Charting the Future of Primary Care: Care Coordination/Case Management
|
|
|
- Cecil Summers
- 10 years ago
- Views:
Transcription
1 Charting the Future of Primary Care: Care Coordination/Case Management ASA-NYAM Forum March 19, 2009 Cheryl Schraeder, RN, PhD Director of Policy & Practice Initiatives Institute for Healthcare Innovation UIC College of Nursing

2 Overview of the Presentation Care Management Overview History Models Definitions Scope of Chronic Conditions Medicare Beneficiaries and Chronic Conditions MCCPRN Mission/Purpose Goals Issues for Ongoing Research

3 History of Care Management Early 1900s Public health nurses and social workers coordinated care through the Department of Public Health Mid 1900s US government hired practitioners to assist World War II soldiers with complex injuries Insurance companies employed nurses, social workers and vocational rehabilitation counselors to manage medical and worker compensation costs

4 History of Care Management Late 1900s Medicaid and Medicare demonstrations and community programs developed case management services for defined populations in the community (e.g., mentally ill, developmentally disabled, low income, frail elderly) Older Americans Act authorized case management for elders through Area Agencies on Aging across the U.S. Health insurers developed case management programs for the catastrophically ill or injured Acute care hospitals, home care agencies, rehabilitation facilities ies and skilled nursing facilities developed case management services

5 Models of Care Management Types Primary Care Case Management Medical/Social Case Management Private Case Management Nursing Case Management Models Hospital-Based/Acute Care Models Community-Based Models System Models Managed Care Models

6 Several Definitions of Care Management The Case Management Society of America (CMSA) states: Case management is a collaborative process of assessment, planning, facilitation and advocacy for options and services to meet an individual s s health needs through communication and available resources to promote quality cost-effective outcomes Source: Case Management Society of America, 2002, p. 5.

7 CCMC Definition of Care Management The Commission on Case Management Certification (CCMC) defines case management as follows: Case management is a collaborative process that assesses, plans, implements, coordinates, monitors, and evaluates the options and services required to meet the client's health and human service needs. It is characterized by advocacy, communication, and resource management and promotes quality and cost-effective interventions and outcomes. Source: CCMC, n.d. para 1

8 ANCC Defines Care Management The American Nurses Credentialing Center (ANCC) is the credentialing arm of the American Nurses Association. They state: Nurse case managers actively participate with their clients to identify i and facilitate options and services, providing and coordinating comprehensive care to meet patient/client health needs, with the goal of decreasing fragmentation and duplication of care, and enhancing ng quality, cost-effective clinical outcomes. Nursing case management is a dynamic and systematic collaborative approach to provide and coordinate health care services to a defined population. Nurse case c managers continually evaluate each individual s s health plan and specific challenges and then seek to overcome obstacles that affect outcomes. Source: ANCC (2008), para.. 1.

9 ANCC Definition, continued A A nurse case manager uses a framework that includes interaction, assessment, planning, implementation, and evaluation. Outcomes are evaluated to determine if additional actions such as reassessment or revision to a plan of care are required to meet client s s health needs. To facilitate patient outcomes, the nurse case manager may fulfill the roles of advocate, collaborator, facilitator, risk manager, educator, mentor, liaison, negotiator, consultant, coordinator, evaluator, and/or researcher. Source: ANCC 2008, para. 1

10 Number Of People With Chronic Conditions In 2000, 125 million Americans had one or more chronic conditions This number is projected to increase by more than one percent each year through 2030 Between 2000 and 2030, the number of Americans with chronic conditions will increase by 46 million people Source: (Anderson, 2007)

11 Chronic Conditions And Health Care Spending In 2004 Source: (Anderson, 2007)

12 The Impact Of Chronic Conditions On Individuals, Their Caregivers, And Physicians People with chronic conditions report not receiving adequate information More than half of people with serious chronic conditions have three or more different physicians People with serious chronic conditions believe they do not receive needed treatment People with serious chronic conditions have trouble accessing specific services Source: (Anderson, 2007)

13 The Impact Of Chronic Conditions On Individuals, Their Caregivers, And Physicians In treating patients with chronic conditions, physicians believe their training did not adequately prepare them to: Coordinate in-home and community services Educate patients with chronic conditions Manage the psychological and social aspects of chronic care Provide effective nutritional guidance Manage chronic pain Source: (Anderson, 2007)

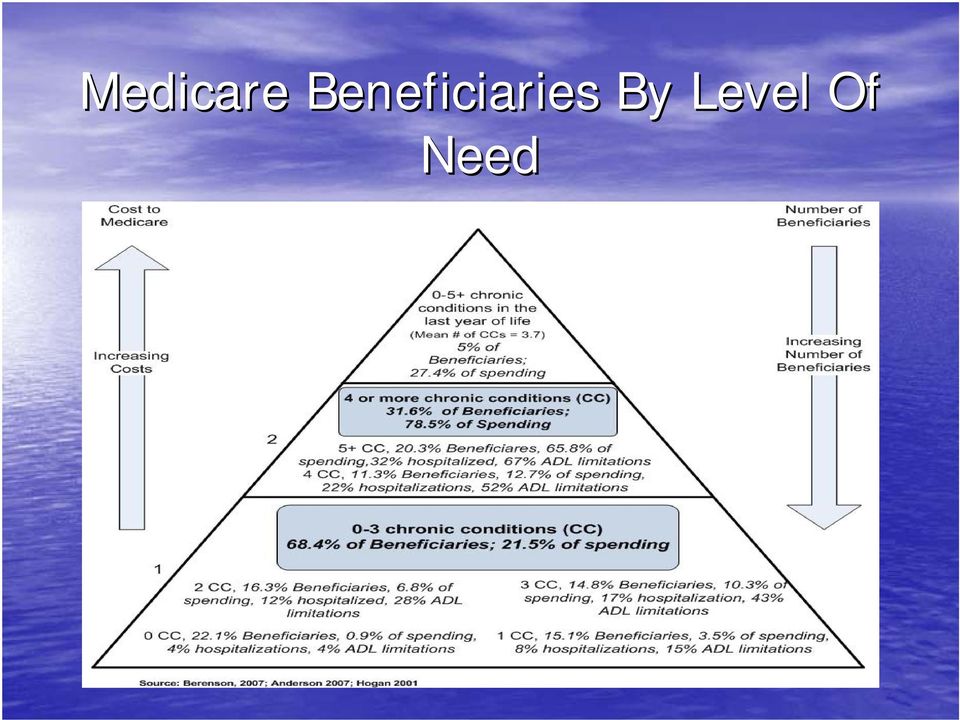
14 Problem Total Medicare spending was over $370 billion in 2006 (CBO, 2007), and is predicted to exceed $420 billion by % of high cost Medicare beneficiaries diagnosed with a major chronic condition (CBO, 2001) 70% of inpatient spending was for beneficiaries with a chronic condition
 70% of inpatient spending was for beneficiaries with a chronic")
15 Medicare Beneficiaries By Level Of Need
16 MCCPRN Network Members
17 Mission and Purpose Develop, execute and evaluate innovative, evidence-based chronic care initiatives focused on high cost, comorbid, fee-for forservice beneficiaries Serve as leading national resource to advance the science and operational standards of care management

18 Goals 1. To identify the most challenging and high cost (due to their complex, interacting chronic illnesses) Medicare beneficiaries; 2. To improve our understanding of which specific interventions and related operational process adjustments can achieve the greatest positive benefit at the lowest possible cost by efficiently researching, designing, implementing, testing and validating better ways to provide care management for these complex chronically ill Medicare beneficiaries;

19 Goals 3. To provide a reproducible, reliable and scalable framework to implement effective standardized care management services nationwide by continually updating best practice processes and guidelines for care of complex chronically ill Medicare beneficiaries; and 4. To implement a comprehensive and dynamic evaluation strategy by identifying new methods and metrics to quickly assess the impact of developments in care management components that have implications for current or future policy.

20 Issues for Ongoing Research What is the optimal target population Should there be episodic vs. continuous enrollment How should transitional care intervention be incorporated How do we provide care coordination as efficiently and effectively as possible What mix of medical care interventions and social service supports is most efficient What is the most effective staffing model What is the optimal caseload What financing mechanism should be put in place

21 Reference List Anderson, Gerard. (2007). Chronic conditions: Making the case for ongoing care. Baltimore, MD: Johns Hopkins University, Bloomberg School of Public Health. Berenson, R.A. The emerging challenge of chronic care. (2001). Retrieved March 4, 2009, from 20presentation.ppt. Hogan C., Lunney J., Gabel J., & Lynn J. (2001) Medicare beneficiaries costs of care in the last year of life. Health Affairs, 20(4),
What is Home Care Case Management?
 What is Home Care Case Management? Printed in USA Arcadia Home Care & Staffing www.arcadiahomecare.com Case Management: What is it why is it important? While different approaches to healthcare today are
What is Home Care Case Management? Printed in USA Arcadia Home Care & Staffing www.arcadiahomecare.com Case Management: What is it why is it important? While different approaches to healthcare today are
Long-Term Care --- an Essential Element of Healthcare Reform
 Long-Term Care --- an Essential Element of Healthcare Reform This chart book was commissioned by and prepared by Avalere Health. December 2008 Avalere Health LLC The intersection of business strategy and
Long-Term Care --- an Essential Element of Healthcare Reform This chart book was commissioned by and prepared by Avalere Health. December 2008 Avalere Health LLC The intersection of business strategy and
2014 Model of Care Training SHP_2014838A
 2014 Model of Care Training SHP_2014838A 1 Model of Care Training This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plans. It also ensures
2014 Model of Care Training SHP_2014838A 1 Model of Care Training This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plans. It also ensures
Care Coordination: Case managers connect the dots in new delivery models
 The Pathway to Certfication is CCMC IssueBrief VOLUME 1, ISSUE 2 Care Coordination: Case managers connect the dots in new delivery models Well before health reform was signed into law, new models for health
The Pathway to Certfication is CCMC IssueBrief VOLUME 1, ISSUE 2 Care Coordination: Case managers connect the dots in new delivery models Well before health reform was signed into law, new models for health
Economic and Financial Considerations in Health Policy. Gerard F. Anderson, PhD Johns Hopkins University
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Rehabilitation Nursing Criteria for Determination and Documentation of Medical Necessity in an Inpatient Rehabilitation Facility
 Rehabilitation Nursing Criteria for Determination and Documentation of Medical Necessity in an Inpatient Rehabilitation Facility An ARN Position Statement The objective of this Position Statement is to
Rehabilitation Nursing Criteria for Determination and Documentation of Medical Necessity in an Inpatient Rehabilitation Facility An ARN Position Statement The objective of this Position Statement is to
Coordination Debate. The Transitional Care and Comprehensive Care. Advances in medical science and technology,
 GENERATIONS Journal of the American Society on Aging By Patricia J. Volland, Cheryl Schraeder, Paul Shelton, and Ida Hess The Transitional Care and Comprehensive Care Coordination Debate Which approach
GENERATIONS Journal of the American Society on Aging By Patricia J. Volland, Cheryl Schraeder, Paul Shelton, and Ida Hess The Transitional Care and Comprehensive Care Coordination Debate Which approach
What is Geriatric Care Management?
 What is Geriatric Care Management? Printed in USA Arcadia Home Care & Staffing www.arcadiahomecare.com What is Geriatric Care Management and Why is it Important? As a health care service, geriatric care
What is Geriatric Care Management? Printed in USA Arcadia Home Care & Staffing www.arcadiahomecare.com What is Geriatric Care Management and Why is it Important? As a health care service, geriatric care
TREATMENT MODALITIES. May, 2013
 TREATMENT MODALITIES May, 2013 Treatment Modalities New York State Office of Alcoholism and Substance Abuse Services (NYS OASAS) regulates the addiction treatment modalities offered in New York State.
TREATMENT MODALITIES May, 2013 Treatment Modalities New York State Office of Alcoholism and Substance Abuse Services (NYS OASAS) regulates the addiction treatment modalities offered in New York State.
Standards of Practice & Scope of Services. for Health Care Delivery System Case Management and Transitions of Care (TOC) Professionals
 Professionals") A M E R I C A N C A S E M A N A G E M E N T A S S O C I A T I O N Standards of Practice & Scope of Services for Health Care Delivery System Case Management and Transitions of Care (TOC) Professionals O
A M E R I C A N C A S E M A N A G E M E N T A S S O C I A T I O N Standards of Practice & Scope of Services for Health Care Delivery System Case Management and Transitions of Care (TOC) Professionals O
Medicare: 2015 Model of Care Training 04/2015
 Medicare: 2015 Model of Care Training 04/2015 1 Model of Care Training This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plans. It also ensures
Medicare: 2015 Model of Care Training 04/2015 1 Model of Care Training This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plans. It also ensures
CCNC Care Management
 CCNC Care Management Community Care of North Carolina (CCNC) is a statewide population management and care coordination infrastructure founded on the primary care medical home model. CCNC incorporates
CCNC Care Management Community Care of North Carolina (CCNC) is a statewide population management and care coordination infrastructure founded on the primary care medical home model. CCNC incorporates
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 Page1 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify G.6 When to Notify G.11 Case Management Services G.14 Special Needs Services G.16 Health Management Programs
Page1 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify G.6 When to Notify G.11 Case Management Services G.14 Special Needs Services G.16 Health Management Programs
CHAPTER 535 HEALTH HOMES. Background... 2. Policy... 2. 535.1 Member Eligibility and Enrollment... 2. 535.2 Health Home Required Functions...
 TABLE OF CONTENTS SECTION PAGE NUMBER Background... 2 Policy... 2 535.1 Member Eligibility and Enrollment... 2 535.2 Health Home Required Functions... 3 535.3 Health Home Coordination Role... 4 535.4 Health
TABLE OF CONTENTS SECTION PAGE NUMBER Background... 2 Policy... 2 535.1 Member Eligibility and Enrollment... 2 535.2 Health Home Required Functions... 3 535.3 Health Home Coordination Role... 4 535.4 Health
The role of t he Depart ment of Veterans Affairs (VA) as
 as") The VA Health Care System: An Unrecognized National Safety Net Veterans who use the VA health care system have a higher level of illness than the general population, and 60 percent have no private or Medigap
The VA Health Care System: An Unrecognized National Safety Net Veterans who use the VA health care system have a higher level of illness than the general population, and 60 percent have no private or Medigap
Q: Rehabilitation Nursing
 Q: Rehabilitation Nursing Alberta Licensed Practical Nurses Competency Profile 163 Priority: One Competency: Q-1 Apply the Rehabilitation Process Q-1-1 Q-1-2 Q-1-3 Q-1-4 Q-1-5 Q-1-6 Demonstrate knowledge
Q: Rehabilitation Nursing Alberta Licensed Practical Nurses Competency Profile 163 Priority: One Competency: Q-1 Apply the Rehabilitation Process Q-1-1 Q-1-2 Q-1-3 Q-1-4 Q-1-5 Q-1-6 Demonstrate knowledge
A predictive analytics platform powered by non-medical staff reduces cost of care among high-utilizing Medicare fee-for-service beneficiaries
 A predictive analytics platform powered by non-medical staff reduces cost of care among high-utilizing Medicare fee-for-service beneficiaries Munevar D 1, Drozd E 1, & Ostrovsky A 2 1 Avalere Health, Inc.
A predictive analytics platform powered by non-medical staff reduces cost of care among high-utilizing Medicare fee-for-service beneficiaries Munevar D 1, Drozd E 1, & Ostrovsky A 2 1 Avalere Health, Inc.
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS. Karen Unholz, RN, BSN
 INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
INTRO TO THE MICHIGAN PIONEER ACO 101: THE BASICS Karen Unholz, RN, BSN Origins of the Accountable Care Organization ACOs originated from the Patient Protection and Affordable Care Act (Healthcare Reform)
Proposed Rule: Medicare Program; Medicare Shared Savings Program; Accountable Care Organizations (CMS-1461-P)
") Via online submission to http://www.regulations.gov February 6, 2015 Sylvia M. Burwell Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS 1461
Via online submission to http://www.regulations.gov February 6, 2015 Sylvia M. Burwell Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS 1461
Recommended Component: Provide a Full-Time Registered School Nurse All Day, Every Day, for Each School
 Recommended Component: Provide a Full-Time Registered School Nurse All Day, Every Day, for Each School Both the American Academy of Pediatrics (AAP) and the National Association of School Nurses (NASN)
Recommended Component: Provide a Full-Time Registered School Nurse All Day, Every Day, for Each School Both the American Academy of Pediatrics (AAP) and the National Association of School Nurses (NASN)
Department of Veterans Affairs VHA HANDBOOK 1140.3. Washington, DC 20420 August 16, 2004 HOME HEALTH AND HOSPICE CARE REIMBURSEMENT HANDBOOK
 Department of Veterans Affairs VHA HANDBOOK 1140.3 Veterans Health Administration Transmittal Sheet Washington, DC 20420 August 16, 2004 HOME HEALTH AND HOSPICE CARE REIMBURSEMENT HANDBOOK 1. REASON FOR
Department of Veterans Affairs VHA HANDBOOK 1140.3 Veterans Health Administration Transmittal Sheet Washington, DC 20420 August 16, 2004 HOME HEALTH AND HOSPICE CARE REIMBURSEMENT HANDBOOK 1. REASON FOR
Billing Frequently Asked Questions
 Billing Frequently Asked Questions What are the general conditions which must be met in order to bill for a service? All billed services except assessment must be medically necessary for the treatment
Billing Frequently Asked Questions What are the general conditions which must be met in order to bill for a service? All billed services except assessment must be medically necessary for the treatment
MODULE 11: Developing Care Management Support
 MODULE 11: Developing Care Management Support In this module, we will describe the essential role local care managers play in health care delivery improvement programs and review some of the tools and
MODULE 11: Developing Care Management Support In this module, we will describe the essential role local care managers play in health care delivery improvement programs and review some of the tools and
School Nurse Section - Introduction
 School Nurse Section - Introduction The Role of the Credentialed School Nurse Role of the Credentialed School Nurse The California School Nurses Organization (CSNO) position statement: The California School
School Nurse Section - Introduction The Role of the Credentialed School Nurse Role of the Credentialed School Nurse The California School Nurses Organization (CSNO) position statement: The California School
Nursing Home to Community Program: A Discharge Planning Manual
 Nursing Home to Community Program: A Discharge Planning Manual March 2006 Portions of this Manual may be cited on condition that proper credit is given to: Broome County Community Alternative Systems Agency
Nursing Home to Community Program: A Discharge Planning Manual March 2006 Portions of this Manual may be cited on condition that proper credit is given to: Broome County Community Alternative Systems Agency
Maryland Data as of July 2003. Mental Health and Substance Abuse Services in Medicaid and SCHIP in Maryland
 Mental Health and Substance Abuse Services in Medicaid and SCHIP in Maryland As of July 2003, 638,662 people were covered under Maryland's Medicaid/SCHIP programs. There were 525,080 enrolled in the Medicaid
Mental Health and Substance Abuse Services in Medicaid and SCHIP in Maryland As of July 2003, 638,662 people were covered under Maryland's Medicaid/SCHIP programs. There were 525,080 enrolled in the Medicaid
Associate Chief Financial Officer Commonwealth Care Alliance Boston, MA
 Associate Chief Financial Officer Commonwealth Care Alliance Boston, MA Position Specification July 2014 The Summary Commonwealth Care Alliance is seeking an Associate Chief Financial Officer (ACFO) for
Associate Chief Financial Officer Commonwealth Care Alliance Boston, MA Position Specification July 2014 The Summary Commonwealth Care Alliance is seeking an Associate Chief Financial Officer (ACFO) for
The Collaborative Models of Mental Health Care for Older Iowans. Model Administration. Collaborative Models of Mental Health Care for Older Iowans 97
 6 The Collaborative Models of Mental Health Care for Older Iowans Model Administration Collaborative Models of Mental Health Care for Older Iowans 97 Collaborative Models of Mental Health Care for Older
6 The Collaborative Models of Mental Health Care for Older Iowans Model Administration Collaborative Models of Mental Health Care for Older Iowans 97 Collaborative Models of Mental Health Care for Older
Brain Injury Association of New Jersey
 Brain Injury Association of New Jersey 825 Georges Road, 2nd Floor North Brunswick, NJ 08902 Phone: 732-745-0200 Helpline: 1-800-669-4323 Website: www.bianj.org E-mail: [email protected] SOURCES OF FUNDING
Brain Injury Association of New Jersey 825 Georges Road, 2nd Floor North Brunswick, NJ 08902 Phone: 732-745-0200 Helpline: 1-800-669-4323 Website: www.bianj.org E-mail: [email protected] SOURCES OF FUNDING
CASE MANAGEMENT F R O M A C U T E C A R E T O T H E C O M M U N I T Y A C R O S S T H E C O N T I N U U M O F C A R E
 CASE MANAGEMENT F R O M A C U T E C A R E T O T H E C O M M U N I T Y A C R O S S T H E C O N T I N U U M O F C A R E CASE MANAGEMENT Case Management is a collaborative process of assessment, planning,
CASE MANAGEMENT F R O M A C U T E C A R E T O T H E C O M M U N I T Y A C R O S S T H E C O N T I N U U M O F C A R E CASE MANAGEMENT Case Management is a collaborative process of assessment, planning,
How To Help Veterans With A Mental Health Diagnosis
 RIGHT CARE RIGHT TIME RIGHT PLACE DEBORAH HARRIS-COBBINAH RN, MSN, CNS, NP, BC Faculty Disclosure Deborah Harris-Cobbinah, MSN, ANP,MHCNS,BC Conflict of Interest: None Employer: Dept. of Veterans Affairs
RIGHT CARE RIGHT TIME RIGHT PLACE DEBORAH HARRIS-COBBINAH RN, MSN, CNS, NP, BC Faculty Disclosure Deborah Harris-Cobbinah, MSN, ANP,MHCNS,BC Conflict of Interest: None Employer: Dept. of Veterans Affairs
Patient Protection and Affordable Care Act [PL 111-148] with Amendments from 2010 Reconciliation Act [PL 111-152] Direct-Care Workforce
![Patient Protection and Affordable Care Act [PL 111-148] with Amendments from 2010 Reconciliation Act [PL 111-152] Direct-Care Workforce](/thumbs/25/6872632.jpg "Patient Protection and Affordable Care Act [PL 111-148] with Amendments from 2010 Reconciliation Act [PL 111-152] Direct-Care Workforce") DIRECT-CARE WORKFORCE AND LONG-TERM CARE PROVISIONS AS ENACTED IN PATIENT PROTECTION AND AFFORDABLE CARE ACT AND HEALTH CARE AND EDUCATION RECONCILIATION ACT OF 2010 Key Provisions Direct-Care Workforce
DIRECT-CARE WORKFORCE AND LONG-TERM CARE PROVISIONS AS ENACTED IN PATIENT PROTECTION AND AFFORDABLE CARE ACT AND HEALTH CARE AND EDUCATION RECONCILIATION ACT OF 2010 Key Provisions Direct-Care Workforce
How To Be A Nurse Practitioner
 NURSE PRACTITIONER PROGRAM THE PENNSYLVANIA STATE UNIVERSITY College of Nursing Preceptor Evaluation of Student Clinical Performance: Adult Gerontology Acute Care Nurse Practitioner Option Nursing 863
NURSE PRACTITIONER PROGRAM THE PENNSYLVANIA STATE UNIVERSITY College of Nursing Preceptor Evaluation of Student Clinical Performance: Adult Gerontology Acute Care Nurse Practitioner Option Nursing 863
Arkansas Behavioral Health Home State Plan Amendment. Draft - 03/11/14
 Arkansas Behavioral Health Home State Plan Amendment Draft - 03/11/14 NOTE: Bolded text within document denotes required health home language by the Centers for Medicare and Medicaid Services (CMS) with
Arkansas Behavioral Health Home State Plan Amendment Draft - 03/11/14 NOTE: Bolded text within document denotes required health home language by the Centers for Medicare and Medicaid Services (CMS) with
Health Information Exchange of Post Acute Care Providers
 April 21, 2013 Ms. Marilyn Tavenner Acting Administrator, Chief Operating Officer Centers for Medicare and Medicaid Services Department of Health and Human Services 7500 Security Boulevard Baltimore, MD
April 21, 2013 Ms. Marilyn Tavenner Acting Administrator, Chief Operating Officer Centers for Medicare and Medicaid Services Department of Health and Human Services 7500 Security Boulevard Baltimore, MD
Federal Recovery Coordination Program. Karen Guice, MD, MPP Executive Director
 Federal Recovery Coordination Program Karen Guice, MD, MPP Executive Director CONCEPT The President s Commission on Care for America s Returning Wounded Warriors Immediately create comprehensive patient-centered
Federal Recovery Coordination Program Karen Guice, MD, MPP Executive Director CONCEPT The President s Commission on Care for America s Returning Wounded Warriors Immediately create comprehensive patient-centered
Subacute Inpatient MH - Adult
 Subacute Inpatient MH - Adult Definition Subacute Inpatient hospital psychiatric services are medically necessary short-term psychiatric services provided to a client with a primary psychiatric diagnosis
Subacute Inpatient MH - Adult Definition Subacute Inpatient hospital psychiatric services are medically necessary short-term psychiatric services provided to a client with a primary psychiatric diagnosis
Parkview Health s Population Health Journey
 Parkview Health s Population Health Journey Susan McAlister DNP, RN Director Enterprise Care Management Christine Howell BSN, RN Community Based Registered Nurse Objectives: By the completion of the webinar
Parkview Health s Population Health Journey Susan McAlister DNP, RN Director Enterprise Care Management Christine Howell BSN, RN Community Based Registered Nurse Objectives: By the completion of the webinar
Community and Social Services
 Developing a path to employment for New Yorkers with disabilities Community and Social Services Mental Health and Substance Abuse Social Workers... 1 Health Educators... 4 Substance Abuse and Behavioral
Developing a path to employment for New Yorkers with disabilities Community and Social Services Mental Health and Substance Abuse Social Workers... 1 Health Educators... 4 Substance Abuse and Behavioral
Master of Science in Nursing. Academic Programs of Study 2015 2016 MSN
 Master of Science in Academic Programs of Study 2015 2016 MSN TABLE OF CONTENTS 1) ACCREDITATION AND EDUCATIONAL OUTCOMES 3 2) REGISTRATION AND ADVISING 3) COURSE LOAD See Policies 4) CLINICAL EXPERIENCES
Master of Science in Academic Programs of Study 2015 2016 MSN TABLE OF CONTENTS 1) ACCREDITATION AND EDUCATIONAL OUTCOMES 3 2) REGISTRATION AND ADVISING 3) COURSE LOAD See Policies 4) CLINICAL EXPERIENCES
Case Management Model Act Supporting Case Management Programs
 Case Management Model Act Supporting Case Management Programs P a g e 0 The leading membership association providing professional collaboration across the health care continuum. Case Management Model Act
Case Management Model Act Supporting Case Management Programs P a g e 0 The leading membership association providing professional collaboration across the health care continuum. Case Management Model Act
Outstanding Outcomes
 Outstanding Outcomes New study reaffirms s industry leading clinical results and long-term savings for catastrophic claims Catastrophic injuries are infrequent, highly complex, and extremely volatile,
Outstanding Outcomes New study reaffirms s industry leading clinical results and long-term savings for catastrophic claims Catastrophic injuries are infrequent, highly complex, and extremely volatile,
Cheryl Schraeder, RN, PhD, FAAN. The demographic landscape of America is changing at an accelerated pace
 Stepping up to the challenge: Changing the way we deliver care Cheryl Schraeder, RN, PhD, FAAN 1 Goals of Presentation To Identify: The key challenges in delivering evidence-based & cost-effective care
Stepping up to the challenge: Changing the way we deliver care Cheryl Schraeder, RN, PhD, FAAN 1 Goals of Presentation To Identify: The key challenges in delivering evidence-based & cost-effective care
Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases
 Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases Epidemiology Over 145 million people ( nearly half the population) - suffer from asthma, depression and other chronic
Johns Hopkins HealthCare LLC: Care Management and Care Coordination for Chronic Diseases Epidemiology Over 145 million people ( nearly half the population) - suffer from asthma, depression and other chronic
Transforming Care for Medicare Beneficiaries with Chronic Conditions and Long-Term Care Needs: Coordinating Care Across All Services
 Transforming Care for Medicare Beneficiaries with Chronic Conditions and Long-Term Care Needs: Coordinating Care Across All Services Harriet L. Komisar and Judy Feder Georgetown University October 2011
Transforming Care for Medicare Beneficiaries with Chronic Conditions and Long-Term Care Needs: Coordinating Care Across All Services Harriet L. Komisar and Judy Feder Georgetown University October 2011
Maryland Medicaid Program. Aaron Larrimore Medicaid Department of Health and Mental Hygiene May 15, 2012
 Maryland Medicaid Program Aaron Larrimore Medicaid Department of Health and Mental Hygiene May 15, 2012 1 Maryland Medicaid In Maryland, Medicaid is also called Medical Assistance or MA. MA is a joint
Maryland Medicaid Program Aaron Larrimore Medicaid Department of Health and Mental Hygiene May 15, 2012 1 Maryland Medicaid In Maryland, Medicaid is also called Medical Assistance or MA. MA is a joint
Scope and Standards of Practice for The Acute Care Nurse Practitioner. American Association of Critical-Care Nurses
 Scope and Standards of Practice for The Acute Care Nurse Practitioner American Association of Critical-Care Nurses Editor: Linda Bell, RN MSN Copy Editor: Anne Bernard Designer: Derek Bennett An AACN Critical
Scope and Standards of Practice for The Acute Care Nurse Practitioner American Association of Critical-Care Nurses Editor: Linda Bell, RN MSN Copy Editor: Anne Bernard Designer: Derek Bennett An AACN Critical
AMERICAN BURN ASSOCIATION BURN CENTER VERIFICATION REVIEW PROGRAM Verificatoin Criterea EFFECTIVE JANUARY 1, 2015. Criterion. Level (1 or 2) Number
 Number") Criterion AMERICAN BURN ASSOCIATION BURN CENTER VERIFICATION REVIEW PROGRAM Criterion Level (1 or 2) Number Criterion BURN CENTER ADMINISTRATION 1. The burn center hospital is currently accredited by The
Criterion AMERICAN BURN ASSOCIATION BURN CENTER VERIFICATION REVIEW PROGRAM Criterion Level (1 or 2) Number Criterion BURN CENTER ADMINISTRATION 1. The burn center hospital is currently accredited by The
Identifying High-Risk Medicare Beneficiaries with Predictive Analytics
 Identifying High-Risk Medicare Beneficiaries with Predictive Analytics September 2014 Until recently, with the passage of the Affordable Care Act (ACA), Medicare Fee-for-Service (FFS) providers had little
Identifying High-Risk Medicare Beneficiaries with Predictive Analytics September 2014 Until recently, with the passage of the Affordable Care Act (ACA), Medicare Fee-for-Service (FFS) providers had little
Presented to: Long Term Care Workgroup May 26, 2011
 Presented to: Long Term Care Workgroup May 26, 2011 Partners in the Grant SC Department of Health and Human Services Sam Waldrep Roy Smith Project Coordinator Office of Research and Statistics Institute
Presented to: Long Term Care Workgroup May 26, 2011 Partners in the Grant SC Department of Health and Human Services Sam Waldrep Roy Smith Project Coordinator Office of Research and Statistics Institute
2.b.vii Implementing the INTERACT Project (Inpatient Transfer Avoidance Program for SNF)
") 2.b.vii Implementing the INTERACT Project (Inpatient Transfer Avoidance Program for SNF) Project Objective: Skilled nursing facilities (SNFs) will implement the evidence based INTERACT program developed
2.b.vii Implementing the INTERACT Project (Inpatient Transfer Avoidance Program for SNF) Project Objective: Skilled nursing facilities (SNFs) will implement the evidence based INTERACT program developed
Connecting the Dots: Understanding the relationship between Case Management and Nurse Life Care Planning
 Connecting the Dots: Understanding the relationship between Case Management and Nurse Life Care Planning Host: AANLCP Presenters: Becky Czarnik, Shelene Giles, Victoria Powell & Carrie Thomas Facilitator:
Connecting the Dots: Understanding the relationship between Case Management and Nurse Life Care Planning Host: AANLCP Presenters: Becky Czarnik, Shelene Giles, Victoria Powell & Carrie Thomas Facilitator:
other caregivers. A beneficiary may receive one diagnostic assessment per year without any additional authorization.
 4.b.(8) Diagnostic, Screening, Treatment, Preventive and Rehabilitative Services (continued) Attachment 3.1-A.1 Page 7c.2 (a) Psychotherapy Services: For the complete description of the service providers,
4.b.(8) Diagnostic, Screening, Treatment, Preventive and Rehabilitative Services (continued) Attachment 3.1-A.1 Page 7c.2 (a) Psychotherapy Services: For the complete description of the service providers,
Optum By United Behavioral Health. 2015 Mississippi Coordinated Access Network (CAN) Medicaid Level of Care Guidelines
 Medicaid Level of Care Guidelines") Optum By United Behavioral Health 2015 Mississippi Coordinated Access Network (CAN) Medicaid Level of Care Guidelines Assertive Community Treatment is a multi-disciplinary, selfcontained clinical team
Optum By United Behavioral Health 2015 Mississippi Coordinated Access Network (CAN) Medicaid Level of Care Guidelines Assertive Community Treatment is a multi-disciplinary, selfcontained clinical team
Administrative Code. Title 23: Medicaid Part 205 Hospice Services
 Title 23: Medicaid Administrative Code Title 23: Medicaid Part 205 Hospice Services Table of Contents Table of Contents Title 23: Division of Medicaid... 1 Part 205: Hospice Services... 1 Part 205 Chapter
Title 23: Medicaid Administrative Code Title 23: Medicaid Part 205 Hospice Services Table of Contents Table of Contents Title 23: Division of Medicaid... 1 Part 205: Hospice Services... 1 Part 205 Chapter
How did the IL Movement get started? What is Independent Living (IL)? Independent Living, CILs & ADRC
? Independent Living, CILs & ADRC") Aging and Disability Resource Center ADRC (Aging and Disability Resource Connection in Oregon) Independent Living, CILs & ADRC A Beginning Discussion Presented by Deb McCuin, State Unit on Aging What is
Aging and Disability Resource Center ADRC (Aging and Disability Resource Connection in Oregon) Independent Living, CILs & ADRC A Beginning Discussion Presented by Deb McCuin, State Unit on Aging What is
Appendix VI. Patient-Centered Medical Homes (Initiative Memorandum) APRIL 2013
 APRIL 2013") Appendix VI. Patient-Centered Medical Homes (Initiative Memorandum) APRIL 2013 http://berkeleyhealthcareforum.berkeley.edu 1 Appendix VI. Patient-Centered Medical Homes (Initiative Memorandum) See Appendix
Appendix VI. Patient-Centered Medical Homes (Initiative Memorandum) APRIL 2013 http://berkeleyhealthcareforum.berkeley.edu 1 Appendix VI. Patient-Centered Medical Homes (Initiative Memorandum) See Appendix
Kaiser Permanente Southern California Depression Care Program
 Kaiser Permanente Southern California Depression Care Program Abstract In 2001, Kaiser Permanente of Southern California (KPSC) adopted the IMPACT model of collaborative care for depression, developed
Kaiser Permanente Southern California Depression Care Program Abstract In 2001, Kaiser Permanente of Southern California (KPSC) adopted the IMPACT model of collaborative care for depression, developed
Opportunities for Home Care Providers in Working with Medical Homes October 2014. EMHS Vice President Continuum of Care Chief Advocacy Officer
 How to Establish Partnerships and Opportunities for Home Care Providers in Working with Medical Homes October 2014 Lisa Harvey-McPherson, RN, MBA, MPPM EMHS Vice President Continuum of Care Chief Advocacy
How to Establish Partnerships and Opportunities for Home Care Providers in Working with Medical Homes October 2014 Lisa Harvey-McPherson, RN, MBA, MPPM EMHS Vice President Continuum of Care Chief Advocacy
Establishing an Advanced Illness Management (AIM) Model in a Community-Based Setting
 Model in a Community-Based Setting") Establishing an Advanced Illness Management (AIM) Model in a Community-Based Setting Health Care Workforce for Older Americans: Promoting Team Care October 7, 2008 Panel on Models of Team Care for the
Establishing an Advanced Illness Management (AIM) Model in a Community-Based Setting Health Care Workforce for Older Americans: Promoting Team Care October 7, 2008 Panel on Models of Team Care for the
Montefiore s Population Health Management Services. October 23, 2015
 Montefiore s Population Health Management Services October 23, 2015 Integrated Delivery System Our Locations 3,092 Acute Beds Across 10 Hospitals Including 132 beds at the Children s Hospital at Montefiore
Montefiore s Population Health Management Services October 23, 2015 Integrated Delivery System Our Locations 3,092 Acute Beds Across 10 Hospitals Including 132 beds at the Children s Hospital at Montefiore
ACCOUNTABLE CARE ORGANIZATIONS. Staff Attorney Legislative Council Service August 17, 2011
 ACCOUNTABLE CARE ORGANIZATIONS OVERVIEW Michael Hely Staff Attorney Legislative Council Service August 17, 2011 What is an Accountable Care Organization (ACO)? No set definition. National Conference of
ACCOUNTABLE CARE ORGANIZATIONS OVERVIEW Michael Hely Staff Attorney Legislative Council Service August 17, 2011 What is an Accountable Care Organization (ACO)? No set definition. National Conference of
Toward Meaningful Use of HIT
 Toward Meaningful Use of HIT Fred D Rachman, MD Health and Medicine Policy Research Group HIE Forum March 24, 2010 Why are we talking about technology? To improve the quality of the care we provide and
Toward Meaningful Use of HIT Fred D Rachman, MD Health and Medicine Policy Research Group HIE Forum March 24, 2010 Why are we talking about technology? To improve the quality of the care we provide and
Optum By United Behavioral Health. 2015 Florida Medicaid Managed Medical Assistance (MMA) Level of Care Guidelines
 Level of Care Guidelines") Optum By United Behavioral Health 2015 Florida Medicaid Managed Medical Assistance (MMA) Level of Care Guidelines Statewide Inpatient Psychiatric Program Services (SIPP) Statewide Inpatient Psychiatric
Optum By United Behavioral Health 2015 Florida Medicaid Managed Medical Assistance (MMA) Level of Care Guidelines Statewide Inpatient Psychiatric Program Services (SIPP) Statewide Inpatient Psychiatric
UW MEDICINE PATIENT EDUCATION. Your Care Team. Helpful information
 UW MEDICINE PATIENT EDUCATION Your Care Team Helpful information In this section: You: The Patient Medical Staff Nursing Staff Allied Health Professionals Support Staff Peer Mentors for People with Spinal
UW MEDICINE PATIENT EDUCATION Your Care Team Helpful information In this section: You: The Patient Medical Staff Nursing Staff Allied Health Professionals Support Staff Peer Mentors for People with Spinal
GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services
 GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services Aged, Blind and Disabled Stakeholder Presentation Indiana Family and Social Services Administration August
GRACE Team Care Integration of Primary Care with Geriatrics and Community-Based Social Services Aged, Blind and Disabled Stakeholder Presentation Indiana Family and Social Services Administration August
Expanding Telemedicine Services in an Effort to Reduce Health Care Costs in the United States
 Expanding Telemedicine Services in an Effort to Reduce Health Care Costs in the United States To: Federal Trade Commission From: Jaime Coffino, MPH Candidate, Mailman School of Public Health, Columbia
Expanding Telemedicine Services in an Effort to Reduce Health Care Costs in the United States To: Federal Trade Commission From: Jaime Coffino, MPH Candidate, Mailman School of Public Health, Columbia
Defining the Role of Nurse Assessment Coordinators: Beyond Paperwork and Reimbursement
 Defining the Role of Nurse Assessment Coordinators: Beyond Paperwork and Reimbursement Copyright 2011, AANAC. All Rights Reserved. 1 Defining the Role of Nurse Assessment Coordinators: Beyond Paperwork
Defining the Role of Nurse Assessment Coordinators: Beyond Paperwork and Reimbursement Copyright 2011, AANAC. All Rights Reserved. 1 Defining the Role of Nurse Assessment Coordinators: Beyond Paperwork
Homecare Health & Medical Billing Data Science Study
 Combining Traditional Statistical Methods with Data Mining Techniques for Predictive Modeling of Homecare Outcomes Bonnie L. Westra, PhD, RN, Assistant Professor University of Minnesota, School of Nursing
Combining Traditional Statistical Methods with Data Mining Techniques for Predictive Modeling of Homecare Outcomes Bonnie L. Westra, PhD, RN, Assistant Professor University of Minnesota, School of Nursing
4. Program Regulations
 Table of Contents iv 437.401: Introduction... 4-1 437.402: Definitions... 4-1 437.403: Eligible Members... 4-2 437.404: Provider Eligibility... 4-3 437.405: Out-of-State Hospice Services... 4-3 437.406:
Table of Contents iv 437.401: Introduction... 4-1 437.402: Definitions... 4-1 437.403: Eligible Members... 4-2 437.404: Provider Eligibility... 4-3 437.405: Out-of-State Hospice Services... 4-3 437.406:
MEDICAL DIRECTOR: ROLE AND RESPONSIBILITIES AS LEADER AND MANAGER
 MEDICAL DIRECTOR: ROLE AND RESPONSIBILITIES AS LEADER AND MANAGER FUNCTIONS AND ASSOCIATED TASKS Function 1 - Administrative The medical director participates in administrative decision making and recommends
MEDICAL DIRECTOR: ROLE AND RESPONSIBILITIES AS LEADER AND MANAGER FUNCTIONS AND ASSOCIATED TASKS Function 1 - Administrative The medical director participates in administrative decision making and recommends
Licensed Mental Health Counselors and the Military Health System
 Licensed Mental Health Counselors and the Military Health System LT Rick Schobitz, Ph.D., USPHS Deputy Director, Behavioral Medicine Division Office of the Chief Medical Officer TRICARE Management Activity
Licensed Mental Health Counselors and the Military Health System LT Rick Schobitz, Ph.D., USPHS Deputy Director, Behavioral Medicine Division Office of the Chief Medical Officer TRICARE Management Activity
Early and Periodic Screening, Diagnosis, and Treatment (EPSDT) Current Approved State Plan Language
 Current Approved State Plan Language") Early and Periodic Screening, Diagnosis, and Treatment (EPSDT) Current Approved State Plan Language Limitations on Attachment 3.1-A Page 9 Type of Service Covered for Medi-Cal eligibles under 21 years
Early and Periodic Screening, Diagnosis, and Treatment (EPSDT) Current Approved State Plan Language Limitations on Attachment 3.1-A Page 9 Type of Service Covered for Medi-Cal eligibles under 21 years
CMS Innovation Center Improving Care for Complex Patients
 CMS Innovation Center Improving Care for Complex Patients ECRI Institute Dr. Patrick Conway, M.D., MSc CMS Chief Medical Officer and Deputy Administrator for Innovation and Quality Director, Center for
CMS Innovation Center Improving Care for Complex Patients ECRI Institute Dr. Patrick Conway, M.D., MSc CMS Chief Medical Officer and Deputy Administrator for Innovation and Quality Director, Center for
Quantifying the ROI of Population Health Solutions March 1, 2016
 Quantifying the ROI of Population Health Solutions March 1, 2016 Curt Magnuson, Principal, The FiscalHealth Group Michael S. Wilson, Principal, The FiscalHealth Group Conflict of Interest Curt Magnuson,
Quantifying the ROI of Population Health Solutions March 1, 2016 Curt Magnuson, Principal, The FiscalHealth Group Michael S. Wilson, Principal, The FiscalHealth Group Conflict of Interest Curt Magnuson,
What Providers Need To Know Before Adopting Bundling Payments
 What Providers Need To Know Before Adopting Bundling Payments Dan Mirakhor Master of Health Administration University of Southern California Dan Mirakhor is a Master of Health Administration student at
What Providers Need To Know Before Adopting Bundling Payments Dan Mirakhor Master of Health Administration University of Southern California Dan Mirakhor is a Master of Health Administration student at
Oncology Competency- Pain, Palliative Care, and Hospice Care
 Pain, Palliative Care, and Hospice Care Palliative medicine relieves suffering and improves the quality of life for patients with advanced illness. The goal is achievement of the best quality of life for
Pain, Palliative Care, and Hospice Care Palliative medicine relieves suffering and improves the quality of life for patients with advanced illness. The goal is achievement of the best quality of life for
Brain Injury Alliance of New Jersey
 Understanding the Rehabilitation Process after No one can prepare a family for the trauma of experiencing brain injury. Following the injury the subsequent move from the hospital to various rehabilitation
Understanding the Rehabilitation Process after No one can prepare a family for the trauma of experiencing brain injury. Following the injury the subsequent move from the hospital to various rehabilitation
OREGON CASCADES WEST SENIOR & DISABILITY SERVICES
 OREGON CASCADES WEST SENIOR & DISABILITY SERVICES DIRECTORY OF SERVICES for Linn, Benton & Lincoln Counties 1 WHERE CAN YOU TURN FOR ANSWERS TO YOUR QUESTIONS ABOUT AGING OR DISABILITY? Oregon Cascades
OREGON CASCADES WEST SENIOR & DISABILITY SERVICES DIRECTORY OF SERVICES for Linn, Benton & Lincoln Counties 1 WHERE CAN YOU TURN FOR ANSWERS TO YOUR QUESTIONS ABOUT AGING OR DISABILITY? Oregon Cascades