Opioids Research to Practice
|
|
|
- Peregrine Cummings
- 10 years ago
- Views:
Transcription
1 Opioids Research to Practice CRIT/FIT 2015 May 2015 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research and Education (CARE) Unit

2 Case 32 yo female brought in after heroin overdose Brisk response to IV naloxone 0.4 mg Re-sedation after 1 hr requiring repeat naloxone Arm cellulitis at injection drug use site Admitted for drug overdose, persistent altered mental status and arm cellulitis

3
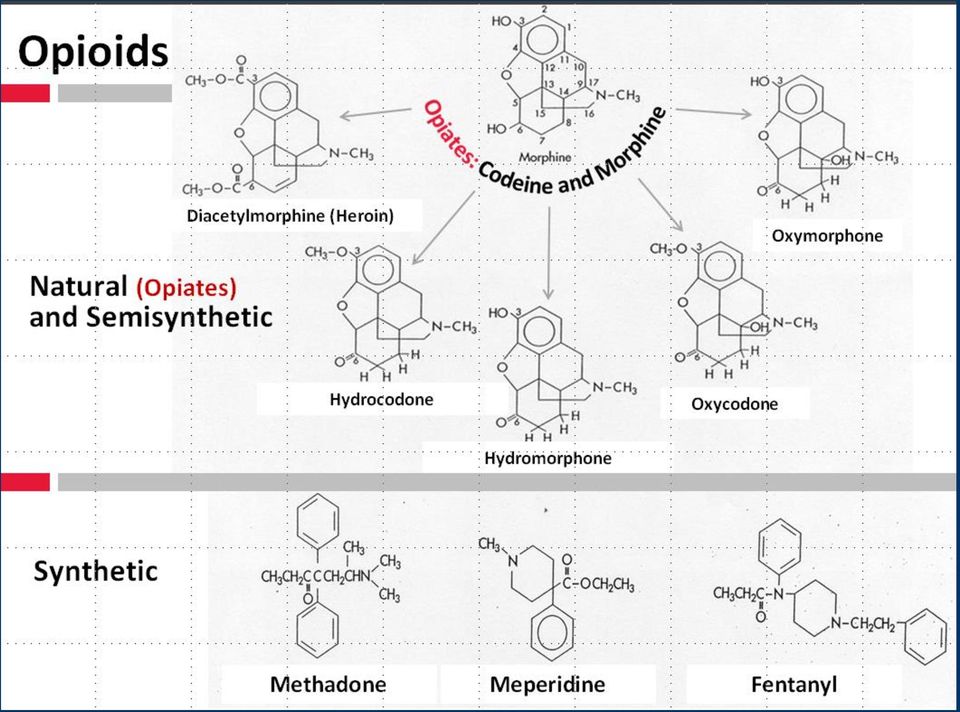
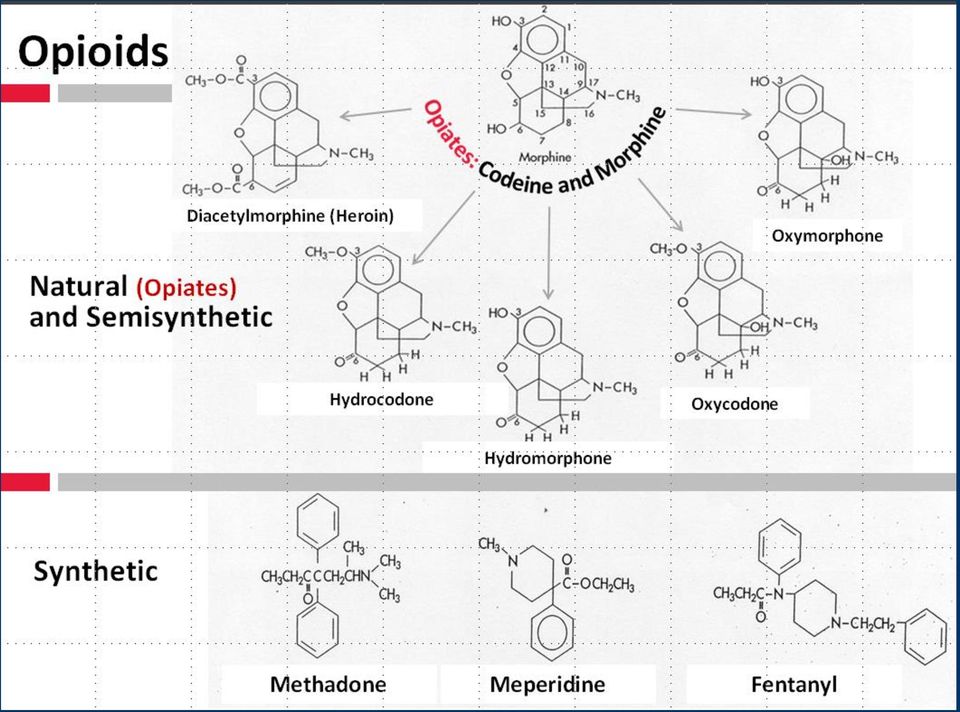
4 Why is heroin so pleasurable? Heroin is highly lipid soluble Crosses blood brain barrier within 15 seconds= rush After IV administration 68% heroin in brain compared to <5% of morphine Within 30 minutes metabolized to morphine HEROIN is a prodrug of MORPHINE

5 Withdrawal Normal Euphoria Natural History of Opioid Use Disorder Tolerance & Physical Dependence Acute use Chronic use

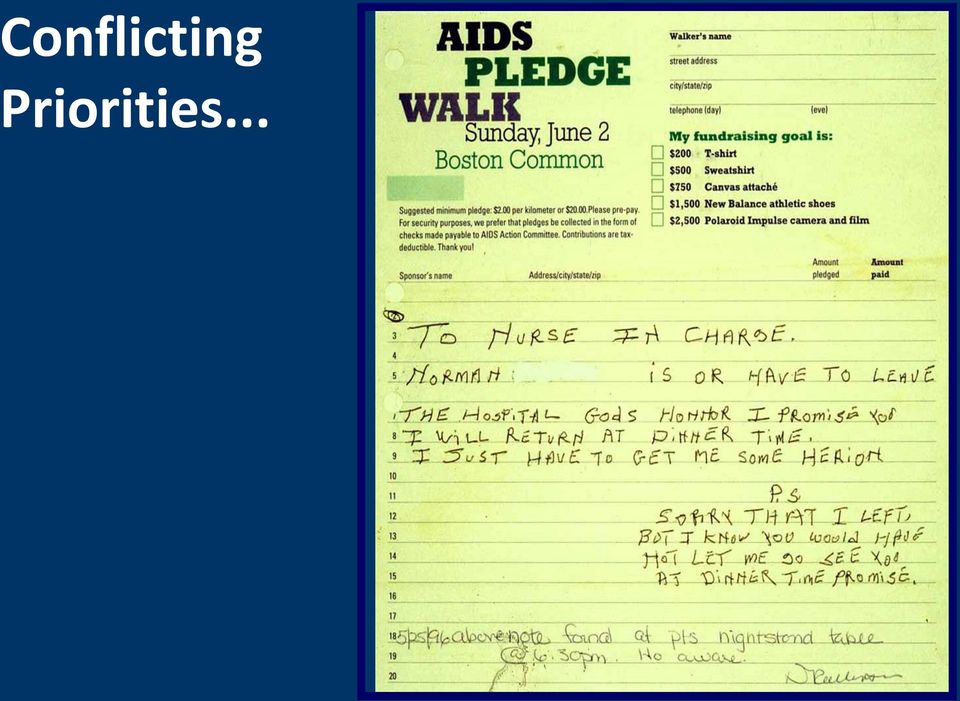
6 Conflicting Priorities...
7 Case continued Substance use history ½ gram of heroin/day Intranasal use for 6 months then IV for 7 years Had been in recovery for 2 years by going to NA but relapsed 3 months ago Denies sharing needles History of 10 detox s, no maintenance treatment No other drug, alcohol or tobacco use HIV and hepatitis C negative Unemployed elementary school teacher Lives with husband (in recovery) and 2 young children Now complaining of opioid withdrawal How will you assess and treat her?
 and 2 young children Now complaining of opioid withdrawal How will you assess")
8 Which is NOT a sign of opioid withdrawal? 1. Vomiting 2. Diarrhea 3. Pinpoint pupils 4. Rhinorrhea 5. Lacrimation 6. Piloerection 0% 0% 0% 0% 0% 0%

9 Opioid Withdrawal Assessment Grade Anxiety, Drug Craving Symptoms / Signs Yawning, Sweating, Runny nose, Tearing eyes, Restlessness Insomnia Dilated pupils, Gooseflesh, Muscle twitching & shaking, Muscle & Joint aches, Loss of appetite Nausea, extreme restlessness, elevated blood pressure, Heart rate > 100, Fever Vomiting / dehydration, Diarrhea, Abdominal cramps, Curled-up body position Clinical Opiate Withdrawal Scale (COWS): pulse, sweating, restlessness & anxiety, pupil size, aches, runny nose & tearing, GI sx, tremor, yawning, gooseflesh (score 5-12 mild, mod, mod sev, severe)

10 How is acute opioid withdrawal treated on your inpatient service? 1. Clonidine 2. Methadone 3. Buprenorphine 4. Don t know 5. Other 0% 0% 0% 0% 0%

11 Inpatient Goals Prevent/treat acute opioid withdrawal Inadequate treatment may prevent full treatment of medical/surgical condition Do not expect to cure opioid dependence during this hospital stay Withholding opioids will not cure patient s addiction Giving opioids will not worsen patient s addiction Diagnose and treat medical illness Initiate substance abuse treatment referral

12 Inpatient Goals Methadone is the best choice! or buprenorphine (more expensive) Other Clonidine (hyperadrenergic state) + NSAIDS (muscle cramps and pain) + Benzodiazepines (insomnia) + Dicyclomine (abdominal cramps) + Bismuth subsalicylate (diarrhea)
 + Dicyclomine (abdominal cramps) +")
13 Inpatient Methadone Dosing Guidelines Assess signs and symptoms of acute opioid withdrawal Reassure patient Discuss specific dose and goals openly with patient and nursing staff Don t use heroin : methadone conversions

14 Inpatient Methadone Dosing Guidelines Start with 20 mg of methadone Reassess q 2-3 hours, give additional 5-10 mg until withdrawal signs abate Do not exceed 40 mg in 24 hours Monitor for CNS and respiratory depression

15 Inpatient Methadone Dosing Guidelines On following day, give total dose QD Goal is to alleviate acute withdrawal Patient will continue to crave opioids Discuss taper vs maintained dose w/ pt daily Referral for long-term substance abuse treatment

16 Inpatient Methadone Dosing Guidelines Maintained dose option Give same dose each daily including day of discharge Allows hour withdrawal-free period after d/c Tapered dose option If patient requests a taper, decrease by 5 mg per day and stop taper if patient requests it Don t prolong hospitalization to complete taper Don t give a prescription for methadone

17 Case continued Hospital course Arm Cellulitis treated with IV Vancomycin Opioid withdrawal Day 1 Methadone 20 mg Day 2 Very anxious, demanded increase in methadone dose Was off the floor for 2 hours Repeat urine drug test was positive for opiates

18 All of the following are possible explanations for her opiate positive drug test EXCEPT? 1. Illicit opioid (heroin) use during hospitalization 2. Heroin use prior to admission 3. Hydromorphone (Dilaudid) given for pain last night 4. Methadone given during hospitalization 0% 0% 0% 0%
 given for pain last night 4.")
19
20 Case continued 6 months later She presents to your primary care clinic requesting treatment for her heroin addiction She has been using heroin since the day she left the hospital

21 Case continued Recommended options from primary care Narcotics Anonymous (NA) Clonidine + NSAID + benzodiazepine + Naltrexone (po or injectable) Buprenorphine maintenance (if waivered) Overdose prevention education and naloxone Referral Detoxification program Needle exchange Acupuncture Outpatient counseling Methadone maintenance Buprenorphine maintenance (if not waivered)
22 Opioid Detoxification Outcomes Low rates of retention in treatment High rates of relapse post-treatment < 50% abstinent at 6 months < 15% abstinent at 12 months Increased rates of overdose due to decreased tolerance O Connor PG JAMA 2005 Mattick RP, Hall WD. Lancet 1996 Stimmel B et al. JAMA 1977
23 Reasons for Relapse Protracted abstinence syndrome Secondary to derangement of endogenous opioid receptor system Symptoms Generalized malaise, fatigue, insomnia Poor tolerance to stress and pain Opioid craving Conditioned cues (triggers) Priming with small dose of drug
 Methadone (full opioid agonist) Buprenorphine (partial opioid")
24 Pharmacotherapy Goals Alleviate physical withdrawal Opioid blockade Alleviate drug craving Normalized deranged brain changes and physiology Some options Naltrexone (opioid antagonist) Methadone (full opioid agonist) Buprenorphine (partial opioid agonist)
25 Withdrawal Normal Euphoria Opioid Agonist Treatment (OAT) Acute use Tolerance & Physical Dependence Chronic use OAT Maintenance
26 Naltrexone Pure opioid antagonist Oral naltrexone Well tolerated, safe Duration of action hours FDA approved 1984 Injectable naltrexone (Vivitrol ) IM injection (w/ customized needle) once/month FDA approved 2010 Patients must be opioid free for a minimum of 7-10 days before treatment
27 Oral Naltrexone 10 RCTs ~700 participants to naltrexone alone or with psychosocial therapy compared with psychosocial therapy alone or placebo No clear benefit in treatment retention or relapse at follow up Benefit in highly motivated patients Impaired physicians > 80% abstinence at 18 months Cochrane Database of Systematic Reviews 2006

28 Injectable Naltrexone (XR-NTX) Multicenter (13 sites in Russia-OAT unavailable) DB RPCT 24 weeks 250 individuals with opioid dependence randomized to XR-NRT vs placebo All offered biweekly individual drug counseling Funded by pharmaceutical company - Alkermes Krupitsky E, et al. Lancet, 2011
29 Methadone Hydrochloride Full opioid agonist PO onset of action minutes Duration of action hours to treat opioid addiction 6-8 hours to treat pain Proper dosing for opioid addiction mg for acute withdrawal > 80 mg for craving, opioid blockade
30 Methadone Maintenance Over 45 Years of Experience JAMA 1965 JAMA 2005
31 METHADONE IN OTPS FOR OUD:
32 Methadone Maintenance Still controversial I don t believe in methadone substituting one drug for another liquid handcuffs
33 Methadone Maintenance Dosing
34 Ball JC, Ross A. The effectiveness of methadone maintenance treatment, 1991
35 Effects of Psychosocial Services McLellan, AT et.al, J AMA 1993
36 What is the single best question to assess a patient s success on methadone maintenance treatment? 1. Are you using drugs? 2. Are you on take home doses? 3. Are you compliant with methadone treatment? 4. How long have you been on methadone treatment? 0% 0% 0% 0%
37 Methadone Maintenance Treatment Highly Structured Daily nursing assessment Weekly individual and/or group counseling Random supervised drug testing Psychiatric services Medical services Methadone dosing Observed daily Take homes
38 In a Comprehensive Rehabilitation Program Increases overall survival Increases treatment retention Decreases illicit opioid use Decreases hepatitis and HIV seroconversion Decreases criminal activity Increases employment Improves birth outcomes
39 Methadone Maintenance Limitations Highly regulated - Narcotic Addict Treatment Act 1974 Created methadone clinics (Opioid Treatment Programs) Separate system not involving primary care or pharmacists Limited access Inconvenient and highly punitive Mixes stable and unstable patients Lack of privacy No ability to graduate from program Stigma
40 DATA 2000 and Buprenorphine 2000: Drug Addiction Treatment Act (DATA) 2000 Allows qualified physician to prescribe scheduled III - V, narcotic FDA approved for opioid maintenance or detoxification treatment limit 30 patients per practice 2002: Suboxone and Subutex FDA approved 2005: Limit to 30 patients per physician 2007: Limit to 100 patients per physician after 1 year
41 Physician Qualifications The physician is licensed under State law and qualified based on one of the following: Certified in Addiction Psychiatry or Medicine Completed eight hours of training List of trainings: Online training:
42 Buprenorphine Buprenorphine (Subutex or generic) mono Buprenorphine + naloxone (Suboxone) combo Schedule III Sublingual tablets, film Treatment of opioid dependence High receptor affinity Slow dissociation Ceiling effect for respiratory depression
43 BUPRENORPHINE FOR OUD: Turner L et al. Am J Addict 2014
44 Remaining in treatment (nr) Buprenorphine Maintenance versus Taper % retention 75% UTS negative 20% mortality in placebo group Control Buprenorphine Treatment duration (days) Kakko J et al. Lancet 2003
45 Buprenorphine Efficacy Studies (RCT) show buprenorphine more effective than placebo and equally effective to moderate doses (80 mg) of methadone on primary outcomes of: Abstinence from illicit opioid use Retention in treatment Decreased opioid craving Johnson et al. NEJM 2000 Fudala PJ et al. NEJM 2003 Kakko J et al. Lancet 2003
46 Methadone vs Buprenorphine 9 OTPs n=1,267 RCT buprenorphine vs methadone 6 month retention Hser Y, et al. Addiction. 2014
47 Opioid Maintenance Treatment and Acute Pain Management Patients on opioid maintenance treatment (i.e. methadone or buprenorphine) have less pain tolerance then matched controls Patients who are physically dependent on opioids (i.e. methadone or buprenorphine) must be maintained on daily equivalence before ANY analgesic effect is realized with opioids used for acute pain management Opioid analgesic requirements are often higher due to increased pain sensitivity and opioid cross tolerance Alford DP, Compton P, Samet JH. Ann Intern Med 2006
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2011 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2011 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Treatment of opioid use disorders
 Treatment of opioid use disorders Gerardo Gonzalez, MD Associate Professor of Psychiatry Director, Division of Addiction Psychiatry Disclosures I have no financial conflicts to disclose I will review evidence
Treatment of opioid use disorders Gerardo Gonzalez, MD Associate Professor of Psychiatry Director, Division of Addiction Psychiatry Disclosures I have no financial conflicts to disclose I will review evidence
Treatment of Opioid Dependence with Buprenorphine/Naloxone (Suboxone )
") Treatment of Opioid Dependence with Buprenorphine/Naloxone (Suboxone ) Elinore F. McCance-Katz, M.D., Ph.D. Professor and Chair, Addiction Psychiatry Virginia Commonwealth University Neurobiology of Opiate
Treatment of Opioid Dependence with Buprenorphine/Naloxone (Suboxone ) Elinore F. McCance-Katz, M.D., Ph.D. Professor and Chair, Addiction Psychiatry Virginia Commonwealth University Neurobiology of Opiate
COMMUNITY BUPRENORPHINE PRESCRIBING IN OPIATE DEPENDENCE
 COMMUNITY BUPRENORPHINE PRESCRIBING IN OPIATE DEPENDENCE INTRODUCTION High dose sublingual buprenorphine (Subutex) tablets are available in the following strengths 0.4 mg, 2 mg, and 8 mg. Suboxone tablets,
COMMUNITY BUPRENORPHINE PRESCRIBING IN OPIATE DEPENDENCE INTRODUCTION High dose sublingual buprenorphine (Subutex) tablets are available in the following strengths 0.4 mg, 2 mg, and 8 mg. Suboxone tablets,
How To Treat Anorexic Addiction With Medication Assisted Treatment
 Medication Assisted Treatment for Opioid Addiction Tanya Hiser, MS, LPC Premier Care of Wisconsin, LLC October 21, 2015 How Did We Get Here? Civil War veterans and women 19th Century physicians cautious
Medication Assisted Treatment for Opioid Addiction Tanya Hiser, MS, LPC Premier Care of Wisconsin, LLC October 21, 2015 How Did We Get Here? Civil War veterans and women 19th Century physicians cautious
Assessment and Management of Opioid, Benzodiazepine, and Sedative-Hypnotic Withdrawal
 Assessment and Management of Opioid, Benzodiazepine, and Sedative-Hypnotic Withdrawal Roger Cicala, M. D. Assistant Medical Director Tennessee Physician s Wellness Program Step 1 Don t 1 It is legal in
Assessment and Management of Opioid, Benzodiazepine, and Sedative-Hypnotic Withdrawal Roger Cicala, M. D. Assistant Medical Director Tennessee Physician s Wellness Program Step 1 Don t 1 It is legal in
Buprenorphine: what is it & why use it?
 Buprenorphine: what is it & why use it? Dr Nicholas Lintzeris, MBBS, PhD, FAChAM Locum Consultant, Oaks Resource Centre, SLAM National Addiction Centre, Institute of Psychiatry Overview of presentation
Buprenorphine: what is it & why use it? Dr Nicholas Lintzeris, MBBS, PhD, FAChAM Locum Consultant, Oaks Resource Centre, SLAM National Addiction Centre, Institute of Psychiatry Overview of presentation
Integrating Medication- Assisted Treatment (MAT) for Opioid Use Disorders into Behavioral and Physical Healthcare Settings
 for Opioid Use Disorders into Behavioral and Physical Healthcare Settings") Integrating Medication- Assisted Treatment (MAT) for Opioid Use Disorders into Behavioral and Physical Healthcare Settings All-Ohio Conference 3/27/2015 Christina M. Delos Reyes, MD Medical Consultant,
Integrating Medication- Assisted Treatment (MAT) for Opioid Use Disorders into Behavioral and Physical Healthcare Settings All-Ohio Conference 3/27/2015 Christina M. Delos Reyes, MD Medical Consultant,
MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION
 MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION Sidarth Wakhlu,M.D. Addiction Team Leader North Texas VA Health Care System Addiction Psychiatry Fellowship Director Associate Professor Of Psychiatry
MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION Sidarth Wakhlu,M.D. Addiction Team Leader North Texas VA Health Care System Addiction Psychiatry Fellowship Director Associate Professor Of Psychiatry
Considerations in Medication Assisted Treatment of Opiate Dependence. Stephen A. Wyatt, D.O. Dept. of Psychiatry Middlesex Hospital Middletown, CT
 Considerations in Medication Assisted Treatment of Opiate Dependence Stephen A. Wyatt, D.O. Dept. of Psychiatry Middlesex Hospital Middletown, CT Disclosures Speaker Panels- None Grant recipient - SAMHSA
Considerations in Medication Assisted Treatment of Opiate Dependence Stephen A. Wyatt, D.O. Dept. of Psychiatry Middlesex Hospital Middletown, CT Disclosures Speaker Panels- None Grant recipient - SAMHSA
MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION
 MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION Mark Fisher Program Administrator State Opioid Treatment Adminstrator Kentucky Division of Behavioral Health OBJECTIVES Learn about types of opioids and
MEDICATION ASSISTED TREATMENT FOR OPIOID ADDICTION Mark Fisher Program Administrator State Opioid Treatment Adminstrator Kentucky Division of Behavioral Health OBJECTIVES Learn about types of opioids and
Treatment and Interventions for Opioid Addictions: Challenges From the Medical Director s Perspective
 Treatment and Interventions for Opioid Addictions: Challenges From the Medical Director s Perspective Dale K. Adair, MD Medical Director/Chief Psychiatric Officer OMHSAS 1 Treatment and Interventions for
Treatment and Interventions for Opioid Addictions: Challenges From the Medical Director s Perspective Dale K. Adair, MD Medical Director/Chief Psychiatric Officer OMHSAS 1 Treatment and Interventions for
Medication-Assisted Addiction Treatment
 Medication-Assisted Addiction Treatment Molly Carney, Ph.D., M.B.A. Executive Director Evergreen Treatment Services Seattle, WA What is MAT? MAT is the use of medications, in combination with counseling
Medication-Assisted Addiction Treatment Molly Carney, Ph.D., M.B.A. Executive Director Evergreen Treatment Services Seattle, WA What is MAT? MAT is the use of medications, in combination with counseling
Care Management Council submission date: August 2013. Contact Information
 Clinical Practice Approval Form Clinical Practice Title: Acute use of Buprenorphine for the Treatment of Opioid Dependence and Detoxification Type of Review: New Clinical Practice Revisions of Existing
Clinical Practice Approval Form Clinical Practice Title: Acute use of Buprenorphine for the Treatment of Opioid Dependence and Detoxification Type of Review: New Clinical Practice Revisions of Existing
Neurobiology and Treatment of Opioid Dependence. Nebraska MAT Training September 29, 2011
 Neurobiology and Treatment of Opioid Dependence Nebraska MAT Training September 29, 2011 Top 5 primary illegal drugs for persons age 18 29 entering treatment, % 30 25 20 15 10 Heroin or Prescription Opioids
Neurobiology and Treatment of Opioid Dependence Nebraska MAT Training September 29, 2011 Top 5 primary illegal drugs for persons age 18 29 entering treatment, % 30 25 20 15 10 Heroin or Prescription Opioids
OVERVIEW OF MEDICATION ASSISTED TREATMENT
 Sarah Akerman MD Assistant Professor of Psychiatry Director of Addiction Services Geisel School of Medicine/Dartmouth-Hitchcock Medical Center OVERVIEW OF MEDICATION ASSISTED TREATMENT Conflicts of Interest
Sarah Akerman MD Assistant Professor of Psychiatry Director of Addiction Services Geisel School of Medicine/Dartmouth-Hitchcock Medical Center OVERVIEW OF MEDICATION ASSISTED TREATMENT Conflicts of Interest
Substitution Therapy for Opioid Dependence The Role of Suboxone. Mandy Manak, MD, ABAM, CCSAM Methadone 101-Hospitalist Workshop, October 3, 2015
 Substitution Therapy for Opioid Dependence The Role of Suboxone Mandy Manak, MD, ABAM, CCSAM Methadone 101-Hospitalist Workshop, October 3, 2015 Objectives Recognize the options available in treating opioid
Substitution Therapy for Opioid Dependence The Role of Suboxone Mandy Manak, MD, ABAM, CCSAM Methadone 101-Hospitalist Workshop, October 3, 2015 Objectives Recognize the options available in treating opioid
KAP Keys. For Physicians. Based on TIP 40 Clinical Guidelines for the Use of Buprenorphine in the Treatment. of Opioid Addiction
 Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Knowledge Application Program KAP Keys For Physicians Based on TIP 40 Clinical Guidelines for the Use of Buprenorphine
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Knowledge Application Program KAP Keys For Physicians Based on TIP 40 Clinical Guidelines for the Use of Buprenorphine
Like cocaine, heroin is a drug that is illegal in some areas of the world. Heroin is highly addictive.
 Heroin Introduction Heroin is a powerful drug that affects the brain. People who use it can form a strong addiction. Addiction is when a drug user can t stop taking a drug, even when he or she wants to.
Heroin Introduction Heroin is a powerful drug that affects the brain. People who use it can form a strong addiction. Addiction is when a drug user can t stop taking a drug, even when he or she wants to.
EPIDEMIOLOGY OF OPIATE USE
 Opiate Dependence EPIDEMIOLOGY OF OPIATE USE Difficult to estimate true extent of opiate dependence Based on National Survey of Health and Mental Well Being: 1.2% sample used opiates in last 12 months
Opiate Dependence EPIDEMIOLOGY OF OPIATE USE Difficult to estimate true extent of opiate dependence Based on National Survey of Health and Mental Well Being: 1.2% sample used opiates in last 12 months
MEDICALLY SUPERVISED OPIATE WITHDRAWAL FOR THE DEPENDENT PATIENT. An Outpatient Model
 MEDICALLY SUPERVISED OPIATE WITHDRAWAL FOR THE DEPENDENT PATIENT An Outpatient Model OBJECTIVE TO PRESENT A PROTOCOL FOR THE EVALUATION AND TREATMENT OF PATIENTS WHO ARE CHEMICALLY DEPENDENT ON OR SEVERLY
MEDICALLY SUPERVISED OPIATE WITHDRAWAL FOR THE DEPENDENT PATIENT An Outpatient Model OBJECTIVE TO PRESENT A PROTOCOL FOR THE EVALUATION AND TREATMENT OF PATIENTS WHO ARE CHEMICALLY DEPENDENT ON OR SEVERLY
Frequently Asked Questions (FAQ s): Medication-Assisted Treatment for Opiate Addiction
: Medication-Assisted Treatment for Opiate Addiction") Frequently Asked Questions (FAQ s): Medication-Assisted Treatment for Opiate Addiction March 3, 2008 By: David Rinaldo, Ph.D., Managing Partner, The Avisa Group In this FAQ What medications are currently
Frequently Asked Questions (FAQ s): Medication-Assisted Treatment for Opiate Addiction March 3, 2008 By: David Rinaldo, Ph.D., Managing Partner, The Avisa Group In this FAQ What medications are currently
Joanna L. Starrels. 2 ND YEAR RESEARCH ELECTIVE RESIDENT S JOURNAL Volume VIII, 2003-2004. A. Study Purpose and Rationale
 Outpatient Treatment of Opiate Dependence with Sublingual Buprenorphine/Naloxone versus Methadone Maintenance: a Randomized Trial of Alternative Treatments in Real Life Settings Joanna L. Starrels A. Study
Outpatient Treatment of Opiate Dependence with Sublingual Buprenorphine/Naloxone versus Methadone Maintenance: a Randomized Trial of Alternative Treatments in Real Life Settings Joanna L. Starrels A. Study
One example: Chapman and Huygens, 1988, British Journal of Addiction
 This is a fact in the treatment of alcohol and drug abuse: Patients who do well in treatment do well in any treatment and patients who do badly in treatment do badly in any treatment. One example: Chapman
This is a fact in the treatment of alcohol and drug abuse: Patients who do well in treatment do well in any treatment and patients who do badly in treatment do badly in any treatment. One example: Chapman
Opiate Abuse and Mental Illness
 visited on Page 1 of 5 LEARN MORE (HTTP://WWW.NAMI.ORG/LEARN-MORE) FIND SUPPORT (HTTP://WWW.NAMI.ORG/FIND-SUPPORT) GET INVOLVED (HTTP://WWW.NAMI.ORG/GET-INVOLVED) DONATE (HTTPS://NAMI360.NAMI.ORG/EWEB/DYNAMICPAGE.ASPX?
visited on Page 1 of 5 LEARN MORE (HTTP://WWW.NAMI.ORG/LEARN-MORE) FIND SUPPORT (HTTP://WWW.NAMI.ORG/FIND-SUPPORT) GET INVOLVED (HTTP://WWW.NAMI.ORG/GET-INVOLVED) DONATE (HTTPS://NAMI360.NAMI.ORG/EWEB/DYNAMICPAGE.ASPX?
Death in the Suburbs: How Prescription Painkillers and Heroin Have Changed Treatment and Recovery
 Death in the Suburbs: How Prescription Painkillers and Heroin Have Changed Treatment and Recovery Marvin D. Seppala, MD Chief Medical Officer Hazelden Betty Ford Foundation This product is supported by
Death in the Suburbs: How Prescription Painkillers and Heroin Have Changed Treatment and Recovery Marvin D. Seppala, MD Chief Medical Officer Hazelden Betty Ford Foundation This product is supported by
 Medication-Assisted Treatment (MAT) & What It Means Long-Term Gary K. Byrd., M.Ed., MAC, CCS, CAMS Methadone is the Gold Standard for treatment of chronic heroin addiction Gary Byrd 2015 1 Gary Byrd 2015
Medication-Assisted Treatment (MAT) & What It Means Long-Term Gary K. Byrd., M.Ed., MAC, CCS, CAMS Methadone is the Gold Standard for treatment of chronic heroin addiction Gary Byrd 2015 1 Gary Byrd 2015
Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction. Frequently Asked Questions
 Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction Frequently Asked Questions What is Naltrexone? Naltrexone is a prescription drug that effectively blocks the effects of heroin, alcohol,
Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction Frequently Asked Questions What is Naltrexone? Naltrexone is a prescription drug that effectively blocks the effects of heroin, alcohol,
Program Assistance Letter
 Program Assistance Letter DOCUMENT NUMBER: 2004-01 DATE: December 5, 2003 DOCUMENT TITLE: Use of Buprenorphine in Health Center Substance Abuse Treatment Programs TO: All Bureau of Primary Health Care
Program Assistance Letter DOCUMENT NUMBER: 2004-01 DATE: December 5, 2003 DOCUMENT TITLE: Use of Buprenorphine in Health Center Substance Abuse Treatment Programs TO: All Bureau of Primary Health Care
Using Drugs to Treat Drug Addiction How it works and why it makes sense
 Using Drugs to Treat Drug Addiction How it works and why it makes sense Jeff Baxter, MD University of Massachusetts Medical School May 17, 2011 Objectives Biological basis of addiction Is addiction a chronic
Using Drugs to Treat Drug Addiction How it works and why it makes sense Jeff Baxter, MD University of Massachusetts Medical School May 17, 2011 Objectives Biological basis of addiction Is addiction a chronic
New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery
 New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery USING THE 48 HOUR OBSERVATION BED USING THE 48 HOUR OBSERVATION BED Detoxification
New York State Office of Alcoholism & Substance Abuse Services Addiction Services for Prevention, Treatment, Recovery USING THE 48 HOUR OBSERVATION BED USING THE 48 HOUR OBSERVATION BED Detoxification
Opioid Agreement for Center for Pain Management S.C.
 Opioid Agreement for Center for Pain Management S.C. Patient Name: DOB: I am the patient named above. I have agreed to use pain medication as part of my treatment for chronic pain. I understand that these
Opioid Agreement for Center for Pain Management S.C. Patient Name: DOB: I am the patient named above. I have agreed to use pain medication as part of my treatment for chronic pain. I understand that these
Update on Buprenorphine: Induction and Ongoing Care
 Update on Buprenorphine: Induction and Ongoing Care Elizabeth F. Howell, M.D., DFAPA, FASAM Department of Psychiatry, University of Utah School of Medicine North Carolina Addiction Medicine Conference
Update on Buprenorphine: Induction and Ongoing Care Elizabeth F. Howell, M.D., DFAPA, FASAM Department of Psychiatry, University of Utah School of Medicine North Carolina Addiction Medicine Conference
OPIOIDS. Petros Levounis, MD, MA Chair Department of Psychiatry Rutgers New Jersey Medical School
 OPIOIDS Petros Levounis, MD, MA Chair Department of Psychiatry Rutgers New Jersey Medical School Rutgers New Jersey Medical School Fundamentals of Addiction Medicine Summer Series Newark, NJ July 24, 2013
OPIOIDS Petros Levounis, MD, MA Chair Department of Psychiatry Rutgers New Jersey Medical School Rutgers New Jersey Medical School Fundamentals of Addiction Medicine Summer Series Newark, NJ July 24, 2013
Buprenorphine Therapy in Addiction Treatment
 Buprenorphine Therapy in Addiction Treatment Ken Roy, MD, FASAM Addiction Recovery Resources, Inc. River Oaks Hospital Tulane Department of Psychiatry www.arrno.org Like Minded Doc What is MAT? Definition
Buprenorphine Therapy in Addiction Treatment Ken Roy, MD, FASAM Addiction Recovery Resources, Inc. River Oaks Hospital Tulane Department of Psychiatry www.arrno.org Like Minded Doc What is MAT? Definition
Treatment of Opioid Dependence: A Randomized Controlled Trial. Karen L. Sees, DO, Kevin L. Delucchi, PhD, Carmen Masson, PhD, Amy
 Category: Heroin Title: Methadone Maintenance vs 180-Day psychosocially Enriched Detoxification for Treatment of Opioid Dependence: A Randomized Controlled Trial Authors: Karen L. Sees, DO, Kevin L. Delucchi,
Category: Heroin Title: Methadone Maintenance vs 180-Day psychosocially Enriched Detoxification for Treatment of Opioid Dependence: A Randomized Controlled Trial Authors: Karen L. Sees, DO, Kevin L. Delucchi,
Minimum Insurance Benefits for Patients with Opioid Use Disorder The Opioid Use Disorder Epidemic: The Evidence for Opioid Treatment:
 Minimum Insurance Benefits for Patients with Opioid Use Disorder By David Kan, MD and Tauheed Zaman, MD Adopted by the California Society of Addiction Medicine Committee on Opioids and the California Society
Minimum Insurance Benefits for Patients with Opioid Use Disorder By David Kan, MD and Tauheed Zaman, MD Adopted by the California Society of Addiction Medicine Committee on Opioids and the California Society
Information for Pharmacists
 Page 43 by 42 CFR part 2. A general authorization for the release of medical or other information is NOT sufficient for this purpose. Information for Pharmacists SUBOXONE (buprenorphine HCl/naloxone HCl
Page 43 by 42 CFR part 2. A general authorization for the release of medical or other information is NOT sufficient for this purpose. Information for Pharmacists SUBOXONE (buprenorphine HCl/naloxone HCl
Office-based Treatment of Opioid Dependence with Buprenorphine
 Office-based Treatment of Opioid Dependence with Buprenorphine David A. Fiellin, M.D Professor of Medicine, Investigative Medicine and Public Health Yale University School of Medicine Dr. Fiellin s Disclosures
Office-based Treatment of Opioid Dependence with Buprenorphine David A. Fiellin, M.D Professor of Medicine, Investigative Medicine and Public Health Yale University School of Medicine Dr. Fiellin s Disclosures
Beyond SBIRT: Integrating Addiction Medicine into Primary Care
 Beyond SBIRT: Integrating Addiction Medicine into Primary Care Community Clinic Association of Los Angeles County 14 th Annual Health Care Symposium March 6, 2015 Keith Heinzerling MD, Karen Lamp MD; Allison
Beyond SBIRT: Integrating Addiction Medicine into Primary Care Community Clinic Association of Los Angeles County 14 th Annual Health Care Symposium March 6, 2015 Keith Heinzerling MD, Karen Lamp MD; Allison
Using Buprenorphine in an Opioid Treatment Program
 Using Buprenorphine in an Opioid Treatment Program Thomas E. Freese, PhD Director of Training, UCLA Integrated Substance Abuse Programs Director, Pacific Southwest Addiction Technology Transfer Center
Using Buprenorphine in an Opioid Treatment Program Thomas E. Freese, PhD Director of Training, UCLA Integrated Substance Abuse Programs Director, Pacific Southwest Addiction Technology Transfer Center
MEDICAL ASSISTANCE BULLETIN
 ISSUE DATE September 4, 2015 SUBJECT EFFECTIVE DATE September 9, 2015 MEDICAL ASSISTANCE BULLETIN NUMBER *See below BY Prior Authorization of Opiate Dependence Treatments, Oral Buprenorphine Agents - Pharmacy
ISSUE DATE September 4, 2015 SUBJECT EFFECTIVE DATE September 9, 2015 MEDICAL ASSISTANCE BULLETIN NUMBER *See below BY Prior Authorization of Opiate Dependence Treatments, Oral Buprenorphine Agents - Pharmacy
The ABCs of Medication Assisted Treatment
 The ABCs of Medication Assisted Treatment J E F F R E Y Q U A M M E, E X E C U T I V E D I R E C T O R C O N N E C T I C U T C E R T I F I C A T I O N B O A R D The ABCs of Medication Assisted Treatment
The ABCs of Medication Assisted Treatment J E F F R E Y Q U A M M E, E X E C U T I V E D I R E C T O R C O N N E C T I C U T C E R T I F I C A T I O N B O A R D The ABCs of Medication Assisted Treatment
Buprenorphine/Naloxone Training Workshop for Medical Practitioners
 Buprenorphine/Naloxone Training Workshop for Medical Practitioners Program developed by Dr Nicholas Lintzeris MBBS, PhD, FAChAM (RACP) Turning Point Alcohol and Drug Centre, Melbourne, Australia Federation
Buprenorphine/Naloxone Training Workshop for Medical Practitioners Program developed by Dr Nicholas Lintzeris MBBS, PhD, FAChAM (RACP) Turning Point Alcohol and Drug Centre, Melbourne, Australia Federation
Prior Authorization Guideline
 Prior Authorization Guideline Guideline: CSD - Suboxone Therapeutic Class: Central Nervous System Agents Therapeutic Sub-Class: Analgesics and Antipyretics (Opiate Partial Agonists) Client: County of San
Prior Authorization Guideline Guideline: CSD - Suboxone Therapeutic Class: Central Nervous System Agents Therapeutic Sub-Class: Analgesics and Antipyretics (Opiate Partial Agonists) Client: County of San
MEDICAL ASSISTANCE BULLETIN
 ISSUE DATE SUBJECT EFFECTIVE DATE MEDICAL ASSISTANCE BULLETIN NUMBER *See below BY Prior Authorization of Opiate Dependence Treatments Pharmacy Service Leesa M. Allen, Deputy Secretary Office of Medical
ISSUE DATE SUBJECT EFFECTIVE DATE MEDICAL ASSISTANCE BULLETIN NUMBER *See below BY Prior Authorization of Opiate Dependence Treatments Pharmacy Service Leesa M. Allen, Deputy Secretary Office of Medical
Frequently asked questions
 Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction Frequently asked questions What is Naltrexone? Naltrexone is a prescription drug that completely blocks the effects of all opioid drugs
Naltrexone Pellet Treatment for Opiate, Heroin, and Alcohol Addiction Frequently asked questions What is Naltrexone? Naltrexone is a prescription drug that completely blocks the effects of all opioid drugs
Opiate Addiction in Ohio: An Update on Scope of Problem Ashland Ohio
 Governor s Cabinet Opiate Action Team Promoting Wellness and Recovery John R. Kasich, Governor Tracy J. Plouck, Director Opiate Addiction in Ohio: An Update on Scope of Problem Ashland Ohio November 14,
Governor s Cabinet Opiate Action Team Promoting Wellness and Recovery John R. Kasich, Governor Tracy J. Plouck, Director Opiate Addiction in Ohio: An Update on Scope of Problem Ashland Ohio November 14,
Heroin Overdose Trends and Treatment Options. Neil A. Capretto, D.O., F.A.S.A.M. Medical Director
 Heroin Overdose Trends and Treatment Options Neil A. Capretto, D.O., F.A.S.A.M. Medical Director Type date here www.gatewayrehab.org Drug Overdose Deaths Increasing in Allegheny County Roberta Lojak holds
Heroin Overdose Trends and Treatment Options Neil A. Capretto, D.O., F.A.S.A.M. Medical Director Type date here www.gatewayrehab.org Drug Overdose Deaths Increasing in Allegheny County Roberta Lojak holds
The Science of Addiction and Its Effective Treatment
 The Science of Addiction and Its Effective Treatment Anne Arundel County Opioid Misuse and Overdose Symposium April 15, 2015 D. Andrew Tompkins, M.D. M.H.S. Agenda 1. Terminology a. Addiction versus Substance
The Science of Addiction and Its Effective Treatment Anne Arundel County Opioid Misuse and Overdose Symposium April 15, 2015 D. Andrew Tompkins, M.D. M.H.S. Agenda 1. Terminology a. Addiction versus Substance
Guidelines for Titration onto Buprenorphine in Opioid Dependence
 NHS Fife Community Health Partnership Addiction Services Guidelines for Titration onto Buprenorphine in Opioid Dependence Intranet Procedure No. A7 Author Dr L. Cockayne Copy No 1 Reviewer Lead Clinician
NHS Fife Community Health Partnership Addiction Services Guidelines for Titration onto Buprenorphine in Opioid Dependence Intranet Procedure No. A7 Author Dr L. Cockayne Copy No 1 Reviewer Lead Clinician
Pharmacotherapy for Opioid Addiction: Drugs in Development
 Pharmacotherapy for Opioid Addiction: Drugs in Development Walter Ling MD UCLA/ISAP Pharmacotherapy for Prescription Opioid Addiction: Implications for Pain Management June 9-10, 2011 Boston, Mass. [email protected]
Pharmacotherapy for Opioid Addiction: Drugs in Development Walter Ling MD UCLA/ISAP Pharmacotherapy for Prescription Opioid Addiction: Implications for Pain Management June 9-10, 2011 Boston, Mass. [email protected]
Use of Vivitrol for Alcohol and Opioid Addiction
 Use of Vivitrol for Alcohol and Opioid Addiction Ken Bachrach, Ph.D. Clinical Director, Tarzana Treatment Centers, Inc. [email protected] What is Vivitrol? An injectable from of naltrexone, which
Use of Vivitrol for Alcohol and Opioid Addiction Ken Bachrach, Ph.D. Clinical Director, Tarzana Treatment Centers, Inc. [email protected] What is Vivitrol? An injectable from of naltrexone, which
Use of Buprenorphine in the Treatment of Opioid Addiction
 Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary Which of the following is an
Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary Which of the following is an
Update and Review of Medication Assisted Treatments
 Update and Review of Medication Assisted Treatments for Opiate and Alcohol Use Disorders Richard N. Whitney, MD Medical Director Addiction Services Shepherd Hill Newark, Ohio Medication Assisted Treatment
Update and Review of Medication Assisted Treatments for Opiate and Alcohol Use Disorders Richard N. Whitney, MD Medical Director Addiction Services Shepherd Hill Newark, Ohio Medication Assisted Treatment
Opioid Dependence Treatment with Buprenorphine/Naloxone: An Overview for Pharmacists and Physicians
 Opioid Dependence Treatment with Buprenorphine/Naloxone: An Overview for Pharmacists and Physicians Phyllis A. Grauer, PharmD, CGP, CPE Clinical Pharmacist Legislation Passed Enabling Office Based Treatment
Opioid Dependence Treatment with Buprenorphine/Naloxone: An Overview for Pharmacists and Physicians Phyllis A. Grauer, PharmD, CGP, CPE Clinical Pharmacist Legislation Passed Enabling Office Based Treatment
Acute & Chronic Pain Management (requiring opioid analgesics) in Patients Receiving Pharmacotherapy for Opioid Addiction
 in Patients Receiving Pharmacotherapy for Opioid Addiction") Acute & Chronic Pain Management (requiring opioid analgesics) in Patients Receiving Pharmacotherapy for Opioid Addiction June 9, 2011 Tufts Health Care Institute Program on Opioid Risk Management Daniel
Acute & Chronic Pain Management (requiring opioid analgesics) in Patients Receiving Pharmacotherapy for Opioid Addiction June 9, 2011 Tufts Health Care Institute Program on Opioid Risk Management Daniel
Oxford Health NHS Foundation Trust. A guide to Opioid Detoxification
 Oxford Health NHS Foundation Trust A guide to Opioid Detoxification If you re considering detox, congratulations. You have obviously been visualising a drug free life and planning your future goals. Detox
Oxford Health NHS Foundation Trust A guide to Opioid Detoxification If you re considering detox, congratulations. You have obviously been visualising a drug free life and planning your future goals. Detox
Naltrexone and Alcoholism Treatment Test
 Naltrexone and Alcoholism Treatment Test Following your reading of the course material found in TIP No. 28. Please read the following statements and indicate the correct answer on the answer sheet. A score
Naltrexone and Alcoholism Treatment Test Following your reading of the course material found in TIP No. 28. Please read the following statements and indicate the correct answer on the answer sheet. A score
In 2010, approximately 8 million Americans 18 years and older were dependent on alcohol.
 Vivitrol Pilot Study: SEMCA/Treatment Providers Collaborative Efforts with the treatment of Opioid Dependent Clients Hakeem Lumumba, PhD, CAADC SEMCA Scott Schadel, MSW, LMSW, CAADC HEGIRA PROGRAMS, INC.
Vivitrol Pilot Study: SEMCA/Treatment Providers Collaborative Efforts with the treatment of Opioid Dependent Clients Hakeem Lumumba, PhD, CAADC SEMCA Scott Schadel, MSW, LMSW, CAADC HEGIRA PROGRAMS, INC.
BUPRENORPHINE TREATMENT
 BUPRENORPHINE TREATMENT Curriculum Infusion Package (CIP) Based on the Work of Dr. Thomas Freese of the Pacific Southwest ATTC Drug Addiction Treatment Act of 2000 (DATA 2000) Developed by Mountain West
BUPRENORPHINE TREATMENT Curriculum Infusion Package (CIP) Based on the Work of Dr. Thomas Freese of the Pacific Southwest ATTC Drug Addiction Treatment Act of 2000 (DATA 2000) Developed by Mountain West
FRN Research Report January 2012: Treatment Outcomes for Opiate Addiction at La Paloma
 FRN Research Report January 2012: Treatment Outcomes for Opiate Addiction at La Paloma Background A growing opiate abuse epidemic has highlighted the need for effective treatment options. This study documents
FRN Research Report January 2012: Treatment Outcomes for Opiate Addiction at La Paloma Background A growing opiate abuse epidemic has highlighted the need for effective treatment options. This study documents
Guidelines for the Prescribing, Supply and Administration of Methadone and Buprenorphine on Transfer of Care
 Hull & East Riding Prescribing Committee Guidelines for the Prescribing, Supply and Administration of Methadone and Buprenorphine on Transfer of Care 1. BACKGROUND Patients who are physically dependent
Hull & East Riding Prescribing Committee Guidelines for the Prescribing, Supply and Administration of Methadone and Buprenorphine on Transfer of Care 1. BACKGROUND Patients who are physically dependent
Financial Disclosures
 Opioid Agonist Therapy: To Maintain or Not To Maintain - A Case Discussion PCSS-MAT American Psychiatric Association Drs. Ed Salsitz, John Renner, Timothy Fong April 14, 2015 Financial Disclosures Edwin
Opioid Agonist Therapy: To Maintain or Not To Maintain - A Case Discussion PCSS-MAT American Psychiatric Association Drs. Ed Salsitz, John Renner, Timothy Fong April 14, 2015 Financial Disclosures Edwin
John R. Kasich, Governor Orman Hall, Director
 John R. Kasich, Governor Orman Hall, Director 2 3 Epidemics of unintentional drug overdoses in Ohio, 1979-2011 1,2,3 1800 1600 1400 1200 1000 800 Prescription drugs are causing a larger overdose epidemic
John R. Kasich, Governor Orman Hall, Director 2 3 Epidemics of unintentional drug overdoses in Ohio, 1979-2011 1,2,3 1800 1600 1400 1200 1000 800 Prescription drugs are causing a larger overdose epidemic
Medication-Assisted Treatment for Opioid Addiction
 Medication-Assisted Treatment for Opioid Addiction This document contains a general discussion of medications approved by the U.S. Food and Drug Administration (FDA) for use in the treatment of opioid
Medication-Assisted Treatment for Opioid Addiction This document contains a general discussion of medications approved by the U.S. Food and Drug Administration (FDA) for use in the treatment of opioid
Opioid/Opiate Dependent Pregnant Women
 Opioid/Opiate Dependent Pregnant Women The epidemic, safety, stigma, and how to help. Presented by Lisa Ramirez MA,LCDC & Kerby Stewart MD The prescription painkiller epidemic is killing more women than
Opioid/Opiate Dependent Pregnant Women The epidemic, safety, stigma, and how to help. Presented by Lisa Ramirez MA,LCDC & Kerby Stewart MD The prescription painkiller epidemic is killing more women than
The Federation of State Medical Boards 2013 Model Guidelines for Opioid Addiction Treatment in the Medical Office
 The Federation of State Medical Boards 2013 Model Guidelines for Opioid Addiction Treatment in the Medical Office Adopted April 2013 for Consideration by State Medical Boards 2002 FSMB Model Guidelines
The Federation of State Medical Boards 2013 Model Guidelines for Opioid Addiction Treatment in the Medical Office Adopted April 2013 for Consideration by State Medical Boards 2002 FSMB Model Guidelines
CLINICAL POLICY Department: Medical Management Document Name: Vivitrol Reference Number: NH.PHAR.96 Effective Date: 03/12
 Page: 1 of 7 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
Page: 1 of 7 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
Opioid Treatment Services, Office-Based Opioid Treatment
 Optum 1 By United Behavioral Health U.S. Behavioral Health Plan, California Doing Business as OptumHealth Behavioral Solutions of California ( OHBS-CA ) 2015 Level of Care Guidelines Opioid Treatment Services,
Optum 1 By United Behavioral Health U.S. Behavioral Health Plan, California Doing Business as OptumHealth Behavioral Solutions of California ( OHBS-CA ) 2015 Level of Care Guidelines Opioid Treatment Services,
methadonefact.qxd 8/11/01 2:05 PM Page 1 INFORMATION Advantages of methadone treatment DEPRESSANT Methadone maintenance Pregnancy METHADONE
 methadonefact.qxd 8/11/01 2:05 PM Page 1 INFORMATION Advantages of methadone treatment 10 DEPRESSANT Methadone maintenance Pregnancy METHADONE methadonefact.qxd 8/11/01 2:05 PM Page 2 WHAT IS METHADONE
methadonefact.qxd 8/11/01 2:05 PM Page 1 INFORMATION Advantages of methadone treatment 10 DEPRESSANT Methadone maintenance Pregnancy METHADONE methadonefact.qxd 8/11/01 2:05 PM Page 2 WHAT IS METHADONE
Substance Abuse Treatment. Naltrexone for Extended-Release Injectable Suspension for Treatment of Alcohol Dependence
 Spring 2007 Volume 6 Issue 1 ADVISORY News for the Treatment Field Naltrexone for Extended-Release Injectable Suspension for Treatment of Alcohol Dependence What is naltrexone for extendedrelease injectable
Spring 2007 Volume 6 Issue 1 ADVISORY News for the Treatment Field Naltrexone for Extended-Release Injectable Suspension for Treatment of Alcohol Dependence What is naltrexone for extendedrelease injectable
It is important that you tell your family and the people closest to you of this increased sensitivity to opioids and the risk of overdose.
 MEDICATION GUIDE VIVITROL (viv-i-trol) (naltrexone for extended-release injectable suspension) Read this Medication Guide before you start receiving VIVITROL injections and each time you receive an injection.
MEDICATION GUIDE VIVITROL (viv-i-trol) (naltrexone for extended-release injectable suspension) Read this Medication Guide before you start receiving VIVITROL injections and each time you receive an injection.
UCLA-SAPC Lecture Series March 13, 2015. Gary Tsai, M.D. Medical Director Substance Abuse Prevention and Control
 UCLA-SAPC Lecture Series March 13, 2015 Gary Tsai, M.D. Medical Director Substance Abuse Prevention and Control Neurobiology 101 Neuroscience of Addiction & Recovery Medication-Assisted Treatment (MAT)
UCLA-SAPC Lecture Series March 13, 2015 Gary Tsai, M.D. Medical Director Substance Abuse Prevention and Control Neurobiology 101 Neuroscience of Addiction & Recovery Medication-Assisted Treatment (MAT)
A G U I D E F O R U S E R S N a l t r e x o n e U
 A GUIDE FOR USERS UNaltrexone abstinence not using a particular drug; being drug-free. opioid antagonist a drug which blocks the effects of opioid drugs. dependence the drug has become central to a person
A GUIDE FOR USERS UNaltrexone abstinence not using a particular drug; being drug-free. opioid antagonist a drug which blocks the effects of opioid drugs. dependence the drug has become central to a person
Treatment of Opioid Addiction. Miriam Komaromy, MD Associate Director, Project ECHO University of New Mexico Health Sciences Center
 Treatment of Opioid Addiction Miriam Komaromy, MD Associate Director, Project ECHO University of New Mexico Health Sciences Center Why does the human brain become addicted? Why can we only become addicted
Treatment of Opioid Addiction Miriam Komaromy, MD Associate Director, Project ECHO University of New Mexico Health Sciences Center Why does the human brain become addicted? Why can we only become addicted
Medication Assisted Treatments for Opioid Dependence & Barriers to Implementation
 Medication Assisted Treatments for Opioid Dependence & Barriers to Implementation 9th Annual Midwest Conference on Problem Gambling and Substance Abuse Erin L. Winstanley, Ph.D. University of Cincinnati
Medication Assisted Treatments for Opioid Dependence & Barriers to Implementation 9th Annual Midwest Conference on Problem Gambling and Substance Abuse Erin L. Winstanley, Ph.D. University of Cincinnati
Use of Pharmacotherapies by Substance Abuse Treatment Facilities
 Use of Pharmacotherapies by Substance Abuse Treatment Facilities Cathie E. Alderks, PhD Substance Abuse and Mental Health Services Administration Department of Health and Human Services November 2007 1
Use of Pharmacotherapies by Substance Abuse Treatment Facilities Cathie E. Alderks, PhD Substance Abuse and Mental Health Services Administration Department of Health and Human Services November 2007 1
ARCHIVED BULLETIN. Product No. 2004-L0424-013 SEPTEMBER 2004 U. S. D E P A R T M E N T O F J U S T I C E
 BULLETIN INTELLIGENCE Product No. 2004-L0424-013 SEPTEMBER 2004 U. S. D E P A R T M E N T O F J U S T I C E NDIC Within the past 2 years buprenorphine a Schedule III drug has been made available for use
BULLETIN INTELLIGENCE Product No. 2004-L0424-013 SEPTEMBER 2004 U. S. D E P A R T M E N T O F J U S T I C E NDIC Within the past 2 years buprenorphine a Schedule III drug has been made available for use
Heroin. How Is Heroin Abused? How Does Heroin Affect the Brain? What Other Adverse Effects Does Heroin Have on Health?
 Heroin Heroin is an opiate drug that is synthesized from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears as a white or brown
Heroin Heroin is an opiate drug that is synthesized from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears as a white or brown
The CCB Science 2 Service Distance Learning Program
 S2S 2055 DETOXIFICATION Module 1 Post-Test 1. A common use of a biochemical marker is. a. to support or refute other information that leads to proper diagnosis b. for forensic purposes c. in detecting
S2S 2055 DETOXIFICATION Module 1 Post-Test 1. A common use of a biochemical marker is. a. to support or refute other information that leads to proper diagnosis b. for forensic purposes c. in detecting
ANCILLARY STABILIZATION AND WITHDRAWAL. The Why And How Of Stabilizing The Patient In A Comprehensive Treatment Setting
 ANCILLARY STABILIZATION AND WITHDRAWAL The Why And How Of Stabilizing The Patient In A Comprehensive Treatment Setting About CASAColumbia A science-based, multidisciplinary organization Focused on transforming
ANCILLARY STABILIZATION AND WITHDRAWAL The Why And How Of Stabilizing The Patient In A Comprehensive Treatment Setting About CASAColumbia A science-based, multidisciplinary organization Focused on transforming
Heroin. How Is Heroin Abused? How Does Heroin Affect the Brain? What Other Adverse Effects Does Heroin Have on Health?
 Heroin Heroin is an opiate drug that is synthesized from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears as a white or brown
Heroin Heroin is an opiate drug that is synthesized from morphine, a naturally occurring substance extracted from the seed pod of the Asian opium poppy plant. Heroin usually appears as a white or brown
Buprenorphine Treatment in Primary Care
 Buprenorphine Treatment in Primary Care Learning Collaborative Thursday March 13, 2:30 Amanda Risser MD MPH Assistant Professor OHSU Family Medicine OUTLINE Opiate addiction Opiate maintenance therapy
Buprenorphine Treatment in Primary Care Learning Collaborative Thursday March 13, 2:30 Amanda Risser MD MPH Assistant Professor OHSU Family Medicine OUTLINE Opiate addiction Opiate maintenance therapy