MARYLAND DEPARTMENT OF HEALTH AND MENTAL HYGIENE FAMILY HEALTH ADMINISTRATION CENTER FOR MATERNAL AND CHILD HEALTH. Maternal Mortality Review Program
|
|
|
- Anne Davis
- 7 years ago
- Views:
Transcription
1
2 MARYLAND DEPARTMENT OF HEALTH AND MENTAL HYGIENE FAMILY HEALTH ADMINISTRATION CENTER FOR MATERNAL AND CHILD HEALTH Maternal Mortality Review Program 2010 ANNUAL REPORT Martin O Malley Governor Anthony G. Brown Lieutenant Governor John M. Colmers Secretary Department of Health & Mental Hygiene Frances B. Phillips Deputy Secretary, Public Health Services Department of Health & Mental Hygiene

3 I. Introduction During the 2000 Maryland General Assembly, Health-General Article was enacted to establish maternal mortality review in Maryland. The statute requires: (1) identification of maternal death cases; (2) review of medical records and other relevant data; (3) determination of preventability of death; (4) development of recommendations for the prevention of maternal deaths; and (5) dissemination of findings and recommendations to policymakers, health care providers, health care facilities, and the public. The Maryland Department of Health and Mental Hygiene (Department) administers the Maternal Mortality Review Program in consultation with the Maryland State Medical Society (MedChi). Funding has been made available from the Department s Center for Maternal and Child Health to MedChi since June 2001 to investigate pregnancy-associated deaths in Maryland and identify opportunities to reduce maternal mortality. MedChi s Maternal and Child Health (MCH) Committee provides consultation to the Department regarding maternal mortality review activities, develops recommendations for the prevention of maternal deaths, and disseminates findings and recommendations to policymakers, health care providers, health care facilities, and the general public. II. National and State Data Maternal mortality is complicated by the use of various definitions. A maternal death is defined by the World Health Organization s (WHO) International Classification of Diseases Ninth Revision (ICD-9) and Tenth Revision (ICD-10) to be the death of a woman while pregnant or within 42 days of conclusion of pregnancy, irrespective of the duration and site of the pregnancy, from any cause related to or aggravated by pregnancy or its management but not from accidental or incidental causes. This definition is used by the Centers for Disease Control and Prevention s National Center for Health Statistics (NCHS) in calculating the maternal mortality ratio (MMR) in the United States. The MMR is defined as the number of maternal deaths per 100,000 live-births in the same time period. This ratio is utilized for national and international comparisons. In 1986, the Centers for Disease Control and Prevention (CDC) and the American College of Obstetricians and Gynecologists (ACOG) collaborated to issue a statement recommending the use of an enhanced surveillance definition as an approach to more accurately identify deaths among women in which pregnancy was a contributing factor. This collaboration also defined pregnancy-associated deaths. A pregnancy-associated death is the death of a woman while pregnant or within one year or 365 days of pregnancy conclusion, regardless of the cause of death. A pregnancy-related death was further defined as the death of a woman while pregnant or within one year of conclusion of pregnancy, irrespective of the duration and site of the pregnancy, from any cause related to or aggravated by her pregnancy or its management, but not from accidental or incidental causes. The three terms maternal death, pregnancy-associated death, and pregnancy-related death, create a challenge when comparing data from different sources and reports for different jurisdictional entities. An enhanced surveillance method is necessary to determine pregnancy-associated deaths and will be discussed below. The NCHS uses strict criteria to define deaths included in the MMR based upon information from the death certificates alone. Enhanced surveillance using multiple sources including case review will identify additional cases at the State level, which meet the WHO definition. It is expected that as Maryland and other states enhance surveillance, the MMR will increase by this improved identification process. 2
 administers the Maternal Mortality Review Program in consultation with the Maryland State Medical Society (MedChi).")
4 The Healthy People 2010 MMR target is 3.3 deaths per 100,000 live births, the same goal as Healthy People 2000, which was not met. Nationally, maternal mortality has declined dramatically since the 1930s when the MMR was 670 maternal deaths per 100,000 live births. The MMR achieved its lowest levels in the early 1980s. However, the MMR rose in the 1990s. The national MMR for was 15.8 maternal deaths per 100,000 live births. For the same period, Maryland s MMR was A fiveyear average ratio is used because maternal deaths are relatively infrequent events that may vary considerably year-to-year, particularly in a small state like Maryland. Figure 1 below provides a comparison between the maternal mortality ratio for the U.S. and Maryland by race. Deaths per 100,000 live births Figure 1. Maternal Mortality Ratio by Race U.S. and Maryland All races White Black U.S. Maryland 36.9 In the U.S., black women have an MMR three times greater than that for white women, a disparity that has persisted since the 1940s. For Maryland, the MMR for black women is over twice the MMR for white women, and is slightly higher than the U.S. average. The MMR for white women in Maryland is also elevated above the national average. In Maryland the number of pregnancy-associated deaths, tracked by the Maternal Mortality Review Program between 2004 and 2008, demonstrated an average of 41 deaths per year. Figure 2 shows the number of pregnancy-associated deaths in Maryland from 2004 to

5 III. Maternal Mortality Review Process in Maryland Case Identification Cases for review are limited to women of childbearing age who were residents of Maryland at the time of their death. Maryland residents who died in other jurisdictions are counted in the official Vital Statistics reports, but may not be included in the case reviews because of the difficulty in obtaining records across jurisdictions. These deaths account for a maximum of two to four per year or approximately percent of the total pregnancy-associated deaths. Pregnancy-associated deaths are identified in one of three ways in Maryland. Individual death certificates are the first method of identifying pregnancy-associated deaths through the use of checkbox questions or because the cause of death is clearly related to pregnancy, such as ruptured ectopic pregnancy. The Maryland death certificate was revised in January 2001 to include questions about pregnancy status and date of delivery for the 12 months preceding death. Maryland is one of at least 18 jurisdictions that include questions specifically designed to improve identification of maternal deaths on the death certificate. The pregnancy checkbox has significantly increased identification of pregnancy-associated deaths from those recognized by cause of death alone. In a 2005 article in the American Journal of Public Health, Dr. Isabelle Horon of the Department s Vital Statistics Administration reported that only 62% of Maryland maternal deaths in the years were identified by cause-of-death information alone. One would expect even fewer pregnancyassociated deaths to be identified in this manner. The second method of determining cases involves linking death certificates for females aged years with birth certificates and fetal death certificates to identify additional cases that were not found by examining death certificates alone. Thirdly, cases are identified through a manual review of files from deaths reported to the Office of the Chief Medical Examiner (OCME), also looking for evidence of pregnancy in deceased women. All deaths occurring within 365 days of pregnancy conclusion are subsequently designated as pregnancy-associated and further investigated. Using these three methods, 42 pregnancy-associated 4

6 deaths were identified in The purpose of this report is to review data for these 42 deaths. Case Review Pregnancy-associated deaths for 2008 underwent several stages of review under the auspices of the MedChi MCH Committee. Once cases were identified, medical records were obtained from the hospitals of death and delivery, when applicable, and available death certificates, hospital records and OCME records were reviewed. The Maternal Mortality Workgroup carries out detailed reviews of selected cases determined to be preventable or potentially preventable. The Workgroup is a subcommittee of the MedChi MCH Committee and includes representatives from general obstetric, perinatology, family practice, pediatric, and nurse-midwifery specialties. The Workgroup s discussion incorporates the CDC framework for case review outlined in Strategies to Reduce Pregnancy-Related Deaths: From Identification to Action. This approach takes into account medical and non-medical factors contributing to maternal death and examines quality and content of medical care. Medical, non-medical or social causes underlying the maternal death include factors such as: Intendedness of pregnancy Woman s and her family s knowledge about pregnancy Timeliness on the part of the woman in recognizing a problem Accessibility and acceptability of health care Cultural competence and communication skills of health care providers Woman s adherence or non-adherence to medical advice and health interventions Individual factors such as pre-existing medical conditions, obesity and substance abuse Quality and content of medical care on a provider team and institutional level includes factors such as: Preventive services Community and patient education Nutrition, substance abuse, and social services Preconception services Prenatal care Labor and delivery services Postpartum care and follow-up Treatment and management Diagnostic procedures Medical interventions Patient education and follow-up Cases discussed by the Workgroup are de-identified and members sign confidentiality statements. The Maternal Mortality Policy Subcommittee meets to review system issues identified through case reviews and to develop recommendations. This Subcommittee includes representation from managed care, nursing, and social work in addition to the Maternal Mortality Workgroup members. All those involved in any phase of the case review process are included in a final review of systems issues and 5

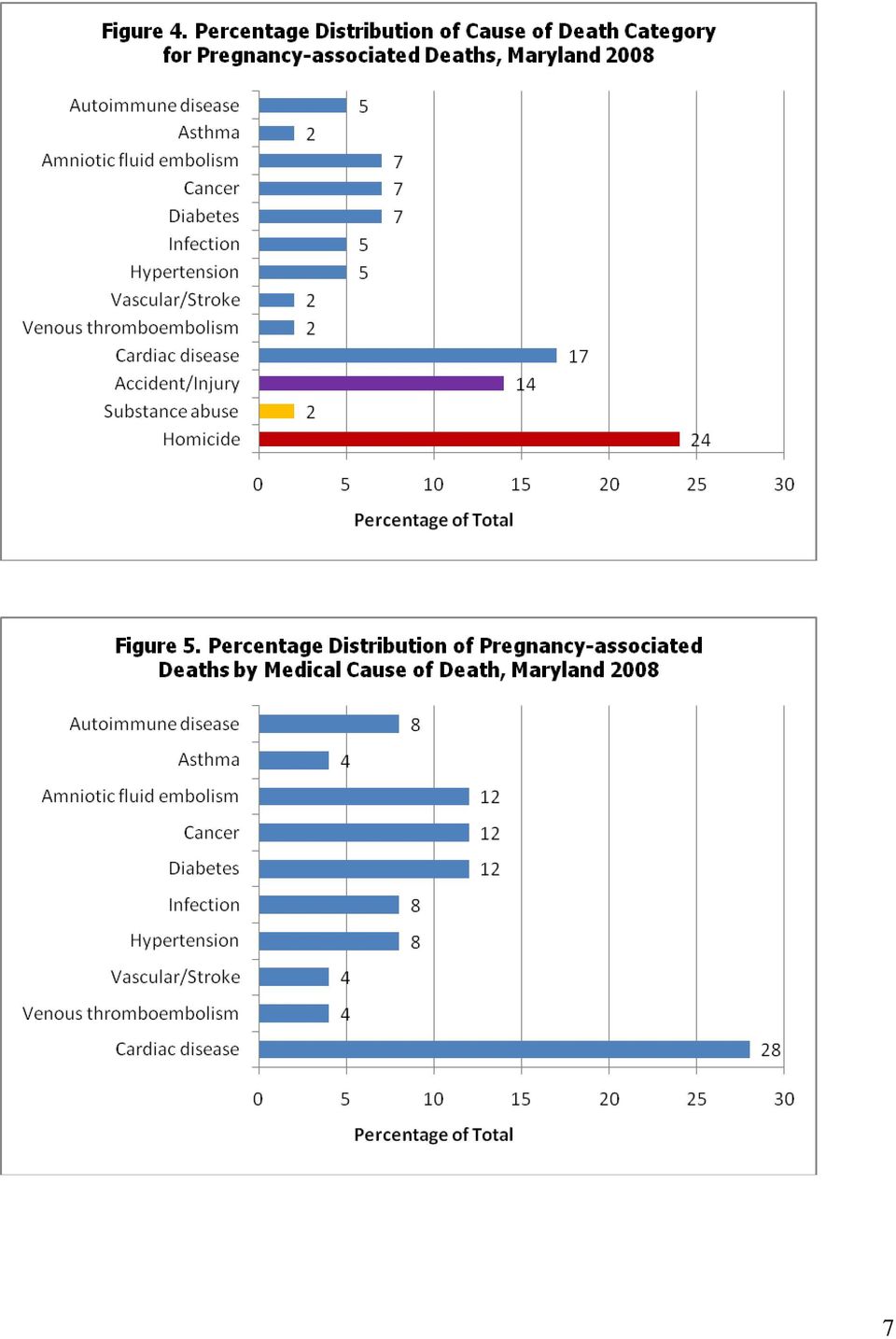
7 recommendations under the auspices of the MedChi MCH Committee. The MedChi Maternal Mortality Review Policy Subcommittee met in October 2010 to review the 2008 pregnancy-associated death data and findings from previous years. Additionally, a report of multiple year data analysis from pregnancy-associated deaths from 2000 to 2008 is being prepared which will include a summary of prior findings and recommendations. A meeting has been scheduled for December in 2010 to continue discussions for the report. IV. Case Findings in Maryland The most recent data in this report are 2008 pregnancy-associated deaths. There were 42 pregnancyassociated deaths identified for Cause of Death Classification The leading causes of 2008 pregnancy-associated deaths were homicide, cardiac disease, and accident. Figure 3 shows the distribution of pregnancy-associated deaths by manner of death. Among the 42 pregnancy-associated deaths, 60 percent were due to natural causes (excludes homicide, suicide, and substance abuse), 24 percent to intentional injury (homicide), and 14 percent to unintentional injury (accident). Figure 4 shows the distribution of deaths from both medical (natural) and non-medical causes. The leading medical cause of death was cardiac disease, which accounted for 17 percent of all deaths occurring in As shown in Figure 5, cardiac disease accounted for 28 percent of deaths resulting from medical causes. 6

8 7
9 Timing of Death Figure 6 illustrates the distribution of deaths by timing of death. The majority of pregnancyassociated deaths occurred after delivery or postpartum. Among the 42 pregnancy-associated deaths, 36 percent occurred within 41 days postpartum, and 28 percent between 42 and 365 days postpartum. Twenty-one percent of the deaths were among women who were pregnant or undelivered at the time of death. The timing of death in relation to pregnancy was unknown for 14 percent of deaths. Intentional and unintentional injury was the most frequent cause of death (60%) among women who died while pregnant or between six months and one year postpartum. Among women who died within six weeks of the conclusion of pregnancy, medical causes accounted for 93 percent of deaths, with cardiac disease being the most frequent (27%) cause of death within that time period. Cases by Maternal Race and Ethnicity Figure 7 illustrates the racial/ethnic distribution of pregnancy-associated deaths and live births. Among the 42 pregnancy-associated deaths, 50 percent occurred among black women, 38 percent occurred among white women, 7 percent among Hispanic women, and 5 percent among Asian/Pacific Islander women. In comparison the distribution of live births is as follows: 34 percent among black women, 46 percent among white women, 14 percent among Hispanic women, and 6 percent among Asian/Pacific Islander women. A persistent racial disparity is evident in the greater proportion of black women who died while pregnant or within 365 days of pregnancy compared to the proportion of black women who had a live birth. Among white women, the leading causes of death were homicide, injury, and cardiac disease. Homicide and cardiac disease were the leading causes among black women. Women of other race/ethnicity were too few in number to identify any trends in cause of death. 8
 among women who died while pregnant or between six months and one year postpartum.")
10 Cases by Maternal Age Pregnancy-associated deaths occurred in women ranging in age from 17 to 42 years, as shown in Figure 8. The majority (62%) of deaths among women less than 25 years of age were a result of homicide and accident/injury, while the majority (69%) of deaths among women 25 years of age and older were due to natural causes. Among women 20 to 24 years of age, diabetes was the leading medical cause of death, accounting for 25 percent of deaths, and cardiac disease accounted for 33 percent of deaths among women aged 25 to 29 years of age. 9

11 Pregnancy Outcome The outcome of pregnancy among the pregnancy-associated deaths in 2008 is shown in Figure 9. Sixty-nine per cent of cases had a live birth, 21% were pregnant at time of death, and in 10% the pregnancy outcome was unknown. V. Recommendations Finding 1: Homicide accounted for 24 percent of all pregnancy-associated deaths in 2008 and 54 percent of deaths among women younger than 25 years of age. Recommendation 1: Providers should include a thorough injury evaluation for pregnant and postpartum women presenting to the emergency department (ED), including consideration of possible intimate partner or domestic violence. This recommendation will require ongoing education of ED and obstetric providers about injury evaluation and management. Finding 2: Cardiac disease was the leading medical cause of death for all women, and for women younger than 30 years of age. Recommendation 2: Health care providers should screen all pregnant and postpartum women for cardiac disease if presenting with symptoms, even at young ages. Ongoing consultation is needed between obstetric and cardiology providers. Finding 3: Diabetes was the leading medical cause of death for women 20 to 24 years of age. Recommendation 3: Diet and weight management should be included in prenatal counseling for women diagnosed with or at risk for diabetes. 10
, including consideration of possible intimate")
12 Finding 4: Obesity and over-weight may be major contributing factors to maternal mortality, particularly to deaths resulting from cardiac disease and diabetes. Recommendation 4: Documentation of pre-pregnancy height and weight should be included in the prenatal medical record. Height and weight should be documented on all inpatient admissions and including in the evaluation of all deceased individuals. Finding 5: Pregnancy-associated deaths occurred most frequently within the first six weeks after pregnancy. For patients at high risk for postpartum complications, routine six-week follow-up may be too late and postpartum discharge instructions may not be adequate for ideal care. Recommendation 5: Women with identified risk factors should follow up with their obstetric providers earlier than six weeks postpartum. Scheduling the postpartum visit prior to discharge from the hospital may help to ensure that high-risk women will return for follow-up. VI. Maternal Mortality Review Related Activities The Maryland Patient Safety Center Perinatal Learning Network The Maryland Patient Safety Center Perinatal Learning Network (PLN), a collaboration between the Delmarva Foundation and the Maryland Hospital Association, was continued in FY10. The PLN provides a forum for hospitals that provide obstetrical services to Maryland residents to share protocols and information to improve team communication and patient safety. Teams communicate though a Listserv maintained by the PLN. There are currently two Listservs that are active: Obstetrical Chair Listserv for Department Chairs in Maryland and Washington, DC, and another for all participants of the PLN. Both Listservs have provided an opportunity for the exchange of knowledge and ideas on a wide variety of topics pertinent to perinatal care. Maryland Advanced Perinatal Systems and Services (MAPSS) Program The University of Maryland School of Medicine, in collaboration with Johns Hopkins, established the Maryland Advanced Perinatal Systems Services (MAPSS) Program. The program is administered by the Department of Obstetrics, Gynecology & Reproductive Sciences at the University of Maryland. MAPSS provides high-risk perinatal consultation to community physicians for the management of complications associated with poor pregnancy outcomes, including maternal death. The University of Maryland uses telemedicine to provide high-risk perinatal consultation to local health care providers in under-served communities, while Johns Hopkins perinatal consultation is offered on-site upon request from local physicians. These high-risk obstetrics services help to address the shortage of obstetrical providers throughout the State as well as increase the capacity of providers to manage complications of pregnancy at the community level. This enables women to have access to specialized consultative services while remaining in their local communities. Both the University of Maryland and Johns Hopkins University have served in an advisory capacity to the Maryland Patient Safety Center Perinatal Learning Network. 11

13 The Governor s Delivery Unit In 2008, Governor O Malley created the Governor s Delivery Unit as an extension of State Stat to work with State agencies to align State and federal resources around 15 strategic and visionary goals to improve the quality of life in Maryland. Recognizing that infant mortality is the most sensitive indicator of the overall health of a community, the Governor has developed a strategic goal to specifically address this issue. The Governor s Strategic Goal is to reduce infant mortality in Maryland by 10% by By the end of 2012, Maryland aims to have 60 fewer infant deaths, resulting in an infant mortality rate of 7.2/1,000 which would be Maryland s lowest recorded infant mortality rate. In 2009, Maryland s infant mortality rate fell by 10% to 7.2. Efforts continue under the GDU in 2010, however, to further address infant mortality and reduce racial disparities. The strategic approach focuses on: (1) assessing the data and targeting disparities; (2) building on strengths and partnerships; and (3) taking a comprehensive systems approach. The GDU Plan concentrates proven intervention strategies at different points along the women s life span: Preconception - interventions before pregnancy to ensure healthier women at time of conception. Prenatal - interventions during pregnancy to ensure earlier entry into prenatal care. Perinatal and neonatal - interventions around and immediately after pregnancy to ensure comprehensive, high quality follow-up care. Baltimore City, Prince George s County, and Somerset County, three jurisdictions with high infant mortality rates, were initially targeted by the GDU Plan. The Plan builds upon efforts currently taking place in those jurisdictions, including the Baltimore City Health Department s Strategy to Improve Birth Outcomes, which was subsequently renamed B More for Healthy Babies, Prince George s County Health Department s Healthy Women, Healthy Lives Program, and the Somerset County Health Department s Babies Born Healthy Program. Efforts developed in these jurisdictions will subsequently be expanded to other jurisdictions in order to effect a systems change throughout the State. Women s Health The Center for Maternal and Child Health (CMCH) has adopted a life-span approach to women s health, viewing it as a critical adjunct to preconception, inter-conception, and prenatal health. This is based on the realization that comprehensive women s health care from infancy, childhood, adolescence, and adulthood, regardless of pregnancy intention or status, will ultimately ensure good health through future pregnancies and afterwards. Recent women s health activities that impact maternal health include: Women s health screening cards, 2010 These cards were updated in 2010 and are sorted by each decade of life: teens, 20s, 30s, 40s, 50s, and 60s and beyond. Each card lists the recommended screening tests and immunizations for women to prevent or lessen their risk for chronic conditions in the future. Age appropriate health tips are provided on the back of each card. A section on Reproductive Health is included on the cards 12

14 for teens through to 40s. The information on these cards is available on the CMCH women s health Web page Women s Health Report The CMCH Report of Maryland Women 2008 is being updated and will be published as a report in February This report will include current data on major causes of death, chronic disorders, health care access, perinatal health, and health status. Intimate Partner Violence Since 1993, homicide has been a leading cause of maternal mortality in Maryland. The majority of these deaths are the result of intimate partner violence. A representative from CMCH s Women s Health Program is a member of the Baltimore City Domestic Violence Fatality Review Team (BCDVFRT), a multi-disciplinary team established in 2006 representing domestic violence agencies, the State Attorney s office, law enforcement, hospitals, and the criminal justice system. Past pregnancy histories are now a routine part of case reviews. Sixteen other counties in Maryland currently participate in DVFRT. The Maryland Healthcare Coalition Against Domestic Violence developed a toolkit on domestic violence for health care providers. This 2010 toolkit workbook, Health Care Response to Domestic Violence: A Toolkit for Hospitals, Facilities, & Providers, includes information on domestic violence definitions and statistics, screening tools, danger assessments, safety planning, privacy issues, medical coding, consent forms, reporting requirements, and recommendations for documentation, intervention, resources, referral sites, and steps to take for the establishment of hospital-based domestic violence programs. The Women s Health Program contributed to the content of the toolkit. Prince George s Hospital Center implemented a new hospital-based domestic violence program in To commemorate the new program, a documentary film, Domestic Violence and Health Care: Best Practices in Action was premiered at the hospital. The movie featured interviews with many Baltimore health care professionals and will serve to increase awareness of abuse. A research article, Intimate Partner Homicide Among Pregnant and Postpartum Women, by Drs. Diana Cheng (CMCH) and Isabelle Horon (Maryland Vital Statistics Administration) was published in the June 2010 issue of Obstetrics & Gynecology. Pregnancy Risk Assessment Monitoring System (PRAMS) The Center for Maternal and Child Health works with the CDC on PRAMS to survey mothers who have recently delivered live born infants in Maryland. Approximately 2,000 women are surveyed each year. Recent data analyses using Maryland PRAMS data includethe Maryland PRAMS Report: 2009 Births, Maryland PRAMS Report Births, and focus briefs entitled Alcohol Use During Pregnancy, Medicaid Births, and Comments from Postpartum Mothers. These reports are available at 13

15 VII. Summary Maryland continues to experience high maternal mortality compared to the US average and the Healthy People 2010 goal of 3.3 deaths per 100,000 live births. The use of multiple sources for identifying pregnancy-associated deaths and extending the definition of maternal death to one year after delivery has resulted in a more complete detection of cases and review of non-medical causes of death such as substance abuse. Information identified in the maternal mortality review process will continue to be incorporated into activities throughout the State by members of the Department, MedChi, and their perinatal partners in an effort to eliminate preventable maternal deaths. Cardiac disease and diabetes are two areas for medical intervention in the provision of health services to pregnant and postpartum women that can impact the risk of maternal mortality. Additional areas of work include conducting injury workups and enhancing medical records information. Some of these efforts can be addressed immediately, while others may require long-term advocacy and educational intervention. VIII. Acknowledgements The review of deaths would not be possible without the data, cooperation, and expertise of the Department of Health and Mental Hygiene s Vital Statistics Administration and the Office of the Chief Medical Examiner. The Maternal Mortality Review Committee would like to offer special thanks to the volunteer members of MedChi s MCH Committee, chaired by Lillian Blackmon, M.D., and those who joined the Maternal Mortality Policy Subcommittee for the hours spent in discussion and the serious attention given to this important public health project. 14

On behalf of the Association of Maternal and Child Health Programs (AMCHP), I am
, I am") Christopher Kus, M.D., M.P.H. Association of Maternal and Child Health Programs, Public Witness Testimony House Labor, Health and Human Services and Education Appropriations Subcommittee March 13, 2013
Christopher Kus, M.D., M.P.H. Association of Maternal and Child Health Programs, Public Witness Testimony House Labor, Health and Human Services and Education Appropriations Subcommittee March 13, 2013
No. 125 April 2001. Enhanced Surveillance of Maternal Mortality in North Carolina
 CHIS Studies North Carolina Public Health A Special Report Series by the 1908 Mail Service Center, Raleigh, N.C. 27699-1908 www.schs.state.nc.us/schs/ No. 125 April 2001 Enhanced Surveillance of Maternal
CHIS Studies North Carolina Public Health A Special Report Series by the 1908 Mail Service Center, Raleigh, N.C. 27699-1908 www.schs.state.nc.us/schs/ No. 125 April 2001 Enhanced Surveillance of Maternal
in children less than one year old. It is commonly divided into two categories, neonatal
 INTRODUCTION Infant Mortality Rate is one of the most important indicators of the general level of health or well being of a given community. It is a measure of the yearly rate of deaths in children less
INTRODUCTION Infant Mortality Rate is one of the most important indicators of the general level of health or well being of a given community. It is a measure of the yearly rate of deaths in children less
MARYLAND MATERNAL MORTALITY REVIEW 2014 ANNUAL REPORT
 MARYLAND DEPARTMENT OF HEALTH AND MENTAL HYGIENE PREVENTION AND HEALTH PROMOTION ADMINISTRATION MARYLAND MATERNAL MORTALITY REVIEW 04 ANNUAL REPORT Health General Article 3-07 Martin O Malley Governor
MARYLAND DEPARTMENT OF HEALTH AND MENTAL HYGIENE PREVENTION AND HEALTH PROMOTION ADMINISTRATION MARYLAND MATERNAL MORTALITY REVIEW 04 ANNUAL REPORT Health General Article 3-07 Martin O Malley Governor
Develop strategies to increase provider participation.
 Critical Component: Access to Health Insurance and Medical Homes Goal 1: Comprehensive Medical Home for Mother and Child * A. Increase the percentage of mothers and children 0-5 who have access to a medical
Critical Component: Access to Health Insurance and Medical Homes Goal 1: Comprehensive Medical Home for Mother and Child * A. Increase the percentage of mothers and children 0-5 who have access to a medical
Meena Abraham, DrPH, MPH Director of Epidemiology Services Baltimore City Health Department
 Meena Abraham, DrPH, MPH Director of Epidemiology Services Baltimore City Health Department 271 Neighborhood Statistical Areas 55 Community Statistical Areas 26 Zip Codes Characteristic Baltimore City
Meena Abraham, DrPH, MPH Director of Epidemiology Services Baltimore City Health Department 271 Neighborhood Statistical Areas 55 Community Statistical Areas 26 Zip Codes Characteristic Baltimore City
GAO VIOLENCE AGAINST WOMEN. Data on Pregnant Victims and Effectiveness of Prevention Strategies Are Limited
 GAO United States General Accounting Office Report to the Honorable Eleanor Holmes Norton, House of Representatives May 2002 VIOLENCE AGAINST WOMEN Data on Pregnant Victims and Effectiveness of Prevention
GAO United States General Accounting Office Report to the Honorable Eleanor Holmes Norton, House of Representatives May 2002 VIOLENCE AGAINST WOMEN Data on Pregnant Victims and Effectiveness of Prevention
A Strategic Plan for Improving Preconception Health and Health Care: Recommendations from the CDC Select Panel on Preconception Care
 1 A Strategic Plan for Improving Preconception Health and Health Care: Recommendations from the CDC Select Panel on Preconception Care Presentation by Kay A. Johnson, MPH, EdM Research Assistant Professor,
1 A Strategic Plan for Improving Preconception Health and Health Care: Recommendations from the CDC Select Panel on Preconception Care Presentation by Kay A. Johnson, MPH, EdM Research Assistant Professor,
Pregnancy-Related Deaths Due to Cardiomyopathy - Florida, 1999-2010
 Pregnancy-Related Deaths Due to Cardiomyopathy - Florida, 1999-2010 THE FLORIDA PREGNANCY-ASSOCIATED MORTALITY REVIEW (FL-PAMR), 1999-2010 Funded through Title V MCH Block Grant FL-PAMR HISTORY In 1996,
Pregnancy-Related Deaths Due to Cardiomyopathy - Florida, 1999-2010 THE FLORIDA PREGNANCY-ASSOCIATED MORTALITY REVIEW (FL-PAMR), 1999-2010 Funded through Title V MCH Block Grant FL-PAMR HISTORY In 1996,
Graduate Student Internship Program
 Maternal and Child Health Information Resource Center Graduate Student Internship Program To promote training in MCH Epidemiology Real-World Experience in: Data Analysis and Monitoring Needs Assessment
Maternal and Child Health Information Resource Center Graduate Student Internship Program To promote training in MCH Epidemiology Real-World Experience in: Data Analysis and Monitoring Needs Assessment
TITLE V OF THE SOCIAL SECURITY ACT MATERNAL AND CHILD HEALTH INFANT MORTALITY EFFORTS
 TITLE V OF THE SOCIAL SECURITY ACT MATERNAL AND CHILD HEALTH INFANT MORTALITY EFFORTS Michele H. Lawler, M.S., R.D. Department of Health and Human Services Health Resources and Services Administration
TITLE V OF THE SOCIAL SECURITY ACT MATERNAL AND CHILD HEALTH INFANT MORTALITY EFFORTS Michele H. Lawler, M.S., R.D. Department of Health and Human Services Health Resources and Services Administration
Access to Care / Care Utilization for Nebraska s Women
 Access to Care / Care Utilization for Nebraska s Women According to the Current Population Survey (CPS), in 2013, 84.6% of Nebraska women ages 18-44 had health insurance coverage, however only 58.2% of
Access to Care / Care Utilization for Nebraska s Women According to the Current Population Survey (CPS), in 2013, 84.6% of Nebraska women ages 18-44 had health insurance coverage, however only 58.2% of
LOUISIANA DEPARTMENT OF HEALTH AND HOSPITALS MATERNAL AND CHILD HEALTH (MCH) BLOCK GRANT*
 BLOCK GRANT*") LOUISIANA DEPARTMENT OF HEALTH AND HOSPITALS MATERNAL AND CHILD HEALTH (MCH) BLOCK GRANT* What is the MCH Block Grant? It is a grant from the U.S. government to State governments. The state must supply
LOUISIANA DEPARTMENT OF HEALTH AND HOSPITALS MATERNAL AND CHILD HEALTH (MCH) BLOCK GRANT* What is the MCH Block Grant? It is a grant from the U.S. government to State governments. The state must supply
Chapter 3: Healthy Start Risk Screening
 Introduction Healthy Start legislation requires that all pregnant women and infants be offered screening for risk factors that may affect their pregnancy, health, or development. The prenatal and infant
Introduction Healthy Start legislation requires that all pregnant women and infants be offered screening for risk factors that may affect their pregnancy, health, or development. The prenatal and infant
Wendy Martinez, MPH, CPH County of San Diego, Maternal, Child & Adolescent Health
 Wendy Martinez, MPH, CPH County of San Diego, Maternal, Child & Adolescent Health Describe local trends in birth Identify 3 perinatal health problems Identify 3 leading causes of infant death Age Class
Wendy Martinez, MPH, CPH County of San Diego, Maternal, Child & Adolescent Health Describe local trends in birth Identify 3 perinatal health problems Identify 3 leading causes of infant death Age Class
Adolescent Mortality. Alaska s adolescent mortality rate is 29% higher than the national rate and almost 1.6 times the Healthy People 2010 target.
 Alaska Maternal and Child Health Data Book 23 15 Adolescent Mortality Nationally, unintentional injury, assault and suicide account for 51% of deaths among adolescents ages 1-14 years in 2. Over the last
Alaska Maternal and Child Health Data Book 23 15 Adolescent Mortality Nationally, unintentional injury, assault and suicide account for 51% of deaths among adolescents ages 1-14 years in 2. Over the last
Populations of Color in Minnesota
 Populations of Color in Minnesota Health Status Report Update Summary Spring 2009 Center for Health Statistics Minnesota Department of Health TABLE OF CONTENTS BACKGROUND... 1 PART I: BIRTH-RELATED HEALTH
Populations of Color in Minnesota Health Status Report Update Summary Spring 2009 Center for Health Statistics Minnesota Department of Health TABLE OF CONTENTS BACKGROUND... 1 PART I: BIRTH-RELATED HEALTH
Flagship Priority: Mental Health and Substance Abuse
 10 Colorado s winnable battles Flagship Priority: Mental Health and Substance Abuse ELEVATING HEALTH AND ENVIRONMENT Mental and emotional well-being is essential to shaping a state of health for Coloradans.
10 Colorado s winnable battles Flagship Priority: Mental Health and Substance Abuse ELEVATING HEALTH AND ENVIRONMENT Mental and emotional well-being is essential to shaping a state of health for Coloradans.
World Health Day Diabetes and RMNCAH in Africa: R for Reproductive Health
 World Health Day Diabetes and RMNCAH in Africa: R for Reproductive Health Managing diabetes and reproductive health in developing contexts. The 2016 World Health Day theme to scale up prevention, strengthen
World Health Day Diabetes and RMNCAH in Africa: R for Reproductive Health Managing diabetes and reproductive health in developing contexts. The 2016 World Health Day theme to scale up prevention, strengthen
Health Care Access to Vulnerable Populations
 Health Care Access to Vulnerable Populations Closing the Gap: Reducing Racial and Ethnic Disparities in Florida Rosebud L. Foster, ED.D. Access to Health Care The timely use of personal health services
Health Care Access to Vulnerable Populations Closing the Gap: Reducing Racial and Ethnic Disparities in Florida Rosebud L. Foster, ED.D. Access to Health Care The timely use of personal health services
FAMILY HEALTH SERVICES DIVISION Profiles 2014 OVERVIEW
 FAMILY HEALTH SERVICES DIVISION Profiles 2014 OVERVIEW Family Health Services Division Overview Data Sources Life Course Perspective and Title V Priorities Population Overview Births Infant Mortality Chapter
FAMILY HEALTH SERVICES DIVISION Profiles 2014 OVERVIEW Family Health Services Division Overview Data Sources Life Course Perspective and Title V Priorities Population Overview Births Infant Mortality Chapter
Racial and Ethnic Disparities in Maternal Mortality in the United States
 Racial and Ethnic Disparities in Maternal Mortality in the United States KYRIAKOS S. MARKIDES, PHD UNIVERSITY OF TEXAS MEDICAL BRANCH GALVESTON, TEXAS PRESENTED AT THE HOWARD TAYLOR INTERNATIONAL SYMPOSIUM
Racial and Ethnic Disparities in Maternal Mortality in the United States KYRIAKOS S. MARKIDES, PHD UNIVERSITY OF TEXAS MEDICAL BRANCH GALVESTON, TEXAS PRESENTED AT THE HOWARD TAYLOR INTERNATIONAL SYMPOSIUM
Implementation Plan for Needs Identified in the Community Health Needs Assessment for Spectrum Health Hospitals d/b/a Spectrum Health Grand Rapids
 Implementation Plan for Needs Identified in the Community Health Needs Assessment for Spectrum Health Hospitals d/b/a Spectrum Health Grand Rapids FY 2013-2015 Covered Facilities: Spectrum Health Hospitals
Implementation Plan for Needs Identified in the Community Health Needs Assessment for Spectrum Health Hospitals d/b/a Spectrum Health Grand Rapids FY 2013-2015 Covered Facilities: Spectrum Health Hospitals
The National Survey of Children s Health 2011-2012 The Child
 The National Survey of Children s 11-12 The Child The National Survey of Children s measures children s health status, their health care, and their activities in and outside of school. Taken together,
The National Survey of Children s 11-12 The Child The National Survey of Children s measures children s health status, their health care, and their activities in and outside of school. Taken together,
VIRGINIA S 2015 MATERNAL AND CHILD HEALTH BLOCK GRANT (Title V) Virginia Department of Health Executive Summary
 Virginia Department of Health Executive Summary") VIRGINIA S 2015 MATERNAL AND CHILD HEALTH BLOCK GRANT (Title V) Virginia Department of Health Executive Summary May 2014 1 VIRGINIA S 2015 MATERNAL AND CHILD HEALTH BLOCK GRANT (Title V) Virginia Department
VIRGINIA S 2015 MATERNAL AND CHILD HEALTH BLOCK GRANT (Title V) Virginia Department of Health Executive Summary May 2014 1 VIRGINIA S 2015 MATERNAL AND CHILD HEALTH BLOCK GRANT (Title V) Virginia Department
SCREENING FOR INTIMATE PARTNER VIOLENCE IN THE PRIMARY CARE SETTING
 SCREENING FOR INTIMATE PARTNER VIOLENCE IN THE PRIMARY CARE SETTING Partner violence can affect one third of the patients cared for in the primary care setting. The primary care setting offers an opportunity
SCREENING FOR INTIMATE PARTNER VIOLENCE IN THE PRIMARY CARE SETTING Partner violence can affect one third of the patients cared for in the primary care setting. The primary care setting offers an opportunity
Intimate Partner Violence among Pregnant and Parenting Women: Local Health Department Strategies for Assessment, Intervention, and Prevention
 ISSUE BRIEF June 2008 Intimate Partner Violence among Pregnant and Parenting Women: Local Health Department Strategies for Assessment, Intervention, and Prevention Introduction This issue brief illustrates
ISSUE BRIEF June 2008 Intimate Partner Violence among Pregnant and Parenting Women: Local Health Department Strategies for Assessment, Intervention, and Prevention Introduction This issue brief illustrates
BabyFirst Solano Perinatal Substance Abuse Project
 BabyFirst Solano Perinatal Substance Abuse Project MCH PHLI Leadership May 2011 Maternal, Child & Adolescent Health Bureau 1 The Perinatal Substance Abuse Project is designed to help babies be born substance
BabyFirst Solano Perinatal Substance Abuse Project MCH PHLI Leadership May 2011 Maternal, Child & Adolescent Health Bureau 1 The Perinatal Substance Abuse Project is designed to help babies be born substance
Appendices. 2006 Bexar County Community Health Assessment Appendices Appendix A 125
 Appendices Appendix A Recent reports suggest that the number of mothers seeking dropped precipitously between 2004 and 2005. Tables 1A and 1B, below, shows information since 1990. The trend has been that
Appendices Appendix A Recent reports suggest that the number of mothers seeking dropped precipitously between 2004 and 2005. Tables 1A and 1B, below, shows information since 1990. The trend has been that
Chapter 13: Transition and Interagency Agreements
 Healthy Start Standards & Guidelines 2007 Chapter 13: Transition and Interagency Agreements Introduction Transition is movement or change from one environment to another. Transition activities are a critical
Healthy Start Standards & Guidelines 2007 Chapter 13: Transition and Interagency Agreements Introduction Transition is movement or change from one environment to another. Transition activities are a critical
Iowa s Maternal Health, Child Health and Family Planning Business Plan
 Iowa s Maternal Health, Child Health and Family Planning Business Plan CHILD HEALTH Who we are... A public-private partnership that... Promotes access to regular preventive health care services for children
Iowa s Maternal Health, Child Health and Family Planning Business Plan CHILD HEALTH Who we are... A public-private partnership that... Promotes access to regular preventive health care services for children
Contra Costa County Fetal Infant Mortality Review Program
 Contra Costa County Fetal Infant Mortality Review Program Suzzette C. Johnson, MSW MPA Sylvia V. Taqi-Eddin, MA-CP Family, Maternal and Child Health Programs Contra Costa Health Services National NFIMR
Contra Costa County Fetal Infant Mortality Review Program Suzzette C. Johnson, MSW MPA Sylvia V. Taqi-Eddin, MA-CP Family, Maternal and Child Health Programs Contra Costa Health Services National NFIMR
Pregnant and Parenting Youth in Foster Care in Washington State: Comparison to Other Teens and Young Women who Gave Birth
 January 2014 RDA Report 11.202 Olympia, Washington Pregnant and Parenting in Care in Washington State: Comparison to Other and Women who Gave Birth Laurie Cawthon, MD, MPH Barbara Lucenko, PhD Peter Woodcox,
January 2014 RDA Report 11.202 Olympia, Washington Pregnant and Parenting in Care in Washington State: Comparison to Other and Women who Gave Birth Laurie Cawthon, MD, MPH Barbara Lucenko, PhD Peter Woodcox,
Child Abuse and Neglect AAP Policy Recommendations
 Child Abuse and Neglect AAP Policy Recommendations When Inflicted Skin Injuries Constitute Child Abuse Committee on Child Abuse and Neglect PEDIATRICS Vol. 110 No. 3 September 2002, pp. 644-645 Recommendations
Child Abuse and Neglect AAP Policy Recommendations When Inflicted Skin Injuries Constitute Child Abuse Committee on Child Abuse and Neglect PEDIATRICS Vol. 110 No. 3 September 2002, pp. 644-645 Recommendations
WATCH OWCH Office of Women s and Children s Health
 WATCH OWCH Office of Women s and Children s Health 150 N. 18th Avenue, Suite 320 Phoenix, AZ 85007-3242 Telephone: (602) 364-1400 Fall 2006 COMMUNITY HEALTH GRANTS The Office of Women s and Children s
WATCH OWCH Office of Women s and Children s Health 150 N. 18th Avenue, Suite 320 Phoenix, AZ 85007-3242 Telephone: (602) 364-1400 Fall 2006 COMMUNITY HEALTH GRANTS The Office of Women s and Children s
Alabama s Rural and Urban Counties
 Selected Indicators of Health Status in Alabama Alabama s Rural and Urban Counties Jointly produced to assist those seeking to improve health care in rural Alabama by The Office of Primary Care and Rural
Selected Indicators of Health Status in Alabama Alabama s Rural and Urban Counties Jointly produced to assist those seeking to improve health care in rural Alabama by The Office of Primary Care and Rural
Logic Model for SECCS Grant Program: Florida Early Childhood Comprehensive Systems (ECCS) Statewide Plan INTERVENTION
 Statewide Plan INTERVENTION") TOTAL FUNDS REQUESTED (for GRANTEE/ PROJECT CHARACTERISTICS (i.e., the first year of the project): goals and description of the project, $155,496 Infant Mental Health Association Updated Florida's statewide
TOTAL FUNDS REQUESTED (for GRANTEE/ PROJECT CHARACTERISTICS (i.e., the first year of the project): goals and description of the project, $155,496 Infant Mental Health Association Updated Florida's statewide
HEAD START PERFORMANCE STANDARDS W/ MENTAL HEALTH FOCUS
 HEAD START PERFORMANCE STANDARDS W/ MENTAL HEALTH FOCUS This list represents a variety of Head Start Performance Standards that include some aspect of mental health; however, it is not exhaustive of every
HEAD START PERFORMANCE STANDARDS W/ MENTAL HEALTH FOCUS This list represents a variety of Head Start Performance Standards that include some aspect of mental health; however, it is not exhaustive of every
Cardiovascular Disease and Maternal Mortality what do we know and what are the key questions?
 Cardiovascular Disease and Maternal Mortality what do we know and what are the key questions? AFSHAN HAMEED, MD, FACOG, FACC Associate Clinical Professor Maternal Fetal Medicine and Cardiology University
Cardiovascular Disease and Maternal Mortality what do we know and what are the key questions? AFSHAN HAMEED, MD, FACOG, FACC Associate Clinical Professor Maternal Fetal Medicine and Cardiology University
Testimony of the American College of Nurse-Midwives. at a Hearing of the House Committee on Energy and Commerce Subcommittee on Health.
 Testimony of the American College of Nurse-Midwives at a Hearing of the House Committee on Energy and Commerce Subcommittee on Health on the Improving Access to Maternity Care Act (H.R.1209) Wednesday,
Testimony of the American College of Nurse-Midwives at a Hearing of the House Committee on Energy and Commerce Subcommittee on Health on the Improving Access to Maternity Care Act (H.R.1209) Wednesday,
WHEREAS, the Medicaid Program operates the Maryland Children s Health Program as a Medicaid expansion with the full benefit package and;
 COOPERATIVE AGREEMENT between MARYLAND STATE DEPARTMENT OF HEALTH AND MENTAL HYGIENE TITLE XIX MEDICAID AGENCY, TITLE V MATERIAL AND CHILD HEALTH AGENCY AND THE SPECIAL SUPPLEMENTAL NUTRITION PROGRAM FOR
COOPERATIVE AGREEMENT between MARYLAND STATE DEPARTMENT OF HEALTH AND MENTAL HYGIENE TITLE XIX MEDICAID AGENCY, TITLE V MATERIAL AND CHILD HEALTH AGENCY AND THE SPECIAL SUPPLEMENTAL NUTRITION PROGRAM FOR
Malisett Health and Wellness Center, Littleton, Maine Photo credit: Flickr/BlakeGumprecht. Reducing Disparities in the Federal Health Care Budget
 Malisett Health and Wellness Center, Littleton, Maine Photo credit: Flickr/BlakeGumprecht Health Care Reducing Disparities in the Federal Health Care Budget The survival and prosperity of tribal communities
Malisett Health and Wellness Center, Littleton, Maine Photo credit: Flickr/BlakeGumprecht Health Care Reducing Disparities in the Federal Health Care Budget The survival and prosperity of tribal communities
Violence Assessment and Follow-up In Public Health Data Sets
 Violence Assessment and Follow-up In Public Health Data Sets Background Summer, 2012 This project was initiated to explore existing data on assessment of violence in the lives of women seeking services
Violence Assessment and Follow-up In Public Health Data Sets Background Summer, 2012 This project was initiated to explore existing data on assessment of violence in the lives of women seeking services
Early Childhood Indicators Report
 2015 Early Childhood Indicators Report Carol Prentice, Prentice Consulting, 2012 Updated by Alaska Department of Health & Social Services, September 2013 Updated by Prentice Consulting, July 2015 Early
2015 Early Childhood Indicators Report Carol Prentice, Prentice Consulting, 2012 Updated by Alaska Department of Health & Social Services, September 2013 Updated by Prentice Consulting, July 2015 Early
Public Health Nurse Home Visiting Frequently Asked Questions When did nurse home visiting begin?
 Public Health Nurse Home Visiting Frequently Asked Questions When did nurse home visiting begin? Home visiting became a national public health strategy to improve the health status of women and children
Public Health Nurse Home Visiting Frequently Asked Questions When did nurse home visiting begin? Home visiting became a national public health strategy to improve the health status of women and children
Perinatal Substance Use: Promoting Healthy Outcomes
 A Guide for Hospitals and Health Care Providers Perinatal Substance Use: Promoting Healthy Outcomes Virginia Legal Requirements and Health Care Practice Implications Perinatal Care To promote healthy maternal
A Guide for Hospitals and Health Care Providers Perinatal Substance Use: Promoting Healthy Outcomes Virginia Legal Requirements and Health Care Practice Implications Perinatal Care To promote healthy maternal
Borgess Health Implementation Strategy
 Borgess Health Implementation Strategy Implementation Strategy Narrative Overview Borgess Medical Center is a 422-bed tertiary care hospital and the flagship of Borgess Health with a continuum of health
Borgess Health Implementation Strategy Implementation Strategy Narrative Overview Borgess Medical Center is a 422-bed tertiary care hospital and the flagship of Borgess Health with a continuum of health
Public Health Services
 Public Health Services FUNCTION The functions of the Public Health Services programs are to protect and promote the health and safety of County residents. This is accomplished by monitoring health status
Public Health Services FUNCTION The functions of the Public Health Services programs are to protect and promote the health and safety of County residents. This is accomplished by monitoring health status
Promoting Family Planning
 Promoting Family Planning INTRODUCTION Voluntary family planning has been widely adopted throughout the world. More than half of all couples in the developing world now use a modern method of contraception
Promoting Family Planning INTRODUCTION Voluntary family planning has been widely adopted throughout the world. More than half of all couples in the developing world now use a modern method of contraception
How To Stop A Pregnant Addict From Getting A Jail Sentence For Drug Use
 Case: 3:14-cv-00870-jdp Document #: 14-9 Filed: 01/07/15 Page 1 of 6 APPENDIX 8 Case: 3:14-cv-00870-jdp Document #: 14-9 Filed: 01/07/15 Page 2 of 6 AMERICAN MEDICAL ASSOCIATION Pregnant women will be
Case: 3:14-cv-00870-jdp Document #: 14-9 Filed: 01/07/15 Page 1 of 6 APPENDIX 8 Case: 3:14-cv-00870-jdp Document #: 14-9 Filed: 01/07/15 Page 2 of 6 AMERICAN MEDICAL ASSOCIATION Pregnant women will be
METHODOLOGICAL ISSUES IN THE MEASURES OF MATERNAL MORBIDITY MORTALITY (MM 1 MM 2 ) Dr. AKO Simon
 Dr. AKO Simon") (1) METHODOLOGICAL ISSUES IN THE MEASURES OF MATERNAL MORBIDITY MORTALITY (MM 1 MM 2 ) Dr. AKO Simon Postgraduate Research Training in Reproductive Health 2004 Faculty of Medicine, University of Yaounde
(1) METHODOLOGICAL ISSUES IN THE MEASURES OF MATERNAL MORBIDITY MORTALITY (MM 1 MM 2 ) Dr. AKO Simon Postgraduate Research Training in Reproductive Health 2004 Faculty of Medicine, University of Yaounde
The Friends of HRSA is a non-partisan coalition of more than 170 national organizations
 Friends of the Health Resources and Services Administration c/o American Public Health Association 800 I Street NW Washington DC, 20001 202-777-2513 Nicole Burda, Government Relations Deputy Director Testimony
Friends of the Health Resources and Services Administration c/o American Public Health Association 800 I Street NW Washington DC, 20001 202-777-2513 Nicole Burda, Government Relations Deputy Director Testimony
A Guide for Hospitals and Health Care Providers Perinatal Substance Use: Promoting Healthy Outcomes
 A Guide for Hospitals and Health Care Providers Perinatal Substance Use: Promoting Healthy Outcomes Virginia Legal Requirements and Health Care Practice Implications Perinatal Care To promote healthy maternal
A Guide for Hospitals and Health Care Providers Perinatal Substance Use: Promoting Healthy Outcomes Virginia Legal Requirements and Health Care Practice Implications Perinatal Care To promote healthy maternal
MATERNAL AND CHILD HEALTH BRIEF #2:
 MATERNAL AND CHILD HEALTH BRIEF #2: OBESITY AMONG CHILDREN AND ADOLESCENTS SEPTEMBER 2012 OBESITY DEFINED Obesity and overweight are typically measured OVERVIEW in terms of Body Mass Index or BMI. BMI
MATERNAL AND CHILD HEALTH BRIEF #2: OBESITY AMONG CHILDREN AND ADOLESCENTS SEPTEMBER 2012 OBESITY DEFINED Obesity and overweight are typically measured OVERVIEW in terms of Body Mass Index or BMI. BMI
Overview. Key Flu Vaccine Coverage Findings. Summary
 2013-14 Season Flu Vaccine Coverage and Hospital Quality Data Centers for Disease Control and Prevention Highlights and Data Summary September 18, 2014 Overview Flu is unpredictable. Even healthy children
2013-14 Season Flu Vaccine Coverage and Hospital Quality Data Centers for Disease Control and Prevention Highlights and Data Summary September 18, 2014 Overview Flu is unpredictable. Even healthy children
2014-16. Orange County Health Improvement Plan. 2014 Annual Report. www.ochealthiertogether.org
 2014-16 Orange County Health Improvement Plan 2014 Annual Report www.ochealthiertogether.org The Orange County Health Improvement Plan (OCHIP) was published in May 2014 for the time period January 2014-December
2014-16 Orange County Health Improvement Plan 2014 Annual Report www.ochealthiertogether.org The Orange County Health Improvement Plan (OCHIP) was published in May 2014 for the time period January 2014-December
Motor Vehicle Deaths Updated: August 2014
 Motor Vehicle Deaths Updated: Motor vehicle death rates rise rapidly during the teen years and remain very high into early adulthood. The rate for teens, however, has followed a downward trend for most
Motor Vehicle Deaths Updated: Motor vehicle death rates rise rapidly during the teen years and remain very high into early adulthood. The rate for teens, however, has followed a downward trend for most
Preventing Pediatric Diabetes: Are Racial Disparities A Factor? A Children s Health Fund Issue Brief February 2004
 Preventing Pediatric Diabetes: Are Racial Disparities A Factor? A Children s Health Fund Issue Brief February 2004 The Children s Health Fund The Children s Health Fund (CHF), working with hospitals and
Preventing Pediatric Diabetes: Are Racial Disparities A Factor? A Children s Health Fund Issue Brief February 2004 The Children s Health Fund The Children s Health Fund (CHF), working with hospitals and
Graduate Student Epidemiology Program
 Graduate Student Epidemiology Program To promote training in MCH Epidemiology Real-World Experience in: Data Analysis and Monitoring Needs Assessment Program Evaluation 2014 Program Guide Submit your application
Graduate Student Epidemiology Program To promote training in MCH Epidemiology Real-World Experience in: Data Analysis and Monitoring Needs Assessment Program Evaluation 2014 Program Guide Submit your application
A Descriptive Study of Depression, Substance Abuse, and Intimate Partner Violence Among Pregnant Women
 A Descriptive Study of Depression, Substance Abuse, and Intimate Partner Violence Among Pregnant Women 1 OVERVIEW This presentation is based on the study of pregnant women enrolled in the Augusta Partnership
A Descriptive Study of Depression, Substance Abuse, and Intimate Partner Violence Among Pregnant Women 1 OVERVIEW This presentation is based on the study of pregnant women enrolled in the Augusta Partnership
ARE FLORIDA'S CHILDREN BORN HEALTHY AND DO THEY HAVE HEALTH INSURANCE?
 infant mortality rate per 1,000 live births ARE FLORIDA'S CHILDREN BORN HEALTHY AND DO THEY HAVE HEALTH INSURANCE? Too Many of Florida's Babies Die at Birth, Particularly African American Infants In the
infant mortality rate per 1,000 live births ARE FLORIDA'S CHILDREN BORN HEALTHY AND DO THEY HAVE HEALTH INSURANCE? Too Many of Florida's Babies Die at Birth, Particularly African American Infants In the
Denver County Births and Deaths 2013
 Denver County Births and Deaths 2013 Selected birth characteristics: County residents, 2013... 2 Selected birth characteristics by age group of mother: County residents, 2013... 3 Selected birth characteristics
Denver County Births and Deaths 2013 Selected birth characteristics: County residents, 2013... 2 Selected birth characteristics by age group of mother: County residents, 2013... 3 Selected birth characteristics
COLORADO REVISED STATUTES
 COLORADO REVISED STATUTES *** This document reflects changes current through all laws passed at the First Regular Session of the Sixty-Ninth General Assembly of the State of Colorado (2013) *** TITLE 25.
COLORADO REVISED STATUTES *** This document reflects changes current through all laws passed at the First Regular Session of the Sixty-Ninth General Assembly of the State of Colorado (2013) *** TITLE 25.
Maternal and Neonatal Health in Bangladesh
 Maternal and Neonatal Health in Bangladesh KEY STATISTICS Basic data Maternal mortality ratio (deaths per 100,000 births) 320* Neonatal mortality rate (deaths per 1,000 births) 37 Births for women aged
Maternal and Neonatal Health in Bangladesh KEY STATISTICS Basic data Maternal mortality ratio (deaths per 100,000 births) 320* Neonatal mortality rate (deaths per 1,000 births) 37 Births for women aged
Quality Maternity Care: the Role of the Public Health Nurse
 Quality Maternity Care: the Role of the Public Health Nurse Lori Webel-Edgar RN, MN Program Manager-Reproductive Health Simcoe Muskoka District Health Unit Barrie, Ontario session overview quality maternity
Quality Maternity Care: the Role of the Public Health Nurse Lori Webel-Edgar RN, MN Program Manager-Reproductive Health Simcoe Muskoka District Health Unit Barrie, Ontario session overview quality maternity
New York State Strategic Plan for. Elimination of Mother-to-Child Transmission of HIV
 New York State Strategic Plan for Elimination of Mother-to-Child Transmission of HIV Introduction Brief Background New York, once the state with the highest reported number of children with AIDS, has made
New York State Strategic Plan for Elimination of Mother-to-Child Transmission of HIV Introduction Brief Background New York, once the state with the highest reported number of children with AIDS, has made
Medical Care Costs for Diabetes Associated with Health Disparities Among Adults Enrolled in Medicaid in North Carolina
 No. 160 August 2009 Among Adults Enrolled in Medicaid in North Carolina by Paul A. Buescher, Ph.D. J. Timothy Whitmire, Ph.D. Barbara Pullen-Smith, M.P.H. A Joint Report from the and the Office of Minority
No. 160 August 2009 Among Adults Enrolled in Medicaid in North Carolina by Paul A. Buescher, Ph.D. J. Timothy Whitmire, Ph.D. Barbara Pullen-Smith, M.P.H. A Joint Report from the and the Office of Minority
New Jersey Home Visiting Initiative
 National Health Policy Forum Promoting Evidence-Based Interventions: Maternal, Infant & Early Childhood Home Visiting (MIECHV) A State Perspective on Home Visiting New Jersey Home Visiting Initiative Contact
National Health Policy Forum Promoting Evidence-Based Interventions: Maternal, Infant & Early Childhood Home Visiting (MIECHV) A State Perspective on Home Visiting New Jersey Home Visiting Initiative Contact
http://english.gov.cn/laws/2005-08/24/content_25746.htm
 Page 1 of 5 Measures for Implementation of the Law of the People's Republic of China on Maternal and Infant Care (Promulgated by Decree No.308 of the State Council of the People's Republic of China on
Page 1 of 5 Measures for Implementation of the Law of the People's Republic of China on Maternal and Infant Care (Promulgated by Decree No.308 of the State Council of the People's Republic of China on
March of Dimes 2016 Chapter Community Grants Program
 March of Dimes 2016 Chapter Community Grants Program Community Award Application March of Dimes Maryland National Capital Area Chapter 175 West Ostend St., Suite C-2 Baltimore, MD 21230 Marchofdimes.org/marylandmetrodc
March of Dimes 2016 Chapter Community Grants Program Community Award Application March of Dimes Maryland National Capital Area Chapter 175 West Ostend St., Suite C-2 Baltimore, MD 21230 Marchofdimes.org/marylandmetrodc
Healthy Families, Better Beginnings
 Healthy Families, Better Beginnings 213 A REPORT ON THE HEALTH OF WOMEN, CHILDREN, AND FAMILIES IN SPOKANE Community Health Assessment, Planning, and Evaluation 111 West College Avenue, Spokane, WA 9921-295
Healthy Families, Better Beginnings 213 A REPORT ON THE HEALTH OF WOMEN, CHILDREN, AND FAMILIES IN SPOKANE Community Health Assessment, Planning, and Evaluation 111 West College Avenue, Spokane, WA 9921-295
Huron County Community Health Profile
 2014 Huron County Community Health Profile ` Prepared by: Eileen Unruh RN, MSN Samantha Fackler RN, MSN 11/1/2014 1 HURON COUNTY COMMUNITY HEALTH PROFILE TABLE OF CONTENTS INTRODUCTION.... 4 DEMOGRAPHICS...
2014 Huron County Community Health Profile ` Prepared by: Eileen Unruh RN, MSN Samantha Fackler RN, MSN 11/1/2014 1 HURON COUNTY COMMUNITY HEALTH PROFILE TABLE OF CONTENTS INTRODUCTION.... 4 DEMOGRAPHICS...
Children s Health and Nursing:
 Children s Health and Nursing: A Summary of the Issues What s the issue? The foundation for healthy growth and development in later years is established to a large degree in the first six years of life.
Children s Health and Nursing: A Summary of the Issues What s the issue? The foundation for healthy growth and development in later years is established to a large degree in the first six years of life.
State Health Assessment Health Priority Status Report Update. June 29, 2015 Presented by UIC SPH and IDPH
 State Health Assessment Health Priority Status Report Update June 29, 2015 Presented by UIC SPH and IDPH 1 Health Priority Presentation Objectives 1. Explain context of how this discussion fits into our
State Health Assessment Health Priority Status Report Update June 29, 2015 Presented by UIC SPH and IDPH 1 Health Priority Presentation Objectives 1. Explain context of how this discussion fits into our
Guidelines for States on Maternity Care In the Essential Health Benefits Package
 Guidelines for States on Maternity Care In the Essential Health Benefits Package Section 2707(a) of the Patient Protection and Affordable Care Act (ACA) requires that all new health insurance plans in
Guidelines for States on Maternity Care In the Essential Health Benefits Package Section 2707(a) of the Patient Protection and Affordable Care Act (ACA) requires that all new health insurance plans in
Joan Wightkin, DrPH jwight@lsuhsc.edu
 Joan Wightkin, DrPH jwight@lsuhsc.edu Education 2002 DrPH, Maternal and Child Health, Department of Community Health Sciences, Tulane University School of Public Health and Tropical Medicine 1978 MPH -
Joan Wightkin, DrPH jwight@lsuhsc.edu Education 2002 DrPH, Maternal and Child Health, Department of Community Health Sciences, Tulane University School of Public Health and Tropical Medicine 1978 MPH -
Statewide Risk Screening Program for Pregnant Women: SBIRT Program
 Statewide Risk Screening Program for Pregnant Women: SBIRT Program Louisiana Community/State Collaborative Michael Kudla,, M.D., FACOG Mary Craig, RN, MSN, MS February 22, 2007 Objectives Participants
Statewide Risk Screening Program for Pregnant Women: SBIRT Program Louisiana Community/State Collaborative Michael Kudla,, M.D., FACOG Mary Craig, RN, MSN, MS February 22, 2007 Objectives Participants
9/8/2014 EPIDEMIOLOGY PUBLIC HEALTH INTERVENTIONS FOR NEONATAL ABSTINENCE SYNDROME DISCLOSURE OBJECTIVES. No financial COI to disclose
 PUBLIC HEALTH INTERVENTIONS FOR NEONATAL ABSTINENCE SYNDROME DISCLOSURE No financial COI to disclose Eric Reynolds MD MPH OBJECTIVES To discuss the epidemiology and current scope of the Neonatal Abstinence
PUBLIC HEALTH INTERVENTIONS FOR NEONATAL ABSTINENCE SYNDROME DISCLOSURE No financial COI to disclose Eric Reynolds MD MPH OBJECTIVES To discuss the epidemiology and current scope of the Neonatal Abstinence
Prevention Agenda 2013 2017 is the state health improvement plan for the next five years.
 Prevention Agenda 2013 2017 is the state health improvement plan for the next five years. It builds on the current plan, the Prevention Agenda toward the Healthiest State. The Prevention Agenda (launched
Prevention Agenda 2013 2017 is the state health improvement plan for the next five years. It builds on the current plan, the Prevention Agenda toward the Healthiest State. The Prevention Agenda (launched
Health Disparities in H.R. 3590 (Merged Senate Bill)
") Health Disparities in H.R. 3590 (Merged Senate Bill) Definitions: Health disparity population is defined in the bill as defined in Section 485E (Sec. 931) Current Law: a population is a health disparity
Health Disparities in H.R. 3590 (Merged Senate Bill) Definitions: Health disparity population is defined in the bill as defined in Section 485E (Sec. 931) Current Law: a population is a health disparity
Model Domestic Violence Hospital Policy
 Model Domestic Violence Hospital Policy A public health approach to providing optimal care to patients who are or may be victims of domestic violence Project Coordinator: Mary Stuart Saint Francis Hospital
Model Domestic Violence Hospital Policy A public health approach to providing optimal care to patients who are or may be victims of domestic violence Project Coordinator: Mary Stuart Saint Francis Hospital
Access to Appropriate Services for High Risk. in New York State. New York State Department of Health
 Access to Appropriate Services for High Risk Neonates in New York State Di i i f F il H l h Division of Family Health New York State Department of Health Perinatal Regionalization in New York State Perinatal
Access to Appropriate Services for High Risk Neonates in New York State Di i i f F il H l h Division of Family Health New York State Department of Health Perinatal Regionalization in New York State Perinatal
Introduction to WIC. Objectives
 Objectives Introduction to WIC After completing this lesson, you will be able to: Describe the participants served by WIC. Describe how WIC improves the health of participants. Identify the history and
Objectives Introduction to WIC After completing this lesson, you will be able to: Describe the participants served by WIC. Describe how WIC improves the health of participants. Identify the history and
2015 HonorHealth Rehabilitation Hospital Community Health Needs Assessment. Approved by the Board Strategic Planning Committee October 2015
 2015 Community Health Needs Assessment Approved by the Board Strategic Planning Committee October 2015 Table of Contents Table of Contents... i Table of Figures... iv Table of Tables... v I. Executive
2015 Community Health Needs Assessment Approved by the Board Strategic Planning Committee October 2015 Table of Contents Table of Contents... i Table of Figures... iv Table of Tables... v I. Executive
The National Survey of Children s Health
 with Current Health Insurance, by Location 91.1 89.4.2.9 Current Health Insurance The survey asked parents if their children currently had coverage through any kind of health insurance, including private
with Current Health Insurance, by Location 91.1 89.4.2.9 Current Health Insurance The survey asked parents if their children currently had coverage through any kind of health insurance, including private
King County City Health Profile Vashon Island
 King County City Health Profile Vashon Island West Seattle North Highline Burien SeaTac/Tukwila Vashon Island Des Moines/Normandy Park Kent-West East Federal Way Fed Way-Dash Point/Woodmont December, 212
King County City Health Profile Vashon Island West Seattle North Highline Burien SeaTac/Tukwila Vashon Island Des Moines/Normandy Park Kent-West East Federal Way Fed Way-Dash Point/Woodmont December, 212
Chapter 16: Performance Based Contracts and Memoranda of Agreement
 Chapter 16: Performance Based Contracts and Memoranda of Agreement Introduction The following standards support activities that are: designated in statute and rule, necessary to accomplish implementation
Chapter 16: Performance Based Contracts and Memoranda of Agreement Introduction The following standards support activities that are: designated in statute and rule, necessary to accomplish implementation
Maternal and Child Health Indicators: Three State Profile
 Indicators: Three State Profile Elizabeth Oftedahl MPH Symposium Pyle Center, August 11, 2006 Preceptor: Kristin Hill, MSHA Mentor: Alexandra Adams, MD, PhD Great Lakes Inter-Tribal Council / Great Lakes
Indicators: Three State Profile Elizabeth Oftedahl MPH Symposium Pyle Center, August 11, 2006 Preceptor: Kristin Hill, MSHA Mentor: Alexandra Adams, MD, PhD Great Lakes Inter-Tribal Council / Great Lakes
Corporate Reimbursement Policy
 Corporate Reimbursement Policy Guidelines for Global Maternity Reimbursement File Name: Origination: Last Review: Next Review: guidelines_for_global_maternity_reimbursement 10/2003 7/2016 7/2017 Description
Corporate Reimbursement Policy Guidelines for Global Maternity Reimbursement File Name: Origination: Last Review: Next Review: guidelines_for_global_maternity_reimbursement 10/2003 7/2016 7/2017 Description
Substance-Exposed Newborns
 Substance-Exposed Newborns State of Oklahoma 2013 Substance-Exposed Newborns State of Oklahoma 2013 Legal Background Federal guidelines in the Child Abuse Prevention and Treatment Act (CAPTA) require states
Substance-Exposed Newborns State of Oklahoma 2013 Substance-Exposed Newborns State of Oklahoma 2013 Legal Background Federal guidelines in the Child Abuse Prevention and Treatment Act (CAPTA) require states
Roles of the Nurse Practitioner. Abby Smith. Auburn University/Auburn Montgomery
 Running Head: ROLES OF THE NURSE PRACTITIONER Roles of the Nurse Practitioner Abby Smith Auburn University/Auburn Montgomery 2 Abstract Advanced practice nursing has many roles in health care today, with
Running Head: ROLES OF THE NURSE PRACTITIONER Roles of the Nurse Practitioner Abby Smith Auburn University/Auburn Montgomery 2 Abstract Advanced practice nursing has many roles in health care today, with
Section IX Special Needs & Case Management
 Section IX Special Needs & Case Management Special Needs and Case Management 179 Integrated Care Management/Complex Case Management The Case Management/Care Coordination (CM/CC) program is a population-based
Section IX Special Needs & Case Management Special Needs and Case Management 179 Integrated Care Management/Complex Case Management The Case Management/Care Coordination (CM/CC) program is a population-based
MEMORANDUM. Dr. Michael Lu, Associate Administrator Maternal and Child Health Bureau, Health Resources and Services Administration
 MEMORANDUM TO: Dr. Michael Lu, Associate Administrator Maternal and Child Health Bureau, Health Resources and Services Administration FROM: AMCHP Board of Directors DATE: February 14, 2014 RE: Final Recommendations
MEMORANDUM TO: Dr. Michael Lu, Associate Administrator Maternal and Child Health Bureau, Health Resources and Services Administration FROM: AMCHP Board of Directors DATE: February 14, 2014 RE: Final Recommendations
How To Help A Pregnant Woman In Texas
 Public Health Nurse Home Visiting Programs Presented by Meredith Krugel, RN, LCSW Douglas County Public Health Nurse Home Visiting Oregon currently has four different nurse home visiting programs: Maternity
Public Health Nurse Home Visiting Programs Presented by Meredith Krugel, RN, LCSW Douglas County Public Health Nurse Home Visiting Oregon currently has four different nurse home visiting programs: Maternity
Pregnancy Intendedness
 Pregnancy Intendedness What moms had to say: "Very excited! We wanted to be pregnant for 8 years!" "I felt too old." "I wanted to have a baby to get some support so I could be on my own; if didn't have
Pregnancy Intendedness What moms had to say: "Very excited! We wanted to be pregnant for 8 years!" "I felt too old." "I wanted to have a baby to get some support so I could be on my own; if didn't have
NEBRASKA 2010 HEALTH GOALS AND OBJECTIVES. A MidCourse Review
 NEBRASKA 21 HEALTH GOALS AND OBJECTIVES A MidCourse Review NEBRASKA 21 HEALTH GOALS AND OBJECTIVES: A MidCourse Review Nebraska Department of Health and Human Services Division of Public Health Joann
NEBRASKA 21 HEALTH GOALS AND OBJECTIVES A MidCourse Review NEBRASKA 21 HEALTH GOALS AND OBJECTIVES: A MidCourse Review Nebraska Department of Health and Human Services Division of Public Health Joann
Facts about Diabetes in Massachusetts
 Facts about Diabetes in Massachusetts Diabetes is a disease in which the body does not produce or properly use insulin (a hormone used to convert sugar, starches, and other food into the energy needed
Facts about Diabetes in Massachusetts Diabetes is a disease in which the body does not produce or properly use insulin (a hormone used to convert sugar, starches, and other food into the energy needed
UF Health Jacksonville CHNA Implementation Strategy
 UF Health Jacksonville CHA Implementation Strategy Adopted by the UF Health Jacksonville Governing Board on: December 7, 2015 This document describes how UF Health Jacksonville (the hospital) plans to
UF Health Jacksonville CHA Implementation Strategy Adopted by the UF Health Jacksonville Governing Board on: December 7, 2015 This document describes how UF Health Jacksonville (the hospital) plans to
Health Profile for St. Louis City
 Health Profile for St. Louis City The health indicators of St. Louis City show that the city has many health problems. To highlight a few, the city s rates of sexually transmitted diseases (i.e., HIV/AIDS,
Health Profile for St. Louis City The health indicators of St. Louis City show that the city has many health problems. To highlight a few, the city s rates of sexually transmitted diseases (i.e., HIV/AIDS,
University Hospital Community Health Needs Assessment FY 2014
 FY 2014 Prepared by Kathy Opromollo Executive Director of Ambulatory Care Services Newark New Jersey is the State s largest city. In striving to identify and address Newark s most pressing health care
FY 2014 Prepared by Kathy Opromollo Executive Director of Ambulatory Care Services Newark New Jersey is the State s largest city. In striving to identify and address Newark s most pressing health care