. SUNY Downstate Department of Surgery Historical Perspective During World War II, failure to treat penetrating colon injuries with diversion could
7. Prostate cancer in PSA relapse
 7. Prostate cancer in PSA relapse A patient with prostate cancer in PSA relapse is one who, having received a primary treatment with intent to cure, has a raised PSA (prostate-specific antigen) level defined
7. Prostate cancer in PSA relapse A patient with prostate cancer in PSA relapse is one who, having received a primary treatment with intent to cure, has a raised PSA (prostate-specific antigen) level defined
The Whipple Operation for Pancreatic Cancer: Optimism vs. Reality. Franklin Wright UCHSC Department of Surgery Grand Rounds September 11, 2006
 The Whipple Operation for Pancreatic Cancer: Optimism vs. Reality Franklin Wright UCHSC Department of Surgery Grand Rounds September 11, 2006 Overview Pancreatic ductal adenocarcinoma Pancreaticoduodenectomy
The Whipple Operation for Pancreatic Cancer: Optimism vs. Reality Franklin Wright UCHSC Department of Surgery Grand Rounds September 11, 2006 Overview Pancreatic ductal adenocarcinoma Pancreaticoduodenectomy
Cancer of the Cardia/GE Junction: Surgical Options
 Cancer of the Cardia/GE Junction: Surgical Options Michael A Smith, MD Associate Chief Thoracic Surgery Center for Thoracic Disease St Joseph s Hospital and Medical Center Phoenix, AZ Michael Smith, MD
Cancer of the Cardia/GE Junction: Surgical Options Michael A Smith, MD Associate Chief Thoracic Surgery Center for Thoracic Disease St Joseph s Hospital and Medical Center Phoenix, AZ Michael Smith, MD
What Is the Role for the Circumferential Margin in the Modern Treatment of Rectal Cancer? Iris D. Nagtegaal and Phil Quirke
 VOLUME 26 NUMBER 2 JANUARY 10 2008 JOURNAL OF CLINICAL ONCOLOGY R E V I E W A R T I C L E What Is the Role for the Circumferential Margin in the Modern Treatment of Rectal Cancer? Iris D. Nagtegaal and
VOLUME 26 NUMBER 2 JANUARY 10 2008 JOURNAL OF CLINICAL ONCOLOGY R E V I E W A R T I C L E What Is the Role for the Circumferential Margin in the Modern Treatment of Rectal Cancer? Iris D. Nagtegaal and
Role of Robotic Surgery in Obese Women with Endometrial Cancer
 Role of Robotic Surgery in Obese Women with Endometrial Cancer Anil Tailor Consultant Gynaecological Oncologist Royal Surrey County Hospital Guildford, Surrey, UK St Peters Hospital Chertsey, Surrey, UK
Role of Robotic Surgery in Obese Women with Endometrial Cancer Anil Tailor Consultant Gynaecological Oncologist Royal Surrey County Hospital Guildford, Surrey, UK St Peters Hospital Chertsey, Surrey, UK
Management of Postmenopausal Women with T1 ER+ Tumors: Options and Tradeoffs. Case Study. Surgery. Lumpectomy and Radiation
 Management of Postmenopausal Women with T1 ER+ Tumors: Options and Tradeoffs Michael Alvarado, MD Associate Professor of Surgery University of California San Francisco Case Study 59 yo woman with new palpable
Management of Postmenopausal Women with T1 ER+ Tumors: Options and Tradeoffs Michael Alvarado, MD Associate Professor of Surgery University of California San Francisco Case Study 59 yo woman with new palpable
The evolution of rectal cancer therapy. Objectives
 The evolution of rectal cancer therapy Hagen Kennecke MD MHA FRCPC Western Canada Consensus Conference September 5, 2014 Objectives Identify standard therapy: stage II/III rectal cancer Update recent adjuvant
The evolution of rectal cancer therapy Hagen Kennecke MD MHA FRCPC Western Canada Consensus Conference September 5, 2014 Objectives Identify standard therapy: stage II/III rectal cancer Update recent adjuvant
RESEARCH ARTICLE. Abstract. Introduction. Materials and Methods
 DOI:http://dx.doi.org/10.7314/APJCP.2015.16.13.5483 Perioperative and Oncologic Outcomes with Laparotomy, and Laparoscopic, and Robotic Surgery for Endometrial Cancer RESEARCH ARTICLE Comparison of Perioperative
DOI:http://dx.doi.org/10.7314/APJCP.2015.16.13.5483 Perioperative and Oncologic Outcomes with Laparotomy, and Laparoscopic, and Robotic Surgery for Endometrial Cancer RESEARCH ARTICLE Comparison of Perioperative
How To Compare The Effects Of A Hysterectomy And A Hysterectomy
 A RANDOMIZED TRIAL COMPARING RADICAL HYSTERECTOMY AND PELVIC NODE DISSECTION VS SIMPLE HYSTERECTOMY AND PELVIC NODE DISSECTION IN PATIENTS WITH LOW RISK EARLY STAGE CERVICAL CANCER A Gynecologic Cancer
A RANDOMIZED TRIAL COMPARING RADICAL HYSTERECTOMY AND PELVIC NODE DISSECTION VS SIMPLE HYSTERECTOMY AND PELVIC NODE DISSECTION IN PATIENTS WITH LOW RISK EARLY STAGE CERVICAL CANCER A Gynecologic Cancer
Adiuwantowe i neoadiuwantowe leczenie chorych na zaawansowanego raka żołądka
 Adiuwantowe i neoadiuwantowe leczenie chorych na zaawansowanego raka żołądka Neoadiuvant and adiuvant therapy for advanced gastric cancer Franco Roviello, IT Neoadjuvant and adjuvant therapy for advanced
Adiuwantowe i neoadiuwantowe leczenie chorych na zaawansowanego raka żołądka Neoadiuvant and adiuvant therapy for advanced gastric cancer Franco Roviello, IT Neoadjuvant and adjuvant therapy for advanced
Re irradiation Using HDR Interstitial Brachytherapy for Locally Recurrent. Disclosure
 Re irradiation Using HDR Interstitial Brachytherapy for Locally Recurrent Cervical lcancer Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan
Re irradiation Using HDR Interstitial Brachytherapy for Locally Recurrent Cervical lcancer Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan
Facing Pancreatic Surgery? Learn about minimally invasive da Vinci Surgery
 Facing Pancreatic Surgery? Learn about minimally invasive da Vinci Surgery The Condition: Pancreatitis/Pancreatic Cancer The pancreas is an organ that produces enzymes and hormones to help your body digest
Facing Pancreatic Surgery? Learn about minimally invasive da Vinci Surgery The Condition: Pancreatitis/Pancreatic Cancer The pancreas is an organ that produces enzymes and hormones to help your body digest
Malignant pleural mesothelioma P/D vs. EPP
 3 rd International Thoracic Oncology Congress Dresden, September 13 15, 2012 Malignant pleural mesothelioma P/D vs. EPP Walter Weder, MD Professor of Surgery Dokumentenname Datum Seite 1 Extrapleural Pneumonectomy
3 rd International Thoracic Oncology Congress Dresden, September 13 15, 2012 Malignant pleural mesothelioma P/D vs. EPP Walter Weder, MD Professor of Surgery Dokumentenname Datum Seite 1 Extrapleural Pneumonectomy
Management of Peritoneal Metastases (PM) from colorectal cancers: New Perspectives. Dominique ELIAS
 from colorectal cancers: New Perspectives. Dominique ELIAS") Management of Peritoneal Metastases (PM) from colorectal cancers: New Perspectives Dominique ELIAS Declaration of interest BOARDS Congress and teaching 0 Merck 0 Ipsen Novartis Sanofi Trials The peritoneum
Management of Peritoneal Metastases (PM) from colorectal cancers: New Perspectives Dominique ELIAS Declaration of interest BOARDS Congress and teaching 0 Merck 0 Ipsen Novartis Sanofi Trials The peritoneum
Loco-regional Recurrence
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer AGO AGO e. e. V. V. Loco-regional Recurrence Loco-regional Recurrence Version 2002: Brunnert / Simon Versions 2003 2012: Audretsch
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer AGO AGO e. e. V. V. Loco-regional Recurrence Loco-regional Recurrence Version 2002: Brunnert / Simon Versions 2003 2012: Audretsch
The main surgical options for treating early stage cervical cancer are:
 INFORMATION LEAFLET ON TOTAL LAPAROSCOPIC RADICAL HYSTERECTOMY (TLRH) FOR EARLY STAGE CERVICAL CANCER (TREATING EARLY STAGE CERVICAL CANCER BY RADICAL HYSTERECTOMY THROUGH KEYHOLE SURGERY) Aim of the leaflet
INFORMATION LEAFLET ON TOTAL LAPAROSCOPIC RADICAL HYSTERECTOMY (TLRH) FOR EARLY STAGE CERVICAL CANCER (TREATING EARLY STAGE CERVICAL CANCER BY RADICAL HYSTERECTOMY THROUGH KEYHOLE SURGERY) Aim of the leaflet
Fourth versus eighth week surgery after neoadjuvant radiochemotherapy in T3-4/N0+ rectal cancer: Istanbul R-01 study
 Original Article Fourth versus eighth week surgery after neoadjuvant radiochemotherapy in T3-4/N0+ rectal cancer: Istanbul R-01 study Sezer Saglam 1, Dursun Bugra 2, Esra K. Saglam 3, Oktar Asoglu 4, Emre
Original Article Fourth versus eighth week surgery after neoadjuvant radiochemotherapy in T3-4/N0+ rectal cancer: Istanbul R-01 study Sezer Saglam 1, Dursun Bugra 2, Esra K. Saglam 3, Oktar Asoglu 4, Emre
These rare variants often act aggressively and may respond differently to therapy than the more common prostate adenocarcinoma.
 Prostate Cancer OVERVIEW Prostate cancer is the second most common cancer diagnosed among American men, accounting for nearly 200,000 new cancer cases in the United States each year. Greater than 65% of
Prostate Cancer OVERVIEW Prostate cancer is the second most common cancer diagnosed among American men, accounting for nearly 200,000 new cancer cases in the United States each year. Greater than 65% of
Frequently Asked Questions About Ovarian Cancer
 Media Contact: Gerri Gomez Howard Cell: 303-748-3933 [email protected] Frequently Asked Questions About Ovarian Cancer What is ovarian cancer? Ovarian cancer is a cancer that forms in tissues
Media Contact: Gerri Gomez Howard Cell: 303-748-3933 [email protected] Frequently Asked Questions About Ovarian Cancer What is ovarian cancer? Ovarian cancer is a cancer that forms in tissues
PANCREATIC AND PERIAMPULLARY TUMORS: PANCREATICODUODENECTOMY. Dr. Shailesh V. Shrikhande
 PANCREATIC AND PERIAMPULLARY TUMORS: PANCREATICODUODENECTOMY Dr. Shailesh V. Shrikhande Associate Professor & Consultant Surgeon GI and HPB Surgical Oncology Tata Memorial Hospital, Mumbai INDIA HELICAL
PANCREATIC AND PERIAMPULLARY TUMORS: PANCREATICODUODENECTOMY Dr. Shailesh V. Shrikhande Associate Professor & Consultant Surgeon GI and HPB Surgical Oncology Tata Memorial Hospital, Mumbai INDIA HELICAL
ESD for colorectal lesions I am in favour. Alessandro Repici, MD Digestive Endoscopy Unit IRCCS Istituto Clinico Humanitas Milano, Italy
 ESD for colorectal lesions I am in favour Alessandro Repici, MD Digestive Endoscopy Unit IRCCS Istituto Clinico Humanitas Milano, Italy Surgery for early colonic lesions 51 pts referred for lap colectomy
ESD for colorectal lesions I am in favour Alessandro Repici, MD Digestive Endoscopy Unit IRCCS Istituto Clinico Humanitas Milano, Italy Surgery for early colonic lesions 51 pts referred for lap colectomy
Rotation Specific Goals & Objectives: University Health Network-Princess Margaret Hospital/ Sunnybrook Breast/Melanoma
 Rotation Specific Goals & Objectives: University Health Network-Princess Margaret Hospital/ Sunnybrook Breast/Melanoma Medical Expert: Breast Rotation Specific Competencies/Objectives 1.0 Medical History
Rotation Specific Goals & Objectives: University Health Network-Princess Margaret Hospital/ Sunnybrook Breast/Melanoma Medical Expert: Breast Rotation Specific Competencies/Objectives 1.0 Medical History
Surgery for rectal cancer
 This information is an extract from the booklet Understanding rectal cancer. You may find the full booklet helpful. We can send you a free copy see page 12. Contents Enhanced recovery programme (ERP) Before
This information is an extract from the booklet Understanding rectal cancer. You may find the full booklet helpful. We can send you a free copy see page 12. Contents Enhanced recovery programme (ERP) Before
Targeted Therapy What the Surgeon Needs to Know
 Targeted Therapy What the Surgeon Needs to Know AATS Focus in Thoracic Surgery 2014 David R. Jones, M.D. Professor & Chief, Thoracic Surgery Memorial Sloan Kettering Cancer Center I have no disclosures
Targeted Therapy What the Surgeon Needs to Know AATS Focus in Thoracic Surgery 2014 David R. Jones, M.D. Professor & Chief, Thoracic Surgery Memorial Sloan Kettering Cancer Center I have no disclosures
Current Status and Perspectives of Radiation Therapy for Breast Cancer
 Breast Cancer Current Status and Perspectives of Radiation Therapy for Breast Cancer JMAJ 45(10): 434 439, 2002 Masahiro HIRAOKA, Masaki KOKUBO, Chikako YAMAMOTO and Michihide MITSUMORI Department of Therapeutic
Breast Cancer Current Status and Perspectives of Radiation Therapy for Breast Cancer JMAJ 45(10): 434 439, 2002 Masahiro HIRAOKA, Masaki KOKUBO, Chikako YAMAMOTO and Michihide MITSUMORI Department of Therapeutic
male sexual dysfunction
 male sexual dysfunction lack of desire Both men and women often lose interest in sex during cancer treatment, at least for a time. At first, concern for survival is so overwhelming that sex is far down
male sexual dysfunction lack of desire Both men and women often lose interest in sex during cancer treatment, at least for a time. At first, concern for survival is so overwhelming that sex is far down
Peritoneal Surface Malignancies. Ira Allen Jacobs, MD, FACS Surgical Oncology San Diego, CA
 Peritoneal Surface Malignancies Ira Allen Jacobs, MD, FACS Surgical Oncology San Diego, CA Cancer dissemination routes Hematogenous metastases Lymphatic metastases Implants on peritoneal surfaces Surgically
Peritoneal Surface Malignancies Ira Allen Jacobs, MD, FACS Surgical Oncology San Diego, CA Cancer dissemination routes Hematogenous metastases Lymphatic metastases Implants on peritoneal surfaces Surgically
Carcinoma of the Cervix. Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology
 Carcinoma of the Cervix Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology Cervical Cancer Treatment Treatment Microinvasive (Stage IA1): Simple (extrafascial) hysterectomy/cone
Carcinoma of the Cervix Kathleen M. Schmeler, MD Associate Professor Department of Gynecologic Oncology Cervical Cancer Treatment Treatment Microinvasive (Stage IA1): Simple (extrafascial) hysterectomy/cone
Evidence tabel Lokaal palliatieve behandelingen
 Auteurs, jaartal Mate van bewijs Studie type Follow-up Populatie (incl. steekproef-grootte) Patienten kenmerken Interventie Controle Resultaten Conclusie Opmerkingen, commentaar Hartgrink, 2002 The Netherlands
Auteurs, jaartal Mate van bewijs Studie type Follow-up Populatie (incl. steekproef-grootte) Patienten kenmerken Interventie Controle Resultaten Conclusie Opmerkingen, commentaar Hartgrink, 2002 The Netherlands
Pathological assessment of the rectal cancer resection specimen
 P R A C T I C E G U I D E L I N E S Pathological assessment of the rectal cancer resection specimen Authors Key words A. Hoorens, M. De Ridder, A. Jouret-Mourin, C. Sempoux, C.A. Cuvelier, N. Nagy, G.
P R A C T I C E G U I D E L I N E S Pathological assessment of the rectal cancer resection specimen Authors Key words A. Hoorens, M. De Ridder, A. Jouret-Mourin, C. Sempoux, C.A. Cuvelier, N. Nagy, G.
Intraoperative Hyperthermic Intraperitoneal Chemotherapy (HIPEC) Volodymyr Labinskyy MD
 Volodymyr Labinskyy MD") Intraoperative Hyperthermic Intraperitoneal Chemotherapy (HIPEC) Volodymyr Labinskyy MD KCHC 8/29/13 52 y.o. F presented with severe pain in the right back and right flank, sharp, 8 out of 10, for 7 days.
Intraoperative Hyperthermic Intraperitoneal Chemotherapy (HIPEC) Volodymyr Labinskyy MD KCHC 8/29/13 52 y.o. F presented with severe pain in the right back and right flank, sharp, 8 out of 10, for 7 days.
da Vinci Prostatectomy Information Guide (Robotically-Assisted Radical Prostatectomy)
") da Vinci Prostatectomy Information Guide (Robotically-Assisted Radical Prostatectomy) Prostate Cancer Overview Prostate cancer is a disease in which malignant (cancer) cells form in the tissues of the
da Vinci Prostatectomy Information Guide (Robotically-Assisted Radical Prostatectomy) Prostate Cancer Overview Prostate cancer is a disease in which malignant (cancer) cells form in the tissues of the
Columbia University Mesothelioma Applied Research Foundation - 2009 - www.curemeso.org. Mesothelioma Center www.mesocenter.org
 Columbia University Mesothelioma Center www.mesocenter.org Multimodal clinical trials, treatment (surgery, radiation, chemotherapy) Peritoneal mesothelioma program Immunotherapy translational, experimental
Columbia University Mesothelioma Center www.mesocenter.org Multimodal clinical trials, treatment (surgery, radiation, chemotherapy) Peritoneal mesothelioma program Immunotherapy translational, experimental
Recurrent & Persistent Papillary Thyroid Cancer Central Nodal Dissection vs. Node-Picking Patterns of Nodal Metastases Recurrent Laryngeal Nerve,
 Recurrent & Persistent Papillary Thyroid Cancer Central Nodal Dissection vs. Node-Picking Patterns of Nodal Metastases Recurrent Laryngeal Nerve, Larynx, Trachea, & Esophageal Management Robert C. Wang,
Recurrent & Persistent Papillary Thyroid Cancer Central Nodal Dissection vs. Node-Picking Patterns of Nodal Metastases Recurrent Laryngeal Nerve, Larynx, Trachea, & Esophageal Management Robert C. Wang,
DA VINCI ROBOTIC HYSTERECTOMY
 DA VINCI ROBOTIC HYSTERECTOMY Until recently, surgery for most gynecologic conditions was performed using a large abdominal incision. This is because while conventional laparoscopic surgery is effective
DA VINCI ROBOTIC HYSTERECTOMY Until recently, surgery for most gynecologic conditions was performed using a large abdominal incision. This is because while conventional laparoscopic surgery is effective
Malignant Mesothelioma State of the Art
 Malignant Mesothelioma State of the Art Paul Baas The Netherlands Cancer Institute August 12, 2011, Carlsbad, CA Summary Diagnosis; epithelial type subdivided Pleiomorphic vs other Staging: IASLC-IMIG
Malignant Mesothelioma State of the Art Paul Baas The Netherlands Cancer Institute August 12, 2011, Carlsbad, CA Summary Diagnosis; epithelial type subdivided Pleiomorphic vs other Staging: IASLC-IMIG
Radiotherapy in Plasmacytoma and Myeloma. David Cutter Multiple Myeloma NSSG Annual Meeting 14 th September 2015
 Radiotherapy in Plasmacytoma and Myeloma David Cutter Multiple Myeloma NSSG Annual Meeting 14 th September 2015 Contents Indications for radiotherapy: Palliation in Multiple Myeloma Solitary Bone Plasmacytoma
Radiotherapy in Plasmacytoma and Myeloma David Cutter Multiple Myeloma NSSG Annual Meeting 14 th September 2015 Contents Indications for radiotherapy: Palliation in Multiple Myeloma Solitary Bone Plasmacytoma
NHS. Surgical repair of vaginal wall prolapse using mesh. National Institute for Health and Clinical Excellence. 1 Guidance.
 Issue date: June 2008 NHS National Institute for Health and Clinical Excellence Surgical repair of vaginal wall prolapse using mesh 1 Guidance 1.1 The evidence suggests that surgical repair of vaginal
Issue date: June 2008 NHS National Institute for Health and Clinical Excellence Surgical repair of vaginal wall prolapse using mesh 1 Guidance 1.1 The evidence suggests that surgical repair of vaginal
Laparoscopic Surgery of the Colon and Rectum (Large Intestine) A Simple Guide to Help Answer Your Questions
 A Simple Guide to Help Answer Your Questions") Laparoscopic Surgery of the Colon and Rectum (Large Intestine) A Simple Guide to Help Answer Your Questions What are the Colon and Rectum? The colon and rectum together make up the large intestine. After
Laparoscopic Surgery of the Colon and Rectum (Large Intestine) A Simple Guide to Help Answer Your Questions What are the Colon and Rectum? The colon and rectum together make up the large intestine. After
Prostate Cancer Treatment Comparison
 Prostate Cancer Treatment Comparison Treatment Comparative Data Outcome Comparison: Surgery vs. Radiotherapy Outcome Radical Prostatectomy* Radiation** Survival duration compared to conservative disease
Prostate Cancer Treatment Comparison Treatment Comparative Data Outcome Comparison: Surgery vs. Radiotherapy Outcome Radical Prostatectomy* Radiation** Survival duration compared to conservative disease
Radiotherapy in locally advanced & metastatic NSC lung cancer
 Radiotherapy in locally advanced & metastatic NSC lung cancer Dr Raj Hegde. MD. FRANZCR Consultant Radiation Oncologist. William Buckland Radiotherapy Centre. Latrobe Regional Hospital. Locally advanced
Radiotherapy in locally advanced & metastatic NSC lung cancer Dr Raj Hegde. MD. FRANZCR Consultant Radiation Oncologist. William Buckland Radiotherapy Centre. Latrobe Regional Hospital. Locally advanced
Mesh Erosion and What to do
 Disclosures Mesh Erosion and What to do None Michelle Y. Morrill, MD Chief of Urogynecology, TPMG Director of Urogynecology, Kaiser San Francisco Assistant Professor, Volunteer Faculty Dept of Ob/Gyn,
Disclosures Mesh Erosion and What to do None Michelle Y. Morrill, MD Chief of Urogynecology, TPMG Director of Urogynecology, Kaiser San Francisco Assistant Professor, Volunteer Faculty Dept of Ob/Gyn,
Laparoscopic Abdominoperineal Resection for Low Rectal Adenocarcinoma
 J Soc Colon Rectal Surgeon (Taiwan) September 2008 Original Article Laparoscopic Abdominoperineal Resection for Low Rectal Adenocarcinoma Tao-Wei Ke William Tzu-Liang Chen 2 Hong-Chang Chen Ting-Ming Huang
J Soc Colon Rectal Surgeon (Taiwan) September 2008 Original Article Laparoscopic Abdominoperineal Resection for Low Rectal Adenocarcinoma Tao-Wei Ke William Tzu-Liang Chen 2 Hong-Chang Chen Ting-Ming Huang
Mini-invasive surgery for colorectal cancer
 Chinese Journal of Cancer Review Wei-Gen Zeng and Zhi-Xiang Zhou Abstract Laparoscopic techniques have been extensively used for the surgical management of colorectal cancer during the last two decades.
Chinese Journal of Cancer Review Wei-Gen Zeng and Zhi-Xiang Zhou Abstract Laparoscopic techniques have been extensively used for the surgical management of colorectal cancer during the last two decades.
Colocutaneous Fistula. Disclosures
 Colocutaneous Fistula Madhulika G. Varma MD Associate Professor Chief, Colorectal Surgery University of California, San Francisco Honoraria Applied Medical Covidien Disclosures 1 Colocutaneous Fistula
Colocutaneous Fistula Madhulika G. Varma MD Associate Professor Chief, Colorectal Surgery University of California, San Francisco Honoraria Applied Medical Covidien Disclosures 1 Colocutaneous Fistula
Clinical Indications and Results Following Chest Wall Resection
 Clinical Indications and Results Following Chest Wall Resection for Recurrent Malignant Pleural Mesothelioma Ali SO, Burt BM, Groth SS, DaSilva MC, Yeap BY, Richards WG, Baldini EH and Sugarbaker DJ. Division
Clinical Indications and Results Following Chest Wall Resection for Recurrent Malignant Pleural Mesothelioma Ali SO, Burt BM, Groth SS, DaSilva MC, Yeap BY, Richards WG, Baldini EH and Sugarbaker DJ. Division
PSA Screening for Prostate Cancer Information for Care Providers
 All men should know they are having a PSA test and be informed of the implications prior to testing. This booklet was created to help primary care providers offer men information about the risks and benefits
All men should know they are having a PSA test and be informed of the implications prior to testing. This booklet was created to help primary care providers offer men information about the risks and benefits
The Role of Laparoscopy in Endometrial Cancer
 The Role of Laparoscopy in Endometrial Cancer Prof. Dr. Tugan BEŞE İstanbul University, Cerrahpaşa Medical Faculty Gynecologic Oncology Department Surgical staging in Endometrial Cancer Laparoscopic surgery
The Role of Laparoscopy in Endometrial Cancer Prof. Dr. Tugan BEŞE İstanbul University, Cerrahpaşa Medical Faculty Gynecologic Oncology Department Surgical staging in Endometrial Cancer Laparoscopic surgery
The enigma of the transsphincteric anal fistula. Per-Olof Nyström, M.D., Ph.D. Karolinska University Hospital, Stockholm, Sweden
 The enigma of the transsphincteric anal fistula Per-Olof Nyström, M.D., Ph.D. Karolinska University Hospital, Stockholm, Sweden Four principles of treatment for anal fistula 1. Inactivate the fistula 2.
The enigma of the transsphincteric anal fistula Per-Olof Nyström, M.D., Ph.D. Karolinska University Hospital, Stockholm, Sweden Four principles of treatment for anal fistula 1. Inactivate the fistula 2.
A Practical Guide to Advances in Staging and Treatment of NSCLC
 A Practical Guide to Advances in Staging and Treatment of NSCLC Robert J. Korst, M.D. Director, Thoracic Surgery Medical Director, The Blumenthal Cancer Center The Valley Hospital Objectives Revised staging
A Practical Guide to Advances in Staging and Treatment of NSCLC Robert J. Korst, M.D. Director, Thoracic Surgery Medical Director, The Blumenthal Cancer Center The Valley Hospital Objectives Revised staging
9/26/14. Joel E. Rand, MPAS, PA-C DMU Luncheon May 1, 2014
 Joel E. Rand, MPAS, PA-C DMU Luncheon May 1, 2014 No financial relationship or commercial interest in any of the technologies discussed Not supporting any non-fda off label uses of any product or service
Joel E. Rand, MPAS, PA-C DMU Luncheon May 1, 2014 No financial relationship or commercial interest in any of the technologies discussed Not supporting any non-fda off label uses of any product or service
The Need for Accurate Lung Cancer Staging
 The Need for Accurate Lung Cancer Staging Peter Baik, DO Thoracic Surgery Cancer Treatment Centers of America Oklahoma Osteopathic Association 115th Annual Convention Financial Disclosures: None 2 Objectives
The Need for Accurate Lung Cancer Staging Peter Baik, DO Thoracic Surgery Cancer Treatment Centers of America Oklahoma Osteopathic Association 115th Annual Convention Financial Disclosures: None 2 Objectives
Considering Endometriosis Surgery? Learn about minimally invasive da Vinci Surgery
 Considering Endometriosis Surgery? Learn about minimally invasive da Vinci Surgery The Condition: Endometriosis Endometriosis is a condition in which the tissue that lines your uterus (the endometrium)
Considering Endometriosis Surgery? Learn about minimally invasive da Vinci Surgery The Condition: Endometriosis Endometriosis is a condition in which the tissue that lines your uterus (the endometrium)
SUNY DOWNSTATE MEDICAL CENTER SURGERY GRAND ROUNDS February 28, 2013 VERENA LIU, MD ROSEANNA LEE, MD
 SUNY DOWNSTATE MEDICAL CENTER SURGERY GRAND ROUNDS February 28, 2013 VERENA LIU, MD ROSEANNA LEE, MD Case Presentation 35 year old male referred from PMD with an asymptomatic palpable right neck mass PMH/PSH:
SUNY DOWNSTATE MEDICAL CENTER SURGERY GRAND ROUNDS February 28, 2013 VERENA LIU, MD ROSEANNA LEE, MD Case Presentation 35 year old male referred from PMD with an asymptomatic palpable right neck mass PMH/PSH:
Laparoscopic Colectomy. What do I need to know about my laparoscopic colorectal surgery?
 Laparoscopic Colectomy What do I need to know about my laparoscopic colorectal surgery? Traditionally, colon & rectal surgery requires a large, abdominal and/or pelvic incision, which often requires a
Laparoscopic Colectomy What do I need to know about my laparoscopic colorectal surgery? Traditionally, colon & rectal surgery requires a large, abdominal and/or pelvic incision, which often requires a
Elective Clinical Target Volumes in Anorectal Cancer: An RTOG Consensus Panel Contouring Atlas
 Elective Clinical Target Volumes in Anorectal Cancer: An RTOG Consensus Panel Contouring Atlas 1 2 1 3 1 1 4 R Myerson, M Garofalo, Iel Naqa, R Abrams, A Apte, W Bosch, P Das, L 5 6 7 8 9 Gunderson, T
Elective Clinical Target Volumes in Anorectal Cancer: An RTOG Consensus Panel Contouring Atlas 1 2 1 3 1 1 4 R Myerson, M Garofalo, Iel Naqa, R Abrams, A Apte, W Bosch, P Das, L 5 6 7 8 9 Gunderson, T
Kidney Cancer OVERVIEW
 Kidney Cancer OVERVIEW Kidney cancer is the third most common genitourinary cancer in adults. There are approximately 54,000 new cancer cases each year in the United States, and the incidence of kidney
Kidney Cancer OVERVIEW Kidney cancer is the third most common genitourinary cancer in adults. There are approximately 54,000 new cancer cases each year in the United States, and the incidence of kidney
Endoscopic Management of Strictures and Leaks. Prepared by Aurora D. Pryor, MD Presented by Dana Portenier, MD Duke University Medical Center
 Endoscopic Management of Strictures and Leaks Prepared by Aurora D. Pryor, MD Presented by Dana Portenier, MD Duke University Medical Center What can go wrong? Bleeding (2%) Sleeve too big Angulated Too
Endoscopic Management of Strictures and Leaks Prepared by Aurora D. Pryor, MD Presented by Dana Portenier, MD Duke University Medical Center What can go wrong? Bleeding (2%) Sleeve too big Angulated Too
Radiation Therapy for Prostate Cancer
 Radiation Therapy for Prostate Cancer Introduction Cancer of the prostate is the most common form of cancer that affects men. About 240,000 American men are diagnosed with prostate cancer every year. Your
Radiation Therapy for Prostate Cancer Introduction Cancer of the prostate is the most common form of cancer that affects men. About 240,000 American men are diagnosed with prostate cancer every year. Your
Accelerated hemithoracic radiation followed by extrapleural pneumonectomy for malignant pleural mesothelioma
 Accelerated hemithoracic radiation followed by extrapleural pneumonectomy for malignant pleural mesothelioma Marc de Perrot, Ronald Feld, Natasha B Leighl, Andrew Hope, Thomas K Waddell, Shaf Keshavjee,
Accelerated hemithoracic radiation followed by extrapleural pneumonectomy for malignant pleural mesothelioma Marc de Perrot, Ronald Feld, Natasha B Leighl, Andrew Hope, Thomas K Waddell, Shaf Keshavjee,
Hand-sewn Bowel Anastomosis: The Only Correct Choice. Ashok Babu, M.D. Department of Surgery University of Colorado
 Hand-sewn Bowel Anastomosis: The Only Correct Choice Ashok Babu, M.D. Department of Surgery University of Colorado Outline History Trial data in specific applications Colorectal Ileocolic Esophagogastric
Hand-sewn Bowel Anastomosis: The Only Correct Choice Ashok Babu, M.D. Department of Surgery University of Colorado Outline History Trial data in specific applications Colorectal Ileocolic Esophagogastric
Cancer research in the Midland Region the prostate and bowel cancer projects
 Cancer research in the Midland Region the prostate and bowel cancer projects Ross Lawrenson Waikato Clinical School University of Auckland MoH/HRC Cancer Research agenda Lung cancer Palliative care Prostate
Cancer research in the Midland Region the prostate and bowel cancer projects Ross Lawrenson Waikato Clinical School University of Auckland MoH/HRC Cancer Research agenda Lung cancer Palliative care Prostate
Surgical therapy of. who should be operated
 SAMO Interdisciplinary Workshop on Chest Tumors Lucerne, 13th and 14th January 2012 Surgical therapy of mesothelioma, who should be operated Walter Weder MD Professor of Surgery University Hospital Zurich
SAMO Interdisciplinary Workshop on Chest Tumors Lucerne, 13th and 14th January 2012 Surgical therapy of mesothelioma, who should be operated Walter Weder MD Professor of Surgery University Hospital Zurich
RADICAL HYSTERECTOMY IN ROBOTIC SURGERY
 RADICAL HYSTERECTOMY IN ROBOTIC SURGERY FLORENCE BOCHU CENTRE OSCAR LAMBRET LILLE PATRICIA VARUMBEKE CENTRE OSCAR LAMBRET LILLE MELANIE FLAMENT CENTRE OSCAR LAMBRET LILLE More and more centers across the
RADICAL HYSTERECTOMY IN ROBOTIC SURGERY FLORENCE BOCHU CENTRE OSCAR LAMBRET LILLE PATRICIA VARUMBEKE CENTRE OSCAR LAMBRET LILLE MELANIE FLAMENT CENTRE OSCAR LAMBRET LILLE More and more centers across the
Colorectal Cancer Care A Cancer Care Map for Patients
 Colorectal Cancer Care A Cancer Care Map for Patients Understanding the process of care that a patient goes through in the diagnosis and treatment of colorectal cancer in BC. Colorectal Cancer Care Map
Colorectal Cancer Care A Cancer Care Map for Patients Understanding the process of care that a patient goes through in the diagnosis and treatment of colorectal cancer in BC. Colorectal Cancer Care Map
Non-Small Cell Lung Cancer Treatment Comparison to NCCN Guidelines
 Non-Small Cell Lung Cancer Treatment Comparison to NCCN Guidelines April 2008 (presented at 6/12/08 cancer committee meeting) By Shelly Smits, RHIT, CCS, CTR Conclusions by Dr. Ian Thompson, MD Dr. James
Non-Small Cell Lung Cancer Treatment Comparison to NCCN Guidelines April 2008 (presented at 6/12/08 cancer committee meeting) By Shelly Smits, RHIT, CCS, CTR Conclusions by Dr. Ian Thompson, MD Dr. James
Facing a Hernia Repair? Learn about minimally invasive da Vinci Surgery
 Facing a Hernia Repair? Learn about minimally invasive da Vinci Surgery The Condition: Hernia A hernia happens when part of an internal organ or tissue bulges through a hole or weak area in the belly wall
Facing a Hernia Repair? Learn about minimally invasive da Vinci Surgery The Condition: Hernia A hernia happens when part of an internal organ or tissue bulges through a hole or weak area in the belly wall
Integrating Chemotherapy and Liver Surgery for the Management of Colorectal Metastases
 I Congresso de Oncologia D Or July 5-6, 2013 Integrating Chemotherapy and Liver Surgery for the Management of Colorectal Metastases Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University
I Congresso de Oncologia D Or July 5-6, 2013 Integrating Chemotherapy and Liver Surgery for the Management of Colorectal Metastases Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University
Post-operative intrapleural chemotherapy for mesothelioma
 Post-operative intrapleural chemotherapy for mesothelioma Robert Kratzke, MD John Skoglund Chair for Lung Cancer Research Section of Heme-Onc-Transplant University of Minnesota Medical School Efficacy
Post-operative intrapleural chemotherapy for mesothelioma Robert Kratzke, MD John Skoglund Chair for Lung Cancer Research Section of Heme-Onc-Transplant University of Minnesota Medical School Efficacy
Implementation Date: April 2015 Clinical Operations
 National Imaging Associates, Inc. Clinical guideline PROSTATE CANCER Original Date: March 2011 Page 1 of 5 Radiation Oncology Last Review Date: March 2015 Guideline Number: NIA_CG_124 Last Revised Date:
National Imaging Associates, Inc. Clinical guideline PROSTATE CANCER Original Date: March 2011 Page 1 of 5 Radiation Oncology Last Review Date: March 2015 Guideline Number: NIA_CG_124 Last Revised Date: