(This is a sample of the injury packet that GENEX will customize for each employer)
|
|
|
- Megan Hodge
- 10 years ago
- Views:
Transcription
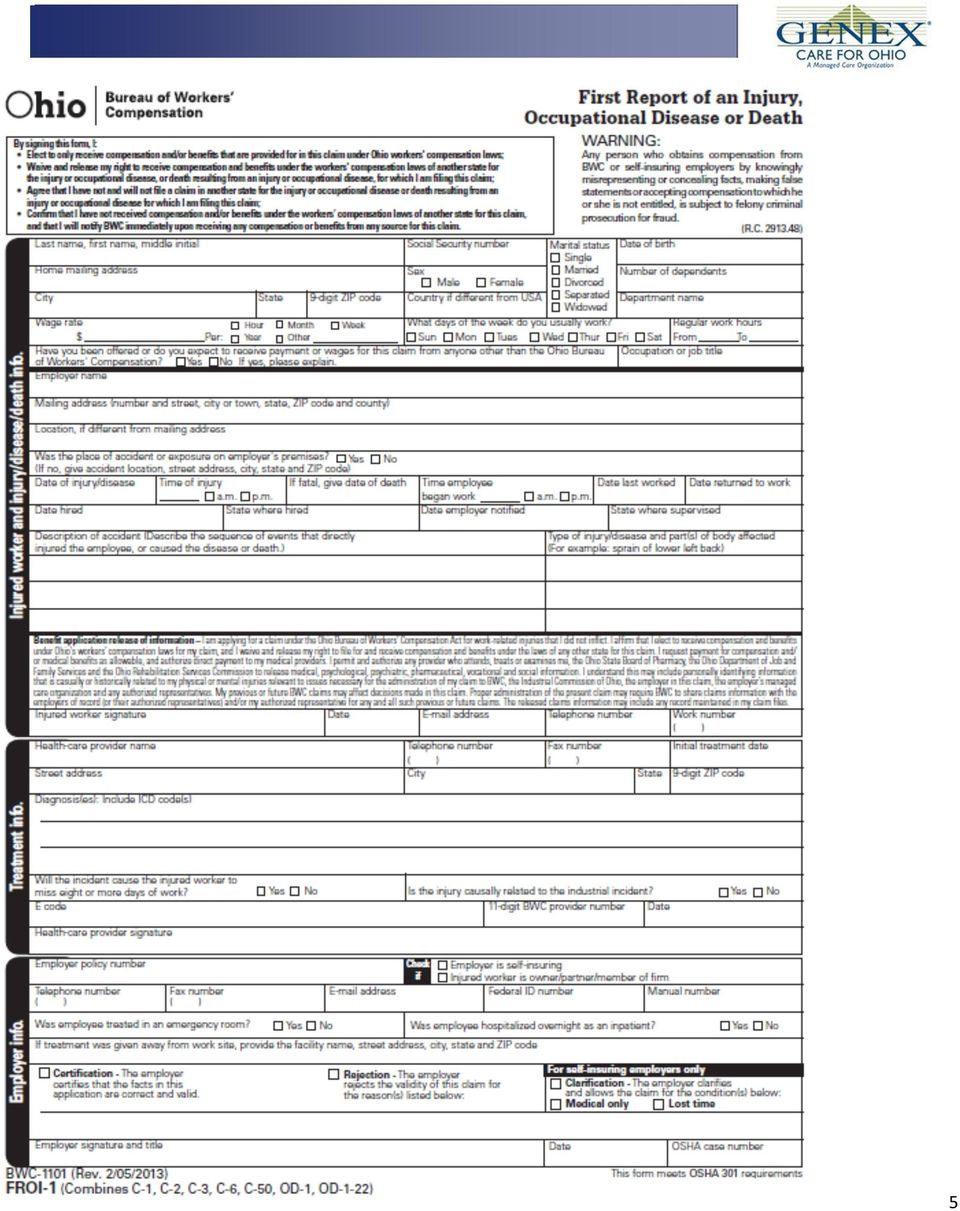
1 Ohio Workers Compensation Injury Packet (This is a sample of the injury packet that GENEX will customize for each employer) Employer: «Employer» «Address1» «City», «ST» «Zip» Phone #: «Phone» BWC Policy #: «Policy» Managed Care Organization (MCO): GENEX Care for Ohio Century Blvd., Suite 202 Cincinnati, Ohio Phone: Fax: [email protected] Third Party Administrator (TPA) 1

2 Workers Compensation Injury Packet Contents Injury Reporting Procedures What to do After the Injury First Report of Injury (FROI) By certifying a claim the employer is stating that they are in agreement that the facts reported are correct and valid to the best of their knowledge. Certification does not mean that BWC will grant the allowance of a claim, just as rejection does not mean that BWC will deny a claim. BWC will conduct an investigation and determine whether the claim should be allowed or denied, regardless of the employer certification. If an employer does not agree with the allowance of a claim they should check off the box marked "rejection." Consult your third party administrator about certifying or rejecting claims. Accident Analysis Forms (Optional) Accident investigations determine how and why these failures occur. By using the information gained through an investigation, a similar or perhaps more disastrous accident may be prevented. Conduct accident investigations with accident prevention in mind. Local Medical Providers (if applicable) GENEX Care for Ohio Claim Team Members Pharmacy Benefits Program Unless a BWC Claim number has been issued the injured worker will need to pay out of pocket for their prescription and get reimbursement from the BWC. Once a claim number has been generated the pharmacy will bill the BWC for prescriptions. Inquiries for pharmacy benefits should be directed to To obtain a claim number immediately you can call the claim into GENEX or file online at Job Analysis Send a job analysis to the doctor with your injured worker. This allows the physician to better determine the job functions of the injured worker and assist them in returning to work with restrictions if needed. 2

3 INJURY REPORTING PROCEDURES Work-related illness/injury occurs. Employee IMMEDIATELY notifies employer of injury. If an emergency, employee should seek immediate medical attention. If not an emergency, employer refers employee to their preferred physician who is BWC Certified Provider. For additional assistance in finding a medical provider: GENEX Care for Ohio (800) Employer and employee should complete the First Report of Injury (FROI) as soon as possible. Three methods of reporting injuries: Fax completed FROI to GENEX Care for Ohio at (888) Call GENEX Care for Ohio at (800) File FROI online at **Please contact GENEX within 24 hours of an injury** Employer and employee should complete accident analysis forms: injury incident report, injury fact sheet and witness statement. If the employee is not going to seek treatment, do not notify GENEX, keep the completed FROI and accident analysis forms in their personnel file. Employer provides employee with a GENEX Care for Ohio ID card and job description. Employee should present their identification card and job description to the medical provider upon arriving for treatment. Employee is to provide employer with medical documents and/or information (e.g.: physician ordered restrictions, physical therapy orders, appointment dates for therapy) in a timely manner. A GENEX Care for Ohio claims specialist and/or nurse case manager will be assigned to each claim. Upon notification of the work-related illness/injury, immediate contact will be made with the employer, injured employee, and medical provider. Transitional work may be available for employees to allow suitable alternate employment or reasonable productive accommodations for those employees who are unable to perform their normal job duties due to work related accident, injury, or illness. 3
 as soon as possible.")
4 ATTENTION MANAGEMENT - What To Do After The Injury GENEX will facilitate return to work and coordination of care Stay in close communication with parties involved in the claim: GENEX, your TPA, the BWC and the injured worker. What is the work status of the injured worker: IW Released Full Duty: notify GENEX of the return to work date. IW Released with Restrictions: GENEX will need to know if you are accommodating the restrictions outlined by the physician. Contact the Injured Worker and let them know that you have transitional work until they can return full duty. Instruct the injured worker to provide you with medical documents and/or information (e.g.: physician ordered restrictions, physical therapy orders, appointment dates for therapy) in a timely manner. Complete and return the Transitional Work Participation Agreement to GENEX. Contact GENEX if you or the injured worker is having difficulty with the restrictions assigned by the physician. Additional assistance may be available onsite; such as remain at work services, job retention program or onsite physical therapy. IW was not released to return to work: It is very important to notify GENEX immediately. Accident Prevention: the safety or transitional work committee should be notified of the incident and should determine how to prevent occurrences. 4

5 5
6 EMPLOYEE S REPORT OF INCIDENT AND INJURY PLEASE PRINT IN INK-To be completed by Employee EMPLOYER: Name Social Sec. Home Address Birth Date City/State/Zip Sex: Male Female Telephone: ( ) Alternate Phone: ( Date of injury or onset of symptoms Time am pm Describe what caused the injury/symptoms, what you were doing just before the incident, and what you did after the incident (if you need more space, write on the back of this form). Be specific - name any objects or substances involved: Did anyone see you get hurt? Yes No If yes, who? Did you report this incident to anyone? Yes No If not, why? If yes, to whom did you report it? (Name and Title/Position) When? (Date and Time) What part(s) of your body was/were affected? (BE SPECIFIC- for example: right elbow, left knee, right index finger): What type of injury did you experience? (BE SPECIFIC- for example: bruise, scrape, laceration, pull): Was any first aid provided at the scene? Yes No If yes, describe: Did you seek other medical treatment? Yes No If yes, when? Where? If treatment was not sought immediately, explain why: 6

7 Is this an aggravation of a previous injury/symptom? Yes No If yes, when were you last treated for the previous injury? By whom or where? Have you ever had a similar injury? Yes No If yes, describe other injury: Medical Release Under current workers compensation provisions, the employer is entitled to a signed medical release I hereby authorize any person or persons who have in the past or will in the future medically attend, treat or examine me, or any person who may have information of any kind which may be used to reach a decision in any claim for injury or disease arising from the injury/illness described above, to disclose such information to my employer, my employer s managed care organization, or to my employer s designated representative. A copy of this form will serve as the original. Employee Name (print) Employee Signature Date (required) 7

8 INDUSTRIAL INJURY FACT SHEET EMPLOYER/SUPERVISOR Employee Name: Soc. Sec. Employer: Date of Injury: Was an investigation completed concerning the circumstances of this injury? Yes No Were there any witnesses to this injury? Yes No If yes, witness statements should be attached. Was the injury a result of horseplay? Under the influence of drugs, or Yes No purposely self-inflicted? If yes, please specify: Has there been any recent disciplinary action taken against this employee? Yes No If yes, please describe (and attach any written documentation): Has the employee missed any work previously due to similar industrial or Yes No non-industrial conditions? If so, when? Has the employee submitted medical documentation for the injury? Yes No If so, please attach. If known, please provide us with the name, address and telephone number of the attending physician: 8
: Has the employee missed any work previously due to similar industrial or Yes No non-industrial conditions? If so, when?")
9 Has the employee returned to work? Yes No Last day worked (date) Returned to work (date) If not, what is the current estimated date of return? With the information you have, would you recommend the claim be accepted? Yes No If no, why not? Employer s signature Title Date PLEASE ATTACH COMPLETED INCIDENT REPORTS, WITNESS STATEMENTS AND ANY ACCUMULATED MEDICAL BILLS AND INFORMATION. ADDITIONAL COMMENTS MAY BE NOTED ON THE REVERSE SIDE. 9

10 STATEMENT OF WITNESS TO ACCIDENT EMPLOYER: I. INCIDENT IDENTIFICATION INFORMATION Name of employee alleging incident Shift _ Occupation Department II. WITNESS STATEMENT Your name has been given as a witness to an incident alleged by the above individual. Through your cooperation, information can be obtained to complete the investigation of this incident. Therefore, it will be appreciated if you will answer each of the following questions and promptly return your completed statement. Your name Your occupation Your address Your telephone number ( ) - Did you see an accident involving the above employee? Yes No If not, how did you learn about the accident? If you did see an accident occur: Date of accident Time of accident am pm Describe what you saw: Your signature Please print your name Date 10

11 State of Ohio County of Before me, a Notary Public in and for said state, personally appeared the above named who acknowledged before me that he/she did sign the foregoing instrument and that the same is his/her free act and deed. (SEAL) In testimony whereof, I have hereunto affixed my name and official seal at day of, 20. (signed), Ohio this Name (printed or typed) My Commission Expires Notary Public, State of Ohio (date) 11
 In testimony whereof, I have hereunto affixed my name and official seal at day of, 20.")
12 In case of injury or illness on the job, please use the following providers in your area. Report claims to: Please seek treatment from the following providers: Occupational Medicine: Hospital / After Hours Care: Provider 1: Provider 1: Provider 2: Provider 2: Provider 3: Provider 3: 12

13 Claim Questions: Managed Care Organization (MCO): GENEX Care for Ohio Phone: Fax: E: Questions regarding injury reporting, treatment authorizations, assistance with provider selections, return to work, transitional work, onsite therapy and medical bill payment: Medical Only Claims: Lost Time Claims: Always confirm that your provider is BWC Certified before receiving treatment. Your benefits may be reduced if you seek services at locations not listed. Some emergency room physicians, anesthesiologists, radiologists and pathologists may not be BWC Certified, even if the hospital is a BWC Certified Provider. For additional providers please contact GENEX Care for Ohio or go to 13

ELGIN LOCAL SCHOOLS. WORKERS COMPENSATION MANUALS AND FORMS For Elgin Administration
 ELGIN LOCAL SCHOOLS WORKERS COMPENSATION MANUALS AND FORMS For Elgin Administration Revised May 2014 1 ELGIN LOCAL SCHOOLS BUREAU OF WORKER S COMPENSATION CLAIM INSTRUCTIONS The Following steps must be
ELGIN LOCAL SCHOOLS WORKERS COMPENSATION MANUALS AND FORMS For Elgin Administration Revised May 2014 1 ELGIN LOCAL SCHOOLS BUREAU OF WORKER S COMPENSATION CLAIM INSTRUCTIONS The Following steps must be
Injury Reporting PACKET. 1-888-627-7586 www.careworksmco.com
 Injury Reporting PACKET 1-888-627-7586 www.careworksmco.com Workplace Injury. Take the Right Steps. Helping Simplify the First Report of Injury (FROI) Process 1 2 3 4 INJURED EMPLOYEE 4-STEP PROCESS Immediately
Injury Reporting PACKET 1-888-627-7586 www.careworksmco.com Workplace Injury. Take the Right Steps. Helping Simplify the First Report of Injury (FROI) Process 1 2 3 4 INJURED EMPLOYEE 4-STEP PROCESS Immediately
Workers Compensation
 Workers Compensation All work-related injuries or illnesses must be reported. If the injury is an emergency, arrange for appropriate medical treatment. The employee has the right to select his or her own
Workers Compensation All work-related injuries or illnesses must be reported. If the injury is an emergency, arrange for appropriate medical treatment. The employee has the right to select his or her own
WORKERS COMPENSATION EMPLOYEE S NOTICE OF INJURY (COMPLETE ALL ITEMS)
") WORKERS COMPENSATION EMPLOYEE S NOTICE OF INJURY (COMPLETE ALL ITEMS) EMPLOYEE S NAME: (last) (first) EMPLOYEE S ADDRESS: (no.) (street) (city) (state) (zip) TELEPHONE: Home: Work: SOCIAL SECURITY NO.
WORKERS COMPENSATION EMPLOYEE S NOTICE OF INJURY (COMPLETE ALL ITEMS) EMPLOYEE S NAME: (last) (first) EMPLOYEE S ADDRESS: (no.) (street) (city) (state) (zip) TELEPHONE: Home: Work: SOCIAL SECURITY NO.
WORKERS' COMPENSATION CLAIMANT INFORMATION PACKET
 WORKERS' COMPENSATION CLAIMANT INFORMATION PACKET Instructions Statement of Rights Prescription ID and Pharmacy Information The New York State Insurance Fund TLC EMERGENCY MEDICAL SERVICES Inc. TLC MEDICAL
WORKERS' COMPENSATION CLAIMANT INFORMATION PACKET Instructions Statement of Rights Prescription ID and Pharmacy Information The New York State Insurance Fund TLC EMERGENCY MEDICAL SERVICES Inc. TLC MEDICAL
BASIC INFORMATION FOR EMPLOYEES WORKERS' COMPENSATION BENEFITS AND INSTRUCTIONS FOR FILING A CLAIM
 BASIC INFORMATION FOR EMPLOYEES WORKERS' COMPENSATION BENEFITS AND INSTRUCTIONS FOR FILING A CLAIM I The Ohio Bureau of Workers' Compensation (BWC) provides employees with the following benefits for work
BASIC INFORMATION FOR EMPLOYEES WORKERS' COMPENSATION BENEFITS AND INSTRUCTIONS FOR FILING A CLAIM I The Ohio Bureau of Workers' Compensation (BWC) provides employees with the following benefits for work
Injury Reporting Packet
 Injury Reporting Packet University of Cincinnati 1-888-627-7586 www.careworks.com IMPORTANT NOTICE FOR WORKPLACE INJURIES In the event of a work-related injury when University Health Services is open,
Injury Reporting Packet University of Cincinnati 1-888-627-7586 www.careworks.com IMPORTANT NOTICE FOR WORKPLACE INJURIES In the event of a work-related injury when University Health Services is open,
Accident/Incident & Workers Compensation. Packet
 Accident/Incident & Workers Compensation Packet Accident/Incident & Workers Compensation Program The following information is to assist you in completing the Accident/Incident & Workers Compensation Program
Accident/Incident & Workers Compensation Packet Accident/Incident & Workers Compensation Program The following information is to assist you in completing the Accident/Incident & Workers Compensation Program
EMPLOYEE INJURY REPORTING PROCEDURE
 Updated 8/1/2014 TDY MEDICAL STAFFING, Inc. EMPLOYEE INJURY REPORTING PROCEDURE STEP 1: IS INJURY LIFE THREATENING/EMERGENCY? Call 911/go to ER if yes. STEP 2: CALL CLAIM INTO TDY 215-736-5147 STEP 3:
Updated 8/1/2014 TDY MEDICAL STAFFING, Inc. EMPLOYEE INJURY REPORTING PROCEDURE STEP 1: IS INJURY LIFE THREATENING/EMERGENCY? Call 911/go to ER if yes. STEP 2: CALL CLAIM INTO TDY 215-736-5147 STEP 3:
Employee Guidelines for Workers Compensation Accidents
 Employee Guidelines for Workers Compensation Accidents The information included in this packet will become important to you in the event that you seek medical attention or lose time from work due to a
Employee Guidelines for Workers Compensation Accidents The information included in this packet will become important to you in the event that you seek medical attention or lose time from work due to a
STANDARD OPERATING PROCEDURE SOP Sec. 5.4 Workers Compensation Incident Reporting
 This SOP implements Section 5.4 of the Policy Manual. A. If an incident occurs in which an employee is injured during the course of and arising out of his/her employment with the County, the employee shall:
This SOP implements Section 5.4 of the Policy Manual. A. If an incident occurs in which an employee is injured during the course of and arising out of his/her employment with the County, the employee shall:
WORKERS= COMPENSATION INCIDENT CHECKLIST
 WORKERS= COMPENSATION INCIDENT CHECKLIST This checklist is to be completed by the IMMEDIATE SUPERVISOR of the injured employee. This packet is VERY TIME-SENSITIVE. All forms in the packet should be completed
WORKERS= COMPENSATION INCIDENT CHECKLIST This checklist is to be completed by the IMMEDIATE SUPERVISOR of the injured employee. This packet is VERY TIME-SENSITIVE. All forms in the packet should be completed
For Employees: Employees: What What to to do do when when an an accident occurs 08/19/14/dmv
 For Employees: What to do when an accident occurs 08/19/14/dmv When there is a work-related accident or illness, procedures must be taken to ensure the employees needs are met with respect to treatment
For Employees: What to do when an accident occurs 08/19/14/dmv When there is a work-related accident or illness, procedures must be taken to ensure the employees needs are met with respect to treatment
Report ALL on-the-job injuries to
 1817 N. Stewart Street, Suite 20 Carson City, NV 89706 Phone: 775-283-0040 Toll Free: 888-873-4234 Fax: 775-283-0035 Report ALL on-the-job injuries to Tri-Odyssey Risk Management Department Phone: 775-283-0040
1817 N. Stewart Street, Suite 20 Carson City, NV 89706 Phone: 775-283-0040 Toll Free: 888-873-4234 Fax: 775-283-0035 Report ALL on-the-job injuries to Tri-Odyssey Risk Management Department Phone: 775-283-0040
STANISLAUS COUNTY OFFICE OF EDUCATION. Safety Department. Employee Workers Compensation Manual
 STANISLAUS COUNTY OFFICE OF EDUCATION Safety Department Employee Workers Compensation Manual T A B L E O F C O N T E N T S S E P T E M B E R 2 0 1 4 Introduction 3 Workers Compensation Defined 3 Workers
STANISLAUS COUNTY OFFICE OF EDUCATION Safety Department Employee Workers Compensation Manual T A B L E O F C O N T E N T S S E P T E M B E R 2 0 1 4 Introduction 3 Workers Compensation Defined 3 Workers
The County of Scotland Transitional Duty Policy
 The County of Scotland Transitional Duty Policy A. PURPOSE This policy defines the County of Scotland s Transitional Duty Program for employees who are injured on the job. B. POLICY/MISSION STATEMENT It
The County of Scotland Transitional Duty Policy A. PURPOSE This policy defines the County of Scotland s Transitional Duty Program for employees who are injured on the job. B. POLICY/MISSION STATEMENT It
Supervisors Workers' Compensation Injury Reporting Procedure Updated January 1, 2012
 Supervisors Workers' Compensation Injury Reporting Procedure Updated January 1, 2012 Call for medical response immediately if the injury is serious Worry about the forms later 1. If the injury is not an
Supervisors Workers' Compensation Injury Reporting Procedure Updated January 1, 2012 Call for medical response immediately if the injury is serious Worry about the forms later 1. If the injury is not an
Employee s Report of Work-Related Injury University of Maryland, College Park
 Employee s Report of Work-Related Injury To be completed immediately after the accident or initial treatment and submitted to your supervisor Employee Name: UID: Male (First) (Last) Female Date of Birth:
Employee s Report of Work-Related Injury To be completed immediately after the accident or initial treatment and submitted to your supervisor Employee Name: UID: Male (First) (Last) Female Date of Birth:
Workers Compensation Program Employee Information Packet
 Workers Compensation Program Employee Information Packet The information included in this packet will become important to you in the event that you seek medical attention or lose time from work due to
Workers Compensation Program Employee Information Packet The information included in this packet will become important to you in the event that you seek medical attention or lose time from work due to
HANOVER COUNTY PUBLIC SCHOOLS
 POLICY The School Board provides Workers Compensation insurance coverage at no cost to employees. This insurance program covers an injury (by accident) or illness (occupational disease) which arises out
POLICY The School Board provides Workers Compensation insurance coverage at no cost to employees. This insurance program covers an injury (by accident) or illness (occupational disease) which arises out
WORKERS COMPENSATION OVERVIEW
 WORKERS COMPENSATION OVERVIEW Personnel Coordinator & Workers Compensation Specialist Stark County Commissioners Human Resources Department Canton, Ohio Pg. 18 Claim reporting Red Flags Table of Contents:
WORKERS COMPENSATION OVERVIEW Personnel Coordinator & Workers Compensation Specialist Stark County Commissioners Human Resources Department Canton, Ohio Pg. 18 Claim reporting Red Flags Table of Contents:
Workers Compensation Claims Reporting. What do I do after a Workers Compensation accident occurs?
 Workers Compensation Claims Reporting What do I do after a Workers Compensation accident occurs? Secure medical treatment for your injured employee. If during normal business hours, use an Occupational
Workers Compensation Claims Reporting What do I do after a Workers Compensation accident occurs? Secure medical treatment for your injured employee. If during normal business hours, use an Occupational
Employee s Report of Injury Form
 Employee s Report of Injury Form Instructions: Employees shall use this form to report all work related injuries, illnesses, or near miss events (which could have caused an injury or illness) no matter
Employee s Report of Injury Form Instructions: Employees shall use this form to report all work related injuries, illnesses, or near miss events (which could have caused an injury or illness) no matter
#6-604 Accident Reporting Policy Page 1 of 5
 Page 1 of 5 Approved By: Cabinet Effective Date: January 2, 2013 Category: Contact: Human Resources Assistant Vice President for Human Resources (585) 245-5516 I. PURPOSE This document outlines the policies
Page 1 of 5 Approved By: Cabinet Effective Date: January 2, 2013 Category: Contact: Human Resources Assistant Vice President for Human Resources (585) 245-5516 I. PURPOSE This document outlines the policies
ACCIDENT, INJURY, AND INCIDENT REPORTING PROCEDURES
 ACCIDENT, INJURY, AND INCIDENT REPORTING PROCEDURES VEHICLE ACCIDENTS/PROPERTY DAMAGE Non-Workers Compensation Accident Report Form Attached is a sample copy of the accident report for vehicle damage,
ACCIDENT, INJURY, AND INCIDENT REPORTING PROCEDURES VEHICLE ACCIDENTS/PROPERTY DAMAGE Non-Workers Compensation Accident Report Form Attached is a sample copy of the accident report for vehicle damage,
Workers Compensation Claim Form (DWC 1) & Notice of Potential Eligibility e3301 (rev. 01/12) DWC 1 (rev. 6/10)
 & Notice of Potential Eligibility e3301 (rev. 01/12) DWC 1 (rev. 6/10)") Workers' Compensation Claim Kit Instructions for Completing the Forms Required to Report a Work-Related Injury or Illness California Department of Human Resources Workers Compensation Program What are
Workers' Compensation Claim Kit Instructions for Completing the Forms Required to Report a Work-Related Injury or Illness California Department of Human Resources Workers Compensation Program What are
ATTORNEY-CLIENT WORKERS COMPENSTATION FEE CONTRACT AND AUTHORIZATION TO REPRESENT
 STATE OF GEORGIA ATTORNEY-CLIENT WORKERS COMPENSTATION FEE CONTRACT AND AUTHORIZATION TO REPRESENT I,, with a Social Security Number of the undersigned, do hereby retain the Ramos Law Firm, LLC, located
STATE OF GEORGIA ATTORNEY-CLIENT WORKERS COMPENSTATION FEE CONTRACT AND AUTHORIZATION TO REPRESENT I,, with a Social Security Number of the undersigned, do hereby retain the Ramos Law Firm, LLC, located
TORT CLAIM FORM PACKET
 TORT CLAIM FORM PACKET Please carefully read all of the information in this packet before completing and presenting your Tort Claim Form. Documents Contained in the Tort Claim Form Packet Instructions
TORT CLAIM FORM PACKET Please carefully read all of the information in this packet before completing and presenting your Tort Claim Form. Documents Contained in the Tort Claim Form Packet Instructions
COUNTY OF ALLEGHENY EMPLOYEE ACCIDENT REPORT
 COUNTY OF ALLEGHENY EMPLOYEE ACCIDENT REPORT Revised 05/13/14 Section 1: Identification Information Completed by Employee (Supervisor should verify that information is correct.) Employee Name Last First
COUNTY OF ALLEGHENY EMPLOYEE ACCIDENT REPORT Revised 05/13/14 Section 1: Identification Information Completed by Employee (Supervisor should verify that information is correct.) Employee Name Last First
An Injured Workers Guide to the Workers Compensation Process Table of Contents
 An Injured Workers Guide to the Workers Compensation Process Table of Contents I. Claim Information A. General Information 1. What is workers compensation? 2. How do I know if I qualify for Workers Compensation?
An Injured Workers Guide to the Workers Compensation Process Table of Contents I. Claim Information A. General Information 1. What is workers compensation? 2. How do I know if I qualify for Workers Compensation?
Patient or Guardian Signature
 Co Payment Policy According to the regulations of individual insurance carriers, patients are responsible for paying co payments at the time of each office visit. PAYMENT POLICY FOR SERVICES RENDERED If
Co Payment Policy According to the regulations of individual insurance carriers, patients are responsible for paying co payments at the time of each office visit. PAYMENT POLICY FOR SERVICES RENDERED If
STATE OF NEW MEXICO WORKERS COMPENSATION ADMINISTRATION. WCA No.: PETITION FOR LUMP SUM PAYMENT RETURN TO WORK
 ,, and, WCA No.: PETITION FOR LUMP SUM PAYMENT RETURN TO WORK This form should be used for lump sums after return to work for 6 months, earning at least 80% of the pre-injury wage pursuant to 52-5-12(B).
,, and, WCA No.: PETITION FOR LUMP SUM PAYMENT RETURN TO WORK This form should be used for lump sums after return to work for 6 months, earning at least 80% of the pre-injury wage pursuant to 52-5-12(B).
WC-1 EMPLOYER S REPORT OF INDUSTRIAL INJURY
 Every work injury to an employee causing abscence for one day or more or which requires medical services other than first aid treatment must be reported within 7 working days after the injury. Failure
Every work injury to an employee causing abscence for one day or more or which requires medical services other than first aid treatment must be reported within 7 working days after the injury. Failure
J. Richard Lilly, M.D., A.B.F.P., & Associates, P.C.
 J. Richard Lilly, M.D., A.B.F.P., & Associates, P.C. PATIENT REGISTRATION - Please PRINT Clearly Patient Name First Middle Last Date of Birth Age Home Address Apt. No. City State Zip code Occupation Social
J. Richard Lilly, M.D., A.B.F.P., & Associates, P.C. PATIENT REGISTRATION - Please PRINT Clearly Patient Name First Middle Last Date of Birth Age Home Address Apt. No. City State Zip code Occupation Social
Delaware State University
 Delaware State University University Responsible Unit: Risk and Safety Management; Office of Human Resources Policy Number and Name: 7-12 Worker s Compensation Policy Approval Date: April 13, 2015 Next
Delaware State University University Responsible Unit: Risk and Safety Management; Office of Human Resources Policy Number and Name: 7-12 Worker s Compensation Policy Approval Date: April 13, 2015 Next
GROUP TOTAL & PERMANENT DISABILITY CLAIM FORM
 GROUP TOTAL & PERMANENT DISABILITY CLAIM FORM A Member of the OCBC Group CLAIM SUBMISSION PROCEDURES Please read carefully before you complete the attached Claim Form. 1. 2. The Great Eastern Life Assurance
GROUP TOTAL & PERMANENT DISABILITY CLAIM FORM A Member of the OCBC Group CLAIM SUBMISSION PROCEDURES Please read carefully before you complete the attached Claim Form. 1. 2. The Great Eastern Life Assurance
Wayne Physical Medicine & Rehabilitation Associates 401 Hamburg Turnpike, Suite 105 Wayne, NJ 07470
 PLEASE FILL OUT THIS SHEET COMPLETELY AND CORRECTLY. PLEASE PROVIDE ALL INSURANCE CARDS TO THE RECEPTIONIST TO COPY. Name Social Security # Address City, State & Zip Code Home Phone No. ( ) Cell Phone
PLEASE FILL OUT THIS SHEET COMPLETELY AND CORRECTLY. PLEASE PROVIDE ALL INSURANCE CARDS TO THE RECEPTIONIST TO COPY. Name Social Security # Address City, State & Zip Code Home Phone No. ( ) Cell Phone
How To File A Worker S Compensation Claim In Azoria
 Workers Compensation Instructions for Filing a Claim Please complete following steps within 24 48 hours of the incident: Report the incident to your supervisor immediately or, if a medical emergency, dial
Workers Compensation Instructions for Filing a Claim Please complete following steps within 24 48 hours of the incident: Report the incident to your supervisor immediately or, if a medical emergency, dial
WORKERS COMPENSATION GUIDELINES Reporting and Processing Workers Compensation Claims
 WORKERS COMPENSATION GUIDELINES Reporting and Processing Workers Compensation Claims In the following pages you will find frequently asked questions and answers regarding the reporting and processing of
WORKERS COMPENSATION GUIDELINES Reporting and Processing Workers Compensation Claims In the following pages you will find frequently asked questions and answers regarding the reporting and processing of
CLAIMANT RIGHTS AND RESPONSIBILITIES RULES FOR FILING A CLAIM AND APPEAL RIGHTS
 DIVISION OF TEMPORARY DISABILITY INSURANCE CLAIM FOR DISABILITY BENEFITS (DS-1) DETACH THIS PAGE AND KEEP FOR YOUR RECORDS CLAIMANT RIGHTS AND RESPONSIBILITIES RULES FOR FILING A CLAIM AND APPEAL RIGHTS
DIVISION OF TEMPORARY DISABILITY INSURANCE CLAIM FOR DISABILITY BENEFITS (DS-1) DETACH THIS PAGE AND KEEP FOR YOUR RECORDS CLAIMANT RIGHTS AND RESPONSIBILITIES RULES FOR FILING A CLAIM AND APPEAL RIGHTS
TEXAS DEPARTMENT OF CRIMINAL JUSTICE Supervisor s Report Packet for Workers Compensation CONTENTS
 Supervisor s Report Packet for Workers Compensation CONTENTS PERS 299-1, Supervisor s Guidelines for Workers Compensation PERS 299-2, Witness Statement PERS 299-3, Supplemental Worksheet PERS 299 (09/15)
Supervisor s Report Packet for Workers Compensation CONTENTS PERS 299-1, Supervisor s Guidelines for Workers Compensation PERS 299-2, Witness Statement PERS 299-3, Supplemental Worksheet PERS 299 (09/15)
ACCIDENT / INJURY REPORTING PROCEDURES FOR GEORGIA STATE UNIVERSITY
 ACCIDENT / INJURY REPORTING PROCEDURES FOR GEORGIA STATE UNIVERSITY FOR ANY LIFE THREATENING EMERGENCY ** SEEK TREATMENT IMMEDIATELY THEN FOLLOW THE PROCEDURES THAT FOLLOW **LIFE THREATENING EMERGENCIES
ACCIDENT / INJURY REPORTING PROCEDURES FOR GEORGIA STATE UNIVERSITY FOR ANY LIFE THREATENING EMERGENCY ** SEEK TREATMENT IMMEDIATELY THEN FOLLOW THE PROCEDURES THAT FOLLOW **LIFE THREATENING EMERGENCIES
Lifetouch Orthopedic Physical Therapy. -- PLEASE PRINT -- Patient Information. Proper Name First Middle Last Name you use
 Lifetouch Orthopedic Physical Therapy How did you find out about Lincoln Orthopedic Physical Therapy? Past patient/friend or family Physician Yellow Pages Web Site Location/Street sign Attorney/Nurse Case
Lifetouch Orthopedic Physical Therapy How did you find out about Lincoln Orthopedic Physical Therapy? Past patient/friend or family Physician Yellow Pages Web Site Location/Street sign Attorney/Nurse Case
Sports Injury CLAIM FORM. Call ATC for assistance on 1800 994 694. 1. You complete Section A and B.
 INSURANCE SOLUTIONS CLAIM FORM Sports Injury EXTF03520130320 Call ATC for assistance on 1800 994 694 1. You complete Section A and B. 2. If you have a Non Medicare Expense claim, you should also complete
INSURANCE SOLUTIONS CLAIM FORM Sports Injury EXTF03520130320 Call ATC for assistance on 1800 994 694 1. You complete Section A and B. 2. If you have a Non Medicare Expense claim, you should also complete
HAMILTON COUNTY WORKERS COMPENSATION HANDBOOK
 HAMILTON COUNTY WORKERS COMPENSATION HANDBOOK Prepared by: Hamilton County Human Resources Risk Management/Workers Compensation Division Last Updated: 12/2013 INTRODUCTION TO WORKERS COMPENSATION Workers
HAMILTON COUNTY WORKERS COMPENSATION HANDBOOK Prepared by: Hamilton County Human Resources Risk Management/Workers Compensation Division Last Updated: 12/2013 INTRODUCTION TO WORKERS COMPENSATION Workers
WORKERS COMPENSATION CLAIM REPORTING PROCEDURES
 WORKERS COMPENSATION CLAIM REPORTING PROCEDURES 1. Complete the enclosed First Report of Injury to ensure that you will have all of the appropriate questions answered during the reporting process. Have
WORKERS COMPENSATION CLAIM REPORTING PROCEDURES 1. Complete the enclosed First Report of Injury to ensure that you will have all of the appropriate questions answered during the reporting process. Have
Virginia South Psychiatric & Family Services
 All forms must be completed before seeing the Physician Information for Medical Records Patient s Name: Social Security #: Date of Birth: Sex: Male Female Marital Status: Single Married Divorced Widow
All forms must be completed before seeing the Physician Information for Medical Records Patient s Name: Social Security #: Date of Birth: Sex: Male Female Marital Status: Single Married Divorced Widow
LAWRENCE COUNTY MEMORIAL HOSPITAL Lawrenceville, Illinois. NOTICE OF PRIVACY PRACTICES Effective April 14, 2003 Revised May, 2013
 LAWRENCE COUNTY MEMORIAL HOSPITAL Lawrenceville, Illinois NOTICE OF PRIVACY PRACTICES Effective April 14, 2003 Revised May, 2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU WILL BE USED AND
LAWRENCE COUNTY MEMORIAL HOSPITAL Lawrenceville, Illinois NOTICE OF PRIVACY PRACTICES Effective April 14, 2003 Revised May, 2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU WILL BE USED AND
Injury Reporting Procedure
 Injury Reporting Procedure Your business is very important to us, and we're dedicated to providing you with the resources you need to help you be as successful as possible. Toward that end, Paychex Business
Injury Reporting Procedure Your business is very important to us, and we're dedicated to providing you with the resources you need to help you be as successful as possible. Toward that end, Paychex Business
CLAIMS REPORTING TO REPORT AN INJURY CALL 1-866-274-6033. 24 hours a day / 7 days a week
 CLAIMS REPORTING TO REPORT AN INJURY CALL 1-866-274-6033 24 hours a day / 7 days a week You will need the following information to report a claim. However, do not delay reporting if you are missing information.
CLAIMS REPORTING TO REPORT AN INJURY CALL 1-866-274-6033 24 hours a day / 7 days a week You will need the following information to report a claim. However, do not delay reporting if you are missing information.
Injury Illness Response and Reporting Procedure
 Injury Illness Response and Reporting Procedure Policy: The following is the procedure for reporting and response to injuries or illnesses for employees, students, official volunteers and/or visitors at
Injury Illness Response and Reporting Procedure Policy: The following is the procedure for reporting and response to injuries or illnesses for employees, students, official volunteers and/or visitors at
WORKER S COMPENSATION TREATMENT AUTHORIZATION FORM
 FLORIDA TECH EMPLOYEE ACCIDENT/ INJURY REPORT Contact Financial Affairs @ 674-7297 OR 8885 IMMEDIATELY regarding an Employee's Injury. Employee AND Supervisor must complete this report. EMPLOYEE INFORMATION
FLORIDA TECH EMPLOYEE ACCIDENT/ INJURY REPORT Contact Financial Affairs @ 674-7297 OR 8885 IMMEDIATELY regarding an Employee's Injury. Employee AND Supervisor must complete this report. EMPLOYEE INFORMATION
Humana short-term income protection claim form
 Humana short-term income protection claim form 1-866-836-6144 Instructions Please read and follow the instructions carefully. 1. If this is the initial claim for benefit payments for this disability, please
Humana short-term income protection claim form 1-866-836-6144 Instructions Please read and follow the instructions carefully. 1. If this is the initial claim for benefit payments for this disability, please
We thank you for your business, and look forward to providing you with the necessary protection and care for your business and employees.
 RE: Workers Compensation Claims Kit Welcome to the Workers Compensation Insurance Program offered through Tower Group Companies. While we hope that your company never has to experience a workers compensation
RE: Workers Compensation Claims Kit Welcome to the Workers Compensation Insurance Program offered through Tower Group Companies. While we hope that your company never has to experience a workers compensation
How To Write A Workers Compensation Check
 WORKERS COMPENSATION Office of Human Resources WHAT IS WORKERS COMPENSATION? Workers Compensation is a University paid benefit for employees and students that are working payroll or work study. Workers
WORKERS COMPENSATION Office of Human Resources WHAT IS WORKERS COMPENSATION? Workers Compensation is a University paid benefit for employees and students that are working payroll or work study. Workers
 WC 101 : From Injury to Closure WC Claim Rights & Responsibilities Jennifer Flood, Ombudsman for Injured Workers Lisa Wilch, Claims Director SAIF Corporation Today s Session Claim filing Claim decisions
WC 101 : From Injury to Closure WC Claim Rights & Responsibilities Jennifer Flood, Ombudsman for Injured Workers Lisa Wilch, Claims Director SAIF Corporation Today s Session Claim filing Claim decisions
BWC Basics. for Injured Workers
 BWC Basics for Injured Workers TABLE OF CONTENTS What s workers comp?...4 Ohio law...4 Staying informed...4 Help is available for you...4 Injured workers rights...5 Claims decisions...6 Claim allowed or
BWC Basics for Injured Workers TABLE OF CONTENTS What s workers comp?...4 Ohio law...4 Staying informed...4 Help is available for you...4 Injured workers rights...5 Claims decisions...6 Claim allowed or
Accident/Illness Claim
 QBE INSURANCE (AUSTRALIA) LIMITED ABN 78 003 191 035 Accident/Illness Claim The issue of this form does not constitute an admission of liability on the part of the insurer. Please complete all sections
QBE INSURANCE (AUSTRALIA) LIMITED ABN 78 003 191 035 Accident/Illness Claim The issue of this form does not constitute an admission of liability on the part of the insurer. Please complete all sections
Journey Injury CLAIM FORM. Call ATC Claims for assistance on 1800 994 694. 1. You complete Section A.
 INSURANCE SOLUTIONS CLAIM FORM Journey Injury EXTF052 Call ATC Claims for assistance on 1800 994 694 1. You complete Section A. 2. Your Medical Practitioner completes Section B. 3. Your Employer completes
INSURANCE SOLUTIONS CLAIM FORM Journey Injury EXTF052 Call ATC Claims for assistance on 1800 994 694 1. You complete Section A. 2. Your Medical Practitioner completes Section B. 3. Your Employer completes
For the purpose of this Procedure the following definitions will apply:
 Procedure 6.5: Workplace Safety and Injury Reporting Volume 6 Managing Office: Office of Human Resources Effective Date: March 15, 2011 Revised: June 2014 I. GENERAL POLICY Alabama A&M University ( AAMU
Procedure 6.5: Workplace Safety and Injury Reporting Volume 6 Managing Office: Office of Human Resources Effective Date: March 15, 2011 Revised: June 2014 I. GENERAL POLICY Alabama A&M University ( AAMU
Claim Filing Instructions & Claim Form
 Claim Filing Instructions & Claim Form Please follow these instructions prior to filing a claim and when completing the Claim Form. Assistance is also available from the IMG Customer Service Department
Claim Filing Instructions & Claim Form Please follow these instructions prior to filing a claim and when completing the Claim Form. Assistance is also available from the IMG Customer Service Department
Workers' Compensation
 Workers' Compensation Accident Reporting Procedures LISD FORMS AVAILABLE AT THE SAFETY WEBSITE ARE IN BOLD LETTERS 1. Employee reports accident or near miss to campus/department Safety Officer. The Safety
Workers' Compensation Accident Reporting Procedures LISD FORMS AVAILABLE AT THE SAFETY WEBSITE ARE IN BOLD LETTERS 1. Employee reports accident or near miss to campus/department Safety Officer. The Safety
Stonebridge Adult Medicine, P.A. Registration Form (Please Print)
") Stonebridge Adult Medicine, P.A. Registration Form (Please Print) PATIENT INFORMATION Last Name: First Name: Is this your legal name? Yes No If not what is your legal name: Date of Birth: Sex: male female
Stonebridge Adult Medicine, P.A. Registration Form (Please Print) PATIENT INFORMATION Last Name: First Name: Is this your legal name? Yes No If not what is your legal name: Date of Birth: Sex: male female
Notice of Claim. Last First Middle Area Code/ Telephone Number. Last First Middle Area Code/ Telephone Number
 Claimant: Notice of Claim Last First Middle Area Code/ Telephone Number Street Address Additional Address City State Zip Date of Birth Social Security Number If Notices and correspondence in connection
Claimant: Notice of Claim Last First Middle Area Code/ Telephone Number Street Address Additional Address City State Zip Date of Birth Social Security Number If Notices and correspondence in connection
PLEASE COMPLETE AND RETURN
 PLEASE COMPLETE AND RETURN Voluntary Care Network Application Name of Client (Last) (First) (Middle Initial) Street Address Telephone (home) City State Zip Telephone (alternate) Date of Birth US Citizen
PLEASE COMPLETE AND RETURN Voluntary Care Network Application Name of Client (Last) (First) (Middle Initial) Street Address Telephone (home) City State Zip Telephone (alternate) Date of Birth US Citizen
Sports Injury CLAIM FORM. Call ATC Claims for assistance on 1800 994 694. 1. You complete Section A and B.
 INSURANCE SOLUTIONS CLAIM FORM Sports Injury EXTF04820140311 Call ATC Claims for assistance on 1800 994 694 1. You complete Section A and B. 2. If you have a Non Medicare Expense claim, you should also
INSURANCE SOLUTIONS CLAIM FORM Sports Injury EXTF04820140311 Call ATC Claims for assistance on 1800 994 694 1. You complete Section A and B. 2. If you have a Non Medicare Expense claim, you should also
HUMAN RESOURCES POLICY Fauquier County, Virginia
 HUMAN RESOURCES POLICY Fauquier County, Virginia Policy Title: Workers Compensation Effective Date: 05/17/04 36 Supersedes Policy: 09/04/90 I. PURPOSE It is the objective of the Board of Supervisors that
HUMAN RESOURCES POLICY Fauquier County, Virginia Policy Title: Workers Compensation Effective Date: 05/17/04 36 Supersedes Policy: 09/04/90 I. PURPOSE It is the objective of the Board of Supervisors that
STANDARD TORT CLAIM FORM PACKET
 STANDARD TORT CLAIM FORM PACKET Please carefully read all of the information in this packet before completing and presenting your Standard Tort Claim. DOCUMENTS CONTAINED IN THE STANDARD TORT CLAIM FORM
STANDARD TORT CLAIM FORM PACKET Please carefully read all of the information in this packet before completing and presenting your Standard Tort Claim. DOCUMENTS CONTAINED IN THE STANDARD TORT CLAIM FORM
Personal Accident / Illness Claim Form
 Thank you for notifying us of your claim. Please complete this claim form and return it to: Specialty Claims Services PO Box 51541 LONDON SE1 0XU If you need any help in completing this form please contact
Thank you for notifying us of your claim. Please complete this claim form and return it to: Specialty Claims Services PO Box 51541 LONDON SE1 0XU If you need any help in completing this form please contact
Workers Compensation Injury/Illness Reporting
 Workers Compensation Injury/Illness Reporting s I. Introductions/Objectives This document outlines the procedures and responsibilities for reporting injuries, illnesses, accidents and medical emergencies
Workers Compensation Injury/Illness Reporting s I. Introductions/Objectives This document outlines the procedures and responsibilities for reporting injuries, illnesses, accidents and medical emergencies
STATE OF ARIZONA DURABLE HEALTH CARE POWER OF ATTORNEY Instructions and Form
 STATE OF ARIZONA DURABLE HEALTH CARE POWER OF ATTORNEY Instructions and Form GENERAL INSTRUCTIONS: Use this Durable Health Care Power of Attorney form if you want to select a person to make future health
STATE OF ARIZONA DURABLE HEALTH CARE POWER OF ATTORNEY Instructions and Form GENERAL INSTRUCTIONS: Use this Durable Health Care Power of Attorney form if you want to select a person to make future health
Claim Filing Instructions & Claim Form
 Claim Filing Instructions & Claim Form Please follow these instructions prior to filing a claim and when completing the Claim Form. Assistance is also available from the International Medical Group (IMG
Claim Filing Instructions & Claim Form Please follow these instructions prior to filing a claim and when completing the Claim Form. Assistance is also available from the International Medical Group (IMG
The ACCG Claims Office staff is here to help you. Please feel free to call us with your questions and concerns.
 1 WELCOME This handbook contains information prepared by the Association County Commissioners of Georgia - Group Self-Insurance Workers Compensation Fund (ACCG - GSIWCF) to assist employees and management
1 WELCOME This handbook contains information prepared by the Association County Commissioners of Georgia - Group Self-Insurance Workers Compensation Fund (ACCG - GSIWCF) to assist employees and management
APPLICATION FOR BENEFITS LAW ENFORCEMENT OFFICERS AND FIRE FIGHTERS DISABILITY BENEFITS TRUST FUND
 EXHIBIT A M S Attorney General s Office Use Only: Application #: Receipt Date: G Approved G Disapproved Claim type: G Law Enforcement Officer G Fire Fighter STOP. Please read the fund policies and procedures
EXHIBIT A M S Attorney General s Office Use Only: Application #: Receipt Date: G Approved G Disapproved Claim type: G Law Enforcement Officer G Fire Fighter STOP. Please read the fund policies and procedures
CLAIMS PROCEDURE Anker Crew Insurance
 CLAIMS PROCEDURE Anker Crew Insurance cm-aci-cpt apr-2014 page 1 of 10 CLAIMS CONTACT DIRECTORY Office Paterswoldseweg 812 NL - 9728 BM Groningen P.O. Box 8002 NL - 9702 KA Groningen T +31 50 520 97 79
CLAIMS PROCEDURE Anker Crew Insurance cm-aci-cpt apr-2014 page 1 of 10 CLAIMS CONTACT DIRECTORY Office Paterswoldseweg 812 NL - 9728 BM Groningen P.O. Box 8002 NL - 9702 KA Groningen T +31 50 520 97 79
FREQUENTLY ASKED QUESTIONS FOR DISABILTY RETIREMENT
 Important: These frequently asked questions provide a general summary of certain features of disability retirement benefits payable from the Maryland State Retirement and Pension System ( SRPS ). SRPS
Important: These frequently asked questions provide a general summary of certain features of disability retirement benefits payable from the Maryland State Retirement and Pension System ( SRPS ). SRPS
NT WORKERS COMPENSATION CLAIM FORM
 Information for Workers Guidance to PART 1 of the Claim Form Notify your employer of your injury, verbally or in writing, as soon as practicable. Fully complete PART 1 (questions 1 to 8) of the following
Information for Workers Guidance to PART 1 of the Claim Form Notify your employer of your injury, verbally or in writing, as soon as practicable. Fully complete PART 1 (questions 1 to 8) of the following
IRVING & ASSOCIATES IN BEHAVIORAL HEALTH, P.C. 5151 Mochel Drive, Suite 307 Downers Grove, IL 60515
 : / / Client Name: _ SSN: / / of Birth: Age: Sex: Male Female Address: City/State/Zip: Home Phone Number Is it okay to leave a message here? Y/N Work Number Is it okay to leave a message here? Y/N Cell
: / / Client Name: _ SSN: / / of Birth: Age: Sex: Male Female Address: City/State/Zip: Home Phone Number Is it okay to leave a message here? Y/N Work Number Is it okay to leave a message here? Y/N Cell
OFFICE OF THE ARIZONA ATTORNEY GENERAL Mark Brnovich. STATE OF ARIZONA DURABLE HEALTH CARE POWER OF ATTORNEY Instructions and Form
 OFFICE OF THE ARIZONA ATTORNEY GENERAL Mark Brnovich STATE OF ARIZONA DURABLE HEALTH CARE POWER OF ATTORNEY Instructions and Form GENERAL INSTRUCTIONS: Use this Durable Health Care Power of Attorney form
OFFICE OF THE ARIZONA ATTORNEY GENERAL Mark Brnovich STATE OF ARIZONA DURABLE HEALTH CARE POWER OF ATTORNEY Instructions and Form GENERAL INSTRUCTIONS: Use this Durable Health Care Power of Attorney form
HIPAA NOTICE OF PRIVACY PRACTICES
 HIPAA NOTICE OF PRIVACY PRACTICES Marden Rehabilitation Associates, Inc. Marden Rehabilitation Associates of Ohio, Inc. Marden Rehabilitation Associates of West Virginia Health Care Plus Preferred Care
HIPAA NOTICE OF PRIVACY PRACTICES Marden Rehabilitation Associates, Inc. Marden Rehabilitation Associates of Ohio, Inc. Marden Rehabilitation Associates of West Virginia Health Care Plus Preferred Care
Patient Demographic Form
 Patient Demographic Form New Patient Returning Patient Primary Care Physician (PCP) Name: Patient Name: Last Name First Name MI Address: P.O. Box City: State: Zip: Cellular Number: Home Number: Work Number:
Patient Demographic Form New Patient Returning Patient Primary Care Physician (PCP) Name: Patient Name: Last Name First Name MI Address: P.O. Box City: State: Zip: Cellular Number: Home Number: Work Number: