The Seubert Safe Workplace
|
|
|
- Christine Nelson
- 8 years ago
- Views:
Transcription
1 The Seubert Safe Workplace The Seubert Safe Workplace is a program initiated to help our commercial insurance clients their control worker compensation costs and improve employee health and well-being. A Seubert Safe Workplace consists of four components: 1. A Physicians Panel 2. A Safety Committee 3. An Accident Investigation Procedure 4. A Return to Work Program * some information provided by Eastern Alliance Insurance Group and Royal and Sun Alliance.

2 Component 1: Physicians Panel Pennsylvania state workers compensation law provides that an employer may post a panel of physicians that employees injured on the job must treat with for a period of 90 days, beginning with the first date of treatment. Setting up a physicians panel has many benefits: Ensures prompt, appropriate treatment for work-related injuries by physicians specially trained in occupational medicine. Prevents doctor shopping by injured workers to seek a medical opinion that will provide or extend their disability. Reduces medical cost and potentially eliminates costly litigation by provides control over the treatment. Decreases or eliminates disability through transitional return to work utilizing medical providers who are familiar with the insurance carrier s protocol. Fosters open lines of communication between employer, medical provider and insurance carrier regarding treatment and return to work. Clearly identifies any work restrictions of an injured worker that may prohibit full duty via a physical capacity form, after evaluating employee for transitional duty. To set up a physicians panel, contact your Seubert representative. Once a panel is in place, have each employee sign an Employee Acknowledgement Form. A copy of the form follows this page.

3
4 Component 2: Safety Committees Safety committees help make employees aware of the need for safety along with giving the insured a 5% credit on their workers compensation policy. The state of Pennsylvania has developed safety committee guidelines and requirements, as well as a Technical Assistance Manual. You can access all the information on the PA Department of Labor and Industry website. The address for the appropriate page is:

5 Component 3: Accident Investigation Procedure Accident investigation can pinpoint problem areas and faulty equipment. This can help companies correct problems and help prevent repeat occurrences. It can also help identify faulty claims. There are eight steps to investigating an accident or injury: 1. Interview the employee regarding the injury. Details are important and the employee may provide more information to you than to the insurance company. Have the employee fill out and sign an Injured Employee s Report form. A copy of the form follows this section. 2. Secure any faulty equipment or photograph any unsafe condition on the premises. This may be important evidence in a third-party subrogation action. 3. Examine the accident scene and compare the condition to the employee s version (ex: water of floor, weight of object being lifted, etc.) 4. Interview witness using the Witness Incident Report form. A copy of the form follows this section. Remember, what a witness doesn t see is sometimes as important as what they do see. 5. Take corrective action. 6. Place a copy of the investigation in the employee s personnel file. 7. Provide your findings to your claims team. 8. Use the accident as a learning tool. Discuss it at safety meetings and focus on prevention.

6 Please complete the entire form INJURED EMPLOYEE S REPORT Name: SS#: Address: (Street) Phone #: (city) (zip) (county) Date of Birth: Marital Status: # of children under 18: Job Title: Date of hire: Accident Information Date of accident: / / Time of accident: a.m./p.m. Date returned to work: / / Start time: a.m./p.m. Exact location of accident: Address of accident: Describe in detail the events leading up to the accident and how it happened: (attach additional pages if necessary) To whom did you report the accident to and when? List the part(s) of your body which were injured. Be specific. Did you seek medical treatment? If yes, where were you treated and by whom? Did defective equipment, material, furnishings, co-workers, or another river contribute to the accident? If yes, describe the how. List the witness(s) to the accident: Please indicate if you have ever injured this part of your body before. Yes No (Please circle) If so, when and where? Employee s Signature Date 10/16/03 Seubert & Associates, Inc.

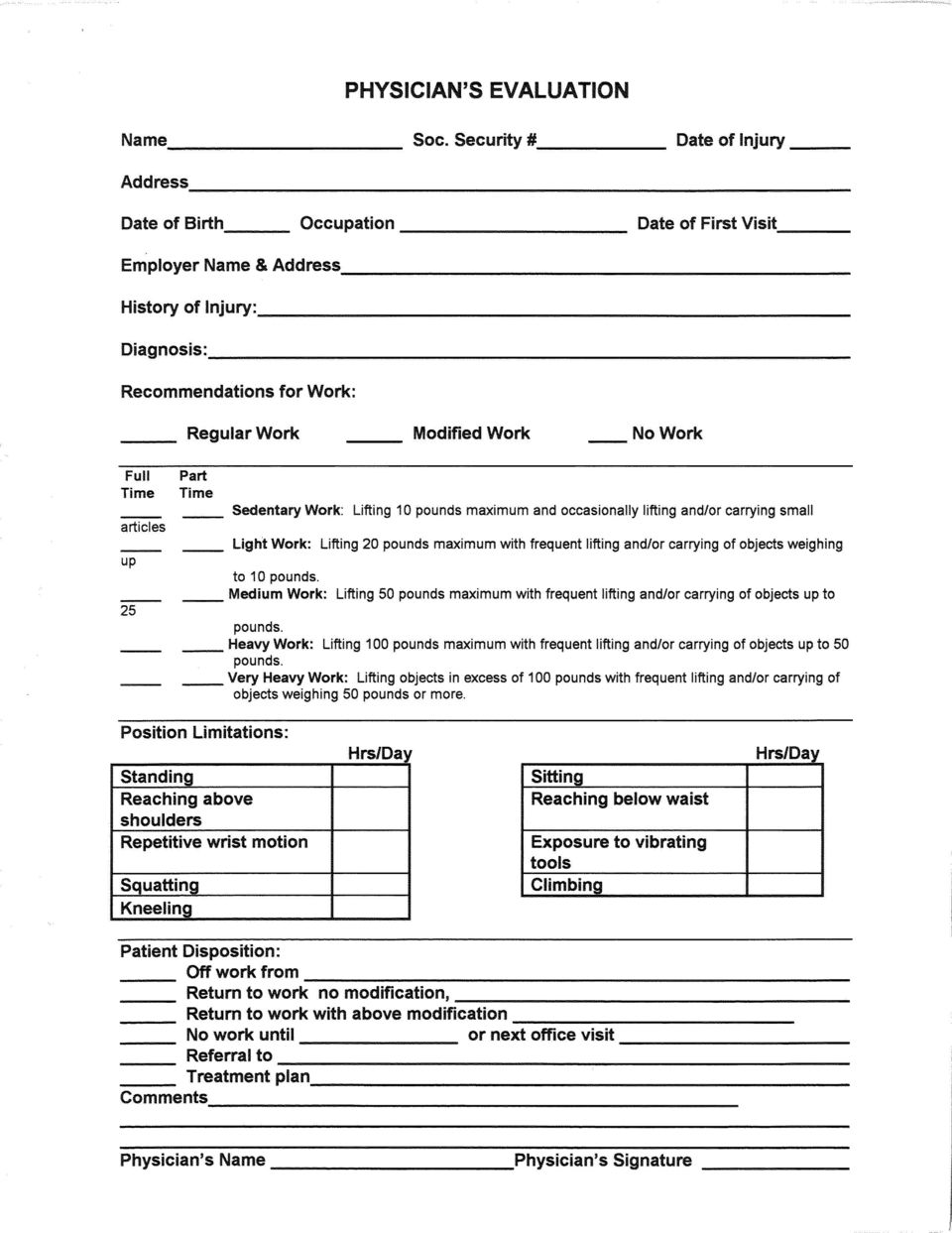
7 Component 4: Return to Work Program You need to provide return to work opportunities for employees who have been injured on the job, because: It s a critical component of claims management. It provides the needed sense of contribution and interaction with peers to legitimately injured employees. It helps prevent abuse of the system for suspect injuries or by employees who exaggerate the extent of their injuries. It controls the cost of lost wages, which is substantially higher than medical costs associated with claims. It helps control the costs of a claim and ultimately the cost of your workers compensation insurance. An effective return to work program can demonstrate a company s commitment to the health and well-being of its employees. At the same time, it can improve a company s productivity and profitability. To implement the program, you ll utilize the following forms, which you can find at the end of this section: Employer s Job Evaluation form Physician s Evaluation form Modified Duty Form

8 WITNESS INCIDENT REPORT To be completed and signed by witness only This report will be submitted to the Worker s Compensation Insurer as part of claim Full Name: Date of Incident: Telephone Number: Time of Incident: Who the accident involved: In your own words describe what you witnessed with as much detail as possible: Names of other witnesses: WITNESS SIGNATURE DATE AND TIME OF REPORT 10/16/03 Seubert & Associates, Inc.

9 Keys to a Successful Return to Work Program Establish a program before you need it. Make sure that management, supervisors and employees understand their roles and responsibilities. Communicate the program s purpose and goals to supervisors. Some may be hesitant to provide a position to an employee who is less than 100%. Emphasize to them the rehabilitative and productivity value of the program and its role in controlling workers compensation costs. When possible, modify the employee s own position to meet their physical limitations. Design modified positions to be productive and useful. To accommodate physical limitations, you may place the employee on another shift or in a different department. An employee may worry that modified duty means menial tasks. However, keep in mind that any work within the employee s physical capabilities is better than no work at all.

10

11

12
13
Employee Guidelines for Workers Compensation Accidents
 Employee Guidelines for Workers Compensation Accidents The information included in this packet will become important to you in the event that you seek medical attention or lose time from work due to a
Employee Guidelines for Workers Compensation Accidents The information included in this packet will become important to you in the event that you seek medical attention or lose time from work due to a
Workers Compensation Claims Reporting. What do I do after a Workers Compensation accident occurs?
 Workers Compensation Claims Reporting What do I do after a Workers Compensation accident occurs? Secure medical treatment for your injured employee. If during normal business hours, use an Occupational
Workers Compensation Claims Reporting What do I do after a Workers Compensation accident occurs? Secure medical treatment for your injured employee. If during normal business hours, use an Occupational
ACCIDENT REPORTING PROCEDURE
 ACCIDENT REPORTING PROCEDURE 1. Employee must notify supervisor immediately. 2. Employee must complete Workers Compensation form 1A (Employee s First Report of Injury) immediately following the accident
ACCIDENT REPORTING PROCEDURE 1. Employee must notify supervisor immediately. 2. Employee must complete Workers Compensation form 1A (Employee s First Report of Injury) immediately following the accident
Workers Compensation Claims Report
 Workers Compensation Claims Report Tel: (866) 402-6600 Fax: (866) 402-6601 In life-threatening situations, immediately seek medical assistance, then complete this claim form! All work-related incidents
Workers Compensation Claims Report Tel: (866) 402-6600 Fax: (866) 402-6601 In life-threatening situations, immediately seek medical assistance, then complete this claim form! All work-related incidents
Office of Physical Plant
 Office of Physical Plant The Pennsylvania State University Physical Plant Building University Park, PA 16802-1118 Please have the employee complete this Workers Compensation Signature Packet as soon as
Office of Physical Plant The Pennsylvania State University Physical Plant Building University Park, PA 16802-1118 Please have the employee complete this Workers Compensation Signature Packet as soon as
CLAIMS REPORTING TO REPORT AN INJURY CALL 1-866-274-6033. 24 hours a day / 7 days a week
 CLAIMS REPORTING TO REPORT AN INJURY CALL 1-866-274-6033 24 hours a day / 7 days a week You will need the following information to report a claim. However, do not delay reporting if you are missing information.
CLAIMS REPORTING TO REPORT AN INJURY CALL 1-866-274-6033 24 hours a day / 7 days a week You will need the following information to report a claim. However, do not delay reporting if you are missing information.
Managing the Care and Return to Work of Injured Workers (and controlling your Workers Compensation Costs)
") Managing the Care and Return to Work of Injured Workers (and controlling your Workers Compensation Costs) This Guide was developed to provide you with valuable information regarding our managed care program,
Managing the Care and Return to Work of Injured Workers (and controlling your Workers Compensation Costs) This Guide was developed to provide you with valuable information regarding our managed care program,
GENERAL BACKGROUND INFORMATION
 Internal Office Use Staff member initials for interview: Date of Incident : Statute of Limitations: Potential Defendants: CLIENT INTAKE FORM Please take the time to answer the questions below as accurately
Internal Office Use Staff member initials for interview: Date of Incident : Statute of Limitations: Potential Defendants: CLIENT INTAKE FORM Please take the time to answer the questions below as accurately
COUNTY OF ALLEGHENY EMPLOYEE ACCIDENT REPORT
 COUNTY OF ALLEGHENY EMPLOYEE ACCIDENT REPORT Revised 05/13/14 Section 1: Identification Information Completed by Employee (Supervisor should verify that information is correct.) Employee Name Last First
COUNTY OF ALLEGHENY EMPLOYEE ACCIDENT REPORT Revised 05/13/14 Section 1: Identification Information Completed by Employee (Supervisor should verify that information is correct.) Employee Name Last First
Employee s Report of Work-Related Injury University of Maryland, College Park
 Employee s Report of Work-Related Injury To be completed immediately after the accident or initial treatment and submitted to your supervisor Employee Name: UID: Male (First) (Last) Female Date of Birth:
Employee s Report of Work-Related Injury To be completed immediately after the accident or initial treatment and submitted to your supervisor Employee Name: UID: Male (First) (Last) Female Date of Birth:
Superintendent s Circular
 Superintendent s Circular School Year 2011-2012 NUMBER: HRS-PP7 DATE: WORKERS COMPENSATION PROCEDURES OBJECTIVE The Boston Public Schools Workers Compensation Service is located within Boston City Hall,
Superintendent s Circular School Year 2011-2012 NUMBER: HRS-PP7 DATE: WORKERS COMPENSATION PROCEDURES OBJECTIVE The Boston Public Schools Workers Compensation Service is located within Boston City Hall,
EMPLOYEE INJURY REPORTING PROCEDURE
 Updated 8/1/2014 TDY MEDICAL STAFFING, Inc. EMPLOYEE INJURY REPORTING PROCEDURE STEP 1: IS INJURY LIFE THREATENING/EMERGENCY? Call 911/go to ER if yes. STEP 2: CALL CLAIM INTO TDY 215-736-5147 STEP 3:
Updated 8/1/2014 TDY MEDICAL STAFFING, Inc. EMPLOYEE INJURY REPORTING PROCEDURE STEP 1: IS INJURY LIFE THREATENING/EMERGENCY? Call 911/go to ER if yes. STEP 2: CALL CLAIM INTO TDY 215-736-5147 STEP 3:
INSTRUCTIONS ON COMPLETING THE WORKERS COMPENSATION- FIRST REPORT OF INJURY REPORT
 INSTRUCTIONS ON COMPLETING THE WORKERS COMPENSATION- FIRST REPORT OF INJURY REPORT I. GENERAL SECTION : Information to be placed in this section only by County Risk Management personnel. The General section
INSTRUCTIONS ON COMPLETING THE WORKERS COMPENSATION- FIRST REPORT OF INJURY REPORT I. GENERAL SECTION : Information to be placed in this section only by County Risk Management personnel. The General section
SAFETY IN THE WORKPLACE By Sharon A. Stewart. January 28, 2005. The Occupational Safety and Health Act (OSHA) includes a General Duty Clause
 includes a General Duty Clause") SAFETY IN THE WORKPLACE By Sharon A. Stewart January 28, 2005 The Occupational Safety and Health Act (OSHA) includes a General Duty Clause requiring employers to "furnish a place of employment which is
SAFETY IN THE WORKPLACE By Sharon A. Stewart January 28, 2005 The Occupational Safety and Health Act (OSHA) includes a General Duty Clause requiring employers to "furnish a place of employment which is
THE SUPERVISOR S ROLE:
 THE SUPERVISOR S ROLE: Workers Compensation Information for CSU, Los Angeles Supervisors Human Resources Management (HRM) Workers Compensation Program August 16, 2010 Table of Contents Introduction..3
THE SUPERVISOR S ROLE: Workers Compensation Information for CSU, Los Angeles Supervisors Human Resources Management (HRM) Workers Compensation Program August 16, 2010 Table of Contents Introduction..3
If you have suffered a work-related injury or illness, you should read this memo and follow the guidelines provided below:
 Telephone: (808) 956-3100 Fax (808) 956-5022 The Research Corporation of the University of Hawaii Human Resources Office First issued: 06/27/2002 Revised: 09/25/2008, 08/26/2013 MEMORANDUM TO: FROM: SUBJECT:
Telephone: (808) 956-3100 Fax (808) 956-5022 The Research Corporation of the University of Hawaii Human Resources Office First issued: 06/27/2002 Revised: 09/25/2008, 08/26/2013 MEMORANDUM TO: FROM: SUBJECT:
Employee s Report of Injury Form
 Employee s Report of Injury Form Instructions: Employees shall use this form to report all work related injuries, illnesses, or near miss events (which could have caused an injury or illness) no matter
Employee s Report of Injury Form Instructions: Employees shall use this form to report all work related injuries, illnesses, or near miss events (which could have caused an injury or illness) no matter
PERSONAL INJURY INTAKE SHEET INITIAL CLIENT STATEMENT HAVE YOU SPOKEN TO ANOTHER ATTORNEY ABOUT THIS CASE?
 PERSONAL INJURY INTAKE SHEET INITIAL CLIENT STATEMENT HAVE YOU SPOKEN TO ANOTHER ATTORNEY ABOUT THIS CASE? IF SO, PLEASE GIVE NAME OF ATTORNEY: DO YOU HAVE A SIGNED RELEASE BY THAT ATTORNEY? SOL: DATE
PERSONAL INJURY INTAKE SHEET INITIAL CLIENT STATEMENT HAVE YOU SPOKEN TO ANOTHER ATTORNEY ABOUT THIS CASE? IF SO, PLEASE GIVE NAME OF ATTORNEY: DO YOU HAVE A SIGNED RELEASE BY THAT ATTORNEY? SOL: DATE
Employee s Report of Incident and the Supervisor's Investigation
 HOW TO REPORT A WORKERS COMPENSATION INJURY 1. The employee must complete the Employee s Report of Incident and submit it to his/her supervisor within 2 hours of the incident. 2. The supervisor must complete
HOW TO REPORT A WORKERS COMPENSATION INJURY 1. The employee must complete the Employee s Report of Incident and submit it to his/her supervisor within 2 hours of the incident. 2. The supervisor must complete
Model Safety Program. Construction CORPORATE HEADQUARTERS 518 EAST BROAD STREET COLUMBUS, OHIO 43215 614.464.5000 STATEAUTO.COM
 TM Model Safety Program Construction CORPORATE HEADQUARTERS 518 EAST BROAD STREET COLUMBUS, OHIO 43215 614.464.5000 STATEAUTO.COM TM Disclaimer: The information contained in this publication was obtained
TM Model Safety Program Construction CORPORATE HEADQUARTERS 518 EAST BROAD STREET COLUMBUS, OHIO 43215 614.464.5000 STATEAUTO.COM TM Disclaimer: The information contained in this publication was obtained
Workers Compensation Injury/Illness Reporting
 Workers Compensation Injury/Illness Reporting s I. Introductions/Objectives This document outlines the procedures and responsibilities for reporting injuries, illnesses, accidents and medical emergencies
Workers Compensation Injury/Illness Reporting s I. Introductions/Objectives This document outlines the procedures and responsibilities for reporting injuries, illnesses, accidents and medical emergencies
WORKERS COMPENSATION CLAIM REPORTING PROCEDURES
 WORKERS COMPENSATION CLAIM REPORTING PROCEDURES 1. Complete the enclosed First Report of Injury to ensure that you will have all of the appropriate questions answered during the reporting process. Have
WORKERS COMPENSATION CLAIM REPORTING PROCEDURES 1. Complete the enclosed First Report of Injury to ensure that you will have all of the appropriate questions answered during the reporting process. Have
Workers Compensation Incident / Accident Investigation Narrative Home Health Care
 WHAT IS THE DEFINITION OF AN INCIDENT AND/OR ACCIDENT? Workers Compensation Incident / Accident Investigation Narrative Incident - is defined as an event that may lead to an insurance claim for bodily
WHAT IS THE DEFINITION OF AN INCIDENT AND/OR ACCIDENT? Workers Compensation Incident / Accident Investigation Narrative Incident - is defined as an event that may lead to an insurance claim for bodily
Checklists for Handling Workers Compensation Claims
 Checklists for Handling Workers Compensation Claims Checklist for handling claims The initial period is critical in handling workers compensation claims. Be sure to: Immediately administer first aid accompany
Checklists for Handling Workers Compensation Claims Checklist for handling claims The initial period is critical in handling workers compensation claims. Be sure to: Immediately administer first aid accompany
SUSQUEHANNA CONFERENCE OF THE UNITED METHODIST CHURCH WORKERS COMPENSATION
 SUSQUEHANNA CONFERENCE OF THE UNITED METHODIST CHURCH WORKERS COMPENSATION I. Workers Compensation Coverage II. Who Is Covered III. Who Is T Covered IV. How to Report a Claim I. WORKERS COMPENSATION COVERAGE
SUSQUEHANNA CONFERENCE OF THE UNITED METHODIST CHURCH WORKERS COMPENSATION I. Workers Compensation Coverage II. Who Is Covered III. Who Is T Covered IV. How to Report a Claim I. WORKERS COMPENSATION COVERAGE
ACCIDENT, INJURY, AND INCIDENT REPORTING PROCEDURES
 ACCIDENT, INJURY, AND INCIDENT REPORTING PROCEDURES VEHICLE ACCIDENTS/PROPERTY DAMAGE Non-Workers Compensation Accident Report Form Attached is a sample copy of the accident report for vehicle damage,
ACCIDENT, INJURY, AND INCIDENT REPORTING PROCEDURES VEHICLE ACCIDENTS/PROPERTY DAMAGE Non-Workers Compensation Accident Report Form Attached is a sample copy of the accident report for vehicle damage,
WORKERS COMPENSATION EMPLOYEE S NOTICE OF INJURY (COMPLETE ALL ITEMS)
") WORKERS COMPENSATION EMPLOYEE S NOTICE OF INJURY (COMPLETE ALL ITEMS) EMPLOYEE S NAME: (last) (first) EMPLOYEE S ADDRESS: (no.) (street) (city) (state) (zip) TELEPHONE: Home: Work: SOCIAL SECURITY NO.
WORKERS COMPENSATION EMPLOYEE S NOTICE OF INJURY (COMPLETE ALL ITEMS) EMPLOYEE S NAME: (last) (first) EMPLOYEE S ADDRESS: (no.) (street) (city) (state) (zip) TELEPHONE: Home: Work: SOCIAL SECURITY NO.
Injury Reporting PACKET. 1-888-627-7586 www.careworksmco.com
 Injury Reporting PACKET 1-888-627-7586 www.careworksmco.com Workplace Injury. Take the Right Steps. Helping Simplify the First Report of Injury (FROI) Process 1 2 3 4 INJURED EMPLOYEE 4-STEP PROCESS Immediately
Injury Reporting PACKET 1-888-627-7586 www.careworksmco.com Workplace Injury. Take the Right Steps. Helping Simplify the First Report of Injury (FROI) Process 1 2 3 4 INJURED EMPLOYEE 4-STEP PROCESS Immediately
Accident Investigation and Reporting Program Required Forms Instructions and Guidance
 Accident Investigation and Reporting Program Required Forms Instructions and Guidance This document contains multiple forms that must be completed for all employee accidents, illnesses or injuries. The
Accident Investigation and Reporting Program Required Forms Instructions and Guidance This document contains multiple forms that must be completed for all employee accidents, illnesses or injuries. The
HANOVER COUNTY PUBLIC SCHOOLS
 POLICY The School Board provides Workers Compensation insurance coverage at no cost to employees. This insurance program covers an injury (by accident) or illness (occupational disease) which arises out
POLICY The School Board provides Workers Compensation insurance coverage at no cost to employees. This insurance program covers an injury (by accident) or illness (occupational disease) which arises out
Telephonic Reporting: 1-800-327-3636 Workers Compensation Call-In Script
 Telephonic Reporting: 1-800-327-3636 Workers Compensation Call-In Script The following script contains the comprehensive list of questions for your loss report. Asterisks denote information that is critical
Telephonic Reporting: 1-800-327-3636 Workers Compensation Call-In Script The following script contains the comprehensive list of questions for your loss report. Asterisks denote information that is critical
THOMPSON, THOMPSON & GLANVILLE, PLC PERSONAL INJURY INITIAL CLIENT INTERVIEW (AUTO) BACKGROUND INFORMATION
 BACKGROUND INFORMATION") THOMPSON, THOMPSON & GLANVILLE, PLC PERSONAL INJURY INITIAL CLIENT INTERVIEW (AUTO) Date: Referral Source: Atty: Legal Asst.: Office: BACKGROUND INFORMATION Full Name: First Middle Last Other names known
THOMPSON, THOMPSON & GLANVILLE, PLC PERSONAL INJURY INITIAL CLIENT INTERVIEW (AUTO) Date: Referral Source: Atty: Legal Asst.: Office: BACKGROUND INFORMATION Full Name: First Middle Last Other names known
Modified Duty/Return to Work (RTW) Program
 Program") Modified Duty/Return to Work (RTW) Program Client Name: Effective Date: PROGRAM OUTLINE 1. Accident Reporting and Return to Work Process 2. Modified Duty/Return to Work (RTW) Program 3. Employee Responsibility
Modified Duty/Return to Work (RTW) Program Client Name: Effective Date: PROGRAM OUTLINE 1. Accident Reporting and Return to Work Process 2. Modified Duty/Return to Work (RTW) Program 3. Employee Responsibility
Accident/Injury Reporting & Workers Compensation Programs For Employees. Administered by the Department of Environmental Health and Safety
 Accident/Injury Reporting & Workers Compensation Programs For Employees Administered by the Department of Environmental Health and Safety Revised July 1, 2011 Slippery Rock University Accident/Injury Reporting
Accident/Injury Reporting & Workers Compensation Programs For Employees Administered by the Department of Environmental Health and Safety Revised July 1, 2011 Slippery Rock University Accident/Injury Reporting
A Transitional Work Program benefits employees in several ways:
 Workmen s Compensation Policy Number: 7390 Effective Date: All employees of Snake River School District 52 are covered by Workmen's Compensation insurance for bodily injury, disease, or death caused by
Workmen s Compensation Policy Number: 7390 Effective Date: All employees of Snake River School District 52 are covered by Workmen's Compensation insurance for bodily injury, disease, or death caused by
INTRODUCTION GENERAL INFORMATION
 Workers Compensation Benefits Summary For dates of injury occurring on or after July 1, 2013 through June 30, 2014 Employment Relations Division Department of Labor and Industry PO Box 8011 Helena, MT
Workers Compensation Benefits Summary For dates of injury occurring on or after July 1, 2013 through June 30, 2014 Employment Relations Division Department of Labor and Industry PO Box 8011 Helena, MT
THIS CLAIM FORM MUST BE FILED WITHIN NINETY DAYS OF ACCIDENT/OCCURRENCE OR YOU MAY FORFEIT YOUR RIGHTS PURSUANT TO N.J.S.A. 59:1 ET SEQ.
 THIS CLAIM FORM MUST BE FILED WITHIN NINETY DAYS OF ACCIDENT/OCCURRENCE OR YOU MAY FORFEIT YOUR RIGHTS PURSUANT TO N.J.S.A. 59:1 ET SEQ. 1) CLAIMAINT INFORMATION DATE OF ACCIDENT $ AMOUNT OF CLAIM LAST
THIS CLAIM FORM MUST BE FILED WITHIN NINETY DAYS OF ACCIDENT/OCCURRENCE OR YOU MAY FORFEIT YOUR RIGHTS PURSUANT TO N.J.S.A. 59:1 ET SEQ. 1) CLAIMAINT INFORMATION DATE OF ACCIDENT $ AMOUNT OF CLAIM LAST
WEEKLY SAFETY MEETING All Euramax Subsidiaries ACCIDENT REPORTING. Safety Meeting Contents. Meeting Notice. Leaders Guide.
 Safety Meeting Contents Meeting Notice Leaders Guide Employee Handout Employee Quiz Meeting Sign-In Sheet Employee Puzzle PRIOR TO THE WEEKLY MEETING: - Post the meeting notice by the timeclock - Read
Safety Meeting Contents Meeting Notice Leaders Guide Employee Handout Employee Quiz Meeting Sign-In Sheet Employee Puzzle PRIOR TO THE WEEKLY MEETING: - Post the meeting notice by the timeclock - Read
Injury Illness Response and Reporting Procedure
 Injury Illness Response and Reporting Procedure Policy: The following is the procedure for reporting and response to injuries or illnesses for employees, students, official volunteers and/or visitors at
Injury Illness Response and Reporting Procedure Policy: The following is the procedure for reporting and response to injuries or illnesses for employees, students, official volunteers and/or visitors at
THIS FORM MUST BE ENTIRELY COMPLETED IN ORDER TO PROCESS YOUR CLAIM
 THIS FORM MUST BE ENTIRELY COMPLETED IN ORDER TO PROCESS YOUR CLAIM COBB COUNTY SCHOOL DISTRICT EMPLOYEE REPORT OF WORK RELATED ACCIDENT (770) 590-4520 FOR WORKERS COMPENSATION (678) 594-8266 Office Fax
THIS FORM MUST BE ENTIRELY COMPLETED IN ORDER TO PROCESS YOUR CLAIM COBB COUNTY SCHOOL DISTRICT EMPLOYEE REPORT OF WORK RELATED ACCIDENT (770) 590-4520 FOR WORKERS COMPENSATION (678) 594-8266 Office Fax
Report ALL on-the-job injuries to
 1817 N. Stewart Street, Suite 20 Carson City, NV 89706 Phone: 775-283-0040 Toll Free: 888-873-4234 Fax: 775-283-0035 Report ALL on-the-job injuries to Tri-Odyssey Risk Management Department Phone: 775-283-0040
1817 N. Stewart Street, Suite 20 Carson City, NV 89706 Phone: 775-283-0040 Toll Free: 888-873-4234 Fax: 775-283-0035 Report ALL on-the-job injuries to Tri-Odyssey Risk Management Department Phone: 775-283-0040
Guide. to Recovery Under The Illinois Workers Compensation Act. The Injured Employee s
 The Injured Employee s Guide to Recovery Under The Illinois Workers Compensation Act Prepared By: Romanucci & Blandin, LLC 33 North LaSalle Street, 20th Floor Chicago, Illinois 60602 Toll Free: 888.458.1145
The Injured Employee s Guide to Recovery Under The Illinois Workers Compensation Act Prepared By: Romanucci & Blandin, LLC 33 North LaSalle Street, 20th Floor Chicago, Illinois 60602 Toll Free: 888.458.1145
Notice of Claim. Last First Middle Area Code/ Telephone Number. Last First Middle Area Code/ Telephone Number
 Claimant: Notice of Claim Last First Middle Area Code/ Telephone Number Street Address Additional Address City State Zip Date of Birth Social Security Number If Notices and correspondence in connection
Claimant: Notice of Claim Last First Middle Area Code/ Telephone Number Street Address Additional Address City State Zip Date of Birth Social Security Number If Notices and correspondence in connection
Workers Compensation Claim Form (DWC 1) & Notice of Potential Eligibility e3301 (rev. 01/12) DWC 1 (rev. 6/10)
 & Notice of Potential Eligibility e3301 (rev. 01/12) DWC 1 (rev. 6/10)") Workers' Compensation Claim Kit Instructions for Completing the Forms Required to Report a Work-Related Injury or Illness California Department of Human Resources Workers Compensation Program What are
Workers' Compensation Claim Kit Instructions for Completing the Forms Required to Report a Work-Related Injury or Illness California Department of Human Resources Workers Compensation Program What are
THE SALAZAR LAW FIRM, P.A. NEW CLIENT INFORMATION SHEET (PERSONAL INJURY MOTOR VEHICLE) PERSONAL INFORMATION:
 PERSONAL INFORMATION:") THE SALAZAR LAW FIRM, P.A. NEW CLIENT INFORMATION SHEET (PERSONAL INJURY MOTOR VEHICLE) TODAY'S DATE PERSONAL INFORMATION: DATE OF ACCIDENT NAME HOME ADDRESS CITY STATE ZIP HOME TELEPHONE ( ) DATE OF BIRTH
THE SALAZAR LAW FIRM, P.A. NEW CLIENT INFORMATION SHEET (PERSONAL INJURY MOTOR VEHICLE) TODAY'S DATE PERSONAL INFORMATION: DATE OF ACCIDENT NAME HOME ADDRESS CITY STATE ZIP HOME TELEPHONE ( ) DATE OF BIRTH
Workers Compensation. Your Guide to Handling Worker s Compensation Reporting and Filing
 Workers Compensation Your Guide to Handling Worker s Compensation Reporting and Filing Filing Worker s Compensation Claims Compensation Claims When the department is notified of an employee s work-related
Workers Compensation Your Guide to Handling Worker s Compensation Reporting and Filing Filing Worker s Compensation Claims Compensation Claims When the department is notified of an employee s work-related
Division of Administration and Finance Planning + Design + Construction PO Box 210186 Cincinnati, Ohio 45221-0186
 1. All forms must be completed in detail, and in legible handwriting or typed. If handwritten, please print 2. 3. Incomplete forms or outdated forms will be sent back to the individual for revisions. 4.
1. All forms must be completed in detail, and in legible handwriting or typed. If handwritten, please print 2. 3. Incomplete forms or outdated forms will be sent back to the individual for revisions. 4.
CLAIMS MANAGEMENT MISSISSIPPI MUNICIPAL SERVICE COMPANY MISSISSIPPI MUNICIPAL WORKERS COMPENSATION GROUP MISSISSIPPI MUNICIPAL LIABILITY PLAN
 CLAIMS MANAGEMENT While accuracy is not guaranteed, this publication was prepared solely for the exclusive use of Mississippi Municipal Service Company customers. It is designed solely to assist our clients
CLAIMS MANAGEMENT While accuracy is not guaranteed, this publication was prepared solely for the exclusive use of Mississippi Municipal Service Company customers. It is designed solely to assist our clients
Workers' Compensation
 Workers' Compensation Accident Reporting Procedures LISD FORMS AVAILABLE AT THE SAFETY WEBSITE ARE IN BOLD LETTERS 1. Employee reports accident or near miss to campus/department Safety Officer. The Safety
Workers' Compensation Accident Reporting Procedures LISD FORMS AVAILABLE AT THE SAFETY WEBSITE ARE IN BOLD LETTERS 1. Employee reports accident or near miss to campus/department Safety Officer. The Safety
How To Write A Workers Compensation Check
 WORKERS COMPENSATION Office of Human Resources WHAT IS WORKERS COMPENSATION? Workers Compensation is a University paid benefit for employees and students that are working payroll or work study. Workers
WORKERS COMPENSATION Office of Human Resources WHAT IS WORKERS COMPENSATION? Workers Compensation is a University paid benefit for employees and students that are working payroll or work study. Workers
WORKERS= COMPENSATION INCIDENT CHECKLIST
 WORKERS= COMPENSATION INCIDENT CHECKLIST This checklist is to be completed by the IMMEDIATE SUPERVISOR of the injured employee. This packet is VERY TIME-SENSITIVE. All forms in the packet should be completed
WORKERS= COMPENSATION INCIDENT CHECKLIST This checklist is to be completed by the IMMEDIATE SUPERVISOR of the injured employee. This packet is VERY TIME-SENSITIVE. All forms in the packet should be completed
Policy and Procedures Date: May 21, 2010
 Virginia Polytechnic Institute and State University No. 4420 Rev.: 3 Policy and Procedures Date: May 21, 2010 Subject: Return to Work Policy 1. Purpose... 1 2. Policy... 1 2.1 Occupational Injuries or
Virginia Polytechnic Institute and State University No. 4420 Rev.: 3 Policy and Procedures Date: May 21, 2010 Subject: Return to Work Policy 1. Purpose... 1 2. Policy... 1 2.1 Occupational Injuries or
Workers' Compensation CLAIMS KIT
 Workers' Compensation CLAIMS KIT CLMCVR ATTENTION WORKERS' COMPENSATION POLICYHOLDERS! Thank you for placing your Workers' Compensation insurance through CIA Managing General Agency. The carrier for your
Workers' Compensation CLAIMS KIT CLMCVR ATTENTION WORKERS' COMPENSATION POLICYHOLDERS! Thank you for placing your Workers' Compensation insurance through CIA Managing General Agency. The carrier for your
(This is a sample of the injury packet that GENEX will customize for each employer)
") Ohio Workers Compensation Injury Packet (This is a sample of the injury packet that GENEX will customize for each employer) Employer: «Employer» «Address1» «City», «ST» «Zip» Phone #: «Phone» BWC Policy
Ohio Workers Compensation Injury Packet (This is a sample of the injury packet that GENEX will customize for each employer) Employer: «Employer» «Address1» «City», «ST» «Zip» Phone #: «Phone» BWC Policy
Accident Investigation FORMS
 English/Español Accident Investigation FORMS How To Use These Important Tools Includes: Employee's Report of Injury Form Accident Witness Statement Form Supervisor's Accident Investigation Form Forms may
English/Español Accident Investigation FORMS How To Use These Important Tools Includes: Employee's Report of Injury Form Accident Witness Statement Form Supervisor's Accident Investigation Form Forms may
Date of Birth: / / Male Female Martial Status: Language: English Spanish Other: E-mail: Occupation: Date Hired: / /
 Early reporting can save you money. Report all injuries immediately! The information below allows Pinnacol Assurance s customer service representatives to quickly and accurately process your claim. Use
Early reporting can save you money. Report all injuries immediately! The information below allows Pinnacol Assurance s customer service representatives to quickly and accurately process your claim. Use
WORKERS' COMPENSATION CLAIMANT INFORMATION PACKET
 WORKERS' COMPENSATION CLAIMANT INFORMATION PACKET Instructions Statement of Rights Prescription ID and Pharmacy Information The New York State Insurance Fund TLC EMERGENCY MEDICAL SERVICES Inc. TLC MEDICAL
WORKERS' COMPENSATION CLAIMANT INFORMATION PACKET Instructions Statement of Rights Prescription ID and Pharmacy Information The New York State Insurance Fund TLC EMERGENCY MEDICAL SERVICES Inc. TLC MEDICAL
WORKERS COMPENSATION RETURN TO WORK PROGRAM
 WORKERS COMPENSATION RETURN TO WORK PROGRAM Contents GOAL of your Workers Compensation Return to Work Program...2 BENEFITS of your Workers Compensation Return to Work Program...3 SET UP your Workers Compensation
WORKERS COMPENSATION RETURN TO WORK PROGRAM Contents GOAL of your Workers Compensation Return to Work Program...2 BENEFITS of your Workers Compensation Return to Work Program...3 SET UP your Workers Compensation
WORKERS COMPENSATION QUICK FACTS
 The Workers' Compensation Handbook // 1 WORKERS COMPENSATION QUICK FACTS Workers Compensation Quick Facts contains general information about the workers compensation system in New Mexico, to provide employers
The Workers' Compensation Handbook // 1 WORKERS COMPENSATION QUICK FACTS Workers Compensation Quick Facts contains general information about the workers compensation system in New Mexico, to provide employers
PETITIONER STATES AS FOLLOWS:
 State of Utah Labor Commission Division of Adjudication 160 East 300 South, 3 rd Floor, P.O. Box 146615 Salt Lake City, Utah 84114 6615 (801) 530 6800 casefiling@utah.gov Note: PLEASE TYPE OR PRINT CLEARLY
State of Utah Labor Commission Division of Adjudication 160 East 300 South, 3 rd Floor, P.O. Box 146615 Salt Lake City, Utah 84114 6615 (801) 530 6800 casefiling@utah.gov Note: PLEASE TYPE OR PRINT CLEARLY
Madison County Board Of Education
 JOB-RELATED INJURY INSTRUCTIONS In compliance with Board Policy FILE: 5.9.4, Absences Due to Job-Related Injuries, the following instructions must be followed when injuries occur on the job. Please read
JOB-RELATED INJURY INSTRUCTIONS In compliance with Board Policy FILE: 5.9.4, Absences Due to Job-Related Injuries, the following instructions must be followed when injuries occur on the job. Please read
The ACCG Claims Office staff is here to help you. Please feel free to call us with your questions and concerns.
 1 WELCOME This handbook contains information prepared by the Association County Commissioners of Georgia - Group Self-Insurance Workers Compensation Fund (ACCG - GSIWCF) to assist employees and management
1 WELCOME This handbook contains information prepared by the Association County Commissioners of Georgia - Group Self-Insurance Workers Compensation Fund (ACCG - GSIWCF) to assist employees and management
Workers Compensation Claim Kit PRAIRIE STATE INSURANCE COOPERATIVE
 Workers Compensation Claim Kit PRAIRIE STATE INSURANCE COOPERATIVE A CMI, A York Risk Services Company, publication November 1, 2013 Table of Contents About CMI.... 1 To Report a Claim... 1 The Importance
Workers Compensation Claim Kit PRAIRIE STATE INSURANCE COOPERATIVE A CMI, A York Risk Services Company, publication November 1, 2013 Table of Contents About CMI.... 1 To Report a Claim... 1 The Importance
THOMPSON, THOMPSON & GLANVILLE, PLC PERSONAL INJURY CLIENT INTERVIEW FORM BACKGROUND INFORMATION
 THOMPSON, THOMPSON & GLANVILLE, PLC PERSONAL INJURY CLIENT INTERVIEW FORM Date: Referral Source: Atty: Legal Asst.: Office: BACKGROUND INFORMATION Full Name: First Middle Last Other names known by (including
THOMPSON, THOMPSON & GLANVILLE, PLC PERSONAL INJURY CLIENT INTERVIEW FORM Date: Referral Source: Atty: Legal Asst.: Office: BACKGROUND INFORMATION Full Name: First Middle Last Other names known by (including
Accident reporting policy and procedure
 Accident reporting policy and procedure Dorset County Council s guide for employees Improving the quality of life for people in Dorset, now and for the future Introduction 1.1 Recent figures show that
Accident reporting policy and procedure Dorset County Council s guide for employees Improving the quality of life for people in Dorset, now and for the future Introduction 1.1 Recent figures show that
Division of Public Health Administrative Manual
 Original Effective Date: 9/01/06 PURPOSE The purpose of this document is to provide specific guidelines for the timely reporting and investigation of all accidents involving property damage or injury of
Original Effective Date: 9/01/06 PURPOSE The purpose of this document is to provide specific guidelines for the timely reporting and investigation of all accidents involving property damage or injury of
Workers Compensation Optimal Claims Management
 OVERALL OBJECTIVE - ECM seeks to provide a consultative relationship in which we work with our clients to influence and improve their Risk Management Process. Following are a few suggestions regarding
OVERALL OBJECTIVE - ECM seeks to provide a consultative relationship in which we work with our clients to influence and improve their Risk Management Process. Following are a few suggestions regarding
Injured at work? WHAT TO DO IF YOU ARE INJURED ON THE JOB:
 Injured at work? WHAT TO DO IF YOU ARE INJURED ON THE JOB: In case of medical emergency seek immediate treatment at the nearest medical facility. tify your supervisor immediately and assist in filing a
Injured at work? WHAT TO DO IF YOU ARE INJURED ON THE JOB: In case of medical emergency seek immediate treatment at the nearest medical facility. tify your supervisor immediately and assist in filing a
What to Do When an Accident Occurs - Work Comp Procedures
 What to Do When an Accident Occurs - Work Comp Procedures Immediate Response Non-emergency Respond with onsite first aid/cpr responders. Employee must select a physician from the Panel of Physicians form
What to Do When an Accident Occurs - Work Comp Procedures Immediate Response Non-emergency Respond with onsite first aid/cpr responders. Employee must select a physician from the Panel of Physicians form
INITIAL CLIENT STATEMENT
 PERSONAL INJURY/AUTO ACCIDENT INTAKE SHEET SOL: INITIAL CLIENT STATEMENT HAVE YOU SPOKEN TO ANOTHER ATTORNEY ABOUT THIS CASE? IF SO, PLEASE GIVE NAME OF ATTORNEY: DO YOU HAVE A SIGNED RELEASE BY THAT ATTORNEY?
PERSONAL INJURY/AUTO ACCIDENT INTAKE SHEET SOL: INITIAL CLIENT STATEMENT HAVE YOU SPOKEN TO ANOTHER ATTORNEY ABOUT THIS CASE? IF SO, PLEASE GIVE NAME OF ATTORNEY: DO YOU HAVE A SIGNED RELEASE BY THAT ATTORNEY?
Instructions for the Incident/Accident Investigation Form (SORM-703)
") Instructions for the Incident/Accident Investigation Form (SORM-703) Purpose of Form: Effective loss control efforts require documentation of incidents and accidents to determine hazards or problem areas,
Instructions for the Incident/Accident Investigation Form (SORM-703) Purpose of Form: Effective loss control efforts require documentation of incidents and accidents to determine hazards or problem areas,
Acalanes Union HSD Board Policy Work-Related Injuries
 Board Policy BP 4157.1 District employees shall be insured for on-the-job specific or cumulative injuries in accordance with law. In order to reduce costs and facilitate employee recovery, the Governing
Board Policy BP 4157.1 District employees shall be insured for on-the-job specific or cumulative injuries in accordance with law. In order to reduce costs and facilitate employee recovery, the Governing
Workplace Injury & Illness Prevention Program
 Workplace Injury & Illness Prevention Program ID Analytics Inc. For non-high hazard employers RESPONSIBILITY The Injury and Illness Prevention (IIP) Program administrator is Janet Wickens, Director Human
Workplace Injury & Illness Prevention Program ID Analytics Inc. For non-high hazard employers RESPONSIBILITY The Injury and Illness Prevention (IIP) Program administrator is Janet Wickens, Director Human
We thank you for your business, and look forward to providing you with the necessary protection and care for your business and employees.
 RE: Workers Compensation Claims Kit Welcome to the Workers Compensation Insurance Program offered through Tower Group Companies. While we hope that your company never has to experience a workers compensation
RE: Workers Compensation Claims Kit Welcome to the Workers Compensation Insurance Program offered through Tower Group Companies. While we hope that your company never has to experience a workers compensation
19. Injury, Accident, and Loss Reporting
 19. Injury, Accident, and Loss Reporting Overview This section discusses the following topics: Where to Report Claims Reporting Workers Compensation Illnesses and Injuries Reporting Automobile Accidents
19. Injury, Accident, and Loss Reporting Overview This section discusses the following topics: Where to Report Claims Reporting Workers Compensation Illnesses and Injuries Reporting Automobile Accidents
WORKERS' COMPENSATION INFORMATION
 Carnegie Mellon University Human Resources Benefits & Compensation Office 5000 Forbes Avenue, 319 SCRG Pittsburgh, PA 15213-3730 (412) 268-2047 Fax: (412) 268-7472 WORKERS' COMPENSATION INFORMATION In
Carnegie Mellon University Human Resources Benefits & Compensation Office 5000 Forbes Avenue, 319 SCRG Pittsburgh, PA 15213-3730 (412) 268-2047 Fax: (412) 268-7472 WORKERS' COMPENSATION INFORMATION In
J. Richard Lilly, M.D., A.B.F.P., & Associates, P.C.
 J. Richard Lilly, M.D., A.B.F.P., & Associates, P.C. PATIENT REGISTRATION - Please PRINT Clearly Patient Name First Middle Last Date of Birth Age Home Address Apt. No. City State Zip code Occupation Social
J. Richard Lilly, M.D., A.B.F.P., & Associates, P.C. PATIENT REGISTRATION - Please PRINT Clearly Patient Name First Middle Last Date of Birth Age Home Address Apt. No. City State Zip code Occupation Social
South Suburban Occupational Medicine Jeffry N. Gerber, M.D., Level II Certified 7780 South Broadway Suite 250 Littleton, Colorado 80122
 South Suburban Occupational Medicine Director of Risk Management Workmans Compensation Dear Risk Manager, On behalf of the staff and myself, I want to welcome you to our practice. I invite you to explore
South Suburban Occupational Medicine Director of Risk Management Workmans Compensation Dear Risk Manager, On behalf of the staff and myself, I want to welcome you to our practice. I invite you to explore
RETURN-TO-WORK SERVICES
 RETURN-TO-WORK SERVICES TABLE OF CONTENTS Early Intervention...2 Creating A Return-To-Work Program...3 Keep in Mind...3 Five Steps for Creating an Effective Return-To-Work Policy...4 Situations to Avoid
RETURN-TO-WORK SERVICES TABLE OF CONTENTS Early Intervention...2 Creating A Return-To-Work Program...3 Keep in Mind...3 Five Steps for Creating an Effective Return-To-Work Policy...4 Situations to Avoid
How To File A Worker S Compensation Claim In Azoria
 Workers Compensation Instructions for Filing a Claim Please complete following steps within 24 48 hours of the incident: Report the incident to your supervisor immediately or, if a medical emergency, dial
Workers Compensation Instructions for Filing a Claim Please complete following steps within 24 48 hours of the incident: Report the incident to your supervisor immediately or, if a medical emergency, dial
Introduction...2. Or Occupational Disease...3. Workers Compensation Benefits...5. Prescription Processing Services...6. Payroll Procedures...
 Table Of Contents Introduction...2 Procedures For Reporting A Work-Related Injury Or Occupational Disease...3 Workers Compensation Benefits...5 Prescription Processing Services...6 Payroll Procedures...6
Table Of Contents Introduction...2 Procedures For Reporting A Work-Related Injury Or Occupational Disease...3 Workers Compensation Benefits...5 Prescription Processing Services...6 Payroll Procedures...6
Investigating Workers Compensation Claims and Complying with Wage and Hour Law
 Investigating Workers Compensation Claims and Complying with Wage and Hour Law Noel C. Shepard 614-559-7223 nshepard@fbtlaw.com Adam R. Hanley 614-559-7238 ahanley@fbtlaw.com Investigating Workers Compensation
Investigating Workers Compensation Claims and Complying with Wage and Hour Law Noel C. Shepard 614-559-7223 nshepard@fbtlaw.com Adam R. Hanley 614-559-7238 ahanley@fbtlaw.com Investigating Workers Compensation
Important Information about Medical Care if you have a Work-Related Injury or Illness
 Important Information about Medical Care if you have a Work-Related Injury or Illness Complete Written Employee Notification regarding Medical Provider Network (Title 8, California Code of Regulations,
Important Information about Medical Care if you have a Work-Related Injury or Illness Complete Written Employee Notification regarding Medical Provider Network (Title 8, California Code of Regulations,
On The Job Injury Procedure:
 On The Job Injury Procedure: If an accident occurs at your job site with a temporary employee, our office must be contacted immediately. Our office numbers are: Sylvania Office 419-882-7646, Monroe Office
On The Job Injury Procedure: If an accident occurs at your job site with a temporary employee, our office must be contacted immediately. Our office numbers are: Sylvania Office 419-882-7646, Monroe Office
HAVE YOU SPOKEN TO ANOTHER ATTORNEY ABOUT THIS CASE? WHO WERE YOU REFERRED BY: (INDIVIDUAL, YELLOW PAGE AD, ETC...) Email Address:
 Email Address:") PERSONAL INJURY/AUTO ACCIDENT INTAKE SHEET SOL: INITIAL CLIENT STATEMENT TODAY S DATE: HAVE YOU SPOKEN TO ANOTHER ATTORNEY ABOUT THIS CASE? IF SO, PLEASE GIVE NAME OF ATTORNEY : DO YOU HAVE A SIGNED RELEASE
PERSONAL INJURY/AUTO ACCIDENT INTAKE SHEET SOL: INITIAL CLIENT STATEMENT TODAY S DATE: HAVE YOU SPOKEN TO ANOTHER ATTORNEY ABOUT THIS CASE? IF SO, PLEASE GIVE NAME OF ATTORNEY : DO YOU HAVE A SIGNED RELEASE
Overview of Sample Drug and Alcohol Abuse Policy
 Overview of Sample Drug and Alcohol Abuse Policy All employers should have a vital interest in maintaining a safe, healthy, and efficient working environment. Being under the influence of a drug or alcohol
Overview of Sample Drug and Alcohol Abuse Policy All employers should have a vital interest in maintaining a safe, healthy, and efficient working environment. Being under the influence of a drug or alcohol
Call (206) 477-3350 M F 8:00 a.m. to 4:15 p.m.
 477-3350 M F 8:00 a.m. to 4:15 p.m.") Section 29: REPORTING WORK-RELATED ACCIDENTS, INJURIES AND ILLNESSES INTRODUCTION This procedure applies to all King County employees, and includes jurors, witnesses, and all reserve Sheriff s Deputies.
Section 29: REPORTING WORK-RELATED ACCIDENTS, INJURIES AND ILLNESSES INTRODUCTION This procedure applies to all King County employees, and includes jurors, witnesses, and all reserve Sheriff s Deputies.
Anne M. Noonan, Commissioner, Vermont Department of Labor WORKERS COMPENSATION FRAUD STUDY AND REPORT
 Memorandum To: From: House Committee on Commerce and Economic Development; Senate Economic Development, Housing and General Affairs Anne M. Noonan, Commissioner, Vermont Department of Labor Date: 1/15/2015
Memorandum To: From: House Committee on Commerce and Economic Development; Senate Economic Development, Housing and General Affairs Anne M. Noonan, Commissioner, Vermont Department of Labor Date: 1/15/2015
Injury Reporting Procedure
 Injury Reporting Procedure Your business is very important to us, and we're dedicated to providing you with the resources you need to help you be as successful as possible. Toward that end, Paychex Business
Injury Reporting Procedure Your business is very important to us, and we're dedicated to providing you with the resources you need to help you be as successful as possible. Toward that end, Paychex Business
APPLICATION FOR BENEFITS LAW ENFORCEMENT OFFICERS AND FIRE FIGHTERS DISABILITY BENEFITS TRUST FUND
 EXHIBIT A M S Attorney General s Office Use Only: Application #: Receipt Date: G Approved G Disapproved Claim type: G Law Enforcement Officer G Fire Fighter STOP. Please read the fund policies and procedures
EXHIBIT A M S Attorney General s Office Use Only: Application #: Receipt Date: G Approved G Disapproved Claim type: G Law Enforcement Officer G Fire Fighter STOP. Please read the fund policies and procedures
Plaintiff s Interrogatories Directed To Defendant(S)
") FIRST JUDICIAL DISTRICT OF PENNSYLVANIA IN THE COURT OF COMMON PLEAS OF PHILADELPHIA COUNTY PLAINTIFF S NAME : Civil Trial Division : : Compulsory Arbitration Program : vs. : : Term, 20 : DEFENDANT S NAME
FIRST JUDICIAL DISTRICT OF PENNSYLVANIA IN THE COURT OF COMMON PLEAS OF PHILADELPHIA COUNTY PLAINTIFF S NAME : Civil Trial Division : : Compulsory Arbitration Program : vs. : : Term, 20 : DEFENDANT S NAME
Workers Compensation
 Workers Compensation All work-related injuries or illnesses must be reported. If the injury is an emergency, arrange for appropriate medical treatment. The employee has the right to select his or her own
Workers Compensation All work-related injuries or illnesses must be reported. If the injury is an emergency, arrange for appropriate medical treatment. The employee has the right to select his or her own
Utah Labor Commission Industrial Accidents Division. Employers Guide to. Workers Compensation
 2015 2016 Utah Labor Commission Industrial Accidents Division E m p l o y e r s G u i d e Employers Guide to Workers Compensation Utah Labor Commission Industrial Accidents Division Employers Guide to
2015 2016 Utah Labor Commission Industrial Accidents Division E m p l o y e r s G u i d e Employers Guide to Workers Compensation Utah Labor Commission Industrial Accidents Division Employers Guide to
POTENTIAL CLIENT INTAKE SHEET - PREMISES LIABILITY IMPORTANT
 POTENTIAL CLIENT INTAKE SHEET - PREMISES LIABILITY Date: Lawyer: Date of Accident: I. CLIENT INFORMATION Client Name: First Middle Last Date of Birth: You would be preferred to be called (nickname): If
POTENTIAL CLIENT INTAKE SHEET - PREMISES LIABILITY Date: Lawyer: Date of Accident: I. CLIENT INFORMATION Client Name: First Middle Last Date of Birth: You would be preferred to be called (nickname): If
Incident Reporting Manual
 Pillar Income Asset Management, Inc. Incident Reporting Manual For use in reporting: Property Losses General Liability Incidents Workers Compensation Incidents Commercial Auto Incidents Prepared by: The
Pillar Income Asset Management, Inc. Incident Reporting Manual For use in reporting: Property Losses General Liability Incidents Workers Compensation Incidents Commercial Auto Incidents Prepared by: The
FIRST JUDICIAL DISTRICT OF PENNSYLVANIA IN THE COURT OF COMMON PLEAS OF PHILADELPHIA COURT TERM: NO.
 FIRST JUDICIAL DISTRICT OF PENNSYLVANIA IN THE COURT OF COMMON PLEAS OF PHILADELPHIA PLAINTIFF(S) v. DEFENDANT(S) CIVIL TRIAL DIVISION Compulsory Arbitration Program COURT TERM: NO. Defendant s Interrogatories
FIRST JUDICIAL DISTRICT OF PENNSYLVANIA IN THE COURT OF COMMON PLEAS OF PHILADELPHIA PLAINTIFF(S) v. DEFENDANT(S) CIVIL TRIAL DIVISION Compulsory Arbitration Program COURT TERM: NO. Defendant s Interrogatories
LUBA Care Prompt Return to Work Program
 LUBA Care Prompt Return to Work Program Introduction At LUBA Workers Comp, our intent in regard to Prompt Return to Work (PRTW) is to create a situation which benefits all parties involved. A PRTW Program
LUBA Care Prompt Return to Work Program Introduction At LUBA Workers Comp, our intent in regard to Prompt Return to Work (PRTW) is to create a situation which benefits all parties involved. A PRTW Program